
Submitted:
11 April 2025
Posted:
14 April 2025
You are already at the latest version
Abstract
Background: Fibromyalgia Syndrome (FMS) is a chronic disorder marked by widespread pain, fatigue, and sleep disturbances. Recent studies suggest that low-grade inflammation and oxidative stress play key roles in FMS pathophysiology. Ultra-processed foods (UPFs), high in inflammatory ingredients, may exacerbate these mechanisms. Objective: This study aims to evaluate the relationship between UPF intake and inflammatory dietary patterns in FMS patients compared to healthy controls. Methods: A cross-sectional case-control study was conducted with 89 participants: 45 FMS patients and 44 healthy controls. The study was approved by the institutional ethics committee of the Complejo Hospitalario Universitario de Canarias (CHUC_2024_27). Data collection took place from January 17, 2025 to April 9, 2025. Dietary intake was assessed using the NOVA classification system for UPF consumption and the Dietary Inflammatory Index (DII) for inflammatory dietary patterns. Symptoms were evaluated using the Visual Analog Scale (VAS) for pain and the Fatigue Severity Scale (FSS). Results: FMS patients consumed significantly more UPFs (34.5%) than controls (26.7%) (p < 0.001). FMS participants also reported higher pain (VAS: 6.8 ± 1.9) and fatigue (FSS: 5.1 ± 1.1) compared to controls (VAS: 1.2 ± 0.5, FSS: 4.8 ± 1.0). Inflammatory dietary patterns were more pronounced in FMS patients, who consumed higher levels of saturated fats (29.4 ± 6.1 g/day vs. 24.8 ± 5.7 g/day; p = 0.02) and lower levels of anti-inflammatory nutrients like magnesium (240.5 ± 36.7 mg/day vs. 278.9 ± 40.2 mg/day;p < 0.001) and vitamin C (58.2 ± 12.9 mg/day vs. 74.6 ± 13.5 mg/day; p < 0.001). Conclusions: The results suggest that higher UPF consumption and a pro-inflammatory dietary pattern are associated with increased pain and fatigue in FMS patients. Reducing UPF intake and improving dietary quality could be beneficial in managing FMS symptoms.
Keywords:
FMS
; ultra-processed foods
; dietary inflammatory index
; chronic pain
; systemic inflammation
; gut microbiota
; NOVA classification
; fatigue
; nutrition
1. Introduction
Fibromyalgia Syndrome (FMS) is a chronic condition characterized by widespread musculoskeletal pain [1,2], persistent fatigue [3], and significant sleep disturbances [4], with an estimated prevalence of 2–4% in the general population [5,6]. As a multifaceted disorder, it impacts patients’ quality of life [7], often limiting daily functioning and contributing to considerable psychological distress [8], including symptoms of anxiety [9] and depression [10]. The condition predominantly affects women, with a female-to-male ratio of approximately 3:1 [11,12], suggesting underlying hormonal and genetic components in its pathophysiology [13].
Although the precise etiology of FMS remains elusive, recent evidence points to a multifactorial origin [14]. Low-grade systemic inflammation [15], oxidative stress [16], and gut microbiota alterations [17,18] have been identified as potential contributors to disease mechanisms. Central sensitization, wherein the nervous system exhibits heightened responsiveness to sensory stimuli, is also considered a key mechanism underlying the chronic pain experienced by FMS patients [19]. Moreover, the imbalance of neurotransmitters such as serotonin, dopamine, and glutamate contributes to the worsening of symptoms, especially those related to pain amplification, fatigue, and cognitive impairment [20,21,22].
Given the growing burden of FMS and its significant public health implications, identifying modifiable risk factors and effective therapeutic strategies remains a pressing priority [23]. With this regard, current pharmacological treatments—including antidepressants, anticonvulsants, and analgesics—typically offer only partial relief and are frequently accompanied by undesirable side effects [24,25]. Consequently, non-pharmacological interventions such as physical activity [26,27], cognitive-behavioral therapy [28], and dietary modification [29] have garnered increasing attention as complementary approaches in the management of FMS. Among these, diet has emerged as a pivotal factor, given its influence on systemic inflammation [30], oxidative balance [31], and the gut microbiome [32]—elements that may collectively shape the course and severity of FMS.
Ultra-processed foods (UPFs), in particular, have attracted scrutiny for their detrimental effects on metabolic, inflammatory, and neurological health [33]. As defined by the NOVA classification, UPFs are industrially manufactured products composed of refined ingredients, chemical additives, and synthetic compounds that may provoke inflammatory responses and disrupt gut microbiota homeostasis [34,35,36]. These products are typically high in added sugars, hydrogenated fats, and artificial preservatives—all linked to increased oxidative stress [37,38] and chronic low-grade inflammation [39], both of which may intensify FMS symptoms. Epidemiological evidence has associated high UPFs consumption with elevated risks of obesity [40], type 2 diabetes [41], and cardiovascular diseases [42], as well as heightened levels of systemic inflammatory markers such as C-reactive protein and interleukin-6 [43,44,45] These pro-inflammatory effects may contribute to FMS pathophysiology via mechanisms involving mitochondrial dysfunction [46], neuroinflammation [47], and altered energy metabolism [48].
Despite growing recognition of the interplay between diet and chronic pain disorders, the specific impact of UPF consumption on individuals with FMS remains insufficiently explored. Preliminary studies suggest that diets rich in minimally processed, anti-inflammatory foods—such as those containing omega-3 fatty acids, polyphenols, and dietary fiber—may alleviate FMS symptoms by modulating inflammatory pathways and promoting gut microbial diversity [49,50,51]. Conversely, excessive intake of UPFs may exacerbate neuroinflammation, heighten pain perception, and impair mitochondrial function—hallmarks of FMS pathology. Additionally, UPFs have been linked to dysbiosis and increased intestinal permeability [52], both of which may foster systemic inflammation and amplify nociceptive responses [53]. Given that many FMS patients report frequent gastrointestinal disturbances, the connection between dietary patterns, gut health, and symptom severity merits deeper investigation.
Given the current lack of robust, large-scale epidemiological research on the role of UPFs in FMS, this case-control study seeks to address a critical gap in the literature. The objective is to examine the association between UPF consumption and the severity of FMS-related symptoms by comparing dietary patterns and clinical profiles between individuals diagnosed with FMS and matched controls without the condition.
2. Methodology
2.1. Study Design
This cross-sectional case-control study was conducted following the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines [54]. A non-probability convenience sampling method was employed to compare UPF consumption between individuals diagnosed with FMS and asymptomatic controls. The study was conducted from January 17, 2025 to April 9, 2025, at the Asociación de Fibromialgia y Fatiga Crónica de Tenerife (Santa Cruz de Tenerife, Spain), following approval from the institutional ethics committee of Complejo Hospitalario Universitario de Canarias, Santa Cruz de Tenerife, Spain (CHUC_2024_27). All participants provided written informed consent, which was obtained by S.M.P. prior to inclusion in the study. Data collection was conducted anonymously, with oversight by I.M.M.P. to ensure compliance with ethical and data protection standards.
2.2. Participants
After signing the informed consent form, participants underwent a medical history review and dietary assessment to determine eligibility based on predefined inclusion and exclusion criteria. The study included (1) adults aged 18 years or older (2) who had been diagnosed with FMS according to the 2016 criteria of the American College of Rheumatology (ACR, 2010) [55]. Eligible participants (3) had no major dietary restrictions that could influence UPF consumption patterns and (4) no severe comorbidities that might affect dietary intake or metabolism. Individuals actively (5) engaged in structured dietary interventions or (6) weight-loss programs were excluded to minimize potential confounding effects.
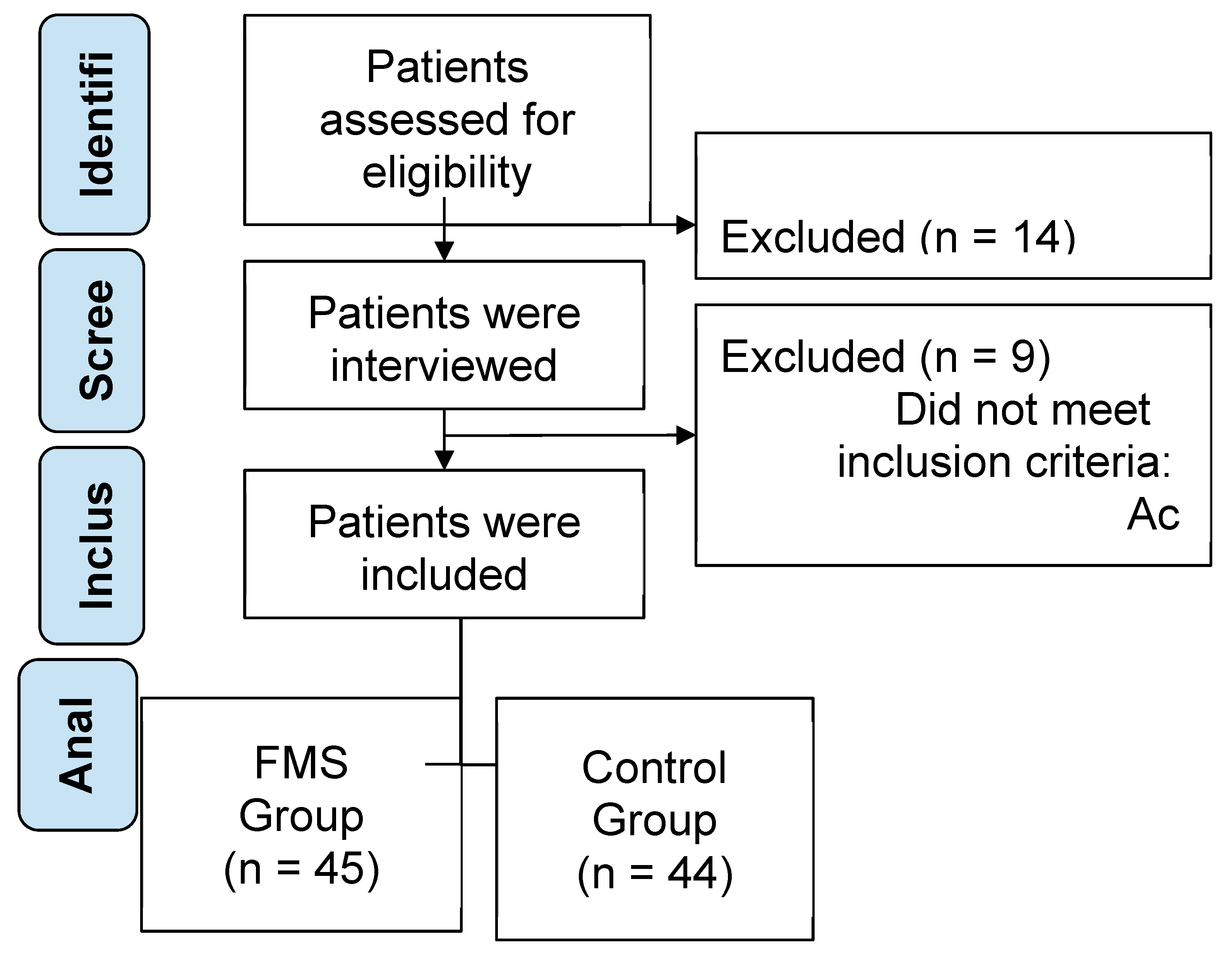
Exclusion criteria included being (1) under 18 years of age, (2) having undiagnosed chronic pain conditions, (3) or presenting with major gastrointestinal disorders such as inflammatory bowel disease or celiac disease, which could impact nutrient absorption and digestion. Participants with (4) severe psychiatric disorders that could interfere with dietary reporting, as well as those taking dietary supplements that significantly altered nutrient intake, were also excluded. Following the initial screening of 112 candidates, 45 were excluded due to lack of informed consent, and 24 were excluded for not meeting the eligibility criteria. The final study sample comprised 89 participants, divided into the case group (FMS patients) and the control group (healthy individuals). See details in Figure 1. Participants selection process.
