Submitted:
01 May 2025
Posted:
05 May 2025
You are already at the latest version
Abstract
Background: Non-adherence to anti-tuberculosis treatment remains a major obstacle to lowering tuberculosis treatment success rates and enhancing healthcare expenses. The aim of this study was to identify determinants contributing to non-adherents to anti-tuberculosis treatment in a public primary healthcare clinic in South Africa. Methods: A cross-sectional study was carried out to collect data from 65 participants using face-to-face interviews from a structured questionnaire. Data were analyzed using SPSS to obtain descriptives for frequency and proportions, and Pearson Chi-Square test to determine factors associated with non-adherents to anti-tuberculosis treatment. The value of P< 0.050 was considered statistically significant. Results: Of 65 interviewed, 41(63.08%) were males and 24(36.92%) females. Majority 26(40.00%) were in age-range of 26-35, 53(81.53%) were singles, 53(81.53%) with high-School level of education, 35(53.85%) unemployed and 35(53.85%) HIV-status of Sero negative. Adherents were 45(69.23%) and 20(30.77%) non-adherents. Gender was major predictor to non-adherence with males committed to treatment than females with a significant association (X2 = 65.00 and P of < .001). Conclusion: Major contributing factors to non-adherents were long distance to clinics, long-waiting times at clinics, no support from clinic-staff and family, drug-shortage, adverse-effects, and unemployment. Comprehensive programs addressing these multifactorial factors are needed for successful treatment and eradication of tuberculosis.
Keywords:
Adherence
; Tuberculosis
; Primary Healthcare
; Direct Observed Treatment
; Public Health
Introduction
Tuberculosis (TB) is an infectious disease that remain the leading cause of death from among adults worldwide as reported by World Health Organization (WHO), 2025). [1] Tuberculosis is a preventable and curable disease, yet it’s likely reclaimed its position as the world’s deadliest infectious disease, surpassing COVID-19. [2] The social value of TB being the world's deadliest infectious disease, as reported by WHO (2025), [1] highlights the immense impact it has on individuals, communities, and the global economy. Tuberculosis causes not only direct health consequences but also significant social and economic burdens, including healthcare costs, lost wages, and psychological distress. It disproportionately affects marginalized populations, exacerbating existing inequalities.
Tuberculosis causes almost twice as many deaths as HIV/AIDS and impacts more than 10 million individuals each year, with case numbers increasing since 2021 (WHO, 2025). [3] Urgent action is required to achieve the United Nations (UN) and WHO target of ending the global TB epidemic by 2030. [1] World Health Organization is calling for an urgent investment of resources to protect and maintain TB care and support services for people in need across regions and countries. The WHO (2025) [4] report states that TB remains the world’s deadliest infectious disease, responsible for over 1 million deaths annually, which brings devastating impacts on families and communities.
Tuberculosis continues to pose a significant global health threat, with the WHO reporting around 10.8 million new cases and 1.25 million deaths each year. In 2023 alone, TB was responsible for 1.25 million deaths, including 161,000 among people living with HIV. Tuberculosis has likely regained its status as the world’s deadliest infectious disease, surpassing COVID-19, which had temporarily taken the top spot. [3] Tuberculosis not only remains a major global health threat but also has a devastating impact on specific populations. Tuberculosis remains the primary cause of death among individuals living with HIV and plays a major role in deaths associated with antimicrobial resistance. WHO supported the above statement that alarmingly, while 1.5 million people succumb to TB annually, over 10 million new cases emerge every year (WHO, 2024). [4] According to Barter et al. (2012), [5] the burden of TB is disproportionately borne by developing countries, where 75% of cases occur among the most economically productive age group (15-54 years), exacerbating the socioeconomic impact.
The WHO aims for a cure rate of at least 85% for all diagnosed TB cases. To achieve this, adherence to treatment needs to be between 85-90%, as stated by Boru et al. (2017). [6] Fortunately, the global efforts to combat TB have been successful, with the Millennium Development Goal (MDG) target to halt and reverse TB incidence by 2015 being achieved. This has resulted in a significant reduction in TB mortality rates, saving an estimated 43 million lives between 2000 and 2014. [7] However, some countries, like South Africa (SA), still struggle with low cure rates, with only about 54% of TB patients being cured, far below the WHO’s target (Mkhavele et al.,2025). [8]
As per WHO Global TB report of 2024, [4] in 2023 approximately 10.8 million people worldwide contracted TB, including 6 million men, 3.5 million women, and 1.3 million children. What’s concerning is that TB is present in all countries and age groups, and multidrug-resistant TB (MDR-TB) remains a significant public health crisis. Nevertheless, it is important to emphasize that TB is both preventable and curable. By 2030, the target is to achieve a 90% reduction in TB-related deaths and an 80% decrease in the TB incidence rate compared to 2015 levels. [9]
Houben and Dodd (2024) [10] highlight that an annual investment of $22 billion is essential for the effective prevention, diagnosis, treatment and care of TB. This level of funding is critical to meeting the global TB targets by 2027, as established during the 2023 UN high-level meeting on TB. The End TB Strategy also sets out clear milestones and objectives aimed at reducing TB incidence and mortality. To address TB, specific milestones were established for 2020, including:
1. A 35% reduction in TB-related deaths,
2. A 20% decrease in the TB incidence rate, and
3. The elimination of catastrophic costs for TB patients and their families.
Looking forward, ending the TB epidemic by 2030 remains a crucial health objective under the United Nations’ Sustainable Development Goals (SDGs). [11]
In 2014, the global TB burden remained high, with 9.6 million new cases and 1.5 million deaths reported. According to Kastien-Hilka et al. (2017), [12] twenty-two countries designated by the WHO as high-burden nations were responsible for 80% of all TB cases. The 2018 Global TB Report [13] emphasized the success of the Directly Observed Treatment Short-Course (DOTS) strategy, which was shown to enhance treatment adherence, lower recurrence rates, and prevent the development of MDR-TB. [13] Introduced by the WHO in 1995, DOTS comprises five essential elements: case detection through sputum smear microscopy and rapid molecular diagnostics, along with standardized treatment supported by supervision and patient care (WHO, 1999). [14]
According to Yin et al. (2016), [15] non-adherence to anti-tuberculosis treatment has far-reaching consequences, leading to prolonged and severe illness, increased risk of death, disease transmission, and drug resistance. These outcomes not only devastate individuals but also impose a substantial economic burden on both patients and the healthcare system. Collins and Njungane (2016) [16] also emphasized that non-adherence to TB treatment poses a major challenge to global TB control, significantly leading to treatment failures and impeding effective disease management.
A 2016 systematic review conducted in developing countries, cited by SIASPU in the Philippines, [17] identified the primary factors associated with non-adherence to TB medication. The review identified socioeconomic and demographic challenges, lack of social support, and limited knowledge about treatment duration as significant barriers to adherence. These factors often result in patients losing follow-up, emphasizing the need for targeted interventions to address these challenges and improve TB treatment outcomes. The WHO, in its reports, identifies several social factors that significantly impact TB treatment adherence, including socioeconomic status, individual behavioral factors, and the health delivery system. These factors, when addressed through social interventions, can lead to improved adherence. (WHO, 2024). [4]
Once again, this study demonstrates a social value in those studies by Grange et al. (2001) [18] and Stybo et al. (1969) [19] came to a conclusion that TB epidemic is strongly influenced by broader social and economic development as well as (often interrelated) risk factors more specifically linked to health, such as nutritional status, diabetes, HIV infection, alcohol use disorders and smoking.
