
Submitted:
26 March 2025
Posted:
27 March 2025
You are already at the latest version
Abstract
Introduction.Despite significant advancements in surgical techniques for reconstructing severely resorbed alveolar bone, achieving predictable regeneration remains a considerable challenge. Many conventional ridge augmentation methods require extended edentulous healing periods and multiple surgical interventions. This clinical study presents an innovative and simplified approach for advanced ridge augmentation using a wide-head tent-pole screw (WHTPS), designed to enhance procedural efficiency while ensuring reliable clinical outcomes. Material and Methods. Thirteen patients with severely vertically resorbed mandibular segments or completely edentulous alveolar ridges, each presenting with a minimum vertical bone defect of 5 mm or more, were included in this study. A single WHTPS was placed at the most severe bone defect site, followed by bone graft placement and coverage with a resorbable membrane. Postoperatively, a panoramic radiograph was taken, with an additional radiograph obtained on the day of WHTPS removal after a healing period of 3 to 6 months. Furthermore, a follow-up panoramic radiograph was taken after the final prosthesis placement, with an average follow-up of 5.5 months, to assess changes in the augmented alveolar bone. Patients were clinically monitored for a period ranging from 8 to 20 months, with an average duration of 13.9 months. Results. The average vertical bone gain immediately after surgery was 8.86 mm (SD: ±2.59 mm), while an average bone resorption of 1.49 mm (17.79%) was observed during the follow-up period. Conclusion. A single WHTPS effectively stabilized the graft material in cases of severe alveolar bone loss, preventing resorption and displacement. This technique simplified the surgical procedure while ensuring predictable vertical bone augmentation. Further clinical studies are required to validate its long-term effectiveness.
Keywords:
vertical ridge augmentation
; guided bone regeneration
; bone grafts
; tenting pole screw
; peri-implantitis
; vertical bone defects
1. Introduction
The loss of teeth not only impairs chewing ability but also adversely affects overall well-being and leads to aesthetic concerns.[1] Dental implants are regarded as the optimal solution for restoring oral function, as they provide natural aesthetics, reliable performance, and long-term durability.[2] However, implant placement in sites with severe vertical bone deficiencies remains a challenging and technically demanding procedure.[3] Various surgical approaches have been proposed for augmenting severely atrophic alveolar ridges.[4,5,6,7,8,9] However, these techniques commonly present drawbacks, including prolonged operative time, increased surgical trauma, and extended edentulous periods.[10] In cases of significant mandibular bone loss, grafts frequently undergo rapid resorption due to inadequate soft tissue coverage, which exerts compressive forces on the graft material. To address these limitations, a technique employing dental implants to induce a tenting effect has been developed, enhancing graft stabilization and preserving bone graft volume. [11,12,13] If simultaneous implant placement is not possible at the defect site, a small-diameter tenting pole screw can be used to facilitate vertical bone augmentation. However, while this surgical approach is relatively simpler compared to other techniques, it has certain drawbacks. When placing a mini screw with a narrow diameter head in areas with severe vertical bone deficiency, the soft tissue matrix expansion effect is reduced, leading to insufficient vertical bone regeneration. Due to this limitation, multiple tenting pole screws must be placed to achieve the desired effect, which can lead to prolonged surgical time. [14,15,16] To overcome this drawback, a wide-head tent pole screw (WHTPS) has been introduced. This study aims to evaluate the effectiveness of a WHTPS in vertical bone augmentation by addressing the limitations of small-diameter tenting pole screws. Through a 24-month clinical and radiographic follow-up, the research assesses WHTPS’s ability to maintain augmented bone height and improve vertical ridge augmentation techniques. The goal is to validate this novel device’s efficacy in overcoming the challenges of severe vertical ridge defects.
2. Materials and Methods
Patient selection. This study included 13 patients treated between 2018 and 2022 at the Catholic University Hospital of Daegu, with approval from the local university ethics committee (IRB No. 2024-11-002). All participants provided informed consent for their treatment and agreed to the use of their data in this study. To ensure reliable outcomes, patients were selected based on strict inclusion criteria. Eligibility criteria required a vertical ridge defect of at least 5 mm, confirmed by cone beam computed tomography (CBCT) and a panoramic radiograph. Patients with systemic conditions that could impair bone healing, such as uncontrolled diabetes or osteoporosis, were excluded from the study. Although smokers were informed of the potential risks of reduced augmentation success, they were not excluded from the study. A comprehensive review of medical histories confirmed that all participants had no contraindications for surgical intervention. All patients had partial or complete edentulism in the mandibular premolar and molar regions, requiring vertical ridge augmentation and bridge restoration supported by multiple connected implants. Preoperative cone beam computed tomogram (CBCT) scans and panoramic radiographs to assess initial bone height and defect dimensions.
Surgical and restoration procedure. The surgical procedure was performed under local anesthesia with 2% lidocaine containing 1:100,000 epinephrine, following the intravenous administration of preoperative antibiotics (Flomoxef, Flumarin®, Ildong Pharm, Korea). Venous blood was drawn from the patient’s forearm to prepare autologous fibrin glue and a concentrated growth factor (CGF) membrane, which were used to create sticky bone, a technique initially described by Sohn et al.17 A crestal incision was made, extending from the retromolar pad, along with anterior and posterior vertical incisions that connected to the crestal incision. These vertical incisions extended divergently beyond the mucogingival junction at a 45-degree angle into the mucosa. The full thickness lingual flap was coronally and lingually mobilized using a periosteal elevator, which dissected the periosteum and superficial fibers of the mylohyoid muscle. Meanwhile, the buccal flap’s periosteum was released using a No. 15c blade. Any residual soft tissue within the bony defect was