
Submitted:
06 May 2025
Posted:
06 May 2025
You are already at the latest version
Abstract
Dementia cases are projected to triple globally by 2050, largely driven by an aging population. While aging remains the primary risk factor, emerging evidence suggests that diet, including total meat intake, may influence dementia risk. This study investigates the relationship between total meat consumption (red and white meat) and dementia incidence using data from 204 countries.
Bivariate correlations revealed a significant positive association between total meat intake and dementia incidence globally (r = 0.588, p < 0.001), with a stronger effect observed in low- and middle-income countries (z = 3.92, p < 0.001). Partial correlation analyses and multiple regression models, controlling for aging, economic status, genetic predisposition, and urbanization, confirmed that meat intake remained a significant predictor of dementia (Beta = 0.202, p < 0.001). Aging showed the strongest influence (Beta = 0.788, p < 0.001), underscoring its dominant role. Regional analyses suggested socio-economic disparities, dietary habits, and limited access to diverse nutrition as factors amplifying the association in developing regions.
These findings identify total meat intake as a modifiable dietary factor contributing to dementia risk, particularly in resource-constrained settings. Implementing tailored dietary interventions may help reduce dementia incidence globally, especially in vulnerable populations.
Keywords:
Meat intake
; Dementia
; Global health
; Aging
; Diet
Introduction
Dementia is a pressing global health issue affecting millions, with its prevalence expected to rise substantially due to an aging population. The World Health Organization (WHO) predicts that by 2050, the number of people living with dementia will triple [1]. This neurodegenerative condition is marked by a progressive decline in cognitive abilities, including memory, reasoning, and behavior [2]. Although aging remains the most critical risk factor, there is an increasing focus on modifiable lifestyle influences, particularly dietary factors, that may contribute to dementia onset and progression [3]. Among these, meat intake has emerged as a potential contributor to dementia risk, though its role remains under-investigated [4].
Dietary habits significantly impact health outcomes, with ample evidence linking certain diets to reduced risks of chronic diseases. Research on diet and dementia has predominantly centered on plant-based diets, such as the Mediterranean diet, which is rich in whole grains, vegetables, fruits and healthy fats [5]. These diets have been associated with lower dementia risk due to their anti-inflammatory and cardioprotective properties [6]. For instance, the Mediterranean diet supports vascular health, which is vital for cognitive function maintenance [7]. However, the potential influence of meat consumption, especially total meat intake, on dementia risk has received comparatively little attention.
In recent decades, global meat intake has surged, doubling or even tripling, particularly within developing regions [8]. This increase has coincided with a rise in dementia prevalence in several low- and middle-income nations, such as Japan, Peru, and Cuba, as suggested by ecological and cross-sectional studies [9,10]. In Sweden, research involving cognitively healthy adults found that lower meat intake correlated with improved cognitive function and greater brain volume over a five-year period [11]. However, the specific effects of different meat types on dementia risk remain inadequately explored, with findings still limited and inconsistent [12,13].
Most existing research has concentrated on individual meat types, such as beef, pork, and lamb [12]. There is a need to differentiate between processed and unprocessed meats, as these forms may have distinct health effects [14]. A systematic review on meat consumption and cognitive disorders, including dementia, found that studies often analyzed meat intake as part of broader dietary patterns, resulting in high variability and limited clarity on the effects of specific meat types or quantities [12].
The focus on red meat alone may overlook the broader dietary context. Populations generally consume both red and white meats, and studies focusing on total meat intake may provide a more comprehensive understanding of potential cognitive health risks [15]. Although white meat, such as poultry, is often considered a healthier alternative to red meat due to its lower saturated fat content, recent findings suggest it may also carry cognitive health risks. White meat contains L-carnitine, a compound metabolized by gut bacteria to produce trimethylamine-N-oxide (TMAO) [16], which is implicated in neuroinflammation, a critical factor in dementia development [17].
In addition to TMAO, both red and white meats contain other compounds that may impact cognitive health [17]. For example, heme iron, primarily found in red meat, can induce oxidative stress, while advanced glycation end products (AGEs), which accumulate in cooked meats, are linked to inflammation and neurodegeneration. Although culinary classifications categorize red and white meats based on color and texture, there is substantial overlap in their biochemical compositions [18]. For instance, iron, a factor associated with dementia risk, is present in both red and white meats, though in different amounts. These factors suggest that total meat intake may be more relevant to dementia risk than red meat alone. Nevertheless, few studies have rigorously examined the role of overall meat consumption in dementia, highlighting a critical research gap [19].
This study investigates the hypothesis that high meat consumption may contribute to increased dementia incidence globally. Addressing a gap in the current literature, this research evaluates whether total meat intake serves as a predictor of dementia risk. Building on prior studies that link high meat consumption to various chronic health conditions, this study explores whether similar patterns appear in relation to dementia. By leveraging global data, the analysis examines the relationship between meat intake and dementia while controlling for factors such as economic status, age, genetic predispositions, and urbanization.
Materials and Methods
Data Collection and Selection
For this population-level analysis, data were gathered from recognized international sources, including United Nations agencies and the Institute for Health Metrics and Evaluation (IHME). The dataset on dementia incidence was specifically sourced from IHME [20], while a comprehensive list of 204 regions was obtained from the World Bank to ensure consistency in variable matching. In this context, the term “country” refers to a geographic region that reports separate health, demographic, and economic data, as defined by international organizations such as the World Bank. This designation does not necessarily imply political sovereignty, and the terms “country” and “population” are used interchangeably in this study [21].
The primary independent variable, meat intake, was measured using the total meat supply per capita for the period 2019-2021. These data were sourced from the FAOSTAT Food Balance Sheet (FBS) and expressed in kg per capita per year [22]. This measure reflects the average quantity of animal-based food available per individual, encompassing both red and white meats. The included types were beef, veal, buffalo, pork, mutton, lamb, goat, horse, poultry (chicken, goose, duck, turkey), rabbit, game, and offal [22].
