
Submitted:
19 May 2025
Posted:
20 May 2025
You are already at the latest version
Abstract
Background: Dystonic cerebral palsy (DCP) is a complex, disabling manifestation of secondary dystonia, which significantly impacts motor function, quality of life, and caregiver wellbeing. Conventional pharmacologic therapies frequently do not relieve symptoms sufficiently. Deep brain stimulation (DBS) of the globus pallidus internal segment (GPi) has garnered increasing attention as a neuromodulatory treatment for refractory dystonia. Still, the experience in the effect of Gpi DBS treatment in adults with DCP has, until recently, been limited.
Methods: We performed a retrospective, two-center case series of 11 adult patients with medically refractory DCP who underwent bilateral GPi-DBS. The clinical outcomes were evaluated based on the Burke-Fahn-Marsden Dystonia Rating Scale (BFMDRS), the Functional İndependence Measure (FIM), the Gross Motor Function Classification System (GMFCS), and the Caregiver Burden Scale (CBS. The assessments were done preoperatively and at 1-year follow-up. Changes in continuous variables were analyzed using paired t-tests.
Results: At the 1-year follow-up, the mean BFMDRS score improved from 69.6 ± 27.6 to 54.3 ± 36.5 (p = 0.001), significantly reducing overall dystonia severity. Functional independence also improved, demonstrated by the rise in FIM scores from 65.3 ± 33.9 to 79.2 ± 43.4 (p = 0.006). Although GMFCS levels did not change in most patients (p = 0.125), the burden on caregivers reduced significantly, with CBS scores falling from 35.7 ± 18.8 to 32.0 ± 17.1 (p = 0.015). There were no surgical complications.
Conclusion: In adults, DCP, bilateral GPi-DBS is a safe and effective intervention that improves motor control and increases functional independence with decreased caregiver burden. These findings lend support to its role in the multidisciplinary management of DCP.
Keywords:
Dystonic Cerebral Palsy
; Deep Brain Stimulation
; Globus Pallidus Internus
; Functional Independence
; Caregiver Burden
1. Introduction
Dystonia is a prominent, disabling feature of dystonic cerebral palsy (DCP), which is a substantial contributor to CP’s global disability. Dystonic CP patients suffer from involuntary muscle contractions and abnormal postures that impact motor function and activities of daily living. These unusual, sustained, repetitive movements lead to painful postures, interfere with positioning, and high energy expenditure, causing significant difficulty for the patient and their caregivers [1,2]. The clinical burden is substantial – dystonia affects not just the functional independence and quality of life of the child or adult with dystonia but also exacts a considerable physical and emotional toll on caregivers who must assist with mobility, positioning, and basic care [2,3,4]. Oral anti-spasticity and anti-dystonic medications (e.g., baclofen, anticholinergics, and benzodiazepines), conventionally used to treat dystonia in children with CP, have limited effectiveness in this population [5]. The pharmacological treatment of dystonic symptoms is usually limited for patients with dyskinetic CP, and side effects often restrict dosages, leaving a significant unmet need for more effective therapies [6,7,8].
In this context, neurosurgical intervention has emerged as a potential alternative. Deep brain stimulation of the globus pallidus interna (GPi-DBS) is an established therapy for primary generalized dystonia [9]. It has been explored in secondary dystonia (including dystonic CP) with promising but variable outcomes. Notably, bilateral GPi-DBS in patients with cerebral palsy has been associated with highly variable improvements in dystonia severity, ranging from negligible change to about 50% reduction in symptom [10] such variability likely reflects the heterogeneous nature of CP-related brain injury, and it underscores the importance of careful patient selection [10,11]. Nonetheless, GPi-DBS remains one of the few viable options for refractory dystonia in CP, with reports of meaningful gains in motor function and quality of life for some individuals [11].
Given the substantial burden of dystonia in CP and the limitations of medical therapy, we conducted a study to evaluate the impact of bilateral GPi-DBS in dystonic CP patients. We aimed to determine whether GPi-DBS can alleviate dystonic symptoms and improve patient outcomes. In particular, we aimed to assess changes in dystonia severity, functional abilities, and caregiver burden following bilateral GPi-DBS. By examining dystonia rating scores, functional status, and caregiver burden indices pre- and post-DBS, this study seeks to clarify the therapeutic value of GPi-DBS in secondary (CP-related) dystonia and provide insight into its potential benefits for patients and their caregivers. The findings will help refine the role of GPi-DBS in managing dystonic CP and guide clinical decision-making for this challenging condition.
