
Submitted:
31 March 2025
Posted:
31 March 2025
You are already at the latest version
Abstract
We used the Queensland acute rheumatic fever (ARF) and rheumatic heart disease (RHD) register to describe the clinical phenotype and the characteristics of consecutive individuals diagnosed with ARF in Far North Queensland, tropical Australia between January 2012 and December 2023. There were 830 episodes of ARF in 740 individuals during the study period; 785/830 (95%) episodes occurred in First Nations Australians and 696/824 (84%) occurred in areas of socioeconomic disadvantage. There was no significant change in overall incidence of ARF during the study period (rs=0.51, p=0.09). The median (interquartile range) age of the cohort was 15 (10-23) years, although 276/830 (33%) episodes occurred in individuals ≥20 years. Individuals with carditis, polyarthritis, an abnormal electrocardiogram, fever and elevated inflammatory markers were more likely to have confirmed ARF. The presence of polyarthralgia, monoarthritis and the skin manifestations of ARF was not associated with a diagnosis of confirmed ARF. Individuals with monoarthralgia were less likely to have confirmed ARF. At the end of the study period 266/706 (38%) of individuals who had access to echocardiography had confirmed RHD. Individuals who did not have documented echocardiography as a component of their episode of care were more likely have severe RHD at the end of the study (25/339 (7%) versus 7/401 (2%), p< 0.0001). ARF and RHD continue to be diagnosed in First Nations Australians in tropical Australia. It seems unlikely that the country will achieve its stated aim of eliminating RHD by 2031.
Keywords:
Acute rheumatic fever
; Rheumatic heart disease
; Group A Streptococcus
; Clinical management
; Skin health.
; Tropical medicine
; Tropical Australia: Aboriginal and Torres Strait Islander people
; Social determinants of health
Introduction
Acute Rheumatic Fever (ARF) is an immune mediated inflammatory condition that can follow Group A Streptococcus pyogenes (GAS) infection [1]. ARF can involve the skin, subcutaneous tissue, joints, brain, and the heart [2]. Severe or recurrent episodes of ARF-induced carditis can result in permanent cardiac damage, a condition termed rheumatic heart disease (RHD). RHD is common and can be life-threatening; it was estimated that globally in 2019 there were 40.5 million people living with RHD and that it caused almost 310,000 deaths [3]. Improvements in the standard of living and earlier treatment of GAS infections mean that ARF and RHD are now rarely diagnosed in resource-rich settings [4].
However, Australia is a notable exception to this observation [5]. The burden of ARF and RHD is borne almost entirely by its Aboriginal and Torres Strait Islander peoples (hereafter respectfully referred to as First Nations peoples). While the overall incidence of ARF in Australia is 69 per 100,000, the incidence in First Nations peoples is up to 121 times that of other Australians [6]. Even in Australia’s well-resourced, universal health system the incidence of ARF in Australia’s First Nations peoples continues to rise, increasing the likelihood of further increases in the prevalence of RHD which in some communities may exceed 5% [7,8].
The RHD Endgame Strategy aims to eliminate RHD in Australia by 2031 by ensuring the optimal delivery of primary, secondary and tertiary prevention strategies [5]. The prompt, accurate diagnosis of ARF, and the subsequent administration of secondary antibiotic prophylaxis to prevent GAS infection and RHD progression is a key element of this strategy [5,9]. However, up to 78% of Australians diagnosed with RHD have no prior diagnosis of ARF suggesting that many episodes of ARF are currently missed [10]. This is likely to be explained, at least in part, by a failure to recognise ARF presentations when they occur.
But the diagnosis of ARF – which can include a variety of dermatological, rheumatological, neurological and cardiac manifestations – can be challenging [11]. While the revised Jones criteria recognise the diverse clinical presentations of ARF, they have imperfect sensitivity and specificity and their clinical utility is influenced strongly by the pre-test probability of ARF in the examined populations [12,13,14,15]. It is therefore essential for clinicians to understand the characteristic presentations of ARF in their local clinical setting to enable the prompt delivery of the suite of interventions that reduce the risk of a future RHD diagnosis [15].
The region of Far North Queensland (FNQ) in tropical northeast Australia has a significant – and increasing – incidence of RHD, and nearly all of its cases are seen in its First Nations peoples [16]. ARF and RHD are both notifiable conditions in Queensland, but almost half of the individuals diagnosed with RHD in the FNQ region have no recorded history of ARF, suggesting that local clinicians may be missing opportunities to recognise and diagnose the condition [16]. This study examined routinely collected epidemiological and clinical data from the Queensland ARF and RHD register to characterise ARF presentations in the FNQ population. It was hoped that these data would facilitate the prompt local diagnosis of ARF and more timely delivery of the multi-faceted care that is required to reduce the local incidence of RHD and its complications [15,16,17].
Methods
Setting
FNQ is a region of 380,000 km2 with a population of approximately 290,000 people, 17% of whom identify as First Nations Australians [18] (Figure 1). The region is served by two public health services: the Cairns and Hinterland Hospital and Health Service (CHHHS) which serves approximately 265,000 people (of whom 12% identify as First Nations Australian Australians) living in the region surrounding the administrative hub of Cairns, and the Torres and Cape Hospital and Health Service (TCHHS) which serves a rural and remote population of approximately 25,000 people (of whom 69% identify as First Nations Australians) living on the Cape York Peninsula or the Torres Strait Islands.
Image taken from Bird, K., Bohanna, I., McDonald, M., Wapau, H., Blanco, L., Cullen, J., McLucas, J., Forbes, S., Vievers, A., Strivens, E. and Barker, R. (2023). A good life for people living with disability: the story from Far North Queensland. Disability and Rehabilitation, 46(9), 1787–1795. https://doi.org/10.1080/09638288.2023.2205172
Data Collection
ARF and RHD have been notifiable conditions in Queensland since 1999 and 2018, respectively, with the demographic and clinical data of notified cases routinely recorded on the Queensland ARF and RHD register. In this study, the register was interrogated to define FNQ residents with a diagnosis of confirmed, probable or possible ARF diagnosis between 1 January 2012 and 31 December 2023. Episodes of ARF > 6 months apart in the same individual were included as separate presentations.
The demographic characteristics of the individual presenting with each episode of ARF were recorded. Socioeconomic disadvantage was defined using the Socio-Economic Indexes for Area (SEIFA) Index of Relative Socio-Economic Advantage and Disadvantage (ISRAD) score, the Australia Bureau of Statistics’ measure of socioeconomic disadvantage [19]. The revised Jones’ criteria that were satisfied in each case of ARF were recorded and used to define whether the case was confirmed, probable or possible (Table 1). If a criterion was not recorded, it was presumed to be absent. High- and low-risk populations were defined using the 2020 Australian guidelines for prevention, diagnosis and management of acute rheumatic fever [15]. The register was also interrogated to determine the presence and severity of severity of RHD in each individual at the end of the study period. The presence and severity of RHD was defined using the 2023 World Heart Federation guidelines [20].
Statistical Analysis
De-identified data were extracted and analysed using statistical software (Stata version 18). Groups were compared using logistic regression and trends over time were determined using Spearman’s test for correlation. If individuals were missing data, they were not included in analyses which evaluated those variables. Australian Bureau of Statistics data were used to calculate disease incidence [18].
Ethical Approval
The Far North Queensland Human Research Ethics Committee provided ethical approval for the study (EX/2022/QCH/92523). As the retrospective data were de-identified and presented in an aggregated manner, the committee waived the requirement for informed consent.
Results
There were 830 notifications of confirmed, probable and possible ARF to the register during the study period; 492 (56%) were confirmed, 180 (20%) were probable and 158 (18%) were possible. The 830 episodes of ARF occurred in 740 individuals. There was enough information in the register to determine whether an episode of ARF was an initial or a recurrent episode in 777/830 (94%) presentations; 191/777 (25%) were recurrent episodes.
