Submitted:
08 April 2025
Posted:
08 April 2025
You are already at the latest version
Abstract
Background/Objectives: The aim of this study was to assess the effects of cold water immersion (CWI) post-eccentric muscle contraction exercise on skin temperature, pain score, Maximum Voluntary Isometric Contraction (MVIC), muscle damage, and muscle mechanical properties. Methods: Twenty-seven male participants (age 20.6±0.6; body mass 69.4±8.1; body fat % 13.7±4.3) were divided into three groups: whole body CWI group (n=9), lower body CWI group (n=9), and control group (n=9). Results: Significant effects were observed in skin temperature (p=.001) and interactions between treatment and time (p=.001). MVIC showed a time effect (p=.001). Pain scale analysis indicated significant effects for treatment (p=.001), time (p=.001), and their interaction (p=.049). Creatine kinase (CK) and lactate dehydrogenase (LDH) showed time effects (p=.001), with LDH also showing an interaction effect (p=.027). Tensiomyography (TMG) results for Dm showed time and interaction effects (p=.001), while Tc had a time effect (p=.044). Conclusions: Whole-body immersion was most effective for reducing skin temperature. Lower limb immersion improved MVIC, CK, and Dm the most. The control group showed significant improvements in pain scale, Tc, Tr, and LDH. Lower limb immersion or active movement is recommended for recovery after high-intensity running training.
Keywords:
cold water immersion
; maximal voluntary isometric contraction
; muscle damage index
; muscle mechanical properties
1. Introduction
In the field of sports, various initiatives are designed to enhance the performance of elite athletes. To achieve these goals, training and periodization strategies are employed to maximize the effectiveness of training. However, overtraining can result in a decline in physical condition, an increased risk of injuries, elevated fatigue levels, and muscle damage. Hence, it is crucial to emphasize the importance of prioritizing recovery following exercise or training [1].
Although recovery methods in sports vary depending on the event, active recovery (e.g., jogging and cycling) is commonly implemented [2]. Low-intensity running, which involves approximately 30–40% of maximum oxygen intake following high-intensity training, has been shown to reduce blood lactate concentration more rapidly than static rest [3]. Additionally, low-intensity running enhances lactate oxidation in skeletal muscles post-exercise, converting lactate into glucose or amino acids, thereby aiding in its removal [4,5]. However, it is important to note that this method has limitations in preventing muscle damage and maintaining exercise performance, both of which are critical for sustaining conditioning.
CWI has gained attention as an effective method for mitigating muscle damage and maintaining conditioning in athletes [6]. Previous studies have demonstrated that CWI affects muscle soreness, biochemical markers of damage such as CK, LDH and muscle function in adolescent elite athletes post-exercise and during training [1]. It also influences indicators of physical recovery, including heart rate variability and muscle power [7]. This method involves immersing the body up to the iliac spine in water at a temperature between 10 to 15°C for 10 to 15 minutes and is widely utilized in sports for effective post-exercise recovery [8].
Previous studies have demonstrated that low-temperature immersion of the lower extremities effectively reduces free oxygen and lactic acid levels in the blood post-training and competition [9]. Moreover, these studies have identified significant benefits of low-temperature immersion in muscle damage recovery, including a decrease in the pain index during recovery. Additionally, this method has been shown to lower the concentrations of CK and myoglobin, which are key indicators of muscle damage, more effectively than general sedentary recovery. Specifically, CWI helps decrease both the depth of tissue impact and the temperature, slowing nerve transmission speed, minimizing pain, increasing hydrostatic pressure, reducing swelling and mass formation by lowering cell membrane permeability, and attenuating the immune response to tissue damage [10,11]. Further research has demonstrated that CWI effectively reduces LDH concentrations, alleviates muscle pain, and facilitates muscle recovery [12]. The efficacy of CWI is contingent upon the immersion depth. Submerging the entire body up to the collarbone following strenuous exercise has been shown to attenuate inflammatory responses, curtail elevations in CK and LDH concentrations, increase levels of Interleukin-10 (IL-10), an anti-inflammatory cytokine, and reduce levels of Interleukin-2 (IL-2), a pro-inflammatory cytokine, as well as Interleukin-8 (IL-8), a chemokine implicated in muscle damage recovery [13]. Post-exercise CWI is effective in reducing the temperature of the exercised area, alleviating fatigue, decreasing markers of muscle damage, and suppressing inflammatory responses. Previous studies have primarily focused on the effects of CWI on the whole-body and lower-body, indicating that results tend to vary depending on the specific body parts submerged [14,15]. Christophe et al reported that CWI may be effective for intrinsic muscle factors, such as damage and recovery, but it is known to potentially have negative effects on muscle function [16]. Following high-intensity exercise, muscle inflammation occurs, resulting in elevated levels of CK and LDH [17]. CWI lowers tissue temperature, thereby attenuating the inflammatory response, and further reduces inflammation levels through vasoconstriction [18]. While there is a paucity of studies investigating the short-term effects on the improvement of CK and LDH levels, as well as on functional recovery, numerous studies have documented that CK and LDH contribute to inflammation, thereby negatively affecting both muscle function and recovery. Consequently, CK and LDH have been extensively utilized as representative biomarkers of muscle damage in previous research [19,20].
TMG has been recognized as an effective tool for addressing the limitations of previous studies, particularly in observing muscle contraction characteristics and fatigue factors. In a study by [21], TMG was used to explore changes in the muscle characteristics of soccer players who underwent four repetitions of 4-minute CWI at 4°C. The findings revealed that repeated CWI significantly altered muscle properties. Notably, the study found a significant reduction in maximal displacement (Dm) among participants subjected to the CWI protocol compared to a control group. Dm, a crucial parameter measured by TMG, indicates the peak displacement of muscle tissue during contraction and serves as a marker of muscle stiffness or muscle hypertrophy has been correlated with an increase in Dm, whereas severe muscle atrophy is associated with a decrease in Dm, suggesting that a reduction in Dm may serve as an indicator of increased muscle stiffness [22,23,24]. Therefore, the application of TMG in the assessment of muscle characteristics facilitates a more thorough evaluation of alterations in muscle function in response to varying depths of CWI. Moreover, MVIC serves as a critical parameter in the assessment of muscle function. Previous research indicates that CWI is acknowledged for its may reduce MVIC [25,26]. However, the specific effects of whole-body CWI versus lower-body CWI in the context of CWI have not been comprehensively explored. Consequently, there is a notable paucity of studies examining changes in TMG metrics and MVIC, particularly in relation to muscle function following both whole-body CWI and lower-body CWI.
The present study seeks to fill the existing research gap through two primary objectives: first, this study aims to investigate the recovery of muscle damage biomarkers and TMG, MVIC following whole-body CWI and lower-body CWI post high-intensity eccentric exercise. Second, these insights aim to contribute to a broader understanding that may subsequently inform studies focused on elite athletic performance. If lower-body CWI proves to be as effective as whole-body CWI in ameliorating muscle damage and enhancing muscle function, it may offer insights into more efficient and convenient methodologies for immersion-based treatments.
2. Materials and Methods
2.1. Design and Setting
The procedure for conducting this study and the detailed steps or the experiment 0are shown in Figure 1.
The study was conducted at the G University Physical Education Science Research Institute in Gyeonggi Province, South Korea. Blood samples were collected from participants to assess changes in muscle damage indices across different treatment groups. In addition, participants underwent MVIC tests and TMG tests to investigate mechanical muscle properties.
During their initial laboratory visit, participants underwent anthropometric assessments. They were then instructed to refrain from eating and exercising for at least 12 hours before the assessment. Participants wore only sportswear during the assessments, which included measurements of height, weight, and body fat percentage. These measurements were obtained using an automatic height scale (SD-102, Biospace Co., Korea) and a bioelectrical impedance analysis (BIA) machine (Inbody 720, Biospace Co., Korea). All participants performed eccentric exercises followed by their assigned treatment. Prior to the eccentric exercise, baseline assessments included measurements of body composition, pain scale, skin temperature, MVIC, and mechanical muscle properties. Blood samples were collected from the main vein of the forearm (10 mL). The same parameters were evaluated immediately after the eccentric exercise, except for body composition. Ten minutes post-exercise, skin temperature, pain scale, and MVIC were assessed, and 0.5 mL of blood was drawn from the finger. Skin temperature was assessed again twenty minutes post-exercise. At the thirty-minute mark post-exercise, skin temperature, MVIC, and mechanical muscle properties were reassessed, and blood samples were collected from the main vein of the forearm (10 mL). Further assessments were conducted forty-eight and seventy-two hours after the muscle contraction exercise, including skin temperature, pain scale, MVIC, and mechanical muscle properties, with blood collected from the main vein of the forearm (10 mL). Nutritional factors that could influence the results were meticulously controlled throughout the experiment, with participants required to maintain a detailed meal diary. Additionally, participants were educated and closely monitored to ensure external factors such as alcohol consumption, exercise, sleep, and smoking did not impact the research outcomes.