2. Materials and Methods
2.1. Participants
This retrospective two-center case series included patients with dystonic cerebral palsy (DCP) who underwent bilateral globus pallidus internus deep brain stimulation (GPi- DBS) for medically refractory dystonia. A total of 11 patients were identified from two tertiary movement disorders clinics based on the following inclusion criteria: documented diagnosis of dystonic CP, treatment with bilateral GPi-DBS, and availability of complete preoperative and postoperative clinical data (including examination records and video documentation). All patients had a dyskinetic form of cerebral palsy with generalized dystonia as the predominant movement disorder. Most patients exhibited a quadriplegic distribution of motor involvement. The study protocol adhered to the principles of the Helsinki Declaration and received approval from the local Institutional Review Board Ins Ethics Committee (Approval number: 09.2023.511), and written informed consent was obtained from all participants (and/or their legal guardians) before inclusion in this retrospective analysis.
2.2. Data Collection
Demographic and clinical data, including age, sex, cerebral palsy subtype, and distribution of motor involvement, were obtained from individual patient medical records. All patients received standardized evaluations both preoperatively and at regular postoperative intervals. Outcomes in this study occurred at 1 year postoperatively for all patients, though total follow-up ranged from 1 to 5 years. Outcomes were documented and compared for baseline (pre-DBS) and 1-year post-DBS.
a)Outcome Measures: Dystonia severity, motor function, functional independence, and caregiver burden were assessed using the following clinical scales:
- Burke-Fahn-Marsden Dystonia Rating Scale (BFM-DRS): Evaluates dystonia severity through a movement subscore and a disability subscore, which are summed to a total score. Higher BFM-DRS scores indicate more severe dystonia and more significant functional impairment. This scale was administered preoperatively and at follow-up to quantify changes in dystonia severity [12].
- Gross Motor Function Classification System (GMFCS): Classifies gross motor function on a five-level ordinal scale from Level I (walking without limitations) to Level V (severe limitations in head/trunk control, requiring wheelchair mobility). A lower GMFCS level denotes better motor function. Each patient’s GMFCS level was recorded at baseline and 1-year post-DBS to assess overall motor function classification changes [13].
- Functional Independence Measure (FIM): Assesses patient’s ability to independently perform activities of daily living across multiple domains (self-care, mobility, communication, etc.) For each domain, a score is assigned based on the level of assistance needed, with total functional independence calculated by summing scores. Higher FIM scores imply higher independence (the highest score of 126 means independent). The FIM was given preoperatively and at 1 year to assess the changes in daily functional status [14].
- Caregiver Burden Scale (CBS): A 22-item questionnaire measuring the perceived burden on caregivers of chronically disabled individuals. Total CBS scores range from 0 to 95, with higher scores indicating more significant caregiver stress/burden. (For context, scores 0–20 reflect little to no burden, 21–40 mild-to-moderate burden, 41–60 moderate-to-severe burden, and above 60 severe burden.) Caregivers (usually a parent or family member) completed the CBS before surgery and at the 1-year follow-up to assess any change in caregiver-reported burden [15].
2.3. Statistical Analyses
All data analyses were performed using IBM SPSS Statistics (version 20.0 for Windows). Descriptive statistics were used to summarize patient demographics and clinical characteristics. Continuous variables are presented as mean ± standard deviation (SD) and, when appropriate, median (range). Categorical variables (e.g., GMFCS levels) are summarized as counts and percentages. The distribution of continuous data was evaluated with the Kolmogorov-Smirnov test to determine the appropriateness of parametric testing. For normally distributed continuous outcomes (e.g., BFM-DRS total score, FIM, and CBS scores), paired two-tailed t-tests were used to compare preoperative and 1-year postoperative values within the same patients. Appropriate non-parametric tests were planned for non-normally distributed or ordinal data (for example, a Wilcoxon signed-rank test for paired ordinal GMFCS levels). Statistical significance was defined as p < 0.05 for all analyses. All results are reported with corresponding p-values. No adjustments were made for multiple comparisons, given the exploratory nature of this small case series.
3. Results
3.1. Patient Characteristics
Eleven patients with dystonic cerebral palsy (8 females and three males) were included in the analysis. The mean age at the last follow-up was 30.1 years (range 19–44 years, SD not available from records), and the mean age at the time of DBS surgery was 24.6 years. All patients received bilateral GPi lead implantation for chronic high-frequency stimulation. No postoperative complications (such as hemorrhage, infection, or hardware-related issues) were observed in any of the 11 patients during the follow-up period. The clinical subtype of CP was dyskinetic in all cases, with diagnoses described as dystonic CP often accompanied by choreoathetosis or mixed tone abnormalities. Most patients had quadriplegic involvement (all four limbs were affected). Detailed demographic and clinical characteristics of the cohort are presented in Table 1.
