
Submitted:
19 May 2025
Posted:
20 May 2025
You are already at the latest version
Abstract
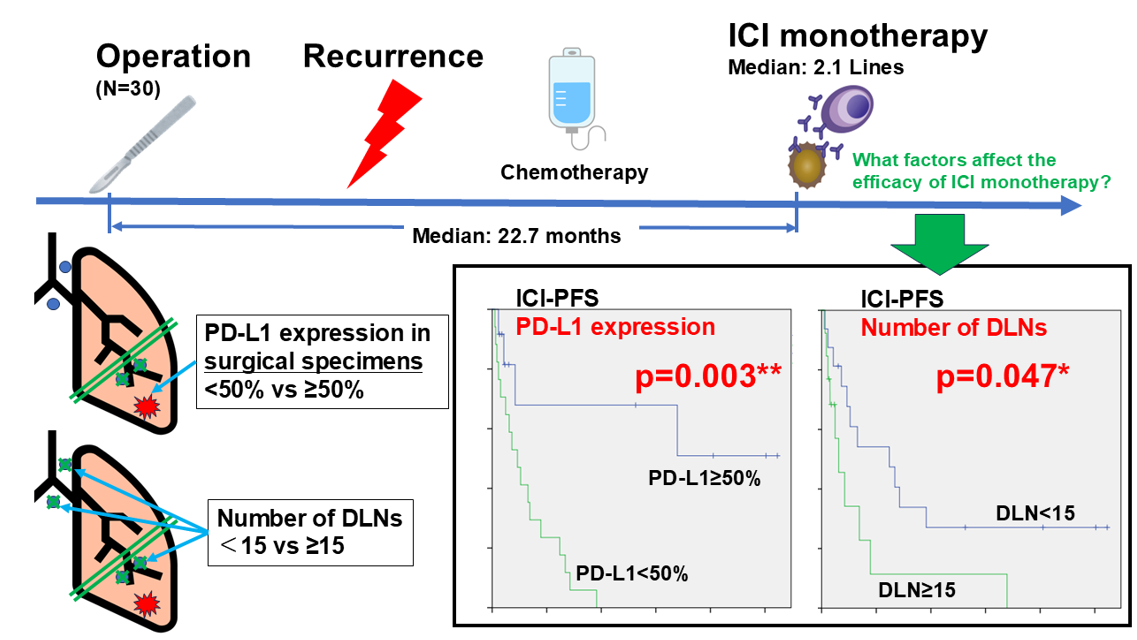
Background: Immune checkpoint inhibitors (ICIs) have emerged as a standard treatment for recurrent non-small cell lung cancer (NSCLC). However, the predictive factors for their efficacy in postoperative recurrence remain unclear. Methods: We retrospectively analyzed 30 patients who underwent complete surgical resection of NSCLC and subsequently received ICI monotherapy for recurrence. Clinicopathological factors, including the programmed death ligand 1 (PD-L1) expression and number of dissected lymph nodes (DLNs), were evaluated for their association with the treatment response and prognosis. Results: The high expression of PD-L1 (≥50%) in surgical specimens was significantly associated with higher response rates, prolonged progression-free survival (PFS), and overall survival (OS) after the initiation of ICI therapy. In contrast, patients with ≥15 DLNs had a significantly shorter PFS than those with < 15 DLNs, particularly in patients without extrathoracic recurrence. A multivariate analysis identified the expression of PD-L1, the number of DLNs, and the presence of extrathoracic metastasis as independent prognostic factors for ICI-PFS. Conclusion: Extensive lymphadenectomy may worsen the prognostic outcomes of ICI monotherapy, possibly by impairing tumor-draining lymph node-mediated immunity. These findings highlight the importance of lymphatic preservation and support the clinical rationale for neoadjuvant ICI therapy for resectable NSCLC.
Keywords:
non-small cell lung cancer
; immune checkpoint inhibitor
; lymph node dissection
; tumor-draining lymph node
; recurrence
; neoadjuvant therapy
; PD-L1 expression
1. Introduction
Non-small cell lung cancer (NSCLC) is one of the most aggressive malignancies, accounting for the majority of cancer-related deaths worldwide [1]. Despite complete resection, approximately half of stage II and two-thirds of stage III patients experience recurrence, and the prognosis is poor [2]. There is an urgent need to develop more curative treatment strategies for both patients with metastatic NSCLC and those with recurrent NSCLC.
Immune checkpoint inhibitors (ICIs) have been used in the treatment of NSCLC, starting with a clinical trial of nivolumab for unresectable squamous cell carcinoma and non-squamous cell carcinoma in 2015 [3,4]. Since then, several clinical trials have been conducted on the combination of ICIs and chemotherapy for unresectable NSCLC [5,6,7,8,9], and this systemic therapy is currently used as the first-line treatment for patients with unresectable NSCLC with negative driver gene mutations.
Recently, the perioperative treatment of resectable NSCLC has attracted attention. Currently, atezolizumab as adjuvant therapy after chemotherapy [10], neoadjuvant nivolumab and chemotherapy combination therapy [11], and neoadjuvant pembrolizumab and chemotherapy combination therapy followed by surgery and adjuvant pembrolizumab therapy are being used in clinical practice [12]. Several clinical trials are currently ongoing for the treatment of ICIs before and after surgery [13,14,15]. While neoadjuvant ICI therapy is expected to achieve the early control of micrometastases throughout the body [16], there is also the issue that a certain number of patients become inoperable due to progression during ICI treatment, and this remains a controversial issue.
The expression of programmed death-ligand 1 (PD-L1) is frequently used as a predictor of the efficacy of ICIs for unresectable NSCLC [17]. On the other hand, although there are some reports on predictors of the efficacy of ICIs for postoperative recurrence [18,19,20], these have not yet been fully elucidated. In this study, we analyzed various clinicopathological factors in patients treated with ICI monotherapy for recurrence after complete resection of NSCLC and clarified the factors that influenced the efficacy of ICI. Furthermore, we discuss the significance of neoadjuvant ICI treatment based on the results obtained.
2. Materials and Methods
2.1. Patient Selection
Thirty patients who underwent complete resection for NSCLC at the Department of Thoracic Surgery, Kagoshima University Hospital and received ICI monotherapy at any line of treatment for postoperative recurrence between January 2017 and December 2021 were included. We investigated whether clinicopathological factors, including those at the time of surgery, are related to the efficacy and prognosis of ICI monotherapy. Patients with known driver gene mutations and those who underwent radiotherapy before ICI therapy were excluded.
2.2. Data Collection and Ethical Approval
Patient clinicopathological information was retrospectively obtained through a review of medical records. This study was approved by the Ethics Committee of Kagoshima University Graduate School of Medicine and Dentistry (Approval No. 220178epi) and conformed to the principles outlined in the Declaration of Helsinki. The research participants and their relatives could opt out by viewing the research content hosted online.
