
Submitted:
10 April 2025
Posted:
10 April 2025
You are already at the latest version
Abstract
Colistin resistance, driven by chromosomal mutations and the spread of plasmid-mediated MCR genes, has emerged as a critical challenge in combating multidrug-resistant gram-negative bacteria. This resistance compromises the efficacy of colistin, leading to higher treatment failure rates, prolonged hospitalizations, and increased mortality. Recent studies highlight key mechanisms, including lipid A modifications, that enable bacteria to evade colistin’s effects. The global spread of MCR genes exacerbates the issue, underlining the need for improved diagnostics and rapid detection of resistant strains to prevent adverse patient outcomes. To combat this growing threat, a multifaceted approach is essential, involving enhanced antimicrobial stewardship, stricter infection control measures, and continued research into alternative therapies and diagnostic methods. Collaborative efforts from researchers, healthcare providers, policymakers, and the pharmaceutical industry are crucial to preserving colistin’s effectiveness and mitigating the broader impact on public health.
Keywords:
Colistin resistance
; MCR genes
; Antibiotic stewardship
; Public health
; MDR
; PmrA
1. Introduction
The emergence of multidrug-resistant bacteria has led to increased reliance on colistin, a last-resort antibiotic. This heightened use has accelerated the development of resistance to colistin itself, which is concerning because it is one of the few remaining antibiotics effective against certain multidrug-resistant bacterial strains. Antimicrobial resistance (AMR) is among the top global health threats as identified by the WHO [1].
Since the pipeline for new antibiotic discoveries is closing and there won't be any soon to treat these "superbugs," there is a renewed interest in bringing back older drugs that were thought to be toxic for clinical utilization. In particular, the polymyxins (colistin and polymyxin B) should be used as "last resort" antimicrobials [1]. The 77th World Health Assembly recognized the urgent need for evidence to inform public health policy as one of WHO's strategic and operational goals to fight drug-resistant bacterial infections between 2025 and 2035 in a resolution on accelerating national and international responses to AMR which was approved on May 30, 2024 [2], the resolution urges WHO member states to collaborate with academia, the private sector, and civil society to support and advance basic, applied, and implementation research on antimicrobial stewardship, vaccines, diagnostic tools, treatments, and infection prevention and control. New antibiotics are therefore desperately needed, especially ones that are effective against Gram-negative "superbugs” [2].
The acquisition and spread of plasmid-mediated resistance genes, specifically the MCR 1 to MCR10 genes, are the main causes of the sharp rise in colistin ineffectiveness [3], which encode enzymes capable of modifying the bacterial cell membrane and reducing colistin's antimicrobial activity. Understanding the mechanisms underlying colistin insusceptibility, along with its clinical implications and potential future directions, is essential for addressing this evolving public health threat.
Due to high rates of morbidity and mortality, longer hospital stays (LOS), higher direct medical expenses, and higher societal infectious costs, AMR can result in significant financial losses [4]. Gram-negative bacteria, such as Enterobacteriaceae, Acinetobacter baumannii, and Pseudomonas aeruginosa, pose a growing threat to international health. On a worldwide scale, it is concerning that resistance to widely used antibiotics, such as beta-lactams, carbapenems, fluoroquinolones, and aminoglycosides, is emerging quickly. In light of the lack of equally effective and less toxic antibiotic substitutes, physicians are forced to reconsider the use of colistin in many healthcare institutions across the globe, highlighting the pressing need for new antimicrobial medicines [5,6,7]. According to the Infectious Diseases Society of America (IDSA) document "Bad Bugs, No Drugs," "as antibiotic discovery stagnates, a public health crisis brews" [8].
This article aims to address the escalating threat of colistin insusceptibility, driven by its increasing use as a last-resort antibiotic and the rapid spread of plasmid-mediated insusceptibility genes. With few new antibiotics in development and growing reliance on colistin to combat multidrug-resistant gram-negative bacteria, the urgency to understand resistance mechanisms and explore innovative solutions is critical. A literature study was conducted to examine global antibiotic resistance, focusing on colistin resistance, AMU, AMR, and stewardship. Databases like Google Scholar, PubMed, and Scopus were searched with relevant keywords. Studies were included based on their focus on colistin resistance mechanisms, clinical outcomes, and mitigation strategies, excluding non-peer-reviewed sources. The study emphasized the impact of AMR on public health and the role of health sectors in combating resistance, categorizing results into mechanisms, clinical implications, epidemiology, surveillance, and future perspectives. This review highlights recent advancements, clinical implications, and future strategies to mitigate this global health challenge.
2. Mechanism of Colistin Resistance
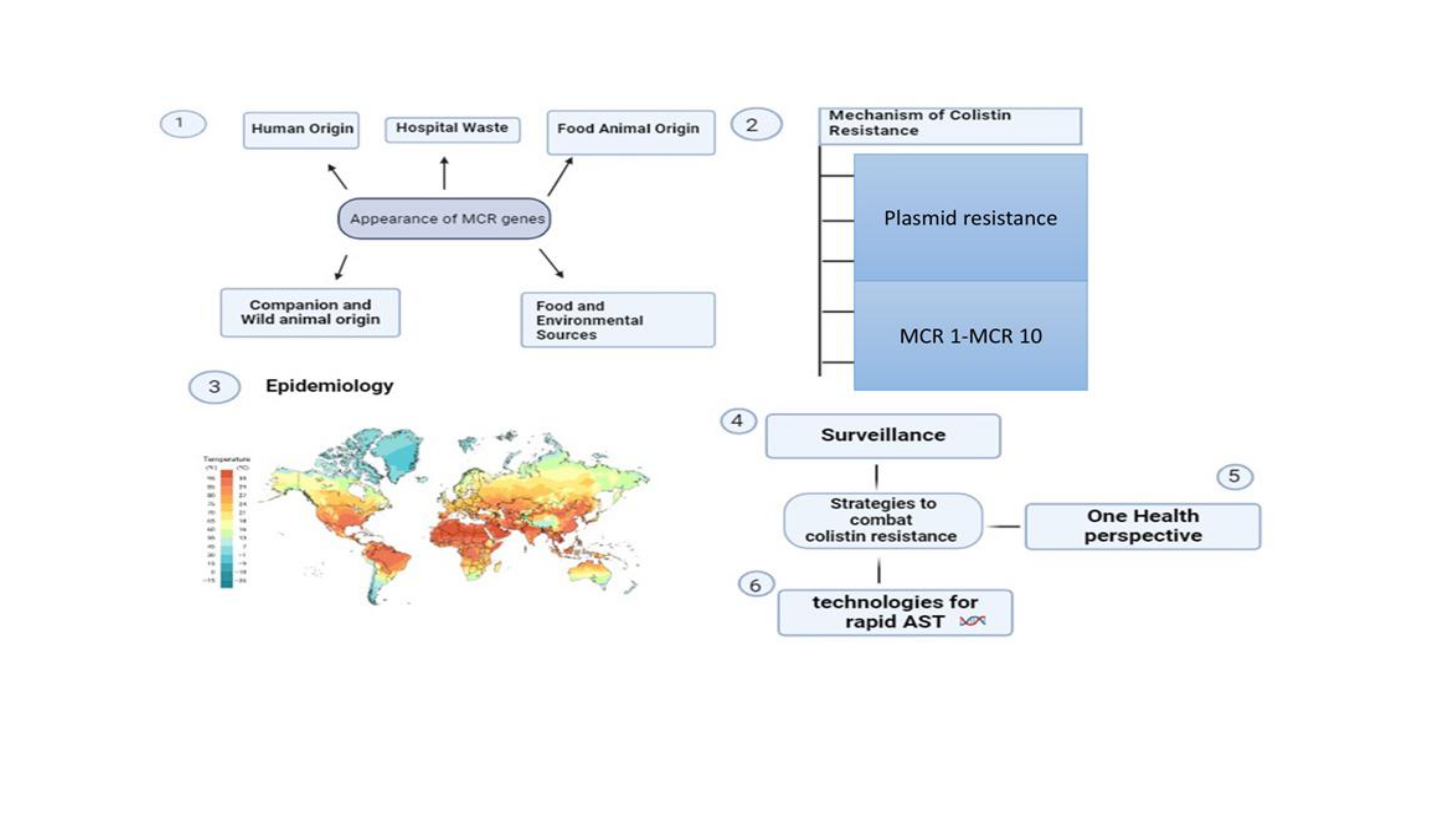
Until the past decade, efforts to combat resistance have primarily focused on research understanding the genetic processes underpinning it (Figure 1). Figure 1 depicts the colistin resistance in gram-negative bacteria arises from lipid A modifications via L-Ara4N and pEtN additions. These are regulated by activated PmrA-PmrB and PhoP-PhoQ systems, with pmrCAB and arnBCADTEF operons driving modification synthesis. Mutations in mgrB overactivated PhoP-PhoQ, enhancing resistance. The existence of the MCR-1 gene, which codes for a protein that alters the bacterial cell membrane and lessens the efficiency of colistin, is one important discovery (Figure 2). Figure 2 explains about various mechanism by which bacteria develop resistance: chromosomal mutation, plasmid borne resistance, lipid A mutation which further enhances the unbinding of colistin to the membrane. This gene can spread across bacteria, which exacerbates the issue even more. It has been identified in a number of bacterial species, including E. coli (Table 1). Table 1 represents the various mechanism responsible for colistin insusceptibility.
2.1. Polymyxin Resistance Mediated by Plasmids
Plasmid-mediated polymyxin insusceptibility poses a substantial barrier to the treatment of multidrug-resistant GNB, particularly those involving MCR 1–10 genes. Horizontal gene transfer is facilitated by plasmids, which spreads resistance in environmental and clinical contexts. This insusceptibility poses a special risk in infections that are resistant to carbapenem, as it may result in treatment failures and unfavourable patient outcomes. The creation of substitute therapies, improved monitoring, and strict antimicrobial stewardship are all necessary to address this problem. To stop it from spreading and keep polymyxin medicines effective, it is essential to comprehend the dynamics of this resistance and how it affects treatment [3].
2.1.1. MCR-1 Gene
The MCR-1 gene, a plasmid-mediated colistin resistance determinant, has gained significant attention due to its role in conferring resistance to one of the last-resort antibiotics, colistin in GNB. MCR-1, which was identified in China in 2015, encodes an enzyme called phosphoethanolamine transferase that alters the lipid a part of the outer membrane of bacteria that inhibits the binding and antibacterial activity of colistin. Because of its placement on plasmids, the gene can move horizontally between bacterial strains and species, which aids in the spread of colistin insusceptibility around the world. The emergence of MCR-1 produces a serious threat to public health, necessitating enhanced surveillance, antimicrobial stewardship, and the development of alternative treatment strategies to combat the spread of colistin-resistant bacteria [9].
2.1.2. MCR-2 Gene
In 2016, the MCR-2 gene was found in Belgium, which revealed a phosphoethanolamine transferase enzyme similar to MCR-1 that codes for a plasmid-mediated colistin resistance determinant. Through alterations to the lipid A layer of the bacterial outer membrane, the resistance mechanism is similar to MCR-1 but genetically different, it reduces the effectiveness of colistin, an essential antibiotic of last resort. The rise in MCR-2 is indicative of the growing danger of colistin insusceptibility, underscoring the need for close observation and rigorous management practices [10,11]. Following its discovery in E. Coli isolated from cattle and pigs in Belgium [11], the MCR-2 was most recently found in human vaginal swabs from China [12]. The MCR-2 (1617 bp), amino acid identity of the PEtN transferases encoded by the genes MCR-1 (541 aa) and MCR-2 (538 aa) is 81% similar to each other. They are 63% and 64% alike to Paenibacillus sophorae and Moraxella osloensis, respectively, according to their phylogenetic research [11].
2.1.3. MCR-3 Gene
Similar to earlier discovered MCR, the MCR-3 gene is a plasmid-mediated colistin resistance determinant that contributes to colistin insusceptibility by encoding a phosphoethanolamine transferase enzyme. Initially discovered in 2017 in an E. coli isolate from pig in China, MCR-3 exhibits genetic divergence from MCR-1 and MCR-2, suggesting independent acquisition and dissemination. This gene's presence on mobile genetic elements facilitates its horizontal transfer between bacterial strains and species, posing a significant challenge to antimicrobial therapy and public health [13].
2.1.4. MCR-4 Gene
The MCR-4 gene is a plasmid colistin resistance determinant that encodes a phosphoethanolamine transferase enzyme, similar to other MCR variants, leading to resistance against colistin. Initially identified in 2017 in an E. coli isolate from Belgium, MCR-4 exhibits distinct genetic features from previously described MCR variants, suggesting independent acquisition and dissemination. Comprehending the genetic traits and prevalence of MCR-4 is crucial in order to execute efficient monitoring tactics and formulate focused interventions aimed at curbing the proliferation of colistin resistance and maintaining the effectiveness of this vital antibiotic [14].
2.1.5. MCR-5 Gene
The discovery of the MCR-5 gene in 2017, found in a d-tartrate fermenting S. enterica subsp. isolated from a pig in China, underscores the plasmid-mediated mechanism of colistin resistance. Similar to other MCR variations, MCR-5 encodes a phosphoethanolamine transferase enzyme, leading to alterations in the lipid A of the bacteria and reducing colistin binding affinity. Its presence on mobile genetic elements facilitates horizontal transfer among bacterial populations, heightening concerns over colistin resistance dissemination. To safeguard the efficacy of this crucial antibiotic in clinical settings, it is imperative to comprehensively characterize the genetic profile and distribution patterns of MCR-5 to implement effective prevention strategies against colistin-resistant bacteria [15,16].
