
Submitted:
16 October 2024
Posted:
17 October 2024
You are already at the latest version
Abstract
Objectives: To evaluate the possible long-term cerebral deposition of amyloid-β in PD patients treated with subthalamic nucleus deep brain stimulation (STN-DBS) and its possible influence on axial and cognitive variables. Methods: Consecutive PD patients treated with bilateral STN-DBS with a long-term follow-up were included. Amyloid-β deposition was evaluated postoperatively through a 18F-flutemetamol positron emission tomography (PET) study. Axial symptoms have been assessed using a standardized clinical-instrumental approach. Speech was assessed by perceptual and acoustic analysis while gait by means of the instrumented timed up and go test (iTUG). Motor severity was evaluated applying the UPDRS part III score and subscores while cognitive functions through a complete neuropsychological assessment. Different stimulation and drug conditions were assessed: on-stimulation/off-medication, off-stimulation/off-medication, on-stimulation/on-medication conditions (single and dual task). Results: 19 PD patients (male: 11; age: 63.52 years; on-stimulation/on-medication UPDRS-III: 17.05) with a five-year postoperative follow-up were included. Amyloid-β deposition was found in 21% of patients (4/19) with a prevalent involvement of prefrontal, limbic and parietal areas. Compared with patients without amyloid-β deposition, PD patients with positive 18F-flutemetamol PET study showed higher preoperative UPDRS-I (p=.037) score and lower postoperative Raven's matrices scores (p=.05). Conclusions: Our results suggest that in the long-term after STN-DBS a significant percentage of PD patients may present brain amyloid-β deposition. However, larger samples are needed to evaluate the possible role of amyloid-β deposition in the development of axial and cognitive alterations after surgery.
Keywords:
amyloid-β
; axial
; cognitive
; Deep Brain Stimulation
; Flutemetamol
; Parkinson’s Disease
; STN-DBS
1. Introduction
Subthalamic nucleus deep brain stimulation (STN-DBS) represents a short- and long-term effective treatment in advanced Parkinson’s disease (PD).[1,2] STN-DBS allows a stable improvement of motor complications, tremor and rigidity with a less relevant effect on axial symptoms (i.e., gait and balance symptoms, speech and swallowing troubles) and cognitive decline, the main causes of long-term disability[3,4,5]. Many studies have analysed axial symptoms in PD patients with an instrumental approach focusing only on gait and postural alterations or speech disturbances. The very few studies that have instrumentally assessed the whole spectrum of axial symptoms in PD have shown the presence of similarities between spatial-temporal gait and speech parameters[6]. Anatomopathological data have confirmed that the neurodegeneration of central dopaminergic pathways, considered the hallmark of PD, is accompanied by a contemporary involvement of other neurotransmitter pathways (i.e., cholinergic, serotoninergic)[7,8,9]. The prevalent involvement of the cholinergic system could be associated with a clinical “cholinergic” phenotype dominated by axial symptoms, cognitive deterioration and cerebral Amyloid-β (Aβ) deposition[10,11]. Based on these premises, the objective of this study was to evaluate the possible long-term cerebral deposition of amyloid-β in a cohort of PD patients treated with STN-DBS and its possible influence on axial and cognitive variables.
2. Materials and Methods
2.1. Participants
This longitudinal cohort study included consecutive PD patients treated with bilateral STN-DBS from 2012 to 2017 at the Neurological Unit of the Ospedale Civile Baggiovara (OCB) University Hospital. All patients fulfilled the diagnosis of PD according to the UK Brain Bank criteria[12] and suffered from disabling motor complications not well controlled with oral medication at the time of surgery. Exclusion criteria were previously published[13]. The study (BASCOSTIM-PD) was approved by the local ethics committee (protocol number: 2019/0056629), and written informed consent was obtained from participants according to the Declaration of Helsinki[14].
2.2. Clinical Assessment
Neurological evaluation, instrumental analysis of gait and acoustic-perceptual assessment of speech were performed in a single day in the following conditions: on-stimulation/off-medication (washout of at least 12-h of dopaminergic medication)[15]; off-stimulation/off-medication (stimulation was temporarily turned off for at least 1-h); on-stimulation/on-medication (stimulation was turned on and dopaminergic therapy was administered [early morning levodopa equivalent daily dose (LEDD) plus 30%]). Disease severity was quantified through the Unified Parkinson’s Disease Rating Scale (UPDRS) part III and the Hoehn and Yahr (H&Y) stage. The following subscores were extrapolated from the UPDRS total motor scale: tremor, postural instability/gait disorders (PIGD) and akinesia subscores[4,13,16]. The PD motor phenotype of each patient (PIGD, indeterminate or tremor dominant [TD])was also calculated[17]. All patients underwent a detailed neuropsychological assessment before surgery and at long-term evaluation including phonemic fluency, spatial perception (localization of numbers), Raven’s progressive matrices, Stroop test and Trail making test part B[5]. In addition all patients were classified as PD without dementia, PD–mild cognitive impairment (PD-MCI) and dementia associated with PD (PDD) based on current criteria[18,19]. All patients were screened for the presence of mutations in the α-synuclein, parkin, glucocerebrosidase-1 (GBA1) and leucine-rich repeat kinase-2 genes[20,21,22]. The total amount of dopaminergic medications per day was calculated as LEDD milligrams[23].