The dependent variable, dementia incidence rate (new cases per 100,000 individuals), was taken from IHME’s 2021 dataset. IHME [20], an independent research institute within the University of Washington, is noted for its comprehensive work in global health statistics and its data-driven strategies addressing health challenges.
Given dementia’s multifactorial etiology, this study accounted for potential confounding variables that could influence the observed relationship between meat intake and dementia incidence. Economic status, quantified through per capita GDP adjusted for purchasing power parity (PPP) in 2018, was one such factor sourced from the World Bank database. Economic affluence correlates with longer life expectancy, higher education levels, and lifestyle-related risk factors like obesity and diabetes [23]. It also influences the capacity for early dementia detection, reflecting variations in healthcare infrastructure globally [24].
The Biological State Index (Ibs) serves as a measure of genetic predisposition, indicating the accumulation of dementia-related genetic traits within a population. This index, with values ranging from 0 to 1.0, was obtained from a 2022 study. The concept behind BSI is that diminished natural selection can lead to an increased prevalence of deleterious genes, which contribute to the risk of non-communicable diseases like dementia [25]. Populations with higher Ibs scores exhibit a greater accumulation of these genetic vulnerabilities, correlating with a higher likelihood of dementia onset [32].
Life expectancy at birth, serving as a proxy for population aging, was obtained from the World Bank database [26]. While dementia can manifest at various life stages, it primarily affects older adults; hence, 2018 life expectancy data were used to represent the aging process in this analysis. Data on urbanization, defined as the proportion of the population residing in urban areas in 2018 [23], were also sourced from the World Bank. Urban environments can shape lifestyle behaviors, influencing choices that affect dementia risk. Modernization and industrial growth have been linked to lifestyle shifts such as increased meat consumption [27,28], greater availability of processed foods rich in salt, sugar, and fats [29], and reduced physical activity [30]. These factors collectively contribute to health outcomes relevant to dementia. However, urban settings may also facilitate earlier detection and diagnosis, potentially affecting reported incidence rates and adding complexity to dementia data interpretation.
During data cleaning, two extreme outliers were identified and excluded from the sequential multiple data analysis models: Japan, with a meat intake of 54.91 kg/capita/year and a dementia incidence rate of 421.62/100,000 people, and Tonga, with a meat intake of 160.50 kg/capita/year and a dementia incidence rate of 64.31/100,000 people. These outliers were removed from the dataset for analysis.
All variables were compiled and organized using Microsoft Excel® 2016 for subsequent analysis. Each country or population was treated as a unique data point within this ecological analysis framework. The total number of countries analyzed varied for different variables, as comprehensive data were not uniformly available across all indicators due to limitations in reporting by relevant United Nations agencies.
Statistical Analyses
The analysis of the relationship between meat intake and dementia incidence followed a structured, multi-step approach, informed by prior research [25,31,32,33,34,35]:
- Initial Data Exploration: Scatter plots were generated using Microsoft Excel® 2016 to visually assess the association between global meat intake and dementia incidence. This preliminary step helped identify any extreme outliers and ensured dataset integrity.
- Bivariate Correlation Analysis: Both Pearson’s and nonparametric methods, were conducted to determine the strength and direction of associations among variables including meat intake, dementia incidence, economic status, genetic predisposition, aging, and urbanization.
- Partial Correlation Analysis: Pearson’s partial correlation was used to explore the relationship between meat intake and dementia incidence while statistically controlling for economic status, genetic predisposition, aging, and urbanization as confounding factors.
- Multiple Linear Regression: A standard (enter) multiple linear regression was performed to delineate the predictive relationship between dementia incidence (dependent variable) and both the main predictor (meat intake) and confounders. This analysis was conducted to evaluate the independent contribution of meat intake in the presence of economic status, genetic predisposition, aging, and urbanization. The regression model quantified the explanatory power of meat intake by comparing results with and without its inclusion as a predictor. Subsequently, stepwise multiple linear regression was applied to identify the most significant predictors of dementia incidence under similar conditions.
-
Regional Correlation Analysis: Bivariate correlations (Pearson’s r and nonparametric) were extended to regional groupings to capture variations in the relationship between meat intake and dementia incidence. The analysis stratified countries according to:
- ○
- World Bank Income Groups: High, upper-middle, lower-middle, and low-income countries. Special attention was given to compare high-income countries with combined low- and middle-income countries, addressing the WHO’s assertion that over 60% of dementia cases occur in LMICs [36]. Fisher’s r-to-z transformation was applied for these comparisons.
- ○
- United Nations Classification: Developed versus developing countries, with correlation differences analyzed using Fisher’s r-to-z transformation to respond to WHO’s regional focus [37].
- ○
- WHO Regional Classifications: Analyses were stratified by regions (Africa, Americas, Eastern Mediterranean, Europe, South-East Asia, and Western Pacific) [38].
- ○
- Cultural and Economic Groupings: Specific country groupings were analyzed, including members of the Asia Cooperation Dialogue (ACD) [39], Asia-Pacific Economic Cooperation (APEC) [40], the Arab World [41], English-speaking countries (based on government data), Latin America [42], Latin America and the Caribbean (LAC) [42], Organisation for Economic Co-operation and Development (OECD) [43], and Southern African Development Community (SADC) [44].
Data analysis was conducted using SPSS version 29 (SPSS Inc., Chicago, IL, USA) and Microsoft Excel 2016®. The significance level was set at 0.05, with results also reported at 0.01 and 0.001 significance levels. Criteria for stepwise multiple linear regression included a probability of F to enter ≤ 0.05 and to remove ≥ 0.10.
