Submitted:
20 March 2025
Posted:
21 March 2025
You are already at the latest version
Abstract
Background: Mesenchymal stem cell (MSC) therapy has garnered increasing attention as a novel therapeutic strategy for type 2 diabetes mellitus (T2DM), owing to its immunomodulatory and regenerative properties. However, the long-term efficacy of a single intravenous MSC infusion on glycemic control remains insufficiently explored.
Objective: This study aimed to evaluate the long-term impact of a single intravenous infusion of MSCs on HbA1c reduction in patients with moderate and severe T2DM and to investigate potential dose- dependent responses.
Methods: A total of 61 patients diagnosed with T2DM (HbA1c ≥6.2%) were enrolled. Patients received a single intravenous infusion of MSCs derived from umbilical cord tissue, bone marrow, or adipose tissue, with doses ranging from 100 million to 2 billion cells, tailored to individual clinical conditions. Patients were categorized into moderate (HbA1c 6.2–8%) and severe (HbA1c >8%) diabetes groups. Follow-up assessments were conducted over a median duration of 35 months (range: 6–68 months), with primary endpoints including changes in HbA1c levels. Statistical analyses were performed using paired t-tests, and correlation analyses evaluated the relationship between MSC dose and glycemic outcomes.
Results: The mean baseline HbA1c level was 7.49%, which significantly decreased to 6.7% post- treatment (p < 0.0001). In the moderate diabetes group, the mean HbA1c reduction was 0.58% (p < 0.0000002), while the severe diabetes group exhibited a more pronounced mean reduction of 1.55% (p = 0.0122). Subgroup analysis suggested a trend toward greater HbA1c reduction in patients receiving higher MSC doses (≥1 billion cells), though this did not reach statistical significance. No serious adverse events were reported during the follow-up period.
Conclusion: A single intravenous infusion of MSCs resulted in significant and sustained HbA1c reduction, particularly in patients with severe diabetes, with effects persisting for over three years. These findings highlight the potential of MSC therapy as a disease-modifying intervention in T2DM management. Further randomized controlled trials are warranted to validate these results and optimize dosing strategies.
Keywords:
stem cell
; diabetes millitus
1. Introduction
Diabetes mellitus remains a global health challenge, with HbA1c levels serving as a critical marker for long-term glycemic control. Conventional treatments, including insulin and oral hypoglycemic agents, often require lifelong management and do not address the underlying disease pathology. MSC therapy, with its potential immunomodulatory and regenerative effects, has shown promise in preclinical and clinical studies. Studies, including those referenced in the reference2), indicate that MSCs can modulate immune responses, reduce inflammation, and enhance beta-cell function, thereby improving glycemic control.
A recent comprehensive review summarized 22 clinical studies investigating the effects of intravenous stem cell therapy in both type 1 and type 2 diabetes patients. Across these studies, a consistent trend of glycemic improvement was reported. Specifically, 18 of the 22 studies documented significant reductions in HbA1c levels, with reductions ranging from 1.31% to 1.36% at 48 weeks. Several studies also reported marked increases in C-peptide levels, indicating enhanced endogenous beta-cell activity. Notably, some studies demonstrated reduced insulin requirements, with insulin independence achieved in up to 59% of patients.
These studies utilized a variety of stem cell types, including autologous hematopoietic stem cells (HSCs), allogeneic umbilical cord-derived MSCs, bone marrow-derived MSCs, and cord blood-derived stem cells. Treatment protocols varied, employing both single and multiple infusion strategies, with doses often tailored based on body weight (e.g., 1 × 10^6 cells/kg). Importantly, the safety profile across these studies was favorable, with most adverse events being mild and transient. Some studies identified factors influencing treatment response, such as shorter disease duration, lower BMI, and higher baseline beta-cell function.
The accumulation of evidence from these 22 studies underscores the broad potential of stem cell therapies in diabetes management. These findings support the rationale for further exploration of MSC therapy, particularly its long-term efficacy and safety in diverse patient populations. Building upon these insights, the present study aims to assess the real-world impact of a single MSC infusion on long-term HbA1c reduction and its implications for diabetes management.
2. Methods
The methodology for this study follows the protocol established in our previous research1), with modifications tailored to evaluate the long-term effects of MSC therapy on diabetes management. Patients with HbA1c levels classified as moderate (6.2-8%) or severe (>8%) diabetes were enrolled and received a single intravenous infusion of MSCs. The MSCs were derived from umbilical cord tissue, bone marrow, or adipose tissue, processed under Good Manufacturing Practice (GMP) standards to ensure sterility, viability, and potency.
The treatment protocol involved a single intravenous administration of MSCs at doses ranging from 100 million to 2 billion cells, determined based on patient body weight and clinical condition. The infusion procedure followed standard aseptic techniques, with patients monitored for immediate adverse reactions.