2.3. Instrumental Analysis of Gait
The instrumental gait evaluation of gait was carried out with a wearable inertial sensor secured with an elastic belt at the sacrum level (S1). The commercial device G-WALK (BTS BioengineeringTM, sampling frequency 100 Hz) was used. This device contains a three-dimensional (3D) accelerometer, gyroscope and magnetometer providing, respectively, the 3D linear acceleration, angular velocity, and magnetic field vector. Each patient performed the instrumented Timed Up and Go test (iTUG)[24] in the different stimulation and medication conditions reported above. In each condition, the patient was asked to perform the test three consecutive times, to obtain a total of twelve acquisitions. The iTUG test was performed using the standard test procedure[25] and videotaped. Data processing has been previously published[4,13]. The following variables were then extracted: the overall duration of the iTUG; the duration of each phase; the root mean square (RMS) of trunk acceleration for each phase; the maximum speed of rotation of the trunk about the cranio-caudal axis (which is related to the subject’s ability to rotate quickly).
2.4. Speech Analysis
Patients’ speech was recorded in a silent environment, using a digital device kept 20 cm from the patient’s lips.[13,16] The following tasks were performed by the patients: spontaneous speech for one minute; sustained production of the phoneme /a/ for as long as possible, performed three times (duration [sec], intensity [dB]); reading of 25 recorded words (word intelligibility calculated as the percentage of words correctly spelt by the patient)[26]; counting from 1 to 20 (speech rate [syllables/second]); oral diadochokinesis, during which participants produced the syllables /pa/, /ta/, /ka/ and the pseudoword /pataka/, as fast as they could with habitual pitch and loudness (parameters estimated; irregular rhythm [presence of absence], uncontrolled acceleration [presence of absence]). These parameters were selected according to recent guidelines[27] because they represent acoustic characteristics involved in hypokinetic dysarthria[28,29]. The perceptual-acoustic analysis was blinded to the patient’s condition using Praat software[30].
2.5. [18F] Flutemetamol PET Study
Each patient underwent a [18F] flutemetamol positron emission tomography (PET) with the aim to quantify cerebral Aβ deposition. PET data has been elaborated with CortexID Suite (GE Healthcaretm) software which allows a fully automated quantification of beta amyloid brain deposition in different predefined cortical and subcortical regions and the comparison with normal databases of healthy controls allowing obtaining uptake ratio and z-score values.
2.6. Statistical Analysis
Descriptive statistics were performed for each parameter; continuous variables were expressed as mean (standard deviation [sd]) and median (range) while frequencies and percentages were calculated for categorical variables. The variables were tested for normal distribution using the Kolmogorov-Smirnov test. The primary objective of the study was to find the prevalence of PD patients with a positive [18F] Flutemetamol PET study, indicative of brain Aβ deposition, in the long-term after surgery. We classify the [18F] Flutemetamol PET study as positive if it shows the presence of at least one cortical or subcortical area with a z-score >2 assessed with the CortexID Suite. The secondary objective of the study was to find the presence of significant differences in clinical and demographic variables between patients with and without brain Aβ deposition. Considering that most variables were not normally distributed, with regards to continuous and ordinal variables, the Mann–Whitney test was used, while for categorical variables the chi-square independence test was applied. Statistical analyses were performed using IBM SPSS Statistics software for Windows version 20.0 (IBM, Armonk, NY, USA) and Matlab® (The MathWorks Inc., Thorofare, USA). Alpha value was set to 0.05, thus p-values <0.05 were considered statistically significant.
3. Results
From 2012 to 2017, 40 PD patients underwent STN-DBS. Of these, 21 subjects were excluded from the analysis because of missing data (eleven patients), lack of PET study (six patients) and lack of consent to participate (four patients). The remaining 19 PD patients (male:11; age:63.52 years; on-stimulation/on-medication UPDRS-III:17.05) with a mean five-year postoperative follow-up were included. Genetic assessment revealed heterozygous mutation in the GBA1 gene in three patients. Table 1 shows the demographic and clinical characteristics of the patients while Table 2 reports motor scores and subscores in the different conditions tested. A detailed description of speech and cognitive variables is reported in Supplementary Table 1.
Amyloid-β deposition was found in 21% of patients (4/19) with a prevalent involvement of prefrontal, limbic and parietal areas. In particular, both right and left lateral temporal cortex were involved in the four patients; right prefrontal cortex in three; anterior cingulate gyrus, left prefrontal, parietal cortex and left precuneus in two; left occipital and right precuneus in one (see Figure 1).
Compared with patients without amyloid-β deposition, PD patients with positive 18F-flutemetamol PET study showed higher preoperative UPDRS-I (p=.037) score. Table 3 summarizes the main demographic and clinical characteristics of PET positive and PET negative cohorts. No differences were found in instrumental speech and gait variables.