The overall annual incidence of ARF in the FNQ population in 2023 (the end of the study period) was 29.1/100,000 population. The incidence of confirmed ARF in FNQ was 9.7/100,000 population. There was no significant change in overall incidence of ARF during the 2012-2023 study period (rs=0.51, p=0.09), but the proportion of episodes that satisfied criteria for confirmed ARF declined (rs= -0.31, p<0.0001) (Figure 2).
At the end of the study period, the annual overall incidence of ARF in the FNQ First Nations Australian population was 157.9/100,000 population and the annual overall incidence in the TCHHS population was 200.6/100,000 population. Meanwhile, the annual incidence of confirmed ARF in the FNQ First Nations Australian population was 59.2/100,000 population and the annual incidence of confirmed ARF in the TCHHS population was 83.6/100,000 population.
Of the 830 episodes, 459 (55%) occurred in the TCHHS and 371 (45%) in the CHHHS (Table 2, Figure 3). The median (interquartile range, range) age of the patient at the time of their ARF episode was 15 (10-23, 3-55) years, however, a diagnosis of confirmed ARF was more common in individuals aged 5-14 (odds ratio (OR), (95% confidence interval (95% CI)): 2.64 (1.98-3.53), p<0.001 (Figure 4).
Of the 830 episodes of ARF, 785 (95%) occurred in First Nations individuals; First Nations Australians were more likely to present with recurrent ARF than non-First Nations Australians (188/734 (26%) versus 3/43 (7%), OR (95% CI): 4.59 (1.40-15.01), p=0.01). Of the 830 presentations, 512 (62%) occurred in individuals residing in regions with a SEIFA score in the lowest decile (Figure 5). Individuals residing in regions with a SEIFA score in the lowest decile were no more likely to present with recurrent ARF than individuals living in other locations (116/478 (24%) versus 75/299 (25%), OR (95% CI): 0.96 (0.68-1.34), p=0.80). The clinical and laboratory characteristics of the cases are presented in Table 3.
Only 441/830 (53%) episodes of ARF had an echocardiography associated with the presentation documented in the register and in 374/441 (85%) there was no evidence of RHD. However, by the end of the study period, 370/740 (50%) individuals with an episode of ARF during the study period had confirmed RHD, including 32/740 (4%) with severe RHD (Figure 6). Individuals who had no echocardiography associated with the presentation documented in the register were more likely to have severe RHD at the end of the study period (25/339 (7%) versus 7/401 (2%), (OR (95% CI): 4.48 (1.91-10.50), p<0.0001). Individuals who had presented with recurrent ARF were more likely to have RHD (OR (95% CI): 2.45 (1.61-3.72), p<0.0001) and more likely to have severe RHD at the end of the study period than those who did not have recurrent ARF (OR (95% CI): 5.55 (2.53-12.18), p<0.0001). At the end of the study period, the median (IQR) age of the 32 individuals with severe RHD was 27 (17-36) years; 21/32 (66%) were female.
Discussion
This study examined the characteristics of individuals presenting with ARF in the FNQ region of tropical Australia. While recognising the challenges of delivering comprehensive healthcare across a region that is larger than the United Kingdom, it emphasises the importance of promptly seeking evidence of carditis with electrocardiogram (ECG) and echocardiography in patients presenting with other symptoms of ARF. The study found that in over 80% of ARF episodes individuals had joint symptoms that represented a major Jones criterion but polyarthritis – and not monoarthritis or polyarthralgia – was associated with a confirmed diagnosis of ARF. Fever, a greater elevation in inflammatory markers and higher titres of antibodies against GAS also increased – while monoarthralgia decreased – the likelihood of confirmed ARF.
The study again confirms the disproportionate burden of ARF in First Nations people, particularly those living in remote communities. Despite an understanding of the strategies that are necessary to address ARF and RHD and reduce their burden and increasing financial investment, the overall incidence of ARF is not yet falling in the region [5,21]. These findings will necessarily result in new cases of RHD and its associated morbidity and premature mortality [3,5]. Over a third of the cohort had established RHD at the end of the study period and over 4% had severe disease. We need to do better if we are to reach our collective goal of eliminating RHD in Australia by 2031.
The international literature suggests that carditis is present in 50-70% of individuals during their first episode of ARF [12,22]. Although carditis was diagnosed in less than 13% of the cohort it was the manifestation that was most associated with a diagnosis of confirmed ARF. The lower proportion of individuals with a diagnosis of carditis in our cohort may be at least partly explained by the challenges with providing timely echocardiography assessment across the region’s 380,000 km2 expanse. Just over half of the ARF episodes had an echocardiography assessment documented, but patients without echocardiography documented were more likely to have severe RHD at the end of the study period. Earlier recognition of cardiac involvement in these individuals may have resulted in intensified efforts to deliver secondary prophylaxis and reduce disease progression [9,23,24].
Our study highlights the importance of considering ARF as a diagnosis in individuals presenting with joint symptoms, particularly in those at higher risk of the disease [12,15]. The proportion of individuals in the cohort with joint symptoms is similar to other Australian and international series [12,25,26,27], although it was notable that individuals with polyarthritis were more likely to have a confirmed ARF diagnosis, which was not the case in individuals with polyarthralgia or monoarthritis. Individuals with monoarthralgia were less likely to have a confirmed ARF diagnosis, but this is likely to be at least partly explained by increased awareness of ARF among local clinicians that evolved over the study period and a lower threshold for notification [16,23].
Erythema marginatum and subcutaneous nodules were documented in less than 4% of the cases, which is, again, similar to the rates seen in the international literature, although it may also represent a lack of familiarity with these manifestations of ARF and challenges in their recognition in a population with more pigmented skin and a higher burden of other skin conditions [12,28,29]. Although erythema marginatum and subcutaneous nodules have been described as highly specific manifestations of ARF, there was no association in this cohort between the presence of these manifestations and a confirmed diagnosis of ARF. Sydenham’s chorea is documented in approximately 10-30% episodes of ARF in the international literature and in 19% and 31% of cases of ARF in other Australian jurisdictions [12,22,27], Sydenham’s chorea was seen in only 6% of this cohort (although 11% of those with confirmed disease) The lower rate of chorea in our cohort compared with other Australian cohorts may represent local clinicians’ lack of familiarity with this unique manifestation of ARF, over-reporting of conditions that were not ARF (generating a greater denominator) or genetic differences in the population of the FNQ region (over 40% of our cohort had Torres Strait Islander heritage).
Most series focus on the prevalence of the different major manifestations of ARF, which is understandable, however, the minor criteria in our cohort were also helpful in establishing a diagnosis of confirmed ARF. Fever, inflammatory markers and a prolonger PR interval were all more common in patients with confirmed ARF, while monoarthralgia was less common. It was also notable that individuals with confirmed ARF were also more likely to have a higher titre of ASOT and anti-DNase B antibodies.
Our study also provides data to support the adds to the growing body of evidence from Australia and New Zealand that suggest a role for GAS infection of the skin in the pathogenesis of ARF [30,31]. Over 5% of individuals had isolation of GAS from a skin lesion before, or at, the time that they presented with ARF symptoms. Meanwhile, a proportion of the 20% with a stated history of skin sores or sore throat would have only had skin sores. A temporal association between the isolation of GAS from a skin lesion and a diagnosis of ARF does not necessarily imply a pathophysiological role of skin infection, however, given the many other benefits of improved skin health there are few downsides to including efforts to address skin health in public health strategies to reduce ARF incidence [15,32].
The greatest number of ARF episodes occurred, as expected, in children aged 5-14 years, although it was notable that greater than 30% of the cases occurred in individuals aged 20 years or older. It is important to consider ARF in older individuals in the appropriate clinical context to ensure that they receive prompt investigation and treatment [33,34]. However, it is also important to note that a confirmed diagnosis of ARF was less common in individuals outside the 5-14 age group and it remains important to actively exclude differential diagnoses – including connective tissue disorders and infection – in older adults with suspected ARF [35,36].