2.2. Participants
A total of thirty-three healthy adults were initially recruited and qualified for this study. The sample size was determined using G-power software (Gpower.software.informer.com/3.1) based on the study's design parameters. The sample size of thirty-three participants was determined based on the principles of the central limit theorem, which was considered in the calculation of the sample size for this study [27]. To account for potential dropout due to personal reasons or illness, thirty-three participants were recruited, ultimately resulting in twenty-seven individuals completing the study. The purpose and methodology of the study were explained to all participants, and written informed consent was obtained.
Initially, thirty-three participants were included in the study. However, due to more than two absences and injuries, six individuals were excluded, resulting in a final cohort of 27 participants. All participants received an explanation of the study’s purpose, protocol, and associated risks before providing written informed consent. This study received approval from the Korea Institute of Sports Science Institutional Review Board under the reference number (KISS-1806-032-01, 2018-06-20).
2.3. Skin Temperature
Skin temperature was assessed at rest, immediately after exercise, and at 10 minutes, 30 minutes, 48 hours, and 72 hours post-exercise. A skin temperature meter (62 MAX/62 MAX+ Users, FLUKE Co., Netherlands) was used to measure temperatures at the chest, upper arm, femur, and calf. Each site was measured twice, and the higher value was used to calculate the average skin temperature using the formula [28]. Thermal imaging was also utilized to capture changes in body temperature, using a thermal imaging camera (T650SC, FLIR Co., Sweden) (Table 1).
2.4. MVIC
The MVIC of the knee joint was measured using an isokinetic dynamometer (Humac/Norm, Model 770, Computer Sports Medicine Inc., USA). Muscle strength was assessed on the dominant-side femoral quadriceps muscle with the knee flexed at 60°, using an isometric contraction for 10 seconds to maintain maximum force [29], which corresponds to a zero-velocity (0°/sec) condition. Assessments were conducted at rest, immediately after exercise, and at 30 minutes, 48 hours, and 72 hours post-exercise.
2.5. Pain Score
The pain scale was developed based on previous studies, utilizing a 0 to 10 scale. (0: no pain, 5: moderate pain, 10: maximum pain) [30]. Evaluations were conducted immediately after exercise and at 10 minutes, 30 minutes, 48 hours, and 72 hours post-exercise.
2.6. Muscle Damage Indices
Muscle damage indices were determined by analyzing blood LDH and CK levels. Blood samples were collected at rest, immediately after exercise, and at 30 minutes, 48 hours, and 72 hours post-exercise.
Blood samples were collected between 6:00 a.m. and 9:00 a.m. after participants had fasted for at least 10 hours. Upon arrival, participants rested for 10-15 minutes before blood was drawn from the main vein of the forearm and the fingertip. LDH and CK analyses were performed on blood collected from the forearm vein, with serum processed at a specialized medical institution using a Cobas C702 analyzer (Roche Co., Germany). On the day of treatment, blood was collected at rest, immediately after eccentric exercise at 10, 20, and 30 minutes post-exercise. Blood samples for LDH and CK analysis were collected from the main forearm vein (10 mL) at rest before eccentric exercise. With the exception of lactate, all blood analyses were performed at a specialized medical institution, and blood collection was conducted by a licensed nurse under the supervision of a specialist. Blood was stored in a sterile specimen container at room temperature for approximately 10 to 30 minutes for coagulation, after which serum was obtained using a centrifuge (3,000 RPM × 15T). The serum was then transferred to a specialized medical institution using a blood transport box maintained at 4°C to 7°C. LDH and CK concentrations were analyzed using a Cobas C702 analyzer (Roche Co., Germany) on the same day.
2.7. Muscle Mechanical Properties
Muscle mechanical properties were evaluated using TMG at four time points: at rest, at 30 minutes, 48 hours, and 72 hours post-exercise (GK40, Panoptik d.o.o., Ljubljana, Slovenia). Participants were positioned with the knee flexed at 120° for the assessment, with full knee extension defined as 180°. During the experiment, participants' arms, legs, and torso were secured as illustrated in Figure 2. This angular reference is used consistently throughout the paper. Electrodes were placed at 5cm intervals around the femoral muscle, with a sensor positioned at the center. Electrical stimulation commenced at 20 mA, increasing in 10-mA increments until peak muscle contraction was achieved. Parameters recorded included Dm, response time, and muscle relaxation time [31].
TMG assessments focused on each participant’s stronger leg to minimize testing duration. The stronger leg was determined based on a questionnaire regarding the participant's dominant leg and by referencing previous studies [32]. The study aimed to evaluate the effects of a cooling treatment on muscle strength, rather than comparing muscle strength performance between legs. Electro des were placed approximately 5 cm apart around the femoral muscle, with the sensor fixed centrally. Electrical stimulation started at 20 mA and was increased by 10 mA increments until the muscle's Dm was reached. The response to each stimulus was recorded via a sensor connected to a computer, which calculated Dm, response time, and muscle relaxation time using specialized software. Dm is used to assess muscle tension or stiffness, where lower Dm values indicate increased muscle tension or stiffness [33]. Response time varies with the number of muscle fibers, being slower with a greater number of fibers and faster with fewer fibers [34]. Muscle relaxation time serves as an index for evaluating potential muscle nerve fatigue [35].
2.8. Eccentric Exercise Protocol
Participants warmed up by running on a treadmill for 5 minutes at 30-40% of their maximum heart rate (HRmax), followed by stretching the femoral quadriceps and hamstrings for 5 minutes (20 seconds each). The eccentric exercise was performed using an isokinetic dynamometer (Humac/Norm, Model 770, Computer Sports Medicine Inc., USA). Seated with their torso and knees securely fastened, participants executed knee joint flexion and extension at a velocity of 270°/sec for 10 repetitions, which were characterized as concentric contractions. Following a 3-minute rest interval, they engaged in eccentric exercises consisting of 10 sets of 10 repetitions at 90°/sec, spanning from full extension 0° to 110°, with a 1-minute rest between sets. This experimental design was implemented to elucidate the rationale behind conducting initial high-velocity concentric contractions before the eccentric exercise regimen [36].
2.9. Whole-Body and Lower-Body CWI, and Active Recovery Treatment Protocols
Post-exercise, participants underwent whole-body or lower-body CWI treatments or active recovery. For CWI, participants were submerged in water at 12-15°C for 10 minutes, wearing only shorts (Figure 2). Whole-body CWI involved submersion up to the collarbone, while lower-body CWI targeted the iliac region. For active recovery, participants ran on a treadmill for 10 minutes at 30-40% HRmax immediately following eccentric exercise. Maximum heart rate was calculated by subtracting the participant’s age from 220. Participants assessed the water temperature using their hands and feet prior to immersion, and no restrictions were imposed during the immersion process. Additionally, there was no movement of the water during the CWI.
2.10. Statistical analysis
The data for this study were analyzed using SPSS statistical software version 23.0 (IBM Corp., Armonk, NY, USA). Descriptive statistics, including means and standard deviations, were computed. To assess changes in body composition, skin temperature, MVIC, pain scale, muscle damage indices, and TMG in relation to recovery interventions and time points, a two-way repeated measures analysis of variance performed. Post-hoc analyses were performed using Bonferroni’s method. Furthermore, the statistical effect size was evaluated using Cohen’s d, with effect sizes interpreted as small (≤ 0.2), medium (0.4–0.5), and large (≥ 0.8) according to Cohen's guidelines (1992). The statistical significance level was set at α = .05.
3. Results
3.1. Participants Body Composition
Participants were selected based on the following criteria: (1) regular exercise participation at least three times per week, (2) no drug intake, and (3) absence of physical injuries or medical conditions. A total of 27 participants were randomly assigned to one of three groups: whole-body CWI treatment (n=9, age, 20±0years; height: 176±6.4cm; body mass, 69.7±9.0kg; body fat %, 14.0±3.4%), lower-body CWI treatment (n=9, age, 20±2years; height: 174.9±3.7cm; body mass, 68.8±6.9kg; body fat %, 11.4±3.8%), and control (active recovery) (n=9, age, 22±3years; height: 174.6±5.6cm; body mass, 69.8±8.4kg; body fat %, 15.7±5.6%).
