
Submitted:
08 May 2025
Posted:
09 May 2025
You are already at the latest version
Abstract
Background/Objectives: Orofacial clefts are congenital anomalies that cause substan-tial morbidity and mortality. This study was performed to evaluate the mortality of Brazilian individuals who had orofacial clefts reported on their death certificates. Methods: A retrospective cross-sectional study was conducted using data from the De-partment of Informatics of the Brazilian Unified Health System (DATASUS) from 1996 to 2023. Results: The mortality information system registered 987 deaths related to oro-facial clefts, with 880 patients under 1 year of age. There was a downward trend in an-nual mortality rates from 1996 to 2019, followed by an increase from 2020 to 2023. The main associated cause of death was respiratory and cardiovascular disorders. The mortality rate for infants under 1 year with orofacial clefts showed greater variation than did the mortality rate of children who died of other causes. The reduction in mor-tality rates from 1996 to 2019 occurred during the expansion and strengthening of DATASUS and its coordination with other levels of healthcare. The rise in mortality between 2020 and 2023 coincided with a reduction in surgical procedures due to the COVID-19 pandemic. Conclusion: This study revealed a decline in deaths from orofa-cial clefts in Brazil over several decades. These findings emphasize the importance of addressing preventable causes of death, including respiratory infections and malnutri-tion. High mortality within the first year of life—particularly among newborns under 28 days—highlights a critical shortage of pediatricians and its impact on care for indi-viduals with craniofacial anomalies.
Keywords:
Unified Health System
; Mortality
; Orofacial cleft
1. Introduction
Orofacial clefts are congenital anomalies that result from failures in the embryonic development of the face and/or palate. These include cleft lip and palate (CLP), cleft lip only (CLO), and cleft palate only (CPO) [1]. The estimated global prevalence of cleft lip and/or palate is 1 in 700 live births, while in Brazil, approximately 1 in 650 live births are affected by this malformation. The prevalence varies according to sex, ethnicity, and geographic region [2,3].
This anomaly has a multifactorial etiology that is influenced by genetic, epigenetic, and environmental factors, such as maternal exposure to smoking, alcohol consumption, and certain medications during pregnancy [4]. Studies have shown that the presence of orofacial clefts increases the risk of mortality compared with the general population [5,6,7,8].
The mortality rate among children with orofacial clefts is higher than that of children without clefts during the first 2 years of life, and the average life expectancy is significantly lower for children with clefts [9,10]. Factors associated with an increased risk of mortality in multivariable regression models include lower birth weight, the presence of other congenital or chromosomal anomalies, and a reduced number of prenatal consultations [9]. Additionally, orofacial clefts may be part of a broader spectrum of congenital anomalies or a syndrome associated with an elevated risk of mortality [10].
Surveillance of birth and mortality related to orofacial clefts is essential for healthcare planning [11]. In many cases, orofacial clefts are not lethal on their own, and with the expansion of CLP treatment centers, more individuals with these congenital defects are surviving into adulthood [6,8,12]. Furthermore, United Nations member states, including Brazil, are committed to achieving the Sustainable Development Goals, which include reducing neonatal and child mortality from preventable causes and non-communicable diseases through prevention and treatment—categories that include children with common congenital defects such as orofacial clefts [13]. The aim of this study was to evaluate mortality among Brazilian individuals with orofacial clefts as reported on death certificates (DCs), examining mortality trends, causes of death, geographic distribution, and the demographic profile of the patients.
2. Materials and Methods
A retrospective, population-based cross-sectional study was conducted using birth and mortality records from the Department of Informatics of the Brazilian Unified Health System (DATASUS) (https://datasus.saude.gov.br/informacoes-de-saude-tabnet/) [14]. Because of the evolution of data management processes and information technology resources, DATASUS has expanded the scope of information collected over the years. As a result, the availability of data used in this research has varied start dates.
The analysis was based on data with national geographical coverage, including regions and federative units of Brazil. For analyses requiring birth information, live birth declarations that recorded infants with orofacial clefts from 2010 to 2023 were used, along with general birth records from 1996 to 2023. Although the Live Birth Information System (SINASC) and the adoption of the Live Birth Certificate as the standard model for use throughout Brazil were implemented in 1990, it was only in 2000 that Brazil adopted a new version of the certificate, which included a field to record the presence or absence of “Congenital malformation and/or chromosomal anomaly.” In 2010, an updated version was introduced, expanding the section on congenital anomalies by adding a space to describe all congenital anomalies observed in the newborn. The study period was defined to begin in 2010, marking the implementation of this updated certificate, and to end in 2023, the most recent year with data free from inconsistencies such as duplications and coding errors at the time of collection. However, 1996 was also set as a starting point for the study because it marks the adoption of the International Classification of Diseases, Tenth Revision (ICD-10) in Brazil. Data from 2024 were excluded because the public database had not yet been finalized and remained subject to updates, including the removal of duplicates, correction of data entry errors, and resolution of data transfer failures. Mortality analyses were based on the underlying cause of death, as recorded on DCs for individuals of all age groups using ICD-10 codes Q35, Q36, and Q37 [15], which refer to CPO, CLO, and CLP, respectively, covering the period from 1996 to 2023.