According to a qualitative study conducted by Boru et al. (2017), [6] most TB deaths globally take place in underdeveloped nations, with 75% of cases occurring in the most economically productive age range (15–54 years). To control transmission and prevent medication resistance, the WHO recommends that at least 85% of all identified TB cases be cured, with a focus on obtaining high cure rates among smear-positive pulmonary TB patients (Ndjeka et al., 2008). [20] Regardless of the availability and affordability of TB medicines, SA has the highest prevalence and incidence rates of TB cases (696 and 834 cases per 100,000 population), according to Kastien-Hilka et al. (2017). [12] The most frequent illness among the estimated 5.5 million South Africans living with HIV/AIDS is TB, which is also the country’s leading cause of death (134 cases per 100,000 people). According to WHO estimates, 73% of all TB cases also have HIV co-infection (WHO, 2025). [19]
In low-income and poverty-stricken developing countries, TB continues to be a significant public health concern, persisting as a major burden despite efforts to control it through the DOTS strategy (Obermeyer et al., 2008). [20] Based on the total number of TB cases, SA came in at number four on the list of countries with a high TB burden in 2018 (Moodley et al., 2020). [21] Social, economic, and clinical barriers to care continue to impede TB control efforts (Goosby et al., 2018). [22] Poor adherence to recommended anti-TB treatment programs, such as those covered by the DOTS strategy, results from this. In the end, this is one of the reasons why TB cure rates are so low.
In addition to complicating drug resistance and disease transmission, poor treatment adherence lengthens and intensifies sickness. According to Collins and Njuguna (2016), [15] each of the afore mentioned elements has detrimental economic effects on the patient, the community, and the healthcare system.
Cramm et al. (2010) [23] noted that despite the introduction of the DOTS program in 1995, TB continues to be a major health challenge in SA, especially in the Eastern Cape (EC). Although TB incidence has been declining in SA since 2009 and deaths due to TB have decreased in recent years, TB remains the number one cause of death in this country. The Global TB Report 2015 estimated that in 2014, SA had the second-highest TB incidence rate in the world, with 834 cases per 100 000 population.
Studies have indicated that perceptions, rather than mere knowledge, heavily influence TB treatment initiation and non-adherence in this region. While the WHO recommends a TB cure rate of 85%, [24] the EC reports a much lower cure rate of 41%, falling short of both the national average and the WHO’s minimum recommended threshold of 65%. The EC province of SA faces a high burden of TB, characterized by elevated incidence and prevalence rates alongside notably low cure rates. In comparison, Indonesia ranks third worldwide in TB prevalence, after India and China. To address this challenge, Indonesia provides free TB treatment, primarily utilizing the DOTS strategy, as noted by Cramm et al. (2010). [23]
A study on determinants of non-adherence to anti-TB drugs has a scientific value as is presented in the literature that has been searched including the knowledge gap that the study is addressing. The World Health Organization (WHO, 2024) [4] reports the prevalence of TB annually in its Global TB Report. This data is crucial for several scientific reasons, including understanding the global TB epidemic, tracking progress towards TB elimination goals, and informing public health interventions. Researching the determinants of TB non-adherence, as reported by the WHO, holds significant scientific value by helping to understand the factors that contribute to treatment failure and the emergence of drug resistance. This knowledge is crucial for developing targeted interventions to improve adherence and ultimately reduce the global TB burden.
A study on the determinants of non-adherence to anti-tuberculosis treatment in a public primary healthcare setting in SAfrica holds significant scientific value. It identifies key factors contributing to treatment failure and drug resistance, informing targeted interventions to improve adherence and treatment outcomes. Furthermore, this research can contribute to a broader understanding of the social and health system factors influencing TB control efforts in the South African context.
Adherence to TB medication is essential to TB treatment’s success. Suboptimal medication adherence is widespread in diseases that require long-term therapy, such as diabetes, hypertension, bronchial asthma, and TB. [24] Medication adherence is a complex human behavior that could be influenced by various factors, including patient-related, health system, condition-related, therapy-related, and socioeconomic factors. The World Health Organization reports the prevalence of TB annually in its Global TB Report. This data is crucial for several scientific reasons, including understanding the global TB epidemic, tracking progress towards TB elimination goals, and informing public health interventions.
Researching the determinants of TB non-adherence, as reported by the WHO, holds significant scientific value by helping to understand the factors that contribute to treatment failure and the emergence of drug resistance. This knowledge is crucial for developing targeted interventions to improve adherence and ultimately reduce the global TB burdens.
Understanding the root causes of non-adherence is very crucial in that specific factors that were identified in other studies are identified. By identifying these factors that influence TB treatment adherence, research can shed light on why some patients struggle to take their medications as prescribed. These factors can include socioeconomic issues, psychological barriers, health system limitations, and patient-related factors like forgetfulness or side effects. A case in question is developing targeted interventions. Once the determinants of non-adherence are understood, researchers can develop and test interventions that address these specific barriers. For example, interventions could focus on improving patient education, strengthening social support systems, simplifying treatment regimens, or addressing the side effects of medications.
Conceptual Framework
To understand further factors contributing to non-adherence, it is necessary to consider the Theoretical frameworks that underpin why people don't adhere to TB treatment. According to these theories one can recognize that non-adherence as a complex issue influenced by a combination of factors, including individual beliefs, social support, economic circumstances, and health system characteristics as stated in the systematic review conducted in developing countries, cited by SIASPU in the Philippines. [16]
To fill in the gaps of studies carried out one has to apply a “Health Brief Model” (HBM). This model can be applicable in this study in that according to this model, people’s beliefs about the severity of the disease, their susceptibility to it, the benefits of treatment, and the barriers to treatment, all influence their adherence. Based on the HBM theoretical concepts, this study used the model to determine the effect of associated factors and individual patient’s perceptions of TB treatment adherence. A case in question is, for example, if some someone doesn’t believe TB is serious or doesn’t see the benefits of treatment, they may be less likely to adhere.
Gebremariam et al. (2021), [24] applied this model in which he stated that there are complex interactions of individual, interpersonal, socio-cultural, and health system factors that influence non-adherence. Understanding the level of adherence and how it relates to perception about its treatment provides an opportunity to design intervention that improves adherence through overcoming misperceptions.
Another module is “The World Health Organization (WHO) Multidimensional Adherence Model (WHO-MAM)”: [25] This is a psychological model that recognizes that adherence is influenced by a combination of factors, including patient-related factors (like beliefs and knowledge), social and economic factors, and health system factors. It recognizes that these factors are interconnected with and influence each other as indicated by Anyaike C et al. (2013). [25]
The two theories are connected and lead to the statement problem of this study that non-adherence to TB treatment among TB patients caused by multifactorial factors remains one of the primary challenges hindering improved cure rates. Non-adherence to TB treatment threatens the success of treatment, increases the risk of TB spread, causes drug resistance, and increases morbidity and mortality.
