Submitted:
25 December 2024
Posted:
26 December 2024
You are already at the latest version
Abstract
Background/Objectives: Gender differences in nutrition-related determinants of mild cognitive impairment (MCI) exist among the elderly. This study aimed to explore gender-specific influencing factors of MCI. Methods: A nested case-control study was conducted in 2020, involving 1086 elderly people aged 55 years and above from 4 sites in Zhejiang Province, China. Data on demographics, cognitive assessment, depression scale, daily food intake and physical examinations were collected. The assessment of plant-based diets pattern depended on an overall plant-based diet index (PDI), a healthful plant-based diet index (hPDI), and an unhealthful plant-based diet index (uPDI). Multivariate logistic regression models were employed to assess the determinants of MCI in females and males. Results: Among 571 females, 141 (24.7%) had MCI, and 126 (24.5%) had MCI among 514 male participants. In females, the multivariate analysis revealed that being unmarried/divorced/widowed (OR = 1.949, 95% CI: 1.102 - 3.445), having depression (OR = 6.061, 95% CI: 1.868 - 19.660), and having a uPDI score ≥ 55 (OR = 2.412, 95% CI: 1.498 - 3.885) were associated with a significantly elevated risk of MCI. Conversely, a cereal consumption of ≥ 300g (OR = 0.318, 95% CI: 0.193 - 0.526) was linked to a significantly reduced risk. In males, vegetable consumption ≥ 150g (OR = 0.391, 95% CI: 0.232 - 0.658), vegetable oil consumption ≥ 22g (OR = 0.502, 95% CI: 0.307 - 0.820), and cereal consumption ≥ 300g (OR = 0.438, 95% CI: 0.271 - 0.709) were associated with a lower MCI risk. Meanwhile, rural residence (OR = 1.904, 95% CI: 1.116 - 3.249) and advanced age, especially 75 years old and above (OR = 4.713, 95% CI: 2.437 - 9.117), were also risk factors in males. Notably, Restricted Cubic Spline (RCS) model showed that females with a uPDI score < 55 had a lower prevalence of MCI, while those with a score ≥ 55 faced a higher risk. Conclusions: This study indicates potential gender disparities in the risk factors for MCI. Future research should prospectively establish causal relationships. Additionally, precise intervention strategies are urgently needed.
Keywords:
mild cognitive impairment
; elder people
; nutrition
; gender
; determinant
1. Introduction
The issue of global aging is becoming increasingly severe. In 2020, 9% of the global population was aged 65 years and older[1]. In 2021, China transitioned into an aged society as the proportion of its elderly population (aged 65 years and above) surpassed 14%.[2]. The health risks entailed by aging can impose substantial burdens on families, health systems, and society. Dementia is a primary age-related disease, particularly Alzheimer's disease (AD). According to the 2019 Global Burden of Disease Study, AD is the leading cause of death in people over 75 years of age[3]. Incidence rates in people over 65 and 85 are 5% and more than 30%, respectively[4]. There are an estimated 50 million worldwide, including 10 million in China. It is estimated that there will be about 130 million Alzheimer’s patients worldwide by 2050[4]. To date, no effective cure is available to delay the progression of AD. Therefore, primary prevention of Alzheimer's disease (AD) is of crucial importance. Mild cognitive impairment (MCI) is an intermediate stage between the expected cognitive decline of normal aging and dementia, the most typical one in which is Alzheimer's disease (AD)[5]. Ten percent to 20% of patients with MCI progress to manifest dementia within 12 months of diagnosis[6]. Exploring the influencing factors of MCI, identifying high-risk groups, providing early warnings, and paying close attention are the keys to preventing AD.
Nutrition plays a crucial and indispensable role in the senescence process of the brain. [7]. Hence, it is critical to explore the evidence on the association between nutrition-related factors and MCI risk in the elderly population to shift focus towards prevention methods of this pre-dementia phase of AD. The associations between dietary and cognitive functions have continuously captured the attention of the general public. Particular attention has been dedicated to fresh vegetables and fruits since they serve as outstanding sources of antioxidant nutrients, including vitamin C, vitamin E, and carotenoids. Moreover, the consumption of fish and nuts has been given emphasis due to their abundance in unsaturated fatty acids, which have been empirically proven to exhibit anti-inflammatory benefits[8,9,10,11]. A stronger adherence to a Mediterranean-style dietary pattern correlates with a diminished risk of contracting Alzheimer's disease and a decelerated rate of cognitive decline as one ages[12]. Some studies have demonstrated that consuming higher amounts of LC ω3 PUFAs could be a preventative strategy against Alzheimer's disease, and it is most effective when dietary LC ω3 PUFAs are consumed prior to or in the early stages of cognitive decline[13]. In addition to the research reports on the association between food nutrient intake and MCI, there are also research reports on the relationship between human nutritional status and MCI. A systematic review and meta-analysis reported that the prevalence of MCI is relatively high in patients with sarcopenia, and sarcopenia may be a risk factor for MCI[14]. Although some research reports have emerged regarding the nutrition-related influencing factors of MCI, the consistency within the available evidence remains inadequate. Moreover, few studies have been dedicated to comparing the disparities in the nutrition-related influencing factors of MCI between males and females, which is due to the fact that women and men both have distinct physiological status, endocrine system and especially dietary habits and exhibit differences in the prevalence of general medical conditions including cognitive domain. It has already been reported that women and men have different risks of cognitive impairment[15,16,17,18]. However, it remains inconclusive differences in nutrition-related predictive factors or preventable influencing factors of MCI between different genders. This study aimed to explore the nutrition-related influencing factors of MCI between males and females by using the method of nested case-control study, thereby achieving precise prevention of MCI.
2. Materials and Methods
2.1. Study Design
Data in the present study were derived from the follow-up of Community-based Cohort Study on Nervous System Diseases, which focused on potential factors associated with risks of three nervous diseases, including epilepsy for subjects aged > 1 year, and AD and Parkinson’s disease in ≥55 year-old population[19]. Present study targeted at subjects recruited in the cohort of AD. In Zhejiang Province, the field investigation and physical examination were conducted in September 2020. Protocol of this project was reviewed and approved by Medical Ethics Committee of National Institute for Nutrition and Health, Chinese Center for Disease Control and Prevention (No. 2017020, 6 November 2017). And written informed consent was obtained for. Each participant provided written informed consent after the research protocols were carefully explained to them.
