
Submitted:
07 April 2025
Posted:
07 April 2025
You are already at the latest version
Abstract
Diabetic nephropathy (DN) is a serious complication of Diabetes mellitus. This clinical condition is diagnosed through detection of microalbuminuria. Molecular biomarkers such as MicroRNA-192 may play a role in early diagnosis of this condition. The objective of this study was to assess the serum concentration of MicroRNA-192 in different stages of DN in comparison to a group of healthy individuals. The study was a retrospective case-control study included three groups. Group I included patients with early DN, group II included patients with late DN and group III included healthy control subjects. Blood samples were obtained from each participant and subjected to full biochemical study including creatinine, albumin and detection of MicroRNA-192 by real time polymerase chain reaction. There was significant difference between MicroRNA-192 levels in the three groups (P=0.001). There was significant increase in MicroRNA-192 level in group I (1.35±7 0.5) compared to group II (0.65±7 0.2, P3=0.001) and group III (0.83±7 0.3, P1=0.001). There was significant reduction in MicroRNA-192 level in group II compared to group III (P2=0.001). The study of diagnostic accuracy of MicroRNA-192 in the patients revealed good accuracy in the differentiation of early DN from control subjects (sensitivity 62% and specificity 86%) and good accuracy in the differentiation of early from late DN (sensitivity and specificity each 82%). The present study highlights that MicroRNA-192 is a good diagnostic tool for early detection of DN. MicroRNA-192 correlates significantly with estimated glomerular filtration rate, albuminuria, and renal functions tests. MicroRNA-192 might play role in the development of DN.
Keywords:
diabetic nephropathy
; DM type 2
; MicroRNA‐192
; albuminuria
; eGFR
1. Introduction
Diabetic nephropathy (DN) is a prevalent consequence of diabetes mellitus, occurring in approximately 9% of people with either type 1 or type 2 diabetes. It has to do with protein in the urine, the glomeruli of the kidneys getting bigger, the rate at which they filter blood slowing down, and the formation of scar tissue in the kidneys [1].
There is a need for expeditious and noninvasive techniques to identify this advancing diabetic nephropathy. Scientists have acknowledged the involvement of microRNAs (miRNAs) in the pathological mechanism of DN. MiRNAs are small, endogenous, noncoding RNA molecules composed of 19–24 nucleotides. MiRNA acts by binding to the 3' untranslated region of a target gene's mRNA. MiRNAs control gene expression through processes that happen after transcription, specifically by making it easier for mRNA to break down or stopping translation [2,3]. Therefore, miRNAs control a wide range of biological processes in cells, such as cell growth, cell specialization, programmed cell death, apoptosis, and passive cell death.
MiR-192 is encoded by a gene located on chromosome 11. Two fully developed transcripts, miR-192 (miR-192-5p) and miR-192* (miR-192-3p), constitute it [4]. Differentiation, proliferation, apoptosis, epithelial-mesenchyme transition, angiogenesis, metabolism, inflammatory responses, oxidative stress, and drug resistance are some of the physiological and pathological processes that MiR-192 controls [5,6]. Inhibiting the miR-192-targeted genes leads to various effects, such as the degradation of mRNA and the suppression of protein translation. A range of ailments, including respiratory, digestive, circulatory, and urinary system disorders, link to the dysregulation of MicroRNA-192.
The renal cortex is the primary location of MicroRNA-192 (miR-192), suggesting its potential role in the development of DN [7].
There have been mixed results from different studies about the levels of miR-192 in blood, urine, and kidney tissue from people with different stages of diabetic nephropathy. These data suggest that the serum's concentration of miR-192 can serve as an early diagnostic marker for diabetic nephropathy. A higher level of miR-192 in the later phases may indicate a deterioration of DN [7]. So, the point of this study was to compare the amount of miRNA-192 in the blood of people with different stages of diabetic nephropathy (DN) to a group of healthy people.
2. Material and Method
This retrospective case-control study enrolled patients from the outpatient clinics of Mansoura University Hospital in Egypt between January 2022 and March 2024. The study also used age- and sex-matching controls. The time-non-probability sampling method, which relied on the study period during which the recruited patients met the inclusion criteria for DN staging, determined the patient sample size.