2.1. Patient Selection
Patients were recruited based on inclusion criteria such as confirmed diagnosis of type 2 diabetes, HbA1c levels of at least 6.2%, and failure to achieve adequate glycemic control with conventional therapy. Exclusion criteria included a history of malignancy, active infections, or autoimmune diseases that could interfere with MSC function.
2.2. MSC Preparation and Characterization
MSC isolation and culture followed previously established protocols. The cells were expanded in a GMP-compliant facility, and quality control measures included viability testing, immunophenotyping (CD73, CD90, CD105 positive; CD34, CD45 negative), and functional assays for differentiation potential.
2.3. MSC Administration Protocol
The prepared MSCs were suspended in normal saline and infused intravenously over 30–60 minutes. Patients were monitored for immediate adverse reactions, including fever, chills, or infusion-related complications. No serious adverse events were reported in our cohort.
2.4. Follow-Up and Outcome Measures
Patients underwent scheduled follow-ups at 3, 6, 12 months, and annually for up to 5 years. Primary outcome measures included changes in HbA1c, fasting blood glucose, and insulin sensitivity indices. Secondary outcomes assessed systemic inflammation markers (CRP, TNF-α, IL-6) and pancreatic beta-cell function.
2.5. Statistical Analysis
Data analysis was performed using Excel application. Paired t-tests were used to compare pre- and post-treatment HbA1c levels, and Pearson correlation analysis examined associations between MSC dose, treatment duration, and metabolic improvements. A p-value <0.05 was considered statistically significant.
3. Results
A total of 61 patients diagnosed with type 2 diabetes were included in this study. The cohort comprised 42 male and 16 female patients, with a mean age of 63.3 years (range: 42 to 89 years). All patients underwent a single intravenous infusion of mesenchymal stem cells (MSCs), with administered doses ranging from 100 million to 2 billion cells. The median dose was 2 billion cells, reflecting the preference for high-dose MSC administration across the cohort.
Before treatment, the mean HbA1c level was 7.49%, with values ranging from 6.3% to 12.4%. Following MSC therapy, the mean HbA1c level decreased to 6.7%, with a post-treatment range of 4.6% to 10.9%. The median follow-up duration after MSC infusion was 35 months, with individual follow-up periods ranging from 6 to 68 months. These patient characteristics underscore the inclusion of a broad spectrum of diabetic severity and provide a solid foundation to evaluate the long-term efficacy of MSC therapy across diverse clinical backgrounds.
-
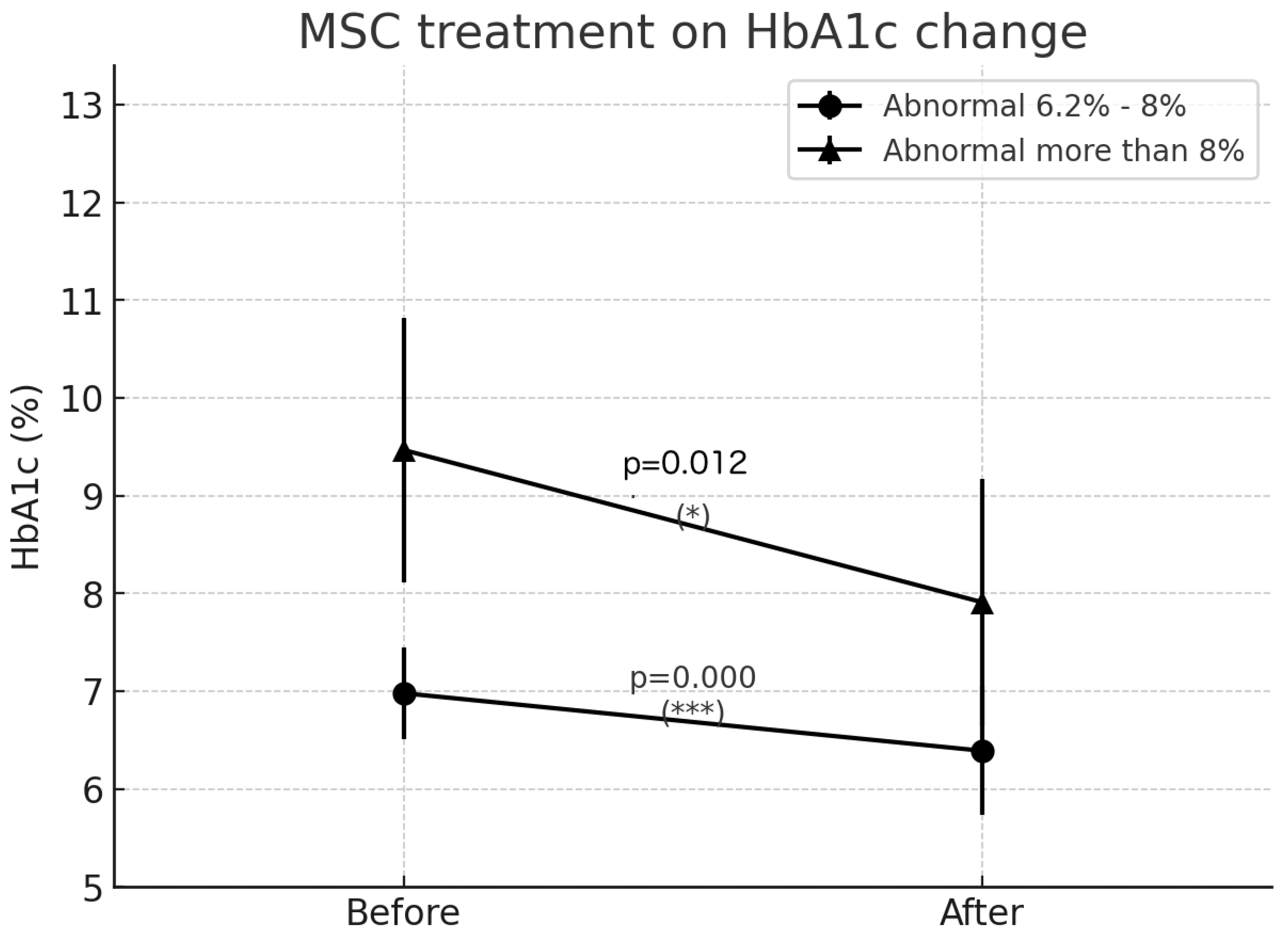
Moderate Diabetes Group (HbA1c 6.2-8%):
- o
- Mean HbA1c reduction: 0.58%
- o
- Statistical significance: p < 0.0000002 (highly significant)
-
Severe Diabetes Group (HbA1c >8%):
- o
