
Submitted:
03 April 2025
Posted:
03 April 2025
You are already at the latest version
Abstract
Background/Objectives: Inflammatory bowel diseases (IBD) include Crohn’s disease (CD) and ulcerative colitis (UC). The availability of an increasing number of new mol-ecules approved for IBD treatment has increased our ability and aspirations to change their natural history. The STRIDE II consensus is the current established suggested strategy for IBD management. Primary objective of this study is to describe the clinical history of IBD in post-STRIDE era, and to quantify the burden of IBD in terms of hos-pitalization rate. Secondary objective is to estimate the 5-years risk of intestinal resec-tion among IBD patiesnts. Methods: Observational time series analysis was conducted on population data; retrospective data from Jan 2011 was collected for Local Health Authority “Roma 1” population (circa 1.5 million residents). Prospective data from hospitalizations among residents since Jan 2018 was also collected. Hospitalization and surgery events among newly diagnosed patients (n= 556) were collected and pro-spectively followed since Jan 2018. Kaplan-Mayer survivor functions were proposed, considering surgical intervention as primary outcome. Results: Current IBD preva-lence is estimated to be 218 (77.2 CD, 141.1 UC) cases/100,000ppl. Incidence trend slowly increased during the last decade up to 5.3 (CD) and 9.4 (UC) cas-es/100,000ppl/year. Yearly hospitalization remained constant near 16.5%, while 6-years risk of surgery is 36% for CD, and 20% for UC. Conclusions: Incidence of IBD increased in the last decades, with substantial stability in the incidence of surgeries and hospitalizations. Thus, current IBD management has only a small effect on changing the natural history of the disease.
Keywords:
inflammatory bowel disease
; crohn’s disease
; ulcerative colitis
; surgery for IBD
; IBD epidemiology
; population study
1. Introduction
Inflammatory Bowel Diseases (IBD), including Crohn’s Disease (CD) and Ulcerative Colitis (UC), are chronic inflammatory conditions with a multifactorial etiopathogenesis affecting the gastrointestinal system, and are characterized by periods of relapse and remission and a progressive course leading to bowel damage and disability [1,2]. Clinical, endoscopic and radiologic assessment are often used in attempt to predict long- and mid- term outcome [3,4].
The burden of IBD is increasing worldwide, and in the past decade IBD emerged as a public health challenge [5,6]. The estimated prevalence (>0.3%) continues to rise in Western countries, with a high burden of disease in North America, Oceania, and Europe, while newly industrialised countries in Asia, Africa and South America are showing a progression in IBD prevalence as they become more westernized and urbanized [7].
Four epidemiological stages of IBD have been proposed to explain the evolution of IBD across epidemiologic transition periods. The 4 stages are: (1) emergence, (2) acceleration of incidence, (3) compounding prevalence and (4) prevalence equilibrium. Western world Countries (i.e., most countries in North America, Western Europe, and Oceania) are in stage 3 (compounding prevalence), where prevalence exceeds 0.5%. Newly industrialized countries in Asia, Latin America, and the Middle East are in stage 2 (acceleration in incidence), with low prevalence but rapidly increasing incidence [8].
In the last decade, a paradigm shift related to the management of IBD occurred [9]. Quality of life (QoL) and clinical endpoints are both target of intervention. Prevention measures (such as smoking prevention, reducing stress factors, and focusing especially on younger age classes) have been proposed in recent times, with a debatable role in causal effect, but with notable impact on symptoms reduction [10,11,12]. Alternative measures for QoL improvement have also been proposed, such as telemedicine usage, whose usage is already suggested for patient monitoring and supervision by several clinical studies, and even recommended in a recent position paper by the European Federation of Internal Medicine Societies [13,14]. On the pharmacological front, the availability of an increasing number of new molecules (including adjuvants, biological therapies and small molecules) has increased our ability and aspirations to reach beyond the conventional treatment goal, such as clinical remission [15,16,17]. Despite the current therapies, a proportion of patients experience relapses and continuous inflammation, which occasionally requires surgical removal of parts of the intestine [18]. The treat-to-target approach, addressed to obtain an even more ambitious objective, represents the current strategy in IBD management [19,20]. The STRIDE I, proposed in 2015, was the first consensus oriented to this paradigmatic shift [21]. This valuable lesson was subsequently developed in the STRIDE II consensus in 2018 [22]. However, despite the novel treatment availability and the new tight-control strategies, including targeted and customized therapies, and attention towards the patients’ immunocompetence or immunosuppression via dedicated vaccination schedules, the burden of disease, and in particular the reduction of risk of surgery and hospitalisation, represents a significant unmet need [23,24].
1.1. IBD Within the Healthcare System in Italy
In the Italian National Healthcare System (NHS), the ticket is a contribution fee individuals are required to pay for certain health services. They do not pay the entire cost of the service; instead, they contribute a portion, and the rest is covered by the NHS. Depending on clinical and\or socio-economic conditions, specific individuals have exemption right from paying the ticket. To obtain exemption, specific criteria must be met. In particular, for IBD patients, after endoscopic and histological evaluation, a gastroenterology specialist can certify the illness condition by issuing a healthcare certificate that exempts IBD patients from ticket payment. After the diagnosis, the healthcare approval by NHS is quite fast, usually requiring up to two weeks [25]. After approval, all IBD-related health services are registered by NHS as provided to the specific patient. A table of procedures the NHS classifies as IBD-related is available in Appendix Table A1.
Concerning hospital services, Italian NHS is a Beveridge Health System which has adopted DRG payments to hospitals; Italian DRGs follow the US (CMS) model ver. 24.0. In order to obtain a DRG payment, each structure must generate and transmit an Hospital Discharge Forms (SDO—Scheda Dimissione Ospedaliera), in anonymous form, for every admitted patient [26]. SDOs are transmitted yearly to Regional Governments, who proceed to refund the hospital structures, and to the Ministry of Health for statistical and administrative purposes.
1.2. Study Objectives
The primary objective of this study is to define the incidence and prevalence of IBD in the recent timespan, describing the current trend concerning hospitalisation rate. Secondary objective is to quantify the risk of surgery among IBD patients, in order to understand if STRIDE II guidelines diffusion and application yielded to a change in global IBD-related hospitalisation rates and surgery events.
2. Materials and Methods
2.1. Study Design and Reporting
The study was designed in two components. First comes an epidemiological description of IBD in the interested territory, conducted as a population-based interrupted time series, with data collected form routinely used administrative records referring to the years 2011-2021. Second, data of all patients with new IBD diagnosis since 2018 was collected and analysed prospectively. The REporting of studies Conducted using Observational Routinely-collected Data (RECORD) guidelines were used for reporting [27].
2.2. Population and Data Sources
The population is comprised of all living residents in the administrative jurisdiction of “Roma 1” Local Health Authority (LHA) in Rome, Italy, which comprises the North-Western sector of the Urban territory of Rome, Italy. It hosts in its own territory more than 15 hospital structures, including 2 directly managed hospital facilities, 3 public-run Hospitals, 13 Emergency Departments (of 22 in the Rome metropolitan area) [28].
Data regarding new IBD diagnosis was available from 1 Jan 2011 to 31 Dec 2022. This data was used for incidence and prevalence estimation. Data regarding older diagnosis was available, but with no extra information regarding the diagnosis date; this was used only for prevalence estimation. Data regarding Hospitalisation was available from 1 Jan 2018 to 1 May 2024, and was used to describe hospitalisation trends.