3.2. Clinical Outcomes at 1-Year Post-DBS Follow-Up
At the 1-year follow-up, dystonia severity and functional independence had significantly improved. On the mean total BFM-DRS dystonia severity score, the preoperative score was 69.6 ± 27.6, which was reduced considerably to 54.3 ± 36.5 at 1 year postoperatively; this reduction corresponds to a mean average of a decrease of about 22% of the severity of patient dystonia. This improvement in BFM-DRS was significant (p = 0.001). Similarly, the functional independence (FIM) mean score increased from a preoperative 65.3 ± 33.9 to 79.2 ± 43.4 at 1 year. Translating this into functional independence corresponds to approximately a 21% gain (p = 0.006). These findings show significant improvements in dystonia and daily living activities one year from GPi-DBS. Figure 1 and Figure 2 show the individual and mean improvements in BFM-DRS and FIM scores before and after DBS, respectively [Figure 1 and Figure 2]. Table 2 summarizes individual patients’ pre- and post-DBS scores and the percentage improvement in these scores [Table 1].
In contrast to the marked changes in dystonia and independence, gross motor function as classified by the GMFCS showed no significant overall change at the 1-year evaluation. Seven out of 11 patients remained at the same GMFCS level as before surgery, while four patients improved by one level (for example, from level V to IV or IV to III). No patient’s GMFCS level worsened after DBS. Statistical analysis of the paired GMFCS levels pre- vs. post-DBS did not reach significance (p = 0.125). Thus, although a few patients moved to a better GMFCS level, the improvement in gross motor function did not achieve significance for the group. This outcome likely reflects the course, ordinal nature of the GMFCS, and the short-term follow-up period, in contrast to the more fine-grained continuous measures of dystonia and independence. Changes in each patient’s GMFCS (baseline vs. 1 year) are also presented in Table 2.
Finally, caregiver burden demonstrated a modest but statistically significant reduction following DBS. Two patients in the cohort were largely independent and did not require a dedicated caregiver at baseline; therefore, caregiver burden was assessed for the remaining nine patients with routine caregivers. Among these patients, the mean Caregiver Burden Scale (CBS) score improved from 35.7 ± 18.8 preoperatively to 32.0 ± 17.1 at 1 year postoperatively (p = 0.015). Lower CBS scores indicate less perceived burden, representing a favorable decrease in caregiver burden. In practical terms, the average caregiver burden shifted from the “mild-to-moderate” range preoperatively toward the lower end of that range at one year (based on CBS categorical interpretation). This finding suggests that improvements in the patient’s dystonia and functional status translated into slightly reduced strain on their caregivers.
Overall, bilateral GPi-DBS was associated with significant improvements in dystonia severity and patient functional abilities at 1 year and a measurable reduction in caregiver burden in this series of patients with dystonic CP. The key outcome data are summarized in Table 2. All patients continued to be monitored beyond 1 year (up to 5 years in some cases), and the therapeutic benefits observed at 12 months appeared to be maintained in those with longer follow-ups (details of long-term outcomes to be reported separately).
4. Discussion
Bilateral GPi-DBS led to a meaningful reduction in dystonia severity and improved functional independence in our cohort of adults with dystonic CP. The average BFMDRS score decreased by ~22%, indicating a substantial amelioration of dystonic movements at 1 year. This magnitude of improvement aligns with prior reports on DBS in secondary dystonia. For example, Vidailhet et al. found a 24.4% reduction in dystonia severity at 1 year in adults with choreoathetosis CP [16]. A meta-analysis by Koy et al. similarly demonstrated a 23.6% mean improvement in BFMDRS motor scores across 68 patients with dyskinetic CP [17]. Our results corroborate these findings, reinforcing that GPi-DBS can significantly lessen dystonic burden even in long-standing, secondary forms of dystonia. Notably, the improved motor control in our patients translated to greater functional independence (FIM), suggesting that relief from dystonic posturing enabled better performance in daily activities. This finding is an encouraging outcome, as earlier studies have variably reported functional benefits – some observing only modest gains in disability scores (on the order of ~9% in one meta-analysis) [17]. The more marked FIM improvement in our series may reflect our use of a comprehensive independence measure and the adult age of our patients (who may better leverage improved motor function in daily living). It is also possible that focused rehabilitation and caregiver support post-DBS amplified these functional gains, an approach that merits further study.
