
Submitted:
20 March 2025
Posted:
20 March 2025
You are already at the latest version
Abstract
Breast cancer is the predominant cause of cancer in developing nations, and screening with breast self-examinations and mammograms is crucial in mitigating morbidity and mortality. Nonetheless, geographic disparities in screening methods persist, attributable to socio-demographic variation and healthcare accessibility. This study aimed to analyze the influence of women’s screening practices for breast cancer and the other risks stratified to urban and rural areas in Indonesia. A case-control design was adopted, including all women who had breast cancer in 2014 as the study subjects. The Indonesian Family Life Survey data from 2007, with subjects aged at least 15 years, and from 2014 were used. Unconditional logistic regression was used to analyse the risk factors of breast cancer. After controlling for confounders, the odds of breast cancer diagnosis were higher in women who performed breast self examination (BSE) (aOR 10.22; 95% CI 1.04-50.81 and aOR 11.10; 95% CI 3.32-37.08) and those married before age of 19 (aOR 4.81;95% CI 1.93-6.05 and aOR 5.35;95% CI 1.49-19.7), respectively in urban-rural. In addition, women who had undergone mammography (aOR 48.04; 95% CI 10.33-83.45) had significantly higher odds of being diagnosed with breast cancer in urban. In rural areas, the paternal history of cancer-related death had higher odds of breast cancer (aOR 30.63; 95%CI 6.04-60.41) than those without a parental history of cancer. This study highlights the importance of intensifying national breast cancer screening, including BSE campaigns and expanding mammography infrastucture, particularly in rural areas, for improving breast cancer prevention and early diagnosis.
Keywords:
Keywords: breast cancer
; screening
; mammogram
; urban
; rural
1. Introduction
The battle against cancer has emerged as a major global public health issue. The International Agency for Research on Cancer (IARC) reported 20 million new cases of cancer and 10 million deaths by 2022, with this number projected to increase to 35 million by 2050 [1,2]. The overall cancer burden continues to rise in low- and middle-income countries (LMICs), particularly in Asia [3]. In Southeast Asia, breast cancer remains the most diagnosed cancer and the leading cause of cancer-related death in Indonesia, with 985,400 new cases and 315,100 deaths reported in 2022. This concerning observation is reflected in adjacent countries, including the Philippines (33,100 cases and 11,900 deaths), Vietnam (24,600 cases and 10,000 deaths), Thailand (21,600 cases and 7,600 deaths), and Malaysia (8,400 cases and 3,500 deaths). These alarming statistics emphasize the urgent need for enhanced awareness, early detection, and access to effective treatment options in this region [4,5].
Notwithstanding global progress in cancer prevention and treatment, most breast cancers are diagnosed late (at an advanced stage), where curative treatment is no longer possible in most cases [6]. Screening practices through breast self-examination (BSE) and mammography are critical to reducing morbidity and enhancing survival rates effectively [7,8]. However, participation in screening programs remains low in many LMICs, including Indonesia [6]. This low participation is affected by various factors, such as sociodemographic variables, healthcare accessibility, and cultural perceptions towards cancer screening [9,10].
The risk factors for breast cancer are multifactorial, encompassing genetic predisposition, hormonal influences, sociodemographic characteristics, and lifestyle. A family history of breast cancer increases risk significantly, with studies reporting a two-fold higher risk among individuals with affected first- or second-degree relatives. Hormonal factors such as age at menarche, parity, breastfeeding history, menopausal status, and contraceptive use have been linked to breast cancer [11,12]. For instance, pre-menopausal women exhibited a 40% higher risk compared to post-menopausal women, necessitating an early screening to ensure timely prevention [13]. In addition, unhealthy behaviors such as smoking, dietary choices, physical inactivity, high-calorie diets, and obesity further exacerbate cancer risk [11,12,14].
Geographic disparities further compound the challenges in addressing breast cancer prevention and management in Indonesia. Screening rates are generally lower in rural areas compared to urban areas, primarily due to barriers such as inadequate healthcare facilities, financial constraints, and lower levels of education. Rural populations are also characterized by older age, lower socioeconomic status, and greater frequency of unhealthy behaviours, including smoking and infrequent physical activity, which contribute to higher incidence cases and late-stage diagnoses [8,11,14,15,16]. In contrast, urban populations, while benefiting from better healthcare access, encounter additional risk factors, including postponed childbirth, diminished parity, and heightened intake of high-fat diets [11]. These contrasting patterns underscore the complexity of breast cancer prevention in diverse populations. However, studies on the geographic factors in breast cancer cases within LMICs, exclusively in Asia, are insufficient. Comprehending the risk factors affecting breast cancer is essential for formulating tailored public health interventions that address the unique challenges faced by each demographic group. Therefore, this study aims to examine the influence of screening practices and other risks on breast cancer cases, differentiated by urban and rural settings.
