Submitted:
09 May 2025
Posted:
12 May 2025
You are already at the latest version
Abstract
Magnesium (Mg2+) has gained oncologists’ attention due to its wide range of biological functions and frequent use as a complementary or integrative agent. This review outlines Mg's actions, its complex role in carcinogenesis and tumor risk, and clinical issues. Mg2+ is essential in numerous biochemical processes, including adenosine triphosphate production, cellular signal transduction, DNA, RNA and protein synthesis, and bone formation. The authors conducted a literature review on MEDLINE, PubMed, EMBASE, and the Web of Science to report the relationship between Mg2+ and cancer. Pertinent full-text articles were thoroughly examined, and the most relevant ones were selected for inclusion in this review. Mg2+ alterations are associated with cancer risk variably since scientific evidence is not univocal, except for colorectal cancer. Chronic Mg2+ deficiency leads to immune dysfunctions and enhanced baseline inflammation associated with oxidative stress related to various age-associated morbidities and cancer. On the other hand, Mg2+ deficiency is associated with several clinical settings, such as drug or chemotherapy-related hypomagnesemia, postoperative pain, cachexia, opioid-induced constipation, normal tissue protection from radiation damage, and prevention of nephrotoxicity. The issue of Mg2+ supplementation is also analyzed. A balanced diet usually provides sufficient Mg2+, but supplementation may be necessary in some clinical settings. Excessive supplementation can negatively impact immune function and should be avoided.
Keywords:
Magnesium
; carcinogenesis
; cancer risk
; hypomagnesemia
; drug interactions
1. Introduction
In the last decades, there has been increasing interest in the role of magnesium (Mg2+) in many clinical settings, including aging and cancer [1,2,3]. Several diseases have been associated with Mg2+ deficits, such as cardiovascular and respiratory diseases, type 2 diabetes, respiratory airways constrictive syndromes, asthma, depression, stress-related, gastrointestinal, neurologic, and muscular diseases, liver cirrhosis, thyroid and parathyroid gland dysfunction, and cancer [4].
The role of Mg2+ in such a wide range of diseases is not surprising since Mg2+ plays an essential role in several cellular and physiological functions. It is involved in more than 300 enzymatic reactions involving ATP transfer, intermediary metabolism, potassium, and calcium transport, and acting as a co-factor in DNA, RNA, protein synthesis, and cellular proliferation [5]. Mg2+ is also essential for efficient energy production, oxidative phosphorylation, and glycolysis [5].
Despite Mg2+ being the second most abundant cation in the cell, its role in cellular physiology and pathology still needs to be elucidated. Mg2+ homeostasis is physiologically regulated by Mg2+ transporters, including mitochondrial RNA splicing protein 2 (MRS2), transient receptor potential cation channel subfamily M, member 6/7 (TRPM6/7), magnesium transporter 1 (MAGT1), solute carrier family 41 member 1 (SCL41A1), and cyclin and CBS domain divalent metal cation transport mediator (CNNM) proteins [6]. Since Mg2+ is a crucial regulator of cell proliferation, Mg2+ transporters have a complex enabling relationship with cancer growth and metastatic dissemination [7]. Aberrant expression of Mg2+ transporters of the TRPM, CNNM, and SCL41 protein families is involved in tumor progression and may represent a potential therapeutic target [7]. Moreover, Mg2+ has complex relationships with aging and inflammation [4]. Chronic Mg2+ insufficiency and aging are frequently associated with low-grade chronic inflammation and an excessive generation of free radicals [2,4].
Preclinical investigations on Mg2+ deficiency have found evidence of complex pro-inflammatory pathways in several cell types [8]. The roles of free radicals, cytokines, neuropeptides, endotoxin, endogenous antioxidants, and vascular permeability, and interventions to limit the inflammatory response associated with these parameters, are outlined in fundamental studies of Mg2+ deficiency. Mg2+ alterations are also associated with several events, such as genomic instability, telomere attrition, epigenetic alterations, loss of proteostasis, deregulated nutrient sensing, mitochondrial dysfunction, cellular senescence, stem cell exhaustion, altered intercellular communication, disabled autophagy, dysbiosis, and chronic inflammation [2,4]. Therefore, maintaining an optimal Mg2+ balance throughout life may help prevent oxidative stress and chronic conditions associated with aging.
Dietary Mg2+ and/or Mg2+ consumed in drinking water (generally more bioavailable than that contained in food) or alternative supplements should be considered in correcting deficits [9]. Besides hard water, dietary sources rich in Mg2+ are whole and unrefined grains, seeds, cocoa, nuts, almonds, and green leafy vegetables known to be beneficial for human health. However, the daily dietary intake of Mg2+ is frequently below that recommended in Western countries [9].
2. Magnesium and Carcinogenesis
Mg2+ plays a pivotal role in several biochemical reactions in the body, and its significance extends to cancer research and treatment. However, it is important to approach this issue knowing that scientific data are in progress and that conclusive findings about the connection between Mg2+ and cancer are still pending.
The relationships between Mg2+, carcinogenesis, and cancer biology are remarkably complex and still need clarification, with conflicting results reported from many experimental, epidemiological, and clinical studies [10,11]. Mg2+ deficiency may result in both anti-neoplastic and pro-tumoral effects [11,12]. Preclinical studies showed that cultured neoplastic cells tend to accumulate Mg2+, and high intracellular levels of this cation may confer a metabolic superiority, contributing to DNA alterations and promoting the acquisition of an immortal phenotype [11]. In Mg2+-deficient mice, low Mg2+ levels have paradoxical effects, both limiting and fostering carcinogenesis, since primary tumor growth inhibition may occur despite increased metastatic potential [11].
Nearly two decades ago, studies in preclinical models showed that Mg2+ depletion may inhibit solid tumor growth and paradoxically increase metastasis formation via enhanced tumor cell adhesion due to altered expression of surface adhesion molecules [13]. Since then, Mg2+ has been demonstrated to have a role in the functionality of membrane ion channels in the tumor compared to normal tissues [13]. Increased expression and altered half-life of transporters/channels create a sustained high intracellular concentration of specific ions, e.g., calcium and chlorine that can activate proteolysis, promoting the invasive capacity of malignant cells by degradation of the extracellular matrix, a necessary step for metastasis formation [14]. High calcium concentrations within tumor cells may also inhibit tumor immunity, and Mg2+, an essential intracellular and physiological calcium antagonist, may inhibit carcinogenesis [13,14].
Mg2+ can inhibit carcinogenesis in an intracellular concentration-dependent manner [8,9]. This phenomenon can be evidenced by the fact that Mg2+-deficient animals are at a higher risk of developing carcinomas, and most cancer patients are Mg2+-deficient. On the other hand, an optimal Mg2+ level reduces cancer risk by protecting cells from DNA damage by free radicals. Mg2+ reduces mutations to cells in vitro, and inactively dividing cells like precancerous cells are most vulnerable to low Mg2+ levels. Mg2+ also reduces tumorigenesis, slows its development, and decreases actin activity, cell motility, and invasion of tumor cells [15,16,17,18]. Low Mg2+ levels are also associated with a poor prognosis of cancer and aggravate systemic inflammation. Increasing extracellular magnesium concentration induces apoptosis of cancer cells; however, Mg2+ supplementation does not cause a cancerous cell to die. It will speed up the growth of a cancerous cell as it needs energy to die.
Mg2+ and calcium ions control a diverse and essential range of cellular processes, such as gene transcription, cell proliferation, metabolism, neoplastic transformation, angiogenesis, metastatic potential, immune response, and treatment [17]. Mg2+ is a co-factor for many enzymes, including those involved in the body's antioxidant defenses and DNA repair mechanisms. By supporting these processes, Mg2+ could theoretically reduce oxidative stress and genomic instability in cancer development. Mg2+ deficiency may also be associated with inflammation and increased free radicals, where inflammatory mediators and free radicals could cause oxidative DNA damage and tumor formation [6,7]. Mg2+ is also involved in mitochondrial function, apoptosis, and resistance to treatment. Alteration in Mg2+ channels' expression and/or activity is frequent in cancer cells and human tumor tissues [7,18]. In vivo, Mg2+ deficiency and the consequent inflammation can trigger anti- and pro-tumor effects. Alterations in the expression of the transient receptor potential melastatin, type 7 (TRPM7) epithelial Mg2+ channel are frequent in cancer cells and human tumor tissues. It correlates with cell proliferation and/or migration [6,7]. TRPM7 may play an essential role due to its channeling function mediating Ca2+ and Mg2+ influx and kinase activity, likely regulating actomyosin contractility [7,18].
Mg2+ plays an essential role in energy production by acting as a co-factor for most glycolysis enzymes, the serine synthesis pathway, and the tricarboxylic acid cycle [19]. Glucose is the primary energy substrate for cancer cells, which can reprogram their metabolism to grow. Recent findings have shown that the dual-specificity phosphatases of regenerating liver (PRL-1, -2, and -3) have a role in oncogenesis and metabolic reprogramming mediated by Mg2+ homeostasis, shifting the energy source preference to glucose consumption and fueling serine/glycine pathway and regulating PI3 kinase/mammalian target of rapamycin complex [19].
Overall, adequate Mg2+ levels are thought to help maintain normal cell function and could potentially protect against the development of certain cancers, although the role of supplementation remains unresolved.