meticulously cleared using a surgical curette. To ensure proper occlusion and precise implant positioning, a surgical guide (BonePen guide, Acrodent Co., Korea) was employed to prepare implant sites. As a final drill, a drill 1 mm narrower than the implant diameter was used to perform an under-osteotomy, optimizing primary implant stability. Implants (Biotem Implant Co, Seoul, Korea) were placed into the edentulous ridge, serving as tenting pole screws to function as space maintainers. They were placed 2 mm subcrestally relative to the adjacent proximal bone height. To facilitate bone over-grafting above the implant platform, a 2 mm high tenting pole abutment (SANTA®, Biotem implant Co, Seoul, Korea) was secured onto the implant platform, serving as a vertical tenting device, and was tightened to 10 Ncm. In the alveolar ridge with the most severe vertical bone defect, no implant was placed to avoid injury to the inferior alveolar nerve, and the site was planned for restoration with a pontic instead. To prevent grafted bone collapse at the pontic site due to soft tissue contraction during the healing period, a 6 mm or 8 mm diameter round and 12-14 mm long WHTPS (SBB®; Biotem Implant Co., Seoul, Korea) was placed in the buccal or lingual cortical bone after site preparation using a 1.2 mm-wide pilot drill. The WHTPS was inserted using a 0.48-inch hex driver connected to an implant motor at 40 rpm, with its head positioned at a height similar to that of the SANTA head on the adjacent implants. Autogenous bone was harvested from the buccal alveolar bone posterior to the most distal implant using an autobone chip maker (ACM, Neobiotec Implant Co, Seoul, Korea). The sticky autogenous bone was then grafted around the exposed implant, followed by the application of sticky bovine bone to the exposed implant, WHTPS and bony defect to facilitate three-dimensional ridge augmentation. The sticky bone graft material was placed to completely cover the heads of both the tenting pole abutment and the WHTPS. A collagen membrane was placed over the graft, followed by a compressed CGF membrane on top to enhance soft tissue healing. To secure the resorbable membrane, neither membrane tacks nor membrane fixation sutures were used, which significantly reduced the surgical time. A tension-free closure was successfully achieved using a non-absorbable 4-0 nylon suture. (Figure 1, Figure 2 and Figure 3) A panoramic radiograph and CBCT were taken immediately after surgery to measure and record both the existing bone height and the augmented bone height. Stitch removal was performed at the 2-week postoperative visit. The uncovering procedure was performed after an average of 5 months of healing, during which the WHTPS was removed. Two weeks later, the sutures were removed, and an impression for the provisional restoration was taken simultaneously. The provisional restoration was placed one week later. After using the provisional restoration for one month, an impression was taken for the final zirconia-based prosthesis, which was placed one week afterward. At the same time, a panoramic radiograph was taken to assess the final augmented bone height and measure bone resorption over a period of 3 to 7 months (average of 5.5 months). Follow-up was conducted 4 to 6 months after the final prosthetic loading, during which suture-less free gingival graft procedures were performed if necessary. (Figure 4 and Figure 5)
Radiographic analysis. Dimensional change of augmented ridge was evaluated using panoramic radiographs according to Park YH et al’s published study.[18] (Figure 5) A reference line was drawn parallel to the long axis of the adjacent teeth, with the top of the tent-pole screw serving as the central point. Measurement 1 represents the total bone height, measured as the distance from the lowest point of the mandible (mandibular base) to the top of the tent-pole screw. Measurement 2 represents the augmented bone height, measured as the distance from the top of the tent-pole screw to the interface where the grafted bone meets the native mandibular bone (graft junction).Original Bone Height, an extension of Measurement 2, is defined as the distance from the graft junction (native mandibular bone) to the lowest point of the mandible (mandibular base), serving as the baseline bone height before augmentation. During the second and third measurement periods, only Measurement 1 was reassessed to evaluate the long-term maintenance of the augmented bone height. All measurements were performed twice by a single examiner, and the average value was used to ensure consistency. The margin of error for these measurements was limited to ±0.1 mm.
3. Results
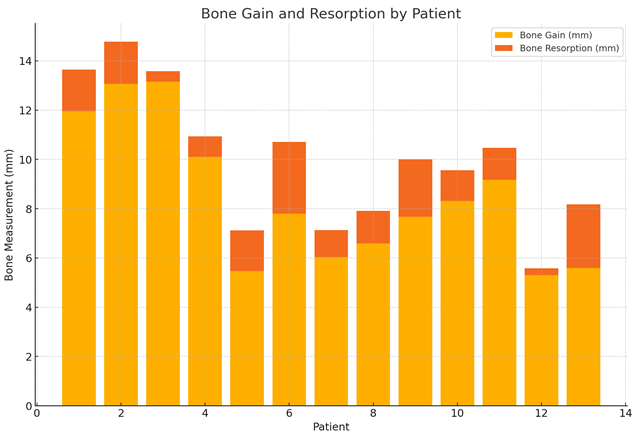
A total of 13 patients (5 males, 8 females; mean age: 52.4 years) with severe vertical ridge deficiencies underwent vertical ridge augmentation using WHTBS. The follow-up period ranged from 8 to 24 months, with an average of 14.9 months. During the study period, no implant exhibited signs of mobility or failure, resulting in a 100% survival rate. Immediately following surgery, as shown in Table 1, radiographic evaluations revealed that the augmented bone height averaged 8.86 mm (range: 5.30 to 13.15 mm, SD: ±2.59 mm), while the preoperative bone height ranged from 5.0 to 7.2 mm (mean: 6.1 mm, SD: ±0.7 mm). During the follow-up period, the mean bone resorption was measured at 1.49 mm (range: 0.28 to 2.91 mm), accounting for 17.79% of the initially augmented height. This trend in bone gain and resorption is visually summarized in Table 2, illustrating the variability among patients. Despite this resorption, radiographs consistently demonstrated stable integration of the graft material, with no signs of significant collapse, migration, or structural compromise. The WHTPS effectively stabilized the graft material in pontic regions, enabling successful vertical ridge augmentation without any signs of severe graft collapse or migration. The use of the tent-pole abutment ((SANTA®, Biotem Implant Co., Seoul, Korea)) also facilitated successful bone grafting over the implant platform, with radiographic evaluations confirming that the graft material remained stable and well supported above the implant platform. Clinically, 12 out of 13 cases exhibited uneventful healing, with no signs of infection, inflammatory reactions, or peri-implant bone resorption below the implant platform. One patient presented with partial wound exposure two weeks postoperatively, resulting in approximately 40% graft resorption. This complication was managed successfully with a secondary grafting procedure performed one month later. Subsequent healing was uneventful, and the implants remained stable throughout the follow-up period.