3.2. Changes Average Skin Temperature
Changes in skin temperature according to the recovery treatment method are presented in <Table 2>. The average skin temperature demonstrated a significant interaction effect between treatment and timing (F=10.927, p=.001). Post-hoc test results indicate that, for whole-body CWI treatment, skin temperature was significantly lower at 10 minutes and 30 minutes after exercise compared to at rest and immediately after exercise (p<.05 for each comparison). Additionally, the average skin temperature was significantly lower at 10 minutes after exercise compared to 30 minutes, 48 hours, and 72 hours after exercise (p<.05 for each comparison).
In an investigation of lower-body CWI treatment, it was found that the average skin temperature 10 minutes after exercise, occurring immediately after the CWI, was significantly higher than at rest and immediately post-exercise (p<.05, respectively). This observation suggests a potential rewarming effect following CWI, which may account for the elevated temperature at the 10-minute interval. Furthermore, skin temperature at this time point was significantly lower than at 30 minutes, 48 hours, and 72 hours post-exercise (p<.05 for each comparison). The effect sizes for these differences were calculated using partial eta-squared. Clarification of the protocol's timing and procedures might be needed to address any potential misunderstandings regarding these findings.
In the context of active recovery treatment, the average skin temperature at 10 minutes post-exercise was significantly lower compared to at rest (p<.05), and was also significantly lower than at 30 minutes, 48 hours, and 72 hours post-exercise (p<.05 for each comparison). The observed increases in temperature at 48 and 72 hours following passive recovery may be attributed to natural physiological processes such as delayed muscle rewarming or inflammation, which warrant further investigation to fully understand their impact.
When comparing treatments, whole-body CWI treatment resulted in significantly lower skin temperatures than both lower-body CWI treatment and active recovery treatment at 10 minutes after exercise (p<.05 for each comparison). Additionally, whole-body CWI treatment was significantly lower than active recovery treatment at 30 minutes after exercise (p<.05).
3.3. Changes in MVIC
Table 3 presents the changes in MVIC according to the recovery treatment method. The MVIC showed a significant main effect at the time (p=.001).
3.4. Changes in Pain Scale
Changes in pain scale scores following whole-body low-temperature CWI, lower-body low-temperature CWI treatment, and active recovery treatment after eccentric muscle contraction exercise are presented in <Table 4>. The pain scale scores demonstrated a significant interaction effect between CWI treatment and time (F= 2.220, p=.049). Post-hoc analyses revealed several significant differences across time points. For the whole-body low-temperature CWI treatment, the pain index was significantly lower at rest compared to immediately after exercise and at 30 minutes post-exercise (p<.05). Furthermore, the pain index was significantly lower immediately after exercise compared to 30 minutes, 48 hours, and 72 hours post-exercise (p<.05). Comparing treatments, whole-body and low-temperature CWI treatment resulted in significantly lower pain indices than active recovery treatment at 30 minutes and 48 hours post-exercise (p<.05).
3.5. Muscle Damage Indices
Changes in blood muscle damage indices according to the recovery treatment method are depicted in <Table 5>. Blood CK concentration showed a significant main effect over time (p=.001), while blood LDH concentration exhibited a significant interaction effect between treatment method and timing (p=.027) in <Table 5, 6>. Post-hoc tests revealed significant differences across time points. For whole-body CWI treatment, blood LDH concentration immediately after exercise was significantly higher compared to 48 hours and 72 hours post-exercise (p<.05). Conversely, for lower-body CWI treatment, blood LDH concentration was significantly lower at 30 minutes post-exercise compared to 72 hours post-exercise (p<.05). When comparing treatments, blood LDH concentration at 48 hours post-exercise was significantly lower in both the whole-body CWI treatment and lower-body CWI treatment compared to active recovery treatment (p<.05, respectively).
3.6. Changes in Muscle Mechanical Properties
The TMG changes according to the recovery treatment method are shown in <Table 6>. Dm demonstrated a significant interaction effect between treatment and timing (p=.047). Post-hoc tests revealed significant differences between time points. For whole-body CWI treatment, Dm was significantly lower at 30 minutes post-exercise compared to at rest (p<.05) and significantly lower at 30 minutes after exercise compared to 48 hours and 72 hours after exercise (p<.05 for each). Similarly, for both lower-body CWI treatment and active recovery treatment, Dm was significantly lower at 30 minutes after exercise compared to at rest (p<.05) and significantly lower at 30 minutes after exercise compared to 48 hours after exercise (p<.05 for each). TC showed a significant main effect based on the time (p=.044), whereas Tr did not show any main effect.
4. Discussion
This study investigated the effects of whole-body and lower-body CWI, and active recovery treatments on average skin temperature, MVIC, muscle damage indices, and muscle mechanical properties in adults following high-intensity eccentric exercise. We observed significant changes in average skin temperature following CWI, with temperatures generally declining in most treated regions. Both whole-body and lower-body CWI, as well as active recovery, exhibited statistically significant differences in average skin temperature across different time intervals. Our findings align with those of previous studies. For instance, previous study reported that CWI treatment significantly reduced skin temperature for cyclists compared to a control group[37]. Similarly, [38] found that CWI treatment administered to 11 adult men following maximal aerobic exercise resulted in significant deviations in average skin temperature compared to a control group during a 20-minute assessment period. These consistent findings suggest that employing CWI treatment post-training or competition may help mitigate inflammation and pain levels, thereby facilitating rapid fatigue recovery. Temperature fluctuations were categorized based on body regions as follows: chest temperature exhibited a significant interaction effect between the administered treatment and assessment timing, with the lowest temperature recorded 10 minutes post-exercise, indicating statistical significance. These findings demonstrated that the lowest upper-body temperature occurred 10 minutes after CWI treatment following high-intensity cycle training, with statistical significance supporting the outcomes of this study [39]. This result aligns with the statistical significance observed in our study. Additionally, consistent with similar effects seen in low-temperature immersion treatments, the use of a cooling tube showed no significant change in temperature 30 minutes post-exercise [40]. This suggests that whole-body CWI treatment may be preferable for more effective temperature reduction post-exercise.
In the thigh area, a significant interaction between treatment and timing was observed, with the lowest temperature consistently recorded 10 minutes post-exercise across all treatment methods. These results demonstrated that lower-body CWI treatment at 8°C for two 5-minute interval significantly reduced thigh temperature [41]. Additionally, lower-body CWI treatment for 10 minutes at 10°C not only decreased femoral and lower-body temperatures but also showed greater reductions compared to cryotherapy at -135°C for 2 minutes, thus supporting the findings of this study [42]. Furthermore, a previous study reported that CWI treatment after high-intensity exercise effectively reduced fatigue in general adult men, yielding statistically significant results [43]. Therefore, athletes who predominantly engage their lower-body may enhance exercise performance and rapid muscle fatigue recovery through the use of CWI treatment. An analysis of prior research on CWI indicates that applying CWI exclusively to the exercised body parts following resistance training resulted in reduced muscle growth. Therefore, in light of this finding, further investigation into the effects of exercise type and CWI protocols is warranted [44].
Generally, studies have shown that maintaining a water temperature of 10 ± 0.3°C during CWI treatment is effective in reducing body temperature [45]. Several previous studies have reported that 10-15 minutes of CWI treatment at temperatures ranging from 8°C to 10°C effectively reduces tissue temperature, blood circulation, capillary blood volume, and metabolic activity in skeletal muscle after exercise [46]. Previous study demonstrated that following resistance exercise, CWI treatment from a sitting position to the collarbone resulted in a decrease in muscle temperature by approximately 7°C compared to active recovery treatment [47]. They also observed a decrease in venous blood oxygen saturation immediately after treatment, lasting up to 2 hours post-treatment, along with a reduction in blood Mb concentration at 2, 4, and 6 hours post-treatment, indicating an advantage in relieving fatigue. Combining the results of these studies, it has been established that lower-body CWI effectively reduces lower-bodyand thigh temperatures. Furthermore, whole-body CWI treatment is effective in reducing average skin temperature by decreasing temperatures in the chest, lower-body, and thighs.
