
Submitted:
11 April 2025
Posted:
14 April 2025
You are already at the latest version
Abstract
Background/Objectives: Pancreatic cancer (PC) is among the most lethal cancers, with increasing incidence and poor survival worldwide. We examined population-based PC incidence and survival trends in the Region of Murcia, Spain, during 1983-2018. Methods: Population-based registry data were obtained. All primary invasive PC cases from 1983–2018 were included and classified as pancreatic neuroendocrine tumors (pNETs), non-pNETs and non-histologically-confirmed tumors. Age-specific and age-standardized incidence rates per 100,000 person-years (py) were calculated. Annual percentage changes (APCs) were estimated via joinpoint regression. Age-standardized net survival was calculated using the Pohar-Perme method. All results were stratified by sex, age, histological group and period. Results: In total, 3819 patients were diagnosed. The incidence rates in men increased from 11.2/100,000 py (1983–1988) to 21.8/100,000 py (2013–2018), and those in women increased from 7.2 to 15.2/100,000 py. The APC was more pronounced in women aged 15-44 years (APC=+5.2%, 95% CI=1.5, 9.0) than in men (APC=+0.5, 95% CI=-1.5, 2.5). Among all confirmed cases, 93.3% were non-pNETs (APC=5.6%), and 6.7% were pNETs (APC=12.6%). Five-year survival rates were 5.1% (95% CI=3.3, 7.0) in the 1990s and 11.4% (95% CI=2.7, 13.1) in the 2010s (non-pNET patients=7.4%, pNET patients=57.5%). Conclusions: PC incidence increased in the Region of Murcia, Spain particularly among younger women and pNET patients. Survival improved, doubling from the 1990s to the 2010s. These findings highlight the need to develop preventive strategies targeting high-risk populations, especially young women, while improving early PC diagnosis to continue increasing PC survival rates.
Keywords:
Pancreatic cancer
; Pancreatic neuroendocrine tumors
; Incidence
; Survival
; Population-based
; Spain
1. Introduction
Pancreatic cancer (PC) is one of the most aggressive cancers worldwide and is the fourth leading cause of cancer-related mortality in Europe and the third leading cause in Spain. In 2022, there were more than half a million incident cases worldwide, with estimates that this number will double by 2040, causing more deaths than prostate, colon, and breast cancers combined [1]. The incidence patterns of PC exhibit significant geographical variation, increasing in most countries, with socioeconomic factors playing a key role. The prognosis of patients with PC is unfavorable, with five-year survival rates less than 6% [2,3]. Despite improvements in PC care, its prognosis remains unfavorable, underscoring the importance of prevention efforts.
Risk factors for PC include tobacco use, obesity, diabetes, chronic pancreatitis and heavy alcohol consumption and exposure to persistent organic pollutants [4,5,6,7]. While this cancer is more common in men than in women [8], recent studies have shown an increase in incidence among women (particularly younger women) compared with men [9,10].
Although several methods have been proposed for the early detection of PC [11], diagnosing it in the initial stages remains challenging, as it usually does not present with symptoms. Therefore, the US Preventive Services Task Force recommends routine screening for this cancer in asymptomatic adults [12].
PCs are broadly categorized into two main groups: pancreatic neuroendocrine tumors (pNETs) and non-pNETs. Non-pNETs, mainly adenocarcinomas, are the most common and aggressive type, whereas pNETs are less common and have a better prognosis than non-pNETs [13].
Population-level monitoring of cancer incidence and survival provides essential indicators for cancer control [3,14]. Studies providing detailed and updated long-term trends in the incidence and survival of patients with PC are scarce. Therefore, the aim of the present study was to determine the population-based incidence and survival trends of PC over a long period in the Region of Murcia, Spain.
2. Materials and Methods
2.1. Study Population
Data on newly diagnosed PC cases were obtained from the population-based Murcia Cancer Registry (RCM) located in southeastern Spain, which covers more than 1.5 million inhabitants in 2023 [15]. The registry has been successfully operating since 1982 and is affiliated with the Murcia Regional Health Council Department of Epidemiology. The RCM is a member of the Spanish Network of Cancer Registries (Red Española de Registros de Cáncer—REDECAN; redecan.org/es/index.cfm) and the European Network of Cancer Registries (ENCR; www.encr.eu). The RCM participates in EUROCARE (www.eurocare.it) and CONCORD (csg.lshtm.ac.uk), and its data are published in successive editions on ‘Cancer Incidence in Five Continents’, a reference publication edited by the International Agency for Research on Cancer (IARC, Lyon, France; ci5.iarc.fr) [16].
2.2. Data Collection
All registered patients with new invasive PC diagnosed within the 35-year period from January 1st, 1983, to December 31st, 2018, were included, except for those under 15 years of age, due to a lack of cases in the youngest age groups. All tumors, including PC, have topographic morphology and behavior codes according to the International Classification of Diseases for Oncology (ICD-O-3). Incident cases of primary invasive pancreatic neoplasms (C25.0 - C25.9), following the IARC-ENCR rules for the definition of primary cancers [17], were eligible for analysis. Tumors that were benign, in situ, or of uncertain nature were excluded.
According to the Third Edition of the ICD-O, incident cases were classified into three histological groups: 1) histologically confirmed non-pNETs, with codes of 8010, 8012, 8020, 8022, 8031, 8050, 8070, 8074, 8140, 8144, 8211, 8230, 8260, 8310, 8440, 8441, 8450, 8452, 8453, 8470, 8480, 8481, 8490, 8500, 8523, 8550, 8560, and 8570; 2) histologically confirmed pNETs, with codes of 8013, 8042, 8150, 8151, 8152, 8153, 8240, 8246, and 8249; and 3) nonhistologically confirmed cases, with codes of 8000 and 8001. Sarcomas and lymphomas were not included in this analysis.
The survival data included complete follow-up data of the study participants from the date of diagnosis until December 31st, 2018. Vital status was ascertained on the basis of whether the participants were alive or dead at the end of follow-up (including the date of death) or were censored because of loss to follow-up or incomplete follow-up. Patients with complete follow-up were those with a known vital status (alive or dead) at one, three or five years after diagnosis. Multiple sources of information, including the National Death Index, the Social Security database, municipal censuses, medical records or hospital notes, primary care records, and pathology laboratories, were used to ascertain vital status. Data quality was verified using both the IARC check [18] and the EUROCARE rules [19]. The variables used for this study were sex, age, date of birth, date of diagnosis, histology group, date of end of follow-up and vital status (alive, dead, censored, unknown).
The study was conducted according to the EU 2016/679 General Data Protection Regulation (GDPR) regarding the use of anonymized population data [20]. All the data extracted and collected from the study database for incidence and survival analyses were anonymous; therefore, no ethical approval was required [21].
2.3. Statistical Analysis
A descriptive analysis was conducted accounting for the total number of cases in the study period (1983 to 2018), both overall and stratified by sex and age groups (15-44, 45-54, 55-64, 65-74 and ≥75 years).
Age-adjusted standardized incidence rates (ASIRs) per 100,000 py (py) and their 95% confidence intervals (95% CI) were also analyzed by sex, six-year period (1983–1988; 1989–1994; 1995–2000; 2001–2006; 2007–2012; 2013–2018), and histological group. ASIRs were calculated via the direct method [22] with the 2013 European Standard Population as the reference [23]. To quantify changes in incidence trends for the entire study period (1983–2018) for the whole population and by age, sex, and histological group, we used joinpoint regression analysis of the ASIR data with their standard deviations. Annual percentage changes (APCs) and their 95% CIs were calculated, with each joinpoint marking a significant change in the trend.
The number of joinpoints was set between 0 and 5, and the grid method and adjustment by permutation test [24] were selected, with an overall significance level of 0.05. The minimum number of data points from the beginning of the series was set at 4 years, and there were at least 5 years between two consecutive joinpoints.
Survival was calculated for patients diagnosed between 1990 and 2018. Age-standardized net survival (ASNS) analysis was performed for the study periods of 1990-1999, 2000-2009, and 2010-2018, which were stratified by sex, age, and histological group.
One (1y), three (3y), and five-year (5y) ASNS were calculated with the Pohar-Perme method [24], following the cohort approach and using International Cancer Survival Standards (ICSS) weights [25].
Analyses were performed using Stata/SE version 14, R packages (Epidemiology Tools 0.5-10.1), and the Joinpoint Regression Program, version 4.6 [26]. P < 0.05 was considered to indicate statistical significance.