The patients' eligibility criteria were that they were adults aged 18 or older, had no previous history of renal problems, and had type 2 DM. The study excluded patients with renal illnesses caused by other factors, such as autoimmune disorders or malignancies. We categorize the patients according to their albuminuria levels and estimated glomerular filtration rate (eGFR). Group I consisted of diabetic patients with normal albuminuria levels below 30 mg/g and an estimated glomerular filtration rate higher than 60 mL/min/1.73 m2. Group II, on the other hand, included diabetic patients with late diabetic nephropathy, characterized by albuminuria levels over 30 mg/g and an eGFR lower than 60 mL/min/1.73 m2 [8]. The control group consisted of adult individuals of matched ages and sexes who had normal fasting blood glucose levels below 100 mg/dL, no history of kidney diseases, and normal results on kidney function testing. Every participant underwent a comprehensive medical history and physical assessment.
We conduct diagnostic examinations to analyze and evaluate many aspects of a subject's medical or chemical composition.
2.1. Laboratory Study
We obtained a blood sample and urine sample from each participant using meticulous aseptic techniques, and we also collected an early morning midstream urine sample and stored it in a sterile container. After isolating the serum, we used it to determine the concentration of creatinine. To separate the urine, we used centrifugation and collected the liquid that was above the sediment. Then, we used the Cobas s201 system (made by Roche Diagnostics, 9115 Hague Road, PO Box 50457, Indianapolis, USA) to check the levels of albumin and creatinine in the urine. We stored the serum at a temperature of -80 °C until we conducted our investigation on micRNA-192. The Cobas C system employs the immunoturbidimetric technique (mg/l) for quantifying urine albumin. The g/l Cobas 201s system, manufactured by Beckman Coulter, utilizes the Jaffe method for quantifying urine creatinine levels. We employed the Cockcroft-Gault formula, developed in 1973, to calculate the estimated glomerular filtration rate (eGFR). The eGFR is determined using the formula: eGFR = {(140–age) x weight/(72xSCr)}x 0.85 (for females). The term SCr refers to serum creatinine.
2.1.1. Investigation of MicroRNA-192
.
2.1.2. Purification of RNA and Reverse Transcriptase
The RNA was isolated from the serum samples using the Direct-zol RNA Miniprep Plus kit (Cat # R2072, Zymo Research, Irvine, CA, USA).
We conducted reverse transcription on the extracted RNA from the samples using reverse transcriptase and real-time PCR.
2.1.3. Real-Time PCR
The experiment employed real-time quantitative polymerase chain reaction (qPCR), with the primer sequences for miR-192 being 5′-GCGGCGGCTGACCTATGAATTG-3′ and 5′-ATCCAGTGCAGGGTCCGAGG-3′. The primer sequences for U6 were 5′-TCCGATCGTGAAGCGTTC-3′ and 5′-GTGCAGGGTCCGAGGT-3′. The reaction was conducted by subjecting it to incubation at 50°C for 2 minutes, followed by subsequent incubation at 95°C for 10 minutes. Subsequently, we performed a cyclic reaction, alternating between a temperature of 95°C for 10 seconds and a temperature of 60°C for 60 seconds. We iterated this cycling procedure for a cumulative total of 45 rounds. We utilized ABI Company's ABI PRISM 7900 system for the analysis. The expression level of miR-192 was quantified using the 2 Ct methods, with U6 acting as the internal reference [9,10].
3. Statistical Analysis
The data was analyzed by SPPS24. The numerical data was expressed as mean and standard deviation (SD) and comparison was performed by ANOVA test. P was considered significant if below 0.,05. Receiver operator characteristics (ROC) were used to evaluate the diagnostic accuracy of different markers in patients with diabetic nephropathy. P value was considered statistically significant when less than 0.05.
4. Results
The study included 150 subjects classified into three groups: group I patients with early diabetic nephropathy, group II patients with late diabetic nephropathy, and group III age- and sex-matched healthy control subjects. There was a significant increase in blood urea nitrogen (BUN), creatinine, fasting blood glucose, HB1c, and albumin in the urine in groups I and II compared to group III (P = 0.001). The duration of DM was significantly longer in group III (7.7± 7 3.3 years) compared to group II (5.23 ± 72.8, P = 0.001). The estimated glomerular filtration rate was significantly lower in groups I and II compared to group III (P = 0.001). Also, the albumin/creatinine ratio had significantly increased values in groups I and II compared to group III (P = 0.001). Table 1.