Therefore, the significance of this study highlighted that non-adherence to TB treatment is associated to some socio-demographic of TB patients. This results in treatment failure, the development of MDR-TB, prolonged infectiousness, and overall poor treatment outcomes (Boru et al., 2017). [6] Additionally, in patients with HIV infection, untreated TB infection accelerates HIV development (Diedrich and Flynn, 2011). [26] Therefore, it is necessary to monitor the non-adherence of TB patients who are taking TB treatment. Comprehensive programs addressing these multifactorial factors are needed for the successful treatment and eradication of TBmmm in this way optimum health outcomes will be achieved. In response to this concern, the present study aims to assess determinants of non-adherence to anti-TB therapy in TB patients.
Aim and Objectives
The study aimed to identify the determinants contributing to non-adherence to anti-tuberculosis treatment among patients attending a TB clinic at a public primary healthcare facility in South Africa in 2023. This aim was achieved through the following specific objectives. The specific objectives were to:
- Describe demographics of TB patients on TB treatment
- Determine the prevalence of non-adherents of TB treatment
- Identify determinants contributing to non-adherents of TB treatments
- Associate demographic characteristics of non-adherents and determinants of non-adherence to ATT.
- Desribe patient program and drug-related factor that affect non-adherence to ATT.
Materials and Methods
Study Design
A descriptive cross-sectional research approach was used in this study to evaluate the main determinants of non-adherence to tuberculosis treatment. The design is used by researchers to analyze various factors, including demographic information, behaviors, conditions, or outcomes, to discern patterns or correlations within the population studied. The design allows researchers to explore the prevalence of certain characteristics, identify potential associations between variables, and make descriptive comparisons. It is also selected for their efficiency, relatively low cost, and ability to examine multiple variables simultaneously.
Setting
The study was conducted at Mthatha Gateway Clinic, a public primary health care clinic, is the Eastern Cape Province of South Africa. The clinic caters for the following local communities: Southridge, Fortgale, Lindale, Qweqwe, Ultra city, Slovo, Mandela Park, Chris Hani, Payne and Zimbane. The health care centre operates from 7am to 4pm on weekdays (Monday-Friday). It is equipped with nine departments- Pharmacy, Antenatal care, Family Planning, Chronic Conditions Department (TB, HPT, HIV/AIDS) Decanting, Minor ailments, Dental, Xray and Mens clinic. etc. The clinic operates under the authority and supervision of the department of health of King Sabata Dalindyebo Local Area (KSD-LSA).
Study Population
The study population were TB patients attending at the public primary health center that are receiving anti-TB treatment from the Clinic.
Inclusion criteria:
- The study focused on adults who were at least 18 years and older.
- Individuals who had been diagnosed with tuberculosis and initiated on TB treatment
- Participants who voluntarily agreed to participate in study
Exclusion Criteria:
- Participants with other active infections, such as MDR TB or XDR TB.
- Participants with severe cognitive impairments affecting their understanding.
Sample Size Calculation and Sampling Strategy
The sample size was calculated using the formula Slovin’s formula Sampling Technique lying formula (Slovin, 1960) [27] n=N/(1+Ne^2) where: n= sample size, N=population size, e= margin of error (<10%) = 0.009
n=N/(1+Ne^2)
n= 280/(1+280×0.09^2)
n = 65/0.5265 × n
n = 0.4735N = 0.5265×137
Therefore, our sample size was 65 participants.
Sampling Strategy
Non-probability sampling strategy: Convenience sampling. Non-probability sampling is often used in studies on non-adherence to anti-TB treatment because it allows researchers to focus on specific groups or individuals who are most likely to have insight into the factors contributing to non-adherence. By focusing on specific groups or individuals, researchers can gain a deeper understanding of the complex challenges faced by patients and develop targeted interventions to improve adherence and treatment outcomes.
Data Collection Process
Data Collection Tool
A standardized questionnaire was used as a data collection tool over a period of one week. Structured questionnaires aim for both validity and reliability. Validity ensures the questionnaire measures what it's intended to, while reliability guarantees consistent results when administered repeatedly. Reliability is generally considered high in structured questionnaires due to the use of standardized, closed-ended questions.
Variables
Demographic variables such as gender, age, marital status, educational status, income status, and HIV status. These were coded as binary: gender (male/female), age (18-25, 26-35, 36-45, 46-55 and >55, marital status (single/married), Educational status (high school/tertiary), Income status (ZAR) (unemployed, 1000-3000, 3001-5000, >5000) and HIV status (Sero positive/Sero negative. Section II consisted of factors contributing to non-adherence of TB treatment including patient program (substance use, distance from the clinic, interaction with the staff clinic, poverty) and drug-related factors (adverse effects of the treatment, shortage of drugs at the clinic). A non-adherent tuberculosis drug is defined as a patient who missed at least one scheduled dose of their tuberculosis medication. To accommodate the language barrier, the questionnaire, participant information sheet and consent form were translated into IsiXhosa, a local language of the participants.
Data Management
Data management involves the processes of collecting, organizing, safeguarding, and storing an organization’s data to enable effective analysis and interpretation. In this study, these activities were carried out as follows:
Data Protection
The data protection and confidentiality protocols included aspects like theft, loss and tempering of data. This was accomplished by restricting access to study data. Hard copies of notes, surveys, questionnaires, and other paper records, for instance, were stored in a secure area off-limits to the general public. For example, a lockable filing cabinet with a key kept by the principal investigator as well as laptop with protected password only known to the principal investigator.
Data Analysis
Data Cleaning: All questionnaires were checked for completeness. The coding was done and captured into the laptop using SPSS Version 29 ready for analysis.
Variables of Interest
The variables of interest of analysis of our included:
1. Dependent variable: TB non-adherents’ patients
2. Independent variables: socio-demographic, program-related and drug-related factors.
The primary outcome variable was prevalence of non-adherents, assessed through patients’ self-reports on medication intake. Patients were asked if they had missed any doses, and those who reported missing more than 10% of their prescribed medication (i.e., taking less than 90%) were classified as non-adherent.
A combination of statistical tests was used to analyze data and identify potential predictors.
Descriptive Statistics: used to summarize and describe the characteristics of the sample.
Examples include calculating means, medians, standard deviations, percentages, and frequencies for various variables.
Pearson Chi-square test: used to examine the association between categorical variables.
Used to determine if there's a statistically significant relationship between, for example, demographic factors (like age, gender) and non-adherence rates, and factors associated with non-adherence.
Ethical Considerations
The study was conducted according to the guidelines of the Declaration of Helsinki. The study proposal received approval from the Human Research Ethics Committee (HREC) of the Faculty of Medicine and Health Sciences at Walter Sisulu University. The certificate letter registration number: 047/2023 was issued. Thereafter permission was obtained from the KSD municipality under which the clinic is located and manager of the clinic to conduct the study. Informed consent was obtained from each participant. The researcher obtained written informed consent prior to data collection. Participants were assured of their details being anonymous and not containing personal information. Data was collected in quiet rooms.