To identify other causes contributing to the deaths of patients with orofacial clefts, records of multiple causes of death from 2006 to 2023 were also included. Multiple causes, also referred to as contributing causes, indicate other diagnoses related to the death. The DC is divided into Part I and Part II. Part I is further subdivided into lines (a, b, c, d), which must be filled out from bottom to top in a logical sequence, with the underlying cause of death recorded on line d and multiple causes on lines a, b, and c. In Part II of the DC, other contributing causes of death that were not part of the causal chain listed in Part I are recorded [16].
All causes recorded on lines a, b, and c of Part I, as well as those listed in Part II of the DC, were identified as multiple causes. Understanding the multiple causes of death in patients with orofacial clefts supports the implementation of preventive care, continuous monitoring, and personalized treatments, helping to reduce the risk of fatal complications and improve the quality of life for this population. Mortality records from DATASUS provided information on skin color, age group, location and region of death, sex, education level, and marital status of all individuals with orofacial clefts who died during the study period.
Information was organized by year. To calculate the infant mortality rate due to orofacial clefts per 1,000 live births, the total number of deaths of children under 1 year of age with orofacial clefts and the total number of live births from 2010 to 2023 were used. To calculate the overall mortality rate due to orofacial clefts, the total number of deaths among individuals with orofacial clefts and the total number of general deaths occurring in the same period (1996–2023) were considered. To analyze trends in mortality due to orofacial clefts, joinpoint regression analysis was applied using Joinpoint Regression Program software, Version 5.2.0 (National Cancer Institute, Bethesda, MD, USA). This model calculates the annual percentage change in the mortality rate. For this study, the dependent variable was the mortality rate due to orofacial clefts (per 1,000 inhabitants), and the independent variable was the year.
The study used secondary data available in the DATASUS database from the Ministry of Health. Because the data did not include subject identification, the study was exempt from ethics committee review.
3. Results
Between 1996 and 2023, the mortality information system of the SUS registered 987 deaths of individuals with orofacial clefts as the underlying cause. Of these, 419 were due to CPO, 355 to CLP, and 213 to CLO. Deaths were predominantly recorded in the southeast region (n = 333), followed by the northeast (n = 288), south (n = 170), north (n = 114), and midwest (n = 82). Figure 1 illustrates the distribution of deaths among patients with orofacial clefts over the 28 years analyzed. The mortality rate reached its highest value of 20.27 in 2012 and its lowest of 9.65 in 2019, demonstrating a significant downward trend. From 1996 to 2013, the annual percentage change in mortality was −4.77% (p = 0.000002; 95% confidence interval: −6.1 to −3.4). Between 2013 and 2017, the decline continued but at a slower pace, suggesting a stabilization in the mortality rate. Subsequently, from 2017 to 2020, a renewed decrease in mortality was observed. However, from 2020 to 2023, the trend reversed, with an increase in the mortality rate among individuals with orofacial clefts.
The profile of the deaths was characterized by infants under 1 year of age (n = 880 deaths), male sex (n = 533), and Caucasian individuals (n = 402). The majority of deaths occurred in a hospital setting (n = 809). Among deaths in infants under 1 year of age, 477 (48.3%) took place within the first 28 days of life (Table 1). Results regarding the type of orofacial clefts by sex indicated that for CLO (n = 130), CPO (n = 223), and CLP (n = 180), mortality was more prevalent in males.
Examining the distribution of deaths in infants under 1 year of age with orofacial clefts, it was observed that reported skin color varied by region of residence in Brazil, with a predominance of deaths among Caucasian infants in the southeast and multiracial infants in the northeast (Figure 2).
The causes of death among individuals with orofacial clefts varied widely, but data available for the 17-year period (2006–2023) showed that in addition to the 664 individuals whose orofacial clefts contributed to death, respiratory and cardiovascular disorders (n = 280) were the most common associated causes, particularly among infants under 1 year of age. Other causes of death reported on the DC included disorders related to gestational duration and growth; influenza and pneumonia; bacterial diseases; congenital malformations of the nervous system, eyes, ears, face, and heart; congenital skeletal malformations; and pulmonary diseases induced by external agents (Figure 3).
When calculating the mortality coefficient for infants under 1 year of age with orofacial clefts from 2010 to 2023 and comparing it with the mortality coefficient for children who died of other causes during the same period, the data in Figure 4 show that mortality among infants with orofacial clefts was higher. Although there was variability over the years studied, a downward trend was observed in the later years of the study. In the years with peaks in infant mortality due to orofacial clefts (2012, 2014, and 2021), the mortality coefficient for children who died of other causes did not show significant fluctuations and displayed a stable trend (Figure 4).
4. Discussion
The risk of mortality among individuals with orofacial clefts is higher in developing than developed countries because of socioeconomic disparities, limited access to healthcare, inadequate service infrastructure, and a higher prevalence of infectious diseases [8,17,18]. Mortality rates vary globally, with 20.3 deaths per 1,000 live births with oral clefts reported in the United States, 36/1,000 in England, 31.8/1,000 in the United Kingdom, and 12.2/1,000 in South Korea [7,11,19,20].
Geographic analysis of death records in the present study revealed regional disparities, with the southeast region exhibiting the highest number of deaths. This may be attributed to the region’s higher population density, which creates greater demand for healthcare services—potentially exposing systemic deficiencies—or to a more comprehensive recording of orofacial cleft-related deaths. Despite receiving the largest allocation of financial resources for orofacial cleft care (US$ 22,896,078.83 [60.3%]) [21], the southeast’s population growth underscores the need for ongoing investment reviews and expansions to ensure efficient resource management and strategic planning. Furthermore, the geographic concentration of orofacial cleft treatment centers near higher education institutions—predominantly located in the southeast—likely contributes to the observed population density. The mortality rates observed in other regions highlight the urgent need for public health policies tailored to the specific needs of each area [17], ensuring equitable access to care and addressing regional disparities in the management of orofacial clefts.