There was a significant difference between MicrRNA-192 levels in the three groups (P = 0.001). There was a significant increase in MicroRNA-192 level in group I (1.35± 7 0.5) compared to group II (0.65± 7 0.2, P3=0.001) and group III (0.83± 7 0.3, P1=0.001). There was a significant reduction in the MicroRNA-192 level in group II compared to group III (P2 = 0.001), see Table 2.P between groups (ANOVA test)
Post hoc test
P1 between control and early DM nephropathy
P2 between the uremic group and the control
P3 between early DM nephropathy and uremic group
Table 3 summarizes the correlation between MicrRNA-192 levels and various clinical and biochemical parameters in the studied subjects. There was a significant negative correlation between creatinine, BUN, urinary albumin, urinary albumin/creatinine ratio, and MicroRNA-192 level (P = 0.001). There was a significant negative correlation between the duration of DM and MicroRNA-192 (P = 0.001). There was a significant positive correlation between eGFR and MicroRNA-192 (P = 0.001) (Table 3).
A study that looked at how well MicroRNA-192 could tell the difference between early diabetic nephropathy and control subjects had a sensitivity of 62% and a specificity of 86%. It also showed that it could tell the difference between early diabetic nephropathy and late diabetic nephropathy with an accuracy of 82% (Table 4, Figure 1 and Figure 2).
5. Discussion
One frequent complication of long-term diabetes mellitus that can lead to end-stage renal failure is diabetic nephropathy [11,12]. In diabetic nephropathy, extracellular matrix buildup and thickening of the glomerular basement membrane make the mesangial enlargement, which leads to extracellular deposition in the glomerulus [13]. Numerous cytokines and microRNAs are among the many variables that contribute to these problems [14,15]. Albuminuria is the first concerning symptom of diabetic kidney disease (DN). It progresses from microalbuminuria to macroalbuminuria, indicating advanced kidney disease. The development from macroalbuminuria to renal failure is irreversible [16].
In the present study, group I had a significantly higher level of MicroRNA-192 (1.35± 7 0.5) than group II (0.65± 7 0.2, P3=0.001) and group III (0.83± 7 0.3, P1=0.001).
Researchers found that the kidney had an enrichment of microRNA-192 compared to other organs, indicating the kidney's essential role [17].
In a previous meta-analysis study, seventy percent of clinical trials suggested that miR-192 might increase early in the DN to play a protective role. In contrast, seventy-eight percent of experimental studies suggested that miR-192 might have a pathogenic role in the DN. Some proteins that microRNA-192 targets are ZEB1, ZEB2, SIP1, GLP1R, and Egr1. It also interacts with signaling pathways like SMAD/TGF-β and PTEN/PI3K/AKT. These interactions can cause DN through fibrosis, extracellular matrix deposition, and epithelial-to-mesenchymal transition (EMT).
Early diabetic nephropathy is associated with an increase in MicroRNA-192, which raises the possibility of using it as a biomarker for DN early identification. Additional validation research requires larger sample sizes [18]. MicroRNA-192 could have a role in the early etiology of diabetic nephropathy. There is typically an imbalance in the expression of several microRNAs, including miR-192, in diabetic nephropathy. According to research, oxidative stress, inflammation, and fibrosis are a few of the pathogenic processes that might result in diabetic nephropathy due to upregulated miR-192 expression. It appears to support the buildup of extracellular matrix proteins in the kidney, which causes more renal damage and ultimately results in renal fibrosis [19].
Adding more miRNA-192 may stop the TGF-β1 signaling pathway and the production of Zeb1 and Zeb2, which would stop the fibrosis in the kidneys. It was discovered that TGF-β1-inhibited miRNA-192 production sped up DN renal fibrosis. This miRNA-192 targeted Zeb1/2 and turned on the TGF-β1 signaling pathway [20].
New therapeutic approaches for the prevention and treatment of diabetic nephropathy may result from our growing understanding of the function played by miR-192 and other microRNAs in this condition.
MicroRNA-192 is still important in the latter stages of diabetic nephropathy, particularly in the uremic stage. Although studies on miR-192 in the late uremic stage are less numerous than those on the early phases, it is still possible that miR-192 plays a role in the development of diabetic nephropathy.
In contrast to control patients and early diabetic nephropathy, the current investigation revealed a significant decrease in MicroRNA-192 levels in late diabetic nephropathy. In the lab, scientists did tests and discovered that renal tubular cells grown with lots of glucose and TGF-β1 had low levels of miR-192. On the other hand, renal biopsy samples from people who already had DN had high levels of miR-192. Researchers connected this to tubulointerstitial fibrosis and a drop in eGFR [20].MicroRNA-192 may be involved in pathways that control the unique features of late diabetic nephropathy, renal fibrosis, and hypertrophy. Some diabetic patients' dysregulation may contribute to the continuation of these degenerative processes, which in turn may result in end-stage renal disease (ESRD) [21].