Data was collected in pseudo-anonymized form via the digital Business Intelligence (BI) platform routinely used in LHA Roma 1: the ID code of each person is represented by an encrypted string, but it is still possible to connect health events attributable to the same individual. Using this pseudo-anonymized ID, information from several sources (Exemptions registry, SDO database).
The study included person-level linkage between exemptions registry and SDO repository. Linkage was provided automatically by Roma 1 BI software. A detailed list of administrative datasets used in this study are provided in Appendix Table A2.
2.3. Outcome Definitions
The date each patient obtained IBD ticket exemption was used as proxy for IBD diagnosis (there may be a few days in delay between clinical diagnosis and administrative exemption recording). Patients have a strong incentive to get their exemption recorded, since they get no charge for visits and drugs related to their pathology. For this reason, there is very low chance of missing diagnosis data.
For the retrospective section of the study, as per current practice in population studies, we defined an IBD-related hospitalisation based on the presence of an International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) discharge diagnosis of either CD or UC as the most responsible comorbid, or primary inter-service or inter-hospital transfer diagnosis [29,30].
For the prospective section of the study, surgical treatments unrelated to IBD, including infectious, biliopancreatic, and traumatic, have not been considered as IBD-related and were therefore excluded from analysis. A comprehensive list of codes and procedures included and excluded is available in Appendix Table A3.
2.4. Statistical Methods
2.4.1. Retrospective Analysis
Monthly incidence of IBD (distinct as either UC or CD) among general population in LHA Roma 1 was calculated, for each age range (stratified in 10-year age groups) and for each observation year; standardization was performed over current (2024) LHA Roma1 population composition. Age-standardised incidence was calculated yearly, and separate linear regression models were used to test if any statistically significant increase was observed during the 10-years timespan. As sensitivity analysis, monthly data was filtered using Baxter-King method for time series decomposition [31]. Trend component was isolated and compared with actual observation (after the flat mean of residuals was added back, to correct for underestimation due to having filtered out both stochastic and cyclic components) after simple smoothing using a 3-period simple autoregressive moving average (3-ARMA).
Monthly hospitalisation trend since 2018 among the cohort of IBD patients currently residing in Roma 1 (N=2191) was calculated using time series decomposition, as per primary analysis. Monthly hospitalisation rate was therefore calculated since Jan 2018 to May 2024. Hospitalisation trend was also described as yearly percentage among IBD patients.
Statistical analysis was done at the Department of Biomedicine and Prevention, University of Rome “Tor Vergata”. MS Excel v.2016 and Stata v.17 were used for calculation and graph drawing.
2.4.2. Prospective Analysis
A cohort of 556 patients diagnosed since January 2018 were included in the prospective analysis. All hospitalisations were screened until May 2024, and recorded interventions were considered as per primary outcome if a relevant ICD-9-CM procedure was registered. A table of relevant procedures is available in Appendix Table A3.
Kaplan-Meier function was then proposed to estimate the cumulative risk for surgery among IBD patients, both in raw data, and after adjustment for gender and age at diagnosis.
2.4.3. Bias and Bias Reduction
A possible source of bias lies in the underestimation of actual IBD cases due to misdiagnosis, or difficult diagnosis, especially for people coming from rural areas, where IBD may need differential diagnosis with other gastro-intestinal affections. The risk of our results being significantly affected is however very low in magnitude, because most of the included population comes from an heavy urbanized area, and because difficult-to-diagnose IBD should contribute minimally to overall hospitalizations and treatment effects.
Another possible source of bias is linked to the retrospective nature of this study, since we could not select patients by excluding confounding factors. No information was available regarding clinical presentation, nor specific risk factors such as drinking or smoking habits; however, adjustment for gender and age at diagnosis was possible, and as such we performed it in inferential analysis.
3. Results
3.1. IBD Epidemiology
Details on yearly IBD incidence are provided in Table 1. 2859 patients were diagnosed with IBD from Jan 2011 to Dec 2021. Raw Incidence of IBD increased slowly in the observed period: new diagnoses of IBD raised from 184 in 2011, to 341 in 2021, raising from 14.7 to 28.5 x 100,000 ab per year (average: 21.2). Figure 1 depicts monthly observations and trend component, filtered for cyclical effects via the Baxter-King method. Figure 2 depicts the population composition by age and gender, both currently and at the time of the diagnosis. For the 2191 patients diagnosed since 2011 and currently residing in Roma 1, hospitalisation trend in the last 5 years was calculated (Figure 3). Raw hospitalisation rate kept somewhat constant during the study period, with 1.38 hospitalisations/100,000 ab per month. This roughly translates to 16.5% yearly hospitalisation rate among IBD patients. Prevalence of IBD is estimated to be 218.3 cases/100,000ppl, with 77.2 cases of CD and 141.1 cases of UC.
3.2. Prospective Cohort
Of the 556 patients constituting the prospective cohort, 194 (34.9%) had CD and 362 (65.1%) UC. Demographic details are available in Table 2. The mean follow-up time was close to 6 years (SD: 10 months).
Among the 196 CD patients (110 M, 86F), 19 (9.8%) surgery events occurred. 2 of them coincided with the diagnosis moment, thus acute presentation can be estimated to happen in 1.0% of all cases. A Cox proportional hazards model, gender and age at diagnosis did not show any significant impact. Kaplan-Meier function shows a 27% risk of surgery at 6 years from diagnosis, after adjusting for gender and age at diagnosis, while unadjusted estimates were of 12% risk of surgery after 6 years.
Among the 362 UC patients (190 M, 172 F), 15 (4.1%) surgery interventions occurred, with acute presentation observed in 12 cases (3.3% of patients). Adjusted Kaplan-Meier function shows a 2% risk of having surgery at 6 years, while observed surgery risk was close to 5%. (Figure 4).
4. Discussion
4.1. Key Results
A small increase in IBD incidence in the last decade was observed in our population study, with an average yearly estimated incidence of 21.2 cases x 100,000 ab. This increasing trend has also been observed elsewhere, for both CD and UC [6,32,33]. The reasons for this increase are largely unknown. Both improved diagnostic accuracy and greater patient awareness could have contributed to the rise in new IBD diagnoses. Nevertheless, unknown environmental factors may also play a key role in increasing IBD prevalence [34].
Robust data from a review of population-based studies (in the pre-STRIDE era) showed that 27% and 50% of CD patients require surgery 5 and 10 years after diagnosis, respectively, with a hospitalization rate of 20% per year. However, in these studies, no data from the biological era were available [35,36]. In our study, the Kaplan-Meier analysis showed the 6-year risk of surgery was 27% and 2% from diagnosis in CD and UC, respectively (adjusted for gender and age at diagnosis), while the hospitalization rate was 16.5% for IBD patients.
4.2. Strengths and Limitations
A significant strength of this study is the usage of data with little to no missing records. This was possible because informatics systems do not allow the treating physician to proceed with a medical record when information on exemption, diagnosis or clinical procedure is missing; also the physician is warned when apparent incongruences are detected by the system (such as a surgical procedure registered within a psychiatric ward DRG), allowing to correct occasional mistakes. Moreover, usage of population databanks allowed us to have a minimal risk of excluding actual IBD patients from our analysis. This is also true for procedures where the patients were lifted from paying a contribution fee, for the prescription charge exemption gets recorded and linked to the specific procedure.
