
Submitted:
15 April 2025
Posted:
16 April 2025
You are already at the latest version
Abstract
Aim: Resin-based restorative materials have been the material of choice for direct dental restorations. However, the selection process remains multifaceted, while dentists often face the challenge of choosing the most suitable materials that not only meet clinical requirements but also align with their preferences, practice settings, and individual characteristics. This pilot study aimed to evaluate professional characteristics, knowledge levels, and selection criteria for resin-based restorative materials among dental clinicians at the National and Kapodistrian University of Athens.Materials and Methods: A cross-sectional questionnaire-based study was conducted between October 2023 and January 2025. A structured instrument comprising 23 closed-ended and 5 open-ended questions was administered to 87 dental clinicians. The questionnaire collected data on demographics, professional background, knowledge of resin materials, material selection preferences for anterior and posterior restorations, and influencing factors including economic and environmental considerations. Statistical analysis was performed using IBM SPSS version 29. Descriptive statistics, Spearman correlation coefficients, and Mann-Whitney tests were utilized to assess relationships between professional characteristics (e.g., clinical experience, age, postgraduate education) and material selection decisions.Results: Findings revealed that clinicians with over five years of experience demonstrated significantly higher knowledge of material composition (r = .230, p < .05) and shelf life (r = .223, p < .05). Less experienced practitioners prioritized anatomical and esthetic features, whereas experienced dentists favored specialized resin materials for anterior restorations. For posterior restorations, the majority (75.9%) selected packable composite resin for its superior mechanical properties and wear resistance. Additionally, procurement responsibility was associated with increased familiarity with industry specifications (r = .254, p < .05). Environmental considerations were noted as secondary factors, with notable gender-based differences observed.Conclusion: The study highlights that clinical experience and procurement involvement significantly influence the selection of restorative materials. While less experienced dentists focus on essential esthetic criteria, experienced clinicians incorporate a wider range of technical and regulatory factors. These insights report on the need for targeted educational interventions to bridge existing knowledge gaps and promote evidence-based decision-making in restorative dentistry.
Keywords:
Resin-based materials
; dental practitioners
; preference
; selection criteria
1. Introduction
In contemporary dental practice, composite resin has been a material of choice for direct restorations for decades [1]. The selection of these materials is crucial for ensuring the effectiveness and longevity of dental treatments [2]. Dentists frequently face the challenge of using a wide variety of products, aiming to meet clinical demands while also aligning with their individual preferences and the realities of their professional setting [3]. As an illustration, when treating a patient with bruxism on the posterior region, a dentist may focus on a composite material with high fracture resistance, whereas for an anterior restoration, esthetic properties might take precedence [4]. The pursuit of the ideal restorative material in dentistry focuses on identifying options that offer long-term stability, successful integration with adjacent tissues, and the ability to withstand functional stresses without compromising their structural integrity [5,6]. However, composite resin restorations face numerous challenges in the oral environment, which necessitate maintaining their intended chemical and mechanical properties over time [4,5,7].
Various methodologies have been employed to evaluate dental materials and ascertain their clinical suitability [8]. Manufacturers tend to develop materials that closely mimic the characteristics of natural teeth, yet achieving perfect replication remains an ongoing challenge [9,10]. To address these complex demands, different classification systems and testing protocols have been created to enhance the performance capabilities of restorative materials [11,12]. ISO standards delineate the requirements and specifications that ensure optimal performance in dental services while safeguarding both practitioners and patients [8]. These standards encompass essential aspects like material composition, physical properties, functional characteristics, and testing procedures to verify their efficacy [11,12]. ISO 4049:2019 specifically outlines requirements for polymer-based restorative materials, ensuring they comply with certain criteria for water sorption, solubility, and compressive strength, which are crucial for clinical success [1,10,13].Considering that many products utilized in everyday dental practice conform to specific ISO standards, it is essential to assess how much dentists consider these factors when choosing materials for conservative restorations based on well-defined criteria [14,15,16,17].
The choice-making process in relation to restorative materials in dentistry is multifaceted and is influenced by several factors [18]. Probably, the individual characteristics of dentists and clinical considerations such as age, experience, and level of education are most likely to affect the type of restoration that would be performed and the choice of material that could be used [19]. The more experienced dentists may have their own approaches to the choice of materials since they have had more time to observe their clinical effectiveness [20,21]. However, recent graduates may prefer to use new materials and methods which they have learned at university [22,23]. In addition, sustainability and recyclability are gradually becoming important factors that affect the purchasing decision [24,25,26]. For instance, some manufacturers are now offering composite packaging that is made from recycled materials or have taken back programs for used dental products to practitioners who are concerned with the environment [27,28,29]. These elements underline the complexity of the overall problem and the difficulty of selecting appropriate resin-based restorative materials for specific clinical situations.
Despite considerable research into the factors influencing preferences for different dental products, there remains a notable gap in the relevant literature regarding the evaluation of restorative material selection in dentistry. This study aims to address this multifaceted research void by adopting a comprehensive approach to selecting resin-based restorative materials. Through a survey-based methodology, gathering data on material choices, decision-making criteria, and awareness of environmental factors, it explores how clinical requirements, individual practitioner preferences, and external influences, such as economic and environmental considerations, affect these choices. The null hypothesis of this study posits that there is no significant relationship between dentists’ selection of resin-based restorative materials and influencing factors such as clinical requirements, individual practitioner preferences, economic considerations, or environmental awareness. In addressing this hypothesis, the study explores several key research questions. It seeks to determine which clinical criteria dentists prioritize when choosing resin-based restorative materials and how practitioner-specific characteristics, such as professional experience, area of specialization, and level of knowledge, affect these decisions. Furthermore, the study examines the role of external influences, including the cost and availability of materials, brand reputation, and broader economic factors. Finally, it investigates the extent to which environmental awareness plays a role in material selection and whether demographic or professional differences among dentists correspond to variations in their preferences.
2. Methods and Materials
2.1. Study Design and Sample
This cross-sectional study employed a questionnaire-based research design, a widely accepted method in healthcare research for collecting large volumes of data efficiently and systematically [30]. The structured questionnaire used in this study was carefully designed to gather both quantitative and qualitative data, allowing for a comprehensive assessment of dentists’ knowledge levels, professional backgrounds, and preferences regarding resin-based restorative materials [31,32]. The study was conducted between October 2023 and January 2025 and involved a total of 87 dentists employed at the Department of Dentistry of the National and Kapodistrian University of Athens. The objective was to evaluate their knowledge of resin-based restorative materials and to identify the key criteria influencing their selection for anterior and posterior restorations. This research adheres to the principles of ethical conduct in research involving human subjects and is conducted following the guidelines outlined in the Declaration of Helsinki. It was also approved by the Ethics and Research Committee of the Department of Dentistry (16.05.2024/44982). The study sample consisted of dental clinicians currently enrolled in the Department of Dentistry at the National and Kapodistrian University of Athens, Greece. Exclusion criteria included dental students, individuals from non-dental disciplines, and those who did not fulfill an informed consent.
2.2. Questionnaire Design
A structured questionnaire served as the primary data collection instrument for this study [33]. The questionnaire was developed based on current literature, expert input from restorative dentistry faculty, and preliminary pilot testing to ensure clarity and relevance [34]. It comprised multiple sections, including 1) Demographic information (e.g., age, gender), 2) Professional characteristics (e.g., years of clinical experience, postgraduate education, employment setting), 3) Knowledge assessment related to resin-based materials [30,35,36,37,38,39,40,41,42,43,44] 4) Material selection preferences for anterior and posterior restorations [16,20], 5) Influencing factors such as clinical, economic, and environmental considerations [45,46,47,48,49,50,51].
The pilot test was conducted on a small group of dentists (not included in the final sample) to assess the clarity, language, and logical flow of the questionnaire [52]. Based on pilot feedback, revisions were made to improve question-wording, remove ambiguity, and refine the structure of response options. The final questionnaire included closed-ended questions, multiple-choice items, and Likert-scale statements grouped into four main sections: demographic information, professional characteristics, knowledge of resin materials, and selection preferences for anterior and posterior restorations. To ensure content validity, the final questionnaire was reviewed by a panel of 2 experts in restorative dentistry from the National and Kapodistrian University of Athens. Their feedback ensured that the questions were relevant, comprehensive, and aligned with current clinical practice and academic standards. Furthermore, internal consistency of the questionnaire, particularly the sections assessing knowledge and preferences, was evaluated using Cronbach’s alpha, ensuring that the grouped items reliably measured their intended answers. A Cronbach’s alpha value above 0.70 was considered acceptable [53,54]. These measures helped confirm that the questionnaire was both valid and reliable for use in the full-scale study.
The questionnaire comprised 23 closed-ended and 5 open-ended questions focused on the decision-making process for selecting resin-based restorative materials, tailored to individual preferences and specific clinical scenarios. It was divided into five sections: The first section included information about the demographics (Part A: Q1–Q5), the second section included general questions concerning each dentist’s personal experience with restorative materials (Part B: Q6-Q12), the third part of the questionnaire included questions related to issues regarding the specifications of resin-based restorative materials and their selection criterion for posterior and anterior teeth (Part C: Q13-Q18). The fourth part contained questions addressing other influential factors during the procurement methods of these materials (Part D: Q19-Q23), and in the final part of the questionnaire, participants were asked to answer open-ended questions related to the subject (Part E: Q24-28).2.3 Bias control strategies
To reduce potential bias, several strategies were implemented throughout the research process [55]. Selection bias was minimized by including a diverse sample of 87 dentists from the Department of Dentistry, encompassing a range of clinical experience levels, specialties, and work environments [55]. Response bias was addressed by ensuring participant anonymity and confidentiality, encouraging honest and accurate responses without fear of judgment or professional repercussions [56]. Additionally, the questionnaire avoided leading or suggestive language to reduce measurement bias [56]. Participation was voluntary, and respondents were informed that there were no right or wrong answers, which helped to reduce social desirability bias, a common issue in self-reported surveys, where respondents may answer in ways they perceive to be more professionally acceptable [57,58]. Finally, data integrity was further ensured through careful data-cleaning procedures, including checks for incomplete responses, outliers, and inconsistencies [59]. Missing data was managed appropriately to avoid skewing results, and non-parametric methods were chosen for analysis where normal distribution assumptions were not met [60]. These methodological precautions aimed to enhance the reliability and validity of the study findings [61].
