Submitted:
29 April 2025
Posted:
30 April 2025
You are already at the latest version
Abstract
For veterinarians and veterinary technicians, it is very important, but difficult, to precisely deter-mine the extent of animal pain. The purpose of this study was to examine postoperative pain in dogs by continuously recording electrocardiograms 24 h after surgery using a Holter monitor and combining heart rate variability, autonomic nervous activity changes, with behavioral indicators. Seventeen dogs that underwent surgery under general anesthesia at the Animal Medical Center of Rakuno Gakuen University were included. Immediately after surgery and 3, 6, 12, and 24 h after surgery, the above mentioned endpoints were evaluated. Heart rate tended to decrease continuously until 12 h after surgery, although relatively large individual differences were observed. In many cases, the coefficient of variation of the R-R interval was the lowest immediately after surgery, indicating that the sympathetic nervous system was dominant during anesthetic recovery. It was possible to reconfirm that the subjectivity of the evaluator was very strong in postoperative pain management using the dog’s acute pain scale. The evaluation of postoperative pain status in dogs is greatly influenced by various factors. In particular, postoperative stress may have a significant effect. Therefore, the combined evaluation of multiple factors is important for accurate assessment.
Keywords:
postoperative pain
; dogs
; heart rate variability
; autonomic nervous system
; electrocardiography
; canine acute pain scale
; pain assessment
; Holter monitoring
; general anesthesia
; physiological pain indicators
1. Introduction
Proper pain management has become common from both medical and welfare perspectives when treating animals with noxious stimuli [1,2,3,4,5]. According to survey data from Great Britain, approximately 70% of pet owners want analgesics to be prescribed after any type of surgery, and the number of veterinarians prescribing analgesics to meet the demands of pet owners is increasing [3,4,6].
When considering prescribing post-surgery analgesics, veterinarians should always consider not only the dosage and types of analgesics that are prescribed, but also whether the animal is properly managed [5,7]. Some of the typical aspects to consider to achieve appropriate management are: preemptive analgesia, in which analgesia is performed before the noxious stimuli are applied under anesthesia; and multimodal analgesia, in which a combination of drugs with different mechanisms and durations of action is used [8]. There are several methods for the evaluation of the degree of pain felt by patients after surgery and effect of analgesic treatment, e.g., the Numerical Rating Scale (NRS), Visual Analogue Scale (VAS) and Glasgow Composite Measure Pain Scale-short form (CMPS-SF) [9,10,11,12]. In the field of veterinary medicine, the main method that is used is a semi-objective method in which the evaluator observes the condition of the animal, with a particular focus on behavioral changes.
There are major limitations with this method, because of which it is very difficult to properly evaluate the degree of pain felt by animals. For example, the evaluation is largely subjective to the evaluator, and animals can show similar behaviors that do not always indicate the same degree of pain. Therefore, while the pain of an animal should be evaluated appropriately, there is no current solution for proper and specific management of further assessed pain [11,13,14,15].
Heart rate (HR) is attracting attention as one of the evaluation methods for pain. It has been reported that changes in the balance between sympathetic and parasympathetic nervous system activities, analyzed by frequency analysis of the electrocardiogram, are very useful for assessing the physiological state of the body, including autonomic nervous system activity and cardiovascular function [16,17]. In addition, there are many studies that use these electrocardiographic evaluations to assess surgery and its prognosis, as maintaining the balance of the sympathetic and parasympathetic nervous systems is beneficial in suppressing the occurrence of atrial fibrillation following surgery [18].
The purpose of this study was to re-examine postoperative pain evaluation in dogs by adding, as an evaluation method, the fluctuation of the balance between sympathetic and parasympathetic nervous system activities by frequency analysis of the electrocardiogram using a Holter monitor.
2. Materials and Methods
2.1. Clinical Cases
Electrocardiograms were continuously recorded for 24 h after the completion of general anesthesia in 17 dogs that underwent surgery at the Animal Medical Center of Rakuno Gakuen University. The general condition of all cases was classified based on the American Society of Anesthesiologists (ASA) status and severity (risk) of each case. An anesthetic protocol was devised taking into account the type of surgery and degree of pain. Table 1, Table 2 and Table 3 show the outline of the cases, types of surgery and expected degree of pain, and anesthetic protocol, respectively.
2.2. Recording and Analysis of Continuous Electrocardiogram
A Holter monitor (QR2600, Fukuda ME Kogyo Co. Ltd., Tokyo, Japan) was attached before maintenance anesthesia was completed to record and measure continuous electrocardiograms after surgery (Figure 1). In all cases, the measurement recording was stopped after 24 h, the electrodes were removed, and the recording was analyzed.
2.3. Postoperative Pain Evaluation
Pain evaluation was performed using the Dog’s Acute Pain Scale (Figure 2) every 3 h after surgery. Evaluation was performed by senior veterinary students (fifth or sixth year) who assisted in perioperative anesthesia management or by the veterinarian in charge of inpatients, based on their own judgment. If evaluated as Point 2 or higher, as described below, additional analgesia was administered by the veterinary anesthetist. Furthermore, according to the results of pain evaluation at the Post-3h, Post-6h, and Post-12h evaluations on the time axis described below, the cases were classified into one of two groups, a group with a high pain evaluation level (high-level group: Levels 1 to 4) and a group with a low pain evaluation level (low-level group: Level 0), and compared.