Another strength of the study is that, during the considered period, no substantial modifications in IBD management strategy occurred. No new molecules were approved, and the STRIDE II approach was proposed at the beginning of the enrolment period. This aspect makes the results reported extremely representative of the present situation. However, baseline characteristics concerning relevant factors that can contribute to the risk of surgery, such as smoking habits and disease pattern, were not available in our database.
4.3. Interpretation and Generalisability
The availability of an increasing number of new molecules approved for IBD treatment has heightened our aspirations to alter the disease's natural history. Changes in the paradigm of IBD management with treat-to-target strategies and the spread of the STRIDE approach are significant sources of bias that make it difficult to evaluate the role of biological therapies in the decline of IBD-related surgery and hospitalization. Likewise, the widespread use of new therapies impacts the changing incidence of these outcomes.
In recent times, few population-based studies have attempted to address the evolution of IBD-related surgery and hospitalization over the years. A UK population-based cohort study evaluated the 5-year risk of surgery in four cohorts followed from 2000 to 2017. The 5-year cumulative risk of surgery was 20.4% in cohort 1 [2000–2004], 18.3% in cohort 2 [2005–2008], 14.7% in cohort 3 [2009–2013], and 13.0% in cohort 4 [2014–2017]. Conversely, the prevalence of biological therapies prescriptions increased in each of the cohorts considered. Thus, the authors concluded that increased and earlier use of biologic therapy in CD patients corresponded with a decreasing requirement for surgery over time [37]. On the other hand, a Canadian population-based interrupted time series study evaluated the effect of the marketplace introduction of infliximab on population rates of hospitalizations and surgeries. Infliximab did not produce significant declines in the rates of CD-related hospitalizations (OR 1.06, 95% CI 0.811 to 1.39) or surgeries (OR 1.10, 95% CI 0.810 to 1.50), or in the rates of UC-related hospitalizations (OR 1.22, 95% CI 1.07 to 1.39) or colectomies (OR 0.933, 95% CI 0.54 to 1.61) [29]. In Italy, another retrospective study conducted over a different population showed that the introduction of biological therapies had only a slight impact on the occurrence of surgery in CD patients over a long observation period, contributing to delaying the first intestinal resection [38]. Furthermore, despite increased post-operative use of anti-TNFα agents in CD patients in the last two decades, the impact of this strategy on the risk of long-term re-operation rate has been modest [39].
5. Conclusions
A slight increase in the raw incidence of IBD was observed in the last decades, with substantial stability in the incidence of surgeries and hospitalizations. However, the estimated incidence and prevalence of IBD are still slightly lower than in other Western countries. This could be due to underdiagnoses or an actual lower incidence among the Italian population. Hospitalization and surgery rates have also remained stable over the past decade. Therefore, change in current IBD management appears to have had only a small effect on altering the natural history of the disease.
Author Contributions
Conceptualization, D.B., M.C., M.V. and A.V.; methodology, F.I., M.M., M.V., C.V. and A.V.; software, A.B.; validation, G.B., M.M., M.V. R.M. and G.L.; formal analysis, F.I., M.M, M.V., and A.V. ; investigation, A.B., C.V., A.V. ; resources, A.V., M.M. and R.M.; data curation, A.V.; writing—original draft preparation, F.I., M.M., M.V., A.V. ; writing—review and editing, A.B., D.B., G.B., M.C. A.Vis. and G.L.; visualization, A.V.; supervision, G.L., and G.B.; project administration, A.Vis.; funding acquisition, M.M. and R.M.. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
This is a register-based research project with no contact with patients, their relatives, or treating physicians. Ethical Review board Lazio 1 approved the study (prot. n° 0593/2024). All authors had access to the study data and have reviewed and approved the final manuscript.
Informed Consent Statement
Not applicable.
Data Availability Statement
Data are property of ASL Roma 1 Public Health Authority. Data are available from the Roma 1 Institutional Data Access (e-mail at: protocollo@pec.aslroma1.it) for researchers who meet the criteria for access to confidential data.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| ARMA | Auto-Regressive Moving Average |
| CD | Crohn’s Disease |
| DRG | Diagnosis-Related Group |
| IBD | Inflammatory Bowel Diseases |
| ICD-9-CM | International Classification of Diseases, 9th Revision, Clinical Modification |
| LHA | Local Health Authority |
| NHS | National Healthcare System |
| QoL | Quality of Life |
| SDO | Scheda di Dimissione Ospedaliera (hospital discharge form) |
| UC | Ulcerative Colitis |
Appendix A

Table A1.
List of possible services provided by NHS for free to patients with IBD diagnosis.
| HEALTH SERVICE WITH TICKET EXEMPTION | TYPE | NOTE |
|---|---|---|
| CHECK-UP VISIT NECESSARY TO MONITOR THE DISEASE, THE MOST FREQUENT COMPLICATIONS AND TO PREVENT FURTHER WORSENING | ||
| VENOUS BLOOD SAMPLING | ||
| ALANINE AMINOTRANSFERASE (ALT) (GPT) | ||
| ALPHA 1 ACID GLYCOPROTEIN | ||
| ASPARTATE AMINOTRANSFERASE (AST) (GOT) | ||
| REFLEX BILIRUBIN (cut-off >1 mg/dL unless more restrictive cut-offs are defined at a regional level. Included: Direct and Indirect Bilirubin | ||
| COBALAMIN (VIT. B12) | ||
| FERRITIN | ||
| IRON | ||
| FOLATE | ||
| ALKALINE PHOSPHATASE | ||
| GAMMA-GLUTAMILTRANSFERASE (gamma GT) | ||
| PANCREATIC LIPASE | ||
| POTASSIUM | ||
| BLOOD PROTEINS (ELECTROPHORESIS) Included: Total protein determination 90.38.5 | ||
| SODIUM | ||
| TRANSFERRIN | ||
| BLOOD CHROME: BLOOD CYTOMETRY EXAM AND DIFFERENTIAL LEUKOCYTE COUNT Hb, GR, GB, HCT, PLT, IND. DERIV. Including any microscopic control | ||
| C-REACTIVE PROTEIN (Quantitative) | ||
| BLOOD SEDIMENTATION RATE (ESR) | ||
| RADIOLOGY | ||
| TRADITIONAL | DOUBLE CONTRAST COLON ENEMA | |
| DOUBLE CONTRAST SMALL BOW ENEMA | ||
| ULTRASOUND | ULTRASOUND OF THE COMPLETE ABDOMEN | possible Colour-Doppler integration |
| ULTRASOUND OF THE INTESTINAL LOOP | ||
| DENSITOMETRY | BONE DENSITOMETRY. LUMBAR DXA | No more than 1 in 12-18 months |
| BONE DENSITOMETRY. FEMORAL DXA | No more than 1 in 12-18 months | |
| BONE DENSITOMETRY. ULTRADISTAL DXA | No more than 1 in 12-18 months | |
| ENDOSCOPY | ||
| UPPER SITES | ESOPHAGOGASTRODUODENOSCOPY [EGDS] | |
| BIOPSY DURING EGDS | Brushing or washing for sample collection | |
| BIOPSY OF THE SMALL INTESTINE DURING ENTEROSCOPY | Brushing or washing for sample collection | |
| LOWER SITES | TOTAL COLONOSCOPY WITH FLEXIBLE ENDOSCOPE | |
| RECTOSIGMOIDOSCOPY WITH FLEXIBLE ENDOSCOPE | ||
| PROCTORECTORECTOSIGMOIDOSCOPY WITH RIGID ENDOSCOPE | ||
| SINGLE SITE BIOPSY OF THE LARGE INTESTINE DURING TOTAL COLONOSCOPY WITH FLEXIBLE TUBE | Brushing or washing for sample collection | |
| BIOPSY DURING PROCTORECTOSIGMOIDOSCOPY | Brushing or washing for sample collection |
Table A2.