2.3. Clinicopathological Factors and Grouping Criteria
Patients were stratified according to the following clinicopathological variables: sex, age at the start of ICI monotherapy (≥70 years or <70 years), Brinkmann Index (≥600 or <600), number of dissected lymph nodes (DLNs) (≥15 or <15), histological type (adenocarcinoma or other), PD-L1 expression rate in surgical specimens (classified into the high expression group [PD-L1 expression: ≥50%] and low expression group of [PD-L1 expression:<50%]), presence or absence of extrathoracic recurrent lesions at the initiation of ICI monotherapy, treatment line of ICI monotherapy after recurrence (≥3rd line or <3rd line), and period from surgery to the initiation of ICI monotherapy (≥2 years or <2 years). The efficacy of ICI therapy and prognosis after the initiation of ICI therapy were compared between the groups.
2.4. Radiological Evaluation Criteria
The radiological response to ICI monotherapy was evaluated using RECIST version 1.1, where a complete response (CR) was defined as the disappearance of all target lesions; a partial response (PR) was defined as a reduction in the sum of the diameters of the target lesions of ≥30% from the sum of the diameters at baseline; progressive disease (PD) was defined as an increase in the sum of the diameters of the target lesions of ≥20% or an absolute increase of ≥5 mm or the appearance of new lesions; and stable disease (SD) was defined as either a reduction sufficient to satisfy PR or an increase sufficient to satisfy PD [21].
2.5. Statistical Analysis
Owing to the small sample size, all analyses were considered exploratory. Associations between the objective response rate (ORR) and disease control rate (DCR) according to the radiological evaluation of ICI monotherapy and clinicopathological factors were analyzed using the chi-square test. ICI-progression-free survival (PFS) was defined as the interval from the initiation of ICI monotherapy to the date of disease progression or death from any cause, censored for patients without events at the last clinic visit. In addition, patients who discontinued ICI monotherapy owing to adverse events were censored at the date of discontinuation. ICI-overall survival (OS) was defined as the interval from the initiation of ICI monotherapy until the date of death from any cause and was censored for patients who were alive at the last clinic visit. Kaplan-Meier curves were plotted for ICI-PFS and ICI-OS, and differences between groups were analyzed using the log-rank test. Due to the limited number of patients in this study, we employed a multivariable Cox proportional hazards regression analysis with propensity score adjustment. Propensity scores were calculated using logistic regression, where the dependent variable was defined as ICI-PFS ≥300 days based on the median ICI-PFS of approximately 300 days observed in our cohort. Covariates included in the propensity score model were those that showed statistical significance (p < 0.05) in a univariate analysis using the log-rank test to minimize overfitting. In the subsequent multivariable Cox regression, propensity scores were used as adjustment covariates, and the primary variable of interest was not included in the propensity score model to avoid overadjustment and ensure independent evaluation [22]. SPSS (ver. 26, SPSS Inc., Chicago, IL, USA) was used to perform the statistical analyses. Statistical significance was set at P <0.05.
3. Results
3.1. Patient Characteristics
The characteristics of the patients included in this study are shown in Table 1. There were 23 men and 7 women, with a median age of 71 years (range: 53–82 years), and most of the patients (27 patients, 90%) were smokers. The most common surgical procedure was lobectomy in 20 patients (66.7%), and the median number of DLNs was 14 (range, 0–39). The histological type of the resected primary tumor was adenocarcinoma in 21 patients (70%) and squamous cell carcinoma in 8 patients (26.7%). The PD-L1 expression in surgical specimens was high in 13 patients (43.3%) and low in 10 (33.3%). Thirteen patients (43.3%) had extrathoracic recurrent lesions at the time of initiation. The drugs used in ICI monotherapy were nivolumab (n=17, 56.7%), pembrolizumab (n=10, 33.3%), and atezolizumab (n=3, 10.0%). The median number of lines of ICI monotherapy after recurrence was 2.1, with the most common being second-line ICI monotherapy (16 patients; 53.3%). The median time from surgery to the initiation of ICI monotherapy was 27.7 months (range: 8.4-69.4 months).
3.2. Radiological Effect of ICI Monotherapy
The best radiological effect was a CR in 5 patients, PR in 6 patients, SD in 8 patients, and PD in 14 patients, with an ORR of 36.7% and a DCR of 63.3%. Table 2 shows the correlation between the ORR and DCR with ICI monotherapy and clinicopathological factors. The ORR was significantly higher in the high PD-L1 expression group than in the low PD-L1 expression group in surgical specimens (p=0.018). Figure 1 shows the radiological response according to PD-L1 expression in surgical specimens, the number of DLNs, and the presence or absence of extrathoracic lesions. Regarding the number of DLNs, the DCR in the group with ≥15 DLNs was 50.0%, which was lower than that in the group with <15 DLNs (75.0%); however, this difference was not statistically significant (p=0.257). Regarding the presence or absence of extrathoracic lesions, the DCR in the presence group was 46.2%, which was lower than the 76.5% in the absence group; however, this difference was not statistically significant (p=0.132).
3.3. Prognosis After Initiation of ICI Monotherapy
The median follow-up period after the initiation of ICI monotherapy was 21.2 months, during which 24 patients developed PD and 26 deaths occurred. Patients whose surgical specimens showed high PD-L1 expression levels had significantly better ICI-PFS and ICI-OS than those with low PD-L1 expression levels (Figure 2A; p=0.003 and Figure 2B; 0.029, respectively). A significant difference was observed only in the PD-L1 expression in ICI-OS patients. The ICI-PFS in the group with ≥15 DLNs was significantly worse than that in the group with <15 DLNs (Figure 3A; p=0.047), but the ICI-OS did not differ to a statistically significant extent (Figure 3B; p=0.228). Furthermore, in patients with extrathoracic recurrent lesions, there was no significant difference in ICI-PFS between the group with ≥15 DLNs and the group with <15 DLNs (Figure 3C; p=0.798); however, in patients without extrathoracic recurrent lesions, the ICI-PFS of the group with ≥15 DLNs was significantly worse than that of the group with <15 DLNs (Figure 3D; p=0.003). The results of the multivariate analysis for ICI-PFS are shown in Table 3. In the multivariate analysis, the number of DLNs (hazard ratio [HR], 2.702; 95% confidence interval [CI], 1.064 – 6.849; p=0.037), PD-L1 expression in surgical specimens (HR, 0.161; 95% CI, 0.044 – 0.598; p=0.006), and the presence of extrathoracic recurrent lesions were identified as independent prognostic factors (HR, 3.521; 95% CI, 1.307 – 9.524; p=0.013).