In this study, most deaths occurred among Caucasian individuals. However, a study conducted in the United States identified a higher number of deaths among Black, Hispanic, and Native American children, with Black individuals with orofacial clefts having a two-fold higher likelihood of death than Caucasians [11]. Despite this, there is limited information regarding the mortality of individuals with orofacial clefts in relation to race. The existing literature on sex aligns with the results presented here, showing higher mortality in males [19,22,23].
In Brazil, care and treatment for orofacial clefts are provided free of charge by SUS in specialized services authorized by the Ministry of Health, with private services acting in a complementary role. The reduction in the mortality rate from 1996 to 2013 can be attributed to several factors, including the expansion and strengthening of SUS, established by law in 1990 [24] (https://www.planalto.gov.br/ccivil_03/leis/l8080.htm). This improved access to universal and equitable medical care for the Brazilian population, including diagnosis and treatment for specialized conditions such as orofacial clefts. Another contributing factor to the reduction in deaths was the creation of the Family Health Program in 1994 and its integration with other levels of healthcare, allowing for increased access to care with continuous monitoring, education and awareness, multidisciplinary support, and improved early detection and treatment. In 1995, nutrition and breastfeeding programs, as well as vaccination campaigns, were developed. These may have contributed to reduced mortality through the prevention of infections and child malnutrition [25,26]. Social and educational support programs also improved families’ ability to seek early treatment and provide better care for children with orofacial clefts [25]. In 1997, partnerships between the government and the American non-governmental organization Operation Smile provided free surgeries, professional training, and multidisciplinary support for orofacial cleft care [27].
Until 1993, Brazil had only two facilities providing assistance to individuals with orofacial clefts, both located in the state of São Paulo. From that point onward, several new services were established throughout the country, with 27 units offering cleft treatment by 2013—likely contributing to the persistent reduction in mortality over the years studied. By 2025, there were 34 cleft treatment units authorized by SUS across Brazil, equipped with the necessary physical infrastructure, equipment, and human resources to provide clinical, surgical, and rehabilitation services for these individuals. However, 12 Brazilian states still do not have authorized treatment centers, with 64.7% of existing facilities concentrated in the southeast and south regions, and only two services located in the north (Tocantins and Pará) [28] (https://cnes2.datasus.gov.br/Mod_Ind_Habilitacoes_Listar.asp?VTipo=0401&VListar=1&VEstado=00&VMun=&VComp=&VContador=34&VTitulo=H).
5. Conclusions
This study provides evidence that after 24 years of declining mortality, there was an increase in the mortality rate for orofacial clefts between 2020 and 2023. This rise coincided with the coronavirus disease 2019 pandemic, during which the World Health Organization recommended a reduction in surgical procedures—a factor that may have impacted the rehabilitation, monitoring, and mortality of individuals with orofacial clefts in the country. The number of children under 1 year of age who died of causes related to orofacial clefts was higher than the mortality rate for children who died of other causes in the same age group. The prevalence of mortality in the first year of life, particularly among neonates under 28 days old, highlights the shortage of pediatric specialists as a public health concern and a critical gap in care for children with orofacial clefts. Deaths due to respiratory infections and malnutrition further underscore the need for targeted interventions to reduce preventable mortality in this vulnerable population.
Author Contributions
Conceptualization, Amanda de Andrade Costa; methodology, Amanda de Andrade Costa; formal analysis, Hildeth Maisa Torres Farias, Daniella Reis Barbosa Martelli, Verônica Oliveira Dias, Ricardo D. Coletta, Hercílio Martelli-Júnior; investigation, Amanda de Andrade Costa; data curation, Amanda de Andrade Costa; writing—original draft preparation, Amanda de Andrade Costa; writing—review and editing, Hildeth Maisa Torres Farias, Ricardo D. Coletta, Hercílio Martelli-Júnior; supervision, Hercílio Martelli-Júnior. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The requirements for ethical review and approval were waived for this study because of the use of secondary data only.
Informed Consent Statement
Not applicable.
Data Availability Statement
The original data presented in this study are openly available at https://datasus.saude.gov.br/informacoes-de-saude-tabnet/.
Acknowledgments
The authors gratefully acknowledge the Minas Gerais State Research Foundation (FAPEMIG, Minas Gerais, Brazil), the National Council for Scientific and Technological Development (CNPq, Brasilia, Brazil), and the Coordination of Training of Higher Education Graduate Foundation (CAPES, Brasilia, Brazil).
Conflicts of Interest
The authors declare no conflicts of interest.
Brazilian Oral Cleft Group investigators: Renato Assis Machado1,2, Letícia Pratali Dolce1, Sara Garcia Azevedo1, Silvia Regina Almeida de Reis3, Maria Paula Vidal Grisi3, Isabelle Farine Cardoso3, Ravena da Silva Araújo3, Viviane Palmeira da Silva3, Luiz Evaristo Ricci Volpato4, Lorraynne Dos Santos Lara4, Rafaela Scariot5, Bernardo Olsson5, Katheleen Miranda dos Santos5, Talita Farias Miksza Skrepetz5, Juliana Feltrin-Souza6, Gabriela Fonseca-Souza6, Ana Lúcia Carrinho Ayroza Rangel7.