2.2. Sampling Method and Study Population
Participants without such diagnosed diseases were recruited using a multistage stratified random sampling approach in baseline. In Zhejiang Province, there were four study sites that represented both urban and rural areas across the province. Subsequently, two cities and two counties were randomly selected in each province. Urban and suburban neighborhoods within the cities, and townships and villages within the counties were selected randomly. Finally, all members meeting the inclusion and exclusion criteria of any of three nervous diseases in a randomly selected household were interviewed[19].
In this study, the eligible samples for inclusion were (1) 55 years old and older, (2) resident population living in the sampled community, (3) free of comorbid conditions that could affect assessment, such as congenital or acquired mental retardation, and visual/hearing abnormalities even after correction[19]. According to the definition of MCI, we excluded subjects because of their inability to perform basic activities of daily living involving eating, dressing, bathing, toileting, grooming, transferring bed or chair, walking across a room, and urinary or fecal continence. For participants locating in the part of <P1 or > P99 (P: percentile) of sleep duration distribution in each age group, we used the corresponding P1 and P99 to replace those of <P1 or > P99, respectively. Finally, a total of 1086 participants were involved in the analysis.
2.3. Data Collection
Investigators with a degree in medicine or public health were required, and received two rounds of training conducted by national experts and provincial professionals, respectively. Then, those who passed a qualification test were appointed to collect information through questionnaires and physical examinations. Questionnaires survey was used to collect basic and health related data regarding age, educational level, occupation, marriage, cognitive assessment, depression scale and dietary information including daily consumption of 81 categories of food through Food Frequency Questionnaire (FFQ). Physical examinations, including height, weight, waist circumference, grip strength, 6-metre gait speed and body composition, were carried out by trained health workers from the local community health center.
2.4. Cognitive Function Assessment
The cognitive function of participants was evaluated using the Montreal Cognitive Assessment (MoCA), which was valid and reliable among Chinese by taking cultural and linguistical differences into account[20,21]. The cultural and linguistic modifications of MoCA Beijing version we used from the original English version were also concretely described[22]. MoCA were conducted strictly face to face following the guidelines and protocols by trained investigators and were completed during 5-10 min and 10-15 min, respectively. The MoCA included 52 items, of which scores of 32 items were calculated for the total MoCA scores ranging from 0 to 30 points which were positively associated with global cognitive function[23]. The criteria for MCI were according to Chinese MoCA norms[21]: total MoCA score ≤13 for illiterate individuals, ≤19 for individuals with 1 to 6 years of education, and ≤24 for those with 7 or more years of education.
2.5. Plant-Based Diet Indices and Dietary Assessment
Extract 18 types of plant-based dietary related foods from the 81 categories of foods in FFQ. The assessment of healthful and unhealthful plant-based diets depended on an overall plant-based diet index (PDI), a healthful plant-based diet index (hPDI), and an unhealthful plant-based diet index (uPDI)[24]. Food groups were ranked into quintiles, and given positive or reverse scores. With positive scores, participants above the highest quintile of a food group received a score of 5, following on through to participants below the lowest quintile who received a score of 1. With reverse scores, this pattern of scoring was inversed. For creating PDI, plant food groups were given positive scores, while animal food groups were given reverse scores. For creating hPDI, positive scores were given to healthy plant food groups, and reverse scores to less healthy plant food groups and animal food groups. Finally, for uPDI, positive scores were given to less healthy plant food groups, and reverse scores to healthy plant food groups and animal food groups. The 18 food group scores were summed to obtain the indices. The grouping cut-off values of cereals, vegetables, fruits, soybean and their products, vegetable oils and nuts were determined through the RCS model. Strong tea grouped according to whether it had been drunk.
2.6. Assessment of Covariates
Geriatric Depression Scale (GDS) was used in this study to screen depressive symptoms. We adopted 11, recommended by the developer and employed in most studies, as the cutoff value for screening depressive symptoms[25]. Central obesity is defined as a waist circumference of ≥90 cm for men and ≥85 cm for women according to the criteria of weight for adults in China[26]. Body Mass Index (BMI) was calculated by dividing weight (in kilograms) by the square of height (in meters), and then the subjects were categorized into three groups[27] (lean: <18.5; normal: 18.5-23.9; overweight/obesity: ≥24 kg/m2). Muscle mass was measured by bioelectrical impedance analysis (BIA) using an TANITA 601 (Tanita Corporation of America, Inc, Arlington Heights, IL) device. Appendicular skeletal muscle mass (ASM) was defined as the mass of skeletal muscle in the arms and legs. ASM was standardized by height expressed in meters squared to yield skeletal muscle mass index (SMI) (kg/m2). Muscle strength was assessed by handgrip strength, measured using a digital grip strength dynamometer (CAMRY EH 101). These measurements were taken in each hand, and only the highest value was recorded. The physical performance was evaluated by 6 min gait speed; the average of two tests was used. The recommendations of the AWGS2019 [28] consensus were followed. This consensus defines sarcopenia with low muscle mass and low muscle strength or performance. Low muscle mass combined with low muscle strength and low physical fitness is considered as severe sarcopenia. Low muscle mass is defined as the ASM index.
2.7. Statistical Analyses
Mean and standard deviations (mean±SD) were used to described continuous normal variables, and median and quartile (median (quartile)) were used for variables with skewed distribution. Frequency and percentage (%) were reported for the categorical variables. Categorical variables were compared using the chi-square test. A series of multiple logistic regression models were conducted to assess the odds ratio (OR) and 95% confidence interval (CI) levels of potential influencing factors, including age, educational level, occupation, marriage, depressive symptoms, daily consumption of coffee, nuts, strong tea, chocolate, overweight/obesity, central obesity, sarcopenia and incidence of MCI. Additionally, the figures were plotted based on Restricted Cubic Spline (RCS) Model. All statistical analyses were performed by using the program SAS version 9.1. p less than 0.05 was considered statistically significant.
3. Results
3.1. Basic Information
A total of 1086 elderly people aged 55 and above, among whom there were 514 men and 572 women, were enrolled in the current study. The main characteristics of the participants are presented in Table 1. Overall, the prevalence of MCI in women was 24.7%, which in men was 24.5%.