2.1.6. MCR-6 Gene
A plasmid originated pathway of colistin resistance is suggested by the MCR-6 gene, which codes for an enzyme called phosphoethanolamine transferase that is comparable to other MCR variants. MCR-6, which was identified in 2017 in an E. Coli isolate from a patient suffering from a bloodstream infection in Switzerland, modifies the lipid A constituent of the bacterial outer membrane to give colistin insusceptibility. Antimicrobial therapy and public health are substantially challenged by its presence on mobile genetic elements, which promotes horizontal transfer between bacterial strains and species. To combat the rise of colistin insusceptibility and maintain the effectiveness of this vital antibiotic, it is imperative to comprehend the genetic makeup and epidemiology of MCR-6 in order to design focused interventions and surveillance plans that are effective [17].
2.1.7. MCR-7 Gene
Understanding colistin insusceptibility has advanced significantly with the 2018 discovery of the MCR-7 gene in K. pneumoniae isolates from China. Because it has the ability to transmit genes horizontally through mobile genetic elements, MCR-7 encodes a phosphoethanolamine transferase enzyme that imparts resistance to colistin, hence posing a severe threat to public health. To effectively apply targeted treatments to minimize its transmission and preserve viable treatment choices for multidrug-resistant infections, it is imperative to have a thorough understanding of the genetic features and epidemiology of MCR-7 [18].
2.1.8. MCR-8 Gene
An important addition to the range of plasmid-associated colistin resistance mechanisms is the MCR-8 gene. MCR-8, which encodes a phosphoethanolamine was identified in 2019 in K. pneumoniae isolates from China that produce New Delhi metallo-β-lactamase (NDM). Because MCR-8 can spread horizontally between bacterial strains and species through mobile genetic components, its introduction significantly complicates the AMR landscape. In order to combat the emergence of colistin-resistant bacteria and maintain the efficacy of this crucial antibiotic for clinical use, MCR-8's presence emphasizes the urgent need for improved surveillance, antimicrobial stewardship, and the creation of alternate therapeutic approaches [19].
2.1.9. MCR-9 Gene
The MCR-9 gene represents a novel addition to the growing repertoire of colistin insusceptibility mechanisms. Identified in 2019 in clinical isolates of K. pneumoniae from China, MCR-9 encodes a phosphoethanolamine transferase enzyme responsible for conferring colistin insusceptibility. The discovery of MCR-9 underscores the ongoing evolution of AMR and highlights the urgent need for robust surveillance and control measures to curb its spread. Given its potential for horizontal transfer between bacterial strains and species via mobile genetic elements, the emergence of MCR-9 further complicates efforts to combat multidrug-resistant infections. To mitigate its spread and maintain the efficacy of colistin for therapeutic use, specific therapies that consider the genetic features and epidemiology of MCR-9 are essential [20].
2.1.10. MCR-10 Gene
A recent finding in the field of plasmid-mediated mechanisms of colistin resistance is the MCR-10 gene. MCR-10, which encodes a phosphoethanolamine transferase enzyme, was discovered in 2020 in clinical samples of E. coli from China. MCR-10's appearance contributes to the increasing complexity of AMR, creating serious problems for clinical care and public health. The spread of MCR-10 highlights the critical need for improved surveillance, antimicrobial stewardship, and the creation of alternative therapeutic approaches in order to effectively combat multidrug-resistant infections. Understanding the genetic characteristics and epidemiology of MCR-10 is essential for informing targeted interventions aimed at mitigating its dissemination and preserving the effectiveness of colistin for clinical use [21].
3. Clinical Implication
The emergence and proliferation of colistin resistance present formidable challenges in clinical management and patient care. Gram-negative pathogens like A. baumannii, K. pneumoniae, and E. coli, already notorious for multidrug insusceptibility, now pose an even greater threat due to dwindling treatment options. Once considered a last resort, colistin now struggles against these resistant strains, leading to treatment failures, prolonged hospitalizations, and increased mortality rates. According to kollef et al., study among 93 patients, the mortality rate was 29.9% [22], and 41% had diabetes as a co-morbid condition. K. pneumoniae was the most common organism isolated, accounting for 91.4% of cases [22]. In another study, colistin-resistant MDR GNB was found in 19.6% of cases, with K. pneumoniae showing 9.2% resistance. Most isolates were from respiratory infections (28.8%) and neurology ICU (54.1%), with a 74.2% recovery rate. Among 122 patients with A. baumannii infection, 14.8% had colistin-resistant isolates. The 14-day mortality rate was 44.4% for colistin-resistant cases and 34.6% for colistin-susceptible cases, with no significant difference. A. baumannii was key risk factors for mortality [23]. In Balkhai et al., study among 585 bloodstream infections, carbapenem resistance was seen in 27.7% of isolates, with A. baumannii (80.4%), K. pneumoniae (46.4%), and P. aeruginosa (29.9%) being the most resistant. Colistin insusceptibility was found in 13.4% of carbapenem-resistant isolates. The 30-day mortality rate was 68.1% for carbapenem-resistant infections versus 21.3% for carbapenem-susceptible cases [24]. In another study, among 77 patients, those with A. baumannii resistant to colistin (ABCR) infections had higher exposure to antibiotics, mechanical ventilation, and invasive procedures compared to A. baumannii sensitive to colistin (ABCS) infections. Prolonged carbapenem use was an independent risk factor for ABCR infection [25]. Out of 3190 patients, 54 (1.6%) developed Multidrug-resistant Urinary tract infection (MDR-UTI), with P. aeruginosa being the most frequent pathogen (63%). Colistin was effective in 66.7% of cases, and MDR-UTI patients had a significantly longer hospital stay (9.28 days) [26]. A therapeutic challenge for clinicians caring for critically ill patients hospitalized for acute infections is the rising prevalence (Table 2) of MDR GNB mortality. The Table 2 highlights the rising prevalence of colistin-resistant infections caused by various multidrug-resistant microorganisms, posing a significant therapeutical challenge associated with clinicians managing critically ill patients. Mortality rates associated with these infections vary widely, from 2.15% for K. pneumoniae in the United Kingdom to 44.4% for A. baumannii in Taiwan (Figure 3) [22]. This is due to the fact that the potential existence of these organisms raises the possibility that improper initial antimicrobial therapy may lead to treatment failures, poor patient outcomes, and increased medical expenses (Table 3). Table 3 underlines the clinical implication of colistin resistance. Overuse of empirical broad-spectrum antibiotics poses a significant risk of antimicrobial drug insusceptibility, potentially leading to unfavorable patient outcomes [22]. It is crucial to promptly administer optimal antimicrobial therapy to hospitalized patients with acute infections to achieve favorable outcomes and minimize the risk of resistance development, thereby reducing morbidity and mortality. The use of colistin increased significantly in the late 1980s among patients with ventilator-associated pneumonia, convulsions, chemical meningitis, bacteremia, multidrug-resistant GNB, cystic fibrosis, and chemical ventriculitis. This underscores the significance of using antibiotics sparingly when treating a variety of clinical conditions [27,28,29].
4. Epidemiology
Colistin insusceptibility has emerged in a number of nations (Table 4) across the world (Figure 4) as a result of the increased utilization of colistin for MDR-GNB infections. The colistin susceptibility of multidrug-resistant A. baumannii from the Western Pacific region was investigated in 2008 as part of the SENTRY antimicrobial surveillance program. The results showed that, with the exception of one isolate, which had a MIC of 128 mg/L, all of the isolates were extremely multi-resistant and had colistin MICs of 0.5–2 mg/L [2,33]. Prevalence of colistin resistance in different countries (Table 5) and in different states in India (Table 6) further indicates raising concern for drug resistant strains.
4.1. American Countries
Resistance rates for A. baumannii and P. aeruginosa are less than 5.5% of data from the USA, however resistance rates for K. pneumoniae are greater. Despite combining oral ciprofloxacin and nebulized colistin-methate sodium, Denmark has not seen the development of colistin insusceptibility in multidrug-resistant P. aeruginosa [58]. In 2007–2008, colistin shown efficacy (MIC90, ~2 mg/L) against a range of Gram-negative bacilli in Canadian hospitals, with MDR P. aeruginosa remaining sensitive [59]. Four percent of the isolates in an Argentine ICU, mostly from clones I and III, had colistin hetero-resistance. P. aeruginosa and A. baumannii resistance rates reach 9% in South America. In Band et al. study 69.2% colistin insusceptibility in 2021 was discovered in United states alone [59].
4.2. European Countries
The prevalence of colistin resistance varies greatly throughout Europe, as several studies have shown worrying patterns. 97% of P. aeruginosa isolates in the UK were found to be colistin-sensitive [59], while 3.1% were resistant, according to a survey of CF patients. 19.1% of A. baumannii isolates in Spain tested positive for colistin using the broth microdilution technique and the E-test. Resistance rates of 17% for Klebsiella spp. and 11% for E. Coli were recorded in Romania [60]. 36.1% of carbapenem-resistant K. pneumoniae isolates were found to be colistin-resistant in a Rome, Italy study, which was associated with higher medication use. Colistin-resistant K. pneumoniae increased from 1% in Greece in 2005 to 19% in 2008 [61]. Data from Hungary in 2008–2009 showed that isolates of K. pneumoniae with several resistance genes had a high level of colistin insusceptibility. Furthermore, epidemiological research conducted in Europe have reported a substantial use of colistin in animal health [62].
4.3. African Countries
Resistant rates to colistin were found to be fewer than 10% in studies from South Africa and less than 10% in those from Nigeria. 121 strains of Enterobacteriaceae resistant to colistin were recovered from 93 individuals by Mezghani Maalej et al. of Tunisia in retrospective research. According to the study, the percentage of E. coli, K. pneumoniae, and E. cloacae that were resistant to colistin varied from 0.09% to 1.2% and 1.5% respectively [63]. Yet cumulative data for P. aeruginosa from two distinct institutions in Zimbabwe revealed 53% resistance rates [64].
4.4. Asian Countries
Studies carried out in the Asia-Pacific region demonstrate that different Enterobacter species and Klebsiella species have different prevalence of colistin insusceptibility, with hetero-resistance patterns being prevalent. 0.3% of Klebsiella species and 21% of Enterobacter species were found to be resistant to colistin; resistance rates varied from 13.8% in India to 50% in the Philippines [33,65,66]. All strains of Acinetobacter and E. coli in Singapore remained susceptible to colistin, whereas 30% of P. aeruginosa isolates showed resistance to the antibiotic. According to a different Chinese investigation, all A. baumannii, A. calcoaceticus complex isolates were vulnerable to polymyxin, although only 8% of them were resistant to carbapenems. In another study done in China by Huang et al., 2020, colistin insusceptibility was 32.7%. In Japan, 7.7 % colistin insusceptibility cases was discovered in 2022, in India colistin resistance percentage was found to be 1.28 %, in Thailand colistin resistance percentage was found to be 3.3% alone further rising the concern for antimicrobial insusceptibility. [65,67].
5. Surveillance
The recommendation of a phenotypic screening method (Figure 5) for colistin resistance identification in a resource-constrained situation is challenging. Figure 5 explains about surveillance methods for colistin resistance with various methods in clinical and environmental settings like phenotypic testing, genotypic testing, research and development related to new therapeutics, multinational collaboration, development of rapid diagnostic tools. In order to handle the technicalities of colistin susceptibility testing with standard controls and procedures to monitor the environmental samples and food-producing animals, there should be at least one standard surveillance laboratory at the national level (Table 7). Table 7 highlights the various surveillance methods for colistin resistance. Effective identification of MCR-mediated colistin insusceptibility necessitates a multimodal strategy that combines selective agar plates such as COL-APSE or CHROMID® Colistin R agar with PCR-based methods for MCR gene identification. Innovations in rapid culture-based testing are essential to accelerating identification procedures. To increase colistin resistance testing throughput, accuracy, and speed, improved automated AST systems are necessary. As a timely and accurate detection approach, the Rapid Polymyxin NP test shows promise in reliably differentiating between susceptible and resistant strains [68]. Innovations in rapid, culture-based testing are essential for accelerating identification procedures, especially in settings with limited resources. Improved automated AST systems are also necessary to increase throughput, accuracy, and speed in colistin resistance testing like VITEK 2. The Rapid Polymyxin NP test has emerged as a promising tool for the timely and accurate detection of colistin insusceptibility, reliably differentiating between susceptible and resistant strains. This method could be particularly beneficial in resource-constrained environments where rapid decision-making is crucial [69].