2. Materials and Methods
This study utilized secondary data from the longitudinal study of the Indonesian Family Life Survey (IFLS), specifically from waves in 2007 and the latest data in 2014. IFLS data are the only cohort data in Indonesia that comprehensively describes the population. It included 7224 households selected from 13 out of 26 provinces in Indonesia, representing approximately 83% of the national population and capturing its diversity [17].
A community-based unmatched case-control study design was employed, considering the relatively low prevalence of cancer in Indonesia, estimated at 1.8% [18], and the nature of the long latency of cancer development [11]. The eligible cases were women diagnosed with breast cancer in 2014. Meanwhile, the controls were women without a breast cancer diagnosis in the same year. We excluded the missing data. To investigate disparities in breast cancer risk factors, participants were stratified based on urban and rural residence, as classified by the Indonesian Bureau of Statistics (BPS) at the time of the survey interview.
The dependent variable was self-reported breast cancer diagnosed by a doctor in 2014 while the independent variables included various risk factors of breast cancer such as screening practices, individual characteristics, behavioural factors, enhancing, and supporting factors. Cancer screening practices were assessed using two questions: “Have you heard about mammograms before?” and “How many times have you had a breast self-examination/mammogram in the past 12 months?”
Individual characteristics included age, education, socioeconomic status, occupation, age at menarche, marital status, age at marriage, number of live births, stillbirth, abortion, miscarriage, and menopause status. Women who married before the age of 19 years were classified as having an early marriage based on Indonesia’s legal age definition.
Behavioral factors included breastfeeding, smoking status, risky eating behavior, and contraception use. Respondents were asked whether they had a smoking habit, while dietary history was evaluated based on food consumption in the past week since the interview. Meanwhile, enhancing factors included obesity status (body mass index) and parental history of cancer-related deaths. The supporting factors, including health insurance ownership and accessibility to the nearest healthcare centers (measured in terms of distance, travel time, and cost), were also evaluated. The mean values were used to determine the cut-off for categorizing the latter variables.
We used IBM SPSS Statistics ver. 29.0 software (IBM Co., Armonk, NY, USA, RRID: SCR_002865) for all analyses. Descriptive data are represented as means and standard deviations (SD). Unconditional logistic regression was performed for bivariate and multivariate analysis to determine the odds ratio (OR) for each potential breast cancer risk factor. Variables with a p-value <0.25 in bivariate analysis were considered potential confounders and were included in the final model to calculate the adjusted odds ratio (aOR). Statistical significance was determined at p-value <0.05, while p-values <0.10 indicated a tendency to associate. Missing data was excluded from the analysis of this study. All analyses were performed without weighting, as each data unit was assigned equal influence. The study adhered to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines to ensure rigorous reporting.
3. Results
3.1. Descriptive Characteristics
A total of 11,911 respondents were included in this study, with 6,926 and 4,983 in urban and rural areas, respectively (Figure 1). Table 1 shows that urban respondents had a lower average age and age at menarche than rural respondents (35.9 vs 36.9 years and 13.9 vs 14.1 years, respectively). Meanwhile, the average age at marriage and menopause was higher in urban areas (22.1 vs 20.9 years and 47.2 vs 46.5 years).
3.2. Bivariate Analysis
Table 2 shows the odds of breast cancer diagnosis based on various factors. In urban areas, women who performed BSE had 4 times higher odds of diagnosis breast cancer (OR 3.6; 95% CI 1.92-6.76), and those aware of mammograms had 5 times higher odds (OR 5.3; 95% CI 2.76-10.12). Furthermore, there is an 8-fold increase in odds for those who carried out a mammogram in the past year (OR 40.9; 95% CI 12.14-137.87). Additional risk factors included mariage before age 19 years (OR 2.5; 95% CI 1.14-5.63), health insurance ownership (OR 1.8; 95% CI 0.95-3.29), education level of at least in high school (OR 2.0; 95% CI 1.09-3.82), and lower economic status (quintile 1-3) with OR 3.2; 95% CI 1.15-8.72, OR 3.3; 95% CI 1.21-9.23, and OR 2.8; 95% CI 1.09-7.28, respectively. Meanwhile, in rural areas, the odds of being diagnosed with breast cancer were 10 times higher for women who had performed BSE (OR 9.9; 95% CI 3.46-28.42), and 6 times higher for those who heard of mammograms (OR 5.7; 95% CI 1.59-20.35). Other significant risk factors included early marriage (OR 2.7; 95% CI 0.89-8.38), a history of paternal cancer-related death (OR 19.9; 95% CI 4.35-91.47), and lower economic status (quintiles 2 and 3) (OR 10.7; 95% CI 1.19-96.39, and OR 8.2; 95% CI 0.92-73.97).
