
Submitted:
26 March 2025
Posted:
26 March 2025
You are already at the latest version
Abstract
Advancements in material science have made biopolymers a reliable solution in treating diseases for which there were previously no effective treatments. Intrauterine adhe-sions (IUAs) are the second leading cause of infertility among women of reproductive age. Despite their negative impacts, the available data reveal that there is currently no effective treatment. Thus, this work serves to provide an overview of the progress in the biomedical application of biopolymers focusing on the clinical management of IUAs. Hysteroscopic adhesiolysis remains the standard treatment for IUAs even though it is linked to recurrence and suboptimal reproductive outcomes. Equally, efforts to improve IUAs treatment by combining hysteroscopy with adjuvants like physical barriers have not resulted in better outcomes. Biopolymers like hyaluronic acid (HA) represent a ground-breaking shift in regenerative medicine and have been used as anti-adhesives in the treatment of IUAs. This is attributed to their excellent biocompatibility, biodegra-dability, low toxicity, and cell growth promotion ability. This review examines naturally occurring biopolymers, underscoring their biomedical applications, limitations such as rapid degradation, limited residence time and bioavailability and poor mechanical properties. Drawing from existing evidence and authors' standpoints, innovative ap-proaches harnessing the power of biopolymer engineering are suggested as future di-rections to overcome ongoing limitations.
Keywords:
biopolymers
; Intrauterine adhesions
; Asherman’s syndrome
; hyaluronic acid
; biomaterials
; chemical cross-linking
1. Introduction
The recent progress in medical technology, material science, and tissue engineering has opened new possibilities for treating some of the most debilitating diseases, including damage to or loss of tissues and organs. As a result, patients can now benefit from clinically active biopolymer-based materials, leading to tissue regeneration and the restoration of lost biological functions [1]. Researchers have shown that biopolymers may have invaluable roles in managing reproductive system disorders notably Intrauterine adhesions (IUAs). These materials can help protect the endometrial lining and improve reproductive health pre- and post-intrauterine surgeries owing to their inherent therapeutic potentials [2]. To achieve this, biopolymers are endowed with excellent physico-chemical and mechanical properties *such as molecular weight, viscoelasticity and flexibility, melting temperatures and gas transitions temperatures in addition to their propensity to accept modifications mainly via crosslinking or bioconjugations [1,3]. This latter is very important because it has led material scientists to manipulate biopolymers with the focus of improving their properties and widening their applications in various fields including tissue engineering and reproductive medicine. Biopolymers are a subtype of polymers sourced from living organisms such as plants and animals and are made of long chains of small repeating units called monomers [4]. These macromolecules have interesting biological properties, including biocompatibility, biodegradability, low toxicity, minimal immune response, strong cell growth promotion ability, and good cell adhesiveness [1,5,6,7]. Table 1 summarizes key properties of biomaterials currently applied in the field of reproductive medicine and tissue engineering. As a result, these distinct properties of biopolymers make them highly suitable for various biomedical applications, such as in regenerative and reproductive medicine, drug delivery, and immunotherapy [2,6,8].
IUAs are the second most common cause of infertility in women of reproductive age, and finding effective treatments for this condition continues to be a critical challenge in the field of reproductive medicine [9]. This debilitating condition not only impairs female reproductive potential by provoking pathophysiological changes in the intrauterine cavity, but also has significant physical, psycho-social, and economic effects [10,11]. Discomforts among affected women are often associated with infrequent or painful menses, recurrent miscarriages, or infertility [12]. Also, in some instances, severe adhesions in the uterus can prevent embryo implantation or disrupt fetal development [13]. Despite the growing prevalence of IUAs, there are currently no effective preventative or therapeutic options available. Additionally, although various management strategies have been proposed, each faces significant limitations that prevent their widespread translational application.
IUAs are acquired endometrial conditions characterized by fibrosis and the formation of scar tissue bands (also called adhesions) in the wall lining the uterine cavity [14]. They result from trauma to, and inflammation of the endometrium precisely during different types of surgical operations or due to microbial infections such as tuberculosis (TB) and schistosomiasis [2,3,4,5,6,7,8,9,10,11,12,13,15]. Although the terms IUAs and Asherman's syndrome are frequently used interchangeably, in their study, Deans & Abbott, (2010) clarified that IUAs are the leading causes of Asherman's syndrome. Figure 1 illustrates the main causes of IUAs and their current treatment approaches. The negative effects of IUAs become more severe when they affect women of childbearing age, where the condition can lead to complete infertility along with physical and mental health problems [12].
To date, hysteroscopic adhesiolysis is regarded as the gold standard for treating IUAs and has been effective in removing adhesions followed by endometrial regeneration [16]. Hysteroscopy is a painless, minimally invasive procedure for diagnosis and treatment of IUAs [17]. After a physician identifies adhesions through diagnostic hysteroscopy, hysteroscopic adhesiolysis is performed to remove them, alleviate related symptoms while ensuring restoration of the anatomical integrity of the uterus via endometrial regeneration. Prior to this, the physician determines the disease prognosis to guide decision-making on a comprehensive approach that includes preoperative, intraoperative, and postoperative strategies, as well as procedures designed to prevent adhesion recurrence and ensure optimal fertility outcomes [18].
However, it has been reported that hysteroscopic adhesiolysis is associated with a high recurrence rate [13,17]. Several studies reported that the recurrence rate of IUAs after hysteroscopic adhesiolysis ranges from 20% to 62.5%, and this is often associated with poor reproductive outcomes [13,17,19,20,21]. Poor reproductive outcomes are largely due to complications such as spontaneous abortions, preterm delivery, intrauterine growth restriction, placenta accreta, and, in severe cases, uterine rupture [19]. There are various medical approaches available to manage the consequences of IUAs or uterine cancers treated through hysteroscopy. These include uterus transplantation and surrogacy. However, ethical concerns, technical and safety issues, as well as the risk of life-threatening tissue rejection continue to be substantial barriers [22,23].
Recent management of IUAs typically includes combining hysteroscopic adhesiolysis with physical barriers, hormone therapy, and stem cell therapy [14,24]. However, the translational use of these approaches faces several challenges. For instance, physical barriers may not be patient-specific to match diverse shapes and sizes of uteruses, and metal-based intrauterine devices (IUDs) were associated with microbial infections [15,25]. Also, although hormone therapy with estrogen has been used to manage IUAs, its low solubility results in limited drug bioavailability and thus, reduced therapeutic effect [26]. Chi et al., (2018) revealed that while estrogen alone can prevent the formation of adhesions, it has limited effectiveness in improving reproductive outcomes. However, in the same study, when estrogen was combined with aspirin, it promoted better endometrial regeneration and reduced the recurrence of adhesions. Despite these benefits, prolonged use of oral estrogen can lead to various negative side effects, such as an increased risk of breast cancer, especially in individuals with higher levels of estrogen receptor alpha (ERα) [27]. Likewise, ex-tended use of estrogen and progesterone may cause hormonal imbalances, contributing to issues such as breast and cervical cancers, thrombosis, neurological disorders, and further infertility [28].
With the mounting advances in material science and bioengineering, biopolymers can be modified to improve their capacities and applicability in clinical management of IUAs [2,29,30]. This has the potential to play a significant role in the discovery of innovative treatments and health technologies for a range of evolving and complex medical conditions, including IUAs. Thus, by advancing our understanding and ability to leverage material science and bioengineering in targeting such conditions, it could pave the way for more effective and tailored therapies, improving patient outcomes and offering novel solutions for other conditions that have long been threatening the human lives worldwide.
Biopolymers such as hyaluronic acid (HA)-based hydrogels were reported to be effective in promoting endometrial regeneration and improving reproductive outcomes after hysteroscopy. However, HA’s therapeutic effect is limited by its quick degradation by endogenous hyaluronidases, which reduce its residence time at the treatment site, bioavailability and, therefore, its therapeutic potential [7]. Effort was made to improve the properties of this biopolymer such as chemical modification by crosslinking [31,32]. However, this could not completely resolve these issues, given the nature of HA and its extensive biomedical applications. Also, a recent study by Buckley et al., (2024) reported that chemical modifications of HA produced a 3D-printed thiolated HA hydrogel, which showed a tailorable degradation profile, a necessary attribute for any medical device. Thus, it is essential to build on existing evidence and expand our horizons to envision innovative health technologies that harness the power of biopolymers like HA to effectively prevent and treat IUAs. These advancements can enhance overall female reproductive health and well-being, reduce the economic burdens related to IUAs, while contributing to the sustainable development goals.
Equally important, there is a need for continued research and development to modify clinically important bio-materials particularly HA to enhance stability and biocompatibility, lower cytotoxicity, and better suit the current and future medical needs [7,13,33]. Furthermore, attention should be directed not only towards chemical modifications but also the development of polymer bio-composites and the use of different dosage forms, such as solid dispersions and implants [34], while carefully considering high diversity in sizes and shapes of the uteruses. These strategies could potentially improve the residence time at the target site, enhance bioavailability, and increase the therapeutic efficacy of the ad-ministered HA biopolymer.
This review aims to discuss the progress in the biomedical application of biopolymers focusing on the status quo and future outlook in managing IUAs. It also examines current treatment strategies, emphasizing the existing gaps, and suggesting innovative approaches that utilize cutting-edge technologies in material science to effectively manage IUAs and improve female reproductive health and quality of life. Despite the promising results from the current therapeutic approaches for IUAs, such as hysteroscopic adhesiolysis combined with antiadhesive biopolymers like crosslinked HA hydrogels, significant challenges persist, including high recurrence rates and limited reproductive outcomes. As a result, based on existing literature and the authors' viewpoints, innovative strategies leveraging biopolymer engineering and regenerative medicine are proposed as future directives to address the current gaps in managing IUAs. To pave the path toward this endeavor, we also examined a range of common biomaterials, discussing their physico-chemical and mechanical characteristics, the latest biomedical applications, and potential limitations, with an emphasis on their roles in tissue engineering and reproductive medicine, particularly in the management of IUAs.
2. Combination Therapy for IUAs (Hysteroscopy & Biomaterials)
The clinical management of IUAs using hysteroscopic adhesiolysis has been associated with high rates of adhesion recurrence. To address this, several studies showed that combining hysteroscopy with biopolymers such as cross-linked HA gel can help prevent adhesions recurrence, maintain endometrial integrity and enhance reproductive outcomes [11,13,35,36]. During their study, Mao et al., (2020) reported that among 306 participants (202 in the treatment group and 104 in the control group), those treated with hysteroscopy plus cross-linked HA gel showed greater endometrial thickness (8 ± 1.4 mm vs. 7.5 ± 0.6 mm), higher implantation (18% vs. 10%) and pregnancy rates (26% vs. 15%). Similarly, a randomized controlled trial (RCT) was conducted to compare HA gel and no treatment in managing IUAs. It was shown that among 82 women in both groups, the HA gel group had a lower rate of IUAs following hysteroscopy (4% versus 11%), and a higher pregnancy rate (61% versus 40%) [36].
A meta-analysis evaluating the effectiveness of HA gel as an adjunct treatment for IUAs in women with a history of miscarriages found that HA gel reduced adhesion scores and significantly enhanced reproductive outcomes in those with moderate to severe IUAs. However, no effect of this therapy was observed in women with mild condition of the disease [37]. Likewise, an RCT was carried out to assess the effectiveness of newly cross-linked hyaluronan (NCH) alone or in combination with an IUD in managing IUAs in 72 women. The results indicated that both treatments improved endometrial thickness (7.5mm for the combined treatment versus 6.5mm for the IUD alone). Also, among the 72 women who later underwent in vitro fertilization, the pregnancy rates were 27% for the IUD alone, 40% for the IUD plus NCH, and 36% for NCH alone [38].
Although the use of auto-cross linked HA (ACP) gel was reported to be associated with no side effects such as allergy, pain and fever [36], the findings of most current clinical trials reveal that there is still a need for further modification of this biopolymer to improve its physio-chemical and biological properties and ensure its routine clinical use in the management of IUAs. These modifications should aim to enhance the stability of HA, prevent its breakdown by hyaluronidases, improve its adhesiveness to cells, and discover a dosage form which can ensure a sustained release of HA within the uterus. By examining different types of biopolymers, with an emphasis on their synthesis, properties, and established biomedical applications, we can establish a solid foundation for further research aimed at developing a biopolymer composite that overcomes the current limitations not only of HA but also other clinically relevant biopolymers.
3. Biopolymers and Potential Biomedical Applications
Although there are several treatment options available for IUAs, issues such as unsuccessful endometrial re-generation, poor reproductive outcomes, and high recurrence rates remain unaddressed medical needs [21]. Nevertheless, bioengineers and material scientists can leverage advanced technologies and innovative approaches to restore fertility and enhance the quality of life among affected patients. These strategies focus on developing, replacing, or regenerating reproductive cells, tissues, and organs using biocompatible and biodegradable materials [39]. The implementation of these innovative strategies offers promising solutions that surpass the complexity and high costs as-sociated with traditional interventions like surgeries and organ transplantation [40].
A wide range of biopolymers with biomedical applications have been well characterised but the current research focuses on biopolymers of natural origin such as HA, alginate, chitosan, gelatin, fibrin, polylactic acid (PLA), polyglycolic acid (PGA), carboxymethylcellulose (CMC) [41]. Table 4 illustrates some examples of naturally-occurring biopolymers, their properties, biomedical applications and limitations. Although biopolymers such as PLA and PGA are commonly used [1] and offer improved biocompatibility and biodegradability, they tend to have higher toxicity and immunogenicity since they differ from the body's natural components [41]. Thus, biopolymers such as HA, gelatin, fibrin, alginate and chitosan are preferred because they replicate essential features of the natural extracellular matrix (ECM), encouraging cellular behaviors like adhesion, migration, and differentiation [42].
Biopolymers particularly in form of hydrogels, implants, membrane scaffolds and films have been used as a primary strategy to prevent direct contact between damaged layers of the endometrium in addition to facilitating endometrial regeneration and improve reproductive outcome among women with IUAs [13,36,43]. Another key point to consider is that biopolymers can be utilised individually, in combination with other materials, or as drug delivery systems (DDSs) to treat IUAs [44]. Also, these materials have shown the potential to revolutionize healthcare by enabling personalized treatments that could enhance therapeutic outcomes, reduce side effects, and further shape the future of healthcare [45].
Among a number of biopolymers, and their biomedical applications reported in the literature [8,45], chitosan, alginate and gelatin-based hydrogels have been extensively used in biomedicine notably in eye care due to high oxygen permeability and lack of irritations leading to inflammatory responses [46]. In reproductive biology, these biomaterials are primarily applied in areas such as follicle culture, artificial ovaries, tissue engineering and regeneration, as well as contraception. Despite the increasing and promising applications of biomaterials, some of them pose potential toxicity risks and involve complex manufacturing processes, necessitating ongoing research and stringent regulation [45]. Furthermore, although natural biomaterials hold significant potential for biomedical applications, many face challenges related to suboptimal mechanical properties, such as gelation time, deformability, and elasticity [47]. To overcome these limitations, chemically modifying natural biomaterials or combining them with synthetic alternatives may offer viable and sustainable solutions [48].
4. Examples of Naturally-occurring Biomaterials and their Applications
4.1. Hyaluronic Acid
HA also known as Hyaluronan is an anionic and non-sulphated naturally occurring biopolymer that falls within the category of mucopolysaccharides, also known as glycosaminoglycans [40,41]. Its chemical structure comprises a long linear chain of two disaccharide repeating units namely d-glucuronic acid and N-acetylglucosamine linked by alternating β-(1–4) and β-(1–3) glycosidic bonds [41]. Figure 2 represents the chemical structure of HA. This biopolymer is found in all vertebrate connective tissues and throughout the human body, especially in synovial fluid, the umbilical cord, urine, and the ECM. It plays a crucial role in cellular processes like cell proliferation, migration, and differentiation [4,49], in addition to exhibiting anti-inflammatory and immunosuppressive properties [25]. In vertebrates, three genes namely Has1, Has2, and Has3 are responsible for HA synthesis, whereas in bacteria, HA synthesis is enabled by the expression of HasA, HasB, and HasC genes [50,51]. Although Streptococcus species naturally produce large quantities of HA, this source is unsuitable for humans and other vertebrates due to high endotoxin levels of these bacteria. Hence, Lactobacillus lactis has been biotechnologically engineered as a safer alternative for HA production [4].
