
Submitted:
01 June 2023
Posted:
07 June 2023
You are already at the latest version
Abstract
It is a well-established fact that inadequate Vitamin D (Vit-D) levels have negative effects on the development and progression of malignant diseases, mainly cancer. The purpose of this paper was to elucidate the effects of Vit-D intake and serum 25-hydroxyvitamin-D (25(OH)D) levels on cancer incidence and mortality, the current evidence in this field, and the biases of this evidence using the meta-meta-analysis method. Meta-analyses focusing on Vit-D intake, serum 25(OH)D levels, and cancer risk/mortality were identified. A structured computer literature search was performed in PubMed/Medline, Web of Science (WoS), and Scopus electronic databases using predetermined keyword combinations. Primary and secondary meta-meta-analyses were carried out, combining odds ratios (ORs), risk ratios (RRs), and hazard ratios (HRs) for outcomes reported in selected meta-analyses. A total of 35 eligible meta-analyses assessing the association between Vit-D and cancer incidence and/or mortality were included in this study. In the pooled analysis, higher Vit-D intake and serum 25(OH)D levels were associated with lower cancer risk (OR = 0.93, 95% CI: 0.90-0.96, p < 0.001; OR = 0.80, 95% CI: 0.72-0.89, p < 0.001, respectively) and cancer-related mortality (RR = 0.89, 95% CI: 0.86-0.93, p < 0.001; RR = 0.67, 95% CI: 0.58-0.78, p < 0.001, respectively). When meta-analyses whose primary reports included only randomized controlled trials were pooled, there was no significant association between Vit-D intake and cancer risk (OR = 0.99, 95% CI: 0.97-1.01, p = 0.320). In subgroup analysis, Vit-D consumption was associated with a significant decrease in colorectal and lung cancer incidence (OR = 0.89, 95% CI: 0.83-0.96, p = 0.002; OR = 0.88, 95% CI: 0.83-0.94, p < 0.001, respectively). Taken together, both Vit-D intake and higher 25(OH)D levels may provide remarkable benefits in terms of cancer incidence and mortality, however, careful evaluation according to cancer types is critically important and recommended.
Keywords:
cancer
; meta-analysis
; vitamin D
; mortality
; incidence
1. Introduction
Cancer, which comprises a diverse set of diseases characterized by irregular cell proliferation and an unregulated cell cycle, remains a major cause of death globally, regardless of human development levels in countries all over the world [1,2,3,4]. According to Global Cancer Observatory (GLOBOCAN) data, approximately 19.3 million new cancer cases were reported, and 10 million deaths were attributed to cancer worldwide in 2020 [2,3]. Based on the 2019 data provided by the World Health Organization (WHO), cancer is identified as the primary or secondary cause of death for individuals under the age of 70 in over half of the world’s nations (183 countries), while it ranks as the third or fourth leading cause of death in other countries [2,5].
Vitamin D (Vit-D) was identified as a pro-hormone that provides a range of health benefits, from bone health to immune function, and plays critical roles in biological processes in human metabolism [6,7]. It is widely acknowledged that inadequate Vit-D levels have negative effects on the development and advancement of malignant disorders, mainly cancer, because they impair immune adequacy, increase the risk of complications, and affect both the physical and mental quality of life (QoL) of individuals [8,9,10]. Observational epidemiological studies on Vit-D have emphasized the importance of Vit-D in both preventing cancer and cancer-related deaths and improving the prognosis of patients with cancer [8,9,10,11].
Numerous studies have reported results suggesting a possible association between Vit-D deficiency and the risk of cancer, as well as cancer-related deaths [12,13,14]. As is well documented, numerous epidemiological studies have demonstrated an inverse relationship between Vit-D levels and various types of cancer. These studies have provided compelling evidence for the association between higher Vit-D levels and a decreased risk of developing cancers such as breast, prostate, colon, and lung cancer [15,16,17]. The findings from these studies strongly suggest that maintaining adequate Vit-D levels may play a protective role in reducing the risk of these cancer types. However, conflicting outcomes have been reported in previous primary studies and meta-analyses regarding serum 25-hydroxyvitamin-D (25(OH)D) levels and Vit-D intake. So that, in a meta-analysis of randomized controlled trials (RCTs) carried out by Goulão et al. [18], which included 18,808 participants, it was reported that there was no evidence that Vit-D intake alone reduced cancer incidence or cancer related deaths, even after long-term follow-up results were included (risk ratio (RR) = 1.03, 95% CI: 0.91-1.15, p > 0.05). Similarly, two recent meta-analyses evaluating Vit-D intake and cancer risk reported that Vit-D intake did not decrease the overall cancer incidence (RR = 0.99, %95 CI: 0.94-1.04, p > 0.05; RR = 0.98, %95 CI: 0.94-1.02, p > 0.05) [19,20]. In contrast to the previously specified meta-analyses, several meta-analyses that incorporated observational epidemiological studies found an association between high Vit-D intake or high serum 25(OH)D levels and a decreased risk of different types of cancer. Some of these meta-analyses reported that high Vit-D intake or high serum 25(OH)D levels were associated with a reduced risk of colorectal cancer. [12,14,21]. Additionally, high Vit-D intake or high serum 25(OH)D levels were associated with a lower risk of liver cancer [13], ovarian cancer [22], and lung cancer [23,24].
In general, studies related to the potential benefits of Vit-D intake and serum 25(OH)D levels in reducing the risk of cancer and cancer-related mortality are important topics of ongoing research and discussion in the scientific society. Also, it is a well-known fact that meta-analyses examining the association between Vit-D intake, serum 25(OH)D levels, and different forms of cancer hold considerable significance due to their high level of evidence in the scientific community. In the last decade, there has been a notable rise in the number of published meta-analyses that specifically evaluate the association between Vit-D and cancer. An additional crucial point for consideration is the ongoing necessity to consistently reevaluate and consolidate the existing evidence regarding the potential advantages or disadvantages of Vit-D in order to decrease the risk of cancer and cancer-related mortality. The primary objective of this reevaluation is to evaluate the current state of the epidemiological landscape, which has evolved extensively over the course of time.
Therefore, in this paper, we aimed to elucidate the effects of Vit-D intake and serum 25(OH)D levels on cancer incidence and mortality, the current evidence in this field, and the biases of this evidence using the meta-meta-analysis method.
2. Methods
Meta-analyses that specifically assessed the relationship between Vit-D intake, serum 25(OH)D levels and the risk of cancer and/or mortality were identified for inclusion in the study. In accordance with this purpose, to ensure methodological rigor and transparency, the study strictly adhered to the standardized methodology guidelines recommended in the "Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA)" [25] and "Meta-analysis of Observational Studies in Epidemiology (MOOSE)" [26] guidelines. These guidelines provided a comprehensive framework for conducting the study, ensuring consistent and reliable methods at all stages of the meta-meta-analysis. The PRISMA Checklist was associated with Supp. Table S1. This checklist served as a tool to verify compliance with the PRISMA guidelines and to ensure the completeness and accuracy of the reporting in the study.
PICOs:
1. Population: “Patients with cancer and individuals without cancer”
2. Intervention: “Vit-D intake and serum 25(OH)D levels”
3. Comparison: “Low and high Vit-D intake / low and high serum 25(OH)D levels”
4. Outcomes: i) “Cancer risk; ii) “Mortality risk”
5. Study: “Systematic reviews with meta-analysis”
2.1. Search Strategy and Data Extraction
A structured computer literature search was carried out in PubMed/Medline, Web of Science (WoS), and Scopus electronic databases using predetermined keyword combinations. Keyword selection was structured by considering three main factors: "cancer", "vitamin D" and "meta-analysis". Once the search strategy was formulated through the Pubmed/Medline database, it was adapted to other databases (WoS and Scopus). Medical Subject Headings (MeSH) and text terms were incorporated into the search strategy via Boolean operators (AND/OR). Keyword combinations are determined as follows: "vitamin D"[Title/Abstract] OR "D vitamin"[Title/Abstract] OR "calciferol"[Title/Abstract] OR "cholecalciferol"[Title/Abstract] OR "cholecalciferol-D3"[Title/Abstract] OR "Vitamin-D3"[Title/Abstract] OR "25 hydroxy vitamin D"[Title/Abstract] OR "25 hydroxy vitamin D3"[Title/Abstract] AND "cancer"[All Fields] OR "tumor"[All Fields] OR "neoplasms"[All Fields] OR "tumours"[All Fields] "malignance"[All Fields] AND "meta-analysis"[Title/Abstract]. Details of the algorithms used for the three databases (Pubmed/Medline, WoS, and Scopus) were illustrated in Supp. Table S2.