2.4. Data Collection and Processing
Data was collected using printed and electronic formats of the questionnaire. All statistical analyses were performed using IBM SPSS (Statistical Package for the Social Sciences) version 29. Before analysis, data were cleaned and checked for normality, outliers, and missing values to ensure the reliability of statistical results. The data was analyzed using descriptive and inferential statistical methods to identify significant trends and associations. Descriptive statistics, including means (M), standard deviations (SD), frequencies (N), and percentages (%), were calculated to summarize the demographic characteristics of the sample and the distribution of responses for each selection criterion. Categorical variables were transformed into dummy variables and Spearman correlation coefficients were used to determine the strength and direction of associations between professional characteristics (such as gender, age, clinical experience, postgraduate education, and employment setting) and factors influencing resin material selection. Statistical significance was set at p < .05, with stronger relationships considered at p < .01. Additionally, non-parametric Mann-Whitney tests were conducted to compare distributions between groups, particularly for variables such as gender (male vs. female) and employment setting (private practice vs. other). These tests allowed for the identification of statistically significant differences in material selection preferences between different professional subgroups.
3. Results
3.1. Demographics
The study sample comprised a balanced mix of dentists, with a slightly higher percentage of females (55.2%), predominantly under the age of 45 (65.5%), which may indicate a younger workforce engaging in resin restorative treatments and mostly educated at domestic dental schools (82.8%). Approximately half of the participants (50.6%) had less than five years of clinical experience and more than half (54.0%) did not pursue further specialization, while 33.3% did. Similarly, regarding employment settings, 55.2% of respondents worked in private clinics, whereas only 21.8% were employed in public dental clinics.
The frequency of purchasing resin restorative materials varied, with 31.0% of respondents acquiring them more than twice per year, 31.0% not being personally responsible for procurement, 14.0% obtaining them through stock sales, and 12.0% ordering them when their previous supply ran out. The clinical practice of resin restorations was also heterogeneous, as 63.9% performed fewer than 20 composite resin restorations per week. These findings indicate a diverse sample in terms of clinical workload and material procurement practices, suggesting potential differences in purchasing behaviors based on experience and employment setting.
3.2. Knowledge About Resin Materials
3.2.1. Knowledge Levels in Resin Materials and Correlation with Professional Characteristics
Dentists demonstrated varying levels of knowledge regarding resin restorative materials across several domains. Practical aspects such as application methods and material types scored highest among participants, suggesting that these aspects of resin materials are well understood by the surveyed professionals. The shelf life of resin materials also received a relatively high mean score, indicating moderate familiarity among participants. Conversely, composition and biocompatibility show lower mean scores, which may indicate gaps in knowledge regarding the chemical properties and biological interactions of resin materials. The side effects of resin materials have one of the lowest mean scores, implying a potential area where further education and awareness may be needed (Figure 1).
The correlations between various professional characteristics and knowledge regarding different aspects of resin restorative materials are featured in Table 1. The results indicate that age (r = .236, p < .05) and clinical experience over five years (r = .214, p < .05) are positively correlated with general knowledge about resin materials, suggesting that older and more experienced practitioners exhibit a greater understanding of these materials. Notably, clinical experience also shows significant positive associations with knowledge of material composition (r = .230, p < .05) and shelf life (r = .223, p < .05), further emphasizing that familiarity with resin materials accumulates with professional practice.
Gender does not appear to significantly influence knowledge, except for biocompatibility, where female dentists report significantly lower knowledge scores (r = -.248, p < .05) compared to their male counterparts. Interestingly, frequent purchases of resin restorative materials do not significantly correlate with increased knowledge, indicating that purchasing behavior does not necessarily reflect a deeper understanding of the materials. However, dentists performing more than 20 composite resin restorations per week demonstrate a trend toward greater knowledge across most domains, particularly in composition (r = .206) and method of application (r = .100), though these correlations do not reach statistical significance (Table 1).
3.2.2. Dentists’ Familiarity and Priorities in Resin Material Selection: Specifications, Features, and Sustainability
The findings in Table 2 demonstrate dentists’ familiarity with specifications and priority features when selecting resin restorative materials. Most respondents (71.4%) reported familiarity with resin material specifications, indicating a strong awareness of regulatory or technical guidelines governing material selection. However, 28.6% stated that they were not familiar with these specifications, suggesting a potential gap in knowledge that could be addressed through continuing education and training programs.
Regarding the importance of material compliance with specifications, more than half (54.0%) considered it quite important, while 32.2% regarded it as very important. This indicates that while compliance is widely acknowledged as significant, a notable percentage (13.8%) rated it as only moderately important, implying that other factors, such as handling properties or price, might sometimes take precedence (Table 2).
In terms of priority features for material selection, bending strength (34.6%) and biocompatibility (25.9%) were the most highly rated characteristics, demonstrating a strong emphasis on mechanical durability and patient safety. Water absorbency and photopolymerization depth were rated lower, suggesting that these factors are considered secondary to mechanical and biological properties (Table 2).
The final section of the table addresses the preference for green practices relative to ISO compliance. A large majority (40.2%) prioritized ISO standards over green practices, while 54.9% indicated that environmental considerations depend on the specific material specifications. Only 4.9% of respondents were fully committed to green practices regardless of compliance. This suggests that while sustainability is acknowledged, it is often weighed against regulatory compliance and material performance, reinforcing the idea that environmental initiatives should be integrated within existing ISO standards rather than replacing them (Table 2).
3.3. Selection of Resin Materials
3.3.1. Resin Selection in Anterior and Posterior Restorations
The selection criteria for resin materials in anterior and posterior restorations, highlighted differences in decision-making factors between these two types of restorations (Figure 2). The results in Figure 2 have demonstrated that anatomical features of the restoration were the most frequently cited criterion for both anterior (54.0%) and posterior (55.2%) restorations, suggesting that dentists prioritize functional and structural considerations regardless of tooth position.
For anterior restorations, transparency and opacity of neighboring teeth (56.3%) and color of neighboring teeth (50.6%) were highly influential factors, reflecting the emphasis on esthetics in anterior regions. Conversely, these factors were less frequently considered for posterior restorations, with color being relevant for only 28.7% of cases. This finding aligns with the reduced esthetic concern in posterior teeth, where functional durability is often prioritized over visual characteristics (Figure 2).
The interdental space was a more significant factor in posterior restorations (27.6%) than in anterior ones (16.1%), likely due to the need for strong contact points and structural stability in posterior occlusion. Notably, a lack of specific selection criteria was more common in posterior restorations (27.6%) compared to anterior restorations (6.9%), indicating that dentists may adopt a more flexible approach when selecting materials for posterior teeth (Figure 2).
A distinctive finding is that special anterior resins were used by 36.8% of dentists for anterior restorations, reporting on the demand for highly esthetic and technique-sensitive materials in the visible esthetic dental zone. This factor was not relevant for posterior restorations, where other material properties such as durability and resistance to occlusal forces likely play a more dominant role (Figure 2).
For extensive immediate esthetic restorations of posterior teeth, most respondents (75.9%) selected packable composite resin as their material of choice, reflecting its widespread acceptance for posterior restorations due to its mechanical properties, wear resistance, and ability to provide esthetic results. The high prevalence of this choice aligns with modern restorative trends that favor composite resins over traditional materials such as amalgam (4,6%). The bulk-fill resin was chosen by 34.5% of practitioners, indicating a substantial preference for materials that allow for more efficient placement techniques while maintaining sufficient strength for posterior load-bearing areas [62]. Bulk-fill resins are known for their reduced polymerization shrinkage and improved depth of cure, making them a practical alternative to traditional layering techniques [63,64]. A smaller proportion (16.1%) opted for flowable composites, which are typically used as liners or in combination with other restorative materials rather than as standalone material for extensive restorations. The use of glass ionomer cement was minimal (5.7%), likely due to its lower wear resistance and mechanical strength, making it less suitable for high-stress posterior restorations [65].
3.4. Professional Characteristics and Resin Material Selection
Selection criteria differed significantly between anterior and posterior restorations based on clinical experience. For anterior restorations, the most frequently reported selection criterion was the anatomical features to be achieved (54.0%), followed closely by transparency and opacity (56.3%) and the color of neighboring teeth (50.6%). Notably, less experienced dentists (70.5%) were significantly more likely to consider anatomical features compared to those with more than five years of experience (37.2%). In contrast, experienced clinicians preferred using special anterior resins (51.2%), whereas only 22.7% of less experienced dentists selected this criterion, suggesting that experience influences the preference for specialized materials (Table 3).
For posterior restorations, a similar trend was observed, anatomical features remained the most important criterion, (55.2%). Less experienced dentists were more likely to prioritize anatomical considerations (65.9%) than their more experienced counterparts (44.2%). Additionally, a higher proportion of experienced dentists (32.6%) reported using whatever material was available in stock compared to their less experienced counterparts (22.7%). This suggests that familiarity with different materials over time may lead to more flexible selection criteria. (Table 3).
The selection of resin restorative materials influenced by dentists’ professional characteristics, including clinical experience, age, postgraduate education, and workload is presented in Table 4.
For anterior restorations, a significant negative correlation was found between clinical experience and the importance assigned to anatomical features (r = -.334, p < .05), suggesting that more experienced dentists rely less on anatomical considerations when selecting materials. Similarly, performing over 20 restorations per week was negatively correlated with prioritizing anatomical features (r = -.315, p < .05), indicating that high-volume practitioners may adopt a more standardized material selection approach. Notably, the use of special anterior resins was positively correlated with both postgraduate studies (r = .337, p < .05) and clinical experience (r = .295, p < .05), suggesting that additional training and professional expertise increase the likelihood of selecting specialized materials (Table 4).