4. Discussion
In our cohort, a significant proportion of PD patients (i.e., 21%) showed the presence of amyloid-β deposition at [18F] Flutemetamol PET study. This is in line with previous studies, which have reported a 20-30% prevalence of positive amyloid PET scans in non-demented PD and MCI-PD[31,32] suggesting that STN-DBS does not seem to promote amyloid deposition, although a possible selection bias should be taken into account (PD patients with cognitive impairment or severe axial symptoms are usually excluded from surgery). In particular one study which included multicenter data from the Parkinson’s Progression Marker Initiative (PPMI) found 10/48 (21%) amyloid positive PD patients[32] assessed with [18F]florbetaben PET scanning[32]. Interestingly the increased widespread cortical and subcortical [18F]florbetaben uptake was associated with poorer performance on global cognition (assessed with the Montreal Cognitive Assessment[MOCA]) and impaired performance on Symbol Digit Modality test (SDMT) which is linked to attention, visual scanning, and motor speed[32]. Another study has assessed brain amyloid-β deposition in twenty-five MCI-PD patients through [18F] Flutemetamol PET study, reporting a 32% rate (8/25) of amyloid PET positivity[31]. Even in this case MCI-PD amyloid-β + showed worse performance in the overall executive domain but not in motor abilities compared to amyloid negative patients. This result was also found in our cohort. However it is important to keep in mind that the previously mentioned overall prevalence of PET-positive scans in PD patients (20-30%) was in the range of literature age-matched control population suggesting that the possible causative role of PD in amyloid-β deposition needs further confirmation in larger samples[33]. This does not detract from the fact that amyloid-β deposition can negatively influence the clinical phenotype in PD patients particularly regarding axial and cognitive domains. The dysfunction of the cholinergic circuits due to the diffusion of the neurodegenerative process at the level of the peduncolo-pontine nucleus, thalamus, basal nucleus of Meynert and associated cortical cholinergic projections, represents one of the main neuropathological substrates of axial disorders in PD[8,11]. Indeed, this cholinergic phenotype would be associated with a PIGD motor phenotype associated with FOG in the ON medication condition and cognitive impairment[34]. This hypothesis was also confirmed by Muller et al., who found a correlation between the presence of cortical cholinergic denervation evaluated by PET with tracer for acetylcholinesterase ([(11) C] PMP) and the presence of RBD, falls, walking disorders and cognitive dysfunctions[35]. Furthermore, comparing PD-fallers vs PD non-fallers another group found that acetylcholinesterase levels (indirect markers of cholinergic denervation) at the pedunculopontine nucleus and basal nucleus of Meynert (the two main cerebral cholinergic centers) were significantly lower in the fallers subgroup regardless of the degree of dopaminergic denervation[36]. A subsequent link between axial features, cholinergic system and amyloid-β was found by Bohnen et al. who analyzed the correlation between cortical cholinergic denervation, beta-amyloid deposition, and FOG. The results of the study conducted on 143 patients showed a direct correlation between the presence of FOG, the degree of cholinergic denervation and the deposition of beta-amyloid at cortical level[8]. The frequency of FOG was also higher in subjects who had both cholinopathy and amyloidopathy at neo-cortical level. 90% of patients with FOG also had at least one of the two pathological conditions[8]. Different cross-sectional studies have also confirmed the correlation between beta-amyloid and the PIGD motor phenotype[37,38]. Alves et al. found significantly lower cerebrospinal fluid (CSF) levels of Aβ42, Aβ38, Aβ42/40 and Aβ38/40 in patients with the PIGD phenotype compared to the tremor dominant phenotype. Multivariate regression analyses documented a significant association between CSF beta-amyloid levels, severity of the PIGD motor phenotype, and lower limb bradykinesia[37]. A subsequent prospective study has confirmed that low CSF levels of Aβ42 in the early stages of the disease are predictive of the development of dopa-resistant gait disturbances (variability of gait duration, variability of gait length) with a three-years follow-up[39]. However, in our cohort, no differences were found in the instrumentally assessed axial symptoms between PET positive and PET negative cohort. This is probably due to the small sample size, supporting the need for larger samples of DBS PD patients. On the contrary, in our cohort, PD patients with positive 18F-flutemetamol PET study showed higher preoperative UPDRS-I score than patients without amyloid-β deposition. This means that PET positive patients had a higher cognitive, behavioural, and humoral burden before surgery (quantified through the UPDRS-I score). Focusing on the specific cortical and subcortical brain areas in which amyloid-β deposition was found, the involvement of lateral temporal cortices is not surprising. Indeed, a previous prospective study which included a small cohort of healthy-controls (n=6), PD without dementia (n=16), and 8 PDD studied with [18F]FDDNP PET scan reported that a higher baseline lateral temporal binding was associated with longitudinal worsening in cognitive performances and progression to dementia among subjects classified as PDND at baseline[40]. The involvement of prefrontal parietal and limbic cortices was also reported in a study by Garon et al., in particular with an increased Aβ uptake in frontal (i.e., middle frontal cortices and pars triangularis) and parietal regions (i.e., paracentral lobule and precuneus), which overall correlated with poor executive performance[31]. We have to keep in mind that our exploratory study has several limitations including the small sample size, which reduced the statistical power of our results, not allowing to perform correlation analyses between [18F] flutemetamol PET Z-scores and clinical/instrumental variables; the variability of the follow-up duration after surgery between the patients; the lack of preoperative [18F] flutemetamol PET study and finally the lack of CSF and ApoE data. However, it represents the first report of the prevalence of amyloid-β deposition in PD patients treated with STN-DBS assessed with a deep clinical instrumental approach focused on axial symptoms. Our results suggest that in the long-term after STN-DBS a significant percentage of PD patients may present brain amyloid-β deposition. Obviously future studies with larger samples and preoperative amyloid-β deposition assessment are needed to assess both the possible effect of DBS on amyloid-β deposition whatever it is (protective, worsening or irrelevant) and the possible role of amyloid-β deposition in the development of axial and cognitive alterations after surgery. If this is confirmed the assessment of amyloid-β deposition might be included in the preoperative workup to identify before the surgery the patients that already bring a higher risk of developing cognitive and axial alterations after STN-DBS.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org. Supplementary Table S1.