3.2. Nutrition-Related Determinants of MCI in Female and Male
Based on the results of the existing research evidence and univariate analysis, region, age, educational level, marriage, intakes of cereals, vegetables, fruits, soybean, nuts and vegetable oils, uPDI, hPDI and sarcopenia were included in the multivariate analysis. Multivariate analysis showed that among all the elderly population cereal intake was associated with MCI in Table 2 and Table 3. Meanwhile, depression, unmarried/ divorced/widowed and high uPDI were risk factors for MCI only in female elderly people, while residing in urban and appropriate intakes of vegetables and vegetable oil were protective factor for MCI only in males. The risk of MCI in females were higher with depression (OR=6.061, 95% CI: 1.868~19.660) or not married (OR=1.949, 95% CI: 1.102~3.445). Consumption of cereal ≥300g (OR=0.318, 95% CI: 0.193~0.526) was associated with a lower MCI risk in females. The risk of MCI in males were higher with residing in rural areas (OR=1.904, 95% CI: 1.116~3.249) and increasing age. Consumption of vegetables ≥150 g (OR=0.391, 95% CI: 0.232~0.658), consumption of vegetable oil ≥22 g (OR=0.502, 95% CI: 0.307~0.820), consumption of cereal ≥300 g (OR=0.438, 95% CI: 0.271~0.709), were linked to a significantly reduced risk in males. Appropriate cereal intake was a nutrition-related protective factor against MCI for both female and male, while high uPDI was to have a risk effect only among female, and appropriate intake of vegetables and vegetable oil was found to have a protective effect only among male.
3.3. Analysis on the Association between Plant-Based Diets and MCI in Female and Male
In the univariate analysis, we found that among women, low PDI (p=0.037), low hPDI (p=0.032) and high uPDI (p=0.0002) were significantly associated with MCI. Among men, only high uPDI (p=0.0058) was significantly associated with MCI. After adjusting for other factors, multivariate analysis showed that uPDI was a risk factor for MCI in female. RCS was established for the relationship between the uPDI and MCI by adjusting the factors including age, educational level, depression, and cereal intake in Figure 1. Females with a uPDI score < 55 had a lower prevalence of MCI, while those with a score ≥ 55 faced a higher risk. After using 55 as the cut-off value for uPDI, the results of the multivariate analysis showed that uPDI score≥55 (OR=2.412, 95% CI: 1.498~3.885) was associated with increased risk of MCI in female.
4. Discussion
Considering that there is no cure for AD, it is particularly important to carry out primary prevention and early warning for MCI previous to AD. Nutrition, as one of the important influencing factors, had drawn the attention of scholars. In order to achieve precise prevention, it is crucial to explore the risk factors for MCI in different genders. However, to date, such research is lacking. This study aimed to explore the nutrition-related influencing factors of MCI between males and females by using the method of nested case-control study, thereby achieving precise prevention of MCI. In this study, among 571 females, 141 (24.7%) had MCI, and 126 (24.5%) had MCI among 514 male participants. In females, the multivariate analysis revealed that being unmarried/divorced/widowed, having depression, and having a uPDI score ≥ 55 were associated with a significantly elevated risk of MCI. Conversely, a cereal consumption of ≥ 300g was linked to a significantly reduced risk. In males, vegetable consumption ≥ 150g, vegetable oil consumption ≥ 22g, and cereal consumption ≥ 300g were associated with a lower MCI risk. Meanwhile, rural residence and advanced age, especially 75 years old and above, were also risk factors in males. Notably, RCS model showed that females with a uPDI score < 55 had a lower prevalence of MCI, while those with a score ≥ 55 faced a higher risk.
In methods, both the Mini-Mental State Examination (MMSE) and the MoCA were used simultaneously to screen for MCI in this research survey. However, the MoCA scale was employed to assess MCI. The reason was that our research team had conducted a study on comparison of the MMSE with the MoCA for mild cognitive impairment screening in Chinese middle-aged and older population suggested that MoCA is a better measure of cognitive function due to lack of ceiling effect and with good detection of cognitive heterogeneity[29].
Synthesizing the existing research evidence so far, at the same time, considering the preference differences in dietary choices between men and women, the factors to be included in the analysis were selected. Since plant-based foods can provide rich antioxidant nutrients and play a significant role in the aging process of the brain, the plant-based diet pattern as well as some food types related to antioxidant and anti-inflammatory effects were introduced in this study, including vegetable, fruit, nuts and vegetable oil. Some research reports in European and American regions suggest that caffeine and chocolate are protective factors against AD. A cohort study suggested that low caffeine intake is associated with higher risk of being amnestic in MCI/AD patients, and Caffeine intake is associated with CSF biomarkers in AD patients[30]. A Spain nested case - control study suggested that habitual dark chocolate consumption might improve cognitive function among the older population[31]. However, it was found in the frequency statistics that the number of Chinese people consuming coffee and chocolate was too small, so they were not included in the analysis. Strong tea is a beverage that Chinese elderly people are quite fond of, and there is also a certain amount of caffeine in strong tea. Therefore, strong tea was analyzed as influencing factor in this study. A study conducted in Japan has indicated that a dietary pattern with a relatively high protein intake is correlated with favorable cognitive function among the elderly population in Japan[32]. Therefore, milk, soybean and meat were analyzed, but only soybeans showed significance in the univariate analysis. Some studies reported[33,34,35] that simple carbohydrates such as sucrose (glucose and fructose) may have an immediate effect on cognition, diets high in complex carbohydrates, such as fruits and cereals, are associated with better cognitive function and a lower risk of dementia in the longer term, so in this study cereal and sweet food were included. However, the consumption of sweet food among Chinese elderly people is very low, and the results were not significant. Meta-analysis reported that the prevalence of MCI is relatively high in patients with sarcopenia, and sarcopenia may be a risk factor for MCI[14].Overall, plant-based diet indices (PDI, hPDI and uPDI), cereal, vegetables, fruit, soybean, vegetable oil, nuts, strong tea and sarcopenia were analyzed in this study. Based on the risk factors of MCI reported in previous studies, factors such as region, age, education level, marital status, living alone, occupation, BMI, and depression were included as adjustment factors. It was reported that loneliness may mediate the relationship between depression and the quality of life among elderly with MCI.
