Submitted:
15 May 2025
Posted:
15 May 2025
You are already at the latest version
Abstract
Candida auris (C. auris) is an emerging multidrug-resistant fungal pathogen recognized by the World Health Organization (WHO) as a critical global health threat. Its rapid transmission, high mortality rate, and frequent misidentification in clinical laboratories present significant challenges for diagnosis and infection control. This review provides a comprehensive overview of current and emerging diagnostic methods for C. auris detection, including culture-based techniques, biochemical assays, matrix-assisted laser desorption/ionization time-of-flight mass spectrometry (MALDI-TOF MS), and molecular diagnostics such as PCR and loop-mediated isothermal amplification (LAMP). We evaluate each method’s sensitivity, specificity, turnaround time, and feasibility in clinical and surveillance settings. While culture remains the diagnostic gold standard, it is limited by slow turnaround and phenotypic overlap with related species. Updated biochemical platforms and MALDI-TOF MS with expanded databases have improved identification accuracy. Molecular assays offer rapid, culture-independent detection. Antifungal susceptibility testing (AFST), primarily using broth microdilution, is essential for guiding treatment, although standardized breakpoints remain lacking. This review proposes an integrated diagnostic workflow and discusses key innovations and gaps in current practice. Our findings aim to support clinicians, microbiologists, and public health professionals in improving early detection, containment, and management of C. auris infections.
Keywords:
Candida auris
; diagnostic methods
; matrix-assisted laser desorption/Ionization time-of-flight mass spectrometry (MALDI-TOF MS)
1. Introduction
Candida auris (C. auris) has emerged as a significant global health threat due to its rapid spread, multidrug resistance, and high associated mortality. Recognized by the World Health Organization (WHO) as a critical priority pathogen in its inaugural fungal priority pathogen list, C. auris poses a serious challenge to public health worldwide [1]. Since its discovery in 2009, this opportunistic fungal pathogen has been reported across six continents, with a sharp rise in case numbers in recent years. In the United States, for example, the incidence of C. auris infections increased by 95% from 2019 to 2021, with new cases identified in 17 additional states during this period [2,3]. Similarly, in Europe, reported cases nearly doubled between 2020 and 2021 [4,5].
Distinct from other Candida species that primarily colonize the gastrointestinal tract, C. auris preferentially colonizes the skin. This enables efficient transmission in hospitals and long-term care facilities. Its ability to form biofilms, persist on surfaces, and resist standard disinfection protocols contributes to its capacity to cause widespread outbreaks [6]. Colonization also significantly elevates the risk of invasive infection. In certain healthcare settings in South Africa and India, C. auris has accounted for up to 25% and 40% of candidemia cases, respectively [2,7]. Global mortality rates linked to C. auris infections range between 40% and 60%, although attributing deaths solely to C. auris is often complicated by patients' underlying comorbidities [8,9,10,11].
Effective infection control and prevention hinge on early and accurate detection. However, this remains a major challenge. Conventional diagnostic tools often misidentify C. auris, particularly conventional culture and biochemical assays, which frequently confuse it with closely related species such as Candida haemulonii, leading to diagnostic delays and inappropriate treatments [12,13]. Earlier iterations of MALDI-TOF MS also failed to correctly identify C. auris due to inadequate reference spectra[14]. Additionally, C. auris is genetically diverse, comprising at least six distinct clades, further complicating species identification and necessitating advanced molecular and proteomic techniques for precise diagnosis and epidemiological surveillance.
This review examines current diagnostic strategies for C. auris, encompassing both culture-dependent and culture-independent approaches. It evaluates the primary diagnostic modalities used in clinical and surveillance settings, with a focus on sensitivity, specificity, turnaround time, and operational feasibility. We highlight recent advancements that improve diagnostic accuracy and efficiency, assess their practical applications in laboratory and clinical contexts, and discuss key limitations. By providing an up-to-date and comprehensive overview, this review aims to guide clinicians, microbiologists, and public health professionals in enhancing early detection, outbreak management, and patient care outcomes.
2. Clinical Diagnostic Approaches of C. auris
The diagnosis of C. auris infection or colonization relies on both clinical and surveillance samples. Clinical cases refer to cultures collected for diagnosing or treating disease, whereas screening cases involve samples obtained for surveillance purposes. Accurate and timely identification is critical for guiding appropriate treatment, implementing effective infection control measures, and preventing healthcare-associated outbreaks. To assist with method selection across varied settings, Table 1 summarizes major diagnostic techniques for C. auris, comparing their performance characteristics and operational feasibility.
An integrated diagnostic workflow follows a multi-step process—from specimen collection to definitive identification—utilizing both culture-based and molecular technologies. As illustrated in Figure 1, this begins with presumptive identification using traditional culture on chromogenic media, followed by confirmatory testing via biochemical assays, MALDI-TOF MS, or molecular techniques such as PCR and LAMP.
Routine microbiological cultures remain the cornerstone of clinical diagnosis and are conducted on both sterile (e.g., blood) and non-sterile (e.g., urine, sputum) specimens. However, optimal growth of C. auris requires incubation at elevated temperatures (37–40°C), a feature that distinguishes it from other Candida species. Without this thermotolerant condition, standard culture protocols may fail to detect the organism. Complete identification of yeast isolates from sterile sites to exclude C. auris is recommended [31]. Detection of in sterile specimens such as blood is clinically significant and indicates invasive candidiasis. Importantly, Candida-positive blood cultures should never be dismissed as contaminants.
In contrast, diagnosing C. auris from non-sterile specimens presents unique challenges. Sites like the respiratory or urinary tract often yield mixed yeast flora, necessitating additional tests to confirm or exclude C. auris. This complexity increases laboratory workload and may delay reporting, particularly in settings with limited resources [32]. Therefore, balancing comprehensive identification with practical laboratory constraints is essential.
To address these limitations, molecular diagnostics such as PCR have been developed. PCR offers high sensitivity and specificity for both clinical and surveillance samples and delivers results significantly faster than traditional culture methods. However, its use is typically reserved for cases with a high index of suspicion, owing to cost and workflow constraints. In parallel, supplementary assays like Beta-D-glucan (BDG) and mannan/anti-mannan antibody detection are available, but they have limited diagnostic utility due to their low specificity and sensitivity for invasive candidiasis [29,30,33].
Ultimately, clinical judgment plays a vital role in interpreting the significance of C. auris isolation. Detection from non-sterile sites may reflect colonization rather than true infection. Nonetheless, even in such cases, identifying colonized individuals is essential, particularly in outbreak settings, as it supports targeted infection prevention and control measures [31].
3. Screening Guidelines and Protocols of
3.1. Importance of Screening for C. auris Colonization
Screening for C. auris colonization plays a pivotal role in early detection and infection control. This pathogen spreads readily through contact with high-touch surfaces, contaminated medical equipment, and colonized patients. Its ability to persist on surfaces for 7 to 14 days facilitates continued environmental contamination and nosocomial transmission. Documented cases show that some patients can acquire C. auris infections within just four days of exposure in healthcare settings [34,35,36,37,38].
Colonization is often prolonged, particularly in intensive care units (ICUs), long-term care environments, and regions where C. auris is endemic [39]. Patients may remain colonized throughout their hospital stay, and even those discharged into the community may carry the fungus for up to eight months [40,41,42]. Although colonization is typically asymptomatic, individuals continue to shed the organism, making them ongoing sources of transmission and elevating the risk of invasive infection.
Progression from colonization to infection is uncommon but significant. One study estimated 0.3 invasive cases per 1,000 patient-days among colonized individuals.[43]. Reported mortality rates for C. auris infections range between 40% and 60%, although the exact contribution is difficult to quantify due to underlying comorbidities [8,9]. Given the severity of potential outcomes, proactive screening is essential for limiting outbreaks. Healthcare facilities may conduct screening either as a preventive measure, targeting high-risk individuals before transmission occurs, or as a response-based intervention following the identification of a confirmed case to assess secondary spread and infection control efficacy.
3.2. Identifying Individuals for Screening
Effective screening strategies begin with identifying populations at elevated risk. High-priority individuals include those with epidemiologic links to known cases, recent exposure to healthcare environments, or clinical factors that predispose them to colonization [44]. Environmental screening is also important, but this study focus on human screening.
Patients transferred from long-term acute care hospitals (LTACHs) or ventilator-capable skilled nursing facilities (vSNFs) are particularly vulnerable [40]. Prolonged hospital stays, especially in ICUs, are also associated with increased colonization rates and a higher risk of invasive candidiasis [45]. Even after a recent negative screen, repeat testing may be warranted upon ICU discharge [39].
Those who have shared rooms or equipment with confirmed C. auris cases or received care from the same healthcare personnel during overlapping timeframes also face heightened risks. Studies have found colonization rates of 5% to 10% among close contacts [46]. Despite this, routine screening of healthcare workers or household members is not recommended unless specific risk factors are present [31].
The necessity of admission screening varies by region [47]. In non-endemic areas, community prevalence is low, and routine screening upon hospital admission is not standard practice. Studies from the UK and USA support this, showing that admission carriage is rare and usually associated with prior hospital exposure [48,49]. In contrast, endemic countries like India report colonization rates as high as 9.3% on admission, supporting the use of targeted screening protocols upon hospital entry in these contexts [50]. Individuals with prior healthcare exposure in these regions should undergo screening upon hospital admission [46,51].
Beyond epidemiological exposure, several clinical risk factors further elevate susceptibility. These include mechanical ventilation, use of central venous catheters, parenteral nutrition, prior antifungal or broad-spectrum antibiotic use, recent surgery, and episodes of sepsis. Patients with immunosuppressive conditions—such as HIV infection, malignancy, neutropenia, corticosteroid therapy, or organ transplantation—are also at greater risk. Additional comorbidities like liver cirrhosis, renal disease, diabetes mellitus, and history of blood transfusions have been linked to increased colonization and infection rates [1,52,53,54]. Screening decisions should ultimately be guided by local epidemiologic data, facility-specific transmission patterns, and individual patient risk profiles.
3.3. Screening Methods, Timing, and Laboratory Protocols
Once at-risk individuals are identified, appropriate screening methods must be selected to ensure diagnostic accuracy and timely intervention. The CDC recommends using a composite swab of the axilla and groin for colonization screening, as these areas consistently exhibit the highest fungal burden and first-detection positivity [55,56] (Figure 2). Some studies suggest that including nasal swabs alongside axilla and groin may improve detection rates further [57]. In contrast, other sites such as urine, throat, pharynx, and axillary-rectal swabs have demonstrated lower sensitivity and are not considered reliable for routine screening [55,58]. Nonetheless, C. auris may colonize additional body surfaces that are not regularly sampled, allowing undetected transmission to persist in clinical settings [58].