- Mean HbA1c reduction: 1.55%
- o
- Statistical significance: p = 0.0122 (significant)
-
Sustained Effect Duration:
- o
- Median follow-up duration: 35.5 months
- o
- Interquartile range: 15.25 - 45.75 months
- o
- Correlation between duration and HbA1c reduction: 0.041 (no significant correlation)
Figure 1.

| Sex | Age | Stem cell Dose x million cells |
HbA1c Before treatment | HbA1c After Treatment | Observed Month |
| M | 66 | 1000 | 7.5 | 6.4 | 27 |
| M | 66 | 2000 | 7.2 | 4.6 | 51 |
| M | 71 | 100 | 7.6 | 6.7 | 45 |
| M | 61 | 2000 | 7.1 | 6.5 | 18 |
| M | 76 | 2000 | 6.8 | 7.7 | 68 |
| M | 66 | 2000 | 6.9 | 6.5 | 13 |
| M | 79 | 1000 | 7.1 | 5.7 | 64 |
| M | 55 | 1000 | 6.8 | 5.9 | 18 |
| M | 72 | 1000 | 6.3 | 5.9 | 64 |
| M | 89 | 400 | 7.4 | 6.3 | 18 |
| F | 42 | 1000 | 7.2 | 8 | 62 |
| F | 60 | 1000 | 6.3 | 5.9 | 7 |
| M | 66 | 500 | 9.3 | 8.5 | 16 |
| M | 61 | 1000 | 7.2 | 6.9 | 53 |
| M | 52 | 2000 | 6.9 | 5.7 | 54 |
| M | 59 | 1000 | 6.4 | 5.1 | 53 |
| M | 63 | 2000 | 6.3 | 5.7 | 45 |
| F | 52 | 2000 | 6.4 | 5.7 | 47 |
| M | 69 | 2000 | 12.4 | 6.5 | 51 |
| M | 61 | 2000 | 7 | 6.9 | 46 |
| F | 53 | 2000 | 8.2 | 7.9 | 37 |
| M | 63 | 2000 | 7.9 | 7.2 | 45 |
| M | 66 | 2000 | 6.4 | 5.8 | 51 |
| F | 59 | 2000 | 10.3 | 7.4 | 44 |
| M | 69 | 2000 | 6.3 | 6.8 | 60 |
| F | 60 | 2000 | 7.3 | 6.3 | 40 |
| M | 64 | 2000 | 6.7 | 6.3 | 40 |
| M | 63 | 2000 | 6.8 | 6.3 | 40 |
| M | 64 | 2000 | 6.5 | 6.3 | 60 |
| F | 71 | 2000 | 8.7 | 7.4 | 39 |
| M | 65 | 2000 | 7.8 | 7.9 | 44 |
| M | 62 | 2000 | 8.7 | 8.5 | 45 |
| M | 47 | 2000 | 6.4 | 6.2 | 35 |
| F | 61 | 2000 | 7.5 | 6.7 | 42 |
| F | 57 | 100 | 8.5 | 7.4 | 14 |
| F | 58 | 2000 | 11.9 | 8.4 | 16 |
| F | 77 | 2000 | 7.5 | 6.4 | 19 |
| M | 59 | 2000 | 6.7 | 6.4 | 27 |
| F | 71 | 2000 | 6.9 | 7.4 | 17 |
| M | 48 | 2000 | 7.2 | 6.6 | 15 |
| F | 70 | 2000 | 6.4 | 5.9 | 17 |
| F | 60 | 2000 | 9.3 | 10.9 | 22 |
| M | 62 | 2000 | 8 | 6.6 | 25 |
| M | 66 | 2000 | 7.1 | 6.4 | 6 |
| M | 59 | 2000 | 6.9 | 6.4 | 11 |
| M | 67 | 400 | 8.2 | 8.2 | 9 |
| M | 45 | 2000 | 7.8 | 6.1 | 12 |
| M | 72 | 1000 | 7.7 | 7.2 | 14 |
| M | 68 | 2000 | 6.9 | 7 | 14 |
| M | 80 | 2000 | 6.5 | 5.8 | 14 |
| M | 76 | 2000 | 6.4 | 5.5 | 15 |
| M | 56 | 1000 | 9.8 | 8.4 | 16 |
| F | 74 | 700 | 6.8 | 6.6 | 7 |
| M | 46 | 2000 | 7.1 | 6.3 | 41 |
| M | 67 | 2000 | 7.3 | 6.1 | 48 |
| M | 64 | 2000 | 8.3 | 5.4 | 36 |
| F | 43 | 500 | 6.9 | 6.5 | 9 |
| M | 72 | 500 | 6.9 | 6.6 | 15 |
Additional subgroup analysis indicated that patients with higher baseline HbA1c levels experienced a more pronounced reduction, suggesting that the initial disease severity influences treatment response. Patients receiving higher doses of MSCs (≥1 billion cells) demonstrated a trend toward greater HbA1c reduction, though this did not reach statistical significance (p > 0.05). Notably, patients who received the highest MSC doses (≥1.5 billion cells) showed a mean HbA1c reduction of 1.72%, compared to 1.12% in those who received doses below 1 billion cells. This suggests a potential dose-dependent response, though variability among individuals highlights the need for further dose-optimization studies.