The overall incidence of ARF did not decline during the study period which aligns with other recent Australian data which highlight a stable, or increasing, incidence of ARF/RHD despite the implementation of a national strategy to address and eliminate these preventable diseases [7,21]. It is likely that this finding is explained, at least partly, by improved case detection and notification, a suggestion that is supported by the significant decline in confirmed episodes of ARF in this cohort during the study period [16,23]. However, ARF is almost entirely preventable and any diagnosis in 21st century Australia is concerning. In recent years Australian programmes have focussed on primary, secondary and tertiary prevention strategies to reduce the incidence of ARF and RHD [37]. These programmes have resulted in improved adherence to secondary prophylaxis which has made some impact on reducing progression to severe RHD across Australia [23]. Improved adherence to secondary prophylaxis would also be anticipated to translate into a decrease in ARF recurrences [38]. However, there is a growing recognition that without similar efforts to address the social determinants of health that drive the incidence of ARF, there is likely to be limited progress [23,39,40].
ARF is the archetypal disease of disadvantage, and our study provides further data, as if this were needed, to highlight its contribution of disadvantage to the incidence of ARF and RHD in 21st century Australia. FNQ has three of the most disadvantaged Local Government Areas in Australia and this disadvantage, borne disproportionately by First Nations Australians living in the region, has an important impact on the local incidence of infectious diseases [16,41,42]. Over 60% of the cohort lived in a region in the lowest decile of the SEIFA Index of Relative Socio-Economic Advantage and Disadvantage score while almost 95% of the cohort identified as a First Nations Australian (despite First Nations Australians comprising only 17% of the local population). Over 55% of the episodes occurred in the TCHHS which serves the remote Cape York Peninsula and Torres Straits islands, although again less than 10% of the FNQ population lives in the region. These data again highlight the primacy of the social determinants of health in the incidence of ARF, RHD and its clinical course [15,16,39,43].
This study had several important limitations. Although the primary source for the data was the Queensland ARF and RHD register, the imperfect specificity of the revised Jones criteria means that this cohort almost certainly contains individuals who did not have ARF. Furthermore, although ARF has been a notifiable disease in Queensland since 1998, many cases are not recognised or are not reported to the register as evidenced by the fact that approximately 50% of the individuals diagnosed with RHD in FNQ have no recorded history of ARF [16,44]. And while the register is maintained diligently, its data’s reliability depends on the thoroughness of the clinical assessment and often, even more importantly, its documentation. The retrospective nature of this study precluded comprehensive data collection, and we were unable to determine how actively clinical findings had been sought. It was not always clear, for any given criterion, whether there was no abnormality detected, or no data were available. The clinical assessment will necessarily depend on the experience of the attending health worker and their familiarity with ARF. Certainly, anecdotally, a detailed skin assessment is not performed in all FNQ patients presenting with ARF symptoms and ECGs may not be performed at the time of presentation or sequentially. Knowing that manifestations of ARF were absent despite being specifically sought by an experienced clinician would have helped characterised the clinical phenotype of ARF in the region more reliably. Our study did not examine the impact of treatment of symptoms on the clinical phenotype. Although monoarthritis was not associated with a diagnosis of confirmed ARF in this cohort, patients treated with non-steroidal anti-inflammatory drugs early in the course of ARF, particularly before the other signs and symptoms of ARF become distinct, may not develop polyarthritis [14]. Similarly, in patients presenting with recurrent ARF we did not examine factors associated with their adherence to secondary prophylaxis which would, of course, be expected to reduce the risk of recurrent ARF. We did not stratify the presentation of our findings by initial and recurrent presentation or whether the individual came from a high- or low-risk population, although over 98% of individuals in the cohort would be considered at high risk of the disease [15].
Acknowledging these limitations, the study provides contemporary insights into the characteristics of individuals with ARF in this region of tropical Australia and their clinical findings at presentation. Future prospective studies might examine individual and systemic factors that delay individuals’ presentation, which could, in turn, inform strategies to expedite presentation for diagnosis and management. They might also ensure that all major and minor criteria are assessed in a standardised manner which may facilitate ARF diagnosis. Evaluation of local individual and systemic factors that affect adherence to secondary prophylaxis would also help develop strategies to reduce the risk of recurrent ARF which represented almost 25% of the presentations in this series.
Conclusions
This study provides contemporary data on the clinical presentations of individuals with ARF in the FNQ region of Australia. It emphasises the importance of prompt ECG and echocardiography assessment and provides insights into the common patterns of joint involvement. It also highlights that while children aged 5-14 are the population that are most likely to have confirmed disease, ARF is not uncommon in older populations. It is hoped that these data will expedite recognition and treatment of ARF in the region, reducing the risk of progression to RHD. However, the study also demonstrates that despite greater awareness and increased financial investment the overall incidence of ARF is not declining, a dispiriting finding in 21st century Australia. The most important risk factor for ARF is the socioeconomic disadvantage that many First Nations Australians in the region continue to experience. It is therefore essential that policy makers developing public health strategies to reduce the local burden of RHD work with local communities to also address the social determinants of health that are the underlying cause of ARF – and many other communicable and non-communicable disease – in the region. Until we address the underlying inequity that drives the incidence of ARF and RHD in Australia, progress will be limited.
Funding
The authors declare that this study received no specific financial support.
Acknowledgments
The authors would like to thank the many health care workers who were involved in the care of the patients. They would also like to thank the staff who work at the Queensland ARF and RHD register who helped with data collation and advice during the manuscript’s preparation.
Conflicts of Interest
The authors have no conflict of interest to declare.
References
- Auala T, Zavale BLG, Mbakwem AÇ, Mocumbi AO. Acute Rheumatic Fever and Rheumatic Heart Disease: Highlighting the Role of Group A Streptococcus in the Global Burden of Cardiovascular Disease. Pathogens (Basel). 2022;11(5):496.
- Karthikeyan G, Guilherme L. Acute rheumatic fever. The Lancet (British edition). 2018;392(10142):161-74.
- Ruan R, Liu X, Zhang Y, Tang M, He B, Zhang QW, et al. Global, Regional, and National Advances Toward the Management of Rheumatic Heart Disease Based on the Global Burden of Disease Study 2019. J Am Heart Assoc. 2023;12(13):e028921.
- Steer, AC. Historical aspects of rheumatic fever. Journal of paediatrics and child health. 2015;51(1):21-7.
- Wyber R, Noonan K, Halkon C, Enkel S, Cannon J, Haynes E, et al. Ending rheumatic heart disease in Australia: the evidence for a new approach. Medical journal of Australia. 2020;213(S10):S3-S31.
- Parnaby MG, Carapetis JR. Rheumatic fever in indigenous Australian children. J Paediatr Child Health. 2010;46(9):527-33.
- Aboriginal and Torres Strait islander Health Performance Framework. Tier 1 - Health status and outcomes. 1.06 Acute rheumatic fever and rheumatic heart disease. Canberra: The Australian Institute of Health and Welfare.; 2025 [Available from: https://www.indigenoushpf.gov.au/measures/1-06-rheumatic-fever-rheumatic-heart-disease.
- Francis JR, Fairhurst H, Hardefeldt H, Brown S, Ryan C, Brown K, et al. Hyperendemic rheumatic heart disease in a remote Australian town identified by echocardiographic screening. Med J Aust. 2020;213(3):118-23.
- Beaton A, Okello E, Rwebembera J, Grobler A, Engelman D, Alepere J, et al. Secondary Antibiotic Prophylaxis for Latent Rheumatic Heart Disease. N Engl J Med. 2022;386(3):230-40.
- Acute rheumatic fever and rheumatic heart disease in Australia, 2022. Canberra: AIHW; 2024.