3. Results
3.1. Incidence Trends
A total of 3819 patients (54% men) with PC were included in the analyses during the study period after excluding cases under 15 years of age, sarcomas, and lymphomas. Microscopic verification was confirmed in 61.4% of all PC patients. The mean age of the patients was 69.7 years (SD 12.4). Overall, the ASIR for both men and women doubled over the study period (1983–2018). In men, it increased from 11.2 to 21.8 per 100,000 py, with an APC of 2.0% (95% CI=1.4, 2.6), whereas in women, it rose from 7.2 to 15.2 per 100,000 py, with an APC of 2.5% (95% CI=2.0, 3.0), which was higher than that in men. There were no statistically significant changes according to age or sex (Figure 1).
The incidence rates were higher in men than in women and increased with age, being lowest in the 15–44 years age group and highest in those aged ≥75 years. Young women presented a significant increase, with an APC of 5.2% (95% CI=1.5, 9.0) in the 15-44-year age group and 4.5% (95% CI=2.8, 6.3) in the 45-54-year age group, compared with lower APCs in men in the same age range, with 0.5% and 2.8%, respectively (Table 1, Figure 2).
The ASIRs of PC were also analyzed according to histological group. Non-pNET cases constituted the majority (93.3%), with an ASIR of 7.9 (95% CI=7.6, 8.2) per 100,000 py, whereas pNET cases were less common (6.7%), with an ASIR of 0.5 (95% CI=0.4, 0.6) per 100,000 py. Nonhistologically confirmed cases made up 38.6% of the total cases, with an ASIR of 5.8 (95% CI=5.5, 6.1) per 100,000 py (Table 2).
An increasing trend in incidence was observed for both histological groups throughout the study period, with a significantly higher APC for pNETs (12.6%) than for non-pNETs (5.6%). With respect to tumors without histological confirmation, the joinpoint analysis revealed an APC of +0.03% per year from 1983 to 2004 no statistically significant. However, from 2004 to 2018, there was a statistically significant reduction in incidence rates, with an APC of -0.27% per year (Figure 3)
3.2. Survival Trends
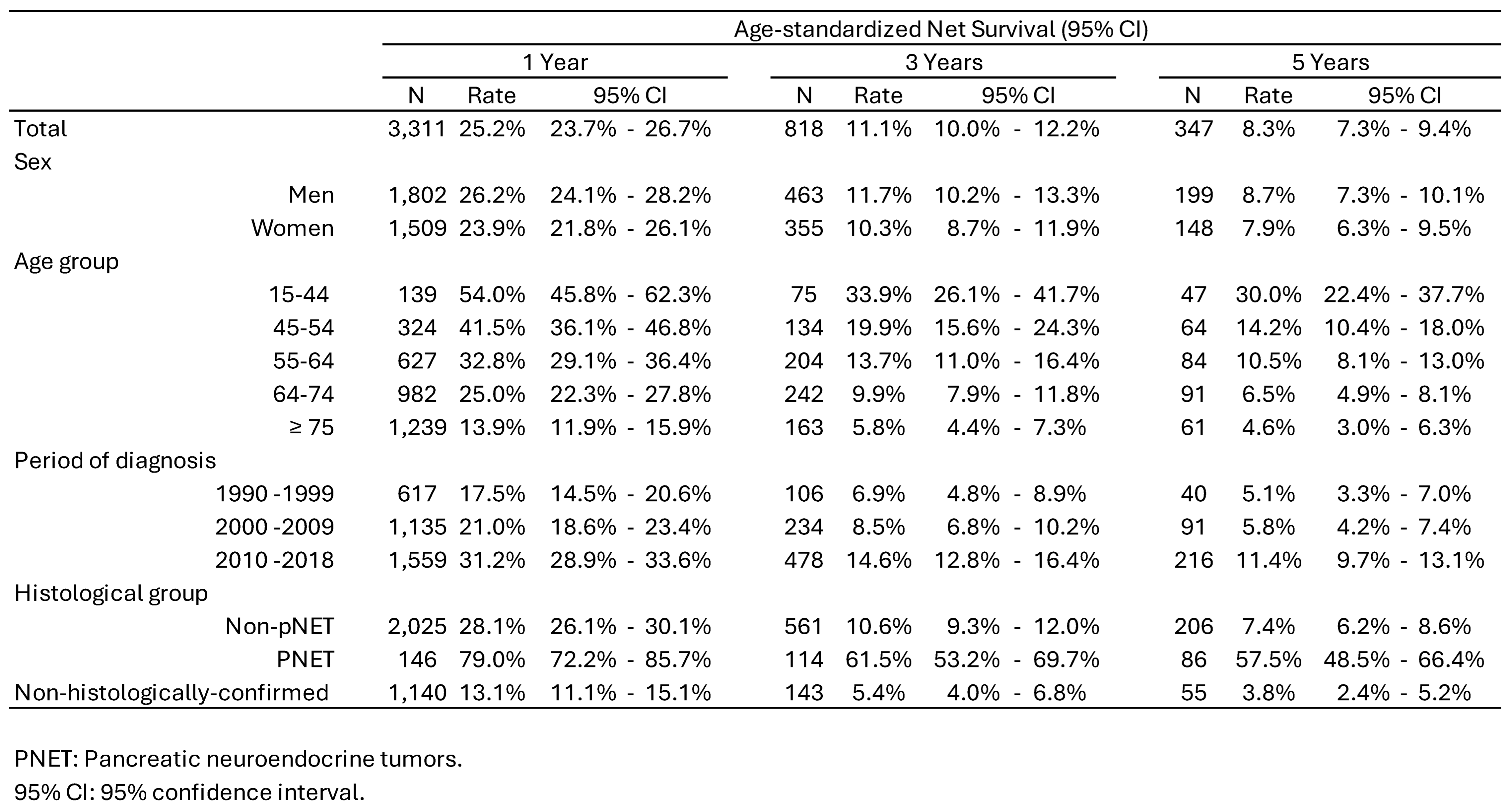
The ASNS rates at one (1y), three (3y), and five (5) years after diagnosis decreased significantly over time, halving from 25.2% (95% CI=23.7%, 26.7%) at 1y to 11.1%, (CI: 10%, 12.2%) at 3y, and further declining to 8.3% (95% CI=7.3%, 9.4%) at 5y after diagnosis. Men had slightly higher survival rates than women did: 1 year (26.2% vs. 23.9%), 3 years (11.7% vs. 10.3%), and 5 years (8.7% vs. 7.9%). Survival rates decline with increasing age. Patients aged 15-44 years had the highest survival rates (54% at 1 y; 33.9% at 3 y; and 30% at 5 y). However, for those over 75 years of age, the rates were the lowest (13.9% at 1 y, 5.8% at 3 y, and 4.6% at 5 y). Survival rates improved over time. For patients diagnosed between 1990 and 2018,1-year survival rates increased from 17.5% to 31.2%, 3-year survival rates rose from 6.9% to 14.6%, and 5-year survival rates improved from 5.1% to 11.4%. Survival rates also varied by histological type. Patients with non-pNETs had very low survival rates, with 28.1% at 1 y, 10.6% at 3 y, and 7.4% at 5 y. In contrast, those with pNETs had significantly higher survival rates: 79.0% at 1 y, 61.5% at 3 y, and 57.5% at 5 y (Table 3, Figure 3).
4. Discussion
In the present study, we analyzed data on 3819 patients with PC who were diagnosed between 1983 and 2018. The incidence was notably higher in men than in women, especially among older individuals. Furthermore, the global literature consistently reports that PC is associated with increasing age and male sex [8]. Overall, the incidence of PC has markedly increased over the past three decades in the Region of Murcia, rising more than double from 1983-1988 to 2013-2018. Recent studies evaluating long-term incidence trends, particularly in developed countries, have shown significant increases in PC incidence, which aligns with our findings [27,28]. Some of the increase could be due to improvements in cancer registration coding and clinical diagnostic accuracy over time. Although our analysis excluded sarcomas and lymphomas and this distinction was not specified in some of the comparative studies, the impact on the results must be minimal given the very low incidence of these cancers.
The incidence rates among women under 55 years increased at a higher rate than those among men of the same age group. This group experienced a significant increase in incidence, in contrast with the oldest age group (≥75 years), where the annual increase was far less pronounced, possibly reflecting the competing risk effects of premature death due to other causes. These findings align with several recent studies, including one study in which national population data from the United States revealed a greater increase in the incidence of PC in women aged 15 to 34 years (APC = 2.36%) than in men in the same age group (APC = 0.62%) between 2001 and 2018 [10]. The reasons for the increase in the ASIR in younger women aged 15 to 54 years are unclear. It is important to consider several aspects. The absolute number of cases was low, with ASIRs ranging from 0.3 to 7.9 in patients younger than 55 years, and small variations can lead to larger fluctuations in the APC. Compared with other population groups, young women might be more exposed to modifiable risk factors. Additionally, changes in lifestyle toward a more unfavorable pattern of risk factors in young adult women with PC cannot be ruled out [29]. Thus, the increase in incidence observed in our study could be partially attributed to an aging population, improved diagnostic capabilities or changing patterns of risk factors.