Results
The results are presented according to the sequence of the aim and objectives of this study
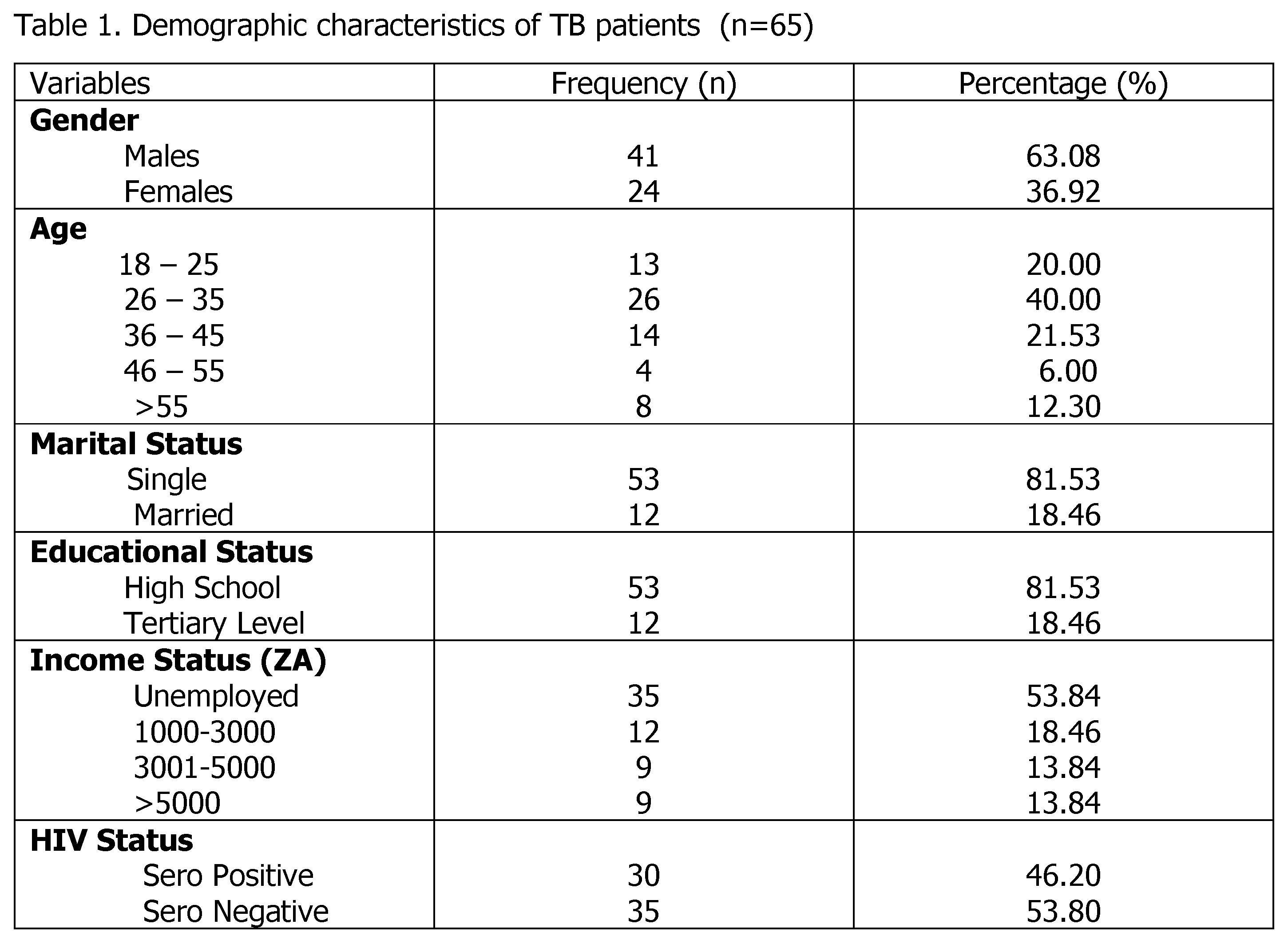
Demographic Characteristics
The sociodemographic characteristics of patients undergoing TB treatment were obtained through face-to-face interviews using a pre-structured questionnaire. Demographics determined were gender, age, marital states, educational background, income status, and HIV status. Of the 65 patients with TB involved in this study, males were 41(63.08%) and 24(36.92%) females. The mean age ± STD age of patients was 36.23 ±11.21 years. The majority of patients were in the age-range of 26-35 with 26(40.00%), singles dominated with 53(81.53%). In terms of educational status, 53(81,53%) were the majority high school level of education. The majority were unemployed accounting for 35(53.84%) and 35(53.80%) had HIV status of Sero negative (Table 1).
Demographics of Patients and Adherence Status
The total number of adherent patients was 45(69.23%) and 20(30.77%) non-adherents. Of these 11(55.00%) were males non-adherents, 9(45%) females of 24(36.92%), 15(33.3%) were adherent and 9(45.00%) non-adherents. Gender has a major impact, with males reporting higher non-adherence 11(55.00%) than females 9(45%). The age distribution reveals a balance of adherence and non-adherence across groups, with somewhat higher adherence in the 26-35 age range with 16(35.60%). Adherence amongst singles was higher with 38(84.4%) followed by married with 7(15.60%); hence marital status has bigger influence. Patients with high school education had a greater rate of non-adherents 40(37.80%), as those with tertiary education with adherents of 5(41.30%). Unemployed participants had the greatest non-compliance patients totaling to 22(45.90%), followed by those earning R 3000-5000 per month at 9(20%) non-adherents. In terms of HIV status, the Sero negative had higher rates of adherents of 19(42.20%) while 11(55.00%) were non-adherents for sero positive and 9(45.00%) were non-adherents of sero negative and Sero positive (Table 1).
Table 1.
Sociodemographic characteristics and their association with adherents to Tb treatment were determined. Of the 65 patients with TB involved in this study demonstrate that 45(69.20% patients adhered to therapy, whereas 20(30.80%) did not. Gender has a major impact, with males reporting higher adherents of 30(66.70%) and non-adherents of 15(33.30%) than females with adherents of 11(55.00%) and 9(45.00%) of non-adherents. The age distribution reveals a balance of adherents and non-adherents across the groups, with somewhat higher adherents in the 26-35 age range with adherents of 16(36.60%) and 10(50.00%) adherents.
In marital status singles adherents accounted for 38(84.4%) and 15(75.00%) non-adherents. Patients with higher education had higher numbers of adherents of 40(88,90%), and 5(45.00%) of non-adherents as compared to those with Tertiary education with 13(65.00%) adherents and non-adherents of 7(35.00%). For employment status, unemployment had the greatest number of adherents of 48.50%, followed by those earning R 3000-5000 with 20.00%, and 17(3.00%) with those earning >5000 and the lowest with 13.30%. With non-adherent unemployment they had 65.00% and lowest 5.00%. In terms of HIV status, Sero negative higher adherents of 26(57.80%), and 9(45.00%) non-adherents as compared to 19(42.20%) Sero positives adherents and 11(55.00%) non-adherents.
Gender is identified as major variables impacting treatment adherence (Table 2). Males were more likely to remain committed to treatment than females as there was a significant association of (X2 = 65.00 and P value of <.001). Age, marital status, educational level, employment status and HIV status were all studied, but none were shown to be statistically significant predictors of non-adherence (Table 2).