HA maintains its optimal stability at neutral pH and 40°C but deteriorates rapidly when exposed to acidic or alkaline environments [52]. The molecular weights (MWs) of HA vary depending on its source. For example, in the human body, the MWs of HA range from 103 to 107 Da in both serum and vitreous humor of the eye, respectively. It has also been reported that different MWs of HA are directly linked to its distinct physiological functions [32,53]. Typically, short and medium HA molecules exhibit immunostimulant, proangiogenic, and antiapoptotic properties, while longer polymers are associated with immunosuppressive and antiangiogenic effects [54]. Thus, this may partly explain the reason why this biopolymer has a diverse range of physiological roles in the body.
The physico-chemical and biological properties of HA, including viscoelasticity, hydrophilicity, biocompatibility, biodegradability, non-toxicity, and non-immunogenicity, make HA-based preparations suitable for a range of biomedical applications [49,53]. Structurally, HA helps maintain the gel-like nature and stability of the ECM by interacting with various ECM proteoglycans, such as aggrecans [55]. HA's exceptional water retention ability allows it to absorb significant amounts of water, holding up to 1,000 times its volume in water. HA is essential for cell-to-cell communication, one of the vital processes for maintaining human body homeostasis. To achieve this, HA has the well-known and characterized membrane glycoprotein receptor called ‘CD44’ to which it attaches, forms a pericellular coat around cells, and interacts with cell membrane proteins to regulate key physiological processes, such as cell adhesion, migration, and proliferation [32,56].
HA plays a vital role in managing IUAs and addressing the rising global issue of female infertility. Numerous recent clinical trials have shown that HA gel supports endometrial regeneration after intrauterine surgeries, encourages angiogenesis and neovascularization and most significantly, enhances reproductive outcomes [11,35,36,38,57,58]. Additionally, as previously noted, Kim et al. (2019) demonstrated in a murine model that HA effectively reduced fibrosis, promoted endometrial regeneration, and improved reproductive outcomes. This was achieved by enhancing the ex-pression of implantation biomarkers, including Desmin, CD44, PECAM, and IGF-1.
The application of crosslinked HA hydrogel for the prevention of IUAs after a hysteroscopic myomectomy was investigated. The research findings showed the reduction in the incidence and severity of IUAs, which discovered the potential of synergistic effects of hysteroscopic myomectomy and HA hydrogels among women undergoing hysteroscopy [11]. Several HA-based implants, such as Hyalobarrier Gel Endo®, Sepracoat® and Intercoat®, have been developed to prevent IUAs. While a Belgian consensus on adhesion prevention noted their potential benefits, their effectiveness is minimal in terms of adhesions prevention, reproductive outcome, and these products were not eligible for reimbursement [59]. The shortcomings of commonly used barrier methods in preventing IUAs may be linked to prior research emphasizing uterine anatomical restoration over endometrial stem cell functionality. HA-based membranes device loaded with estrogen and growth factors have been recommended to promote cell regeneration. However, as noted earlier prolonged estrogen use is not advisable due to reported adverse effects and may compromise the device's effectiveness [60].
Notwithstanding the increasing biomedical applications of HA in developing treatments for various medical conditions, it is evident that the use of HA has been linked to certain drawbacks. The limited HA mechanical strength was found to interfere with some of its biomedical applications. Once in non-crosslinked form, this biopolymer has a life span of less than 3 days since it can only last between 24-48-hours in the body [54]. This is due to HA being rapidly degraded by hyaluronidase enzymes [7,54] which potentially limits its residence time at the action site. It has been reported that due to its simple structure, the main chain of HA can be chemically modified primarily at the hydroxyl and carboxyl ends. Crosslinking and bioconjugation methods can nowadays allow for the precise tuning of various HA properties, such as mechanical, rheological, and swelling behaviors. Additionally, these modifications help protect the polymer from enzymatic degradation and increase the biomaterial's residence time at the therapeutic site [3].
Similarly, Buckley et al., (2024) revealed that chemical modification of HA by thiolation and methacrylation in-creased HA receptor interaction while improving mechanical strength required for peripheral nerve regeneration. Additionally, HA Chemical modification leads to tailored biodegradation, increased adhesiveness, and allows cross-linking and bioconjugation [56]. Likewise, acetylated hyaluronic acid-divinyl sulfone hydrogels have been identified as an innovative approach to enhance the physical properties of HA while increasing its retention time and therapeutic effect [7]. Limited cell adhesion and inability to undergo UV-induced photo-crosslinking hinder HA's therapeutic effects and biodegradability. To address this, modifying HA through thiolation and methacrylation was proven to enable the creation of a new pho-to-crosslinkable polymer, offering enhanced physicochemical properties, improved biocompatibility, and the ability to tailor its biodegradation rate [56]. Thus, chemical modification of HA cannot only serve to improve its physico-chemical properties and current biomedical applications, rather, it can pave the path for bioengineers and material scientists to discover its novel therapeutic applications. Equally important is the creation of new HA formulations and delivery methods to improve their stability, bioavailability and therapeutic effectiveness in preventing and treating reproductive disorders, especially female IUAs.
4.2. Alginate
Alginate (ALG) is a polyanionic and water-soluble polysaccharide [61], the second most abundant natural polymer which is primarily extracted from brown seaweed species [62,63]. As illustrated in Figure 3, ALG is a polysaccharide made up of linear α-L-guluronic acid (G-blocks) and somewhat more branched β-D-mannuronic acid (M-blocks) copolymers. These blocks are connected by (1,4)-glycosidic bonds and can form gels when hydrated [63]. ALG's superior degradation profile makes it particularly well-suited for drug delivery applications. It has thickening, gel-forming, and stabilizing properties, and high-water retention capacity. ALG forms acid gels at low pH and these gels are stable at temperature ranging from 0-1000c [64]. As a result, it is commonly used as a therapeutic delivery system and an excipient in con-trolled-release drugs [64,65].
ALG is renowned for its exceptional properties including biocompatibility, biodegradability, mechanical properties, bioresorption ability, and low cost making it highly suitable for a wide range of biomedical applications [62,66]. Similar to most other natural polymers, to enhance its therapeutic efficacy and broaden its applications, ALG should be chemically modified or combined with other biomaterials to improve cellular compatibility, gelation properties, biodegradability, and mechanical strength [42]. Nevertheless, deformability of ALG for an is influenced by its structural composition. It was indicated that ALG with rich in M-blocks is more flexible and deformable than ALG with more G-blocks [63]. This implies that material scientists should choose M-blocks-rich ALG when seeking to modify this polymer for targeted biomedical applications. ALG’s chemical modification by crosslinking which occurred at 230°C improved their biodegradability in artificial urine. Using both barium and calcium ion crosslinkers, instead of calcium ions alone, resulted in a hydrogel with enhanced tensile strength, which in turn influenced the resorption rate and swelling properties, leading to more efficient degradation. Better degradation profile makes ALG better suited to its use in drug delivery [66].
The medical application of ALG in wounds, scars, and bone injury healing, cell regeneration, and scaffold for cell growth and in DDSs have been reported [45,63]. ALG has been proven effective for encapsulating isolated follicles in in vitro culture and for developing artificial ovaries. Moreover, ALG-based hydrogels have demonstrated their ability to replicate the natural microenvironment prior to ovary cryopreservation [67] highlighting their potential in addressing female infertility issue. However, this biomaterial showed enhanced therapeutic effects when used in combination with others. An IUD composed of ALG combined with Matrigel and poly (lactic-co-glycolic acid) (PLGA) exhibited improved properties, enhancing its effectiveness in the manufacture of artificial ovaries [46,62]. Also, a study on the development of a biodegradable artificial ovary showed that ALG-Matrigel matrix was able to facilitate ovarian cells proliferation and after ovarian cells grafting, the matrix degraded effectively while allowing angiogenesis and showing minimal inflammatory responses [46]. A porous scaffold composed of ALG, and gelatin was designed to address IUAs. Testing both in vitro using human hepatocarcinoma cell lines and in vivo in rats revealed that the scaffold demonstrated excellent compatibility and effectively promoted endometrial repair while preventing adhesions, respectively [68].
4.3. Chitosan
Chitosan, a natural cationic polysaccharide, is typically derived from the shells of crustaceans such as shrimp, crab and lobster. As illustrated in Figure 4, chitosan is a linear polysaccharide composed of glucosamine and N-acetylglucosamine units linked by β (1-4) glycosidic bonds. Its various forms arise primarily from differences in the degree of deacetylation and molecular weights, which range from 300 to 1000 kDa [69,70]. As a cationic biopolymer, chitosan can readily interact with anionic biological molecules like heparin and heparan sulphate, influencing the activity of various cytokines and growth factors crucial for tissue regeneration. In addition to being a biodegradable biopolymer, chitosan has a hydrophilic surface that confers it the capacity to promote cell adhesion and proliferation, and its degradation by-products are not toxic [71]. Chitosan is synthesized through either chemical or enzymatic processes. The chemical method, widely used for chitosan synthesis, involves an acetylation reaction where acetyl groups are removed from N-acetylglucosamine to generate D-glucosamine which increases chitosan solubility in water. This reaction must take place in a heterogeneous phase, using sodium or potassium hydroxide in an inert atmosphere to prevent de-polymerization. Alternatively, biosynthesis using chitinases offers a different acetylation route for chitosan production from chitin and is currently being utilized [72]. Chitosan contains reactive primary amines as well as primary and secondary hydroxyl groups, which provide flexibility for chemical modifications. These modifications can enhance its physicochemical and biological properties, making it suitable for a wide range of biomedical applications [71].
Chitosan has been recognized as a safe material for use in food, cosmetics, and medical devices in several countries, including Finland, the USA, Italy, and Japan [73]. Several studies assessing the safety of chitosan have shown that this biomaterial causes no side effects in the study subjects [74,75]. In addition to being considered a safe biomaterial for pharmaceutical and biomedical applications, chitosan is also recognized for its cost-effectiveness, biodegradability, biocompatibility, hydrophilicity, nontoxicity, high bioavailability, amenability to modifications, affinity to proteins and high films and gel forming capacity [4,76]. Thus, a variety of chitosan-based therapeutic biomaterials have been developed for diverse biomedical applications, such as treating cancer, immune disorders, microbial infections, hypertension, inflammatory conditions, coagulation disorders, high cholesterol, diabetes, drug/gene delivery systems, wound dressing, tissue engineering and cell encapsulation [76,77]. Medical chitosan has been shown to mitigate the sequelae of abdominal, fallopian tube, and other hysteroscopic surgeries, including preventing adhesions formation and recurrence. It achieves this by promoting fibrocyte growth while preventing fibrosis [25,78]. In addition, this biopolymer uniquely supports local hemostasis and prevents bacterial growth. With its lubricant properties, along with its physical barrier function, biodegradability, and resorbability. It has been suggested that combining medical chitosan with estrogen therapy could work synergistically to enhance endometrial regeneration and prevent adhesion recurrence after hysteroscopic adhesiolysis [25].
Similar to other natural polymers, chitosan by itself offers limited health benefits. This is mainly due to its limited mechanical strength [79]. However, combining it with other biopolymers such as ALG, HA, collagen, PEG, chitosan to name a few can enhance its characteristics, expanding its therapeutic applications. For example, blending chitosan with ALG creates a polyelectrolyte complex scaffold with markedly improved modulus, strength, and stability. Additionally, its excellent water retention and swelling properties boost porosity and surface area, which are vital for cell adhesion and tissue regeneration [69]. Correspondingly, chitosan demonstrated enhanced therapeutic effects when used in combi-nation with HA. Leveraging their common antimicrobial, antioxidant, and anti-inflammatory properties, researchers have combined chitosan and HA to enhance skin care. This synergistic approach has led to improved health outcomes, particularly in tissue regeneration and wound healing [70]. Equally noteworthy, Singh et al. (2020) employed fused filament fabrication-based 3D printing technology to combine chitosan and PLA, aiming to overcome the limitations of chitosan’s weak mechanical properties and PLA’s natural hydrophobicity and lack of essential functional groups for biological activity. The resulting PLA-chitosan composites were shown to be both mechanically and biologically effective, making them more promising for clinical applications.
4.4. Collagen
Collagen is the most prevalent structural protein in mammals and aquatic organisms, playing a vital role in the formation of the ECM and basement membrane structures [42]. It is widely known for its outstanding structural strength and versatility. It plays a vital role in maintaining the durability, flexibility, and connectivity of various parts of the body [80]. Collagen is characterized by its triple helix structure, where tightly coiled amino acid chains provide exceptional tensile strength [81]. Figure 5 represents the structural formula of collagen. This polymeric biomaterial has a wide range of biomedical applications, primarily due to its inherent characteristics, including excellent biocompatibility, bioresorbability, non-toxicity, non-antigenicity, adhesiveness, and strong tissue integration ability. Furthermore, its high flexibility, tensile strength, and mechanical properties make it adaptable to modifications that enhance its biomedical performance [61].
A variety of hydrogels including collagen-based hydrogels have shown encouraging results in tissue engineering and reproductive medicine. Collagen can act as a signaling molecule, impacting cell behavior, tissue development, and wound healing [81]. ECM-derived hydrogels are highly recommended due to preclinical trial findings demonstrating their ability to closely replicate the natural microenvironment, exhibit excellent biocompatibility, and deliver superior clinical outcomes [67]. The literature reveals numerous studies investigating the biomedical applications of collagen in the field of reproductive medicine, particularly using animal models. Collagen has been reported to successfully deliver stem cells and growth factors in murine models of IUAs, premature ovarian failure, and vaginal atrophy [46,67,82]. This biomaterial has additional uses in various areas of biomedicine, including dental surgery, drug delivery, and cardiology. For instance, collagen in dental implants aids in the integration of the implants and supports the regeneration of periodontal tissue. It also enables controlled drug release within implants, promoting localized and extended drug delivery. Moreover, collagen-based materials are used in the creation of vascular grafts and heart valve prostheses [80].
Although collagen possesses excellent properties that make it reliable for various biomedical applications, it is not advised to use it on its own. This is because collagen has limited mechanical stability and requires a long cross-linking time due to its slow gelation process [61]. Type I collagen self-assembles into fibrous hydrogels at 37°C. collagen-based polymeric composites have shown significant potential in tissue engineering, especially for regenerating skin and cartilage [61]. For example, the application of collagen and HA polymeric composites were reported to result in improved cell proliferation, migration and cell functions. Additionally, in a mouse model, with an effort to address the issue of skin graft with limited duration at the graft site, a mixture of epidermal keratocytes, dermal fibroblasts mixed with collagen showed promising results in wound healing and regenerating the skin [83,84].
4.5. Gelatin
Gelatin is a biomaterial derived from the partial breakdown of collagen. Figure 6 illustrates the structural formula of gelatin. It is extracted from the bones, skin, and connective tissues of animals such as cattle, horses, pigs, chickens, and fish [40]. It is readily sourced from natural resources, offers great stability, and can modify drug release patterns. This late implies that gelatin can control drug release dynamics, effectively delaying the release of the drug until it reaches the intended target sites [81]. This property allows for more precise and controlled delivery, improving the therapeutic efficacy and minimizing potential side effects by preventing premature drug release. Gelatin is recognized for its notable qualities, including excellent gelation, biocompatibility, and biodegradability. However, it also has some limitations, such as low thermal stability and weak mechanical strength [85]. These drawbacks might have hindered its translational uses since it often necessitates modifications and blending with other materials. Chemical modification of gelatin by blending it with other biopolymers has been identified as a promising approach to improve its mechanical properties.