Author Contributions
Conceptualization, F.C., A.F., A.M., A.V., F.V.; data collection, F.C., A.F., A.A., I.C., A.M., A.G., V.F., M.A.M., G.D.R, F.A., V.R., A.F., R.S., B.D., S.S., L.C., B.E., C.M.G., G.B., G.P., M.L., C.B., Francesca.C., A.M., A.V., F.V.; methodology, F.C., A.F., A.M., F.V; formal analysis, F.C., A.M.; writing—original draft preparation, F.C., A.F.; writing—review and editing, F.C., A.F., A.M., A.V., F.V.; data collection, F.C., A.F., A.A., I.C., A.M., A.G., V.F., M.A.M., G.D.R, F.A., V.R., A.F., R.S., B.D., S.S., L.C., B.E., C.M.G., G.B., G.P., M.L., C.B., Francesca.C., A.M., A.V., F.V.; supervision, A.V., F.V.; all authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was approved by the local ethics committee (Area Vasta Emilia Nord, protocol number: 2019/0056629), and written informed consent was obtained from participants according to the Declaration of Helsinki.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data that support the findings of this study are available on request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.
Acknowledgments
This study was partially supported by the Italian Ministry of Health–Ricerca Corrente Annual Program 2024.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Bove, F.; Mulas, D.; Cavallieri, F.; Castrioto, A.; Chabardès, S.; Meoni, S.; Schmitt, E.; Bichon, A.; Di Stasio, E.; Kistner, A.; et al. Long-Term Outcomes (15 Years) After Subthalamic Nucleus Deep Brain Stimulation in Patients With Parkinson Disease. Neurology 2021, 10.1212/WNL.0000000000012246, doi:10.1212/WNL.0000000000012246. [CrossRef]
- Cavallieri, F.; Fraix, V.; Bove, F.; Mulas, D.; Tondelli, M.; Castrioto, A.; Krack, P.; Meoni, S.; Schmitt, E.; Lhommée, E.; et al. Predictors of Long-Term Outcome of Subthalamic Stimulation in Parkinson Disease. Ann Neurol 2021, 89, 587–597, doi:10.1002/ana.25994. [CrossRef]
- Zampogna, A.; Cavallieri, F.; Bove, F.; Suppa, A.; Castrioto, A.; Meoni, S.; Pélissier, P.; Schmitt, E.; Bichon, A.; Lhommée, E.; et al. Axial Impairment and Falls in Parkinson’s Disease: 15 Years of Subthalamic Deep Brain Stimulation. NPJ Parkinsons Dis 2022, 8, 121, doi:10.1038/s41531-022-00383-y. [CrossRef]
- Cavallieri, F.; Campanini, I.; Gessani, A.; Budriesi, C.; Fioravanti, V.; Di Rauso, G.; Feletti, A.; Damiano, B.; Scaltriti, S.; Guagnano, N.; et al. Long-Term Effects of Bilateral Subthalamic Nucleus Deep Brain Stimulation on Gait Disorders in Parkinson’s Disease: A Clinical-Instrumental Study. J Neurol 2023, doi:10.1007/s00415-023-11780-5. [CrossRef]
- Di Rauso, G.; Cavallieri, F.; Campanini, I.; Gessani, A.; Fioravanti, V.; Feletti, A.; Damiano, B.; Scaltriti, S.; Bardi, E.; Corni, M.G.; et al. Freezing of Gait in Parkinson’s Disease Patients Treated with Bilateral Subthalamic Nucleus Deep Brain Stimulation: A Long-Term Overview. Biomedicines 2022, 10, 2214, doi:10.3390/biomedicines10092214. [CrossRef]
- Cantiniaux, S.; Vaugoyeau, M.; Robert, D.; Horrelou-Pitek, C.; Mancini, J.; Witjas, T.; Azulay, J.-P. Comparative Analysis of Gait and Speech in Parkinson’s Disease: Hypokinetic or Dysrhythmic Disorders? J Neurol Neurosurg Psychiatry 2010, 81, 177–184, doi:10.1136/jnnp.2009.174375. [CrossRef]
- Bohnen, N.I.; Yarnall, A.J.; Weil, R.S.; Moro, E.; Moehle, M.S.; Borghammer, P.; Bedard, M.-A.; Albin, R.L. Cholinergic System Changes in Parkinson’s Disease: Emerging Therapeutic Approaches. The Lancet Neurology 2022, 21, 381–392, doi:10.1016/S1474-4422(21)00377-X. [CrossRef]
- Bohnen, N.I.; Frey, K.A.; Studenski, S.; Kotagal, V.; Koeppe, R.A.; Constantine, G.M.; Scott, P.J.H.; Albin, R.L.; Müller, M.L.T.M. Extra-nigral Pathological Conditions Are Common in Parkinson’s Disease with Freezing of Gait: An in Vivo Positron Emission Tomography Study. Movement Disorders 2014, 29, 1118–1124, doi:10.1002/mds.25929. [CrossRef]