3. Magnesium and Cancer Treatment
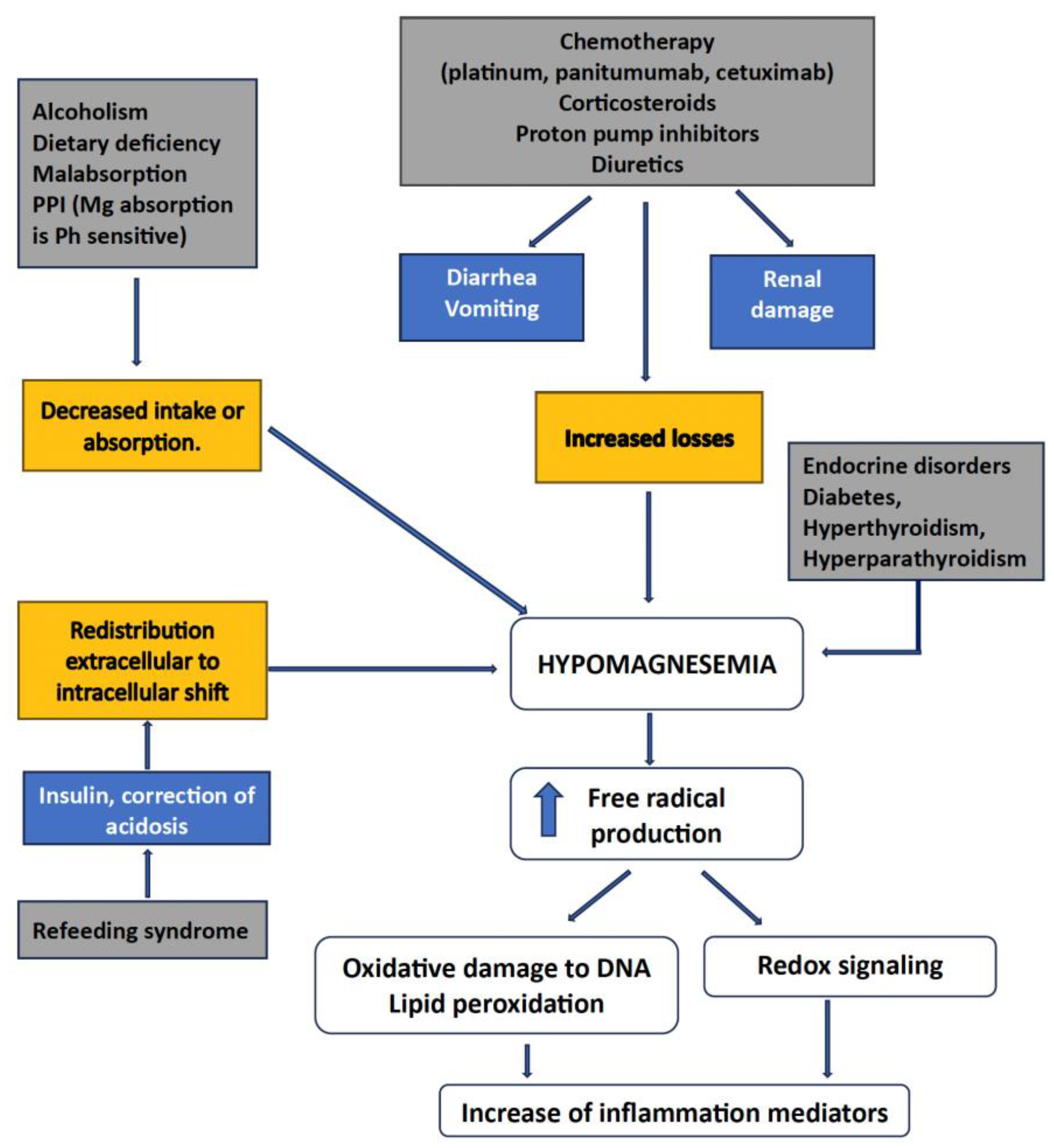
Mg2+'s role in cancer treatment is multifaceted and not entirely clear. Some anti-cancer agents can cause hypomagnesemia, which often necessitates Mg2+ supplementation to alleviate symptoms and support overall health during treatment [20]. However, whether Mg2+ supplementation directly contributes to cancer treatment efficacy or outcomes is still uncertain. Figure n. 1 shows the interelations between hypomagnesemia and cancer-associated features.
Figure 1.
Interrelations between Mg++ and cancer.
3.1. Hypomagnesemia
Disorders of the divalent ions are frequently observed in cancer patients, most notably hypomagnesemia, hypocalcemia, hypercalcemia, and hypophosphatemia [21]. These electrolyte imbalances may be related both to the side effects of anti-cancer therapy and the underlying malignancy as paraneoplastic syndromes. Electrolyte imbalances impact negatively on patients’ quality of life, leading to potentially life-threatening complications that may require hospitalization and usually carry a dismal prognosis [21,22]. Drugs linked to hypomagnesemia include antibiotics (e.g., aminoglycosides, amphotericin B), diuretics, anti-neoplastic drugs (platinum salts and anti-EGFR antibodies), calcineurin inhibitors, and proton pump inhibitors. Recognition, treatment, and prevention of hypomagnesemia in patients receiving high-risk anti-cancer agents is mandatory, as well as developing effective therapeutic and preventive strategies [23].
The causes of hypomagnesemia can be categorized according to the pathophysiologic mechanism: decreased intake, transcellular shift, and gastrointestinal and renal losses [24,25]. Cancer patients may suffer from opportunistic infections and cardiovascular complications therefore receiving drugs that can cause or exacerbate hypomagnesemia [21,25]. Moreover, several anti-cancer therapies are directly responsible for hypomagnesemia, including platinum-based chemotherapy, anti-EGFR monoclonal antibodies, human EGFR-2 target inhibitors, and calcineurin inhibitors [25]. Urinary indicators, such as the fractional excretion of Mg2+, can help etiology identification.
The management of hypomagnesemia depends on the degree of hypomagnesemia and the underlying cause. Serum Mg2+ levels should be obtained before oncological treatments and routinely monitored throughout treatment. Hsieh et al. conducted a systematic review and meta-analysis of retrospective and randomized trials comparing hypomagnesemia with normal Mg2+ levels in 1723 wild-type KRAS metastatic colorectal cancer (CRC) patients [26]. Patients with hypomagnesemia demonstrated better progression-free survival (Hazard Ratio [HR]: 0.64; 95% Confidence Interval [CI): 0.47-0.88), overall survival (HR 0.72; 95% CI: 0.53-0.92), and objective response rate (Risk ratio [RR]: 1.81; 95% CI 1.30-2.52) confirmed for progression-free survival also in subgroup analysis [26].
3.2. Platinum Salts
Platinum salts are still the cornerstone of many chemotherapeutic regimens. The use of platinum salts, particularly cisplatin, may cause symptomatic hypomagnesemia and significant nephrotoxicity [27]. Several systematic reviews showed that fluid hydration and parenteral Mg2+ supplementation prevent cisplatin-induced hypomagnesemia and nephrotoxicity, although the best schedule is uncertain [28,29].
3.3. Anti-EGFR Antibodies
Hypomagnesemia is a recognized side-effect of the anti-epidermal growth factor receptor (EGFR) antibodies cetuximab- or panitumumab-based regimens for metastatic CRC [30,31,32,33]. Moreover, these monoclonal antibodies are often delivered with oxaliplatin, another potential contributing cause. These anti-EGFR agents may cause hypomagnesemia by impeding EGF-dependent activation of TRPM6, the principal cation channel responsible for Mg2+ transcellular absorption in the intestine and kidney. Limited observations also suggest that hypomagnesemia could influence tumor response to cetuximab [30]. Petrelli et al. conducted a systematic review and pooled analysis of randomized studies on the risk of anti-EGFR monoclonal antibody-related hypomagnesemia [34]. The incidence of hypomagnesemia was 17% among the patients treated with anti-EGFR agents. These patients show a risk of developing hypomagnesemia, significantly increased compared with control patients (overall relative risk of 5.83; p < 0.00001). The risk is even higher for panitumumab, which is correlated with the increased incidence of other side effects such as diarrhea and dehydration. However, hypomagnesemia does not seem linked with any severe complications.
3.4. Proton Pump Inhibitors
Proton pump inhibitors are reportedly potential risk factors for hypomagnesemia [35]. A multicenter study with a propensity score-matched analysis assessed the impact of proton pump inhibitors on the risk of grade 3-4 hypomagnesemia in 165 patients with metastatic CRC receiving panitumumab [35]. The incidence of grade 3-4 hypomagnesemia was significantly higher in the proton pump inhibitors group than in the control group, both before (20.0% versus 8.0%, p=0.026) and after propensity score matching (16.2% versus 0%, p = 0.025). In the propensity score-matched cohort, the risk of grade 3-4 hypomagnesemia was significantly higher in the proton pump inhibitors group (OR 2.19; 95% CI 1.69-2.84; p=0.025).
3.5. Dietary Mg2+ Supplementation
Adequate dietary Mg2+ may be protective against chemotherapy-associated hypomagnesemia. Liu et al. carried out a daily dietary replacement approach through Mg2+-rich foods to maintain adequate magnesium levels during platinum-based treatment for ovarian cancer [36]. Among 26 patients enrolled, those who were adherent to diet (76%) had a significantly lower incidence of hypomagnesemia (19% versus 80%, p=0.03) and less need for intravenous Mg2+ (6% versus 60%, p =0.03) than those who were non-adherent.
3.6. Cardiotoxicity
Chemotherapy and newer targeted therapies may cause dangerous cardiovascular adverse events. The National Health and Nutrition Examination surveyed 1807 cancer survivors, followed up for seven years. Overall, 51% of patients died of cancer and 33% of heart disease [37]. The potential cardiovascular toxicity of anti-cancer agents included QT prolongation syndrome, which is associated with potentially lethal cardiac arrhythmias. The treatment of such adverse events consists of intravenous administration of Mg2+ sulfate and electrical cardioversion [38] Mg2+ dependent TRPM7 has a potential role in cardiovascular toxicity of tyrosine kinase inhibitors during cancer treatment [39].
3.7. Nephrotoxicity and Nephroprotection from Chemotherapy
Nephrotoxicity is the primary dose-limiting toxicity of several anti-neoplastic agents, primarily platinum salts [40,41]. Various hydration regimens and supplementation protocols prevent cisplatin-induced kidney injury in clinical practice. However, evidence-based recommendations on specific hydration regimens are limited. A systematic review evaluated clinical studies that have explored cisplatin-induced nephrotoxicity preventive strategies [40]. Reported four investigated Mg2+ supplementations showed a role as a nephroprotection. Besides hydration and forced diuresis with mannitol, Mg2+ supplementation (8-16 milliequivalents) is beneficial and essential for all patients to prevent cisplatin-induced nephrotoxicity.