Roma 1 Administrative databases used to Capture Study Information.
| VARIABLE | DATABASE |
|---|---|
| IBD PATIENT STATUS | Roma 1 Ticket exemptions Database |
| IBD PATIENTS DIAGNOSIS DATE | Roma 1 Ticket exemptions Database |
| DEMOGRAPHIC VARIABLES | Roma 1 Healthcare registered persons Database |
| SURGERY INTERVENTIONS | Roma 1 Hospital records administrative Database |
| HOSPITALISATIONS | Roma 1 Hospital records administrative Database |
Table A3.
Table of ICD-9CM codes used as surgical intervention outcome in prospective cohort analysis. *: excluded for Ulcerative Colitis cohort.
Table A3.
Table of ICD-9CM codes used as surgical intervention outcome in prospective cohort analysis. *: excluded for Ulcerative Colitis cohort.
| ICD CODE | MEANING |
|---|---|
| IBD-RELATED (INCLUDED): | |
| * 42.33 | Endoscopic Excision Or Destruction Of Lesion Or Tissue Of Esophagus |
| * 42.52 | Intrathoracic Esophagogastrostomy |
| * 43.91 | Total Gastrectomy With Intestinal Interposition |
| * 45.30 | Endoscopic Excision Or Destruction Of Lesion Of Duodenum |
| * 45.62 | Other Partial Resection Of Small Intestine |
| * 45.72 | Open And Other Cecectomy |
| 45.73 | Open And Other Right Hemicolectomy |
| 45.75 | Open And Other Left Hemicolectomy |
| 45.79 | Other And Unspecified Partial Excision Of Large Intestine |
| 45.8 | Total Intra-Abdominal Colectomy |
| 45.91 | Small-To-Small Intestinal Anastomosis |
| 45.93 | Other Small-To-Large Intestinal Anastomosis |
| 45.94 | Large-To-Large Intestinal Anastomosis |
| 46.02 | Resection Of Exteriorized Segment Of Small Intestine |
| 46.81 | Intra-Abdominal Manipulation Of Small Intestine |
| 48.63 | Other Anterior Resection Of Rectum |
| 48.69 | Other Resection Of Rectum |
| 49.93 | Other Incision Of Anus |
| 54.21 | Laparoscopy |
| * 54.3 | Excision Or Destruction Of Lesion Or Tissue Of Abdominal Wall Or Umbilicus |
| * 54.63 | Other Suture Of Abdominal Wall |
| * 83.39 | Excision Of Lesion Of Other Soft Tissue |
| NOT IBD-RELATED (EXCLUDED): | |
| 45.16 | Esophagogastroduodenoscopy [EGD] with closed biopsy |
| 45.19 | Other diagnostic procedures on small intestine |
| 45.23 | Colonoscopy |
| 45.24 | Flexible sigmoidoscopy |
| 45.25 | Closed [endoscopic] biopsy of large intestine |
| 45.26 | Open biopsy of large intestine |
| 45.27 | Intestinal biopsy, site unspecified |
| 45.28 | Other diagnostic procedures on large intestine |
| 45.29 | Other diagnostic procedures on intestine, site unspecified |
| 48.23 | Rigid proctosigmoidoscopy |
| 48.24 | Closed [endoscopic] biopsy of rectum |
| 48.25 | Open biopsy of rectum |
| 48.29 | Other diagnostic procedures on rectum, rectosigmoid and perirectal tissue |
| 48.36 | [Endoscopic] polypectomy of rectum |
| 49.21 | Anoscopy |
| 49.29 | Other diagnostic procedures on anus and perianal tissue |
| 50.11 | Closed (percutaneous) [needle] biopsy of liver |
| 51.10 | Endoscopic retrograde cholangiopancreatography [ERCP] |
| 51.11 | Endoscopic retrograde cholangiography [ERC] |
| 54.24 | Closed [percutaneous] [needle] biopsy of intra-abdominal mass |
| 46.10 | Colostomy, not otherwise specified |
| 46.11 | Temporary colostomy |
| 46.20 | Ileostomy, not otherwise specified |
| 46.21 | Temporary ileostomy |
| 46.23 | Other permanent ileostomy |
| 46.51 | Closure of stoma of small intestine |
| 48.73 | Closure of other rectal fistula |
| 49.51 | Left lateral anal sphincterotomy |
| 49.59 | Other anal sphincterotomy |
| 00.34 | Imageless computer assisted surgery |
| 25.1 | Excision or destruction of lesion or tissue of tongue |
| 25.2 | Partial glossectomy |
| 27.29 | Other diagnostic procedures on oral cavity |
| 27.42 | Wide excision of lesion of lip |
| 27.49 | Other excision of mouth |
| 27.56 | Other skin graft to lip and mouth |
| 27.79 | Other operations on uvula |
| 30.09 | Other excision or destruction of lesion or tissue of larynx |
| 30.22 | Vocal cordectomy |
| 40.41 | Radical neck dissection, unilateral |
| 41.5 | Total splenectomy |
| 42.33 | Endoscopic excision or destruction of lesion or tissue of esophagus |
| 42.52 | Intrathoracic esophagogastrostomy |
| 43.89 | Other partial gastrectomy |
| 43.91 | Total gastrectomy with intestinal interposition |
| 44.19 | Other diagnostic procedures on stomach |
| 44.43 | Endoscopic control of gastric or duodenal bleeding |
| 44.67 | Laparoscopic procedures for creation of esophagogastric sphincteric competence |
| 44.68 | Laparoscopic gastroplasty |
| 45.13 | Other endoscopy of small intestine |
| 45.42 | Endoscopic polypectomy of large intestine |
| 46.81 | Intra-abdominal manipulation of small intestine |
| 46.85 | Dilation of intestine |
| 48.76 | Other proctopexy |
| 48.93 | Repair of perirectal fistula |
| 49.11 | Anal fistulotomy |
| 49.12 | Anal fistulectomy |
| 49.73 | Closure of anal fistula |
| 49.93 | Other incision of anus |
| 50.22 | Partial hepatectomy |
| 50.3 | Lobectomy of liver |
| 51.04 | Other cholecystotomy |
| 51.22 | Cholecystectomy |
| 51.23 | Laparoscopic cholecystectomy |
| 51.83 | Pancreatic sphincteroplasty |
| 51.98 | Other percutaneous procedures on biliary tract |
| 54.11 | Exploratory laparotomy |
| 54.19 | Other laparotomy |
| 54.21 | Laparoscopy |
| 54.91 | Percutaneous abdominal drainage |
| 54.95 | Incision of peritoneum |
| 70.52 | Repair of rectocele |
| 70.73 | Repair of rectovaginal fistula |
| 86.63 | Full-thickness skin graft to other sites |
| 86.69 | Other free skin graft |
| 86.70 | Pedicle or flap graft, not otherwise specified |
| 86.72 | Advancement of pedicle graft |
| 86.74 | Attachment of pedicle or flap graft to other sites |
| 86.83 | Size reduction plastic operation |
| 96.22 | Dilation of rectum |
References
- Maaser, C.; et al. ECCO-ESGAR Guideline for Diagnostic Assessment in IBD Part 1: Initial diagnosis, monitoring of known IBD, detection of complications. Journal of Crohn’s and Colitis 13, 144-164K (2019). [CrossRef]
- Volkers, A. G.; et al. Fecal Calprotectin, Chitinase 3-Like-1, S100A12 and Osteoprotegerin as Markers of Disease Activity in Children with Crohn’s Disease. Gastrointestinal Disorders, 4, 180–189 (2022).