As this study showed, residing in rural areas and older age, especially aged 75 and above were risk factors of MCI, which was consistent with most of the current research evidence[36,37]. However, residing in rural areas as a risk of MCI only observed in males, which needed further exploring the reasons. The educational level, which is a common influencing factor of MCI reported in previous studies, showed no significance in our study. It was most likely related to the fact that the proportion of the elderly with a high educational level included in this study was very low and the distribution of educational levels was unbalanced. unmarried/ divorced/widowed and depression were reported as risk factors of MCI only in elder females. Women with depressive symptoms have a six - times - greater risk of MCI than women without depressive symptoms. The result was consistent with the previous research report that depression is a risk factor for MCI among women[38], which may be caused by the relatively high incidence of depression among women[39]. However, the OR was a little higher than the depression relative risk (RR) and OR of mild MCI reported in current cohort and cross-sectional data[38,40,41]. It was reported that loneliness may mediate the relationship between depression and the quality of life among elderly with MCI. Therefore, not being in a marital status may be a risk factor for depression. Moreover, findings suggested that among older adults with MCI, being married may be a protective factor and being unmarried may be a risk factor for experiencing loneliness and subsequent intrusive thoughts[42]. Therefore, marriage and depression were both included in the multivariate analysis to rule out the interference of collinearity and the results demonstrated that both factors were risk factors for MCI among women. The analysis of the common risk factors for MCI in different genders as mentioned above indicated a relatively high data reliability and was in good consistency with previous studies[16]. There were few reports on the correlation analysis between the plant - based diet pattern and MCI in previous studies. Consequently, this represents a relatively novel research endeavor. A study on association between plant-based dietary patterns and cognitive function in middle-aged and older residents of China demonstrated that there was a significant association between higher uPDI scores and higher odds of MCI, with Quintile 4 compared with Quintile 1 showing an odds ratio of 2.21[43], which it was similar to the results of our research. Compared with this research, our advantage lies in the fact that we have a larger sample size. Moreover, the possible influencing factors of MCI that we used for correction are more comprehensive, such as depression. More importantly, we found that in the correlation analysis between the plant-based diet pattern and MCI, the plant-based diet pattern was significant as an influencing factor only in women. Hence, females with an unhealthy plant-based dietary pattern are among the high-risk groups for MCI. Furthermore, it is worth noting that there is an interesting phenomenon that females with a uPDI score < 55 had a lower prevalence of MCI, while those with a score ≥ 55 faced a higher risk. This can provide a basis for the dietary guidance and suggestions for the high - risk population of MCI. we found that a low intake of cereals might be a risk factor for MCI in two genders. At present, there were hardly any correlational studies on cereals and MCI, but only on carbohydrates and MCI[33,34]. Research on food types is of greater public health significance compared to nutrients. It can not only provide a basis for the Chinese Dietary Guidelines or the Food Pagoda but also offer references for the dietary intake of elderly people. The influence of the rational consumption of vegetable oils and vegetables on MCI exhibits a disparity in genders. Whether this gender difference is caused by different physiological functions between men and women or food - preference still requires further investigation. Existing research reported that consuming PFBc in vegetable oil might enhance cognitive function via its anti-inflammatory antioxidant functions[44]. However, the threshold value for the intake of vegetable oil has not been reported. The threshold value of 22 g obtained through the RCS curve in this study showed a significant difference in the risk of MCI. In the research on the association between vegetable intake and MCI, there is relatively little quantitative comparison of vegetable intake, and most of it is in the form of semi-quantitation such as frequency or quantile distribution[9,45,46]. Therefore, the strength of this study was providing a scientific basis for dietary recommendations for the prevention of MCI.
There were several strengths in our study. Firstly, this study explored the nutrition-related influencing factors of MCI, especially explored the association between plant-based dietary patterns and MCI. Secondly, this study compared the differences in general influencing factors and nutrition-related influencing factors of MCI between different genders, and, to date, only a limited number of similar studies have been reported. Finally, the quantitative cut-off value of the effects of uPDI in the plant-based dietary pattern, cereal, vegetables, and vegetable oils on MCI are reported in the study.
However, this study has the following limitations, and caution should be exercised in interpreting and extrapolating the results. Firstly, a nested case-control design was adopted in this study. Consequently, this design can only suggest the possible influencing factors for MCI and cannot clarify the causal relationships. Secondly, the information such as dietary data were self-reported and might have been influenced by recall bias. Thirdly, the cognitive level status may vary at different periods and under different interventions. Since this study only selected single sample, it cannot objectively present the dynamic change process. Future studies can collect the results of multiple blood samples as well as information on interventions. Finally, the sample size was limited, resulting in relatively wide confidence intervals. For example, educational levels as an influencing factors of MCI distributed unbalance, making it difficult to interpret the results. Therefore, it is still necessary to conduct larger-scale studies in the future.
5. Conclusions
To summarize, this study indicates potential gender disparities in the risk factors for MCI. Women who are not in a marital status, or depressed, or have a low uPDI score, or have a low intake of grains, along with men living in rural areas or having a relatively low intake of grains, vegetables, and vegetable oils, constitute the key populations that merit particular attention regarding MCI. Future research should prospectively establish causal relationships. Additionally, precise intervention strategies are urgently needed.
Author Contributions
Yan Zou conceptualized and designed the study, Mengjie He, Danting Su, Dong Zhao, Ronghua Zhang and Dan Han conduct on-site investigations, Mengjie He, Peiwei Xu and Lichun Huang analyzed the data; Mengjie He wrote the paper; and Yan Zou were responsible for the study. All authors have read and agreed to the published version of the manuscript.
Funding
This research was supported by the Ministry of Finance of China, the National Key R&D Program of China, Precision Medicine Project-Cohort Study on Nervous System Diseases (2017YFC0907700), Community-based Cohort Study on Nervous System Diseases (2017YFC0907701). All funders had no role in the design, analysis, or writing of this article.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Institutional Review Board of the Chinese Center for Disease Control and Prevention (protocol code No. 2017020 and approval date 6 November 2017).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data presented in this study are available on request from the corresponding author. The data are not publicly available due to privacy and ethical concerns in this survey.