- Sauerbier, A.; Jenner, P.; Todorova, A.; Chaudhuri, K.R. Non Motor Subtypes and Parkinson’s Disease. Parkinsonism & Related Disorders 2016, 22, S41–S46, doi:10.1016/j.parkreldis.2015.09.027. [CrossRef]
- Müller, M.L.T.M.; Frey, K.A.; Petrou, M.; Kotagal, V.; Koeppe, R.A.; Albin, R.L.; Bohnen, N.I. Β-amyloid and Postural Instability and Gait Difficulty in Parkinson’s Disease at Risk for Dementia. Movement Disorders 2013, 28, 296–301, doi:10.1002/mds.25213. [CrossRef]
- Kings Parcog groupMDS Nonmotor study group; Lim, E.W.; Aarsland, D.; Ffytche, D.; Taddei, R.N.; Van Wamelen, D.J.; Wan, Y.-M.; Tan, E.K.; Ray Chaudhuri, K. Amyloid-β and Parkinson’s Disease. J Neurol 2019, 266, 2605–2619, doi:10.1007/s00415-018-9100-8. [CrossRef]
- Hughes, A.J.; Daniel, S.E.; Kilford, L.; Lees, A.J. Accuracy of Clinical Diagnosis of Idiopathic Parkinson’s Disease: A Clinico-Pathological Study of 100 Cases. J Neurol Neurosurg Psychiatry 1992, 55, 181–184, doi:10.1136/jnnp.55.3.181. [CrossRef]
- Cavallieri, F.; Gessani, A.; Merlo, A.; Campanini, I.; Budriesi, C.; Fioravanti, V.; Di Rauso, G.; Feletti, A.; Damiano, B.; Scaltriti, S.; et al. Interplay between Speech and Gait Variables in Parkinson’s Disease Patients Treated with Subthalamic Nucleus Deep Brain Stimulation: A Long-term Instrumental Assessment. Euro J of Neurology 2023, 30, 1963–1972, doi:10.1111/ene.15803. [CrossRef]
- World Medical Association World Medical Association Declaration of Helsinki: Ethical Principles for Medical Research Involving Human Subjects. JAMA 2013, 310, 2191–2194, doi:10.1001/jama.2013.281053. [CrossRef]
- Defer, G.L.; Widner, H.; Marié, R.M.; Rémy, P.; Levivier, M. Core Assessment Program for Surgical Interventional Therapies in Parkinson’s Disease (CAPSIT-PD). Mov Disord 1999, 14, 572–584, doi:10.1002/1531-8257(199907)14:4<572::aid-mds1005>3.0.co;2-c. [CrossRef]
- Gessani, A.; Cavallieri, F.; Fioravanti, V.; Campanini, I.; Merlo, A.; Di Rauso, G.; Damiano, B.; Scaltriti, S.; Bardi, E.; Corni, M.G.; et al. Long-Term Effects of Subthalamic Nucleus Deep Brain Stimulation on Speech in Parkinson’s Disease. Sci Rep 2023, 13, 11462, doi:10.1038/s41598-023-38555-2. [CrossRef]
- Stebbins, G.T.; Goetz, C.G.; Burn, D.J.; Jankovic, J.; Khoo, T.K.; Tilley, B.C. How to Identify Tremor Dominant and Postural Instability/Gait Difficulty Groups with the Movement Disorder Society Unified Parkinson’s Disease Rating Scale: Comparison with the Unified Parkinson’s Disease Rating Scale. Mov Disord 2013, 28, 668–670, doi:10.1002/mds.25383. [CrossRef]
- Emre, M.; Aarsland, D.; Brown, R.; Burn, D.J.; Duyckaerts, C.; Mizuno, Y.; Broe, G.A.; Cummings, J.; Dickson, D.W.; Gauthier, S.; et al. Clinical Diagnostic Criteria for Dementia Associated with Parkinson’s Disease. Movement Disorders 2007, 22, 1689–1707, doi:10.1002/mds.21507. [CrossRef]
- Litvan, I.; Goldman, J.G.; Tröster, A.I.; Schmand, B.A.; Weintraub, D.; Petersen, R.C.; Mollenhauer, B.; Adler, C.H.; Marder, K.; Williams-Gray, C.H.; et al. Diagnostic Criteria for Mild Cognitive Impairment in Parkinson’s Disease: Movement Disorder Society Task Force Guidelines. Movement Disorders 2012, 27, 349–356, doi:10.1002/mds.24893. [CrossRef]
- Grisanti, S.; Ferri, L.; Cavallieri, F.; Fioravanti, V.; Vincenzi, C.; Toschi, G.; Grisendi, I.; Sabadini, R.; Paul, J.J.; Bauer, P.; et al. Increased Stroke Risk in Patients with Parkinson’s Disease with LRRK2 Mutations. Mov Disord 2022, 37, 1117–1118, doi:10.1002/mds.28996. [CrossRef]