For posterior restorations, clinical experience was negatively correlated with prioritizing anatomical features (r = -.218, p < .05), implying that experienced dentists may focus on other material properties when selecting posterior restoratives. No significant relationships were found between purchasing frequency and material selection, indicating that procurement habits do not necessarily dictate material selection criteria (Table 4).
The variety of professional characteristics and familiarity with material specifications, importance of compliance, prioritized features, and preferences for green practices in resin restorative material selection is demonstrated in Table 5. A key finding in Table 5 is that clinical experience (r = .231, p < .05) and frequent purchasing of resin materials (r = .254, p < .05) were positively correlated with familiarity with material specifications, indicating that practitioners with more experience or greater involvement in procurement tend to be more knowledgeable about material standards. Conversely, those not responsible for supply were significantly less familiar with specifications (r = -.341, p < .05), highlighting the role of procurement responsibility in material literacy.
Regarding the importance of compliance with specifications, no statistically significant correlations were found with professional characteristics, suggesting that most dentists view regulatory compliance as a universally important factor, regardless of experience or educational background. In feature prioritization, biocompatibility was significantly correlated with gender (r = .232, p < .05), suggesting that female dentists place higher importance on patient safety in material selection. Meanwhile, bending strength was negatively correlated with clinical experience (r = -.233, p < .05), implying that less experienced dentists may overemphasize mechanical durability, whereas experienced clinicians might consider a broader range of factors. The preference for green practices showed an interesting trend. Those purchasing resin materials frequently were significantly more likely to prioritize environmental considerations (r = .211, p < .05), suggesting that practitioners who are actively involved in procurement may be more exposed to sustainability discussions. However, ISO compliance remained the dominant concern for most respondents, regardless of experience or background. (Table 5).
In correlation with the above, Figure 3 illustrates the importance of environmental factors when purchasing resin restorative materials for conservative restorations, segmented by gender. The results indicate a clear gender difference, with female dentists placing significantly higher importance on environmental considerations compared to their male counterparts. The highest proportion of respondents who rated environmental factors as “very important” or “the most important” were female dentists (22.99% and 12.64%, respectively), while only 10.34% and 4.60% of male dentists rated them as highly significant. Conversely, a larger percentage of male dentists (13.79%) rated environmental factors as only “somewhat important” compared to females (5.75%), suggesting that men may consider sustainability but not as a decisive factor in their material selection process. A small percentage of both male and female respondents (3.45% and 1.15%, respectively) did not consider environmental factors important at all, indicating that while sustainability is increasingly acknowledged, it remains a secondary concern for a minority of practitioners (Figure 3).
4. Discussion
The present study aimed to investigate the factors influencing the selection of resin-based restorative materials among practicing dentists, with particular attention to the role of professional characteristics, clinical experience, and procurement responsibilities. The findings offer important insights into how these variables interact with material knowledge, specification awareness, and clinical decision-making, contributing to the existing literature on restorative material selection.
4.1. Influence of Professional Characteristics on Material Selection
This study confirmed that professional characteristics, particularly clinical experience and procurement involvement, play a central role in the selection of resin-based restorative materials, as also reported by Pratap (2019) [4]. Most participants were under the age of 45, reflecting a younger demographic actively engaged in restorative procedures, consistent with recent findings by Ulku and Unlu (2024) [66]. Within this group, those with greater clinical experience demonstrated significantly higher knowledge of material composition (r = .230, p < .05) and shelf life (r = .223, p < .05), particularly regarding ISO specifications and mechanical properties. These results suggest that clinical exposure enhances familiarity with the scientific and functional aspects of materials. This aligns with previous research showing that practical experience strengthens the application of scientific knowledge in daily clinical decision-making [14,15].
Furthermore, experienced dentists in the present study were more likely to select specialized resin materials, particularly for anterior restorations, demonstrating a preference for advanced, esthetically driven options that require a higher level of clinical competence. In contrast, less experienced practitioners placed greater emphasis on anatomical detailing and basic esthetic parameters, such as shape and shade matching. These observations are consistent with the findings of Lorenz et al. (2024) [67], who reported that expert evaluators tend to assess anterior restorations with a more critical and detailed understanding of material performance and esthetic integration compared to less experienced clinicians. It was also demonstrated that expert evaluators apply more refined and critical criteria when assessing anterior restorations, emphasizing subtle esthetic integration and long-term performance. Moreover, this supports the conclusions of Al-Asmar et al. (2021) [68], who emphasized that clinical decision-making in restorative dentistry becomes increasingly evidence-based with professional maturity, as more experienced practitioners tend to rely on a broader integration of clinical evidence, patient-specific factors, and material science. Overall, these results show that experience not only shapes material preferences but also informs the depth and quality of esthetic evaluation in anterior restorative procedures [67].
4.2. Regional Differences in Resin Material Criteria
Our data indicates that dentists apply distinct selection criteria based on the anatomical location of the restoration, a finding that aligns with previous work by Girotto et al. (2021) [69], who reported significant variation in restorative approaches between anterior and posterior regions due to differences in esthetic expectations and functional demands. In our study, esthetic attributes, such as transparency, opacity, and shade matching, were prioritized for anterior restorations, where visual integration with the surrounding dentition is essential. Conversely, posterior restorations were more strongly associated with the prioritization of mechanical properties, including wear resistance, compressive strength, and fracture toughness, due to their exposure to higher occlusal forces. These results corroborate the findings of Pizzolotto and Moraes (2022) [70], who emphasized that the selection of posterior restorative materials is predominantly influenced by their ability to withstand long-term functional stress rather than their esthetic qualities. Similarly, Ilie et al. (2017) [16] highlighted that the anatomical region plays a decisive role in material selection, as anterior restorations demand superior optical properties and polishability, whereas posterior restorations require enhanced strength, marginal integrity, and low wear. Taken together, these findings suggest that clinicians adapt their material selection strategies in response to the specific biomechanical and esthetic requirements of the restoration site, thereby reinforcing the importance of site-specific material knowledge in clinical decision-making as also mentioned elsewhere [71].
Moreover, less experienced dentists in our study placed greater emphasis on anatomical features and optical properties, particularly in anterior restorations, highlighting a focus on visual accuracy and surface morphology. In contrast, clinicians with more than five years of experience demonstrated a preference for specialized anterior composites, indicating a shift toward the use of advanced materials that offer improved esthetic integration, polishability, and long-term performance. This pattern is consistent with prior studies that suggest clinical expertise is associated with the adoption of more sophisticated techniques and a broader understanding of material behavior in esthetically demanding cases [20,21]. Also, recent clinical evidence supports these trends too. For instance, Murchie et al. (2025) [72] reported that the long-term success of anterior restorations in cases of localized wear is more closely associated with the use of high-performance materials and tailored placement protocols, typically employed by more experienced clinicians. Furthermore, the growing use of chairside CAD/CAM technology and customized resin composites, as discussed by Ille et al. (2025) [73], reinforces the idea that familiarity with advanced restorative options and their indications is more prevalent among seasoned practitioners. These findings collectively suggest that clinical experience not only informs material selection but also expands the scope of available techniques, enabling more durable and esthetically precise outcomes in anterior restorative treatments.
4.3. Procurement Responsibility and Specification Awareness
Additionally, procurement responsibility was positively associated in our study with greater knowledge of material standards, including ISO certification, product longevity, and regulatory compliance. Dentists who were directly involved in the acquisition of resin-based restorative materials demonstrated higher familiarity with manufacturer specifications and performance data, suggesting that active engagement with procurement processes may facilitate deeper material literacy [5,48]. This finding supports the important role of hands-on exposure to product documentation and supplier communication in informing evidence-based clinical decisions. Moreover, this association echoes broader insights from organizational research. Barakat et al. (2023) [74] for example, found that increased involvement in supply chain processes and sustainability-oriented training enhances a more informed and proactive approach to material evaluation and procurement. In the context of dental practice, comparable mechanisms to those observed in broader organizational and healthcare environments may be present as our data show. Clinicians involved in the procurement of restorative materials appeared to be more attuned to regulatory compliance, product innovation, and life cycle performance. This finding supports prior work by Kaurani et al. (2022) [75], which emphasized that direct engagement with procurement and supply chain processes enhances both technical knowledge and strategic awareness of product standards. In our study, this relationship was particularly evident among dentists who reported frequent purchasing responsibilities, as they demonstrated higher levels of familiarity with ISO specifications and material performance indicators. These findings also align with broader discussions on the intersection of sustainability and clinical responsibility. Boulding and Hinrichs-Krapels (2021) [76] have argued that procurement is a critical leverage point for embedding quality and environmental standards into institutional practices. Similarly, Antoniadou et al. (2023) [77] demonstrated that Greek dental professionals who are actively engaged with environmental issues, especially those involved in decision-making roles, are more likely to integrate sustainability principles into clinical workflows. Our results reinforce this pattern, suggesting that procurement responsibility functions not only as a vehicle for regulatory compliance but also as an entry point for the adoption of environmentally responsible practices. As such, enhancing procurement literacy may be a valuable strategy for promoting both material competence and sustainability awareness in dental practice [78]. Interestingly, while a substantial proportion of participants in this study emphasized the importance of compliance with ISO standards, particularly ISO 4049:2019 [13], which governs the physical and mechanical properties of resin-based restorative materials, no statistically significant correlation was observed between professional characteristics (such as age, experience, or postgraduate education) and the priority given to regulatory adherence. This suggests that compliance with established standards is regarded as a baseline requirement, independent of demographic or experiential variables. These findings align with previous research by Yap et al. (2018) [17], who similarly reported that ISO compliance is broadly acknowledged across diverse professional groups as essential to clinical success and patient safety. The absence of variation in attitudes toward compliance in our data reinforces the notion that regulatory awareness is now a normative expectation in restorative dentistry, reflecting both professional training and institutional procurement practices. This widespread consensus may indicate the successful dissemination of ISO-related knowledge through dental education and continuing professional development, establishing compliance not as a differentiator, but as a foundational aspect of responsible clinical practice [79].