The concentrations of CK and LDH in the blood are well-established indicators of muscle damage [48]. In this study, a significant main effect of the treatment was observed in blood CK concentration, with no significant difference noted between whole-body CWI, lower-body CWI, and active recovery treatments. Notably, at 48 hours post-exercise, the blood CK concentration following whole-body CWI and lower-body CWI treatments was lower than that following active recovery treatment, with whole-body CWI resulting in the lowest levels. Similarly, blood LDH concentration was significantly lower at 48 hours post-exercise for both whole-body CWI and lower-body CWI treatments compared to active recovery treatment. In particular, the lowest blood LDH concentration was observed in the whole-body CWI treatment results. Based on the statistical significance of blood LDH concentration, it can be concluded that CWI treatment had a positive effect on the muscle damage index, regardless of the treatment site. However, the primary effect of the treatment was confirmed only for blood CK concentration, indicating no significant difference between whole-body CWI and active recovery treatments. Despite this, the numerical data showed that blood CK concentration was lower following both whole-body and lower-body CWI treatments compared to active recovery 48 hours post-exercise, with whole-body CWI treatment yielding the lowest levels. Blood LDH concentration also followed a similar trend, being significantly lower 48 hours post-exercise in whole-body CWI and lower-body CWI treatments compared to active recovery treatment. In particular, whole-body CWI treatment displayed the lowest numerical LDH concentration. Considering the statistical significance of blood LDH concentration, it can be concluded that CWI treatment had a positive effect on the muscle damage index, irrespective of the treatment site. Active recovery over and adequate duration may be more effective for muscle recovery than CWI when considering muscle damage indices. It is important to note that blood CK and LDH concentrations tend to be higher in the evening than in the morning [49]. To control for this variability, data collection in this study was conducted in the early morning during periods of low activity. Previous research has indicated that exercise can influence daily activity levels [50]. Although this study observed enhanced outcomes associated with CWI treatment, potential influences from daily activities were likely minimized, as all participants were assessed at the same time. Based on these findings, CWI treatment is an effective approach for mitigating indicators of muscle damage, regardless of the treatment site.
Post-exercise CWI treatment resulted in an increase in MVIC at 24 and 48 hours post-treatment. Additionally, there was a reduction in blood CK and Mb levels, suggesting that CWI treatment offers benefits for muscle damage recovery [51]. Previous study reported that 10 minutes of lower-body CWI at 10°C decreased femoral and lower-body temperatures while enhancing MVIC and vertical jump capacity to steady-state levels after 24 hours [52]. Conversely, some previous studies found no changes in isometric muscle strength in adult men following 20 minutes of CWI treatment or control treatment at water temperatures of 5°C and 15°C after inducing muscle fatigue through drop jumping. However, these studies reported faster recovery with CWI treatment compared to control treatment in recoil jumping [53]. Additionally, other studies indicated that CWI treatment at 10 ± 1°C for 10 minutes did not lead to significant changes in MVIC, passive longitudinal stiffness, or passive transverse stiffness compared to control treatment [54]. In this study, only the main effect of timing was observed, indicating no significant difference in muscle strength recovery between whole-body CWI treatment, lower-body CWI treatment, and active recovery treatment. However, the MVIC at 48 and 72 hours post-exercise increased in the following order: whole-body CWI treatment, lower-body CWI treatment, and active recovery treatment. In other previous studies, it has been reported that MVIC temporarily decreases further with low-temperature immersion [55,56]. However, it is clear that while MVIC decreases temporarily depending on the duration or time, it commonly recovers after 24 or 48 hours. Whole-body CWI and lower-body CWI do not seem to confer immediate benefits to muscle function when compared to dynamic recovery methods [19,20]. However, they are posited to more effectively enhance potential muscle function recovery by mitigating inflammation [57]. Despite these findings, the generalization of such results may be problematic. Depending on the timing, generalizing these findings presents challenges. Future studies should aim to clearly identify the effect of MVIC based on the low-temperature immersion area by recruiting a larger number of study participants and simplifying the treatment protocol.
Dm primary variable measured by TMG, represents the furthest travel distance of muscle movement caused by contraction, allowing for the assessment of muscle stiffness or tension. An increase in Dm indicates muscle expansion, while a decrease suggests muscle atrophy. Consequently, a decreasing Dm signifies increased muscle stiffness [58], there are also cases where Dm increases with stable rest, leading to opposite results [59]. Additionally, Tc refers to the duration of muscle contraction, with longer Tc indicating greater muscle fatigue. Tr represents the muscle relaxation phase and serves as an index to evaluate potential muscle nerve fatigue. In previous studies, the application of CWI was reported to have a positive effect over time on leg muscle contraction characteristics, as assessed using TMG [60]. Previous studies have documented significant changes associated with TMG, demonstrating its utility in various research contexts. Moreover, TMG exhibits excellent inter-rater reliability, with intra-class correlation coefficients (ICC) ranging from 0.77 to 0.97, underscoring its consistency and dependability across different evaluators [61].
The findings of this study demonstrate that CWI effectively alleviates pain, reduces muscle damage, and facilitates intrinsic muscle recovery. This suggests that CWI offers substantial recovery benefits for both the general population and athletes. Also, a significant decrease in Dm was observed 30 minutes post-exercise across all treatment groups compared to baseline. When examining the MVIC results of this study, caution should be exercised in the use of CWI if immediate muscle strength is required after treatment. Based on these results, it is highly recommended to implement lower-body CWI at a temperature of 10-15°C for 10 minutes between training sessions or after competitions. Coaches and trainers should consider integrating these findings into their practices promptly. Nonetheless, it is crucial to be aware that prolonged exposure to cooling can lead to burns and muscle contractions, necessitating cautious application [62]. Extended application of CWI has the potential to hinder muscle hypertrophy and neuromuscular adaptation. Consequently, it is imperative to conduct research to ascertain the optimal duration for CWI application [63]. In both the CWI and active recovery treatments, Dm decreased significantly 30 minutes post-exercise, indicating that both CWI and active recovery are effective in increasing muscle tension and stiffness. However, examining the numerical changes, Dm was significantly lower 30 minutes post-exercise in both the whole-body CWI and lower-body CWI treatments compared to active recovery. Additionally, only the main effect of the time point was observed in Tc, with no interaction effect or main effect of the treatment and time points observed in Tr. In a study by [64], participants performed a total of eight sets recoil jumps for 30 seconds, followed by CWI treatment at 12°C for 12 minutes. The study found no significant changes in the TMG variables of the vastus lateralifs and the biceps femoris, and no statistical significance was observed in Tc and Tr between treatment and time points. These results suggest the need to consider various muscle areas in future investigations. In this study, only TMG for the vastus lateralis was examined to assess muscle characteristics following CWI treatment after eccentric exercise. However, for more comprehensive verification, investigating TMG for various muscle areas, including the outer and inner thigh muscles, is essential. Additionally, due to the potential limitations posed by the relatively small sample size or extensive assessment points, observing changes in TMG across various muscles is crucial to minimize the impact of these factors in future research.
Previous research has identified sufficient sleep, proper nutrition, and adequate hydration as critical determinants impacting the efficacy of CWI [65]. Moreover, circadian rhythms and hormonal levels have also been acknowledged as influential factors in the effectiveness of CWI [66]. It is posited that a thorough assessment of variables such as the subject's physiological status, circadian rhythm, and training periodization, conducted prior to the administration of CWI, may enhance its overall effectiveness.
4.1. Methodological Quality and Limitation
In this study, 27 physically healthy adult male participants were initially recruited. This selection may limit the applicability of the findings to women, the elderly, and adolescents. The recruited participants were drawn from the general public, and the minimum required number of participants was met for each treatment group. However, the psychological and physiological factors among the participants during the experimental period could not be feasibly controlled. To accurately assess the impact of cooling treatment, it is imperative to recruit a larger sample size in future studies and identify muscle damage indicators, muscle function, and fatigue-related variables based on whole-body CWI and lower-body CWI. Additionally, efforts should be made to minimize the number of assessment time points, standardize muscle damage protocols and blood analysis methods, and utilize measuring equipment capable of detecting tremors. The present study is limited by its short duration. To enhance the reliability and validity of the findings, future research should be conducted over an extended period. Furthermore, this study did not consider the potential impact of sleep, nutrition, and hydration, factors that may significantly influence the results.
Most importantly, identifying the effects of various cooling treatments is crucial to facilitate the practical application of low-temperature immersion in diverse settings.
5. Conclusions
The results of this study indicate that CWI treatment effectively reduces lower-body and femoral temperatures, with whole-body CWI showing particular efficacy in lowering average skin temperature by decreasing chest, lower-body, and femoral temperatures. Additionally, both whole-body CWI and lower-body CWI treatments significantly decreased the pain index 30 minutes and 48 hours post-exercise compared to active recovery, confirming the pain relief benefits of CWI treatments.
Regarding MVIC, significant differences were observed at every time point for whole-body CWI, lower-body CWI, and active recovery treatments, demonstrating that all three approaches improve MVIC. Compared to active recovery, whole-body CWI and lower-body CWI treatments significantly reduced blood LDH concentration at 48 hours post-exercise, suggesting that both CWI treatments effectively mitigate muscle damage indicators.