Acknowledgments
The authors would like to thank all the participants who took part in this study, especially nutrition monitoring surveyors from local CDCs in 4 regions. In addition, sincere gratitude was given to Dr. Wang Le from Zhejiang Cancer Hospital for his support in the suggestion on statistical methods of this article.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Behr L C, Simm A, Kluttig A, et al. 60 years of healthy aging: On definitions, biomarkers, scores and challenges[J]. Ageing Research Reviews, 2023,88:101934. [CrossRef]
- Zhao L. A review of healthy aging in China, 2000–2019[J]. Health Care Science, 2022,1(2):111-118. [CrossRef]
- V N. Global burden of 369 diseases and injuries in 204 countries and territories, 1990-2019: a systematic analysis for the Global Burden of Disease Study 2019[J]. Lancet, 2020,396(10258):1204-1222. [CrossRef]
- Cao Y, Yu F, Lyu Y, et al. Promising candidates from drug clinical trials: Implications for clinical treatment of Alzheimer's disease in China[J]. Frontiers in Neurology, 2022,13. [CrossRef]
- DeCarli C. Mild cognitive impairment: prevalence, prognosis, aetiology, and treatment.[J]. The Lancet. Neurology., 2003(1):15-21.
- Petersen R C, Roberts R O, Knopman D S, et al. Mild cognitive impairment: ten years later[J]. Arch Neurol, 2009,66(12):1447-1455. [CrossRef]
- Flanagan E, Lamport D, Brennan L, et al. Nutrition and the ageing brain: Moving towards clinical applications[J]. Ageing Res Rev, 2020,62:101079. [CrossRef]
- Solfrizzi V, Custodero C, Lozupone M, et al. Relationships of Dietary Patterns, Foods, and Micro- and Macronutrients with Alzheimer's Disease and Late-Life Cognitive Disorders: A Systematic Review[J]. J Alzheimers Dis, 2017,59(3):815-849. [CrossRef]
- Ngabirano L, Samieri C, Feart C, et al. Intake of Meat, Fish, Fruits, and Vegetables and Long-Term Risk of Dementia and Alzheimer's Disease[J]. J Alzheimers Dis, 2019,68(2):711-722. [CrossRef]
- Li M, Shi Z. A Prospective Association of Nut Consumption with Cognitive Function in Chinese Adults aged 55+ _ China Health and Nutrition Survey[J]. J Nutr Health Aging, 2019,23(2):211-216. [CrossRef]
- Zhang Y, Chen J, Qiu J, et al. Intakes of fish and polyunsaturated fatty acids and mild-to-severe cognitive impairment risks: a dose-response meta-analysis of 21 cohort studies[J]. Am J Clin Nutr, 2016,103(2):330-340. [CrossRef]
- Kuczmarski M F, Allegro D, Stave E. The association of healthful diets and cognitive function: a review[J]. J Nutr Gerontol Geriatr, 2014,33(2):69-90. [CrossRef]
- Wood A H R, Chappell H F, Zulyniak M A. Dietary and supplemental long-chain omega-3 fatty acids as moderators of cognitive impairment and Alzheimer's disease[J]. Eur J Nutr, 2022,61(2):589-604. [CrossRef]
- Yang Y, Xiao M, Leng L, et al. A systematic review and meta-analysis of the prevalence and correlation of mild cognitive impairment in sarcopenia[J]. J Cachexia Sarcopenia Muscle, 2023,14(1):45-56. [CrossRef]
- Sachdev P S, Lipnicki D M, Crawford J, et al. Risk profiles for mild cognitive impairment vary by age and sex: the Sydney Memory and Ageing study[J]. Am J Geriatr Psychiatry, 2012,20(10):854-865. [CrossRef]
- Lee L K, Shahar S, Chin A, et al. Prevalence of gender disparities and predictors affecting the occurrence of mild cognitive impairment (MCI)[J]. Arch Gerontol Geriatr, 2012,54(1):185-191. [CrossRef]
- Song M, Wang Y, Wang R, et al. Prevalence and risks of mild cognitive impairment of Chinese community-dwelling women aged above 60 years: A cross-sectional study[J]. Arch Womens Ment Health, 2021,24(6):903-911. [CrossRef]
- Xu S, Xie B, Song M, et al. High prevalence of mild cognitive impairment in the elderly: a community-based study in four cities of the Hebei province, china[J]. Neuroepidemiology, 2014,42(2):123-130. [CrossRef]
- Huang Q, Jia X, Zhang J, et al. Diet–Cognition Associations Differ in Mild Cognitive Impairment Subtypes[J]. Nutrients, 2021,13(4):1341. [CrossRef]
- Katzman R, Zhang M Y, Ouang-Ya-Qu, et al. A Chinese version of the Mini-Mental State Examination; impact of illiteracy in a Shanghai dementia survey[J]. Journal of clinical epidemiology, 1988,41(10):971. [CrossRef]
- Lu J, Li D, Li F, et al. Montreal Cognitive Assessment in Detecting Cognitive Impairment in Chinese Elderly Individuals: A Population-Based Study[J]. Journal of Geriatric Psychiatry and Neurology, 2011,24(4):184-190. [CrossRef]
- Winblad B, Palmer K, Kivipelto M, et al. Mild cognitive impairment – beyond controversies, towards a consensus: report of the International Working Group on Mild Cognitive Impairment[J]. Journal of internal medicine, 2004,256(3):240-246. [CrossRef]
- Julayanont P, Brousseau M, Chertkow H, et al. Montreal Cognitive Assessment Memory Index Score (MoCA-MIS) as a Predictor of Conversion from Mild Cognitive Impairment toA lzheimer's Disease[J]. Journal of the American Geriatrics Society, 2014,62(4):679-684. [CrossRef]
- Satija A, Bhupathiraju S N, Spiegelman D, et al. Healthful and Unhealthful Plant-Based Diets and the Risk of Coronary Heart Disease in U.S. Adults[J]. Journal of the American College of Cardiology, 2017,70(4):411-422. [CrossRef]
- Huang F, Wang H, Wang Z, et al. Is geriatric depression scale a valid instrument to screen depression in Chinese community-dwelling elderly?[J]. BMC Geriatrics, 2021,21(1). [CrossRef]
- China N H A F. Criteria of Weight for Adults[S]. Beijing, China: Standards Press of China, 2013.