A second systematic review, including 22 articles of placebo-controlled trials, extracted the number of patients, doses of cisplatin and protectant, qualitative (acute kidney injury incidence), and quantitative (plasma creatinine, blood urea nitrogen, and creatinine clearance) indicators of renal function [41]. The results showed significant variability in the nephroprotective capacity of various products evaluated. Of all the compounds tested, only Mg2+ sulfate and cystone were found to exert protective effects. A more recent systematic review comprising 11 studies fulfilling the research criteria showed that Mg2+ supplementation protected significantly against cisplatin-induced nephrotoxicity (OR = 0.22, 95% CI 0.14 to 0.35) [42]. However, more studies need to be conducted to confirm these results.
A recent multicenter cohort study of 13719 cancer patients who received prophylactic intravenous Mg2+ showed a lower risk of cisplatin-related acute renal injury as compared to those who did not receive supplementation [Gupta 43]. Tanzawa et al. reported that early serum Mg2+ reduction in patients with advanced lung squamous cell carcinoma treated with chemo-immunotherapy is associated with a poor prognosis in terms of progression-free and overall survival even after multivariate analyses [44 Tanzawa]. Both papers suggest however caution in interpreting data until randomized clinical trials will confirm these findings. A recent systematic review showed only weak evidence that Mg2+ supplementation may prevent the development of worsening of anti-EGFR antibody-related hypomagnesemia and reduce arrhythmia incidence [Kato 45]. On the other hand, Feng et al. recently reported a better outcome in cancer patients with elevated Mg2+ treated with anti-EFGR agents [Feng 46].
3.8. Radiotherapy Protection
Radiotherapy may damage the tumor's surrounding tissues, disrupting normal physiological functions. This negative effect often causes symptoms such as diarrhea, tenesmus, incontinence, and rectal bleeding, which can all significantly alter the patient's quality of life. In some cases, patients are at increased risk of developing protein-calorie malnutrition and micronutrient deficiencies. In a broader nutritional plan including Energy: 28-31 kcal/kg/day, using the Harris-Benedict formula adjusted for body weight in obese patients; protein: 20-30%; fat: 30-40%; and carbohydrates: 40-50%, the maintenance of adequate levels of Vitamin D, Vitamin E, Vitamin A, calcium, Mg2+, thiamin, riboflavin, and niacin is also necessary. Nutrient requirements must be established integrally, considering the patient's age, nutritional status, and the presence of comorbidities [43,47].
3.9. Cachexia
The European Palliative Care Research Collaboration developed clinical guidelines for cancer patients suffering from cachexia [44]. Of the 21 publications included in the systematic literature research, only one study examined the use of Mg2+, which had no effect on weight loss. There is insufficient solid evidence to support using minerals, vitamins, proteins, or other supplements to treat cancer. No serious adverse effects have been reported with dietary supplementation [44,48].
3.10. Chemotherapy-Induced Peripheral Neuropathy
Platinum salts, taxanes, vinca alkaloids, and antimetabolites commonly induce peripheral neuropathy, which may significantly impair patients' physical abilities and quality of life, often leading to dose reduction and/or discontinuation of chemotherapy treatments. Unfortunately, a systematic review of the potential use of nutraceuticals, including Mg2+, did not show significant evidence of clinical benefit to recommend supplements for the treatment or prophylaxis of peripheral neuropathy [45,46,49,50]. The management of chemotherapy-induced peripheral neuropathy remains a critical challenge, and future studies are warranted before recommendations for the use of supplements are made [47,51].
Loprinzi et al. reported a large trial that failed to show differences in the incidence of grade ≥2 neuropathy (National Cancer Institute Common Terminology Criteria for Adverse Events, NCI-CTC) between patients treated with Mg2+ infusions and control ones (RR 0.81, 95% CI 0.60-1.11) [48,52]. A systematic review by Jordan et al., including five trials with 694 evaluable patients, failed to show a beneficial effect of Ca and Mg2+ infusions to prevent oxaliplatin-induced peripheral neuropathy [49,53]. Efficacy endpoints were chronic neurotoxicity measured with NCI-CTC and the oxaliplatin-specific scale.
A review by Tofthagen et al. analyzed four studies exploring the relationship between Mg2+ levels and chemotherapy-induced peripheral peuropathy in patients with CRC treated with oxaliplatin [54]. Overall, there was a prevalence of hypomagnesemia of 13.8-26% with significant differences (p = 0.05) between patients people who developed neuropathy and those woho did not. Pre-treatment hypomagnesemia was present in 80% of cases who developed grade 2–3 neuropathy, compared to only 20% of those who only developed grade 0–1 neuropathy (p = 0.0001). An higher dietary Mg2+intake was associated with a lower prevalence and less severe CIPN symptoms among CRC patients who received adjuvant chemotherapy with oxaliplatin [55]. However, further studies are needed to confirm our findings and to provide a solid basis for future recommendations directed towards the intake of magnesium before and during chemotherapy.
3.11. Cancer Pain
Mg2+ is frequently used daily to reduce pain intensity and analgesic consumption. Results are, however, only partially accepted. A review investigated randomized clinical trials on the effectiveness of Mg2+ treatment on pain and analgesics consumption in postoperative pain, renal pain, chronic pain, and neuropathic pain. The evidence for the efficacy of Mg2+ in reducing pain and analgesic consumption is modest globally. The literature has identified some gaps, especially in methodology, rheumatic diseases of disease, and cancer [50,56].
Surgically treated women with breast cancer commonly suffer from neuropathic pain syndrome, which is a common yet debilitating neuropathic complication that often causes a decrease in patients' quality of life. Recently, emerging evidence has supported the therapeutic effect of Mg2+ administration in chronic pain. Ny et al. performed a randomized, double-masked, placebo-controlled clinical trial on 109 patients who received oral magnesium-L-threonate (n = 48) or placebo (n = 61) for 12 weeks [51,57]. Chronic pain incidence was evaluated at 3- and 6-month follow-ups. Nearly 31% of patients reported chronic pain after Mg2+ supplementation and 26% of the control group at 6-month follow-up, respectively. Total scores of the short form of the Mc Gill Pian Questionnaire were significantly increased in the control group 6 months after surgical intervention (mean difference, 1.475; 95% CI, -2.730 to -0.2211) but not in the Mg2+ treated group (mean difference, 1.250; 95% CI, -2.775 to 0.2748). No significant differences were found between the two cohorts regarding questionnaire scores each time. Oral supplementation of magnesium-L-threonate did not effectively prevent the development of persistent pain in breast cancer survivors nor provide sufficient pain relief over placebo. However, data showed improved pain, mood, sleep disorder, or cognitive function after the 12-week Mg2+ supplementation. Patients treated with intravenous Mg2+ needed significantly fewer narcotics for pain control on postoperative days, even if recovery parameters, including maximal pain scores, postoperative mobilization, and length of hospital stay, did not significantly differ between the two groups [52,58]. Preemptive use of Mg2+SO4 reduces postoperative pain scores without affecting hemodynamic parameters during induction and maintenance of general anesthesia [53,59].
3.12. Opioid-Induced Constipation
Constipation is a frequent gastrointestinal side-effect of opioid treatment with a prevalence of up to 59%, usually managed with osmotic agents, stimulant laxatives, peripherally acting µ-opioid receptor antagonists, or naloxone [54,60]. International guidelines recommend standard laxatives such as macrogol/electrolytes and Mg2+ hydroxide to prevent opioid-induced constipation, although evidence from randomized controlled trials is weak. A systematic review and meta-analysis of twenty-two trials analyzed the scientific evidence on pharmacological strategies for the prevention and treatment of opioid-induced constipation in cancer patients. Overall, data failed to show apparent differences in the efficacy of the laxatives [55,61]. Only one cohort study showed a significant benefit of Mg2+ oxide compared with no laxatives. One randomized trial found a significant benefit for naldemedine compared with Mg2+ oxide. A large Japanese retrospective study on naldemedine or Mg2+ oxide as the first-line laxative prescription employed a nationwide hospital claims database for a long-term opioid prescription for cancer pain with ≥6 months post-opioid observation period [56,62]. After propensity score matching, the incidence of death was not adjusted enough and was significantly higher in the naldemedine arm (1717 patients) than in the Mg2+ oxide arm (544) in the non-early group but comparable in the early group. The incidence of addition, change, or dose increase was significantly higher in the naldemedine arm than in the Mg2+ oxide arm of the early prescription group (HR 1.08; 95% CI 1.00-1.17; p=0.0402). Overall, Mg2+ and naldemedine are most likely the most effective agents for the prevention of opioid-induced constipation in cancer patients. An open-label, randomized, multicenter study on 330 patients with opioids for pain management to examine if Mg2+ hydroxide is non-inferior to macrogol/electrolytes in the prevention of opioid-induced constipation is ongoing [57,63]. Magnesium oxide and naldemedine are most likely effective for the prevention of opioid-induced constipation in cancer patients, even if more studies are needed before establishing sound recommendations for clinical practice.
3.12. Other Drug Interactions
Mg2+ salts retain water in the intestine and act as an osmotic laxative. They may affect the bioavailability of concomitantly administered drugs by forming insoluble chelate complexes with those drugs, substantially reducing their bioavailability [58,64]. Besides calcium, bisphosphonates and high-dose antiviral agents may affect Mg2+ levels [59,60,65,66]. Mg2+ may reduce the absorption of the antifungal itraconazole and several antibiotics, including fluoroquinolones, tetracyclines, and nitrofurantoin [61,62,63,67,68,69].
4. Magnesium and Cancer Risk
Consumption of Mg2+ from dietary sources may be beneficial in reducing all-cause and cancer mortality and thus have practical importance for public health. Some epidemiological studies have suggested a non-causative correlation between higher dietary Mg2+ intake and a lower risk of some malignancies, such as CRC cancer [64,70]. These studies often rely on dietary surveys and need more accuracy. Despite these limitations, the data hints at Mg2+ potentially beneficial role in cancer prevention.
