
Submitted:
25 March 2025
Posted:
26 March 2025
You are already at the latest version
Abstract
Background/Objectives: Art-based community projects positively impact mental health recovery by fostering creativity, self-expression, and social engagement. Despite growing evidence on participatory art interventions, limited studies have used a mixed-methods approach to examine their effects. The present study examines how participation in Artistic Couples influences individuals’ subjective perceptions of recovery, psychological well-being, and self-stigma. Methods: This exploratory multi-centre study employed an embedded mixed-methods design, integrating qualitative Photovoice methodology with a quantitative pre-post survey. Participants (N=30) from five mental health institutions across Catalonia engaged in collaborative art creation with local artists. Qualitative data from Photovoice discussions and semi-structured interviews were analyzed using thematic analysis, while quantitative data from standardized measures were examined using paired t-tests and correlation analysis. Results: Qualitative findings revealed three key themes: (1) Artmaking as an artistic couple, emphasizing the collaborative process and art as a means of self-expression; (2) Social connections, highlighting increased belonging, emotional support, and reduced loneliness; and (3) Understanding mental health recovery, showcasing art’s role in identity reconstruction and personal growth. Quantitative results indicated a significant improvement in the Connecting and Belonging subscale of the RAS-DS (t=-2.51, p=0.023), particularly among women (t=-2.85, p=0.019), suggesting enhanced social integration. However, no statistically significant changes were observed in overall recovery, well-being, or self-stigma scores. Conclusions: This study provides evidence that participatory community art projects enhance social connections and self-expression, key elements of mental health recovery. Findings suggest that creative collaborations facilitate emotional processing and challenge stigma. The improvement in social belonging supports integrating arts-based interventions in recovery-oriented care. Future research should examine long-term effects and gender-sensitive approaches.
Keywords:
mental health
; art-based
; recovery
; stigma
; photovoice
; community
; social
; connecting and belonging
; person-centered
; mixed-method
1. Introduction
Art-based community projects support a positive effect between art participation and mental health improvement [1,2,3,4], offering valuable opportunities to foster creativity and self-expression [5,6]. These practices enable people to engage in their social environment [7], thereby developing stronger social connections [8,9]. Such relationships can significantly reduce the stigma associated with mental health challenges [4,10].
Influenced by consumers and caregivers, the concept of personal recovery in mental health has evolved into a holistic, person-centered approach that incorporates lived experiences and non-medical perspectives [11,12], prioritizing individual experiences over standardized treatments [13,14]. Research suggests that traditional models may not fully address recovery needs or social dimensions [15,16]. The CHIME framework [17] outlines essential elements of recovery—Connectedness, Hope, Identity, Meaning, and Empowerment—derived from narrative synthesis and systematic review. These components are validated in research as central to both the practical application and theoretical understanding of recovery [18,19,20]. Emerging recommendations suggest that recovery-oriented mental health services should adopt person-centered approaches that align with users’ lived experience [21,22], thus giving the recovery model a more subjective perspective and moving away from professionally dominated interventions [23,24].
Studies indicate that mental health recovery can be enhanced and perceived as a community effort [25]. Collaborative exploration of recovery through creative engagement, as a relational component, presents opportunities to nurture equitable, appreciative and interconnected communities [26,27]. The body of evidence demonstrating the beneficial effects of creative arts on health continues to grow steadily [28,29]. Notably, community arts initiatives have been linked to promoting self-expression, enhancing skills and achievements, reducing social isolation, and improving self-efficacy [30]. Community-based arts programs provide significant mental health benefits, but their effectiveness can be constrained by challenges related to accessibility and long-term sustainability, particularly in rural or underserved communities [3]. These initiatives promote inclusivity and enhance social connections [8]), yet their success relies on the presence of safe, non-stigmatizing environments and consistent opportunities for participation. The authors recommend that future studies should adopt prospective designs that utilize mixed-methods approaches, incorporating validated recovery outcome measures alongside subjective assessments of participants' perceptions of their recovery process.
Building on these recommendations, the present study aims to examine how a community art project influences participants' subjective perceptions of their recovery process, psychological well-being, and self-stigma. To the best of our knowledge, no mixed-methods study has yet evaluated the experiences and self-perception of individuals participating in an art-based community project through a participatory research approach. To address the need for a deeper understanding of art-based interventions within the recovery framework, this study focuses on participants from the Artistic Couples project. The purpose is to identify the specific elements of these interventions that provide the greatest benefits to individuals, recognizing that the impact may vary among different participants.
1.1. The study
1.1.1. Aim
The aims of this study are:
a) To examine the impact of participating in Artistic Couples and its influence on subjective perceptions of the recovery process in mental health, psychological well-being, and self-stigma.
b) To explore the experiences, satisfaction and opportunities for participation in Artistic Couples among individuals linked to mental health services.
c) To understand how mental health recovery is perceived and connected to the experiences within the Artistic Couples project.
1.1.2. About project Artistic Couples
Artistic Couples (translated from the original Catalan name “Parelles Artístiques”) [31]) project was launched in 2006 at Osonament, a non-profit organization dedicated to promoting the holistic development of individuals with mental health diagnoses and enhancing their quality of life. The project involves the creation and subsequent exhibition of works produced by pairs consisting of an individual with mental health concerns and a local artist. Meetings between participants take place at community services such as artistic workshops, civic centers, urban areas, academic institutions and arts schools. Over seventeen editions, 1,089 artists have participated in the program, resulting 824 artworks across various artistic disciplines including plastic arts, visual arts, performance, and literature. This achievement is largely due to the extensive network of Artistic Couples in Catalonia involving diverse mental health institutions that contribute to the initiative. A total of 28 institutions from 15 different counties have participated at least once over the 17 years of the project. Qualitative outcomes from the participants’ process was already published [32].
2. Materials and Methods
2.1. Design
This study adopts a qualitatively driven embedded mixed-methods design [33], initiated in October 2022, involving multiple mental health units across Catalonia. The primary focus is on the subjective recovery experiences of participants, explored through the Photovoice method. This process captures the richness and depth of participants' recovery processes, aligning with the principles of person-centered and recovery-oriented mental health care. Consistent with the subjectivity inherent in the recovery model, this approach highlights not only individuals' experiences but also the personal significance they attributed to those experiences.
The qualitative methodology is based on the Photovoice method, which uses photography to explore personal experiences and empower participants to document their lives visually [34]. This participatory approach fosters collective meaning-making through group discussions [35], enabling participants to highlight community strengths, raise awareness of key issues, and advocate for change [36]. Adaptable to diverse populations, Photovoice is particularly effective in mental health contexts [37,38,39], promoting accessibility and emphasizing the principle that "people are the experts of their own lives" ([40] p.911, [41]). It plays a vital role in recovery by amplifying participants' voices and encouraging community engagement through dissemination activities like public exhibitions [42].
The qualitative component, anchored in the Photovoice process, is complemented by a quantitative pre-post survey using standardized Patient-Reported Outcome Measures (PROMs), satisfaction surveys, and subjective assessments to provide contextual data, support qualitative data and triangulate findings.
2.2. Procedure of Recruitment
The first author contacted to mental health units that were part of the Artistic Couple network and were up to participate in the 17th Artistic Couple edition (7 units). It was presented the research project and its objectives to each center. Finally, 5 units agreed to participate. A professional from each institution was in charge of making the recruitment and be the direct contact with the first author. A total of 40 people from the 5 units were informed about the research project. Ultimately, 30 participants, 7 from Osonament, 7 from Institut Pere Mata, 7 from El Far, 5 from La Muralla, and 4 from Alterarte, agreed to take part in the study. All participants provided written consent. To maintain confidentiality and ensure data protection, participants' names were anonymized. Participants were included if they were: 1) aged 18 or above; 2) participating in the 17th Artistic Couple edition; 3) diagnosed with a mental health diagnosis; 4) linked in one of the network institutions; and 5) willing to participate and capable of understanding verbal and written Catalan or Spanish language.
2.3. Ethical Considerations
All participants provided written consent prior to their involvement in the study. The first author managed and securely stored the data, with all documentation archived by the institution overseeing the research. To protect confidentiality, participants' names were anonymized, ensuring compliance with data protection protocols. Participants could withdraw from study at any time without repercussions. The use of the Photovoice method emphasized the need to safeguard participants and upholding ethical standards, particularly when employing visual methods that involve personal disclosure. The research underscored the importance of creating a safe environment and adhering to ethical guidelines throughout the process.