A standard protocol involves using a nylon-flocked swab (e.g., ESwab) to firmly sample both axillae and the groin. The swab is then placed in a transport medium [59], labeled accurately, sealed in a biohazard bag, and submitted to the laboratory for processing. To avoid false-negative results, screening should be postponed for at least 48 hours if the patient has recently received topical antiseptics [13].
The optimal laboratory method for detecting C. auris colonization remains under investigation. However, the CDC currently endorses several approaches, including culture on chromogenic or salt/dulcitol agar, molecular detection via PCR, and salt/dulcitol enrichment broth. Each method varies in sensitivity, turnaround time, and resource requirements.
A positive screening result confirms colonization, indicating the presence of C. auris on the patient's skin even in the absence of symptoms. Because colonized individuals are capable of transmitting the pathogen, a confirmed result necessitates the immediate implementation of transmission-based precautions. Additionally, healthcare facilities are required to report cases to the CDC and notify appropriate local or state health departments to support regional infection control measures.
4. Diagnostic Methods for C. auris Detection
4.1. Culture-Based Methods
4.1.1. Differential and Selective Media
Culture-based diagnostics remain the gold standard for the detection of C. auris in both clinical and surveillance samples. These methods are particularly important because advanced identification techniques such as biochemical assimilation tests and MALDI-TOF MS require isolated yeast colonies as input. However, conventional culture methods alone are often insufficient for accurate identification, as C. auris shares significant phenotypic similarity with other Candida species—most notably C. haemulonii and C. duobushaemulonii—making morphological differentiation unreliable [60,61,62,63].
Phenotypic variability in response to temperature and salinity further complicates the identification process. The CDC has cautioned against relying solely on colony morphology for screening purposes, emphasizing the need for more selective approaches [64,65].
To address these limitations, selective media have been developed by exploiting the unique thermotolerance, halotolerance, and carbohydrate assimilation profile of C. auris. The fungus grows on standard media such as Sabouraud dextrose agar (SDA) and various chromogenic formulations at optimal temperatures of 37–40°C but shows reduced growth at 42°C—an important differentiator from related species [66]. Its ability to tolerate saline environments, including concentrations of 10–12.5% NaCl, has been used in selective formulations to suppress competing flora [57,67]. Additionally, unlike C. haemulonii, which depends on glucose, C. auris can metabolize dulcitol and mannitol [6,35].
The first targeted selective medium was developed by Welsh et al. (2017), incorporating 10% NaCl and elevated temperatures (40°C) into Sabouraud or yeast nitrogen base broth with dulcitol or mannitol as the carbon source [6]. Since then, newer non-commercial formulations have emerged. The Selective Auris Medium, a modified Yeast Extract Peptone Dextrose agar (YPD agar) with 12.5% NaCl and 9 mM ferrous sulfate, allows direct plating from blood cultures at 42°C [15].Similarly, the Specific C. auris Medium (SCA), developed by Walsh et al., contains crystal violet to inhibit Candida tropicalis and has shown promising results in ICU settings in Algeria [16,68]. Despite these advances, additional validation against closely related species in the C. haemulonii complex remains necessary to ensure specificity.
In resource-limited settings, simpler media can be supplemented with fluconazole to exploit C. auris' intrinsic triazole resistance, or with chloramphenicol and gentamycin to suppress bacterial and fungal contaminants [35,69]. These adaptations offer cost-effective alternatives for presumptive screening in endemic regions.
4.1.2. Chromogenic Media
Chromogenic media are frequently used for presumptive identification due to their accessibility, affordability, and ease of use. These media enable visual differentiation of yeast species based on colony color (Figure 3), typically within five days. Specimens can be applied directly or after broth enrichment, which, although more labor-intensive, improves detection sensitivity by one log₁₀ CFU/mL [70]. However, colony color alone is not a reliable identifier; C. auris colonies may appear cream, pink, red, or purple—colors shared with other Candida species—thus complicating interpretation [20].
Recent formulations have aimed to address this limitation. CHROMagar™ Candida Plus (CHROMagar, France) produces a distinctive light blue colony with a blue halo for all four known C. auris lineages after 36–48 hours of incubation at 37°C, effectively differentiating it from most other Candida species, including members of the C. haemulonii complex. Despite high sensitivity and specificity, some false positives have been reported with species such as Candida diddensiae, C. metapsilosis, and C. orthopsilosis [18,71,72].
Other formulations, such as Pal’s medium used in combination with CHROMagar Candida, have demonstrated promise in distinguishing C. auris from similar species, though broader validation is still required [17]. HiCrome™ C. auris medium offers results within 24 hours but has demonstrated variable accuracy across studies [20,69].
Temperature and media supplementation can enhance performance. Although manufacturers typically recommend 37°C incubation, raising the temperature to 40°C can suppress the growth of competing species (CDC). Additionally, the use of fluconazole-supplemented CHROMagar improves specificity by inhibiting susceptible strains [57,64].
4.1.3. Conclusion of Culture-Based Methods
Despite the high risk of misidentification and relatively long turnaround times—typically 24 to 48 hours, and up to 10 days in some cases [73]—culture-based methods, including both traditional and selective approaches, remain essential components of the diagnostic pathway for . These methods serve as the foundation for subsequent analyses such as biochemical identification, MALDI-TOF MS, and AFST. Given the potential for diagnostic errors, all presumptive positive cultures should be confirmed using high-resolution diagnostic tools to ensure accurate species identification and inform appropriate clinical management.
4.2. Biochemical Assimilation Tests
Biochemical assimilation tests identify C. auris based on the organism's metabolic profile, evaluating carbohydrate and nitrogen assimilation, as well as enzymatic activity. A standardized yeast suspension is inoculated into wells containing various biochemical substrates. These panels are incubated, and identification is made by observing metabolic-induced color changes or turbidity, which are then compared against a reference database [74].
Despite their widespread use, these methods frequently misidentify C. auris due to significant overlap in metabolic profiles with other Candida species. Rather than yielding “no identification,” they often produce incorrect matches, particularly with species from the C. haemulonii complex.
Historically, early C. auris isolates were commonly misidentified by biochemical platforms. For example, the API 20C AUX and API ID 32C systems often reported isolates as Rhodotorula glutinis, Saccharomyces cerevisiae, or Candida sake, while the VITEK 2 system misclassified them as C. haemulonii [75,76,77,78]. Subsequent updates to the VITEK 2 system, particularly version 8.01, improved the accuracy of identifying isolates belonging to the South American Clade (Clade IV). However, identification remains inconsistent for isolates from the South Asian (Clade I) and African (Clade III) clades [79,80]. Misidentifications continue to occur, with isolates reported as C. haemulonii, C. duobushaemulonii, or even as unidentified Candida species [76]. Although VITEK 2 version 9.01 has been released, its performance in identifying a broader range of clades has not yet been fully evaluated.
Other commonly used biochemical platforms, such as MicroScan WalkAway and BD Phoenix, currently lack database support for C. auris, resulting in frequent misclassification or failed identification [74,75]. Given these limitations, the CDC recommends that biochemical test results always be interpreted cautiously and in conjunction with confirmatory diagnostics, such as MALDI-TOF MS or DNA sequencing, as outlined in their 2019 algorithm (Table 2) [21].
In resource-limited settings, where MALDI-TOF MS and molecular diagnostics may not be available, biochemical assimilation tests remain a practical and cost-effective alternative. Among available platforms, the VITEK 2 system (version 8.01) has demonstrated relatively reliable performance for identifying C. auris and may also support rapid antifungal susceptibility testing, as discussed in the subsequent susceptibility testing section.
4.3. Matrix-Assisted Laser Desorption/Ionization Time-of-Flight Mass Spectrometry (MALDI-TOF MS)
4.3.1. The evolution of MALDI-TOF on Detecting C. auris
Since its introduction in the late 1990s, matrix-assisted laser desorption/ionization time-of-flight mass spectrometry (MALDI-TOF MS) has transformed clinical microbiology due to its speed, cost-effectiveness, and high diagnostic accuracy [81]. Initially employed for bacterial identification, the platform was expanded to include yeasts such as Candida spp. by 2009 [82,83]. The subsequent inclusion of C. auris spectra in commercial and curated databases has established MALDI-TOF MS as a powerful tool for the rapid and reliable identification of this emerging pathogen.
This technique is culture-dependent and typically uses colonies from agar plates, enrichment broths, or blood culture bottles. The process works by ionizing microbial proteins to generate a unique mass-to-charge ratio spectrum, which is compared against reference databases (Figure 4). MALDI-TOF MS offers over 90% identification accuracy and is particularly effective in distinguishing C. auris from closely related species within the C. parapsilosis complex (C. parapsilosis, C. orthopsilosis, and C. metapsilosis), where conventional biochemical and culture-based methods often fall short [84,85,86].
In addition to its high precision, MALDI-TOF MS delivers results rapidly—typically within 4 to 5 hours following culture growth—making it a critical tool for timely diagnosis and confirmation of C. auris infections in clinical settings [86]. Its utility depends heavily on the quality of reference libraries and appropriate sample preparation.
4.3.2. Sample Preparation and Database Considerations
The diagnostic performance of MALDI-TOF MS is influenced by multiple factors, including extraction methods, database versions, and instrument calibration. Common sample preparation protocols include Direct Smear, On-Plate Extraction, Full Tube Extraction, and Partial Tube Extraction. Among these, Full Tube and Partial Tube Extraction methods generally yield superior confidence scores for C. auris identification compared to Direct Smear or On-Plate Extraction [87,88].
Recent studies recommend Partial Tube Extraction for its balance of diagnostic accuracy and workflow efficiency [88]. On-Plate Extraction, although slightly less sensitive, remains a viable cost- and time-effective method for settings with limited resources or during high-throughput testing, such as in bloodstream infection management [89].
The effectiveness of MALDI-TOF MS also depends on the version and comprehensiveness of its reference database. Major platforms such as the VITEK MS (bioMérieux) and Microflex LT Biotyper (Bruker Daltonics) have improved C. auris identification with updated databases like bioMérieux’s IVD v3.2 or RUO Saramis v4.14, and Bruker’s CA System (version 4) or RUO 2014 (5627). However, older library versions may still misidentify C. auris as C. haemulonii or C. lusitaniae, emphasizing the need for continuous database updates and confirmatory testing when results are ambiguous.
4.4. Molecular Methods for C auris Detection
4.4.1. Overview of DNA-Based Detection
DNA-based methods such as polymerase chain reaction (PCR) and loop-mediated isothermal amplification (LAMP) have proven highly effective for early C. auris detection. PCR typically produces results within 2 to 5 hours, while LAMP assays can deliver detection within 30 minutes [86,92,93,94]. These tools are ideal for colonization screening and outbreak control due to their speed and operational ease.
However, limitations exist. PCR assays cannot differentiate between viable and non-viable cells, leading to possible overestimation of colonization, especially in non-sterile samples [13]. Similarly, LAMP's performance is sensitive to sample integrity, with reduced sensitivity reported in cases of poor specimen handling or prolonged storage.