4. Discussion
Vertical ridge augmentation remains one of the most technically demanding procedures in implant dentistry due to the challenge of restoring adequate vertical bone height for predictable implant placement. [19] Various techniques, including guided bone regeneration (GBR), onlay block grafting, titanium mesh, distraction osteogeensis and sandwich augmentation with interpositional bone graft have been utilized to address these defects. While these approaches have demonstrated clinical efficacy, their limitations—such as procedural complexity, higher resorption rates, and increased patient morbidity—highlight the need for more reliable and efficient solutions. [20] Onlay block grafting is widely regarded as the gold standard for vertical ridge augmentation, typically involving the harvesting of autogenous bone from secondary donor sites such as the iliac crest or mandibular chin.[18] While autogenous bone offers osteogenic, osteoinductive, and osteoconductive properties, its clinical application is often limited due to significant donor site morbidity. Patients frequently experience postoperative pain, prolonged healing times, and increased surgical trauma associated with bone harvesting procedures. Additionally, block grafts are prone to resorption, with reported rates ranging from 25% to 40% within the first year, particularly in vertical ridge augmentation cases. [21,22] Titanium mesh has emerged as an alternative approach for vertical ridge augmentation due to its rigid structure, which effectively maintains space for the graft material. [23] The open architecture of titanium mesh promotes vascularization of the graft, facilitating bone regeneration. However, titanium mesh introduces additional challenges, including soft tissue irritation and mesh exposure, which increase the risk of infection and graft contamination. [24,25] Distraction osteogenesis enables vertical bone augmentation without requiring bone harvesting from other sites. However, it has limitations, including difficulties in precisely controlling force vectors and the potential for improper positioning of the distracted segment. Additionally, this technique does not facilitate horizontal bone augmentation, often necessitating supplementary horizontal grafting procedures. [26] The sandwich technique with an interpositional bone graft enables vertical bone augmentation of 6-10 mm without requiring bone harvesting from other areas. [27] This method involves a pedicled bone graft, which offers the benefit of reduced resorption over time compared to a free autogenous bone block. However, it does not contribute to horizontal ridge augmentation. To manage vertical bone deficiencies, the ramus split bone technique has been used as an alternative to block bone grafting. [28] Guided bone regeneration is recognized for its relative simplicity and reduced trauma compared to more complex bone augmentation procedures. However, it also has inherent limitations, particularly in achieving significant vertical bone augmentation. In guided bone regeneration, non-resorbable membranes with excellent space-making ability were shown to result in greater vertical bone augmentation compared to resorbable membranes. However, they are also associated with an increased risk of membrane exposure. [29,30] Another drawback is that the membrane must be secured with multiple membrane tacks, which extends the surgical time. Additionally, since implants are not placed simultaneously, the number of surgical procedures increases, and the overall treatment duration until the final prosthesis is significantly prolonged. Additionally, guided bone regeneration is associated with high resorption rates, ranging from 20% to 37% within the first six months, particularly in cases involving significant vertical ridge augmentation. [31] Guided bone regeneration has demonstrated vertical bone gain with fewer complications compared to bone block techniques in vertical bone regeneration. However, due to its limitations in achieving vertical augmentation, a modified approach incorporating guided bone regeneration with tenting pole screws has been introduced to maintain the desired space for bone regeneration. This technique enhances space maintenance, facilitating the formation of new bone. [32,33,34] Vertical augmentation using tent-pole screws has the advantage of being less technically demanding compared to other techniques. However, due to the small head diameter of mini screws, the effect of soft tissue matrix expansion is limited. As a result, multiple mini screws must be placed simultaneously, even in areas with minimal bone ridge width to achieve the desired space maintenance, resulting in prolonged surgical time, Additionally, since implants cannot be placed simultaneously, the healing period for edentulous patients is significantly delayed. Moreover, the placement of multiple mini screws increases the risk of damage to the adjacent teeth and surrounding structures. To overcome the limitations of vertical bone augmentation using multiple narrow-head tenting pole screws, a single WHTPS was placed in the edentulous ridge where vertical augmentation was required in the pontic area between simultaneously placed implants in this study. This approach offers the advantages of reducing surgical time and enhancing the tenting effect on the periosteum and soft tissue matrix due to its wider head. In this study, implants were placed simultaneously as an alternative tent pole technique. This method reduces the number of surgical procedures while significantly shortening the patient’s edentulous period. [15,35,36,37] The augmented ridge undergoes remodeling over time, some degree of dimensional resorption is inevitable. [38,39] To mitigate this, over-grafting above the implant platform is necessary to preserve bone volume. In this study, a tenting pole abutment (SANTA®, Biotem Implant Co., Seoul, Korea) was placed on the implant platform to create space for bone grafting material, counteracting remodeling-related resorption. When combined with guided bone regeneration, this technique effectively maintained the grafted space, preventing collapse due to soft tissue contraction during healing and ensuring long-term bone stability over the implant platform. This approach was technically less complex and associated with fewer complications than advanced augmentation methods such as block bone grafting or mesh-assisted ridge augmentation. Additionally, it shortened the edentulous healing period and reduced the need for multiple surgical interventions. [40,41,42]