Importantly, our study documented a significant reduction in caregiver burden one year after DBS. The mean Caregiver Burden Scale score fell by about 10%, indicating that caregivers perceived less strain in their daily support of the patients. Any decrease in this score is clinically meaningful, given that most caregivers of adults with DCP experience considerable physical, emotional, and social stress. The improvement in CBS can be interpreted as a downstream benefit of the patients’ enhanced independence and more manageable dystonia. With less severe dystonic posturing, patients required less constant positioning or manual help, and their improved ability to perform basic tasks likely lightened the caregivers’ workload. This finding extends the impact of DBS beyond the patients themselves, underscoring its value for the family or support network. While few prior studies have quantitatively assessed caregiver burden in dystonia, our results align with reports of better health-related quality of life in families following successful DBS. For instance, Vidailhet et al. noted significant gains in functional disability and mental health quality-of-life measures after GPi-DBS in dystonic CP [16]. Similarly, a recent pediatric series observed improvements in caregiver-reported quality of life (CPCHILD questionnaire) at longer-term follow-up in some DBS recipients [17]. Our data add to this literature by showing a measurable alleviation of caregiver stress. From a clinical perspective, this reinforces that improving the patient’s condition can have broad psychosocial benefits. It also highlights the importance of including caregiver-oriented outcomes in future DBS studies, as reduced burden may translate to better care and sustainability of home support for these individuals with chronic disability.
Our findings broadly align with previously published studies on DBS in secondary dystonia and specifically dystonic CP, though there are some differences in emphasis. Early pioneering work by Vidailhet and colleagues established that GPi-DBS can benefit patients with dystonic CP, with sustained dystonia reduction and functional gains observed in their multicenter pilot study [16]. Subsequent case series (mostly in pediatric populations) reported variable outcomes, from moderate improvements to occasional non-responders, reflecting the heterogeneous nature of DCP. A systematic review by Elia et al. highlighted this variability, noting that improvements ranged from ~1% to as high as 50% in the literature, depending on patient selection and outcome metrics [18]. Our cohort’s mean improvement (~22%) falls in the middle of that range, and importantly, every patient experienced at least some reduction in dystonia severity. Many groups have struggled to demonstrate significant gains using standard scales regarding functional outcomes. For example, the meta-analysis by Koy et al. found only a 9% mean improvement in BFMDRS disability scores after DBS in CP [17], and the recent prospective STIM-CP trial in children did not achieve significant changes in gross motor function or disability at 1 year despite reduction in dystonia [17]. Against this backdrop, our study’s significant FIM improvement and caregiver burden reduction is encouraging. They suggest that, at least for adult DCP patients, DBS coupled with appropriate postoperative management can yield tangible functional benefits. It should be noted that some of the best functional outcomes have been reported in those patients whose disability is largely dystonia-driven [19]. In other words, individuals without substantial spastic or ataxic components tend to gain more function from dystonia improvement. This principle may explain part of the variability across studies. In our series, although most patients had mixed CP subtypes (spastic-dystonic or choreoathetosis), they were selected for surgery based on prominent dystonic features, which might have predisposed them to better functional gains once dystonia was treated. Finally, regarding long-term efficacy, our follow-up is ongoing. Still, prior studies indicate that the benefits of GPi-DBS in secondary dystonia can be maintained for years and, in some cases, continue to increase with prolonged stimulation [16]. However, hardware-related issues (e.g., infections, lead replacements) are more frequently encountered in dystonic CP (primarily pediatric cases) than in primary dystonia, and this must be kept in mind when comparing outcomes across the literature [16].
Despite these encouraging results, this study has relevant limitations. First, the study is limited by its retrospective design and small sample size (n=11), and therefore, the strength of our conclusions is limited. In the absence of a parallel group of similar patients receiving non-intervention, it is impossible to rule out placebo effects or regression to the mean; however, the progressive course of disability in untreated dystonic CP makes spontaneous improvement an unlikely contributor to the significant gains achieved. Second, our cohort was heterogeneous in terms of age, CP subtype, and baseline function. Although everyone had dystonia, there were additional movement disorders (chorea, athetosis) or spasticities of varying degrees that may impact the outcome. The study might thus not reflect the nuances of how different DCP phenotypes respond to DBS. Third, although one-year follow-up is likely adequate to evaluate short-term results, it might prove insufficient to determine the lasting efficacy of the procedure for functional recovery or durability of improvement of dystonia. Dystonic cerebral palsy is lifelong; longer follow-up is needed to assess whether there is a sustained benefit or an even more progressive increase and to monitor for late complications or depletion of the stimulator battery. Finally, there are inherent limitations in the very outcome measures. The GMFCS, as previously described, may not be responsive to some regions of improvement; moreover, despite being novel in this cohort, the caregiver burden scale measures subjective perceptions that external factors may influence. Future studies should use a more comprehensive battery of assessments (including quality of life measures and goal attainment scales) to understand better the impact of DBS on patients’ lives.