- Laterza, L.; et al. Multiparametric Evaluation Predicts Different Mid-Term Outcomes in Crohn’s Disease. Dig Dis, 36, 184–193 (2018). [CrossRef]
- Bohra, A. , Van Langenberg, D. R. & Vasudevan, A. Intestinal Ultrasound in the Assessment of Luminal Crohn’s Disease. Gastrointestinal Disorders, 4, 249–262 (2022). [CrossRef]
- Caviglia, G. P.; et al. Epidemiology of Inflammatory Bowel Diseases: A Population Study in a Healthcare District of North-West Italy. JCM, 12, 641 (2023). [CrossRef]
- Kaplan, G. G. The global burden of IBD: from 2015 to 2025. Nat Rev Gastroenterol Hepatol, 12, 720–727 (2015). [CrossRef]
- Ng, S. C.; et al. Worldwide incidence and prevalence of inflammatory bowel disease in the 21st century: a systematic review of population-based studies. Lancet, 390, 2769–2778 (2017). [CrossRef]
- Buie, M. J.; et al. Global Hospitalization Trends for Crohn’s Disease and Ulcerative Colitis in the 21st Century: A Systematic Review With Temporal Analyses. Clinical Gastroenterology and Hepatology, 21, 2211–2221 (2023). [CrossRef]
- Dignass, A. , Rath, S., Kleindienst, T. & Stallmach, A. Review article: Translating STRIDE-II into clinical reality – Opportunities and challenges. Aliment Pharmacol Ther, 58, 492–502 (2023). [CrossRef]
- Marino, M. G. , Fusconi, E., Magnatta, R., Panà, A. & Maurici, M. Epidemiologic Determinants Affecting Cigarette Smoking Cessation: A Retrospective Study in a National Health System (SSN) Treatment Service in Rome (Italy). Journal of Environmental and Public Health, 2010, 1–9 (2010). [CrossRef]
- Zaghini, F.; et al. The influence of work context and organizational well-being on psychophysical health of healthcare providers. La Medicina del Lavoro, 111, 306–320 (2020). [CrossRef]
- Saeid Seyedian, S.; et al. A review of the diagnosis, prevention, and treatment methods of inflammatory bowel disease. JMedLife, 12, 113–122 (2019). [CrossRef]
- Pietrantonio, F.; et al. Intra- and Extra-Hospitalization Monitoring of Vital Signs—Two Sides of the Same Coin: Perspectives from LIMS and Greenline-HT Study Operators. Sensors, 23, 5408 (2023). [CrossRef]
- Pietrantonio, F.; et al. Applications to augment patient care for Internal Medicine specialists: a position paper from the EFIM working group on telemedicine, innovative technologies & digital health. Front. Public Health, 12, 1370555 (2024). [CrossRef]
- Gordon, H.; et al. ECCO Guidelines on Therapeutics in Crohn’s Disease: Medical Treatment. Journal of Crohn’s and Colitis jjae091 (2024). [CrossRef]
- Raine, T.; et al. ECCO Guidelines on Therapeutics in Ulcerative Colitis: Medical Treatment. Journal of Crohn’s and Colitis 16, 2–17 (2022). [CrossRef]
- Vinci, A.; et al. Cannabinoid Therapeutic Effects in Inflammatory Bowel Diseases: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Biomedicines, 10, 2439 (2022). [CrossRef]
- Arosa, L. , Camba-Gómez, M. & Conde-Aranda, J. Neutrophils in Intestinal Inflammation: What We Know and What We Could Expect for the Near Future. Gastrointestinal Disorders, 4, 263–276 (2022). [CrossRef]
- Viscido, A.; et al. Systematic review and meta-analysis: the advantage of endoscopic Mayo score 0 over 1 in patients with ulcerative colitis. BMC Gastroenterol, 22, 92 (2022). [CrossRef]
- Maconi, G.; et al. Factors correlated with transmural healing in patients with Crohn’s disease in long-term clinical remission on anti-TNF medication. Digestive and Liver Disease S1590865824007849 (2024). [CrossRef]
- Peyrin-Biroulet, L.; et al. Selecting Therapeutic Targets in Inflammatory Bowel Disease (STRIDE): Determining Therapeutic Goals for Treat-to-Target. American Journal of Gastroenterology, 110, 1324–1338 (2015). [CrossRef]
- Turner, D.; et al. STRIDE-II: An Update on the Selecting Therapeutic Targets in Inflammatory Bowel Disease (STRIDE) Initiative of the International Organization for the Study of IBD (IOIBD): Determining Therapeutic Goals for Treat-to-Target strategies in IBD. Gastroenterology, 160, 1570–1583 (2021). [CrossRef]
- Casella, G.; et al. Vaccination in Inflammatory Bowel Disease: Utility and Future Perspective. Gastrointestinal Disorders, 2, 175–192 (2020). [CrossRef]
- Bodini, G.; et al. Response to COVID-19 Vaccination in Patients with Inflammatory Bowel Disease on Biological Treatment. Gastrointestinal Disorders, 4, 77–83 (2022). [CrossRef]
- Definizione e aggiornamento dei livelli essenziali di assistenza, di cui all’articolo 1, comma 7, del decreto legislativo 30 dicembre. Decreto del presidente del consiglio dei ministri (2017).