More research is required to fully comprehend the unique role that miR-192 plays in the late uremic stage of diabetic nephropathy, as well as its potential as a therapeutic target for this advanced stage of the disease.
So, while research has linked MicroRNA-192 to higher levels in the early stages of diabetic nephropathy, its role may change as the disease gets worse, especially in end-stage renal disease. The expression of miR-192 may decline in more severe forms of diabetic nephropathy, such as end-stage renal disease (ESRD). The drop in MicroRNA-192 in late-stage diabetic nephropathy could be due to several things, such as severe fibrosis, loss of renal function, and damage to kidney cells. [21] MicroRNA-192 and eGFR exhibited a strong positive connection (P = 0.001). Furthermore, the length of DM and MicroRNA-192 exhibited a strong inverse relationship. A previous study found a correlation between renal fibrosis acceleration, DN GFR reduction, and a decrease in MicroRNA-192 levels. Additionally, the longer the period, the lower the expression of miR-192 [21]. In a separate study, Wang et al. [22] found that TGF-β1 decreased the amount of miR-192 in human podocytes, mesangial cells, and rat proximal tubular cells. The biopsy results from diabetes patients showed a decrease in miR-192 levels.
MicroRNA-192 may mediate senescence and oxidative stress, two important pathogenic processes in DN development. Diabetes degree and duration impact microRNA-192 levels, potentially serving as early indicators for DN [23].
MicroRNA-192 showed a negative correlation with both renal function and albuminuria in the current investigation. These results show that changes in the amount of miR-192 in the blood could be useful biomarkers for finding kidney damage and the risk of diabetic kidney disease early [18].The current study demonstrated the potential utility of MicroRNA-192 as a DN early biomarker. ROC analysis suggests that MicroRNA-192 can distinguish patients with early diabetic nephropathy from healthy individuals and those with late nephropathy. We discovered this result online in conjunction with a prior study [18]. One study that looked at miRNA-192 biomarkers in kidney disease found that miR-192 in urine extracellular vesicles can help find people who are just starting to develop diabetic kidney disease (DN) [24]. The microRNA-192 (miR-192) ROC curve demonstrates that miR-192 levels can indicate differences between different cell groups. This suggests that miR-192 may be a useful biomarker for finding people who have early-stage diabetic nephropathy. It also shows good performance in differentiating early diabetic nephropathy from control subjects. As a result, MicroRNA-192 may be able to show early changes in certain biological processes in the kidney. It may also be useful as a biomarker for microvascular problems in diabetes [25]. The present study highlights that MicroRNA-192 is a good diagnostic tool for the early detection of diabetic nephropathy. MicroRNA-192 correlates significantly with the estimated glomerular filtration rate, albuminuria, and renal function tests. MicroRNA-192 may contribute to the development of diabetic nephropathy.
Supplementary Materials
Highlights file is attached
Authors Contribution: Mohamad Mohsen Motawea, shared in the clinical data collection, and draft preparation of the article. Fady azmy Kyrillos shared in the clinical data collection and analysis. Mayada Khalel shared in data analysis and draft preparation of the article. Ismail Kandil shared in revision of the draft and the statistical analysis. Ahmed Mohsen Faheem shared in the laboratory study, the draft preparation of the article data analysis of the study, and revision of the draft of the article. Maysaa El Sayed Zaki shared in the laboratory study, the draft preparation of the article data analysis of the study and revision of the draft of the article. Mostafa Abdelsalam Ramadan shared in the clinical data collection, and draft preparation of the article.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Institutional Review Board Statement
All methods were performed by the ethical standards as laid down in the Declaration of Helsinki and its later amendments or comparable ethical standards. The ethical approval of the study was obtained from the ethical committee of Mansoura Faculty of Medicine (R.24.05.2618 ) and written approval was obtained from each child's parent.
Data Availability Statement
The datasets generated and analyzed during the current study are available in the fighshare repository at: https://doi.org/10.6084/m9.figshare.25999315.v1
Acknowledgments
Not applicable
Conflicts of Interest
There is no conflict of interest for any of the authors.