2.3.Sociodemographic Characteristics and Their Association with Treatment Adherents
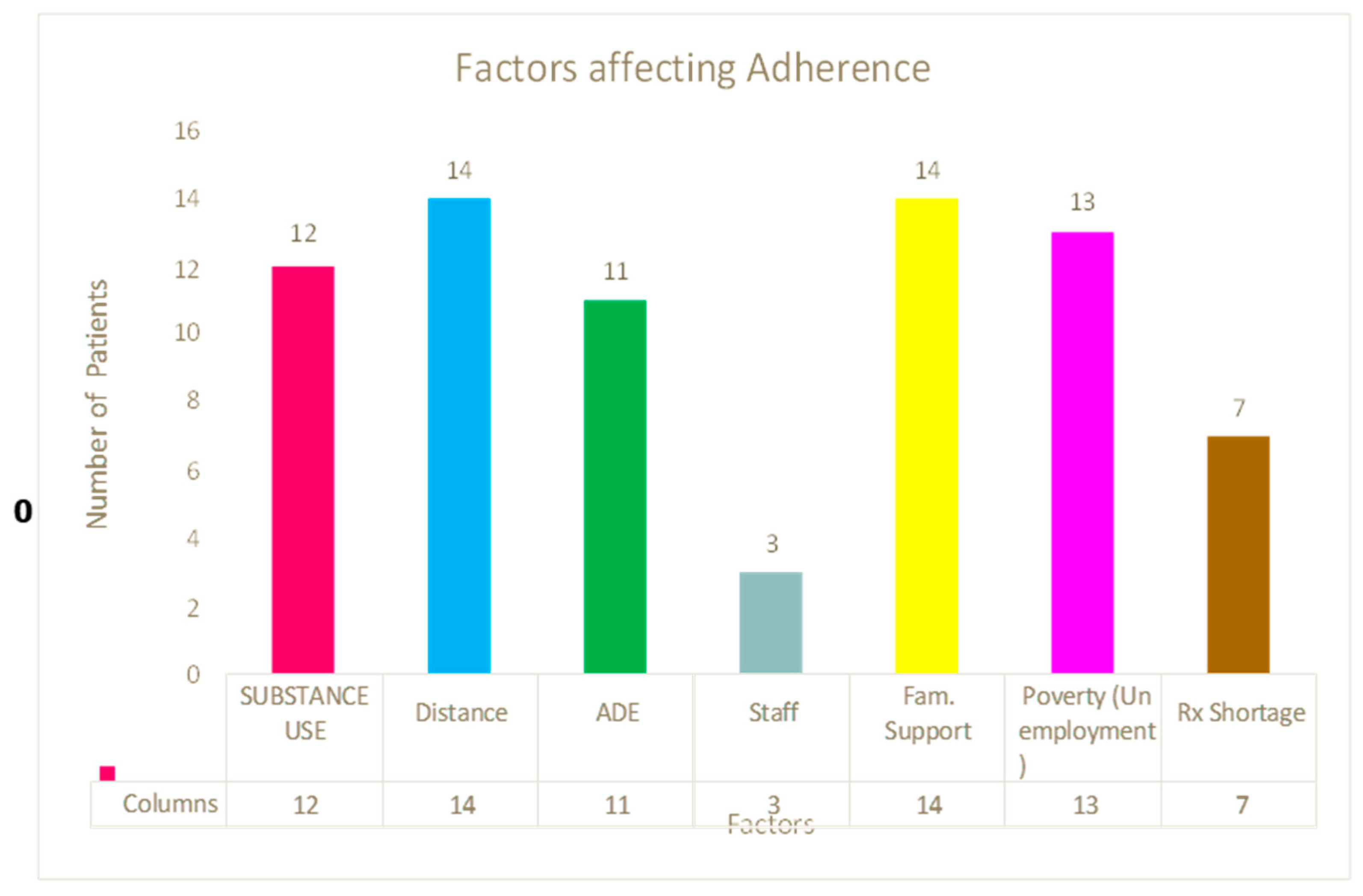
2.3. Factors influencing TB patients’ noncompliance with therapy.
Both Table 3 and Bar chart 1, illustrates factors of TB patients that affect non-adherence.
Chart 1.
Patient Program and drug related factors affecting non-adherence.
Discussion
Key Findings
The study sample consisted of 65 patients of which males were more than females with the majority in age range of 26-35 years. The majority were singles. In terms of level education, the greater had high school level and unemployed with the highest with HIV status of sero negative. In terms of the prevalence of adherents, males were more adherents than females. The age range of 26-35 had more adherents. Singles had the highest number of adherents. Patients with high school education had a greater rate of non-adherents. Unemployed participants had the greatest non-compliance patients and in terms of HIV status, the Sero negative had higher rates of adherents. Factors that affected adherence were distance from home to clinic, lack of family support, unemployment and substance of abuse.
Discussion of Key Findings
The aim of this study was to assess determinants of non-adherence in TB patients receiving TB treatment attending from a public primary health care setting. For effective TB control and eradication, treatment adherence is essential. The sample size in this study consists of 63.00% males and 37.00% female participants with the age distribution leaning towards the range of 26-35 years. In this study, 69.20% of the participants were able to follow their anti-TB regimen and 30.76% non-adherent. Results of adherence obtained in this study was 6.3% less than what was reported by Woimo et al. (2017) [31] in a study done in South Ethiopia with adherence of 75.50%, then in North East Ethiopia, Tesfahuneygn et al. (2015) [32] reported adherence of 77.50%, while Kebede and Wabe (2022) [33] reported 79.20% in South West Ethiopia. It has been proposed that the disparity in outcomes might be explained by differences in definitions of non-adherence to anti-TB medication. There is presently no agreed-upon definition of adherence to anti-TB therapy, despite the WHO’s recommendations on the quantity and timing of missed medications or hospital appointments (WHO 2023). [23]
In this study, about 30,76% of the patients were non-adherent to anti-TB treatment, which was 5,5 % higher than the reported non-adherents in South Ethiopia and East Ethiopia (Woimo et al., 2017). [31] This could be attributed to factors such as level of education, socio-economic status, HIV co-infection, adverse effects and waiting period at the health facility which correlates with previous study (Woimo et al., 2017). [31] This is further supported by the results of this investigation, as patients with inadequate understanding of tuberculosis and its treatment demonstrated a high number of non-adherents (65.00%) in North East Ethiopia, Tesfahuneygn et al. (2015) [32] reported adherents of 77.50% in South Ethiopia, while Kebede and Wabe (2022) [33] reported 79.20% in South West Ethiopia.
Additionally, this may be because self-reports were used to quantify non-adherence, and patients are prone to overestimate their adherence when using this approach. [23] Because of this, some patients may be mistakenly labeled as adherent when, in reality, they are not. An overestimation of 27.00% in the degree of adherence when self-reports were utilized was discovered in one study that examined whether the overestimation of adherence using self-reports would be noticeable when objective measures of adherence were employed. [30] Nonetheless, patients who acknowledge and disclose noncompliance readily embrace and execute treatments aimed at improving their everyday life. [34,36,37]
Due to the increased risk of developing X-Drug resistant TB and multi-drug resistant TB, these non-adherence percentages are quite concerning. This will raise the price of managing an already significant disease and substantially increase its burden5. Therefore, in order to reduce the levels of non-adherence, adherence support measures must be used. It has been discovered that doctors typically do not properly anticipate the adherence levels of their patients based on their knowledge of these patients, even when the key informants believed the degree of non-adherence was low. [34]
A lack of financial resources (poverty) was also linked to non-adherence to anti-TB medication. In this study, a significant number of participants (65.00%) that were non-adherent to treatment were unemployed receiving less than one thousand rand (<R1000) monthly. Clearly lack of economic resources is a barrier to adherence, which is in correspondence with a previous study performed by Naidoo et al. (2013). [38]
Results from this study revealed that 55% of Sero positive patients as compared to 45% Sero negative were non-adherent. Arentz et al. (2014), [39] claimed that people with TB/HIV co-infection are more likely to acquire active TB and that its incidence has greatly raised the burden of infectious diseases globally, support these findings. It’s possible that these patients won’t follow their TB treatment plan. In comparison to those on anti-TB treatment and HIV-negative, the researchers found that approximately 55% of participants on dual therapy (ART and anti-TB medications) did not adhere to anti-TB treatment. Patient-related factors like a heavy pill load, bad responses, and anxiety over not being able to handle both anti-tuberculosis medicine and ART could be the cause of this. These findings correlate with those reported previously by Naidoo et al. (2014) [38] that lack of economic resources is a barrier to adherence.