4. Discussion
Accoring to Systematic review regarding Insulin Requirements, many studies reported reductions in insulin requirements following stem cell therapy, with some patients achieving insulin independence. Key findings include:
- D’Addio et al. (2014) reported that 59% of patients achieved insulin independence within 6 months, with 32% remaining insulin-free at the last follow-up.
- Hu et al. (2016) observed a significant reduction in insulin requirements, with 32.3% of patients achieving insulin withdrawal.
- Voltarelli et al. (2009) found that 14 out of 15 patients became insulin-free for varying durations.
- Zang et al. (2022) reported a significant reduction in insulin requirements, with a higher percentage of insulin reduction in the UC-MSCs group compared to placebo.
- Snarski et al. (2011) observed that all patients became independent of exogenous insulin after treat- ment, although one patient resumed low-dose insulin after 7 months.
The degree of insulin reduction varied across studies, with some patients experiencing complete insulin independence and others showing partial reductions in insulin requirements. The durability of these effects also varied, with some studies reporting sustained benefits and others noting a gradual return to insulin dependence in some patients.
The results indicate a greater HbA1c reduction in patients with severe diabetes, supporting the hypothesis that MSC therapy has a stronger impact in more advanced cases. The long-term efficacy, with a median effect duration exceeding three years, is particularly noteworthy. These findings align with prior research2), which suggests that MSCs may exert their effects through paracrine signaling, immune modulation, and potential beta-cell regeneration.
Our analysis also suggests a possible dose-response relationship, where patients receiving higher doses of MSCs exhibited greater reductions in HbA1c. The findings from broader clinical trials reinforce this observation, indicating that a tailored MSC dosing strategy could further enhance treatment efficacy. Future studies should investigate whether multiple doses or repeated infusions could further enhance therapeutic outcomes.
The results of this study demonstrate a significant and sustained reduction in HbA1c levels following a single intravenous infusion of MSCs, particularly in patients with severe diabetes. Notably, the median follow-up duration exceeded three years, yet the correlation analysis revealed no significant relationship between follow-up duration and the magnitude of HbA1c reduction (correlation coefficient: 0.041). This suggests that the therapeutic effect is not transient but rather maintained over several years after only one administration.