- Bray JJ, Thompson S, Seitler S, Ali SA, Yiu J, Salehi M, et al. Long-term antibiotic prophylaxis for prevention of rheumatic fever recurrence and progression to rheumatic heart disease. Cochrane database of systematic reviews. 2024;9:CD015779.
- Gewitz MH, Baltimore RS, Tani LY, Sable CA, Shulman ST, Carapetis J, et al. Revision of the Jones Criteria for the diagnosis of acute rheumatic fever in the era of Doppler echocardiography: a scientific statement from the American Heart Association. Circulation (New York, NY). 2015;131(20):1806-18.
- Pulle J, Ndagire E, Atala J, Fall N, Okello E, Oyella LM, et al. Specificity of the Modified Jones Criteria. Pediatrics. 2024;153(3).
- Carapetis JR, Currie BJ. Rheumatic fever in a high incidence population: the importance of monoarthritis and low grade fever. Arch Dis Child. 2001;85(3):223-7.
- Ralph AP, Noonan S, Wade V, Currie BJ. The 2020 Australian guideline for prevention, diagnosis and management of acute rheumatic fever and rheumatic heart disease. Med J Aust. 2021;214(5):220-7.
- Kang K, Chau KWT, Howell E, Anderson M, Smith S, Davis TJ, et al. The temporospatial epidemiology of rheumatic heart disease in Far North Queensland, tropical Australia 1997-2017; impact of socioeconomic status on disease burden, severity and access to care. PLoS Negl Trop Dis. 2021;15(1):e0008990.
- Hempenstall A, Howell E, Kang K, Chau KWT, Browne A, Kris E, et al. Echocardiographic Screening Detects a Significant Burden of Rheumatic Heart Disease in Australian Torres Strait Islander Children and Missed Opportunities for its Prevention. Am J Trop Med Hyg. 2021;104(4):1211-4.
- Australian census Canberra: Australian Bureau of Statistics; 2021 [Available from: https://www.abs.gov.au/census.
- Socio-Economic Indexes for Areas (SEIFA), Australia. Canberra: Australian Bureau of Statistics; 2021.
- Rwebembera J, Marangou J, Mwita JC, Mocumbi AO, Mota C, Okello E, et al. 2023 World Heart Federation guidelines for the echocardiographic diagnosis of rheumatic heart disease. Nat Rev Cardiol. 2024;21(4):250-63.
- Casey D, Turner P. Australia's rheumatic fever strategy three years on. Med J Aust. 2024;220(4):170-1.
- Kumar M, Little J, Pearce S, MacDonald B, Greenland M, Tarca A, et al. Clinical profile of paediatric acute rheumatic fever and rheumatic heart disease in Western Australia: 1987 to 2020. Journal of paediatrics and child health. 2024;60(8):375-83.
- Stacey I, Ralph A, de Dassel J, Nedkoff L, Wade V, Francia C, et al. The evidence that rheumatic heart disease control programs in Australia are making an impact. Australian and New Zealand journal of public health. 2023;47(4):100071-.
- Quinn E, Girgis S, Van Buskirk J, Matthews V, Ward JE. Clinic factors associated with better delivery of secondary prophylaxis in acute rheumatic fever management. Aust J Gen Pract. 2019;48(12):859-65.
- Lindholm DE, Whiteman IJ, Oliver J, Cheung MMH, Hope SA, Brizard CP, et al. Acute rheumatic fever and rheumatic heart disease in children and adolescents in Victoria, Australia. Journal of paediatrics and child health. 2023;59(2):352-9.
- Jack S, Moreland NJ, Meagher J, Fittock M, Galloway Y, Ralph AP. Streptococcal Serology in Acute Rheumatic Fever Patients: Findings From 2 High-income, High-burden Settings. The Pediatric infectious disease journal. 2019;38(1):e1-e6.
- Lawrence JG, Carapetis JR, Griffiths K, Edwards K, Condon JR. Acute Rheumatic Fever and Rheumatic Heart Disease: Incidence and Progression in the Northern Territory of Australia, 1997 to 2010. Circulation (New York, NY). 2013;128(5):492-501.
- Davidson L, Knight J, Bowen AC. Skin infections in Australian Aboriginal children: a narrative review. Med J Aust. 2020;212(5):231-7.
- Ricciardo BM, Kessaris HL, Cherian S, Kumarasinghe SP, Amgarth-Duff I, Sron D, et al. Healthy skin for children and young people with skin of colour starts with clinician knowledge and recognition: a narrative review. Lancet Child Adolesc Health. 2025;9(4):262-73.
- Baker MG, Gurney J, Moreland NJ, Bennett J, Oliver J, Williamson DA, et al. Risk factors for acute rheumatic fever: A case-control study. The Lancet regional health Western Pacific. 2022;26:100508-.
- Oliver J, Bennett J, Thomas S, Zhang J, Pierse N, Moreland NJ, et al. Preceding group A streptococcus skin and throat infections are individually associated with acute rheumatic fever: evidence from New Zealand. BMJ global health. 2021;6(12):e007038.
- Thomas HMM, Enkel SL, Mullane M, McRae T, Barnett TC, Carapetis JR, et al. Trimodal skin health programme for childhood impetigo control in remote Western Australia (SToP): a cluster randomised, stepped-wedge trial. Lancet Child Adolesc Health. 2024;8(11):809-20.
- Woods JA, Sodhi-Berry N, MacDonald BR, Ralph AP, Francia C, Stacey I, et al. A multijurisdictional cohort study. Australian health review. 2024.
- Ben-Dov I, Berry E. Acute rheumatic fever in adults over the age of 45 years: an analysis of 23 patients together with a review of the literature. Semin Arthritis Rheum. 1980;10(2):100-10.
- Chan K, Cullen T, Ralph A, Ilton M, Marangou J. Acute Rheumatic Fever Diagnosis in Older Adults. Heart, Lung and Circulation. 2019;28:S50.
- Basaglia A, Kang K, Wilcox R, Lau A, McKenna K, Smith S, et al. The aetiology and incidence of infective endocarditis in people living with rheumatic heart disease in tropical Australia. Eur J Clin Microbiol Infect Dis. 2023;42(9):1115-23.
- Ralph AP, Noonan S, Wade V, Currie BJ. The 2020 Australian guideline for prevention, diagnosis and management of acute rheumatic fever and rheumatic heart disease. Medical Journal of Australia. 2021;214(5):220-7.
- de Dassel JL, de Klerk N, Carapetis JR, Ralph AP. How Many Doses Make a Difference? An Analysis of Secondary Prevention of Rheumatic Fever and Rheumatic Heart Disease. J Am Heart Assoc. 2018;7(24):e010223.
- Coffey PM, Ralph AP, Krause VL. The role of social determinants of health in the risk and prevention of group A streptococcal infection, acute rheumatic fever and rheumatic heart disease: A systematic review. PLOS Neglected Tropical Diseases. 2018;12(6):e0006577.
- Doran J, Canty D, Dempsey K, Cass A, Kangaharan N, Remenyi B, et al. Surgery for rheumatic heart disease in the Northern Territory, Australia, 1997-2016: what have we gained? BMJ Glob Health. 2023;8(3).
- Socio-Economic Indexes for Areas (SEIFA), Australia Canberra: Australian Bureau of Statistics; 2021 [Available from: https://www.abs.gov.au/statistics/people/people-and-communities/socio-economic-indexes-areas-seifa-australia/latest-release.
- Hanson J, Smith S, Stewart J, Horne P, Ramsamy N. Melioidosis - a disease of socioeconomic disadvantage. PLoS Negl Trop Dis. 2021;15(6):e0009544.
- Rheumatic fever and rheumatic heart disease: Report by the Director-General. Geneva, Switzerland World Health Organisation (WHO) Executive Board; 2018.