- Sheaff, R.; et al. Managerial workarounds in three European DRG systems. JHOM, 34, 295–311 (2020). [CrossRef]
- Nicholls, S. G.; et al. The REporting of Studies Conducted Using Observational Routinely-Collected Health Data (RECORD) Statement: Methods for Arriving at Consensus and Developing Reporting Guidelines. PLoS, 10, e0125620 (2015). [CrossRef]
- Furia, G.; et al. Appropriateness of frequent use of emergency departments: A retrospective analysis in Rome, Italy. Front. Public Health, 11, 1150511 (2023). [CrossRef]
- Murthy, S. K.; et al. Introduction of anti-TNF therapy has not yielded expected declines in hospitalisation and intestinal resection rates in inflammatory bowel diseases: a population-based interrupted time series study. Gut, 69, 274–282 (2020). [CrossRef]
- Hou, J. K.; et al. Accuracy of Diagnostic Codes for Identifying Patients with Ulcerative Colitis and Crohn’s Disease in the Veterans Affairs Health Care System. Dig Dis Sci, 59, 2406–2410 (2014). [CrossRef]
- Baxter, M. & King, R. G. Measuring Business Cycles: Approximate Band-Pass Filters for Economic Time Series. Review of Economics and Statistics, 81, 575–593 (1999). [CrossRef]
- Kuenzig, M. E.; et al. Twenty-first Century Trends in the Global Epidemiology of Pediatric-Onset Inflammatory Bowel Disease: Systematic Review. Gastroenterology, 162, 1147-1159.e4 (2022). [CrossRef]
- Wang, R. , Li, Z., Liu, S. & Zhang, D. Global, regional and national burden of inflammatory bowel disease in 204 countries and territories from 1990 to 2019: a systematic analysis based on the Global Burden of Disease Study 2019. BMJ Open, 13, e065186 (2023). [CrossRef]
- Szilagyi, A. Relationship(s) between obesity and inflammatory bowel diseases: possible intertwined pathogenic mechanisms. Clin J Gastroenterol, 13, 139–152 (2020). [CrossRef]
- Peyrin-Biroulet, L. , Loftus, E. V., Colombel, J.-F. & Sandborn, W. J. The Natural History of Adult Crohn’s Disease in Population-Based Cohorts. American Journal of Gastroenterology, 105, 289–297 (2010). [CrossRef]
- Solberg, I. C.; et al. Clinical Course in Crohn’s Disease: Results of a Norwegian Population-Based Ten-Year Follow-Up Study. Clinical Gastroenterology and Hepatology, 5, 1430–1438 (2007). [CrossRef]
- Jenkinson, P. W.; et al. Temporal Trends in Surgical Resection Rates and Biologic Prescribing in Crohn’s Disease: A Population-based Cohort Study. Journal of Crohn’s and, 14, 1241–1247 (2020). [CrossRef]
- Valvano, M.; et al. The long-term effect on surgery-free survival of biological compared to conventional therapy in Crohn’s disease in real world-data: a retrospective study. BMC Gastroenterol, 23, 438 (2023). [CrossRef]
- Aratari, A.; et al. Crohn’s disease after surgery: Changes in post-operative management strategies over time and their impact on long-term re-operation rate—A retrospective multicentre real-world study. Aliment Pharmacol Ther, 59, 1579–1588 (2024). [CrossRef]
Figure 1.
IBD monthly incidence (x 100,000 ab) with trend component (with 95% Confidence Interval) and linear fit. 2011-2021.
Figure 1.
IBD monthly incidence (x 100,000 ab) with trend component (with 95% Confidence Interval) and linear fit. 2011-2021.
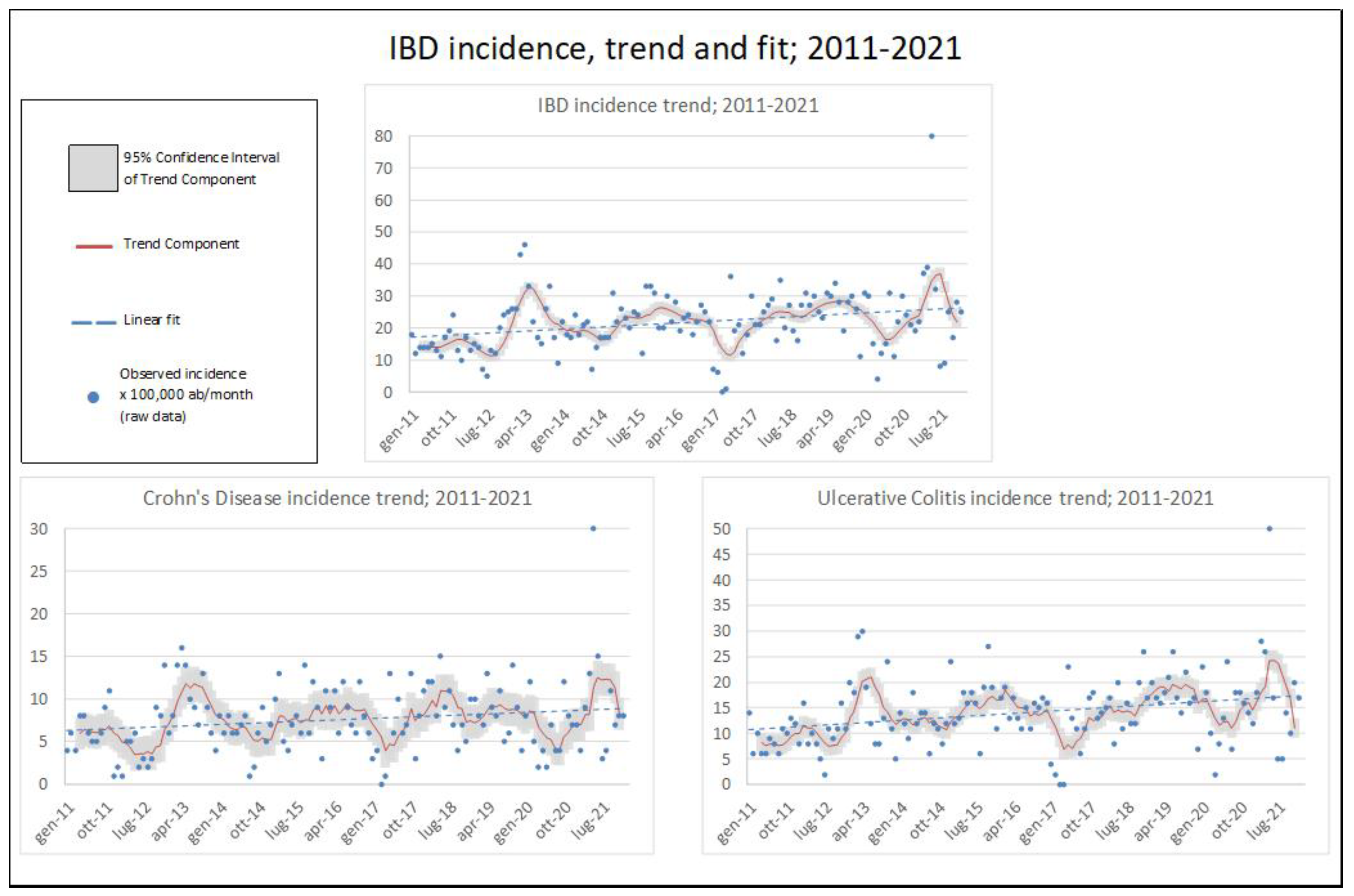
Figure 2.
IBD prevalence at May 2024: age and gender composition.