Results
Figure 1 presents the unadjusted correlation between total meat intake and dementia incidence, modeled by a polynomial regression equation (y = -0.0218x² + 4.185x - 23.683, R² = 0.3919). This equation reflects a moderately strong relationship (r = .626, p < .001), indicating that variations in meat consumption align with changes in dementia rates. The absence of significant outliers in the plot supports a good alignment with the polynomial curve, suggesting that the data points conform well to the observed pattern (Figure 1).
Table 1 highlights that both Pearson and nonparametric analyses identified significant, strong associations between total meat intake and dementia incidence (r = .588 for Pearson and r = .678 for nonparametric, p < .001). Moreover, moderate to strong significant associations were observed between dementia incidence and factors such as economic affluence, genetic predisposition, aging, and urbanization. These results provided a rationale for considering these variables as potential confounders in the analysis of the link between meat intake and dementia incidence.
Partial correlation analysis revealed that total meat intake remained a significant predictor of dementia incidence when economic affluence, genetic predisposition, aging, and urban living were statistically controlled (r = .227, p < .010, Table 2). Furthermore, when meat intake was treated as a confounding factor, partial correlations indicated that each of the confounding variables—economic affluence, genetic predisposition, aging, and urban living—remained significantly associated with dementia incidence (r = .376, .372, .587, and .257, respectively, p < .001). These findings suggest that dementia onset is influenced by multiple interconnected factors.
Standard multiple linear regression (enter) analysis was conducted to predict dementia incidence using meat intake, economic affluence, genetic predisposition, aging, and urban living as predictor variables. When total meat intake was excluded, aging emerged as the only significant predictor of dementia incidence (Beta = .788, p < .001, Table 3-1). However, when meat intake was included, it became a significant predictor (Beta = .202, p < .001), along with economic affluence (Beta = .082, p < .010) and urban living (Beta = - .017, p < .001), although the contributions of economic affluence and urban living were small but statistically significant (Table 3-1).
In the stepwise multiple linear regression analysis, aging was again identified as the only significant predictor of dementia incidence when meat intake was excluded, yielding an adjusted R² of .539 (Table 3-2). Once meat intake was included, it became the second most significant predictor, increasing the adjusted R² to .563. Genetic predisposition was identified as the third most important factor, while economic affluence and urban living remained non-significant in the stepwise model.
A standard multiple linear regression (enter method) was conducted to predict dementia incidence using meat intake, economic affluence, genetic predisposition, aging, and urban living as predictors. When meat intake was excluded, aging was the only significant predictor of dementia incidence (β=.788, p < .001, Table 3-1). However, when meat intake was included, it became a significant predictor (beta = .202, p < .001), along with economic affluence (beta = .082, p < .010) and urban living (beta = - .017, p < .001), though the contributions of economic affluence and urban living were small but statistically significant (Table 3-1).
In the stepwise multiple linear regression analysis, aging remained the only significant predictor of dementia incidence when meat intake was excluded, yielding an adjusted R2 of .539 (Table 3-2). When meat intake was added, it emerged as the second most significant predictor, raising the adjusted R2 to .563. Genetic predisposition was identified as the third predictor, while economic affluence and urban living remained non-significant in the stepwise model.
Table 4 displays the bivariate correlations examining the relationship between meat intake and dementia incidence across different country classifications. Overall, the analysis found positive correlations between meat consumption and dementia rates across most country categories, evaluated using both Pearson and nonparametric tests. The observed correlation strength and statistical significance varied, potentially influenced by differences in sample sizes and the level of homogeneity within each group. Fisher’s r-to-z transformation analysis indicated that the association between meat intake and dementia incidence was notably stronger in low- and middle-income countries than in high-income nations (z = 3.92, p < .001 for Pearson’s r; z = 5.64, p < .001 for the nonparametric analysis). Additionally, the correlation was significantly greater in developing countries compared to developed ones (z = 2.5, p < .010 for Pearson’s r; z = 3.94, p < .001 for the nonparametric analysis). These results point to a potentially more substantial influence of meat intake on dementia incidence in lower-income regions compared to higher-income regions (Table 4).
Discussion
This study explored the global relationship between total meat intake and dementia incidence, broadening the focus beyond red meat to assess the collective impact of both red and white meat on cognitive health. Results indicate that total meat intake is a significant predictor of dementia incidence, even after controlling for key factors such as economic status, genetic predisposition, aging, and urbanization. This suggests that both red and white meats, each contributing unique compounds potentially affecting cognitive health, may collectively influence dementia risk.
This study findings demonstrate a positive correlation between total meat intake and dementia incidence worldwide, consistent with previous research linking high meat consumption to adverse health outcomes. However, the association is more pronounced in low- and middle-income countries compared to high-income countries. This discrepancy may be due to differences in dietary patterns, healthcare access, and overall nutritional diversity, underscoring the importance of cultural and socioeconomic factors in assessing dementia risk.
The study’s emphasis on total meat intake contributes valuable insights into dietary patterns and their broader implications for cognitive health. Both red and white meats contain compounds—such as L-carnitine and heme iron—that may contribute to inflammatory processes and oxidative stress [45], which are well-documented mechanisms in dementia development. Although white meat is often considered healthier due to lower saturated fat content [46], recent evidence suggests it may also pose cognitive health risks through compounds like trimethylamine-N-oxide (TMAO) [47], which is linked to neuroinflammation and may play a role in dementia progression [48].