4. Discussion
In this study, we investigated the factors influencing the efficacy of ICI monotherapy for postoperative recurrence of NSCLC. It was revealed that patients with a large number of lymph nodes dissected at surgery had significantly worse ICI-PFS than those with a small number of lymph nodes dissected at surgery, and that patients whose surgical specimens had high PD-L1 expression levels had significantly better ICI-PFS and ICI-OS than those with low PD-L1 expression levels. Furthermore, in the multivariate analysis of ICI-PFS, the number of DLNs, PD-L1 expression rate in surgical specimens, and presence or absence of extrathoracic recurrent lesions were identified as independent prognostic predictors.
Several preclinical models have shown that tumor-draining lymph nodes (TDLNs) play a central role in cancer immune responses. Fransen et al. showed that PD-1 blockade by ICIs activates CD8+ T cells in TDLNs and induces the influx of these effector cells into the tumor microenvironment [23]. Dammeijer et al. showed that TDLNs, rather than the tumor microenvironment, are important regulators of ICI efficacy [24]. Furthermore, Saddawi-Konefka et al. used a lymphadenectomy mouse model to show that lymphadenectomy markedly reduced the response to ICI therapy [25]. They attributed this to the loss of conventional type I dendritic cells and type I interferon signaling, which are upregulated in TDLNs.
In addition, a retrospective clinical study was conducted to examine whether there was a difference in the therapeutic effect of ICIs depending on the extent of lymph node dissection in 26 patients with recurrent NSCLC. As a result, patients who underwent systematic lymph node dissection had significantly worse PFS than those who underwent selective lymph node dissection [18], which was partly in accordance with our current study results. However, more than half of the patients in this study were administered ICIs in combination with chemotherapy; therefore, the results should be interpreted with caution.
Central memory T cells and stem cell-like memory T cells in the bone marrow maintain long-term antigen-specific immune memory and are rapidly reactivated when the antigen reappears [26]. In the current study, the presence of extrathoracic recurrent lesions was an independent prognostic factor for ICI-PFS. Furthermore, in patients with extrathoracic recurrent lesions, the number of LNDs did not affect ICI-PFS, whereas in patients with only intrathoracic disease, the number of DLNs was significantly lower than that of the small number of DLNs. This suggests that in cases of intrathoracic recurrence, in addition to reactivated memory T cells, the antitumor immune response of the remaining TDLNs is strongly involved in the efficacy of ICIs.
Sentinel lymph nodes close to tumors are susceptible to cancer and have suppressed immune activity [27,28]. Our previous studies have also shown that the closer the lymph node is to the tumor, the lower the immune activity of monocytic cells [29,30]. To maximize the efficacy of ICI therapy, it is important to reactivate the immune system of the suppressed lymph nodes. Therefore, it is thought that administering ICI before resection of sentinel lymph nodes in an immune-tolerant state, that is, before surgery, will enable more effective induction of antitumor immunity. Liu et al. showed that the therapeutic effect of neoadjuvant ICI therapy was significantly stronger than that of adjuvant ICI therapy in a mouse model of metastatic breast cancer [31]. In advanced melanoma, the group that received three courses of pembrolizumab before surgery and 15 courses after surgery showed significantly better event-free survival than the group that received 18 courses of pembrolizumab only after surgery [32]. A large-scale cohort study of stage II-IIIB NSCLC patients using data from the National Cancer Database in the United States showed that neoadjuvant immunochemotherapy was associated with significantly better OS than adjuvant immunochemotherapy [33]. The results of the current study suggest that dissection of many lymph nodes downregulates antitumor immune activity; therefore, using ICIs before lymph node dissection may maximize the effect of ICI therapy.
The high expression of PD-L1 is a favorable prognostic factor for ICI monotherapy [17]. In the present study, the high expression of PD-L1 in surgical specimens was strongly associated with the response rate of patients receiving ICI therapy, even for recurrent lesions relatively long after surgery, and was a favorable factor for ICI-PFS and OS. Although the immune environment in tumors is heterogeneous, Kitazono et al. showed a good agreement between the PD-L1 expression in biopsy and surgical specimens [34]. In addition, Cho et al. compared the PD-L1 expression in biopsy or surgical specimens separated by an average of 20 months and showed a significant positive correlation between paired samples [35]. However, it has been reported that chemotherapy changes the PD-L1 expression both in vitro and in clinical practice [36,37,38], and it is therefore important to reassess the PD-L1 expression before treatment with ICIs.
The present study was associated with several limitations. First, it was a single-center retrospective study and the number of subjects was limited. Currently, ICI therapy for NSCLC is mainly combined with chemotherapy, which makes it difficult to study ICI monotherapy. Therefore, it is desirable to collect and analyze large-scale data from more institutions. Another limitation was that the factors examined as predictors of recurrence were limited. The high response rate of patients receiving ICI therapy has been examined in various cancers, and in addition to the expression of PD-L1, there have been reports of tumor mutation burden and oncogenic virus infection status [39,40,41,42], Future studies should also examine the relationship with other biological factors.
5. Conclusion
Minimal lymph node dissection may be beneficial in achieving better outcomes after ICI therapy for postoperative intrathoracic recurrence after the resection of NSCLC, providing a rationale to recommend preoperative ICI treatment when the lymphatic immune system is intact.
Author Contributions
Conceptualization, M.A.; Methodology, M.A.; Software, M.A.; Validation, M.A. and G.K.; Investigation, M.A., G.K., Y.T., S.M. T.T., A.H-T., T.N. K.K. and K.U.; Data Curation, M.A.; Writing – Original Draft Preparation, M.A.; Writing – Review & Editing, K.U. and G.K.; Visualization, M.A.; Supervision, K.U. All authors read and approved the final manuscript.
Funding
This research received no external funding.
Ethics Statement
The use of the information was approved by the Ethics Committee of Kagoshima University Graduate School of Medicine and Dentistry (Approval No. 220178epi) and conformed to the principles outlined in the Declaration of Helsinki. Research participants and their relatives could opt out by viewing the research content hosted online.
Data Availability Statement
The original contributions presented in this study are included in the article/supplementary material. Further inquiries can be directed to the corresponding author(s).
Conflicts of Interest
The authors declare no conflicts of interest in association with the present study.