The Colorado State University Dog’s Acute Pain Scale is a pain scale that combines a numerical rating scale and complex behavioral observations. The evaluation includes items on psychological and behavioral status, palpation, and body tension. Scores were determined from 0 to 4, and additional analgesics were administered if the score was 2 or higher, according to the scale’s rules.( Mich MP, Hellyer WP, Kogan L, Schoenfeld-Tacher R. Effects of a pilot training program on veterinary students’ pain knowledge, attitude, and assessment skills. J Vet Med Educ 2010;37:358–68)
2.4. Electrocardiographic Analysis
The electrocardiography data obtained were analyzed using a Holter analyzer (HS1000, Fukuda ME Industry Co. Ltd., Tokyo, Japan). Changes in the observed HR data and coefficient of variation of the R-R interval (CVR-R) were compared at the following five analysis points:
a) Immediately after surgery (Post)
b) 3 h after the end of surgery (Post-3h)
c) 6 h after the end of surgery (Post-6h)
d) 12 h after the end of surgery (Post-12h)
e) 24 h after the end of surgery (Post-24h)
2.5. Statistical Analyses
All measurement data were expressed as the mean ± standard deviation. Differences between HR and CVR-R values at each measurement point were compared using the paired t -test and Wilcoxon signed rank sum test. In addition, the correlation between HR and CVR-R at each measurement point was examined using Spearman’s rank correlation coefficient test and Pearson’s correlation coefficient test. Mann-Whitney U test was used to compare HR and CVR-R between high and low levels on the Dog’s Acute Pain Scale. All statistical analyses were performed using SPSS software(IBM SPSS Statistics, TD SYNNEX K.K., Tokyo, Japan). In each case, p < 0.05 was set as statistically significant.
3. Results
Changes in HR in each case are shown in Figure 3-1-1, and changes in CVR-R are shown in Figure 3-2-1. Detailed data analysis is shown in -2 and 3-2-2.
HR was the highest immediately after the completion of the surgery in 13 of the 17 measured cases, and there were statistically significant differences between immediately post-surgery (Post) and all of the other measurement points. Furthermore, statistically significant differences were observed between post-3h and post-6h and between post-12h and post-24h (Figure 3-1-1). HR was highest at post-3h in a dog that underwent bladder lithotomy in combination with partial splenectomy and intraperitoneal lymph node resection (Case 13). The highest value at post-6h was in a dog that underwent left eye (oculus sinister) phacoemulsification / intraocular lens insertion (Case 15) and at Post-24h in a dog that underwent left knee extra-articular braking (lateral suture) (Case 16) (Figure 3-1-2).
CVR-R showed the lowest value at post in 13 of 17 cases and the highest value at Post-12h in 9 cases, and statistically significant differences were observed between all measurement points and Post. Furthermore, a statistically significant difference in CVR-R was also observed between post-6h and post-12h (Figure 3-2-1). However, some cases showed different dynamics. Case 14 (right knee joint extra-articular braking method [lateral suture]) had the lowest CVR-R value at post-6h, and Cases 15 (left eye phacoemulsification and intraocular lens insertion), 16 (left knee extra-articular braking [lateral suture]), and 17 (left phacoemulsification and intraocular lens insertion) had the lowest value at post-24h (Figure 3-2-2). In addition, Cases 2 (mastocytoma resection and superficial cervical / axillary lymph node resection), 5 (bile cystectomy and castration), 10 (binocular cherry eye restoration and right eye conjunctival flap), 12 (mastocytoma resection), and 15 (phacoemulsification of the left eye and intraocular lens insertion) showed the highest CVR-R value at post-3h (Figure 3-2-3). Cases 8 (partial mandibular resection and mandibular lymph node resection) and 11 (right femoral head / neck resection) showed the highest CVR-R value at post-6h, and Case 14 (right knee joint extra-articular braking method [lateral suture]) showed the highest value at post-24h (Figure 3-2-4).
Table 4 shows the results of postoperative pain management using the Dog’s acute pain scale and additional analgesic treatments performed.
In many cases, pain was evaluated as Score 0, but 1 case was evaluated as Score 3 or higher (strong pain), 1 case was evaluated as Score 2 (moderate pain), and some cases were evaluated as Score 1 (slight pain). In addition, the mean values of HR and CVR-R in the high-Score (Score 1 to 3) and low-Score groups (Score 0) using the Dog’s Acute Pain Scale were compared between each measurement point (Figure 3-3-1).
There was no statistically significant difference between the high-score and low-score groups in either HR or CVR-R at all measurement points.
Figure 3-3-2 (a and b) shows that the changes in HR and pain score, as evaluated using the Dog’s Acute Pain Scale, had similar movements. In these movements, a high pain score of Score 3 at post-3h occurred when HR showed a high value, and then the pain score reduced as HR decreased. Similarly, fluctuations in HR and pain level were recognized in conjunction with one another.
However, Figure 3-3-2 (c and d) shows that the changes in HR and pain score evaluated using the Dog’s Acute Pain Scale had different movements. In these cases, the pain score was evaluated as Level 1 at post-3h and post-6h when HR was low, although the pain score was low (Score 0) at Post with a high HR.
4. Discussion
There are many reports of changes in HR during the perioperative period, especially those related to surgery. For example, a study of surgical stress response during surgery in dogs with pyometra undergoing ovariohysterectomy found that HR increased during uterine horn manipulation and mesovarium incision and ligation compared with skin incision [19]. In addition, in a study comparing the surgical stress response during surgery, there was no significant difference in HR between dogs diagnosed with pyometra and healthy dogs that underwent ovariohysterectomy [20].
The HR measurements in this study showed the highest value at Post in many cases, and a statistically significant decrease was observed up to post-24h. The high HR value at Post confirmed that the effects of maintenance anesthesia and analgesics used during surgery disappeared when recovering from anesthesia, and circulatory depression was restored accordingly. At the same time, Post was considered to be the time when discomfort and pain sensation began to be felt as consciousness and sensation restored [21,22].