Non-pNET types predominated over pNET types, with a greater proportion of cases in men (56.9%) than in women (43.1%). Another population-based study conducted in a region of northern Spain also highlighted a greater incidence of non-pNETs than pNETs [30]. Although pNETs accounted for only 7% of the total confirmed cases, their incidence significantly increased over the analyzed period, which is consistent with findings of other studies [31].
In several studies, the number of confirmed PC cases has been reported to be relatively low compared with that of other types of cancer. In this study, the proportion of cases with microscopic confirmation was 61.4%, which is higher than that reported in a previous study in Spain [30], which was based on a population-based registry (52%). However, comparisons should be performed cautiously given that the proportion of microscopically confirmed cases has increased worldwide with increasing years since diagnosis. Notably, microscopic confirmation and more specific typing of the cancer are both mandatory for access to the best adjuvant treatment and whenever there is surgical cancer resection, which is the only hope for long-term healing. Therefore, it is not surprising that patients with PC without microscopic confirmation had the worst prognosis in our study and others [32]. Microscopic confirmation involves, at least, the acquisition of cancer cells through fine needle aspiration; even this (not to mention the retrieval of a biopsy sample) is an invasive procedure and is associated with an important risk for serious complications, given the location of the pancreas. Nearly half of the cases of PC are diagnosed at advanced ages, in the 7th and 8th decades of life, where comorbidities are frequent and, in many instances, contraindicate an aggressive approach for the management of disease, negating any possible benefit from microscopic assessment.
Since 2004, there has been a notable and statistically significant decrease in the number of nonhistologically confirmed cases. This decline suggests improvements in diagnostic practices, with more cases being confirmed histologically, although further progress is still needed.
Although the prognosis remains poor, survival has doubled from 1990 to 2018, reaching 11.4% at five years compared with 5.1%, which was higher in men than in women and decreased with increasing age, in line with what has been reported in the literature. Similarly, a study analyzing the overall evolution of relative survival rates for pancreatic cancer also reports a slight increase in survival since 2000, although it concludes that no significant progress has been made in overall survival [33]. The SUDCAN study, whose data were extracted from the EUROCARE-5 study, reported an age-adjusted standardized net survival (5y-ASNS) lower than that reported in our study, which was 6% in 2000-2004 [34]. A study that analyzes the global evolution of pancreatic cancer survival identifies similarities with our findings. While our analysis indicates an improvement in survival over time, the global study concludes that, based on relative survival analysis, no significant progress in overall survival has been observed, although a slight increase has been reported after the year 2000.
The low survival rates are partly attributed to the advanced tumor stage at diagnosis in most cases; only approximately 10% to 15% of patients are diagnosed with early-stage (stage I) and surgically resectable disease [35].
In 2020, Siegel’s study highlighted an overall trend of improved cancer survival rates due to advancements in early detection and treatment techniques [36]. However, for PC, no major improvements in prognosis have been achieved, especially for non-pNETs [37]. Neither advances in therapeutic approaches with new selective molecules against specific cellular targets nor earlier detection using new high-resolution imaging techniques in recent years have significantly improved PC prognosis [38,39].
The survival of patients with pNETs was significantly greater than that of patients with non-pNETs. These findings are in line with better survival rates for pNETs reported globally [40], as well as in populations in Spain [30]. The biological behavior of pNETs leads to earlier symptomatic presentation and thus earlier detection than non-pNETs. PNETs also usually grow more slowly than other types of PC. Because of these factors, pNETs are also more likely to be resectable [41]. Additionally, pNETs tend to respond better to chemotherapy and radiation therapy than other types of PC do [42]. The 5-year survival rate for pNET patients is approximately 50% for all stages combined, whereas the 5-year survival rate for non-pNET patients is less than 10% [30]. However, importantly, individual patient factors, such as age, overall health, and the stage of cancer, can also impact survival outcomes.
The major strength of this research is that the results are based on data from a population-based cancer registry that adheres to high-quality international standards. Additionally, the study period of more than three decades allows for an accurate assessment of population incidence trends and survival rates, providing a valid analysis of the epidemiological trend of this tumor. The results of the Region of Murcia could be similar to those of other regions in Spain because of the similarities in the health care system and sociodemographic and lifestyle backgrounds.
The percentage of cases without microscopic confirmation was 38.6%, which may affect the calculation of incidence and survival by introducing potential classification biases. Additionally, the small number of cases in certain subgroups could reduce the statistical precision of the indicator calculated. The lack of information on the stage of the tumor at diagnosis is another limitation.
5. Conclusions
In conclusion, in the Region of Murcia, Spain the incidence of PC has risen significantly over three decades, with a pronounced increase among younger women and in cases of pNETs. The one-year, three-year, and five-year survival rates improved significantly over the study period, doubling at each time point. The survival rate in the pNET group was much higher than that in the non-pNET group and the nonhistologically confirmed group. These findings highlight the better prognosis associated with pNETs compared with other types of PC and underscore the impact of histological classification on survival outcomes. While the overall burden of pancreatic cancer remains highest among older adults, where its impact in terms of mortality is most significant, the rise in incidence among young women is especially concerning. Targeted prevention in high-risk populations and improved early diagnosis are essential to achieve the goal of increasing pancreatic cancer survival rates.
Author Contributions
Conceptualization, S.C.-Y. and M.D.C.; Methodology, S.C.-Y, R.V-M., M.D.C.; Software, M.B.-R. and D.S.; Validation, S.C.-Y. and M.D.C; Formal Analysis, S.C.-Y. and M.D.C.; Investigation, S.C.-Y., M.D.C., R.V.-M.; Resources, not applicable; Data Curation, M.B.-R and D.S.; Writing – Original Draft Preparation, S.C.-Y.; Writing – Review & Editing, S.C.-Y., M.B.-R., R.V.-M, D.S., J.C., R.M.-G, M.D.C.; Visualization, S.C.-Y., M.B.-R. M.D.C; Supervision, MDC; Project Administration, S.C.Y and M.D.C; Funding Acquisition, not applicable.
Funding
This research received no external funding.
Institutional Review Board Statement
Informed Consent Statement
Not applicable in accordance with the EU 2016/679 General Data Protection Regulation (GDPR) regarding the use of anonymized population data.
Data Availability Statement
The dataset is not available on public links. It can be shared in an anonymous version upon reasonable request.
Acknowledgments
We appreciate the commitment of our respective institutions in enabling our research efforts. Our sincere thanks go to the staff of the Cancer Registry of Murcia (under the General Directorate of Public Health, Health Council of Murcia) for their dedicated work, which provided the majority of the raw data used in this study.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Bray, F.; Laversanne, M.; Sung, H.; Ferlay, J.; Siegel, R.L.; Soerjomataram, I.; Jemal, A. Global Cancer Statistics 2022: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA: a cancer journal for clinicians 2024, 74, 229–263. [CrossRef]
- Red Española de Registros de Cáncer; REDECAN 2024. Estimaciones de La Incidencia de Cáncer En España, 2024. Available online: https://redecan.org/es/proyectos/15/estimaciones-de-la-incidencia-del-cancer-en-espana-2023.