Such a long-lasting effect is unprecedented in the field of diabetes management. Conventional antidiabetic agents, including insulin, GLP-1 receptor agonists, and oral hypoglycemic agents, typically require continuous and lifelong administration to maintain glycemic control. In contrast, our findings indicate that a single MSC infusion yields durable improvements in glycemic parameters, reducing HbA1c levels significantly without ongoing therapy. This highlights a unique, disease-modifying potential of MSC treatment that differentiates it from standard pharmacological approaches.
Additionally, the absence of a significant decline in therapeutic efficacy over time implies that MSC therapy may induce long-term modulation of the immune environment, reduction of systemic inflammation, or enhancement of endogenous beta-cell function. These mechanisms align with previous studies suggesting that MSCs exert their beneficial effects through paracrine signaling, immune regulation, and promotion of pancreatic islet regeneration.
Importantly, our findings are consistent with multiple clinical trials summarized in the recent systematic review, which reported sustained HbA1c reductions and increased C-peptide levels over extended periods following stem cell therapy. However, unlike those studies where multiple infusions were often required, our results underscore the efficacy of a single high-dose MSC treatment in achieving long-term glycemic control.
These observations suggest a paradigm shift in diabetes management, offering the possibility of achieving lasting metabolic improvement with minimal therapeutic burden. Future research should focus on elucidating the precise biological mechanisms responsible for this sustained effect and verifying these findings in larger, randomized controlled trials.
5. Conclusions
In conclusion, a single intravenous infusion of mesenchymal stem cells (MSCs) resulted in a significant and durable reduction in HbA1c levels in patients with type 2 diabetes, with the effect being particularly pronounced in those with severe diabetes. Remarkably, the median follow-up duration exceeded three years, and no significant correlation was observed between follow-up duration and the magnitude of HbA1c reduction. This suggests that the glycemic improvement achieved after a single MSC infusion is sustained long-term without the need for repeated treatments—an outcome that is unprecedented compared to conventional antidiabetic therapies, which typically require continuous administration.
The findings of this study support the concept that MSC therapy may possess disease-modifying properties, potentially through immune modulation, reduction of systemic inflammation, and enhancement of endogenous beta-cell function. Our results, together with evidence from prior clinical trials, indicate that MSC therapy has the potential to fundamentally change the management paradigm for diabetes by offering long-lasting metabolic benefits with minimal therapeutic burden.
Further large-scale randomized controlled trials and mechanistic studies are warranted to validate these findings, clarify the underlying biological mechanisms, and determine optimal dosing strategies to maximize therapeutic efficacy.
Author Contributions
All authors contributed to the study conception and design. T.M., N.K., T.I. and Y.H. treated the patients as attending physicians and contributed to the collection of clinical data on patients. T.M. prepared the materials and analyses, wrote the first draft of the manuscript, and commented on previous versions of the manuscript. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
This study was approved by the Helene Ethical Committee (approval number: HCS-20140601 on 1 June 2014). Written informed consent was obtained from all study participants.
Informed Consent Statement
Not applicable.
Data Availability Statement
All data generated or analyzed during this study are included in this article.
Acknowledgments
Not applicable.
Conflicts of Interest
All authors declare no financial or non-financial competing interests.
References
- Matsuoka T, Itohara T, Hara Y, Kobayashi N. Systematic Intravenous Administration of Autologous Mesenchymal Stem Cells Is Safe. J Clin Med. 2024 Dec 7;13(23):7460. [CrossRef] [PubMed] [PubMed Central]
- Hu J, Wang Y, Gong H, Yu C, Guo C, Wang F, Yan S, Xu H. Long term effect and safety of Wharton’s jelly-derived mesenchymal stem cells on type 2 diabetes. Exp Ther Med. 2016 Sep;12(3):1857-1866. Epub 2016 Jul 26. [CrossRef] [PubMed] [PubMed Central]
- Bhansali, Premkumar Asokumar, R. Walia, S. Bhansali, Vivek Gupta, Ashish Jain, N. Sachdeva, R. Sharma, N. Marwaha, and N. Khandelwal.. Efficacy and Safety of Autologous Bone Marrow-Derived Stem Cell Transplantation in Patients with Type 2 Diabetes Mellitus: A Randomized Placebo-Controlled Study. Bhansali, Premkumar Asokumar, R. Walia, S. Bhansali, Vivek Gupta, Ashish Jain, N. Sachdeva, R. Sharma, N. Marwaha, and N. Khandelwal. “Efficacy and Safety of Autologous Bone Marrow-Derived Stem Cell Transplantation in Patients with Type 2 Diabetes Mellitus: A Randomized Placebo-Controlled Study.” Cell Transplantation. 2014.