4.4. Sustainability and Gender-Based Preferences
Environmental sustainability emerged as a secondary, yet increasingly relevant, consideration among respondents in this study. While clinical performance, biocompatibility, and regulatory compliance remained dominant selection criteria, a subset of participants, predominantly female dentists, demonstrated greater awareness of environmental impacts, particularly concerning material packaging, manufacturing practices, and waste management. This gender-based differentiation aligns with previous studies suggesting that female practitioners are generally more responsive to environmental and health-related concerns in clinical settings [49,77].
Despite this trend, only a limited proportion of respondents identified sustainability as a primary or high-priority factor in material selection. This finding parallels the observations of Tancu et al. (2025) [80], who reported that although sustainability is gaining visibility in dental discourse, it has yet to be fully integrated into daily decision-making processes. Similarly, Rundh (2013) [26] highlighted the early stage of sustainability consciousness in product marketing and procurement, noting that environmental considerations often remain subordinate to technical performance, cost, and brand familiarity. So, there is an indication that while there is a growing recognition of the importance of environmentally responsible dentistry, particularly among specific demographic groups, the integration of sustainable criteria into restorative material selection remains limited. The challenge moving forward lies in bridging the gap between awareness and actionable change by embedding environmental performance within existing regulatory and quality frameworks [26,77,81]. This trend though is consistent with previous research suggesting that the integration of sustainability into restorative dentistry remains in its formative stages. As demonstrated by Duane et al. (2019) [27], although awareness of sustainable concepts in dental practice is increasing, their practical application, particularly in material selection, remains limited by the absence of formal guidance and standardized environmental criteria. Similarly, Klamain et al. (2016) [46] emphasized the lack of established eco-certification systems tailored specifically to dental products, making it difficult for practitioners to systematically evaluate the environmental impact of restorative materials. In our study, this gap was evident in the low proportion of respondents who rated environmental factors as highly influential in their material choices, despite general awareness of sustainability issues. But while ISO compliance emerged as the dominant selection criterion across all professional groups, there was a discernible undercurrent of interest in sustainability, suggesting an opportunity for alignment between environmental goals and existing regulatory frameworks. Moreover, recent perspectives, such as those by Ogiemwonyi et al. (2023) [24], argue for the integration of environmental performance metrics within standard procurement and quality assurance protocols. Such an approach would not only normalize sustainability within clinical workflows but also empower practitioners to make environmentally informed decisions without compromising on safety or efficacy. Our findings reinforce this need, highlighting the importance of developing comprehensive, practice-relevant eco-standards that complement existing ISO regulations.
Further, the prioritization of material features in this study was also shaped by gender and experience-related differences. Female dentists placed greater importance on biocompatibility, suggesting a stronger inclination toward patient safety and the biological compatibility of restorative materials. In contrast, clinicians with less professional experience were more likely to emphasize mechanical criteria, particularly bending strength, which may indicate a reliance on tangible, quantifiable properties during early clinical decision-making. This divergence in priorities echoes recent findings by Kichenin et al. (2025) [82], who highlighted gender-related patterns in dental education and career orientation. Their study revealed that female dental students tend to exhibit higher levels of concern for patient-centered outcomes and long-term clinical effects, whereas male students often show greater interest in technical aspects of care delivery. These distinctions may persist beyond training, shaping professional behavior and material preferences throughout clinical practice. Rather than viewing these patterns as limiting, they point to the diverse ways in which dentists evaluate materials, whether through the lens of biological performance, mechanical efficiency, or esthetic adaptability. It seems then that understanding how gender and experience influence evaluative frameworks for material selection not only enriches clinical insight but also supports the development of more tailored and inclusive approaches to dental education, procurement policies, and evidence-based practice. As Wolbring and Nguyen (2023) [83] emphasize in their review of equity, diversity, and inclusion (EDI) frameworks in professional education, acknowledging diverse perspectives and experiences is essential for supporting fair and responsive systems. Applying this principle to dentistry, incorporating gender- and experience-informed preferences into educational curricula and procurement training may enhance both the relevance and equity of restorative material selection, ultimately improving clinical outcomes and practitioner engagement. In addition, as shown by Al-Sbei et al. (2024) [84], targeted, structured interventions in restorative dentistry education, such as web-based modules, can significantly improve learning outcomes, particularly when they are aligned with the real-world needs and diversity of clinical practitioners. In parallel, Wang and Chang (2022) [85] have supported the systematic integration of gender mainstreaming in dental education, emphasizing that recognizing gendered patterns in learning and clinical priorities is not only a matter of equity but also one of optimizing professional development and patient care.
4.5. Implications for Clinical Education and Future Research
The findings of this study highlight a clear need for strengthened professional education and ongoing training in the science of restorative materials. Specific emphasis should be placed on deepening clinicians’ understanding of biocompatibility, long-term clinical performance, and the environmental implications of resin-based composites. Expanding educational efforts in these areas is essential for bridging current knowledge gaps and enhancing more informed, evidence-based material selection. Furthermore, the integration of sustainability criteria into established regulatory frameworks, such as ISO and ADA standards [12,13], may offer a structured approach to aligning clinical excellence with environmental responsibility, a dual imperative in contemporary dental practice [42,48]. To build on these findings, future research should examine the clinical outcomes associated with different material selection strategies, particularly concerning long-term durability and performance of eco-conscious resin systems. In parallel, institutional strategies for embedding green procurement principles into dental practice, through policy, education, and industry partnerships, warrant further exploration. Multi-center and cross-national studies would also be valuable in validating the generalizability of current results and identifying regional variations in material preferences, professional training, and regulatory environments [86].
Limitations of the Study
While the present study provides meaningful insights into the factors influencing resin-based material selection among dental professionals, several limitations must be acknowledged. The sample was restricted to dentists affiliated with the National and Kapodistrian University of Athens, which may limit the generalizability of the findings to broader populations. Institutional affiliation often shapes clinical protocols, procurement procedures, and educational exposure, potentially introducing contextual bias that may not reflect practices in other national or international settings [87,88] .However, it is important to note that the study was designed as a pilot investigation, the primary purpose of which is to explore patterns, test the feasibility of research instruments, and identify potential variables and relationships for further study. As it is reported, pilot studies serve as essential precursors to larger-scale investigations, providing preliminary data that can inform the refinement of research questions, methodological design, and sampling strategies [89,90]. In this context, the current findings should be viewed as exploratory rather than definitive, offering a foundational understanding of professional decision-making regarding resin materials, which can be tested and expanded upon in future multi-center or longitudinal research as mentioned also elsewhere [91,92]. Additionally, as the study employed a self-administered questionnaire, it is subject to common limitations inherent in self-report methodologies, including social desirability bias and recall inaccuracies [58]. While participant anonymity was preserved and the questionnaire was pilot-tested for clarity and neutrality, these limitations should be considered in interpreting the results.
Despite these limitations, the study offers several strengths. It addresses a notable gap in the literature by empirically examining how professional characteristics influence restorative material selection, with a focus on both clinical and sustainability-related factors. Furthermore, it contributes original data from an underrepresented professional population and provides a validated survey tool that can be adapted for broader future research contexts.
5. Conclusion
This study highlights key factors influencing dentists’ selection of resin-based restorative materials, particularly clinical experience and procurement responsibility. Less experienced practitioners tend to prioritize anatomical and esthetic features, while more experienced clinicians demonstrate greater flexibility and familiarity with material options. The variation in selection criteria between anterior and posterior restorations reinforces the need for context-specific decision-making where esthetics dominate anterior choices and mechanical properties are prioritized posteriorly. Although sustainability is an emerging consideration, clinical performance remains the primary determinant. Notably, gaps in knowledge regarding material properties and regulatory standards point to the need for targeted educational initiatives. Future research should explore how green practices can be integrated into dental material manufacturing without compromising quality or compliance. Overall, this study contributes to a broader understanding of evidence-based material selection and supports improved clinical decision-making in restorative dentistry.
References
- Yadav, R.; Lee, H.H. Ranking and selection of dental restorative composite materials using FAHP-FTOPSIS technique: An application of multi criteria decision making technique. Journal of the Mechanical Behavior of Biomedical Materials 2022, 132, 105298. [Google Scholar] [CrossRef] [PubMed]
- Demarco, F.F.; Cenci, M.S.; Montagner, A.F.; et al. Longevity of composite restorations is definitely not only about materials. Dental materials: official publication of the Academy of Dental Materials 2023, 39, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Shaw, K.; Martins, R.; Hadis, M.A.; et al. ‘Own-Label’ Versus Branded Commercial Dental Resin Composite Materials: Mechanical And Physical Property Comparisons. Eur J Prosthodont Restor Dent 2016, 24, 122–129. [Google Scholar] [CrossRef] [PubMed]
- Pratap, B.; Gupta, R.K.; Bhardwaj, B.; et al. Resin based restorative dental materials: characteristics and future perspectives. Jpn Dent Sci Rev 2019, 55, 126–138. [Google Scholar] [CrossRef]
- Heintze, S.D.; Ilie, N.; Hickel, R.; et al. Laboratory mechanical parameters of composite resins and their relation to fractures and wear in clinical trials—A systematic review. Dental materials 2017, 33, e101–e114. [Google Scholar] [CrossRef]
- Huang, W.; Ren, L.; Cheng, Y.; et al. Evaluation of the Color Stability, Water Sorption, and Solubility of Current Resin Composites. Materials 2022, 15, 6710. [Google Scholar] [CrossRef]
- Aminoroaya A, Neisiany RE, Khorasani SN, et al. A review of dental composites: Challenges, chemistry aspects, filler influences, and future insights. Composites Part B: Engineering 2021, 216, 108852. [Google Scholar] [CrossRef]
- Schmalz G, Watts DC and Darvell BW. Dental materials science: Research, testing and standards. Dental materials: official publication of the Academy of Dental Materials 2021, 37, 379–381. [Google Scholar] [CrossRef]
- Schmalz G, Schwendicke F, Hickel R, et al. Alternative Direct Restorative Materials for Dental Amalgam: A Concise Review Based on an FDI Policy Statement. International dental journal 2023, 74. [CrossRef]
- Soni N, Bairwa S, Sumita S, et al. Mechanical Properties of Dental Resin Composites: A Review. International Journal of Research Publication and Reviews 2024, 5, 7675–7683. [Google Scholar] [CrossRef]
- (ISO) IOfS. Scopes -ISO/TC 106 Dentistry Subcommittees 1 and 2.