- Guevara, M.; Molinuevo, A.; Salmerón, D.; Marcos-Gragera, R.; Carulla, M.; Chirlaque, M.-D.; Rodríguez Camblor, M.; Alemán, A.; Rojas, D.; Vizcaíno Batllés, A.; et al. Cancer Survival in Adults in Spain: A Population-Based Study of the Spanish Network of Cancer Registries (REDECAN). Cancers 2022, 14. [CrossRef]
- World Cancer Research Fund/American Institute for Cancer Research. Diet, Nutrition, Physical Activity and Pancreatic Cancer. Continuous Update Project 2018. Available: Dietandcancerreport.Org; Available at dietandcancerreport.org, 2018;
- Naudin, S.; Li, K.; Jaouen, T.; Assi, N.; Kyro, C.; Tjonneland, A.; Overvad, K.; Boutron-Ruault, M.-C.; Rebours, V.; Vedie, A.-L.; et al. Lifetime and Baseline Alcohol Intakes and Risk of Pancreatic Cancer in the European Prospective Investigation into Cancer and Nutrition Study. International journal of cancer 2018, 143, 801–812. [CrossRef]
- Molina-Montes, E.; Van Hoogstraten, L.; Gomez-Rubio, P.; Löhr, M.; Sharp, L.; Molero, X.; Márquez, M.; Michalski, C.W.; Farré, A.; Perea, J.; et al. Pancreatic Cancer Risk in Relation to Lifetime Smoking Patterns, Tobacco Type, and Dose-Response Relationships. Cancer epidemiology, biomarkers & prevention : a publication of the American Association for Cancer Research, cosponsored by the American Society of Preventive Oncology 2020, 29, 1009–1018. [CrossRef]
- Porta, M.; Gasull, M.; Pumarega, J.; Kiviranta, H.; Rantakokko, P.; Raaschou-Nielsen, O.; Bergdahl, I.A.; Sandanger, T.M.; Agudo, A.; Rylander, C.; et al. Plasma Concentrations of Persistent Organic Pollutants and Pancreatic Cancer Risk. International Journal of Epidemiology 2022, 51, 479–490. [CrossRef]
- Ferlay, J.; Colombet, M.; Soerjomataram, I.; Dyba, T.; Randi, G.; Bettio, M.; Gavin, A.; Visser, O.; Bray, F. Cancer Incidence and Mortality Patterns in Europe: Estimates for 40 Countries and 25 Major Cancers in 2018. European journal of cancer (Oxford, England : 1990) 2018, 103, 356–387. [CrossRef]
- Cavazzani, A.; Angelini, C.; Gregori, D.; Cardone, L. Cancer Incidence (2000-2020) among Individuals under 35: An Emerging Sex Disparity in Oncology. BMC medicine 2024, 22, 363. [CrossRef]
- Abboud, Y.; Samaan, J.S.; Oh, J.; Jiang, Y.; Randhawa, N.; Lew, D.; Ghaith, J.; Pala, P.; Leyson, C.; Watson, R.; et al. Increasing Pancreatic Cancer Incidence in Young Women in the United States: A Population-Based Time-Trend Analysis, 2001-2018. Gastroenterology 2023, 164, 978-989.e6. [CrossRef]
- Sakai, Y.; Honda, M.; Matsui, S.; Komori, O.; Murayama, T.; Fujiwara, T.; Mizuno, M.; Imai, Y.; Yoshimura, K.; Nasti, A.; et al. Development of Novel Diagnostic System for Pancreatic Cancer, Including Early Stages, Measuring MRNA of Whole Blood Cells. Cancer science 2019, 110, 1364–1388. [CrossRef]
- Owens, D.K.; Davidson, K.W.; Krist, A.H.; Barry, M.J.; Cabana, M.; Caughey, A.B.; Curry, S.J.; Doubeni, C.A.; Epling, J.W.J.; Kubik, M.; et al. Screening for Pancreatic Cancer: US Preventive Services Task Force Reaffirmation Recommendation Statement. JAMA 2019, 322, 438–444. [CrossRef]
- Stang, A.; Wellmann, I.; Holleczek, B.; Fell, B.; Terner, S.; Lutz, M.P.; Kajüter, H. Incidence and Relative Survival of Pancreatic Adenocarcinoma and Pancreatic Neuroendocrine Neoplasms in Germany, 2009-2018. An in-Depth Analysis of Two Population-Based Cancer Registries. Cancer epidemiology 2022, 79, 102204. [CrossRef]
- Galceran, J.; Ameijide, A.; Carulla, M.; Mateos, A.; Quiros, J.R.; Rojas, D.; Aleman, A.; Torrella, A.; Chico, M.; Vicente, M.; et al. Cancer Incidence in Spain, 2015. Clinical & translational oncology : official publication of the Federation of Spanish Oncology Societies and of the National Cancer Institute of Mexico 2017, 19, 799–825. [CrossRef]
- Centro Regional de Estadística de la Región de Murcia Padrón Municipal de Habitantes.
- Bray F, Colombet M, Mery L, Piñeros M, Znaor A, Z.R. and F.J. Cancer Incidence in Five Continents, Vol. XI (Electronic Version). (IARC Scientific Publication No. 166).
- IACR-ENCR. International Rules for Multiple Primary Cancers (ICD-O 3rd Ed). Lyon: IACR. 2004.
- Ferlay J, Burkhard C, Whelan S, P.D. Check Conversion Programs for Cancer Registries. (IARC/IACR Tools for Cancer Registries).; Lyon, France: IARC, 2005;
- De Angelis, R.; Francisci, S.; Baili, P.; Marchesi, F.; Roazzi, P.; Belot, A.; Crocetti, E.; Pury, P.; Knijn, A.; Coleman, M.; et al. The EUROCARE-4 Database on Cancer Survival in Europe: Data Standardisation, Quality Control and Methods of Statistical Analysis. European journal of cancer (Oxford, England : 1990) 2009, 45, 909–930. [CrossRef]
- Regulation General Data Protection. Regulation (EU) 2016/679 of the European Parliament and of the Council of 27 April 2016. Available online: https://eur-lex.europa.eu/eli/reg/2016/679/oj (accessed on 15 January 2022).
- European Network of Cancer Registries. Guidelines on Confidentiality in Population- Based Cancer Registration in the European Union. Lyon 2002.
- Breslow, N.E.; Day, N.E. Statistical Methods in Cancer Research. Volume II--The Design and Analysis of Cohort Studies. IARC scientific publications 1987, 1–406.
- Commission., E. Revision of the European Standard Population—Report of Eurostat’s Task Force. 2013.
- Perme, M.P.; Henderson, R.; Stare, J. An Approach to Estimation in Relative Survival Regression. Biostatistics (Oxford, England) 2009, 10, 136–146. [CrossRef]
- Corazziari, I.; Quinn, M.; Capocaccia, R. Standard Cancer Patient Population for Age Standardising Survival Ratios. European journal of cancer (Oxford, England : 1990) 2004, 40, 2307–2316. [CrossRef]
- Joinpoint Regression Program, Version 4.6.0.0 - April 2018; Statistical Methodology and Applications Branch, Surveillance Research Program, N.C.I. No Title 2018.
- Gaddam, S.; Abboud, Y.; Oh, J.; Samaan, J.S.; Nissen, N.N.; Lu, S.C.; Lo, S.K. Incidence of Pancreatic Cancer by Age and Sex in the US, 2000-2018. JAMA 2021, 326, 2075–2077. [CrossRef]
- Samaan, J.S.; Abboud, Y.; Oh, J.; Jiang, Y.; Watson, R.; Park, K.; Liu, Q.; Atkins, K.; Hendifar, A.; Gong, J.; et al. Pancreatic Cancer Incidence Trends by Race, Ethnicity, Age and Sex in the United States: A Population-Based Study, 2000-2018. Cancers 2023, 15. [CrossRef]
- Keyes, K.M.; Jager, J.; Mal-Sarkar, T.; Patrick, M.E.; Rutherford, C.; Hasin, D. Is There a Recent Epidemic of Women’s Drinking? A Critical Review of National Studies. Alcoholism, clinical and experimental research 2019, 43, 1344–1359. [CrossRef]
- García-Velasco, A.; Zacarías-Pons, L.; Teixidor, H.; Valeros, M.; Liñan, R.; Carmona-Garcia, M.C.; Puigdemont, M.; Carbajal, W.; Guardeño, R.; Malats, N.; et al. Incidence and Survival Trends of Pancreatic Cancer in Girona: Impact of the Change in Patient Care in the Last 25 Years. International journal of environmental research and public health 2020, 17. [CrossRef]
- Jiang, Y.; Abboud, Y.; Liang, J.; Larson, B.; Osipov, A.; Gong, J.; Hendifar, A.E.; Atkins, K.; Liu, Q.; Nissen, N.N.; et al. The Disproportionate Rise in Pancreatic Cancer in Younger Women Is Due to a Rise in Adenocarcinoma and Not Neuroendocrine Tumors: A Nationwide Time-Trend Analysis Using 2001-2018 United States Cancer Statistics Databases. Cancers 2024, 16. [CrossRef]
- Huang, L.; Jansen, L.; Balavarca, Y.; Babaei, M.; van der Geest, L.; Lemmens, V.; Van Eycken, L.; De Schutter, H.; Johannesen, T.B.; Primic-Žakelj, M.; et al. Stratified Survival of Resected and Overall Pancreatic Cancer Patients in Europe and the USA in the Early Twenty-First Century: A Large, International Population-Based Study. BMC medicine 2018, 16, 125. [CrossRef]
- Chen, Jun; Xiao, Yu-Xuan; Li, Zhuo-Ying; Zou, Yi-Xin; Zhou, Xiao-Hui; Zhang, Wei; Li, Hong-Lan; Qu, Xu; Xiang, Y.-B. Global Characteristics of Pancreatic Cancer Survival: A Comprehensive Overview of Survival Analysis from Cancer Registration Data. Journal of Pancreatology.