- Skrahina, V.; Gaber, H.; Vollstedt, E.; Förster, T.M.; Usnich, T.; Curado, F.; Brüggemann, N.; Paul, J.; Bogdanovic, X.; Zülbahar, S.; et al. The Rostock International Parkinson’s Disease ( ROPAD ) Study: Protocol and Initial Findings. Movement Disorders 2021, 36, 1005–1010, doi:10.1002/mds.28416. [CrossRef]
- Westenberger, A.; Skrahina, V.; Usnich, T.; Beetz, C.; Vollstedt, E.-J.; Laabs, B.-H.; Paul, J.J.; Curado, F.; Skobalj, S.; Gaber, H.; et al. Relevance of Genetic Testing in the Gene-Targeted Trial Era: The Rostock Parkinson’s Disease Study. Brain 2024, 147, 2652–2667, doi:10.1093/brain/awae188. [CrossRef]
- Tomlinson, C.L.; Stowe, R.; Patel, S.; Rick, C.; Gray, R.; Clarke, C.E. Systematic Review of Levodopa Dose Equivalency Reporting in Parkinson’s Disease. Mov Disord 2010, 25, 2649–2653, doi:10.1002/mds.23429. [CrossRef]
- Palmerini, L.; Mellone, S.; Avanzolini, G.; Valzania, F.; Chiari, L. Quantification of Motor Impairment in Parkinson’s Disease Using an Instrumented Timed up and Go Test. IEEE Trans Neural Syst Rehabil Eng 2013, 21, 664–673, doi:10.1109/TNSRE.2012.2236577. [CrossRef]
- Zampieri, C.; Salarian, A.; Carlson-Kuhta, P.; Aminian, K.; Nutt, J.G.; Horak, F.B. The Instrumented Timed up and Go Test: Potential Outcome Measure for Disease Modifying Therapies in Parkinson’s Disease. J Neurol Neurosurg Psychiatry 2010, 81, 171–176, doi:10.1136/jnnp.2009.173740. [CrossRef]
- Cavallieri, F.; Budriesi, C.; Gessani, A.; Contardi, S.; Fioravanti, V.; Menozzi, E.; Pinto, S.; Moro, E.; Valzania, F.; Antonelli, F. Dopaminergic Treatment Effects on Dysarthric Speech: Acoustic Analysis in a Cohort of Patients With Advanced Parkinson’s Disease. Front Neurol 2020, 11, 616062, doi:10.3389/fneur.2020.616062. [CrossRef]
- Rusz, J.; Tykalova, T.; Ramig, L.O.; Tripoliti, E. Guidelines for Speech Recording and Acoustic Analyses in Dysarthrias of Movement Disorders. Movement Disorders 2021, 36, 803–814, doi:10.1002/mds.28465. [CrossRef]
- Skodda, S.; Visser, W.; Schlegel, U. Short- and Long-Term Dopaminergic Effects on Dysarthria in Early Parkinson’s Disease. J Neural Transm 2010, 117, 197–205, doi:10.1007/s00702-009-0351-5. [CrossRef]
- Rusz, J.; Bonnet, C.; Klempíř, J.; Tykalová, T.; Baborová, E.; Novotný, M.; Rulseh, A.; Růžička, E. Speech Disorders Reflect Differing Pathophysiology in Parkinson’s Disease, Progressive Supranuclear Palsy and Multiple System Atrophy. J Neurol 2015, 262, 992–1001, doi:10.1007/s00415-015-7671-1. [CrossRef]
- Boersma, P.; Weenink, D. Praat: Doing Phonetics by Computer [Computer Program]. Version 5.3.51. (2013).
- Garon, M.; Weis, L.; Fiorenzato, E.; Pistonesi, F.; Cagnin, A.; Bertoldo, A.; Anglani, M.; Cecchin, D.; Antonini, A.; Biundo, R. Quantification of Brain β-Amyloid Load in Parkinson’s Disease With Mild Cognitive Impairment: A PET/MRI Study. Front. Neurol. 2022, 12, 760518, doi:10.3389/fneur.2021.760518. [CrossRef]
- Fiorenzato, E.; Biundo, R.; Cecchin, D.; Frigo, A.C.; Kim, J.; Weis, L.; Strafella, A.P.; Antonini, A. Brain Amyloid Contribution to Cognitive Dysfunction in Early-Stage Parkinson’s Disease: The PPMI Dataset. JAD 2018, 66, 229–237, doi:10.3233/JAD-180390. [CrossRef]
- Roberts, R.O.; Aakre, J.A.; Kremers, W.K.; Vassilaki, M.; Knopman, D.S.; Mielke, M.M.; Alhurani, R.; Geda, Y.E.; Machulda, M.M.; Coloma, P.; et al. Prevalence and Outcomes of Amyloid Positivity Among Persons Without Dementia in a Longitudinal, Population-Based Setting. JAMA Neurol 2018, 75, 970, doi:10.1001/jamaneurol.2018.0629. [CrossRef]
- Titova, N.; Chaudhuri, K.R. Nonmotor Parkinson’s and Future Directions. In International Review of Neurobiology; Elsevier, 2017; Vol. 134, pp. 1493–1505 ISBN 978-0-12-812603-5.