Bagheri et al. carried out a meta-analysis of nineteen prospective studies, including 11,408 cancer-related deaths, to examine the association of total, supplemental, and dietary Mg2+ intakes with risk of all-cause, cancer, and cardiovascular disease mortality and identify the dose-response relations involved in these associations [65,71]. Dietary Mg2+ intake was associated with a lower risk of all-cause [P < 0.001] and cancer mortality (p=0.027). However, the analysis did not show any statistically significant associations between supplemental and total Mg2+ intakes with cancer and risks of all-cause. However, linear dose-response meta-analysis indicated that each additional intake of 100 mg/d of dietary Mg2+ was associated with a 6% and 5% reduced risk of all-cause and cancer mortality, respectively [65,71].
In 2022, the US Preventive Services Task Force reported a large, pooled analysis to establish the role of vitamins and mineral supplements for primary cancer prevention, including eighty-four studies and 739,803 patients [66,72]. While multivitamin use was significantly associated with a lower incidence of any cancer in 4 clinical randomized trials comprising 48859 cases (OR 0.93; 95% CI 0.87-0.99), the evidence for the benefit of other supplements was equivocal, minimal, or absent or even dangerous. Beta carotene was significantly associated with an increased risk of lung cancer (OR 1.20, 95% CI 1.01-1.42] and cardiovascular mortality (OR 1.10; 95% CI 1.02-1.19) [67,73].
4.1. Colorectal Cancer
Epidemiologic studies have suggested that Mg2+ intake may be correlated to a decreased risk of CRC, but the findings have been inconsistent [68,74]. A study of 412,000 subjects from 12 prospective studies followed up for 8-14 years showed an inverse relationship between Mg2+ intake and risk of CRC in men but not women [69,75]. In the U.S., states with Mg2+ levels in drinking water and living at the highest quartile have a significantly lower risk of all cancers in both genders.
Song et al. conducted a metanalysis to explore the relationships between the risk of CRC and intakes of individual dietary elements, including Mg2+ [70,76]. Metanalysis of cohort studies showed that high intakes of dietary Mg2+ were negatively associated with the risk of CRC as the HR were 0.76 (95% CI 0.72, 0.80) and 0.80 (95% CI 0.73, 0.87), respectively. A meta-analysis of case-control studies indicated that high intakes of dietary Ca, Mg2+, and K were negatively related to the occurrence of CRC. The OR were 0.36 (95% CI 0.32, 0.40), 0.80 (95% CI 0.63, 0.98) and 0.97 (95% CI 0.74, 1.21), respectively.
Chen et al. reported a meta-analysis of eight prospective studies comprising 338,979 participants and 8000 CRC cases, showing that a higher Ma2+ intake may be associated with a modest decrease in CRC risk, particularly colon cancer [69,75]. The summary relative risk (RR) for the highest vs lowest category of Mg2+ intake for CRC was 0.89 (95% CI, 0.79-1.00), with little evidence of heterogeneity. For colon and rectal cancer, the pooled RR was 0.81 (95% CI, 0.70-0.93) and 0.94 (95% CI, 0.72-1.24), respectively. In the dose-response analyses, the summary RRs for an increment of Mg2+ intake of 50 mg/day for colorectal, colon, and rectal cancer were, respectively, 0.95 (95% CI, 0.89-1.00), 0.93 (95% CI, 0.88-0.99) and 0.93 (95% CI, 0.83-1.04), and there was some evidence of heterogeneity; omitting one study that substantially contributed to the heterogeneity yielded generally similar results, but with low heterogeneity.
Another review evaluated the evidence across 80 meta-analyses of interventional and observational studies of CRC prevention using medications, vitamins, supplements, and dietary factors [71,77]. Mg2+, aspirin, non-steroidal anti-inflammatory drugs, folate, and high consumption of fruits and vegetables, fiber, and dairy products were associated with a decreased incidence of CRC [71,77]. The relationship between all prescriptions of nearly 400 drugs other than anti-neoplastic ones and the mortality of CRC patients was analyzed in 2,618 cases registered in the Korean National Health Insurance Service-National Sample Cohort database, controlling for multiple comparisons with the false discovery rate [72,78]. Results suggested that Mg2+ may have a detrimental effect on CRC prognosis.
4.2. Esophageal Cancer
4.3. Lung Cancer
Whether serum Mg2+ levels are lower in lung cancer patients than healthy controls is still controversial. A meta-analysis by Song et al. suggests that the relationship between serum Mg2+ levels and lung cancer is insignificant. Eleven papers comprising 707 cases of lung cancer and 7595 healthy controls were included in the study [74,80]. Serum Mg2+ levels were not significantly lower in patients with lung cancer compared to health controls, with significant heterogeneity (I2 = 99.6%, p<0.001). Zhai et al. reviewed the possible role of magnesium in reducing lung cancer risk since this cation shows protective effects against lung function loss [75,81].
4.4. Thyroid Cancer
A systematic review of 11 epidemiological studies on the association between dietary supplements minerals, including Mg2+, and thyroid cancer risk resulted largely inconsistent across studies [76,82]. Data supporting the correlation between serum levels of selenium, copper, and Mg2+ with thyroid cancer are conflicting. However, a meta-analysis involving 1291 subjects and pooled analysis indicated that subjects with thyroid cancer had lower serum levels of selenium and Mg2+ but higher levels of copper than the healthy controls, supporting a significant association between serum levels of such cations and thyroid cancer [77,83]. However, the subgroup analysis found a significant effect modification of selenium and copper by ethnicities. Therefore, this finding needs further confirmation by a trans-regional multicenter study to better understand the causal relationship between selenium, copper, and Mg2+ with thyroid cancer of different human races or regions [77,83].
4.5. Breast Cancer (BC)
Viable breast cancer cells increase the expression of Mg2+ transport channels, which raises the intracellular concentration of the mineral [78,79,84,85]. This contributes to tumor growth by increasing energy demand [78,79]. These data, however, need confirmation. Kim et al. analyzed micronutrient levels' causally estimated effects on cancer by applying the Mendelian randomization method, using single-nucleotide polymorphisms associated with micronutrient levels as instrumental variables [80,86]. Results favored an increased risk of breast cancer correlated with Mg2+ levels (OR = 1.281; p<0.0001).
A review on the alterations in Mg2+ homeostasis in BC suggest a possibile interfernce with BC progression, even if the existing data are scarce and inconsistent [87]. A case-control study of 1050 patients and 1229 controls showed that a higher Mg2+ intake was associated with a lower BC risk possibly via its effect on inflammatory markers C-reactive protein (CRP) and interleukin-6 (IL-6). A positive association was found between the CRP level and BC risk (adjusted OR = 1.43) while IL-6 showed no association [88]. However, in a cohort of 1,170 women with BC, higher dietary intake of Mg2+ was inversely associated with risk of all-cause mortality primarily among postmenopausal women who had a high Ca:Mg intake ratio. There were no clear associations for prognosis with intake of calcium [89]. Results suggest that Mg2+ intake alone may improve BC overall survival. In women with BC reduced serum Mg2+ concentrations may impair the antioxidant defense systems involved in the carcinogenesis process as evaluated by superoxide dismutase activity and its relationship with oxidative stress markers. Bazerra et a. showed that the mean value of the amount of dietary Mg2+ and erytrocyed levels was below the recommended level in women with BC were reduced in relation to the control group (p < 0.0001) and inadequate according to the reference values [90]. Urinary excretion was high, with a significant difference between groups (p < 0.0001).
4.6. Cervical Cancer
The National Health and Nutrition Examination Survey study explored dietary intake correlations among 215 women affected by cervical cancer and 860 without cancer [81,91]. The research implemented the univariate analysis and the least absolute shrinkage and selection operator regression to estimate the association of 29 variables with cervical cancer, subsequently identifying the most pertinent variables linked to cervical cancer. Among the six covariates examined (age, race, fiber, Mg2+, caffeine, vitamin C), Mg2+ was linked to cervical cancer in univariate analyses (p<0.05).
4.7. Endometrial Cancer
Obesity and endometrial cancer risk are strongly associated. Therefore, dietary habits may play an essential role in developing this cancer. Wang et al. conducted a study using two-sample mendelian randomization to explore the effects of circulating levels of 15 micronutrients, including Mg2+, as well as corrected relative macronutrient intake (protein, carbohydrate, sugar, and fat) on risks of endometrial cancer and its subtypes (endometrioid and non-endometrioid histology) [82,92].
4.8. Hepatocellular Carcinoma (HCC)
Mg2+ deficiency is commonly associated with liver diseases, and Mg2+ supplementation can improve liver function. Mg2+ deficiency may result from low dietary uptake, increased urinary secretion, hypoalbuminemia, or hormone inactivation. Low Mg2+ content in serum and liver tissue may foster disease progression due to disruption in mitochondrial function, defective protein kinase C translocation, inflammatory responses, oxidative stress, or metabolic disorders [83,93]. In preclinical models high expression of protein phosphatase Mg2+-dependent 1H (PPM1H) mRNA and protein correlated with better prognosis. PPM1H inhibited proliferation, migration, and invasion of hepatoma cell, and inhibited induced HCC nodule formation [94].
Epidemiological data on Mg2+ level and its relation to HCC are occasional. Nonalcoholic fatty liver disease is a major contributive factor to the increasing incidence of HCC. Yu et al. explored the associations between serum Mg2+ levels and the risk of HCC among 26,053 patients with nonalcoholic fatty liver disease [84,95]. Overall, 395 patients developed HCC after the first measurement of serum Mg2+. Patients with nonalcoholic fatty liver disease who developed HCC had significantly lower mean levels of serum Mg2+ (0.769 ± 0.131 mmol/L) than cancer-free ones (0.789 ± 0.125 mmol/L; p = 0.003). This finding suggests higher levels of serum Mg2+ were significantly associated with decreased risk of HCC among patients with nonalcoholic fatty liver disease. A retrospective study showed that serum levels of Mg2+ were significantly lower in cirrhotic patients with HCC than in cancer-free ones on multivariate logistic regression [96].