- E. Snarski, A. Milczarczyk, T. Torosian, M. Paluszewska, E. Urbanowska, M. Król, P. Boguradzki, et al.. Independence of Exogenous Insulin Following Immunoablation and Stem Cell Reconstitution in Newly Diagnosed Diabetes Type I. Snarski, A. Milczarczyk, T. Torosian, M. Paluszewska, E. Urbanowska, M. Król, P. Boguradzki, et al. “Independence of Exogenous Insulin Following Immunoablation and Stem Cell Reconstitution in Newly Diagnosed Diabetes Type I.” Bone Marrow Transplantation. 2011.
- F. D’Addio, Alessandro Valderrama Vasquez, M. Ben Nasr, Edward Franek, Dalong Zhu, Lirong Li, G. Ning, E. Snarski, and P. Fiorina.. Autologous Nonmyeloablative Hematopoietic Stem Cell Transplantation in New-Onset Type 1 Diabetes: A Multicenter Analysis. D’Addio, Alessandro Valderrama Vasquez, M. Ben Nasr, Edward Franek, Dalong Zhu, Lirong Li, G. Ning, E. Snarski, and P. Fiorina. “Autologous Nonmyeloablative Hematopoietic Stem Cell Transplantation in New-Onset Type 1 Diabetes: A Multicenter Analysis.” Diabetes. 2014.
- J. G. Penaforte-Saboia, R. Montenegro, C. Couri, L. Batista, A. P. Montenegro, V. Fernandes, H. Akhtar, et al.. Microvascular Complications in Type 1 Diabetes: A Comparative Analysis of Patients Treated with Autologous Nonmyeloablative Hematopoietic Stem-Cell Transplantation and Conventional Medical Therapy. G. Penaforte-Saboia, R. Montenegro, C. Couri, L. Batista, A. P. Montenegro, V. Fernandes, H. Akhtar, et al. “Microvascular Complications in Type 1 Diabetes: A Comparative Analysis of Patients Treated with Autologous Nonmyeloablative Hematopoietic Stem-Cell Transplantation and Conventional Medical Therapy.” Frontiers in Endocrinology. 2017.
- J. Gan, Yingjin Wang, and Xiaodong Zhou.. Stem Cell Transplantation for the Treatment of Patients with Type 1 Diabetes Mellitus: A Meta-Analysis. Gan, Yingjin Wang, and Xiaodong Zhou. “Stem Cell Transplantation for the Treatment of Patients with Type 1 Diabetes Mellitus: A Meta-Analysis.” Experimental and Therapeutic Medicine. 2018.
- J. Markmann, A. Naji, M. Rickels, Maria Alba, G. Marigowda, Leorah Ross, Chenkun Wang, et al.. 259-OR: Stem Cell–Derived, Fully Differentiated Islet Cells for Type 1 Diabetes. Markmann, A. Naji, M. Rickels, Maria Alba, G. Marigowda, Leorah Ross, Chenkun Wang, et al. “259-OR: Stem Cell–Derived, Fully Differentiated Islet Cells for Type 1 Diabetes.” Diabetes. 2022.
- J. Skyler, V. Fonseca, K. Segal, and J. Rosenstock.. Allogeneic Mesenchymal Precursor Cells in Type 2 Diabetes: A Randomized, Placebo-Controlled, Dose-Escalation Safety and Tolerability Pilot Study. Skyler, V. Fonseca, K. Segal, and J. Rosenstock. “Allogeneic Mesenchymal Precursor Cells in Type 2 Diabetes: A Randomized, Placebo-Controlled, Dose-Escalation Safety and Tolerability Pilot Study.” Diabetes Care. 2015.
- J. Voltarelli, C. Couri, A. Stracieri, M. Oliveira, D. Moraes, F. Pieroni, M. Coutinho, et al.. Autologous Non- myeloablative Hematopoietic Stem Cell Transplantation in Newly Diagnosed Type 1 Diabetes Mellitus. Voltarelli, C. Couri, A. Stracieri, M. Oliveira, D. Moraes, F. Pieroni, M. Coutinho, et al. “Autologous Non- myeloablative Hematopoietic Stem Cell Transplantation in Newly Diagnosed Type 1 Diabetes Mellitus.” Journal of the American Medical Association (JAMA). 2009.
- Jianxia Hu, Yangang Wang, Huimin Gong, Chundong Yu, Caihong Guo, F. Wang, Shengli Yan, and Hongmei Xu.. Long Term Effect and Safety of Wharton’s Jelly-Derived Mesenchymal Stem Cells on Type 2 Diabetes. Wang, Shengli Yan, and Hongmei Xu. “Long Term Effect and Safety of Wharton’s Jelly-Derived Mesenchymal Stem Cells on Type 2 Diabetes.” Experimental and Therapeutic Medicine. 2016.