Abbreviations
The following abbreviations are used in this manuscript:
| SUS | Unified Health System |
| CLP | Cleft lip and palate |
| CLO | Cleft lip only |
| CPO | Cleft palate only |
| DATASUS | Department of Informatics of the Brazilian Unified Health System |
| SINASC | Live Birth Information System |
| ICD-10 | International Classification of Diseases, Tenth Revision |
| DC | Death certificate |
References
- Machado, R.A.; Martelli-Junior, H.; Reis, S.R.A.; Küchler, E.C.; Scariot, R.; das Neves, L.T.; Coletta, R.D. Identification of novel variants in cleft palate-associated genes in Brazilian patients with non-syndromic cleft palate only. Front. Cell Dev. Biol. 2021, 9, 638522. [Google Scholar] [CrossRef] [PubMed]
- Hlongwa, P.; Levin, J.; Rispel, L.C. Epidemiologia e perfil clínico de indivíduos com fissura labiopalatina que utilizam centros de tratamento acadêmico especializados na África do Sul. PLoS One. 2019, 14, e0215931. [Google Scholar] [CrossRef]
- Martelli-Júnior, H.; Orsi Júnior, J.; Chaves, M.R.; Barros, L.M.; Bonan, P.R.F.; Freitas, J.A. [Epidemiological study of cleft lip and palate in Alfenas - Minas Gerais - 1986 to 1998]. RPG. 2006, 13, 31–35. [Google Scholar]
- Vyas, T.; Gupta, P.; Kumar, S.; Gupta, R.; Gupta, T.; Singh, H.P. Cleft of lip and palate: a review. J. Family Med. Prim. Care. 2020, 9. [Google Scholar] [CrossRef]
- Hujoel, P.P.; Bollen, A.M.; Mueller, B.A. First-year mortality among infants with facial clefts. Cleft Palate Craniofac. J. 1992, 29. [Google Scholar] [CrossRef]
- Christensen, K.; Juel, K.; Herskind, A.M.; Murray, J.C. Long term follow up study of survival associated with cleft lip and palate at birth. BMJ. 2004, 328, 1405. [Google Scholar] [CrossRef] [PubMed]
- Ngai, C.W.; Martin, W.L.; Tonks, A.; Wyldes, M.P.; Kilby, M.D. Are isolated facial cleft lip and palate associated with increased perinatal mortality? A cohort study from the West Midlands Region, 1995–1997. J. Matern. Fetal Neonatal Med. 2005, 17, 203–206. [Google Scholar] [CrossRef]
- Carlson, L.; Hatcher, K.W.; Burg, R.V. Elevated infant mortality rates among oral cleft and isolated oral cleft cases: a meta-analysis of studies from 1943 to 2010. Cleft Palate Craniofac. J. 2013, 50, 2–12. [Google Scholar] [CrossRef]
- Malic, C.C.; Lam, M.; Donelle, J.; Richard, L.; Vigod, S.N.; Benchimol, E.I. Incidence, risk factors, and mortality associated with orofacial cleft among children in Ontario, Canada. JAMA Netw. Open. 2020, 3, e1921036. [Google Scholar] [CrossRef]
- van Nunen, D.P.F.; van den Boogaard, M.-J.H.; Don Griot, J.P.W.; Rüttermann, M.; van derVeken, L.; Breugem, C.C. Elevated infant mortaity rate among Dutch oral cleft cases: a retrospective analysis from 1997 to 2011. Front. Surg. 2014, 1, 48. [Google Scholar] [CrossRef]
- Huang, R.S.; Mihalache, A.; Riff, K.W.Y.W. Cleft lip and/or palate mortality trends in the USA: a retrospective population-based study. BMJ Paediatr. Open 2024, 8, e002305. [Google Scholar] [CrossRef]
- Goldrick, N.M.; Revie, G.; Groisman, B.; Hurtado-Villa, P.; Sipek, A.; Khoshnood, B.; Rissmann, A.; Dastgiri, S.; Landau, D.; Tagliabue, G.; Pierini, A.; Gatt, M.; Mutchinick, O.M.; Martínez, L.; Walle, H.E.K.; Szabova, E.; Camelo, J.L. A multi-program analysis of cleft lip with cleft palate prevalence and mortality using data from 22 International Clearinghouse for Birth Defects Surveillance and Research programs, 1974–2014. Birth Defects Res. 2023, 115, 980–997. [Google Scholar] [CrossRef] [PubMed]
- IPEA, Institute for Applied Economic Research. [Sustainable Development Goals]. 2019. Available online: https://www.ipea.gov.br/ods/ods3.html#:~:text=At%C3%A9%202030%2C%20acabar%20com%20as,25%20por%201.000%20nascidos%20vivos.Acesso%20em%2028%20de%20junho%20de%202024. [In Portuguese]. Accessed in march, 2024.
- DATASUS. Tabnet. Available online: https://datasus.saude.gov.br/informacoes-de-saude-tabnet/ (accessed on 21 June 2024).