However, there were some cases where it took longer for HR to decrease than in others, and there were some cases in which HR increased after a time lapse from the end of surgery. Post did not show the highest value in these cases. Factors that may cause high HR at measurement points other than Post include persistent pain due to surgery, burden on the surgical site caused by body movements or repositioning, and persistent tension [23,24]. Further, looking back at the hospitalization records, the measurement points set in this study happened to coincide with the time of hospitalization management and treatment of animals, and cases in which HR did not show the highest value at Post were strongly suspected to be related to the effects of hospitalization management.
The results of the HR evaluation obtained in this study are useful to show that it is important to fully understand the occurrence of pain. Further, the results are also useful for showing that it is necessary to keep a record of hospitalization, nursing management, and treatment with the elapsed time and observation time after surgery, as well as to fully consider the psychological effects of the patient being agitated and tensed due to treatment.
In this study, statistically significant differences (p < 0.05) were observed in HR between Post and each measurement point, post-3h, post-6h, post-12h and post-24h. As mentioned above, HR is most likely to increase at Post due to restoration of the pain response with consciousness and sensation. Furthermore, bleeding caused by surgery and insensitive evaporation from surgical wounds was also related to the increase in HR after surgery (Post) [25].
The hemodynamics of animals are also regulated by the activity of autonomic nerve function and its balance. CVR-R, which is relatively widely used as a simple method for evaluating this nerve balance, is defined as the ratio of the mean to the standard deviation of the R-R interval on electrocardiography and is used for the quantitative evaluation of the activity of the entire autonomic nervous system [26]. In addition, the ratio of the power spectrum of the low-frequency component (LF) (low frequency ms2) and high-frequency component (HF) (high frequency ms2) can be used as a frequency domain index in heart rate variability, which could evaluate the balance of sympathetic nervous system activity. When this value is high, it can be evaluated as sympathetic nerve dominance, and when it is low, it can be evaluated as parasympathetic nerve dominance [26,27].
In this study, we combined parameters that show the activity and balance of the autonomic nervous system with the fluctuation of HR and attempted to perform a complex evaluation of the pain that animals feel after surgery. In many cases, the CVR-R showed a minimum value at Post that increased over time [28].
As mentioned above, the fluctuations in CVR-R reflect mental status. These fluctuations not only cause stress due to pain, but they also reflect psychological stress due to anxiety and tension [23,24].
A comprehensive evaluation of the changes in CVR-R and HR in this study confirmed that the sympathetic nervous system was dominant immediately after extubation/surgery. Furthermore, statistically significant differences were observed between Post and each measurement point and between post-6h and post-12h (all p < 0.01). In a study on the effects of electric acupuncture on the autonomic nervous system in dogs, the LF/HF values of healthy Beagle dogs were similar to those of dogs who had sympathetic dominance during the day and parasympathetic dominance during the night and when asleep [26].
In this study, we used the data from dogs undergoing surgery, unlike several previous studies, which have focused on healthy dogs. Therefore, it was considered that the increase in CVR-R observed in this study was mainly due to escape from the excitatory state immediately after the extubation and the relief of pain due to preoperative analgesic administration. However, in many cases, post-12h was around midnight or early morning, because of which the large fluctuations observed in this study were thought to be related to the daily cycle of autonomic nerve activity and parasympathetic dominance at night due to sleep. However, there were some cases in which CVR-R fluctuations showed unusual dynamics where the highest value was at post-12h and the lowest at Post. The autonomic function is thought to change depending on the degree of pain that an animal feels, the nature and temperament of the animal, changes in the environment, and drugs used for treatment and care [28,29]. As mentioned above, CVR-R has a low value when there is pain due to the burden on the surgical site during repositioning, tension, and excitement due to hospitalization. In addition, although there were individual differences, the animals were often sleeping in a cage in the hospital during daytime after surgery. Therefore, increases in CVR-R were observed even during the daytime.
In this postoperative pain management study, 6 of 17 cases were evaluated as having high pain scores on the Dog’s Acute Pain Scale. A dog undergoing partial maxillary resection (Case 3) underwent three additional analgesic procedures after surgery (first: 7 min after Post, second: 5 min before post-3h, third: post -1.5 h before -6h [4.5 post-surgery]). In this case, the post-3h pain score was evaluated as Score 3, and an increase in HR was observed from the first additional analgesic treatment to post-3h. From this, the dog was likely feeling severe pain due to surgery. In addition, the pain scores at post-6h and post-12h were both evaluated as Score 1, the pain score at post-24h was evaluated as Score 0, and HR decreased continuously to post-24h. It is possible that this indicated a change in the degree of pain. However, there were no statistically significant differences between the HR and CVR-R in the high-score group and those in the low-score group at each measurement point. Therefore, it was confirmed that HR and CVR-R fluctuated similarly in both groups. Contrary to that mentioned above, it is possible that HR and CVR-R are not able to accurately represent the degree of pain and that the pain scale evaluation does not match the patient’s pain level.
In the two cases shown in Figure 3-3-2, the changes in pain score and HR matched, and both the pain score and HR showed a high degree of pain. However, in the 2 cases shown in Figure 3-3-2, the pain score was high (Score 1) when HR was low, and the pain score was low (Score 0) when HR was high. It is difficult to assert that each of the pain scores indicates the degree of pain. In the veterinary field, it has been reported that VAS and NRS vary by 36.1% and 32.3%, respectively, even when different veterinarians evaluate the degree of pain in the same case [9,30]. Overall, integrating subjective evaluations, such as CMPS-SF, with objective physiological measures, like HR and CVR-R analyses, enhances the accuracy of postoperative pain assessment [12,30]. Generally, it is very difficult to objectively evaluate and share evaluation values of pain felt by animals. In our center, one case is often evaluated by multiple veterinarians and veterinary students at different evaluation points. For this reason, the results of pain scales will vary.