Looking forward, our findings suggest several directions for future research. A priority is to conduct larger, prospective studies (ideally multicenter trials) to validate the benefits of GPi-DBS in dystonic CP under more controlled conditions [17]. Such studies should stratify patients by key factors – for example, degree of spasticity, presence of fixed contractures, or age at surgery – to identify which subgroups derive the most significant functional benefit. There is evidence that younger patients, or those with shorter duration of dystonia, respond better to DBS [20]. This evidence raises the question of whether DBS should be considered earlier during dystonic CP before decades of abnormal motor patterns lead to irreversible changes. Prospective trials could help establish an optimal window for intervention. Extended follow-up is also critical: assessments at 2-, 3-, or 5-year post-surgery would determine whether improvements plateau or continue to accrue with ongoing stimulation and rehabilitation. Long-term data will also inform us about the durability of hardware and any late-emerging adverse effects in this population (for instance, stimulation-induced hypokinesia or tolerance over time).
Additionally, future research may explore adjunctive therapies to maximize outcomes. Combining DBS with intensive postoperative physiotherapy or novel neurorehabilitation approaches (such as task-specific training, neurofeedback, or adaptive devices) might facilitate more significant gains in gross motor function – essentially leveraging the more favorable neuromuscular state created by DBS. Some authors have advocated a more “dynamic” approach to treating this static encephalopathy, including investigating alternative neuromodulation targets. There is ongoing interest in targeting cerebello-thalamic pathways (e.g., the ventral thalamus or even cerebellar outflow tracts) instead of, or in addition to, pallidal stimulation for secondary dystonia [21]. While GPi remains the standard target with the most evidence, future trials could evaluate whether tailored targeting (perhaps multi-target DBS or directional leads) offers superior control of CP’s complex dystonic–dyskinetic movements. Finally, systematic studies on caregiver and family outcomes are warranted. The reduction in caregiver burden we observed is encouraging, and it would be valuable to confirm this in larger samples and to investigate the ripple effects (for example, on caregivers’ health, psychosocial status, and ability to maintain employment). Such data could strengthen the health-economic case for DBS in severe dystonic CP by demonstrating benefits beyond the patient.
5. Conclusions
This study demonstrates that bilateral GPi deep brain stimulation is a safe and effective treatment for adults with dystonic cerebral palsy, offering significant improvements in dystonia severity, functional independence, and caregiver burden. While gross motor function, as classified by GMFCS, remained unchanged over the first year, the marked gains in patient autonomy and caregiver strain reduction underscore DBS’s real-world impact beyond motor symptom control. These findings support the integration of GPi-DBS into the multidisciplinary management of pharmacoresistant dystonic CP and highlight the importance of comprehensive outcome evaluation—including both patient- and caregiver-centered measures. Future prospective, multicenter studies with longer follow-up are warranted to define further optimal patient selection, long-term efficacy, and the potential role of adjunctive therapies in maximizing outcomes for this complex population.
Author Contributions
Conceptualization: Hatice Ömercikoğlu Özden, Nazlı Durmaz Çelik, Özge Gönül Öner. Data curation: Hatice Ömercikoğlu Özden, Nazlı Durmaz Çelik, Formal analysis: Hatice Ömercikoğlu Özden, Nazlı Durmaz Çelik, Investigation: Hatice Ömercikoğlu Özden, Nazlı Durmaz Çelik, Özge Gönül Öner. Methodology: Hatice Ömercikoğlu Özden, Nazlı Durmaz Çelik. Supervision: Serhat Özkan, Dilek İnce Günal, Fatih Bayraklı, Murat Vural. Writing-original draft: Hatice Ömercikoğlu Özden, Nazlı Durmaz Çelik. Writing-review and editing: Serhat Özkan, Dilek İnce Günal, Fatih Bayraklı, Murat Vural.
Funding
Sources The authors have no funding to disclose.
Data Availability Statement
The datasets generated during and/or analyzed during the current study are available from the corresponding author upon reasonable request..
Conflicts of Interest
The authors have no conflicts of interest to disclose.
References
- Lewis, S.A., et al., Evolving understanding of CP phenotypes: the importance of dystonia. Pediatr Res, 2024.
- Loutou, A., et al., Social support, depression, and quality of life among parents of children with cerebral palsy in Benin, West Africa: a cross-sectional case-control study. Int J Rehabil Res, 2025.
- Kondekar, A., Q. Ansari, and H. Ghatol, The quality of life of primary caretakers of children with cerebral palsy. J Family Med Prim Care, 2024. 13(10): p. 4457-4461.
- Ozkan, Y., Child’s quality of life and mother’s burden in spastic cerebral palsy: a topographical classification perspective. J Int Med Res, 2018. 46(8): p. 3131-3137.