4.4.2. PCR-Based Detection
Quantitative PCR (qPCR) assays for C. auris vary based on DNA extraction protocols, primer design, and amplification chemistry. Commonly targeted genetic regions include the internal transcribed spacer (ITS1 and ITS2), 5.8S, 18S, and 28S ribosomal DNA (rDNA), and the glycosylphosphatidylinositol (GPI) gene [93,95,96,97]. Among these, the ITS2 region is the most frequently used due to its multiple genome copies and enhanced sensitivity. The CDC has developed specific primers targeting ITS2 for public health use [98]. While the GPI gene offers improved specificity, it remains underutilized in routine diagnostics [96,97]. More recently, the NADH dehydrogenase subunit 5 (nad5) gene has been explored as an alternative target with promising specificity [99].
A comprehensive 2025 review of 28 studies identified eight commercial PCR assays and 16 laboratory-developed tests (LDTs) targeting C. auris. Commercial platforms demonstrated high diagnostic performance, with sensitivity ranging from 94.9% to 100% and specificity from 98.2% to 100%, while LDTs showed similar sensitivity (93.3%–100%) and specificity (92%–100%) [23,100].
In terms of regulatory approvals, the GenMark ePlex BCID-FP and BioFire FilmArray BCID2 panels have received FDA clearance for C. auris detection from blood cultures (510(k) Numbers: K182690, K200010) [101,102]. The DiaSorin Molecular Simplexa C. auris assay was granted FDA De Novo authorization in July 2024 and validated for axilla/groin swab screening [103,104,105]. In Europe, three CE-IVD–marked PCR assays include the OLM AurisID, RealCycler C. auris PCR, and Eazyplex C. auris assays [23,39,94,106,107]. However, no FDA-approved high-throughput molecular platform currently exists for colonization screening, highlighting an urgent need for automation-compatible, scalable solutions.
4.4.3. Loop-Mediated Isothermal Amplification (LAMP)
LAMP is an isothermal amplification technique performed at 60–65°C using 4–6 primers and a strand-displacing DNA polymerase. It is praised for its simplicity, speed, and cost-effectiveness. Commercial LAMP assays such as Eazyplex C. auris and LAMPAuris have demonstrated sensitivity between 66% and 86% and specificity from 96.8% to 100% across a range of clinical, surveillance, and environmental samples [94,108,109].
DH Lim et al. (2022) developed a multiplex Pan-Candida LAMP assay using Chelex-100 DNA extraction, achieving 100% sensitivity and specificity in candidemia blood samples and effectively distinguishing six Candida species [109]. Nevertheless, LAMP performance is susceptible to sample quality. Studies have shown that improper storage or lack of pre-processing—such as brief vortexing—can significantly reduce sensitivity [94,108].
4.4.4. T2 Magnetic Resonance (T2MR) Assay
The T2MR assay, originally developed for bloodstream infections, has been adapted for C. auris colonization screening using the fully automated T2DX system. This platform enables rapid (<3 hours), highly sensitive detection at levels as low as 1–3 CFU/mL [24].
In a study by Sexton et al. (2018), T2MR demonstrated 89% sensitivity and 98% specificity when applied to axilla/groin swab samples. This led to the development of the T2Cauris panel, which expands detection to include C. auris, C. haemulonii, C. duobushaemulonii, and C. lusitaniae in both blood and environmental samples [24]. However, the assay remains designated for research use only and currently lacks regulatory approval for clinical diagnostics.
4.4.5. Summary for Molecular Testing
Molecular diagnostics offer rapid, culture-independent detection of, critical for outbreak management and colonization screening. Compared to culture-based methods, they provide faster turnaround and higher sensitivity, even in resource-limited settings. Real-time PCR remains the gold standard, delivering high sensitivity and specificity, while LAMP offers a faster, cost-effective alternative, though it is more susceptible to sample quality issues. T2MR provides highly sensitive results from blood and swab samples but is currently limited to research use. PCR should be prioritized for routine screening, with LAMP as a complementary option where PCR is unavailable. Despite advances, scalable, FDA-approved high-throughput assays for colonization detection are urgently needed to strengthen clinical and public health responses.
5. Genomic Typing and Outbreak Investigation in
Molecular typing plays a critical role in outbreak detection, strain surveillance, and understanding the transmission dynamics of C. auris. These methods help identify strain-specific characteristics, including patterns of antimicrobial resistance, virulence, and geographic dissemination, thereby informing clinical management and infection control strategies [73,110].
Among available methods, whole-genome sequencing (WGS) is considered the gold standard for high-resolution phylogenetic analysis. WGS enables the differentiation of local transmission from new introductions by comparing single nucleotide polymorphisms (SNPs) across isolates [111]. To support standardized genomic surveillance, Welsh et al. developed an empirical benchmark dataset containing 23 C. auris genomes, which serves as a reference for evaluating phylogenomic pipelines [25]. Complementing this, the CDC maintains a public C. auris genomic surveillance project on the National Center for Biotechnology Information (NCBI) platform (accession no. PRJNA642852), along with various open-access analytical tools to support outbreak investigations [112].
Although WGS provides unparalleled resolution, its cost, turnaround time, and infrastructure requirements can limit its routine use. As a result, alternative genotyping methods have been developed to balance accuracy with feasibility. Short tandem repeat (STR) typing has emerged as a reliable alternative, offering high reproducibility and strong correlation with WGS findings. STR can effectively differentiate isolates that vary by more than 30 SNPs, making it suitable for both local and regional epidemiological surveillance [26,50,113].
Multilocus sequence typing (MLST), which targets four conserved loci (ITS, D1/D2, RPB1, and RPB2), is effective in distinguishing C. auris from phylogenetically related species. It is useful in tracking antifungal resistance patterns across clades but lacks the resolution required for investigating transmission within hospital outbreaks [27,114].
Amplified fragment length polymorphism (AFLP) has also been explored as a low-cost genotyping option. While it offers a rapid turnaround, its poor reproducibility and inconsistent concordance with WGS and STR data limit its reliability in high-stakes outbreak scenarios [28].
In summary, genomic analyses consistently demonstrate that isolates involved in hospital outbreaks or clonal clades often exhibit minimal genomic variation, reinforcing the need for high-resolution tools for accurate differentiation [111,115]. While WGS remains the most precise method for outbreak tracking and global surveillance, STR typing offers a practical compromise between speed, cost, and phylogenetic resolution. In contrast, MLST and AFLP, while useful for species-level identification and broader resistance surveillance, are less suitable for resolving transmission events during hospital outbreaks [28].
6. Antifungal Susceptibility Testing (AFST) for C. auris
6.1. Multidrug Resistance in C. auris
C. auris presents significant therapeutic challenges due to its high rates of multidrug resistance. In the United States, approximately 90% of isolates exhibit resistance to fluconazole, 30% to amphotericin B (AMB), and under 2% to echinocandins [116]. The global emergence of pan-resistant strains underscores the urgent need for accurate antifungal susceptibility testing (AFST) to guide effective treatment and support infection control strategies [1,117].
6.2. Reference Methods and Interpretive Challenges
Broth microdilution (BMD) is recommended as the reference method for AFST by both the Clinical and Laboratory Standards Institute (CLSI) and the European Committee on Antimicrobial Susceptibility Testing (EUCAST). While tentative clinical breakpoints (CBPs) and epidemiologic cutoff values (ECVs) have been proposed, formal susceptibility thresholds for C. auris remain unestablished [118]. Interpretation of minimum inhibitory concentration (MIC) values is further complicated by inter-clade variability and regional differences in MIC distributions [62,119]. In practice, many laboratories follow the CDC's tentative breakpoints, which are informed by MIC trends, animal model data, and known resistance markers [116].
One unique complication in C. auris testing is the Eagle effect, where isolates appear inhibited at lower caspofungin concentrations but demonstrate regrowth at higher levels. This phenomenon may result in inconsistent MIC readings and misclassification of susceptible isolates as resistant, particularly if additional echinocandins are not tested alongside caspofungin [120].
6.3. Performance of Commercial Testing Platforms
Commercial AFST systems—including VITEK 2, Sensititre YeastOne (SYO), MICRONAUT-AM, and gradient diffusion methods such as Etest and MIC Test Strip (MTS)—provide faster results than BMD but show variable concordance. Gradient diffusion tests offer a broader MIC range but are prone to subjective interpretation, especially near susceptibility thresholds. Among these, Etest generally aligns more closely with BMD than VITEK 2, although it tends to overestimate AMB resistance [121,122].
SYO may also overestimate AMB resistance and, due to the Eagle effect, inaccurately assess caspofungin susceptibility [123]. The MICRONAUT-AM platform has improved the accuracy of AMB susceptibility results but may underestimate fluconazole resistance [124]. In 2022, CLSI advised laboratories to interpret AMB MICs with caution due to variability across methods. Despite producing MIC values, these platforms lack definitive interpretive criteria, as no clinical trials have established susceptibility breakpoints for C. auris. This variability necessitates careful clinical interpretation of automated results.
6.4. Genotypic Resistance Mechanisms and Molecular Testing
Molecular studies have revealed key genetic mutations that confer antifungal resistance in C. auris. Resistance to fluconazole is commonly linked to mutations in the ERG11 gene, while ERG2 mutations affect amphotericin B susceptibility. Echinocandin resistance is associated with mutations in FKS1, and resistance to 5-fluorocytosine has been traced to alterations in FCY2, FCY1, and FUR1 genes [32,125]. Genotypic testing enables earlier detection of resistance profiles, allowing clinicians to make timely therapeutic adjustments before phenotypic test results become available [126].
6.5. MALDI-TOF MS-Based AFST: Emerging Innovations
MALDI-TOF MS is emerging as a novel tool for AFST. The Minimal Profile Change Concentration (MPCC), developed by Marinach et al. (2009), measures changes in the mass spectrum of microbial proteins in response to antifungal exposure. These changes are quantified using the Composite Correlation Index (CCI), a statistical measure that compares protein spectra before and after antifungal exposure to detect drug-induced alterations. The CCI has demonstrated over 90% accuracy in identifying resistance to fluconazole and caspofungin, although its performance is more variable for anidulafungin [127,128].
Further innovations include the MALDI Biotyper Antibiotic Susceptibility Test Rapid Assay (MBT ASTRA), which has shown over 95% accuracy in identifying echinocandin resistance in C. auris [84]. While promising, these tools require additional validation and the establishment of clinical breakpoints before they can be reliably adopted into routine practice [129].
6.6. Summary for AFST
In summary, BMD remains the gold standard for C. auris susceptibility testing but requires improved clinical breakpoints for accurate interpretation. Etest generally aligns well with the reference method, while commercial platforms show variable reliability. Genotypic assays offer faster detection of resistance markers but cannot replace phenotypic testing, which remains essential for confirmation. MALDI-TOF MS–based AFST shows promise but requires further clinical validation before routine use.