5. Conclusions
This retrospective study demonstrated that a single WHTPS is a reliable and effective solution for managing severe vertical ridge defects in sites where implants are not placed simultaneously. It simplified surgical procedures, enhancing efficiency and predictability. However, the study's short follow-up period and small dataset may limit the generalizability of the findings. Despite these limitations, WHTPS remains a promising option for complex vertical augmentation cases.
Author Contributions
Conceptualization, D.S. Sohn; methodology, investigation, resources, data curation, N.Y. Yoon; writing—original draft preparation, N.Y. Kim, H.G. Kim, and H.K.; writing, review and editing. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Institutional Review Board at the Catholic University Hospital of Daegu, with approval from the local university ethics committee (IRB No. 2024-11-002).
Informed Consent Statement
Written informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data presented in this study are available on request from the corresponding author.
Conflicts of Interest
D.D Sohn is the developer of WHTPS. All other authors declare that they have no conflicts of interest with the content of this manuscript.
References
- Gerritsen, A.E.; Allen, P.F.; Witter, D.J.; Bronkhorst, E.M.; Creugers, N.H. Tooth loss and oral health-related quality of life: a systematic review and meta-analysis. Health Qual Life Outcomes 2010, 8, 126. [Google Scholar] [CrossRef] [PubMed]
- Chiapasco M Casentini, P. Zaniboni M. Bone augmentation procedures in implant dentistrry. Int J Oral Maxillofacial Implants. 2009, 24, 237–259. [Google Scholar]
- Gerritsen, A.E.; Allen, P.F.; Witter, D.J.; Bronkhorst, E.M.; Creugers, N.H. Tooth loss and oral health-related quality of life: a systematic review and meta-analysis. Health Qual Life Outcomes 2010, 8, 126. [Google Scholar] [CrossRef] [PubMed]
- Nobuto, T.; Imai, H.; Suwa, F.; Kono, T.; Suga, H.; Jyoshi, K.; Obayashi, K. Microvascular response in the periodontal ligament following mucoperiosteal flap surgery. J Periodontol. 2003, 74, 521–528. [Google Scholar] [CrossRef] [PubMed]
- Botticelli, D.; Berglundh, T.; Lindhe, J. Hard-tissue alterations following immediate implant placement in extraction sites. J Clin Periodontol 2004, 31, 820–828. [Google Scholar] [CrossRef]
- Minetti, E.; Celko, M.; Contessi, M.; Carini, F.; Gambardella, U.; Giacometti, E.; Santillana, J.; Beca Campoy, T.; Schmitz, J.H.; Libertucci, M.; Ho, H.; Haan, S.; Mastrangelo, F. Implants Survival Rate in Regenerated Sites with Innovative Graft Biomaterials: 1 Year Follow-Up. Materials 2021, 14, 5292. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Tulio, A.V.; Kang, C.D.; Fabian, O.A.; Kim, G.E.; Kim, H.G.; Sohn, D.S. Socket preservation using demineralized tooth graft: A case series report with histological analysis. Int J Growth Factors Stem Cells Dent 2020, 3, 28–35. [Google Scholar]
- Menchini-Fabris, G.B.; Cosola, S.; Toti, P.; Hwan Hwang, M.; Crespi, R.; Covani, U. Immediate Implant and Customized Healing Abutment for a Periodontally Compromised Socket: 1-Year Follow-Up Retrospective Evaluation. J Clin Med. 2023, 12, 2783. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Dhadse, P.V.; Yeltiwar, R.K.; Bhongade, M.L.; Pendor, S.D. Soft tissue expansion before vertical ridge augmentation: Inflatable silicone balloons or self-filling osmotic tissue expanders? J Indian Soc Periodontol. 2014, 18, 433–440. [Google Scholar] [CrossRef]
- Bera, R.N.; Tandon, S.; Singh, A.K.; Bhattacharjee, B.; Pandey, S.; Chirakkattu, T. Sandwich osteotomy with interpositional grafts for vertical augmentation of the mandible: A meta-analysis. Natl J Maxillofac Surg. 2022, 13, 347–356, Khoury F, Hanser T. Mandibular bone block harvesting from the retromolar region: a 10-year prospective clinical study. Int J Oral Maxillofac Implants. 2015, 30, 688–697. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Urban, I.A.; Lozada, J.L.; Wessing, B.; Suárez-López del Amo, F.; Wang, H.L. Vertical bone grafting and periosteal vertical mattress suture for the fixation of resorbable membranes and stabilization of particulate grafts in horizontal guided bone regeneration to achieve more predictable results: a technical report. Int J Periodontics Restor. Dent. 2016, 36, 153–159. [Google Scholar] [CrossRef]
- Chavda, S.; Levin, L. Human Studies of Vertical and Horizontal Alveolar Ridge Augmentation Comparing Different Types of Bone Graft Materials: A Systematic Review. J Oral Implantol. 2018, 44, 74–84. [Google Scholar] [CrossRef] [PubMed]
- Fekry, Y.E.; Mahmoud, N.R. Vertical ridge augmentation of atrophic posterior mandible with corticocancellous onlay symphysis graft versus sandwich technique: clinical and radiographic analysis. Odontology. 2023, 111, 993–1002. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Sáez-Alcaide, L.M.; González Gallego, B.; Fernando Moreno, J.; Moreno Navarro, M.; Cobo-Vázquez, C.; Cortés-Bretón Brinkmann, J.; Meniz-García, C. Complications associated with vertical bone augmentation techniques in implant dentistry: A systematic review of clinical studies published in the last ten years. J Stomatol Oral Maxillofac Surg. 2023, 124, 101574. [Google Scholar] [CrossRef]
- Marx, R.E.; Shellenberger, T.; Wimsatt, J.; Correa, P. Severely resorbed mandible: predictable reconstruction with soft tissue matrix expansion (tent pole) grafts. J Oral Maxillofac Surg. 2002, 60, 878–888, discussion 888-889. [Google Scholar] [CrossRef] [PubMed]
- Woo, R.H.; Kim, H.G.; Kim, G.; Park, W.E.; Sohn, D.S. Simplified 3-dimensional ridge augmentation using a tenting abutment. Adv Dent & Oral Health 2020, 12, 185–205. [Google Scholar]
- Sohn, D.S.; Huang, B.; Kim, J.; Park, W.E.; Park, C.C.; et al. Utilization of autologous concentrated growth factors (CGF) enriched bone graft matrix (Sticky Bone) and CGF-enriched fibrin membrane in implant dentistry. J. Implant. Adv. Clin. Dent. 2015, 7, 11–29. [Google Scholar]
- Park, Y.H.; Choi, S.H.; Cho, K.S.; Lee, J.S. Dimensional alterations following vertical ridge augmentation using collagen membrane and three types of bone grafting materials: A retrospective observational study. Clin Implant Dent Relat Res. 2017, 19, 742–749. [Google Scholar] [CrossRef] [PubMed]
- Misch, C.M.; et al. Reconstruction of maxillary alveolar defects with mandibular symphysis grafts for dental implants; a preliminary procedural report. Int J Oral Maxillofac Implants. 1992, 7, 360–366. [Google Scholar]