References
- Shahin DHH: Sultana R, Farooq J, Taj T, Khaiser UF, Alanazi N, Alshammari MK, Alshammari MN, Alsubaie FH, Asdaq SMB, Alotaibi AA, Alamir AA, Imran M and Jomah S. Insights into the uses of traditional plants for diabetes nephropathy: a review. Curr Issues Mol Biol 2022, 44, 2887–2902. [Google Scholar] [CrossRef] [PubMed]
- Ma X, Lu C, Lv C, et al. The expression of miR-192 and its significance in diabetic nephropathy patients with different urine albumin creatinine ratio. J Diabetes Res. 7894.
- Martinez-Hernandez R, Marazuela M. MicroRNAs in autoimmune thyroid diseases and their role as biomarkers. Best Pract Res Clin Endocrinol Metab 2023, 37, 101741. [Google Scholar] [CrossRef] [PubMed]
- Krattinger R, Bostrom A, Schioth HB, Thasler WE, Mwinyi J, Kullak-Ublick GA. 13microRNA-192 suppresses the expression of the farnesoid X receptor. Am J PhysiolGastrointest Liver Physiol 2016, 310, G1044–51. [Google Scholar] [CrossRef] [PubMed]
- Mishan MA, Tabari M, Parnian J, Fallahi J, Mahrooz A, Bagheri A. Functional mechanisms of miR-192 family in cancer. Genes Chromosomes Cancer (2020). [CrossRef]
- Ren FJ, Yao Y, Cai XY, Fang GY. Emerging role of MiR-192-5p in human diseases. Front Pharmacol 2021, 12, 614068. [Google Scholar] [CrossRef] [PubMed]
- Wan X, Liao J, Lai H, Zhang S, Cui J, Chen C. Roles of microRNA-192 in diabetic nephropathy: the clinical applications and mechanisms of action. Front Endocrinol (Lausanne). 2023, 14, 1179161. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Kidney Disease: Improving Global Outcomes (KDIGO) Diabetes Work Group. KDIGO 2020 Clinical Practice Guideline for Diabetes Management in Chronic Kidney Disease. Kidney Int. 2020, 98, S1–S115. [Google Scholar] [CrossRef] [PubMed]
- Jiang F, Li C, Han J, Wang L. Diagnostic Value of Combination of MicroRNA-192 in Urinary Sediment and B-Ultrasound for Bladder Cancer. Technology in Cancer Research & Treatment. [CrossRef]
- Elsayed, A.G.A. , Badr, D.F., El Kheir, N.Y.A. et al. Prevalence of extended-spectrum beta-lactamase and molecular detection of blaTEM, blaSHV, and blaCTX-M genotypes among gram-negative Bacilli isolates from hospital acquired infections in pediatrics, one institutional study. Ital J Pediatr 2024, 50, 31. [Google Scholar] [CrossRef] [PubMed]
- Shahbazian H and Rezaii I: Diabetic kidney disease; review of the current knowledge. J Renal Inj Prev. 2013, 2, 73–80.
- Dronavalli S, Duka I and Bakris GL: The pathogenesis of diabetic nephropathy. Nat Clin Pract Endocrinol Metab. 2008, 4, 444–452. [CrossRef] [PubMed]
- Hu C, Sun L, Xiao L, Han Y, Fu X, Xiong X, Xu X, Liu Y, Yang S, Liu F and Kanwar YS: Insight into the mechanisms involved in the expression and regulation of extracellular matrix proteins in diabetic nephropathy. Curr Med Chem. 2015, 22, 2858–2870. [CrossRef] [PubMed]
- Arora MK and Singh UK: Molecular mechanisms in the pathogenesis of diabetic nephropathy: An update. Vascul Pharmacol. 58:259–271.
- Chang AS, Hathaway CK, Smithies O and Kakoki M: Transforming growth factor-β1 and diabetic nephropathy. Am J Physiol Renal Physiol. 2016, 310, F689–F696. [CrossRef] [PubMed]
- Lutale JJ, Thordarson H, Abbas ZG and Vetvik K: Microalbuminuria among type 1 and type 2 diabetic patients of African origin in Dar Es Salaam, Tanzania. BMC Nephrol. 8:22007.