2.2. Selection Criteria
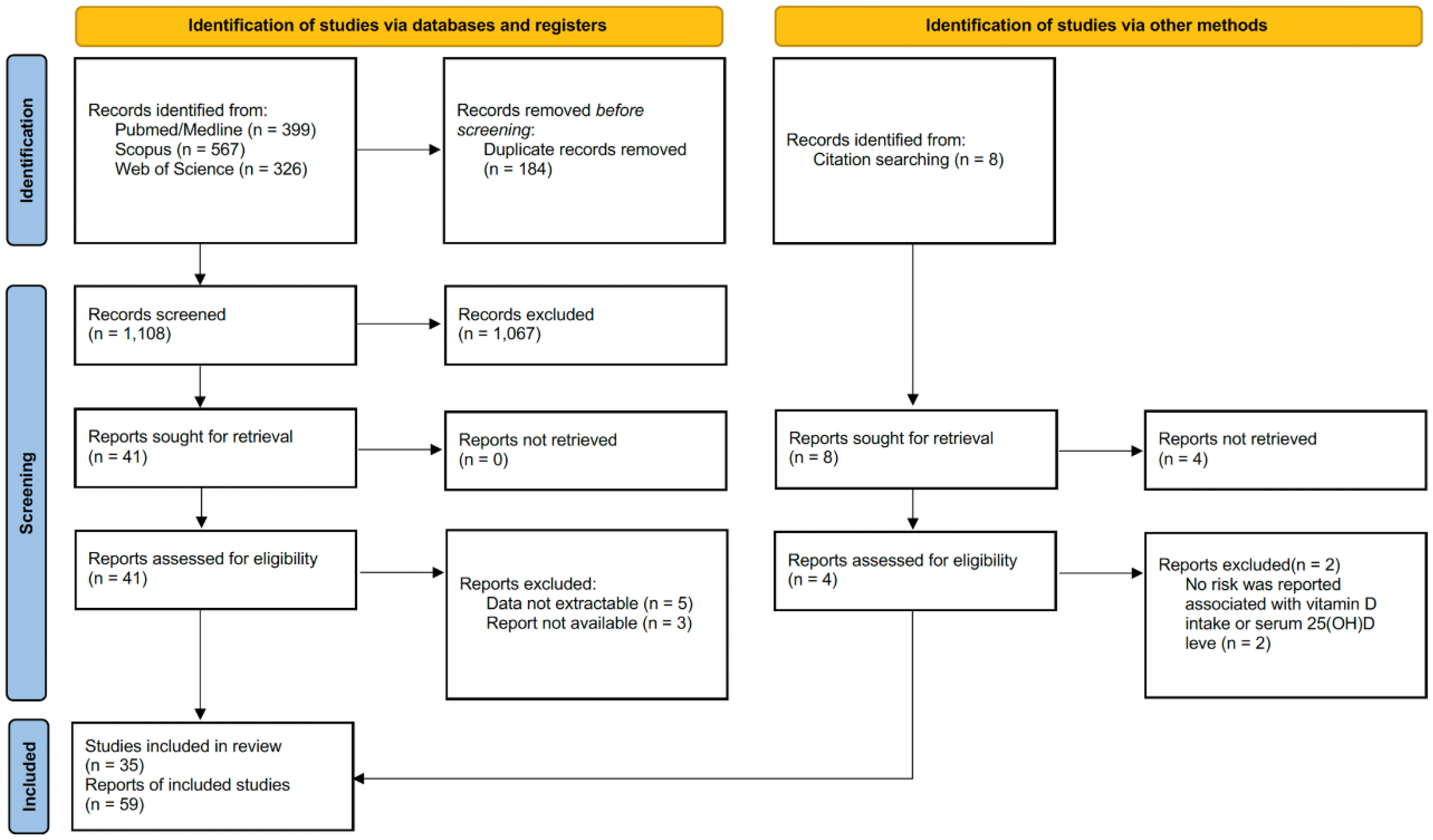
Initially, a preliminary data review was conducted to assess the relevance of systematic reviews (with meta-analysis) concerning the questions and objectives of the research. During the initial assessment, the title, abstract, and keywords of each meta-analysis were thoroughly scrutinized. This evaluation process involved carefully reviewing the provided information to determine the relevance of the meta-analysis to the research question or topic of interest. If the abstracts contain insufficient information, the full text has been reviewed. In the second evaluation, the full texts were examined in detail to determine whether the studies met all the inclusion criteria. The data illustrated in the results section were extracted using a structured protocol that was designed to capture the most applicable information from each study [27]. The PRISMA flowchart showing the selection process for included and excluded studies was available in Figure 1.
Meta-analyses reporting a risk in terms of incidence and/or mortality associated with cancer and Vit-D intake (low and high intake) or serum 25(OH)D levels (low and high level) were included in the study. The study exclusively considered reports and studies that were published in English and were accessible in full text. Animal model experiments, cell culture studies, non-original publications (letter to the editor, case report), systematic reviews without meta-analysis, outcomes not reported as risks [odds ratios (OR), risk ratios (RR), or hazard ratios (HR)] has been excluded from the study. The results reported in each systematic review with meta-analysis were synthesized by two independent and qualified investigators (MEA and HE). Data extracted from each study was processed in a predefined and structured Microsoft Excel® spreadsheet. After removing all data from the meta-analyses included in the study by two investigators (MEA and HE), the other researcher (YB) independently reviewed and cross-checked the data to ensure accuracy, consistency, and reliability to reach a consensus. Any discrepancies or inconsistencies that arose were thoroughly discussed, evaluated, and resolved through consensus among the research team.
Figure 1.
The PRISMA flowchart showing the relevant literature (Pubmed/Medline, Scopus, and Web of Science) scans and the study selection process.
Figure 1.
The PRISMA flowchart showing the relevant literature (Pubmed/Medline, Scopus, and Web of Science) scans and the study selection process.
2.3. Methodological Quality Assessment
The quality of meta-analyses was evaluated using the 16-item AMSTAR-2 (A MeaSurement Tool to Assess Systematic Reviews) tool (Table S3) [28]. Seven of the 16 items in AMSTAR-2 were classified as critical items (items 2, 4, 7, 9, 11, 13, 15). AMSTAR-2 has been defined as an evaluation tool developed to enable the evaluation of systematic reviews of randomized and non-randomized studies of health interventions. AMSTAR-2 was not intended to constitute an overall score. Each item was evaluated as “yes”, “partial yes” or “no” according to the standard. The overall evaluation of studies (high, moderate, low, or critically low) was based on the evaluation of critical and non-critical items. The quality of the included systematic reviews with meta-analysis was also evaluated by two independent researchers.
2.4. Assessment of Risk of Bias
The Risk of Bias in Systematic Reviews (ROBIS) (Table S4) [29] tool was used to assess the risk of bias in the included studies. The ROBIS tool is designed to assess the risk of bias in systematic reviews and/or meta-analysis. The risk of bias is assessed in three phases. In the first phase, “assessment relevance” is evaluated. The aim of the second phase is to “identify concerns with the review process”. In the third phase, a comprehensive evaluation related to “data collection and study appraisal” is presented.
2.5. Data Appraisal, Synthesis, and Statistical Analysis
Primary and secondary meta-meta-analyses were carried out combining OR, RR, and HR for outcomes reported in selected meta-analyses. Initially, an analysis was performed that summarized all available data into a single pooled estimate. After initial pooling, subgroup analyses were performed to assess the heterogeneity of results and to examine the effects of Vit-D intake and serum 25(OH)D levels in different cancer and study types. Pooled effect sizes (ES) and ORs, RRs and/or HRs were calculated at 95% confidence intervals (CI) for all groups in primary and secondary meta-meta-analyses. A predefined spreadsheet was created using Microsoft Excel® to systematically document key qualitative and quantitative data from the included meta-analyses.
Egger’s linear regression asymmetry (statistical significance set at p < 0.10) test [30], schematic illustration of the funnel plots, and Begg and Mazumdar’s rank correlation test [31], which reported the z-value for Kendall’s tau, were used to quantify the possibility of publication bias. The trim and fill method was used to adjust for publication bias where possible when reporting bias was detected [32]. The heterogeneity of the results from the different meta-analyses was evaluated using the χ2-based Cochran’s Q test (p < 0.05) and I2 statistics (percentage of variances in the effect estimates due to statistical heterogeneity). The I2 statistics describes the observed percentages based on the variance in the true effects. In the assessment of I2 values, a result of 25% is considered low heterogeneity, 50% is considered moderate heterogeneity, and 75% is considered high heterogeneity [33]. In the statistical calculations of primary and secondary meta-meta-analyses, method selection was performed taking into account heterogeneity among the studies. When significant heterogeneity was detected among the studies, analyses were conducted using the random effects model. If there was no significant heterogeneity, analyses were carried out via a fixed effects model. Statistical significance in all meta-meta-analyses was quantified at the two-tailed p < 0.05 level. Meta-meta-analysis statistical calculations were performed using Prometa3® meta-analysis software [34] and R version 4.2.0 [35].
2.6. Sensitivity Analysis
The robustness of the results was evaluated through sensitivity analysis. In sensitivity analyses, each study is excluded from the pooled analysis separately, and then the change in ES is examined. Studies reporting outliers are identified by this method. When necessary, these studies are excluded from the pooled analysis and the confidence intervals are strengthened.
2.7. Mapping
A visual map of the scientific evidence was created for each systematic review to visually display the information via a bubble chart. Review information was based on three dimensions:
1. Study population (bubble size and bubble color): The size of each bubble is structured to be directly proportional to the sample size of the original studies included in each of the systematic reviews. Moreover, studies with a relatively large sample, studies with a medium sample, and studies with a relatively small sample were colored separately.
2. Impact (x) axis: Each of the reviews was classified according to the year of publication.
3. Strength of results (y-axis): It was structured as the number of primary studies included in each study.
3. Results
3.1. Search Results
A total of 1,292 papers were identified in the initial search of the relevant databases [Pubmed/Medline (n = 399), Scopus (n = 567), and WoS (n = 326)], and 184 of these studies were removed without review due to duplicate records. After the duplicate records were removed, the studies (n = 1,108) yielded were evaluated by examining the titles and abstracts. In this preliminary review, 1,067 ineligible research were excluded from the study. The full texts of 49 papers were evaluated in detail, including 41 articles in the main search and eight articles in the citation search. After all reviews, 59 reports from 35 papers [12,13,14,18,19,20,21,22,23,24,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60] that ultimately met the inclusion criteria were included in the meta-meta-analysis. The included (Table S6) and excluded meta-analyses and the reasons for excluding the removed studies are summarized in Supp. Table S7. The PRISMA flowchart showing the relevant literature scans and the study selection process was also illustrated in Figure 1.
3.2. Baseline Characteristics of the Meta-analyses
A total of 35 eligible meta-analyses [12,13,14,18,19,20,21,22,23,24,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60] examining the association between Vit-D and cancer incidence and/or mortality as well as reporting risk for cancer incidence and/or mortality were included in the current study. The sample sizes of the studies varied between 1,902 and 1,566,662. Of these meta-analyses, 20 studies [12,13,14,18,21,22,36,37,40,42,44,45,46,47,48,53,54,57,59,60] reported risk for total cancer and various cancer types, three studies [49,50,52] reported mortality, and 12 studies [19,20,23,24,38,39,41,43,51,55,56,58] reported both mortality and risk. In eight meta-analyses [18,19,20,39,41,56,58,60], the primary studies consisted of RCTs. One of these meta-analyses reported breast cancer-related risk [60], while other studies documented total cancer incidence and/or mortality. The primary reports of three meta-analyses [46,49,50] were included cohort studies. In other studies, case-control, cohort, and/or RCTs were evaluated in various combinations. The baseline characteristics of the meta-analyses included in the study are associated with Table 1.

Table 1.
Baseline characteristics and odds ratios (ORs), hazard ratios (HRs), and/or risk ratios (RRs) of studies on vitamin D included in the meta-meta-analysis.
Table 1.