5. Conclusions
In this study, we examined whether we could evaluate pain more objectively using HR and CVR-R obtained by 24-h electrocardiogram recording immediately after surgery compared with the Dog’s Acute Pain Scale that is usually used. As a result, definite associations between the pain scale and HR and CVR-R could not be confirmed, and HR and CVR-R were not necessarily accurate evaluation scales for pain evaluation; thus, the Dog’s Acute Pain Scale was used. The evaluation was highly subjective and showed that there was a possibility of variation. However, evaluating HR and CVR-R and using the Dog’s Acute Pain Scale at the same time, trying to think more objectively about whether an animal is feeling pain, and removing prejudice and other subjectivity as much as possible are necessary. These practices will enable the proper assessment of pain levels in animals and practice of appropriate nursing care based on them.
Author Contributions
Conceptualization, Tadashi Sano and Kazuto Yamashita; methodology, Hiroshi Ueno; software, Tadashi Sano; validation, Kazuto Yamashita and Hiroshi Ohta; formal analysis, Tadashi Sano; investigation, Tadashi Sano; resources, Toshikazu Sakai, Hiroshi Ueno, and Seiya Maehara; data curation, Tadashi Sano; writing—original draft preparation, Tadashi Sano; writing—review and editing, Tadashi Sano; visualization, Tadashi Sano; supervision, Kazuto Yamashita; project administration, Tadashi Sano. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Ethical review and approval were waived for this study due to this data collection in patient management of regular surgical cases.
Informed Consent Statement
When performing surgical procedures, all possible risks, including general anesthesia management, are explained to the owner and consent was obtained before the surgery was performed.
Data Availability Statement
Not applicable.
Acknowledgments
I would like to thank all patient animals and their owners who contributed data for this study. I wish to thank all parties involved at Rakuno Gakuen University Veterinary Teaching Hospital for providing us with a place to manage our patients. I wish to thank Fukuda ME Kogyo Co. Ltd. for analysis of ECG data.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Muir, W.M. Acid–base physiology. In Veterinary Anesthesia and Analgesia: The Fifth Edition of Lumb and Jones, 5th ed.; Grimm, K.A., Lamont, L.A., Tranquilli, W.J., Greene, S.A., Robertson, S.A., Eds.; Wiley-Blackwell: Ames, Iowa, USA, 2015; pp. 357–371. [Google Scholar]
- Mosley, C.A. Anesthesia equipment. In Veterinary Anesthesia and Analgesia: The Fifth Edition of Lumb and Jones, 5th ed.; Grimm, K.A., Lamont, L.A., Tranquilli, W.J., Greene, S.A., Robertson, S.A., Eds.; Wiley-Blackwell: Ames, Iowa, USA, 2015; pp. 23–85. [Google Scholar]
- Stanway, G.W.; Taylor, P.M.; Brodbelt, D.C. A preliminary investigation comparing pre-operative morphine and buprenorphine for postoperative analgesia and sedation in cats. Vet Anaesth Analg 2002, 29, 29–35. [Google Scholar] [CrossRef] [PubMed]
- Demetriou, J.L.; Geddes, R.F.; Jeffery, N.D. Survey of pet owners’ expectations of surgical practice within first opinion veterinary clinics in Great Britain. J Small Anim Pract 2009, 50, 478–487. [Google Scholar] [CrossRef]
- Brodbelt, D.C.; Blissitt, K.J.; Hammond, R.A.; Neath, P.J.; Young, L.E.; Pfeiffer, D.U.; Wood, J.L.N. The risk of death: the confidential enquiry into perioperative small animal fatalities. Vet Anaesth Analg 2008, 35, 365–373. [Google Scholar] [CrossRef] [PubMed]
- Hunt, J.R.; Knowles, T.G.; Lascelles, B.D.X.; Murrell, J.C. Prescription of perioperative analgesics by UK small animal veterinary surgeons in 2013. Vet Rec 2015, 176, 493. [Google Scholar] [CrossRef] [PubMed]
- McGrath, P.A.; Hillier, L.M. The enigma of pain in children: an overview. Pediatrician 1989, 16, 6–15. [Google Scholar]
- Epstein, M.; Rodan, I.; Griffenhagen, G.; Kadrlik, J.; Petty, M.; Robertson, S.; Simpson, W. 2015 AAHA/AAFP pain management guidelines for dogs and cats. J Am Anim Hosp Assoc 2015, 51, 67–84. [Google Scholar] [CrossRef]
- Holton, L.L.; Scott, E.M.; Nolan, A.M.; Reid, J.; Welsh, E.; Flaherty, D. Comparison of three methods used for assessment of pain in dogs. J Am Vet Med Assoc 1998, 212, 61–66. [Google Scholar] [CrossRef]
- Yamagiwa, M.; Sakakura, Y. [Evaluation of throat discomfort with visual analogue scale (VAS)]. Nihon Jibiinkoka Gakkai Kaiho 1994, 97, 67–74. [Google Scholar] [CrossRef]
- Bech, R.D.; Lauritsen, J.; Ovesen, O.; Overgaard, S. The verbal rating scale is reliable for assessment of postoperative pain in hip fracture patients. Pain Res Treat 2015, 2015, 676212. [Google Scholar] [CrossRef]