- Vermeeren, J.I.; Wismeijer, D.; van Waas, M.A. One-step reconstruction of the severely resorbed mandible with onlay bone grafts and endosteal implants. A 5-year follow-up. Int J Oral Maxillofac Surg. 1996, 25, 112–115. [Google Scholar] [CrossRef]
- Sbordone, L.; Toti, P.; Menchini-Fabris, G.B.; Sbordone, C.; Piombino, P.; Guidetti, F. Volume changes of autogenous bone grafts after alveolar ridge augmentation of atrophic maxillae and mandibles. Int J Oral Maxillofac Surg. 2009, 38, 1059–1065. [Google Scholar] [CrossRef] [PubMed]
- Sakkas, A.; Schramm, A.; Winter, K.W. Risk factors for post-operative complications after procedures for autologous bone augmentation from different donor sites. J Craniomaxillofac Surg. 2018, 46, 312–322. [Google Scholar] [CrossRef]
- Sanz-Sánchez, I.; Sanz-Martín, I.; Ortiz-Vigón, A.; Molina, A.; Sanz, M. Complications in bone-grafting procedures: Classification and management. Periodontol 2022, 88, 86–102. [Google Scholar] [CrossRef] [PubMed]
- Chiapasco, M.; Consolo, U.; Bianchi, A.; Ronchi, P. Alveolar distraction osteogenesis for the correction of vertically deficient edentulous ridges: a multicenter prospective study on humans. Int J Oral Maxillofac Implants. 2004, 19, 399–407. [Google Scholar] [CrossRef] [PubMed]
- Melikov, E.A.; Dibirov, T.M.; Klipa, I.A.; Drobyshev, A.Y. Al'veolyarnyi distraktsionnyi osteogenez: vozmozhnye oslozhneniya i sposoby ikh ustraneniya [Alveolar distraction osteogenesis: possible complications and methods of their treatment]. Stomatologiia 2022, 101, 25–30. [Google Scholar] [CrossRef] [PubMed]
- Khoury, F.; Hanser, T. Three-Dimensional Vertical Alveolar Ridge Augmentation in the Posterior Maxilla: A 10-year Clinical Study. Int J Oral Maxillofac Implants. 2019, 34, 471–480. [Google Scholar] [CrossRef]
- Troeltzsch, M.; Troeltzsch, M.; Kauffmann, P.; Gruber, R.; Brockmeyer, P.; Moser, N.; Rau, A.; Schliephake, H. Clinical efficacy of grafting materials in alveolar ridge augmentation: A systematic review. J Craniomaxillofac Surg. 2016, 44, 1618–1629. [Google Scholar] [CrossRef]
- Soldatos, N.K.; Stylianou, P.; Koidou, V.P.; Angelov, N.; Yukna, R.; Romanos, G.E. Limitations and options using resorbable versus nonresorbable membranes for successful guided bone regeneration. Quintessence Int. 2017, 48, 131–147. [Google Scholar]
- Urban, I.A.; Montero, E.; Monje, A.; Sanz-Sánchez, I. Effectiveness of vertical ridge augmentation interventions: A systematic review and meta-analysis. J Clin Periodontol. 2019, 46, 319–339. [Google Scholar] [CrossRef]
- Cucchi, A.; Vignudelli, E.; Napolitano, A.; Marchetti, C.; Corinaldesi, G. Evaluation of complication rates and vertical bone gain after guided bone regeneration with non-resorbable membranes versus titanium meshes and resorbable membranes. A randomized clinical trial. Clin Implant Dent Relat Res. 2017, 19, 821–832. [Google Scholar] [CrossRef]
- Li, S.; Zhao, J.; Xie, Y.; et al. Hard tissue stability after guided bone regeneration: a comparison between digital titanium mesh and resorbable membrane. Int J Oral Sci 2021, 13, 37. [Google Scholar] [CrossRef]
- Le, B.; Rohrer, M.D.; Prasad, H.S. Screw "tent-pole" grafting technique for reconstruction of large vertical alveolar ridge defects using human mineralized allograft for implant site preparation. J Oral Maxillofac Surg. 2010, 68, 428–435. [Google Scholar] [CrossRef] [PubMed]
- Daga, D.; Mehrotra, D.; Mohammad, S.; Singh, G.; Natu, S.M. Tent pole technique for bone regeneration in vertically deficient alveolar ridges: A review. J Oral Biol Craniofac Res. 2015, 5, 92–97. [Google Scholar] [CrossRef] [PubMed]
- Deeb, G.R.; Tran, D.; Carrico, C.K.; Block, E.; Laskin, D.M.; Deeb, J.G. How Effective Is the Tent Screw Pole Technique Compared to Other Forms of Horizontal Ridge Augmentation? J Oral Maxillofac Surg. 2017, 75, 2093–2098. [Google Scholar] [CrossRef] [PubMed]
- Fenton, C.C.; Nish, I.A.; Carmichael, R.P.; Sàndor, G.K. Metastatic mandibular retinoblastoma in a child reconstructed with soft tissue matrix expansion grafting: a preliminary report. J Oral Maxillofac Surg. 2007, 65, 2329–2335. [Google Scholar] [CrossRef]
- Manfro, R.; Batassini, F.; Bortoluzzi, M.C. Severely Resorbed Mandible Treated by Soft Tissue Matrix Expansion (Tent Pole) Grafts: Case Report, Implant Dentistry. 2008, 17, 408–413.
- Elnayef, B.; Monje, A.; Gargallo-Albiol, J.; Galindo-Moreno, P.; Wang, H.L.; Hernández-Alfaro, F. Vertical Ridge Augmentation in the Atrophic Mandible: A Systematic Review and Meta-Analysis. Int J Oral Maxillofac Implants. 2017, 32, 291–312. [Google Scholar] [CrossRef]
- Tay, J.R.H.; Ng, E.; Lu, X.J.; Lai, W.M.C. Healing complications and their detrimental effects on bone gain in vertical-guided bone regeneration: A systematic review and meta-analysis. Clin Implant Dent Relat Res. 2022, 24, 43–71. [Google Scholar] [CrossRef] [PubMed]
- Palkovics, D.; Solyom, E.; Somodi, K.; Pinter, C.; Windisch, P.; Bartha, F.; Molnar, B. Three-dimensional volumetric assessment of hard tissue alterations following horizontal guided bone regeneration using a split-thickness flap design: A case series. BMC Oral Health. 2023, 23, 118. [Google Scholar] [CrossRef]
- Woo, R.H.; Kim, H.G.; Kim, G.; Park, W.; Sohn, D. Simplified 3-Dimensional ridge augmentation using a tenting abutment. Adv Dent Oral Health 2020, 12, 185–205. [Google Scholar]
- Sohn, D.S. Reconstruction of three-dimensional alveolar ridge defects utilizing screws and implant abutments for the tent-pole grafting` techniques. In Tolstunov L, ed. Essential techniques of alveolar bone augmentation in implant dentistry, 2nd ed.; Wiley Blackwell: 2023; 404-418.
- Sohn, D.S.; Lui, A.; Choi, H. Utilization of Tenting Pole Abutments for the Reconstruction of Severely Resorbed Alveolar Bone: Technical Considerations and Case Series Reports. J. Clin. Med. 2024, 13, 1156. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
Figure 1.
Preoperative intraoral image and periapical radiograph. (a) Severe soft and hard tissue vertical defect observed after implant removal due to peri-implantitis. (b) Radiographic image confirming the presence of a significant vertical bone defect.
Figure 1.
Preoperative intraoral image and periapical radiograph. (a) Severe soft and hard tissue vertical defect observed after implant removal due to peri-implantitis. (b) Radiographic image confirming the presence of a significant vertical bone defect.
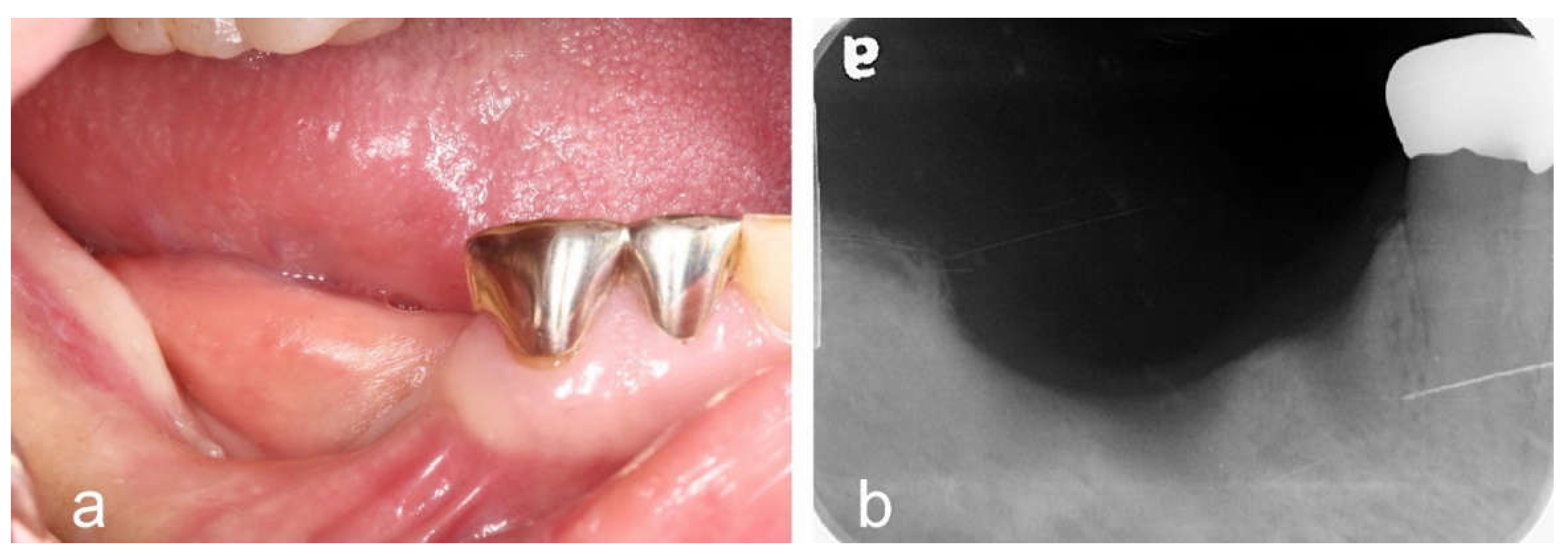
Figure 2.