- Agenson T, Katzenellenbogen JM, Seth R, Dempsey K, Anderson M, Wade V, et al. Case Ascertainment on Australian Registers for Acute Rheumatic Fever and Rheumatic Heart Disease. International journal of environmental research and public health 2020, 17, 5505. [CrossRef] [PubMed]
Figure 1.
Map of Far North Queensland, Australia, showing catchment area for current study.
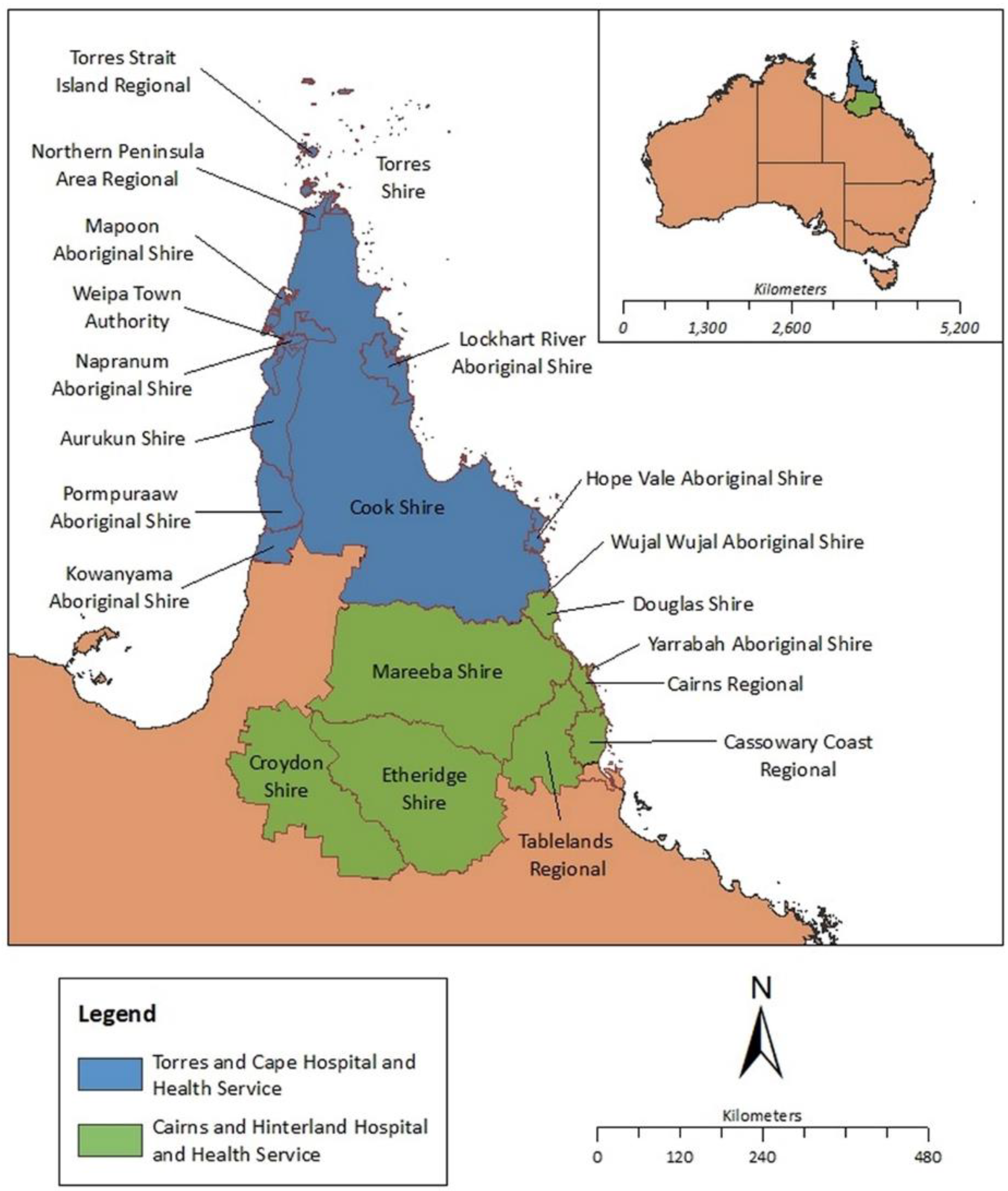
Figure 2.
ARF cases in Far North Queensland diagnosed between January 2012 to December 2023. The number of cases and the incidence in the general population are presented.
Figure 2.
ARF cases in Far North Queensland diagnosed between January 2012 to December 2023. The number of cases and the incidence in the general population are presented.
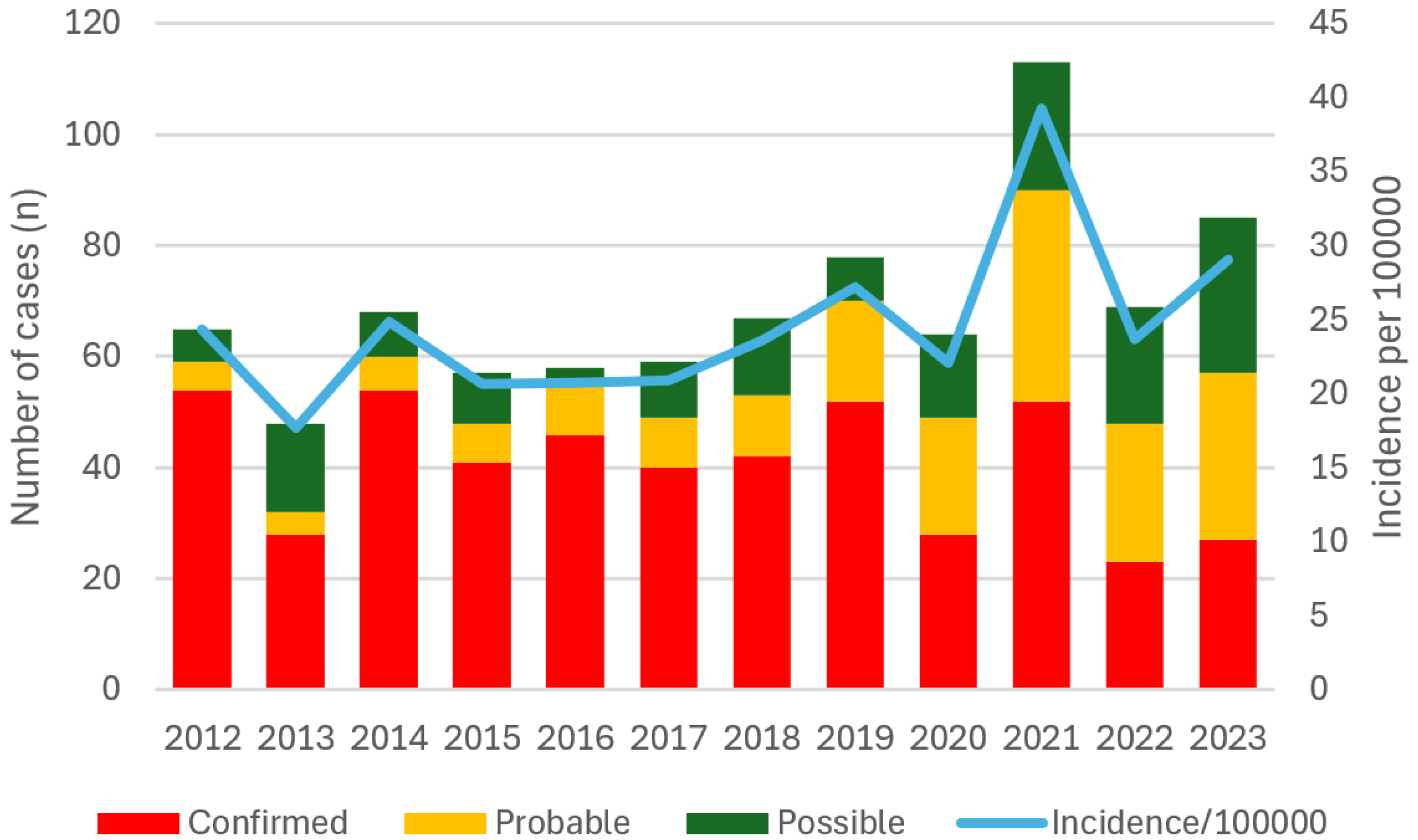
Figure 3.