Baseline characteristics and odds ratios (ORs), hazard ratios (HRs), and/or risk ratios (RRs) of studies on vitamin D included in the meta-meta-analysis.
| First author/year | Cancer type | Characteristics of the primary studies | Vit-D exposure | Total number of studies (n) | Total sample size (n) | Outcome | NoP studies included for incidence (n) | NoP studies included for mortality (n) | Effect size (ES) and confidence interval (CI) for incidence | Effect size (ES) and confidence interval (CI) for mortality |
| Boughanem 2022 (a)x (21) | Colorectal cancer | Case-control, prospective cohort | Vit-D intake | 31 | 926.237 | Incidence | 12 | N/A | OR = 0.75 (0.67-0.85) | N/A |
| Boughanem 2022 (b)y (21) | Colorectal cancer | Case-control, prospective cohort | Vit-D intake | 31 | 926.237 | Incidence | 6 | N/A | HR = 0.94 (0.79-1.11) | N/A |
| Cheema 2022 (19) | Total cancer | RCTs | Vit-D intake | 13 | 109.543 | Incidence, mortality | 12 | 7 | RR = 0.99 (0.94-1.04) | RR = 0.93 (0.84-1.03) |
| Chen 2022 (a) (36) | Gastric cancer | Case-control, prospective cohort | Serum 25(OH)D | 11 | N/A | Incidence | 11 | N/A | OR = 0.93 (0.77-1.11) | N/A |
| Chen 2022 (b) (36) | Gastric cancer | Case-control, prospective cohort | Vit-D intake | 11 | N/A | Incidence | 4 | N/A | OR = 1.00 (0.86-1.16) | N/A |
| Ekmekcioglu 2017 (12) | Colorectal cancer | Case-control, prospective cohort | Serum 25(OH)D | 14 | 12.110 | Incidence | 14 | N/A | RR = 0.62 (0.56-0.70) | N/A |
| Gao 2018 (37) | Prostate cancer | Case-control, prospective cohort | Serum 25(OH)D | 19 | 48.369 | Incidence | 19 | N/A | RR = 1.15 (1.06-1.24) | N/A |
| Goulão 2018 (18) | Total cancer | RCTs | Vit-D intake | 30 | 18.808 | Incidence | 24 | 7 | RR = 1.03 (0.91-1.15) | RR = 0.88 (0.70-1.09) |
| Guo 2020 (13) | Liver cancer | Case-control, prospective cohort | Serum 25(OH)D | 6 | 60.811 | Incidence | 6 | N/A | RR = 0.78 (0.63-0.95) | N/A |
| Guo 2022 (20) | Total cancer | RCTs | Vit-D intake | 26 | 121.529 | Incidence, mortality | 19 | 11 | RR = 0.98 (0.94-1.02) | RR = 0.88 (0.80-0.96) |
| Han 2019 (38) | Total cancer | Prospective cohort | Serum 25(OH)D | 23 | 170.618 | Incidence, mortality | 8 | 16 | RR = 0.86 (0.73-1.02) | RR = 0.81 (0.71-0.93) |
| Haykal 2019 (39) | Total cancer | RCTs | Vit-D intake | 10 | 79.055 | Incidence, mortality | 9 | 5 | RR = 0.96 (0.86-1.07) | RR = 0.87 (0.79-0.96) |
| Hernandez-Alonso 2023 (a) (14) | Colorectal cancer | Case-control | Serum 25(OH)D | 28 | 140.112 | Incidence | 11 | N/A | OR = 0.61 (0.52-0.71) | N/A |
| Hernandez-Alonso 2023 (b) (14) | Colorectal cancer | Prospective cohort | Serum 25(OH)D | 28 | 140.112 | Incidence | 6 | N/A | HR = 0.80 (0.66-0.97) | N/A |
| Huncharek 2009 (40) | Colorectal cancer | Case-control, cohort | Vit-D intake | 60 | N/R | Incidence | 10 | N/A | RR = 0.94 (0.83-1.06) | N/A |
| Keum 2014 (41) | Total cancer | RCTs | Vit-D intake | 4 | 45.151 | Incidence, mortality | 4 | 3 | RR = 1.00 (0.94-1.06) | RR = 0.88 (0.78-0.98) |
| Khayatzadeh 2015 (a) (42) | Gastric cancer | Case-control, cohort | Vit-D intake | 7 | 59.626 | Incidence | 4 | N/A | OR = 1.09 (0.94-1.25) | N/A |
| Khayatzadeh 2015 (b) (42) | Gastric cancer | Case-control, cohort | Serum 25(OH)D | 7 | 59.626 | Incidence | 3 | N/A | OR = 0.92 (0.74-1.14) | N/A |
| Kim 2014 (a) (43) | Breast cancer | Case-control, cohort | Vit-D intake | 30 | 762.859 | Incidence | 12 | N/A | RR = 0.95 (0.88-1.01) | N/A |
| Kim 2014 (b) (43) | Breast cancer | Case-control, cohort | Serum 25(OH)D | 30 | 762.859 | Incidence, mortality | 14 | 4 | RR = 0.92 (0.83-1.02) | RR = 0.58 (0.40-0.85) |
| Lee 2011 (44) | Colorectal cancer | Case-control, cohort | Serum 25(OH)D | 8 | N/A | Incidence | 8 | N/A | OR = 0.66 (0.54-0.81) | N/A |
| Liao 2015 (45) | Bladder cancer | Case-control, cohort | Serum 25(OH)D | 5 | 89.610 | Incidence | 5 | N/A | RR = 0.75 (0.65-0.87) | N/A |
| Liao 2020 (22) | Ovarian cancer | Case-control, cohort | Vit-D intake | 29 | 963.604 | Incidence | 6 | N/A | RR = 0.80 (0.67-0.95) | N/A |
| Liu 2015 (46) | Colorectal cancer | Cohort | Vit-D intake | 47 | 870.330 | Incidence | 17 | N/A | RR = 0.87 (0.77-0.99) | N/A |
| Liu 2017 (a) (23) | Lung cancer | Case-control, cohort | Vit-D intake | 22 | 813.801 | Incidence | 6 | N/A | OR = 0.89 (0.83-0.97) | N/A |
| Liu 2017 (b) (23) | Lung cancer | Case-control, cohort | Serum 25(OH)D | 22 | 813.801 | Incidence, mortality | 8 | 3 | OR = 0.72 (0.61-0.85) | OR = 0.39 (0.28-0.54) |
| Liu 2018 (a)* (47) | Pancreatic cancer | Case-control, cohort, RCTs |
Vit-D intake | 25 | 1.213.821 | Incidence | 11 | N/A | RR = 0.90 (0.83-0.98) | N/A |
| Liu 2018 (b)** (47) | Pancreatic cancer | Case-control, cohort, RCTs |
Vit-D intake | 25 | 1.213.821 | Incidence | 14 | N/A | RR = 0.79 (0.73-0.85) | N/A |
| Lopez-Caleya 2022 (48) | Colorectal cancer | Case-control | Vit-D intake | 55 | 55.522 | Incidence | 23 | N/A | OR = 0.96 (0.93-0.98) | N/A |
| Maalmi 2014*** (49) | Breast cancer | Cohort | Serum 25(OH)D | 5 | 4.413 | Mortality | N/A | 3 | N/A | HR = 0.57 (0.38-0.84) |
| Maalmi 2018*** (50) | Colorectal cancer | Cohort | Serum 25(OH)D | 11 | 7.718 | Mortality | N/A | 6 | N/A | HR = 0.67 (0.57-0.78) |
| Pu 2021 (a) (51) | Head and neck cancer | Case-control, cohort | Vit-D intake | 16 | 81.908 | Incidence | 3 | N/A | OR = 0.77 (0.65-0.92) | N/A |
| Pu 2021 (b) (51) | Head and neck cancer | Case-control, cohort | Serum 25(OH)D | 16 | 81.908 | Incidence, mortality | 5 | 3 | OR = 0.68 (0.59-0.78) | OR = 0.75 (0.60-0.94) |
| Shahvazi 2019 (52) | Prostate cancer | Clinical trials | Vit-D intake | 22 | 1.902 | Mortality | N/A | 3 | N/A | RR = 1.05 (0.81-1.36) |
| Sun 2021 (a) (24) | Lung cancer | Case-control, cohort, RCTs | Serum 25(OH)D | 40 | 1.566.662 | Incidence, mortality | 16 | 9 | RR = 0.91 (0.84-0.98) | RR = 0.71 (0.53-0.97) |
| Sun 2021 (b) (24) | Lung cancer | Case-control, cohort, RCTs | Vit-D intake | 40 | 1.566.662 | Incidence | 4 | N/A | RR = 0.90 (0.80-1.03) | N/A |
| Wei 2018 (a) (53) | Lung cancer | Case-control, cohort | Serum 25(OH)D | 16 | 280.127 | Incidence | 12 | N/A | RR = 1.04 (0.94-1.15) | N/A |
| Wei 2018 (b) (53) | Lung cancer | Case-control, cohort | Vit-D intake | 16 | 280.127 | Incidence | 5 | N/A | RR = 0.85 (0.74-0.98) | N/A |
| Xu 2021 (54) | Colorectal cancer | Case-control, cohort | Vit-D intake | 25 | 911.638 | Incidence | 21 | N/A | OR = 0.87 (0.82-0.92) | N/A |
| Zhang 2017 (a) (55) | Pancreatic cancer | Case-control, cohort | Serum 25(OH)D | 12 | 893.168 | Incidence, mortality | 5 | 5 | RR = 1.02 (0.66-1.57) | HR = 0.81 (0.68-0.96) |
| Zhang 2017 (b) (55) | Pancreatic cancer | Case-control, cohort | Vit-D intake | 12 | 893.168 | Incidence | 2 | N/A | RR = 1.11 (0.67-1.86) | N/A |
| Zhang 2019 (56) | Total cancer | RCTs | Vit-D intake | 10 | 81.362 | Incidence, mortality | 10 | 7 | RR = 0.99 (0.94-1.03) | RR = 0.87 (0.79-0.95) |
| Zhang 2021 (57) | Liver cancer | Kohort | Serum 25(OH)D | 6 | 6.357 | Incidence | 6 | N/A | HR = 0.53 (0.41-0.68) | N/A |
| Zhang 2022 (58) | Total cancer | RCTs | Vit-D intake | 12 | 72.669 | Incidence, mortality | 11 | 6 | RR = 0.99 (0.93-1.06) | RR = 0.96 (0.80-1.16) |
| Zhao 2016 (59) | Bladder cancer | Case-control, cohort | Serum 25(OH)D | 7 | 90.757 | Incidence | 7 | N/A | OR = 0.76 (0.66-1.87) | N/A |
| Zhou 2020 (60) | Breast cancer | RCTs | Vit-D intake | 8 | 72.275 | Incidence | 6 | N/A | RR = 1.04 (0.85-1.29) | N/A |
NOP number of studies, HR hazard ratio, OR odds ratio, RR risk ratio, CI confidence interval, RCTs randomized controlled trials, Vit-D Vitamin D, 25(OH)D 25-hidroksivitamin-D, N/R not reported, N/A not available or data missing,.x case-control studies, y prospective cohort studies, *prospective studies, **retrospective studies, *** cancer related mortality.