7. Conclusions
Effective management of depends on a layered diagnostic approach combining culture-based methods, species identification, molecular tools, and antifungal susceptibility testing. While culture is foundational, it should be paired with confirmatory methods due to limitations in speed and accuracy. MALDI-TOF MS enables rapid, reliable identification when supported by updated databases, and real-time PCR offers high-sensitivity, culture-independent detection—crucial for screening and outbreak control.
Genomic tools like WGS and STR typing enhance outbreak tracking and resistance surveillance, while broth microdilution remains the gold standard for susceptibility testing despite interpretive limitations. Diagnostic strategies should be adapted to local resources and epidemiology. To support implementation, we provide a recommended diagnostic workflow (Figure 1) and a comparative summary of tools (Table 1).
Abbreviations
The following abbreviations are used in this manuscript:
| AFST | Antifungal Susceptibility Testing |
| AFLP | Amplified Fragment Length Polymorphism |
| AMB | Amphotericin B |
| API 20C AUX | Analytical Profile Index 20C Auxanographic Yeast Identification System |
| API ID 32C | Analytical Profile Index ID 32C Yeast Identification System |
| ASTRA | Antibiotic Susceptibility Test Rapid Assay |
| BDG | Beta-D-Glucan |
| BMD | Broth Microdilution |
| BCID | Blood Culture Identification |
| CA System | Chromogenic Agar System (Bruker’s MALDI-TOF MS software) |
| CDC | Centers for Disease Control and Prevention |
| CCI | Composite Correlation Index |
| CE-IVD | Conformité Européenne – In Vitro Diagnostic |
| CFU | Colony Forming Unit |
| CHROMagar™ | Chromogenic Agar (commercial medium) |
| CLSI | Clinical and Laboratory Standards Institute |
| DNA | Deoxyribonucleic Acid |
| DOAJ | Directory of Open Access Journals |
| ECV | Epidemiologic Cutoff Value |
| FDA | U.S. Food and Drug Administration |
| GPI | Glycosylphosphatidylinositol |
| HIV | Human Immunodeficiency Virus |
| ICU | Intensive Care Unit |
| ITS | Internal Transcribed Spacer |
| IVD | In Vitro Diagnostic |
| LAMP | Loop-Mediated Isothermal Amplification |
| LD | Linear Dichroism |
| MALDI-TOF MS | Matrix-Assisted Laser Desorption/Ionization Time-of-Flight Mass Spectrometry |
| MBT ASTRA | MALDI Biotyper Antibiotic Susceptibility Test Rapid Assay |
| MDPI | Multidisciplinary Digital Publishing Institute |
| MIC | Minimum Inhibitory Concentration |
| MLST | Multilocus Sequence Typing |
| nad5 | NADH Dehydrogenase Subunit 5 |
| NCBI | National Center for Biotechnology Information |
| PCR | Polymerase Chain Reaction |
| qPCR | Quantitative Polymerase Chain Reaction |
| RAPID Yeast Plus | Enzyme-based Yeast Identification Panel (Remel/Thermo Fisher) |
| RUO | Research Use Only |
| SCA | Specific *Candida auris* Medium |
| SDA | Sabouraud Dextrose Agar |
| Se | Sensitivity |
| SNP | Single Nucleotide Polymorphism |
| Sp | Specificity |
| STR | Short Tandem Repeat |
| SYO | Sensititre YeastOne |
| T2MR | T2 Magnetic Resonance |
| TLA | Three Letter Acronym |
| VITEK 2 | VITEK 2 Biochemical Identification System |
| vSNF | Ventilator-Capable Skilled Nursing Facility |
| WHO | World Health Organization |
| WGS | Whole Genome Sequencing |
| YST | Yeast Susceptibility Testing |
References
- Eix, E.F. and J.E. Nett, Candida auris: Epidemiology and Antifungal Strategy. Annu Rev Med, 2025. 76(1): p. 57-67.
- Nelson, R. , Emergence of resistant Candida auris. Lancet Microbe, 2023. 4(6): p. e396.
- Lyman, M. , et al., Worsening Spread of Candida auris in the United States, 2019 to 2021. Ann Intern Med, 2023. 176(4): p. 489-495.
- Kohlenberg, A., D. L. Monnet, and D. Plachouras, Increasing number of cases and outbreaks caused by Candida auris in the EU/EEA, 2020 to 2021. Euro Surveill, 2022. 27(46).
- Sticchi, C. , et al., Increasing Number of Cases Due to Candida auris in North Italy, 19-December 2022. J Clin Med, 2023. 12(5).
- Ahmad, S. and W. Alfouzan, Candida auris: Epidemiology, Diagnosis, Pathogenesis, Antifungal Susceptibility, and Infection Control Measures to Combat the Spread of Infections in Healthcare Facilities. Microorganisms, 2021. 9(4).
- Shastri, P.S. , et al., Candida auris candidaemia in an intensive care unit - Prospective observational study to evaluate epidemiology, risk factors, and outcome. J Crit Care, 2020. 57: p. 42-48.
- Shaukat, A. , et al., Experience of treating Candida auris cases at a general hospital in the state of Qatar. IDCases, 2021. 23: p. e01007.
- Al-Rashdi, A. , et al., Characteristics, Risk Factors, and Survival Analysis of Candida auris Cases: Results of One-Year National Surveillance Data from Oman. J Fungi (Basel), 2021. 7(1).
- Pandya, N. , et al., International Multicentre Study of Candida auris Infections. J Fungi (Basel), 2021. 7(10).
- Chen, J. , et al., Is the superbug fungus really so scary? A systematic review and meta-analysis of global epidemiology and mortality of Candida auris. BMC Infect Dis, 2020. 20(1): p. 827.
- Garcia-Bustos, V. , et al., What Do We Know about Candida auris? State of the Art, Knowledge Gaps, and Future Directions. Microorganisms, 2021. 9(10).
- Fasciana, T. , et al., Candida auris: An Overview of How to Screen, Detect, Test and Control This Emerging Pathogen. Antibiotics (Basel), 2020. 9(11).
- Welker, M. , et al., An update on the routine application of MALDI-TOF MS in clinical microbiology. Expert Rev Proteomics, 2019. 16(8): p. 695-710.
- Das, S. , et al., A Selective Medium for Isolation and Detection of Candida auris, an Emerging Pathogen. J Clin Microbiol, 2021. 59(2).
- Ibrahim, A. , et al., SCA Medium: A New Culture Medium for the Isolation of All Candida auris Clades. J Fungi (Basel), 2021. 7(6).
- Kumar, A. , et al., Simple low cost differentiation of Candida auris from Candida haemulonii complex using CHROMagar Candida medium supplemented with Pal's medium. Rev Iberoam Micol, 2017. 34(2): p. 109-111.
- Mulet Bayona, J.V. , et al., Evaluation of a novel chromogenic medium for Candida spp. identification and comparison with CHROMagar™ Candida for the detection of Candida auris in surveillance samples. Diagn Microbiol Infect Dis, 2020. 98(4): p. 115168.
- Borman, A.M., M. Fraser, and E.M. Johnson, CHROMagarTM Candida Plus: A novel chromogenic agar that permits the rapid identification of Candida auris. Med Mycol, 2021. 59(3): p. 253-258.
- de Jong, A.W. , et al., Performance of Two Novel Chromogenic Media for the Identification of Multidrug-Resistant Candida auris Compared with Other Commercially Available Formulations. J Clin Microbiol, 2021. 59(4).
- CDC. Algorithm to identify Candida auris based on phenotypic laboratory method and initial species identification. 2019 [cited April 2025. Available online: https://www.cdc.gov/candida-auris/media/pdfs/Testing-algorithm_by-Method_508.pdf.
- Kathuria, S. , et al., Multidrug-Resistant Candida auris Misidentified as Candida haemulonii: Characterization by Matrix-Assisted Laser Desorption Ionization-Time of Flight Mass Spectrometry and DNA Sequencing and Its Antifungal Susceptibility Profile Variability by Vitek 2, CLSI Broth Microdilution, and Etest Method. J Clin Microbiol, 2015. 53(6): p. 1823-30.
- Wong, R.C. , et al., Current Updates on Molecular Diagnostic Assays Used for Detection of Candida auris: A Systematic Review. Diagnostics (Basel), 2025. 15(2).
- Sexton, D.J. , et al., Evaluation of a new T2 Magnetic Resonance assay for rapid detection of emergent fungal pathogen Candida auris on clinical skin swab samples. Mycoses, 2018. 61(10): p. 786-790.
- Welsh, R.M. , et al., Candida auris Whole-Genome Sequence Benchmark Dataset for Phylogenomic Pipelines. J Fungi (Basel), 2021. 7(3).
- de Groot, T. , et al., Development of Candida auris Short Tandem Repeat Typing and Its Application to a Global Collection of Isolates. mBio, 2020. 11(1).
- Sathi, F.A. , et al., Clonal Diversity of Candida auris, Candida blankii, and Kodamaea ohmeri Isolated from Septicemia and Otomycosis in Bangladesh as Determined by Multilocus Sequence Typing. J Fungi (Basel), 2023. 9(6).
- Vatanshenassan, M. , et al., Evaluation of Microsatellite Typing, ITS Sequencing, AFLP Fingerprinting, MALDI-TOF MS, and Fourier-Transform Infrared Spectroscopy Analysis of Candida auris. J Fungi (Basel), 2020. 6(3).
- Nguyen, M.H. , et al., Performance of Candida real-time polymerase chain reaction, β-D-glucan assay, and blood cultures in the diagnosis of invasive candidiasis. Clin Infect Dis, 2012. 54(9): p. 1240-8.
- Wang, K. , et al., Diagnostic value of Candida mannan antigen and anti-mannan IgG and IgM antibodies for Candida infection. Mycoses, 2020. 63(2): p. 181-188.
- CDC. Screening Recommendations for Healthcare Facilities. 2024 [cited 2025 April]; Available from: https://www.cdc.gov/candida-auris/hcp/screening-hcp/index.html.
- Chowdhary, A. , et al., A multicentre study of antifungal susceptibility patterns among 350 Candida auris isolates (2009-17) in India: role of the ERG11 and FKS1 genes in azole and echinocandin resistance. J Antimicrob Chemother, 2018. 73(4): p. 891-899.
- Mikulska, M. , et al., The use of mannan antigen and anti-mannan antibodies in the diagnosis of invasive candidiasis: recommendations from the Third European Conference on Infections in Leukemia. Crit Care, 2010. 14(6): p. R222.
- Piedrahita, C.T. , et al., Environmental Surfaces in Healthcare Facilities are a Potential Source for Transmission of Candida auris and Other Candida Species. Infect Control Hosp Epidemiol, 2017. 38(9): p. 1107-1109.