References
- Bray, F.; Laversanne, M.; Sung, H.; Ferlay, J.; Siegel, RL.; Soerjomataram, I.; et al. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2024, 74, 229–263. [Google Scholar] [CrossRef] [PubMed]
- Okami, J.; Shintani, Y.; Okumura, M.; Ito, H.; Ohtsuka, T.; Toyooka, S.; et al. Demographics, Safety and Quality, and Prognostic Information in Both the Seventh and Eighth Editions of the TNM Classification in 18,973 Surgical Cases of the Japanese Joint Committee of Lung Cancer Registry Database in 2010. J Thorac Oncol. 2019, 14, 212–222. [Google Scholar] [CrossRef] [PubMed]
- Brahmer, J.; Reckamp, KL.; Baas, P.; Crinò, L.; Eberhardt, WE.; Poddubskaya, E.; et al. Nivolumab versus Docetaxel in Advanced Squamous-Cell Non-Small-Cell Lung Cancer. N Engl J Med. 2015, 373, 123–35. [Google Scholar] [CrossRef]
- Borghaei, H.; Paz-Ares, L.; Horn, L.; Spigel, DR.; Steins, M.; Ready, NE.; et al. Nivolumab versus Docetaxel in Advanced Nonsquamous Non-Small-Cell Lung Cancer. N Engl J Med. 2015, 373, 1627–39. [Google Scholar] [CrossRef]
- Socinski, MA.; Nishio, M.; Jotte, RM.; Cappuzzo, F.; Orlandi, F.; Stroyakovskiy, D.; et al. IMpower150 Final Overall Survival Analyses for Atezolizumab Plus Bevacizumab and Chemotherapy in First-Line Metastatic Nonsquamous NSCLC. J Thorac Oncol. 2021, 16, 1909–1924. [Google Scholar] [CrossRef]
- West, H.; McCleod, M.; Hussein, M.; Morabito, A.; Rittmeyer, A.; Conter, HJ.; et al. Atezolizumab in combination with carboplatin plus nab-paclitaxel chemotherapy compared with chemotherapy alone as first-line treatment for metastatic non-squamous non-small-cell lung cancer (IMpower130): a multicentre, randomised, open-label, phase 3 trial. Lancet Oncol. 2019, 20, 924–937. [Google Scholar] [CrossRef]
- Nishio, M.; Barlesi, F.; West, H.; Ball, S.; Bordoni, R.; Cobo, M.; et al. Atezolizumab Plus Chemotherapy for First-Line Treatment of Nonsquamous NSCLC: Results From the Randomized Phase 3 IMpower132 Trial. J Thorac Oncol. 2021, 16, 653–664. [Google Scholar] [CrossRef]
- Garassino, MC.; Gadgeel, S.; Speranza, G.; Felip, E.; Esteban, E.; Dómine, M.; et al. Pembrolizumab Plus Pemetrexed and Platinum in Nonsquamous Non-Small-Cell Lung Cancer: 5-Year Outcomes From the Phase 3 KEYNOTE-189 Study. J Clin Oncol. 2023, 41, 1992–1998. [Google Scholar] [CrossRef]
- Novello, S.; Kowalski, DM.; Luft, A.; Gümüş, M.; Vicente, D.; Mazières, J.; et al. Pembrolizumab Plus Chemotherapy in Squamous Non-Small-Cell Lung Cancer: 5-Year Update of the Phase III KEYNOTE-407 Study. J Clin Oncol. 2023, 41, 1999–2006. [Google Scholar] [CrossRef]
- Felip, E.; Altorki, N.; Zhou, C.; Vallières, E.; Martínez-Martí, A.; Rittmeyer, A.; et al. Overall survival with adjuvant atezolizumab after chemotherapy in resected stage II-IIIA non-small-cell lung cancer (IMpower010): a randomised, multicentre, open-label, phase III trial. Ann Oncol. 2023, 34, 907–919. [Google Scholar] [CrossRef]
- Forde, PM.; Spicer, J.; Lu, S.; Provencio, M.; Mitsudomi, T.; Awad, MM.; et al. Neoadjuvant Nivolumab plus Chemotherapy in Resectable Lung Cancer. N Engl J Med. 2022, 386, 1973–1985. [Google Scholar] [CrossRef] [PubMed]
- Spicer, JD.; Garassino, MC.; Wakelee, H.; Liberman, M.; Kato, T.; Tsuboi, M.; et al. Neoadjuvant pembrolizumab plus chemotherapy followed by adjuvant pembrolizumab compared with neoadjuvant chemotherapy alone in patients with early-stage non-small-cell lung cancer (KEYNOTE-671): a randomised, double-blind, placebo-controlled, phase 3 trial. Lancet. 2024, 404, 1240–1252. [Google Scholar] [CrossRef] [PubMed]
- Heymach, JV.; Harpole, D.; Mitsudomi, T.; Taube, JM.; Galffy, G.; Hochmair, M.; et al. Perioperative Durvalumab for Resectable Non-Small-Cell Lung Cancer. N Engl J Med. 2023, 389, 1672–1684. [Google Scholar] [CrossRef]
- Cascone, T.; Awad, MM.; Spicer, JD.; He, J.; Lu, S.; Sepesi, B.; et al. Perioperative Nivolumab in Resectable Lung Cancer. N Engl J Med. 2024, 390, 1756–1769. [Google Scholar] [CrossRef]
- Lu, S.; Zhang, W.; Wu, L.; Wang, W.; Zhang, P.; Fang, W.; et al. Perioperative Toripalimab Plus Chemotherapy for Patients With Resectable Non-Small Cell Lung Cancer: The Neotorch Randomized Clinical Trial. JAMA. 2024, 331, 201–211. [Google Scholar] [CrossRef]
- Mountzios, G.; Remon, J.; Hendriks, LEL. ; García-Campelo, R.; Rolfo, C.; Van Schil, P.; et al. Immune-checkpoint inhibition for resectable non-small-cell lung cancer - opportunities and challenges. Nat Rev Clin Oncol. 2023, 20, 664–677. [Google Scholar] [CrossRef]
- Reck, M.; Rodríguez-Abreu, D.; Robinson, AG.; Hui, R.; Csőszi, T.; Fülöp, A.; et al. Pembrolizumab versus Chemotherapy for PD-L1-Positive Non-Small-Cell Lung Cancer. N Engl J Med. 2016, 375, 1823–1833. [Google Scholar] [CrossRef]
- Kawaguchi, Y.; Nishioka, N.; Nakamura, T.; Imai, K.; Aoki, T.; Kajiwara, N.; et al. Impact of lymph node dissection on the efficacy of immune checkpoint inhibitors in patients with postoperative recurrence of non-small cell lung cancer. J Thorac Dis. 2024, 16, 1960–1970. [Google Scholar] [CrossRef]
- Kuroda, H.; Takahashi, Y.; Shirai, S.; Takahara, H.; Nakada, T.; Sakakura, N.; et al. Survival benefit of immune checkpoint inhibitor monotherapy in patients with non-small cell lung cancer recurrence after completely pulmonary resection. Ann Transl Med. 2021, 9, 1225. [Google Scholar] [CrossRef]