- Lumsden, D.E., et al., Pharmacological management of abnormal tone and movement in cerebral palsy. Arch Dis Child, 2019. 104(8): p. 775-780.
- Li, S., et al., Management Approaches to Spastic Gait Disorders. Muscle Nerve, 2025.
- Vitrikas, K., H. Dalton, and D. Breish, Cerebral Palsy: An Overview. Am Fam Physician, 2020. 101(4): p. 213-220.
- Aisen, M.L., et al., Cerebral palsy: clinical care and neurological rehabilitation. Lancet Neurol, 2011. 10(9): p. 844-52.
- Bronte-Stewart, H., et al., Inclusion and exclusion criteria for DBS in dystonia. Mov Disord, 2011. 26 Suppl 1: p. S5-16.
- Elia, A.E., et al., Deep brain stimulation for dystonia due to cerebral palsy: A review. Eur J Paediatr Neurol, 2018. 22(2): p. 308-315.
- Bohn, E., et al., Pharmacological and neurosurgical interventions for individuals with cerebral palsy and dystonia: a systematic review update and meta-analysis. Dev Med Child Neurol, 2021. 63(9): p. 1038-1050.
- Burke, R.E., et al., Validity and reliability of a rating scale for the primary torsion dystonias. Neurology, 1985. 35(1): p. 73-7.
- Morris, C. and D. Bartlett, Gross Motor Function Classification System: impact and utility. Dev Med Child Neurol, 2004. 46(1): p. 60-5.
- Kidd, D., et al., The Functional Independence Measure: a comparative validity and reliability study. Disabil Rehabil, 1995. 17(1): p. 10-4.
- Teriö, M., et al., Preventing frailty with the support of a home-monitoring and communication platform among older adults-a study protocol for a randomised-controlled pilot study in Sweden. Pilot Feasibility Stud, 2022. 8(1): p. 190.