- Bouvier, A.-M.; Bossard, N.; Colonna, M.; Garcia-Velasco, A.; Carulla, M.; Manfredi, S. Trends in Net Survival from Pancreatic Cancer in Six European Latin Countries: Results from the SUDCAN Population-Based Study. European journal of cancer prevention : the official journal of the European Cancer Prevention Organisation (ECP) 2017, 26 Trends, S63–S69. [CrossRef]
- Blackford, A.L.; Canto, M.I.; Klein, A.P.; Hruban, R.H.; Goggins, M. Recent Trends in the Incidence and Survival of Stage 1A Pancreatic Cancer: A Surveillance, Epidemiology, and End Results Analysis. Journal of the National Cancer Institute 2020, 112, 1162–1169. [CrossRef]
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer Statistics, 2020. CA: a cancer journal for clinicians 2020, 70, 7–30. [CrossRef]
- McGuigan, A.; Kelly, P.; Turkington, R.C.; Jones, C.; Coleman, H.G.; McCain, R.S. Pancreatic Cancer: A Review of Clinical Diagnosis, Epidemiology, Treatment and Outcomes. World journal of gastroenterology 2018, 24, 4846–4861. [CrossRef]
- Halbrook, C.J.; Lyssiotis, C.A.; Pasca di Magliano, M.; Maitra, A. Pancreatic Cancer: Advances and Challenges. Cell 2023, 186, 1729–1754. [CrossRef]
- Del Chiaro, M.; Sugawara, T.; Karam, S.D.; Messersmith, W.A. Advances in the Management of Pancreatic Cancer. BMJ (Clinical research ed.) 2023, 383, e073995. [CrossRef]
- Nikšić, M.; Matz, M.; Valkov, M.; Marcos-Gragera, R.; Stiller, C.; Rosso, S.; Coleman, M.P.; Allemani, C. World-Wide Trends in Net Survival from Pancreatic Cancer by Morphological Sub-Type: An Analysis of 1,258,329 Adults Diagnosed in 58 Countries during 2000-2014 (CONCORD-3). Cancer epidemiology 2022, 80, 102196. [CrossRef]
- Kenney, L.M.; Hughes, M. Surgical Management of Gastroenteropancreatic Neuroendocrine Tumors. Cancers 2025, 17. [CrossRef]
- Benderli Cihan, Y. Are PNETs Radiotherapy Resistant? Turkish journal of surgery 2020, 36, 238–239. [CrossRef]
Figure 1.
Trend change age standardized incidence rates (ASIR) of pancreatic cancer by both sexes and year of diagnosis in the Region of Murcia, Spain (1983-2018). ASIR: Age Standardized Incidence Rates per 100,000 person-years (2013 European Standard Population). *Indicates that Annual Percent Change (APC) is significantly different from zero at the alpha = 0.05 level Final Selected Model: 0 Joinpoints.
Figure 1.
Trend change age standardized incidence rates (ASIR) of pancreatic cancer by both sexes and year of diagnosis in the Region of Murcia, Spain (1983-2018). ASIR: Age Standardized Incidence Rates per 100,000 person-years (2013 European Standard Population). *Indicates that Annual Percent Change (APC) is significantly different from zero at the alpha = 0.05 level Final Selected Model: 0 Joinpoints.
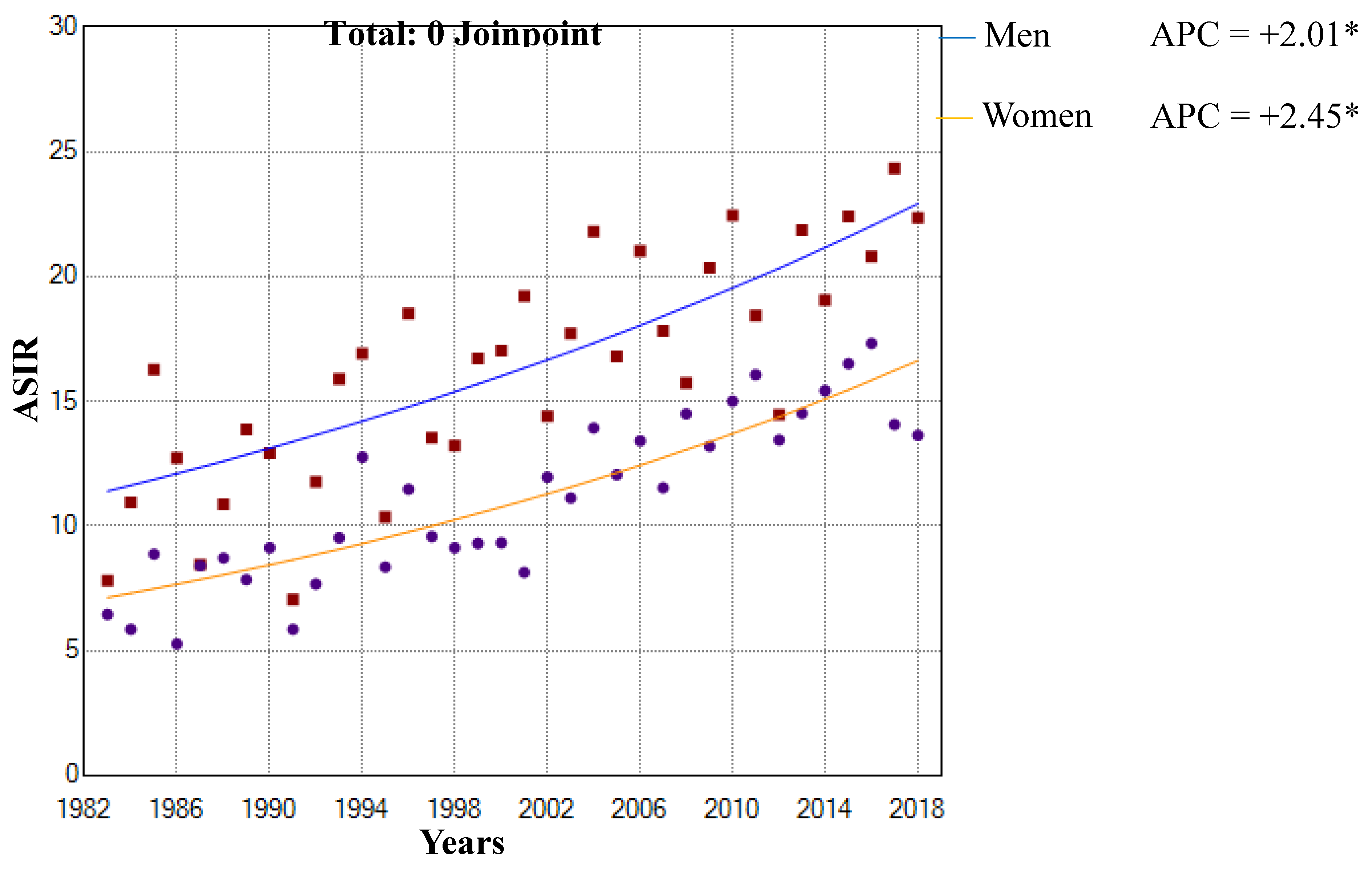
Figure 2.
Trend change age standardized incidence rates (ASIR) of pancreatic cancer by sex and age groups in the Region of Murcia, Spain (1983-2018). ASIR: Age Standardized Incidence Rates per 100,000 person-years (2013 European Standard Population). *Indicates that Annual Percent Change (APC) is significantly different from zero at the alpha = 0.05 level Final Selected Model: 0 Joinpoints.
Figure 2.
Trend change age standardized incidence rates (ASIR) of pancreatic cancer by sex and age groups in the Region of Murcia, Spain (1983-2018). ASIR: Age Standardized Incidence Rates per 100,000 person-years (2013 European Standard Population). *Indicates that Annual Percent Change (APC) is significantly different from zero at the alpha = 0.05 level Final Selected Model: 0 Joinpoints.