- Müller, M.L.T.M.; Bohnen, N.I.; Kotagal, V.; Scott, P.J.H.; Koeppe, R.A.; Frey, K.A.; Albin, R.L. Clinical Markers for Identifying Cholinergic Deficits in Parkinson’s Disease. Movement Disorders 2015, 30, 269–273, doi:10.1002/mds.26061. [CrossRef]
- Perez-Lloret, S.; Barrantes, F.J. Deficits in Cholinergic Neurotransmission and Their Clinical Correlates in Parkinson’s Disease. npj Parkinson’s Disease 2016, 2, 16001, doi:10.1038/npjparkd.2016.1. [CrossRef]
- Alves, G.; Pedersen, K.F.; Bloem, B.R.; Blennow, K.; Zetterberg, H.; Borm, G.F.; Dalaker, T.O.; Beyer, M.K.; Aarsland, D.; Andreasson, U.; et al. Cerebrospinal Fluid Amyloid-Beta and Phenotypic Heterogeneity in de Novo Parkinson’s Disease. J. Neurol. Neurosurg. Psychiatry 2013, 84, 537–543, doi:10.1136/jnnp-2012-303808. [CrossRef]
- Kang, J.-H. Association of Cerebrospinal Fluid β-Amyloid 1-42, T-Tau, P-Tau 181 , and α-Synuclein Levels With Clinical Features of Drug-Naive Patients With Early Parkinson Disease. JAMA Neurol 2013, doi:10.1001/jamaneurol.2013.3861. [CrossRef]
- Rochester, L.; Galna, B.; Lord, S.; Yarnall, A.J.; Morris, R.; Duncan, G.; Khoo, T.K.; Mollenhauer, B.; Burn, D.J. Decrease in Aβ42 Predicts Dopa-Resistant Gait Progression in Early Parkinson Disease. Neurology 2017, 88, 1501–1511, doi:10.1212/WNL.0000000000003840. [CrossRef]
- Buongiorno, M.; Antonelli, F.; Compta, Y.; Fernandez, Y.; Pavia, J.; Lomeña, F.; Ríos, J.; Ramírez, I.; García, J.R.; Soler, M.; et al. Cross-Sectional and Longitudinal Cognitive Correlates of FDDNP PET and CSF Amyloid-β and Tau in Parkinson’s Disease. Journal of Alzheimer’s Disease 2017, 55, 1261–1272, doi:10.3233/JAD-160698. [CrossRef]
Figure 1.
number of positive cortical areas.
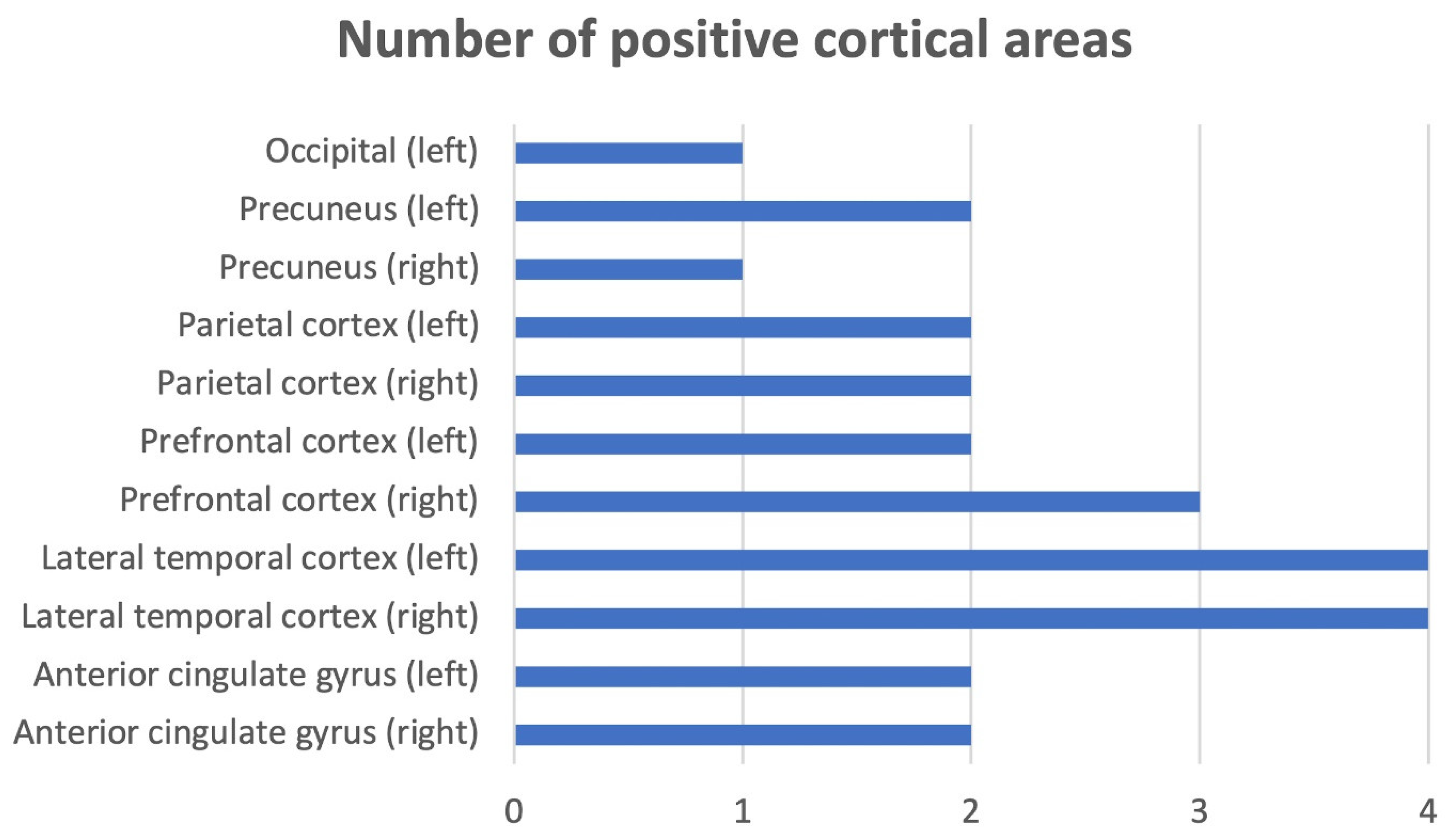

Table 1.