Methodological quality assessment of 35 meta-analyses was performed using the AMSTAR-2 tool (Table S3). In the vast majority of evaluated studies, two or more critical defects were identified (especially item 7). Therefore, it was observed that most of the meta-analyses did not have very high-quality scores. Detailed assessment results are shown in Supp. Table S3. All included systematic reviews with meta-analysis were considered low risk in phase 1 and domain 1 according to ROBIS guidelines. We observed that there was no obvious risk of bias in the most of studies. In other domains, there was no obvious risk of bias in most studies. Detailed assessment results are summarized in Table S5.
3.3. Outcomes
The primary meta-meta-analysis included 59 reports from a total of 35 eligible studies [12,13,14,18,19,20,21,22,23,24,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60] evaluating Vit-D and cancer incidence/mortality. Vit-D intake and cancer risk were documented in 25 reports; serum 25(OH)D levels and cancer risk were documented in 18 reports; Vit-D intake and cancer-related mortality were documented in eight reports; and serum 25(OH)D levels and cancer-related mortality were documented in eight reports (Table 1).
3.4. Vitamin D Intake and Cancer Risk/Mortality
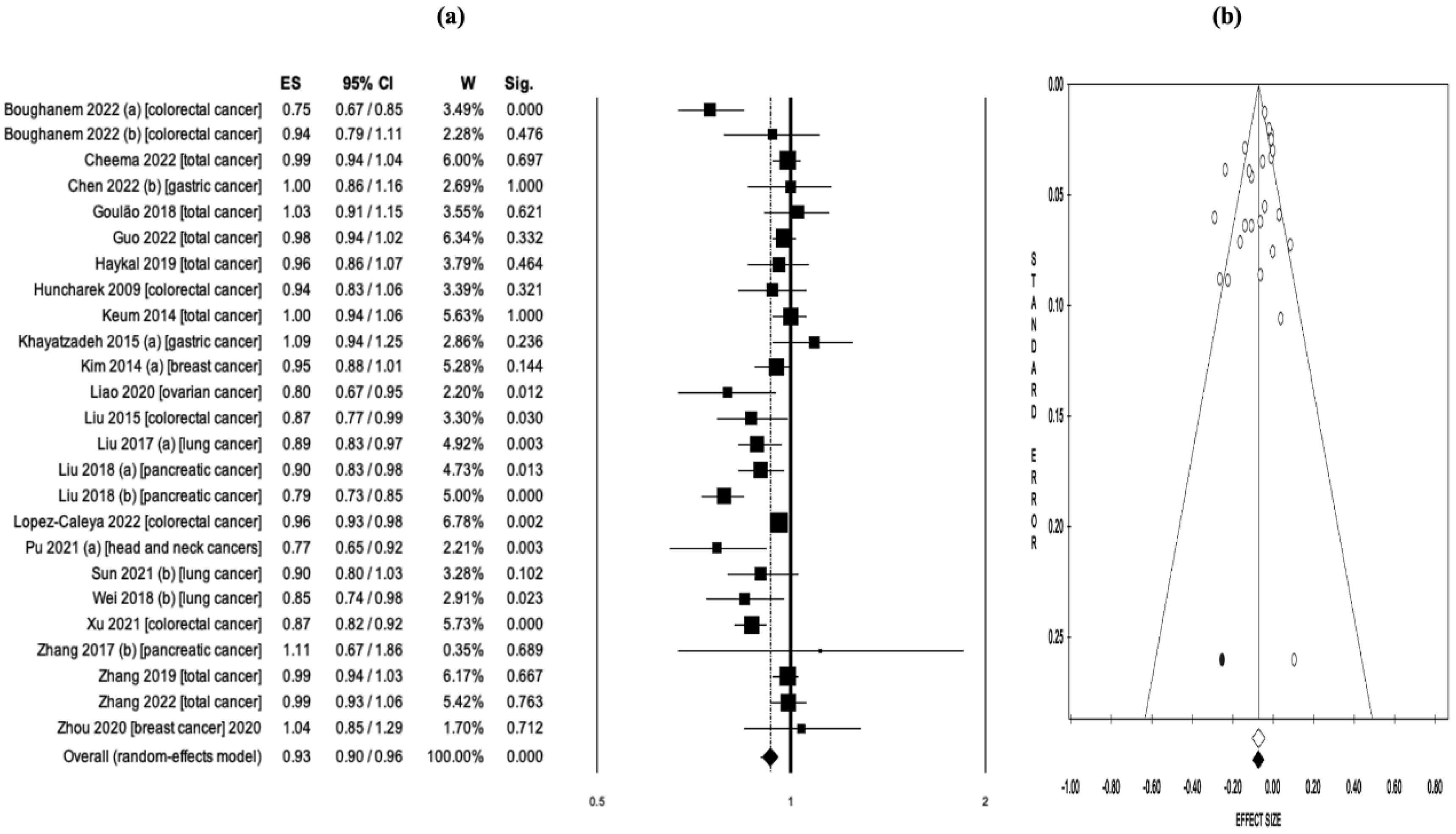
A pooled analysis of a total of 25 reports evaluating Vit-D intake and cancer risk concluded that higher Vit-D intake was associated with lower cancer risk (OR = 0.93, 95% CI: 0.90–0.96, p < 0.001) (Figure 2a). Significant heterogeneity was detected between studies (Q = 85.1, df = 24, I2 = 71.8%, p < 0.001), and analyses were performed using the random effects model. There was no evidence of publication bias in the study reports according to the results of Egger’s linear regression asymmetry test (intercept = –1.05, t = –1.55, p = 0.134) and Begg and Mazumdar’s rank correlation test (z = –1.26, p = 0.207) (Figure 2b). Sensitivity analyses were also performed, excluding each study from the analysis (individually exclusion). Sensitivity analysis confirmed the robustness of the test results (Figure S1).
Figure 2.
(a) Pooled effect size (ES) associated with vitamin D intake (low and high intake) and cancer risk, and (b) funnel plot. There was no evidence of publication bias in the study reports according to the results of Egger’s linear regression asymmetry test (intercept = -1.05, t = -1.55, p = 0.134) and Begg and Mazumdar’s rank correlation test (z = -1.26, p = 0.207).
Figure 2.
(a) Pooled effect size (ES) associated with vitamin D intake (low and high intake) and cancer risk, and (b) funnel plot. There was no evidence of publication bias in the study reports according to the results of Egger’s linear regression asymmetry test (intercept = -1.05, t = -1.55, p = 0.134) and Begg and Mazumdar’s rank correlation test (z = -1.26, p = 0.207).
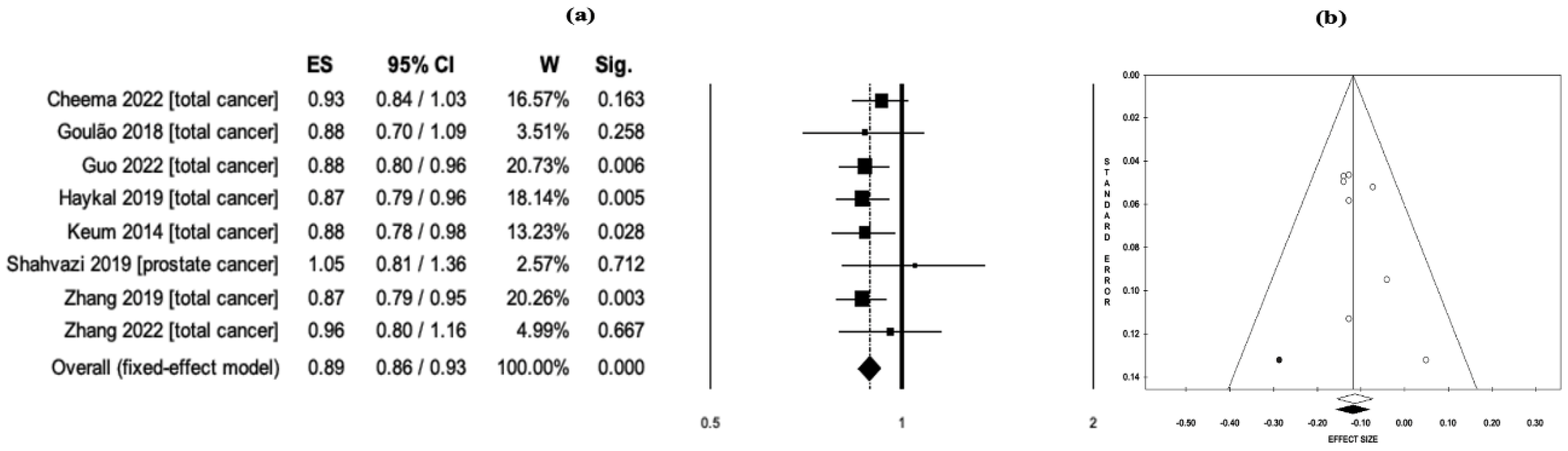
In a pooled analysis of a total of eight meta-analyses evaluating Vit-D intake and cancer-related mortality, higher Vit-D intake was associated with lower mortality (RR = 0.89, 95% CI: 0.86–0.93, p < 0.001) (Figure 3a). No significant heterogeneity was detected among the studies included in the analysis (Q = 3.45, df = 7, I2 = 0.0%, p = 0.840). Therefore, the meta-meta-analysis was carried out using the fixed effects model. The evaluation of the funnel plot did not reveal any evidence of publication bias among the included studies (Figure 3b). The robustness of the results was confirmed by the sensitivity analysis.
Figure 3.
(a) Pooled effect size (ES) associated with vitamin D intake (low and high intake) and cancer-related mortality, and (b) funnel plot. No publication bias was detected among studies in the schematic evaluation of the funnel plot.
Figure 3.
(a) Pooled effect size (ES) associated with vitamin D intake (low and high intake) and cancer-related mortality, and (b) funnel plot. No publication bias was detected among studies in the schematic evaluation of the funnel plot.