- Vidailhet, M., et al., Bilateral pallidal deep brain stimulation for the treatment of patients with dystonia-choreoathetosis cerebral palsy: a prospective pilot study. Lancet Neurol, 2009. 8(8): p. 709-17.
- Koy, A., et al., Effects of deep brain stimulation in dyskinetic cerebral palsy: a meta-analysis. Mov Disord, 2013. 28(5): p. 647-54.
- Poulen, G., et al., Deep Brain Stimulation and Hypoxemic Perinatal Encephalopathy: State of Art and Perspectives. Life (Basel), 2021. 11(6).
- Cif, L., Deep brain stimulation in dystonic cerebral palsy: for whom and for what? Eur J Neurol, 2015. 22(3): p. 423-5.
- Lin, J.P., et al., The impact and prognosis for dystonia in childhood including dystonic cerebral palsy: a clinical and demographic tertiary cohort study. J Neurol Neurosurg Psychiatry, 2014. 85(11): p. 1239-44.
- San Luciano, M., et al., Thalamic deep brain stimulation for acquired dystonia in children and young adults: a phase 1 clinical trial. J Neurosurg Pediatr, 2021. 27(2): p. 203-212.
Figure 1.
BFM-DRS Scale Results Before DBS and at the End of the First Year.
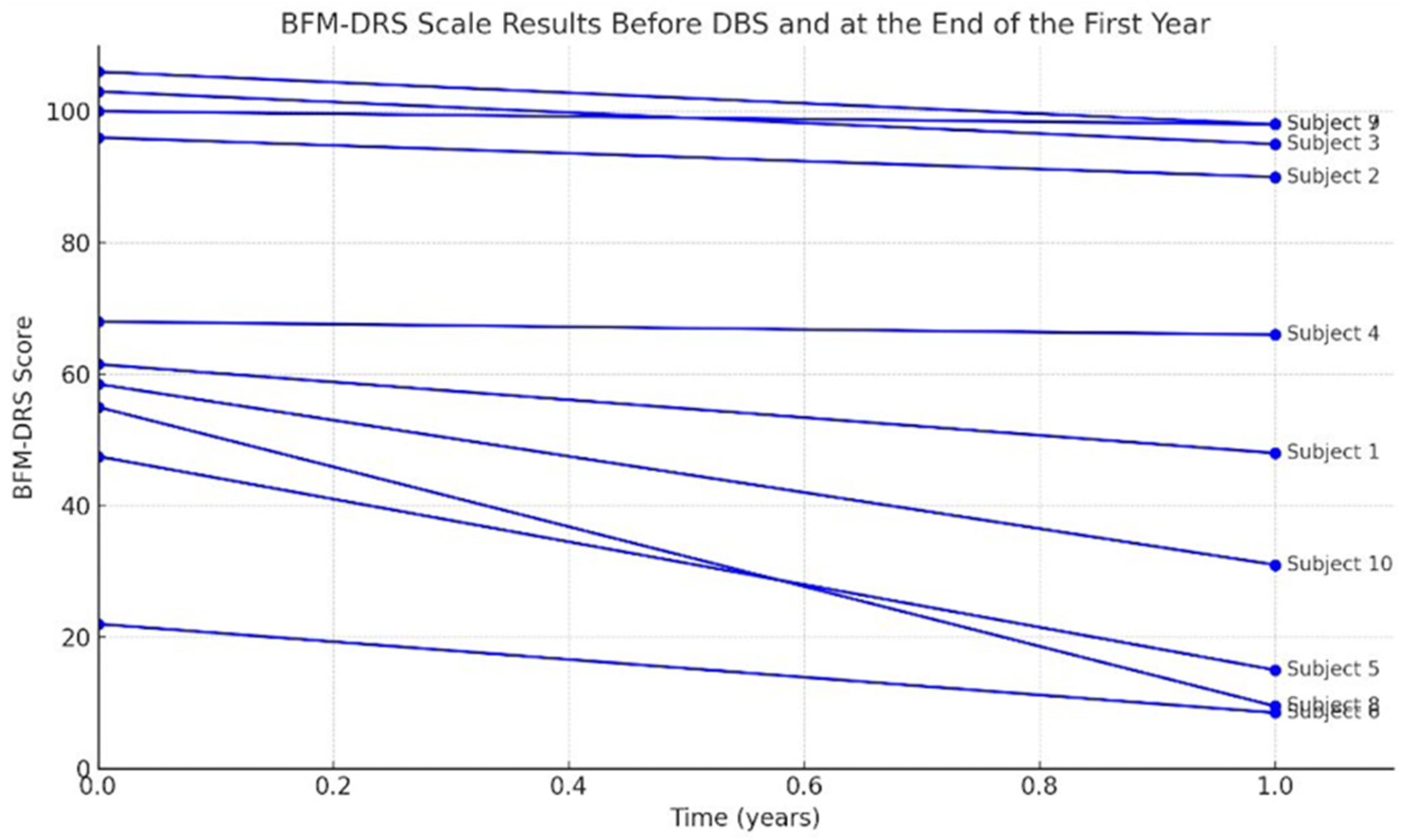
Figure 2.
FIS Results Before DBS and at the End of the First Year.
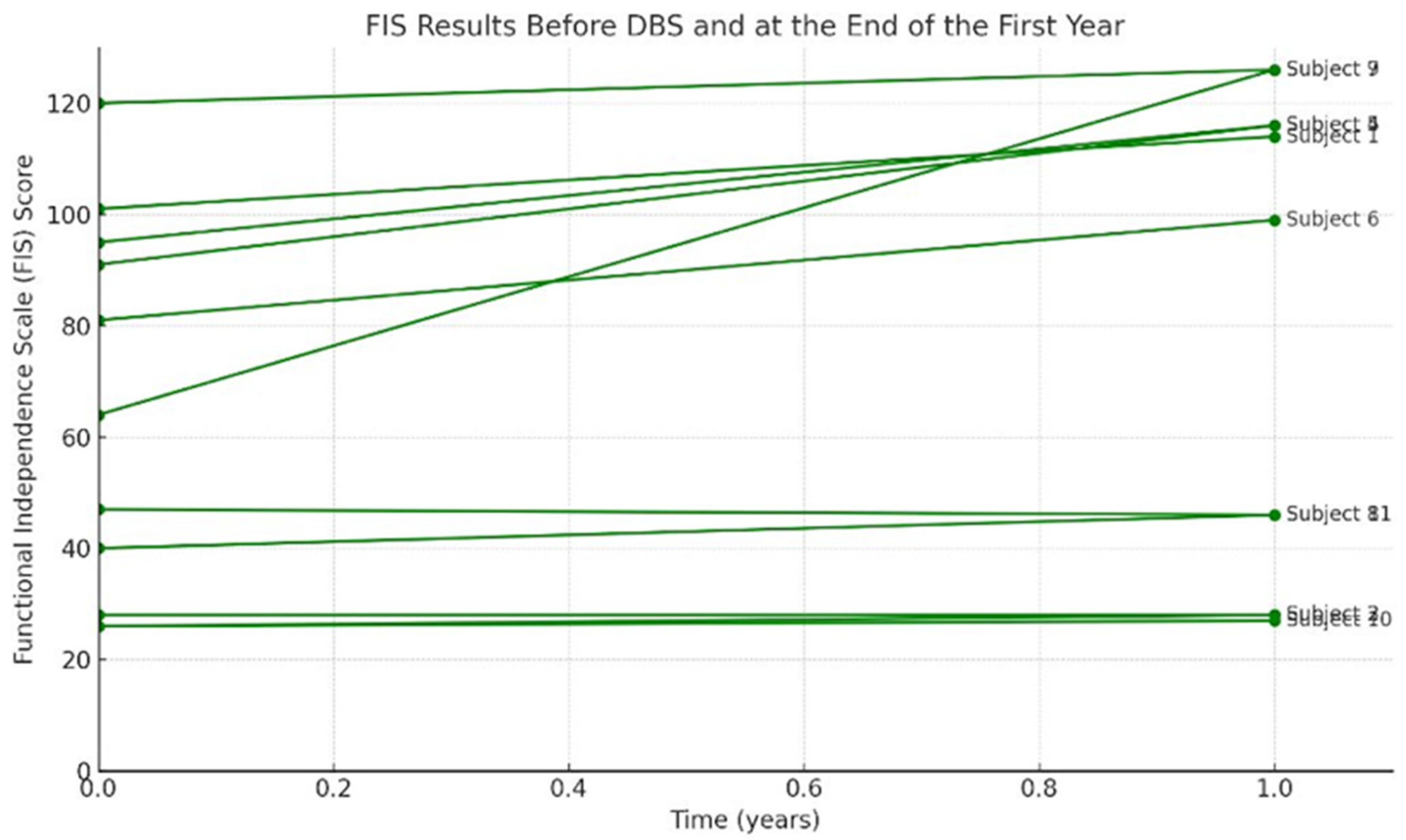

Table 1.
Demographic and clinical characteristics of the patients.
|
Patient No |
Sex | Age during op | Age | CP clinical type | CP involvement pattern |
|---|---|---|---|---|---|
| 1 | F | 21 | 23 | chorea-atetoid, dystonic | Quadriplegia |
| 2 | F | 21 | 23 | mix | Quadriplegia |
| 3 | F | 19 | 21 | chorea-atetoid, dystonic | Quadriplegia |
| 4 | M | 55 | 59 | dyskinetic | Quadriplegia |
| 5 | M | 33 | 37 | mix | Diplegia |