As for Dm, both CWI and active recovery treatments significantly decreased Dm 30 minutes post-exercise compared to at rest. Moreover, for CWI treatments, Dm was significantly lower at 30 minutes post-exercise compared to 48 hours post-exercise.
In conclusion, both whole-body CWI and lower-body CWI treatments have been demonstrated to effectively reduce pain indices and blood LDH concentrations. Based on these findings, it is proposed that lower-body CWI may offer a more convenient approach compared to whole-body CWI for the efficient application of CWI.
Author Contributions
Conceptualization, Methodology, Introduction, J.S.Lee; Analysis, result, J.H.Moon; Writing, review, resources, N.S. Kim. All authors have read and agreed to the published version of the manuscript and contributed this study.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approval from the Korea Institute of Sports Science Institutional Review Board under the reference number (KISS-1806-032-01).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Data are available on request due to privacy/ethical restrictions.
Acknowledgments
In this section, you can acknowledge any support given which is not covered by the author contribution or funding sections. This may include administrative and technical support, or donations in kind (e.g., materials used for experiments).
Conflicts of Interest
The authors declare no conflict of interest.
Abbreviations
The following abbreviations are used in this manuscript
| CWI | Cold Water Immersion |
| MVIC | Maximum Voluntary Isometric Contraction |
| CK | Creatine Kinase |
| LDH | Lactate DeHydrogenase |
| TMG | Tensiomyography |
| IL-10 | Interleukin-10 |
| IL-2 | Interleukin-2 |
| IL-8 | Interleukin-8 |
| Dm | Muscle's maximum travel Distance |
| HRmax | MAXimum Heart Rate |
| TC | Contraction Time |
| TR | Relaxation time |
References
- Tuxtaevich, A.T. Physiological Mechanisms and patterns of recovery process in sports. Frontline Medical Sciences and Pharmaceutical Journal 2023, 3, 70–76. [Google Scholar] [CrossRef]
- Masodsai, K.; Chaunchaiyakul, R. Dynamic Cardiopulmonary and Metabolic Functions during Jogging with and without Breast Supports. Journal of Exercise Physiology Online 2022, 25. [Google Scholar]
- Bishop, D.; Edge, J.; Thomas, C.; Mercier, J. Effects of high-intensity training on muscle lactate transporters and post-exercise recovery of muscle lactate and hydrogen ions in women. American Journal of Physiology-Regulatory, Integrative and Comparative Physiology 2008, 295, R1991–R1998. [Google Scholar] [CrossRef] [PubMed]
- Jones, S.; D'Silva, A.; Bhuva, A.; Lloyd, G.; Manisty, C.; Moon, J.C.; Hughes, A.D. Improved exercise-related skeletal muscle oxygen consumption following uptake of endurance training measured using near-infrared spectroscopy. Frontiers in Physiology 2017, 8, 299464. [Google Scholar] [CrossRef]
- Peng, Y.; Meng, L.; Zhu, H.; Wan, L.; Chen, F. Effect of Normobaric Oxygen Inhalation Intervention on Microcirculatory Blood Flow and Fatigue Elimination of College Students After Exercise. Frontiers in Genetics 2022, 13, 901862. [Google Scholar] [CrossRef]
- Peake, J.M.; Roberts, L.A.; Figueiredo, V.C.; Egner, I.; Krog, S.; Aas, S.N.; Raastad, T. The effects of cold water immersion and active recovery on inflammation and cell stress responses in human skeletal muscle after resistance exercise. The Journal of physiology 2017, 595, 695–711. [Google Scholar] [CrossRef]
- Zandvoort, C.S.; De Zwart, J.R.; Van Keeken, B.L.; Viroux, P.J.; Tiemessen, I.J. A customised cold-water immersion protocol favours one-size-fits-all protocols in improving acute performance recovery. European Journal of Sport Science 2018, 18, 54–61. [Google Scholar] [CrossRef]
- Bastos, F.N.; Vanderlei, L.C.M.; Nakamura, F.Y.; Bertollo, M.; Godoy, M.F.; Hoshi, R.A. Effects of cold water immersion and active recovery on post-exercise heart rate variability. International Journal of Sports Medicine 2012, 33, 873–879. [Google Scholar] [CrossRef]
- Ziemann, E. Muscle Exercise. In Whole-Body Cryostimulation: Clinical Applications; Springer International Publishing: Cham, 2024; pp. 67–79. [Google Scholar] [CrossRef]
- Mcgorm, H.; Roberts, L.; Coombes, J.; Peake, J. Cold water immersion: Practices, trends and avenues of effect. Aspetar Sports Medicine Journal 2015, 4, 106–111. [Google Scholar]
- White, G.E.; Wells, G.D. Cold-water immersion and other forms of cryotherapy: Physiological changes potentially affecting recovery from high-intensity exercise. Extreme physiology & medicine 2013, 2, 1–11. [Google Scholar] [CrossRef]
- Erdoğan, R.; Tizar, E.; Tizar, G.R. The Effect of Cold-Water Immersion Application on Biochemical Parameters in Athletes. International Archives of Medical Research 2024, 16, 20–27. [Google Scholar] [CrossRef]
- Lubkowska, A.; Szygula, Z.; Klimek, A.J.; Torii, M. Do sessions of cryostimulation have influence on white blood cell count, level of IL6 and total oxidative and antioxidative status in healthy men? European Journal of Applied Physiology 2010, 109, 67–72. [Google Scholar] [CrossRef]
- Rech, N.; Bressel, E.; Louder, T. Predictive ability of body fat percentage and thigh anthropometrics on tissue cooling during cold-water immersion. Journal of Athletic Training 2021, 56, 548–554. [Google Scholar] [CrossRef]
- Schimpchen, J.; Wagner, M.; Ferrauti, A.; Kellmann, M.; Pfeiffer, M.; Meyer, T. Can cold water immersion enhance recovery in elite Olympic weightlifters? An individualized perspective. The Journal of Strength & Conditioning Research 2017, 31, 1569–1576. [Google Scholar]
- Christophe, H. Conditioning recovery strategy to improve exercise performance (Korean edition): Seoul, South korea, 2017; pp. 105–122.