- Sun Y, Koo S, White N, Peralta E, Esau C, Dean NM, Perera RJ. Development of a micro-array to detect human and mouse microRNAs and characterization of expression in human organs. Nucleic Acids Res. 2004, 32, e188. [Google Scholar] [CrossRef] [PubMed]
- Al-Kafaji G, Al-Muhtaresh HA. Expression of microRNA-377 and microRNA-192 and their potential as blood-based biomarkers for early detection of type 2 diabetic nephropathy. Mol Med Rep. 2018, 18, 1171–1180. [Google Scholar] [CrossRef] [PubMed]
- Tang J, Yao D, Yan H, Chen X, Wang L, Zhan H. The Role of MicroRNAs in the Pathogenesis of Diabetic Nephropathy. Int J Endocrinol. 2019, 2019, 8719060. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Krupa A, Jenkins R, Luo DD, Lewis A, Phillips A and Fraser D: Loss of microRNA-192 promotes fibrogenesis in diabetic nephropathy. J Am Soc Nephrol. 2010, 21, 438–447. [CrossRef] [PubMed]
- Ma X, Lu C, Lv C, Wu C, Wang Q. The Expression of miR-192 and Its Significance in Diabetic Nephropathy Patients with Different Urine Albumin Creatinine Ratio. J Diabetes Res. 2016, 2016, 6789402. [CrossRef] [PubMed] [PubMed Central]