The current literature on meat consumption and dementia risk remains varied, with mixed findings from cohort studies. For example, a UK Biobank cohort study found that processed meat was associated with an increased risk of dementia, while unprocessed red meat was linked to a reduced risk [49]. In contrast, the Three-City (3C) cohort study reported that lower meat consumption (≤1 time per week) was linked to higher dementia risk compared to higher consumption (≥4 times per week), though differences in methodology and categorization could explain these inconsistencies [50]. Similarly, a French cohort study observed a non-significant association between infrequent meat consumption and dementia incidence, likely due to small sample sizes [51]. In a German cohort, no significant relationship was found between meat consumption and dementia risk over four years, though this study examined specific meat items only [52]. Such inconsistencies point to the need for further research clarifying the effects of different meat types and consumption levels on dementia risk.
Variations in meat composition may partially explain these divergent findings. Compounds commonly found in processed meats, such as nitrites and N-nitroso compounds, are known to promote oxidative stress, lipid peroxidation, and inflammation, all of which may contribute to dementia [53]. Additionally, increased meat consumption is associated with higher intake of saturated fatty acids, which have been linked to dementia risk [54]. Processed meats also contain high sodium levels, which could adversely impact cognitive health. Studies in animal models show that high-salt diets can elevate blood pressure and reduce cerebral blood flow, potentially impairing cognitive function [55].
Distinctions between processed and unprocessed meats may help clarify why processed meats are more consistently associated with dementia risk compared to unprocessed meats, such as poultry and red meat. Conversely, high protein intake from meat could potentially protect against dementia, as adequate protein levels have been associated with reduced cognitive impairment risk [56]. Age-related iron accumulation in the brain, however, may increase neurodegeneration risk, with abnormal iron metabolism inducing oxidative stress, a contributing factor in cognitive decline [57]. Some studies even suggest that iron in red meat supports brain health by reducing iron deficiency—a condition associated with cognitive decline—further complicating the relationship between meat consumption and dementia [58].
This study found that associations between meat intake and dementia incidence were weaker in high-income countries, likely due to more diverse diets, higher plant-based food consumption, and greater healthcare access, which may offset some negative effects of meat consumption on cognitive health. By contrast, in low- and middle-income countries, where dietary diversity and healthcare access are more limited, the positive correlation between meat consumption and dementia incidence suggests that high-meat diets could exacerbate dementia risk in these regions.
Our regression analysis identified aging as the strongest predictor of dementia incidence, affirming the well-established role of aging as the primary non-modifiable risk factor for dementia. However, total meat intake also emerged as a secondary predictor, underscoring its potential as a modifiable factor that could be addressed in dementia prevention strategies. Although factors like economic status and urbanization were also significant, their contributions to dementia risk were relatively minor, suggesting that broader lifestyle factors—including dietary choices, healthcare access, and physical activity—may indirectly influence dementia risk. These findings support the need for comprehensive, multifaceted approaches to dementia prevention that address modifiable risk factors, including dietary intake.
Limitation of this Study
First, its reliance on population-level data may overlook individual differences in dietary habits and health behaviours, posing a risk of ecological fallacy. Observed relationships may apply at the country level but may not hold true for individuals.
Second, dementia incidence data were sourced from international databases, such as IHME, which may be incomplete, particularly in developing nations with limited record-keeping. Although controls for economic affluence, genetic predisposition, aging, and urbanization were applied, some residual bias might persist.
Third, meat intake was broadly defined as “flesh of animals,” without accounting for the effects of processing and cooking methods, which can influence health outcomes. Additionally, the study used FAO data on general meat supply, not direct human consumption, making meat intake an approximation rather than a precise measure.
Finally, other influential factors, such as physical activity and healthcare access, were not directly addressed. Future research should use longitudinal data to assess causality and examine whether reducing meat intake could lower dementia risk across diverse contexts. These limitations highlight the need for caution in interpreting results and the importance of further research to confirm these findings.
Conclusion
Globally, access to total meat (flesh) could play a critical role in predicting dementia risk, particularly within low- and lower-middle-income nations. This study contributes to understanding dietary risk factors for dementia by examining total meat intake rather than focusing solely on red meat. The study findings suggest that high total meat consumption may increase dementia risk, particularly in low- and middle-income countries, highlighting the importance of considering total dietary intake in public health strategies and dietary recommendations for cognitive health.
Data availability
Details of the data sources are outlined in the “Materials and Methods” section. All datasets utilized in this study were freely accessed and downloaded from publicly available resources on United Nations (UN) agency websites. Since the data were sourced from open-access repositories, formal participant consent was not applicable. The use of these datasets aligns with the public use policies specified by the UN agencies, eliminating the need for additional permissions for academic research, as discussed in the “Materials and Methods” with appropriate references.
Ethics approval
The data utilized in this study were limited to population-level statistics and could not be linked back to any individual, their family, or their community. As such, there was no risk of personal identification or re-identification. The University of Adelaide’s Office of Research Ethics, Compliance, and Integrity (ORECI) reviewed and exempted this study from requiring formal ethical approval (Ethics Approval Number: 36289).
Competing interests
The author declares no conflicts of interests.
Author’s contributions
The sole author’s contributions include Conceptualization, Data Curation, Formal Analysis, Funding Acquisition, Investigation, Methodology, Project Administration, Resources, Software, Supervision, Validation, Visualization, Writing – Original Draft, Writing – Review & Editing.
References
- WHO. Dementia. 2023 March 22 2024]; Available from: https://www.who.int/news-room/fact-sheets/detail/dementia#:~:text=It%20mainly%20affects%20older%20people,high%20blood%20pressure%20(hypertension).
- von Gunten, A., et al., Neurocognitive disorders in old age: Alzheimer’s disease, frontotemporal dementia, dementia with Lewy bodies, and prion and infectious diseases. Primary Care Mental Health in Older People: A Global Perspective, 2019: p. 251-298.
- Wahl, D., et al., Aging, lifestyle and dementia. Neurobiology of disease, 2019. 130: p. 104481.