- Sarkar, S.; Debnath, M.; Das, M.; Bandyopadhyay, A.; Dey, S.K.; Datta, G. Effect of high intensity interval training on antioxidant status, inflammatory response and muscle damage indices in endurance team male players. Sports Medicine 2021, 56, 100352. [Google Scholar] [CrossRef]
- Pawłowska, M.; Mila-Kierzenkowska, C.; Boraczyński, T.; Boraczyński, M.; Szewczyk-Golec, K.; Sutkowy, P.; Woźniak, A. The influence of ambient temperature changes on the indicators of inflammation and oxidative damage in blood after submaximal exercise. Antioxidants 2022, 11, 2445. [Google Scholar] [CrossRef]
- Bassit, R.A.; Pinheiro, C.H.D.J.; Vitzel, K.F.; Sproesser, A.J.; Silveira, L.R.; Curi, R. Effect of short-term creatine supplementation on markers of skeletal muscle damage after strenuous contractile activity. European journal of applied physiology 2010, 108, 945–955. [Google Scholar] [CrossRef]
- Brancaccio, P.; Lippi, G.; Maffulli, N. Biochemical markers of muscular damage. Clinical chemistry and laboratory medicine 2010, 48, 757–767. [Google Scholar] [CrossRef]
- García-Manso, J.M.; Rodríguez-Ruiz, D.; Rodríguez-Matoso, D.; de Saa, Y.; Sarmiento, S.; Quiroga, M. Assessment of muscle fatigue after an ultra-endurance triathlon using tensiomyography (TMG). Journal of sports sciences 2011, 29, 619–625. [Google Scholar] [CrossRef]
- Pišot, R.; Narici, M.V.; Šimunič, B.; De Boer, M.; Seynnes, O.; Jurdana, M.; Mekjavić, I.B. Whole muscle contractile parameters and thickness loss during 35-day bed rest. European journal of applied physiology 2008, 104, 409–414. [Google Scholar] [CrossRef]
- Rey, E.; Lago-Penas, C.; Lago-Ballesteros, J. Tensiomyography of selected lower-limb muscles in professional soccer players. Journal of Electromyography and Kinesiology 2012, 22, 866–872. [Google Scholar] [CrossRef] [PubMed]
- Valenčič, V.; Knez, N. Measuring of skeletal muscles' dynamic properties. Artificial organs 1997, 21, 240–242. [Google Scholar] [CrossRef]
- Peiffer, J.J.; Abbiss, C.R.; Nosaka, K.; Peake, J.M.; Laursen, P.B. Effect of cold water immersion after exercise in the heat on muscle function, body temperatures, and vessel diameter. Journal of science and medicine in sport 2009, 12, 91–96. [Google Scholar] [CrossRef]
- Wakabayashi, H.; Wijayanto, T.; Tochihara, Y. Neuromuscular function during knee extension exercise after cold water immersion. Journal of physiological anthropology 2017, 36, 1–8. [Google Scholar] [CrossRef]
- Chow, S.C.; Shao, J.; Wang, H.; Lokhnygina, Y. Sample size calculations in clinical research. Chapman and Hall/CRC, 2017. [Google Scholar]
- Ramanathan, N.L. A new weighting system for mean surface temperature of the human body. Journal of applied physiology 1964, 19, 531–533. [Google Scholar] [CrossRef]
- Selkowitz, D.M. Improvement in isometric strength of the quadriceps femoris muscle after training with electrical stimulation. Physical therapy 1985, 65, 186–196. [Google Scholar] [CrossRef] [PubMed]
- Ascensão, A.; Leite, M.; Rebelo, A.N.; Magalhäes, S.; Magalhäes, J. Effects of cold water immersion on the recovery of physical performance and muscle damage following a one-off soccer match. Journal of sports sciences 2011, 29, 217–225. [Google Scholar] [CrossRef] [PubMed]
- Alvarez-Diaz, P.; Alentorn-Geli, E.; Ramon, S.; Marin, M.; Steinbacher, G.; Rius, M.; Cugat, R. Comparison of tensiomyographic neuromuscular characteristics between muscles of the dominant and non-dominant lower extremity in male soccer players. Knee Surgery, Sports Traumatology, Arthroscopy 2016, 24, 2259–2263. [Google Scholar] [CrossRef]
- van Melick, N.; Meddeler, B.M.; Hoogeboom, T.J.; Nijhuis-van der Sanden, M.W.; van Cingel, R.E. . How to determine leg dominance: The agreement between self-reported and observed performance in healthy adults. PLoS ONE 2017, 12, e0189876. [Google Scholar] [CrossRef]
- Križaj, D.; Šimunič, B.; Žagar, T. Short-term repeatability of parameters extracted from radial displacement of muscle belly. Journal of Electromyography and Kinesiology 2008, 18, 645–651. [Google Scholar] [CrossRef]
- Valenčič, V.; Knez, N. Measuring of skeletal muscles' dynamic properties. Artificial organs 1997, 21, 240–242. [Google Scholar] [CrossRef] [PubMed]
- García-Manso, J.M.; Rodríguez-Ruiz, D.; Rodríguez-Matoso, D.; de Saa, Y.; Sarmiento, S.; Quiroga, M. Assessment of muscle fatigue after an ultra-endurance triathlon using tensiomyography (TMG). Journal of sports sciences 2011, 29, 619–625. [Google Scholar] [CrossRef] [PubMed]
- Byrne, C.; Eston, R.G.; Edwards, R.H.T. Characteristics of isometric and dynamic strength loss following eccentric exercise-induced muscle damage. Scandinavian journal of medicine & science in sports 2001, 11, 134–140. [Google Scholar] [CrossRef]
- Peiffer, J.J.; Abbiss, C.R.; Watson, G.; Nosaka, K.; Laursen, P.B. Effect of cold-water immersion duration on body temperature and muscle function. Journal of sports sciences 2009, 27, 987–993. [Google Scholar] [CrossRef] [PubMed]
- Choo, H.C.; Peiffer, J.J.; Lopes-Silva, J.P.; Mesquita, R.N.; Amano, T.; Kondo, N.; Abbiss, C.R. Effect of ice slushy ingestion and cold water immersion on thermoregulatory behavior. PLoS ONE 2019, 14, e0212966. [Google Scholar] [CrossRef]
- Stephens, J.M.; Sharpe, K.; Gore, C.; Miller, J.; Slater, G.J.; Versey, N.; Halson, S.L. Core temperature responses to cold-water immersion recovery: A pooled-data analysis. International Journal of Sports Physiology and Performance 2018, 13, 917–925. [Google Scholar] [CrossRef]
- Song, H.S.; Kim, K.J.; Chun, B.O.; Lee, K.H.; Noh, J.H. The effect of cooling tubing intervention on recovery in elite wrestler competition simulation. Exercise Science 2019, 28, 221–231. [Google Scholar] [CrossRef]
- Joo, C.H.; Allan, R.; Drust, B.; Close, G.L.; Jeong, T.S.; Bartlett, J.D.; Gregson, W. Passive and post-exercise cold-water immersion augments PGC-1α and VEGF expression in human skeletal muscle. European Journal of Applied Physiology 2016, 116, 2315–2326. [Google Scholar] [CrossRef]
- Hohenauer, E.; Costello, J.T.; Deliens, T.; Clarys, P.; Stoop, R.; Clijsen, R. Partial-body cryotherapy and cold-water immersion after muscle damage in females. Scandinavian journal of medicine & science in sports 2020, 30, 485–495. [Google Scholar] [CrossRef]
- Yeung, S.S.; Ting, K.H.; Hon, M.; Fung, N.Y.; Choi, M.M.; Cheng, J.C.; Yeung, E.W. Effects of cold water immersion on muscle oxygenation during repeated bouts of fatiguing exercise: A randomized controlled study. Medicine 2016, 95. [Google Scholar] [CrossRef]
- Grgic, J. Effects of post-exercise cold-water immersion on resistance training-induced gains in muscular strength: A meta-analysis. European Journal of Sport Science 2023, 23, 372–380. [Google Scholar] [CrossRef] [PubMed]
- Bleakley, C.M.; Davison, G.W. What is the biochemical and physiological rationale for using cold-water immersion in sports recovery? A systematic review. British journal of sports medicine 2010, 44, 179–187. [Google Scholar] [CrossRef]
- Broatch, J.R.; Petersen, A.; Bishop, D.J. Postexercise cold water immersion benefits are not greater than the placebo effect. Medicine & Science in Sports & Exercise 2014, 46, 2139–2147. [Google Scholar] [CrossRef]
- Roberts, L.A.; Nosaka, K.; Coombes, J.S.; Peake, J.M. . Cold water immersion enhances recovery of submaximal muscle function after resistance exercise. American Journal of Physiology-Regulatory, Integrative and Comparative Physiology 2014, 307, R998–R1008. [Google Scholar] [CrossRef] [PubMed]
- Carvalho, T.; Crisp, A.; Lopes, C.; Crepaldi, M.; Calixto, R.; Pereira, A.; Verlengia, R. Effect of eccentric velocity on muscle damage markers after bench press exercise in resistance-trained men. Gazzetta Medica Italiana 2015, 174, 105–111. [Google Scholar]
- Hammouda, O.; Chtourou, H.; Chahed, H.; Ferchichi, S.; Kallel, C.; Miled, A.; Souissi, N. Diurnal variations of plasma homocysteine, total antioxidant status, and biological markers of muscle injury during repeated sprint: Effect on performance and muscle fatigue—A pilot study. Chronobiology international 2011, 28, 958–967. [Google Scholar] [CrossRef]
- Dalton, B.; McNaughton, L.; Davoren, B. Circadian rhythms have no effect on cycling performance. International journal of sports medicine 1997, 18, 538–542. [Google Scholar] [CrossRef]
- Bailey, D.M.; Erith, S.J.; Griffin, P.J.; Dowson, A.; Brewer, D.S.; Gant, N.; Williams, C. Influence of cold-water immersion on indices of muscle damage following prolonged intermittent shuttle running. Journal of Sports Sciences 2007, 25, 1163–1170. [Google Scholar] [CrossRef]
- Hohenauer, E.; Costello, J.T.; Deliens, T.; Clarys, P.; Stoop, R.; Clijsen, R. Partial-body cryotherapy and cold-water immersion after muscle damage in females. Scandinavian journal of medicine & science in sports 2020, 30, 485–495. [Google Scholar] [CrossRef]
- Vieira, A.; Siqueira, A.F.; Ferreira-Junior, J.B.; do Carmo, J.; Durigan, J.L.Q.; Blazevich, A.; Rodrigues, P.; Wassmansdorf, R.; Salgueirosa, F.M.; Hernandez, S.G.; Nascimento, V.B.; Daros, L.B.; Osiecki, R. Time-course of changes in indirect markers of muscle damage responses following a 130-km cycling race. Revista Brasileira de Cineantropometria & Desempenho Humano 2016, 18, 322–331. [Google Scholar] [CrossRef]
- Pinto, J.; Rocha, P.; Torres, R. Cold-Water Immersion Has No Effect on Muscle Stiffness after Exercise-Induced Muscle Damage. Clinical Journal of Sport Medicine 2020, 30, 533–538. [Google Scholar] [CrossRef] [PubMed]
- Peiffer, J.J.; Abbiss, C.R.; Nosaka, K.; Peake, J.M.; Laursen, P.B. Effect of cold water immersion after exercise in the heat on muscle function, body temperatures, and vessel diameter. Journal of science and medicine in sport 2009, 12, 91–96. [Google Scholar] [CrossRef]
- Wakabayashi, H.; Wijayanto, T.; Tochihara, Y. Neuromuscular function during knee extension exercise after cold water immersion. Journal of physiological anthropology 2017, 36, 1–8. [Google Scholar] [CrossRef]
- Urso, M.L. Anti-inflammatory interventions and skeletal muscle injury: Benefit or detriment? Journal of applied physiology 2013, 115, 920–928. [Google Scholar] [CrossRef] [PubMed]
- Rey, E.; Lago-Penas, C.; Lago-Ballesteros, J. Tensiomyography of selected lower-limb muscles in professional soccer players. Journal of Electromyography and Kinesiology 2012, 22, 866–872. [Google Scholar] [CrossRef] [PubMed]
- Dakić, M.; Ilić, V.; Toskić, L.; Duric, S.; Šimenko, J.; Marković, M.; Cuk, I. Acute effects of short-term massage procedures on neuromechanical contractile properties of rectus femoris muscle. Medicina 2024, 60, 125. [Google Scholar] [CrossRef]
- Mur-Gimeno, E.; Sebio-Garcia, R.; Solé, J.; Lleida, A.; Moras, G. Short-term effects of two different recovery strategies on muscle contractile properties in healthy active men: A randomised cross-over study. Journal of Sports Sciences 2022, 40, 646–654. [Google Scholar] [CrossRef] [PubMed]
- Mur Gimeno, E.; Campa, F.; Badicu, G.; Castizo-Olier, J.; Palomera-Fanegas, E.; Sebio-Garcia, R. Changes in muscle contractile properties after cold-or warm-water immersion using tensiomyography: A cross-over randomised trial. Sensors 2020, 20, 3193. [Google Scholar] [CrossRef]
- Christophe, H. Conditioning recovery strategy to improve exercise performance (Korean edition): Seoul, South korea, 2017; pp. 105–122.