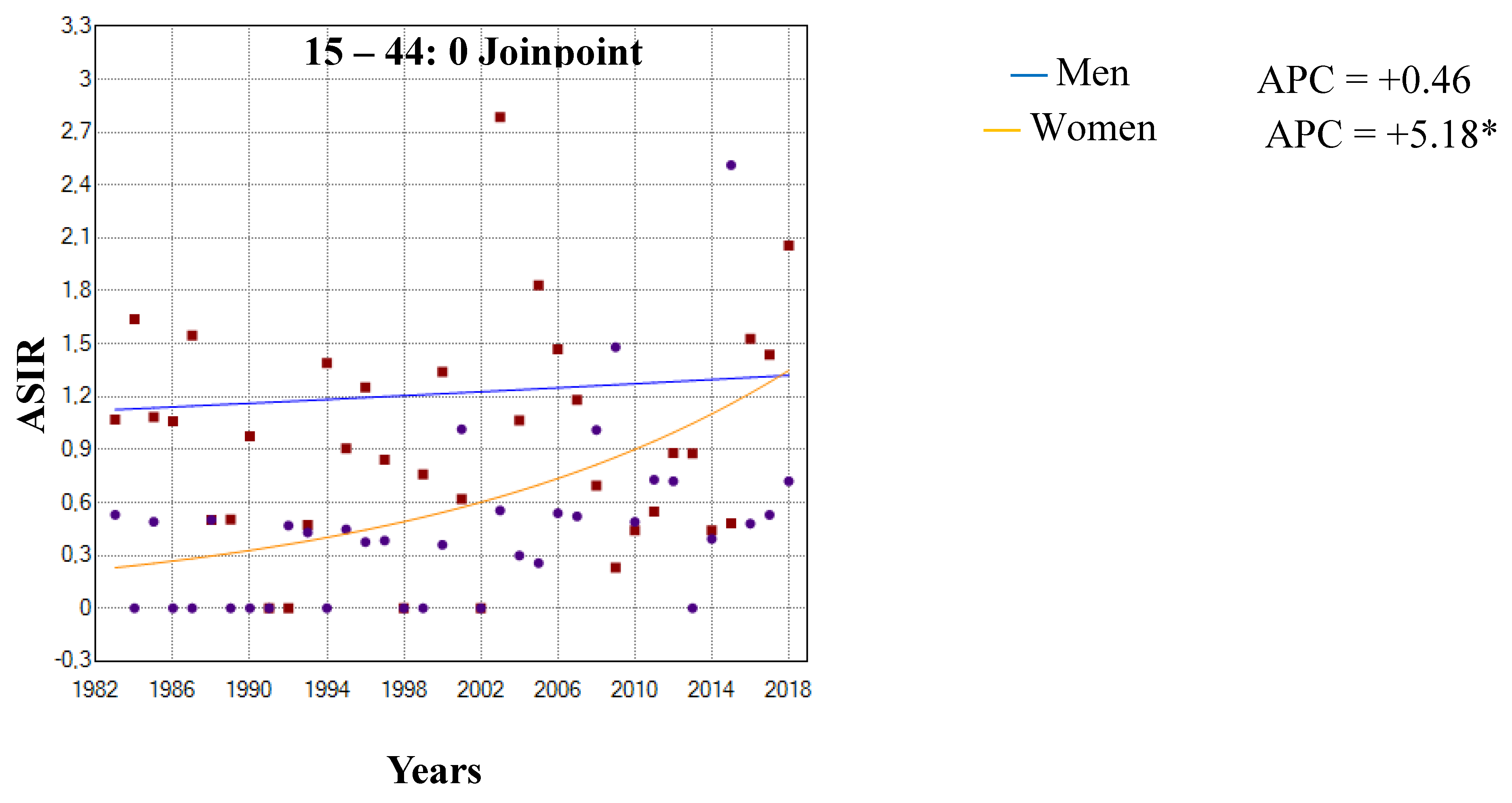
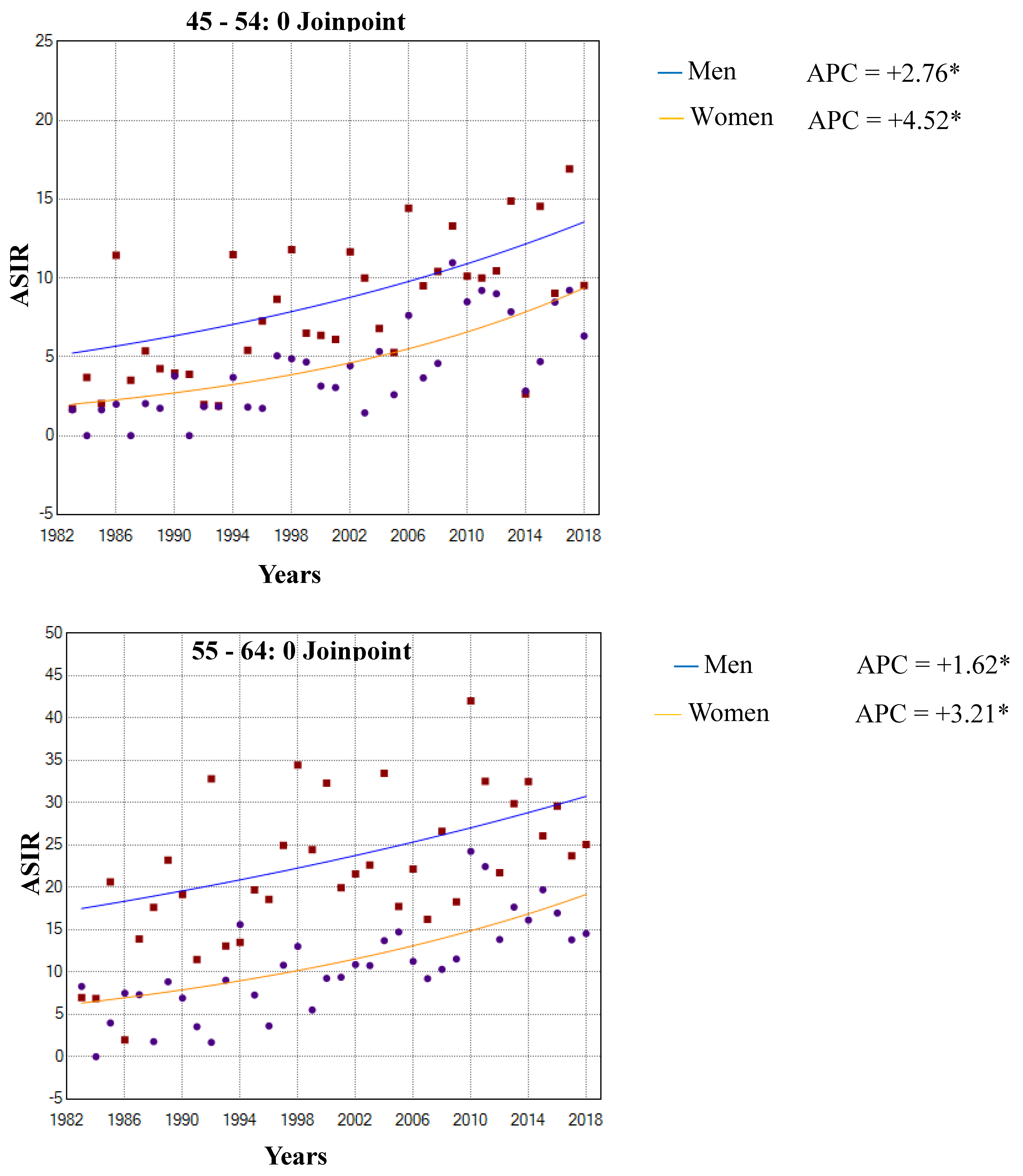
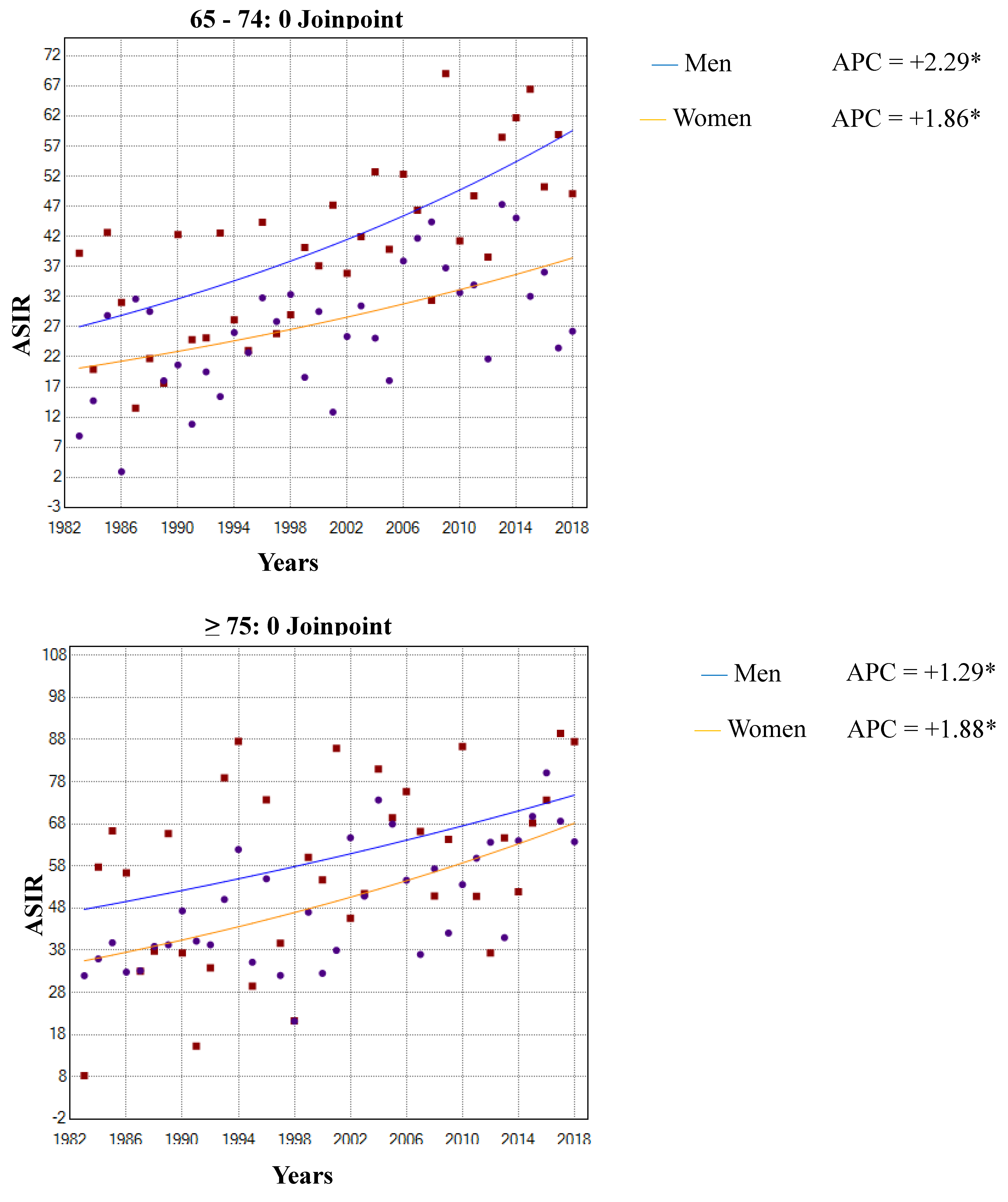
Figure 3.