- Yuasa, I.; Hamaji, M.; Ozasa, H.; Sakamori, Y.; Yoshida, H.; Yutaka, Y.; et al. Outcomes of immune checkpoint inhibitors for postoperative recurrence of non-small cell lung cancer. Gen Thorac Cardiovasc Surg. 2023, 71, 534–541. [Google Scholar] [CrossRef]
- Eisenhauer, EA.; Therasse, P.; Bogaerts, J.; Schwartz, LH.; Sargent, D.; Ford, R.; et al. New response evaluation criteria in solid tumours: revised RECIST guideline (version 1.1). Eur J Cancer. 2009, 45, 228-47. [CrossRef]
- Devasia, RA.; Blackman, A.; Gebretsadik, T.; Griffin, M.; Shintani, A.; May, C.; et al. Fluoroquinolone resistance in Mycobacterium tuberculosis: the effect of duration and timing of fluoroquinolone exposure. Am J Respir Crit Care Med. 2009, 180, 365–70. [Google Scholar] [CrossRef] [PubMed]
- Fransen, MF.; Schoonderwoerd, M.; Knopf, P.; Camps, MG.; Hawinkels, LJ.; Kneilling, M.; et al. Tumor-draining lymph nodes are pivotal in PD-1/PD-L1 checkpoint therapy. JCI Insight. 2018, 3, e124507. [Google Scholar] [CrossRef] [PubMed]
- Dammeijer F, van Gulijk M, Mulder EE, Lukkes M, Klaase L, van den Bosch T, et al. The PD-1/PD-L1-Checkpoint Restrains T cell Immunity in Tumor-Draining Lymph Nodes. Cancer Cell. 2020, 38, 685-700.e8. [CrossRef]
- Saddawi-Konefka R, O'Farrell A, Faraji F, Clubb L, Allevato MM, Jensen SM, et al. Lymphatic-preserving treatment sequencing with immune checkpoint inhibition unleashes cDC1-dependent antitumor immunity in HNSCC. Nat Commun. 2022, 13, 4298. [CrossRef]
- Mazo, IB.; Honczarenko, M.; Leung, H.; Cavanagh, LL.; Bonasio, R.; Weninger, W.; et al. Bone marrow is a major reservoir and site of recruitment for central memory CD8+ T cells. Immunity. 2005, 22, 259–70. [Google Scholar] [CrossRef] [PubMed]
- Cochran, AJ.; Huang, RR.; Lee, J.; Itakura, E.; Leong, SP.; Essner, R. ; Tumour-induced immune modulation of sentinel lymph nodes. Nat Rev Immunol. 2006, 6, 659–70. [Google Scholar] [CrossRef]
- Munn, DH.; Mellor, AL. The tumor-draining lymph node as an immune-privileged site. Immunol Rev. 2006, 213, 146–58. [Google Scholar] [CrossRef]
- Sonoda, T.; Arigami, T.; Aoki, M.; Matsushita, D.; Shimonosono, M.; Tsuruda, Y.; et al. Difference between sentinel and non-sentinel lymph nodes in the distribution of dendritic cells and macrophages: An immunohistochemical and morphometric study using gastric regional nodes obtained in sentinel node navigation surgery for early gastric cancer. J Anat. 2025, 246, 272–287. [Google Scholar] [CrossRef]
- Aoki, M.; Kamimura, G.; Harada-Takeda, A.; Nagata, T.; Murakami, G.; Ueda K. Topohistology of dendritic cells and macrophages in the distal and proximal nodes along the lymph flow from the lung. J Anat. 2025. Online ahead of print. [CrossRef]
- Liu, J.; Blake, SJ.; Yong, MC.; Harjunpää, H.; Ngiow, SF.; Takeda, K.; et al. Improved Efficacy of Neoadjuvant Compared to Adjuvant Immunotherapy to Eradicate Metastatic Disease. Cancer Discov. 2016, 6, 1382–1399. [Google Scholar] [CrossRef]
- Patel, SP.; Othus, M.; Chen, Y.; Wright, GP Jr.; Yost, KJ.; Hyngstrom, JR.; et al. Neoadjuvant-Adjuvant or Adjuvant-Only Pembrolizumab in Advanced Melanoma. N Engl J Med. 2023, 388, 813-823. [CrossRef]
- Martins, RS.; Razi, SS.; Alnajar, A.; Poulikidis, K.; Latif, MJ.; Luo, J.; et al. Neoadjuvant vs Adjuvant Chemoimmunotherapy for Stage II-IIIB Non-Small Cell Lung Cancer. Ann Thorac Surg. 2024, 118, 672–681. [Google Scholar] [CrossRef]
- Kitazono, S.; Fujiwara, Y.; Tsuta, K.; Utsumi, H.; Kanda, S.; Horinouchi, H.; et al. Reliability of Small Biopsy Samples Compared With Resected Specimens for the Determination of Programmed Death-Ligand 1 Expression in Non--Small-Cell Lung Cancer. Clin Lung Cancer. 2015, 16, 385–90. [Google Scholar] [CrossRef]
- Cho, JH.; Sorensen, SF.; Choi, YL.; Feng, Y.; Kim, TE.; Choi, H.; et al. Programmed Death Ligand 1 Expression in Paired Non-Small Cell Lung Cancer Tumor Samples. Clin Lung Cancer. 2017, 18, e473–e479. [Google Scholar] [CrossRef]
- Rojkó, L.; Reiniger, L.; Téglási, V.; Fábián, K.; Pipek, O.; Vágvölgyi, A.; et al. Chemotherapy treatment is associated with altered PD-L1 expression in lung cancer patients. J Cancer Res Clin Oncol. 2018, 144, 1219–1226. [Google Scholar] [CrossRef] [PubMed]
- Lacour, M.; Hiltbrunner, S.; Lee, SY.; Soltermann, A.; Rushing, EJ.; Soldini, D.; et al. Adjuvant Chemotherapy Increases Programmed Death-Ligand 1 (PD-L1) Expression in Non-small Cell Lung Cancer Recurrence. Clin Lung Cancer. 2019, 20, 391–396. [Google Scholar] [CrossRef] [PubMed]
- Ng, HY.; Li, J.; Tao, L.; Lam, AK.; Chan, KW.; Ko, JMY.; et al. Chemotherapeutic Treatments Increase PD-L1 Expression in Esophageal Squamous Cell Carcinoma through EGFR/ERK Activation. Transl Oncol. 2018, 11, 1323-1333. [CrossRef]
- Yarchoan, M.; Hopkins, A.; Jaffee, EM. Tumor mutational burden and response rate to PD-1 inhibition. N. Engl. J. Med. 2017, 377, 2500–2501. [Google Scholar] [CrossRef]
- Topalian, SL.; Hodi, FS.; Brahmer, JR.; Gettinger, SN.; Smith, DC.; McDermott, DF,l et al. Safety, activity, and immune correlates of anti-PD-1 antibody in cancer. N Engl J Med. 2012, 366, 2443-54. [CrossRef]
- Nghiem, PT.; Bhatia, S.; Lipson, EJ.; Kudchadkar, RR.; Miller, NJ.; Annamalai, L.; et al. PD-1 Blockade with Pembrolizumab in Advanced Merkel-Cell Carcinoma. N Engl J Med. 2016, 374, 2542–52. [Google Scholar] [CrossRef]
- Topalian, SL.; Taube, JM.; Anders, RA.; Pardoll, DM. Mechanism-driven biomarkers to guide immune checkpoint blockade in cancer therapy. Nat Rev Cancer. 2016, 16, 275–287. [Google Scholar] [CrossRef]
Figure 1.