5. Therapeutic Perspectives
Understanding tumor biology and progressing studies on ion transporters give new insight into the theoretical possibility of Mg2+ being used in cancer treatment by adding to or depleting these ion levels in specifically targeted tissues [85,86,97,98]. Given its role in ion competition, these findings lead to questions about the possibility of Mg2+ being a tumor suppressor and protector of host tissue. Mg2+ nanocluster may enhance Palbociclib activity [85,96]. Mg2+-based compounds may represent a new therapeutic option in the future. A series of novel mixed transition metal-Mg2+ tartrate complexes were screened in vitro for their anti-cancer activity against the human breast cancer cell lines, showing antiproliferative activity and cell migration inhibition [86,98]. A double-blind, placebo-controlled clinical study failed to show the activity of Mg2+ in reducing hot flashes in patients with breast cancer [99].
6. Conclusions
The role of Mg2+ in cancer is a complex and intriguing area of study, with experimental and epidemiological evidence presenting a conflicting picture [87,100]. On the one hand, its involvement in cellular metabolism and maintaining genetic stability, regulation of cell proliferation, and protection against insulin resistance, oxidative stress, and systemic inflammation are considered cancer-preventive attributes [88,89,101,102]. On the other hand, hypomagnesemia, as a side effect of some cancer treatments, may produce an inhibitory effect on tumor growth and neo-angiogenesis. However, Mg2+ levels also increase in both in vivo and in vitro tumors, suggesting its multiple and possibly dichotomous roles in cancer [18,90,103]. Preclinical and clinical research has shown low Mg2+ having both pro- and anti-tumor effects, including facilitating tumor implantation at metastatic sites and inhibiting tumor growth at its originating site. The controlled and coordinated variations of intracellular Mg2+ are drastically disrupted in several cell types by neoplastic transformation, which provides selective advantages to the cells. Moreover, this scenario is further complicated by inflammatory responses to hypomagnesemia even if Mg2+ immunomodulatory function regulates NF-kB activation and cytokine production and limits systemic inflammation such as C-reactive protein and endothelial dysfunction [91,92,104,105].
The Nordic Nutrition Recommendations suggested a recommended intake based on balance studies [93,106]. However, the average requirement still needs to be set. Functional indicators of magnesium status still need to be improved. A scoping review reveals new research on Mg2+ intake's beneficial effect on several health outcomes (cardiovascular disease, diabetes, and some cancers). A causal association is suggested based on meta-analyses of cohort and randomized controlled trials. However, the optimal intake cannot be set based on these study designs, and new balance studies have yet to be found [93,106].
Applying the knowledge gained on Mg2+ from experimental models to real-world situations is challenging [94]. Epidemiological research indicates that a Mg2+ deficit is associated with a higher risk of some malignancies. The issue is further complicated by evidence of Mg2+ homeostasis disturbance in cancer patients. More translational and clinical research is required to determine Mg2+'s role in tumor development [94,107]. Despite evidence suggesting the potential protective effect of Mg2+ against cancer and its importance in managing treatment-related side effects, the current consensus is that there is insufficient data to recommend Mg2+ supplements specifically for cancer prevention or treatment [95,108]. Unless a healthcare professional advises supplementation, the best approach is to maintain adequate Mg2+ levels through a balanced diet rich in Mg+-containing foods, such as nuts, seeds, whole grains, and leafy green vegetables.
Scientists are continuously studying the relationship between Mg2+ and cancer to understand better how nutritional factors influence cancer risk, development, and treatment outcomes. These data may help clinicians decide whether to regulate the intake of certain micronutrients, particularly in high-risk groups without nutritional deficiencies. They may help in the design of future clinical trials. Future research may provide more precise insights into whether Mg2+ can play a significant role in cancer prevention and therapy. In conclusion, maintaining adequate Mg2+ levels benefit overall health and may also affect cancer risk and treatment. However, further research is needed to understand its role and efficacy in these contexts fully.
Author Contributions
Conceptualization, D.S, V.G.; methodology, D.S., L.S.; validation, G.S.; formal analysis, L.D.; investigation, G.S., D.S.; data curation, G.S., D.S.; writing—original draft preparation, V.G., D.S.; writing—review and editing, V.G. D.S.; supervision, L.D., M.R.V. All authors have read and agreed to the published version of the manuscript.”.
Funding
This research received no external funding.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| Mg2+ | Magnesium2+ |
| CRC | Colorectal carcinoma |
| EGFR | Epidermal growth factor receptor |
| HCC | Hepatocellular carcinoma |
References
- Behers, B.J.; Melchor, J.; Behers, B.M.; Meng, Z.; Swanson, P.J.; Paterson, H.I.; Araque, S.J.M.; Davis, J.L.; Gerhold, C.J.; Shah, R.S.; et al. Vitamins and Minerals for Blood Pressure Reduction in the General, Normotensive Population: A Systematic Review and Meta-Analysis of Six Supplements. Nutrients 2023, 15, 4223. [Google Scholar] [CrossRef] [PubMed]
- Dominguez, L.J.; Veronese, N.; Barbagallo, M. Magnesium and the Hallmarks of Aging. Nutrients 2024, 16, 496. [Google Scholar] [CrossRef] [PubMed]
- Ashique, S.; Kumar, S.; Hussain, A.; Mishra, N.; Garg, A.; Gowda, B.H.J.; Farid, A.; Gupta, G.; Dua, K.; Taghizadeh-Hesary, F. A narrative review on the role of magnesium in immune regulation, inflammation, infectious diseases, and cancer. J. Heal. Popul. Nutr. 2023, 42, 74. [Google Scholar] [CrossRef]
- Barbagallo, M.; Veronese, N.; Dominguez, L.J. Magnesium in Aging, Health and Diseases. Nutrients 2021, 13, 463. [Google Scholar] [CrossRef]
- Schwalfenberg, G.K.; Genuis, S.J. The Importance of Magnesium in Clinical Healthcare. Scientifica 2017, 2017, 1–14. [Google Scholar] [CrossRef]
- Trapani, V.; Wolf, F.I. Dysregulation of Mg2+ homeostasis contributes to acquisition of cancer hallmarks. Cell Calcium 2019, 83, 102078. [Google Scholar] [CrossRef] [PubMed]
- Trapani, V.; Arduini, D.; Cittadini, A.; Wolf, F.I. From magnesium to magnesium transporters in cancer: TRPM7, a novel signature in tumour development. Magnes. Res. 2013, 26, 149–155. [Google Scholar] [CrossRef]
- Weglicki, W.B. Hypomagnesemia and Inflammation: Clinical and Basic Aspects. Annu. Rev. Nutr. 2012, 32, 55–71. [Google Scholar] [CrossRef]
- Razzaque, M.S. Magnesium: Are We Consuming Enough? Nutrients 2018, 10, 1863. [Google Scholar] [CrossRef]
- Durlach, J.; Bara, M.; Guiet-Bara, A.; Collery, P. Relationship between magnesium, cancer, and carcinogenic or anti-cancer metals. Anti-cancer Res. 1986, 6, 1353–1361. [Google Scholar] [PubMed]
- Castiglioni, S.; Maier, J.A. Magnesium and cancer: a dangerous liason. Magnes. Res. 2011, 24, 92–100. [Google Scholar] [CrossRef]
- Błaszczyk, U.; Duda-Chodak, A. Magnesium: its role in nutrition and carcinogenesis. Rocz Panstw Zakl Hig. 2013, 64, 165–71. [Google Scholar] [PubMed]
- Nasulewicz, A.; Wietrzyk, J.; Wolf, F.I.; Dzimira, S.; Madej, J.; Maier, J.A.M.; Rayssiguier, Y.; Mazur, A.; Opolski, A. Magnesium deficiency inhibits primary tumor growth but favors metastasis in mice. Biochim. Biophys. Acta (BBA) - Mol. Basis Dis. 2004, 1739, 26–32. [Google Scholar] [CrossRef]
- Karska, J.; Kowalski, S.; Saczko, J.; Moisescu, M.G.; Kulbacka, J. Mechanosensitive Ion Channels and Their Role in Cancer Cells. Membranes 2023, 13, 167. [Google Scholar] [CrossRef]