- Reid, J. , Nolan, A.M., Hughes, J.M., Lascelles, B.D.X., Pawson, P., Scott, E.M. Development of the short-form Glasgow Composite Measure Pain Scale (CMPS-SF) and derivation of an analgesic intervention score. Anim Welf 2007, 16, 97–104. [Google Scholar] [CrossRef]
- Breivik, H.; Borchgrevink, P.C.; Allen, S.M.; Rosseland, L.A.; Romundstad, L.; Breivik Hals, E.K.; Kvarstein, G.; Stubhaug, A. Assessment of pain. Br J Anaesth 2008, 101, 17–24. [Google Scholar] [CrossRef] [PubMed]
- Akyrou, D.; Plati, C.; Baltopoulos, G.; Anthopoulos, L. Pain assessment in acute myocardial infarction patients. Intensive Crit Care Nurs 1995, 11, 252–255. [Google Scholar] [CrossRef]
- Holton, L.L.; Scott, E.M.; Nolan, A.M.; Reid, J.; Welsh, E. Relationship between physiological factors and clinical pain in dogs scored using a numerical rating scale. J Small Anim Pract 1998, 39, 469–474. [Google Scholar] [CrossRef]
- Pagani, M.; Lombardi, F.; Guzzetti, S.; Rimoldi, O.; Furlan, R.; Pizzinelli, P.; Sandrone, G.; Malfatto, G.; Dell’Orto, S.; Piccaluga, E. Power spectral analysis of heart rate and arterial pressure variabilities as a marker of sympatho-vagal interaction in man and conscious dog. Circ Res 1986, 59, 178–193. [Google Scholar] [CrossRef]
- Piccirillo, G.; Ogawa, M.; Song, J.; Chong, V.J.; Joung, B.; Han, S.; Magrì, D.; Chen, L.S.; Lin, S.F.; Chen, P.S. Power spectral analysis of heart rate variability and autonomic nervous system activity measured directly in healthy dogs with tachycardia-induced heart failure. Heart Rhythm 2009, 6, 546–552. [Google Scholar] [CrossRef] [PubMed]
- Amar, D.; Zhang, H.; Miodownik, S.; Kadish, A.H. Competing autonomic mechanisms precede the onset of postoperative atrial fibrillation. J Am Coll Cardiol 2003, 42, 1262–1268. [Google Scholar] [CrossRef]
- Lövebrant, J. Surgical stress response in dogs diagnosed with pyometra undergoing ovariohysterectomy. Sveriges lantbruksuniversitet (Swedish University of Agricultural Sciences), Uppsala, Sweden, 2013.
- Höglund, O.V.; Lövebrant, J.; Olsson, U.; Höglund, K. Blood pressure and heart rate during ovariohysterectomy in pyometra and control dogs: a preliminary investigation. Acta Vet Scand 2016, 58, 80. [Google Scholar] [CrossRef]
- McKune, C.M.; Murrell, J.C.; Nolan, A.M.; White, K.L.; Wright, B.D. Nociception and pain. In Veterinary Anesthesia and Analgesia: The Fifth Edition of Lumb and Jones, 5th ed.; Grimm, K.A., Lamont, L.A., Tranquilli, W.J., Greene, S.A., Robertson, S.A., Eds.; Wiley-Blackwell: Ames, Iowa, USA, 2015; pp. 584–626. [Google Scholar]
- Sessler, D.I. Perioperative thermoregulation and heat balance. Lancet 2016, 387, 2655–2664. [Google Scholar] [CrossRef]
- Morino, M.; Masaki, C.; Seo, Y.; Mukai, C.; Mukaibo, T.; Kondo, Y.; Shiiba, S.; Nakamoto, T.; Hosokawa, R. Non-randomized controlled prospective study on perioperative levels of stress and dysautonomia during dental implant surgery. J Prosthodont Res 2014, 58, 177–183. [Google Scholar] [CrossRef]
- McDonell, W.N.; Kerr, C.L. Physiology, pathophysiology, and anesthetic management of patients with respiratory disease. In Veterinary Anesthesia and Analgesia: The Fifth Edition of Lumb and Jones, 5th ed.; Grimm, K.A., Lamont, L.A., Tranquilli, W.J., Greene, S.A., Robertson, S.A., Eds.; Wiley-Blackwell: Ames, Iowa, USA, 2015; pp. 513–558. [Google Scholar]
- Teramoto, M. [The effect of hemorrhagic acute anemia on wound healing]. Japanese Journal of Oral and Maxillofacial Surgery 1980, 26, 919–928. [Google Scholar] [CrossRef]
- Kimura, Y.; Hara, S. The effect of electro-acupuncture stimulation on rhythm of autonomic nervous system in dogs. J Vet Med Sci 2008, 70, 349–352. [Google Scholar] [CrossRef] [PubMed]
- Matsumoto, Y.; Mori, N.; Mitajiri, R.; Jiang, Z. [Study of mental stress evaluation based on analysis of heart rate variability]. Journal of Life Support Engineering 2010, 22, 105–111. [Google Scholar] [CrossRef]
- Matsunaga, T.; Harada, T.; Mitsui, T.; Inokuma, M.; Hashimoto, M.; Miyauchi, M.; Murano, H.; Shibutani, Y. Spectral analysis of circadian rhythms in heart rate variability of dogs. Am J Vet Res 2001, 62, 37–42. [Google Scholar] [CrossRef] [PubMed]
- Bille, C.; Auvigne, V.; Libermann, S.; Bomassi, E.; Durieux, P.; Rattez, E. Risk of anesthetic mortality in dogs and cats: an observational cohort study of 3546 cases. Vet Anaesth Analg 2012, 39, 59–68. [Google Scholar] [CrossRef]
- Mathews, K.A. , Kronen, P.W., Lascelles, B.D.X., Nolan, A., Robertson, S., Steagall, P.V. Guidelines for recognition, assessment and treatment of pain. J Small Anim Pract 2014, 55, E10–E68. [Google Scholar] [CrossRef]
Figure 1.
Holter monitor (QR2600, Fukuda ME Kogyo Co. Ltd., Tokyo, Japan).