Radiological response to ICI therapy according to the PD-L1 expression in surgical specimens, number of DLNs, and the presence or absence of extrathoracic lesions. ICI, immune checkpoint inhibitor; PD-L1, programmed death ligand 1; DLN, dissected lymph node; DCR, disease control rate; OR, objective response rate; CR, complete response; PR, partial response; SD, stable disease; PD, progressive disease; * p<0.05.
Figure 1.
Radiological response to ICI therapy according to the PD-L1 expression in surgical specimens, number of DLNs, and the presence or absence of extrathoracic lesions. ICI, immune checkpoint inhibitor; PD-L1, programmed death ligand 1; DLN, dissected lymph node; DCR, disease control rate; OR, objective response rate; CR, complete response; PR, partial response; SD, stable disease; PD, progressive disease; * p<0.05.
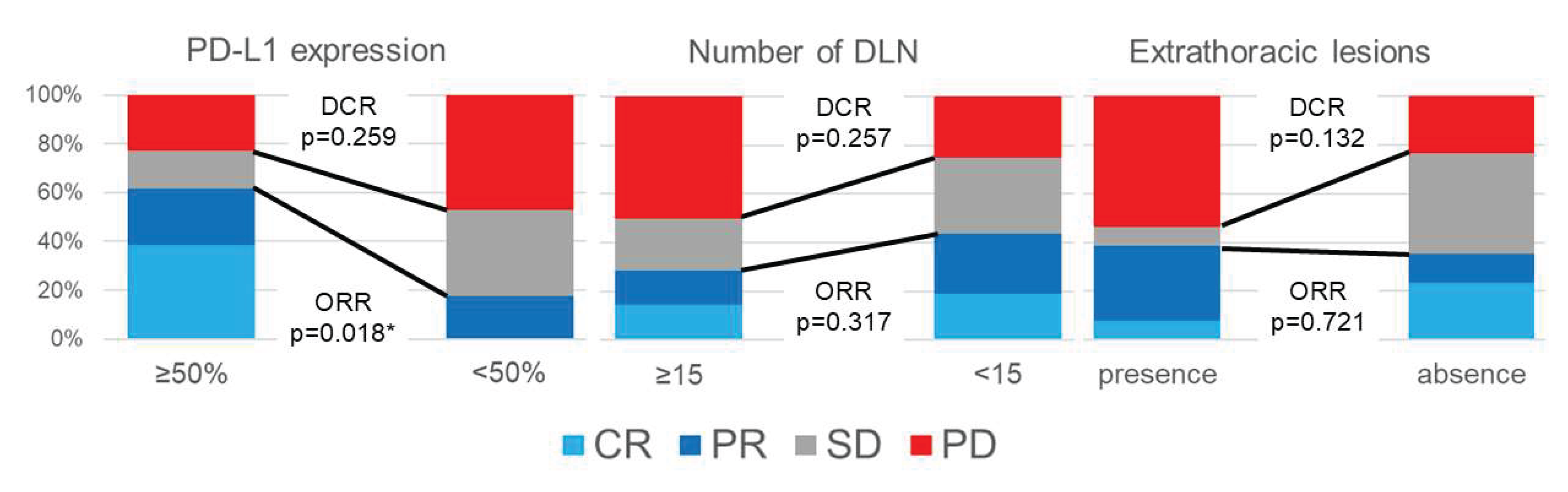
Figure 2.
Association of the PD-L1 expression with the prognosis. (A) The association between the PD-L1 expression and ICI-PFS in all patients. (B) The association between the PD-L1 expression and ICI-OS in all patients. PD-L1, programmed death ligand 1; ICI, immune checkpoint inhibitor; ICI-PFS, progression-free survival after the initiation of ICI therapy; ICI-OS, overall survival after the initiation of ICI therapy; *p<0.05, **p<0.01.
Figure 2.
Association of the PD-L1 expression with the prognosis. (A) The association between the PD-L1 expression and ICI-PFS in all patients. (B) The association between the PD-L1 expression and ICI-OS in all patients. PD-L1, programmed death ligand 1; ICI, immune checkpoint inhibitor; ICI-PFS, progression-free survival after the initiation of ICI therapy; ICI-OS, overall survival after the initiation of ICI therapy; *p<0.05, **p<0.01.