Global health organizations play a vital role in standardizing surveillance and reporting methods for colistin insusceptibility. By providing guidelines, training, and support, these organizations can help ensure that monitoring programs are consistent, accurate, and effective across different regions. Standardized reporting methods would facilitate the comparison of data on a global scale, enabling better tracking of colistin resistance patterns and more collaborative responses. In resource-limited settings, international collaborations and support from global health organizations are essential for building capacity, providing necessary resources, and ensuring that even the most constrained environments can contribute to the global effort to monitor and combat colistin insusceptibility. Consideration of recent advancements in genome-based rapid detection tools could further revolutionize colistin resistance diagnostics. These methods leverage next-generation sequencing and other molecular approaches to rapidly and accurately detect resistance genes [70]. However, their implementation in resource-limited settings poses challenges, such as high costs, the need for specialized training, and infrastructure requirements. Addressing these barriers is vital to ensuring global applicability and impact. International collaborations and capacity-building initiatives, supported by global health organizations, could facilitate the adoption of these technologies even in constrained environments. By overcoming these hurdles, genome-based tools could significantly enhance the precision and efficiency of colistin resistance surveillance, contributing to a more coordinated global response.
5.1. The initial Screening Process Using Selective Culture Medium
Novel selective culture media, like chromogenic variants, are pivotal in clinical microbiology, especially for detecting infections in high-risk groups such as recent hospital admissions or those with antibiotic exposure. These media aid in implementing tailored infection control measures and hold promise for community-acquired infections pending further validation. Additionally, their application extends to veterinary surveillance, where screening for antibiotic resistance in animal bacteria is becoming imperative. The advent of Super Polymyxin selective medium showcases significant advancements in identifying polymyxin-resistant gram-negative isolates with high sensitivity and specificity, facilitating prompt and accurate diagnosis for optimized treatment strategies [71,72,73].
5.2. Automated AST, Antibiotic Gradient Testing, and Disk Diffusion Assays
The limitations of disk diffusion and gradient testing for colistin insusceptibility highlight the need for rapid, reproducible culture-based Antimicrobial Susceptibility Testing (AST). Broth microdilution (BMD) is currently the most accurate method, but it's time-consuming [74]. Accurate colistin Minimum Inhibitory Concentration (MIC) testing is crucial due to its significant side effects. A cost-effective and globally applicable solution is the colorimetric test, providing quick results within four hours, crucial for timely treatment decisions, especially in cases of bacteraemia and sepsis amidst multidrug insusceptibility challenges [74]. The importance of rapid phenotypic test confirmation of resistance has been highlighted by Jayol et al., especially if it can be carried out straight from blood culture broth instantaneously and enable early antimicrobial medication adaptation in the event of multidrug insusceptibility [75].
5.3. Molecular Diagnostics
While MALDI-TOF MS shows potential for identifying specific proteins, directly detecting the MCR protein still remains elusive. Advancements in Mass Spectroscopy technology may enable future tests to find out enzymatic activity or altered LPS molecules [73]. However, pinpointing resistance via LPS-modifying enzymes poses challenges, as resistance can stem from subtle alterations. Molecular identification of MCR-like genes via PCR is straightforward, aided by rapid real-time techniques [76]. Yet, complete diagnosis may be hindered by co-occurring resistance mechanisms, including amino acid changes in regulatory proteins. Connecting mutations to susceptibility alterations requires extensive sequencing, highlighting the complexity of resistance detection [77].
6. Combating
In acute care and hospital settings, strict infection control protocols are vital to curb the spread of MDR GNB. This involves promptly identifying resistant infections, educating healthcare staff on hand hygiene, and adhering to Clinical and laboratory standards institute (CLSI) standards for early resistance detection. Surveillance cultures should be conducted regularly until no new cases emerge, with prompt notification to infection control specialists upon detection of resistant organisms. Robust antimicrobial stewardship programs are crucial for effective therapy, optimizing antibiotic regimens and reducing hospital stays through quicker positive blood culture notifications and timely medication administration [78].
6.1. Colistin Combination Therapy
It is necessary to combine colistin with other antibiotics due to the growing resistance to it. Colistin and other medications can work in synergy, according to studies. Sorli et al.'s study, for instance, demonstrated that imipenem and colistin worked synergistically to combat K. pneumoniae, but only 11% of isolates that were resistant to colistin exhibited this synergy. Colistin-heteroresistant bacteria frequently arise with colistin-only treatment. 22 patients with MDR A. baumannii pneumonia received intravenous treatment with colistin and rifampicin in another trial by Bassetti et al.; the patients had good results with few side effects [79].
Similarly, Song et al. studied ten patients suffering from ventilator-associated pneumonia treated with colistin and rifampicin, demonstrating the safety and efficacy of combination therapy. While reports on the efficacy of combination therapy versus monotherapy have been conflicting, some studies have shown a higher clinical cure rate and microbiological eradication rate with combination therapy, though not statistically significant [80]. Data indicate that combinations of ciprofloxacin, piperacillin, aztreonam, imipenem, rifampicin, and arbekacin are both safe and effective, with colistin and rifampicin demonstrating the highest synergy. Additionally, combinations containing tigecycline, carbapenems, and gentamicin have shown varying degrees of synergy. While colistin and vancomycin together significantly increase the risk of renal failure in critically sick patients with carbapenem-resistant A. baumannii infections, the clinical outcomes are comparable whether vancomycin is used or not [81,82].
6.2. One Health Perspective
The overuse of antibiotics in the human, animal, and environmental sectors has led to the urgent worldwide concern known as AMR. The widespread usage of colistin in animal husbandry, especially in China and Southeast Asia, has accelerated the emergence of Enterobacteriaceae resistant to colistin, making the treatment of multidrug-resistant infections more difficult. A multimodal strategy including enhanced antimicrobial policies, surveillance, stewardship, infection control, and sanitation measures is needed to address AMR [83,84]. The need for concerted measures to protect medically important antibiotics is highlighted by international programs like the WHO Global Action Plan on AMR and the US National Action Plan for Combating Antibiotic-Resistant Bacteria. In order to stop the spread of resistant diseases, countries need to strengthen their monitoring capacities. This can be done with the help of the WHO's Global AMR monitoring System (GLASS) [85]. New research from a country in South America emphasizes the value of infection control and stewardship measures in stopping the spread of high-risk clones that cause AMR. Developing comprehensive policies to reduce the deleterious effects of AMR on global health, security, and the economy requires stakeholder engagement [86,87].
7. Future Perspective
Carbapenem-resistant GNB develop colistin resistance through mechanisms like plasmid-mediated LPS modifications and mutations such as LAra4N. Despite its bactericidal action, the exact mechanism of colistin's activity remains unclear, emphasizing the need for further research. Spontaneous insusceptibility raises concerns about its efficacy against multidrug-resistant infections, making it critical to understand and address these resistance mechanisms to prevent widespread dissemination [86]. Fluopsin C, a metal-containing antibiotic from Streptomyces and Pseudomonas species, exhibits potent activity against Gram-negative, and drug-resistant bacteria. Terrein, derived from fungi, is effective against S. aureus, A. hydrophila, and E. faecalis, while ellipticine, known for anticancer properties, shows antibacterial activity against colistin-insusceptibility strain of E. coli. Emerging strategies like repurposing drugs (e.g., niclosamide, PFK-158), CRISPR-based approaches, nanotechnology, and photodynamic therapy (PDT) enhance colistin's efficacy. Phage therapy combined with colistin offers a promising avenue to mitigate insusceptibility and treat multidrug-resistant infections [88].
Future perspectives in colistin insusceptibility research are poised to address the pressing need for effective strategies against multidrug-resistant bacteria (Figure 6). Figure 6 depicts the potential strategies and innovations for future perspectives in colistin resistance research for novel therapeutic approaches like vaccination therapy, antimicrobial peptide, phage therapy, antibody used as drug, synergy treatment. Investigating the molecular mechanisms of colistin resistance is essential to counteracting it. Effective management requires One Health approach that takes into account environmental, animal, and human issues. Thorough surveillance in environmental and clinical contexts can offer important insights into resistance epidemiology and help direct management strategies. Emerging technologies like genomics and bioinformatics are playing a pivotal role in understanding and combating colistin insusceptibility. Genomic sequencing allows for the detailed analysis of resistance mechanisms at a molecular level, enabling the identification of specific genes, such as the MCR gene, responsible for colistin insusceptibility [89]. Bioinformatics tools can analyse vast datasets to track the evolution and spread of resistance genes across different regions and environments. These technologies are crucial for developing targeted interventions and guiding the use of colistin in clinical settings. However, the effective deployment of these tools requires robust policy frameworks and international cooperation.
Role of policy and international cooperation: Policymakers must prioritize investment in these technologies and collaborate globally to share data and standardize approaches to surveillance. International organizations like the WHO play a critical role in coordinating efforts to address antimicrobial resistance, ensuring that resources and knowledge are shared across borders to combat this global health threat [90].
7.1. Contemporary Instruments for Quick AMR Diagnosis
Outpatient clinics urgently require rapid and decentralized diagnostics to mitigate antibiotic overuse, a pressing issue at present. It's imperative to swiftly identify the causative pathogen, differentiate between bacterial and viral infections, detect microbial antibiotic resistance, and ascertain the most suitable antimicrobial treatment. By doing so, the over prescription of antibiotics can be minimized, and the emergence of antibiotic insusceptibility more effectively managed [91].
Global health threats in the twenty-first century are deemed to be greatest by the WHO, who calls for immediate response. For resistance testing, prompt diagnosis is essential, particularly in areas with high AMR rates. The current AST standards require the assessment of antimicrobial effectiveness using pure culture isolates; nevertheless, it might be difficult to differentiate between benign and dangerous species. Misuse of empirical treatment continues despite advancements in diagnosis [92].
7.2. Available Technologies for Rapid AST
Though labour-intensive stages like enrichment cultures and pure culture separation are frequently needed, several approaches promise fast AST within minutes or hours. In theory, non-purified polymicrobial samples might be used with Nucleic Acid Amplification Tests (NAAT) based techniques, nucleic acid hybridization, or immunodiagnostics. NAAT can be used to determine MIC and detect AR after a brief antibiotic culture. Some very sensitive immunodiagnostics track growth in real time, but most quick AST techniques rely on endpoint analysis. Clinical studies using biosensor technology for motility, thermal changes, or microbial metabolism are, nevertheless, scarce. Outpatient clinics have limited access to inexpensive, dependable, quick, and easy-to-use AST devices [93].
7.3. NAAT
Aided by diagnostic panels from firms such as BioMérieux, Elitech, and Qiagen, which may detect specific AR genes, while their presence alone does not always suggest insusceptibility, NAAT are particularly successful in syndromic detection of infections. NAAT is unable to provide treatment plans or establish MICs, but it can update for new resistance indicators. MIC values can be estimated by qPCR and qRT-PCR, but the latter is still expensive. Enrichment cultures and nucleic acid purification are frequently required for precise identification, reducing impurities and template loss. While advances like T2Biosystems' magnetic resonance panel and molecular beacons in real-time PCR highlight important advancements in resistance gene detection from blood, DNA array hybridization improves sensitivity and specificity [94].
7.4. Whole Genome Sequencing
WGS has progressed to a stage where it serves as a viable method for identifying pathogens and determining AST. Third-generation sequencing platforms capable of swiftly providing reasonably long reads include the Oxford Nanopore MiniON and PromethION, the Illumina MiniSeq, and the PacBio Sequel system from Pacific Biosciences. WGS holds the promise of simultaneously offering rapid pathogen identification, epidemiological typing, and detection of medication susceptibility genes. However, interpreting WGS results, which yield a vast amount of fragmented data, necessitates sophisticated algorithms [95].
The European Committee for Antimicrobial Susceptibility Testing assessed WGS's potential for AST in 2017. Since there is currently not enough information to use WGS as an AST tool for most bacteria, they came to the conclusion that it is not appropriate for clinical decision-making. To make system and bioinformatics tool comparisons easier, they emphasized the vital requirement for a single database that contains all known resistance genes and mutations [96].
8. Discussion
Colistin, a treatment for MDR infections of gram-negative bacteria, is increasingly facing resistance due to both chromosomal mutations and plasmid-borne MCR genes [97]. The growing prevalence of colistin insusceptibility is particularly concerning given its vital role in treating severe infections where other antibiotics fail. The mechanisms driving this resistance, the clinical implications, and the global efforts to combat its spread represent significant challenges for healthcare systems worldwide. This review delves into the current understanding of colistin resistance and the multidimensional strategies necessary to mitigate its impact on global health [98].
Colistin insusceptibility arises from two primary mechanisms; chromosomal mutations and plasmid-mediated resistance genes. Chromosomal mutations, especially those affecting the bacterial outer membrane’s lipid A component, alter the binding affinity of colistin, rendering it less effective like a study which highlights the emerging colistin resistance in A. baumannii isolates from ICU patients in Bhubaneswar, India, with 7% showing resistance. The findings emphasize the urgent need for continuous surveillance and alternative treatment strategies to combat multidrug-resistant infections [99]. These mutations modify the lipid A structure by adding molecules such as phosphoethanolamine (pEtN), which reduces the drug's ability to interact with the bacterial cell membrane d-mediated resistance, driven by MCR genes (MCR-1 through MCR-10), poses a particularly significant threat due to its potential for horizontal gene transfer between bacterial species [100]. MCR-1, the most extensively studied gene, was first discovered in E. coli isolates from food animals in China in 2015 has been detected in human clinical isolates, environmental samples, and various animal species across the globe. MCR-1 encodes a pEtN transferase enzyme that modifies lipid A, similarly to chromosomal mutations, and reduces colistin’s bactericidal activity [101]. The discovery of additional MCR variants (MCR-2 through MCR-10) indicates that colistin resistance is evolving rapidly, compounding the complexity of controlling its spread [102].