- Wang B, Herman-Edelstein M, Koh P, Burns W, Jandeleit-Dahm K, Watson A, Saleem M, Goodall GJ, Twigg SM, Cooper ME, Kantharidis P. E-cadherin expression is regulated by miR-192/215 by a mechanism that is independent of the profibrotic effects of transforming growth factor-β. Diabetes. 2010, 59, 1794–1802. [Google Scholar] [CrossRef] [PubMed]
- Gong Z, Banchs PAP, Liu Y, Fu H, Arena VC, Forno E, Libman I, Ho J, Muzumdar R. Serum α-KL, a potential early marker of diabetes complications in youth with T1D, is regulated by miRNA 192. Front Endocrinol (Lausanne). 2022, 13, 937093. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Jia Y, Guan M, Zheng Z, Zhang Q, Tang C, Xu W, Xiao Z, Wang L and Xue Y: miRNAs in urine extracellular vesicles as predictors of early-stage diabetic nephropathy. J Diabetes Res. 2016, 79327652016.
- El-Monem A, A. , Mahfouz M H., Mohamed M A., Abd El-Aziz H G, Hussien N. Microrna 192 Gene Expression in Type II Diabetic Nephropathy. The Egypt J of Hosp Med 2017, 68, 885–893. [Google Scholar] [CrossRef]
Figure 1.
MicroRNA-192 in early diabetic nephropathy compared to control subjects.
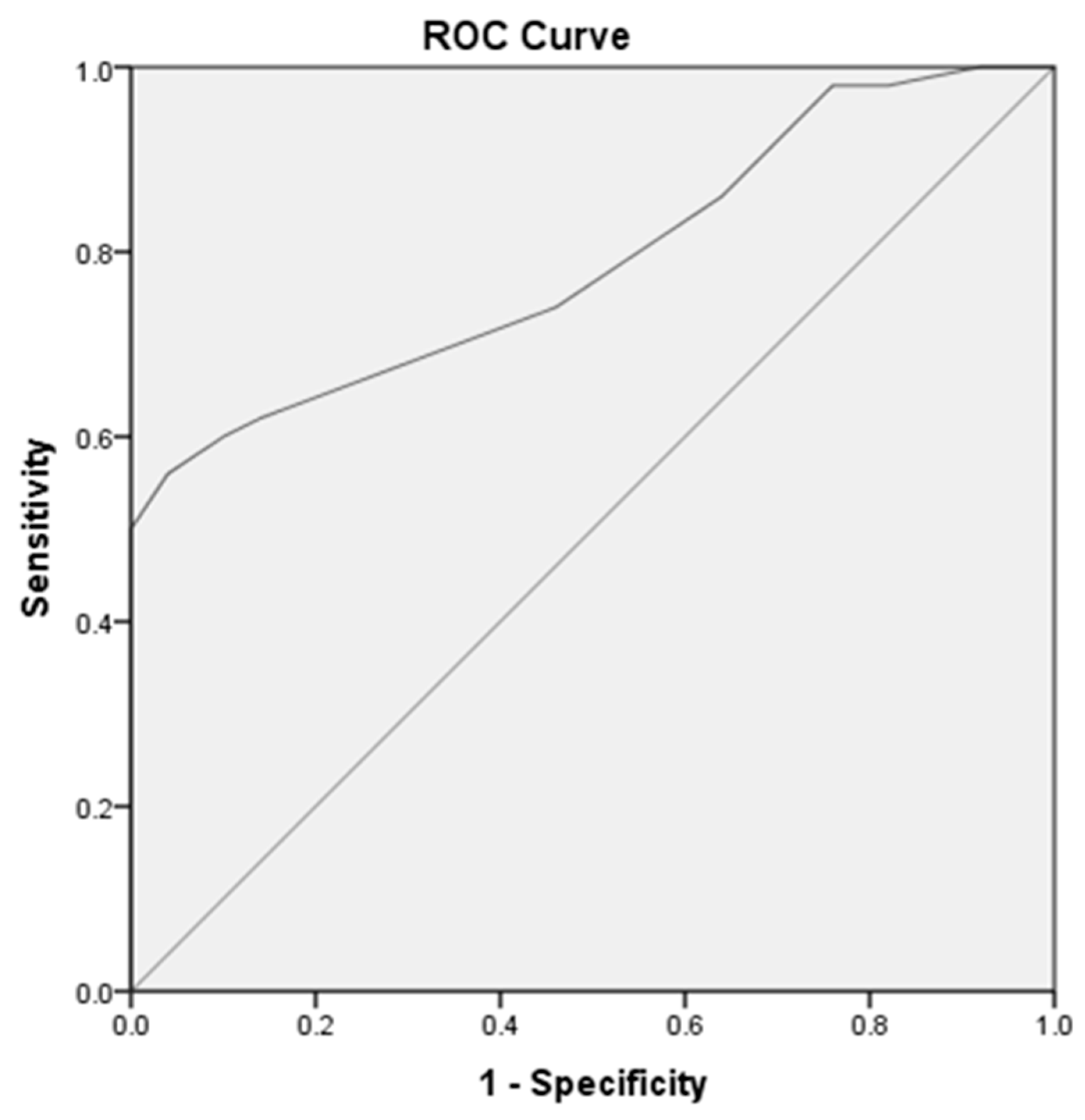
Figure 2.
MicroRNA-192 in early diabetic nephropathy compared to late diabetic nephropathy.
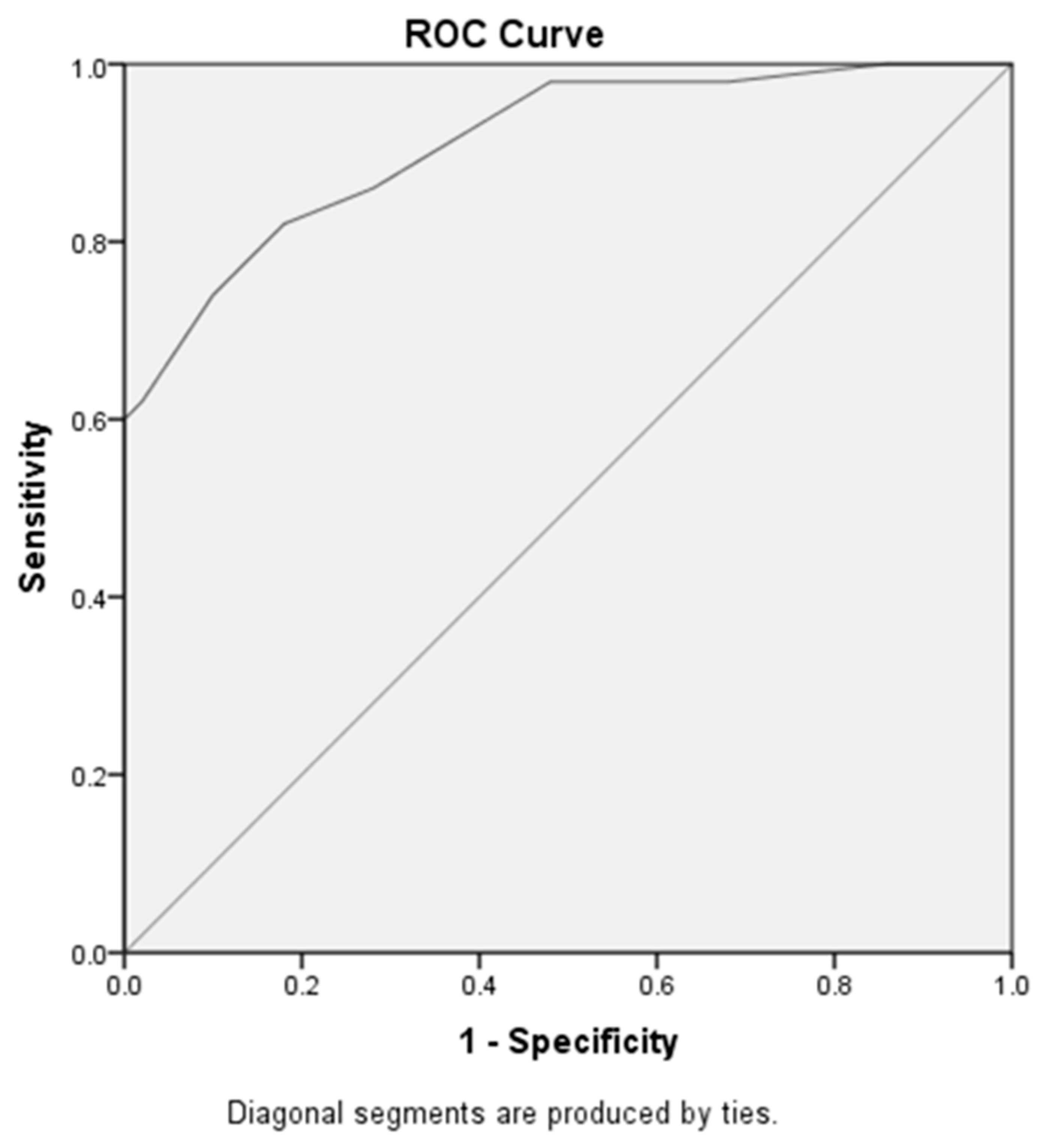

Table 1.