- Welsh, R.M. , et al., Survival, Persistence, and Isolation of the Emerging Multidrug-Resistant Pathogenic Yeast Candida auris on a Plastic Health Care Surface. J Clin Microbiol, 2017. 55(10): p. 2996-3005.
- Biswal, M. , et al., Controlling a possible outbreak of Candida auris infection: lessons learnt from multiple interventions. J Hosp Infect, 2017. 97(4): p. 363-370.
- Tharp, B. , et al., Role of Microbiota in the Skin Colonization of Candida auris. mSphere, 2023. 8(1): p. e0062322.
- Kumar, J. , et al., Environmental Contamination with Candida Species in Multiple Hospitals Including a Tertiary Care Hospital with a Candida auris Outbreak. Pathog Immun, 2019. 4(2): p. 260-270.
- Magnasco, L. , et al., Frequency of Detection of Candida auris Colonization Outside a Highly Endemic Setting: What Is the Optimal Strategy for Screening of Carriage? J Fungi (Basel), 2023. 10(1).
- Chowdhary, A., C. Sharma, and J.F. Meis, Candida auris: A rapidly emerging cause of hospital-acquired multidrug-resistant fungal infections globally. PLoS Pathog, 2017. 13(5): p. e1006290.
- Bergeron, G. , et al., Candida auris Colonization After Discharge to a Community Setting: New York City, 2017-2019. Open Forum Infect Dis, 2021. 8(1): p. ofaa620.
- Schwartz, I.S., S. W. Smith, and T.C. Dingle, Something wicked this way comes: What health care providers need to know about Candida auris. Can Commun Dis Rep, 2018. 44(11): p. 271-276.
- Southwick, K., E. H. Adams, and J. Greenko, 2039. New York State 2016–2018: Progression from Candida auris Colonization to Bloodstream Infection. Open Forum Infectious Diseases, 2018.
- Silva, I., I. M. Miranda, and S. Costa-de-Oliveira, Potential Environmental Reservoirs of Candida auris: A Systematic Review. J Fungi (Basel), 2024. 10(5).
- Zhang, Z. , et al., Risk of invasive candidiasis with prolonged duration of ICU stay: a systematic review and meta-analysis. BMJ Open, 2020. 10(7): p. e036452.
- Eyre, D.W. , Infection prevention and control insights from a decade of pathogen whole-genome sequencing. J Hosp Infect, 2022. 122: p. 180-186.
- Sabino, R. , et al., Candida auris, an Agent of Hospital-Associated Outbreaks: Which Challenging Issues Do We Need to Have in Mind? Microorganisms, 2020. 8(2).
- Sharp, A. , et al., Screening for Candida auris in patients admitted to eight intensive care units in England, 2017 to 2018. Euro Surveill, 2021. 26(8).
- Forsberg, K. , et al., Candida auris: The recent emergence of a multidrug-resistant fungal pathogen. Med Mycol, 2019. 57(1): p. 1-12.
- Yadav, A. , et al., Colonisation and Transmission Dynamics of Candida auris among Chronic Respiratory Diseases Patients Hospitalised in a Chest Hospital, Delhi, India: A Comparative Analysis of Whole Genome Sequencing and Microsatellite Typing. J Fungi (Basel), 2021. 7(2).
- Tsay, S. , et al., Approach to the Investigation and Management of Patients With Candida auris, an Emerging Multidrug-Resistant Yeast. Clin Infect Dis, 2018. 66(2): p. 306-311.
- Ruiz-Gaitán, A. , et al., An outbreak due to Candida auris with prolonged colonisation and candidaemia in a tertiary care European hospital. Mycoses, 2018. 61(7): p. 498-505.
- Caceres, D.H. , et al., Candida auris: A Review of Recommendations for Detection and Control in Healthcare Settings. J Fungi (Basel), 2019. 5(4).
- Thomas-Rüddel, D.O. , et al., Risk Factors for Invasive Candida Infection in Critically Ill Patients: A Systematic Review and Meta-analysis. Chest, 2022. 161(2): p. 345-355.
- Southwick, K. , et al., A description of the first Candida auris-colonized individuals in New York State, 2016-2017. Am J Infect Control, 2022. 50(3): p. 358-360.
- Eyre, D.W. , et al., A Candida auris Outbreak and Its Control in an Intensive Care Setting. N Engl J Med, 2018. 379(14): p. 1322-1331.
- Zhu, Y. , et al., Laboratory Analysis of an Outbreak of Candida auris in New York from 2016 to 2018: Impact and Lessons Learned. J Clin Microbiol, 2020. 58(4).
- Proctor, D.M. , et al., Integrated genomic, epidemiologic investigation of Candida auris skin colonization in a skilled nursing facility. Nat Med, 2021. 27(8): p. 1401-1409.
- CDC, Screening: Patient Swab Collection. 2024.
- CDC. Identification of. 2024 [cited April 2025; Available from: https://www.cdc.gov/candida-auris/hcp/laboratories/identification-of-c-auris.html. /.
- Cortegiani, A. , et al., Epidemiology, clinical characteristics, resistance, and treatment of infections by Candida auris. J Intensive Care, 2018. 6: p. 69.
- Hata, D.J., R. Humphries, and S.R. Lockhart, Candida auris: An Emerging Yeast Pathogen Posing Distinct Challenges for Laboratory Diagnostics, Treatment, and Infection Prevention. Arch Pathol Lab Med, 2020. 144(1): p. 107-114.
- Osei Sekyere, J. , Candida auris: A systematic review and meta-analysis of current updates on an emerging multidrug-resistant pathogen. Microbiologyopen, 2018. 7(4): p. e00578.
- Bentz, M.L. , et al., Phenotypic switching in newly emerged multidrug-resistant pathogen Candida auris. Med Mycol, 2019. 57(5): p. 636-638.
- Du, H. , et al., Candida auris: Epidemiology, biology, antifungal resistance, and virulence. PLoS Pathog, 2020. 16(10): p. e1008921.
- Satoh, K. , et al., Candida auris sp. nov., a novel ascomycetous yeast isolated from the external ear canal of an inpatient in a Japanese hospital. Microbiol Immunol, 2009. 53(1): p. 41-4.
- Mahmoudi, S. , et al., Methods for identification of Candida auris, the yeast of global public health concern: A review. J Mycol Med, 2019. 29(2): p. 174-179.
- Zerrouki, H. , et al., Emergence of Candida auris in intensive care units in Algeria. Mycoses 2022, 65, 753–759. [Google Scholar] [CrossRef] [PubMed]
- Ruiz-Gaitán, A. , et al., Usefulness of Chromogenic Media with Fluconazole Supplementation for Presumptive Identification of Candida auris. Diagnostics (Basel), 2023. 13(2).
- Komorowski, A.S. , et al., Verification, Analytical Sensitivity, Cost-effectiveness, and Comparison of 4 Candida auris Screening Methods. Open Forum Infect Dis, 2024. 11(6): p. ofae017.
- Marathe, A. , et al., Utility of CHROMagar™ Candida Plus for presumptive identification of Candida auris from surveillance samples. Mycopathologia, 2022. 187(5-6): p. 527-534.
- Tamura, T., M. M. Alshahni, and K. Makimura, Evaluation of CHROMagar™ Candida Plus chromogenic agar for the presumptive identification of Candida auris. Microbiol Immunol, 2022. 66(6): p. 292-298.
- Keighley, C. , et al., Candida auris: Diagnostic Challenges and Emerging Opportunities for the Clinical Microbiology Laboratory. Curr Fungal Infect Rep, 2021. 15(3): p. 116-126.
- Snayd, M. , et al., Misidentification of Candida auris by RapID Yeast Plus, a Commercial, Biochemical Enzyme-Based Manual Rapid Identification System, in J Clin Microbiol. 2018: United States.
- Mizusawa, M. , et al., Can Multidrug-Resistant Candida auris Be Reliably Identified in Clinical Microbiology Laboratories?, in J Clin Microbiol. 2017: United States. p. 638-640.
- Lee, W.G. , et al., First three reported cases of nosocomial fungemia caused by Candida auris. J Clin Microbiol, 2011. 49(9): p. 3139-42.
- Ruiz Gaitán, A.C. , et al., Nosocomial fungemia by Candida auris: First four reported cases in continental Europe. Rev Iberoam Micol, 2017. 34(1): p. 23-27.
- Ding, C.H. , et al., The Pitfall of Utilizing a Commercial Biochemical Yeast Identification Kit to Detect Candida auris. Ann Clin Lab Sci, 2019. 49(4): p. 546-549.
- Ambaraghassi, G. , et al., Identification of Candida auris by Use of the Updated Vitek 2 Yeast Identification System, Version 8.01: a Multilaboratory Evaluation Study. J Clin Microbiol, 2019. 57(11).
- Tan, Y.E. , et al., Candida auris in Singapore: Genomic epidemiology, antifungal drug resistance, and identification using the updated 8.01 VITEK(Ⓡ)2 system. Int J Antimicrob Agents, 2019. 54(6): p. 709-715.
- Arnold, R.J. and J.P. Reilly, Fingerprint matching of E. coli strains with matrix-assisted laser desorption/ionization time-of-flight mass spectrometry of whole cells using a modified correlation approach. Rapid Commun Mass Spectrom, 1998. 12(10): p. 630-6.
- Marklein, G. , et al., Matrix-assisted laser desorption ionization-time of flight mass spectrometry for fast and reliable identification of clinical yeast isolates. J Clin Microbiol, 2009. 47(9): p. 2912-7.
- Bader, O. , et al., Improved clinical laboratory identification of human pathogenic yeasts by matrix-assisted laser desorption ionization time-of-flight mass spectrometry. Clin Microbiol Infect, 2011. 17(9): p. 1359-65.
- Vatanshenassan, M. , et al., Candida auris Identification and Rapid Antifungal Susceptibility Testing Against Echinocandins by MALDI-TOF MS. Front Cell Infect Microbiol, 2019. 9: p. 20.
- Xie, T.A. , et al., Accuracy of matrix-assisted LASER desorption ionization-time of flight mass spectrometry for identification of Candida. Biosci Rep, 2019. 39(10).
- Ahmad, A. , et al., A high-throughput and rapid method for accurate identification of emerging multidrug-resistant Candida auris. Mycoses, 2019. 62(6): p. 513-518.
- Sterkel, A. , et al., Viability of Candida auris and Other Candida Species after Various Matrix-Assisted Laser Desorption Ionization-Time of Flight (MALDI-TOF) Mass Spectrometry-Based Extraction Protocols, in J Clin Microbiol. 2018: United States.
- Normand, A.C. , et al., Optimization of MALDI-ToF mass spectrometry for yeast identification: a multicenter study. Med Mycol, 2020. 58(5): p. 639-649.