Trend change age standardized incidence rates (ASIR) of pancreatic cancer by histological groups and year of diagnosis in the Region of Murcia, Spain (1983-2018).
Figure 3.
Trend change age standardized incidence rates (ASIR) of pancreatic cancer by histological groups and year of diagnosis in the Region of Murcia, Spain (1983-2018).
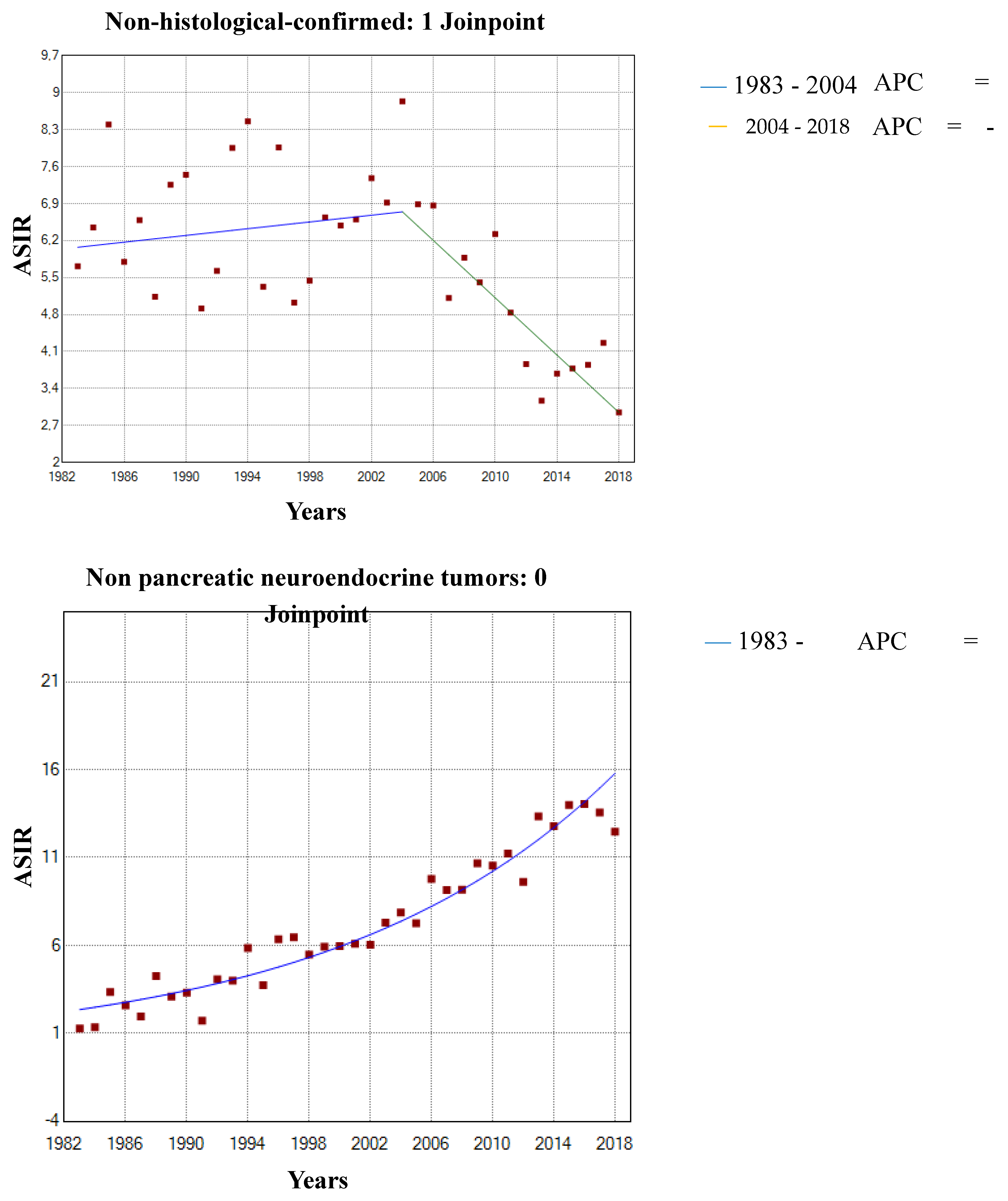
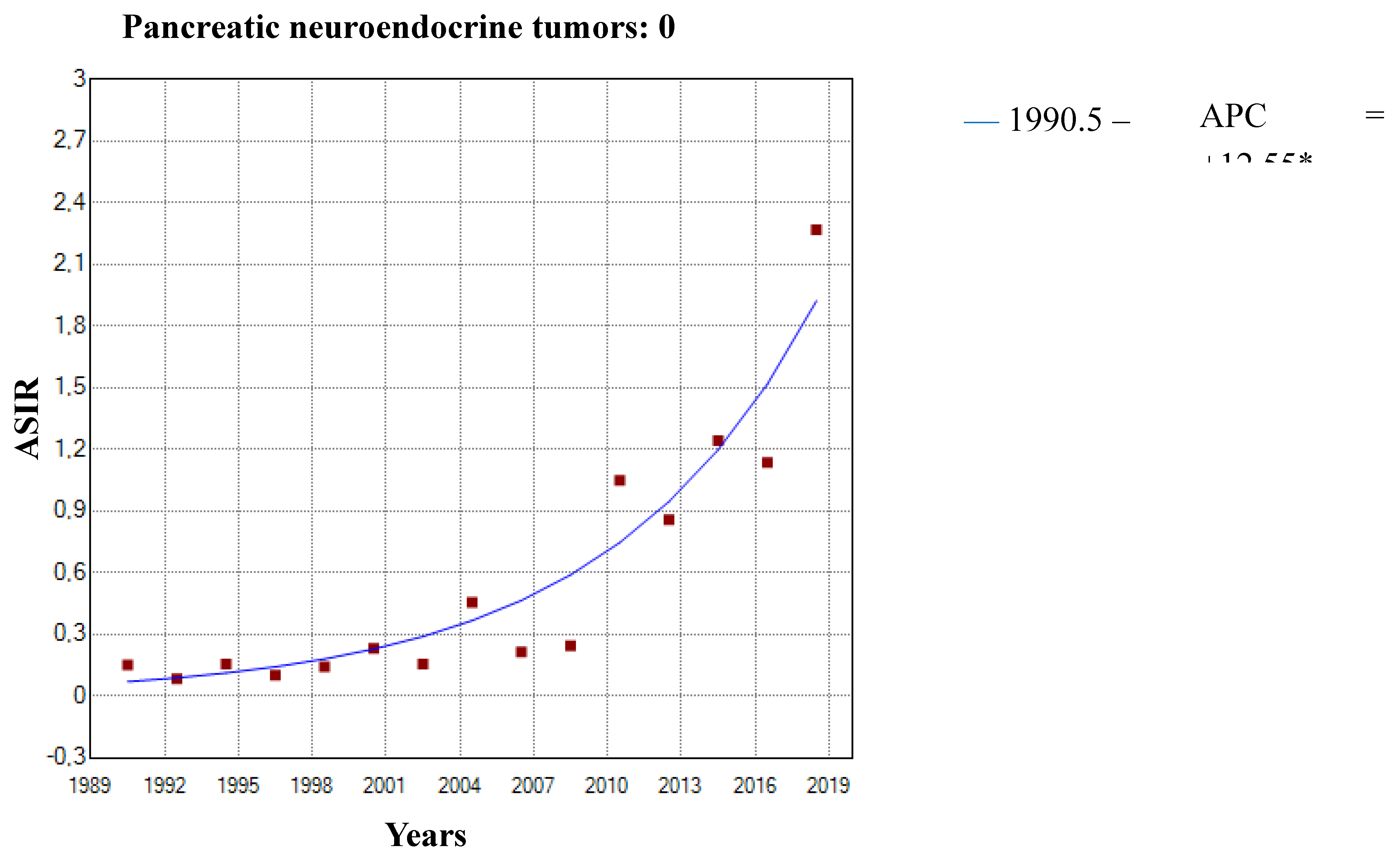

Table 1.