- Chen C. Guidelines for the Prevention and Control of Overweight and Obesity in Chinese Adults [M]. 3. Beijing: People's Medical Publishing House, 2006.
- Chen L, Woo J, Assantachai P, et al. Asian Working Group for Sarcopenia: 2019 Consensus Update on Sarcopenia Diagnosis and Treatment[J]. Journal of the American Medical Directors Association, 2020,21(3):300-307. [CrossRef]
- Jia X, Wang Z, Huang F, et al. A comparison of the Mini-Mental State Examination (MMSE) with the Montreal Cognitive Assessment (MoCA) for mild cognitive impairment screening in Chinese middle-aged and older population: a cross-sectional study[J]. BMC Psychiatry, 2021,21(1). [CrossRef]
- Blum D, Cailliau E, Behal H, et al. Association of caffeine consumption with cerebrospinal fluid biomarkers in mild cognitive impairment and Alzheimer's disease: A BALTAZAR cohort study[J]. Alzheimers Dement, 2024,20(10):6948-6959. [CrossRef]
- Orozco Arbelaez E, Banegas J R, Rodriguez Artalejo F, et al. [Influence of habitual chocolate consumption over the Mini-Mental State Examination in Spanish older adults][J]. Nutr Hosp, 2017,34(4):841-846. [CrossRef]
- Sakurai K, Okada E, Anzai S, et al. Protein-Balanced Dietary Habits Benefit Cognitive Function in Japanese Older Adults[J]. Nutrients, 2023,15(3). [CrossRef]
- Gagnon C, Greenwood C E, Bherer L. The acute effects of glucose ingestion on attentional control in fasting healthy older adults[J]. Psychopharmacology, 2010,211(3):337-346. [CrossRef]
- Ooi C P, Loke S C, Yassin Z, et al. Carbohydrates for improving the cognitive performance of independent-living older adults with normal cognition or mild cognitive impairment[J]. Cochrane Database Syst Rev, 2011,2011(4):CD007220. [CrossRef]
- Best T, Kemps E, Bryan J. Saccharide Effects on Cognition and Well-Being in Middle-Aged Adults: A Randomized Controlled Trial[J]. Developmental neuropsychology, 2010,35(1):66-80. [CrossRef]
- Xue J, Jiao Y, Wang J, et al. The Incidence and Burden of Risk Factors for Mild Cognitive Impairment in Older Rural Chinese Persons[J]. Gerontol Geriatr Med, 2022,8:1682809665. [CrossRef]
- Wennberg A M V, Wu M N, Rosenberg P B, et al. Sleep Disturbance, Cognitive Decline, and Dementia: A Review[J]. Semin Neurol, 2017,37(4):395-406. [CrossRef]
- Jokisch M, Schramm S, Weimar C, et al. Fluctuation of depressive symptoms in cognitively unimpaired participants and the risk of mild cognitive impairment 5 years later: Results of the Heinz Nixdorf Recall study[J]. Front Behav Neurosci, 2022,16:988621. [CrossRef]
- Zafar J, Malik N I, Atta M, et al. Loneliness may mediate the relationship between depression and the quality of life among elderly with mild cognitive impairment[J]. Psychogeriatrics, 2021,21(5):805-812. [CrossRef]
- Toloraia K, Meyer A, Beltrani S, et al. Anxiety, Depression, and Apathy as Predictors of Cognitive Decline in Patients With Parkinson's Disease-A Three-Year Follow-Up Study[J]. Front Neurol, 2022,13:792830. [CrossRef]
- Goveas J S, Espeland M A, Woods N F, et al. Depressive symptoms and incidence of mild cognitive impairment and probable dementia in elderly women: the Women's Health Initiative Memory Study[J]. J Am Geriatr Soc, 2011,59(1):57-66. [CrossRef]
- Van Bogart K, Harrington E E, Witzel D D, et al. Momentary loneliness and intrusive thoughts among older adults: the interactive roles of mild cognitive impairment and marital status[J]. Aging Ment Health, 2024,28(12):1785-1792. [CrossRef]
- Peng J, Li X, Wang J, et al. Association between plant-based dietary patterns and cognitive function in middle-aged and older residents of China[J]. Journal of Alzheimer’s Disease, 2024. [CrossRef]
- Hewlings S J, Draayer K, Kalman D S. Palm Fruit Bioactive Complex (PFBc), a Source of Polyphenols, Demonstrates Potential Benefits for Inflammaging and Related Cognitive Function[J]. Nutrients, 2021,13(4). [CrossRef]
- Smith L, Lopez Sanchez G F, Veronese N, et al. Association of Fruit and Vegetable Consumption With Mild Cognitive Impairment in Low- and Middle-Income Countries[J]. J Gerontol A Biol Sci Med Sci, 2023,78(8):1410-1416. [CrossRef]
- Fangfang H, Qiong W, Shuai Z, et al. Vegetable and Fruit Intake, Its Patterns, and Cognitive Function: Cross-Sectional Findings among Older Adults in Anhui, China[J]. J Nutr Health Aging, 2022,26(5):529-536. [CrossRef]
Figure 1.
Relationship between continuous changes of uPDI and the occurrence of MCI among female elder population based on the RCS model.
Figure 1.
Relationship between continuous changes of uPDI and the occurrence of MCI among female elder population based on the RCS model.