- Jing Lu, S. Shen, Qing Ling, Bin Wang, Li-rong Li, Wei Zhang, Duo-duo Qu, Y. Bi, and Dalong Zhu.. One Repeated Transplantation of Allogeneic Umbilical Cord Mesenchymal Stromal Cells in Type 1 Diabetes: An Open Parallel Controlled Clinical Study. Shen, Qing Ling, Bin Wang, Li-rong Li, Wei Zhang, Duo-duo Qu, Y. Bi, and Dalong Zhu. “One Repeated Transplantation of Allogeneic Umbilical Cord Mesenchymal Stromal Cells in Type 1 Diabetes: An Open Parallel Controlled Clinical Study.” Stem Cell Research & Therapeutics. 2020.
- L. Nguyen, Duc M. Hoang, Kien T. Nguyen, D. Bui, Hieu T Nguyen, Hong T A Le, Van T. Hoang, et al.. Type 2 Diabetes Mellitus Duration and Obesity Alter the Efficacy of Autologously Transplanted Bone Marrow-derived Mesenchymal Stem/Stromal Cells. Nguyen, Duc M. Hoang, Kien T. Nguyen, D. Bui, Hieu T Nguyen, Hong T A Le, Van T. Hoang, et al. “Type 2 Diabetes Mellitus Duration and Obesity Alter the Efficacy of Autologously Transplanted Bone Marrow-derived Mesenchymal Stem/Stromal Cells.” Stem Cells Translational Medicine. 2021.
- L. Zang, Yijun Li, Hao-jie Hao, Jiejie Liu, Qian Zhang, Fei Gao, Haibin Wang, et al.. Efficacy of Umbilical Cord-Derived Mesenchymal Stem Cells in the Treatment of Type 2 Diabetes Assessed by Retrospective Continuous Glucose Monitoring. Zang, Yijun Li, Hao-jie Hao, Jiejie Liu, Qian Zhang, Fei Gao, Haibin Wang, et al. “Efficacy of Umbilical Cord-Derived Mesenchymal Stem Cells in the Treatment of Type 2 Diabetes Assessed by Retrospective Continuous Glucose Monitoring.” Stem Cells Translational Medicine. 2023.
- L. Zang, Yijun Li, Hao-jie Hao, Jiejie Liu, Yu Cheng, Bing Li, Y. Yin, et al.. Efficacy and Safety of Umbilical Cord-Derived Mesenchymal Stem Cells in Chinese Adults with Type 2 Diabetes: A Single-Center, Double- Blinded, Randomized, Placebo-Controlled Phase II Trial. Zang, Yijun Li, Hao-jie Hao, Jiejie Liu, Yu Cheng, Bing Li, Y. Yin, et al. “Efficacy and Safety of Umbilical Cord-Derived Mesenchymal Stem Cells in Chinese Adults with Type 2 Diabetes: A Single-Center, Double- Blinded, Randomized, Placebo-Controlled Phase II Trial.” Stem Cell Research & Therapeutics. 2022.
- Lirong Li, S. Shen, J. Ouyang, Yun Hu, Limin Hu, Weijuan Cui, Ning Zhang, et al.. Autologous Hematopoi- etic Stem Cell Transplantation Modulates Immunocompetent Cells and Improves -Cell Function in Chi- nese Patients with New Onset of Type 1 Diabetes. Shen, J. Ouyang, Yun Hu, Limin Hu, Weijuan Cui, Ning Zhang, et al. “Autologous Hematopoi- etic Stem Cell Transplantation Modulates Immunocompetent Cells and Improves -Cell Function in Chi- nese Patients with New Onset of Type 1 Diabetes.” Journal of Clinical Endocrinology and Metabolism. 2012.
- M. Izadi, Anavasadat Sadr Hashemi Nejad, M. Moazenchi, S. Masoumi, A. Rabbani, Farzad Kompani, Amir Abbas Hedayati Asl, et al.. Mesenchymal Stem Cell Transplantation in Newly Diagnosed Type-1 Diabetes Patients: A Phase I/II Randomized Placebo-Controlled Clinical Trial. Izadi, Anavasadat Sadr Hashemi Nejad, M. Moazenchi, S. Masoumi, A. Rabbani, Farzad Kompani, Amir Abbas Hedayati Asl, et al. “Mesenchymal Stem Cell Transplantation in Newly Diagnosed Type-1 Diabetes Patients: A Phase I/II Randomized Placebo-Controlled Clinical Trial.” Stem Cell Research & Therapeutics. 2021.
- P. Carlsson, D. Espes, L. Davies, and M. Svahn. “Dose-Dependent Preservation of Beta-Cell Function in Type i Diabetes by Mesenchymal Stromal Cells,” 2020.