- Ghosh, A.K. , et al., Matrix-assisted laser desorption ionization time-of-flight mass spectrometry for the rapid identification of yeasts causing bloodstream infections. Clin Microbiol Infect, 2015. 21(4): p. 372-8.
- CDC. MicrobeNet. 2024 [cited April 2025; Available from: https://www.cdc.gov/microbenet/php/about/index.html.
- Ceballos-Garzon, A. , et al., Development and Validation of an in-House Library of Colombian Candida auris Strains with MALDI-TOF MS to Improve Yeast Identification. J Fungi (Basel), 2020. 6(2).
- Leach, L., Y. Zhu, and S. Chaturvedi, Development and Validation of a Real-Time PCR Assay for Rapid Detection of Candida auris from Surveillance Samples. J Clin Microbiol, 2018. 56(2).
- Kordalewska, M. , et al., Rapid and Accurate Molecular Identification of the Emerging Multidrug-Resistant Pathogen Candida auris. J Clin Microbiol, 2017. 55(8): p. 2445-2452.
- Hernández Felices, F.J. , et al., Evaluation of Eazyplex® LAMP test for fast Candida auris direct detection of colonized patients. Mycoses, 2024. 67(1): p. e13665.
- Ruiz-Gaitán, A.C. , et al., Molecular identification of Candida auris by PCR amplification of species-specific GPI protein-encoding genes. Int J Med Microbiol, 2018. 308(7): p. 812-818.
- Ibrahim, A. , et al., Development and standardization of a specific real-time PCR assay for the rapid detection of Candida auris. Eur J Clin Microbiol Infect Dis, 2021. 40(7): p. 1547-1551.
- Alvarado, M. , et al., Identification of Candida auris and related species by multiplex PCR based on unique GPI protein-encoding genes. Mycoses, 2021. 64(2): p. 194-202.
- CDC. Real-Time PCR Based Identification. 2024 [cited April 2025; Available from: https://www.cdc.gov/candida-auris/hcp/laboratories/real-time-pcr-identification.html.
- Berlau, A. , et al., Evaluation of the Eazyplex(®)Candida ID LAMP Assay for the Rapid Diagnosis of Positive Blood Cultures. Diagnostics (Basel), 2024. 14(19).
- Lin, Z.Z. , et al., A Pooled Analysis of the PCR for the Detection of Candida Auris. Clin Lab, 2022. 68(7).
- Caméléna, F. , et al., Multicenter Evaluation of the FilmArray Blood Culture Identification 2 Panel for Pathogen Detection in Bloodstream Infections. Microbiol Spectr, 2023. 11(1): p. e0254722.
- Zhang, S.X. , et al., Multicenter Evaluation of a PCR-Based Digital Microfluidics and Electrochemical Detection System for the Rapid Identification of 15 Fungal Pathogens Directly from Positive Blood Cultures. J Clin Microbiol, 2020. 58(5).
- Franco, L.C. , et al., Validation of a qualitative real-time PCR assay for the detection of Candida auris in hospital inpatient screening. J Clin Microbiol, 2024. 62(6): p. e0015824.
- Ramírez, J.D. , et al., Molecular Detection of Candida auris Using DiaSorin Molecular Simplexa(®) Detection Kit: A Diagnostic Performance Evaluation. J Fungi (Basel), 2023. 9(8).
- Rosa, R. , et al., Impact of In-house Candida auris Polymerase Chain Reaction Screening on Admission on the Incidence Rates of Surveillance and Blood Cultures With and Associated Cost Savings. Open Forum Infect Dis, 2023. 10(11): p. ofad567.
- Sattler, J. , et al., Comparison of Two Commercially Available qPCR Kits for the Detection of Candida auris. J Fungi (Basel), 2021. 7(2).
- Mulet Bayona, J.V. , et al., Validation and implementation of a commercial real-time PCR assay for direct detection of Candida auris from surveillance samples. Mycoses, 2021. 64(6): p. 612-615.
- Yamamoto, M. , et al., Rapid Detection of Candida auris Based on Loop-Mediated Isothermal Amplification (LAMP), in J Clin Microbiol. 2018: United States.
- Lim, D.H. , et al., Development of a Simple DNA Extraction Method and Candida Pan Loop-Mediated Isothermal Amplification Assay for Diagnosis of Candidemia. Pathogens, 2022. 11(2).
- Narayanan, A. , et al., ClaID: a Rapid Method of Clade-Level Identification of the Multidrug Resistant Human Fungal Pathogen Candida auris. Microbiol Spectr, 2022. 10(2): p. e0063422.
- Lockhart, S.R. , et al., Simultaneous Emergence of Multidrug-Resistant Candida auris on 3 Continents Confirmed by Whole-Genome Sequencing and Epidemiological Analyses. Clin Infect Dis, 2017. 64(2): p. 134-140.
- CDC. GITHUB. 2021 [cited April 2025; Available from: https://github.com/CDCgov/mycosnp.
- de Groot, T. , et al., Optimization and Validation of Candida auris Short Tandem Repeat Analysis. Microbiol Spectr, 2022. 10(5): p. e0264522.
- Magobo, R. , et al., Multilocus sequence typing of azole-resistant Candida auris strains, South Africa. S Afr J Infect Dis, 2020. 35(1): p. 116.
- Biswas, C. , et al., Genetic Heterogeneity of Australian Candida auris Isolates: Insights From a Nonoutbreak Setting Using Whole-Genome Sequencing. Open Forum Infect Dis, 2020. 7(5): p. ofaa158.
- CDC. Antifungal Susceptibility Testing for. 2024 [cited April 2025; Available from: https://www.cdc.gov/candida-auris/hcp/laboratories/antifungal-susceptibility-testing.html.
- Jones, C.R. , et al., The laboratory investigation, management, and infection prevention and control of Candida auris: a narrative review to inform the 2024 national guidance update in England. J Med Microbiol, 2024. 73(5).
- Arendrup, M.C. , et al., Comparison of EUCAST and CLSI Reference Microdilution MICs of Eight Antifungal Compounds for Candida auris and Associated Tentative Epidemiological Cutoff Values. Antimicrob Agents Chemother, 2017. 61(6).
- Szekely, A., A. M. Borman, and E.M. Johnson, Candida auris Isolates of the Southern Asian and South African Lineages Exhibit Different Phenotypic and Antifungal Susceptibility Profiles In Vitro. J Clin Microbiol, 2019. 57(5).
- Kordalewska, M. , et al., Understanding Echinocandin Resistance in the Emerging Pathogen Candida auris. Antimicrob Agents Chemother, 2018. 62(6).
- Ceballos-Garzon, A. , et al., Head-to-head comparison of CLSI, EUCAST, Etest and VITEK®2 results for Candida auris susceptibility testing. Int J Antimicrob Agents, 2022. 59(4): p. 106558.
- Siopi, M. , et al., Evaluation of the Vitek 2 system for antifungal susceptibility testing of Candida auris using a representative international panel of clinical isolates: overestimation of amphotericin B resistance and underestimation of fluconazole resistance. J Clin Microbiol, 2024. 62(4): p. e0152823.
- Patwardhan, S.A. , et al., Candida auris - Comparison of sensititre YeastOne and Vitek 2 AST systems for antifungal susceptibility testing - A single centre experience. Indian J Med Microbiol, 2024. 50: p. 100618.
- Asadzadeh, M. , et al., Evaluation of Etest and MICRONAUT-AM Assay for Antifungal Susceptibility Testing of Candida auris: Underestimation of Fluconazole Resistance by MICRONAUT-AM and Overestimation of Amphotericin B Resistance by Etest. Antibiotics (Basel), 2024. 13(9).
- Frías-De-León, M.G. , et al., Antifungal Resistance in Candida auris: Molecular Determinants. Antibiotics (Basel), 2020. 9(9).
- Kordalewska, M. and D.S. Perlin, Molecular Diagnostics in the Times of Surveillance for Candida auris. J Fungi (Basel), 2019. 5(3).
- Marinach, C. , et al., MALDI-TOF MS-based drug susceptibility testing of pathogens: the example of Candida albicans and fluconazole. Proteomics, 2009. 9(20): p. 4627-31.
- Vella, A. , et al., Potential Use of MALDI-ToF Mass Spectrometry for Rapid Detection of Antifungal Resistance in the Human Pathogen Candida glabrata. Sci Rep, 2017. 7(1): p. 9099.
- Theparee, T., S. Das, and R.B. Thomson, Jr., Total Laboratory Automation and Matrix-Assisted Laser Desorption Ionization-Time of Flight Mass Spectrometry Improve Turnaround Times in the Clinical Microbiology Laboratory: a Retrospective Analysis. J Clin Microbiol, 2018. 56(1).
Figure 1.
Workflow Algorithm for Detection in Clinical and Surveillance Samples. Legend: Clinical and surveillance samples are detected using culture-based methods, with colonies confirmed by MALDI-TOF and biochemical tests (e.g., VITEK 2). Biochemical tests risk misidentification and require CDC algorithm interpretation (Table 2). Alternative screening includes DNA-based confirmatory tests and chromogenic agar for presumptive identification. WGS aids outbreak and epidemiological investigations. Red lines indicate confirmatory tests. Abbreviations: AFST, Antifungal Susceptibility Testing; BDG, Beta-D-Glucan; CDC, Centers for Disease Control and Prevention; MALDI-TOF MS, Matrix-Assisted Laser Desorption/Ionization Time-of-Flight Mass Spectrometry; PCR, Polymerase Chain Reaction; VITEK 2, VITEK 2 Biochemical Identification System; WGS, Whole Genome Sequencing.
Figure 1.
Workflow Algorithm for Detection in Clinical and Surveillance Samples. Legend: Clinical and surveillance samples are detected using culture-based methods, with colonies confirmed by MALDI-TOF and biochemical tests (e.g., VITEK 2). Biochemical tests risk misidentification and require CDC algorithm interpretation (Table 2). Alternative screening includes DNA-based confirmatory tests and chromogenic agar for presumptive identification. WGS aids outbreak and epidemiological investigations. Red lines indicate confirmatory tests. Abbreviations: AFST, Antifungal Susceptibility Testing; BDG, Beta-D-Glucan; CDC, Centers for Disease Control and Prevention; MALDI-TOF MS, Matrix-Assisted Laser Desorption/Ionization Time-of-Flight Mass Spectrometry; PCR, Polymerase Chain Reaction; VITEK 2, VITEK 2 Biochemical Identification System; WGS, Whole Genome Sequencing.