Gelatin has known potential applications in various areas including drug delivery, scaffolds for tissue regeneration, and wound dressings [80]. In tissue engineering, gelatin-based scaffolds serve as a supportive 3D structure that promotes cell adhesion, growth, and tissue regeneration. However, to counteract its inherent limitations, enhance its properties, and optimize its uses, gelatin has been combined with other materials through chemical modifications. For example, incorporating polyvinyl alcohol into gelatin increased the gelling temperature of the composites from 41°C to 80°C. Additionally, the tensile strength and elongation at break improved from 2.89 MPa to 3.40 MPa and from 342% to 367%, respectively [86]. By utilizing electrospinning and the self-assembly process, highly porous, 3D nanofiber scaffolds were created via cross-linking PCL and gelatin with genipin cross-linker. The resulting polymer scaffold resembled the nanofibrous structure of endogenous ECM and demonstrated strong mechanical strength, biocompatibility, as well as promoting the proliferation and adhesion of dermal fibroblast cells [87].
Embryonic stem cells from early blastocysts are able for self-renewal in undifferentiated state and differentiating into all types of adult cells. Yet, sustaining them long-term has been challenging its clinical applications. To overcome this, research has demonstrated that gelatin-based, structurally dynamic hydrogels, which mimic the natural dynamics of the ECM, can support clonal expansion and enhance cell viability more effectively than covalently crosslinked gelatin hydrogels with similar stiffness and biodegradability [88].
4.6. Polylactic Acid
Polylactic acid (PLA), a white powder at room temperature, is an aliphatic, environmental-friendly biopolymer with various biomedical applications, largely due to its thermoplasticity, excellent processability, mechanical strength, bio-degradability, bioresorbability and biocompatibility properties [89]. This biomaterial is well recognized for being cost-effective, dimensionally stable, and more rigid [90]. PLA is produced through polymerization of lactic acid (LA), a naturally occurring organic acid produced through sugar fermentation process. Figure 7 illustrates the structural formula of PLA. LA is recognized as a chiral molecule and exists in two enantiomeric forms: L- and D-LA [91]. Consequently, PLA can exist as pure poly-L-LA (PLLA), pure poly-D-LA (PDLA) and a mixed form of poly-D, L- LA (PDLLA) [1,89]. PLA with over 90% PLLA content tends to be crystalline. As the amount of PLLA decreases, both the melting and glass transition temperatures of PLA also decrease. These temperature values are vital for predicting the polymer's physical, chemical, and biological properties. Whereas PLA glass transition temperature ranges between 45 and 65°C, its melting point varies between 150–162°C [90,92]. The melting point of semi-crystalline PLLA ranges from 170-180°C but when blended with PDLA, the melting temperature increases to 220-230°C, enhancing its thermostability [89]. Additionally, being semi-permeable to oxygen and water makes this biopolymer more prone to biodegradation compared to other biomedical polymers [93].
Regarding the PLA degradation profile, PLA is mainly degraded through hydrolysis mechanism though enzyme-catalysed degradation is also known [93]. It was reported that this biopolymer has relatively shorter degradation time (2-6months) [95]. The biodegradability and mechanical properties of PLA are affected by the monomer's chirality. Studies show that the D and D/L forms of PLA degrade faster than the L form, which has higher crystallinity [93,96]. To tackle the problem of shorter PLA degradation time, it has been suggested that increasing the surface area-to-volume ratio or the porosity of the polymer can improve its degradation rate [97]. While this thermoplastic polymer degrades in the body, the rapid degradation of PLA in vivo has been shown to produce LA concentrations that can trigger inflammatory responses, which may hinder cell proliferation and differentiation [98]. Therefore, controlling the degradation rate from weeks to years by adjusting the initial molecular mass, crystallinity, and copolymer ratios should be considered to resolve this issue [42]. Another factor to consider is that the temperature and pH of the surrounding environment directly impact PLA degradation. PLA degrades quickly at room temperature (around 25°C), while its degradation is slower at lower pH compared to physiological pH. This is because, at a pH above 4, lactic acid exists in its dissociated form, which accelerates hydrolysis [99]. Table 2 summarizes key mechanical properties of PLA, PLLA, and PDLLA. Although several methods for synthesizing PLA such as direct polycondensation, azeotropic dehydration condensation or ring opening polymerization are known, none of them is straightforward or easy to implement [92]. Figure 8 illustrates three pathways through which PLA can be synthesized. These methods require the use of catalysts under carefully controlled conditions of temperature, pressure, and pH, along with extended polymerization times, making it a highly energy demanding process [1].
Beyond its key role as a building block of PLA, lactic acid is also known to affect cellular functions in the body. Being a small, and nonpolar molecule, it can easily cross cell membrane lipid bilayer and converted into glucose inside the cell where it acts as an energy source. Due to its outstanding properties notably mechanical and biological properties as well as thermoplastic potential, PLA is the mostly used synthetic biomaterial with the mounting biomedical applications notably once it undergoes some chemical modifications [1]. This biomaterial is widely used in the production of DDSs, bioresorbable implants and sutures, as well as scaffold membranes for tissue engineering. It plays a key role in aiding the recovery of biological functions in damaged cells, tissues, and organs within the body [89].
In a study aimed at designing a prototype degradable medical device to prevent the formation and recurrence of IUAs, a biodegradable film made from the PLA-(b)-PEG-(b)-PLA copolymer was created and compared with an HA gel sample. The results showed that the three-block copolymer swelled within the uterus and was fully degraded within 12 days. Furthermore, unlike the HA hydrogel, it effectively prevented adhesion formation and promoted endometrial repair [100].
The extensive clinical use of PLA-based products is partly due to its approval by the US Food and Drug Administration (FDA) for direct contact with biological fluids [89,92]. PLA has been utilized in the production of various medical devices and implants. Given this, researchers have emphasized the importance of considering factors such as PLA's degradation profile, cytotoxicity, tensile strength, and elastic modulus. However, PLA's slow degradation rate, hydro-phobic nature, high permeability to gases and vapors through its films, and low impact toughness are recognized as major limitations [92,101] which dictate continuous research for the improvement of PLA properties. Chemical modifications of PLA, through either copolymerization, grafting, crosslinking, UV-irradiation, plasma treatment, or physical methods like heating and blending with various modifiers, have been shown to potentially alleviate PLA weaknesses [101]. For in-stance, while assessing the effect of blending PLA with polyacrylates in a 1:1 weight ratio, the analysis performed dis-closed that the blends were highly crosslinked, rigid, and heterogeneous, with some exhibiting semicrystalline properties. Additionally, it was found that the PLA-polyacrylate blends displayed greater photostability compared to pure PLA [101].
4.7. Polyglycolic Acid
Polyglycolic acid (PGA) is a biodegradable and biocompatible polymer known for its exceptional rigidity, strength, tensile modulus, abrasion and solvent resistance as well as excellent gas barrier capabilities [80,102,103]. In comparison with the previously discussed synthetic biomaterials, PGA has extraordinary mechanical properties. This polymer has tensile strength of 109 MPa together with tensile modulus of 7.0 GPa. Table 3 illustrates the main physical and mechanical properties of PGA. These properties make PGA well-suited for various fields notably in biomedical applications, although its high production cost limits its widespread use [104]. As shown in Figure 9, while this biomaterial has one of the simplest structures, its physicochemical and mechanical properties enable it to deliver exceptional performances [102].
Despite its increasingly promising applications, PGA encounters common limitations such as low thermal stability, reduced toughness, and rapid hydrolysis and biodegradation, which have hypothetically restricted its wider use [104,105]. For example, limited thermal stability complicates PGA synthesis, and unlike the widely applied polylactides, even though the first PGA synthesis via melt polycondensation was performed in 1938, this biomaterial wasn't commercially produced by Kureha chemical through ring-opening polymerization of glycolide until 2008 [103]. The synthesis of PGA through ring-opening polymerization uses a tin octoate catalyst, and since tin octoate-catalysed reaction is rapid, it helps prevent potential thermal decomposition of PGA [105]. Nevertheless, a key challenge for PGA manufacturers remains the efficient and lucrative production of the glycolide starting monomers. As a result, global production of PGA is still limited, and its applications are confined to very few areas, including biomedical applications [102].
Efforts have been made to overcome the limitations of PGA, such as its limited thermostability. In this regard, PGA has been modified through copolymerization, physical blending, or multilayer lamination, resulting in a PGA-PLA co-polymer that combines the enhanced mechanical strength of PLA and the improved thermostability of PGA. Although this copolymer offers promising benefits, the process is still expensive, and as a result, the material has not seen widespread use in biomedical applications [104]. Another study focused on copolymerizing glycolic acid with a small amount of ε-caprolactone through melt polycondensation to create random poly (glycolic acid-co-ε-caprolactone) copolymers. These copolymers exhibited enhanced thermal stability, preventing significant thermal degradation during the poly-condensation and processing stages. This marked the development of the first PGA-based material with a wide processing temperature range, high molecular weight, and enhanced performance through melt polycondensation [102].
PGA is known to have significant role in tissue engineering, where it can serve as a structural framework that supports cell growth and tissue regeneration while gradually degrading to allow for the integration of new tissues. This material is commonly used in DDSs, especially in the production of implantable devices, as PGA-based microspheres or nanoparticles can offer controlled and sustained drug release at the target site [80]. The use of PGA as an animal-free biomaterial scaffold for 3D endometrial cell culture was compared with the widely used natural fibrin-agarose. After culturing primary endometrial cells on both fibrin-agarose and PGA scaffolds, the results showed that both materials were capable of replicating the natural human endometrium, promoting the growth and proliferation of endometrial cells on each scaffold [106]. Although this should serve as a foundation for PGA applications in regenerative medicine, especially for endometrial repair or regeneration, research and development of 3D scaffold materials still encounter challenges. These include high production costs and a lack of consensus on the ideal porosity and pore size for various materials needed to effectively repair defects [106].
The clinical benefit of PGA in nerve cell regeneration was explored. It was found that PGA conduits could promote the regeneration of the nerve cells which was followed by its effective biodegradation. Nonetheless, further research and innovations are needed to enhance the stability and biocompatibility of PGA, particularly due to its rapid degradation and the reported inflammatory responses triggered when PGA and PGA-based materials are used [107]. This will be crucial for achieving optimal clinical application of these products while ensuring patient safety and health outcomes.
It is evident that the real-world application of PGA and PGA-based products is still a long way off. Therefore, research and development should prioritize discovering new, innovative, and cost-effective sources of glycolide monomers, which are the key raw materials for PGA synthesis. By doing so, the production costs of PGA and PGA-based materials could be significantly reduced, making these materials more accessible and commercially viable for a broader range of applications. This could equally involve revolutionizing government policies regarding bioplastics, exploring alternative feedstocks such as industrial waste, improving synthesis processes, or developing sustainable manufacturing techniques that not only lower costs but also enhance the overall sustainability of PGA production process [104].
4.8. Carboxymethylcellulose
Carboxymethylcellulose (CMC) is a polymer composite derived from cellulose natural polymer that is gaining in-creasing attention for its applications in various fields, particularly in tissue engineering and drug delivery [108,109]. CMC is an ionic and water-soluble biopolymer currently considered as the most common additive particularly since it is less expensive and easy applied in various applications. In addition, it is synthesized from cellulose, the most abundant polymer in the world via alkalization and etherification reactions [109,110]. Regarding the chemical structure of CMC, the repeating units in this polymer are linked by β-1,4-glycosidic linkages. The key structural difference between CMC and cellulose is the presence of anionic carboxymethyl groups in CMC, which replace the hydrogen atoms of certain hydroxyl groups found in cellulose [109]. CMC exhibits varying degrees of substitution and molecular weights, which are key factors that determine its properties and applications. It has been reported that an increase in the degree of substitution is directly proportional to an improvement in the compatibility of CMC with other materials [111].
CMC offers strong mechanical properties and resistance to degradation in vivo, along with reactive surfaces that enable protein binding through controlled surface chemistry. It also demonstrates biocompatibility, supporting both granulation tissue and bone formation. Nevertheless, Rahman et al., (2021) reported that the mechanical strength, viscosity, and rheological properties limit the range of applications for synthesized CMC products. As a result, they recommended effective characterization of CMC products is a crucial step in determining its potential applications. Recognized as a promising biomaterial in biomedical applications, CMC is particularly valued for its ability to undergo chemical modifications, which enhance its physical, chemical, and mechanical properties to suit specific and tailored applications [108]. With an aim to enhance the applicability of CMC while address their issues related to poor degradation profile, this polymer was combined with other biomaterials to produce biopolymer composites or scaffolds with desired properties [108]. It has been reported that CMC is valuable in various industries, including biomedical, pharmaceutical, food, and oil sectors. Moreover, its effectiveness in these fields is significantly influenced by factors like purity, degree of polymerization (DP), degree of substitution (DS), and uniformity, which impact the performance of the resulting products, such as solubility, particle size, viscosity, and rheological properties.
For instance, composite gels and films made from CMC and polyethylene oxide (PEO) have been developed for use in separating healing tissues. These materials have been shown to reduce postsurgical adhesions in animal models of adhesion formation [112] and the high porosity and excellent biocompatibility of these scaffolds supports cell adhesion and migration, while also promoting tissue regeneration [108]. Two clinical studies evaluating the efficacy of CMC-PEO copolymers in managing IUAs have shown promising results. In the first study, 110 IUAs eligible for surgical treatment were randomly assigned to two groups. Group 1 underwent hysteroscopy followed by application of Intercoat (CMC-PEO), while group 2 received hysteroscopy alone. One month later, office hysteroscopy revealed a significant reduction in both the incidence (6% vs. 22%; p < 0.05) and severity (33% vs. 92%) of IUAs in group 1 compared to group 2 [113]. Similarly, women undergoing hysteroscopy for RPOC were randomly assigned to two groups. In the first group, 26 women received Intercoat, while the second group of 26 women received no treatment. The results showed that moderate to severe adhesions developed in 1 woman (4%) in the treatment group, compared to 3 women (14%) in the control group. After a 20-month follow-up, 7 women (27%) in the treatment group became pregnant, compared to 3 women (14%) in the control group [114]. More clinical studies are required to validate the safety and efficacy of CMC and CMC-based products with therapeutic potentials in the field of tissue engineering and particularly reproductive medicine.

Table 4.
Common natural and synthetic biomaterials, biomedical applications and limitations. Tm = melting temperature.
Table 4.
Common natural and synthetic biomaterials, biomedical applications and limitations. Tm = melting temperature.
| Biomaterial | Nature | Source | Tm (°C) | Applications/Advantages | Disadvantages | Reference |
|---|---|---|---|---|---|---|
| HA | Polysaccharide-based | Mainly in extracellular matrices of vertebrates and humans | N/A | Reproductive & regenerative medicine Tissue engineering Drug delivery Endometrial regeneration Abundant in ECM High biocompatibility and fluidity |
Rapid degradation Limited mechanical strength Immunosuppressive and antiangiogenic (long chains) |
[52,54] |
| ALG | Polysaccharide-based | Seaweed and bacterial origin | 99 | FDA approved and Ph. Eur adopted Stable in the form of hydrogel Facilitate cell encapsulation and 3D printing Artificial ovaries making DDSs High level of deformability Relatively less expensive |
Limited degradation and renal clearance Deficiency in the property of cell adhesion Limited ability to promote cell migration and cell adhesion Cannot be used alone |
[64,65] |
| Chitosan | Polysaccharide-based | Crustacean shells | 102.5 | Wound dressings Hemostatic properties Implants Tissue engineering DDSs |
Limited mechanical strength Poor water resistance, and low thermal stability |
[70,79] |
| Collagen | Protein-based | ECM component in mammals and aquatic organisms | 71-96 | Cell adhesion and regeneration Amenability to modifications Stem cells and DDSs |
Low mechanical stability Cannot be used alone |
[47,115] |
| Gelatin | Protein-based | Extracted from bones, skin, and connective tissues of animals | 40 | Excellent gelation Flexible for modifications Promote cell proliferation and adhesion Low cost |
Low thermal stability and weak mechanical strength | [86,116] |
| PLA | Polymer of lactic acid | Extracted from sugar cane, corn, cassava and maize or Synthesized via direct polycondensation, azeotropic condensation or ring opening polymerization |
170-180 | FDA-approved Used as Implants Good biodegradability Excellent mechanical properties and chemical stability Less expensive The most commonly used poly-lactone |
Complex synthesis Rapid degradation Can elicit inflammatory responses from acidic by-products High permeability of gases or vapors via PLA films |
[1,43] |
| PGA | Polymer of glycolic acid | Synthesized via melt polycondensation or ring opening polymerization | 220 | FDA-approved Excellent mechanical strength, solvent resistance as well as excellent gas barrier capabilities |
Glycolic acid accumulation can elicit inflammation and lead to impaired cell proliferation and differentiation High production cost Reduced toughness, and rapid hydrolysis and biodegradation Thermal instability |
[42,104,105] |
| CMC | Polysaccharide-based | Synthesized from plants via alkalization and etherification reactions | 274 | Biocompatibility Common additive Less expensive Derivative of cellulose, the most abundant polymer Strong mechanical properties |
Poor degradation profile Limited viscosity, and poor rheological properties | [108,109,110] |
5. Marketed Biomaterial Products for Cell/Tissue Regeneration
Several biomaterial-based products have been developed and approved for use in preventing or treating various medical conditions and complications resulting from surgical procedures [41,42,62,117]. These products are commonly used as anti-adhesives to prevent the formation of fibrous tissues due to abnormal wound healing process while con-tributing to effective tissue regeneration [94]. Traditional physical barriers were found to be insufficient in alleviating symptoms associated with adhesions, as well as in controlling inflammation and promoting cell regeneration. To address these challenges, biomaterial-based products were developed to be used in combination with surgical procedures. The current biomaterial-based products include drugs such as anti-inflammatory, anticoagulant, and fibrinolytic agents, along with antibacterial agents or growth factors meant to support tissue regeneration. However, further research is recommended to evaluate the efficacy and safety of these emerging products in both animal and human subjects [94].