2.4. Data Collection
Data were collected in three phases. At the outset of the project (Phase 1), the first author met with participants at each mental health institution involved. Meetings were held in private rooms, with support from institutional professionals provided when needed. Each participant received an anonymized participant file coded to ensure confidentiality.
Questionnaires were completed in small groups of three to four people. While the questionnaires were self-administered, the first author was present to answer any questions or address doubts. Each initial meeting lasted approximately 60–70 minutes. Participants completed a questionnaire package consisting of the following: Sociodemographic information and PROMs: The Questionnaire about the Process of Recovery (QPR) [43]: A 15-item psychometric tool validated in Spanish [44]; Recovery Assessment Scale—Domains and Stages (RAS-DS) [45]: A 38-item Spanish version [46]; European Quality of Life-5 Dimensions (EQ-5D) [47]: A Spanish adaptation [48]; Ryff Psychological Well-being Scale (PWB) [49]: A 39-item Spanish adaptation [50]; and Internalized Stigma of Mental Illness Inventory (ISMI) [51]: A 29-item Spanish adaptation [52].
At the end of the first meeting, the first author collaborated with participants to schedule the next meeting. At this point, Osonament, Alterarte, and Institut Pere Mata began the Photovoice intervention, each forming a unique group. With El Far and La Muralla, challenges in finding joint meeting spaces arose. To accommodate this, the data collection method was adapted in collaboration with institutional professionals, allowing participants to engage in the qualitative part. The first author conducted individual semi-structured interviews with participants from El Far and two focus groups with La Muralla participants.
The Photovoice intervention (Phase 2) involved a series of meetings guided by the study protocol, during which participants were asked to take photos of their daily lives based on proposed themes. These photos could depict objects, places, situations, and more. Groups discussed whether identifiable images of people could be included and agreed that such photos could be used with the explicit consent of those depicted. Participants committed to respecting and protecting the data generated in the group.
The first author offered cameras for participants to use, but all chose to use their own smartphones. Before each session, the first author collected and uploaded participants’ photos to a secure computer and printed them for use in discussions. Participants were encouraged to provide titles and short descriptions for their photos if desired. The groups were guided using a modified SHOWED prompt [53], which serves as a question guide. Sessions were scheduled collaboratively with participants.
All Photovoice sessions lasted 1–2 hours and were conducted in rooms provided by the institutions, equipped with necessary materials (e.g., tables, chairs, blackboards, and artistic supplies). At the end of the meetings, participants completed a satisfaction questionnaire. All sessions were audio-recorded and transcribed verbatim with prior consent from participants. The first author also took detailed notes during the sessions to document observations.
The last phase (Phase 3) encompassed the administration of the same standardized questionnaires from phase 1. First author also collected a self-developed survey asking the satisfaction of participants in their Artistic Couples’ experience. Finally, a research self-made Patient-Reported Experience Measures (PREMs) was assembled. Both, the satisfaction survey and measure of experience were anonymized, and no participant codes were linked to responses.
2.5. Data Analysis
Qualitative data obtained from the Photovoice process were analysed using Thematic Analysis following Braun and Clarke’s approach [54]. ATLAS.TI 24 was the software used to analyze qualitative data. Once the data were transcribed, the first author read and re-read the data to become familiar with the information. By identifying text fragments, codes were generated. These codes formed the basis for identifying patterns and themes in the text, allowing for the systematic organization of information. Second and third author, conducted a second coding. Then a general revision of codes generated was done. Afterwards, codes were grouped into categories, which were then consolidated into broader themes, allowing the researchers to classify and link common categories. Finally, authors refined and reviewed the emerging themes.
A quantitative analysis was conducted using SPSS 29.0.2.0, incorporating various statistical approaches to explore the data. A descriptive analysis was performed to characterize the variables and provide an overview of the sample. Paired data analysis was applied to assess changes in key variables before and after the intervention. Additionally, subgroup analyses were conducted to identify potential differences among participant groups. Finally, a correlation analysis was performed. The process was reviewed and refined by co-authors.
3. Results
3.1. Sociodemographic Data of Participants
A final sample of 30 participants (Table 1) was included in the study. An equal number of women (n=15, range 18-65 years, mean 44.13 years, sd=15.49) and men (n=15, range 22-59 years, mean 44.40, sd=13.21) participated in the study. Mental health diagnoses were classified according to the DSM-V handbook [55].
3.2. Qualitative Findings
Data analysis disclosed multiple and interconnected findings that align with the objectives of the study. The findings are organized into four main themes and subthemes (Table 2). Some narratives are presented without the photo to ensure confidentiality. Additionally, group conversations and complementary experiences were included. A satisfaction questionnaire assessing the Photovoice sessions (Table 3) is also presented.
3.2.1. Artmaking as an Artistic Couple
Creative and collaborative process
Participants emphasized the value of engaging in the creative process over focusing solely on the final product, aligning with participatory art principles. Participant 3 reflected: “Things do not appear; things are created,” highlighting the significance of the journey. Participant 4 described her experience:
“We started walking in the forest, collecting elements like pine cones and logs. From there, we built without a set plan, creating something with volume. I enjoyed the entire process—making the mold, turning it, and documenting it with my artistic partner’s photos.” (Figure 1).
Participants found enjoyment in the "making-of" aspect of their work. For example, some participants expressed a preference for the process of creating, enjoying even the “behind-the-scenes” moments, sometimes valuing it more than the final artwork itself. This reflects a broader appreciation of the journey, as well as the therapeutic impact of engaging deeply with the process, capturing moments, and recording the stages of creation, which offered a lasting reminder of their efforts and growth.
The dynamic between clients and local artists also revealed power imbalances, as the artists’ expertise sometimes overshadowed collaborative efforts. Yet, these dynamics highlighted the balance between technical guidance and creative expression.
To express, to explain
Art served as a tool for participants to express emotions and thoughts difficult to articulate verbally. Participant 1 noted: “Art expresses what you cannot with words,”. Through art, they express not only their feelings but also attempt to make sense of them, thereby facilitating both self-understanding and communication with those around them. Art acts as a mirror of their internal states, enabling others to understand their experiences more accurately.
For Participant 25, art became a channel to release emotions from a difficult work situation:
“My work is called incomprehension. I didn’t know how to capture it, but after brainstorming, I realized it reflected my struggle at work, where colleagues didn’t treat me well. That’s when the idea to capture incomprehension in a painting came to me.”
Art through nature
Some participants engaged in the artistic process within a natural setting, which became a significant space for reflection, inspiration, and connection. Participants integrated natural elements into their practices, highlighting the interplay between nature and creativity. During a group discussion, Participant 1 shared a landscape photo alongside Vincent van Gogh’s quote (Figure 2):
This sparked a debate about whether nature is art or merely a canvas for human creativity. While some, like Participant 1, viewed “nature as art,” others, like Participant 2, argued that “art is generated solely by human beings.”
3.2.2. Social Connections
A recurring theme among participants was the dynamic exchange of personal and artistic experiences within the artistic couple process. Some participants delved deeply into personal topics, while others maintained a primary focus on the art itself. These interactions often reflected the level of connection and trust developed between partners.
A conversation starts
Participant 23, the youngest participant at 19 years old, collaborated with two high school students (local artists) to create graffiti artwork. She described how their process began with a two-hour conversation, focusing on personal topics like dreams and emotions. This dialogue inspired their project, which explored adolescence through a character navigating emotional worlds such as anger, sadness, fear, euphoria, and shame. Participant 23 explained:
"When we started, we first got to know each other and spent two hours just talking. Only talking. We didn’t talk about the artwork; we talked about ourselves. We realized we had things in common. The topic of emotions came up, especially the world of dreams and the subconscious. The main idea was to create a character that went through different emotional worlds, representing adolescence. While we were sketching, I came up with the idea of 'teenmare,' which is a fusion of 'teenager' and 'nightmare. We depicted anger, which is a very common emotion among teenagers. Sadness was also included because it's a time when you begin to realize that life isn’t the world you thought it was when you were a child. Problems start to arise, and you have to decide what to do with your life. Fear was represented because adolescence brings many changes, and we have to try new things and choose our future. Fitting in with others also creates fear. Then there was euphoria and shame, the chains that stop you from being or doing what you want. I had never created an artistic piece with someone else before. I had always worked individually. Relationships are very difficult for me, but with them, it just clicked instantly. It was very easy, and everything went really well. I was nervous in this regard, but I came out delighted."