demographic and clinical characteristics of the patients.
| VARIABLE | TOTAL N= 19 NO. (%), MEAN, [± SD]; MEDIAN {RANGE} |
|---|---|
|
Sex Male Female |
11 (58%) 8 (42%) |
| Preoperative assessment | |
| Age at surgery (years) | 58.89 [± 5.69]; 59.00 {46.00–71.00} |
| Age at PD onset (years) | 48.21 [± 5.93]; 47.00 {38.00-57.00} |
| Disease duration at surgery (years) | 10.47 [±4.88]; 8.00 {5.00–25.00} |
|
Genetic analysis Negative Positive |
16 (85.00%) 3 (GBA1; 15.00%) |
|
PD motor subtype PIGD Indeterminate TD |
14 (73.70%) 2 (10.50%) 3 (15.80%) |
| Levodopa equivalent daily dose (LEDD) (mg) | 924.23 [± 451.49]; 1045 {200-1898} |
| Levodopa responsiveness (%) | 58.83 [± 15.357]; 58.00 {34.00–93.94} |
| Post-operative evaluation | |
| Follow-up duration (years) | 4.73 [± 1.38]; 5 {3-7} |
| Age (years) | 63.52 [± 5.14]; 65 {53 - 74} |
| Disease duration (years) | 15.00 [± 4.78]; 13 {8-28} |
|
PD motor subtype PIGD Indeterminate TD |
17 (89.40%) 1 (5.30%) 1 (5.30%) |
| LEDD (mg) | 778.68 [±336.68]; {118.00-1460.00} |
|
PD cognitive status PD without dementia MCI-PD PDD |
9 (58%) 8 (41.40%) 2 (10.60%) |
Table 2.
motor scores and subscores in the different conditions tested.
| VARIABLES | STIMULATION/MEDICATIONS CONDITIONS | ||||
|---|---|---|---|---|---|
| mean, [±SD]; median {range} | |||||
| Off-medication | On-medication | On-stimulation/off-medication | Off-stimulation/off-medication | On-stimulation/on-medication | |
| UPDRS part-III | 36.82 [±9.86]; 34.00 {25.00-62.00} |
15.47 [±6.69]; 13.00 {6.00-31.00} |
31.05 [±13.97]; 13.97 {13.00-58.00} |
48.88 [±.12.83]; 49.00 {29.00-73.00} |
17.05 [±9.71]; 13.00 {5.00-38.00} |
| Akinesia subscore | 13.00 [±3.31]; 13.00 {7.00-18.00} |
5.05 [±3.23]; 4.00 {1.00-12.00} |
11.70 [±6.23]; 11.00 {2.00-23.00} |
18.07 [±5.69]; 18.00 {8.00-28.00} |
7.35 [±5.06]; 6.00 {1.00-17.00} |
| Tremor subscore | 4.41 [±4.30]; 3.00 {.00-14.00} |
1.35 [±2.31]; .00 {.00-9.00} |
3.11 [±2.39]; 3.00 {.00-7.00} |
4.94 [±2.90]; 4.00 {.00-10.00} |
.52 [±1.06]; .00 {.00-4.00} |
| PIGD subscore | 8.47 [±3.69]; 8.00 {3.00-16.00} |
2.82 [±1.97]; 2.00 {.00-7.00} |
8.23 [±3.43]; 9.00 {1.00-13.00} |
9.76 [±3.92]; 10.00 {1.00-15.00} |
5.52 [±3.57]; 5.00 {1.00-12.00} |
| Hoehn & Yahr | 2.86 [±.57]; 2.50 {2.00-4.00} |
2.13 [±.22]; 2.00 {2.00-2.50} |
2.86 [±.76]; 2.50 {2.00-5.00} |
3.84 [±.1.00]; 4.00 {2.00-5.00} |
2.42 [±.53]; 2.50 {2.00-4.00} |
Abbreviations: postural instability/gait disorders: PIGD; Unified Parkinson’s Disease Rating Scale: UPDRS.
Table 3.
Demographic and clinical characteristics of PET positive and PET negative cohorts.
| VARIABLE | PET positive (n= 4) | PET negative (n= 15) |
|---|---|---|
|
Sex Male Female |
2 (50%) 2 (50%) |
11 (58%) 8 (42%) |
| Follow-up duration (years) | 5.25 [± .50]; 5 {5-6} | 4.46 [± 1.50]; 4 {3-7} |
| Age (years) | 62.75 [± 4.03]; 63 {58 - 67} | 63.73 [± 5.50]; 65 {53 - 74} |
| Disease duration (years) | 13.75 [± 2.21]; 13 {12-17} | 15.33 [± 5.27]; 13 {8-28} |
|
PD motor subtype PIGD Indeterminate TD |
4 (100%) 0 (.00%) 0 (.00%) |
13 (86.70%) 1 (6.70%) 1 (6.70%) |
| Levodopa equivalent daily dose (mg) | 707.75 [±123.01] {580.00-819.00} |
797.60 [±375.30] {118.00-1460.00} |
|
PD cognitive status PD without dementia MCI-PD PDD |
1 (25.00%) 2 (50.00%) 1 (25.00%) |
8 (53.30%) 6 (40.00%) (6.70%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