- Petersen, A.C.; Fyfe, J.J. Post-exercise cold water immersion effects on physiological adaptations to resistance training and the underlying mechanisms in skeletal muscle: A narrative review. Frontiers in sports and active living 2021, 3, 1–26. [Google Scholar] [CrossRef]
- Sánchez-Ureña, B.; Rojas-Valverde, D.; Gutiérrez-Vargas, R. Effectiveness of two cold water immersion protocols on neuromuscular function recovery: A tensiomyography study. Frontiers in physiology 2018, 9, 766. [Google Scholar] [CrossRef]
- Edholm, P.; Ørtenblad, N.; Holmberg, H.C.; Sperlich, B. Optimizing recovery strategies for winter athletes: Insights for Milano-Cortina 2026 Olympic Games. Sport Sciences for Health 2024, 20, 1169–1182. [Google Scholar] [CrossRef]
- An, J.; Lee, I.; Yi, Y. The thermal effects of water immersion on health outcomes: An integrative review. International journal of environmental research and public health 2019, 16, 1280. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Procedure of experiment.
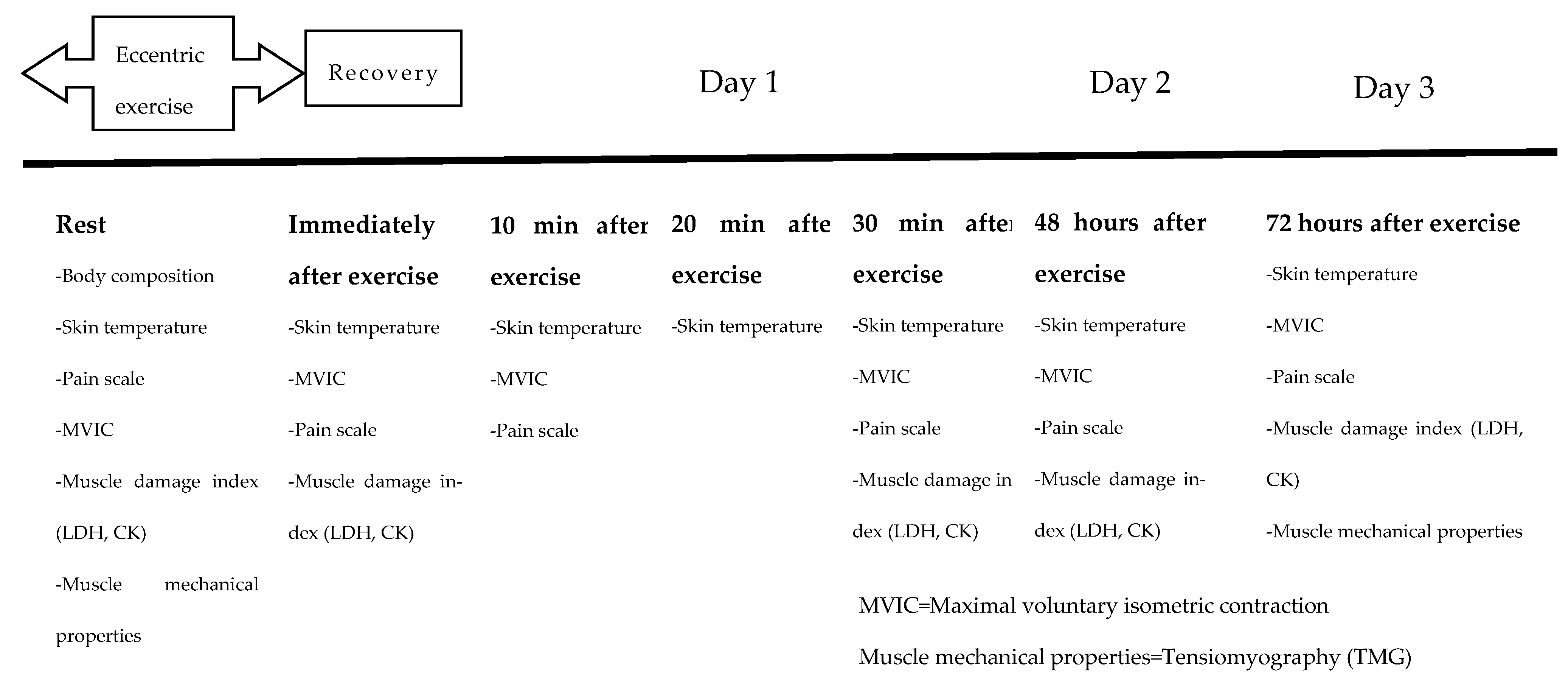
Figure 2.
The eccentric exercise and CWI treatment.


Table 1.
Formula for calculating average skin temperature.
| Average skin temperature=0. 3×(Chest+Upper arm)+0.2×(Thigh+Calf) |
Table 2.
Changes in skin temperature according to recovery treatment method.