Their conversations laid the foundation for trust, collaboration, and creativity, blending personal insights with artistic expression to address the transitional challenges of adolescence.
To share with my artistic couple
Interactions between participants often extended beyond their artistic projects, fostering deeper personal connections. Such exchanges created spaces for trust and understanding. However, they also highlighted challenges. Participant 21 recounted an initial conflict with her partner, who treated her unequally due to her mental health:
“I said, ‘No, we are equal.’ People are not bad; they are ignorant.”
By addressing the comment directly, she fostered mutual respect, concluding: “The process went very well, and now we are friends.” This moment underscores the importance of open communication in challenging stigma and promoting understanding within partnerships.
Solitude
Participants reflected on solitude as both a challenge and an opportunity for growth. While some struggled with being alone, they also found it could foster creativity and self-expression. Several participants reflected on the role of solitude in their recovery, with some struggling to cope with it while others found it a source of creative inspiration. For some, solitude became a companion that fostered artistic expression and personal reflection. However, the Artistic Couples project provided a space to counteract loneliness by fostering social connections through shared creative experiences. Collaborative art-making not only strengthened participants' sense of belonging but also enhanced their mental well-being, offering a meaningful way to engage with others and the artistic community.
3.2.3. Understanding Mental Health Recovery
Mental health recovery is a deeply personal and multifaceted journey that intertwines emotional, social, and creative dimensions. The outcomes of this project reveal how participants navigated their individual paths, using art and meaningful activities as tools for self-expression, empowerment, and connection. Through their experiences, we gain insight into the complexities of recovery, from overcoming stigma and personal struggles to rediscovering identity and finding joy in everyday moments.
Overcoming my current situation
Participant 2 reflected on his lifelong relationship with music, sharing a photograph of the iconic His Master’s Voice logo, which holds personal significance from his time working at RCA Victor (Figure 3). He explained:
“Music was the reason why they stigmatized and damaged my brain. But it’s also always been the center of my life.” As he grew older, personal circumstances distanced him from music. He shared, “I’ve really been a fish out of water for 15 years. That’s why it feels so good to be making music again and to have the whole studio set up. I feel like I am regaining my identity as a musician.” When he got the studio ready, he invited his artistic couple to work there. “And for me, this is a very, very significant aspect of my recovery because what I needed was to regain my artistic identity as a musician”.
Some participants experienced emotional challenges during their creative process. One participant was unable to complete their work due to personal reasons, while others had fewer meetings due to external circumstances.
“Don’t treat me this way”
Participant 22 shared her journey of coping with mental health stigma, using three symbolic photographs to illustrate her experiences. She recounted how her challenges began at 15 years old, with panic attacks, anxiety, and depression. Despite these struggles, she pursued her studies and career by “putting on a mask” to appear normal:
“Even when I was shattered inside, I would dress well, do my hair, put on makeup, and just carry on. Now, I know I have bipolar disorder, but it took me a long time to accept it.” Art became her refuge, “I use art to express my emotions and feelings but also as a way to entertain myself because I enjoy it.”. Her second photo, titled "Don’t Treat Me This Way," depicted a collage of stigmatizing phrases she had encountered, such as: “What you want is to avoid working” or “Others have it much worse than you”. In contrast, her third photo, "Get to Know Me First and Discover Who I Am," revealed empowering statements like: “I’m fun “, I want to make a difference” or “Ask me if you don’t understand”.
Reflecting on the Artistic Couples project, she acknowledged the sensitivity of participants but noted occasional moments of discomfort:
“They mean well, but it can still feel bad when they explain things as if you were a child.”
Her narrative highlights the dual role of art as a tool for self-expression and a means of confronting societal stigma, underscoring her resilience and the need for greater understanding.
Engaging in meaningful activities
Participants highlighted the importance of engaging in both artistic and non-artistic activities to support mental health recovery and provide meaningful ways to occupy their time. Examples included:
Listening to music: “Music makes me feel powerful emotions with every song I love,” said Participant 3, who chose colourful vinyl records to represent its impact (Figure 4).
Climbing: Participant 1 also described the exhilaration of a via ferrata: “It’s the adrenaline, feeling alive, and enjoying nature.”
Other activities: Archery, visiting museums, and spending time in nature were also mentioned as meaningful practices.
These activities not only provided enjoyment but also contributed to participants’ emotional well-being and connection to the world around them.
3.3. Quantitative Findings
The pre- and post-intervention analysis provide insights into the project's impact on participants' mental health recovery, quality of life, and self-stigma (Table 4). Seventeen out of thirty participants completed the questionnaires, while the remaining participants did not complete the test due to difficulties in understanding it. Moreover, a satisfaction questionnaire assessing participants' experiences in the project (Table 5) and a measure of PREMs (Table 6) were included. It is the latter that highlights the high levels of pleasure and well-being generated by the experience received in the research. Although overall recovery as measured by the QPR and RAS-DS showed no statistically significant changes, the 'Connecting and Belonging' subdomain of the RAS-DS revealed a notable improvement (t= -2.51, p=0.023), suggesting that participants experienced increased social integration and support. The overall recovery as measured by the RAS-DS (Recovery Assessment Scale—Domains and Stages) showed an increase in mean scores from 111.18 (SD = 19.69) pre-intervention to 116.71 (SD = 17.82) post-intervention, with the median rising from 113 to 118. Although the improvement was not statistically significant (t = -1.525, p=0.147), this increase in scores suggests a positive trend in participants’ perceived recovery. Regarding quality of life and psychological well-being, no significant changes were observed in the overall EQ-5D and PWB scores. Lastly, self-stigma levels, as assessed by the ISMI, remained stable across all domains, indicating that while stigma reduction was not significant, the intervention did not exacerbate negative self-perceptions.
The analysis of the RAS-DS 'Connecting and Belonging' subscale revealed significant differences in recovery trajectories based on gender. Women demonstrated a statistically significant improvement, with mean scores increasing from 20.20 (SD = 3.39) pre-intervention to 22.30 (SD = 3.23) post-intervention (t = -2.85, p = 0.019) (Figure 5). In contrast, men showed no significant change, with mean scores shifting only slightly from 21.00 (SD = 3.16) to 21.43 (SD = 3.36) (t = -0.55, p = 0.604). The direct comparison of improvements between genders yielded no statistically significant differences (t = -1.55, p = 0.142), though women exhibited a higher mean change (2.10 for women vs. 0.43 for men). Age-based analyses, including an ANOVA comparing three age subgroups (18–30, 31–50, and 51+), did not show statistically significant differences in recovery scores between groups (F = 0.45, p = 0.649 for all participants; F = 1.46, p = 0.295 for women only). Notably, older women (51+) showed the highest mean improvement (4.50, SD = 3.54), whereas younger and middle-aged women (18–30 and 31–50) exhibited smaller changes (1.50, SD = 2.08, and 1.50, SD = 1.73, respectively). While these findings were not statistically significant, they suggest that age and gender may influence recovery experiences and warrant further exploration. The results show a low positive correlation between women's age and improvement in the subscale (r=0.278), but it is not statistically significant (p=0.436), indicating that there is not enough evidence to confirm a relationship between these variables in this sample.
The one-way ANOVA showed no significant differences in improvement across diagnostic categories (F = 1.264, p = 0.327). However, the Depressive Disorders group exhibited the highest improvement trend (M = 3.00).
4. Discussion
This mixed-methods study explored how the Artistic Couples project influences participants' mental health recovery, psychological well-being, and self-stigma while also examining their experiences, satisfaction, and the opportunities created through participation. Photovoice emerged as a central methodology, enabling participants to take an active role in the project's development and offering a platform to express their emotions and insights [56]. Through their photographs and group discussions, participants highlighted key themes, such as artmaking as a collaborative process, social connections, and their journey toward understanding mental health recovery. It is been stablished that mental health recovery concepts are effectively communicated by visual-arts based research [57,58].
Participatory art activities such Artistic Couples encourage individuals to express themselves creatively, promoting autonomy in self-expression [59]. The findings highlight those participants valued the creative process itself, emphasizing the journey over the final product. This aligns with participatory art principles, where making, experimenting, and collaborating become central to personal and collective growth. Art also functioned as a powerful means of communication, allowing participants to externalize emotions and experiences that were difficult to verbalize [60]. Whether through visual metaphors, symbolic representations, or the physical act of creating, art provided a language of expression beyond words. Art can contribute to reduce stigma associated with mental health [1,61], as exemplified by participant 22, who directly confronted stigma with her artistic couple. However, this study did not find statistically significant changes in self-stigma.