Demographic and biochemical findings in the studied groups.
| Group III (n=50) |
Group I (n=50) |
Group II (n=50) |
P | |
|---|---|---|---|---|
| Sex Male Female |
34 16 |
29 21 |
32 18 |
0.58 |
| age | 51.8 ± 7.37 | 52.28± 7 6.15 | 53.34± 7 5.47 | 0.47 |
| BUN | 26.38± 7 2.77 | 27.68± 7 2.83 | 56.8± 7 4.73 | 0.001 |
| creatinine | 0.92± 7 0.2 | 1.02± 7 0.13 | 4.1± 7 0.6 | 0.001 |
| Fasting blood glucose | 90.1± 7 11.4 | 150.4 ± 740.4 | 158.2± 7 60.4 | 0.001 |
| HB1c | 4.4± 7 0.6 | 8.9 ± 7 2.01 | 8.5 ± 71.8 | 0.001 |
| duration | 5.23 ± 72.8 | 7.7± 7 3.3 | 0.001 | |
| Albumin | 4.04± 7 0.45 | 3.9 ± 7 0.2 | 3.7 ± 70.35 | 0.001 |
| Albumin in urine | 11.0± 7 4.9 | 17.01 ± 73.6 | 83.3 ± 716.6 | 0.001 |
| Urinary creatinine | 1. 71 ±0.4 | 1.1± 7 0.3 | 0.7± 7 0.13 | 0.001 |
| Albumin/creatinine ratio | 12.5± 7 7.4 | 16.0± 71 5.0 | 117.6± 7 27.23 | 0.001 |
| eGFR | 90.2 ± 719.2 | 69.6 ± 710.33 | 17.3± 7 4.02 | 0.001 |
Table 2.
Comparison of MicroRNA-192 between studied groups.
| MicroRNA-192 | Group III (n=50) |
Group I (n=50) |
Group II (n=50) |
P |
|---|---|---|---|---|
| MicroRNA-192 | 0.83± 7 0.3 | 1.35± 7 0.5 | 0.65± 7 0.2 | P=0.001 P1=0.004 P2=0.001 P3=0.001 |
Table 3.
Correlation between different clinical and biochemical parameters and MicroRNA-192.
| MicroRNA-192 | |
|---|---|
| Creatinine R P |
-.651 0.001 |
| eGFR R P |
0.744 0.001 |
| Urinary creatinine R P |
0.488 0.001 |
| Urinary albumin R P |
-.616 0.001 |
| Duration R P |
-0.302 0.001 |
| Urinary albumin/creatinine ratio R P |
-.624 0.001 |
| eGFR R P |
.354** .000 |
| BUN R P |
-.419-** .000 |
Table 4.
Diagnostic accuracy of MicroRNA-192 in diabetic nephropathy.
| Area under curve | Cut off value | Sensitivity | Specificity | ||
|---|---|---|---|---|---|
| MicroRNA-192 at early diabetic nephropathy versus control subjects | 0.79 | 1,05 | 62% | 86% | |
| MicroRNA-192 at early diabetic nephropathy versus late diabetic nephropathy | .91 |
0.85 |
82% | 82% |
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