- Pistollato, F., et al., Nutritional patterns associated with the maintenance of neurocognitive functions and the risk of dementia and Alzheimer’s disease: A focus on human studies. Pharmacological research, 2018. 131: p. 32-43. [CrossRef]
- Valls-Pedret, C., et al., Mediterranean diet and age-related cognitive decline: a randomized clinical trial. JAMA internal medicine, 2015. 175(7): p. 1094-1103.
- Aridi, Y.S., J.L. Walker, and O.R. Wright, The association between the Mediterranean dietary pattern and cognitive health: a systematic review. Nutrients, 2017. 9(7): p. 674. [CrossRef]
- Martínez-Lapiscina, E.H., et al., Mediterranean diet improves cognition: the PREDIMED-NAVARRA randomised trial. Journal of Neurology, Neurosurgery & Psychiatry, 2013. 84(12): p. 1318-1325. [CrossRef]
- Bruinsma, J., World agriculture: towards 2015/2030: an FAO study. 2017: Routledge.
- Albanese, E., et al., Dietary fish and meat intake and dementia in Latin America, China, and India: a 10/66 Dementia Research Group population-based study. The American journal of clinical nutrition, 2009. 90(2): p. 392-400.
- Grant, W.B., Trends in diet and Alzheimer’s disease during the nutrition transition in Japan and developing countries. Journal of Alzheimer’s Disease, 2014. 38(3): p. 611-620. [CrossRef]
- Titova, O.E., et al., Mediterranean diet habits in older individuals: associations with cognitive functioning and brain volumes. Experimental gerontology, 2013. 48(12): p. 1443-1448. [CrossRef]
- Zhang, H., et al., Meat consumption, cognitive function and disorders: a systematic review with narrative synthesis and meta-analysis. Nutrients, 2020. 12(5): p. 1528. [CrossRef]
- Ylilauri, M.P., et al., Associations of dairy, meat, and fish intakes with risk of incident dementia and with cognitive performance: the Kuopio Ischaemic Heart Disease Risk Factor Study (KIHD). European Journal of Nutrition, 2022. 61(5): p. 2531-2542. [CrossRef]
- Kouvari, M., S. Tyrovolas, and D.B. Panagiotakos, Red meat consumption and healthy ageing: A review. Maturitas, 2016. 84: p. 17-24. [CrossRef]
- Kim, K., et al., Role of total, red, processed, and white meat consumption in stroke incidence and mortality: a systematic review and meta-analysis of prospective cohort studies. Journal of the American Heart Association, 2017. 6(9): p. e005983.
- Wang, Z., et al., Impact of chronic dietary red meat, white meat, or non-meat protein on trimethylamine N-oxide metabolism and renal excretion in healthy men and women. European heart journal, 2019. 40(7): p. 583-594. [CrossRef]
- Quan, W., et al., Association of dietary meat consumption habits with neurodegenerative cognitive impairment: an updated systematic review and dose–response meta-analysis of 24 prospective cohort studies. Food & Function, 2022. 13(24): p. 12590-12601. [CrossRef]
- Stadnik, J., Nutritional Value of Meat and Meat Products and Their Role in Human Health. 2024, MDPI. p. 1446. [CrossRef]
- Juárez, M., et al., Enhancing the nutritional value of red meat through genetic and feeding strategies. Foods, 2021. 10(4): p. 872. [CrossRef]
- IHME, Global Burden of Disease Collaborative Network. Global Burden of Disease Study 2019 (GBD 2019) Results. 2020, Seattle, United States: Institute for Health Metrics and Evaluation (IHME): http://ghdx.healthdata.org/gbd-results-tool.
- The World Bank. How does the World Bank classify countries? 2022 December 24 2022]; Available from: https://datahelpdesk.worldbank.org/knowledgebase/articles/378834-how-does-the-world-bank-classify-countries.
- FAO. FAOSTAT-Food Balance Sheet. 2017 November 26 2022]; Available from: http://faostat3.fao.org/.
- The World Bank. Indicators | Data. 2018; Available from: https://data.worldbank.org/indicator.
- Gaziano, T.A., et al., Growing epidemic of coronary heart disease in low-and middle-income countries. Current problems in cardiology, 2010. 35(2): p. 72-115. [CrossRef]
- You, W. and M. Henneberg, Large household reduces dementia mortality: A cross-sectional data analysis of 183 populations. PloS one, 2022. 17(3): p. e0263309. [CrossRef]
- The World Bank. Life expectancy at birth, total (years). 2022 05 April 2022]; Available from: https://data.worldbank.org/indicator/SP.DYN.LE00.IN.
- You, W. and M. Henneberg, Meat consumption providing a surplus energy in modern diet contributes to obesity prevalence: an ecological analysis. BMC Nutrition, 2016. 2(1): p. 1-11.
- You, W. and M. Henneberg, Meat in modern diet, just as bad as sugar, correlates with worldwide obesity: an ecological analysis. J Nutr Food Sci, 2016. 6(517): p. 4.
- Smith, S., J. Ralston, and K. Taubert. Urbanization and cardiovascular disease- Raising heart-healthy children in today’s cities 2012 December 24 2022]; Available from: https://world-heart-federation.org/wp-content/uploads/2017/05/FinalWHFUrbanizationLoResWeb.pdf.