Geographical distribution of episodes of ARF (both initial and recurrent) in Far North Queensland January 2012 to December 2023.
Figure 3.
Geographical distribution of episodes of ARF (both initial and recurrent) in Far North Queensland January 2012 to December 2023.
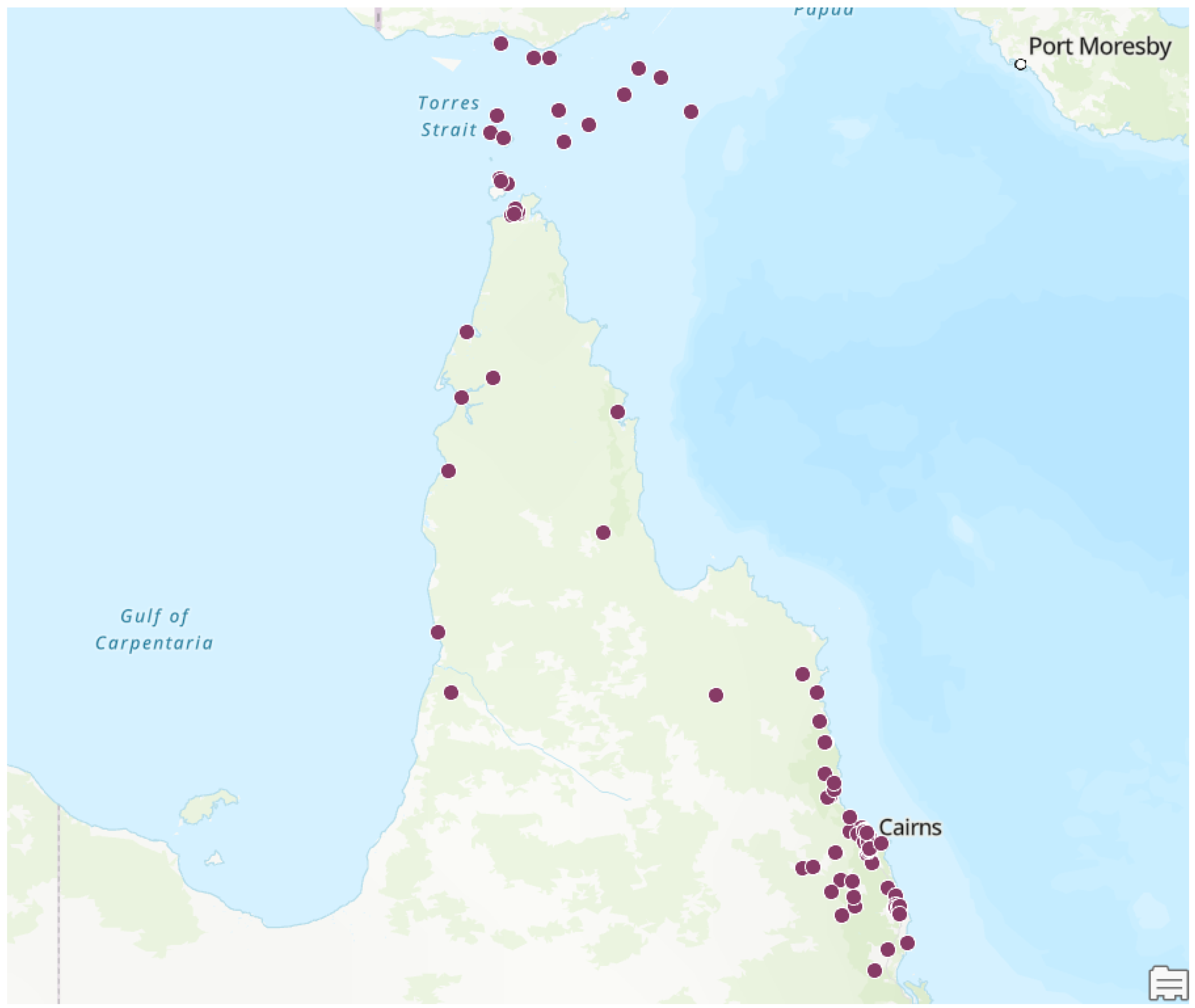
Figure 4.
Age at ARF onset, by case definition in Far North Queensland January 2012 to December 2023.
Figure 4.
Age at ARF onset, by case definition in Far North Queensland January 2012 to December 2023.
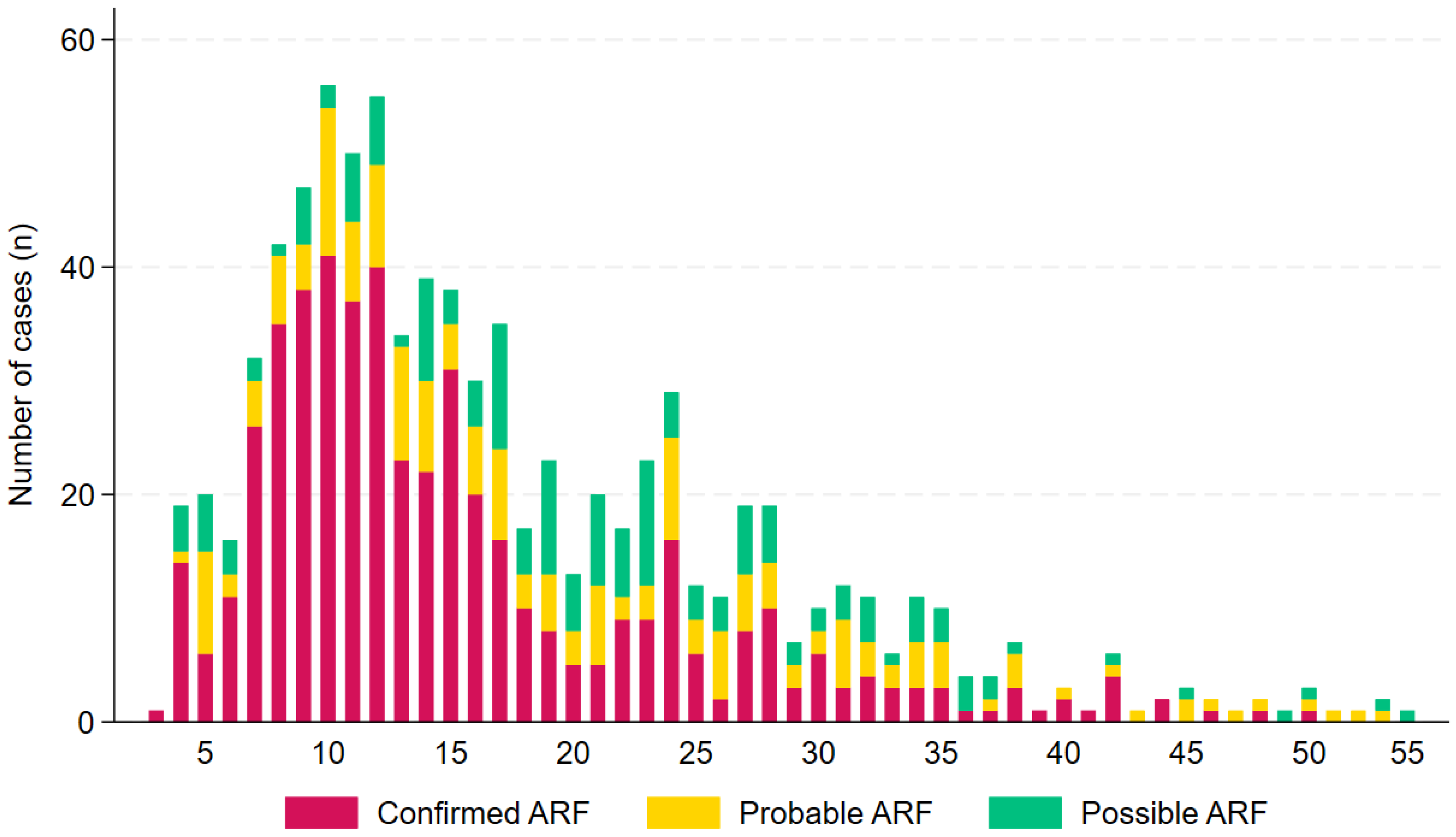
Figure 5.