3.5. Serum 25-hidroxyvitamin-D Levels and Cancer Risk/Mortality
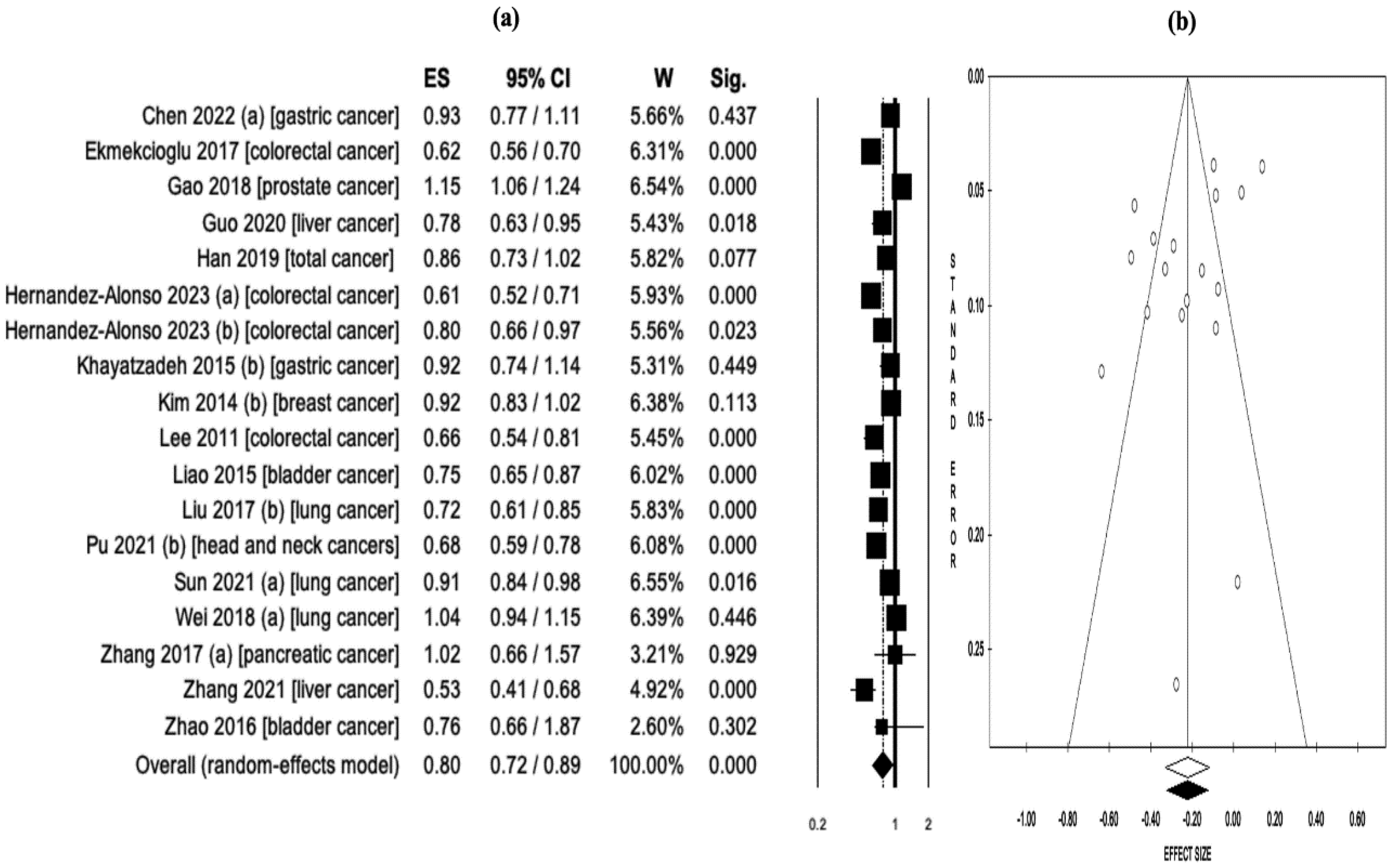
A pooled analysis of a total of 18 reports assessing serum 25(OH)D levels and cancer risk found that higher serum 25(OH)D levels were associated with lower cancer risk (OR = 0.80, 95% CI: 0.72–0.89, p < 0.001) (Figure 4a). There was significant heterogeneity among studies (Q = 164.3, df = 17, I2 = 89.6%, p < 0.001). Therefore, analyses were performed using a random effects model. There was no publication bias in the study reports according to the results of Begg and Mazumdar’s rank correlation test (z = -0.87, p = 0.384) (Figure 4b). Sensitivity analyses were performed by excluding each study from the analysis (excluded separately). The sensitivity analysis conducted in this synthesis confirmed the stability and reliability of the test results (Figure S2).
Figure 4.
(a) Pooled effect size (ES) associated with serum 25(OH)D levels (low and high levels) and cancer risk, and (b) funnel plot. There was no publication bias in the study reports according to the results of Begg and Mazumdar’s rank correlation test (z = -0.87, p = 0.384).
Figure 4.
(a) Pooled effect size (ES) associated with serum 25(OH)D levels (low and high levels) and cancer risk, and (b) funnel plot. There was no publication bias in the study reports according to the results of Begg and Mazumdar’s rank correlation test (z = -0.87, p = 0.384).
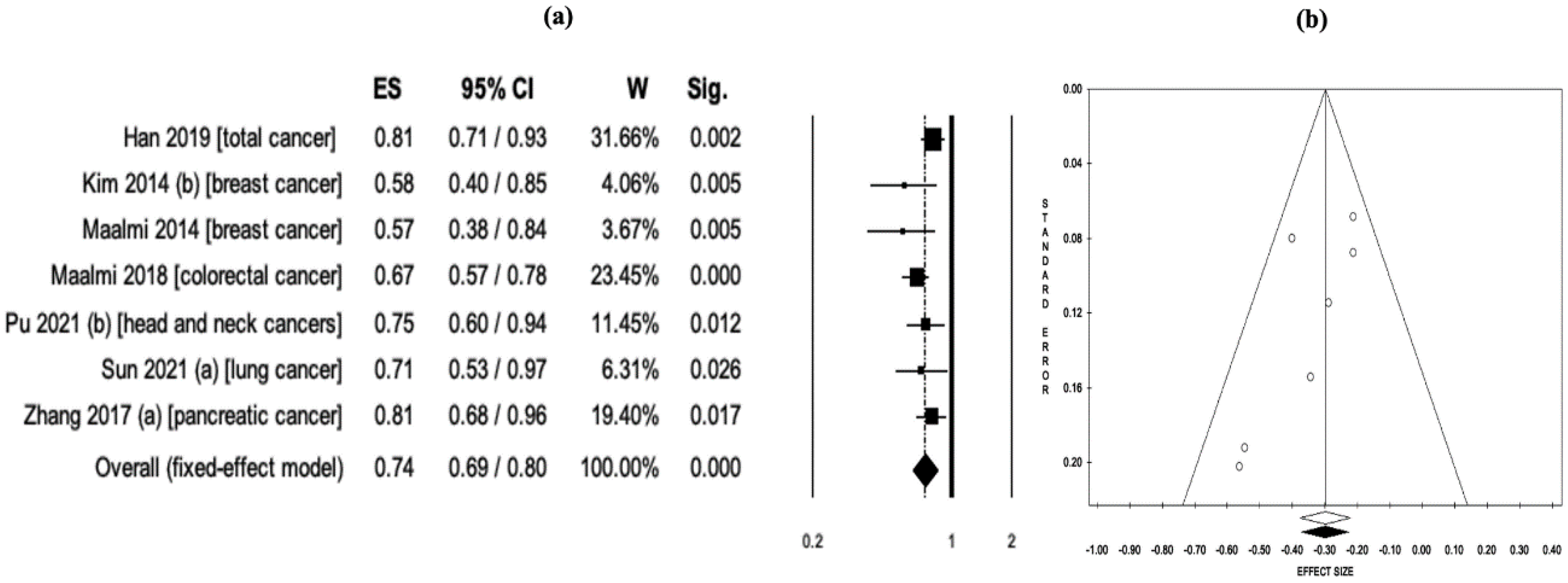
In a pooled analysis of a total of eight meta-analyses evaluating serum 25(OH)D and cancer-related mortality, higher serum 25(OH)D levels were associated with 33% lower mortality (RR = 0.67, 95% CI: 0.58–0.78, p < 0.001). However, among the studies included in the analysis, a meta-analysis [23] reported a very low risk, thus creating a negative outlier in the analyses. The results of Egger’s linear regression asymmetry test (intercept = -3.09, t = -2.33, p = 0.059) and Begg and Mazumdar’s rank correlation test (z = -2.23, p = 0.026) suggested that there may be publication bias in study reports. Therefore, this study [23] was excluded from the analysis. In a re-pooled analysis of a total of seven studies, higher serum 25(OH)D levels were associated with 26% lower mortality (RR = 0.74, 95% CI: 0.69-0.80, p < 0.001) (Figure 5a). No significant heterogeneity was detected between studies (Q = 7.67, df = 6, I2 = 21.7%, p = 0.263), and the meta-meta-analysis was carried out using the fixed effects model. There was no publication bias in the study reports according to the results of Egger’s linear regression asymmetry test (intercept = -1.95, t = -2.01, p = 0.101) and Begg and Mazumdar’s rank correlation test (z = -1.65, p = 0.099) (Figure 5b). Sensitivity analyses also confirmed the robustness of the results.
Figure 5.
(a) Pooled effect size (ES) associated with serum 25(OH)D levels (low and high levels) and cancer-related mortality, and (b) funnel plot. There was no publication bias in the study reports according to the results of Egger’s linear regression asymmetry test (intercept = -1.95, t = -2.01, p = 0.101) and Begg and Mazumdar’s rank correlation test (z = -1.65, p = 0.099).
Figure 5.
(a) Pooled effect size (ES) associated with serum 25(OH)D levels (low and high levels) and cancer-related mortality, and (b) funnel plot. There was no publication bias in the study reports according to the results of Egger’s linear regression asymmetry test (intercept = -1.95, t = -2.01, p = 0.101) and Begg and Mazumdar’s rank correlation test (z = -1.65, p = 0.099).
3.6. Subgroup Analysis
In order to measure the sensitivity of the analyses and the robustness of the results, subgroup analyses were carried out in terms of Vit-D intake (low and high intake) and serum 25(OH)D levels (low and high levels).
In the secondary meta-meta-analyses, subgroup analyses were performed according to study types (RCTs and observational) and cancer types. Meta-meta-analyses were conducted if there were at least three studies for different cancer types in the subgroup analyses. Accordingly, in the pooled analysis of studies evaluating Vit-D intake and total cancer risk, it was observed that Vit-D intake did not cause a remarkable change in cancer risk (OR = 0.99, 95% CI: 0.97-1.01, p = 0.300) (Table 2). In subgroup analyses of colorectal and lung cancer, Vit-D intake was associated with a significant reduction in cancer risk (OR = 0.89, 95% CI: 0.83-0.96, p = 0.002; OR = 0.88, 95% CI: 0.83-0.94, p < 0.001, respectively). The relationship between Vit-D intake and cancer mortality was evaluated with data from a total of seven reports. Accordingly, it was concluded that Vit-D intake was associated with a significant reduction in total cancer mortality (RR = 0.89, 95% CI: 0.85-0.93, p < 0.001).
A meta-meta-analysis was conducted in two types of cancer associated with serum 25(OH)D levels. As seen in Table 2, serum 25(OH)D levels were associated with a non-significant reduction in the incidence of lung cancer (OR = 0.89, 95% CI: 0.75-1.05, p = 0.178). In colorectal cancer, the analysis results strongly suggested that higher serum 25(OH)D levels were associated with a lower risk of colorectal cancer (OR = 0.65, 95% CI: 0.60-0.70, p < 0.001) (Table 2).