- ADA Division of Science ACoSA. Resin-based composites. Journal of the American Dental Association (1939) 2003, 134, 510–512. [Google Scholar] [CrossRef] [PubMed]
- International Organization for Standardization G, Switzerland. ISO 4049:2019. DentistryPolymer-based restorative materials. 2019, 29.
- Cho K, Rajan G, Farrar P, et al. Dental resin composites: A review on materials to product realizations. Composites Part B: Engineering 2021, 230, 109495. [Google Scholar] [CrossRef]
- Ferracane JL, Hilton TJ, Stansbury JW, et al. Academy of Dental Materials guidance-Resin composites: Part II-Technique sensitivity (handling, polymerization, dimensional changes). Dental materials: official publication of the Academy of Dental Materials 2017, 33, 1171–1191. [Google Scholar] [CrossRef]
- Ilie N, Hilton TJ, Heintze SD, et al. Academy of Dental Materials guidance -Resin composites: Part I-Mechanical properties. Dental materials: official publication of the Academy of Dental Materials 2017, 33, 880–894. [Google Scholar] [CrossRef] [PubMed]
- Yap AU, Eweis AH and Yahya NA. Dynamic and Static Flexural Appraisal of Resin-based Composites: Comparison of the ISO and Mini-flexural Tests. Operative dentistry 2018, 43, E223–e231. [Google Scholar] [CrossRef]
- Nouf mohamed saeed shaabin RHK, Hibah Saad Al-Ahmadi, Rasha Nabeel Halal, Afaf Ahmed Tawati, Maram mohamed saeed shaabin, Nadia Abdulrahman addas, Maha sameer linjawi, Waleed saleh balubaid, Mohamed fouad Garanbish,; Abeer Abdullatif Alomarey. Materia l Selection for Posterior Restorations: An Observational Study Evaluating Dentists’ Preferences in Jeddah, Saudi Arabia. Journal of Population Therapeutics and Clinical Pharmacology 2022, 30, 649–659. [Google Scholar]
- Ghoneim A, Yu B, Lawrence H, et al. What influences the clinical decision-making of dentists? A cross-sectional study. PloS one 2020, 15, e0233652–2020. [Google Scholar] [CrossRef]
- Arandi, NZ. Current trends in placing posterior composite restorations: Perspectives from Palestinian general dentists: A questionnair study. Journal of International Society of Preventive & Community Dentistry 2024, 14, 112–120. [Google Scholar] [CrossRef]
- Nascimento GG, Correa MB, Opdam N, et al. Do clinical experience time and postgraduate training influence the choice of materials for posterior restorations? Results of a survey with Brazilian general dentists. Brazilian dental journal 2013, 24, 642–646. [Google Scholar] [CrossRef]
- Khaleefa S, Yeslam H and Hasanain F. Knowledge and Attitude of Recent Dental Graduates towards Smart/Bioactive Dental Composites. Journal of Pharmaceutical Research International 2021, 33, 34–44. [Google Scholar] [CrossRef]
- WD AL, Ingle N, Assery M, et al. Dentists’ Knowledge, Attitude, and Practice Regarding Evidence-Based Dentistry Practice in Riyadh, Saudi Arabia. Journal of pharmacy & bioallied sciences 2019, 11, S507–s514. [Google Scholar] [CrossRef]
- Ogiemwonyi O, Alam M, Alshareef R, et al. Environmental factors affecting green purchase behaviors of the consumers: Mediating role of environmental attitude. Cleaner Environmental Systems 2023, 100130. [CrossRef]
- Ririn Y, Rahmat STY and Rina A. How packaging, product quality and promotion affect the purchase intention? Russian Journal of Agricultural and Socio-Economic Sciences 2019, 92, 46–55.
- Rundh, B. Linking packaging to marketing: how packaging is influencing the marketing strategy. British Food Journal 2013, 115, 1547–1563. [Google Scholar] [CrossRef]
- Duane B, Ramasubbu D, Harford S, et al. Environmental sustainability and procurement: purchasing products for the dental setting. British dental journal 2019, 226, 453–458. [Google Scholar] [CrossRef]
- Moshkbid E, Cree DE, Bradford L, et al. Biodegradable Alternatives to Plastic in Medical Equipment: Current State, Challenges, and the Future. 2024, 8, 342.
- Mulimani, P. Green dentistry: the art and science of sustainable practice. British dental journal 2017, 222, 954–961. [Google Scholar] [CrossRef]
- Maier C, Thatcher J, Grover V, et al. Cross-sectional research: A critical perspective, use cases, and recommendations for IS research. International Journal of Information Management 2023, 70, 102625. [Google Scholar] [CrossRef]
- Ahmed A, Pereira L and Jane K. Mixed Methods Research: Combining both qualitative and quantitative approaches. 2024.
- Chai HH, Gao SS, Chen KJ, et al. A Concise Review on Qualitative Research in Dentistry. International journal of environmental research and public health 2021, 18 2021/01/28. [CrossRef]
- Ranganathan P and Caduff, C. Designing and validating a research questionnaire - Part 1. Perspectives in clinical research 2023, 14, 152–155. [Google Scholar] [CrossRef]
- Khanal B and Chhetri, D. A Pilot Study Approach to Assessing the Reliability and Validity of Relevancy and Efficacy Survey Scale. Janabhawana Research Journal 2024, 3, 35–49. [Google Scholar] [CrossRef]
- Brewster J and Roberts, HW. 12-Month flexural mechanical properties of conventional and self-adhesive flowable resin composite materials. Dental materials journal 2023, 42, 598–609. [Google Scholar] [CrossRef]
- Calabrese L, Fabiano F, Bonaccorsi LM, et al. Evaluation of the Clinical Impact of ISO 4049 in Comparison with Miniflexural Test on Mechanical Performances of Resin Based Composite. International journal of biomaterials 2015, 2015, 149798–2015. [Google Scholar] [CrossRef]
- Erickson RL and Barkmeier, WW. Comparisons of ISO depth of cure for a resin composite in stainless-steel and natural-tooth molds. European journal of oral sciences 2019, 127, 556–563. [Google Scholar] [CrossRef] [PubMed]
- Fan PL, Schumacher RM, Azzolin K, et al. Curing-light intensity and depth of cure of resin-based composites tested according to international standards. Journal of the American Dental Association (1939) 2002, 133, 429–434. [Google Scholar] [CrossRef] [PubMed]
- Flury S, Hayoz S, Peutzfeldt A, et al. Depth of cure of resin composites: is the ISO 4049 method suitable for bulk fill materials? Dental materials: official publication of the Academy of Dental Materials 2012, 28, 521–528. [CrossRef]
- Heintze S and Zimmerli, B. Relevance of in-vitro tests of adhesive and composite dental materials. A review in 3 parts. Part 2: non-standardized tests of composite materials. Schweizer Monatsschrift für Zahnmedizin = Revue mensuelle suisse d’odonto-stomatologie = Rivista mensile svizzera di odontologia e stomatologia/SSO 2011, 121, 916–930. [Google Scholar]
- Heintze SD and Zimmerli, B. Relevance of in vitro tests of adhesive and composite dental materials, a review in 3 parts. Part 1: Approval requirements and standardized testing of composite materials according to ISO specifications. Schweiz Monatsschr Zahnmed 2011, 121, 804–816. [Google Scholar]
- Ilie, N. ISO 4049 versus NIST 4877: Influence of stress configuration on the outcome of a three-point bending test in resin-based dental materials and interrelation between standards. Journal of dentistry 2021, 110, 103682–2021. [Google Scholar] [CrossRef]
- Moore BK, Platt JA, Borges G, et al. Depth of cure of dental resin composites: ISO 4049 depth and microhardness of types of materials and shades. Operative dentistry 2008, 33, 408–412. [Google Scholar] [CrossRef]
- Zhang N and Xie, C. Polymerization shrinkage, shrinkage stress, and mechanical evaluation of novel prototype dental composite resin. Dental materials journal 2020, 39, 1064–1071. [Google Scholar] [CrossRef]
- Burke, FJ. The evidence base for ‘own label’ resin-based dental restoratives. Dent Update 2013, 40, 5–6. [Google Scholar] [CrossRef]
- Klaiman K, Ortega D and Garnache C. Consumer preferences and demand for packaging material and recyclability. Resources, Conservation and Recycling 2016, 115. [CrossRef]
- Mallinson DJ and Hatemi, PK. The effects of information and social conformity on opinion change. PloS one 2018, 13, e0196600–20180502. [Google Scholar] [CrossRef] [PubMed]
- Megremis, SJ. Assuring the Safety of Dental Materials: The Usefulness and Application of Standards. Dental clinics of North America 2022, 66, 673–689. [Google Scholar] [CrossRef] [PubMed]
- Mittal R, Maheshwari R, Tripathi S, et al. Eco-friendly dentistry: Preventing pollution to promoting sustainability. Indian Journal of Dental Sciences 2020, 12, 251. [Google Scholar] [CrossRef]
- Prudnikov Y and Nazarenko A. The role of content marketing in the promotion of medical goods and services. 2021.
- Zaware PDN. Exploration of market potential towards dental material brands: An assessment with preferences of dentists in India. Available at SSRN 3819251 2020.