Substance use proved to be one of the common characteristics shared among the non-adhering patients (60.00%). It affects their ability to stay in care and is linked to a higher likelihood of missing treatment follow-up sessions and neglecting their health. Some patients waited for 4 hours and more upon arrival to the health facility, but from the study it was observed that as much as in all time interval of waiting, there was poor adherence to anti-TB treatment. Therefore, the study has shown that waiting hours are less likely to be associated with poor adherence because about 60.00% (of the total sample) of those who waited for such time adhered to treatment.
Out of the non-adherent patients, 35% stated to have stopped taking their medication due to a shortage of treatment at the clinics. So, they would be referred to other areas such as their closest public pharmacies to be given their treatment or buy from private pharmacies. Shortage of medications in public pharmacies is a very serious public health challenge. Results from this study also indicated that 65.00% were unemployed, which meant that they could not afford to buy the medicines or no transport money to go to other public pharmacies. All this leads to patients not completing their recommended dose leading to uncompromised immune system further leading to TB complications like MDR-TB further aggravating to XDR-TB.
According to WHO’s report on the worldwide plan to halt TB, the evolution of Mycobacterium tuberculosis strains that do not respond to treatment with standard first line combinations of anti-TB medicines has led to inadequate treatment, resulting in the emergence of multi-drug-resistant TB (MDR-TB) in almost every country in the world. [40] This is also supported by Rieder (2002) [41] claiming that a patient who discontinues TB treatment for any reason is one of the main problems and difficulties that most TB programs face. To which given the fact that they are given a solution to the problem but rather them failing to go to a local dispensary, makes us conclude that Drug Shortage in Health facilities would be a less likely reason for patients to choose not to maintain their treatment regimen. There was also the noted trend in reasoning behind why the unemployed (35.00%) were also not maintaining the treatment regimen which was that working hours clashed with their preferred working hours if their employers had no idea of their TB status.
If a person asked for a few hours off, the waiting time at the clinic would already impede the efforts made to collect and leave without doing so. The reinfection of TB was also a factor that was emerging among the non-adherent patients, as having TB for the second or third time is discouraging to the patients and consider taking medication as useless and doesn’t prevent them from getting sick. It can also be taken into consideration that they could be having the re-occurrence of TB because of lacking sufficient understanding of TB, hence exposing themselves to being re-infected with TB. Lack of proper education leads to lack of them not knowing the importance of adhering to the full course treatment.
The participants also stated having history of a poor relationship and poor communication with the healthcare nurses in the facility. This meant that they were not given time and space to properly communicate their experience with the treatment, such as having adverse effects. This leads them not to have enough knowledge about the disease and why they have to be taking the medication. The patients become more prone to non - adherence due to a negative conception against the clinic, which will now also include their attitude towards their own welfare, like the points made in a study performed by Wohlleben et al., (2017). [42]
Strengths and Limitations
The following are the strengths:
Snapshot of Prevalence: Cross-sectional studies are well-suited for capturing the prevalence of non-adherence and its associated factors within a population at a specific time point.
Efficiency and Cost-Effectiveness: They are often simpler and less expensive to conduct than longitudinal studies, making them useful for preliminary investigations or when resources are limited.
Identifying Potential Risk Factors : They can help identify potential risk factors associated with non-adherence, such as socioeconomic factors, health system issues, or individual characteristics, according to a study on TB treatment adherence. However, it faces limitations in establishing causality and longitudinal trends, as it only collects data at one point in time.
Limitations of This Study
Difficulty in Establishing Causality: Since data is collected at one time, it's difficult to determine if a particular factor directly causes non-adherence or if there's a causal relationship between variables, notes a study on medication adherence and associated factors.
Limited Longitudinal Tracking: They don't allow for tracking changes in adherence over time, making it harder to understand the dynamics of non-adherence behaviors.
Potential for Bias: Self-reported data, common in cross-sectional study, can be prone to recall bias or social desirability bias.
Generalizability Concerns: The sample selected was not be representative of the broader population, limiting the generalizability of findings says a study on non-adherence to anti-TB drugs.
Implications and Recommendations
Implications
Treatment Failure: Non-adherence can lead to treatment failure, continued infectiousness, and the development of drug-resistant TB.
Public Health Risk: Untreated or improperly treated TB poses a significant risk of transmission to others.
Increased Treatment Costs: Non-adherence can lead to increased healthcare costs due to readmissions, longer treatment durations, and the need for more expensive treatments.
Recommendations
Comprehensive Counseling: TB patients should be thoroughly counseled on the importance of adhering to treatment, potential side effects, and the need for follow-up appointments.
Improved Health Education: Patients and their families should receive comprehensive education about TB, its transmission, and the importance of adherence to treatment.
Stronger Social Support: Strengthening social support networks through family involvement, community support groups, and peer support can significantly improve adherence.
Addressing Systemic Barriers: Addressing systemic barriers such as long waiting times, inadequate transportation, and lack of access to healthcare facilities can improve adherence.
Directly Observed Therapy (DOTS): Implementing DOTS, where healthcare providers directly observe patients taking their medication, can significantly improve adherence.
Conclusions
In conclusion, this study evaluated determinants of non-adherence and prevalence of non-adherents taking anti-TB drugs. Compared to the earlier research mentioned, this study discovered a rather modest rate of non-adherence among non-adherents’ patients on anti-TB therapy. Gender was identified as major variables impacting treatment adherence (Table 2). Males were more likely to remain committed to treatment than females as there was a significant association of (X2 = 65.00; P value of <.001). Age, marital status, educational level, employment status and HIV status were all studied, but none were shown to be statistically significant predictors of non-adherence.
Socioeconomic status, educational level, side effects of drugs, HIV co-infection, and length of stay at the medical institution, support from clinic staff and family were all factors linked to non-adherents to anti-TB medication. The study’s results showed that the facility’s waiting period was less likely to be a factor in non-adherence, although it cannot be ruled out entirely.
A thorough treatment program utilizing a patient-centered strategy is recommended considering the elements this study showed to be linked to non-adherence in TB patients at a South African public health clinic. The comprehensive treatment program that is being promoted should address risky behaviors (like alcohol and tobacco use), structural factors (like poverty), and psychosocial well-being. For instance, TB patients (with or without HIV) should receive relationship counseling on how to deal with a sexually discordant partner. They should also receive counseling on their perceived health status and co-morbid illnesses.