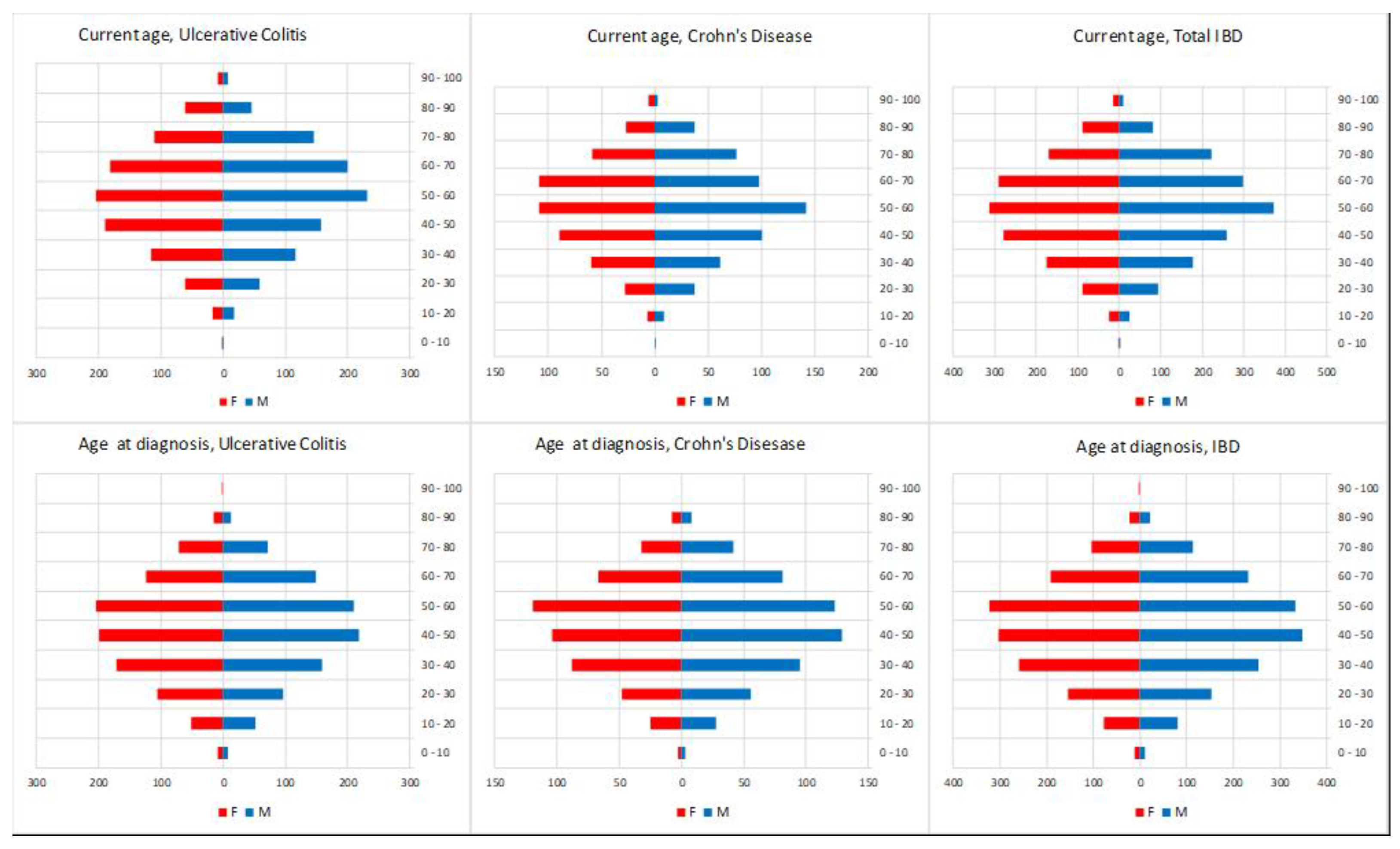
Figure 3.
Unadjusted IBD-related hospitalisations, 2018-2024.
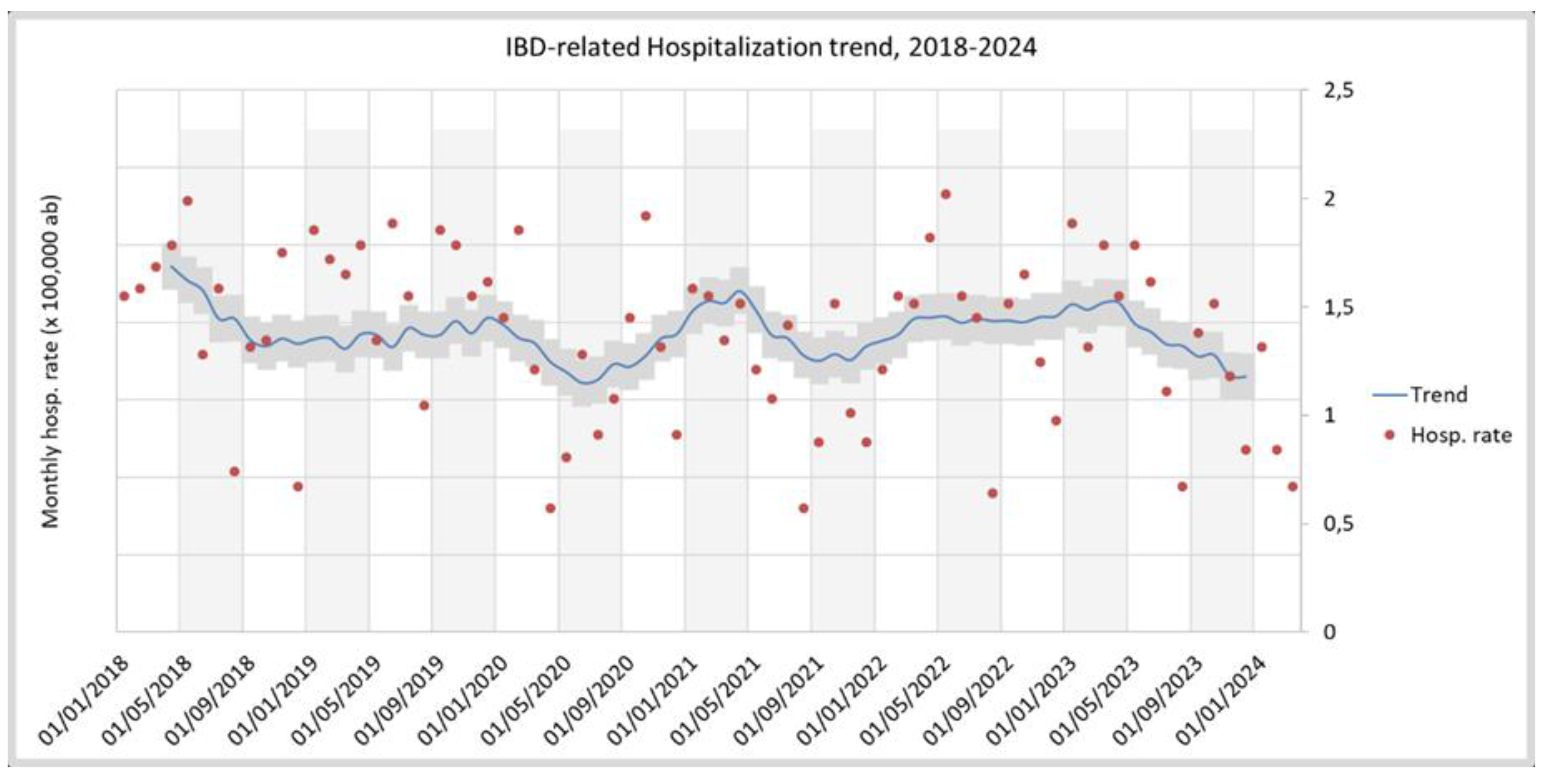
Figure 4.
Kaplan-Meier failure functions for Ulcerative Colitis (UC) and Crohn’s Disease (CD) patients, raw data (left) and adjusted for age at diagnosis and gender (right). Outcome of interest is the first occurrence of surgery.
Figure 4.
Kaplan-Meier failure functions for Ulcerative Colitis (UC) and Crohn’s Disease (CD) patients, raw data (left) and adjusted for age at diagnosis and gender (right). Outcome of interest is the first occurrence of surgery.