Age standardized incidence rates (ASIR) of pancreatic cancer by sex and period in the Region of Murcia, Spain. (1983-2018). (n= 3,819).
Table 1.
Age standardized incidence rates (ASIR) of pancreatic cancer by sex and period in the Region of Murcia, Spain. (1983-2018). (n= 3,819).
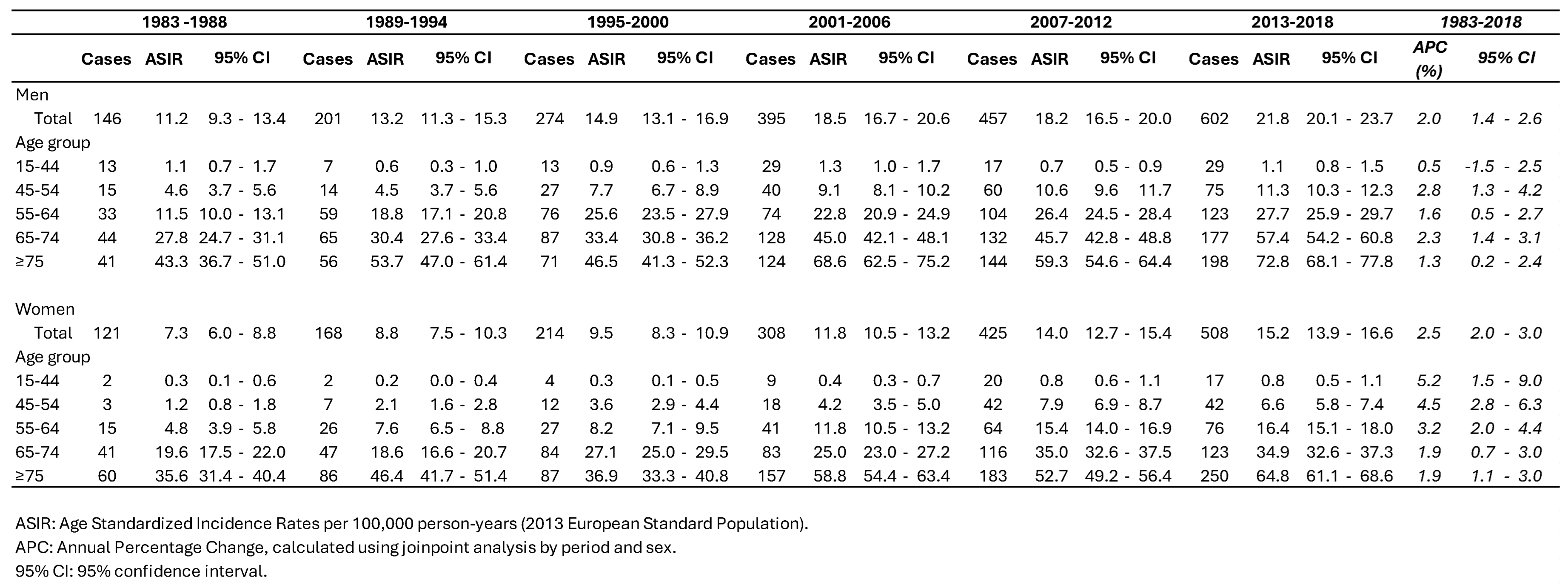
Table 2.
Age standardized incidence rates (ASIR) of pancreatic cancer by sex and age groups according to histological group in the Region of Murcia, Spain. (1983-2018).
Table 2.
Age standardized incidence rates (ASIR) of pancreatic cancer by sex and age groups according to histological group in the Region of Murcia, Spain. (1983-2018).
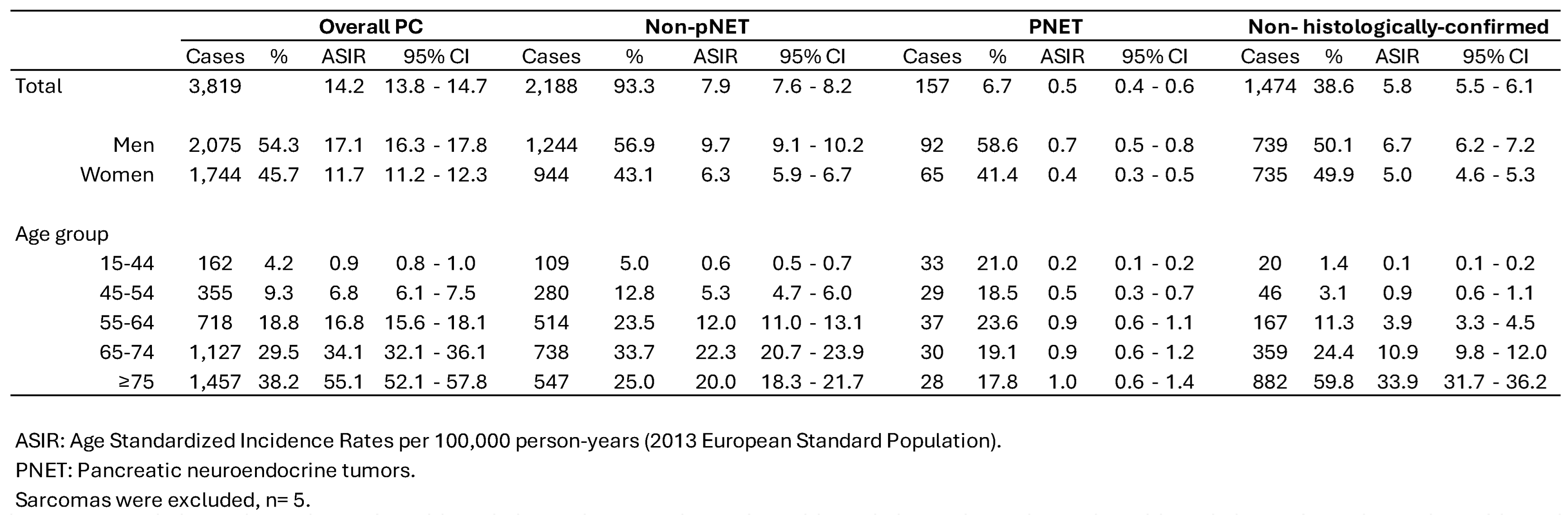
Table 3.
Age standardized net survival at one, three and five years after diagnosis of pancreatic cancer by sex, age groups, period of diagnosis and histological groups in the Region of Murcia, Spain (1990-2018).
Table 3.
Age standardized net survival at one, three and five years after diagnosis of pancreatic cancer by sex, age groups, period of diagnosis and histological groups in the Region of Murcia, Spain (1990-2018).
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