- Cappadone, C.; Merolle, L.; Marraccini, C.; Farruggia, G.; Sargenti, A.; Locatelli, A.; Morigi, R.; Iotti, S. Intracellular magnesium content decreases during mitochondria-mediated apoptosis induced by a new indole-derivative in human colon cancer cells. Magnes. Res. 2012, 25, 104–111. [Google Scholar] [CrossRef] [PubMed]
- Wolf, F.I.; Maier, J.A.M.; Nasulewicz, A.; Feillet-Coudray, C.; Simonacci, M.; Mazur, A.; Cittadini, A. Magnesium and neoplasia: From carcinogenesis to tumor growth and progression or treatment. Arch. Biochem. Biophys. 2006, 458, 24–32. [Google Scholar] [CrossRef]
- Anghileri, L.J. Magnesium, calcium and cancer. Magnes. Res. 2009, 22, 247–255. [Google Scholar] [CrossRef] [PubMed]
- Wolf, F.I.; Trapani, V. Magnesium and its transporters in cancer: a novel paradigm in tumour development. Clin. Sci. 2012, 123, 417–427. [Google Scholar] [CrossRef]
- Abdollahi, P.; Vandsemb, E.N.; Børset, M. Phosphatases of regenerating liver are key regulators of metabolism in cancer cells – role of Serine/Glycine metabolism. Curr. Opin. Clin. Nutr. Metab. Care 2021, 25, 50–55. [Google Scholar] [CrossRef]
- Wolf, F.I.; Maier, J.A.M.; Nasulewicz, A.; Feillet-Coudray, C.; Simonacci, M.; Mazur, A.; Cittadini, A. Magnesium and neoplasia: From carcinogenesis to tumor growth and progression or treatment. Arch. Biochem. Biophys. 2006, 458, 24–32. [Google Scholar] [CrossRef]
- Bonilla, M.; Workeneh, B.T.; Uppal, N.N. Hypomagnesemia in Patients With Cancer: The Forgotten Ion. Semin. Nephrol. 2022, 42, 151347. [Google Scholar] [CrossRef] [PubMed]
- Rosner, M.H.; Renaghan, A.D. Disorders of Divalent Ions (Magnesium, Calcium, and Phosphorous) in Patients With Cancer. Adv. Chronic Kidney Dis. 2022, 28, 447–459.e1. [Google Scholar] [CrossRef] [PubMed]
- Liamis, G.; Hoorn, E.J.; Florentin, M.; Milionis, H. An overview of diagnosis and management of drug-induced hypomagnesemia. Pharmacol. Res. Perspect. 2021, 9, e00829. [Google Scholar] [CrossRef] [PubMed]
- Whang, R. Magnesium deficiency: Pathogenesis, prevalence, and clinical implications. Am. J. Med. 1987, 82, 24–29. [Google Scholar] [CrossRef]
- Workeneh, B.T.; Uppal, N.N.; Jhaveri, K.D.; Rondon-Berrios, H. Hypomagnesemia in the Cancer Patient. Kidney360 2021, 2, 154–166. [Google Scholar] [CrossRef]
- Hsieh, M.-C.; Wu, C.-F.; Chen, C.-W.; Shi, C.-S.; Huang, W.-S.; Kuan, F.-C. Hypomagnesemia and clinical benefits of anti-EGFR monoclonal antibodies in wild-type KRAS metastatic colorectal cancer: a systematic review and meta-analysis. Sci. Rep. 2018, 8, 2047. [Google Scholar] [CrossRef]
- Oronsky, B.; Caroen, S.; Oronsky, A.; Dobalian, V.E.; Oronsky, N.; Lybeck, M.; Reid, T.R.; Carter, C.A. Electrolyte disorders with platinum-based chemotherapy: mechanisms, manifestations and management. Cancer Chemother. Pharmacol. 2017, 80, 895–907. [Google Scholar] [CrossRef]
- Sikking, C.; Niggebrugge-Mentink, K.L.; van der Sman, A.S.E.; Smit, R.H.P.; Bouman-Wammes, E.W.; Beex-Oosterhuis, M.M.; van Kesteren, C. Hydration Methods for Cisplatin Containing Chemotherapy: A Systematic Review. Oncol. 2023, 29, e173–e186. [Google Scholar] [CrossRef]
- Li, J.; Wu, Y.; Chen, C.; Zhang, W.; Yue, L.; Liu, T. A systematic review for prevention of cisplatin-induced nephrotoxicity using different hydration protocols and meta-analysis for magnesium hydrate supplementation. Clin. Exp. Nephrol. 2023, 28, 1–12. [Google Scholar] [CrossRef]
- Fujii, H.; Iihara, H.; Suzuki, A.; Kobayashi, R.; Matsuhashi, N.; Takahashi, T.; Yoshida, K.; Itoh, Y. Hypomagnesemia is a reliable predictor for efficacy of anti-EGFR monoclonal antibody used in combination with first-line chemotherapy for metastatic colorectal cancer. Cancer Chemother. Pharmacol. 2016, 77, 1209–1215. [Google Scholar] [CrossRef]
- Alem, A.; Edae, C.K.; Wabalo, E.K.; Tareke, A.A.; Bedanie, A.A.; Reta, W.; Bariso, M.; Bekele, G.; Zawdie, B. Factors influencing the occurrence of electrolyte disorders in cancer patients. SAGE Open Med. 2021, 9. [Google Scholar] [CrossRef] [PubMed]
- Schrag, D.; Chung, K.Y.; Flombaum, C.; Saltz, L. Cetuximab Therapy and Symptomatic Hypomagnesemia. JNCI J. Natl. Cancer Inst. 2005, 97, 1221–1224. [Google Scholar] [CrossRef] [PubMed]
- Miltiadous, G.; Christidis, D.; Kalogirou, M.; Elisaf, M. Causes and mechanisms of acid–base and electrolyte abnormalities in cancer patients. Eur. J. Intern. Med. 2008, 19, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Petrelli, F.; Borgonovo, K.; Cabiddu, M.; Ghilardi, M.; Barni, S. ; Md Risk of anti-EGFR monoclonal antibody-related hypomagnesemia: systematic review and pooled analysis of randomized studies. Expert Opin. Drug Saf. 2011, 11, S9–S19. [Google Scholar] [CrossRef]
- Katsura, H.; Suga, Y.; Kubo, A.; Sugimura, H.; Kumatani, K.; Haruki, K.; Yonezawa, M.; Narita, A.; Ishijima, R.; Ikesue, H.; et al. Risk Evaluation of Proton Pump Inhibitors for Panitumumab-Related Hypomagnesemia in Patients with Metastatic Colorectal Cancer. Biol. Pharm. Bull. 2024, 47, 98–103. [Google Scholar] [CrossRef]
- Liu, W.; Meyer, L.; Morse, M.; Li, Y.; Song, J.; Engle, R.; Lopez, G.; Narayanan, S.; Soliman, P.T.; Ramondetta, L.; et al. Dietary Magnesium Replacement for Prevention of Hypomagnesemia in Patients With Ovarian Cancer Receiving Carboplatin-Based Chemotherapy. JCO Oncol. Pr. 2024, 20, 517–524. [Google Scholar] [CrossRef]
- Vejpongsa, P.; Yeh, E.T. Prevention of Anthracycline-Induced Cardiotoxicity. Circ. 2014, 64, 938–945. [Google Scholar] [CrossRef]
- Coppola, C.; Rienzo, A.; Piscopo, G.; Barbieri, A.; Arra, C.; Maurea, N. Management of QT prolongation induced by anti-cancer drugs: Target therapy and old agents. Different algorithms for different drugs. Cancer Treat. Rev. 2018, 63, 135–143. [Google Scholar] [CrossRef]
- Liu, Q.; Li, S.; Qiu, Y.; Zhang, J.; Rios, F.J.; Zou, Z.; Touyz, R.M. Cardiovascular toxicity of tyrosine kinase inhibitors during cancer treatment: Potential involvement of TRPM7. Front. Cardiovasc. Med. 2023, 10, 1002438. [Google Scholar] [CrossRef]
- Crona, D.J.; Faso, A.; Nishijima, T.F.; McGraw, K.A.; Galsky, M.D.; Milowsky, M.I. A Systematic Review of Strategies to Prevent Cisplatin-Induced Nephrotoxicity. Oncol. 2017, 22, 609–619. [Google Scholar] [CrossRef]
- Casanova, A.G.; Hernández-Sánchez, M.T.; López-Hernández, F.J.; Martínez-Salgado, C.; Prieto, M.; Vicente-Vicente, L.; Morales, A.I. Systematic review and meta-analysis of the efficacy of clinically tested protectants of cisplatin nephrotoxicity. Eur. J. Clin. Pharmacol. 2019, 76, 23–33. [Google Scholar] [CrossRef]
- Li, J.; Wu, Y.; Chen, C.; Zhang, W.; Yue, L.; Liu, T. A systematic review for prevention of cisplatin-induced nephrotoxicity using different hydration protocols and meta-analysis for magnesium hydrate supplementation. Clin. Exp. Nephrol. 2023, 28, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Gupta, S.; Glezerman, I.G.; Hirsch, J.S.; Chewcharat, A.; Wells, S.L.; Ortega, J.L.; Pirovano, M.; Kim, R.; Chen, K.L.; Jhaveri, K.D.; et al. Intravenous Magnesium and Cisplatin-Associated Acute Kidney Injury. JAMA Oncol. 2025. [Google Scholar] [CrossRef] [PubMed]
- Tanzawa, S.; Yoshioka, H.; Misumi, T.; Miyauchi, E.; Ninomiya, K.; Murata, Y.; Takeshita, M.; Kinoshita, F.; Fujishita, T.; Sugawara, S.; et al. Clinical impact of hypomagnesemia induced by necitumumab plus cisplatin and gemcitabine treatment in patients with advanced lung squamous cell carcinoma: a subanalysis of the NINJA study. Ther. Adv. Med Oncol. 2025, 17. [Google Scholar] [CrossRef]
- Kato, T.; Kawaguchi, T.; Funakoshi, T.; Fujiwara, Y.; Yasuda, Y.; Ando, Y. Efficacy of Magnesium Supplementation in Cancer Patients Developing Hypomagnesemia Due to Anti-EGFR Antibody: A Systematic Review. Cancer Diagn. Progn. 2024, 4, 390–395. [Google Scholar] [CrossRef] [PubMed]