Surgical procedure. (a) After elevating full-thickness buccal and lingual flaps, an approximately 8mm vertical deficiency was revealed. A 6mm wide × 12mm long WHTPS was placed at the pontic site, and tent-pole abutments were placed on each implant to facilitate over-grafting above the implant platform. (b) Sticky autogenous bone harvested from the buccal cortex was grafted into the bone defect. (c) Sticky bovine bone was placed in the remaining defect to enhance graft stability. (d) A collagen barrier was placed over the bone graft without the use of membrane tacks.
Figure 2.
Surgical procedure. (a) After elevating full-thickness buccal and lingual flaps, an approximately 8mm vertical deficiency was revealed. A 6mm wide × 12mm long WHTPS was placed at the pontic site, and tent-pole abutments were placed on each implant to facilitate over-grafting above the implant platform. (b) Sticky autogenous bone harvested from the buccal cortex was grafted into the bone defect. (c) Sticky bovine bone was placed in the remaining defect to enhance graft stability. (d) A collagen barrier was placed over the bone graft without the use of membrane tacks.
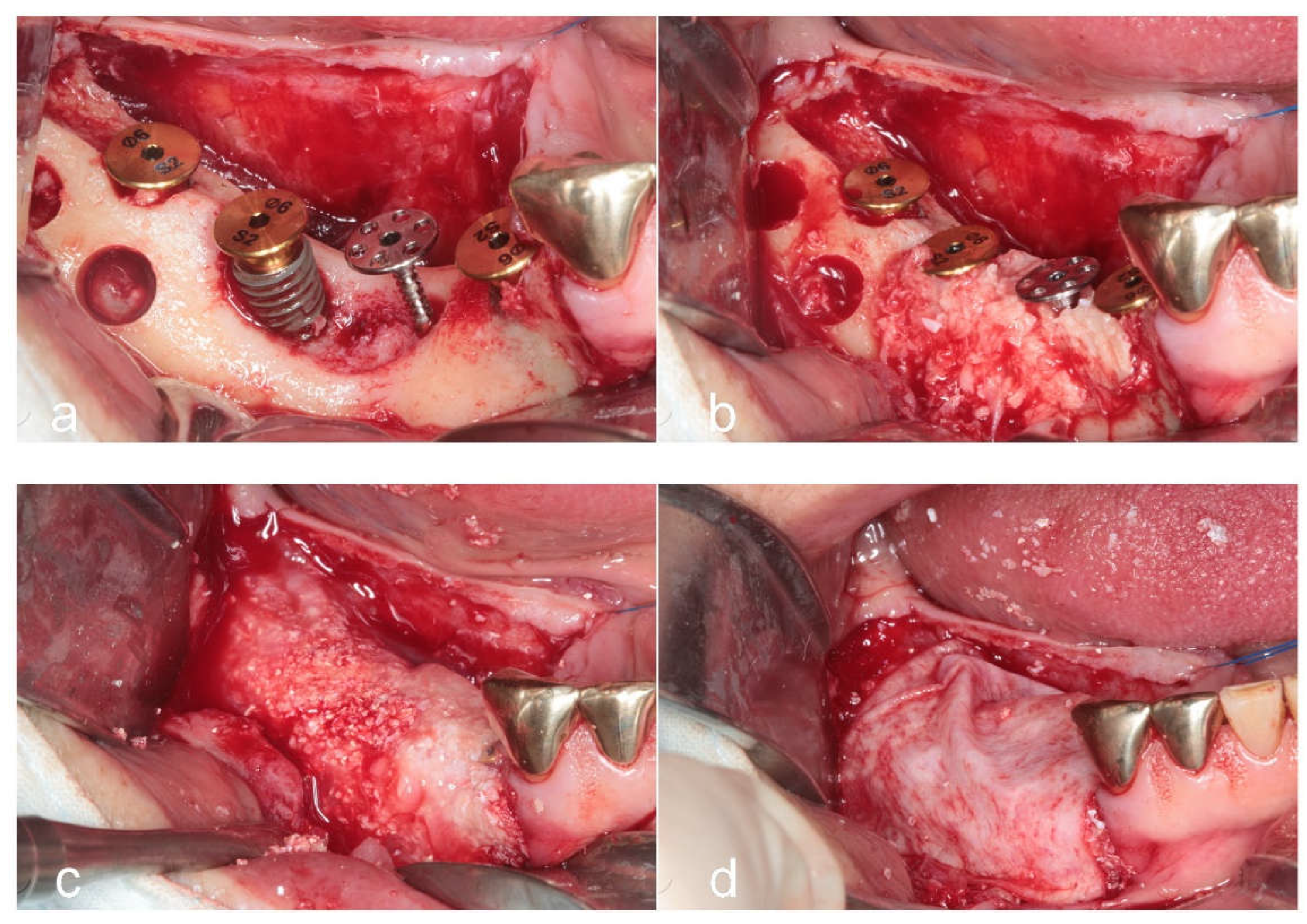
Figure 3.
Uncovering after 4 months of healing and placement of restoration. (a) Intraoral image after 4 months of healing on the day of implant uncovering. (b) Suture-less free gingival graft performed to provide attached keratinized gingiva following the delivery of a provisional restoration. (c) Intraoral image after the placement of the Zirconia-based final restoration. (d) Intraoral image after 2 years of function, demonstrating the stability of peri-implant tissues.
Figure 3.
Uncovering after 4 months of healing and placement of restoration. (a) Intraoral image after 4 months of healing on the day of implant uncovering. (b) Suture-less free gingival graft performed to provide attached keratinized gingiva following the delivery of a provisional restoration. (c) Intraoral image after the placement of the Zirconia-based final restoration. (d) Intraoral image after 2 years of function, demonstrating the stability of peri-implant tissues.