The effectiveness of the administered drug partly depends on its dosage form. Most of the currently available biomaterial-based products used as physical barriers to prevent adhesions in various tissues come in the form of hydrogels, biofilms, electro-spun fibrous membranes, and microspheres. While each dosage form offers certain ad-vantages, they also present some challenges such as difficult administration [13,118], rapid degradation (in the case of electro-spun fibrous membranes, hydrogels and biofilms) [7], toxicity (for hydrogels crosslinked with chemical agents), and instability of incorporated proteins and peptides (in microspheres) [94]. Therefore, exploring novel dosage forms, administration methods, and crosslinking strategies for clinically relevant biomaterials could help overcome these issues and improve their clinical effectiveness while widening their biomedical applications. For example, this could be through development of solid dispersion implants that can ensure sustained release of the biopolymer to ensure its longer residence and higher bioavailability at the action site. Table 5 below summarizes the key factors affecting release kinetics from biopolymer-based DDSs. While developing an implantable device especially from biopolymer composites, it is important to know that the stability of the drug, its bioavailability and therapeutic effect at the action site are all influenced by the properties of drug itself, biopolymer matrix (carrier) as well as the surrounding environment [119].
Biomaterial-based products available on the market include those designed to manage adhesions in the pericardial, tendon, abdominal, and pelvic regions. For instance, Womed leaf is an IUA barrier film developed by the Institut des Biomolecules Max Mousseron in France, to prevent the formation of IUAs post intrauterine procedures. A preclinical study conducted on rats to assess the safety and efficacy of Womed Leaf showed that the implant did not enhance endometrial thickness or reproductive outcomes when comparing the treatment group to the control group. However, it was confirmed that Womed Leaf did not induce irritations and efficiently showed potential to prevent IUAs formation [121]. Moreover, this minimally invasive device is inserted into the uterus through the cervix, and is naturally expelled after use. In a clinical study aimed at evaluating the efficacy and safety of Womed Leaf, the device successfully prevented the formation of IUAs, and no cases of uterine perforation or cervical trauma were reported, confirming the implant's efficacy and safety. However, the clinical data suggests that the tested device, measuring 4.5 cm in length, is insufficient to cover the entire uterine cavity due to significant variations in the sizes and shapes of women's uteruses [122].
Seprafilm®, a solid physical barrier composed of both HA and CMC, has been approved by the FDA and CE for use in pericardial, peritoneal, and tendon adhesions. Additionally, Interceed®, a solid barrier made from oxidized cellulose, Adept®, a liquid barrier containing 4% Icodextrin, and SurgiWrap®, a PLA-based solid gel, have all been FDA and CE-approved and are currently used for treating peritoneal adhesions [94]. Finally, Hyalobarrier®, developed by Anika therapeutics, INC. in Italy, a crosslinked HA gel approved by CE is known as a gel barrier used in the management of IUAs. A study comparing the efficacy of 4DryField and Hyalobarrier® for preventing the recurrence of IUA following hysteroscopic adhesiolysis in patients with Asherman’s syndrome found that both biomaterials were effective in pre-venting the recurrence of adhesions and enhancing reproductive outcomes, particularly in terms of restoring menstruation [94,123]. However, based on the available clinical evidence, it has been recommended that additional research is needed to optimize adhesion management. This could involve advancing the development of multifunctional bio-materials by incorporating multiple drugs into the biopolymer complex to address various adhesion-related issues. Additionally, selecting the appropriate biomaterials and conducting safety studies on their by-products could enhance adhesion management [92]. Ultimately, any developed health technology should prioritize ensuring the treatment is affordable and free from adverse effects for patients.
A number of clinical studies were conducted to evaluate the efficacy of these biomaterial-based products in preventing post-operative adhesions. A randomized controlled trial was conducted to assess the efficacy of SprayGel, a sprayable adhesion barrier for laparoscopic and open pelvic and abdominal surgeries. After 10 weeks, results showed that 27.8 percent of patients in the treatment group (5 out of 18) were free from adhesions, compared to 7.7 percent in the control group (1 out of 13) [124]. In a similar manner, a meta-analysis of 11 clinical studies on barrier agents for preventing adhesions after gynecological surgery found that the Interceed® barrier is safe and significantly reduces the occurrence of new adhesions and the reformation of adhesions, compared to no treatment in laparoscopy [125]. In the same study, a clinical trial demonstrated that Seprafilm® resulted in better prevention of adhesion and adhesion recurrence in the treatment group compared to the control group [125]. Additional clinical studies are needed to prove the safety and efficacy of both the existing and newly developed biomaterials, in order to optimize their translational ap-plications, particularly in the field of reproductive medicine and the treatment of IUAs.
6. Conclusions and Future Outlook
6.1. Conclusions
Despite the significant impact of IUAs such as reduced female fertility and considerable physical and psychological distress, which continue to be a growing global concern and an unmet medical need in reproductive medicine, no effective treatment strategy is currently available. Hysteroscopic adhesiolysis, the standard treatment for IUAs, has been associated with the growing recurrence rates and poor reproductive outcomes. To improve IUAs management, innovative approaches like combining hysteroscopy with various physical barriers, hormone therapy, and cell therapy have been studied. Nevertheless, these methods have shown a number of limitations, including adhesions recurrence, high costs, and insufficient restoration of endometrium and menstrual cycle which potentially results into circumscribed reproductive outcomes.
Among the wide range of biopolymers, the most frequently used in biomedical applications particularly in medical device industry include HA, ALG, chitosan, and gelatin [41], as well as PLA, and PGA [1]. While increasing research supports the potential of HA in treating IUAs, further improvements are needed in its physical, chemical, and mechanical properties to boost its therapeutic effectiveness and meet the rising medical demands notably in tissue engineering and reproductive medicine. Similarly, despite their remarkable properties that make them suitable for various biomedical applications, each of the existing biopolymers discussed has inherent downsides often related to their inherent characteristics.
The combination of hysteroscopy and biopolymer like crosslinked HA hydrogels has demonstrated significant potential in effectively managing reproductive system disorders, including IUAs. This is primarily due to HA's physico-chemical properties, excellent biocompatibility, biodegradability, and its ability to promote cell migration, proliferation, and regeneration [11]. However, issues such as limited strength and rapid degradation by hyaluronidases have resulted in a reduced residence time and therapeutic effect of crosslinked HA in preventing and treating IUAs after hysteroscopic adhesiolysis [7]. Considering these factors, further chemical modifications, blending HA with another biopolymer to create a well-defined biopolymer composite, and the selection of appropriate dosage forms can improve HA physicochemical, mechanical, and biological properties essential for treating IUAs, while also expanding its potential biomedical applications.
6.2. Future Outlook
Tissue engineering is a rapidly growing field within regenerative medicine. This innovative medical technology has become a promising alternative for treating damaged or lost organs. It utilizes the patient's own cells, cultured on a polymer scaffold, to support the regeneration of tissue from natural cells [1]. Significant advancements in bioengineering have resulted in the discovery of innovative biomaterials with improved physico-chemical, mechanical, and biological properties for biomedical applications. However, the pace of development of these advanced materials and health technologies has not been matched by neither their clinical adoption, nor by the increasing complexity of medical conditions [67]. Additionally, there are still reported limitations in clinically relevant biomaterials, highlighting the need for ongoing research in this field.
Recent reports suggest that due to insufficient biomaterial research, particularly in reproductive medicine, and the complex requirements and dynamic function of the uterus, a suitable biopolymer scaffold or effective anti-adhesive for treating IUAs has yet to be developed [94]. For instance, increased efforts have been made to manage IUAs, such as using hysteroscopy in combination with physical barriers like biopolymers as antiadhesives. However, recent research shows that this approach is still associated with high recurrence rates and does not result in effective endometrial repair or improved reproductive outcomes, which remains the primary goal of treatment. Another significant challenge is the high cost associated with using physical barriers in the management of IUAs. While human amnion, cell/hormone therapy, growth factors, and umbilical-cord-derived cells have demonstrated promising results in managing IUAs, they are not cost-effective, demand highly skilled professionals, and require long-term post-administration surveillance [94]. Hence, researchers and manufacturers should focus on creating affordable biomaterials that can efficiently prevent or treat IUAs, ensuring that all patients, regardless of their socio-economic background, can access the treatment.
As mentioned earlier, although there are some limitations to HA hydrogels, such as rapid degradation by hyaluronidases, which reduces their residence time and bioavailability at the treatment site, increasing evidence from clinical trials suggests that combining hysteroscopic adhesiolysis with crosslinked HA hydrogels is a promising strategy for managing IUAs [35,36,38,57]. The importance of HA in biomedical applications, including tissue engineering, drug delivery, and reproductive medicine, has been emphasized in the literature [52]. However, Buckley et al. (2022) and Trucilo (2024) recommended that further research is necessary to fully explore the intracellular behaviors, biocompatibility, and regulatory considerations of this biomaterial to enhance its clinical effectiveness. This is crucial because, although chemical crosslinking can improve the resistance of HA hydrogels to enzymatic degradation [126], it may also lead to increased hardness, which could cause a foreign body sensation and trigger inflammation or other adverse effects [45,127].
Thus, future studies should focus on finding the right balance in the degree of modification to preserve HA's biocompatibility and biodegradability [7] along with identifying and characterizing the suitable carrier matrix that can be combined with HA to enhance its stability and sustained release. The choice of the carrier matrix should take into account both the device's end user specific requirements and the conditions of the site where it will be applied, such as the physiological environment of the uterus. Therefore, besides essential biological properties like biocompatibility, bio-degradability, low toxicity, and non-immunogenicity, the carrier matrix must also possess excellent physical and mechanical properties, including tensile strength, formability, elastic modulus, hardness, and phase-transition characteristics [128]. Building on the points discussed above, we suggest that chemically modifying HA through cross-linking and combining it with a well-defined, highly processable, and biocompatible biopolymer as a carrier matrix could address the current limitations of HA, enhance its therapeutic effects, and help bridge the existing gaps in managing IUAs. For instance, this could be accomplished by developing a minimally invasive HA-coated solid dispersion device that can be implanted in the uterus to provide sustained release of the HA biomaterial. The implantable device must be designed to accommodate the wide variation in uterine sizes and shapes, as well as the specific characteristics and therapeutic outcomes of the implant. This approach could help prevent IUAs, promote the restoration of the endometrium after different types of damage, and enhance reproductive outcomes in women with IUAs.