Figure 1.
STROBE participants selection process.
2.3. Sample Size Calculation
Sample size was calculated using G*Power software (version 3.1.9.7; Düsseldorf University, Germany) [56] based on an expected medium effect size (Cohen’s d = 0.65), derived from preliminary data on dietary intake differences between individuals with FMS and healthy controls. With a significance level of α = 0.05 and power (1 – β) of 0.80 for two-tailed comparisons, a minimum of 84 participants (42 per group) was required to detect statistically significant differences. The final sample included 89 participants (45 with FMS and 44 controls), exceeding the minimum requirement and ensuring adequate power for the analyses conducted.
2.4. Outcomes
2.4.1. Anthropometric and Clinical Measurements
To begin with, anthropometric parameters such as body weight, height, and body mass index (BMI) were measured. BMI was calculated using the standard formula (weight in kilograms divided by the square of height in meters, kg/m²). These data were obtained using calibrated digital scales and wall-mounted stadiometer (Harpedem, Holtain Ltd., Crymych, United Kingdom), following standardized measurement protocols to ensure consistency and reliability across participants. Subsequently, body composition was assessed using bioelectrical impedance analysis (BIA), specifically with the InBody 770 multi-frequency analyzer (InBody Co., Ltd., Seoul, South Korea) [57], a device widely validated for use in clinical populations. This non-invasive method estimates key components of body composition, including fat mass, lean mass, and total body water, by analyzing the resistance and reactance of electrical currents as they pass through body tissues.
In terms of clinical symptom assessment, the Fibromyalgia Impact Questionnaire (FIQ) [58] was employed to evaluate the overall impact of FMS. This validated instrument captures multiple symptom domains, including pain, fatigue, physical functioning, and quality of life, providing a comprehensive measure of disease severity [59]. Additionally, pain intensity was quantified using the Visual Analog Scale (VAS), a sensitive and widely adopted tool in clinical research for measuring subjective pain experience [60]. Moreover, fatigue levels were evaluated using the Fatigue Severity Scale (FSS) [61], which assesses the impact of fatigue on physical, social, and cognitive functioning. The FSS has demonstrated high reliability and validity in both general and clinical populations, including patients with fibromyalgia [62].
2.3.2. Dietary Assessment
UPFs consumption was categorized using the NOVA classification system [35], which stratifies foods into four groups based on their degree of processing. These groups include unprocessed or minimally processed items (e.g., fresh fruits, vegetables, and whole grains), processed culinary ingredients (e.g., oils, salt, and sugar), processed foods (e.g., canned vegetables and cheese), and ultra-processed foods (e.g., sugary beverages, ready-to-eat meals, packaged snacks, and industrially processed bakery products). Participants reported their UPF consumption frequency, and their total UPF intake was expressed as a percentage of their overall energy intake.
In addition, the Dietary Inflammatory Index (DII) [63] was employed as a validated measure to assess the inflammatory potential of the participants’ diets. By examining the intake of specific nutrients and food items, the DII generates a score indicating whether a diet tends toward a pro-inflammatory or anti-inflammatory profile.
2.4. Statistical Analysis
Statistical analyses were conducted using SPSS v.29.0.2.0 (IBM Corp., Armonk, NY, USA) [64]. Dietary intake and clinical data were entered into an electronic database, with a second researcher performing double data entry to ensure accuracy and data integrity. Descriptive statistics—including mean, median, standard deviation, minimum, and maximum values—were calculated for all study variables.
Afterwards, the normality of data distribution was assessed using the W Shapiro–Wilk test with p-values > 0.05 indicating normal distribution. For intergroup comparisons, independent samples t-tests were used for variables with normal distribution, while the Mann–Whitney U test was applied for non-normally distributed variables. Lastly, effect sizes were calculated to assess the magnitude of differences between groups: Cohen’s d was used for parametric analyses, and the biserial correlation coefficient was applied for nonparametric tests. Statistical significance was set at p < 0.05.
3. Results
3.1. Description of Sample
A total of 89 participants were included in the study, with 45 individuals assigned to the FMS group and 44 to the control group. Specifically, the FMS group consisted of 33 women and 12 men, with a mean age of 50.1 ± 8.5 years, whereas the control group included 30 women and 14 men, with a mean age of 48.7 ± 9.1 years. Notably, age was normally distributed in both groups, as confirmed by the Shapiro–Wilk test (FMS: W = 0.973, p = 0.293; Control: W = 0.976, p = 0.348).
In relation to the anthropometric characteristics, participants in the FMS group exhibited higher body weight (72.5 ± 10.3 kg) and BMI (27.5 ± 4.2 kg/m²) compared to those in the control group (68.9 ± 9.7 kg and 24.9 ± 3.8 kg/m², respectively). It is worth noting that BMI did not follow a normal distribution in either group (FMS: W = 0.945, p = 0.014; Control: W = 0.951, p = 0.018), while body weight was marginally non-normal. In contrast, height was similar between groups (FMS: 1.62 ± 0.08 m; Control: 1.63 ± 0.07 m), and the distribution was normal in both cases.
In addition, the waist-to-hip ratio (WHR) was slightly higher in the FMS group (0.89 ± 0.05) than in the control group (0.85 ± 0.04). Despite this difference, WHR followed a normal distribution in both groups (FMS: W = 0.970, p = 0.182; Control: W = 0.975, p = 0.225). Regarding body composition, the analysis revealed significantly higher fat mass in the FMS group (34.5 ± 5.3%) compared to controls (28.1 ± 4.7%). Conversely, fat-free mass (FMS: 65.5 ± 5.3% ; Control: 71.9 ± 4.7%) and muscle mass (FMS: 47.5 ± 4.8% ; Control: 49.3 ± 4.2%) were lower in the FMS group. Importantly, all body composition variables demonstrated non-normal distributions in both groups (p < 0.05).
Furthermore, participants in the FMS group reported significantly greater pain intensity, as measured by the Visual Analog Scale (VAS: 6.8 ± 1.9), in contrast to the control group (1.2 ± 0.5). Similarly, fatigue symptoms—assessed using the Fatigue Severity Scale (FSS)—were markedly elevated in the FMS group across all subdomains, including daily interference, task initiation, motivation, post-effort fatigue, and social engagement. All clinical variables exhibited highly significant deviations from normality (p < 0.001 in all cases). The anthropometric and clinical characteristics of the FMS and control groups are presented in Table 1.

Table 1.
Anthropometric and clinical characteristics of FMS and control groups.
| Characteristics | FMS Group (n = 45) |
W | p-value | Control Group (n = 44) |
W | p-value |
|---|---|---|---|---|---|---|
| Gender (Female/Male) | 33/12 | 30/14 | ||||
| Age (years) | 50.1 ± 8.5 | 0.973 | 0.293 | 48.7 ± 9.1 | 0.976 | 0.348 |
| Weight (Kg) | 72.5 ± 10.3 | 0.958 | 0.057 | 68.9 ± 9.7 | 0.963 | 0.064 |
| Height (m) | 1.62 ± 0.08 | 0.979 | 0.481 | 1.63 ± 0.07 | 0.981 | 0.507 |
| BMI (Kg/m2) | 27.5 ± 4.2 | 0.945 | 0.014* | 24.9 ± 3.8 | 0.951 | 0.018* |
| WHR | 0.89 ± 0.05 | 0.970 | 0.182 | 0.85 ± 0.04 | 0.975 | 0.225 |
| BIA (%) | ||||||
| Fat mass (%) | 34.5 ± 5.3 | 0.942 | 0.011* | 28.1 ± 4.7 | 0.946 | 0.015* |
| Fat-free mass (%) | 65.5 ± 5.3 | 0.940 | 0.02* | 71.9 ± 4.7 | 0.911 | 0.021* |
| Muscle mass (%) | 47.5 ± 4.8 | 0.943 | 0.019* | 49.3 ± 4.2 | 0.905 | 0.020* |
| VAS - Visual Analog Scale | ||||||
| Pain intensity (0-10 scale) | 6.8 ± 1.9 | 0.882 | <0.001*** | 1.2 ± 0.5 | 0.911 | <0.001*** |
| FSS - Fatigue Severity Scale | ||||||
| Total score | 5.1 ± 1.1 | 0.894 | <0.001*** | 4.8 ± 1.0 | 0.905 | <0.001*** |
| Daily Interference | 6.1 ± 1.2 | 0.890 | <0.001*** | 2.3 ± 0.8 | 0.907 | <0.001*** |
| Task Initiation | 5.8 ± 1.4 | 0.888 | <0.001*** | 2.0 ± 0.7 | 0.904 | <0.001*** |
| Motivation | 5.7 ± 1.3 | 0.891 | <0.001*** | 2.2 ± 0.9 | 0.902 | <0.001*** |
| Post-effort Fatigue | 6.0 ± 1.5 | 0.889 | <0.001*** | 1.9 ± 0.6 | 0.903 | <0.001*** |
| Social Engagement | 6.0 ± 1.5 | 0.886 | <0.001*** | 1.9 ± 0.6 | 0.904 | <0.001*** |
Table 1.Anthropometric and clinical characteristics of FMS and control groups. Abbreviation: BMI: Body Mass Index; WHR: Waist-to-Hip Ratio; BIA: Bioelectrical Impedance Analysis; VAS: Visual Analog Scale for pain intensity (0 = no pain, 10 = worst pain imaginable); FSS: Fatigue Severity Scale. *p < 0.05; **p < 0.01; ***p < 0.001 indicates statistically significant differences between groups. Several variables showed a non-normal distribution, as determined by the Shapiro–Wilk test.