Colistin-resistant infections are associated with increased morbidity and mortality, particularly in critically ill patients. Infections caused by strains such as carbapenem-resistant Enterobacteriaceae (CRE) and A. baumannii lead to higher rates of treatment failure, prolonged hospital stays, and the necessity for more toxic or less effective antibiotics. Studies indicate that mortality rate with colistin-resistant infections can exceed 40%, especially when alternative therapeutic options are limited [88].
The rise of colistin-resistant immense pressure on healthcare systems, particularly in resource-limited settings where diagnostic capabilities and access to alternative treatments are constrained [103]. Clinicians often resort to combination therapies, pairing colistin with other antibiotics like carbapenems or tigecycline, in an attempt to overcome resistance. However, the effectiveness of such regimens is in consideration have shown no significant improvement in patient outcomes. Moreover, the nephrotoxicity associated with colistin use further complicates in critically ill patients, necessitating careful monitoring and dose adjustments [104].
Colistin insusceptibility is a global phenomenon, with valence across different regions. In Europe, resistance rates among K. pneumoniae isolates range from 3.1% in the United Kingdom to as high as 19% in Greece [105]. In the United States, recent studies have reported resistance rates as high as 13.4% among carbapenem-resistant strains. In Asia, colistin insusceptibility is particularly concerning in countries like China, where the increased use of colistin in agriculture, facilitated the emergence and dissemination of MCR genes [106].
The spread of colistin insusceptibility in low- and middle-income countries is further exacerbated by the misuse of antibiotics in the clinical settings. In countries where colistin is still used as a growth promoter in animal husbandry, the risk of transmission from animals to humans is significant, which integrates human, animal, and environmental health, is critical in addressing this issue. Effective surveillance and strict regularization in agriculture are essential for curbing the spread of resistance [107].
The detection of colistin insusceptibility in clinical settings remains a challenge. Current diagnostic methods, such as broth microdilution, a resource-intensive, making them less suitable for routine use in many laboratories. Newer methods, such as the Rapid Polymyxin NP test, offer promise for faster detection of colistin resistance, allowing for more timely interventions [108]. However, these tests are not yet widely available, co-limited settings where colistin insusceptibility is most prevalent.
Global surveillance efforts, such as those led by the World Health Organization (WHO) in tracking the spread of colistin insusceptibility. The WHO GLASS has provided a framework for standardized data collection, helping to identify hotspots of resistance and inform public health interventions [109]. However, more comprehensive surveillance systems are needed, particularly in low-income countries where the burden of antimicrobial insusceptibility is highest.
Antimicrobial stewardship containing programs play a crucial role in reducing the inappropriate use of antibiotics, in programs emphasize the need for judicious antibiotic use, ensuring that colistin is reserved for cases where no other therapeutic options are available. Infection control measures, such as stringent hand hygiene practices and environmental cleaning protocols, are also essential in preventing the spread of resistant organisms in healthcare settings [110].
In addition to stewardship and infection control, advance treatments are urgently needed for MDR bacterial infectious diseases. Novel antibiotics targeting colistin-resistant bacteria are in development, but their clinical availability is still several years away. In the meantime, combination involving colistin and other antibiotics, such as rifampicin, have shown promise in some studies, although their efficacy is not guaranteed [111]. Nanotechnology and PDT also offer potential as adjunctive treatments, enhanced activity and reducing the likelihood of resistance [112].
Finally, the development of rapid diagnostic tools and molecular assays for detecting MCR genes is critical for early determinant of colistin-resistant infections. Whole genome sequencing (WGS) has emerged as a powerful tool for tracking the evolution and spread of resistance genes, offering insights the mechanisms underlying colistin insusceptibility and guiding public health interventions [112].
9. Conclusion
The rapid rise of colistin insusceptibility in gram negative bacteria represents a significant public health challenge, demanding immediate and integrated effort. As recent research reveals, the mechanisms behind colistin resistance are complex, involving both chromosomal mutations and plasmid-mediated genes, complicating efforts to combat this threat. Clinically, the emergence of colistin insusceptibility drastically limits treatment options for infections caused by multidrug-resistant organisms, underscoring the need for alternative therapeutic strategies. Future studies should prioritize understanding resistance dynamics, developing rapid diagnostics, exploring combination therapies, and assessing environmental factors influencing resistance. Vigilant global surveillance is crucial for early detection and containment, while a comprehensive approach that includes antimicrobial stewardship, stringent infection control, and the development of novel treatments such as combination therapy is essential. The gravity of this issue necessitates a concerted effort from researchers, clinicians, and policymakers to invest in further research, develop rapid diagnostic tools, and implement effective strategies to curb the spread of colistin insusceptibility and safeguard the efficacy of antibiotics for future generations.
Acknowledgments
This work was supported by Centre for Biotechnology, Siksha ‘O’ Anusandhan Deemed to be university, Bhubaneswar. Author is thankful to Dean Research, SOA University and Director, ICMR-RMRC, Bhubaneswar for extend facility in research.
Credit Authorship statement
Dr. Mahesh Chandra Sahu developed the concept of review article and Miss. Shreya Singh wrote the article and Dr. Rajesh Kumar Sahoo read and corrected the manuscript.
Funding
None.
Availability of data and materials
Not applicable.
Ethics approval and consent to participate:
Not applicable.
Consent for publication
All authors consented to submission and publication of the manuscript.
Competing interests
The authors declare that they have no competing interests.
Author details:
1Centre for Biotechnology, Siksha ‘O’ Anusandhan Deemed to be University, Kalinganagar, Bhubaneswar-751003, Odisha, India; 2Department of Microbiology, Odisha University of Agriculture and Technology, Suryanagar, Bhubaneswar-751003, Odisha, India; b Division of Microbiology, ICMR -Regional Medical Research Centre, Chandrasekharpur, Bhubaneswar, India.
Abbreviation
- GNB: Gram negative bacteria
- MCR: Mobilised colistin resistance
- MDR: Multidrug Resistance
- WHO: World Health Organization
- AMR: Antimicrobial resistance
- KPC: Klebsiella pneumoniae carbapenemase
- LOS: longer hospital stays
- IDSA: Infectious Diseases Society of America
- NDM: New Delhi metallo-β-lactamase
- AST: Antimicrobial susceptibility testing
- MIC: Minimum Inhibitory Concentration
- ICU: Intensive Care Unit
- MALDI-TOF MS: Matrix-assisted laser desorption/ionization time-of-flight mass spectrometry
- LPS: Lipopolysaccharide
- EUCAST: European Committee on Antimicrobial Susceptibility Testing
- BMD: Broth microdilution
- GLASS: Global Antimicrobial Resistance Surveillance System
- FISH: Fluorescence In Situ Hybridization
- NAAT: Nucleic Acid Amplification Technology
- PDT: Photodynamic therapy
- CLSI: Clinical and laboratory standards institute
- WGS: Whole Genome Sequencing
- ABCR: A. baumanii resistant to colistin
- ABCS: A. baumanii sensitive to colistin
- MDR UTI: Multidrug-resistant Urinary tract infection
References
- Lim, L.M.; Ly, N.; Anderson, D.; Yang, J.C.; Macander, L.; Jarkowski III, A.; Forrest, A.; Bulitta, J.B.; Tsuji, B.T. Resurgence of colistin: a review of resistance, toxicity, pharmacodynamics, and dosing. Pharmacotherapy: The Journal of Human Pharmacology and Drug Therapy 2010, 30, 1279–1291. [Google Scholar] [CrossRef] [PubMed]
- Bialvaei, A.Z.; Samadi Kafil, H. Colistin, mechanisms and prevalence of resistance. Current medical research and opinion 2015, 31, 707–721. [Google Scholar] [CrossRef] [PubMed]
- Hussein, N.H.; Al-Kadmy, I.M.; Taha, B.M.; Hussein, J.D. Mobilized colistin resistance (mcr) genes from 1 to 10: a comprehensive review. Molecular biology reports 2021, 48, 2897–2907. [Google Scholar] [CrossRef]
- Wozniak, T.M.; Barnsbee, L.; Lee, X.J.; Pacella, R.E. Using the best available data to estimate the cost of antimicrobial resistance: a systematic review. Antimicrobial Resistance & Infection Control 2019, 8, 1–12. [Google Scholar] [CrossRef]
- Kasiakou, S.K.; Michalopoulos, A.; Soteriades, E.S.; Samonis, G.; Sermaides, G.J.; Falagas, M.E. Combination therapy with intravenous colistin for management of infections due to multidrug-resistant Gram-negative bacteria in patients without cystic fibrosis. Antimicrobial agents and chemotherapy 2005, 49, 3136–3146. [Google Scholar] [CrossRef]
- America, I.D.S.o. Combating antimicrobial resistance: policy recommendations to save lives. Clinical Infectious Diseases 2011, 52, S397–S428. [Google Scholar] [CrossRef]
- Nation, R.L.; Velkov, T.; Li, J. Colistin and polymyxin B: peas in a pod, or chalk and cheese? Clinical infectious diseases 2014, 59, 88–94. [Google Scholar] [CrossRef]
- Velkov, T.; Thompson, P.E.; Nation, R.L.; Li, J. Structure− activity relationships of polymyxin antibiotics. Journal of medicinal chemistry 2010, 53, 1898–1916. [Google Scholar] [CrossRef]
- Gelbicova, T.; Kolackova, I.; Krutova, M.; Karpiskova, R. The emergence of mcr-1-mediated colistin-resistant Escherichia coli and Klebsiella pneumoniae in domestic and imported turkey meat in the Czech Republic 2017–2018. Folia Microbiologica 2020, 65, 211–216. [Google Scholar] [CrossRef]
- Ilbeigi, K.; Askari Badouei, M.; Vaezi, H.; Zaheri, H.; Aghasharif, S.; Kafshdouzan, K. Molecular survey of mcr1 and mcr2 plasmid mediated colistin resistance genes in Escherichia coli isolates of animal origin in Iran. BMC Research Notes 2021, 14, 1–5. [Google Scholar] [CrossRef]
- Xavier, B.B.; Lammens, C.; Ruhal, R.; Kumar-Singh, S.; Butaye, P.; Goossens, H.; Malhotra-Kumar, S. Identification of a novel plasmid-mediated colistin-resistance gene, mcr-2, in Escherichia coli, Belgium, June 2016. Eurosurveillance 2016, 21, 30280. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Chen, L.; Wang, J.; Butaye, P.; Huang, K.; Qiu, H.; Zhang, X.; Gong, W.; Wang, C. Molecular detection of colistin resistance genes (mcr-1 to mcr-5) in human vaginal swabs. BMC Research Notes 2018, 11, 1–4. [Google Scholar] [CrossRef] [PubMed]
- Xu, Y.; Chen, H.; Zhang, H.; Ullah, S.; Hou, T.; Feng, Y. The MCR-3 inside linker appears as a facilitator of colistin resistance. Cell Reports 2021, 35. [Google Scholar] [CrossRef] [PubMed]
- Furlan, J.P.R.; dos Santos, L.D.R.; Ramos, M.S.; Gallo, I.F.L.; Stehling, E.G. Presence of colistin resistance mcr-4 gene and clinically relevant antimicrobial resistance genes in sand samples from a public beach. Water, Air, & Soil Pollution 2020, 231, 1–6. [Google Scholar] [CrossRef]
- Cherak, Z.; Loucif, L.; Ben Khedher, M.; Moussi, A.; Benbouza, A.; Baron, S.A.; Rolain, J.-M. MCR-5-producing colistin-resistant Cupriavidus gilardii strain from well water in Batna, Algeria. Msphere 2021, 6. [Google Scholar] [CrossRef]