Furthermore, nature emerged as a significant element in the artistic process, serving as both inspiration and a reflective space. The integration of natural materials and outdoor settings enriched participants’ creative experiences, reinforcing the interplay between artistic creation and environmental connection. However, this relationship between nature and artistic expression requires further exploration [62], particularly in understanding how natural spaces shape and enhance the self-perception of individuals engaged in creative practices.
Quantitative results revealed that, while overall recovery and well-being measures (RAS-DS and PWB) showed trends toward improvement, only the "Connecting and Belonging" subscale of the RAS-DS demonstrated statistically significant changes (t = -2.51, p = 0.023), suggesting enhanced social integration and support. Gender-specific analyses showed that women experienced significant improvement in this domain (t = -2.85, p = 0.019), whereas men did not show significant changes. These findings underline the importance of targeted approaches to address gender-specific needs in community-based art interventions. Studies emphasize the need to pay particular attention to addressing the gender gap in mental health services [28]). However, the small sample size limits the robustness of these quantitative results, which should be interpreted with caution. Although some quantitative results did not show statistical significance, this does not necessarily indicate a lack of impact from the intervention. The absence of significance may be due to the small sample size or the subjective nature of the mental health recovery process, which may not be easily captured through standardized measures. However, the qualitative findings clearly demonstrate a positive experience among participants, with narratives highlighting improvements in social connection, self-expression, and emotional well-being. Solitude, a recurring theme, was viewed both as a challenge and an opportunity for introspection and personal growth. Aligned with prior studies suggesting that engaging in social interactions during art activities helps reduce feelings of loneliness [63].
The results of this study align with the CHIME framework [17], which highlights Connectedness, Hope and optimism, Identity, Meaning, and Empowerment as essential components of mental health recovery. Participants reported emotional release, self-expression, and positive experiences, contributing to a sense of hope and optimism about their recovery journey. The meaningful engagement in artmaking fostered a sense of purpose and value. Moreover, using PROMs allowed to focus on patient centred needs, fostering empowerment, and providing a sense of meaning, aligning with a holistic mental health approach [64]. Self-perception emerged as a cornerstone for reclaiming autonomy and reinforcing self-worth, ultimately supporting recovery outcomes.
Satisfaction surveys underscored participants' positive experiences with Artistic Couples, with high ratings for activity functionality (mean = 8.9, SD = 1.53) and overall satisfaction (mean = 9, SD = 1.01). Participants praised the opportunity to share meaningful moments, explore diverse forms of art, and connect with others, despite challenges like scheduling conflicts and occasional mismatches with artistic partners. The project’s ability to create a supportive and inclusive environment was also reflected in the positive feedback regarding the research process (PREMs), with all participants indicating they were treated respectfully and found the study easy to understand.
4.1. Practical Implications
Art can play a key role in improving mental health, well-being, and social participation [65]). This study highlights the potential for integrating participatory art interventions, such as the Artistic Couples project, into mental health recovery programs to enhance self-expression, social connection, and emotional well-being. The significant improvement observed in women emphasizes the importance of considering gender-specific approaches, while the use of natural settings and collaborative art processes suggests additional therapeutic benefits. Empowering participants by involving them as co-creators, rather than passive recipients, fosters a sense of ownership and resilience in their recovery journey. Besides, a photovoice exhibition was held to address community population. Addressing logistical and power dynamics challenges, such as ensuring equitable relationships between participants and professional artists, can further enhance program effectiveness. A key consideration is the potential for emotional vulnerability and psychological distress when participants take part in the project. Support systems within art partnerships are essential to help navigate emotional journeys safely. This includes the presence of mental health professionals or peer support networks [66,67], where experienced participants provide guidance and assistance.
4.2. Study Limitations
The study presents several limitations that should be considered when interpreting the results. First, the lack of larger sample size and a control group, which was initially planned in the study protocol, limited the ability to compare the intervention's effects against a non-intervention scenario. This decision was made due to the insufficient number of participants meeting the inclusion criteria. Additionally, exploring the long-term effects of such participatory art interventions may provide further insights into their potential for sustained impact on mental health recovery, while also considering diagnostic categories. Second, the sample size was too small to ensure that the statistical significance observed in the quantitative analyses is robust enough to definitively confirm the intervention’s impact. However, the results suggest a trend toward stabilization or even improvement. Third, the findings may be influenced by the specific sociocultural context of the participants, as they were all from a specific geographic region. This may limit the generalizability of the results. Finally, logistical challenges arose as the first author was responsible for leading and supervising all photovoice sessions and administering questionnaires across various geographic areas. This could have affected the consistency of data collection.
5. Conclusions
This study highlights the impact of participatory art interventions in mental health recovery, particularly through the Artistic Couples project. Findings demonstrate that engaging in creative collaboration fosters self-expression, social connectedness, and a renewed sense of identity, aligning with the CHIME framework. Notably, significant improvements in social integration were observed, especially among women, reinforcing the importance of gender-sensitive approaches. While overall recovery and self-stigma measures showed no statistical significance, qualitative insights reveal the deep personal impact of artistic engagement. Addressing power dynamics in collaborations and integrating nature-based elements may further enhance the therapeutic benefits of such initiatives. Despite limitations such as sample size constraints and the lack of a control group, this study underscores the need for sustained, inclusive, and structured art-based programs within mental health services to promote holistic well-being and long-term recovery.
Author Contributions
Conceptualization, J.C.C., R.R.S. and S.S.A.; Methodology, J.C.C., R.R.S. and S.S.A.; Validation, R.R.S. and S.S.A..; Formal Analysis, J.C.C., R.R.S., S.S.A. and JM.S.L.; Investigation, J.C.C., R.R.S. and S.S.A.; Resources, R.R.S. and S.S.A.; Writing – Original Draft Preparation, J.C.C.; Writing – Review & Editing, R.R.S., JM.S.L. and S.S.A.; Visualization, J.C.C. and S.S.A.; Supervision, R.R.S. and S.S.A.; Project Administration, S.S.A.; Funding Acquisition, S.S.A. All authors have read and agreed to the published version of the manuscript.
Funding
This research was financially supported by Doctorats Industrials by the Agency for the Management of University and Research Grants (AGAUR) (grant number 2021 DI 90).
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki, and approved by the Clinical Research Ethics Committee of the Osona Foundation for Research and Education Health (CEIC Code: 2022212; Own code: PR344) on 25/10/2022.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Acknowledgments
We would like to extend our gratitude to all the participants and members of the project team who have contributed to this study. Special thanks to Psychopedagogical Medical Center Foundation of Osona (Osonament) and the University of Vic-Central University of Catalunya.
Conflicts of Interest
The authors declare no conflict of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| PROMs | Patient-Reported Outcomes Measures |
| QPR | The Questionnaire bout the Process of Recovery |
| RAS-DS | Recovery Assessment Scale—Domains and Stages |
| EQ-5D | European Quality of Life-5 Dimensions |
| PWB | Ryff Psychological Well-being Scale |
| ISMI | Internalized Stigma of Mental Illness Inventory |
| PREMs | Patient-Reported Experience Measures |
References
- Fancourt, D.; Finn, S. What is the evidence on the role of the arts in improving health and well-being? A scoping review. Health Evid. Netw. Synth. Rep. World Health Organization: Geneva, Switzerland, 2019. Available online: https://apps.who.int/iris/handle/10665/329834. 2019, 67. [Google Scholar]
- Gómez-Restrepo, C.; Godoy-Casasbuenas, N.; Ortiz-Hernández, N.; Bird, V.; Acosta, M.P.J.; Uribe-Restrepo, J.M.; Sarmiento, B.A.M.; Steffen, M.; Priebe, S. Role of the arts in the life and mental health of young people that participate in artistic organizations in Colombia: A qualitative study. BMC Psychiatry 2022, 22, 1–12. [Google Scholar] [CrossRef]
- Hui, A.; Stickley, T.; Stubley, M.; Baker, F. Project eARTh: Participatory arts and mental health recovery, a qualitative study. Perspect. Public Health 2019, 139, 296–302. [Google Scholar] [CrossRef]
- World Health Organization. Transforming Mental Health for All—Executive Summary; World Health Organization: Geneva, Switzerland, 2022; Available online: https://www.who.int/publications/i/item/9789240050860.