3.2. Inflammatory Dietary Intake and Ultra-processed Food Consumption
3.2.1. Ultra-processed Food Consumption (NOVA Classification)
According to the NOVA classification system [35], the FMS group consumed significantly fewer unprocessed or minimally processed foods (35.1 ± 9.2%) than the control group (45.3 ± 8.7%; p < 0.001). Likewise, processed culinary ingredient consumption was slightly lower in the FMS group (14.3 ± 5.6%) than in controls (16.7 ± 4.9%; p = 0.04). In contrast, the intake of processed foods (16.1 ± 5.3%) was higher in the FMS group compared to controls (11.3 ± 4.6%; p < 0.01). Notably, UPF consumption was significantly elevated in the FMS group (34.5 ± 8.9%) relative to the control group (26.7 ± 7.1%; p < 0.001), underscoring the potential role of industrial food products in modulating symptomatology in FMS.
3.3.2. Inflammatory Dietary Intake (DII/E-DII)
- Pro-inflammatory components
After the application of DII/E-DII [63] participants with FMS exhibited significantly higher intake of pro-inflammatory dietary components compared to controls (45.3 ± 8.7% vs. 35.1 ± 9.2%, p < 0.001), with a large effect size (d = 1.14). This suggests a more pro-inflammatory dietary pattern in the FMS group. Regarding macronutrient intake, individuals in the FMS group consumed significantly more saturated fats (29.4 ± 6.1 g/day) than controls (24.8 ± 5.7 g/day), with a large effect size (d = 0.97, p = 0.02). Conversely, the intake of trans fats was lower in the FMS group (3.2 ± 1.0 g/day) compared to controls (4.1 ± 1.1 g/day), although the effect size was small (d = –0.48, p = 0.045).
Cholesterol intake was also higher among participants with FMS (210.5 ± 35.4 mg/day) compared to controls (187.6 ± 30.7 mg/day), with a small effect size (d = 0.42, p= 0.04). Additionally, refined carbohydrate intake was greater in the FMS group (220.4 ± 35.2 g/day vs. 198.7 ± 32.4 g/day; p = 0.01), corresponding to a medium effect size (d = 0.64). Interestingly, sodium intake was significantly lower in the FMS group (1850.0 ± 320.0 mg/day) than in the control group (2040.0 ± 340.0 mg/day; p = 0.039), with a medium effect size (d = –0.56).
- Anti-inflammatory components
- 1.
- Macronutrient Intake
The FMS group showed a significantly lower protein intake (68.4 ± 12.7 g/day) compared to the control group (74.3 ± 11.8 g/day; p = 0.04). Although fat consumption was slightly higher in the FMS group (82.6 ± 15.1 g/day) than in controls (76.5 ± 13.9 g/day), the difference was not statistically significant (p = 0.09). Notably, carbohydrate intake was significantly elevated in the FMS group (220.4 ± 35.2 g/day) versus the control group (198.7 ± 32.4 g/day; p = 0.03). Fiber intake tended to be lower in the FMS group (18.6 ± 4.5 g/day) compared to controls (21.3 ± 5.2 g/day; p = 0.05), which may contribute to altered gut microbiota and inflammatory response.
- 2.
- Micronutrient Intake
Significant group differences were also found in micronutrient intake. Vitamin C consumption was markedly lower in the FMS group (58.2 ± 12.9 g/day) compared to the control group (74.6 ± 13.5 g/day; p < 0.001), with a large effect size (Cohen’s d = -1.24). Similarly, magnesium intake was significantly reduced among individuals with FMS (240.5 ± 36.7 g/day) in comparison to controls (278.9 ± 40.2 g/day; p < 0.001; d = -1.00). Iron intake was also lower in the FMS group (10.3 ± 2.1 g/day) versus the control group (11.2 ± 2.3 g/day; p = 0.021). Although zinc intake showed a similar trend—being lower in the FMS group (8.1 ± 1.6 g/day) than in controls (9.4 ± 1.7 g/day)—this difference did not reach statistical significance (p = 0.234).
- 3.
- Bioactive Compounds
In terms of bioactive compounds, significant differences were observed between groups. Alcohol consumption was lower in the FMS group (2.4 ± 1.1 g/day) compared to the control group (3.7 ± 1.4 g/day; p = 0.01). Similarly, caffeine intake was reduced in individuals with FMS (182.3 ± 45.2 mg/day) relative to controls (219.7 ± 52.8 mg/day; p = 0.03). Notably, the intake of flavonoids and polyphenols was significantly lower in the FMS group (185.2 ± 38.6 mg/day) than in the control group (229.4 ± 41.3 mg/day; p = 0.009), which suggests a diminished dietary exposure to these anti-inflammatory phytochemicals.
- 4.
- Food-Based Items
In the analysis of specific food-based components, garlic intake was slightly lower in the FMS group (1.6 ± 0.7 g/day) compared to controls (2.1 ± 0.9 g/day; p = 0.05). Interestingly, curcumin intake was significantly higher in the FMS group (5.8 ± 2.3 g/day vs. 4.1 ± 1.9 g/day; p = 0.03), which may reflect a higher prevalence of supplement use or dietary adjustments in response to chronic pain symptoms. Piperine intake was also higher in the FMS group (1.3 ± 0.6 g/day vs. 0.9 ± 0.5 g/day; p = 0.06), though the difference did not reach statistical significance. A detailed comparison of UPFs consumption and pro-inflammatory dietary intake between individuals diagnosed with FMS and healthy controls is provided in Table 2.
Table 2.
Difference in dietary intake and UPF consumption in FMS and control groups.
| Characteristics | FMS Group |
Control Group |
Statistic | p-value | Size effect |
|---|---|---|---|---|---|
| NOVA - Ultra-Processed Food Classification System | |||||
| Unprocessed/minimally processed foods | 35.1 ± 9.2% | 45.3 ± 8.7% | 264.0 | <0.001*** | -1.14 |
| Processed culinary ingredients | 14.3 ± 5.6% | 16.7 ± 4.9% | 272.0 | 0.04* | -0.46 |
| Processed foods | 16.1 ± 5.3% | 11.3 ± 4.6% | 675.0 | <0.01** | 0.97 |
| Ultra-processed foods | 34.5 ± 8.9 % | 26.7 ± 7.1 % | 695.0 | <0.001*** | 0.97 |
| DII/E-DII-Dietary Inflammatory Index | |||||
| Energy-adjusted score | 14.3 ± 5.6 | 16.7 ± 4.9 | 348.0 | 0.013* | -0.46 |
| Pro-inflammatory components (%) | 45.3 ± 8.7 | 35.1 ± 9.2 | 162.0 | <0.001*** | 1.14 |
| Macronutrients (g/day) | |||||
| Saturated Fats | 29.4 ± 6.1 | 24.8 ± 5.7 | 530.0 | 0.02* | 0.97 |
| Trans Fats | 4.1 ± 1.1 | 3.2 ± 1.0 | 488.0 | 0.045* | -0.48 |
| Cholesterol (mg/day) | 210.5 ± 35.4 | 187.6 ± 30.7 | 606.0 | 0.04* | 0.42 |
| Refined carbohydrates / sugar | 220.4 ± 35.2 | 198.7 ± 32.4 | 777.0 | 0.01* | 0.64 |
| Sodium | 1850.0 ± 320.0 | 2040.0 ± 340.0 | 502.0 | 0.039* | -0.56 |
| Anti-inflammatory components (%) | 16.1 ± 5.3 | 11.3± 4.6 | 595.0 | 0.03* | 0.97 |
| Macronutrients (g/day) | |||||
| Proteins | 68.4 ± 12.7 | 74.3 ± 11.8 | 316.0 | 0.048* | -0.48 |
| Fats | 82.6 ± 15.1 | 76.5 ± 13.9 | 487.0 | 0.058 | 0.42 |
| Carbohydrates | 220.4 ± 35.2 | 198.7 ± 32.4 | 777.0 | 0.01* | 0.64 |
| Fibers | 18.6 ± 4.5 | 21.3 ± 5.2 | 357.0 | 0.17 | -0.56 |
| Micronutrients (g/day) | |||||
| Vitamine C | 58.2 ± 12.9 | 74.6 ± 13.5 | 186.0 | <0.001*** | -1.24 |
| Magnesium | 240.5 ± 36.7 | 278.9 ± 40.2 | 223.0 | <0.001*** | -1.0 |
| Iron | 10.3 ± 2.1 | 11.2 ± 2.3 | 294.0 | 0.021* | -0.41 |
| Zinc | 8.1 ± 1.6 | 9.4 ± 1.7 | 369.0 | 0.234* | -0.79 |
| Bioactive compounds (g/day) | |||||
| Alcohol | 2.4 ± 1.1 | 3.7 ± 1.4 | 198.0 | 0.01* | -1.03 |
| Caffeine (mg/day) | 182.3 ± 45.2 | 219.7 ± 52.8 | 216.0 | 0.03* | -0.76 |
| Flavonoids / Polyphenols | 185.2 ± 38.6 | 229.4 ± 41.3 | 204.0 | 0.009** | -1.08 |
| Food-based items (g/day) | |||||
| Turmeric | 5.8 ± 2.3 | 4.1 ± 1.9 | 574.0 | 0.03* | 0.81 |
| Garlic and onion | 1.6 ± 0.7 | 2.1 ± 0.9 | 220.0 | 0.05 | -0.62 |
| Ginger | 1.6 ± 0.7 | 2.1 ± 0.9 | 220.0 | 0.05 | -0.62 |
| Piperine | 1.3 ± 0.6 | 0.9 ± 0.5 | 574.0 | 0.06 | 0.72 |
Table 2.Difference in dietary intake and UPF consumption in FMS and control groups. Data are presented as mean ± SD. p-values were obtained using Mann-Whitney U tests (p < 0.05 considered significant). ***p < 0.001 indicates highly significant differences between groups. Abbreviations: FMS: FMS Syndrome; CTRL: Control; VAS: Visual Analog Scale; FSS: Fatigue Severity Scale; FFQ: Food Frequency Questionnaire; NOVA: Ultra-Processed Food Classification System; SD: Standard Deviation.