- Pin Chen, Qin Huang, Xiangjin Xu, Z. Shao, Huang Lh, Yang Xz, W. Guo, Li Cm, and C. Chen.. [The Effect of Liraglutide in Combination with Human Umbilical Cord Mesenchymal Stem Cells Treatment on Glucose Metabolism and Cell Function in Type 2 Diabetes Mellitus]. Shao, Huang Lh, Yang Xz, W. Guo, Li Cm, and C. Chen. “[The Effect of Liraglutide in Combination with Human Umbilical Cord Mesenchymal Stem Cells Treatment on Glucose Metabolism and Cell Function in Type 2 Diabetes Mellitus].” Zhonghua Nei Ke Za Zhi. 2016.
- U. Thakkar, H. Trivedi, A. Vanikar, and S. Dave.. Insulin-Secreting Adipose-Derived Mesenchymal Stromal Cells with Bone Marrow-Derived Hematopoietic Stem Cells from Autologous and Allogenic Sources for Type 1 Diabetes Mellitus. Thakkar, H. Trivedi, A. Vanikar, and S. Dave. “Insulin-Secreting Adipose-Derived Mesenchymal Stromal Cells with Bone Marrow-Derived Hematopoietic Stem Cells from Autologous and Allogenic Sources for Type 1 Diabetes Mellitus.” Cytotherapy. 2015.
- V. Sood, A. Bhansali, B. Mittal, Baljinder Singh, N. Marwaha, Ashish Jain, and N. Khandelwal.. Autologous Bone Marrow Derived Stem Cell Therapy in Patients with Type 2 Diabetes Mellitus - Defining Adequate Administration Methods. Sood, A. Bhansali, B. Mittal, Baljinder Singh, N. Marwaha, Ashish Jain, and N. Khandelwal. “Autologous Bone Marrow Derived Stem Cell Therapy in Patients with Type 2 Diabetes Mellitus - Defining Adequate Administration Methods.” World Journal of Diabetes. 2017.
- Wenwen Li, X. Jiao, Jing-yun Song, B. Sui, Zhili Guo, Yingji Zhao, Jun Li, S. Shi, and Qin Huang.. Therapeutic Potential of Stem Cells from Human Exfoliated Deciduous Teeth Infusion into Patients with Type 2 Diabetes Depends on Basal Lipid Levels and Islet Function. Jiao, Jing-yun Song, B. Sui, Zhili Guo, Yingji Zhao, Jun Li, S. Shi, and Qin Huang. “Therapeutic Potential of Stem Cells from Human Exfoliated Deciduous Teeth Infusion into Patients with Type 2 Diabetes Depends on Basal Lipid Levels and Islet Function.” Stem Cells Translational Medicine. 2021.
- Xianliang Gu, Xi Yu, Chen Zhao, P. Duan, Tongtao Zhao, Yong Liu, Shiying Li, et al.. Efficacy and Safety of Autologous Bone Marrow Mesenchymal Stem Cell Transplantation in Patients with Diabetic Retinopathy. Duan, Tongtao Zhao, Yong Liu, Shiying Li, et al. “Efficacy and Safety of Autologous Bone Marrow Mesenchymal Stem Cell Transplantation in Patients with Diabetic Retinopathy.” Cellular Physiology and Biochemistry. 2018.
- Xiaoyu Lian, Dong-Hui Lu, Hong-Li Liu, Yanjun Liu, Xiu-Qun Han, Yang Yang, Yuan Lin, et al.. Effectiveness and Safety of Human Umbilical Cord-Mesenchymal Stem Cells for Treating Type 2 Diabetes Mellitus. “Effectiveness and Safety of Human Umbilical Cord-Mesenchymal Stem Cells for Treating Type 2 Diabetes Mellitus.” World Journal of Diabetes. 2022.
- Yong Zhao, Zhaoshun Jiang, Tingbao Zhao, Mingliang Ye, Chengjin Hu, Hui-min Zhou, Zhaohui Yin, et al.. Targeting Insulin Resistance in Type 2 Diabetes via Immune Modulation of Cord Blood-Derived Multipotent Stem Cells (CB-SCs) in Stem Cell Educator Therapy: Phase I/II Clinical Trial. “Targeting Insulin Resistance in Type 2 Diabetes via Immune Modulation of Cord Blood-Derived Multipotent Stem Cells (CB-SCs) in Stem Cell Educator Therapy: Phase I/II Clinical Trial.” BMC Medicine. 2013.
- Yong Zhao, Zhaoshun Jiang, Tingbao Zhao, Mingliang Ye, Chengjin Hu, Zhaohui Yin, Heng Li, et al.. Reversal of Type 1 Diabetes via Islet Cell Regeneration Following Immune Modulation by Cord Blood- Derived Multipotent Stem Cells. “Reversal of Type 1 Diabetes via Islet Cell Regeneration Following Immune Modulation by Cord Blood- Derived Multipotent Stem Cells.” BMC Medicine. 2012.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