- Borowiak, M.; Fischer, J.; Hammerl, J.A.; Hendriksen, R.S.; Szabo, I.; Malorny, B. Identification of a novel transposon-associated phosphoethanolamine transferase gene, mcr-5, conferring colistin resistance in d-tartrate fermenting Salmonella enterica subsp. enterica serovar Paratyphi B. Journal of Antimicrobial Chemotherapy 2017, 72, 3317–3324. [Google Scholar] [CrossRef]
- Borowiak, M.; Baumann, B.; Fischer, J.; Thomas, K.; Deneke, C.; Hammerl, J.A.; Szabo, I.; Malorny, B. Development of a novel mcr-6 to mcr-9 multiplex PCR and assessment of mcr-1 to mcr-9 occurrence in colistin-resistant Salmonella enterica isolates from environment, feed, animals and food (2011–2018) in Germany. Frontiers in microbiology 2020, 11, 80. [Google Scholar] [CrossRef]
- Yang, Y.-Q.; Li, Y.-X.; Lei, C.-W.; Zhang, A.-Y.; Wang, H.-N. Novel plasmid-mediated colistin resistance gene mcr-7.1 in Klebsiella pneumoniae. Journal of Antimicrobial Chemotherapy 2018, 73, 1791–1795. [Google Scholar] [CrossRef]
- Wang, X.; Wang, Y.; Zhou, Y.; Li, J.; Yin, W.; Wang, S.; Zhang, S.; Shen, J.; Shen, Z.; Wang, Y. Emergence of a novel mobile colistin resistance gene, mcr-8, in NDM-producing Klebsiella pneumoniae. Emerging microbes & infections 2018, 7, 1–9. [Google Scholar] [CrossRef]
- Carroll, L.M.; Gaballa, A.; Guldimann, C.; Sullivan, G.; Henderson, L.O.; Wiedmann, M. Identification of novel mobilized colistin resistance gene mcr-9 in a multidrug-resistant, colistin-susceptible Salmonella enterica serotype Typhimurium isolate. MBio 2019, 10. [Google Scholar] [CrossRef]
- Wang, C.; Feng, Y.; Liu, L.; Wei, L.; Kang, M.; Zong, Z. Identification of novel mobile colistin resistance gene mcr-10. Emerging microbes & infections 2020, 9, 508–516. [Google Scholar] [CrossRef]
- Kollef, M.H.; Golan, Y.; Micek, S.T.; Shorr, A.F.; Restrepo, M.I. Appraising contemporary strategies to combat multidrug resistant gram-negative bacterial infections–proceedings and data from the Gram-Negative Resistance Summit. Clinical infectious diseases 2011, 53, S33–S55. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y.-T.; Sun, J.-R.; Wang, Y.-C.; Chiu, C.-H.; Kuo, S.-C.; Chen, T.-L.; Yang, Y.-S.; Group, A.S. Multicentre study of risk factors for mortality in patients with Acinetobacter bacteraemia receiving colistin treatment. International journal of antimicrobial agents 2020, 55, 105956. [Google Scholar] [CrossRef]
- Balkhair, A.; Al Saadi, K.; Al Adawi, B. Epidemiology and mortality outcome of carbapenem-and colistin-resistant Klebsiella pneumoniae, Escherichia coli, Acinetobacter baumannii, and Pseudomonas aeruginosa bloodstream infections. IJID regions 2023, 7, 1–5. [Google Scholar] [CrossRef]
- Mantzarlis, K.; Makris, D.; Zakynthinos, E. Risk factors for the first episode of Acinetobacter baumannii resistant to colistin infection and outcome in critically ill patients. Journal of Medical Microbiology 2020, 69, 35–40. [Google Scholar] [CrossRef]
- Ejaz, H.; Younas, S.; Qamar, M.U.; Junaid, K.; Abdalla, A.E.; Abosalif, K.O.A.; Alameen, A.A.M.; Elamir, M.Y.M.; Ahmad, N.; Hamam, S.S.M. Molecular epidemiology of extensively drug-resistant mcr encoded colistin-resistant bacterial strains co-expressing multifarious β-lactamases. Antibiotics 2021, 10, 467. [Google Scholar] [CrossRef]
- Landman, D.; Georgescu, C.; Martin, D.A.; Quale, J. Polymyxins revisited. Clinical microbiology reviews 2008, 21, 449–465. [Google Scholar] [CrossRef]
- Shen, Z.; Wang, Y.; Shen, Y.; Shen, J.; Wu, C. Early emergence of mcr-1 in Escherichia coli from food-producing animals. The Lancet infectious diseases 2016, 16, 293. [Google Scholar] [CrossRef]
- Bargiacchi, O.; Rossati, A.; Car, P.; Brustia, D.; Brondolo, R.; Rosa, F.; Garavelli, P.; De Rosa, F.G. Intrathecal/intraventricular colistin in external ventricular device-related infections by multi-drug resistant Gram negative bacteria: case reports and review. Infection 2014, 42, 801–809. [Google Scholar] [CrossRef]
- Coates, A.R.; Hu, Y.; Holt, J.; Yeh, P. Antibiotic combination therapy against resistant bacterial infections: synergy, rejuvenation and resistance reduction. Expert review of Anti-infective therapy 2020, 18, 5–15. [Google Scholar] [CrossRef]
- Sorlí, L.; Luque, S.; Li, J.; Campillo, N.; Danés, M.; Montero, M.; Segura, C.; Grau, S.; Horcajada, J.P. Colistin for the treatment of urinary tract infections caused by extremely drug-resistant Pseudomonas aeruginosa: dose is critical. Journal of Infection 2019, 79, 253–261. [Google Scholar] [CrossRef] [PubMed]
- Aydın, M.; Ergönül, Ö.; Azap, A.; Bilgin, H.; Aydın, G.; Çavuş, S.; Demiroğlu, Y.; Alışkan, H.; Memikoğlu, O.; Menekşe, Ş. Rapid emergence of colistin resistance and its impact on fatality among healthcare-associated infections. Journal of Hospital Infection 2018, 98, 260–263. [Google Scholar] [CrossRef] [PubMed]
- Yau, W.; Owen, R.J.; Poudyal, A.; Bell, J.M.; Turnidge, J.D.; Heidi, H.Y.; Nation, R.L.; Li, J. Colistin hetero-resistance in multidrug-resistant Acinetobacter baumannii clinical isolates from the Western Pacific region in the SENTRY antimicrobial surveillance programme. Journal of Infection 2009, 58, 138–144. [Google Scholar] [CrossRef]
- Band, V.I.; Satola, S.W.; Smith, R.D.; Hufnagel, D.A.; Bower, C.; Conley, A.B.; Rishishwar, L.; Dale, S.E.; Hardy, D.J.; Vargas, R.L. Colistin heteroresistance is largely undetected among carbapenem-resistant Enterobacterales in the United States. MBio 2021, 12. [Google Scholar] [CrossRef]
- Huang, H.; Dong, N.; Shu, L.; Lu, J.; Sun, Q.; Chan, E.W.-C.; Chen, S.; Zhang, R. Colistin-resistance gene mcr in clinical carbapenem-resistant Enterobacteriaceae strains in China, 2014–2019. Emerging microbes & infections 2020, 9, 237–245. [Google Scholar] [CrossRef]
- Sodhi, K.; Mittal, V.; Arya, M.; Kumar, M.; Phillips, A.; Kajla, B. Pattern of colistin resistance in Klebsiella isolates in an Intensive Care Unit of a tertiary care hospital in India. Journal of Infection and Public Health 2020, 13, 1018–1021. [Google Scholar] [CrossRef]
- Kawamoto, Y.; Kaku, N.; Akamatsu, N.; Sakamoto, K.; Kosai, K.; Morinaga, Y.; Ohmagari, N.; Izumikawa, K.; Yamamoto, Y.; Mikamo, H. The surveillance of colistin resistance and mobilized colistin resistance genes in multidrug-resistant Enterobacteriaceae isolated in Japan. International Journal of Antimicrobial Agents 2022, 59, 106480. [Google Scholar] [CrossRef]
- Luk-In, S.; Chatsuwan, T.; Kueakulpattana, N.; Rirerm, U.; Wannigama, D.L.; Plongla, R.; Lawung, R.; Pulsrikarn, C.; Chantaroj, S.; Chaichana, P. Occurrence of mcr-mediated colistin resistance in Salmonella clinical isolates in Thailand. Scientific Reports 2021, 11, 14170. [Google Scholar] [CrossRef]
- Cheong, H.S.; Kim, S.Y.; Seo, J.; Wi, Y.M.; Peck, K.R.; Ko, K.S. Colistin resistance and extensive genetic variations in PmrAB and PhoPQ in Klebsiella pneumoniae isolates from South Korea. Current microbiology 2020, 77, 2307–2311. [Google Scholar] [CrossRef]
- Makarov, D.A.; Ivanova, O.E.; Karabanov, S.Y.; Gergel, M.A.; Pomazkova, A.V. Antimicrobial resistance of commensal Escherichia coli from food-producing animals in Russia. Veterinary World 2020, 13, 2053. [Google Scholar] [CrossRef]
- Bir, R.; Gautam, H.; Arif, N.; Chakravarti, P.; Verma, J.; Banerjee, S.; Tyagi, S.; Mohapatra, S.; Sood, S.; Dhawan, B. Analysis of colistin resistance in carbapenem-resistant Enterobacterales and XDR Klebsiella pneumoniae. Therapeutic Advances in Infectious Disease 2022, 9, 20. [Google Scholar] [CrossRef] [PubMed]
- Manohar, P.; Shanthini, T.; Ayyanar, R.; Bozdogan, B.; Wilson, A.; Tamhankar, A.J.; Nachimuthu, R.; Lopes, B.S. The distribution of carbapenem-and colistin-resistance in Gram-negative bacteria from the Tamil Nadu region in India. Journal of medical microbiology 2017, 66, 874–883. [Google Scholar] [CrossRef] [PubMed]
- Reddy, B.R.C.; Geetha, R.; Singh, M.; Rani, R.U.; Nekkanti, K.N. Mcr-1 expression in progression of colistin resistance gram negative bacilli of clinical specimens derived from Intensive Care Units, wards and hospital setting of Deccan Eco Region of Southern India. Journal of Pharmaceutical Negative Results 2022, 295–305. [Google Scholar] [CrossRef]
- Sharma, A.; Agrawal, M. Colistin Susceptibility for Carbapenem-Resistan t Gram-Negative Bacilli; Comparative Study of E-test and Vitek 2 Compact™ with Broth Microdilution. Galore International Journal of Health Sciences an d Research 2019, 4, 110–115, P-ISSN: 2456-9321. [Google Scholar]
- Das, S.; Roy, S.; Roy, S.; Goelv, G.; Sinha, S.; Mathur, P.; Walia, K.; Bhattacharya, S. Colistin susceptibility testing of gram-negative bacilli: Better performance of vitek2 system than E-test compared to broth microdilution method as the gold standard test. Indian journal of medical microbiology 2020, 38, 58–65. [Google Scholar] [CrossRef]
- Chakraverti, T.K.; Tripathi, P.C. Prevalence and Antibiotic Resistant Pattern of Pseudomonas aeruginosa at a Tertiary Care Centre of North India. Int. J. Curr. Microbiol. App. Sci 2018, 7, 1061–1069. [Google Scholar] [CrossRef]
- Choudhary, A.K. Isolation prevalence and antimicrobial resistance pattern of pseudomonas aeruginosa from urine samples in a tertiary care hospital udaipur, rajasthan. International Journal of Life Sciences, Biotechnology and Pharma Research, 2023, 12, 3, 2250-3137.
- Satpathy, M.; Sharma, N.; Kaur, P.; Arora, A. Detection of antimicrobial resistance genes in extended spectrum beta-lactamase-producing Escherichia coli from milk of indigenous Beetal goats of Punjab. Iranian Journal of Veterinary Research 2023, 24, 37. [Google Scholar] [CrossRef]
- Malik, S.; Rana, J.S.; Nehra, K. Prevalence and antibiotic susceptibility pattern of uropathogenic Escherichia coli strains in Sonipat region of Haryana in India. Biomedical and Biotechnology Research Journal (BBRJ) 2021, 5, 80–87. [Google Scholar] [CrossRef]
- Rudrapathy, P.; Samuel, S.; Murugesan, S. Microbiological Profile and Antibiotic Resistance of Bloodstream Infections among Cancer Patients at a Tertiary Care Cancer Centre in North Kerala, India. The Hospital 2022, 6, 16. [Google Scholar] [CrossRef]
- Kar, P.; Behera, B.; Mohanty, S.; Jena, J.; Mahapatra, A. Detection of colistin resistance in carbapenem resistant Enterobacteriaceae by reference broth microdilution and comparative evaluation of three other methods. Journal of Laboratory Physicians 2021, 13, 263–269. [Google Scholar] [CrossRef]
- Gupta, M.; Naik, A.K.; Singh, S.K. Bacteriological profile and antimicrobial resistance patterns of burn wound infections in a tertiary care hospital. Heliyon 2019, 5. [Google Scholar] [CrossRef] [PubMed]
- Kumar, R.; Akhtar, N.; Kesharwani, R.; Chandra, P.; Ayub, A. The Antimicrobial Resistance Pattern of pathogens isolated from patients with Health Care Associated Infections in a Tertiary Care Hospital of Chhattisgarh, India. European Journal of Molecular & Clinical Medicine, 2022 9, ISSN 2515-8260.
- Kishore, N.; Kakati, B.; Khanduri, S. Study of colistin and tigecycline sensitivity for carbapenem resistant isolates of klebsiella pneumoniae (crkp) patients in the intensive care unit (icu) of hims, dehradun uttarakhand. Int J Acad Med Pharm 2022, 4, 71–75. [Google Scholar]
- Chauhan, R.; Sharma, P. Phenotypic detection of Metallo-β-lactamase (MBL) producers among multidrug resistant (MDR) strains of P. aeruginosa in Himachal Pradesh. Indian J Basic App Med Res 2013, 3, 303–313. [Google Scholar]
- Samom, P.; Preeti, G.; Laifangbam, S.; Nahakpam, M. Bacteriological Profile Andantibiogram of ICU Isolates in A Tertiary Care Institute in Manipur–A Six-Year Study. BLOOD, 023, 554, 20.47. https://www.ncbi.nlm.nih.gov/nlmcatalog/474373.