4. Discussion
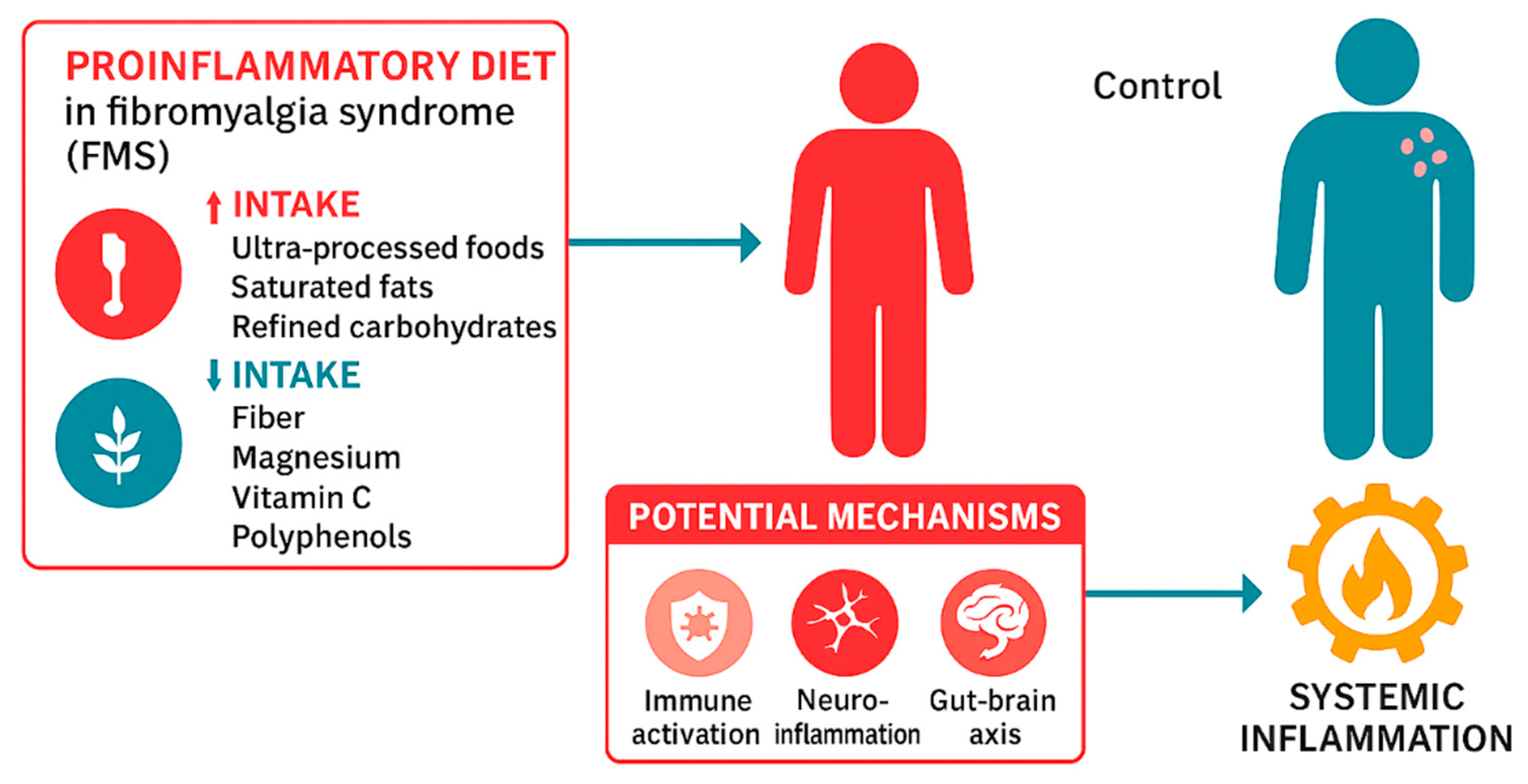
The consumption of UPFs has been linked to various chronic diseases [65], including FMS [66], and may worsen symptoms like fatigue, pain, and inflammation in individuals with FMS through immune activation, neuroinflammation, and the gut-brain axis, potentially leading to systemic inflammation [29,67]. The potential mechanisms through which UPFs may influence the pathophysiology of FMS are illustrated in Figure 2.
Figure 2.
Summary of differences in dietary patterns between individuals with FMS and healthy controls. Compared to controls, participants with FMS showed higher intake of ultra-processed foods, saturated fats, and refined carbohydrates, along with lower consumption of anti-inflammatory nutrients such as vitamin C, magnesium, polyphenols, and fiber. These dietary characteristics may contribute to systemic inflammation, oxidative stress, and central sensitization, which are key mechanisms in the pathophysiology of chronic pain in FMS.
Figure 2.
Summary of differences in dietary patterns between individuals with FMS and healthy controls. Compared to controls, participants with FMS showed higher intake of ultra-processed foods, saturated fats, and refined carbohydrates, along with lower consumption of anti-inflammatory nutrients such as vitamin C, magnesium, polyphenols, and fiber. These dietary characteristics may contribute to systemic inflammation, oxidative stress, and central sensitization, which are key mechanisms in the pathophysiology of chronic pain in FMS.
In our study, participants with FMS reported significantly higher UPF consumption than healthy controls. This dietary pattern may worsen overall well-being by increasing systemic inflammation and oxidative stress, thereby exacerbating fatigue and pain which have been identified higher than controls [48]. Furthermore, most individuals with FMS presented with overweight status (BMI = 27.5 ± 4.2), a known risk factor for the development and progression of FMS. These participants also reported moderate pain intensity (VAS = 6.8 ± 1.9) and clinically significant fatigue that interfered with daily activities (FSS = 6.1 ± 1.2). Given the centrality of fatigue in FMS and its established link to chronic inflammation and impaired energy metabolism, these findings highlight the need to explore diet as a modifiable risk factor [68].
The first tool employed in our study was the NOVA classification [35], which categorizes foods into four groups based on processing levels: unprocessed, processed culinary ingredients, processed foods, and ultra-processed foods. Our results showed that participants with FMS consumed fewer unprocessed foods (35.1 ± 9.2%) compared to the control group (45.3 ± 8.7%; p < 0.001), and fewer culinary ingredients (14.3 ± 5.6% vs. 16.7 ± 4.9%; p = 0.04). Conversely, their intake of processed foods was slightly higher (16.1 ± 5.3% vs. 11.3 ± 4.6%; p < 0.01), and UPF intake was markedly elevated (34.5 ± 8.9% vs. 26.7 ± 7.1%; p < 0.001).
UPFs are characterized by poor nutritional quality and are rich in trans fats, refined sugars, highly processed flours, artificial additives, and preservatives [69,70]. These components trigger inflammatory responses through several mechanisms, including NLRP3 inflammasome activation, oxidative stress, and intestinal dysbiosis, all contributing to a persistent proinflammatory state [39,71]. In contrast, a diet based on fresh and minimally processed foods—rich in antioxidants, fiber, polyunsaturated fatty acids, and essential micronutrients—has shown beneficial effects on inflammatory mechanisms and may improve pain, function, and quality of life in individuals with FMS [72].
A second tool used in this study was the DII, which highlighted a dietary pattern rich in proinflammatory nutrients in the FMS group [63]. Among these, cholesterol intake was notably high (210.5 ± 35.4 mg/day), although its role in FMS remains controversial. Some studies suggest a positive association between high cholesterol and fatigue, potentially due to overweight and dyslipidemia-related mitochondrial dysfunction [73]. However, others report no significant correlation between lipid profiles and symptom severity [74], emphasizing the need to consider confounding factors such as familial hypercholesterolemia.
Trans fat intake was also elevated among FMS participants (4.1 ± 1.1 g/day). These fats, mainly produced during industrial food processing, are associated with low-grade inflammation, as evidenced by elevated systemic inflammatory response markers such as hs-CRP, IL-6, and TNF-α [39,75]. Experimental models further support this association; diets rich in fats increase pain sensitivity in animal models of FMS and raise TNF-α levels in plasma, muscle, and dorsal root ganglia [76]. Refined carbohydrate intake was also significantly higher in the FMS group (220.4 ± 35.2 g/day). These nutrients are linked to inflammation and fatigue and have shown a negative correlation with quality of life scores in patients with FMS, as measured by the FIQ [77]. While findings regarding sugar intake are contradictory, the high glycemic index and glycemic load of these carbohydrates contribute to insulin resistance and systemic inflammation [78].
UPFs are also known to increase intestinal permeability [34,53,79]. Studies, such as one conducted in France with 862 adults, have identified associations between UPF intake and biomarkers of intestinal barrier dysfunction [80]. However, these associations were not observed in the PREDIMED-PLUS study, possibly due to lower UPF consumption in the Spanish elderly population [39].
Another critical issue is the nutritional deficiency of anti-inflammatory micronutrients in UPF-based diets. FMS participants showed inadequate intake of magnesium (240.5 ± 36.7 mg/day), vitamin C, vitamin D, zinc, and niacin. Magnesium deficiency is particularly relevant, as it has been linked to increased systemic inflammation, higher levels of substance P and proinflammatory cytokines, poor sleep quality, insulin resistance, and reduced exercise tolerance [81,82,83].