- World Health Organization. International Statistical Classification of Diseases and Related Health Problems, 10th revision. Vol. 3; University of São Paulo Press: São Paulo, Brazil, 2012. [Google Scholar]
- Ishitani, L.H.; França, E. Uso das Causas Múltiplas de Morte em Saúde Pública. Informe Epidemiológico do SUS. 2001, 10, 163–175. [Google Scholar] [CrossRef]
- Higashi, H.; Barendregt, J.J.; Kassebaum, N.J.; Weiser, T.G.; Bickler, S.W.; Vos, T. The burden of selected congenital anomalies amenable to surgery in low and middle-income regions: cleft lip and palate, congenital heart anomalies and neural tube defects. Arch. Dis. Child 2015, 100, 233–238. [Google Scholar] [CrossRef] [PubMed]
- Mullassery, D.; Llewellyn, R.S.; Almond, S.L.; Jesudason, E.C.; Losty, P.D. Oesophageal atresia with cleft lip and palate: a marker for associated lethal anomalies? Pediatr. Surg. Int. 2008, 24, 815–817. [Google Scholar] [CrossRef]
- Kang, S.L.; Narayanan, S.B.; Kelsall, W. Oral/perioral reactions to injectable soft tissue fillers: a clinicopathological multicentric study. Cleft Palate Craniofac. J. 2012, 49, 508–511. [Google Scholar] [CrossRef]
- Ryu, J.Y.; Park, T.H.; Cho, B.C.; Choi, K.Y. The prevalence, risk of premature births, mortality and causes of death of cleft lip with or without palate in South Korea: a nationwide population-based cohort study. Int. J. Epidemiol. 2022, 51. [Google Scholar] [CrossRef]
- Silveira, D.M.M.L.; Martelli, D.R.B.; Dias, V.O.; Silveira, M.S.C.; Almeida, I.L.F.; Martelli Júnior, H. Surgical rehabilitation of cleft lip and/or palate: evaluation of the Brazilian public health system. Braz. J. Otorhinolaryngol. 2022, 88, S126–S132. [Google Scholar] [CrossRef]
- Bell, J.C.; Nassar, N.; Bower, C.; Turner, R.M; Raynes-Greenow, C. Long-term survival for infants born with orofacial clefts in Western Australia. Birth Defects Res. A Clin. Mol. Teratol. 2016, 106, 172–177. [Google Scholar] [CrossRef]
- Zhou, X.; Jiang, Y.; Fang, J.; Wang, H.; Xie, D.; Kuang, H.; Li, T.; Liu, Q.; He, J. Incidence of cleft lip and palate, and epidemiology of perinatal deaths related to cleft lip and palate in Hunan Province, China, 2016–2020. Sci. Rep. 2023, 13, 10304. [Google Scholar] [CrossRef]
- Brazil. Presidency of the Republic. Civil House. Subdepartment for Legal Affairs. Law No. 8,080 of September 19, 1990; Brasilia, Brazil, 1990, 128, 18055–18059. [Google Scholar]
- Fertonani, H.P.; Pires, D.E.P.; Biff, D.; Scherer, M.D.A. [Healthcare model: concepts and challenges for Brazilian primary care]. Ciência & Saúde Coletiva 2015, 20, 1869–1878, [In Portuguese]. Accessed in march, 2024. [Google Scholar] [CrossRef]
- Molen, M.V.; Breugel, J.M.M.V.; Janssen, N.G.; Admiraal, R.J.C.; van Adrichem, L.N.A.; Bierenbroodspot, F.; Bittermann, D.; van den Boogaard, M.-J.H.; Broos, P.H.; DijkstraPutkamer, J.J.M. Clinical practice guidelines on the treatment of patients with cleft lip, alveolus, and palate: an executive summary. J. Clin. Med. 2021, 10, 4813. [Google Scholar] [CrossRef]
- Operation Smile. [Report on Services Provided in Brazil]. Available online: https://www.operacaosorriso.org.br/wp-content/uploads/2024/04/Relatorio-de-atendimentos-final-2024.pdf [In Portuguese]. Accessed in march, 2024.
- CNES. National Register of Health Facilities. [Reports: Accreditations]. Available online: https://cnes2.datasus.gov.br/Mod_Ind_Habilitacoes_Listar.asp?VTipo=0401&VListar=1&VEstado=00&VMun=&VComp=&VContador=34&VTitulo=H. [In Portuguese]. Accessed in march, 2024.
Figure 1.
Mortality trend of patients with orofacial clefts, 1996–2023.