- Allender, S., et al., Quantification of urbanization in relation to chronic diseases in developing countries: a systematic review. J Urban Health, 2008. 85(6): p. 938-951. [CrossRef]
- You, W. and F. Donnelly, Physician care access plays a significant role in extending global and regional life expectancy. European Journal of Internal Medicine, 2022. [CrossRef]
- You, W., et al., Cutaneous malignant melanoma incidence is strongly associated with European depigmented skin type regardless of ambient ultraviolet radiation levels: evidence from Worldwide population-based data. AIMS Public Health, 2022. 9(2): p. 378. [CrossRef]
- You, W., R. Henneberg, and M. Henneberg, Healthcare services relaxing natural selection may contribute to increase of dementia incidence. Scientific Reports, 2022. 12(1): p. 1-10. [CrossRef]
- You, W., et al., Gluten consumption may contribute to worldwide obesity prevalence. Anthropological Review, 2020. 83(3): p. 327-348. [CrossRef]
- You, W. and M. Henneberg, Relaxed natural selection contributes to global obesity increase more in males than in females due to more environmental modifications in female body mass. PloS one, 2018. 13(7): p. e0199594. [CrossRef]
- WHO. Dementia. 2023 March 20 2024]; Available from: https://www.who.int/news-room/fact-sheets/detail/dementia.
- United Nations Statistics Division. Composition of macro geographical (continental) regions, geographical sub-regions, and selected economic and other groupings. 2013 03.10.2016]; Available from: http://unstats.un.org.
- WHO. WHO regional offices. 2018 11.26.2015]; Available from: http://www.who.int.
- Asia Cooperation Dialogue. Member Countries. 2018; Available from: http://www.acddialogue.com.
- Asia-Pacific Economic Cooperation. Member Economies-Asia-Pacific Economic Cooperation. 2015 [11.26.2015]; Available from: http://www.apec.org.
- The World Bank. Arab World | Data. 2015; Available from: http://data.worldbank.org/region/ARB.
- The United Nations Educational Scientific and Cultural Organization. UNESCO Regions-Latin America and the Caribbean. 2014 [11.26.2015]; Available from: http://www.unesco.org.
- OECD. List of OECD Member countries. 2015; Available from: http://www.oecd.org.
- South Africa Development Community. Southern African Development Community: Member States. 2015 [18.06.2015]; Available from: http://www.sadc.int.
- Shiraseb, F., et al., Red, white, and processed meat consumption related to inflammatory and metabolic biomarkers among overweight and obese women. Frontiers in nutrition, 2022. 9: p. 1015566. [CrossRef]
- Ospina-E, J., et al., Substitution of saturated fat in processed meat products: A review. Critical reviews in food science and nutrition, 2012. 52(2): p. 113-122. [CrossRef]
- Buawangpong, N., et al., Increased plasma trimethylamine-N-oxide levels are associated with mild cognitive impairment in high cardiovascular risk elderly population. Food & Function, 2022. 13(19): p. 10013-10022. [CrossRef]
- Xie, L., et al., Research progress on the association between trimethylamine/trimethylamine-N-oxide and neurological disorders. Postgraduate Medical Journal, 2024. 100(1183): p. 283-288. [CrossRef]
- Zhang, H., et al., Meat consumption and risk of incident dementia: cohort study of 493,888 UK Biobank participants. The American journal of clinical nutrition, 2021. 114(1): p. 175-184. [CrossRef]
- Ngabirano, L., et al., Intake of meat, fish, fruits, and vegetables and long-term risk of dementia and Alzheimer’s disease. Journal of Alzheimer’s Disease, 2019. 68(2): p. 711-722.
- Barberger-Gateau, P., et al., Fish, meat, and risk of dementia: cohort study. Bmj, 2002. 325(7370): p. 932-933.
- Fischer, K., et al., Prospective associations between single foods, Alzheimer’s dementia and memory decline in the elderly. Nutrients, 2018. 10(7): p. 852. [CrossRef]
- De la Monte, S.M., et al., Epidemiological trends strongly suggest exposures as etiologic agents in the pathogenesis of sporadic Alzheimer’s disease, diabetes mellitus, and non-alcoholic steatohepatitis. Journal of alzheimer’s disease, 2009. 17(3): p. 519-529.
- Barnard, N.D., A.E. Bunner, and U. Agarwal, Saturated and trans fats and dementia: a systematic review. Neurobiology of aging, 2014. 35: p. S65-S73. [CrossRef]
- Guo, C.-P., et al., High salt induced hypertension leads to cognitive defect. Oncotarget, 2017. 8(56): p. 95780. [CrossRef]
- Roberts, R.O., et al., Relative intake of macronutrients impacts risk of mild cognitive impairment or dementia. Journal of Alzheimer’s disease, 2012. 32(2): p. 329-339. [CrossRef]
- Liu, J.-L., et al., Iron and Alzheimer’s disease: from pathogenesis to therapeutic implications. Frontiers in neuroscience, 2018. 12: p. 632. [CrossRef]
- Piñero, D.J. and J.R. Connor, Iron in the brain: an important contributor in normal and diseased states. The Neuroscientist, 2000. 6(6): p. 435-453. [CrossRef]
Figure 1.
Polynomial correlation plot of total meat intake and dementia incidence. Data sources and variable definitions: Meat intake, defined as the average annual meat supply per capita (kg/year) over the period 2019–2021, was obtained from the Food and Agriculture Organization. The dementia incidence rate, representing new cases per 100,000 individuals in 2021, was sourced from the Institute for Health Metrics and Evaluation.
Figure 1.
Polynomial correlation plot of total meat intake and dementia incidence. Data sources and variable definitions: Meat intake, defined as the average annual meat supply per capita (kg/year) over the period 2019–2021, was obtained from the Food and Agriculture Organization. The dementia incidence rate, representing new cases per 100,000 individuals in 2021, was sourced from the Institute for Health Metrics and Evaluation.