| Variables | Treatment | Rest | IAE | 10min after exercise |
30min after exercise |
48hours after exercise |
72hours after exercise |
Sig | η ² |
| Average skin temperature (°C) |
Whole-body CWI (n=9) | 33.20 ±0.66 c,d |
32.72±0.70 c,d | 28.63±1.00#,+,e,f | 31.61±0.49+ | 33.23±0.49 | 33.10±0.82 | Treatment .761 | .022 |
| Lower-body CWI (n=9) | 32.55 ±0.50 c |
32.32±1.02 c | 30.84±1.39 d,e,f | 32.33±0.93 | 32.57±0.94 | 33.04±0.69 | Time .001* | .742 | |
| Control;Active recovery (n=9) | 32.40 ±0.78 c |
31.81±0.62 | 31.14±0.91d,e,f | 32.35±0.79 | 32.35±0.79 | 32.76±0.65 | Treatment .001*×Time | .488 | |
| Chest temperature (°C) |
Whole-body CWI (n=9) | 33.58 ±1.03 c |
32.29 ±0.99 c |
26.41±2.26#,+,d,e,f | 31.61±1.38#,+ | 33.72±0.83 | 33.44±1.72 | Treatment .111 | .167 |
| Lower-body CWI (n=9) | 33.17 ±1.16 |
31.61 ±1.18 |
31.90±1.40 | 33.23±1.58 | 32.84±1.27 | 33.19±1.36 | Time .001* | .595 | |
| Control;Active recovery (n=9) | 32.68 ±1.26 c |
31.40 ±0.97 |
30.41±1.02d,e,f | 32.77±1.71 | 33.44±1.58 | 33.11±1.74 | Treatment .001* ×Time |
.441 | |
| Thigh temperature (°C) |
Whole-body CWI (n=9) | 32.64 ±0.82 c |
32.97 ±1.51 c,d |
26.90±1.92+,d,e,f | 31.12±1.20 f | 32.94±0.73 | 32.86±0.50 | Treatment .423 | .069 |
| Lower-body CWI (n=9) | 32.33 ±1.22 c |
33.30±1.51 c | 29.17±2.47d,e,f | 31.79±1.03 | 32.22±1.18 | 32.77±0.81 | Time .001* | .691 | |
| Control;Active recovery (n=9) | 31.93 ±0.97 |
32.56±1.16 | 31.27±2.68 | 32.30±1.16 | 32.37±0.87 | 32.77±0.71 | Treatment ×Time.001* | .422 | |
| Upper-body temperature (°C) |
Whole-body CWI (n=9) | 33.67 ±0.50 |
33.43±0.80 | 33.22±1.07 | 32.92±0.96 | 33.58±0.75 | 33.18±0.91 | Treatment .036 | .242 |
| Lower-body CWI (n=9) | 32.42 ±0.61 |
32.87±1.28 | 32.87±1.79 | 33.18±1.08 | 32.78±0.85 | 32.89±0.84 | Time .399 | .041 | |
| Control;Active recovery (n=9) | 32.86 ±1.10 |
32.44±0.55 | 31.83±0.80 | 32.66±0.67 | 32.88±0.84 | 32.79±0.69 | Treatment ×Time .128 | .121 | |
| Lower-body temperature (°C) |
Whole-body CWI (n=9) | 32.55 ±1.12 c,d |
32.23 ±0.95 c,d |
26.63±1.41+,e,f | 30.41±0.67#,e,f | 32.18±0.80 | 32.79±0.58 | Treatment .206 | .140 |
| Lower-body CWI (n=9) | 32.01 ±0.66 c |
31.39±0.46 c | 28.00±2.30#,d,e | 30.18±0.58#,e,f | 32.13±1.47 | 32.79±0.66 | Time .001* | .755 | |
| Control;Active recovery (n=9) | 31.79 ±0.75 |
30.83±1.08 e,f | 31.11±0.88 | 31.39±0.94 | 32.15±0.52 | 32.26±0.80 | Treatment ×Time.001* | .529 |

Table 3.
Changes in MVIC according to recovery treatment method(%BW).
| Variables | Treatment | Rest | IAE | 30min after exercise |
48hours after Exercise |
72hours after exercise |
Sig | η ² |
|
MVIC (%BW) |
Whole-body (n=9) | 353.56 ±52.99 |
306.22 ±57.14 |
327.11 ±57.71 |
346.44 ±37.55 |
357.89 ±44.90 |
Treatment .131 | .156 |
| Lower-body (n=9) | 342.89 ±30.25 |
274.78 ±39.77 |
319.56 ±48.39 |
330.33 ±27.35 |
344.67 ±46.24 |
Time .001* | .466 | |
| Control;Active recovery(n=9) | 323.56 ±48.27 |
265.89 ±51.57 |
277.89 ±65.67 |
283.00 ±66.67 |
316.89 ±78.69 |
Treatment×Time .452 | .075 |
Values are mean±SD, *: p<.05, IAE: immediately after exercise, BW: body weight, *The values should be understood as a percentage of the body weight force.
Table 4.
Changes in pain score according to recovery treatment method.
| Variables | Treatment | Rest | IAE | 30min after exercise |
48hours after exercise |
72hours after exercise |
Sig | η2 |
| Pain scale (score) |
Whole-body CWI (n=9) | 0.67±1.12b,c | 7.11±2.14c,d,e | 2.89±1.36† | 1.11±1.53† | 1.22±1.20 | Treatment .001* | .486 |
| Lower-body CWI (n=9) | 0.78±1.30b,c | 6.33±1.50c,d,e | 2.56±1.01†,e | 1.00±1.23† | 0.44±0.53 | Time .001* | .826 | |
| Control;Active recovery (n=9) | 0.89±0.78b,c,d | 8.00±1.11c,d,e | 4.44±1.42e | 3.78±1.64e | 1.22±1.09 | Treatment*time .049* | .156 |
Values are mean±SD, *: p<.05., IAE: immediately after exercise; †: Compare to dynamic recovery, b: Difference from immediately post-exercise, c: Differences post-exercise 10minutes, d: Differences post-exercise 30minutes, e: Differences post-exercise 48hours, f: Differences post-exercise 72hours.
Table 5.
Changes in Muscle Damage Indices according to Recovery Treatment Method.
| Variables | Treatment | Rest | IAE | 30min after exercise |
48hours after exercise |
72hours after exercise |
Sig | η ² |
| CK (IU/L) |
Whole-body(n=9) | 207.56 ±77.40 |
230.00 ±78.34 |
240.89 ±77.28 |
311.33 ±160.75 |
235.44 ±88.94 |
Treatment .714 | .028 |
| Lower-body (n=9) |
209.22 ±89.34 |
251.33 ±106.12 |
241.56 ±106.14 |
360.44 ±168.68 |
308.11 ±183.98 |
Time .001* | .400 | |
| Control;Active recovery(n=9) | 175.00 ±74.05 |
189.44 ±41.36 |
196.56 ±52.85 |
391.11 ±184.16 |
261.11 ±109.28 |
Treatment*time .316 |
.092 | |
| LDH (U/L) |
Whole-body (n=9) |
249.63 ±40.67 |
275.25 ±52.01d,e |
232.50 ±38.70 |
204.88 ±46.55† |
198.13 ±47.35 |
Treatment .759 | .023 |
| Lower-body (n=9) |
224.88 ±41.52 |
241.25 ±48.44 |
234.00 ±47.85 e |
219.00 ±61.96† |
199.63 ±33.76 |
Time 001* | .378 | |
| Control;Active recovery(n=9) | 225.25 ±37.09 |
268.13 ±61.46 |
254.13 ±30.69 |
268.00 ±40.08 |
214.13 ±44.91 |
Treatment*time.027* | .171 |
Values are mean±SD, *: p<.05, IAE: immediately after exercise; †: Compare to dynamic recovery, d: Different post-exercise 48 hours, e: different post-exercise 72hours.
Table 6.
Changes in TMG according to recovery treatment method.
| Variables | Treatment | Rest | 30min after exercise |
48hours after exercise |
72hours after exercise |
Sig. | η ² |
| Dm(mm) | Whole-body(n=9) | 7.3±1.8ᵇ | 4.5±2.2ᶜ | 7.6±2.4 | 7.5±1.8 | Treatment .839 | .014 |
| Lower-body(n=9) | 7.3±1.4ᵇ | 4.2±2.2ᶜ | 7.3±2.4 | 6.4±2.8 | Time .001* | .485 | |
| Control;Active recovery(n=9) | 7.1±2.5ᵇ | 6.1±2.2ᶜ | 7.3±2.3 | 6.6±1.6 | Treatment*time.047* | .165 | |
| Tc(ms) | Whole-body(n=9) | 29.9±6.0 | 32.1±9.0 | 29.0±5.4 | 29.7±4.3 | Treatment .373 | .079 |
| Lower-body(n=9) | 27.9±3.6 | 28.6±6.2 | 27.6±3.8 | 25.6±5.1 | Time .044* | .125 | |
| Control;Active recovery(n=9) | 28.8±3.3 | 31.6±5.3 | 27.0±5.2 | 28.2±3.8 | Treatment*time .749 | .037 | |
| Tr(ms) | Whole-body(n=9) | 34.7±40.7 | 47.5±48.6 | 33.1±40.8 | 52.9±72.2 | Treatment .236 | .113 |
| Lower-body(n=9) | 13.7±4.1 | 22.3±12.7 | 26.8±27.1 | 19.1±21.2 | Time .194 | .066 | |
| Control;Active recovery(n=9) | 23.3±29.8 | 57.3±45.4 | 26.8±27.2 | 28.2±35.0 | Treatment*time .498 | .067 |
Values are mean±SD, *: p<.05, IAE: immediately after exercise; b: Differences post-exercise 30 minutes, c: Differences c: Differences post-exercise 48 hours.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