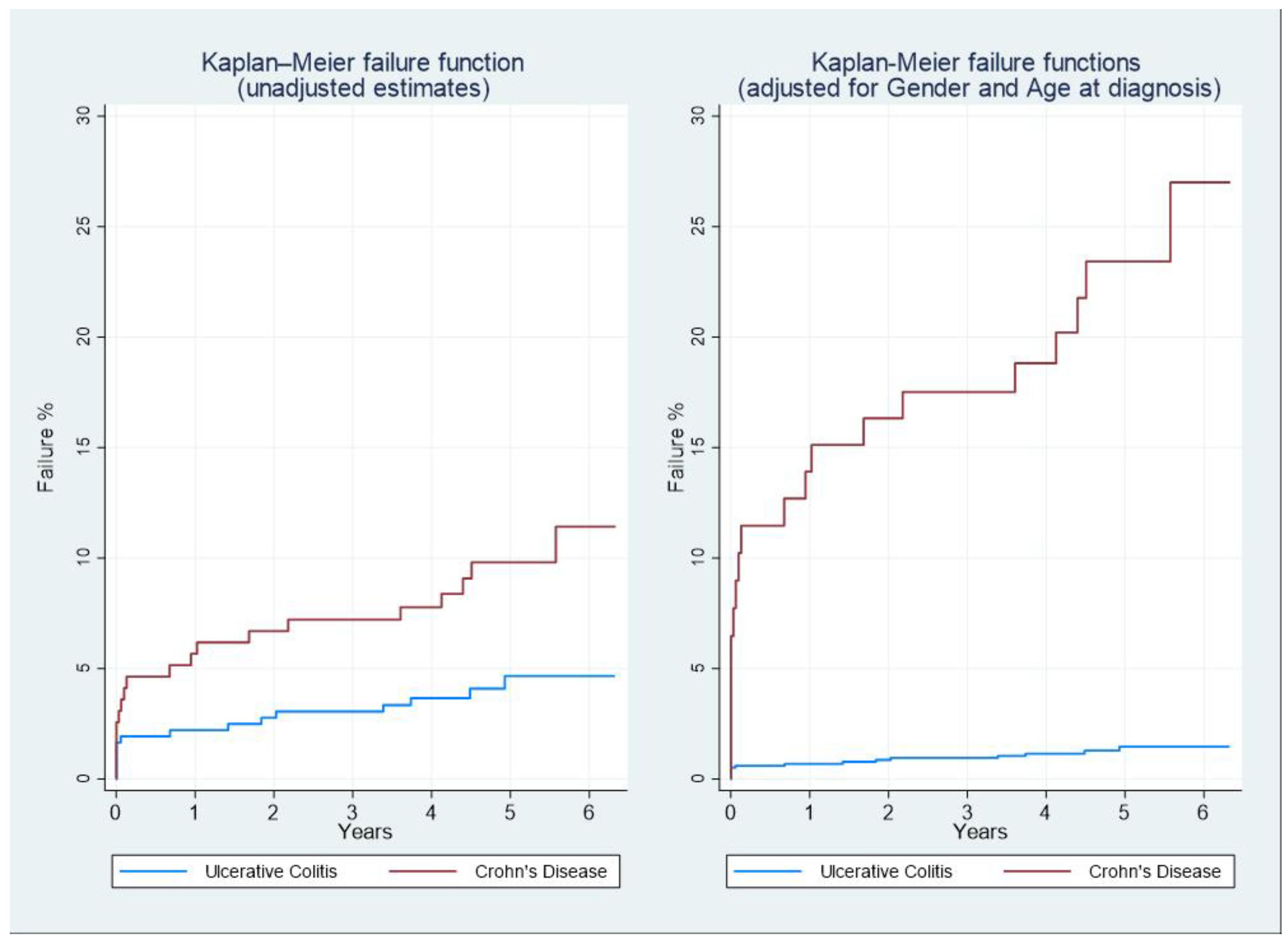
Table 1.
Raw incidence of IBD by age range, and standardised incidence x 100,000 ab (ref. population: 2024 LHA Roma 1 residents); 2011-2021. UC: Ulcerative colitis. CD: Crohn’s Disease.
Table 1.
Raw incidence of IBD by age range, and standardised incidence x 100,000 ab (ref. population: 2024 LHA Roma 1 residents); 2011-2021. UC: Ulcerative colitis. CD: Crohn’s Disease.
| IBD CASES | AGE AT DIAGNOSIS | AGE-STANDARDISED INCIDENCE X 100,000PPL | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| YEAR | 0 -10 | 10 - 20 | 20 - 30 | 30 - 40 | 40 - 50 | 50 - 60 | 60 - 70 | 70 - 80 | 80 - 90 | 90 - 100 | TOTAL | UC | CD | IBD |
| 2011 | 5 | 11 | 17 | 38 | 45 | 35 | 19 | 10 | 4 | 0 | 184 | 8.83 | 5.83 | 14,67 |
| 2012 | 2 | 11 | 15 | 41 | 39 | 33 | 24 | 8 | 2 | 0 | 175 | 9.22 | 4.81 | 14,03 |
| 2013 | 1 | 9 | 18 | 65 | 74 | 67 | 55 | 19 | 5 | 0 | 313 | 16.13 | 9.45 | 25,58 |
| 2014 | 0 | 12 | 15 | 36 | 58 | 53 | 29 | 10 | 1 | 0 | 214 | 11.30 | 5.81 | 17,11 |
| 2015 | 2 | 8 | 29 | 38 | 72 | 74 | 43 | 26 | 8 | 0 | 300 | 16.05 | 8.18 | 24,23 |
| 2016 | 0 | 14 | 28 | 37 | 48 | 71 | 54 | 21 | 7 | 0 | 280 | 14.63 | 8.19 | 22,82 |
| 2017 | 1 | 11 | 20 | 35 | 30 | 43 | 34 | 15 | 3 | 0 | 192 | 9.60 | 6.07 | 15,68 |
| 2018 | 2 | 16 | 30 | 50 | 66 | 71 | 34 | 27 | 3 | 0 | 299 | 15.59 | 9.21 | 24,79 |
| 2019 | 1 | 19 | 42 | 32 | 67 | 63 | 53 | 34 | 4 | 0 | 315 | 16.95 | 8.36 | 25,31 |
| 2020 | 2 | 16 | 35 | 51 | 46 | 52 | 25 | 15 | 4 | 0 | 246 | 13.99 | 6.16 | 20,15 |
| 2021 | 4 | 22 | 44 | 69 | 74 | 70 | 34 | 20 | 3 | 1 | 341 | 18.55 | 9.98 | 28,54 |
| TOTAL | 20 | 149 | 293 | 492 | 619 | 632 | 404 | 205 | 44 | 1 | 2859 | - | - | - |
Table 2.
Demographic composition of prospective cohort. UC: Ulcerative colitis; CD: Crohn’s Disease; IQR: Interquartile range; SD: Standard Deviation.
Table 2.
Demographic composition of prospective cohort. UC: Ulcerative colitis; CD: Crohn’s Disease; IQR: Interquartile range; SD: Standard Deviation.
| CD: N=194 | UC: N=362 | |
|---|---|---|
| Age at diagnosis (mean; SD) | 47.0; 15.9 | 48.5; 15.8 |
| Male (N;%) | 109; 56.2% | 190; 52.5% |
| Total interventions(N;%) | 21; 10.8% | 36; 9.9% |
| Median follow-up duration (months; IQR) | 59.7 (50.9 – 69.0) | 58.1 (49.2 – 65.5) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