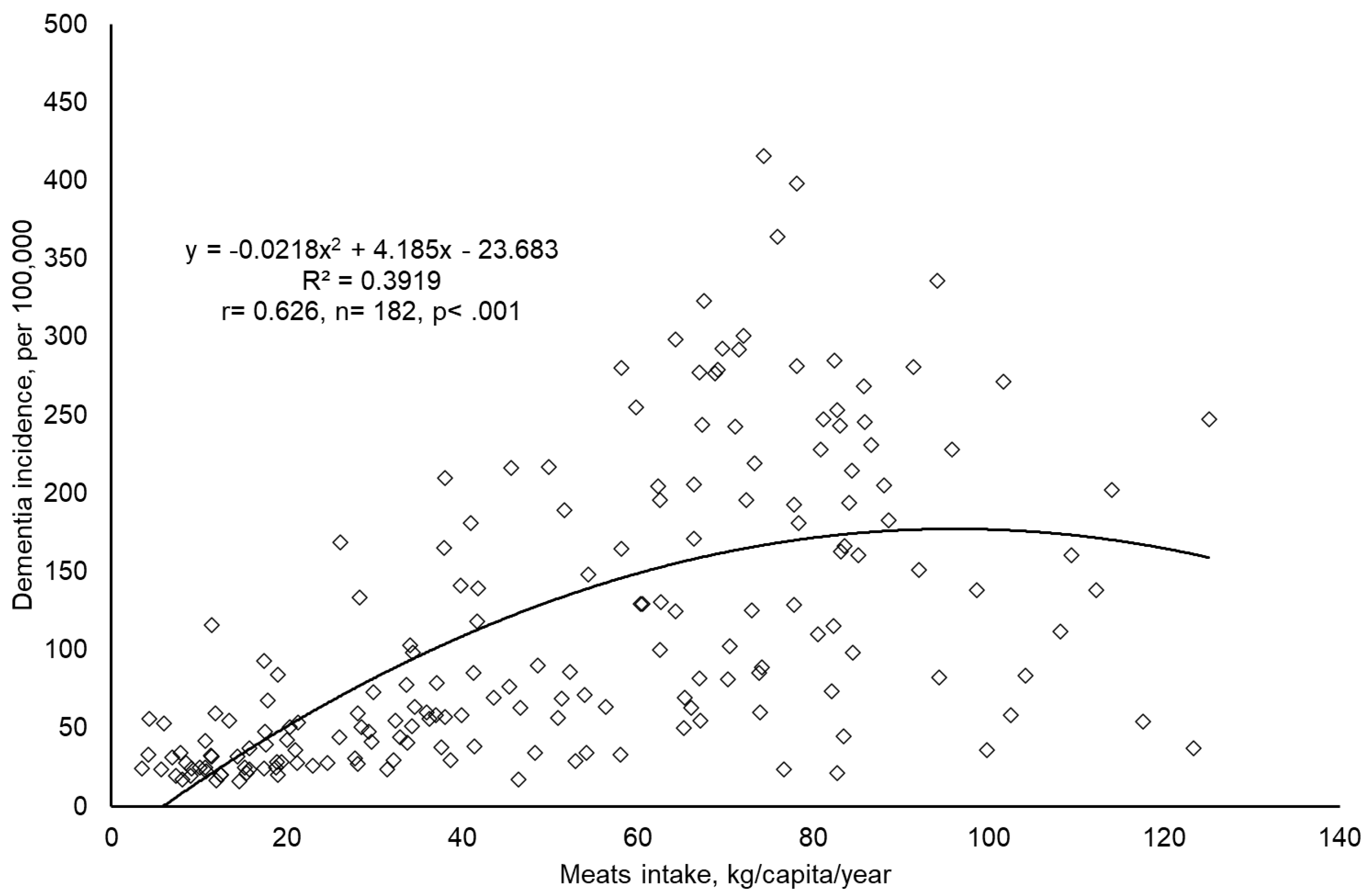

Table 1.
Pearson’s r and nonparametric correlation matrix between all variables.
| Meat intake | Dementia Incidence | Economic Affluence | Genetic Predisposition | Ageing | Urban Living | |
| Meat intake | 1 | .588*** | .622*** | .638*** | .639*** | .562*** |
| Dementia Incidence | .678*** | 1 | .604*** | .606*** | .741*** | .502*** |
| Economic Affluence | .759*** | .777*** | 1 | .567*** | .733*** | .649*** |
| Genetic Predisposition | .751*** | .848*** | .895*** | 1 | .876*** | .523*** |
| Ageing | .682*** | .829*** | .880*** | .930*** | 1 | .604** |
| Urban Living | .578*** | .525*** | .720*** | .630*** | .640*** | 1 |
Correlations were evaluated using Pearson’s r (above the diagonal) and nonparametric methods (below the diagonal). Statistical significance is denoted as ***p < 0.01, with the number of countries ranging between 176 and 204. Data sources and variable definitions: Meat intake, defined as the average annual meat supply per capita (kg/year) over the period 2019–2021, was obtained from the Food and Agriculture Organization. The dementia incidence rate, representing new cases per 100,000 individuals in 2021, was sourced from the Institute for Health Metrics and Evaluation. The measure for genetic predisposition to dementia was based on the Biological State Index by You & Henneberg (2022). Economic affluence was represented by per capita GDP, adjusted for purchasing power parity (PPP), as reported by the World Bank (2018). Aging was assessed through life expectancy at birth, and urbanization was quantified by the proportion of the population residing in urban areas, both sourced from the World Bank (2018).
Table 2.
Partial correlations of dementia incidence with variables, considering meat intake as both independent variable and confounder.
Table 2.