- Daykin, N.; de Viggiani, N.; Pilkington, P.; Moriarty, Y. Music making for health, well-being and behaviour change in youth justice settings: A systematic review. Health Promot. Int. 2013, 28, 197–210. [Google Scholar] [CrossRef] [PubMed]
- Van der Vaart, G. Insights and inspiration from explorative research into the impacts of a community arts project. In Springer eBooks; Springer: Cham, Switzerland, 2021; pp. 205–227. [Google Scholar] [CrossRef]
- Tew, J.; Ramon, S.; Slade, M.; Bird, V.; Melton, J.; Le Boutillier, C. Social factors and recovery from mental health difficulties: A review of the evidence. Br. J. Soc. Work 2012, 42, 443–460. [Google Scholar] [CrossRef]
- Nitzan, A.; Orkibi, H. “We’re All in the Same Boat” – The Experience of People With Mental Health Conditions and Non-clinical Community Members in Integrated Arts-Based Groups. Front. Psychol. 2021, 12, 661831. [Google Scholar] [CrossRef] [PubMed]
- Stickley, T.; Hui, A. Social prescribing through arts on prescription in a UK city: Participants’ perspectives (part 1). Public Health 2012, 126, 574–579. [Google Scholar] [CrossRef]
- Corrigan, P.W.; Watson, A.C. Understanding the impact of stigma on people with mental illness. World Psychiatry 2002, 1, 16–20. [Google Scholar]
- Anthony, W.A. Recovery from mental illness: The guiding vision of the mental health service system in the 1990s. Psychosoc. Rehabil. J. 1993, 16, 11–23. [Google Scholar] [CrossRef]
- Roe, D.; Mashiach-Eizenberg, M.; Lysaker, P.H. The relation between objective and subjective domains of recovery among persons with schizophrenia-related disorders. Schizophr. Res. 2011, 131, 133–138. [Google Scholar] [CrossRef]
- Shepherd, G.; Boardman, J.; Slade, M. Making Recovery a Reality; Sainsbury Centre for Mental Health: London, UK, 2008. [Google Scholar]
- Slade, M.; Amering, M.; Farkas, M.; Hamilton, B.; O’Hagan, M.; Panther, G.; Perkins, R.; Shepherd, G.; Tse, S.; Whitley, R. Uses and abuses of recovery: Implementing recovery-oriented practices in mental health systems. World Psychiatry 2014, 13, 12–20. [Google Scholar] [CrossRef] [PubMed]
- Jacob, S.; Munro, I.; Taylor, B.J. Mental health recovery: Lived experience of consumers, carers, and nurses. Contemp. Nurse 2015, 50, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Leamy, M.; Foye, U.; Hirrich, A.; et al. A systematic review of measures of the personal recovery orientation of mental health services and staff. Int. J. Ment. Health Syst. 2023, 17, 33. [Google Scholar] [CrossRef]
- Leamy, M.; Bird, V.; Le Boutillier, C.; Williams, J.; Slade, M. Conceptual framework for personal recovery in mental health: Systematic review and narrative synthesis. Br. J. Psychiatry 2011, 199, 445–452. [Google Scholar] [CrossRef]
- van Weeghel, J.; van Zelst, C.; Boertien, D.; Hasson-Ohayon, I. Conceptualizations, assessments, and implications of personal recovery in mental illness: A scoping review of systematic reviews and meta-analyses. Psychiatr. Rehabil. J. 2019, 42, 169–181. [Google Scholar] [CrossRef] [PubMed]
- Bird, V.; Leamy, M.; Tew, J.; Boutillier, C.L.; Williams, J.; Slade, M. Fit for purpose? Validation of a conceptual framework for personal recovery with current mental health consumers. Aust. N. Z. J. Psychiatry 2014, 48, 644–653. [Google Scholar] [CrossRef]
- Vogel, J.S.; Bruins, J.; Halbersma, L.; Lieben, R.J.; De Jong, S.; Van Der Gaag, M.; Castelein, S. Measuring personal recovery in people with a psychotic disorder based on CHIME: A comparison of three validated measures. Int. J. Ment. Health Nurs. 2020, 29, 808–819. [Google Scholar] [CrossRef]
- Keet, R.; de Vetten-McMahon, M.; Shields-Zeeman, L.; et al. Recovery for all in the community; position paper on principles and key elements of community-based mental health care. BMC Psychiatry 2019, 19, 174. [Google Scholar] [CrossRef]
- Slade, M.; Leamy, M.; Bacon, F.; Janosik, M.; Le Boutillier, C.; Williams, J.; Bird, V. International differences in understanding recovery: Systematic review. Epidemiol. Psychiatr. Sci. 2012, 21, 353–364. [Google Scholar] [CrossRef]
- Sánchez-Guarnido, A.J.; Ruiz-Granados, M.I.; Garrido-Cervera, J.A.; Herruzo, J.; Herruzo, C. Implementation of the Recovery Model and Its Outcomes in Patients with Severe Mental Disorder. Healthcare 2024, 12, 952. [Google Scholar] [CrossRef]
- Slade, M.; Longden, E. Empirical evidence about recovery and mental health. BMC Psychiatry 2015, 15, 285. [Google Scholar] [CrossRef] [PubMed]
- Reed, N.P.; Josephsson, S.; Alsaker, S. A narrative study of mental health recovery: Exploring unique, open-ended and collective processes. Int. J. Qual. Stud. Health Well-being 2020, 15, 1747252. [Google Scholar] [CrossRef]
- Clift, S.; Camic, P.M. Oxford Textbook of Creative Arts, Health, and Well-Being: International Perspectives on Practice, Policy, and Research; Oxford University Press: Oxford, UK, 2016. [Google Scholar]
- Crawford, P.; Lewis, L.; Brown, B.; Manning, N. Creative practice as mutual recovery in mental health. Ment. Health Rev. J. 2013, 18, 55–64. [Google Scholar] [CrossRef]
- Goodman-Casanova, J.M.; Guzman-Parra, J.; Mayoral-Cleries, F.; Cuesta-Lozano, D. Community-based art groups in mental health recovery: A systematic review and narrative synthesis. J. Psychiatr. Ment. Health Nurs. 2024, 31, 158–173. [Google Scholar] [CrossRef]
- Tymoszuk, U.; Spiro, N.; Perkins, R.; Mason-Bertrand, A.; Gee, K.; Williamon, A. Arts engagement trends in the United Kingdom and their mental and social wellbeing implications: HEartS Survey. PLoS ONE 2021, 16, e0246078. [Google Scholar] [CrossRef] [PubMed]
- Bungay, H.; Vella-Burrows, T. The effects of participating in creative activities on the health and well-being of children and young people: A rapid review of the literature. Perspect. Public Health 2013, 133, 44–52. [Google Scholar] [CrossRef]
- Cases-Cunillera, J.; del Río Sáez, R.; Vila-Mumbrú, N.; Simó-Algado, S. Artistic Couples: Creative experiences for mental health (2006-2023). Arteterapia 2024, 19, e91702. [Google Scholar] [CrossRef]
- Cases-Cunillera, J.; Del Río Sáez, R.; Simó-Algado, S. Personal narratives from a mental health community art-based project: Insights from collaborative creation. Qual. Health Res. Advance online publication. 2024. [Google Scholar] [CrossRef]
- Creswell, J.W.; Plano Clark, V.L. Designing and Conducting Mixed Methods Research, 3rd ed.; SAGE Publications: Thousand Oaks, CA, USA, 2018. [Google Scholar]
- Wang, C.; Burris, M.A. Photovoice: Concept, methodology, and use for participatory needs assessment. Health Educ. Behav. 1997, 24, 369–387. [Google Scholar] [CrossRef]
- Anderson Clarke, L.M.; Warner, B. Exploring recovery perspectives in individuals diagnosed with mental illness. Occup. Ther. Ment. Health 2016, 32, 400–418. [Google Scholar] [CrossRef]
- Wang, C.; Burris, M.A. Empowerment through photo novella: Portraits of participation. Health Educ. Q. 1994, 21, 171–186. [Google Scholar] [CrossRef] [PubMed]
- Dulek, E.B.; Stein, C.H. The way I see it: Older adults with mental illness share their views of community life using Photovoice. Community Ment. Health J. 2024, 60, 457–469. [Google Scholar] [CrossRef]
- Golden, T. Reframing Photovoice: Building on the method to develop more equitable and responsive research practices. Qual. Health Res. 2020, 30, 960–972. [Google Scholar] [CrossRef]
- Han, C.; Oliffe, J. Photovoice in mental illness research: A review and recommendations. Health 2016, 20, 110–126. [Google Scholar] [CrossRef] [PubMed]
- Charlton, J. Nothing About Us Without Us: Disability Oppression and Empowerment; University of California Press: Berkeley, CA, USA, 1998. [Google Scholar]
- Wang, C.C.; Morrel-Samuels, S.; Hutchison, P.M.; Bell, L.; Pestronk, R.M. Flint Photovoice: Community building among youths, adults, and policymakers. Am. J. Public Health 2004, 94, 911–913. [Google Scholar] [CrossRef] [PubMed]
- Budig, K.; Diez, J.; Conde, P.; Sastre, M.; Hernán, M.; Franco, M. Photovoice and empowerment: Evaluating the transformative potential of a participatory action research project. BMC Public Health 2018, 18, 432. [Google Scholar] [CrossRef]
- Law, H.; Neil, S.T.; Dunn, G.; Morrison, A.P. Psychometric properties of the questionnaire about the process of recovery (QPR). Schizophr. Res. 2014, 156, 184–189. [Google Scholar] [CrossRef]
- Goodman-Casanova, J.M.; Cuesta-Lozano, D.; García-Gallardo, M.; Durán-Jiménez, F.J.; Mayoral-Cleries, F.; Guzmán-Parra, J. Measuring mental health recovery: Cross-cultural adaptation of the 15-item Questionnaire about the Process of Recovery in Spain (QPR-15-SP). Int. J. Ment. Health Nurs. 2022, 31, 650–664. [Google Scholar] [CrossRef]
- Hancock, N.; Scanlan, J.N.; Honey, A.; Bundy, A.C.; O’Shea, K. Recovery assessment scale–domains and stages (RAS-DS): Its feasibility and outcome measurement capacity. Aust. N. Z. J. Psychiatry 2015, 49, 624–633. [Google Scholar] [CrossRef]
- Hancock, N. The University of Sydney. Recovery Assessment Scale – Domains and Stages (RAS-DS) – Research Version 3 [Spanish translation by Daniela Fuentes O. & Sofía Astorga P., 2018]. Available online: https://ras-ds.net.au/wp-content/uploads/2018/10/RAS-DS_2016_Spanish.pdf.