Author Contributions
Conceptualization, P.N and C.B; investigation, P.N.; resources, C.B.; writing—original draft preparation, P.N.; writing—review and editing, D.M.C. and C.B; supervision, D.M.C and C.B.; project administration, D.M.C, I.M and C.B.; funding acquisition, C.B. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Data Availability Statement
No new data was generated in the writing of this review.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- M. Savioli Lopes, A. L. Jardini, and R. Maciel Filho, “Poly (lactic acid) production for tissue engineering applications,” Procedia Eng., vol. 42, no. August, pp. 1402–1413, 2012. [CrossRef]
- J. Wang et al., “Application of Bioactive Hydrogels for Functional Treatment of Intrauterine Adhesion,” Front. Bioeng. Biotechnol., vol. 9, no. September, pp. 1–16, 2021. [CrossRef]
- C. Buckley, E. J. Murphy, T. R. Montgomery, and I. Major, “Hyaluronic Acid: A Review of the Drug Delivery Capabilities of This Naturally Occurring Polysaccharide,” Polymers (Basel)., vol. 14, no. 17, 2022. [CrossRef]
- E. J. Murphy et al., “Polysaccharides—Naturally Occurring Immune Modulators,” Polymers (Basel)., vol. 15, no. 10, 2023. [CrossRef]
- S. S. Lee et al., “Self-healing and adhesive artificial tissue implant for voice recovery,” ACS Appl. Bio Mater., vol. 1, no. 4, pp. 1134–1146, 2018. [CrossRef]
- S. Pina, J. M. Oliveira, and R. L. Reis, “Natural-based nanocomposites for bone tissue engineering and regenerative medicine: A review,” Adv. Mater., vol. 27, no. 7, pp. 1143–1169, 2015. [CrossRef]
- S. J. Gwak, Y. Bin Lee, E. J. Lee, K. H. Park, S. W. Kang, and K. M. Huh, “The use of acetylation to improve the performance of hyaluronic acid-based dermal filler,” Korean J. Chem. Eng., vol. 40, no. 8, pp. 1963–1969, 2023. [CrossRef]
- S. S. Lee, X. Du, I. Kim, and S. J. Ferguson, “Scaffolds for bone-tissue engineering,” Matter, vol. 5, no. 9, pp. 2722–2759, 2022. [CrossRef]
- L. Feng et al., “Engineering self-healing adhesive hydrogels with antioxidant properties for intrauterine adhesion prevention,” Bioact. Mater., vol. 27, no. March, pp. 82–97, 2023. [CrossRef]
- L. Schmerold et al., “A cost-effectiveness analysis of intrauterine spacers used to prevent the formation of intrauterine adhesions following endometrial cavity surgery,” J. Med. Econ., vol. 27, no. 1, pp. 170–183, 2024. [CrossRef]
- C. Y. Huang et al., “Crosslinked hyaluronic acid gels for the prevention of intrauterine adhesions after a hysteroscopic myomectomy in women with submucosal myomas: A prospective, randomized, controlled trial,” Life, vol. 10, no. 5, 2020. [CrossRef]
- P. H. Wang, S. T. Yang, W. H. Chang, C. H. Liu, H. H. Liu, and W. L. Lee, “Intrauterine adhesion,” Taiwan. J. Obstet. Gynecol., vol. 63, no. 3, pp. 312–319, 2024. [CrossRef]
- L. Kou, X. Jiang, S. Xiao, Y. Z. Zhao, Q. Yao, and R. Chen, “Therapeutic options and drug delivery strategies for the prevention of intrauterine adhesions,” J. Control. Release, vol. 318, no. December 2019, pp. 25–37, 2020. [CrossRef]
- X. W. Huang et al., “A prospective randomized controlled trial comparing two different treatments of intrauterine adhesions,” Reprod. Biomed. Online, vol. 40, no. 6, pp. 835–841, 2020. [CrossRef]
- J. Cen et al., “Research progress of stem cell therapy for endometrial injury,” Mater. Today Bio, vol. 16, no. August, p. 100389, 2022. [CrossRef]
- A. B. Hooker, F. J. Mansvelder, R. G. Elbers, and Z. Frijmersum, “Reproductive outcomes in women with mild intrauterine adhesions; a systematic review and meta-analysis,” J. Matern. Neonatal Med., vol. 35, no. 25, pp. 6933–6941, 2022. [CrossRef]
- Y. Chen, L. Liu, Y. Luo, M. Chen, Y. Huan, and R. Fang, “Prevalence and Impact of Chronic Endometritis in Patients With Intrauterine Adhesions: A Prospective Cohort Study,” J. Minim. Invasive Gynecol., vol. 24, no. 1, pp. 74–79, 2017. [CrossRef]
- F. Di Guardo and M. Palumbo, “Asherman syndrome and insufficient endometrial thickness: A hypothesis of integrated approach to restore the endometrium,” Med. Hypotheses, vol. 134, no. November 2019, pp. 2019–2020, 2020. [CrossRef]
- D. Yu, Y. M. Wong, Y. Cheong, E. Xia, and T. C. Li, “Asherman syndrome-one century later,” Fertil. Steril., vol. 89, no. 4, pp. 759–779, 2008. [CrossRef]
- M. M. F. Hanstede, E. Van Der Meij, L. Goedemans, and M. H. Emanuel, “Results of centralized Asherman surgery, 2003-2013,” Fertil. Steril., vol. 104, no. 6, pp. 1561-1568.e1, 2015. [CrossRef]
- J. Bosteels et al., “Anti-adhesion therapy following operative hysteroscopy for treatment of female subfertility,” Cochrane Database Syst. Rev., vol. 2017, no. 11, 2017. [CrossRef]
- H. Chen et al., “Collagen-based materials in reproductive medicine and engineered reproductive tissues,” J. Leather Sci. Eng., vol. 4, no. 1, 2022. [CrossRef]
- S. W. Kim, Y. Y. Kim, H. Kim, and S. Y. Ku, “Recent Advancements in Engineered Biomaterials for the Regeneration of Female Reproductive Organs,” Reprod. Sci., vol. 28, no. 6, pp. 1612–1625, 2021. [CrossRef]
- G. Tabeeva et al., “The Therapeutic Potential of Multipotent Mesenchymal Stromal Cell—Derived Extracellular Vesicles in Endometrial Regeneration,” Int. J. Mol. Sci., vol. 24, no. 11, 2023. [CrossRef]
- J. Ma et al., “Recent trends in therapeutic strategies for repairing endometrial tissue in intrauterine adhesion,” Biomater. Res., vol. 25, no. 1, pp. 1–25, 2021. [CrossRef]
- A. Z. Liu, H. G. Zhao, Y. Gao, M. Liu, and B. Z. Guo, “Effectiveness of estrogen treatment before transcervical resection of adhesions on moderate and severe uterine adhesion patients,” Gynecol. Endocrinol., vol. 32, no. 9, pp. 737–740, 2016. [CrossRef]
- Y. Chi et al., “Transdermal estrogen gel and oral aspirin combination therapy improves fertility prognosis via the promotion of endometrial receptivity in moderate to severe intrauterine adhesion,” Mol. Med. Rep., vol. 17, no. 5, pp. 6337–6344, 2018. [CrossRef]
- A. Shukla, R. Jamwal, and K. Bala, “Adverse effect of combined oral contraceptive pills,” Asian J. Pharm. Clin. Res., vol. 10, no. 1, pp. 17–21, 2017. [CrossRef]
- W. L. Lee, C. H. Liu, M. Cheng, W. H. Chang, W. M. Liu, and P. H. Wang, “Focus on the primary prevention of intrauterine adhesions: Current concept and vision,” Int. J. Mol. Sci., vol. 22, no. 10, 2021. [CrossRef]
- Y. Y. Kim et al., “Synergistic regenerative effects of functionalized endometrial stromal cells with hyaluronic acid hydrogel in a murine model of uterine damage,” Acta Biomater., vol. 89, pp. 139–151, 2019. [CrossRef]
- Z. Luo, Y. Wang, Y. Xu, J. Wang, and Y. Yu, “Modification and crosslinking strategies for hyaluronic acid-based hydrogel biomaterials,” Smart Med., vol. 2, no. 4, pp. 1–18, 2023. [CrossRef]
- C. Buckley, T. R. Montgomery, T. Szank, and I. Major, “Hyaluronic acid hybrid formulations optimised for 3D printing of nerve conduits and the delivery of the novel neurotrophic-like compound tyrosol to enhance peripheral nerve regeneration via Schwann cell proliferation,” Int. J. Pharm., vol. 661, no. July, p. 124477, 2024. [CrossRef]
- J. Tang, J. Chen, J. Guo, Q. Wei, and H. Fan, “Construction and evaluation of fibrillar composite hydrogel of collagen/konjac glucomannan for potential biomedical applications,” Regen. Biomater., vol. 5, no. 4, pp. 239–250, 2018. [CrossRef]
- J. Holländer et al., “Three-Dimensional Printed PCL-Based Implantable Prototypes of Medical Devices for Controlled Drug Delivery,” J. Pharm. Sci., vol. 105, no. 9, pp. 2665–2676, 2016. [CrossRef]
- X. Mao et al., “Cross-linked hyaluronan gel to improve pregnancy rate of women patients with moderate to severe intrauterine adhesion treated with IVF: a randomized controlled trial,” Arch. Gynecol. Obstet., vol. 301, no. 1, pp. 199–205, 2020. [CrossRef]
- H. Chen et al., “Efficacy and safety of auto-cross-linked hyaluronic gel to prevent intrauterine adhesion after hysteroscopic electrosurgical resection: a multi-center randomized controlled trial,” Ann. Transl. Med., vol. 10, no. 22, pp. 1217–1217, 2022. [CrossRef]
- Z. Fei, X. Xin, H. Fei, and C. Yuechong, “Meta-analysis of the use of hyaluronic acid gel to prevent intrauterine adhesions after miscarriage,” Eur. J. Obstet. Gynecol. Reprod. Biol., vol. 244, pp. 1–4, 2020. [CrossRef]
- E. G. Pabuçcu, E. Kovanci, Ö. Şahin, E. Arslanoğlu, Y. Yıldız, and R. Pabuçcu, “New crosslinked hyaluronan gel, intrauterine device, or both for the prevention of intrauterine adhesions,” J. Soc. Laparoendosc. Surg., vol. 23, no. 1, 2019. [CrossRef]
- E. C. R. Leonel et al., “New Solutions for Old Problems: How Reproductive Tissue Engineering Has Been Revolutionizing Reproductive Medicine,” Ann. Biomed. Eng., vol. 51, no. 10, pp. 2143–2171, 2023. [CrossRef]
- A. Tamadon, K. H. Park, Y. Y. Kim, B. C. Kang, and S. Y. Ku, “Efficient biomaterials for tissue engineering of female reproductive organs,” Tissue Eng. Regen. Med., vol. 13, no. 5, pp. 447–454, 2016. [CrossRef]
- M. Wu et al., “Biomaterials and advanced technologies for the evaluation and treatment of ovarian aging,” J. Nanobiotechnology, vol. 20, no. 1, pp. 1–41, 2022. [CrossRef]
- G. Peng, H. Liu, and Y. Fan, “Biomaterial Scaffolds for Reproductive Tissue Engineering,” Ann. Biomed. Eng., vol. 45, no. 7, pp. 1592–1607, 2017. [CrossRef]
- E. Hoveizi and T. Mohammadi, “Differentiation of endometrial stem cells into insulin-producing cells using signaling molecules and zinc oxide nanoparticles, and three-dimensional culture on nanofibrous scaffolds,” J. Mater. Sci. Mater. Med., vol. 30, no. 9, pp. 1–11, 2019. [CrossRef]
- G. Cai et al., “Recent Developments in Biomaterial-Based Hydrogel as the Delivery System for Repairing Endometrial Injury,” Front. Bioeng. Biotechnol., vol. 10, no. June, pp. 1–16, 2022. [CrossRef]
- P. Trucillo, “Biomaterials for Drug Delivery and Human Applications,” Materials (Basel)., vol. 17, no. 2, 2024. [CrossRef]
- J. Vanacker et al., “Transplantation of an alginate-matrigel matrix containing isolated ovarian cells: First step in developing a biodegradable scaffold to transplant isolated preantral follicles and ovarian cells,” Biomaterials, vol. 33, no. 26, pp. 6079–6085, 2012. [CrossRef]
- J. M. Zuidema, C. J. Rivet, R. J. Gilbert, and F. A. Morrison, “A protocol for rheological characterization of hydrogels for tissue engineering strategies,” J. Biomed. Mater. Res. - Part B Appl. Biomater., vol. 102, no. 5, pp. 1063–1073, 2014. [CrossRef]
- M. H. Cai et al., “Design and Development of Hybrid Hydrogels for Biomedical Applications: Recent Trends in Anticancer Drug Delivery and Tissue Engineering,” Front. Bioeng. Biotechnol., vol. 9, no. February, pp. 1–18, 2021. [CrossRef]
- P. N. Sudha and M. H. Rose, Beneficial effects of hyaluronic acid, 1st ed., vol. 72. Elsevier Inc., 2014. [CrossRef]
- T. Kisukeda, J. Onaya, and K. Yoshioka, “Effect of diclofenac etalhyaluronate (SI-613) on the production of high molecular weight sodium hyaluronate in human synoviocytes,” BMC Musculoskelet. Disord., vol. 20, no. 1, pp. 1–9, 2019. [CrossRef]
- N. Mohan, S. R. R. Tadi, S. S. Pavan, and S. Sivaprakasam, “Deciphering the role of dissolved oxygen and N-acetyl glucosamine in governing higher molecular weight hyaluronic acid synthesis in Streptococcus zooepidemicus cell factory,” Appl. Microbiol. Biotechnol., vol. 104, no. 8, pp. 3349–3365, 2020. [CrossRef]
- M. B. Caspersen et al., “Thermal degradation and stability of sodium hyaluronate in solid state,” Carbohydr. Polym., vol. 107, no. 1, pp. 25–30, 2014. [CrossRef]
- P. Snetkov, K. Zakharova, S. Morozkina, and R. Olekhnovich, “Hyaluronic Acid : The Influence of Molecular Weight and Degradable Properties of Biopolymer,” Polymers (Basel)., vol. 12, p. 1800, 2020.
- P. Paulino, M. B. Da Cruz, and V. Santos, “Hyaluronic Acid Aesthetic Fillers: A Review of Rheological and Physicochemical Properties,” J. Cosmet. Sci., vol. 74, no. 2, pp. 132–142, 2023.
- G. Abatangelo, V. Vindigni, G. Avruscio, L. Pandis, and P. Brun, “Hyaluronic acid: Redefining its role,” Cells, vol. 9, no. 7, pp. 1–19, 2020. [CrossRef]
- C. Buckley, T. R. Montgomery, T. Szank, B. A. Murray, C. Quigley, and I. Major, “Modification of hyaluronic acid to enable click chemistry photo-crosslinking of hydrogels with tailorable degradation profiles,” Int. J. Biol. Macromol., vol. 240, no. April, p. 124459, 2023. [CrossRef]
- L. J. Lin, X. Y. Qiao, X. P. Chen, L. Z. Xu, and H. Chen, “Efficacy of Reducing Recurrence of Intrauterine Adhesions and Improving Pregnancy Outcome after Hysteroscopic Adhesiolysis: A Systematic Review and Network Meta-Analysis of Randomized Controlled Trials,” Clin. Exp. Obstet. Gynecol., vol. 51, no. 4, 2024. [CrossRef]
- B. Devi, R. Devi, S. Pradhan, D. Giri, N. Lepcha, and S. Basnet, “Application of Correlational Research Design in Nursing and Application of Correlational Research Design in Nursing,” J. Xi’an Shiyou Univ. Nat. Sci. Ed., vol. 65, no. 11, pp. 60–69, 2022. [CrossRef]
- V. Jasper et al., “Belgian consensus on adhesion prevention in hysteroscopy and laparoscopy,” Gynecol. Surg., vol. 12, no. 3, pp. 179–187, 2015. [CrossRef]
- C. H. Tu, X. L. Yang, X. Y. Qin, L. P. Cai, and P. Zhang, “Management of intrauterine adhesions: A novel intrauterine device,” Med. Hypotheses, vol. 81, no. 3, pp. 394–396, 2013. [CrossRef]
- S. Saska, L. Pilatti, A. Blay, and J. A. Shibli, “Bioresorbable polymers: Advanced materials and 4D printing for tissue engineering,” Polymers (Basel)., vol. 13, no. 4, pp. 1–24, 2021. [CrossRef]
- X. Wang, D. Wu, W. Li, and L. Yang, “Emerging biomaterials for reproductive medicine,” Eng. Regen., vol. 2, no. November 2021, pp. 230–245, 2021. [CrossRef]
- A. Kaczmarek-Pawelska, “Alginate-Based Hydrogels in Regenerative Medicine,” Alginates - Recent Uses This Nat. Polym., no. July, 2020. [CrossRef]
- H. H. Tønnesen and J. Karlsen, “Alginate in drug delivery systems,” Drug Dev. Ind. Pharm., vol. 28, no. 6, pp. 621–630, 2002. [CrossRef]
- D. R. Sahoo and T. Biswal, “Alginate and its application to tissue engineering,” SN Appl. Sci., vol. 3, no. 1, pp. 1–19, 2021. [CrossRef]
- J. Kurowiak, A. Kaczmarek-Pawelska, A. G. Mackiewicz, and R. Bedzinski, “Analysis of the degradation process of alginate-based hydrogels in artificial urine for use as a bioresorbable material in the treatment of urethral injuries,” Processes, vol. 8, no. 3, 2020. [CrossRef]
- E. Francés-Herrero, A. Rodríguez-Eguren, M. Gómez-álvarez, L. de Miguel-Gómez, H. Ferrero, and I. Cervelló, “Future Challenges and Opportunities of Extracellular Matrix Hydrogels in Female Reproductive Medicine,” Int. J. Mol. Sci., vol. 23, no. 7, 2022. [CrossRef]
- Y. Cai et al., “Porous scaffolds from droplet microfluidics for prevention of intrauterine adhesion,” Acta Biomater., vol. 84, pp. 222–230, 2019. [CrossRef]
- S. K. L. Levengood and M. Zhang, “Chitosan-based scaffolds for bone tissue engineering,” J. Mater. Chem. B, vol. 2, no. 21, pp. 3161–3184, 2014. [CrossRef]
- J. Alkabli, “Recent advances in the development of chitosan/hyaluronic acid-based hybrid materials for skin protection, regeneration, and healing: A review,” Int. J. Biol. Macromol., vol. 279, no. P3, p. 135357, 2024. [CrossRef]
- M. Amidi, E. Mastrobattista, W. Jiskoot, and W. E. Hennink, “Chitosan-based delivery systems for protein therapeutics and antigens,” Adv. Drug Deliv. Rev., vol. 62, no. 1, pp. 59–82, 2010. [CrossRef]
- S. (Gabriel) Kou, L. M. Peters, and M. R. Mucalo, “Chitosan: A review of sources and preparation methods,” Int. J. Biol. Macromol., vol. 169, pp. 85–94, 2021. [CrossRef]
- P. Baldrick, “The safety of chitosan as a pharmaceutical excipient,” Regul. Toxicol. Pharmacol., vol. 56, no. 3, pp. 290–299, 2010. [CrossRef]
- L. Col, M. Moore, B. Whisman, and R. Gomez, “Safety of Chitosan Bandages in Shellfi sh Allergic Patients,” vol. 176, no. October 2011, pp. 1153–1156, 2018.