- Feng, Y.; Gao, M.; Xu, X.; Liu, H.; Lu, K.; Song, Z.; Yu, J.; Liu, X.; Han, X.; Li, L.; et al. Elevated serum magnesium levels prompt favourable outcomes in cancer patients treated with immune checkpoint blockers. Eur. J. Cancer 2024, 213, 115069. [Google Scholar] [CrossRef]
- Castro-Eguiluz, D.; Leyva-Islas, J.A.; Luvián-Morales, J.; Martínez-Roque, V.; Sánchez-López, M.; Trejo-Durán, G.E.; Jiménez-Lima, R.; Leyva-Rendón, F.J. Nutrient Recommendations for Cancer Patients Treated with Pelvic Radiotherapy, with or without Comorbidities. Rev. de Investig. Clin. organo del Hosp. de Enfermedades de la Nutr. 2018, 70, 130–135. [Google Scholar] [CrossRef]
- Mochamat; Cuhls, H.; Marinova, M.; Kaasa, S.; Stieber, C.; Conrad, R.; Radbruch, L.; Mücke, M. A systematic review on the role of vitamins, minerals, proteins, and other supplements for the treatment of cachexia in cancer: a European Palliative Care Research Centre cachexia project. J. Cachex- Sarcopenia Muscle 2016, 8, 25–39. [Google Scholar] [CrossRef]
- Schloss, J.M.; Colosimo, M.; Airey, C.; Masci, P.P.; Linnane, A.W.; Vitetta, L. Nutraceuticals and chemotherapy induced peripheral neuropathy (CIPN): A systematic review. Clin. Nutr. 2013, 32, 888–893. [Google Scholar] [CrossRef]
- Schloss, J.; Colosimo, M.; Vitetta, L. Herbal medicines and chemotherapy induced peripheral neuropathy (CIPN): A critical literature review. Crit. Rev. Food Sci. Nutr. 2015, 57, 1107–1118. [Google Scholar] [CrossRef]
- Liu, Y.-W.; Liu, C.-T.; Su, Y.-L.; Tsai, M.-Y. A Narrative Review of Complementary Nutritional Supplements for Chemotherapy-induced Peripheral Neuropathy. Altern Ther Health Med. 2020, 26, 43–49. [Google Scholar] [PubMed]
- Loprinzi, C.L.; Qin, R.; Dakhil, S.R.; Fehrenbacher, L.; Flynn, K.A.; Atherton, P.; Seisler, D.; Qamar, R.; Lewis, G.C.; Grothey, A. Phase III Randomized, Placebo-Controlled, Double-Blind Study of Intravenous Calcium and Magnesium to Prevent Oxaliplatin-Induced Sensory Neurotoxicity (N08CB/Alliance). J. Clin. Oncol. 2014, 32, 997–1005. [Google Scholar] [CrossRef]
- Jordan, B.; Jahn, F.; Beckmann, J.; Unverzagt, S.; Müller-Tidow, C.; Jordan, K. Calcium and Magnesium Infusions for the Prevention of Oxaliplatin-Induced Peripheral Neurotoxicity: A Systematic Review. Oncology 2016, 90, 299–306. [Google Scholar] [CrossRef]
- Tofthagen, C.; Tanay, M.; Perlman, A.; Starr, J.; Advani, P.; Sheffield, K.; Brigham, T. A Systematic Review of Nutritional Lab Correlates with Chemotherapy Induced Peripheral Neuropathy. J. Clin. Med. 2022, 11, 355. [Google Scholar] [CrossRef] [PubMed]
- Wesselink, E.; Winkels, R.M.; Van Baar, H.; Geijsen, A.J.M.R.; Van Zutphen, M.; Van Halteren, H.K.; Hansson, B.M.E.; Radema, S.A.; De Wilt, J.H.W.; Kampman, E.; et al. Dietary Intake of Magnesium or Calcium and Chemotherapy-Induced Peripheral Neuropathy in Colorectal Cancer Patients. Nutrients 2018, 10, 398. [Google Scholar] [CrossRef] [PubMed]
- Morel, V.; Pickering, M.-E.; Goubayon, J.; Djobo, M.; Macian, N.; Pickering, G. Magnesium for Pain Treatment in 2021? State of the Art. Nutrients 2021, 13, 1397. [Google Scholar] [CrossRef]
- Ni, Y.; Deng, F.; Yu, S.; Zhang, J.; Zhang, X.; Huang, D.; Zhou, H. A Randomized, Double-Blind, Placebo-Controlled Trial to Evaluate the Therapeutic Effect of Magnesium-L-Threonate Supplementation for Persistent Pain After Breast Cancer Surgery. Breast Cancer: Targets Ther. 2023, 15, 495–504. [Google Scholar] [CrossRef]
- Lu, Y.-H.; Jeon, J.; Mahajan, L.; Yan, Y.; Weichman, K.E.; Ricci, J.A. Postoperative Magnesium Sulfate Repletion Decreases Narcotic Use in Abdominal-Based Free Flap Breast Reconstruction. J. Reconstr. Microsurg. 2024, 40, 559–565. [Google Scholar] [CrossRef]
- Akbudak, I.H.; Yilmaz, S.; Ilhan, S.; Tanriverdi, S.Y.; Erdem, E. The effect of preemptive magnesium sulfate on postoperative pain in patients undergoing mastectomy: a clinical trial. Clin Nutr. 2023, 27, 7907–7913. [Google Scholar] [CrossRef]
- Crockett, S.D.; Greer, K.B.; Heidelbaugh, J.J.; Falck-Ytter, Y.; Hanson, B.J.; Sultan, S. American Gastroenterological Association Institute Guideline on the Medical Management of Opioid-Induced Constipation. Gastroenterology 2019, 156, 218–226. [Google Scholar] [CrossRef]
- Kistemaker, K.; Sijani, F.; Brinkman, D.; de Graeff, A.; Burchell, G.; Steegers, M.; van Zuylen, L. Pharmacological prevention and treatment of opioid-induced constipation in cancer patients: A systematic review and meta-analysis. Cancer Treat. Rev. 2024, 125, 102704. [Google Scholar] [CrossRef]
- Kessoku, T.; Higashibata, T.; Morioka, Y.; Naya, N.; Koretaka, Y.; Ichikawa, Y.; Hisanaga, T.; Nakajima, A. Naldemedine and Magnesium Oxide as First-Line Medications for Opioid-Induced Constipation: A Comparative Database Study in Japanese Patients With Cancer Pain. Cureus 2024, 16, e55925. [Google Scholar] [CrossRef] [PubMed]
- Kistemaker, K.; de Graeff, A.; Crul, M.; de Klerk, G.; van de Ven, P.; van der Meulen, M.; van Zuylen, L.; Steegers, M. Magnesium hydroxide versus macrogol/electrolytes in the prevention of opioid-induced constipation in incurable cancer patients: study protocol for an open-label, randomized controlled trial (the OMAMA study). BMC Palliat. Care 2023, 22, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Ogawa, R.; Echizen, H. Clinically Significant Drug Interactions with Antacids. Drugs 2011, 71, 1839–1864. [Google Scholar] [CrossRef]
- Bradford, C.; McElduff, A. An Unusual Cause of Hypocalcaemia: Magnesium Induced Inhibition of Parathyroid Hormone Secretion in a Patient with Subarachnoid Haemorrhage. Crit. Care Resusc. 2006, 8, 36–39. [Google Scholar] [CrossRef] [PubMed]
- Muller, M.P.; Dresser, L.; Raboud, J.; McGeer, A.; Rea, E.; Richardson, S.E.; Mazzulli, T.; Loeb, M.; Louie, M. Adverse Events Associated with High-Dose Ribavirin: Evidence from the Toronto Outbreak of Severe Acute Respiratory Syndrome. Pharmacother. J. Hum. Pharmacol. Drug Ther. 2007, 27, 494–503. [Google Scholar] [CrossRef]
- Lohitnavy, M.; Lohitnavy, O.; Thangkeattiyanon, O.; Srichai, W. Reduced oral itraconazole bioavailability by antacid suspension. J. Clin. Pharm. Ther. 2005, 30, 201–206. [Google Scholar] [CrossRef]
- Mallet, L.; Huang, A. Coadministration of Gatifloxacin and Multivitamin Preparation Containing Minerals: Potential Treatment Failure in an Elderly Patient. Ann. Pharmacother. 2005, 39, 150–152. [Google Scholar] [CrossRef]
- Naggar, V.F.; Khalil, S.A. Effect of magnesium trisilicate on nitrofurantoin absorption. Clin. Pharmacol. Ther. 1979, 25, 857–863. [Google Scholar] [CrossRef]
- Auwercx, J.; Rybarczyk, P.; Kischel, P.; Dhennin-Duthille, I.; Chatelain, D.; Sevestre, H.; Van Seuningen, I.; Ouadid-Ahidouch, H.; Jonckheere, N.; Gautier, M. Mg2+ Transporters in Digestive Cancers. Nutrients 2021, 13, 210. [Google Scholar] [CrossRef]
- Bagheri, A.; Naghshi, S.; Sadeghi, O.; Larijani, B.; Esmaillzadeh, A. Total, Dietary, and Supplemental Magnesium Intakes and Risk of All-Cause, Cardiovascular, and Cancer Mortality: A Systematic Review and Dose–Response Meta-Analysis of Prospective Cohort Studies. Adv. Nutr. Int. Rev. J. 2021, 12, 1196–1210. [Google Scholar] [CrossRef]
- O’connor, E.A.; Evans, C.V.; Ivlev, I.; Rushkin, M.C.; Thomas, R.G.; Martin, A.; Lin, J.S. Vitamin and Mineral Supplements for the Primary Prevention of Cardiovascular Disease and Cancer. JAMA 2022, 327, 2334–2347. [Google Scholar] [CrossRef] [PubMed]
- Kordiak, J.; Bielec, F.; Jabłoński, S.; Pastuszak-Lewandoska, D. Role of Beta-Carotene in Lung Cancer Primary Chemoprevention: A Systematic Review with Meta-Analysis and Meta-Regression. Nutrients 2022, 14, 1361. [Google Scholar] [CrossRef] [PubMed]
- Meng, Y.; Sun, J.; Yu, J.; Wang, C.; Su, J. Dietary Intakes of Calcium, Iron, Magnesium, and Potassium Elements and the Risk of Colorectal Cancer: a Meta-Analysis. Biol. Trace Element Res. 2018, 189, 325–335. [Google Scholar] [CrossRef]
- Chen, G.-C.; Pang, Z.; Liu, Q.-F. Magnesium intake and risk of colorectal cancer: a meta-analysis of prospective studies. Eur. J. Clin. Nutr. 2012, 66, 1182–1186. [Google Scholar] [CrossRef] [PubMed]