Author Contributions
L.N.K.K. conceptualization formal analysis and validation, data collection, creation of the initial draft, writing, editing, and reviewing. Project management included data gathering, analysis, and interpretation; paper preparation; and the choice to publish the findings.
Funding
There was no funding for this study.
Acknowledgments
The author acknowledges the manager of the clinic where the data was collected from. The patients who agreed to take part in the study after giving their consent. Miss Zingisa Kholiwe who did the final editing of the article.
Competing interest
The author declares that there is no financial or personal relation that may have inappropriately influenced in writing this article
Disclaimer
The views and opinions expressed in this article are those of the author and do not necessarily reflect the official policy or position of any affiliated agency of the authors.
References
- World Health Organization. Tuberculosis, Key facts. WHO 2025. Available from: https://www.who.int/news-room/fact-sheets/detail/tuberculosis. Accessed on 6 Jan 2025.
- World Health organization. TB Overview. WHO 2025. Available from: https://www.who.int/news-room/fact-sheets/detail/tuberculosis. Accessed on 1 Feb 2025.
- World Health Organization. Tuberculosis. WHO 2025. Available from: https://www.who.int/news-room/fact-sheets/detail/tuberculosis. Accessed on 7 June 2025.
- World Health organization. Global Tuberculosis Report, Tuberculosis. WHO 2024. Available from: https://www.who.int/health-topics/tuberculosis#tab=tab_1. Accessed on 2 Feb 2025.
- World Health Organization. Tuberculosis resurges as top infectious disease killer. WHO 2024. Available from: https://www.who.int/news/item/29-10-2024-tuberculosis-resurges-as-top-infectious-disease-killer. Accessed on 5 Feb 2025.
- Barter, D.M.; Agboola, S.O.; Murray, M.B.; Bärnighausen, T. Tuberculosis and poverty: the contribution of patient costs in sub-Saharan Africa – a systematic review. BMC Public Health 2012, 14, 12:980. Available from: http://www.biomedcentral.com/1471-2458/12/980doi:10.1186/1471-2458-12-980. Accessed on 11 Jan 2025.
- Boru, C.G.; Shimels, T.; Arebu, I.; Bilal, C. Factors contributing to non-adherence with treatment among TB patients in Sodo Woreda, Gura.ge Zone, Southern Ethiopia: A qualitative study. J. of Infect. Pub. Health 2017, 10, 527-533. https://doi.org/10.1016/j.jiph.2016.11.018. Available from: https://www.sciencedirect.com/science/article/pii/S1876034117300333. Accessed on 5 Apr 2025.
- World Health Organization. WHO calls for urgent action to address worldwide disruptions in tuberculosis services putting millions of lives at risk. WHO, 2025. Available from: https://www.who.int/news/item/20-03-2025. Accessed on 5 March 2025.
- Mkhavele, B.; Zondi, S.; Cele, L.; Mogale, M.; Mbelle, M. Factors associated with successful treatment outcomes among tuberculosis patients in a district municipality of Vhembe, Limpopo. S. Afr. Fam. Pract. 2025, 67, a6030. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. WHO Global Tuberculosis report of 2024. TB Incidence. WHO 2025. Available from: https://www.who.int/teams/global-programme-on-tuberculosis-and-lung-health/. Accessed on 25 Jan 2025.
- Floyd, K.; Glaziou, P.; Houben, R.; M.; G.; J.; Sumner, T.; White, R.; Raviglion, M. Global tuberculosis targets and milestones set for 2016–2035: definition and rationale. Int J Tuberc Lung Dis. 2018, 1;22(7):723–730. doi: 10.5588/ijtld.17.0835. https://pmc.ncbi.nlm.nih.gov/.
- Houben, R.; M.; Dodd, P.; J. The global burden of latent tuberculosis infection: a re-estimation using mathematical modelling. Sustainable Development Goals [website]. New York: United Nations 2024. https://sdgs.un.org.
- United Nations. Sustainable Development Goals. Ensure healthy lives and promote well-being for all ages. New York: United Nations 2024. https://www.un.org/sustainabledevelopment/health. Accessed on 8 June 2024.
- Kastien-Hilka, T.; Rosenkranz, B.; Schwenkglenks, M.; Bennett, B.M.; Sinanovic, E. Association between health-related quality of life and medication adherence in pulmonary tuberculosis in South Africa. Frontiers in pharmacology 2017, 8, p.919.
- WHO. What is DOTS? A guide to understanding the WHO recommended TB control strategy known as DOTS. WHO 1999. WHO/CDS/CPC/TB/99.270.
- Yin, J.; Yuan, J.; Hu, Y.; Wei, X. Association between Directly Observed Therapy and Treatment Outcomes in Multidrug-Resistant Tuberculosis: A Systematic Review and Meta-Analysis. PLoS ONE 2016, 11, 3: e0150511. https://doi.org/10.1371/journal.pone.0150511. Available from: https://journals.plos.org/plosone/article?id=10.1371/journal.pone.0150511. PMID: 26930287. Accessed on Dec. 2024.
- Collins, D.; Njuguna, C. The economic cost of non-adherence to TB medicines resulting from stock-outs and loss to follow-up in Kenya. In: Submitted to the US Agency for International Development by the Systems for Improved Access to pharmaceuticals and services (SIAPS) program. Arlington: Management Sciences for Health; 2016.
- SIAPS, U. Economic cost of Nonadherence to TB medicines resulting from stock-outs and loss to follow-up in the Philippines (Report) [Internet]. 2016. Available from: https://siapsprogram.org/publication/the-economic-cost-of-non-adherence-to-tb-medicines-resulting-from-stock-outs-and-loss-to-follow-upin-the-philippines/. Accessed on 10 Apr 2025.
- Grange, J.M.; Gandy, M.; Farmer, P.; Zumla, A. Historical declines in tuberculosis: nature, nurture and the biosocial model. Int J Tuberc Lung Dis. 2001, 5, 208–12. Available from: https://www.ncbi.nlm.nih.gov/pubmed/11326817. Accessed on 7 Feb 2025.
- Styblo K, Meijer J, Sutherland I. [The transmission of tubercle bacilli: its trend in a human population]. Bull World Health Organ. 1969, 41, 137–78. Available from: https://www.ncbi.nlm.nih.gov/pubmed/5309081. Accessed on 5 Jan 2025.
- Ndjeka, N. O.; Matji, R.; Ogunbanjo, G.A. An approach to the diagnosis, treatment and referral of tuberculosis patients: The family practitioner’s role. SA Fam Pract. 2008, 50, 44-50.
- World Health Organisation. Tuberculosis. TB and HIV. WHO, 2025. Available from:https://www.who.int/news-room/fact-sheets/detail/tuberculosis. Accessed in Feb 2025.0.
- Obermeyer, Z.; Abbott-Klafter, J.; Murray, C.; J. Has the DOTS strategy improved case finding or treatment success? An empirical assessment. PLoS One 2008, 3, e1721. 000. 0001721 PMID: 18320042.
- World Health Organization. Geneva: WHO. Adherence to long-term therapies: evidence for action. WHO 2003. [Internet] [cited Dec 26]. Available from: https://apps.who.int/iris/handle/10665/42682.