Meta-analyses whose primary reports included only RCTs were also pooled in subgroup analyses. Accordingly, there was no significant association between Vit-D intake and cancer incidence (OR = 0.99, 95% CI: 0.97-1.01, p = 0.320). However, Vit-D intake was associated with 11% reduced cancer-related mortality (RR = 0.89, 95% CI: 0.85-0.93, p < 0.001) (Table 2).
Table 2.
Subgroup analyses of vitamin D-related studies included in the meta-meta-analysis.
| Analysis | Model | Number of reports (n) | Effect size (ES) [OR or RR] | 95% CI | p value | I2 | p value | Intercept | Tau (t) | p value |
| Vitamin D intake and cancer risk* | ||||||||||
| Total cancer | Fixed | 7 | 0.99** | 0.97-1.01 | 0.300 | 0.00 | 0.983 | 0.37 | 0.72 | 0.506 |
| Colorectal cancer | Random | 6 | 0.89** | 0.83-0.96 | 0.002 | 79.4 | < 0.001 | -2.11 | -1.70 | 0.164 |
| Lung cancer | Fixed | 3 | 0.88** | 0.83-0.94 | < 0.001 | 0.00 | 0.817 | -0.72 | -0.59 | 0.658 |
| RCTs*** | Fixed | 8 | 0.99** | 0.97-1.01 | 0.320 | 0.00 | 0.988 | 0.49 | 1.35 | 0.227 |
| Observational | Random | 14 | 0.90** | 0.86-0.95 | < 0.001 | 68.43 | < 0.001 | -1.09 | -1.51 | 0.156 |
| Serum 25 (OH)D levels ve and cancer risk* | ||||||||||
| Colorectal cancer | Fixed | 4 | 0.65** | 0.60-0.70 | < 0.001 | 48.4 | 0.121 | 3.23 | 1.21 | 0.351 |
| Lung cancer | Random | 3 | 0.89** | 0.75-1.05 | 0.178 | 85.84 | 0.001 | -4.32 | -0.68 | 0.619 |
| Vitamin D intake and cancer related mortality* | ||||||||||
| Total cancer | Fixed | 7 | 0.89**** | 0.85-0.93 | < 0.001 | 0.00 | 0.929 | 0.77 | 0.98 | 0.372 |
| RCTs*** | Fixed | 7 | 0.89**** | 0.85-0.93 | < 0.001 | 0.00 | 0.929 | 0.77 | 0.98 | 0.372 |
ES effect size, OR odds ratio, RR odds ratio, CI confidence interval, RCTs randomized controlled trials, N/R not reported, N/A not available or missing data, * Meta-meta-analysis was not conducted for types of cancer with fewer than three reports ** OR, *** studies containing only RCTs were included, studies with a combination of other study types and RCTs were excluded, **** RR.
3.7. Mapping
A visual map was created for systematic reviews to visually display the study information via a bubble chart. Review information was evaluated in three dimensions. Bubble size varies in direct proportion to the sample size included in the study. The publication years of the meta-analyses are included in the effect (x) axis. The y-axis indicates the number of primary studies that were selected and included in the related meta-analyses. Studies with relatively large samples, studies with medium samples, and studies with relatively small samples are colored separately. The bubble chart associated with the mapping of the meta-analysis of 32 studies from 35 studies on Vit-D is presented in Figure S3. Three studies [36,40,44] were not included in the visual map because the sample size was not clearly reported.
4. Discussion
It is established that Vit-D deficiency and inadequate serum 25(OH)D levels are important risk factors for many cancers [8,12,13,14]. Many epidemiological studies have shown an inverse association between Vit-D levels and many types of cancer, including breast, prostate, colon, and lung cancer [15,16,17]. Our analysis suggests that there may be strong associations between Vit-D intake, serum 25(OH)D levels, and cancer risk, especially cancer-related mortality. Although most of the studies identified in our meta-meta-analysis (27 of 35 studies) included observational (cohort and/or case-control) studies, a combined evaluation of multiple meta-analyses yielded strong evidence. We supported the results with subgroup analyses in order to examine the differences in terms of study types.
The most recent meta-analyses [14,19,20,21,36,48,58] included in our study were documented in the literature in 2022 and 2023. Three of these studies included meta-analyses of RCTs [19,20,58], and primary reports of other studies included observational epidemiological studies [14,21,36,48]. Meta-analyses of RCTs in these most recent studies reported no notable variation between Vit-D intake and total cancer risk (RR = 0.99, 95% CI: 0.94-1.04, p > 0.05; RR = 0.98, 95% CI: 0.94-1.02, p > 0.05; RR = 0.99, 95% CI: 0.93-1.06, p > 0.05) [19,20,57]. In observational studies, however, two meta-analysis conducted by Hernandez-Alonso et al. [14] and Lopez-Caleya et al. [48] revealed an inverse relationship between serum 25(OH)D levels or Vit-D intake and the risk of colorectal cancer (OR = 0.61, 95% CI: 0.52–0.71, p < 0.05; OR = 0.96, 95% CI: 0.93–0.98, p < 0.05). Boughhanem et al. [21], on the other hand, reported that Vit-D intake was associated with a lower risk of cancer in case-control studies (OR = 0.75, 95% CI: 0.67–0.85, p < 0.05), while this association was not confirmed in prospective cohort studies (OR = 0.94, 95% CI: 0.79–1.11, p > 0.05). Similar to these current meta-meta-analyses, we found no significant difference between Vit-D intake and total cancer risk in pooled analyzes of RCTs in our study (OR = 0.99, 95% CI: 0.97–1.01, p = 0.320). However, in a pooled analysis of observational studies, intake of Vit-D was associated with a 10% lower risk of cancer (OR = 0.90, 95% CI: 0.86–0.95, p < 0.001).
The results of current primary studies and meta-analyses regarding serum 25(OH)D levels and Vit-D intake have revealed conflicting reports. In particular, meta-analyses focusing on RCTs have reported no remarkable evidence of a significant association between Vit-D intake and cancer. For example, in a meta-analysis of RCTs by Goulão et al. [18] that involved 18,808 participants, it was reported that there was no evidence that Vit-D intake alone reduced cancer incidence or cancer deaths, even after long-term follow-up results were included (RR = 1.03, 95% CI: 0.91–1.15, p > 0.05). Similarly, two recent (2022) meta-analyses that evaluating Vit-D intake and cancer risk suggested that Vit-D intake did not reduce the overall cancer incidence (RR = 0.99, 95% CI: 0.94–1.04, p > 0.05; RR = 0.98, 95% CI: 0.94–1.02, p > 0.05) [19,20]. Contrary to these results, a meta-analysis carried out by Han et al. [38] in 2019 that included prospective cohort studies provided evidence that higher serum 25(OH)D concentrations are marginally associated with lower cancer incidence and mortality (RR = 0.86, 95% CI: 0.73–1.02, p < 0.05; RR = 0.81, 95% CI: 0.71–0.93, p < 0.05, respectively). Similarly, in many meta-analyses that included observational epidemiological studies, high Vit-D intake or high serum 25(OH)D levels have been associated with a reduced risk of several types of cancer, such as colorectal [12,14,21], liver [13], ovarian [22], and lung cancer [23,24]. Similar results were emphasized in the literature in meta-analyses of RCTs evaluating Vit-D intake and cancer risk. While these studies revealed that there was no significant reduction in cancer risk with Vit-D intake, it was reported that Vit-D intake was associated with a significant decrease in cancer-related mortality [18,19,20,39,41,55,58,60]. Meta-analyses of observational epidemiological studies provided evidence of an inverse relationship between Vit-D and cancer risk [12,14,21,45,46,48]. Similar to the literature, in this study, we also concluded that higher Vit-D intake was associated with lower cancer risk in a pooled analysis of a total of 25 reports evaluating Vit-D intake and cancer risk (OR = 0.93, 95% CI: 0.90–0.96, p < 0.001). However, when only meta-analyses of RCTs were included in the pooled analysis, there was no significant association between Vit-D intake and cancer incidence. The majority of the studies included in our research (77.1%) were also observational studies. Therefore, based on these findings, it can be inferred that these results can be attributed to the data gathered from observational studies included in this research.
Another critical issue to address and discuss is the investigation of the reasons behind the discrepancies in findings observed between RCTs and observational studies. One considerable reason for the differences is that the primary endpoint in most of the primary studies included in the meta-analyses of RCTs did not focus on cancer incidence or cancer-related death. Furthermore, another contributing factor to the discrepancies between RCTs and observational studies may be that the participants included in the RCTs were not specifically selected from groups known to have a higher risk of Vit-D deficiency. Hence, due to the absence of participants specifically at higher risk for Vit-D deficiency in the RCTs, a notable effect of Vit-D intake may not have been observed in this group. Additionally, the differences in the specific dosing protocols employed in RCTs versus observational studies contribute to the differences between the findings of these two types of studies. Furthermore, another significant factor is that the majority of RCTs did not measure serum 25(OH)D levels at the conclusion of the study to evaluate the actual impact of Vit-D. Therefore, it is crucial to thoroughly consider and take into account these confounding factors when interpreting and comparing the results between RCTs and observational studies.
In a pooled analysis of a total of 18 reports evaluating serum 25(OH)D level and cancer risk, we observed that higher 25(OH)D levels were associated with lower cancer risk (OR = 0.80, 95% CI: 0.72–0.89, p < 0.001). This result also suggested that serum 25(OH)D levels are a better indicator for cancer risk. A total of seven meta-analyses assessing serum 25(OH)D levels and cancer-related mortality were pooled and analyzed. Accordingly, the results of the analysis revealed that higher serum 25(OH)D levels were associated with 26% lower mortality (RR = 0.74, 95% CI: 0.69–0.80, p < 0.001). Similarly, in a pooled analysis of a total of eight meta-analyses evaluating Vit-D intake and cancer-related mortality, higher Vit-D intake was associated with 11% lower mortality (RR = 0.89, 95% CI: 0.86–0.93, p < 0.001). These results also confirmed that serum 25(OH)D levels are a better indicator for cancer-related mortality.
In subgroup analyses, it was found that Vit-D intake did not significantly reduce or increase total cancer risk (OR = 0.99, 95% CI: 0.97–1.01, p = 0.300), whereas Vit-D intake was associated with a significant decrease in cancer risk in colorectal and lung cancer (OR = 0.89, 95% CI: 0.83–0.96, p = 0.002; OR = 0.88, 95% CI: 0.83–0.94, p < 0.001, respectively). Our results are compatible with the literature [14,18,19,21,23,40] and provided a high level of evidence. Although a meta-meta-analysis of RCTs showed that Vit-D intake was not associated with a reduction in cancer risk, the results of this study suggest that Vit-D intake and high serum 25(OH)D levels can significantly reduce the incidence and mortality of various cancers. Vit-D intake and high serum 25(OH)D levels may be associated with cancer risk and survival.