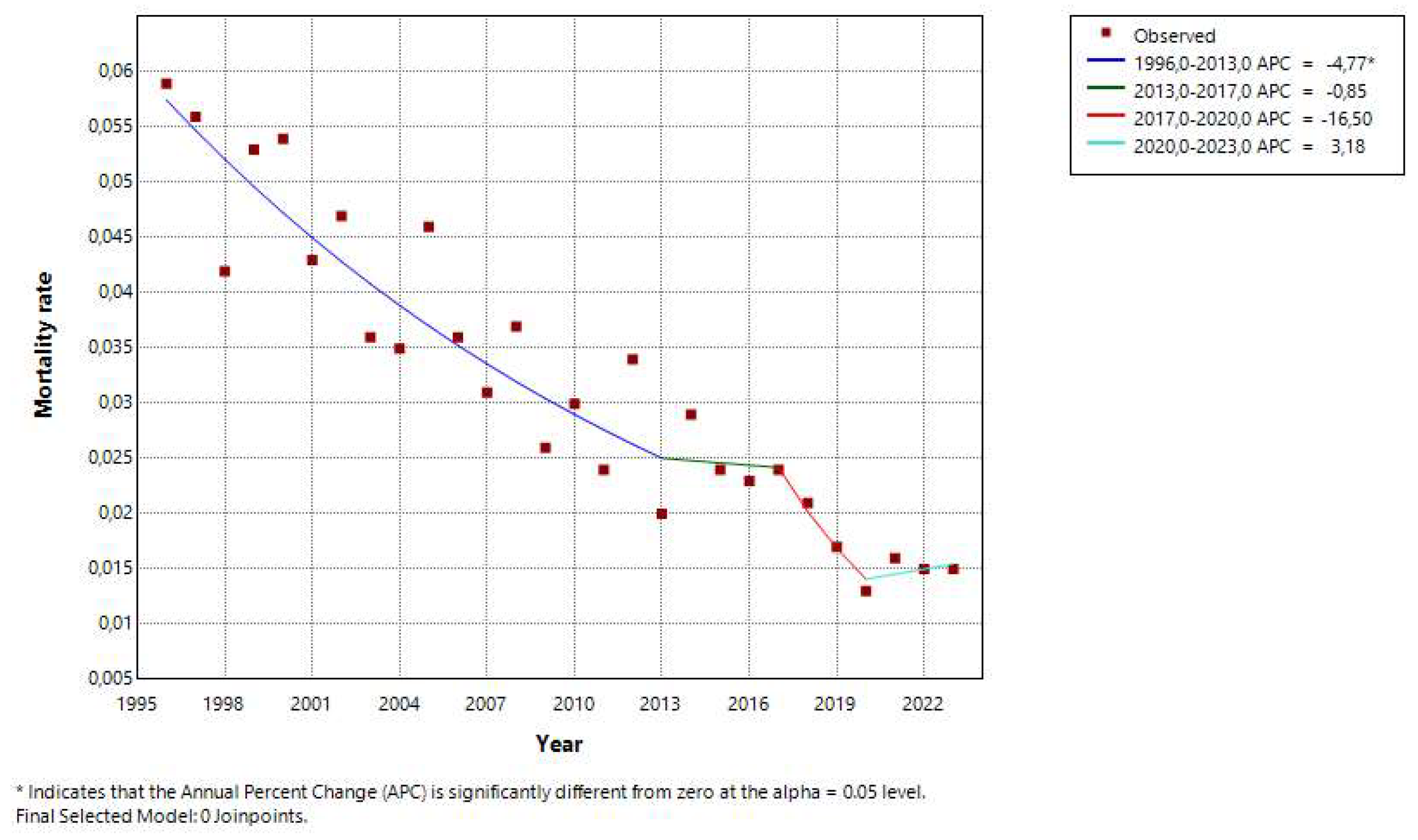
Figure 2.
Number of deaths of individuals under 1 year of age with orofacial clefts by region of Brazil and race/ethnicity. DATASUS, 1996–2023.
Figure 2.
Number of deaths of individuals under 1 year of age with orofacial clefts by region of Brazil and race/ethnicity. DATASUS, 1996–2023.
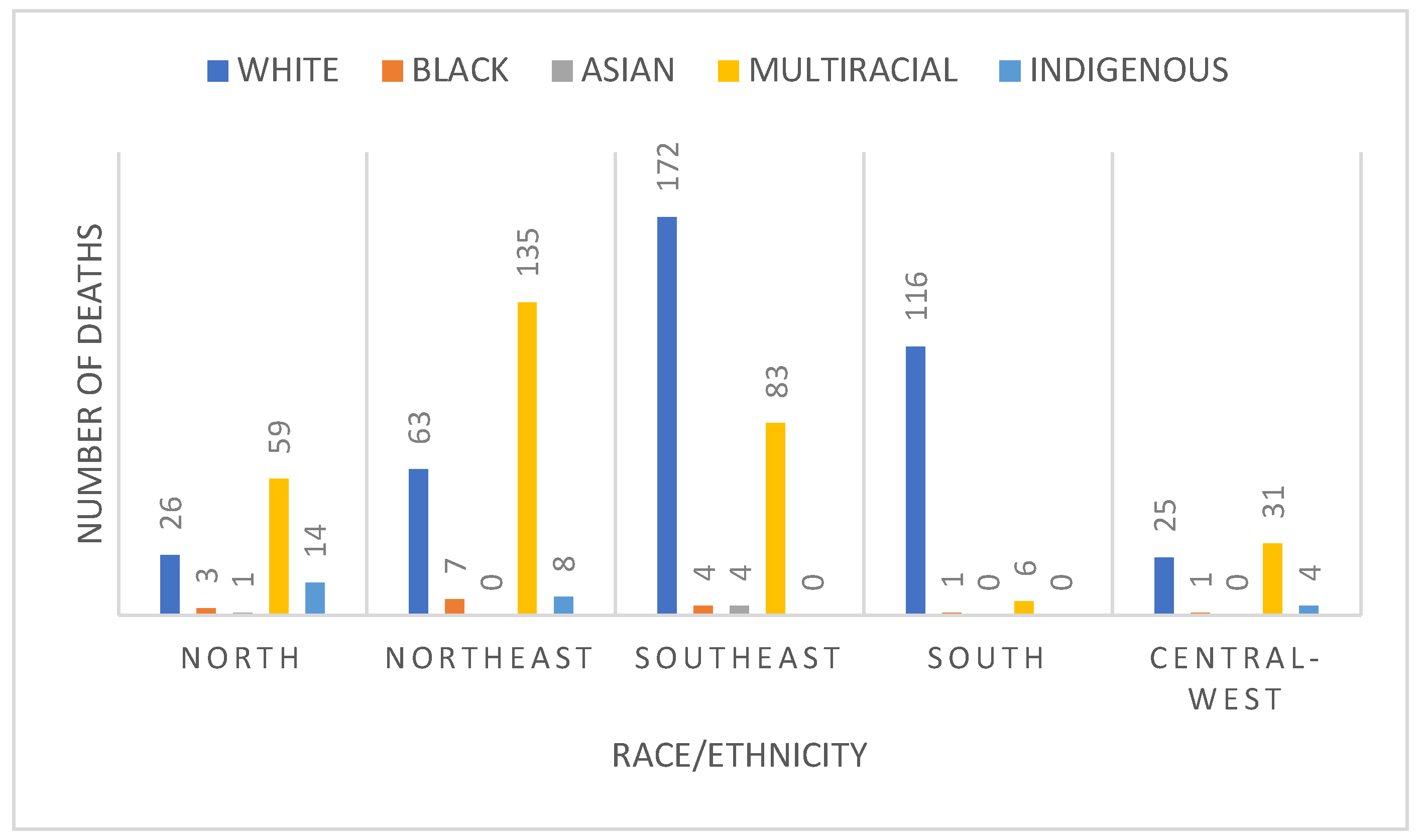
Figure 3.