- The EuroQol Group. EuroQol—A new facility for the measurement of health-related quality of life. Health Policy 1990, 16, 199–208. [Google Scholar] [CrossRef]
- Herdman, M.; Badia, X.; Berra, S. The EuroQol-5D: A simple alternative for measuring health-related quality of life in primary care. Aten. Primaria 2001, 28, 425–430. [Google Scholar] [CrossRef] [PubMed]
- Ryff, C.D.; Keyes, C.L.M. The structure of psychological well-being revisited. J. Pers. Soc. Psychol. 1995, 69, 719–727. [Google Scholar] [CrossRef] [PubMed]
- Díaz, D.; Rodríguez-Carvajal, R.; Blanco, A.; Moreno-Jiménez, B.; Gallardo, I.; Valle, C.; van Dierendonck, D. Spanish adaptation of the Psychological Well-Being Scales (PWBS). Psicothema 2006, 18, 572–577. Available online: https://reunido.uniovi.es/index.php/PST/article/view/8474 (accessed on 10 February 2024).
- Boyd, J.E.; Adler, E.P.; Otilingam, P.G.; Peters, T. Internalized stigma of mental illness (ISMI) scale: A multinational review. Compr. Psychiatry 2014, 55, 221–231. [Google Scholar] [CrossRef] [PubMed]
- Bengochea-Seco, R.; Arrieta-Rodríguez, M.; Fernández-Modamio, M.; Santacoloma-Cabero, I.; De Tojeiro-Roce, J.G.; García-Polavieja, B.; Santos-Zorrozúa, B.; Gil-Sanz, D. Adaptation into Spanish of the Internalised Stigma of Mental Illness scale to assess personal stigma. Rev. Psiquiatr. Salud Ment. 2018, 11, 244–254. [Google Scholar] [CrossRef]
- Hergenrather, K.C.; Rhodes, S.D.; Cowan, C.A.; Bardhoshi, G.; Pula, S. PhotoVoice as community-based participatory research: A qualitative review. Am. J. Health Behav. 2009, 33, 686–698. [Google Scholar] [CrossRef]
- Braun, V.; Clarke, V. Using thematic analysis in psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Publishing: Washington, DC, USA, 2013. [Google Scholar] [CrossRef]
- Rai, S.; Gurung, D.; Kohrt, B. The PhotoVoice method for collaborating with people with lived experience of mental health conditions to strengthen mental health services. Cambridge Prisms Glob. Ment. Health 2023, 10, e80–1. [Google Scholar] [CrossRef]
- Jay, E.; Patterson, C.F.; Fernandez, R.; Moxham, L. Experiences of recovery among adults with a mental illness using visual art methods: A systematic review. J. Psychiatr. Ment. Health Nurs. 2022, 30, 361–374. [Google Scholar] [CrossRef]
- Vansteenkiste, T.; Morrens, M.; Westerhof, G.J. Images of recovery: A PhotoVoice study on visual narratives of personal recovery in persons with serious mental illness. Community Ment. Health J. 2021, 57, 1151–1163. [Google Scholar] [CrossRef]
- Gorny-Wegrzyn, E.; Perry, B. Creative Art: Connection to Health and Well-Being. Open J. Soc. Sci. 2022, 10, 290–303. [Google Scholar] [CrossRef]
- Boumans, J.; Oderwald, A.; Kroon, H. Self-perceived relations between artistic creativity and mental illness: A study into lived experiences. Front. Public Health 2024, 12, 1353757. [Google Scholar] [CrossRef] [PubMed]
- Lamb, J. Creating change: Using the arts to help stop the stigma of mental illness and foster social integration. J. Holist. Nurs. 2009, 27, 57–65. [Google Scholar] [CrossRef] [PubMed]
- Zaragoza Bernal, J.M. Mental health, subjective experiences and environmental change. Med. Humanit. 2024, 50, 417–420. [Google Scholar] [CrossRef]
- Dadswell, A.; Wilson, C.; Bungay, H.; Munn-Giddings, C. The role of participatory arts in addressing the loneliness and social isolation of older people: A conceptual review of the literature. J. Arts Communities 2017, 9, 109–128. [Google Scholar] [CrossRef] [PubMed]
- Garrido-Cervera, J.A.; Ruiz-Granados, M.I.; Cuesta-Vargas, A.I.; Sánchez-Guarnido, A.J. Patient-reported outcome measures (PROMs) for recovery in mental health: A scoping review. Community Ment. Health J. Advance online publication. 2024. [Google Scholar] [CrossRef]
- Simó, S. Unveiling the Power of Art and Culture: Enhancing Mental Health and Social Engagement in the South Mediterranean with Insights from Catalonia; Euro-Mediterranean Economists Association (EMEA): Barcelona, Spain, 2024. [Google Scholar]
- Kim, S.-Y.; Kweon, Y.-R. The Poetry of Recovery in Peer Support Workers with Mental Illness: An Interpretative Phenomenological Analysis. Healthcare 2024, 12, 123. [Google Scholar] [CrossRef]
- Vigué, G.P.; Prieto, I.C.; Del Río Sáez, R.; Masana, R.V.; Algado, S.S. Training peer support workers in mental health care: A mixed methods study in Central Catalonia. Front. Psychiatry 2022, 13, 791724. [Google Scholar] [CrossRef]
Figure 1.
A photo from participant 4 used to describe her creative process, entitled “The mold”.

Figure 2.
A photo from participant 1 that entitled “Keep your love for nature, because it is the true way to understand art more and more”.
Figure 2.
A photo from participant 1 that entitled “Keep your love for nature, because it is the true way to understand art more and more”.

Figure 3.
Title: His Master’s Voice.
Figure 4.
Title: Plasticized emotions.

Figure 5.
Boxplot comparison of pre- and post-intervention scores (PRERASDS4 and POSTRASDS4) for men and women.
Figure 5.
Boxplot comparison of pre- and post-intervention scores (PRERASDS4 and POSTRASDS4) for men and women.