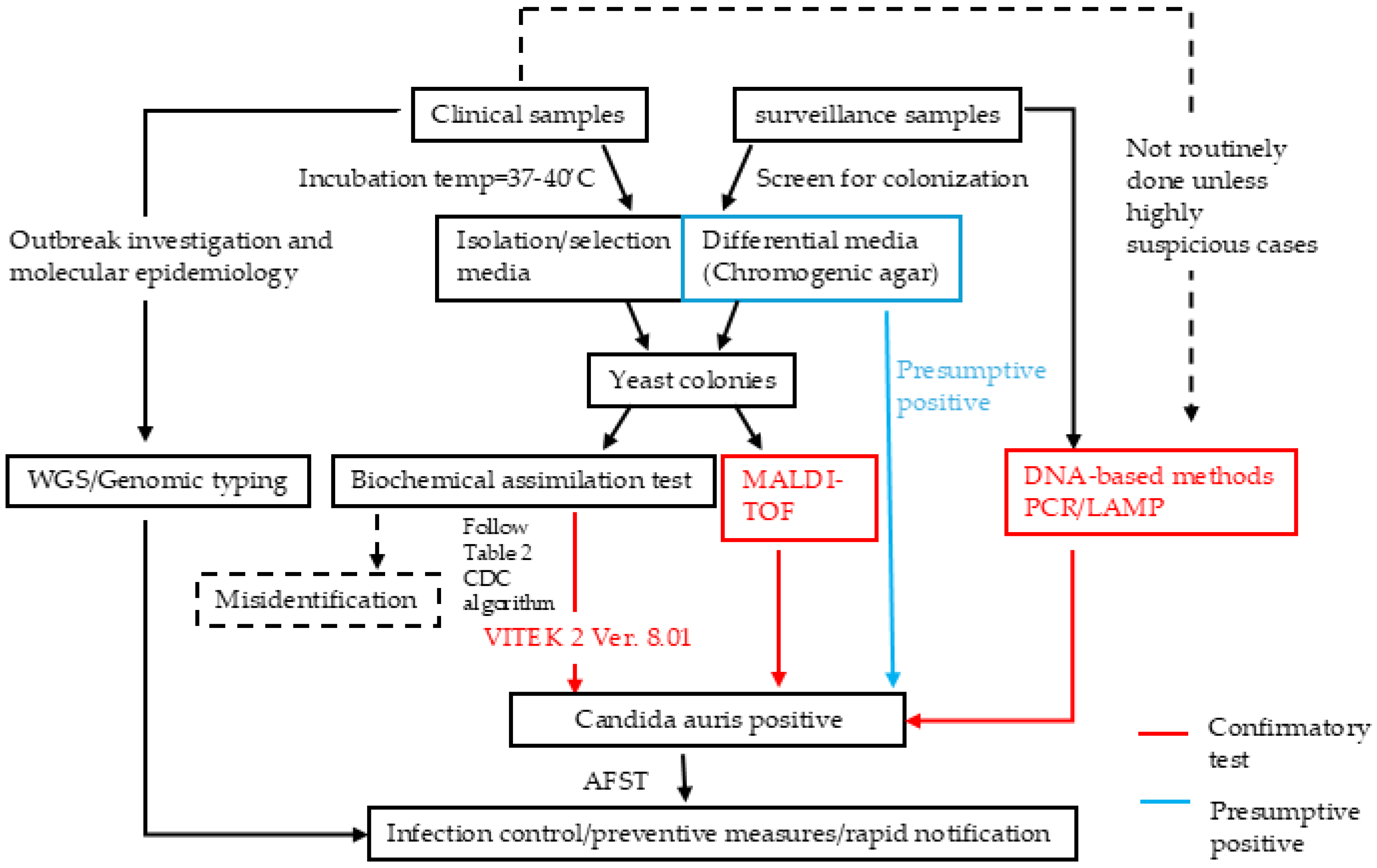
Figure 2.
Recommended Sample Collection Sites for Screening. Legend: Swab the bilateral axillae and groins 3–5 times with the soft end of the collection swab. Recent studies suggest including nasal swabs to improve sensitivity.
Figure 2.
Recommended Sample Collection Sites for Screening. Legend: Swab the bilateral axillae and groins 3–5 times with the soft end of the collection swab. Recent studies suggest including nasal swabs to improve sensitivity.
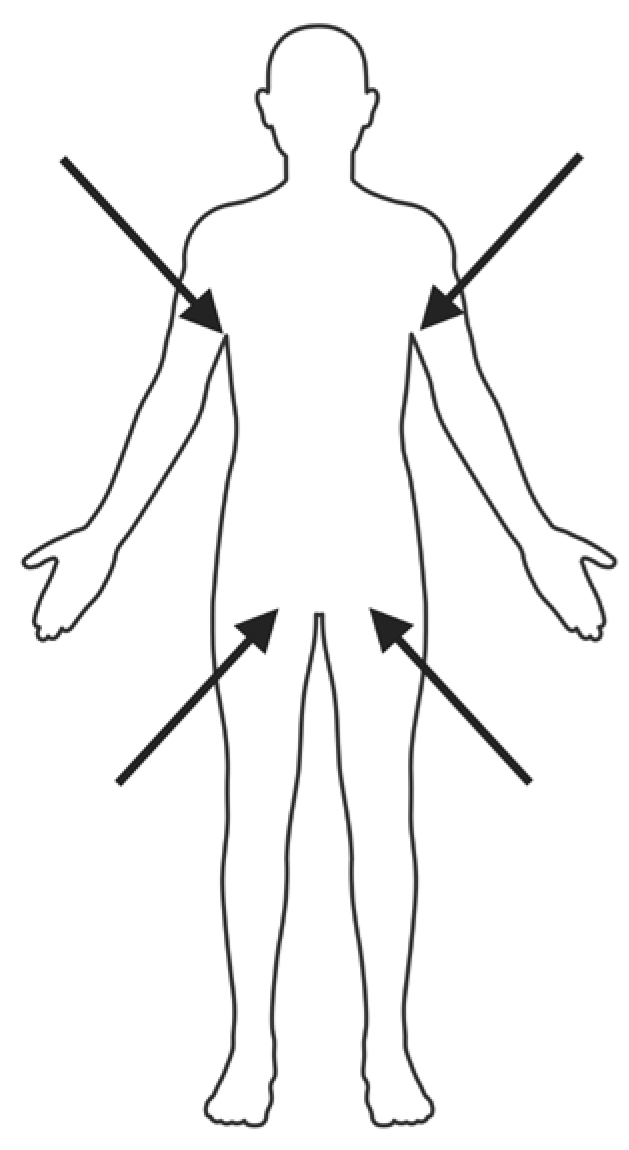
Figure 3.
Workflow of Surveillance Sample Testing Using Chromogenic Agar. Legend:10 µl of surveillance sample was streaked onto the culture media in a Z-pattern for optimal isolation. Plates were incubated at 37°C for 48 to 72 h, with presumptive C. auris appearing green colonies on the media (per manufacturer’s recommendation).
Figure 3.
Workflow of Surveillance Sample Testing Using Chromogenic Agar. Legend:10 µl of surveillance sample was streaked onto the culture media in a Z-pattern for optimal isolation. Plates were incubated at 37°C for 48 to 72 h, with presumptive C. auris appearing green colonies on the media (per manufacturer’s recommendation).
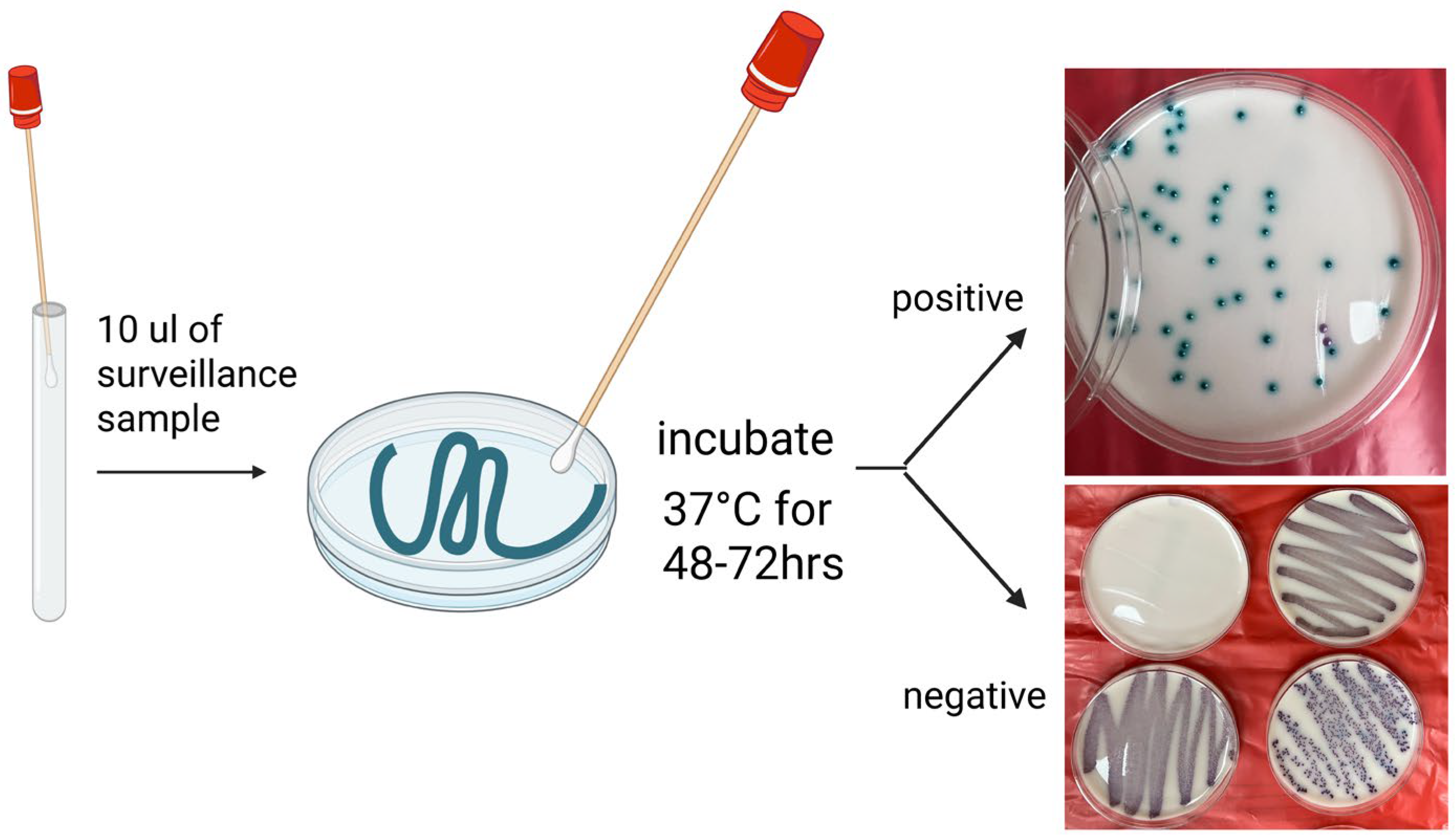
Figure 4.