- M. Rizzo et al., “Effects of chitosan on plasma lipids and lipoproteins: A 4-month prospective pilot study,” Angiology, vol. 65, no. 6, pp. 538–542, 2014. [CrossRef]
- Z. Shariatinia, “Pharmaceutical applications of chitosan,” Adv. Colloid Interface Sci., vol. 263, pp. 131–194, 2019. [CrossRef]
- D. I. Sánchez-Machado, J. López-Cervantes, M. A. Correa-Murrieta, R. G. Sánchez-Duarte, P. Cruz-Flores, and G. S. la Mora-López, Chitosan. Elsevier Inc., 2018. [CrossRef]
- C. Nagori, S. Panchal, and H. Patel, “Endometrial regeneration using autologous adult stem cells followed by conception by in vitro fertilization in a patient of severe Ashermans syndrome,” J. Hum. Reprod. Sci., vol. 4, no. 1, pp. 43–48, 2011. [CrossRef]
- S. Singh, G. Singh, C. Prakash, S. Ramakrishna, L. Lamberti, and C. I. Pruncu, “3D printed biodegradable composites: An insight into mechanical properties of PLA/chitosan scaffold,” Polym. Test., vol. 89, p. 106722, 2020. [CrossRef]
- A. Ershad-Langroudi, N. Babazadeh, F. Alizadegan, S. Mehdi Mousaei, and G. Moradi, “Polymers for implantable devices,” J. Ind. Eng. Chem., vol. 137, no. November 2023, pp. 61–86, 2024. [CrossRef]
- P. Kulkarni and M. Maniyar, “Utilization of Fish Collagen in Pharmaceutical and Biomedical Industries: Waste To Wealth Creation,” Res. J. Life Sci. Bioinformatics, Pharm. Chem. Sci., vol. 6, no. 3, pp. 11–20, 2020. [CrossRef]
- H. Lu et al., “Targeting cancer stem cell signature gene SMOC-2 Overcomes chemoresistance and inhibits cell proliferation of endometrial carcinoma,” EBioMedicine, vol. 40, pp. 276–289, 2019. [CrossRef]
- M. Yanez, J. Rincon, A. Dones, C. De Maria, R. Gonzales, and T. Boland, “In vivo assessment of printed microvasculature in a bilayer skin graft to treat full-thickness wounds,” Tissue Eng. - Part A, vol. 21, no. 1–2, pp. 224–233, 2015. [CrossRef]
- J. Y. Park et al., “A comparative study on collagen type i and hyaluronic acid dependent cell behavior for osteochondral tissue bioprinting,” Biofabrication, vol. 6, no. 3, 2014. [CrossRef]
- Y. Liu, D. Jia, L. Li, and M. Wang, “Advances in Nanomedicine and Biomaterials for Endometrial Regeneration: A Comprehensive Review,” Int. J. Nanomedicine, vol. 19, pp. 8285–8308, 2024. [CrossRef]
- D. Qiao et al., “Enhancing thermal stability and mechanical resilience in gelatin/starch composites through polyvinyl alcohol integration,” Carbohydr. Polym., vol. 344, no. January, p. 122528, 2024. [CrossRef]
- F. Silva, “Regenerative medicine,” J. Transl. Med., vol. 22, no. 1, pp. 1–15, 2024. [CrossRef]
- Xiayi xu et al., “Dynamic gelatin-based hydrogels promote the proliferation and self-renewal of embryonic stem cells in long-term 3D culture,” Biomaterials, vol. 289, no. September, p. 121802, 2022. [CrossRef]
- M. S. Singhvi, S. S. Zinjarde, and D. V. Gokhale, “Polylactic acid: synthesis and biomedical applications,” J. Appl. Microbiol., vol. 127, no. 6, pp. 1612–1626, 2019. [CrossRef]
- R. P. Pawar, S. U. Tekale, S. U. Shisodia, J. T. Totre, and A. J. Domb, “Biomedical applications of poly(lactic acid),” Rec. Pat. Regen. Med., vol. 4, no. 1, pp. 40–51, 2014. [CrossRef]
- L. S. Nair and C. T. Laurencin, “Biodegradable polymers as biomaterials,” Prog. Polym. Sci., vol. 32, no. 8–9, pp. 762–798, 2007. [CrossRef]
- M. Hussain, S. M. Khan, M. Shafiq, and N. Abbas, “A review on PLA-based biodegradable materials for biomedical applications,” Giant, vol. 18, 2024. [CrossRef]
- D. da Silva et al., “Biocompatibility, biodegradation and excretion of polylactic acid (PLA) in medical implants and theranostic systems,” Chem. Eng. J., vol. 340, pp. 9–14, 2018. [CrossRef]
- B. Kheilnezhad and A. Hadjizadeh, “A review: Progress in preventing tissue adhesions from a biomaterial perspective,” Biomater. Sci., vol. 9, no. 8, pp. 2850–2873, 2021. [CrossRef]
- J. Pal, N. Kankariya, S. Sanwaria, B. Nandan, and R. K. Srivastava, “Control on molecular weight reduction of poly(ε-caprolactone) during melt spinning - A way to produce high strength biodegradable fibers,” Mater. Sci. Eng. C, vol. 33, no. 7, pp. 4213–4220, 2013. [CrossRef]
- M. H. Rahaman and H. Tsuji, “Synthesis and Characterization of Stereo Multiblock Poly(lactic acid)s with Different Block Lengths by Melt Polycondensation of Poly(L-lactic acid)/Poly(D-lactic acid) Blends,” Macromol. React. Eng., vol. 6, no. 11, pp. 446–457, 2012. [CrossRef]
- A. Goyanes, A. B. M. Buanz, A. W. Basit, and S. Gaisford, “Fused-filament 3D printing (3DP) for fabrication of tablets,” Int. J. Pharm., vol. 476, no. 1, pp. 88–92, 2014. [CrossRef]
- U. Nöth, L. Rackwitz, A. F. Steinert, and R. S. Tuan, “Cell delivery therapeutics for musculoskeletal regeneration,” Adv. Drug Deliv. Rev., vol. 62, no. 7–8, pp. 765–783, 2010. [CrossRef]
- L. Xu, K. Crawford, and C. B. Gorman, “Effects of temperature and pH on the degradation of poly(lactic acid) brushes,” Macromolecules, vol. 44, no. 12, pp. 4777–4782, 2011. [CrossRef]
- S. Leprince et al., “Preliminary design of a new degradable medical device to prevent the formation and recurrence of intrauterine adhesions,” Commun. Biol., vol. 2, no. 1, 2019. [CrossRef]
- H. Kaczmarek, M. Nowicki, I. Vuković-Kwiatkowska, and S. Nowakowska, “Crosslinked blends of poly(lactic acid) and polyacrylates: AFM, DSC and XRD studies,” J. Polym. Res., vol. 20, no. 3, 2013. [CrossRef]
- P. Qin, L. Wu, and S. Jie, “Poly(glycolic acid) materials with melt reaction/processing temperature window and superior performance synthesized via melt polycondensation,” Polym. Degrad. Stab., vol. 220, no. November 2023, 2024. [CrossRef]
- Kureha Corporation, “Polyglycolic Acid ( PGA ) - Technical Guidebook,” no. November 2011, p. 1, 2011, [Online]. Available: http://www.kuredux.com/pdf/Kuredux_technical_EN.pdf.
- K. J. Jem and B. Tan, “The development and challenges of poly (lactic acid) and poly (glycolic acid),” Adv. Ind. Eng. Polym. Res., vol. 3, no. 2, pp. 60–70, 2020. [CrossRef]
- K. Yamane, H. Sato, Y. Ichikawa, K. Sunagawa, and Y. Shigaki, “Development of an industrial production technology for high-molecular-weight polyglycolic acid,” Polym. J., vol. 46, no. 11, pp. 769–775, 2014. [CrossRef]
- S. Amiri et al., “Evaluation of polyglycolic acid as an animal-free biomaterial for three-dimensional culture of human endometrial cells,” Clin. Exp. Reprod. Med., vol. 49, no. 4, pp. 259–269, 2022. [CrossRef]
- R. Supra and D. K Agrawal, “Peripheral Nerve Regeneration: Opportunities and Challenges,” J. Spine Res. Surg., vol. 05, no. 01, pp. 10–18, 2023. [CrossRef]
- S. Y. Lee et al., “Synthesis and in vitro characterizations of porous carboxymethyl cellulose-poly(ethylene oxide) hydrogel film,” Biomater. Res., vol. 19, no. 1, pp. 1–11, 2015. [CrossRef]
- M. S. Rahman et al., “Recent developments of carboxymethyl cellulose,” Polymers (Basel)., vol. 13, no. 8, 2021. [CrossRef]
- S. D. Yuwono, E. Wahyuningsih, Noviany, A. A. Kiswandono, W. Simanjuntak, and S. Hadi, “Characterization of carboxymethyl cellulose (CMC) synthesized from microcellulose of cassava peel,” Mater. Plast., vol. 57, no. 4, pp. 225–235, 2021. [CrossRef]
- H. Toǧrul and N. Arslan, “Production of carboxymethyl cellulose from sugar beet pulp cellulose and rheological behaviour of carboxymethyl cellulose,” Carbohydr. Polym., vol. 54, no. 1, pp. 73–82, 2003. [CrossRef]
- L. S. Liu and R. A. Berg, “Adhesion barriers of carboxymethylcellulose and polyethylene oxide composite gels,” J. Biomed. Mater. Res., vol. 63, no. 3, pp. 326–332, 2002. [CrossRef]
- A. Di Spiezio Sardo et al., “Efficacy of a Polyethylene Oxide-Sodium Carboxymethylcellulose Gel in Prevention of Intrauterine Adhesions After Hysteroscopic Surgery,” J. Minim. Invasive Gynecol., vol. 18, no. 4, pp. 462–469, 2011. [CrossRef]
- N. Fuchs et al., “Intercoat (Oxiplex/AP Gel) for Preventing Intrauterine Adhesions After Operative Hysteroscopy for Suspected Retained Products of Conception: Double-Blind, Prospective, Randomized Pilot Study,” J. Minim. Invasive Gynecol., vol. 21, no. 1, pp. 126–130, 2014. [CrossRef]
- K. K. Fujii, Y. Taga, Y. K. Takagi, R. Masuda, S. Hattori, and T. Koide, “The Thermal Stability of the Collagen Triple Helix Is Tuned According to the Environmental Temperature,” Int. J. Mol. Sci., vol. 23, no. 4, 2022. [CrossRef]
- Y. Liu, S. Cheong NG, J. Yu, and W. B. Tsai, “Modification and crosslinking of gelatin-based biomaterials as tissue adhesives,” Colloids Surfaces B Biointerfaces, vol. 174, no. October 2018, pp. 316–323, 2019. [CrossRef]
- J. Kurowiak, T. Klekiel, and R. Będziński, “Biodegradable Polymers in Biomedical Applications: A Review—Developments, Perspectives and Future Challenges,” Int. J. Mol. Sci., vol. 24, no. 23, 2023. [CrossRef]
- B. Xu et al., “Injectable Mesenchymal Stem Cell-Laden Matrigel Microspheres for Endometrium Repair and Regeneration,” vol. 2000202, pp. 1–11, 2021. [CrossRef]
- A. Raval, J. Parikh, and C. Engineer, “Mechanism of controlled release kinetics from medical devices,” Brazilian J. Chem. Eng., vol. 27, no. 2, pp. 211–225, 2010. [CrossRef]
- Y. Fu and W. J. Kao, “Drug release kinetics and transport mechanisms of non-degradable and degradable polymeric delivery systems,” Expert Opin. Drug Deliv., vol. 7, no. 4, pp. 429–444, 2010. [CrossRef]
- S. Huberlant et al., “In Vivo Evaluation of the Efficacy and Safety of a Novel Degradable Polymeric Film for the Prevention of Intrauterine Adhesions,” J. Minim. Invasive Gynecol., vol. 28, no. 7, pp. 1384–1390, 2021. [CrossRef]
- S. Weyers et al., “Safety and Efficacy of a Novel Barrier Film to Prevent Intrauterine Adhesion Formation after Hysteroscopic Myomectomy: The PREG1 Clinical Trial,” J. Minim. Invasive Gynecol., vol. 29, no. 1, pp. 151–157, 2022. [CrossRef]
- Z. Lisa et al., “4DryField vs. hyalobarrier gel for preventing the recurrence of intrauterine adhesions–a pilot study,” Minim. Invasive Ther. Allied Technol., vol. 0, no. 0, pp. 1–7, 2024. [CrossRef]
- L. Mettler, A. Audebert, E. Lehmann-Willenbrock, K. Schive, and V. R. Jacobs, “Prospective clinical trial of SprayGel as a barrier to adhesion formation: An interim analysis,” J. Am. Assoc. Gynecol. Laparosc., vol. 10, no. 3, pp. 339–344, 2003. [CrossRef]
- G. Ahmad et al., “Barrier agents for adhesion prevention after gynaecological surgery,” Cochrane Database Syst. Rev., no. 2, 2008. [CrossRef]
- S. Khunmanee, Y. Jeong, and H. Park, “Crosslinking method of hyaluronic-based hydrogel for biomedical applications,” J. Tissue Eng., vol. 8, 2017. [CrossRef]
- S. P. Fundarò, G. Salti, D. M. H. Malgapo, and S. Innocenti, “The Rheology and Physicochemical Characteristics of Hyaluronic Acid Fillers: Their Clinical Implications,” Int. J. Mol. Sci., vol. 23, no. 18, 2022. [CrossRef]
- A. Biesiekierski, K. Munir, Y. Li, and C. Wen, Material selection for medical devices. LTD, 2020. [CrossRef]
Figure 1.
The common causes of IUAs and current treatment methods. IUAs commonly result from endometrial injury, inflammation or infections. While hysteroscopy is the standard treatment, current additional management methods include pharmacotherapy, stem cell therapy, and physical barriers [15].
Figure 1.
The common causes of IUAs and current treatment methods. IUAs commonly result from endometrial injury, inflammation or infections. While hysteroscopy is the standard treatment, current additional management methods include pharmacotherapy, stem cell therapy, and physical barriers [15].
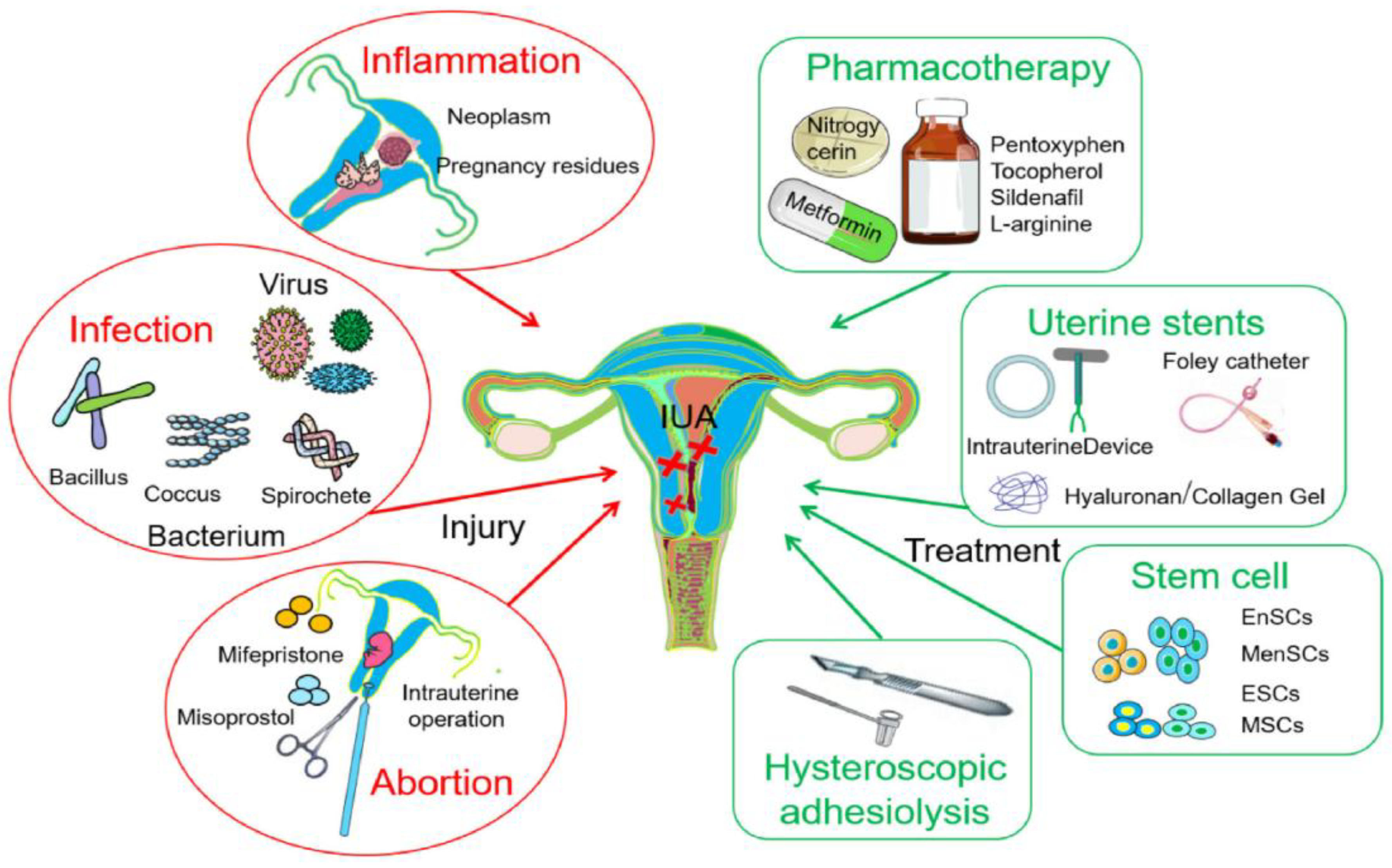
Figure 2.