- Biswas, U.; Biswas, R.; Samanta, I.; Das, S. Global emergence of mcr-mediated colistin resistance in gram-negative bacteria: focusing the current status in India under one health lens. 2022. [CrossRef]
- Keen III, E.F.; Robinson, B.J.; Hospenthal, D.R.; Aldous, W.K.; Wolf, S.E.; Chung, K.K.; Murray, C.K. Prevalence of multidrug-resistant organisms recovered at a military burn center. Burns 2010, 36, 819–825. [Google Scholar] [CrossRef]
- Falagas, M.E.; Rafailidis, P.I.; Matthaiou, D.K. Resistance to polymyxins: mechanisms, frequency and treatment options. Drug resistance updates 2010, 13, 132–138. [Google Scholar] [CrossRef]
- Li, J.; Nation, R.L.; Turnidge, J.D.; Milne, R.W.; Coulthard, K.; Rayner, C.R.; Paterson, D.L. Colistin: the re-emerging antibiotic for multidrug-resistant Gram-negative bacterial infections. The Lancet infectious diseases 2006, 6, 589–601. [Google Scholar] [CrossRef]
- Walkty, A.; DeCorby, M.; Nichol, K.; Karlowsky, J.; Hoban, D.; Zhanel, G. In vitro activity of colistin (polymyxin E) against 3,480 isolates of gram-negative bacilli obtained from patients in Canadian hospitals in the CANWARD study, 2007-2008. Antimicrobial agents and chemotherapy 2009, 53, 4924–4926. [Google Scholar] [CrossRef]
- Kontopoulou, K.; Protonotariou, E.; Vasilakos, K.; Kriti, M.; Koteli, A.; Antoniadou, E.; Sofianou, D. Hospital outbreak caused by Klebsiella pneumoniae producing KPC-2 β-lactamase resistant to colistin. Journal of Hospital Infection 2010, 76, 70–73. [Google Scholar] [CrossRef]
- Maalej, S.M.; Meziou, M.R.; Mahjoubi, F.; Hammami, A. Epidemiological study of Enterobacteriaceae resistance to colistin in Sfax (Tunisia). Médecine et maladies infectieuses 2012, 42, 256–263. [Google Scholar] [CrossRef]
- Igumbor, E.; Gwanzura, L.; Chirara, M.; Obi, C.; Muza, D. Antibiotic sensitivity and plasmid profiles of Pseudomonas aeruginosa. The Central African Journal of Medicine 2000, 46, 296–300. [Google Scholar] [CrossRef] [PubMed]
- Chen, S.; Hu, F.; Zhang, X.; Xu, X.; Liu, Y.; Zhu, D.; Wang, H. Independent emergence of colistin-resistant Enterobacteriaceae clinical isolates without colistin treatment. Journal of clinical microbiology 2011, 49, 4022–4023. [Google Scholar] [CrossRef] [PubMed]
- Vakili, B.; Fazeli, H.; Shoaei, P.; Yaran, M.; Ataei, B.; Khorvash, F.; Khaleghi, M. Detection of colistin sensitivity in clinical isolates of Acinetobacter baumannii in Iran. Journal of research in medical sciences: the official journal of Isfahan University of Medical Sciences 2014, 19, S67, https://pubmed.ncbi.nlm.nih.gov/25002899/. [Google Scholar] [PubMed]
- Lin, L.; Ling, B.-D.; Li, X.-Z. Distribution of the multidrug efflux pump genes, adeABC, adeDE and adeIJK, and class 1 integron genes in multiple-antimicrobial-resistant clinical isolates of Acinetobacter baumannii–Acinetobacter calcoaceticus complex. International journal of antimicrobial agents 2009, 33, 27–32. [Google Scholar] [CrossRef] [PubMed]
- Ahsan, A.; Gull, S.; Imran, H.; Khan, Z. Mechanistic Insights of Colistin Resistance and Its Public Health Implications. Applied Biochemistry and Microbiology 2023, 59, 597–607. [Google Scholar] [CrossRef]
- Noster, J.; Thelen, P.; Hamprecht, A. Detection of multidrug-resistant Enterobacterales—from ESBLs to carbapenemases. Antibiotics 2021, 10, 1140. [Google Scholar] [CrossRef]
- Feng, J.; Zhuang, Y.; Luo, J.; Xiao, Q.; Wu, Y.; Chen, Y.; Chen, M.; Zhang, X. Prevalence of colistin-resistant mcr-1-positive Escherichia coli isolated from children patients with diarrhoea in Shanghai, 2016–2021. Journal of Global Antimicrobial Resistance 2023, 34, 166–175. [Google Scholar] [CrossRef]
- McGann, P.; Snesrud, E.; Maybank, R.; Corey, B.; Ong, A.C.; Clifford, R.; Hinkle, M.; Whitman, T.; Lesho, E.; Schaecher, K.E. Escherichia coli harboring mcr-1 and bla CTX-M on a novel IncF plasmid: first report of mcr-1 in the United States. Antimicrobial agents and chemotherapy 2016, 60, 4420–4421. [Google Scholar] [CrossRef]
- Nordmann, P.; Jayol, A.; Poirel, L. A universal culture medium for screening polymyxin-resistant Gram-negative isolates. Journal of clinical microbiology 2016, 54, 1395–1399. [Google Scholar] [CrossRef]
- Caniaux, I.; Van Belkum, A.; Zambardi, G.; Poirel, L.; Gros, M. MCR: modern colistin resistance. European Journal of Clinical Microbiology & Infectious Diseases 2017, 36, 415–420. [Google Scholar] [CrossRef]
- Nordmann, P.; Jayol, A.; Poirel, L. Rapid detection of polymyxin resistance in Enterobacteriaceae. Emerging infectious diseases 2016, 22, 1038. [Google Scholar] [CrossRef]
- Jayol, A.; Dubois, V.; Poirel, L.; Nordmann, P. Rapid detection of polymyxin-resistant Enterobacteriaceae from blood cultures. Journal of clinical microbiology 2016, 54, 2273–2277. [Google Scholar] [CrossRef] [PubMed]
- Bontron, S.; Poirel, L.; Nordmann, P. Real-time PCR for detection of plasmid-mediated polymyxin resistance (mcr-1) from cultured bacteria and stools. Journal of Antimicrobial Chemotherapy 2016, 71, 2318–2320. [Google Scholar] [CrossRef] [PubMed]
- Nijhuis, R.; Veldman, K.; Schelfaut, J.; Van Essen-Zandbergen, A.; Wessels, E.; Claas, E.; Gooskens, J. Detection of the plasmid-mediated colistin-resistance gene mcr-1 in clinical isolates and stool specimens obtained from hospitalized patients using a newly developed real-time PCR assay. Journal of antimicrobial chemotherapy 2016, 71, 2344–2346. [Google Scholar] [CrossRef]
- Pogue, J.M.; Mynatt, R.P.; Marchaim, D.; Zhao, J.J.; Barr, V.O.; Moshos, J.; Sunkara, B.; Chopra, T.; Chidurala, S.; Kaye, K.S. Automated alerts coupled with antimicrobial stewardship intervention lead to decreases in length of stay in patients with gram-negative bacteremia. Infection Control & Hospital Epidemiology 2014, 35, 132–138. [Google Scholar] [CrossRef]
- Sorlí, L.; Luque, S.; Grau, S.; Berenguer, N.; Segura, C.; Montero, M.M.; Álvarez-Lerma, F.; Knobel, H.; Benito, N.; Horcajada, J.P. Trough colistin plasma level is an independent risk factor for nephrotoxicity: a prospective observational cohort study. BMC infectious diseases 2013, 13, 1–9. [Google Scholar] [CrossRef]
- Gu, W.-J.; Wang, F.; Tang, L.; Bakker, J.; Liu, J.-C. Colistin for the treatment of ventilator-associated pneumonia caused by multidrug-resistant Gram-negative bacteria: a systematic review and meta-analysis. International journal of antimicrobial agents 2014, 44, 477–485. [Google Scholar] [CrossRef]
- Nagaoka, R.; Ikawa, K.; Onodera, M.; Koba, Y.; Hara, T.; Joichi, Y.; Yokozaki, M.; Ohge, H.; Morikawa, N. In vitro combined effects of double antibacterial drugs against multidrug-resistant Pseudomonas aeruginosa isolates: comparison among combinations of colistin, arbekacin, aztreonam, rifampicin and piperacillin. The Japanese Journal of Antibiotics 2014, 67, 167–174. [Google Scholar] [PubMed]
- Batirel, A.; Balkan, I.; Karabay, O.; Agalar, C.; Akalin, S.; Alici, O.; Alp, E.; Altay, F.A.; Altin, N.; Arslan, F. Comparison of colistin–carbapenem, colistin–sulbactam, and colistin plus other antibacterial agents for the treatment of extremely drug-resistant Acinetobacter baumannii bloodstream infections. European journal of clinical microbiology & infectious diseases 2014, 33, 1311–1322. [Google Scholar] [CrossRef]
- Petrosillo, N.; Taglietti, F.; Granata, G. Treatment options for colistin resistant Klebsiella pneumoniae: present and future. Journal of clinical medicine 2019, 8, 934. [Google Scholar] [CrossRef]
- Kempf, I.; Fleury, M.A.; Drider, D.; Bruneau, M.; Sanders, P.; Chauvin, C.; Madec, J.-Y.; Jouy, E. What do we know about resistance to colistin in Enterobacteriaceae in avian and pig production in Europe? International journal of antimicrobial agents 2013, 42, 379–383. [Google Scholar] [CrossRef]
- Tornimbene, B.; Eremin, S.; Escher, M.; Griskeviciene, J.; Manglani, S.; Pessoa-Silva, C.L. WHO global antimicrobial resistance surveillance system early implementation 2016–17. The Lancet Infectious Diseases 2018, 18, 241–242. [Google Scholar] [CrossRef] [PubMed]
- Gogry, F.A.; Siddiqui, M.T.; Sultan, I.; Haq, Q.M.R. Current update on intrinsic and acquired colistin resistance mechanisms in bacteria. Frontiers in medicine 2021, 8, 677720. [Google Scholar] [CrossRef] [PubMed]
- Claudia, S.-S.; Carmen, S.-S.; Andrés, D.; Marcela, M.-A.; Kerly, C.-A.; Bryan, B.M.; John, C.J.; José, G.-F. Risk factors associated with colistin resistance in carbapenemase-producing Enterobacterales: a multicenter study from a low-income country. Annals of Clinical Microbiology and Antimicrobials 2023, 22, 64. [Google Scholar] [CrossRef] [PubMed]
- Sharma, J.; Sharma, D.; Singh, A.; Sunita, K. Colistin resistance and management of drug resistant infections. Canadian Journal of Infectious Diseases and Medical Microbiology 2022, 2022, 4315030. [Google Scholar] [CrossRef]
- Novović, K.; Jovčić, B. Colistin resistance in Acinetobacter baumannii: molecular mechanisms and epidemiology. Antibiotics 2023, 12, 516. [Google Scholar] [CrossRef]
- Mudenda, S.; Chabalenge, B.; Daka, V.; Mfune, R.L.; Salachi, K.I.; Mohamed, S.; Mufwambi, W.; Kasanga, M.; Matafwali, S.K. Global strategies to combat antimicrobial resistance: a one health perspective. Pharmacology & Pharmacy 2023, 14, 271–328. [Google Scholar] [CrossRef]
- Vasala, A.; Hytönen, V.P.; Laitinen, O.H. Modern tools for rapid diagnostics of antimicrobial resistance. Frontiers in cellular and infection microbiology 2020, 10, 308. [Google Scholar] [CrossRef]
- Mashalla, Y.; Setlhare, V.; Massele, A.; Sepako, E.; Tiroyakgosi, C.; Kgatlwane, J.; Chuma, M.; Godman, B. Assessment of prescribing practices at the primary healthcare facilities in Botswana with an emphasis on antibiotics: findings and implications. International journal of clinical practice 2017, 71, e13042. [Google Scholar] [CrossRef]
- Van Belkum, A.; Bachmann, T.T.; Lüdke, G.; Lisby, J.G.; Kahlmeter, G.; Mohess, A.; Becker, K.; Hays, J.P.; Woodford, N.; Mitsakakis, K. Developmental roadmap for antimicrobial susceptibility testing systems. Nature Reviews Microbiology 2019, 17, 51–62. [Google Scholar] [CrossRef]
- Nijhuis, R.; Guerendiain, D.; Claas, E.; Templeton, K. Comparison of ePlex respiratory pathogen panel with laboratory-developed real-time PCR assays for detection of respiratory pathogens. Journal of clinical microbiology 2017, 55, 1938–1945. [Google Scholar] [CrossRef]
- Van Belkum, A.; Rochas, O. Laboratory-based and point-of-care testing for MSSA/MRSA detection in the age of whole genome sequencing. Frontiers in microbiology 2018, 9, 1437. [Google Scholar] [CrossRef] [PubMed]
- Ellington, M.; Ekelund, O.; Aarestrup, F.M.; Canton, R.; Doumith, M.; Giske, C.; Grundman, H.; Hasman, H.; Holden, M.; Hopkins, K.L. The role of whole genome sequencing in antimicrobial susceptibility testing of bacteria: report from the EUCAST Subcommittee. Clinical microbiology and infection 2017, 23, 2–22. [Google Scholar] [CrossRef] [PubMed]
- Mondal, A.H.; Khare, K.; Saxena, P.; Debnath, P.; Mukhopadhyay, K.; Yadav, D. A Review on Colistin Resistance: An Antibiotic of Last Resort. Microorganisms 2024, 12, 772. [Google Scholar] [CrossRef] [PubMed]
- Ajayi, A.O.; Odeyemi, A.T.; Akinjogunla, O.J.; Adeyeye, A.B.; Ayo-Ajayi, I. Review of antibiotic-resistant bacteria and antibiotic resistance genes within the one health framework. Infection Ecology & Epidemiology 2024, 14, 2312953. [Google Scholar] [CrossRef]
- Behera IC, Swain SK, Chandra M. Incidence of colistin-resistant Acinetobacter baumannii in an Indian tertiary care teaching hospital. Int J Adv Res (Indore), 2394.