Socio-Economic Disadvantage of the episodes of ARF (both initial and recurrent) in Far North Queensland January 2012 to December 2023 (decile of ISRAD score presented) [19].
Figure 5.
Socio-Economic Disadvantage of the episodes of ARF (both initial and recurrent) in Far North Queensland January 2012 to December 2023 (decile of ISRAD score presented) [19].
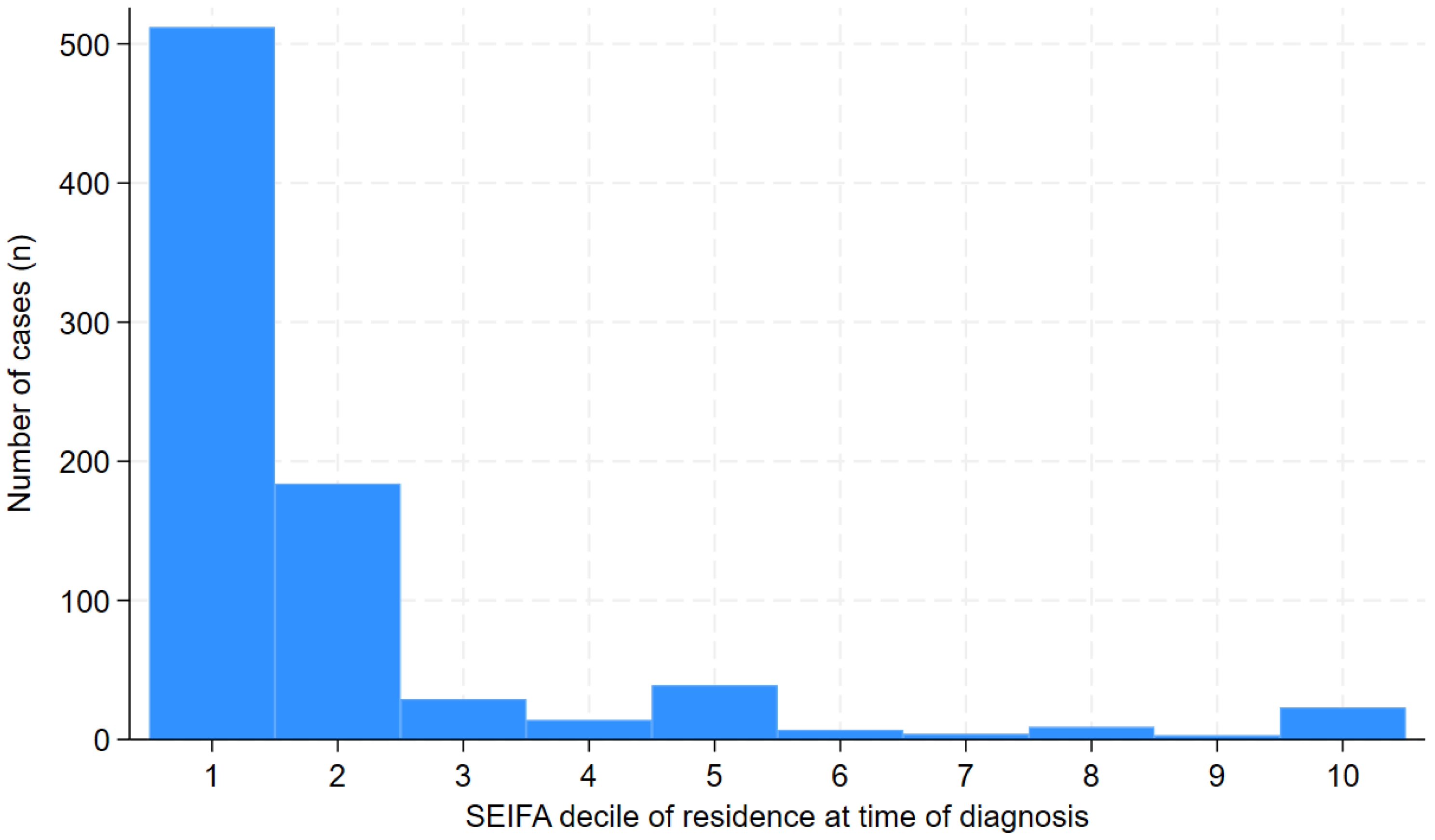
Figure 6.
Prevalence and severity of RHD on latest ECHO in individuals diagnosed with ARF in Far North Queensland, 2012 to 2023.
Figure 6.
Prevalence and severity of RHD on latest ECHO in individuals diagnosed with ARF in Far North Queensland, 2012 to 2023.
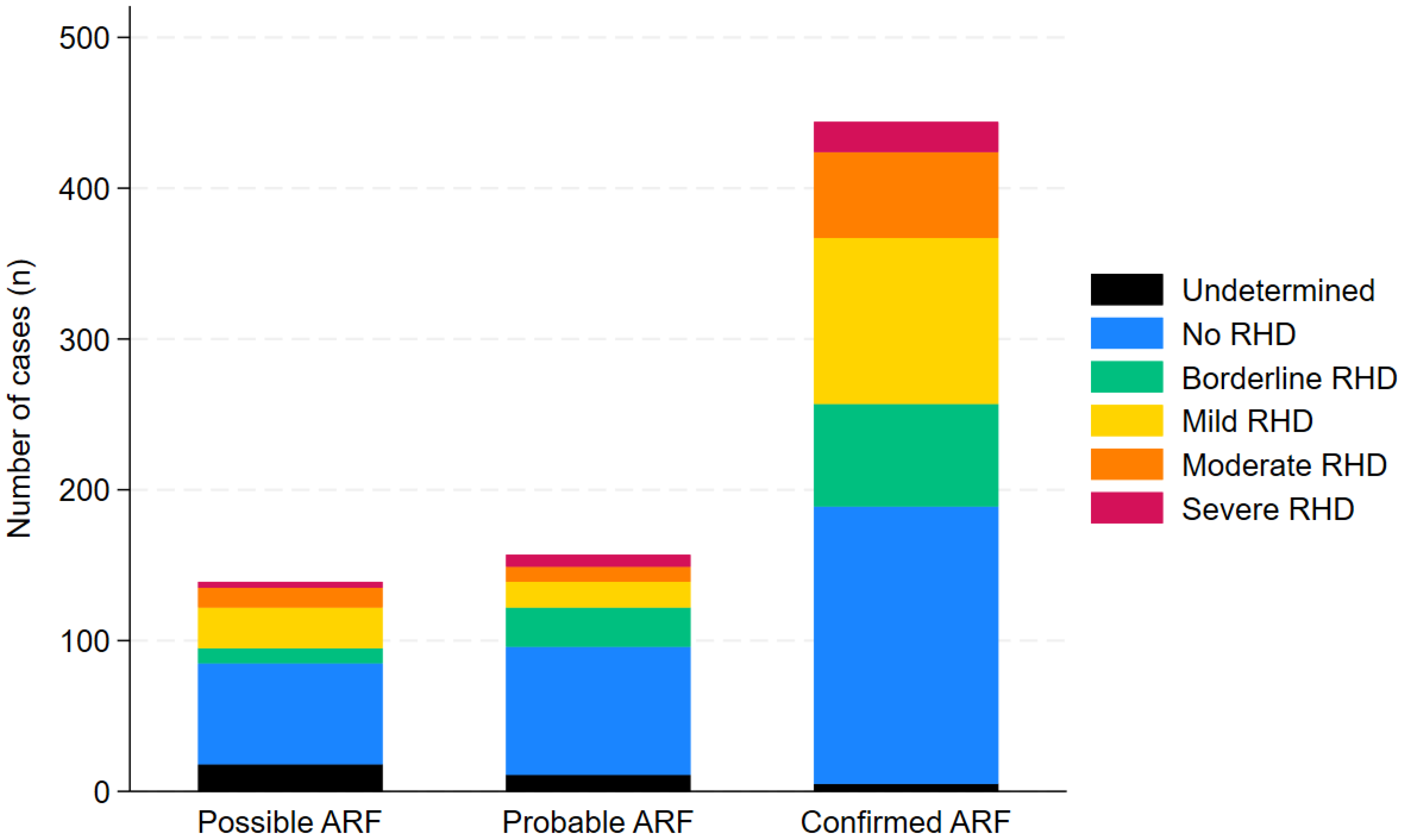

Table 1.