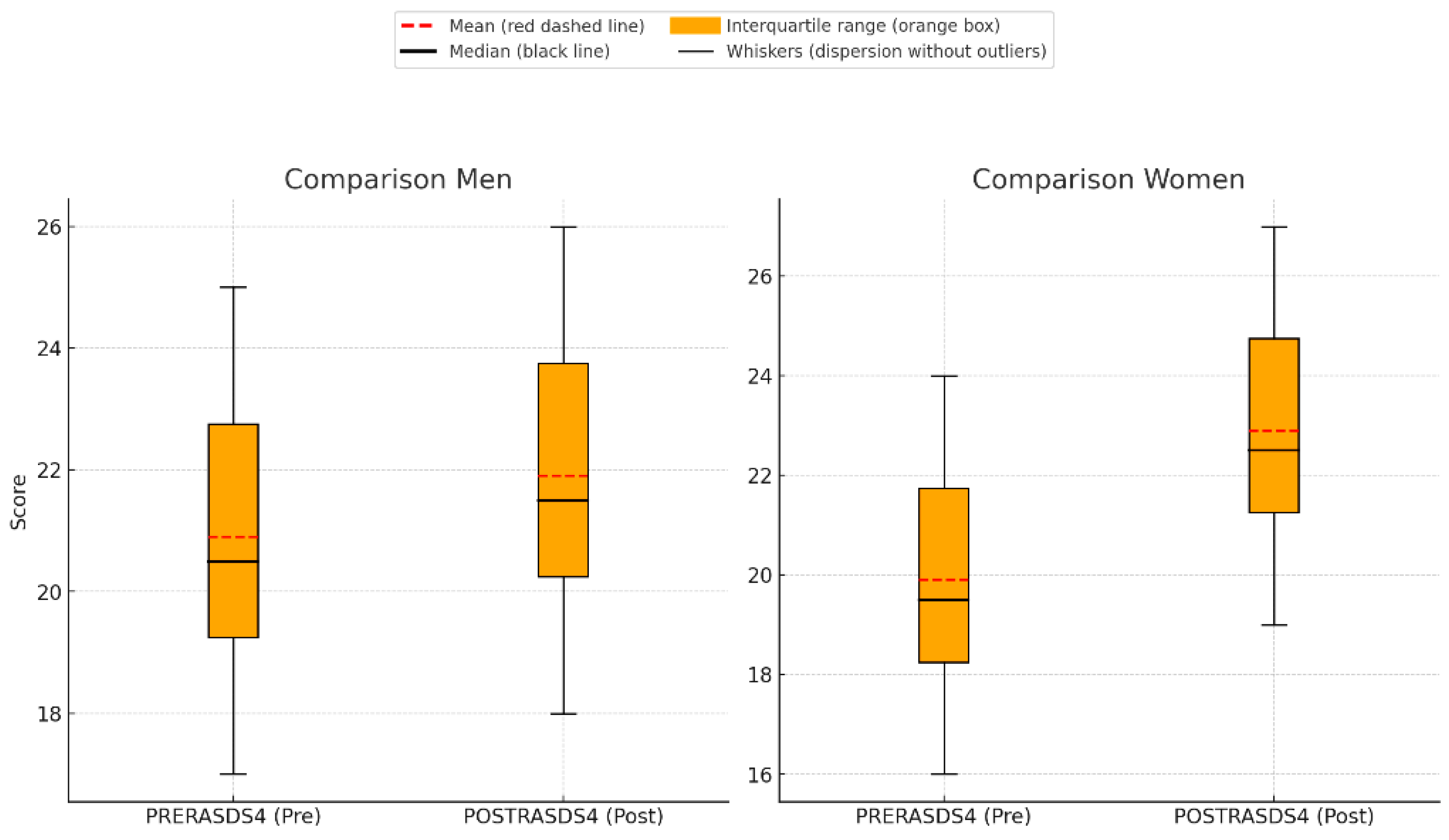

Table 1.
Study participants (N=30).
| Variables | N | % |
|---|---|---|
| Age (years) | ||
| 18-30 | 8 | 26.66 |
| 31-50 | 10 | 33.33 |
| 51-65 | 12 | 40 |
| Gender | ||
| Women | 15 | 50 |
| Men | 15 | 50 |
| Civil status | ||
| Single | 22 | 73.33 |
| Married | 3 | 10 |
| Divorced | 2 | 6.66 |
| Unspecified | 2 | 6.66 |
| Unmarried couple | 1 | 3.33 |
| Living with | ||
| My family | 18 | 60 |
| Alone | 7 | 23.33 |
| Supported household | 2 | 6.66 |
| In group | 2 | 6.66 |
| With partner | 1 | 3.33 |
| Academic training | ||
| University degree | 7 | 23.33 |
| Secondary education | 6 | 20 |
| Primary education | 5 | 16.66 |
| Advanced education | 4 | 13.33 |
| High school | 4 | 13.33 |
| Without studies | 2 | 6.66 |
| Third-cycle university studies | 1 | 3.33 |
| Unclassified | 1 | 3.33 |
| Job situation | ||
| Transitory/permanent incapacity | 12 | 42,85 |
| Unspecified | 8 | 28.57 |
| Unemployed (with or without subsidy) | 4 | 14.28 |
| In active (working) | 3 | 10.71 |
| Retired | 1 | 3.57 |
| Mental health diagnoses categories (main) | ||
| Schizophrenia Spectrum and Other Psychotic Disorders | 14 | 46.67 |
| Bipolar and Related Disorders | 7 | 23.33 |
| Depressive Disorders | 4 | 13.33 |
| Personality Disorder | 4 | 13.33 |
| Disruptive, Impulse-Control, and Conduct disorders | 1 | 3.33 |
| Institution (Region) | ||
| Osonament (Osona) | 7 | 23.33 |
| Institut Pere Mata (Tarragonès) | 7 | 23.33 |
| El Far (Vallès Oriental) | 7 | 23.33 |
| La Muralla (Tarragonès) | 5 | 16.66 |
| Alterarte (Maresme) | 4 | 13.33 |
| Specific service | ||
| Community Rehabilitation Service | 16 | 53.33 |
| Social Club: | 14 | 46.66 |
| Artistic discipline used in the project | ||
| Visual arts | 25 | 83.33 |
| Literary arts | 3 | 10 |
| Music | 1 | 3.33 |
| Applied arts | 1 | 3.33 |
Table 2.
Overarching themes, sub-themes and quotes from participants.
| Themes | Sub themes | Quotes |
|---|---|---|
| Artmaking as an artistic couple | Creative and collaborative process | “The final work, the result, is very important because it is what is seen, the visual aspect. But I believe that the meaning, the process, is equally important.” Participant 23 |
| "It also helps me relax, enjoy the process, and it's a moment we share—an hour and a half, two hours. And many times, we meet up and don’t even paint; we just go to have a chat." Participant 1 | ||
| To express, to explain | “It wasn't therapy for me, but a way to explain what happened to me or how I was inside. As a child, I didn’t express myself clearly, and they always said, ‘Get me a drawing.’” Participant 23 | |
| “For me, it’s about understanding myself and communicating what I do not understand about myself. I try to make sense of it and hope others can as well.” Participant 21 | ||
| “It helps me a lot to express, to externalize.” Participant 19 | ||
| Art through nature | “My process has been in a wonderful place, in the middle of nature. The calm and disconnection that I have had. For me, it has been a very beautiful and wonderful experience.” Participant 4 | |
| “Contact with nature is very healthy for me” Participant 30 | ||
| Social connections | A conversation starts | "We talked a bit about what we liked to paint or what we liked to express. I was in a process when Artistic Couples started where I felt overwhelmed. I thought, if I’m going to dedicate so much time to a project, to a piece, working with someone where it doesn’t just depend on me, I want it to be personal. And, in fact, that’s how it was." Participant 1 |
| To share with my artistic couple | "I think that when you have feeling and stick more you relax and end up talking about personal things. So, we talked about our things. They had nothing to do with ceramics. His life, my life, this happened to me, it happened to me the other..." Participant 4 | |
| "So now I really enjoy being in contact with my artistic couple and seeing that she adapts to what I do, and that what she suggests to expand my work also appeals to me. I mean, it's a very interesting and productive exchange." Participant 2 | ||
| Solitude | “Being an artistic couple helps me get through unwanted loneliness.” Participant 6 | |
| “The power of feeling connected to others… helps me grow. It’s therapy for me.” Participant 8 | ||
| “I meet more people, expand my circle of friends, and experiment.” Participant 19 | ||
| Understanding mental health recovery | Overcoming my current situation | “I tried to paint, but nothing came out. I was struggling and felt like I wasn’t making any progress. It was overwhelming, and I decided I wanted to stop. I felt very anxious.” Participant 24 |
| "I wanted to approach Artistic Couples in connection with my personal process. Like, how do I feel right now? I feel a bit like 'hear, see, and stay silent,' and I don’t want to feel that way." Participant 1 | ||
| "Don't treat me this way" | “My artistic couple told me, I had prejudices about how you would be, and, you’re just a very normal person.' That whole idea of normality—like, you have your studies 'Yes, yes, I do,' you have your family. So, just very normal. And cool, but I wasn’t expecting that." Participant 3 | |
| Engaging in meaningful activities | “I need to occupy my mind.” Participant 21 | |
| “When I pick up a book, I escape reality and enter a new one,” Participant 1 |
Table 3.