- Bujang MA, Omar E, Foo D, et al. Sample size determination for conducting a pilot study to assess reliability of a questionnaire. Restorative Dentistry & Endodontics 2024, 49. [CrossRef]
- Hussey I, Alsalti T, Bosco F, et al. An Aberrant Abundance of Cronbach’s Alpha Values at.70. Advances in Methods and Practices in Psychological Science 2025, 8, 25152459241287123. [CrossRef]
- Tavakol M and Dennick, R. Making Sense of Cronbach’s Alpha. International Journal of Medical Education 2011, 2, 53–55. [Google Scholar] [CrossRef]
- Agrawal AA, Prakash N, Almagbol M, et al. Synoptic review on existing and potential sources for bias in dental research methodology with methods on their prevention and remedies. World journal of methodology 2023, 13, 426–438. [Google Scholar] [CrossRef]
- Vaidyanathan, AK. Controlling bias in research. Journal of Indian Prosthodontic Society 2022, 22, 311–313. [Google Scholar] [CrossRef]
- Bispo Júnior, JP. Social desirability bias in qualitative health research. Revista de saude publica 2022, 56, 101–2022. [Google Scholar] [CrossRef]
- Latkin CA, Edwards C, Davey-Rothwell MA, et al. The relationship between social desirability bias and self-reports of health, substance use, and social network factors among urban substance users in Baltimore, Maryland. Addictive behaviors 2017, 73, 133–136. [Google Scholar] [CrossRef]
- Guo M, Wang Y, Yang Q, et al. Normal Workflow and Key Strategies for Data Cleaning Toward Real-World Data: Viewpoint. Interactive journal of medical research 2023, 12, e44310–2023. [Google Scholar] [CrossRef]
- Ranganathan P and Hunsberger, S. Handling missing data in research. Perspectives in clinical research 2024, 15, 99–101. [Google Scholar] [CrossRef] [PubMed]
- Ahmed I and Ishtiaq, S. Reliability and validity: Importance in Medical Research. JPMA The Journal of the Pakistan Medical Association 2021, 71, 2401–2406. [Google Scholar] [CrossRef] [PubMed]
- Sengupta A, Naka O, Mehta SB, et al. The clinical performance of bulk-fill versus the incremental layered application of direct resin composite restorations: a systematic review. Evidence-based dentistry 2023, 24, 143–2023. [Google Scholar] [CrossRef] [PubMed]
- Chesterman J, Jowett A, Gallacher A, et al. Bulk-fill resin-based composite restorative materials: A review. BDJ 2017, 222, 337–344. [Google Scholar] [CrossRef]
- Matos JD, Nakano LJ, Scalzer G, et al. Characterization of Bulk-Fill Resin Composites in Terms of Physical, Chemical, Mechanical and Optical Properties and Clinical Behavior. International Journal of Odontostomatology 2021, 15, 226–233. [Google Scholar] [CrossRef]
- Sikka N and Brizuela M. Glass Ionomer Cement. StatPearls. Treasure Island (FL) ineligible companies. Disclosure: Melina Brizuela declares no relevant financial relationships with ineligible companies.: StatPearls Publishing Copyright © 2025, StatPearls Publishing LLC., 2025.
- Ulku SG and Unlu, N. Factors influencing the longevity of posterior composite restorations: A dental university clinic study. Heliyon 2024, 10, e27735–2024. [Google Scholar] [CrossRef]
- Lorenz J, Wilhelm C, Urich J, et al. Different Esthetic Assessment of Anterior Restorations by Patient and Expert: A Prospective Clinical Study. Journal of esthetic and restorative dentistry: official publication of the American Academy of Esthetic Dentistry [et al] 2024 2024/12/27. [CrossRef]
- Al-Asmar AA, Al-Hiyasat AS, Abu-Awwad M, et al. Reframing Perceptions in Restorative Dentistry: Evidence-Based Dentistry and Clinical Decision-Making. International journal of dentistry 2021, 2021, 4871385–2022. [Google Scholar] [CrossRef]
- Girotto LPS, Dotto L, Pereira GKR, et al. Restorative preferences and choices of dentists and students for restoring endodontically treated teeth: A systematic review of survey studies. The Journal of prosthetic dentistry 2021, 126, 489–489.e485. [Google Scholar] [CrossRef]
- Pizzolotto L and Moraes RR. Resin Composites in Posterior Teeth: Clinical Performance and Direct Restorative Techniques. Dentistry journal 2022, 10 2022/12/23. 2022. [CrossRef]
- Caussin E, Izart M, Ceinos R, et al. Advanced Material Strategy for Restoring Damaged Endodontically Treated Teeth: A Comprehensive Review. Materials 17(15)(2024).
- Murchie B, Jiwan N and Edwards D. What are the success rates of anterior restorations used in localised wear cases? Evidence-based dentistry 2025, 26, 54–56. [CrossRef]
- Ille CE, Jivănescu A, Pop D, et al. Exploring the Properties and Indications of Chairside CAD/CAM Materials in Restorative Dentistry. Journal of functional biomaterials 2025, 16 2025/02/25. [CrossRef]
- Barakat B, Milhem M, Naji GM, et al. Assessing the Impact of Green Training on Sustainable Business Advantage: Exploring the Mediating Role of Green Supply Chain Practices. Sustainability 15(19)(2023).
- Kaurani P, Batra K, Rathore Hooja H, et al. Assessing the Compliance of Dental Clinicians towards Regulatory Infection Control Guidelines Using a Newly Developed Survey Tool: A Pilot Cross-Sectional Study in India. Healthcare (Basel, Switzerland) 2022, 10 2022/10/28. [CrossRef]
- Boulding H and Hinrichs-Krapels, S. Factors influencing procurement behaviour and decision-making: an exploratory qualitative study in a UK healthcare provider. BMC Health Services Research 2021, 21. [Google Scholar] [CrossRef]
- Antoniadou M, Chrysochoou G, Tzanetopoulos R, et al. Green Dental Environmentalism among Students and Dentists in Greece. Sustainability 15(12)( 2023.
- Beske-Janssen P, Johnsen T, Constant F, et al. New competences enhancing Procurement’s contribution to innovation and sustainability. Journal of Purchasing and Supply Management 2023, 29, 100847. [Google Scholar] [CrossRef]
- Barnes E, Bullock AD, Bailey SE, et al. A review of continuing professional development for dentists in Europe(*). European journal of dental education: official journal of the Association for Dental Education in Europe 2013, 17 Suppl 1, 5-17. 2013/04/23. [CrossRef]
- Țâncu AMC, Imre M, Iosif L, et al. Is Sustainability Part of the Drill? Examining Knowledge and Awareness Among Dental Students in Bucharest, Romania. Dentistry journal 2025, 13 2025/03/26. [CrossRef]
- Antoniadou M, Intzes A, Kladouchas C, et al. Factors Affecting Water Quality and Sustainability in Dental Practices in Greece. Sustainability 2023, 15, 9115. [Google Scholar] [CrossRef]
- Kichenin J, Vallaeys K, Arbab Chirani R, et al. How does gender influence student learning, stress and career choice in endodontics? International endodontic journal 2025 2025/03/14. [CrossRef]
- Wolbring G and Nguyen, A. Equity/Equality, Diversity and Inclusion, and Other EDI Phrases and EDI Policy Frameworks: A Scoping Review. Trends in Higher Education 2(1)( 2023. [CrossRef]
- Al-Sbei R, Ataya J, Jamous I, et al. The Impact of a Web-Based Restorative Dentistry Course on the Learning Outcomes of Dental Graduates: Pre-Experimental Study. JMIR formative research 2024, 8, e51141–2024. [Google Scholar] [CrossRef]
- Wang YM and Chang, YC. Initiating gender mainstreaming in dentistry. Journal of dental sciences 2022, 17, 1411–1412. [Google Scholar] [CrossRef]
- Gheorghe A, Roberts TE, Ives JC, et al. Centre selection for clinical trials and the generalisability of results: a mixed methods study. PloS one 2013, 8, e56560–2013. [Google Scholar] [CrossRef]
- Patino CM and Ferreira, JC. Inclusion and exclusion criteria in research studies: definitions and why they matter. Jornal brasileiro de pneumologia: publicacao oficial da Sociedade Brasileira de Pneumologia e Tisilogia 2018, 44, 84–2018. [Google Scholar] [CrossRef]
- Torgerson DJ and Torgerson, CJ. Pilot Randomised Controlled Trials. In: Torgerson DJ and Torgerson CJ (eds) Designing Randomised Trials in Health, Education and the Social Sciences: An Introduction. London: Palgrave Macmillan UK, 2008, pp.119-126.
- Leon AC, Davis LL and Kraemer HC. The role and interpretation of pilot studies in clinical research. Journal of psychiatric research 2011, 45, 626–629. [Google Scholar] [CrossRef]
- Thabane L, Ma J, Chu R, et al. A tutorial on pilot studies: the what, why and how. BMC Medical Research Methodology 2010, 10, 1. [Google Scholar] [CrossRef]
- Hallingberg B, Turley R, Segrott J, et al. Exploratory studies to decide whether and how to proceed with full-scale evaluations of public health interventions: a systematic review of guidance. Pilot and Feasibility Studies 2018, 4, 104. [Google Scholar] [CrossRef]
- Bornstein M, Al-Nawas B, Kuchler U, et al. Consensus Statements and Recommended Clinical Procedures Regarding Contemporary Surgical and Radiographic Techniques in Implant Dentistry. The International journal of oral & maxillofacial implants 2014, 29, 78–82. [Google Scholar] [CrossRef]
Figure 1.
Mean scores and 95% confidence intervals (CIs) for different aspects of knowledge regarding resin materials.
Figure 1.
Mean scores and 95% confidence intervals (CIs) for different aspects of knowledge regarding resin materials.