Major and minor manifestations for the diagnosis of acute rheumatic fever in Australia [15].
Table 1.
Major and minor manifestations for the diagnosis of acute rheumatic fever in Australia [15].
| High-risk individuals | All other individuals |
|---|---|
| Major manifestations | |
|
|
| Minor manifestations | |
|
|
a High-risk individuals include: an Aboriginal and/or Torres Strait Islander person living in a rural or remote area; an Aboriginal and/or Torres Strait Islander person, or a Māori and/or Pacific person, living in a household affected by overcrowding or experiencing socioeconomic disadvantage; a person with a history of acute rheumatic fever or rheumatic heart disease; part of a family or household in which a member has a recent history of acute rheumatic fever or rheumatic heart disease; living in a household affected by overcrowding and experiencing socioeconomic disadvantage; current or prior residence in, or frequent or recent travel to, an Australian setting with a high rate of acute rheumatic fever; current or prior residence in, or frequent or recent travel to, an international setting with a high rate of acute rheumatic fever. bIf Sydenham chorea is present, provided other causes of chorea are excluded, other clinical manifestations of acute rheumatic fever and evidence of preceding S. pyogenes infection are not required to make a diagnosis of definite acute rheumatic fever.
Table 2.
Demographic characteristics of episodes of ARF (both initial and recurrent) in Far North Queensland January 2012 to December 2023.
Table 2.
Demographic characteristics of episodes of ARF (both initial and recurrent) in Far North Queensland January 2012 to December 2023.
| All n=830 | Confirmedn=492 | Probablen=180 | Possiblen=158 | |
|---|---|---|---|---|
| Age | ||||
| <5 years | 20 (2%) | 15 (3%) | 1 (1%) | 4 (3%) |
| 5-9 years | 157 (19%) | 116 (24%) | 25 (14%) | 16 (10%) |
| 10-14 years | 234 (28%) | 163 (33%) | 47 (26%) | 24 (15%) |
| 15-19 years | 143 (17%) | 85 (17%) | 26 (14%) | 32 (20%) |
| 20-24 years | 102 (12%) | 44 (9%) | 24 (13%) | 34 (22%) |
| ≥ 25 years | 174 (21%) | 69 (14%) | 57 (32%) | 48 (30%) |
| Population group | ||||
| Aboriginal | 429 (52%) | 248 (50%) | 96 (53%) | 85 (54%) |
| Torres Strait Islander | 237 (29%) | 145 (29%) | 52 (29%) | 40 (25%) |
| Aboriginal and Torres Strait Islander | 119 (14%) | 64 (13%) | 25 (14%) | 30 (19%) |
| Māori | 6 (1%) | 5 (1%) | 1 (1%) | 0 |
| Pacific Islander | 12 (1%) | 11 (2%) | 0 | 1 (1%) |
| Other High Risk | 13 (1%) | 10 (2%) | 3 (2%) | 0 |
| Other Low Risk | 14 (1%) | 9 (2%) | 3 (2%) | 2 (1%) |
| Sex | ||||
| Female | 475 (57%) | 264 (54%) | 111 (62%) | 100 (63%) |
| Male | 355 (43%) | 228 (46%) | 69 (38%) | 58 (37%) |
| Geography | ||||
| CHHHS | 371 (45%) | 217 (44%) | 88 (49%) | 66 (42%) |
| TCHHS | 459 (55%) | 275 (56%) | 92 (51%) | 92 (58%) |
CHHHS: Cairns and Hinterland Hospital and Health Service; TCHHS: Torres and Cape Hospital and Health Service.
Table 3.
Clinical characteristics of ARF episodes (both initial and recurrent) in Far North Queensland, January 2012 to December 2023.
Table 3.
Clinical characteristics of ARF episodes (both initial and recurrent) in Far North Queensland, January 2012 to December 2023.
| Confirmedn=492 | Probablen=180 | Possiblen=158 | Odds ratio a(95% CI) | p | |
|---|---|---|---|---|---|
| Major Criteria | |||||
| Polyarthralgia | 231 (47%) | 95 (53%) | 76 (48%) | 0.86 (0.66-1.14) | 0.30 |
| Monoarthritis | 59 (12%) | 17 (9%) | 23 (15%) | 1.02 (0.66-1.56) | 0.95 |
| Polyarthritis | 130 (26%) | 37 (21%) | 14 (9%) | 2.02 (1.41-2.89) | <0.001 |
| Carditis | 89 (18%) | 13 (7%) | 2 (1%) | 4.76 (2.70-8.38) | <0.001 |
| Sydenham's Chorea | 53 (11%) | 0 | 0 | - | - |
| Erythema Marginatum | 8 (2%) | 4 (2%) | 1 (1%) | 1.10 (0.36-3.39) | 0.87 |
| Subcutaneous Nodules | 6 (1%) | 3 (2%) | 1 (1%) | 1.03 (0.29-3.68) | 0.96 |
| Minor Criteria | |||||
| Monoarthralgia | 32 (7%) | 14 (8%) | 21 (13%) | 0.60 (0.36-0.99) | 0.047 |
| Fever | 295 (60%) | 69 (38%) | 45 (28%) | 2.94 (2.20-3.93) | <0.001 |
| Prolonged PR interval | 161 (33%) | 23 (13%) | 12 (8%) | 4.21 (2.83-6.27) | <0.001 |
| CRP >30mg/L | 358 (73%) | 104 (58%) | 48 (30%) | 3.27 (2.44-4.38) | <0.001 |
| ESR >30mm/hr | 296 (60%) | 102 (57%) | 52 (33%) | 1.80 (1.36-2.39) | <0.001 |
| Evidence of GAS infection | |||||
| Median (IQR) ASOT (U/mL) | 768 (496-1190) | 578 (347-1000) | 395 (223-597) | 1.10 (1.07-1.14) b | <0.001 |
| Median (IQR) Anti-DNase B (U/mL) | 650 (429-1015) | 586 (389-954) | 391 (257-735) | 1.06 (1.03-1.10)b | <0.001 |
| Positive skin swab | 26 (5%) | 9 (5%) | 8 (5%) | 1.05 (0.56-1.97) | 0.87 |
| Positive throat swab | 43 (9%) | 15 (8%) | 12 (8%) | 1.10 (0.67-1.82) | 0.70 |
| Positive blood culture | 1 (0.2%) | 0 | 0 | - | - |
| Stated history | 96 (20%) | 43 (24%) | 27 (17%) | 0.93 (0.66-1.31) | 0.67 |
| Unknown | 326 (66%) | 113 (63%) | 111 (70%) | 1.00 (0.75-1.34) | 1.0 |
a Of presence in cases of confirmed ARF. b For every increase of 100U/mL.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