Magnesium also inhibits NMDA receptor activation in the spinal cord, a key mechanism involved in ascending pain transmission and central sensitization [84]. Its intravenous administration has shown analgesic effects, and estrogen decline after menopause may exacerbate this deficiency [85,86]. Low magnesium levels have been associated with decreased muscle strength and respiratory endurance in FMS patients, alongside greater symptom intensity and impaired ATP production [82,87]. These observations underscore the need to consider micronutrient profiles in FMS dietary interventions.
Our data show higher turmeric consumption among FMS participants (5.8 ± 2.3 g/day) compared to controls (4.1 ± 1.7 g/day). Curcumin, the main active compound in turmeric, has well-documented anti-inflammatory and antioxidant effects via modulation of NF-κB, STAT3, Nrf2, COX-2, and TRPV1 pathways. In preclinical models, curcumin reduced visceral hyperalgesia, TRPV1 receptor expression, oxidative stress, and excitatory neurotransmitter levels (e.g., substance P), with effects comparable to those of gabapentinoids [88,89]. These results suggest that while patients may attempt to self-modulate symptoms through functional foods, the potential benefits of compounds like curcumin might be diminished in the context of an overall proinflammatory diet.
Moreover, we found that patients with FMS have a significantly lower intake of flavonoids compared to healthy individuals (185.2 mg/day vs. 229 mg/day; p = 0.009), which may contribute to increased oxidative stress, inflammation, and pain sensitivity, characteristics commonly associated with this condition. It is well established that flavonoids exert their beneficial effects mainly through their antioxidant properties. They act as antioxidants by capturing free radicals through hydrogen donation (protons and electrons), helping to neutralize these harmful compounds [90]. Additionally, their antioxidant activity is due to the presence of the catechol group in ring B. Indirectly, flavonoids can also act as chelators of transition metal ions, such as iron (Fe) and copper (Cu), binding to them and reducing their ability to generate free radicals [91]. Furthermore, they can influence low-density lipoproteins (LDL), decreasing the consumption of antioxidants such as vitamin E and carotenoids, while regenerating oxidized vitamin E in LDL particles [92].
Flavonoids have been shown to possess anti-inflammatory and analgesic properties, modulating molecular pathways such as opioid receptor inhibition, ion channel regulation, and suppression of MAPK and NF-κB pathways, all of which help reduce inflammation and pain [93]. Several flavonoids target key pathways, inhibiting pro-inflammatory cytokines and enzymes, enhancing their pain-relieving effects. They also affect enzyme systems involved in inflammation, particularly tyrosine and serine-threonine protein kinases [94] helping to attenuate chronic inflammation, a hallmark of conditions like FMS.
An effective nutritional intervention for patients with FMS should focus on reducing the consumption of UPFs and increasing the intake of anti-inflammatory nutrients, as this may help attenuate neuroinflammation and central sensitization. However, socioeconomic factors must be taken into account, as individuals from lower-income backgrounds often rely more heavily on UPFs due to economic constraints and the reduced physical and time demands associated with preparing fresh meals [95].
Therefore, any dietary recommendation should not only be evidence-based, but also accessible, affordable, and socially adapted to the realities of FMS patients. Moreover, intergroup differences in UPF consumption may be influenced by socioeconomic status (SES), as highlighted in the cited study, which did not control for these potential confounding factors. It is well established that lower SES is associated with higher UPF consumption, which may affect the observed outcomes and complicate the interpretation of group differences.
4.1. Limitations
This study presents several limitations that should be considered when interpreting its findings. First, the cross-sectional design precludes the ability to infer causality between UPF consumption, pro-inflammatory dietary patterns, and symptom severity in individuals with fibromyalgia (FMS). To establish temporal or causal relationships, longitudinal and interventional studies are warranted.
Second, the use of a non-probability convenience sampling method may have introduced selection bias, potentially limiting the external validity of the findings. Participants were recruited from a single patient association, which may result in a sample with specific sociodemographic characteristics and health-seeking behaviors that do not reflect the general population of individuals with FMS.
Third, dietary intake was assessed via self-reported food frequency questionnaires (FFQs), a method prone to recall bias, underreporting, and social desirability bias. These biases may be especially pronounced in populations experiencing cognitive fatigue or chronic pain, such as individuals with FMS. Although validated tools like the DII/E-DII and the NOVA classification system were used, potential misclassification of food items or inaccuracies in portion size estimation may affect the reliability of dietary assessments.
To gain a more precise understanding of the factors that influence UPF consumption, future studies should conduct subgroup analyses considering variables such as sex, comorbidities (e.g., gastrointestinal disorders affecting digestion, absorption, synthesis, or elimination), clinical health status (e.g., confirmation of participants as generally healthy or diagnosed), medication use, smoking status, and specific nutrient intakes. Although the sample size was adequate according to power analysis, such subgroup analyses may have been underpowered to detect small to moderate effects. Therefore, subsequent research should utilize larger, more diverse, and representative cohorts to strengthen the validity and generalizability of findings, and to better understand how socioeconomic and health-related factors influence UPF consumption patterns in this population.
4.2. Recommendations of Clinical practice
Given the well-established associations between ultra-processed food (UPF) consumption, pro-inflammatory dietary components, and increased symptom severity in fibromyalgia (FMS), dietary intervention should be recognized as a key complementary strategy within its clinical management. Healthcare providers and dietitians are strongly encouraged to work collaboratively, using validated instruments—such as the NOVA food classification system and the Dietary Inflammatory Index (DII)—to conduct personalized dietary assessments that can effectively identify and quantify pro-inflammatory dietary patterns.
Patients should be systematically educated on the detrimental effects of UPF consumption and the protective benefits of a diet rich in whole, minimally processed foods—especially those high in antioxidants, dietary fiber, and essential micronutrients. A gradual shift toward an anti-inflammatory dietary profile should be promoted, emphasizing increased intake of unprocessed foods while reducing the consumption of trans fats, refined carbohydrates, and added sugars.
Special attention must be given to identifying and addressing potential micronutrient deficiencies—particularly magnesium, vitamin C, and iron—through targeted supplementation and individualized nutritional counseling. To ensure long-term adherence and optimize clinical outcomes, dietary modifications should be regularly monitored, with ongoing nutritional follow-up integrated into a multidisciplinary care framework.
Incorporating anti-inflammatory nutritional strategies into standard clinical practice holds considerable promise for reducing systemic inflammation, modulating central sensitization, and ultimately improving the quality of life in individuals with FMS. These insights reinforce the urgent need for well-designed clinical trials to rigorously evaluate the efficacy of dietary interventions in managing FMS-related symptoms.
Furthermore, recent evidence supports the value of adopting an integrative therapeutic approach to fibromyalgia—combining pharmacological treatments with complementary strategies such as nutraceuticals (including polyphenols), balanced nutrition, appropriate supplementation, weight management, regular physical activity, and specialized physiotherapy. Together, these interventions may offer a synergistic effect, addressing both the biological and lifestyle dimensions of this complex condition.
5. Conclusions
This case-control study demonstrates that adults with FMS exhibit a more proinflammatory dietary profile compared to healthy controls, characterized by greater consumption of ultra-processed foods and reduced intake of anti-inflammatory nutrients such as magnesium, vitamin C, and polyphenols.
These dietary imbalances may contribute to the chronic inflammation and symptom severity observed in FMS. The findings support the integration of targeted nutritional strategies into multidisciplinary care and highlight the need for future clinical trials to assess the therapeutic impact of anti-inflammatory dietary interventions in this population.
Supplementary Materials
None.
Author Contributions
Conceptualization, S.E.M.P. and I.M.M.P.; methodology, S.E.M.P. and I.M.M.P.; software, S.E.M.P. and I.M.M.P.; validation, S.E.M.P. and I.M.M.P.; formal analysis, S.E.M.P. and I.M.M.P.; investigation, S.E.M.P. and I.M.M.P.; resources, S.E.M.P. and I.M.M.P.; data curation, S.E.M.P. and I.M.M.P.; writing—original draft preparation, S.E.M.P. and I.M.M.P..;writing—review and editing, S.E.M.P. and I.M.M.P.; visualization, S.E.M.P. and I.M.M.P.; supervision, S.E.M.P. and I.M.M.P.; and project administration, S.E.M.P. and I.M.M.P. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Institutional Review Board (or Ethics Committee) of Complejo Hospitalario Universitario de Canarias, Santa Cruz de Tenerife, Spain (CHUC_2024_27).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study in accordance with the Declaration of Helsinki. Participants were informed of the study’s objectives, procedures, and their right to withdraw at any time without consequences.
Data Availability Statement
Data supporting the reported results can be found in the manuscript.
Conflicts of Interest
The authors declare no conflicts of interest. The funders had no role in the design of the study, in the collection, analyses, or interpretation of data, in the writing of the manuscript, or in the decision to publish the results.