| 6 | F | 34 | 39 | mix | Diplegia |
| 7 | F | 32 | 39 | mix | Quadriplegia |
| 8 | M | 7 | 16 | mix | Quadriplegia |
| 9 | F | 21 | 38 | dystonic | Quadriplegia |
| 10 | F | 6 | 9 | dystonic | Quadriplegia |
| 11 | F | 22 | 28 | mix | Quadriplegia |
Table 2.
Changes in on Burke-Fahn-Marsden Dystonia Rating Scale (BFMDRS) , Functional Independence Scale (FIS) and Gross Motor Function Classification System (GMFCS) at baseline and 1 years after deep brain stimulation.
Table 2.
Changes in on Burke-Fahn-Marsden Dystonia Rating Scale (BFMDRS) , Functional Independence Scale (FIS) and Gross Motor Function Classification System (GMFCS) at baseline and 1 years after deep brain stimulation.
| Patient No | CP-Clinical Type | BFMDRS preop | BFMDRS postop 1 year | Improvement (%) |
FIS preop | FIS postop | Improvement (%) |
GMFCS preop | GMFCS postop |
|---|---|---|---|---|---|---|---|---|---|
| 1 | Chorea-atetoid, dystonic | 61,5 | 48 |
21.9 |
101 | 114 |
11.4 |
2 | 1 |
| 2 | mix | 96 | 90 | 6.25 | 26 | 28 | 7.1 | 5 | 5 |
| 3 | chorea-atetoid, dystonic | 103 | 95 |
7.7 |
28 | 28 |
0 |
5 | 5 |
| 4 | dyskinetic | 68 | 66 | 2.9 | 91 | 116 | 24.1 | 2 | 2 |
| 5 | mix | 47,5 | 39 | 17.8 | 95 | 116 | 18.1 | 2 | 2 |
| 6 | mix | 48,5 | 15 | 69 | 81 | 99 | 18.1 | 2 | 1 |
| 7 | mix | 22 | 8,5 | 60 | 120 | 126 | 4.7 | 1 | 1 |
| 8 | mix | 100 | 98 | 2 | 47 | 46 | -2.1 | 5 | 5 |
| 9 | dystonic | 55 | 9,5 | 82.7 | 64 | 126 | 49.2 | 3 | 1 |
| 10 | dystonic | 106 | 98 | 7.5 | 26 | 27 | 3.7 | 5 | 5 |
| 11 | mix | 58,5 | 31 | 47 | 40 | 46 | 13 | 4 | 3 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