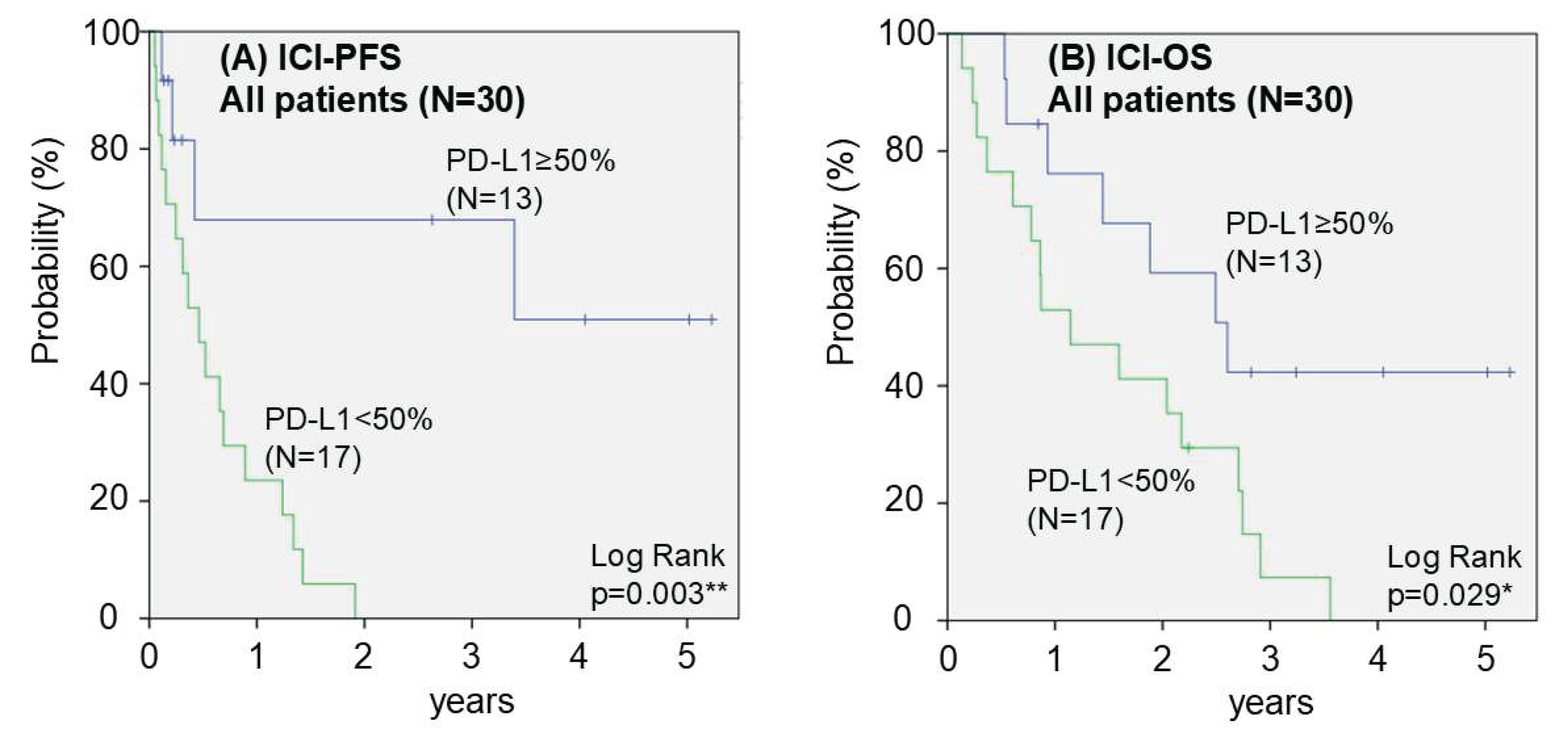
Figure 3.
Association of the number of DLNs with the prognosis. (A) Association between the number of DLNs and ICI-PFS in all patients. (B) Association between the number of DLNs and ICI-OS in all patients. (C) Association between the number of DLNs and ICI-PFS in patients with extrathoracic recurrent lesions. (D) Association between the number of DLNs and ICI-PFS in patients without extrathoracic recurrent lesions. DLN, dissected lymph node; ICI, immune checkpoint inhibitor; ICI-PFS, progression-free survival after the initiation of ICI therapy; ICI-OS, overall survival after the initiation of ICI therapy; *p<0.05, **p<0.01.
Figure 3.
Association of the number of DLNs with the prognosis. (A) Association between the number of DLNs and ICI-PFS in all patients. (B) Association between the number of DLNs and ICI-OS in all patients. (C) Association between the number of DLNs and ICI-PFS in patients with extrathoracic recurrent lesions. (D) Association between the number of DLNs and ICI-PFS in patients without extrathoracic recurrent lesions. DLN, dissected lymph node; ICI, immune checkpoint inhibitor; ICI-PFS, progression-free survival after the initiation of ICI therapy; ICI-OS, overall survival after the initiation of ICI therapy; *p<0.05, **p<0.01.
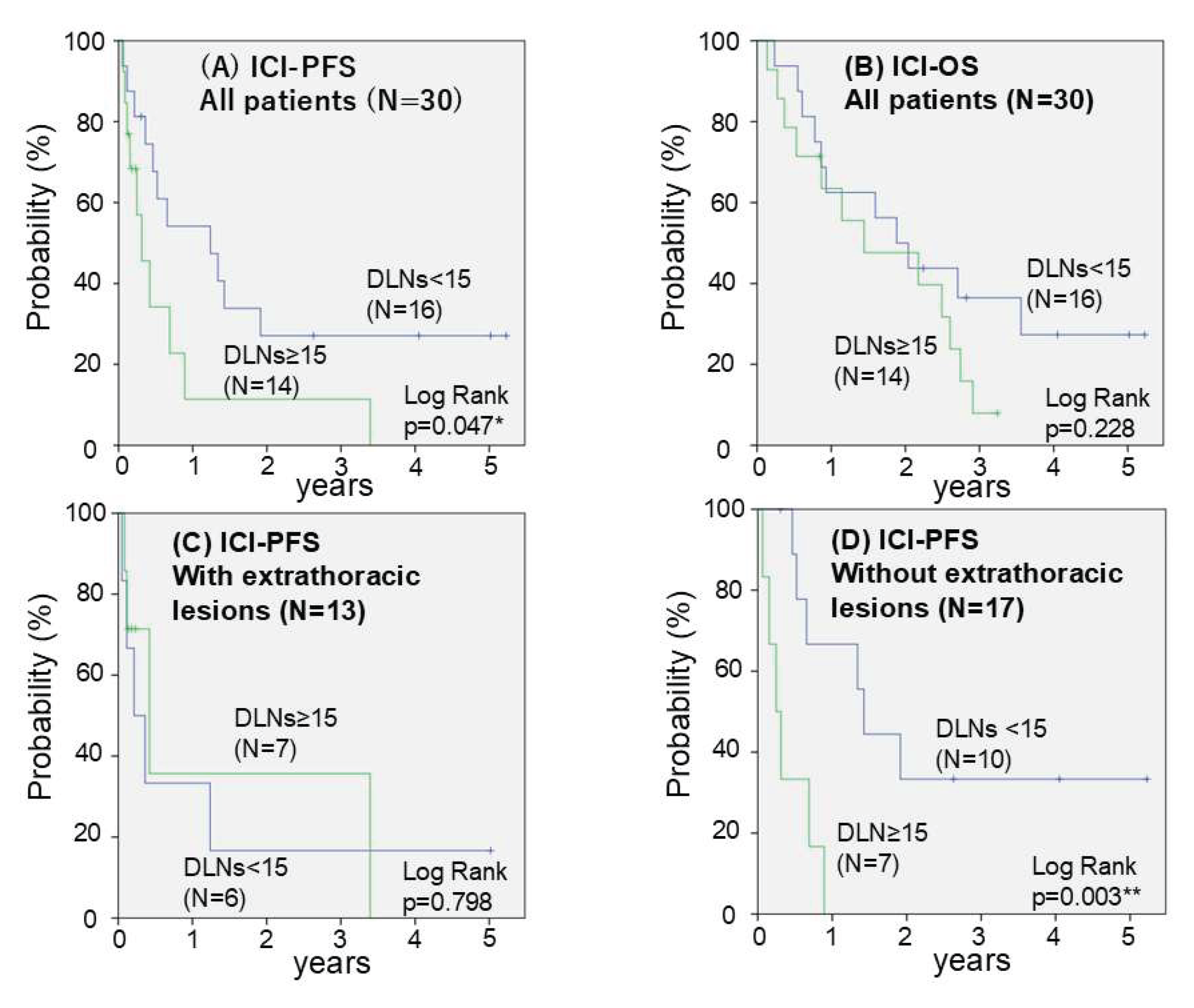

Table 1.