Schematic representation of the chemical structure of HA with two repeating disaccharide sugars monomer glucuronic acid and acetylglucosamine linked by a glycosidic linkage [4].
Figure 2.
Schematic representation of the chemical structure of HA with two repeating disaccharide sugars monomer glucuronic acid and acetylglucosamine linked by a glycosidic linkage [4].
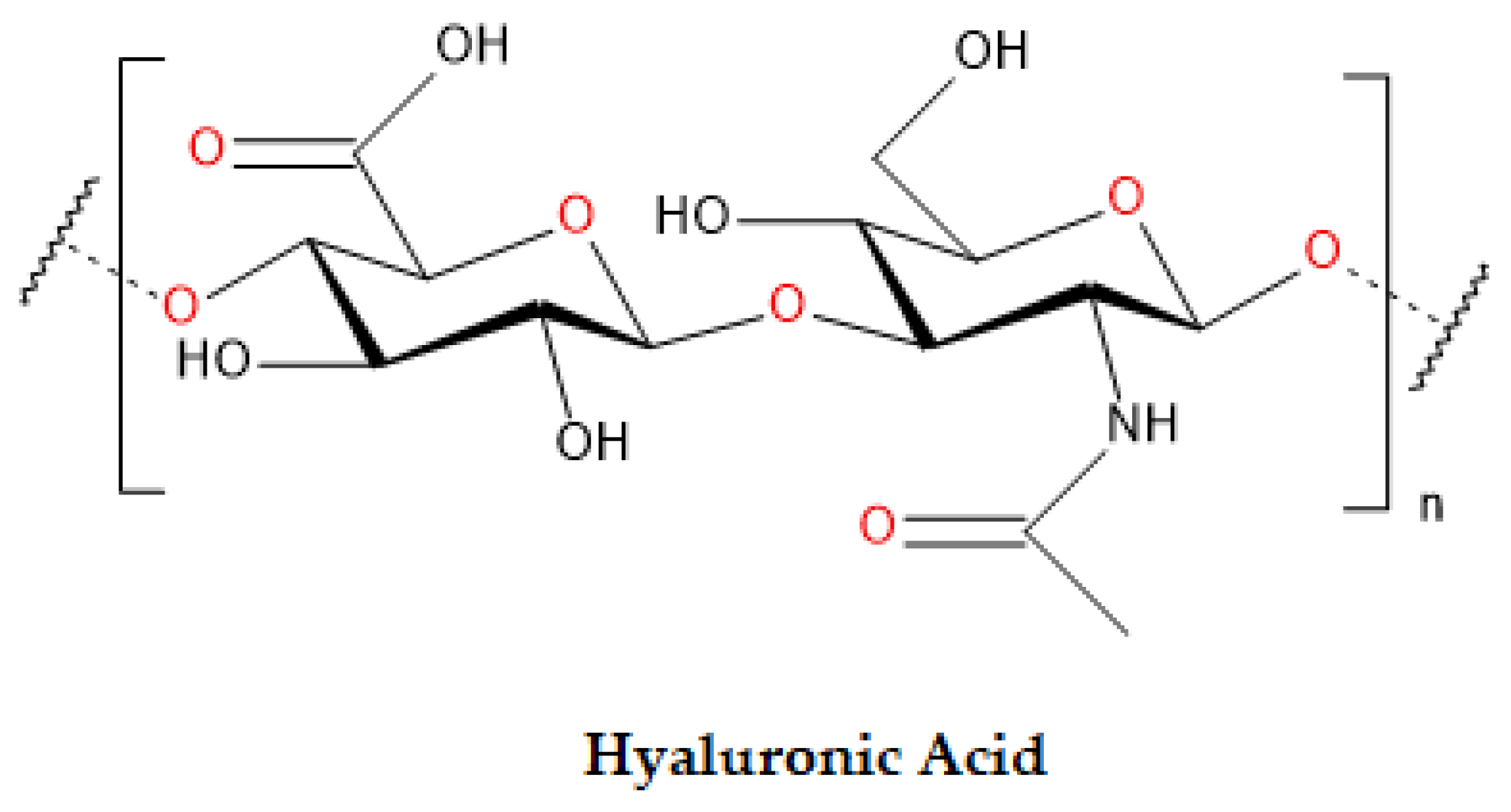
Figure 3.
Chemical structure of Alginate with α-L-guluronic acid (G-blocks) and β-D-mannuronic acid (M-blocks) copolymers linked up with (1,4)-glycosidic [4].
Figure 3.
Chemical structure of Alginate with α-L-guluronic acid (G-blocks) and β-D-mannuronic acid (M-blocks) copolymers linked up with (1,4)-glycosidic [4].
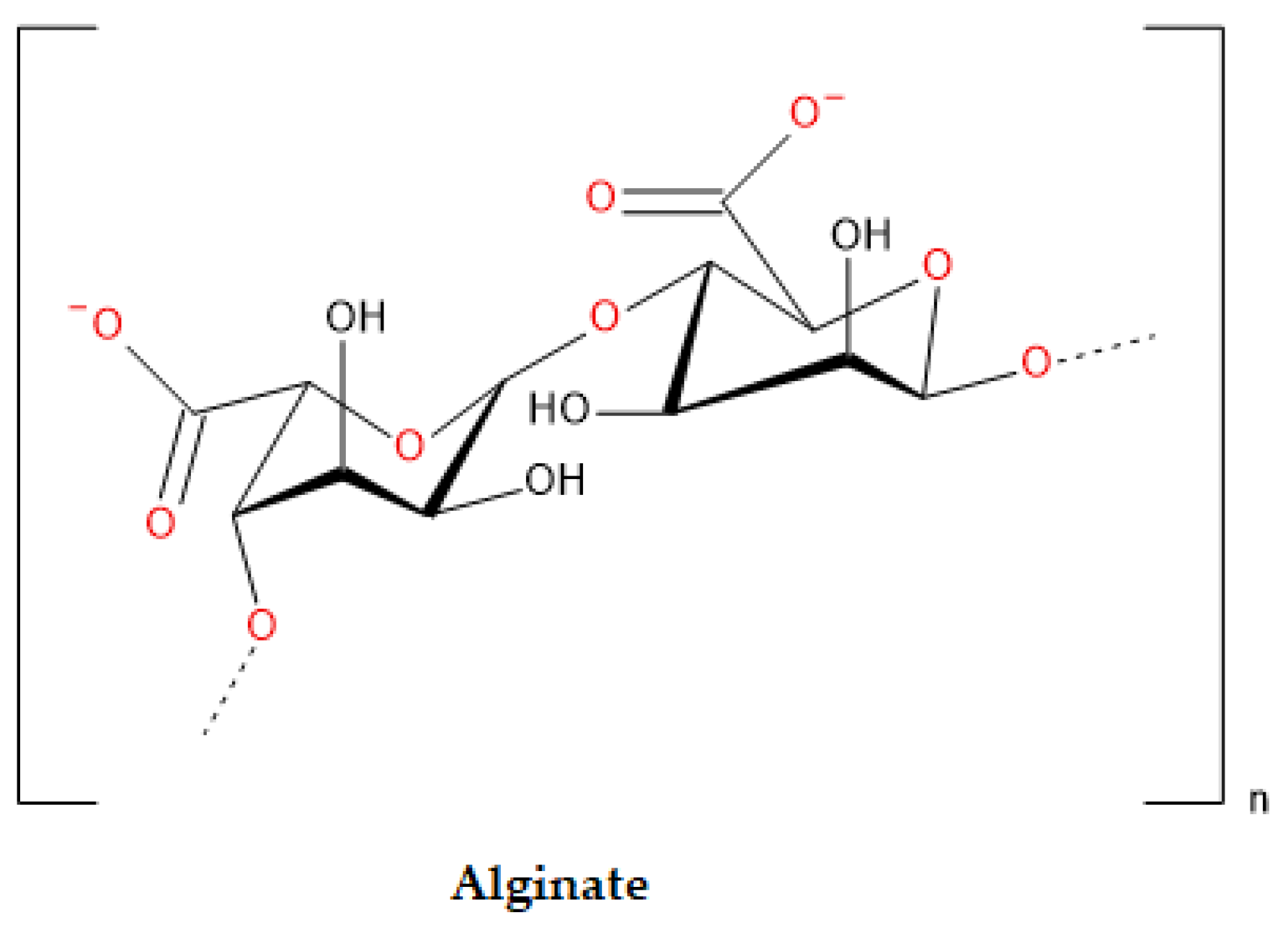
Figure 4.
Chemical structure of chitosan with glucosamine and N-acetylglucosamine units linked by β (1-4) glycosidic bonds [70].
Figure 4.
Chemical structure of chitosan with glucosamine and N-acetylglucosamine units linked by β (1-4) glycosidic bonds [70].
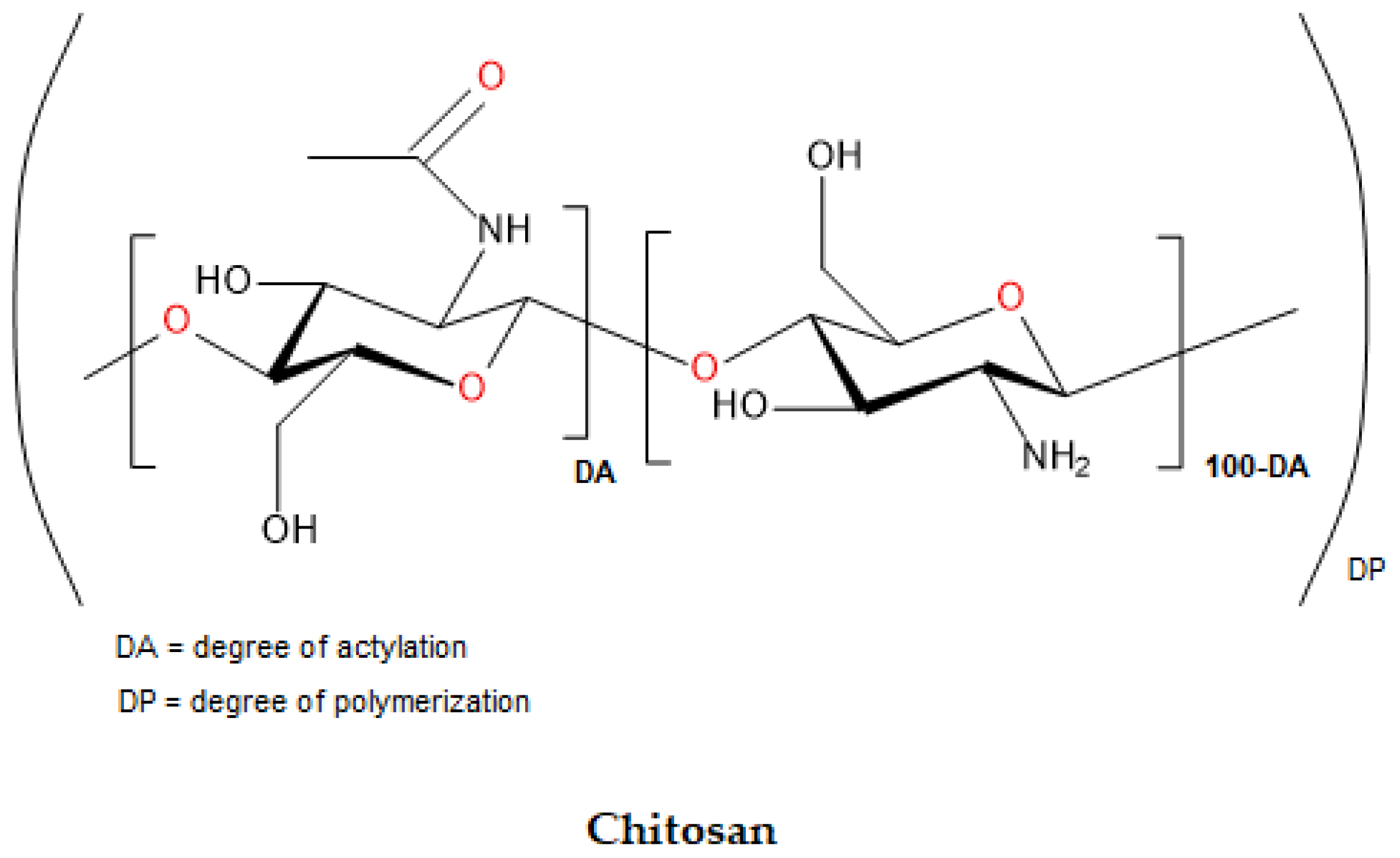
Figure 5.
The image represents the structural formula of collagen [80].
Figure 5.
The image represents the structural formula of collagen [80].
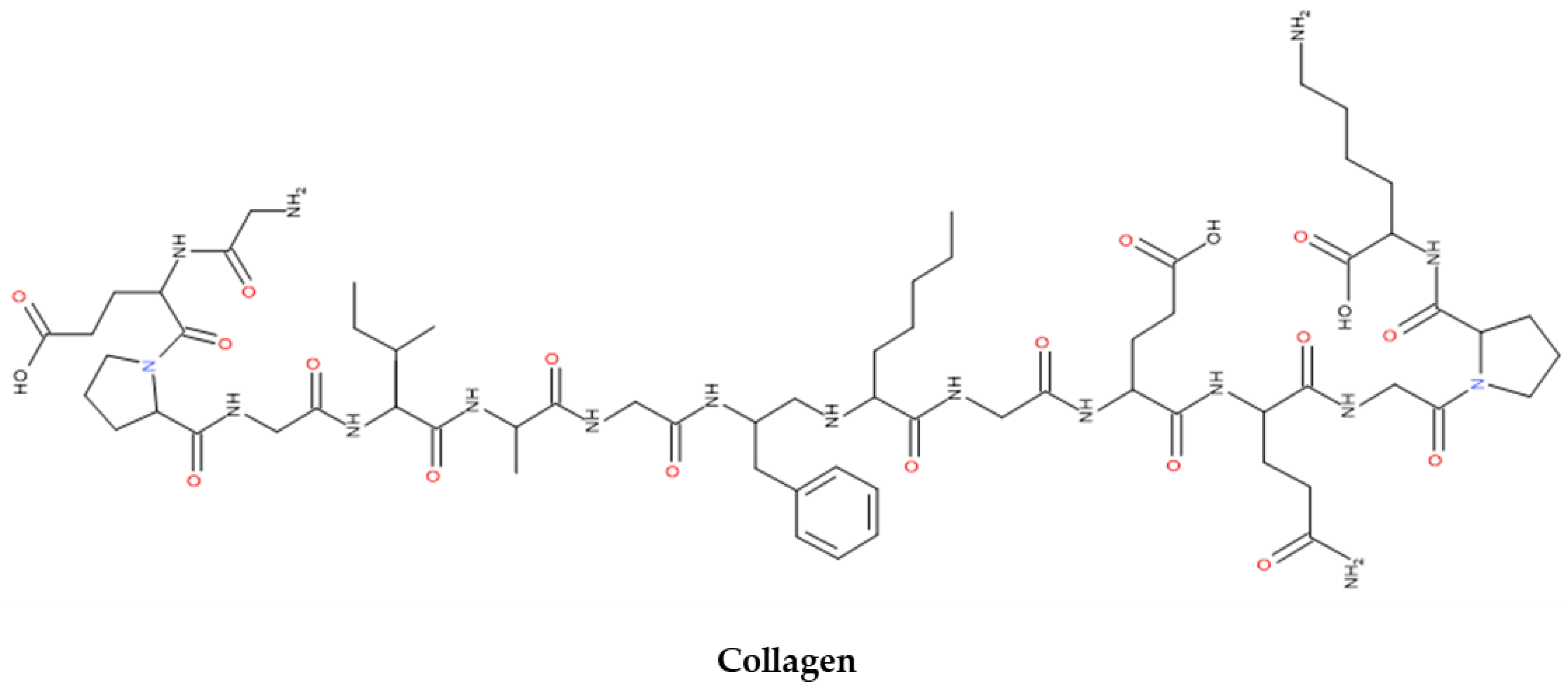
Figure 6.