Abbreviations
| ACR | American College of Rheumatology |
| ATP | Adenosine Triphosphate |
| BIA | Bioelectrical Impedance Analysis |
| BMI | Body Mass Index |
| DII | Dietary Inflammatory Index |
| E-DII | Energy-adjusted Dietary Inflammatory Index |
| FIQ | Fibromyalgia Impact Questionnaire |
| FMS | Fibromyalgia Syndrome |
| FSS | Fatigue Severity Scale |
| IL-6 | Interleukin 6 |
| NMDA | N-methyl-D-aspartate |
| NF-κB | Nuclear Factor Kappa-light-chain-enhancer of Activated B Cells |
| NOVA | Ultra-Processed Food Classification System |
| SD | Standard Deviation |
| SES | Socioeconomic Status |
| SIR | Systemic Inflammatory Response |
| TNF-α | Tumor Necrosis Factor Alpha |
| UPF | Ultra-Processed Food |
| VAS | Visual Analog Scale |
| WHR | Waist-to-Hip Ratio |
References
- García-Domínguez, M. Fibromyalgia and Inflammation: Unrevealing the Connection. Cells 2025, 14, 271. [Google Scholar] [CrossRef]
- Filipovic, T.; Filipović, A.; Nikolic, D.; Gimigliano, F.; Stevanov, J.; Hrkovic, M.; Bosanac, I. Fibromyalgia: Understanding, Diagnosis and Modern Approaches to Treatment. J. Clin. Med. 2025, 14, 955. [Google Scholar] [CrossRef] [PubMed]
- Jones, E.A.; Asaad, F.; Patel, N.; Jain, E.; Abd-Elsayed, A. Management of Fibromyalgia: An Update. Biomedicines 2024, 12, 1266. [Google Scholar] [CrossRef] [PubMed]
- Martín Pérez, S.E.; Lucas Hernández, L.; Oliva de la Nuez, J.L.; Soussi El-Hammouti, A.; González Cobiella, T.; del Castillo Rodríguez, J.C.; Herrera Pérez, M.; Martín Pérez, I.M. Evaluation of Sleep Patterns and Chronotypes in Spanish Women with Fibromyalgia Syndrome: A Descriptive Cross-Sectional Study. J. Sleep Med. 2024, 21, 88–97. [Google Scholar] [CrossRef]
- Sumpton, J.E.; Moulin, D.E. Fibromyalgia. Handb. Clin. Neurol. 2014, 119, 513–527. [Google Scholar] [CrossRef]
- Fitzcharles, M.A.; Yunus, M.B. The Clinical Concept of Fibromyalgia as a Changing Paradigm in the Past 20 Years. Pain Res. Treat. 2012, 2012, 184835. [Google Scholar] [CrossRef]
- Fernandez-Feijoo, F.; Samartin-Veiga, N.; Carrillo-de-la-Peña, M.T. Quality of Life in Patients with Fibromyalgia: Contributions of Disease Symptoms, Lifestyle and Multi-Medication. Front. Psychol. 2022, 13, 924405. [Google Scholar] [CrossRef]
- Galvez-Sánchez, C.M.; Duschek, S.; Reyes Del Paso, G.A. Psychological Impact of Fibromyalgia: Current Perspectives. Psychol. Res. Behav. Manag. 2019, 12, 117–127. [Google Scholar] [CrossRef]
- Cetingok, S.; Seker, O.; Cetingok, H. The Relationship between Fibromyalgia and Depression, Anxiety, Anxiety Sensitivity, Fear Avoidance Beliefs, and Quality of Life in Female Patients. Medicine (Baltimore) 2022, 101, e30868. [Google Scholar] [CrossRef]
- Gormsen, L.; Rosenberg, R.; Bach, F.W.; Jensen, T.S. Depression, Anxiety, Health-Related Quality of Life and Pain in Patients with Chronic Fibromyalgia and Neuropathic Pain. Eur. J. Pain 2010, 14, 127.e1–127.e8. [Google Scholar] [CrossRef]
- Asensi Cabo-Meseguer, A.; Cerdá-Olmedo, G.; Trillo-Mata, J.L. Fibromyalgia: Prevalence, Epidemiologic Profiles and Economic Costs. Med. Clin. 2017, 149, 441–448. [Google Scholar] [CrossRef]
- Queiroz, L.P. Worldwide epidemiology of fibromyalgia. Curr. Pain Headache Rep. 2013, 17, 356. [Google Scholar] [CrossRef]
- Ovrom, E.A.; Mostert, K.A.; Khakhkhar, S.; McKee, D.P.; Yang, P.; Her, Y.F. A Comprehensive Review of the Genetic and Epigenetic Contributions to the Development of Fibromyalgia. Biomedicines 2023, 11, 1119. [Google Scholar] [CrossRef] [PubMed]
- Siracusa, R.; Di Paola, R.; Cuzzocrea, S.; Impellizzeri, D. Fibromyalgia: Pathogenesis, Mechanisms, Diagnosis and Treatment Options Update. Int. J. Mol. Sci. 2021, 22, 3891. [Google Scholar] [CrossRef] [PubMed]
- Zhou, W.B.S.; Meng, J.; Zhang, J. Does Low Grade Systemic Inflammation Have a Role in Chronic Pain? Front. Mol. Neurosci. 2021, 14, 785214. [Google Scholar] [CrossRef] [PubMed]
- Assavarittirong, C.; Samborski, W.; Grygiel-Górniak, B. Oxidative Stress in Fibromyalgia: From Pathology to Treatment. Oxid. Med. Cell. Longev. 2022, 2022, 1582432. [Google Scholar] [CrossRef]
- Kunst, C.; Schmid, S.; Michalski, M.; Tümen, D.; Buttenschön, J.; Müller, M.; Gülow, K. The Influence of Gut Microbiota on Oxidative Stress and the Immune System. Biomedicines 2023, 11, 1388. [Google Scholar] [CrossRef]
- Palma-Ordóñez, J.F.; Moreno-Fernández, A.M.; Ramírez-Tejero, J.A.; Durán-González, E.; Martínez-Lara, A.; Cotán, D. Implication of Intestinal Microbiota in the Etiopathogenesis of Fibromyalgia: A Systematic Review. Int. J. Rheum. Dis. 2024. [Google Scholar] [CrossRef]
- Cagnie, B.; Coppieters, I.; Denecker, S.; Six, J.; Danneels, L.; Meeus, M. Central Sensitization in Fibromyalgia? A Systematic Review on Structural and Functional Brain MRI. Semin. Arthritis Rheum. 2014, 44, 68–75. [Google Scholar] [CrossRef]
- Becker, S.; Schweinhardt, P. Dysfunctional Neurotransmitter Systems in Fibromyalgia, Their Role in Central Stress Circuitry and Pharmacological Actions on These Systems. Pain Res. Treat. 2012, 2012, 741746. [Google Scholar] [CrossRef]
- Alfaro-Rodríguez, A.; Reyes-Long, S.; Roldan-Valadez, E.; González-Torres, M.; Bonilla-Jaime, H.; Bandala, C.; Avila-Luna, A.; Bueno-Nava, A.; Cabrera-Ruiz, E.; Sanchez-Aparicio, P.; et al. Association of the Serotonin and Kynurenine Pathways as Possible Therapeutic Targets to Modulate Pain in Patients with Fibromyalgia. Pharmaceuticals 2024, 17, 1205. [Google Scholar] [CrossRef]
- Jurado-Priego, L.N.; Cueto-Ureña, C.; Ramírez-Expósito, M.J.; Martínez-Martos, J.M. Fibromyalgia: A Review of the Pathophysiological Mechanisms and Multidisciplinary Treatment Strategies. Biomedicines 2024, 12, 1543. [Google Scholar] [CrossRef]
- Munipalli, B.; Allman, M.E.; Chauhan, M.; Niazi, S.K.; Rivera, F.; Abril, A.; Wang, B.; Wieczorek, M.A.; Hodge, D.O.; Knight, D.; Perlman, A.; Abu Dabrh, A.M.; Dudenkov, D.; Bruce, B.K. Depression: A Modifiable Risk Factor for Poor Outcomes in Fibromyalgia. J. Prim. Care Community Health 2022, 13, 21501319221120738. [Google Scholar] [CrossRef] [PubMed]
- Cohen, H. Controversies and Challenges in Fibromyalgia: A Review and a Proposal. Ther. Adv. Musculoskelet. Dis. 2017, 9, 115–127. [Google Scholar] [CrossRef]
- Tzadok, R.; Ablin, J.N. Current and Emerging Pharmacotherapy for Fibromyalgia. Pain Res. Manag. 2020, 2020, 6541798. [Google Scholar] [CrossRef] [PubMed]
- Masquelier, E.; D'haeyere, J. Physical Activity in the Treatment of Fibromyalgia. Jt. Bone Spine 2021, 88, 105202. [Google Scholar] [CrossRef] [PubMed]
- Andrade, A.; Dominski, F.H.; Sieczkowska, S.M. What We Already Know about the Effects of Exercise in Patients with Fibromyalgia: An Umbrella Review. Semin. Arthritis Rheum. 2020, 50, 1465–1480. [Google Scholar] [CrossRef]
- Bernardy, K.; Klose, P.; Busch, A.J.; Choy, E.H.; Häuser, W. Cognitive Behavioural Therapies for Fibromyalgia. Cochrane Database Syst. Rev. 2013, 2013, CD009796. [Google Scholar] [CrossRef]
- Metyas, C.; Aung, T.T.; Cheung, J.; Joseph, M.; Ballester, A.M.; Metyas, S. Diet and Lifestyle Modifications for Fibromyalgia. Curr. Rheumatol. Rev. 2024, 20, 405–413. [Google Scholar] [CrossRef]
- Tel Adıgüzel, K.; Köroğlu, Ö.; Yaşar, E.; Tan, A.K.; Samur, G. The Relationship between Dietary Total Antioxidant Capacity, Clinical Parameters, and Oxidative Stress in Fibromyalgia Syndrome: A Novel Point of View. Turk. J. Phys. Med. Rehabil. 2022, 68, 262–270. [Google Scholar] [CrossRef]
- Bjørklund, G.; Dadar, M.; Chirumbolo, S.; Aaseth, J. Fibromyalgia and Nutrition: Therapeutic Possibilities? Biomed. Pharmacother. 2018, 103, 531–538. [Google Scholar] [CrossRef] [PubMed]
- Minerbi, A.; Khoutorsky, A.; Shir, Y. Decoding the Connection: Unraveling the Role of Gut Microbiome in Fibromyalgia. Pain Rep. 2024, 10, e1224. [Google Scholar] [CrossRef] [PubMed]