Number of deaths of individuals with orofacial clefts by multiple causes, according to ICD-10 chapters. DATASUS, 2006–2023.
Figure 3.
Number of deaths of individuals with orofacial clefts by multiple causes, according to ICD-10 chapters. DATASUS, 2006–2023.
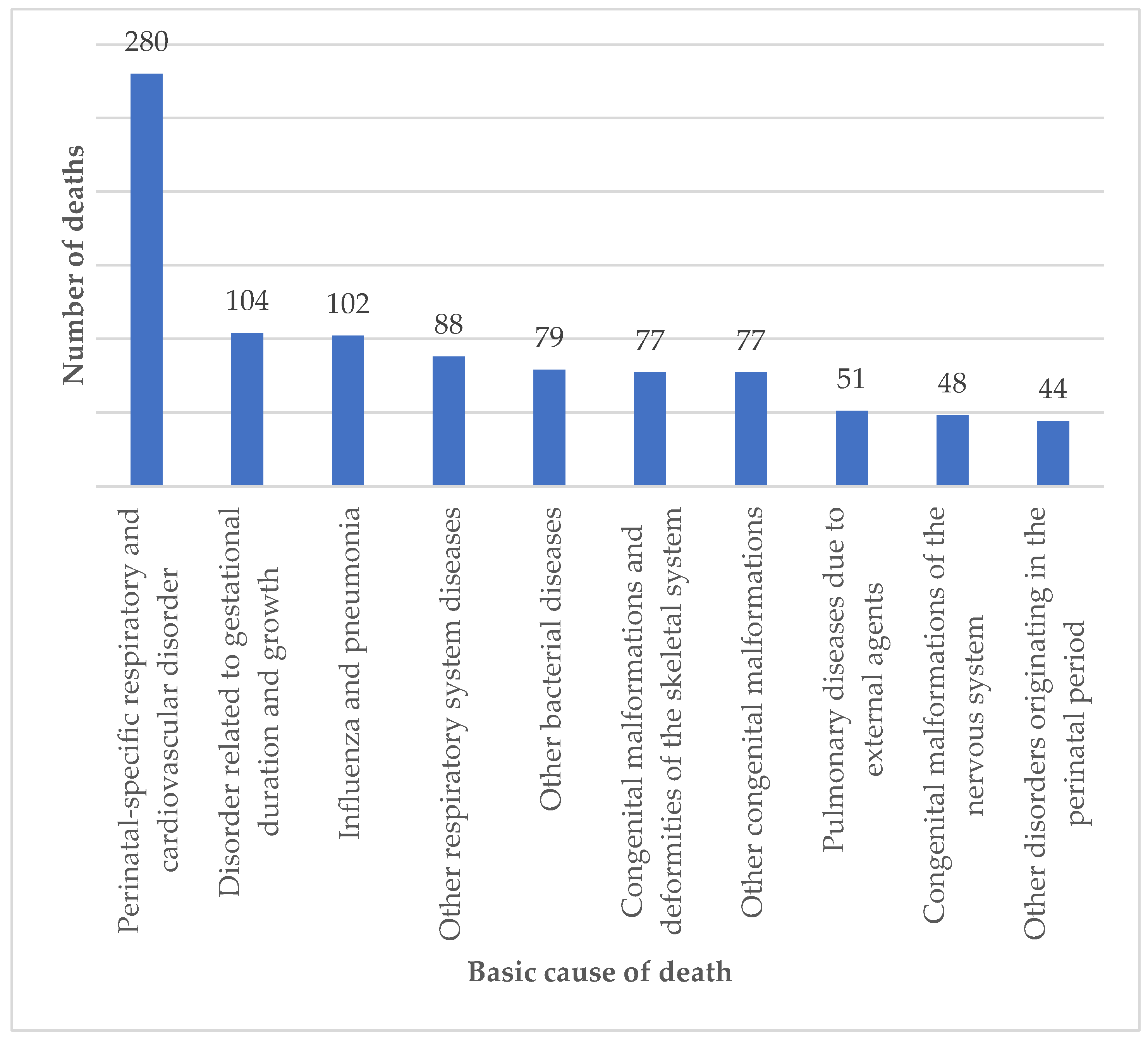
Figure 4.