Partial correlations of dementia incidence with variables, considering meat intake as both independent variable and confounder.
| Variables | Partial Correlation to Dementia Incidence | Partial Correlation to Dementia Incidence | ||||
| r | P | df | r | p | df | |
| Meat intake | .227 | < .010 | 170 | - | - | - |
| Economic Affluence | - | - | - | .376 | <.001 | 173 |
| Genetic Predisposition | - | - | - | .372 | <.001 | 176 |
| Ageing | .587 | <.001 | 178 | |||
| Urban Living | - | - | - | .257 | <.001 | 178 |
Data sources and variable definitions: Meat intake, defined as the average annual meat supply per capita (kg/year) over the period 2019–2021, was obtained from the Food and Agriculture Organization. The dementia incidence rate, representing new cases per 100,000 individuals in 2021, was sourced from the Institute for Health Metrics and Evaluation. The measure for genetic predisposition to dementia was based on the Biological State Index by You & Henneberg (2022). Economic affluence was represented by per capita GDP, adjusted for purchasing power parity (PPP), as reported by the World Bank (2018). Aging was assessed through life expectancy at birth, and urbanization was quantified by the proportion of the population residing in urban areas, both sourced from the World Bank (2018). - Included as the confounding factor.
Table 3.
Results of multiple linear regression analyses to sort significant predictors of dementia incidence.
Table 3.
Results of multiple linear regression analyses to sort significant predictors of dementia incidence.
| Table 3-1: ENTER | Excluding Meat Intake | Including Meat Intake | |||
| Variables Entered | Beta | Sig. | Beta | Sig. | |
| Meats intake | Not added | Not applicable | .202 | < .001 | |
| Economic Affluence | .063 | .447 | .082 | < .010 | |
| Genetic Predisposition | - .141 | .201 | - .183 | .344 | |
| Ageing | .788 | < .001 | .721 | .113 | |
| Urban Living | .043 | .525 | - .017 | < .001 | |
| Table 3-1: STEPWISE | Meat Intake not Added | Meat Intake Added | |||
| Rank | Variables Entered | Adjusted R Square | Rank | Variables Entered | Adjusted R Square |
| 1 | Ageing | .539 | 1 | Ageing | .544 |
| Meats Intake | Not significant | 2 | Meats Intake | .563 | |
| Genetic Predisposition | Not significant | 3 | Genetic Predisposition | .571 | |
| Economic Affluence | Not significant | Economic Affluence | Not significant | ||
| Urban Living | Not significant | Urban Living | Not significant | ||
Stepwise multiple linear regression modelling is reported. Contribution of variables is listed in order of how much they contribute to dementia incidence. Data sources and variable definitions: Meat intake, defined as the average annual meat supply per capita (kg/year) over the period 2019–2021, was obtained from the Food and Agriculture Organization. The dementia incidence rate, representing new cases per 100,000 individuals in 2021, was sourced from the Institute for Health Metrics and Evaluation. The measure for genetic predisposition to dementia was based on the Biological State Index by You & Henneberg (2022). Economic affluence was represented by per capita GDP, adjusted for purchasing power parity (PPP), as reported by the World Bank (2018). Aging was assessed through life expectancy at birth, and urbanization was quantified by the proportion of the population residing in urban areas, both sourced from the World Bank (2018).
Table 4.
Meat intake correlated to dementia incidence in various country groupings.
| Country Groupings | Pearson r | p | Nonparametric | p | n |
| Worldwide | .588 | < .001 | .678 | < .001 | 182 |
| United Nations common practice | |||||
| Developed countries | .098 | .526 | - .004 | .978 | 44 |
| Developing countries | .496 | . < .001 | .604 | < .001 | 138 |
| Fisher r-to-z transformation | Developing vs Developed:z= 2. 5, p < .010 | Developing vs Developed:z= 3.94, p < .001 | |||
| World Bank income classifications | |||||
| High Income (HI) countries | -.073 | .598 | -.129 | .353 | 54 |
| Low Income (LI) countries | .184 | .349 | .236 | 0.226 | 28 |
| Low Middle Income (LMI) countries | .368 | < .010 | .478 | < .001 | 49 |
| Upper Middle Income (UMI) countries | .198 | .165 | .260 | .066 | 51 |
| Low- and middle-income countries (LI, LMI, UMI) | .521 | < .001 | .668 | < .001 | 128 |
| Fisher r-to-z transformation | Low- and middle-income vs High: z= 3.92, p< .001 | Low- and middle-income vs High: z= 5.64, p< .001 | |||
| WHO regions | |||||
| African region countries | .587 | < .001 | .453 | < .010 | 45 |
| American region countries | .578 | < .001 | .590 | < .001 | 35 |
| Eastern Mediterranean region countries | - .095 | .682 | .113 | .626 | 21 |
| European region countries | .471 | < .001 | .348 | < .050 | 50 |
| South-East Asian Region countries | .197 | .585 | .321 | .365 | 10 |
| Western Pacific Region countries | .302 | .183 | .183 | .427 | 21 |
| Countries grouped with various factors | |||||
| Asia Cooperation Dialogue (ACD) | .150 | .456 | .002 | .990 | 27 |
| Asia-Pacific Economic Cooperation (APEC) | .658 | < .010 | .696 | < .010 | 17 |
| Arab World | - .185 | .423 | - .061 | .793 | 21 |
| English as official language (EOL) | .651 | < .001 | .775 | < .001 | 51 |
| Latin America (LA) | .640 | < .001 | .723 | < .001 | 23 |
| Latin America and the Caribbean (LAC) | .491 | < .010 | .538 | < .001 | 33 |
| Organization for Economic Cooperation and Development (OECD) | - .035 | .838 | - .143 | .407 | 36 |
| Southern African Development Community (SADC) | .685 | < .010 | .553 | < .050 | 16 |
Bivariate correlations (Pearson r and nonparametric) between meat intake and dementia incidence within country groupings were reported. Data sources and variable definitions: Meat intake, defined as the average annual meat supply per capita (kg/year) over the period 2019–2021, was obtained from the Food and Agriculture Organization. The dementia incidence rate, representing new cases per 100,000 individuals in 2021, was sourced from the Institute for Health Metrics and Evaluation.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