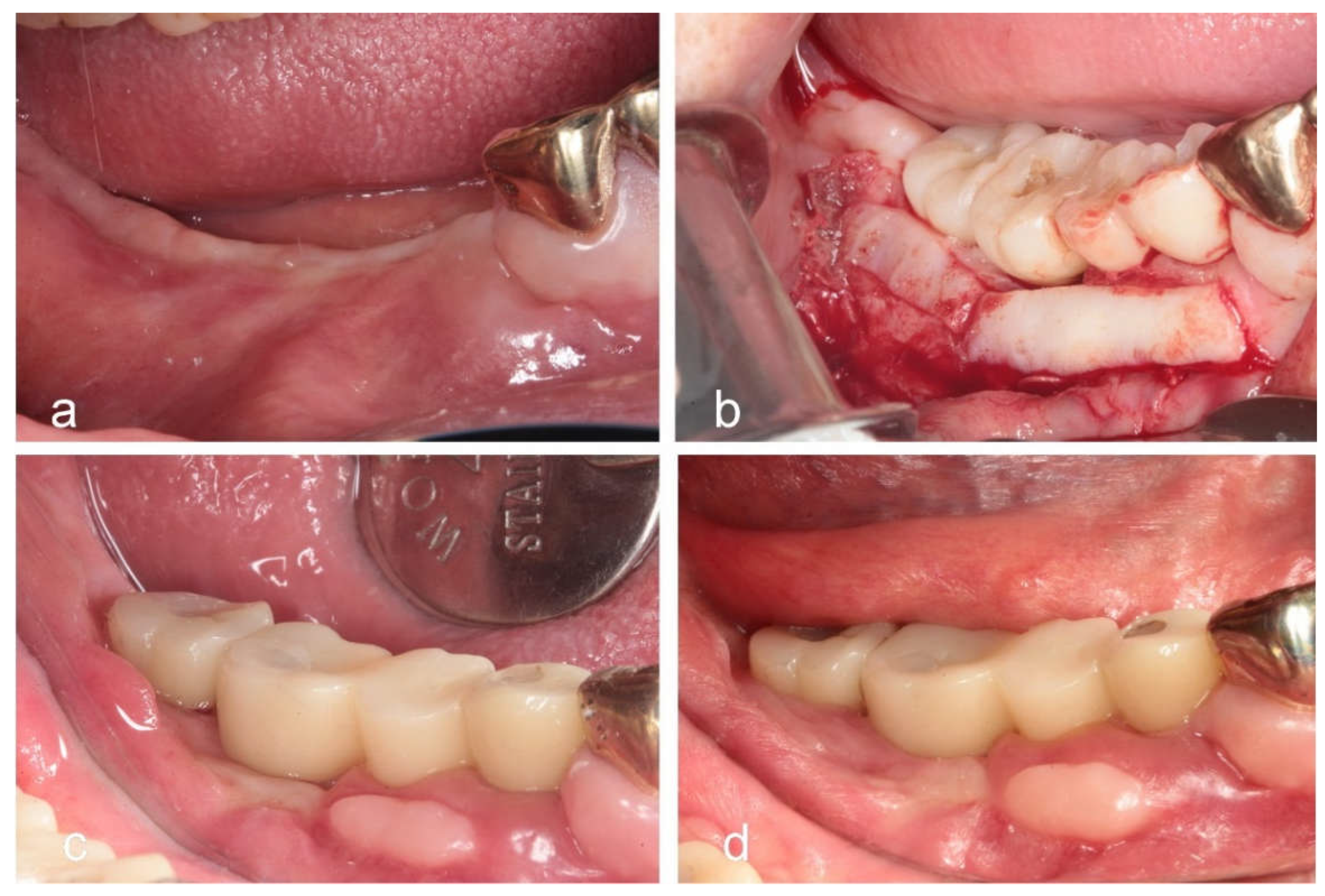
Figure 4.
Serial radiographs. (a) Postoperative radiograph taken immediately after surgery. (b) Radiograph taken 4 months postoperatively at the time of implant uncovering. (c) Baseline radiograph at the time of final prosthesis delivery. (d) Radiograph after 2 years of functional loading, showing the stability of the augmented ridge over the implant platform.
Figure 4.
Serial radiographs. (a) Postoperative radiograph taken immediately after surgery. (b) Radiograph taken 4 months postoperatively at the time of implant uncovering. (c) Baseline radiograph at the time of final prosthesis delivery. (d) Radiograph after 2 years of functional loading, showing the stability of the augmented ridge over the implant platform.
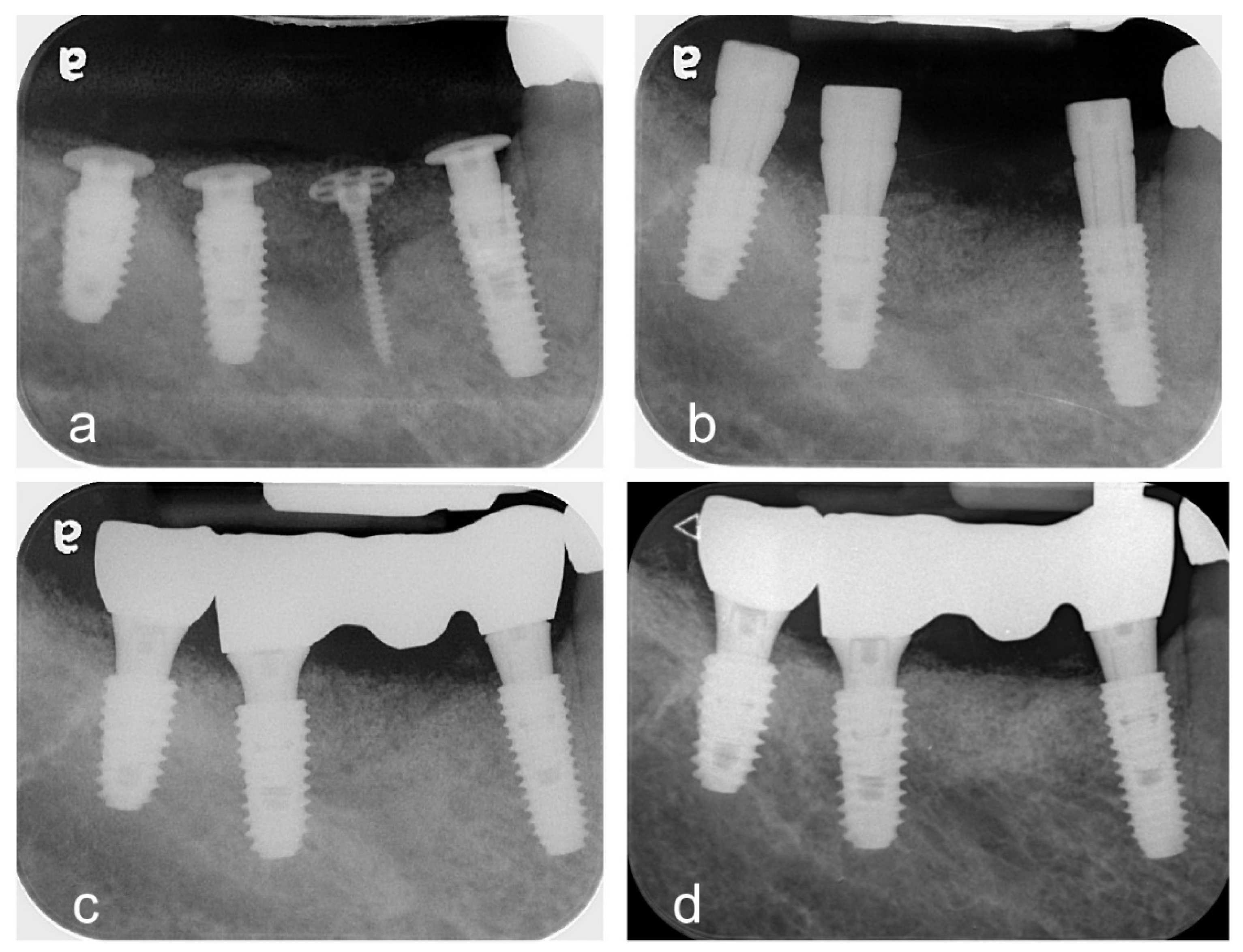
Figure 5.