General Workflow of matrix-assisted laser desorption ionization–time of flight mass spectrometry (MALDI-ToF MS)-Based Identification Analysis. Legend: (1) C. auris colonies are cultivated on solid agar, followed by sample preparation via tube-based protein extraction or direct smear methods. (2) Prepared samples are transferred onto a MALDI-TOF MS target plate and overlaid with a suitable matrix solution. (3) Samples are analyzed using MALDI-TOF MS to generate mass spectra. (4) Experimental mass spectra are matched against a database of reference strain spectra to achieve species-level identification.
Figure 4.
General Workflow of matrix-assisted laser desorption ionization–time of flight mass spectrometry (MALDI-ToF MS)-Based Identification Analysis. Legend: (1) C. auris colonies are cultivated on solid agar, followed by sample preparation via tube-based protein extraction or direct smear methods. (2) Prepared samples are transferred onto a MALDI-TOF MS target plate and overlaid with a suitable matrix solution. (3) Samples are analyzed using MALDI-TOF MS to generate mass spectra. (4) Experimental mass spectra are matched against a database of reference strain spectra to achieve species-level identification.
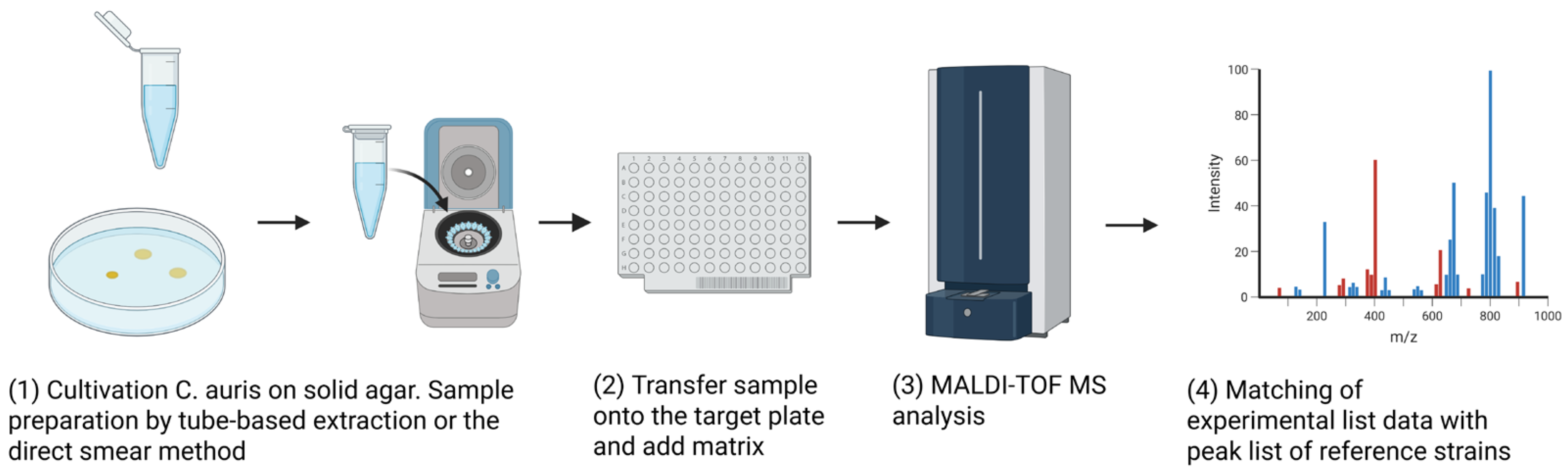

Table 1.
Summary of Diagnostic tools for C. auris.
| Category | Diagnostic Method | Mechanism | Highlights | Strengths | Weaknesses/Limitations | References |
|---|---|---|---|---|---|---|
| Culture-Based | Mycological media/ Selective media/ Chromogenic media | 1. Requires higher incubation temperature(37-40'C) than routine culture. 2. Add saline, carbohydrates, or color indicators to differentiate from similar species |
1. SCA/SAM Media Se/Sp:100%/100% 2. CHROMagarTM with Pal’s medium Se/Sp: 100%/100% 3. CHROMagar™ Candida Plus Se/Sp: 90-100%/98-100% |
1. basis for culture-based methods (eg. Biochemical assimilation methods and MALDI-TOF) 2. Simple, widely available, low-cost 3. Gold-standard for diagnosis in clinical samples. Enables AFST. |
1. Slow (48-72 hrs) 2. Various accuracy among different media. Non-specific colony morphology, prone to misidentification, requires additional confirmation (MALDI-TOF MS or molecular methods) |
[15,16,17,18,19,20] |
| Culture-Based | Biochemical Tests (VITEK, API, Microscan) | Analysis of metabolic profile through carbohydrate assimilation, nitrogen utilization, and enzymatic activity | 1. Vitek 2 Version. 8.01 is confirmatory 2. API 20C AUX or API ID 32C leads to frequent misidentification 3. MicroScan/ BD Pheonix has no C. auris database |
1. Low cost and easy to use (automated) 2. A rapid AFST tool reliable for azoles |
1. Requires database updates 2. Various misidentification rates among different commercial assays. Often requires confirmatory test following CDC algorithm (Table 2) |
[21] |
| Culture-Based | MALDI-TOF MS | Analysis of protein profiles and comparing them to reference databases. (Figure 4) | 1. Accuracy depends on databases, sample preparation, and instrument calibration 2. Limited use for AFST with no clinical breakpoint of MPCC |
1. Rapid (4-5 hrs post culture) 2. Highly specific(Sp>90%) when database is updated 3. Cost-effective |
1. Requires database updates, 2. Expensive equipment, limited access in resource-poor settings |
Kathuria [22] et al., 2015 Kwon et al., 2019 |
| Culture-Independent | DNA-Based Assays (PCR/LAMP) | DNA amplification using species-specific primers (e.g., ITS, D1/D2 regions) | 1. Both LDTs and Commercial assays demonstrate reliable accuracy(Se/ Sp>90%), LAMP has lower sensitivity 2. Current FDA-approved Commercial assays for blood culture: GenMark ePlex BCID-FP and BioFire FilmArray BCID2 |
1. Accurate and rapid, useful for colonization screening and outbreak control in healthcare settings | 1. Cannot determine antifungal susceptibility and detect DNA from both viable and non-viable C. auris cells 2. LAMP has lower sensitivity |
[23] |
| Culture-Independent | T2 MR assay | Superparamagnetic nanoparticles bind target DNA/RNA, altering T2 relaxation for MR detection | Rapid (<3 hours) and highly sensitive detection for surveillance and bloodstream infection | Research use only | [24] | |
| Culture-Independent | Whole-Genome Sequencing (WGS)/ genomic typing | High-resolution genetic analysis | Tracking outbreaks, identifying strains, and analyzing resistance, virulence, and epidemiology. Not usually used for individual diagnosis. | WGS: High resolution, gold standard for outbreaks investigation | Costly, requires specialized analysis | [25,26,27,28] |
| STR typing: High reproducibility, aligns well with WGS | Differentiate C. auris strains only if >30 SNP differences | |||||
| MLST: Differentiates C. auris, supports resistance surveillance | Low resolution within clades,limited for outbreaks | |||||
| AFLP: Rapid, cost-effectiveness | Poor reproducibility, inconsistent clustering |
|||||
| Culture-Independent | Beta-D-glucan (BDG) assays | Detection of fungal cell wall components | Non-invasive, useful for early detection for clinical samples | Limited sensitivity and low specificity for invasive candidiasis | [29,30] |
Legend: Diagnostic tools for C. auris are broadly divided into culture-dependent and culture-independent methods; this table summarizes the mechanisms, updated highlights, strengths, and limitations of each tool. Abbreviations: Se, Sensitivity; Sp, Specificity; SCA, Specific C. auris Medium; SAM, Selective Auris Medium; CHROMagar™, Chromogenic Agar; AFST, Antifungal Susceptibility Testing; VITEK 2, VITEK 2 Biochemical Identification System; API, Analytical Profile Index; MALDI-TOF MS, Matrix-Assisted Laser Desorption/Ionization Time-of-Flight Mass Spectrometry; MPCC, Minimal Profile Change Concentration; PCR, Polymerase Chain Reaction; LAMP, Loop-Mediated Isothermal Amplification; FDA, U.S. Food and Drug Administration; T2 MR, T2 Magnetic Resonance; WGS, Whole Genome Sequencing; STR, Short Tandem Repeat; SNP, Single Nucleotide Polymorphism; MLST, Multilocus Sequence Typing; AFLP, Amplified Fragment Length Polymorphism; BDG, Beta-D-Glucan.
Table 2.
Summary of CDC Algorithm Based on Initial Laboratory Findings.
| Identification Method | Database/Software, if applicable | is confirmed if initial identification is C auris. | is possible if the following initial identifications are given. Further work-up is needed to determine if the isolate is . |
|---|---|---|---|
| Bruker Biotyper MALDI-TOF | RUO libraries (Versions 2014 [5627] and more recent) | n/a | |
| CA System library (Version Claim 4) | n/a | ||
| bioMérieux VITEK MS MALDI- TOF | RUO library (withSaccharomycetaceae update) | n/a | |
| IVD library (v3.2) | n/a | ||
| Older IVD libraries | n/a |
C. haemulonii C. lusitaniae No identification |
|
| VITEK 2 YST | Software version 8.01* |
C. haemulonii C. duobushaemulonii Candida spp. not identified |
|
| Older versions | n/a |
C. haemulonii C. duobushaemulonii Candida spp. not identified |
|
| API 20C | n/a |
Rhodotorula glutinis (without characteristic red color) C. sake Candida spp. not identified |
|
| API ID 32C | n/a |
C.intermedia C.sake Saccharomyces kluyveri |
|
| BD Phoenix | n/a |
C. catenulata C. haemulonii Candida spp. not identified |
|
| MicroScan | n/a |
C. lusitaniae** C. guilliermondii** C. parapsilosis** C. famata Candida spp. not identified |
|
| RapID Yeast Plus | n/a |
C. parapsilosis** Candida spp. not identified |
|
| GenMark ePlex BCID-FP Panel | n/a |
Legend: CDC guidelines for confirming or suspecting based on biochemical assimilation tests and database versions. Abbreviations: RUO, Research Use Only; CA System, Chromogenic Agar System; IVD, In Vitro Diagnostic; VITEK 2 YST, VITEK 2 Yeast Susceptibility Testing; API 20C AUX, Analytical Profile Index 20C Auxanographic Yeast Identification System; API ID 32C, Analytical Profile Index ID 32C Yeast Identification System; BD Phoenix, Becton Dickinson Phoenix Identification System; MicroScan, MicroScan WalkAway Identification System; RapID, RapID Yeast Plus System; GenMark ePlex BCID-FP, GenMark ePlex Blood Culture Identification–Fungal Pathogen Panel.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