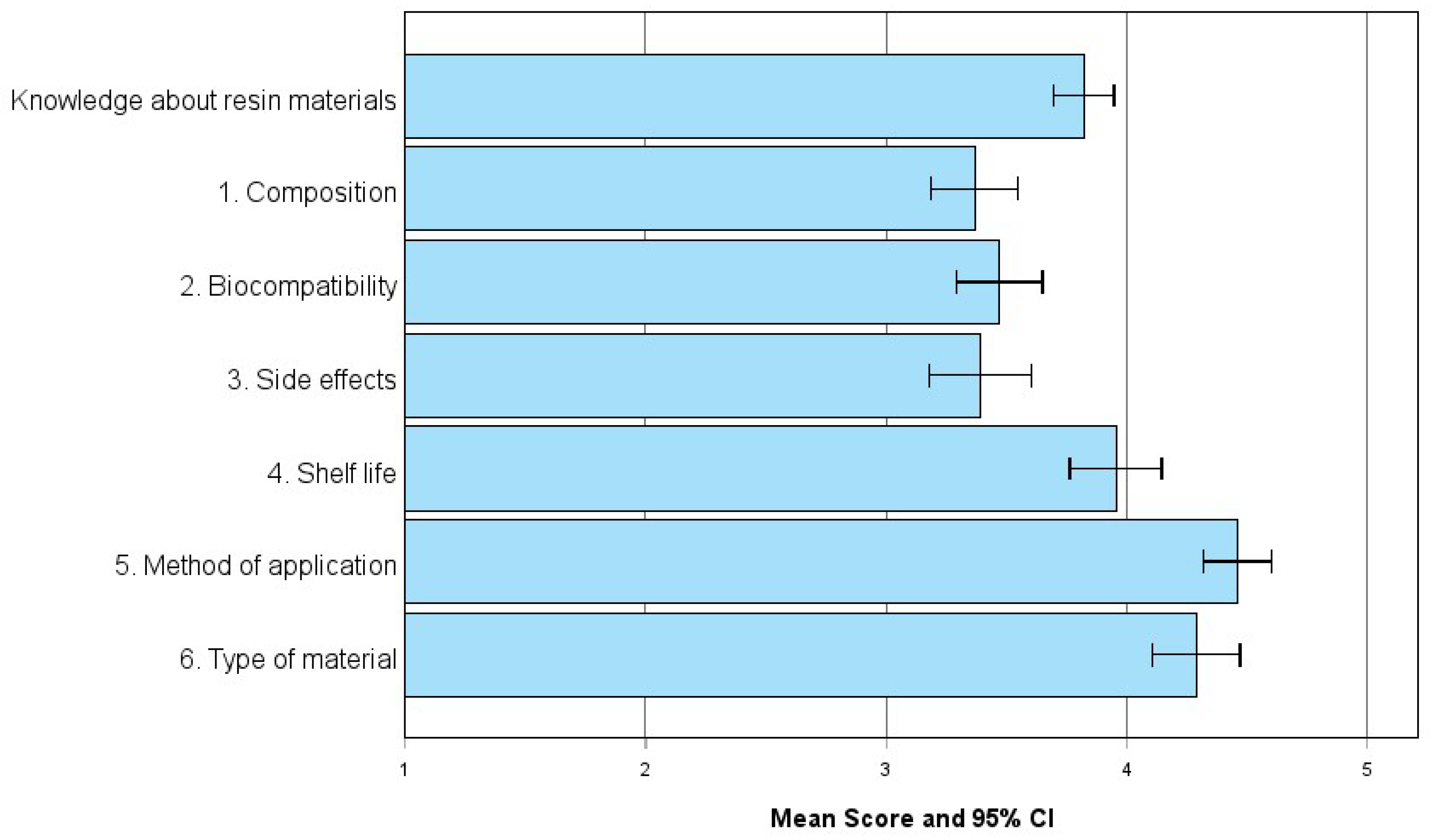
Figure 2.
Selection criteria for resin materials in anterior and posterior restorations.
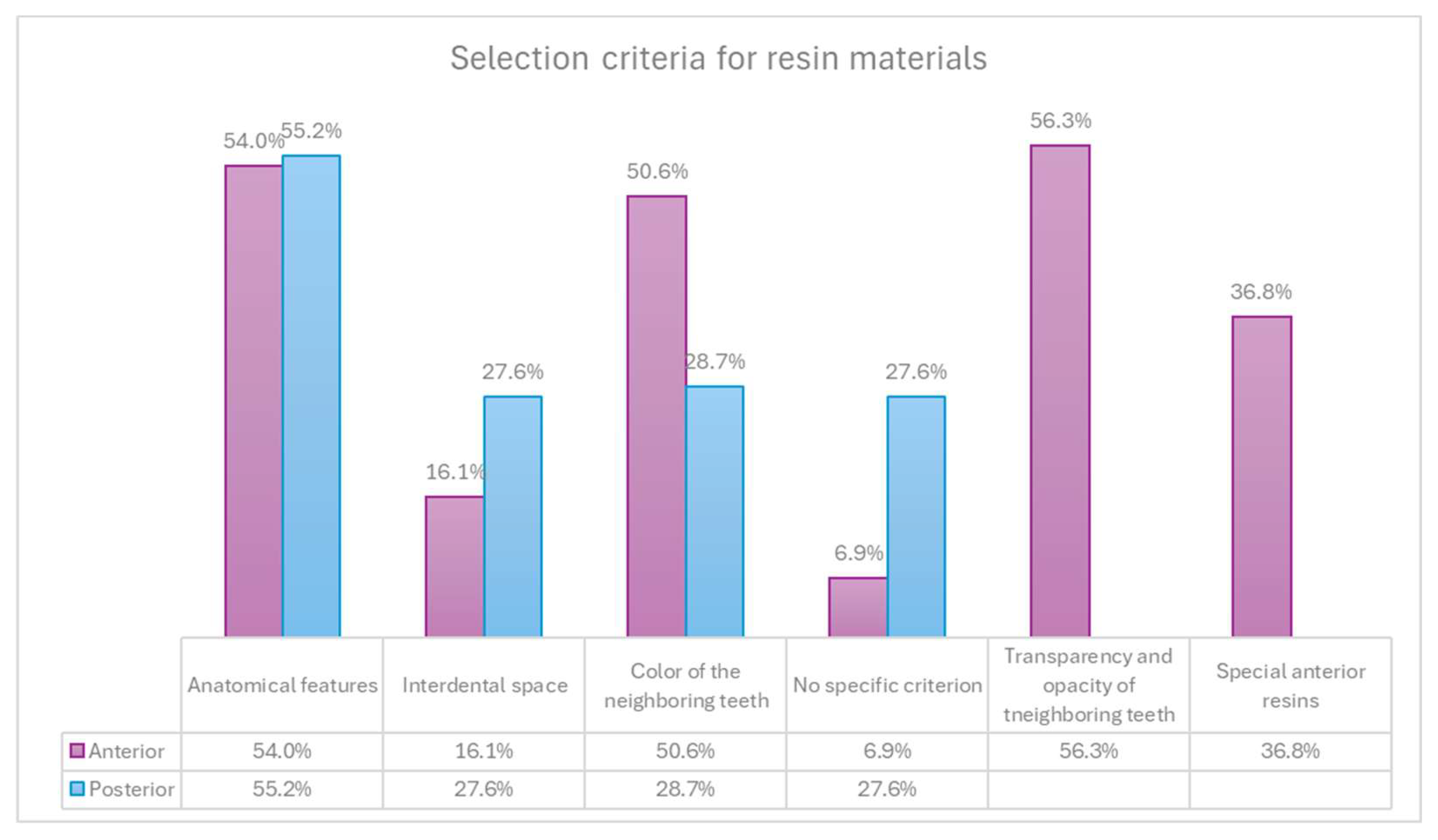
Figure 3.
Importance of environmental factors when purchasing resin restorative materials for conservative restorations, segmented by gender.
Figure 3.
Importance of environmental factors when purchasing resin restorative materials for conservative restorations, segmented by gender.
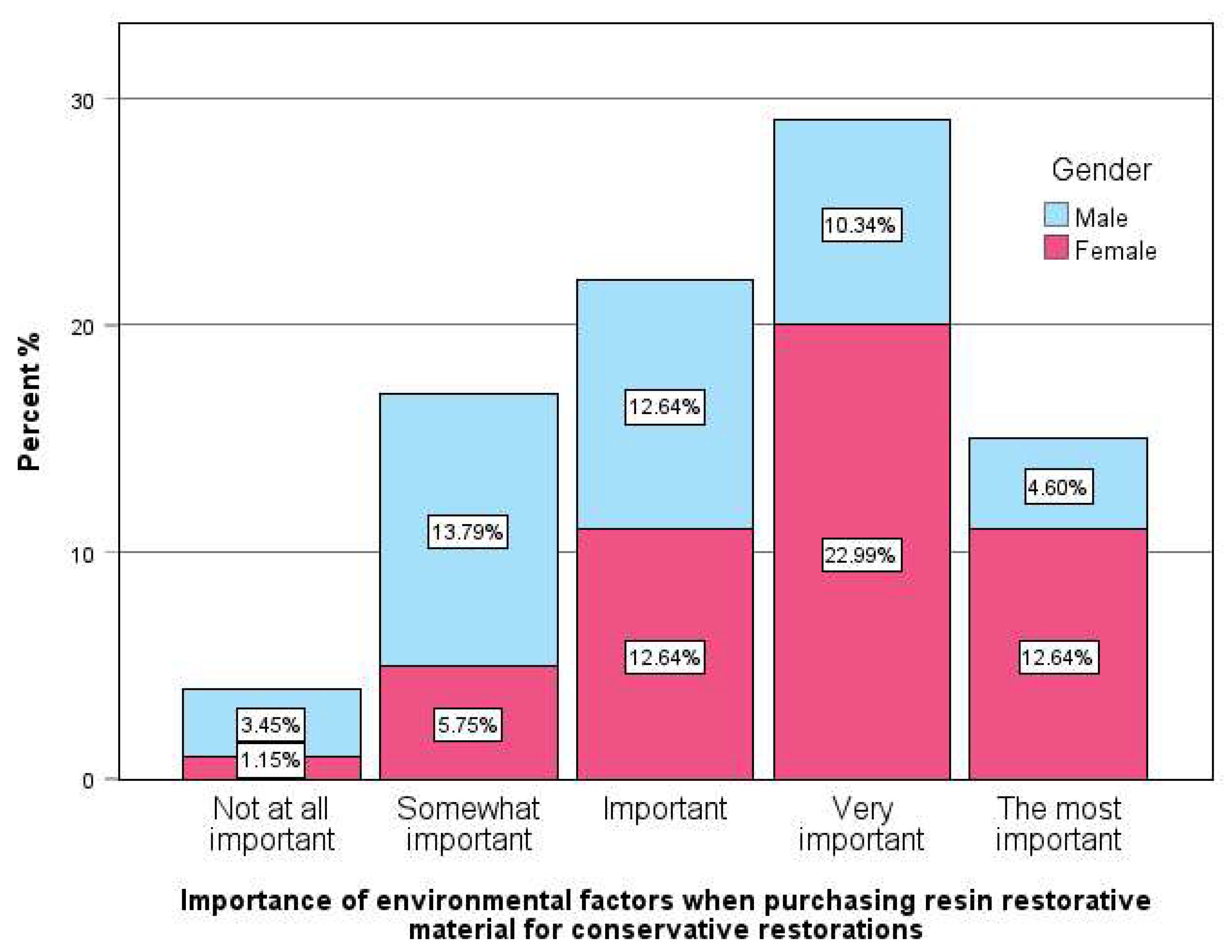

Table 1.