It is widely recognized that public health policies are formulated based on the evaluation of systematic reviews and meta-analyses, which are considered to provide the highest level of evidence. The present meta-meta-analysis has remarkably raised the level of evidence by incorporating numerous systematic reviews (with meta-analysis) and reassessing analyses with increased power. It also simplified the researcher’s task of evaluating these studies together, as it gathered the meta-analyses examining Vit-D intake, serum 25(OH)D levels, and cancer risk/mortality under one umbrella. Although this paper provided valuable evidence, it had several limitations that are worth considering. One limitation of this paper is the possibility of variations in patient selection and treatment protocols across the primary studies included in the meta-analyses. This could lead to heterogeneity across the studies, potentially affecting the overall conclusions. Another limitation of this investigation is the lack of an evaluation of the impact of the treatments received by cancer patients. The effect of treatments, such as chemotherapy and radiation therapy, on the relationship between Vit-D intake and cancer mortality, was not taken into account. Furthermore, the primary reports included in the meta-analyses within this study selected patients from various countries and geographical regions, which could lead to variations in Vit-D status and cancer incidence/mortality rates due to differences in diet, lifestyle, and other factors. This could impact the generalizability of the study’s conclusions to different populations.
5. Conclusions
In conclusion, in this synthesis of systematic reviews and meta-analyses with the meta-meta-analysis method, it was clearly revealed that Vit-D intake and serum 25(OH)D levels are associated with cancer incidence and mortality. Taken together, both Vit-D intake and higher 25(OH)D levels may provide significant benefits in terms of cancer incidence and mortality, but careful evaluation on the basis of cancer types is recommended. Furthermore, it is crucial to implement accurate confounding controls in future research, particularly RCTs. Future research should place emphasis on enhancing study designs, incorporating larger sample sizes, implementing more precise confounding controls, and exploring the potential dose-response relationship between Vit-D intake and oncology outcomes. Continual evaluation of the evidence is critical to assess the changing epidemiological landscape in studies of Vit-D and cancer, as well as to provide a solid basis for medical guidelines and clinical decision-making. The findings of this study may provide a solid basis for individual decision-making regarding Vit-D in the context of cancer.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org.
Author Contributions
MEA: Conceptualization, Methodology, Software, Data-Analysis, Writing-Original draft preparation, Writing-Reviewing and Editing, Critical Review. YB: Visualization, Investigation, Validation, Writing-Original draft preparation, Critical Review. HE: Conceptualization, Methodology, Software, Writing-Original draft preparation, Writing-Reviewing and Editing, Critical Review. The final manuscript was reviewed and approved by all authors.
Funding
Mehmet Emin Arayici is supported by the 100/2000 YOK (Council of Higher Education) PhD Scholarship and The Scientific and Technological Research Council of Turkey (TUBITAK) 2211/A National PhD Scholarship Program. It is important to note that the funders did not have any involvement in the study design, data collection, and analysis, decision to publish, or preparation of the manuscript.
Data availability statement
To obtain the datasets, interested parties should contact the corresponding author (MEA) directly and submit a reasonable request for access to the data. The corresponding author (MEA) will provide further information and guidance on accessing the datasets.
Conflicts of Interest statement
All authors of this study declare that they have no conflicts of interest to disclose. They have no financial, personal, or professional relationships that could potentially influence or bias the research findings presented in the study. The authors have provided this declaration to ensure transparency and maintain the integrity of the research.
Ethics approval statement
Ethical approval was not required for this study.
Abbreviations
GLOBOCAN: Global Cancer Observatory; WHO: World Health Organization; QoL: Quality of life; Vit-D: Vitamin-D; 25(OH)D: 25-hydroxyvitamin-D; MeSH: Medical Subject Headings; WoS: Web of Science; RR: Risk ratio; OR: Odds ratio; HR: Hazard ratio.
References
- Matthews HK, Bertoli C, de Bruin RAM. Cell cycle control in cancer. Nat Rev Mol Cell Biol. 2022;23:74–88. https://doi.org/10.1038/s41580-021-00404-3. [CrossRef]
- Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, Jemal A ve ark. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021;71:209-249. https://doi.org/10.3322/caac.21660. [CrossRef]
- Siegel RL, Miller KD, Fuchs HE, Jemal A. Cancer Statistics, 2021. CA Cancer J Clin. 2021;71(1):7-33. https://doi.org/10.3322/caac.21654. [CrossRef]
- Arayici ME, Basbinar Y, Ellidokuz H. The impact of cancer on the severity of disease in patients affected with COVID-19: an umbrella review and meta-meta-analysis of systematic reviews and meta-analyses involving 1,064,476 participants. Clin Exp Med. 2022:1-9. https://doi.org/10.1007/s10238-022-00911-3. [CrossRef]
- World Health Organization (WHO). Global Health Estimates 2020: Deaths by Cause, Age, Sex, by Country and by Region, 2000-2019. WHO; 2020. Accessed March 11, 2023. who.int/data/gho/data/themes/mortality-and-global-health-estimates/ghe-leading-causes-of-death.
- Gil Á, Plaza-Diaz J, Mesa MD. Vitamin D: Classic and Novel Actions. Ann Nutr Metab. 2018;72(2):87-95. https://doi.org/10.1159/000486536. [CrossRef]
- Raiten DJ, Picciano MF. Vitamin D and health in the 21st century: bone and beyond. Executive summary. Am J Clin Nutr. 2004;80(6Suppl):1673S-7S. https://doi.org/10.1093/ajcn/80.6.1673S. [CrossRef]
- Muñoz A, Grant WB. Vitamin D and Cancer: An Historical Overview of the Epidemiology and Mechanisms. Nutrients. 2022;14(7):1448. https://doi.org/10.3390/nu14071448. [CrossRef]
- Jeon SM, Shin E. Exploring vitamin D metabolism and function in cancer. Exp Mol Med. 2019;50:1-14. https://doi.org/10.1038/s12276-018-0038-9. [CrossRef]
- Li M, Chen P, Li J, Chu R, Xie D, Wang H. Review: the impacts of circulating 25-hydroxyvitamin D levels on cancer patient outcomes: a systematic review and meta-analysis. J Clin Endocrinol Metab. 2014;99(7):2327-36. https://doi.org/10.1210/jc.2013-4320. [CrossRef]
- Ordóñez Mena JM, Brenner H. Vitamin D and cancer: an overview on epidemiological studies. Adv Exp Med Biol. 2014;810:17-32.
- Ekmekcioglu C, Haluza D, Kundi M. 25-Hydroxyvitamin D Status and Risk for Colorectal Cancer and Type 2 Diabetes Mellitus: A Systematic Review and Meta-Analysis of Epidemiological Studies. Int J Environ Res Public Health. 2017;14(2):127. https://doi.org/10.3390/ijerph14020127. [CrossRef]
- Guo XF, Zhao T, Han JM, Li S, Li D. Vitamin D and liver cancer risk: A meta-analysis of prospective studies. Asia Pac J Clin Nutr. 2020;29(1):175-182. https://doi.org/10.6133/apjcn.202003_29(1).0023. [CrossRef]
- Hernández-Alonso P, Boughanem H, Canudas S, Becerra-Tomás N, Fernández de la Puente M, Babio N, et al. Circulating vitamin D levels and colorectal cancer risk: A meta-analysis and systematic review of case-control and prospective cohort studies. Crit Rev Food Sci Nutr. 2023;63(1):1-17. https://doi.org/10.1080/10408398.2021.1939649. [CrossRef]
- Chowdhury R, Kunutsor S, Vitezova A, Oliver-Williams C, Chowdhury S, Kiefte-de-Jong JC, et al. Vitamin D and risk of cause specific death: systematic review and meta-analysis of observational cohort and randomised intervention studies. BMJ. 2014;348:g1903. https://doi.org/10.1136/bmj.g1903. [CrossRef]
- Feldman D, Krishnan AV, Swami S, Giovannucci E, Feldman BJ. The role of vitamin D in reducing cancer risk and progression. Nat Rev Cancer. 2014;14(5):342-57. https://doi.org/10.1038/nrc3691. [CrossRef]
- Giovannucci E. The epidemiology of vitamin D and cancer incidence and mortality: a review (United States). Cancer Causes Control. 2005;16(2):83-95. https://doi.org/10.1007/s10552-004-1661-4. [CrossRef]
- Goulão B, Stewart F, Ford JA, MacLennan G, Avenell A. Cancer and vitamin D supplementation: a systematic review and meta-analysis. Am J Clin Nutr. 2018;107(4):652-663. https://doi.org/doi:10.1093/ajcn/nqx047. [CrossRef]
- Cheema HA, Fatima M, Shahid A, Bouaddi O, Elgenidy A, Rehman AU, et al. Vitamin D supplementation for the prevention of total cancer incidence and mortality: An updated systematic review and meta-analysis. Heliyon. 2022;8(11):e11290. https://doi.org/10.1016/j.heliyon.2022.e11290. [CrossRef]
- Guo Z, Huang M, Fan D, Hong Y, Zhao M, Ding R, et al. Association between vitamin D supplementation and cancer incidence and mortality: A trial sequential meta-analysis of randomized controlled trials. Crit Rev Food Sci Nutr. 2022:1-15. https://doi.org/10.1080/10408398.2022.2056574. [CrossRef]
- Boughanem H, Canudas S, Hernandez-Alonso P, Becerra-Tomás N, Babio N, Salas-Salvadó J, et al. Vitamin D Intake and the Risk of Colorectal Cancer: An Updated Meta-Analysis and Systematic Review of Case-Control and Prospective Cohort Studies. Cancers (Basel). 2021;13(11):2814. https://doi.org/10.3390/cancers13112814. [CrossRef]
- Liao MQ, Gao XP, Yu XX, Zeng YF, Li SN, Naicker N, et al. Effects of dairy products, calcium and vitamin D on ovarian cancer risk: a meta-analysis of twenty-nine epidemiological studies. Br J Nutr. 2020;124(10):1001-1012. https://doi.org/10.1017/S0007114520001075. [CrossRef]
- Liu J, Dong Y, Lu C, Wang Y, Peng L, Jiang M, et al. Meta-analysis of the correlation between vitamin D and lung cancer risk and outcomes. Oncotarget. 2017;8(46):81040-81051. https://doi.org/10.18632/oncotarget.18766. [CrossRef]
- Sun K, Zuo M, Zhang Q, Wang K, Huang D, Zhang H. Anti-Tumor Effect of Vitamin D Combined with Calcium on Lung Cancer: A Systematic Review and Meta-Analysis. Nutr Cancer. 2021;73(11-12):2633-2642. https://doi.org/10.1080/01635581.2020.1850812. [CrossRef]
- Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71. https://doi.org10.1136/bmj.n71.