- Poursalehi, D.; Tirani, S.A.; Shahdadian, F.; et al. Ultra-Processed Foods Intake in Relation to Metabolic Health Status, Serum Brain-Derived Neurotrophic Factor and Adropin Levels in Adults. Nutr. J. 2024, 23, 121. [Google Scholar] [CrossRef]
- Monteiro, C.A.; Cannon, G.; Levy, R.B.; Moubarac, J.C.; Louzada, M.L.; Rauber, F.; Khandpur, N.; Cediel, G.; Neri, D.; Martinez-Steele, E.; Baraldi, L.G.; Jaime, P.C. Ultra-Processed Foods: What They Are and How to Identify Them. Public Health Nutr. 2019, 22, 936–941. [Google Scholar] [CrossRef]
- Monteiro, C.A.; Cannon, G.; Lawrence, M.; Costa Louzada, M.L.; Pereira Machado, P. Ultra-Processed Foods, Diet Quality, and Health Using the NOVA Classification System; FAO: Rome, Italy, 2019. [Google Scholar]
- Gibney, M.J. Ultra-Processed Foods: Definitions and Policy Issues. Curr. Dev. Nutr. 2018, 3, nzy077. [Google Scholar] [CrossRef]
- Quetglas-Llabrés, M.M.; Monserrat-Mesquida, M.; Bouzas, C.; Mateos, D.; Ugarriza, L.; Gómez, C.; Tur, J.A.; Sureda, A. Oxidative Stress and Inflammatory Biomarkers Are Related to High Intake of Ultra-Processed Food in Old Adults with Metabolic Syndrome. Antioxidants 2023, 12, 1532. [Google Scholar] [CrossRef]
- Martínez Leo, E.E.; Meza Peñafiel, A.; Hernández Escalante, V.M.; Cabrera Araujo, Z.M. Ultra-Processed Diet, Systemic Oxidative Stress, and Breach of Immunologic Tolerance. Nutrition 2021, 91–92, 111419. [Google Scholar] [CrossRef]
- Asensi, M.T.; Napoletano, A.; Sofi, F.; Dinu, M. Low-Grade Inflammation and Ultra-Processed Foods Consumption: A Review. Nutrients 2023, 15, 1546. [Google Scholar] [CrossRef]
- Poti, J.M.; Braga, B.; Qin, B. Ultra-Processed Food Intake and Obesity: What Really Matters for Health—Processing or Nutrient Content? Curr. Obes. Rep. 2017, 6, 420–431. [Google Scholar] [CrossRef]
- Vallianou, N.G.; Evangelopoulos, A.; Tzivaki, I.; Daskalopoulou, S.; Adamou, A.; Michalaki Zafeiri, G.C.; Karampela, I.; Dalamaga, M.; Kounatidis, D. Ultra-Processed Foods and Type 2 Diabetes Mellitus: What Is the Evidence So Far? Biomolecules 2025, 15, 307. [Google Scholar] [CrossRef]
- Juul, F.; Vaidean, G.; Parekh, N. Ultra-Processed Foods and Cardiovascular Diseases: Potential Mechanisms of Action. Adv. Nutr. 2021, 12, 1673–1680. [Google Scholar] [CrossRef] [PubMed]
- Lane, M.M.; Lotfaliany, M.; Forbes, M.; Loughman, A.; Rocks, T.; O'Neil, A.; Machado, P.; Jacka, F.N.; Hodge, A.; Marx, W. Higher Ultra-Processed Food Consumption Is Associated with Greater High-Sensitivity C-Reactive Protein Concentration in Adults: Cross-Sectional Results from the Melbourne Collaborative Cohort Study. Nutrients 2022, 14, 3309. [Google Scholar] [CrossRef] [PubMed]
- Lopes, A.E.D.S.C.; Araújo, L.F.; Levy, R.B.; Barreto, S.M.; Giatti, L. Association between Consumption of Ultra-Processed Foods and Serum C-Reactive Protein Levels: Cross-Sectional Results from the ELSA-Brasil Study. Sao Paulo Med. J. 2019, 137, 169–176. [Google Scholar] [CrossRef] [PubMed]
- Martins, G.M.D.S.; França, A.K.T.D.C.; Viola, P.C.A.F.; Carvalho, C.A.; Marques, K.D.S.; Santos, A.M.D.; Batalha, M.A.; Alves, J.D.A.; Ribeiro, C.C.C. Intake of Ultra-Processed Foods Is Associated with Inflammatory Markers in Brazilian Adolescents. Public Health Nutr. 2022, 25, 591–599. [Google Scholar] [CrossRef]
- Carrasco-Querol, N.; Cabricano-Canga, L.; Bueno Hernández, N.; Gonçalves, A.Q.; Caballol Angelats, R.; Pozo Ariza, M.; Martín-Borràs, C.; Montesó-Curto, P.; Castro Blanco, E.; Dalmau Llorca, M.R.; et al. Nutrition and Chronobiology as Key Components of Multidisciplinary Therapeutic Interventions for Fibromyalgia and Associated Chronic Fatigue Syndrome: A Narrative and Critical Review. Nutrients 2024, 16, 182. [Google Scholar] [CrossRef]
- Almirall, M.; Musté, M.; Serrat, M.; Touriño, R.; Espartal, E.; Marsal, S. Restrictive Diets in Patients with Fibromyalgia: State of the Art. Biomedicines 2024, 12, 629. [Google Scholar] [CrossRef]
- Elma, Ö.; Brain, K.; Dong, H.J. The Importance of Nutrition as a Lifestyle Factor in Chronic Pain Management: A Narrative Review. J. Clin. Med. 2022, 11, 5950. [Google Scholar] [CrossRef]
- Silva, A.R.; Bernardo, A.; Costa, J.; Cardoso, A.; Santos, P.; de Mesquita, M.F.; Vaz Patto, J.; Moreira, P.; Silva, M.L.; Padrão, P. Dietary Interventions in Fibromyalgia: A Systematic Review. Ann. Med. 2019, 51 (Suppl. 1), 2–14. [Google Scholar] [CrossRef]
- Silva, A.R.; Bernardo, A.; de Mesquita, M.F.; Vaz-Patto, J.; Moreira, P.; Silva, M.L.; Padrão, P. An Anti-Inflammatory and Low Fermentable Oligo-, Di-, and Monosaccharides and Polyols Diet Improved Patient Reported Outcomes in Fibromyalgia: A Randomized Controlled Trial. Front. Nutr. 2022, 9, 856216. [Google Scholar] [CrossRef]
- Maddox, E.K.; Massoni, S.C.; Hoffart, C.M.; Takata, Y. Dietary Effects on Pain Symptoms in Patients with Fibromyalgia Syndrome: Systematic Review and Future Directions. Nutrients 2023, 15, 716. [Google Scholar] [CrossRef]
- Erdrich, S.; Hawrelak, J.A.; Myers, S.P.; Harnett, J.E. Determining the Association between Fibromyalgia, the Gut Microbiome and Its Biomarkers: A Systematic Review. BMC Musculoskelet. Disord. 2020, 21, 181. [Google Scholar] [CrossRef] [PubMed]
- Rondinella, D.; Raoul, P.C.; Valeriani, E.; Venturini, I.; Cintoni, M.; Severino, A.; Galli, F.S.; Mora, V.; Mele, M.C.; Cammarota, G.; et al. The Detrimental Impact of Ultra-Processed Foods on the Human Gut Microbiome and Gut Barrier. Nutrients 2025, 17, 859. [Google Scholar] [CrossRef] [PubMed]
- von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P.; STROBE Initiative. Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement: Guidelines for Reporting Observational Studies. BMJ 2007, 335, 806–808. [Google Scholar] [CrossRef]
- Wolfe, F.; Clauw, D.J.; Fitzcharles, M.-A.; Goldenberg, D.L.; Khan, R.L.; Mayer, E.A.; Russell, I.J.; Walitt, B. The American College of Rheumatology Preliminary Diagnostic Criteria for Fibromyalgia and Measurement of Symptom Severity. Arthritis Care Res. 2010, 62, 600–610. [Google Scholar] [CrossRef] [PubMed]
- Faul, F.; Erdfelder, E.; Lang, A.-G.; Buchner, A. G*Power 3: A Flexible Statistical Power Analysis Program for the Social, Behavioral, and Biomedical Sciences. Behav. Res. Methods 2007, 39, 175–191. [Google Scholar] [CrossRef]
- Brewer, G.J.; Blue, M.N.M.; Hirsch, K.R.; Saylor, H.E.; Gould, L.M.; Nelson, A.G.; Smith-Ryan, A.E. Validation of InBody 770 Bioelectrical Impedance Analysis Compared to a Four-Compartment Model Criterion in Young Adults. Clin. Physiol. Funct. Imaging 2021, 41, 317–325. [Google Scholar] [CrossRef]
- Burckhardt, C.S.; Clark, S.R.; Bennett, R.M. The Fibromyalgia Impact Questionnaire: Development and Validation. J. Rheumatol. 1991, 18, 728–733. [Google Scholar]
- Miró, J.; Sánchez, A.; Nieto, R.; et al. Validación del Fibromyalgia Impact Questionnaire (FIQ) en población española. Rev. Esp. Reumatol. 2008, 35, 392–400. [Google Scholar] [CrossRef]
- García-Leiva, J.M.; Sánchez, J.; et al. Aplicación de la escala visual analógica (VAS) para la evaluación del dolor en pacientes con fibromialgia en una muestra española. Med. Clin. (Barc.) 2009, 132, 268–272. [Google Scholar] [CrossRef]
- Rivas, M.; Martínez, M.; et al. Validación de la Fatigue Severity Scale (FSS) en población española con fibromialgia. Rev. Esp. Reumatol. 2010, 37, 1–7. [Google Scholar] [CrossRef]
- Lupiáñez, J.; Ballesteros, S.; et al. Validación de la Fatigue Severity Scale en población española con fibromialgia: Un estudio multicéntrico. Rev. Neurol. 2011, 53, 12–19. [Google Scholar] [CrossRef]
- Shivappa, N.; Steck, S.E.; Hurley, T.G.; Hussey, J.R.; Ma, Y.; Ockene, I.S.; Wirth, M.D.; Fitzgerald, S.; Blair, C.K.; Hebert, J.R. Designing and Developing a Dietary Inflammatory Index. J. Nutr. 2014, 144, 881–890. [Google Scholar] [CrossRef]
- IBM Corp. IBM SPSS Statistics for Windows, Version 29.0.2.0; IBM Corp.: Armonk, NY, USA, 2023. [Google Scholar]