Figure 2.
The Dog’s Acute Pain Scale. (https://vetmedbiosci.colostate.edu/vth/wp-content/uploads/sites/7/2020/12/canine-pain-scale.pdf).
Figure 2.
The Dog’s Acute Pain Scale. (https://vetmedbiosci.colostate.edu/vth/wp-content/uploads/sites/7/2020/12/canine-pain-scale.pdf).
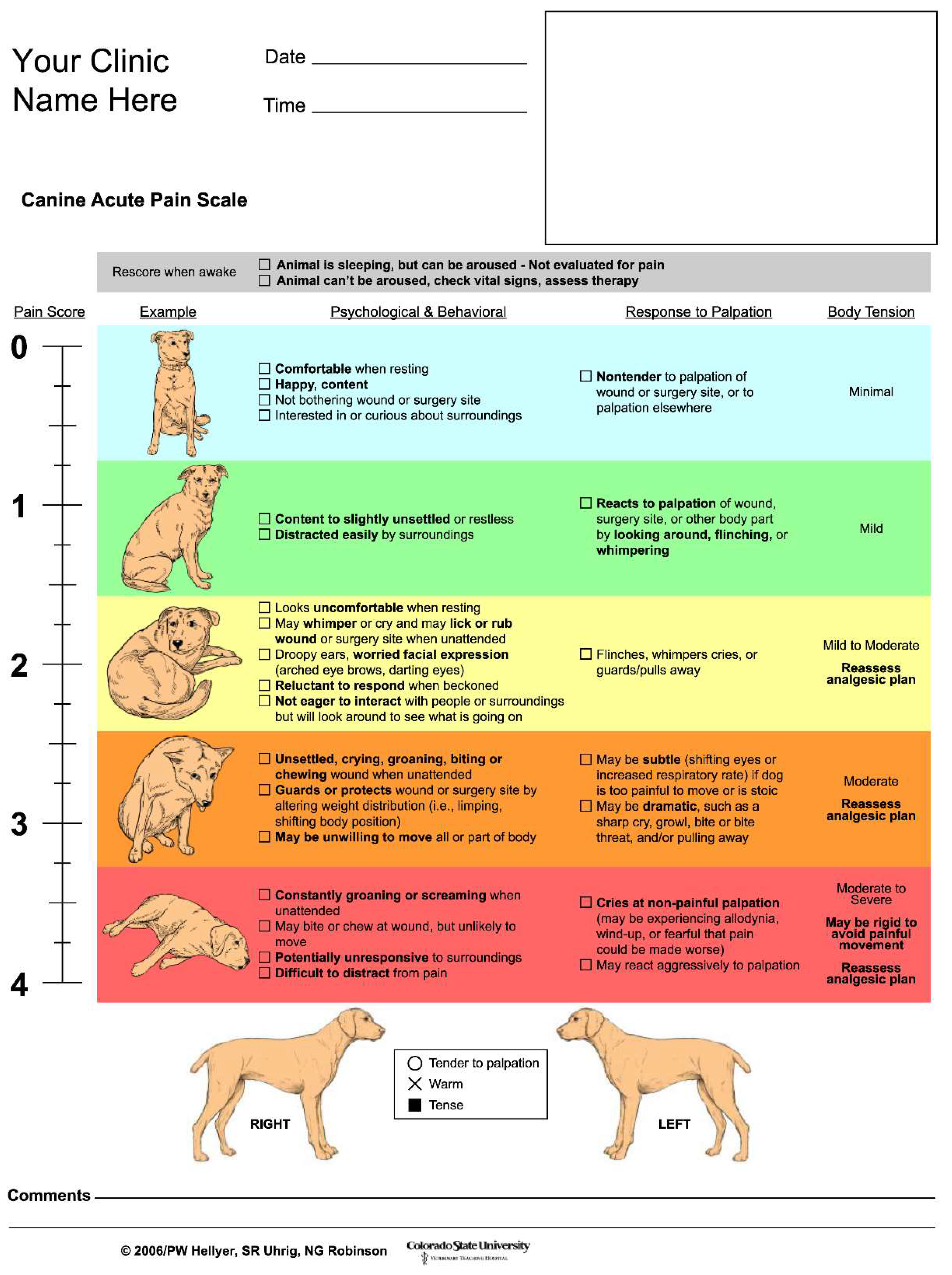
Figure 3.
Figure 3-1-1. Changes over time in HR. Figure 3-1-2. Detailed kinetics of HR in 4 cases that did not show the highest value at Post. Figure 3-2-1. Changes over time in CVR-R. Figure 3-2-2. Detailed kinetics of CVR-R in 4 cases that did not show the highest value at Post. Figure 3-2-3. Detailed kinetics of CVR-R in 5 cases that showed the highest value at Post-3h. Figure 3-2-4. Detailed kinetics of CVR-R in 3 cases that showed the highest value at Post-6h or Post-24h. Figure 3-3-1. Comparison of HR and CVRR between high-score and low-score groups on the dog acute pain scale at each measurement point. Figure 3-3-2. The changes in HR and pain score, as evaluated using the dog acute pain scale.
Figure 3.
Figure 3-1-1. Changes over time in HR. Figure 3-1-2. Detailed kinetics of HR in 4 cases that did not show the highest value at Post. Figure 3-2-1. Changes over time in CVR-R. Figure 3-2-2. Detailed kinetics of CVR-R in 4 cases that did not show the highest value at Post. Figure 3-2-3. Detailed kinetics of CVR-R in 5 cases that showed the highest value at Post-3h. Figure 3-2-4. Detailed kinetics of CVR-R in 3 cases that showed the highest value at Post-6h or Post-24h. Figure 3-3-1. Comparison of HR and CVRR between high-score and low-score groups on the dog acute pain scale at each measurement point. Figure 3-3-2. The changes in HR and pain score, as evaluated using the dog acute pain scale.