Correlations between professional characteristics and knowledge of resin restorative materials.
Table 1.
Correlations between professional characteristics and knowledge of resin restorative materials.
|
Gender (female vs male dentists) |
Age (over 45 years vs younger) |
Dental school (foreign vs domestic) |
Postgrad studies in Dentistry |
Clinical experience (over 5 years vs up to 5 years) |
Employment (private clinic vs other) |
Purchasing resin restorations over 2 times/year |
Not responsible for supply of resin restorations |
Performing over 20 composite resin restorations per week. | |
| Knowledge about resin materials | -0.152 | .236* | 0.118 | 0.175 | .214* | 0.055 | 0.062 | -0.052 | 0.195 |
| 1. Composition | -0.085 | 0.163 | 0.118 | 0.164 | .230* | -0.044 | 0.061 | -0.153 | 0.206 |
| 2. Biocompatibility | -.248* -0.084 -0.024 -0.012 -0.165 |
0.045 0.135 0.208 .214* 0.137 |
0.158 -0.052 0.116 0.107 0.072 |
0.138 0.072 0.039 0.186 0.161 |
-0.014 0.033 .223* 0.159 0.177 |
-0.015 -0.041 0.170 0.028 0.097 |
0.129 0.072 0.110 -0.164 -0.099 |
0.098 0.179 -0.145 0.039 -0.115 |
0.081 0.041 0.149 0.100 0.141 |
| 3. Side effects 4. Shelf life 5. Method of application 6. Type of material |
Table 2.
Familiarity with specifications and features priority in choosing resin restorative materials.
Table 2.
Familiarity with specifications and features priority in choosing resin restorative materials.
| N | % | ||
| Familiarity with specifications for dental resin restorative materials | Yes | 55 | 71.4% |
| No | 22 | 28.6% | |
| Importance of resin restorative material compliance with specifications | Very high | 28 | 32.2% |
| High | 47 | 54.0% | |
| Moderate | 12 | 13.8% | |
| Features priority when choosing resin restorative materials | Biocompatibility | 21 | 25.9% |
| Photopolymerization depth | 13 | 16.0% | |
| Bending strength | 28 | 34.6% | |
| Water absorbency, Solubility, etc. | 19 | 23.5% | |
| Green practice but falls slightly short of some of the ISO specifications | Certainly yes | 4 | 4.9% |
| It depends on the specifications | 45 | 54.9% | |
| No, for me ISO standards are the most important selection criterion | 33 | 40.2% |
Note: *p < .05.
Table 3.
Selection criteria for resin materials in anterior and posterior tooth restorations.
| Total sample | Clinical experience (in years) | |||||
| up to 5 years | over 5 years | |||||
| N | % | N | % | |||
|
What are the selection criteria for the resin materials you choose for anterior tooth restorations? | ||||||
| It depends on the anatomical features I want to achieve It depends on the interdental space that exists |
47 |
54.0% |
31 |
70.5% |
16 |
37.2% |
| 14 | 16.1% | 10 | 22.7% | 4 | 9.3% | |
| It depends on the color of the neighboring teeth | 44 | 50.6% | 25 | 56.8% | 19 | 44.2% |
| It depends on the transparency and opacity of the neighboring teeth | 49 | 56.3% | 29 | 65.9% | 20 | 46.5% |
| I do not have a specific criterion, I use what I have in stock | 6 | 6.9% | 4 | 9.1% | 2 | 4.7% |
| I only use special anterior resins | 32 | 36.8% | 10 | 22.7% | 22 | 51.2% |
| What are the selection criteria for the resin materials you choose for posterior tooth restorations? | ||||||
| It depends on the anatomical features I want to achieve | 48 | 55.2% | 29 | 65.9% | 19 | 44.2% |
| It depends on the interdental space that exists | 24 | 27.6% | 15 | 34.1% | 9 | 20.9% |
| It depends on the color of the neighboring teeth | 25 | 28.7% | 14 | 31.8% | 11 | 25.6% |
| I do not have a specific criterion, I use what I have in stock | 24 | 27.6% | 10 | 22.7% | 14 | 32.6% |
Table 4.
Correlations between selection criteria for resin materials and professional characteristics.
Table 4.
Correlations between selection criteria for resin materials and professional characteristics.
| Selection criteria for the resin materials |
Gender (female vs male) |
Age (over 45 years) |
Dental school (foreign vs domestic) |
Postgrad studies in dentistry |
Clinical experience (>5 years) |
Employment (private clinic vs other) | Purchasing resin restorations over 2 times/year | Not responsible for supply of resin restorations | Performing over 20 restorations/ week |
| What are the selection criteria for the resin materials you choose for anterior tooth restorations? | |||||||||
| It depends on the anatomical features I want to achieve | -0.043 | -0.204 | 0.055 | -0.134 | -.334** | -0.090 | 0.021 | 0.120 | -.315** |
| It depends on the interdental space that exists | -0.108 | -0.054 | -0.117 | -0.020 | -0.183 | 0.017 | 0.044 | 0.112 | -0.071 |
| It depends on the color of the neighboring teeth | 0.080 | -0.105 | 0.025 | -0.127 | -0.126 | 0.033 | 0.166 | 0.017 | -0.160 |
| It depends on the transparency and opacity of the neighboring teeth | 0.185 | -.239* | -0.028 | -0.076 | -0.196 | -0.188 | 0.090 | 0.040 | -0.164 |
| I do not have a specific criterion, I use what I have in stock | -0.028 | -0.007 | -0.124 | 0.068 | -0.088 | 0.154 | -0.085 | 0.014 | 0.126 |
| I only use special anterior resins | 0.017 | 0.199 | 0.030 | .337** | .295** | -0.127 | 0.004 | -0.151 | 0.113 |
| What are the selection criteria for the resin materials you choose for posterior tooth restorations? | |||||||||
| It depends on the anatomical features I want to achieve | 0.071 | -0.173 | 0.044 | 0.085 | -.218* | -0.162 | 0.105 | 0.055 | -0.133 |
| It depends on the interdental space that exists | 0.091 | -0.123 | -0.077 | -0.058 | -0.147 | -0.012 | 0.142 | -0.025 | -0.037 |
| It depends on the color of the neighboring teeth | -0.041 | 0.020 | -0.021 | 0.132 | -0.069 | 0.164 | 0.178 | -0.097 | -0.057 |
| I do not have a specific criterion; I use what I have in stock | -0.116 | -0.015 | -0.009 | -0.164 | 0.110 | 0.039 | -0.192 | 0.086 | -0.018 |
| I do not know / do not answer | 0.097 | -0.078 | -0.049 | -0.084 | -0.107 | 0.097 | -0.072 | -0.072 | -0.083 |
Table 5.
Correlations between professional characteristics and familiarity with specifications and features priority in resin restorative materials.
Table 5.
Correlations between professional characteristics and familiarity with specifications and features priority in resin restorative materials.
| Gender (female vs male) | Age (over 45 years) | Dental school (foreign vs domestic) | Post-grad studies in dentistry | Clinical experience (over 5 years) | Employment (private clinic vs other) | Purchasing resin restorations over 2 times/year | Not responsible for supply of resin restorations | Performing over 20 restorations/ week | |
| Familiarity with specifications | -0.033 | 0.076 | 0.132 | -0.108 | .231* | -0.041 | .254* | -.341** | 0.163 |
| Specifications importance | 0.109 | 0.150 | 0.094 | 0.038 | 0.195 | -0.025 | 0.052 | -0.092 | 0.095 |
| Features priority when choosing resin restorative materials | |||||||||
| Biocompatibility | .232* | 0.136 | 0.177 | 0.213 | 0.106 | -0.106 | -0.105 | 0.093 | -0.026 |
| Photopolymerization depth | -0.162 | -0.084 | -0.022 | -0.147 | 0.050 | -0.117 | -0.084 | -0.001 | 0.113 |
| Bending strength | -0.204 | -0.111 | 0.011 | -0.056 | -.233* | 0.181 | 0.112 | -0.092 | -0.078 |
| Water absorbency, Solubility, etc. | 0.130 | 0.056 | -0.176 | -0.030 | 0.108 | 0.009 | 0.056 | 0.009 | 0.019 |
| Green practice but falls slightly short of some of the ISO specifications | |||||||||
| Certainly yes | 0.092 | 0.181 | 0.066 | 0.057 | 0.113 | -0.028 | 0.211 | -0.021 | 0.182 |
| It depends on the specifications | 0.114 | -0.176 | 0.029 | -0.001 | -0.025 | -0.061 | -0.172 | 0.099 | 0.020 |
| No, for me ISO standards are the most important selection criterion | -0.155 | 0.099 | -0.058 | -0.024 | -0.025 | 0.075 | 0.082 | -0.091 | -0.102 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