Postoperative radiographic measurement of subject. (a) Reference line – A baseline parallel to the long axis of the adjacent teeth.(b) Measurement 1 line – Represents the total bone height, measured from the lowest point of the mandible to the top of the wide head tent-pole screw. (c) Measurement 2 line – Indicates the augmented bone height, measured from the top of the tent-pole screw to the graft junction where the native mandibular bone meets the grafted bone. (d) Original bone line – Represents the pre-augmentation bone height, measured from the lowest point of the mandible to the graft junction.
Figure 5.
Postoperative radiographic measurement of subject. (a) Reference line – A baseline parallel to the long axis of the adjacent teeth.(b) Measurement 1 line – Represents the total bone height, measured from the lowest point of the mandible to the top of the wide head tent-pole screw. (c) Measurement 2 line – Indicates the augmented bone height, measured from the top of the tent-pole screw to the graft junction where the native mandibular bone meets the grafted bone. (d) Original bone line – Represents the pre-augmentation bone height, measured from the lowest point of the mandible to the graft junction.
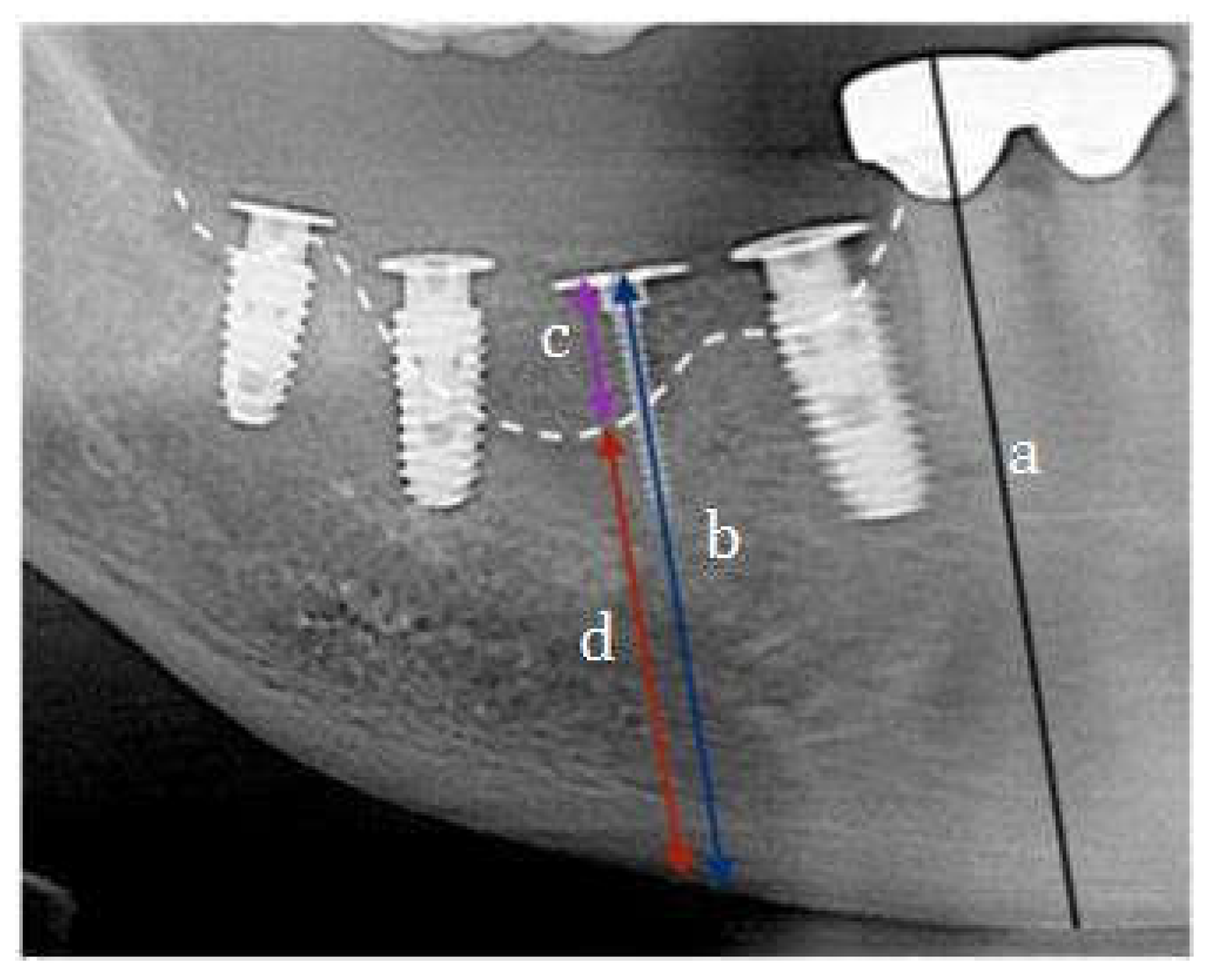

Table 1.
Radiographic assessment of post operative outcomes.
| Patient | Post-op height (mm) | Prosthetic Loading (mm, month) | Functional Loading (mm, month) | Bone Gain (mm) | Bone Resorption (mm) |
| 1 | 29.57 | 28.91(5m) | 27.87(11m) | 11.95 | 1.7 |
| 2 | 25.82 | 25.3(4m) | 24.1(8m) | 13.06 | 1.72 |
| 3 | 32.86 | 32.63(3m) | 32.43(8m) | 13.15 | 0.43 |
| 4 | 16.52 | 15.8(4m) | 15.68(16m) | 10.10 | 0.84 |
| 5 | 25.33 | 24.06(3m) | 23.68(14m) | 5.47 | 1.65 |
| 6 | 23.97 | 21.56(6m3w) | 21.06(18m) | 7.8 | 2.91 |
| 7 | 30.20 | 29.13(6m) | 29.1(10m) | 6.03 | 1.1 |
| 8 | 22.96 | 22.12(6m) | 21.64(20m) | 6.59 | 1.32 |
| 9 | 28.99 | 27.19(7m) | 26.65(13m) | 7.67 | 2.34 |
| 10 | 29.37 | 28.19(7m) | 28.13(20m) | 8.32 | 1.24 |
| 11 | 24.20 | 23.7(5m) | 22.9(8m) | 9.17 | 1.3 |
| 12 | 25.68 | 25.56(7m) | 25.4(16m) | 5.3 | 0.28 |
| 13 | 23.78 | 21.69(7m) | 21.19(19m) | 5.59 | 2.59 |
Table 2.
Measurement of Bone gain and Bone resorption.
 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