Photovoice sessions (16 sessions).
| Measures | Mean | Median | SD | |
|---|---|---|---|---|
| Participants' attendance sessions | 73.81% | 79.16% | 25.29% | |
| Photographs taken by each participant | 6.5 | 5 | 6.20 | |
| Satisfaction survey of each Photovoice session (52 answers) | ||||
| Quantitative part | Mean | Median | SD | Range (0 (low)-10 (high) |
| 1. Degree of functioning of the activity | 9.48 | 10 | 0.80 | 0-10 |
| 2. Timetable and duration of the activity | 9.15 | 10 | 1.19 | 0-10 |
| 3. Overall level of satisfaction | 9.48 | 10 | 0.92 | 0-10 |
| Qualitative part | Overarching themes | Quotes | ||
| 4. Strenghts | Social interaction and support,Empathy and sharing emotions, andLearning and discovery | "Being able to listen to the points of view of other participants and share opinions", "The empathy among attendees", "It ended up being a very pleasant and friendly group", "I really enjoy it when we get together as a group and exchange impressions, discovering things and places... That’s what I think happened today, and it’s something I truly enjoyed". | ||
| 5. Weaknesses | Dynamics and structure of the session,Environmental comfort, andAttendance and participation | "At the beginning of the activity, there were more people, and later there were fewer of us", "We can almost never all be present", "Going deeper", "It felt short to me", "Very hot in the classroom. A bit long in duration today". | ||
| 6. Improvement actions | Group duration and structure, and Environmental comfort (physical conditions) | "Do it in different places", "Go outside to the street", "Take more external material", "More interesting questions", "That the session was not excessively long". | ||
SD: Standard deviation.
Table 4.
Comparison of standardized questionnaires pre and post intervention (n=17).
| Pre-Intervention | Post-Intervention | Test | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Variable (Range) | Mean | Median | SDa | Mean | Median | SD | tb | Zc | p-valued |
| Mental health recovery | |||||||||
| QPR (15-60) | 37.53 | 38 | 16.1 | 36.29 | 37 | 12.34 | 0.54 | p=0,593 | |
| RAS-DS (38-152) | 111.18 | 113 | 19.69 | 116.71 | 118 | 17.82 | 1,525 | p=0,147 | |
| Doing things I value (6-24) | 19.35 | 20 | 3.48 | 20 | 21 | 3.58 | 0.79 | p=0,425 | |
| Looking forward (18-72) | 50.35 | 51 | 11.83 | 52.06 | 50 | 8.79 | 0.84 | p=0,413 | |
| Managing my illness (7-28) | 20.94 | 20 | 4.05 | 21.47 | 21 | 3.59 | 0.62 | p=0,540 | |
| Connecting and belonging (7-28) | 20.53 | 21 | 3.22 | 21.94 | 22 | 3.21 | 2.51 | p=0,023 | |
| Quality of life and psychological wellbeing | |||||||||
| EQ-5D (5-15) | 7.71 | 7 | 2.25 | 7.88 | 8 | 2.14 | 0.41 | p=0,687 | |
| EQ-5D scale (0-100) | 56.47 | 65 | 28.31 | 60.59 | 60 | 20.30 | 0.90 | p=0,379 | |
| PWB (39-234) | 142.53 | 143 | 35.1 | 142.88 | 145 | 33.16 | 0.08 | p=0,935 | |
| Self-acceptance (6-36) | 19.53 | 16 | 7.68 | 18.35 | 16 | 6.55 | 0.96 | p=0,334 | |
| Positive relations with others (6-36) | 21 | 22 | 6.72 | 22.65 | 23 | 7.85 | 1.13 | p=0,276 | |
| Autonomy (8-48) | 29.29 | 30 | 8.86 | 29.35 | 30 | 7.7 | 0.060 | p=0,953 | |
| Environmental mastery (6-36) | 20.65 | 20 | 7.32 | 20.53 | 19 | 6.31 | 0.12 | p=0,907 | |
| Purpose in life (7-42) | 33 | 35 | 6.47 | 33.24 | 35 | 7.4 | 0.25 | p=0,800 | |
| Personal growth (6-36) | 19.06 | 17 | 9.06 | 18.76 | 16 | 7.78 | 2.57 | p=0,801 | |
| Self-stigma in mental health | |||||||||
| ISMI (29-116) | 58.94 | 56 | 12.68 | 58 | 59 | 12.79 | 0.87 | p=0,395 | |
| Aligment (6-24) | 13.29 | 14 | 4.07 | 13.24 | 13 | 3.64 | 0.09 | p=0,924 | |
| Assumption of stereotype or self-stigma (7-28) | 11.47 | 11 | 2.91 | 11.18 | 11 | 3.2 | 0.62 | p=0,545 | |
| Perceived discrimiation or experience of discrimination (5-20) | 10.47 | 10 | 3.2 | 10.76 | 11 | 2.92 | 0.67 | p=0,509 | |
| Social isolation (6-24) | 11.76 | 11 | 4.17 | 11.76 | 13 | 4.22 | 0.00 | p=1,000 | |
| Resistance to stigma (5-20) | 11.94 | 11 | 3.47 | 11.06 | 11 | 2.9 | 1.06 | p=0,304 | |
aSD: Standard Deviation. bt indicates the statistic of the t-Student. cZ refers to the statistic of the Wilcozon test. d p-value for comparison between pre and post intervention by the pareid t-student or Wilcoxon test. QPR: Questionarie about the Process of Recovery. EQ-5D: European Quality of Life-5 Dimensions RAS-DS: Recovery Assessment Scale—Domains and Stages. PWB: Psychological Well-being Scale. ISMI: Internalized Stigma of Mental Illness Inventory.
Table 5.
Satisfaction survey of Artistic Couples participation (n=30).
| Quantitative part | Mean | Median | SD | Range (0 (low)-10 (high) |
|---|---|---|---|---|
| 1. Degree of functioning of the activity | 8.9 | 9 | 1.53 | 0-10 |
| 2. Timetable and duration of the activity | 8.7 | 9 | 1.83 | 0-10 |
| 3. Overall level of satisfaction | 9 | 9 | 1.01 | 0-10 |
| Qualitative part | Overarching themes | Quotes | ||
| 4. Strenghts | Social interaction and personal connection, Emotional and therapeutic support, andLearning and personal development | "Share moments with a person", "For a moment you feel free of everything that disturbs you", "Exploring different ways of expression with art", "To interact and gain new knowledge from other people". | ||
| 5. Weaknesses | Lack of time and organization,Space and logistics limitations, andCompatibility and communication issues | "I didn't have the chance to see my partner as much as I would have liked", "The displacement distance to the artist’s studio", "We are two people with very different character and styles and sometimes we have not fully understood or connected.", | ||
| 6. Improvement actions | Having more time,Having a shared creative space, andOrganizing more meetings between artists | "Having more time", "Have a creative space to do the project", "Diversify in different disciplines and touching them all to enrich you", “I would love to keep painting more. I enjoy recreational activities; they relax me”. | ||
SD: Standard deviation.
Table 6.
Patient-Reported Experience Measures (PREMs) (n=30).
| Questions | Definitely yes | Yes | No | Definitely No | Do not want to answer |
|---|---|---|---|---|---|
| Did the main researcher explain things in a way that was easy to understand? | 19 | 11 | 0 | 0 | 0 |
| Did the main researcher treat you with courtesy and respect? | 22 | 8 | 0 | 0 | 0 |
| Did you feel satisfied with the research process you experienced? | 21 | 9 | 0 | 0 | 0 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