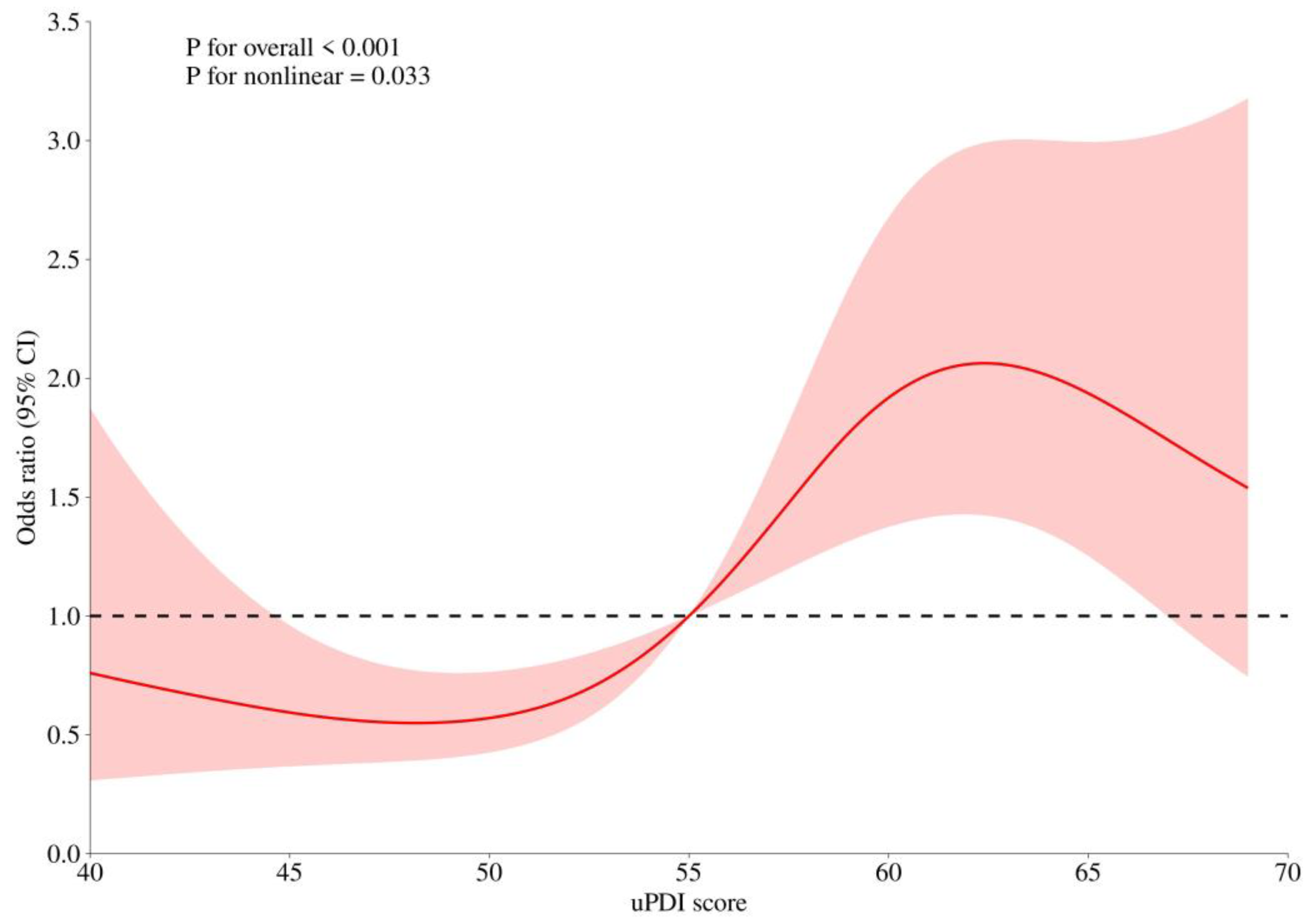

Table 1.
Main characteristics of study participants stratified by gender.
| Variables | Women | Men | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| MCI, n (%) | Normal, n (%) | χ2 | P | MCI, n (%) | Normal, n (%) | χ2 | P | ||||
| Total | 141(24.7) | 430(75.3) | 126(24.5) | 388(75.5) | |||||||
| Region | 4.408 | 0.036 | 0.114 | 0.736 | |||||||
| Urban | 90(63.8) | 231(53.7) | 59(46.8) | 175(45.1) | |||||||
| Rural | 51(36.2) | 199(46.3) | 67(53.2) | 213(54.9) | |||||||
| Age, year | 19.480 | <0.001 | 24.590 | <0.0001 | |||||||
| 55~65 | 37(26.2) | 166(38.6) | 26(20.6) | 143(36.9) | |||||||
| 65~75 | 58(41.1) | 195(45.4) | 52(41.3) | 175(45.1) | |||||||
| 75~ | 46(32.6) | 69(16.1) | 48(38.1) | 70(18.0) | |||||||
| Educational level | 1.415 | 0.234 | 3.281 | 0.070 | |||||||
| Junior school or below | 126(91.3) | 374(87.6) | 110(89.4) | 318(82.6) | |||||||
| High school or above | 12(8.7) | 53(12.4) | 13(10.6) | 67(17.4) | |||||||
| Occupation | 0.434 | 0.51 | 0.915 | 0.339 | |||||||
| employed or re-employ after retirement or seeking employment | 127(90.1) | 395(91.9) | 101(80.2) | 295(76.0) | |||||||
| Retirement or unemployed | 14(9.9) | 35(8.1) | 25(19.8) | 93(24.0) | |||||||
| Marital status | 4.616 | 0.032 | 1.443 | 0.230 | |||||||
| married | 104(73.7) | 353(82.1) | 117(92.9) | 346(89.2) | |||||||
| unmarried/ divorced/widowed | 37(26.2) | 77(17.9) | 9(7.1) | 42(10.8) | |||||||
| BMI(kg/m2) | 0.25 | 0.882 | 2.229 | 0.328 | |||||||
| <24.0 | 74(54.8) | 241(57.0) | 73(59.4) | 194(52.2) | |||||||
| ≥24~<28 | 45(33.3) | 137(32.4) | 43(35.0) | 147(39.5) | |||||||
| ≥28 | 16(11.9) | 45(10.6) | 7(5.7) | 31(8.3) | |||||||
| Live alone | 3.108 | 0.078 | 0.354 | 0.552 | |||||||
| Yes | 128(90.8) | 408(94.9) | 122(96.8) | 371(95.6) | |||||||
| No | 13(9.2) | 22(5.1) | 4(3.2) | 17(4.4) | |||||||
| Depression | 20.655 | <0.001 | 3.339 | 0.068 | |||||||
| Yes | 127(90.1) | 423(98.4) | 117(92.9) | 375(96.7) | |||||||
| No | 14(9.9) | 7(1.6) | 9(7.1) | 13(3.4) | |||||||
| Cereal# | 16.685 | <0.001 | 25.162 | <0.0001 | |||||||
| <300 g | 94(66.5) | 201(46.9) | 75(59.5) | 133(34.3) | |||||||
| ≥300 g | 47(33.3) | 228(53.2) | 51(40.5) | 255(65.7) | |||||||
| Vegetables intake | 7.996 | 0.005 | 10.374 | 0.001 | |||||||
| <150 g | 89(63.1) | 212(49.4) | 72(57.1) | 158(40.7) | |||||||
| ≥150 g | 52(36.9) | 217(50.6) | 54(42.9) | 230(59.3) | |||||||
| Fruit intake | 9.030 | 0.003 | 6.122 | 0.013 | |||||||
| <50 g | 95(67.4) | 227(52.9) | 92(73.0) | 236(60.8) | |||||||
| ≥50 g | 46(32.6) | 202(47.1) | 34(27.0 | 152(39.2) | |||||||
| Soybean intake | 4.154 | 0.004 | 1.503 | 0.002 | |||||||
| <38 g | 106(75.2) | 283(66.0) | 84(66.7) | 235(60.6) | |||||||
| ≥38g | 35(24.8) | 146(34.0) | 42(33.3) | 153(39.4) | |||||||
| Vegetable oil intake | 6.830 | 0.009 | 6.610 | 0.010 | |||||||
| <22 g | 93(66.0) | 229(53.4) | 84(66.7) | 208(53.6) | |||||||
| ≥22g | 48(34.0) | 200(46.6) | 42(33.3) | 180(46.4) | |||||||
| Strong teat intake | 0.386 | 0.535 | 0.347 | 0.556 | |||||||
| no | 130(91.2) | 389(90.5) | 94(74.6) | 279(71.9) | |||||||
| yes | 11(7.8) | 41(9.5) | 32(25.4) | 109(28.1) | |||||||