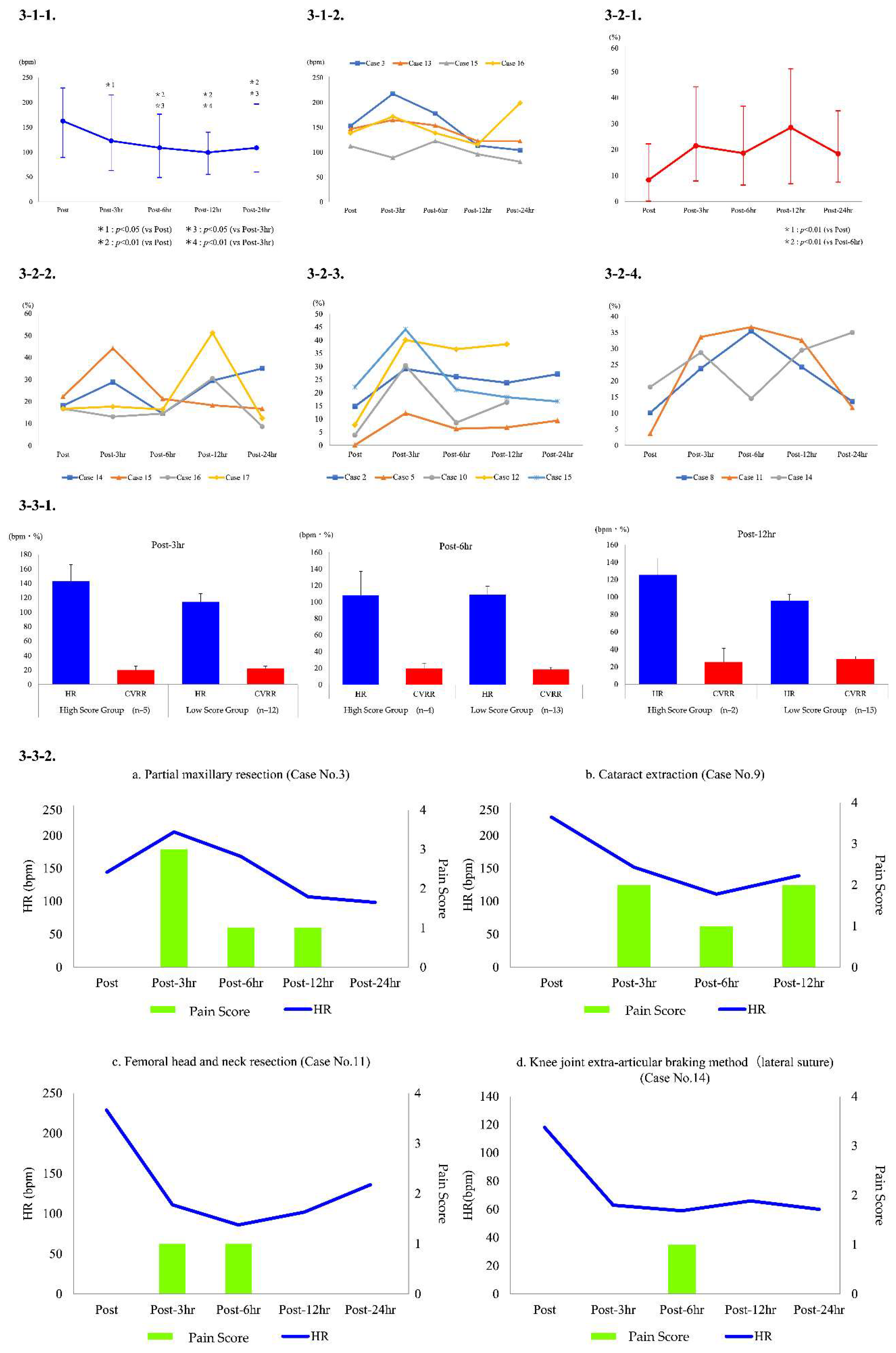

Table 1.
Outline of the cases.
| Case No. | Breed | Age | Sex |
|---|---|---|---|
| 1 | Labrador Retriever | 11y | Male |
| 2 | Shiba Inu | 6y 2m | Female |
| 3 | Chihuahua | 14y 1m | Spayed Female |
| 4 | Miniature Dachshund | 11y | Male |
| 5 | French Bulldog | 9y 5m | Male |
| 6 | Beagle | 12y 11m | Spayed Female |
| 7 | Pug | 12y 10m | Spayed Female |
| 8 | Miniature Dachshund | 11y 7m | Male |
| 9 | Papillon | 11y | Castrated Male |
| 10 | Pembroke Welsh Corgi | 13y 3m | Spayed Female |
| 11 | French Bulldog | 8m | Castrated Male |
| 12 | Miniature Dachshund | 10y 7m | Spayed Female |
| 13 | Shih Tzu | 10y 10m | Castrated Male |
| 14 | American Cocker Spaniel | 9y 11m | Castrated Male |
| 15 | Jack Russell Terrier | 2y 11m | Female |
| 16 | Toy Poodle | 9y 3m | Spayed Female |
| 17 | Cavalier King Charles Spaniel | 5y 1m | Male |
y: years; m: months.
Table 2.