- Srour, B.; Fezeu, L.K.; Kesse-Guyot, E.; Allès, B.; Méjean, C.; Andrianasolo, R.M.; Chazelas, E.; Deschasaux, M.; Hercberg, S.; Galan, P.; Monteiro, C.A.; Julia, C.; Touvier, M. Ultra-Processed Food Intake and Risk of Cardiovascular Disease: Prospective Cohort Study (NutriNet-Santé). BMJ 2019, 365, l1451. [Google Scholar] [CrossRef]
- Field, R.; Pourkazemi, F.; Hashempur, M.H.; Thiruvengadam, M.; Rooney, K. Editorial: Diet, Nutrition, and Functional Foods for Chronic Pain. Front. Nutr. 2024, 11, 1456706. [Google Scholar] [CrossRef]
- Minerbi, A.; Gonzalez, E.; Brereton, N.J.B.; Anjarkouchian, A.; Dewar, K.; Fitzcharles, M.-A.; Chevalier, S. Altered microbiome composition in individuals with fibromyalgia. Pain 2019, 160, 2589–2602. [Google Scholar] [CrossRef]
- González-Gil, A.M.; Elizondo-Montemayor, L.; Moreno-Rodríguez, A.; González-González, J.G.; Galván-Salazar, H.R.; Rodríguez-Gutiérrez, R.; Lavalle-González, F.J. The Role of Diet as a Modulator of the Inflammatory Process in the Neurological Diseases. Nutrients. 2023, 15(6), 1304. [CrossRef]
- Song, Y.; Li, Y.; Wang, Y.; Wang, Y.; Li, Y.; Wang, Y. Ultra-Processed Food and Gut Microbiota: Do Additives Affect the Microbiome? Nutrients 2025, 17, 2. [Google Scholar] [CrossRef]
- Di Lorenzo, M.; Aurino, L.; Cataldi, M.; Cacciapuoti, N.; Di Lauro, M.; Lonardo, M.S.; Gautiero, C.; Guida, B. A Close Relationship Between Ultra-Processed Foods and Adiposity in Adults in Southern Italy. Nutrients 2024, 16, 3923. [Google Scholar] [CrossRef]
- Gibney, M.J.; Forde, C.G.; Mullally, D.; Gibney, E.R. Ultra-Processed Foods: A Narrative Review of the Impact on Human Health. Nutrients 2023, 16, 1738. [Google Scholar] [CrossRef]
- Reyneke, G.L.; Lambert, K.; Beck, E.J. Food-Based Indexes and Their Association with Dietary Inflammation. Adv. Nutr. 2025, 16, 100400. [Google Scholar] [CrossRef]
- Cordero, M.D.; Alcocer-Gómez, E.; Cano-García, F.J.; Sánchez-Domínguez, B.; Fernández-Riejo, P.; Moreno Fernández, A.M.; Fernández-Rodríguez, A.; De Miguel, M. Clinical Symptoms in Fibromyalgia Are Associated to Overweight and Lipid Profile. Rheumatol. Int. 2014, 34, 419–422. [Google Scholar] [CrossRef]
- Sundaram, S.; Prabhu, R.; Rangaswami, R.; Marappa, S.; Venkatesan, R.; Prevalence of Dyslipidemia in Fibromyalgia: A Single-Center Case Control Study from South India. ACR Convergence 2021. Available online: https://acrabstracts.org/abstract/prevalence-of-dyslipidemia-in-fibromyalgia-a-single-center-case-control-study-from-south-india (accessed on 11 April 2025).
- Lopez-Garcia, E.; Schulze, M.B.; Manson, J.E.; Meigs, J.B.; Albert, C.M.; Rifai, N.; Willett, W.C.; Hu, F.B. Consumption of Trans Fatty Acids is Related to Plasma Biomarkers of Inflammation and Endothelial Dysfunction. J. Nutr. 2005, 135, 562–566. [Google Scholar] [CrossRef]
- Tian, Y.; Zhang, H.; Xu, L.; Ma, L.; Zhang, S.; Zheng, Y.; Lu, J.; Seo, J.H. High-Fat Diet Enhances Pain Sensitivity in Mice with Acid Saline-Induced Fibromyalgia-like Condition through Upregulation of TNF-α in Dorsal Root Ganglia. PLoS ONE 2018, 13, e0190861. [Google Scholar] [CrossRef]
- García-González, Á.; Fernández-Sánchez, M.; Martínez-López, E.; Rodríguez-Blanque, R.; Aguilar-Cordero, M.J.; Sánchez-López, A.M. Nutrition and Chronobiology as Key Components of Multidisciplinary Management in Fibromyalgia. Nutrients 2024, 16, 182. [Google Scholar] [CrossRef]
- Jiménez-Cruz, A.; Bacardí-Gascón, M.; Turnbull, W.H.; Rosales-Garay, P.; Severino-Lugo, I. A Flexible, Low-Glycemic Index Mexican-Style Diet in Overweight and Obese Subjects with Type 2 Diabetes Improves Metabolic Parameters During a 6-Week Treatment Period. Diabetes Care 2003, 26, 1967–1970. [Google Scholar] [CrossRef]
- Escaffi, M.J.; Navia, C.; Quera, R.; Simian, D. Nutrición y enfermedad inflamatoria intestinal: posibles mecanismos en la incidencia y manejo. Rev. Med. Clin. Condes 2021, 32, 73–82. [Google Scholar] [CrossRef]
- Schnabel, L.; Buscail, C.; Sabate, J.-M.; Bouchoucha, M.; Kesse-Guyot, E.; Allès, B.; Touvier, M.; Monteiro, C.A.; Hercberg, S.; Benamouzig, R.; Julia, C. Association Between Ultra-Processed Food Consumption and Functional Gastrointestinal Disorders: Results From the French NutriNet-Santé Cohort. Am. J. Gastroenterol. 2018, 113, 1217–1228. [Google Scholar] [CrossRef]
- Rosanoff, A.; Dai, Q.; Shapses, S.A. Magnesium and Inflammation: Advances and Perspectives. Semin. Cell Dev. Biol. 2020, 115, 37–44. [Google Scholar] [CrossRef]
- Dominguez, L.J.; Veronese, N.; Barbagallo, M. The Role of Magnesium in the Pathogenesis of Metabolic Disorders. Nutrients 2022, 14, 3896. [Google Scholar] [CrossRef]
- Barbagallo, M.; Veronese, N.; Dominguez, L.J. Magnesium and Aging: Current Concepts and Future Perspectives. Nutrients 2021, 13, 463. [Google Scholar] [CrossRef]
- Martín Pérez, S.E.; Fernández Carnero, J.; Sosa Reina, M.D. Mecanismos y efectos terapéuticos de la terapia manual ortopédica. En Terapia manual ortopédica en el tratamiento del dolor; Quevedo García, A., Alonso Sal, A., Alonso Pérez, J.L., Eds.; Elsevier España: Madrid, España, 2022; pp. 87–110. ISBN 978-84-1382-020-0. [Google Scholar]
- Zhang, Y.; Xie, Y.; Xu, Y.; Zhang, X.; Zhang, Y.; Wang, Y.; Zhang, Y.; Li, Y.; Wang, Y.; Wang, Y. The Causal Role of Magnesium Deficiency in the Neuroinflammation, Chronic Pain, Memory and Emotional Deficits Induced by Estrogen Decline. Front. Pharmacol. 2021, 12, 784119. [Google Scholar] [CrossRef]
- Rosanoff, A.; Dai, Q.; Shapses, S.A. Essential Nutrient Interactions: Does Low or Suboptimal Magnesium Status Interact with Vitamin D and/or Calcium Status? Adv. Nutr. 2016, 7, 25–43. [Google Scholar] [CrossRef] [PubMed]
- Gerdle, B.; Ghafouri, B.; Ernberg, M.; Larsson, B. Evidence of Mitochondrial Dysfunction in Fibromyalgia: Deviating Muscle Energy Metabolism Detected Using Microdialysis and Magnetic Resonance. J. Clin. Med. 2020, 9, 3527. [Google Scholar] [CrossRef] [PubMed]
- Zhou, H.; Beevers, C.S.; Huang, S. The Therapeutic Potential of Curcumin in Inflammatory Diseases. Anti-Inflammatory & Anti-Allergy Agents in Medicinal Chemistry 2011, 10, 221–230. [Google Scholar] [CrossRef]
- Menon, V.P.; Sudheer, A.R. Antioxidant and Anti-inflammatory Properties of Curcumin. Advances in Experimental Medicine and Biology 2007, 595, 105–125. [Google Scholar] [CrossRef]
- Chaudhary, P.; Janmeda, P.; Docea, A.O.; Yeskaliyeva, B.; Abdull Razis, A.F.; Modu, B.; Calina, D.; Sharifi-Rad, J. Oxidative Stress, Free Radicals and Antioxidants: Potential Crosstalk in the Pathophysiology of Human Diseases. Front. Chem. 2023, 11, 1158198. [Google Scholar] [CrossRef]
- Zahra, M.; Abrahamse, H.; George, B.P. Flavonoids: Antioxidant Powerhouses and Their Role in Nanomedicine. Antioxidants 2024, 13, 922. [Google Scholar] [CrossRef]
- Młynarska, E.; Biskup, L.; Możdżan, M.; Grygorcewicz, O.; Możdżan, Z.; Semeradt, J.; Uramowski, M.; Rysz, J.; Franczyk, B. The Role of Oxidative Stress in Hypertension: The Insight into Antihypertensive Properties of Vitamins A, C and E. Antioxidants 2024, 13, 848. [Google Scholar] [CrossRef]
- Antonelli, A.; Bianchi, M.; Fear, E.J.; Giorgi, L.; Rossi, L. Management of Fibromyalgia: Novel Nutraceutical Therapies Beyond Traditional Pharmaceuticals. Nutrients 2025, 17, 530. [Google Scholar] [CrossRef]
- Jomova, K.; Alomar, S.Y.; Valko, R.; Liska, J.; Nepovimova, E.; Kuca, K.; Valko, M. Flavonoids and Their Role in Oxidative Stress, Inflammation, and Human Diseases. Chem. Biol. Interact. 2025, 413, 111489. [Google Scholar] [CrossRef]
- Soares, P.; Oliveira, B.; Lopes, C.; Freitas, P.; Moreira, P. The Association between Socioeconomic Status and Ultra-Processed Food Consumption in Portuguese Adults: The PORMETS Study. Nutrients 2024, 16, 4127. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