Patients' characteristics.
| Gender | Male | 23 (76.7%) |
| Female | 7 (23.3%) | |
| Age | Median (range) | 71years (53-82) |
| Smoking | Ever | 27 (90.0%) |
| Never | 3 (10.0%) | |
| Brinkman Index | Median (range) | 970 (0-3600) |
| Surgical Procedure | Wedge resection | 3 (10.0%) |
| Segmentectomy | 2 (6.7%) | |
| Lobectomy | 20 (66.7%) | |
| Bi-lobectomy | 2 (6.7%) | |
| Pneumonectomy | 3 (10.0%) | |
| Number of DLN | Median (range) | 14 (0-39) |
| Histlogical type | Adenocarcinoma | 21 (70.0%) |
| Squamous cell carcinoma | 8 (26.7%) | |
| Large cell carcinoma | 1 (3.3%) | |
| PD-L1 expression in surgical specimens | no expression | 7 (23.3%) |
| Low expression | 10 (33.3%) | |
| High expression | 13 (43.3%) | |
| Extrathoracic lesions | presence | 13 (43.3%) |
| absence | 17 (56.7%) | |
| Generic name of ICIs | Nivolumab | 17 (56.7%) |
| Pembrolizumab | 10 (33.3%) | |
| Atezolizumab | 3 (10.0%) | |
| Therapeutic Lines of ICIs | First | 7 (23.3%) |
| Second | 16 (53.3%) | |
| Third | 5 (16.7%) | |
| More | 2 (6.7%) | |
| Duration from surgery to initiation of ICIs | Median (range) | 27.7 months(8.4-69.4 months) |
| DLN: Dissected lymph Nodes, PD-L1: Programmed Death-Ligand 1, ICI: Immune Checkpoint Inhibitor | ||
Table 2.
Relationship between response rate of ICIs and clinicopathological factors.
| Factors | RECIST | ORR (%) |
ORR p-value |
DCR (%) |
DCR p-value |
||||
| CR | PR | SD | PD | ||||||
| Gender | Male | 3 | 5 | 5 | 10 | 34.8 | 0.515 | 56.5 | 0.215 |
| Female | 2 | 1 | 3 | 1 | 42.9 | 85.7 | |||
| Age | >= 70 | 3 | 4 | 4 | 5 | 43.8 | 0.371 | 68.8 | 0.707 |
| < 70 | 2 | 2 | 4 | 6 | 28.6 | 57.1 | |||
| Brinkman Index | >= 600 | 3 | 4 | 5 | 9 | 33.3 | 0.429 | 57.1 | 0.419 |
| < 600 | 2 | 2 | 3 | 2 | 44.4 | 77.8 | |||
| Number of DLN | >= 15 | 2 | 2 | 3 | 7 | 28.6 | 0.317 | 50.0 | 0.257 |
| < 15 | 3 | 4 | 5 | 4 | 43.8 | 75.0 | |||
| Histlogical type | AD | 3 | 5 | 6 | 7 | 38.1 | 0.571 | 66.7 | 0.687 |
| Others | 2 | 1 | 2 | 4 | 33.3 | 55.6 | |||
| PD-L1 expression in surgical specimens | >= 50% | 5 | 3 | 2 | 3 | 61.5 | 0.018* | 76.9 | 0.259 |
| < 50% | 0 | 3 | 6 | 8 | 17.6 | 52.9 | |||
| Extrathoracic lesions | Presence | 1 | 4 | 1 | 7 | 38.5 | 0.721 | 46.2 | 0.132 |
| Absence | 4 | 2 | 7 | 4 | 35.3 | 76.5 | |||
| Therapeutic Lines of ICIs | >= 3rd line | 1 | 1 | 3 | 2 | 28.6 | 0.485 | 71.4 | 1.000 |
| < 3rd line | 4 | 5 | 5 | 9 | 39.1 | 60.9 | |||
| Duration from surgery to initiation of ICIs | >= 2 years | 1 | 4 | 3 | 4 | 41.7 | 0.61 | 66.7 | 1.000 |
| < 2 years | 4 | 2 | 5 | 7 | 33.3 | 61.1 | |||
| ICI: Immune Checkpoint Inhibitor, RECIST: Response Evaluation Criteria in Solid Tumors, CR: Complete Response, PR: Partial Response, SD: Stable Disease, PD: Progressive Disease, ORR: Objective Response Rate, DCR: Disease Control Rate, DLN: Dissected Lymph Nodes, AD: Adenocarcinoma, PD-L1: Programmed Death-Ligand 1*: p<0.05 | |||||||||
Table 3.
Univariate and multivariate analyses of ICI-PFS.
| Factors | Univariate p-value (log-rank test) |
Multivariate | ||
| HR | 95% CI | p-value | ||
| Gender (Male vs Female) |
0.596 | 1.019 | 0.324 - 3.204 | 0.974 |
| Age (>= 70 vs < 70) |
0.228 | 0.846 | 0.345 - 2.074 | 0.714 |
| Brinkmann Index (>= 600 vs < 600) |
0.425 | 0.985 | 0.364 - 2.668 | 0.977 |
| Number of DLN (>= 15 vs < 15) |
0.047* | 2.702 | 1.064 - 6.849 | 0.037* |
| Histlogical type (AD vs others) |
0.476 | 0.843 | 0.322 - 2.207 | 0.728 |
| PD-L1 expression in surgical specimens (>= 50% vs < 50%) |
0.003** | 0.161 | 0.044 - 0.598 | 0.006** |
| Extrathoracic lesions (Presence vs Absence) |
0.335 | 3.521 | 1.307 - 9.524 | 0.013* |
| Therapeutic Lines of ICIs (>= 3rd vs < 3rd) |
0.342 | 1.295 | 0.477 - 3.516 | 0.612 |
| Duration from surgery to initiation of ICIs | 0.745 | - | ||
| ICI: Immune Checkpoint Inhibitor, ICI-PFS: Progression Free Survival after initiation of ICI, HR: Hazard Ratio, CI: Confidence Interval, DLN: Dissected Lymph Nodes, AD: adenocarcinoma, PD-L1: Programmed Death-Ligand 1 *: p<0.05, **: p<0.01 | ||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