- Moodley, N.; Saimen, A.; Zakhura, N.; Motau, D.; Setswe, G.; Charalambous, S.; Chetty-Makkan, C.M. They are inconveniencing us’-exploring how gaps in patient education and patient centered approaches interfere with TB treatment adherence: perspectives from patients and clinicians in the Free State Province, South Africa. BMC Public Health 2020, 20, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Goosby, E.; Jamison, D.; Swaminathan, S.; Reid, M.; Zuccala, E. The Lancet Commission on tuberculosis: building a tuberculosis-free world. The Lancet 2018, 391, 1132–1133. [Google Scholar] [CrossRef] [PubMed]
- Gebremariam, R.B.; Wolde, M.; Beyene, A. Determinants of adherence to anti-TB treatment and associated factors among adult TB patients in Gondar city administration, Northwest, Ethiopia: based on health belief model perspective. J. Health, Population and Nutrition 2021, 40:49. [CrossRef]
- Anyaike, C.; Musa, O.I.; Babatunde, O.; Bolarinwa, O.; Durowade, K.A.; Ajayi, O.S. Adherence to tuberculosis therapy in Unilorin teaching hospital, Ilorin, north-central Nigeria. Int. J. Sci. Technol, 2013, 2, 2278–3687.
- Cramm, J.M.; Finkenflügel, H.J.; Møller, V.; and Nieboer, A.P. TB treatment initiation and adherence in a South African community influenced more by perceptions than by knowledge of tuberculosis. BMC public health 2010, 10, pp.1-8.
- Slovin, E. Slovin’s Formula for Sampling Technique. 1960. https://prudencexd.weebly.com/.
- Diedrich, C.R.; Flynn, J.L. HIV-1/mycobacterium tuberculosis coinfection immunology: how does HIV-1 exacerbate tuberculosis? Infection and immunity, 2011, 79, 1407-1417.
- Woimo, T.T.; Yimer, W.K.; Bati, T.; Gesesew, H.A. The prevalence and factors associated for anti-tuberculosis treatment non-adherence among pulmonary tuberculosis patients in public health care facilities in South Ethiopia: across-sectional study. BMC Public Health 2017, 17, 269. Available from: https://bmcpublichealth.biomedcentral.com/articles/10.1186/s12889-017-4188-9.
- Tesfahuneygn, G.; Medhin, G.; Legesse, M. Adherence to Anti-tuberculosis treatment and treatment outcomes among tuberculosis patients in Alamata District, northeast Ethiopia. BMC. Res. Notes 2015, 8, 503. [Google Scholar] [CrossRef] [PubMed]
- Kebede, A.; Wabe, N.; T. Medication adherence and its determinants among patients on concomitant tuberculosis and antiretroviral therapy in Southwest Ethiopia. N Am J Med Sci. 2012, 4, 67–71. [Google Scholar] [PubMed]
- Sackett, L.D.; Haynes, R.B.; Gordon, H.G.; Tugwell, P. Clinical Epidemiology. A basic science for clinical medicine. Textbook of Clinical Epidemiology London. 2nd ed. London: Little, Brown and Company; 1991.
- Adams, S.A.; Soumeraj, B.S.; Jonathan, L.; Doss-Degan, D. Evidence of self report bias in assessing adherence to guidelines. Intern. J. for. Qual. In. Health Care 1999, 187–192. [Google Scholar] [CrossRef] [PubMed]
- Fairley, C.K.; Permana, A.; Read, T.R.H. Long term utility of measuring adherence by self-report compared with pharmacy record in a routine clinic setting. HIV Medicine 2005, 6:366369.
- World Health Organisation. Global TB report. TB incidence. WHO, 2023. Available from: https://www.who.int/teams/global-programme-on- tuberculosis-and-lung-health/. Accessed on 15 Dec 2024.
- Naidoo, P.; Peltzer, K.; Louw, J.; Matseke, G.; Mchunu, G.; Tutshana, B. Predictors of tuberculosis (TB) and antiretroviral (ARV) medication non-adherence in public primary care patients in South Africa: a cross-sectional study Pamela. BMC Public Health 2013, 13:396. http://www.biomedcentral.com/1471-2458/13/396.
- Arentz, M.; Pavlinac, P.; Kimerling, M.E.; Horne, D.J.; Falzon, D.; Schünemann, H.; J. et al. Use of Anti-Retroviral Therapy in Tuberculosis Patients on Second-Line Anti-TB Regimens: A Systematic Review. PLoS ONE 2012, 7, e47370. ttps://doi.org/10.1371/journal.pone.0047370.
- World Health Organisation. Tuberculosis: Multidrug-resistant (MDR-TB) or rifampicin-resistant TB (RR-TB). WHO 2024. Available from: https://www.who.int/news-room/questions-and-answers/item/tuberculosis-multidrug-resistant-tuberculosis. Accessed on Mar 2025.
- Rieder, H. L. Interventions for tuberculosis control and elimination: International Union Against Tuberculosis and Lung Disease Paris; International Union Against Tuberculosis and Lung Disease 2002.
- Wohlleben, J.; Makhmudova, M.; Saidova, F.; Azamova, S.; Mergenthaler, C.; Verver, S. Risk factors associated with loss to follow-up from tuberculosis treatment in Tajikistan: a case-control study. BMC infectious diseases 2017, 17, pp.1-8.

Table 2.
Sociodemographic characteristics and their association with treatment adherents.
|
Sociodemographic variables |
Treatment Adherents | Pearson chi-Square Tests | ||
| Adherents n % | Non-Adherents n % | X2 | P Value | |
|
Gender n % Male 41 (63.08) Female 24 (36.92) |
30 (66.70) 15 (33.30) |
11 (55.00) 9 (45.00) |
65 | <.001 |
|
Age range 18-25 13(20.00) 26-35 26(40.00) 36-45 14(21.53) 46-55 4(6.15) >55 8(12.30) |
10 (22.20) 16 (35.60) 10 (22.20) 4 (8.90) 5(11.10) |
3 (15.00) 10 (50.00) 4 (20.00) 0 (0.00) 3 (15.00) |
3.394 | 0.494 |
|
Marital Status Single 53(81.54) Married 12(18.46) |
38 (84.40) 7 (15.60) |
15 (75.00) 5 (25.00) |
0.142 | 0.706 |
|
Educational Status High School 53(81.54) Tertiary Level 12(18.54) |
40 (75.47) 5 (45.10) |
13 (24.53) 7 (35.00) |
0.142 | 0.706 |
|
Income Status Unemployed 35(53.84) 1000-3000 12(18.46) 3001-5000 9(13.84) >5000 9(13.84) |
22 (48.90) 6 (13.30) 9 (20.00) 8 (17.80) |
13 (65.00) 6 (30.00) 0 (0.00) 1 (5.00) |
4.035 | 0.258 |
|
HIV Status Sero Positive 30(46.20) Sero Negative 35(53.80) |
19(42.20) 26(57.80) |
11 (55.00) 9 (45.00) |
0.002 | 0.968 |
Table 3.
Patient Program and drug related factors affecting non-adherence.
| Factors affecting the patients | Prevalence (n) | Percentage (%) |
| Substance use | 11 | 55 |
| Distance to the clinic | 14 | 70 |
| Adverse effects of the treatment | 11 | 55 |
| Poor interaction with the staff at the clinic | 3 | 15 |
| Lack of family support | 14 | 70 |
| Unemployment/Poverty | 13 | 65 |
| Shortage of drugs at the clinic | 7 | 35 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