- Mmatli, M.; Mbelle, N.M.; Osei Sekyere, J. Global epidemiology, genetic environment, risk factors and therapeutic prospects of mcr genes: A current and emerging update. Frontiers in Cellular and Infection Microbiology 2022, 12, 941358. [Google Scholar] [CrossRef]
- Zhang, W.; Zhang, T.; Wang, C.; Liang, G.; Lu, Q.; Wen, G.; Guo, Y.; Cheng, Y.; Wang, Z.; Shao, H. Prevalence of colistin resistance gene mcr-1 in Escherichia coli isolated from chickens in central China, 2014 to 2019. Journal of Global Antimicrobial Resistance 2022, 29, 241–246. [Google Scholar] [CrossRef]
- Hamame, A.; Davoust, B.; Cherak, Z.; Rolain, J.-M.; Diene, S.M. Mobile colistin resistance (mcr) genes in cats and dogs and their zoonotic transmission risks. Pathogens 2022, 11, 698. [Google Scholar] [CrossRef]
- Cohn, J.; Mendelson, M.; Kanj, S.S.; Shafiq, N.; Boszczowski, I.; Laxminarayan, R. Accelerating antibiotic access and stewardship: a new model to safeguard public health. The Lancet Infectious Diseases 2024. [Google Scholar] [CrossRef]
- Karakonstantis, S.; Kritsotakis, E.I.; Gikas, A. Treatment options for K. pneumoniae, P. aeruginosa and A. baumannii co-resistant to carbapenems, aminoglycosides, polymyxins and tigecycline: an approach based on the mechanisms of resistance to carbapenems. Infection 2020, 48, 835–851. [Google Scholar] [CrossRef]
- Protonotariou, E.; Meletis, G.; Pilalas, D.; Mantzana, P.; Tychala, A.; Kotzamanidis, C.; Papadopoulou, D.; Papadopoulos, T.; Polemis, M.; Metallidis, S. Polyclonal endemicity of carbapenemase-producing Klebsiella pneumoniae in ICUs of a Greek tertiary care hospital. Antibiotics 2022, 11, 149. [Google Scholar] [CrossRef]
- Luo, Q.; Wang, Y.; Xiao, Y. Prevalence and transmission of mobilized colistin resistance (mcr) gene in bacteria common to animals and humans. Biosafety and Health 2020, 2, 71–78. [Google Scholar] [CrossRef]
- Andrade, F.F.; Silva, D.; Rodrigues, A.; Pina-Vaz, C. Colistin update on its mechanism of action and resistance, present and future challenges. Microorganisms 2020, 8, 1716. [Google Scholar] [CrossRef] [PubMed]
- Banerjee, R.; Humphries, R. Clinical and laboratory considerations for the rapid detection of carbapenem-resistant Enterobacteriaceae. Virulence 2017, 8, 427–439. [Google Scholar] [CrossRef]
- Mathew, P.; Jaguga, C.; Mpundu, M.; Chandy, S.J. Building knowledge and evidence base on antimicrobial resistance in Africa, through ‘One Health’based surveillance. Clinical Epidemiology and Global Health 2020, 8, 313–317. [Google Scholar] [CrossRef]
- Allegranzi, B.; Pittet, D. Role of hand hygiene in healthcare-associated infection prevention. Journal of hospital infection 2009, 73, 305–315. [Google Scholar] [CrossRef]
- Giacobbe, D.R.; Mikulska, M.; Viscoli, C. Recent advances in the pharmacological management of infections due to multidrug-resistant Gram-negative bacteria. Expert review of clinical pharmacology 2018, 11, 1219–1236. [Google Scholar] [CrossRef]
- Talat, A.; Khan, F.; Khan, A.U. Genome analyses of colistin-resistant high-risk bla NDM-5 producing Klebsiella pneumoniae ST147 and Pseudomonas aeruginosa ST235 and ST357 in clinical settings. BMC microbiology 2024, 24, 174. [Google Scholar] [CrossRef]
Figure 1.
Colistin resistance mechanisms involve regulatory genes and proteins modifying lipid A's structure via L-Ara4N and pEtN additions, activated by phosphorylated PmrA and PhoP. The pmrCAB and arnBCADTEF operons synthesize protective modifications, while mutations in MgrB overactivate the PhoP-PhoQ system, enhancing resistance.
Figure 1.
Colistin resistance mechanisms involve regulatory genes and proteins modifying lipid A's structure via L-Ara4N and pEtN additions, activated by phosphorylated PmrA and PhoP. The pmrCAB and arnBCADTEF operons synthesize protective modifications, while mutations in MgrB overactivate the PhoP-PhoQ system, enhancing resistance.
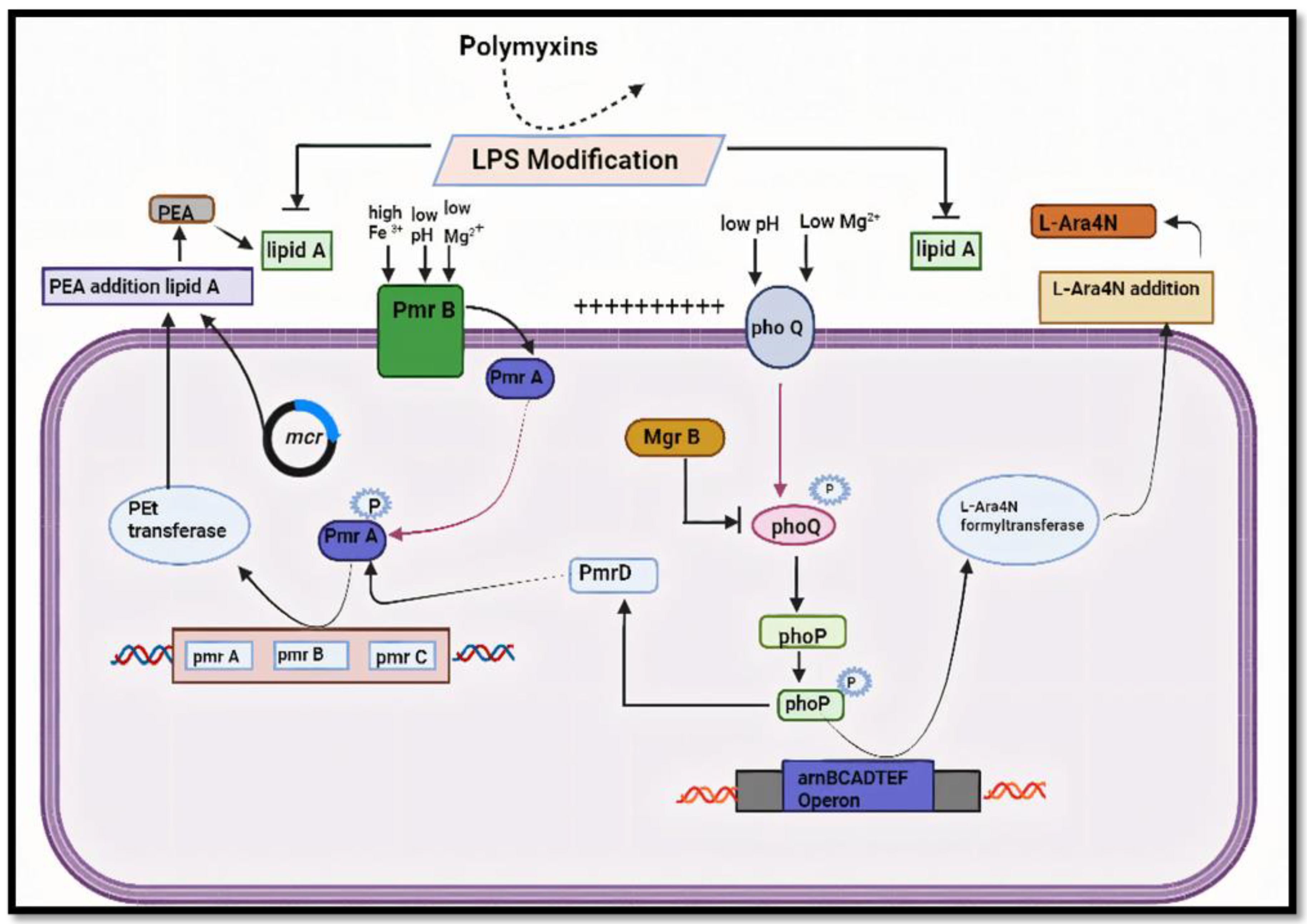
Figure 2.
Various mechanism by which bacteria develop resistance: Chromosomal mutation, Plasmid borne resistance, Lipid A mutation which further enhances the unbinding of colistin to the membrane.
Figure 2.
Various mechanism by which bacteria develop resistance: Chromosomal mutation, Plasmid borne resistance, Lipid A mutation which further enhances the unbinding of colistin to the membrane.
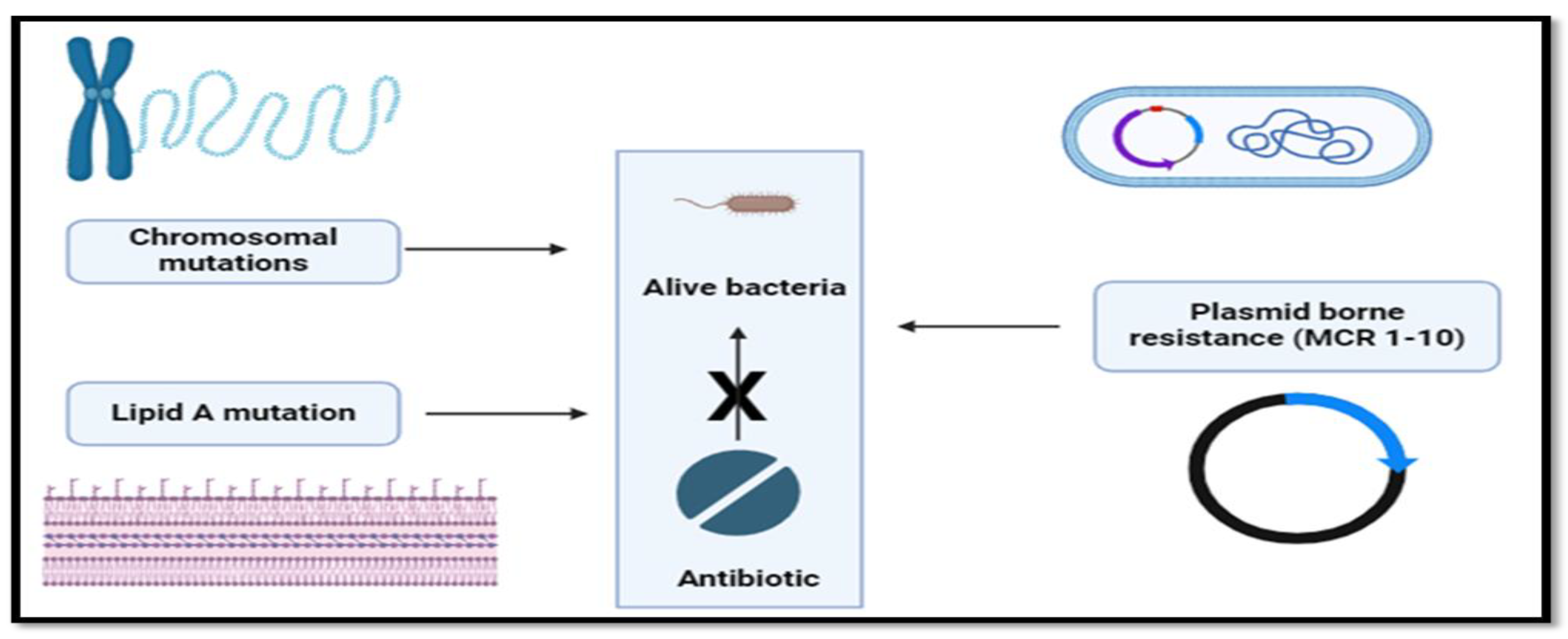
Figure 3.
Clinical impact on mortality rate due to different colistin resistance bacteria.