- Brooke BS, Schwartz TA, Pawlik TM. MOOSE Reporting Guidelines for Meta-analyses of Observational Studies. JAMA Surg. 2021;156(8):787-788. https://doi.org/10.1001/jamasurg.2021.0522. [CrossRef]
- Furlan AD, Pennick V, Bombardier C, van Tulder M; Editorial Board, Cochrane Back Review Group. 2009 updated method guidelines for systematic reviews in the Cochrane Back Review Group. Spine (Phila Pa 1976). 2009;34(18):1929-41. https://doi.org/10.1097/BRS.0b013e3181b1c99f. [CrossRef]
- Shea BJ, Reeves BC, Wells G, Thuku M, Hamel C, Moran J, et al. AMSTAR 2: a critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ. 2017;358:j4008. https://doi.org/10.1136/bmj.j4008. [CrossRef]
- Whiting P, Savović J, Higgins JP, Caldwell DM, Reeves BC, Shea B, et al. ROBIS: A new tool to assess risk of bias in systematic reviews was developed. J Clin Epidemiol. 2016;69:225-34. https://doi.org/10.1016/j.jclinepi.2015.06.005. [CrossRef]
- Egger M, Davey Smith G, Schneider M, Minder C. Bias in meta-analysis detected by a simple, graphical test. BMJ. 1997;315(7109):629-34. https://doi.org/10.1136/bmj.315.7109.629. [CrossRef]
- Begg CB, Mazumdar M. Operating characteristics of a rank correlation test for publication bias. Biometrics. 1994;50(4):1088-101.
- Duval S, Tweedie R. A nonparametric “Trim and Fill” method of accounting for Publication Bias in Meta-Analysis. J Am Stat Assoc. 2000;95:89–98.
- Higgins JPT, Thomas J, Chandler J, Cumpston M, Li T, Page MJ, Welch VA, Cochrane Collaboration, 2008. Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 [M]. Wiley-Blackwell.
- ProMeta-3 professional statistical software for conducting meta-analysis. It is based on ProMeta 2.1 deployed by Internovi in 2015. https://idostatistics.com/prometa3/.
- Balduzzi S, Rücker G, Schwarzer G. How to perform a meta-analysis with R: a practical tutorial. In Evidence-Based Mental Health. 2019;22:153-160.
- Chen X, Li L, Liang Y, Huang T, Zhang H, Fan S, Sun W, Wang Y. Relationship of vitamin D intake, serum 25(OH) D, and solar ultraviolet-B radiation with the risk of gastric cancer: A meta-analysis. J Cancer Res Ther. 2022;18(5):1417-1424. https://doi.org/10.4103/jcrt.jcrt_527_21. [CrossRef]
- Gao J, Wei W, Wang G, Zhou H, Fu Y, Liu N. Circulating vitamin D concentration and risk of prostate cancer: A dose-response meta-analysis of prospective studies. Ther Clin Risk Manag. 2018;14:95-104. https://doi.org/10.2147/TCRM.S149325. [CrossRef]
- Han J, Guo X, Yu X, Liu S, Cui X, Zhang B, et al. 25-Hydroxyvitamin D and Total Cancer Incidence and Mortality: A meta-analysis of prospective cohort studies. Nutrients. 2019;11(10):1-17. https://doi.org/10.3390/nu11102295. [CrossRef]
- Haykal T, Samji V, Zayed Y, Gakhal I, Dhillon H, Kheiri B, et al. The role of vitamin D supplementation for primary prevention of cancer: meta-analysis of randomized controlled trials. J Community Hosp Intern Med Perspect. 2019;9(6):480-488. https:///doi.org/10.1080/20009666.2019.1701839. [CrossRef]
- Huncharek M, Muscat J, Kupelnick B. Colorectal cancer risk and dietary intake of calcium, vitamin D, and dairy products: A meta-analysis of 26,335 cases from 60 observational studies. Nutr Cancer. 2009;61(1):47-69. https://doi.org/10.1080/01635580802395733. [CrossRef]
- Keum N, Giovannucci E. Vitamin D supplements and cancer incidence and mortality: A meta-analysis. Br J Cancer. 2014;111(5):976-80. https://doi.org/10.1038/bjc.2014.294. [CrossRef]
- Khayatzadeh S, Feizi A, Saneei P, Esmaillzadeh A. Vitamin D intake, serum Vitamin D levels, and risk of gastric cancer: A systematic review and meta-analysis. J Res Med Sci. 2015;20(8):790-6. https://doi.org/10.4103/1735-1995.168404. [CrossRef]
- Kim Y, Je Y. Vitamin D intake, blood 25(OH)D levels, and breast cancer risk or mortality: A meta-analysis. Br J Cancer. 2014;110(11):2772-84. https://doi.org/10.1038/bjc.2014.175. [CrossRef]
- Lee JE, Li H, Chan AT, Hollis BW, Lee IM, Stampfer MJ, et al. Circulating levels of vitamin D and colon and rectal cancer: the Physicians’ Health Study and a meta-analysis of prospective studies. Cancer Prev Res (Phila). 2011;4(5):735-43. https://doi.org10.1158/1940-6207.CAPR-10-0289.
- Liao Y, Huang JL, Qiu MX, Ma ZW. Impact of serum vitamin D level on risk of bladder cancer: a systemic review and meta-analysis. Tumour Biol. 2015;36(3):1567-72. https://doi.org/10.1007/s13277-014-2728-9. [CrossRef]
- Liu Y, Yu Q, Zhu Z, Zhang J, Chen M, Tang P, et al. Vitamin and multiple-vitamin supplement intake and incidence of colorectal cancer: a meta-analysis of cohort studies. Med Oncol. 2015;32(1):1-10. https://doi.org/10.1007/s12032-014-0434-5. [CrossRef]
- Liu Y, Wang X, Sun X, Lu S, Liu S. Vitamin intake and pancreatic cancer risk reduction: A meta-analysis of observational studies. Medicine (Baltimore). 2018;97(13):e0114. https://doi.org/10.1097/MD.0000000000010114. [CrossRef]
- Lopez-Caleya JF, Ortega-Valín L, Fernández-Villa T, Delgado-Rodríguez M, Martín-Sánchez V, Molina AJ. The role of calcium and vitamin D dietary intake on risk of colorectal cancer: systematic review and meta-analysis of case-control studies. Cancer Causes Control. 2022;33(2):167-182. https://doi.org/10.1007/s10552-021-01512-3. [CrossRef]
- Maalmi H, Ordóñez-Mena JM, Schöttker B, Brenner H. Serum 25-hydroxyvitamin D levels and survival in colorectal and breast cancer patients: Systematic review and meta-analysis of prospective cohort studies. Eur J Cancer. 2014;50(8):1510-21. https://doi.org/10.1016/j.ejca.2014.02.006. [CrossRef]
- Maalmi H, Walter V, Jansen L, Boakye D, Schöttker B, Hoffmeister M, et al. Association between blood 25-hydroxyvitamin D levels and survival in colorectal cancer patients: An updated systematic review and meta-analysis. Nutrients. 2018;10(7). https://doi.org/10.3390/nu10070896. [CrossRef]
- Pu Y, Zhu G, Xu Y, Zheng S, Tang B, Huang H, et al. Association Between Vitamin D Exposure and Head and Neck Cancer: A Systematic Review With Meta-Analysis. Front Immunol. 2021;12(February):1-11. https://doi.org/10.3389/fimmu.2021.627226. [CrossRef]
- Shahvazi S, Soltani S, Ahmadi SM, de Souza RJ, Salehi-Abargouei A. The Effect of Vitamin D Supplementation on Prostate Cancer: A Systematic Review and Meta-Analysis of Clinical Trials. Horm Metab Res. 2019;51(1):11-21. https://doi.org/10.1055/a-0774-8809. [CrossRef]
- Wei H, Jing H, Wei Q, Wei G, Heng Z. Associations of the risk of lung cancer with serum 25-hydroxyvitamin D level and dietary vitamin D intake: A dose-response PRISMA meta-analysis. Medicine (Baltimore). 2018;97(37):e12282. https://doi.org/10.1097/MD.0000000000012282. [CrossRef]
- Xu Y, Qian M, Hong J, Ng DM, Yang T, Xu L, Ye X. The effect of vitamin D on the occurrence and development of colorectal cancer: a systematic review and meta-analysis. Int J Colorectal Dis. 2021;36(7):1329-1344. https://doi.org/10.1007/s00384-021-03879-w. [CrossRef]
- Zhang X, Huang XZ, Chen WJ, Wu J, Chen Y, Wu CC, et al. Plasma 25-hydroxyvitamin D levels, vitamin D intake, and pancreatic cancer risk or mortality: A meta-analysis. Oncotarget. 2017;8(38):64395-406. https://doi.org/10.18632/oncotarget.18888. [CrossRef]
- Zhang X, Niu W. Meta-analysis of randomized controlled trials on vitamin D supplement and cancer incidence and mortality. Biosci Rep. 2019;39(11):BSR20190369. https://doi.org/10.1042/BSR20190369. [CrossRef]
- Zhang Y, Jiang X, Li X, Găman MA, Kord-Varkaneh H, Rahmani J, et al. Serum Vitamin D Levels and Risk of Liver Cancer: A Systematic Review and Dose-Response Meta-Analysis of Cohort Studies. Nutr Cancer. 2021;73(8):1-9. https://doi.org/10.1080/01635581.2020.1797127. [CrossRef]
- Zhang R, Zhang Y, Liu Z, Pei Y, Xu P, Chong W, et al. Association between Vitamin D Supplementation and Cancer Mortality: A Systematic Review and Meta-Analysis. Cancers (Basel). 2022;14(15):3717. https://doi.org/10.3390/cancers14153717. [CrossRef]
- Zhao Y, Chen C, Pan W, Gao M, He W, Mao R, et al. Comparative efficacy of vitamin D status in reducing the risk of bladder cancer: A systematic review and network meta-analysis. Nutrition. 2016;32(5):515-23. https://doi.org/10.1016/j.nut.2015.10.023. [CrossRef]
- Zhou L, Chen B, Sheng L, Turner A. The effect of vitamin D supplementation on the risk of breast cancer: a trial sequential meta-analysis. Breast Cancer Res Treat. 2020;182(1):1-8. https://doi.org/10.1007/s10549-020-05669-4. [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