- Song, X.; Zhong, X.; Tang, K.; Wu, G.; Jiang, Y. Serum magnesium levels and lung cancer risk: a meta-analysis. World J. Surg. Oncol. 2018, 16, 137. [Google Scholar] [CrossRef]
- Chapelle, N.; Martel, M.; Toes-Zoutendijk, E.; Barkun, A.N.; Bardou, M. Recent advances in clinical practice: colorectal cancer chemoprevention in the average-risk population. Gut 2020, 69, 2244–2255. [Google Scholar] [CrossRef] [PubMed]
- Woo, H.-T.; Jeong, S.-Y.; Shin, A. The association between prescription drugs and colorectal cancer prognosis: a nationwide cohort study using a medication-wide association study. BMC Cancer 2023, 23, 1–11. [Google Scholar] [CrossRef]
- Hashemian, M.; Poustchi, H.; Sharafkhah, M.; Pourshams, A.; Mohammadi-Nasrabadi, F.; Hekmatdoost, A.; Malekzadeh, R. Iron, Copper, and Magnesium Concentration in Hair and Risk of Esophageal Cancer: A Nested Case-Control Study. Int. J. Infect. Dis. 2023, 26, 665–670. [Google Scholar] [CrossRef]
- Song, X.; Zhong, X.; Tang, K.; Wu, G.; Jiang, Y. Serum magnesium levels and lung cancer risk: a meta-analysis. World J. Surg. Oncol. 2018, 16, 137. [Google Scholar] [CrossRef]
- Zhai, T.; Li, S.; Hu, W.; Li, D.; Leng, S. Potential Micronutrients and Phytochemicals against the Pathogenesis of Chronic Obstructive Pulmonary Disease and Lung Cancer. Nutrients 2018, 10, 813. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.R.; Sawka, A.M.; Adams, L.; Hatfield, N.; Hung, R.J. Vitamin and mineral supplements and thyroid cancer. Eur. J. Cancer Prev. 2013, 22, 158–168. [Google Scholar] [CrossRef] [PubMed]
- Shen, F.; Cai, W.-S.; Li, J.-L.; Feng, Z.; Cao, J.; Xu, B. The Association Between Serum Levels of Selenium, Copper, and Magnesium with Thyroid Cancer: a Meta-analysis. Biol. Trace Elem. Res. 2015, 167, 225–235. [Google Scholar] [CrossRef]
- Yang, D.K.; Tungalag, T.; Lee, S.-J.; Kim, S.-J. Methyl Jasmonate-induced Increase in Intracellular Magnesium Promotes Apoptosis in Breast Cancer Cells. Anticancer. Res. 2024, 44, 1087–1095. [Google Scholar] [CrossRef] [PubMed]
- Mendes, P.M.V.; Bezerra, D.L.C.; dos Santos, L.R.; Santos, R.d.O.; Melo, S.R.d.S.; Morais, J.B.S.; Severo, J.S.; Vieira, S.C.; Marreiro, D.D.N. Magnesium in Breast Cancer: What Is Its Influence on the Progression of This Disease? Biol. Trace Element Res. 2017, 184, 334–339. [Google Scholar] [CrossRef]
- Kim, J.Y.; Song, M.; Kim, M.S.; Natarajan, P.; Do, R.; Myung, W.; Won, H.-H. An atlas of associations between 14 micronutrients and 22 cancer outcomes: Mendelian randomization analyses. BMC Med. 2023, 21, 1–12. [Google Scholar] [CrossRef]
- Mendes, P.M.V.; Bezerra, D.L.C.; dos Santos, L.R.; Santos, R.d.O.; Melo, S.R.d.S.; Morais, J.B.S.; Severo, J.S.; Vieira, S.C.; Marreiro, D.D.N. Magnesium in Breast Cancer: What Is Its Influence on the Progression of This Disease? Biol. Trace Element Res. 2017, 184, 334–339. [Google Scholar] [CrossRef]
- Huang, W.-Q.; Long, W.-Q.; Mo, X.-F.; Zhang, N.-Q.; Luo, H.; Lin, F.-Y.; Huang, J.; Zhang, C.-X. Direct and indirect associations between dietary magnesium intake and breast cancer risk. Sci. Rep. 2019, 9, 5764. [Google Scholar] [CrossRef]
- Tao, M.-H.; Dai, Q.; Millen, A.E.; Nie, J.; Edge, S.B.; Trevisan, M.; Shields, P.G.; Freudenheim, J.L. Associations of intakes of magnesium and calcium and survival among women with breast cancer: results from Western New York Exposures and Breast Cancer (WEB) Study. Am J Cancer Res. 2016, 6, 105–113. [Google Scholar] [CrossRef]
- Bezerra, D.L.C.; Mendes, P.M.V.; Melo, S.R.d.S.; dos Santos, L.R.; Santos, R.d.O.; Vieira, S.C.; Henriques, G.S.; Freitas, B.d.J.e.S.d.A.; Marreiro, D.D.N. Hypomagnesemia and Its Relationship with Oxidative Stress Markers in Women with Breast Cancer. Biol. Trace Element Res. 2021, 199, 4466–4474. [Google Scholar] [CrossRef]
- Xu, L.; Tan, Y.; Xiang, P.; Luo, Y.; Peng, J.; Xiao, H.; Liu, F. Diet-Related Risk Factors for Cervical Cancer: Data from National Health and Nutrition Examination Survey 1999–2018. Nutr. Cancer 2023, 75, 1892–1899. [Google Scholar] [CrossRef]
- Wang, X.; Glubb, D.M.; O’mara, T.A. Dietary Factors and Endometrial Cancer Risk: A Mendelian Randomization Study. Nutrients 2023, 15, 603. [Google Scholar] [CrossRef] [PubMed]
- Liu, M.; Yang, H.; Mao, Y. Magnesium and liver disease. Ann. Transl. Med. 2019, 7, 578–578. [Google Scholar] [CrossRef]
- Yang, X.; Guo, J.; Li, W.; Li, C.; Zhu, X.; Liu, Y.; Wu, X. PPM1H is down-regulated by ATF6 and dephosphorylates p-RPS6KB1 to inhibit progression of hepatocellular carcinoma. Mol. Ther. - Nucleic Acids 2023, 33, 164–179. [Google Scholar] [CrossRef]
- Yu, Y.; Paragomi, P.; Wang, R.; Liang, F.; Luu, H.N.; Behari, J.; Yuan, J. High serum magnesium is associated with lower risk of hepatocellular carcinoma among patients with nonalcoholic fatty liver disease. Cancer 2023, 129, 2341–2347. [Google Scholar] [CrossRef] [PubMed]
- Parisse, S.; Ferri, F.; Persichetti, M.; Mischitelli, M.; Abbatecola, A.; Di Martino, M.; Lai, Q.; Carnevale, S.; Lucatelli, P.; Bezzi, M.; et al. Low serum magnesium concentration is associated with the presence of viable hepatocellular carcinoma tissue in cirrhotic patients. Sci. Rep. 2021, 11, 1–8. [Google Scholar] [CrossRef]
- Mehata, A.K.; Singh, V.; Vikas; Srivastava, P.; Koch, B.; Kumar, M.; Muthu, M.S. Chitosan nanoplatform for the co-delivery of palbociclib and ultra-small magnesium nanoclusters: dual receptor targeting, therapy and imaging. Nanotheranostics 2024, 8, 179–201. [Google Scholar] [CrossRef]
- A Betallu, M.; Bhalara, S.R.; Sapnar, K.B.; Tadke, V.B.; Meena, K.; Srivastava, A.; Kundu, G.C.; Gorain, M. Hybrid Inorganic Complexes as Cancer Therapeutic Agents: In-vitro Validation. Nanotheranostics 2023, 7, 270–280. [Google Scholar] [CrossRef]
- Park, H.; Qin, R.; Smith, T.J.; Atherton, P.J.; Barton, D.L.; Sturtz, K.; Dakhil, S.R.; Anderson, D.M.; Flynn, K.; Puttabasavaiah, S.B.; et al. North Central Cancer Treatment Group N10C2 (Alliance). Menopause 2015, 22, 627–632. [Google Scholar] [CrossRef]
- Wolf, F.I.; Cittadini, A.R.M.; Maier, J.A.M. Magnesium and tumors: Ally or foe? Cancer Treat. Rev. 2009, 35, 378–382. [Google Scholar] [CrossRef] [PubMed]
- A Wark, P.; Lau, R.; Norat, T.; Kampman, E. Magnesium intake and colorectal tumor risk: a case-control study and meta-analysis. Am. J. Clin. Nutr. 2012, 96, 622–631. [Google Scholar] [CrossRef]
- Mahabir, S.; Wei, Q.; Barrera, S.L.; Dong, Y.Q.; Etzel, C.J.; Spitz, M.R.; Forman, M.R. Dietary magnesium and DNA repair capacity as risk factors for lung cancer. Carcinog. 2008, 29, 949–956. [Google Scholar] [CrossRef]
- Maier, J.A.; Nasulewicz-Goldeman, A.; Simonacci, M.; Boninsegna, A.; Mazur, A.; Wolf, F.I. Insights Into the Mechanisms Involved in Magnesium-Dependent Inhibition of Primary Tumor Growth. Nutr. Cancer 2007, 59, 192–198. [Google Scholar] [CrossRef]
- Sugimoto, J.; Romani, A.M.; Valentin-Torres, A.M.; A Luciano, A.; Kitchen, C.M.R.; Funderburg, N.; Mesiano, S.; Bernstein, H.B. Magnesium Decreases Inflammatory Cytokine Production: A Novel Innate Immunomodulatory Mechanism. J. Immunol. 2012, 188, 6338–6346. [Google Scholar] [CrossRef]
- Song, Y.; Li, T.Y.; van Dam, R.M.; E Manson, J.; Hu, F.B. Magnesium intake and plasma concentrations of markers of systemic inflammation and endothelial dysfunction in women. Am. J. Clin. Nutr. 2007, 85, 1068–1074. [Google Scholar] [CrossRef]
- Henriksen, C.; Aaseth, J.O. Magnesium: a scoping review for Nordic Nutrition Recommendations 2023. Food Nutr. Res. 2023, 67. [Google Scholar] [CrossRef]
- Leidi, M.; Wolf, F.; Maier, J.A.M. Magnesium and cancer: more questions than answers. In Magnesium in the Central Nervous System [Internet]; Vink, R., Nechifor, M., Eds.; University of Adelaide Press: Adelaide (AU), 2011. [Google Scholar] [PubMed]
- Schwalfenberg, G.K.; Genuis, S.J. The Importance of Magnesium in Clinical Healthcare. Scientifica 2017, 2017, 1–14. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