Types of surgery and the expected degree of pain.
| Case No. | Types of surgery | Expected degree of pain |
|---|---|---|
| 1 | Partial mandibular resection / mandibular lymph node resection | Maximum |
| 2 | Body surface mast cell tumor resection / superficial cervical and axillary lymph node resection | Maximum |
| 3 | Partial maxillary resection | Maximum |
| 4 | Partial maxillary resection / mandibular lymph node resection | Maximum |
| 5 | Cholecystectomy / castration | Maximum |
| 6 | Liver mass removal / splenectomy | Maximum |
| 7 | Partial mandibular resection / mandibular lymph node resection / medial retropharyngeal lymph node resection | Maximum |
| 8 | Partial mandibular resection / mandibular lymph node resection | Maximum |
| 9 | Cataract extraction(OU) | Mild to moderate |
| 10 | Cherry eye repositioning (OU) / conjunctival flap surgery(OD) | Mild to moderate |
| 11 | Femoral head and neck resection | Moderate to severe |
| 12 | Mammary gland tumor resection | Mild to moderate |
| 13 | Splenectomy / intraperitoneal lymph node resection / cystolithiasis extraction | Maximum |
| 14 | Knee joint extra-articular braking method(lateral suture) | Maximum |
| 15 | Phacoemulsification and aspiration (OS) / intraocular lens implantation(OS) | Mild to moderate |
| 16 | Knee joint extra-articular braking method (lateral suture) | Maximum |
| 17 | Phacoemulsification and aspiration (OS) / intraocular lens implantation(OS) | Mild to moderate |
OU: oculus uterque; OD: oculus dexter; OS: oculus sinister.
Table 3.
Anesthetic protocol.
| Case No. | Anesthetic protocol | ||||
|---|---|---|---|---|---|
| Premedication | Induction agent | Maintenance anesthesia/Intraoperative analgesics | Post-operative analgesics | ASA classification | |
| 1 | Mid-Ket-Fent-Atr-Melx | P | OS/RFK | Fent-Ket | 2 |
| 2 | Mid-Ket-Fent-Atr-Melx | P | OS/RFK | Fent-Ket | 2 |
| 3 | Mid-Ket-Fent-Atr | P | OS/RFK | Fent-Ket | 2 |
| 4 | Mid-Ket-Fent-Atr-Melx | P | OS/RFK | Fent-Ket | 2 |
| 5 | Mid-Ket-Fent-Atr-Melx | P | OS/RFK | Fent-Ket | 2 |
| 6 | Mid-Ket-Fent-Atr | P | OS/RFK | Fent-Ket | 2 |
| 7 | Mid-Ket-Fent-Atr-Melx | P | OS/RFK | Fent-Ket | 2 |
| 8 | Mid-Ket-Fent-Atr-Melx | P | OS/RFK | Fent-Ket | 2 |
| 9 | Mid-Btr-Lid | P | OS/BL | Btr | 2 |
| 10 | Mid-Mor-Melx | P | OS | Bupre | 3 |
| 11 | Mid-Fent-Atr-Melx | P | P-TIVA/RF | Fent | 2 |
| 12 | Mid-Tram | A | OS | Bupre | 2 |
| 13 | Mid-Ket-Fent-Atr-Melx | P | OS/RFK | Fent-Ket | 2 |
| 14 | Mid-Ket-Fent-Atr-Melx | P | OS/RFK | Fent-Ket | 2 |
| 15 | Mid-Btr-Lid | P | P-TIVA/BL | Btr | 1 |
| 16 | Mid-Ket-Fent-Atr-RBCX | P | OS/RFK | Fent-Ket | 2 |
| 17 | Mid-Btr-Lid | P | P-TIVA/BL | Btr | 2 |
ASA: American Society of Anesthesiologists; Mid: midazolam; Ket, K: ketamine; Fent, F: fentanyl; Atr: atropine; Melx: meloxicam; Btr, B: butorphanol; Lid, L: lidocaine; Mor: morphine; Tram: tramadol; RBCX: robenacoxib; P: propofol; A: alfaxalone; OS: oxygen-sevoflurane; R: remifentanil; P-TIVA: total intravenous anesthesia with propofol; Bupre: buprenorphine.
Table 4.
Evaluation of each case using the Dog’s Acute Pain Scale and presence or absence of additional postoperative analgesics.
Table 4.
Evaluation of each case using the Dog’s Acute Pain Scale and presence or absence of additional postoperative analgesics.
| Case No. | Presence or absence of additional postoperative analgesia and administered drug information | The Dog’s Acute Pain Scale | |||
|---|---|---|---|---|---|
| Post-3h | Post-6h | Post-12h | Post-24h | ||
| 1 | Absent | 1 | 0 | 0 | 0 |
| 2 | Absent | 0 | 0 | 0 | 0 |
| 3 | Present; Fent i.v., ACE i.v. ×3 | 3 | 1 | 1 | 0 |
| 4 | Absent | 0 | 0 | 0 | 0 |
| 5 | Absent | 0 | 0 | 0 | 0 |
| 6 | Absent | 0 | 0 | 0 | 0 |
| 7 | Absent | 0 | 0 | 0 | 0 |
| 8 | Absent | 0 | 0 | 0 | 0 |
| 9 | Absent | 2 | 1 | 2 | |
| 10 | Absent | 1 | 0 | 0 | |
| 11 | Absent | 1 | 1 | 0 | 0 |
| 12 | Absent | 0 | 0 | 0 | |
| 13 | Absent | 0 | 0 | 0 | 0 |
| 14 | Absent | 0 | 1 | 0 | 0 |
| 15 | Absent | 0 | 0 | 0 | 0 |
| 16 | Absent | 0 | 0 | 0 | 0 |
| 17 | Absent | 0 | 0 | 0 | 0 |
i.v.: intravenous administration; ACE: acepromazine (first time: 0.05 mg/kg; second and third time: 0.025 mg/kg); Fent: fentanyl (5 μg/kg).
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