The image represents the structural formula of gelatin [80].
Figure 6.
The image represents the structural formula of gelatin [80].
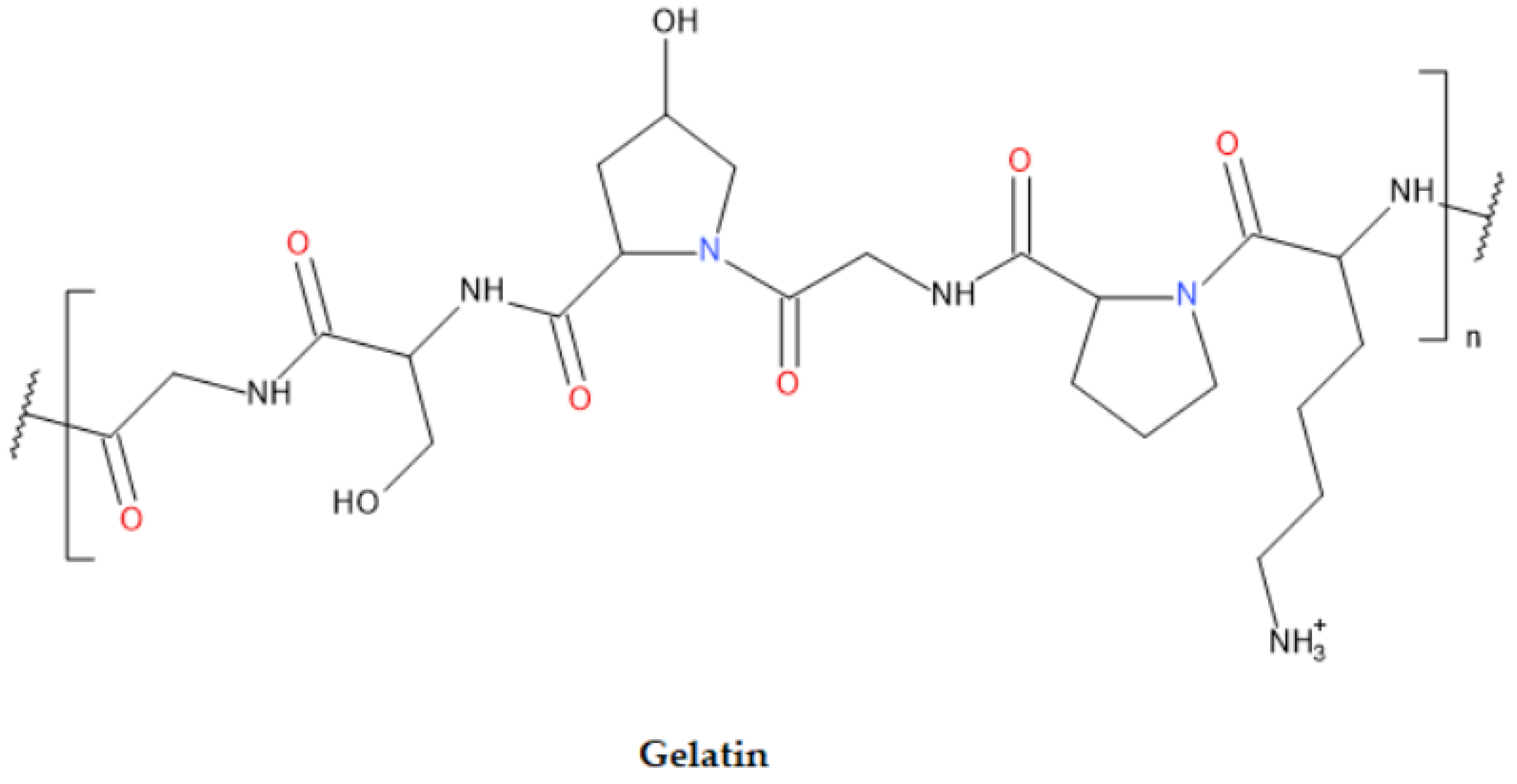
Figure 7.
Structural formula of PLA [94].
Figure 7.
Structural formula of PLA [94].
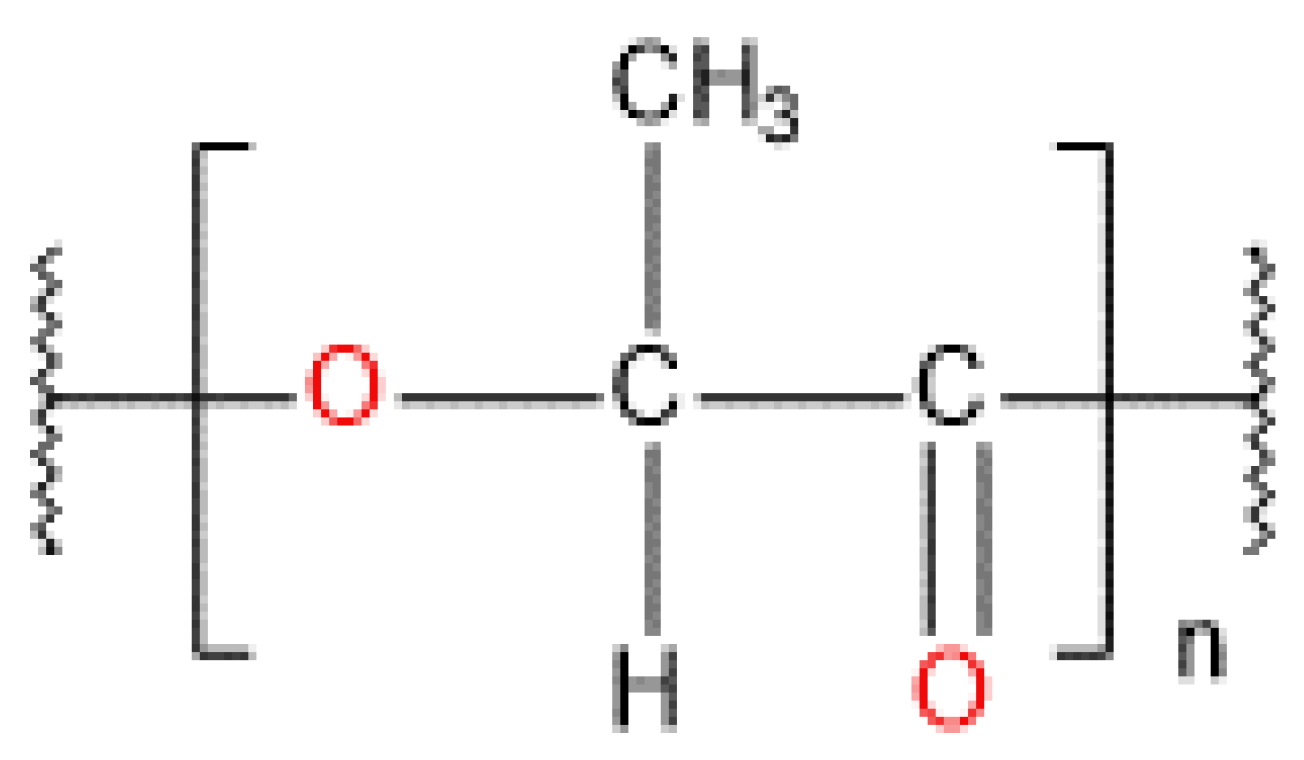
Figure 8.
PLA synthesis pathways: As shown above, PLA can be synthesized from LA monomers using various pathways, including direct polycondensation, azeotropic dehydration condensation, or ring-opening polymerization. These processes occur under controlled conditions such as temperature, pressure, and pH, with the presence of a catalyst [92].
Figure 8.
PLA synthesis pathways: As shown above, PLA can be synthesized from LA monomers using various pathways, including direct polycondensation, azeotropic dehydration condensation, or ring-opening polymerization. These processes occur under controlled conditions such as temperature, pressure, and pH, with the presence of a catalyst [92].
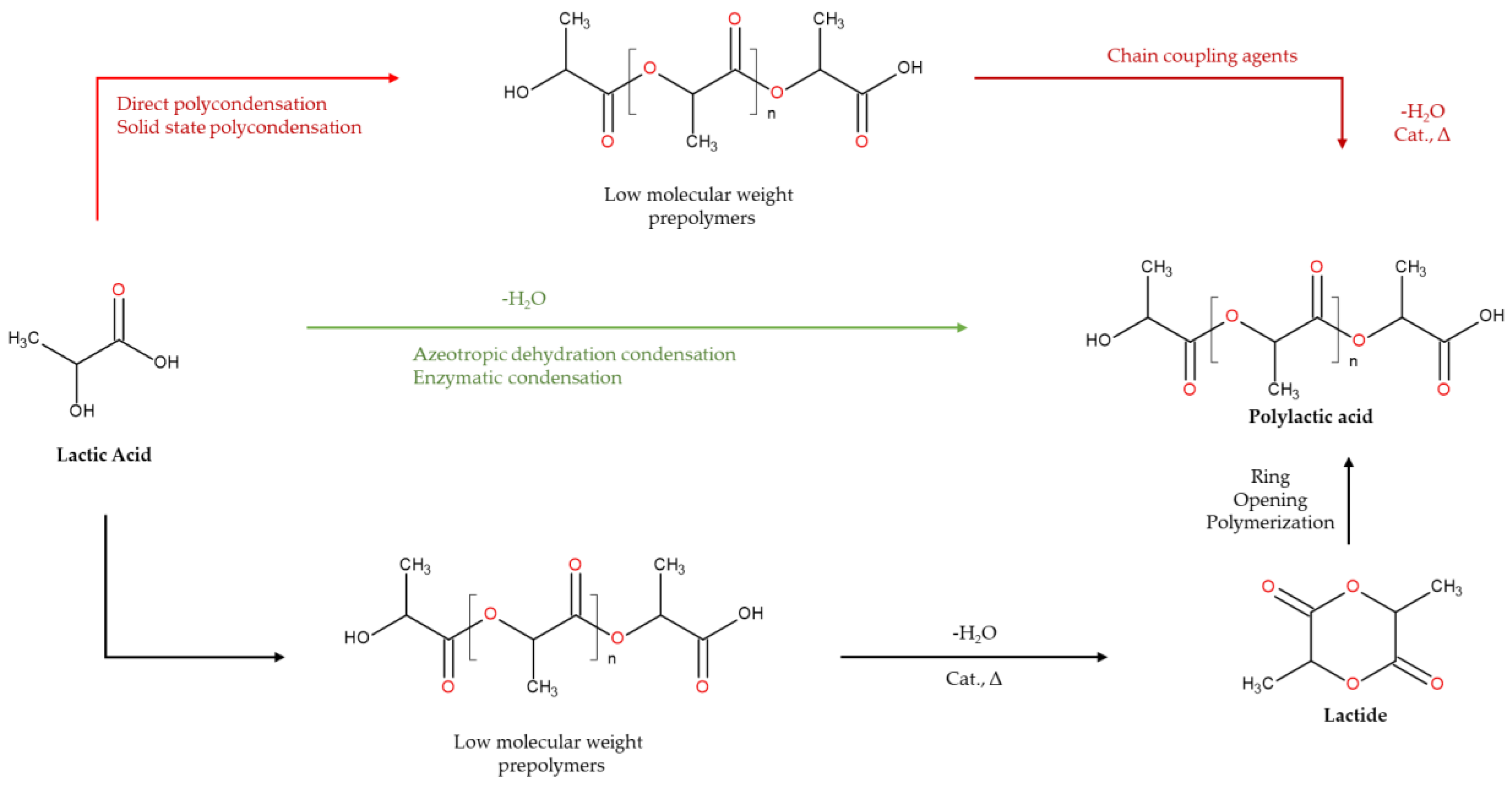
Figure 9.
The image depicts the structural formula of PGA with its glycolide as monomer.
Table 1.
Desirable characteristics of biomaterials for use in tissue engineering applications.
| Characteristics | Descriptions |
|---|---|
| Biocompatibility | Biomaterials should not trigger adverse immune responses when interacting with the body, while also providing biological and functional benefits to the construct |
| Biodegradability | After interacting with the body, the biomaterial should degrade, and either be excreted or absorbed by the body |
| Lack of toxicity | The by-products generated by biomaterials should be non-toxic and pose no harm to the body or surrounding tissues |
| Mechanical properties | Biomaterials should have strong mechanical properties that match the structure of reproductive organ tissues and support their functions effectively |
| Biomimicry | Biomaterials should be designed to align with the anatomical and physiological characteristics of specific native tissues |
Table 2.
Key PLA physical and mechanical properties [92].
Table 2.
Key PLA physical and mechanical properties [92].
| Property | PLA | PLLA | PDLLA |
|---|---|---|---|
| Melting temperature, (°C) | 150–162 | 170–200 | Amorphous |
| Glass transition temperature (°C) | 45–60 | 55–65 | 50–60 |
| Ultimate tensile strength, (MPa) | 21–60 | 15.5–150 | 27.6–50 |
| Tensile modulus (GPa) | 0.35–0.5 | 2.7–4.14 | 1–3.45 |
| Ultimate tensile strain (%) | 2.5–6 | 3.0–10.0 | 2.0–10.0 |
| Specific tensile modulus (kNm/g) | 0.28–2.8 | 0.80 | 2.23–3.85 |
Table 3.
Main PGA physical and mechanical properties [103].
Table 3.
Main PGA physical and mechanical properties [103].
| Property | PGA |
|---|---|
| Melting temperature, (°C) | 220 |
| Glass transition temperature (°C) | 40 |
| Heat deflection temperature (°C) | 168 |
| Tensile elongation, (%) | 2.1 |
| Tensile modulus (GPa) | 7.0 |
| Tensile strength (MPa) | 109 |
Table 5.
summarizes the key factors affecting release kinetics from implantable drug delivery devices [119,120].
| Parameters | Effects |
|---|---|
| 1. Drug properties | Impacts the aqueous solubility, which subsequently influences various factors such as protein binding, tissue retention, localized drug concentration, and the kinetics of drug release. |
| Hydrophilicity/hydrophobicity | |
| Diffusion/dissolution characteristics | |
| Charge | |
| Stability | |
| Solubility in biopolymer matrix | |
| 2. Biopolymer properties | Biopolymers influence degradation, hydrophobicity, drug release, and drug solubility. |
| Thermal property | |
| Degree of crystallinity | |
| Molecular weight | |
| 3. Release medium | Influences the degradation profile of biopolymers and the solubility of drugs. |
| pH | |
| Temperature | |
| Ionic strength | |
| Enzymes |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