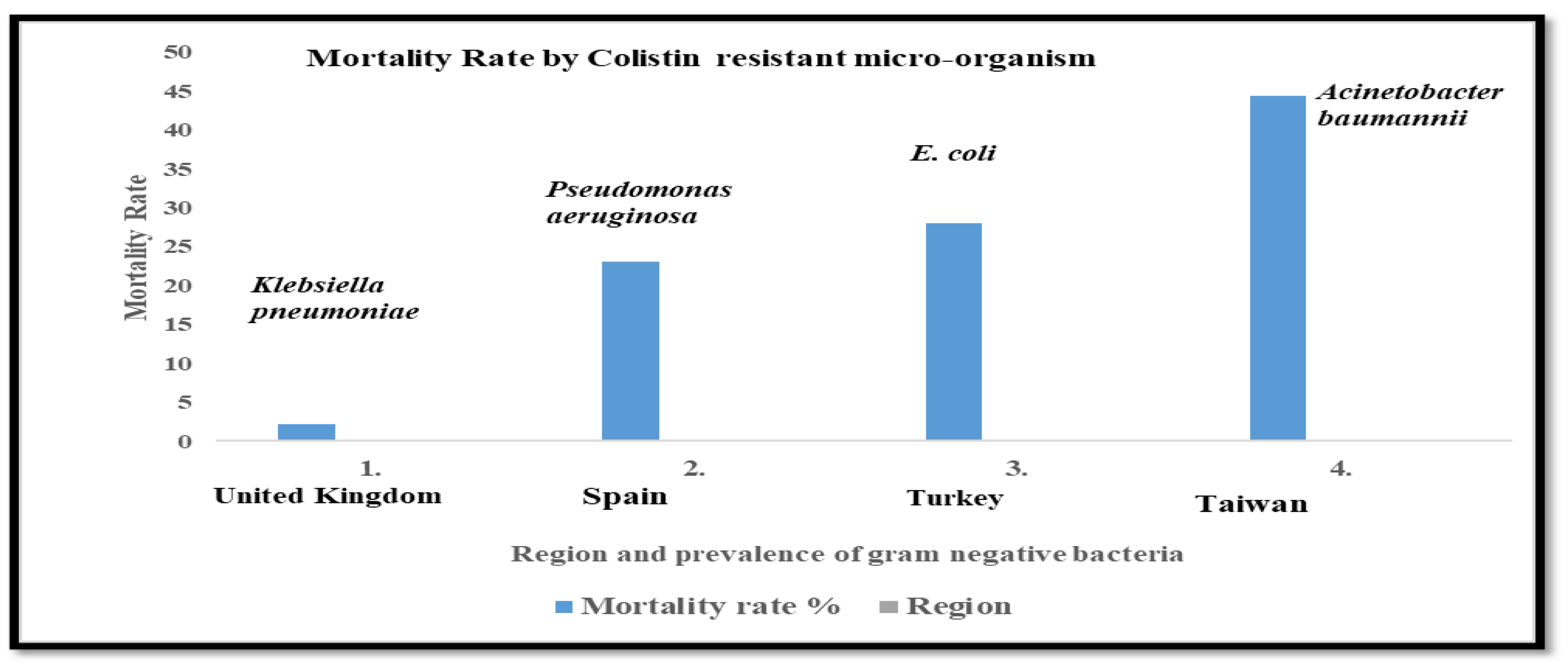
Figure 4.
Epidemiology of Colistin Resistance and its global prevalence over time.

Figure 5.
Surveillance Methods for Colistin Resistance with various methods in clinical and environmental settings.
Figure 5.
Surveillance Methods for Colistin Resistance with various methods in clinical and environmental settings.
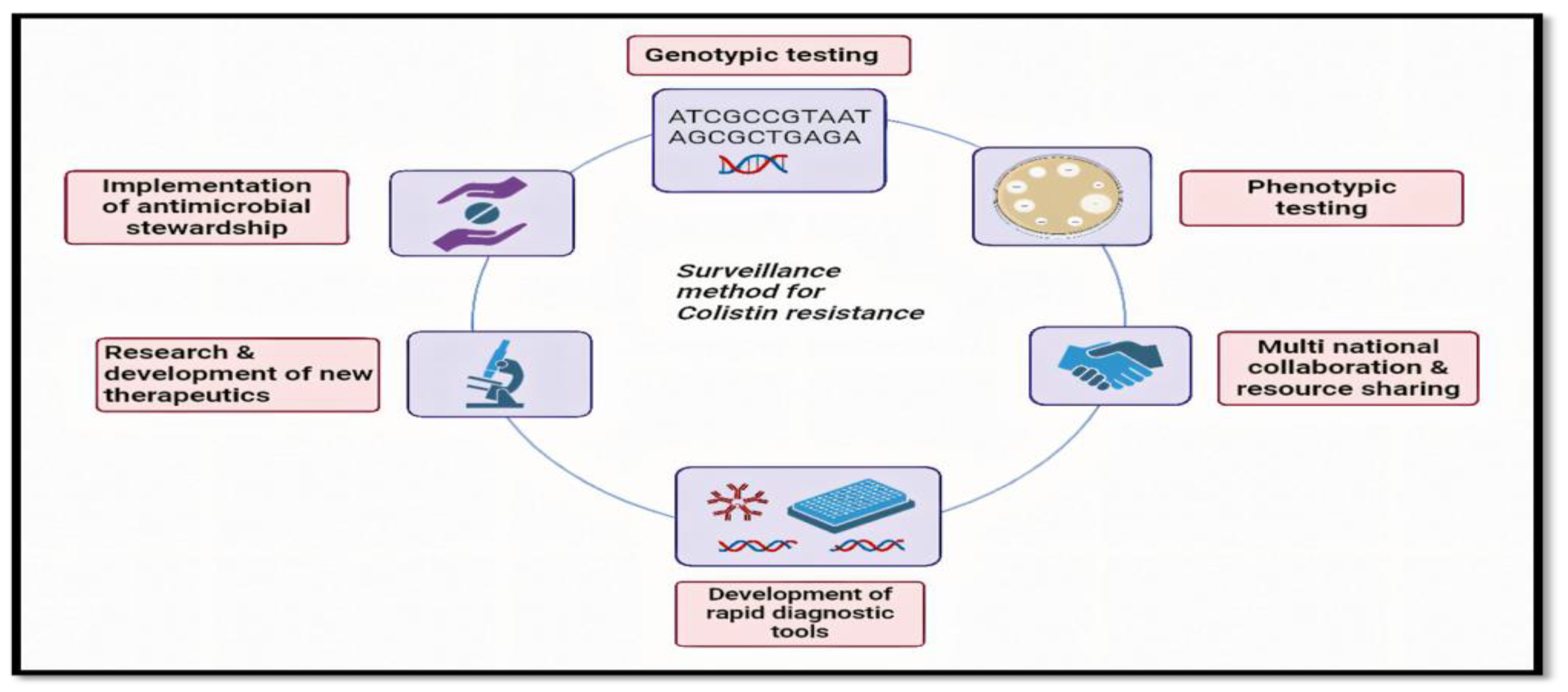
Figure 6.
Potential strategies and innovations for Future Perspectives in Colistin Resistance Research for novel therapeutic approaches.
Figure 6.
Potential strategies and innovations for Future Perspectives in Colistin Resistance Research for novel therapeutic approaches.
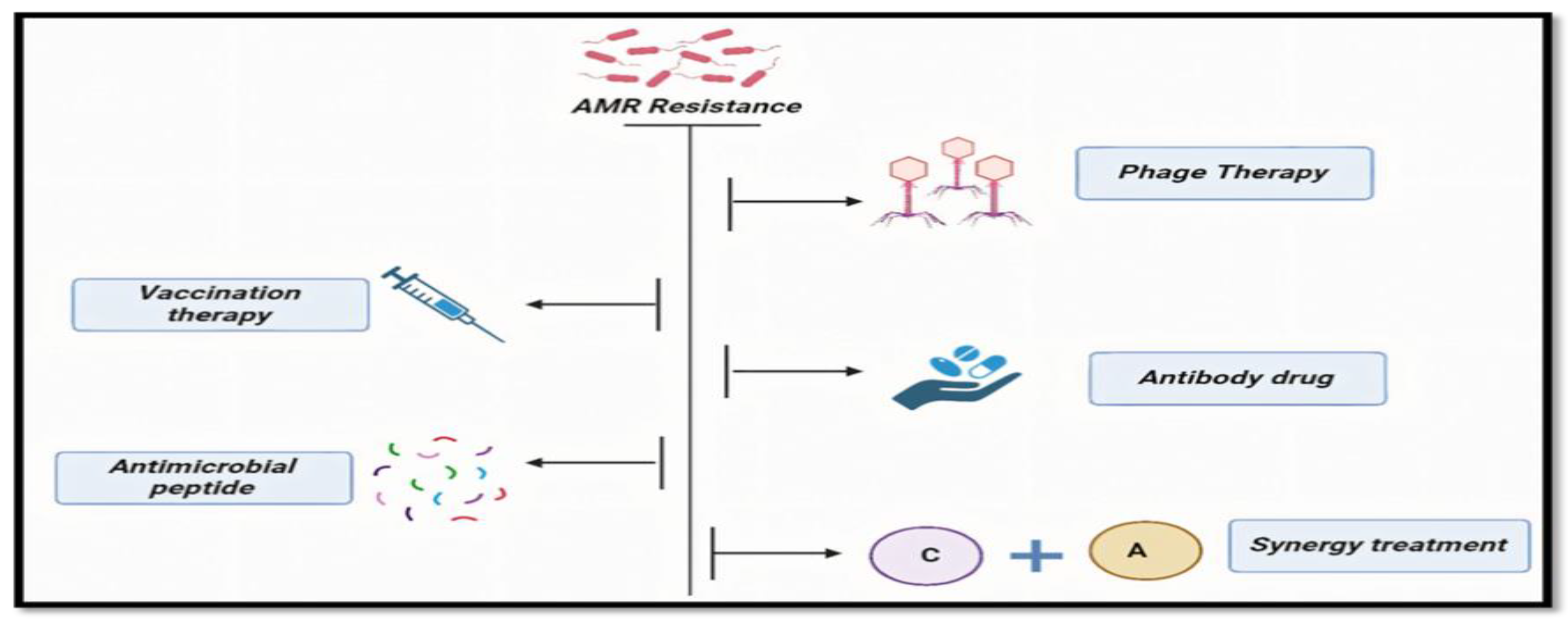

Table 1.
Mechanisms of Colistin Resistance.
| Mechanism | Description |
|---|---|
| Modification of LPS | Addition of positively charged molecules to lipopolysaccharide (LPS) structure, reducing colistin binding |
| Mutations in pmrAB | Alterations in regulatory genes controlling LPS modification |
| Mutations in mgrB | Loss of function mutations in the negative regulator of PhoPQ signaling pathway |
| Plasmid-mediated mechanisms | Acquisition of mobile genetic elements carrying resistance genes |
| Efflux pump overexpression | Increased expression of efflux pumps, reducing intracellular colistin concentration |
Table 2.
Clinical Implication of Gram-negative bacteria related to mortality rate.
| S.No. | Mortality Rate % | Colistin Resistance Associated Infection (Micro-Organism Name) |
Region | Reference |
|---|---|---|---|---|
| 1. | 2.15 | Klebsiella pneumoniae | United Kingdom | [30] |
| 2. | 23.1 | Pseudomonas aeruginosa | Spain | [31] |
| 3. | 28 | E. coli | Turkey | [32] |
| 4. | 44.4 | Acinetobacter baumannii | Taiwan | [23] |
Table 3.
Clinical Implications of Colistin Resistance.
| Implication | Description |
|---|---|
| Limited Treatment Options | Reduced efficacy of colistin and polymyxins against resistant strains |
| Increased Morbidity/Mortality | Higher rates of treatment failure and patient mortality |
| Spread of Resistance | Potential for dissemination of resistant strains within healthcare settings |
| Need for Surveillance | Importance of monitoring colistin resistance rates for infection control |
| Development of Novel Therapies | Urgency for research into alternative treatment options |
Table 4.
Epidemiology of Colistin Resistance.
| Region | Prevalence of Resistance (%) | Contributing Factors |
|---|---|---|
| North America | Low | Stringent antibiotic stewardship practices |
| Europe | Moderate | Increased use of colistin in agriculture |
| Asia | High | Widespread use of colistin in human medicine and agriculture |
| Africa | Varies | Limited surveillance and healthcare resources |
| South America | Varies | Variable regulatory oversight of antibiotic use |
Table 5.
Prevalence of Colistin Resistance in Different Countries.
| Country | Prevalence of Colistin Resistance (%) | References |
|---|---|---|
| United States | 69.2 % | [34] |
| China | 32.7 % | [35] |
| India | 1.28 % | [36] |
| Japan | 7.7 % | [37] |
| Thailand | 3.3 % | [38] |
| South Korea | 4.4 % | [39] |
| Russia | 30 % | [40] |
Table 6.
Prevalence of Colistin Resistance in Different States of India.
| State | Prevalence of Colistin Resistance (%) | Reference |
|---|---|---|
| Delhi | 15 | [41] |
| Tamil Nadu | 33 | [42] |
| Karnataka | 1.6 | [43] |
| Jaipur | 6.2 | [44] |
| West Bengal | 22.5 | [45] |
| Madhya Pradesh | 17 | [46] |
| Rajasthan | 17.4 | [47] |
| Punjab | 12.5 | [48] |
| Haryana | 3.8 | [49] |
| Kerala | 25 | [50] |
| Odisha | 13.5 | [51] |
| Jharkhand | 9.09 | [52] |
| Chhattisgarh | 0 | [53] |
| Uttarakhand | 8 | [54] |
| Himachal Pradesh | 11.76 | [55] |
| Manipur | 2 | [56] |
| Meghalaya | 2.5 | [57] |
Table 7.
Surveillance Methods for Colistin Resistance.
| Method | Description |
|---|---|
| MIC Determination | Minimum inhibitory concentration testing to assess bacterial susceptibility to colistin |
| Whole-genome sequencing | Comprehensive analysis of bacterial genomes for resistance determinants |
| PCR-based assays | Polymerase chain reaction assays targeting specific resistance genes |
| Phenotypic Screening | High-throughput screening methods to detect resistant isolates |
| Epidemiological Surveillance | Monitoring of resistance trends in healthcare settings and communities |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