| Nuts intake | 6.761 | 0.009 | 2.725 | 0.099 | |||||||
| <5 g | 109(77.3) | 282(65.6) | 94(74.6) | 259(66.8) | |||||||
| ≥5 g | 32(22.7) | 148(34.4) | 32(25.4) | 129(33.3) | |||||||
| Plant-based diet indices* | PDI | 48.2±6.4 | 49.7±6.5 | 2.10 | 0.037 | 48.6±5.9 | 50.1±6.7 | 2.11 | 0.35 | ||
| hPDI | 56.4±5.6 | 57.6±4.8 | 2.16 | 0.032 | 57.3±4.8 | 57.4±5.0 | 0.19 | 0.847 | |||
| uPDI | 57.7±7.4 | 54.7±7.6 | -3.78 | 0.0002 | 56.32±7.4 | 54.05.9±7.5 | -2.77 | 0.0058 | |||
| Sarcopenia related | |||||||||||
| Sarcopenia | 0.342 | 0.559 | 1.650 | 0.199 | |||||||
| No | 134(97.1) | 410 (96.0) |
113(90.4) | 362(93.8) | |||||||
| Yes | 4(2.9) | 17(4.0) | 12(9.6) | 24(6.2) | |||||||
| low muscle mass | 1.352 | 0.245 | 1.348 | 0.246 | |||||||
| No | 122(95.3) | 347(92.3) | 92(85.2) | 285(89.3) | |||||||
| Yes | 6(4.7) | 29(7.7) | 16(14.8) | 34(10.7) | |||||||
| low muscle strength or performance | 7.303 | 0.026 | 4.200 | 0.122 | |||||||
| No low muscle strength or performance | 69(50.4) | 216(50.8) | 49(39.5) | 158(41.9) | |||||||
| Low muscle strength or performance | 48(35.0) | 178(41.9) | 50(40.3) | 171(45.4) | |||||||
| low muscle strength and performance | 20(14.6) | 31(7.3) | 25(20.2) | 48(12.7) | |||||||
* Values are mean ± SD; # Cereal included rice and wheat and their product.
Table 2.
Analysis of the risk of MCI in elderly women aged 55 and above by multivariate logistic regression model.
Table 2.
Analysis of the risk of MCI in elderly women aged 55 and above by multivariate logistic regression model.
| Variables | β | sxˉ | Wald χ2 | OR(95%CI) | P | |
|---|---|---|---|---|---|---|
| intercept | -3.9696 | 0.8982 | 19.5336 | <.0001 | ||
| Marital status | ||||||
| married | ||||||
| unmarried/ divorced/ widowed |
0.6672 | 0.2907 | 5.2669 | 1.949(1.102~3.445) | 0.0217 | |
| Depression | ||||||
| Yes | 1.8018 | 0.6004 | 9.0059 | 6.061 (1.868~19.660) | 0.0027 | |
| No | ||||||
| Cereal | ||||||
| <300 g | ||||||
| ≥300 g | -1.1450 | 0.2562 | 19.9714 | 0.318(0.193~0.526) | <0.0001 | |
| uPDI | 0.0545 | 0.0156 | 12.2135 | 1.056 (1.024~1.089) | 0.0005 |
Table 3.
Analysis of the risk of MCI in elderly men aged 55 and above by multivariate logistic regression model.
Table 3.
Analysis of the risk of MCI in elderly men aged 55 and above by multivariate logistic regression model.
| Variables | β | sxˉ | Wald χ2 | OR(95%CI) | P | |
|---|---|---|---|---|---|---|
| intercept | 0.9000 | 0.3106 | 8.3991 | 0.0038 | ||
| Region | ||||||
| Urban | ||||||
| Rural | 0.6438 | 0.2727 | 5.5734 | 1.904(1.116~3.249) | 0.0182 | |
| Age, year | ||||||
| 55~65 | ||||||
| 65~75 | 0.6729 | 0.3062 | 4.8286 | 1.96 (1.075~3.572) | 0.0280 | |
| 75~ | 1.5504 | 0.3366 | 21.2155 | 4.713 (2.437~9.117) | <0.0001 | |
| Vegetables intake | ||||||
| <150 g | ||||||
| ≥150 g | -0.9390 | 0.2658 | 12.4781 | 0.391 (0.232~0.658) | 0.0004 | |
| Vegetable oil intake | ||||||
| <22 g | ||||||
| ≥22g | -0.6901 | 0.2511 | 7.5516 | 0.502 (0.307~0.820) | 0.006 | |
| Cereal | ||||||
| <300 g | ||||||
| ≥300 g | -0.8251 | 0.2456 | 11.2892 | 0.438 (0.271~0.709) | 0.0008 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