Mortality rate of children under 1 year of age who died of orofacial clefts and other causes. DATASUS, 2010–2023.
Figure 4.
Mortality rate of children under 1 year of age who died of orofacial clefts and other causes. DATASUS, 2010–2023.
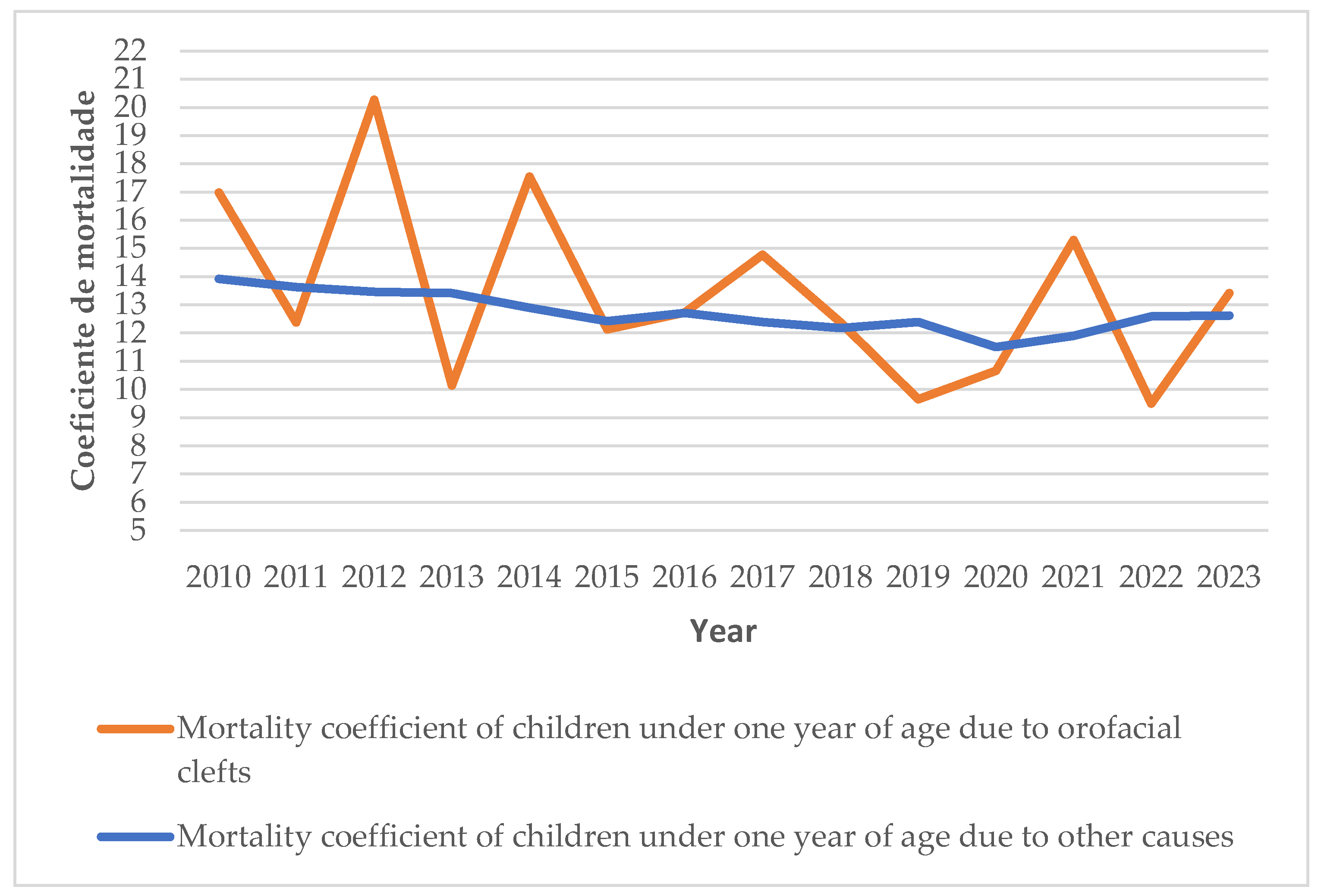

Table 1.
Characterization of deaths according to age, sex, and race, 1996–2023.
| Age | n |
|---|---|
| 0–27 days | 477 |
| 28–364 days | 403 |
| 1–4 years | 68 |
| 5–9 years | 8 |
| 10–14 years | 6 |
| 15–19 years | 3 |
| 25–29 years | 2 |
| 30–34 years | 4 |
| 40–44 years | 1 |
| 45–49 years | 1 |
| 50–54 years | 4 |
| 65–69 years | 1 |
| 70–74 years | 3 |
| 75–79 years | 2 |
| ≥80 years | 3 |
| Unknown | 1 |
| Sex | n |
| Male | 533 |
| Female | 446 |
| Race | n |
| Caucasian | 402 |
| Multiracial | 314 |
| Unknown | 224 |
| Indigenous | 26 |
| Black | 16 |
| Asian | 5 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