3.3. Multivariate Analysis
The multivariate analysis showed that in urban areas, women who had undergone a mammogram in the past 12 months had significantly higher odds of being diagnosed with breast cancer (aOR 48; 95% CI 10.33-83.45) Additionally, women who had performed BSE had 10 times higher odds (aOR 10.22; 95% CI 1.04-50.81) and 5 times if age at marriage below 19 years (aOR 4.8; 95% CI 1.93-6.05). In rural areas, the odds of breast cancer were 11 times higher among women who had performed BSE (aOR 11.1; 95% CI 3.32-37.08) and greater in those who aged at marriage below 19 years (adOR 5.3; 95% CI 1.49-19.08) while those with a paternal history of cancer-related death had 19.4 times higher odds(aOR 19.4; 95% CI 3.75-100.78) (Table 3).
4. Discussion
This study is the first to associate the breast cancer risk factors, stratified by urban and rural areas in Indonesia, using secondary data from the longitudinal Indonesian Family Life Survey (IFLS). The results confirmed that higher screening participation is strongly associated with breast cancer diagnosis in both settings. Despite the critical role of screening in breast cancer management, preventive initiatives in Indonesia remain underpromoted and underutilized [19]. Similar patterns of low screening participation have been observed in other LMICs, including countries in Africa and India [20,21]. The underlying causes may include limited patient preference, insufficient physician recommendations, and systemic barriers to healthcare access [8,9].
Our findings indicated that women who participate in screening are more likely to be diagnosed with breast cancer. This conclusion is corroborated by a previous study mentioning that increased screening efforts aligned with the rising incidence of breast cancer. Early diagnosis of breast cancer facilitates timely treatment, leading to higher survival rates and lower mortality rates [3]. While mammography, a gold standard breast cancer screening [3], is occasionally criticized for false positives, false negatives, and overdiagnosis [22], yet its role in reducing breast cancer death are well-documented [23]. Another screening for breast cancer, BSE, continues to be promoted as an accessible screening method in Indonesia despite ongoing debates regarding its effectiveness [19,24]. While less accurate than mammograms, BSE is feasible, economical, and serves as an option for women under 40 years or those without access to mammography. Evidence suggests that BSE can aid in early tumor detection and improve survival outcomes [25,26,27]. A randomized controlled trial in Iran concluded that the women trained in regular BSE were diagnosed at earlier stages than the control group, thereby reducing breast cancer mortality [28]. However, limited knowledge about BSE techniques and timing remains a challenge, with many women unsure whether they are performing the procedure correctly [20,29]. Furthermore, intensifying BSE campaigns and incorporating mammography with well-trained healthcare personnel should be considered to broaden screening coverage.
This study also highlights significant geographic disparities in screening participation influenced by socioeconomic and healthcare-related factors. Women in rural areas face additional barriers, including limited healthcare facilities, insufficient physician advocacy, and fewer mammogram devices, as reported in previous studies in the United States and China [30]. Currently, Indonesia has only 43 mammograms registered in clinics and hospitals nationwide, with only four actively providing services [31]. These resources are disproportionately concentrated only in urban areas, further marginalizing rural populations. Additionally, economic constraints and lack of health insurance significantly influence participation in mammogram screening [11]. However, our results indicate that women having health insurance have a greater chance of diagnosing breast cancer (OR 1.78; 90% CI 0.954; 3.287) than uninsured women. It contradicts a report from other LMICs, where limited insurance coverage contributes to lower screening rates [27]. This discrepancy may be due to the fact that we do not distinguish whether the screening was self-initiated or based on a doctor’s recommendation. Individuals diagnosed with breast cancer may often receive a physician’s suggestion for routine mammography before the diagnosis. Although the implementation of Universal Health Coverage via the National Health Insurance program was established in Indonesia over one decade ago, mammography is recommended primarily for symptomatic cases [19]. To improve early detection, we recommend expanding resources to enhance mammogram accessibility, particularly in rural areas.
Socioeconomic conditions are critical determinants of screening participation and the occurrence of breast cancer and are correlated with the determination of marriage age. The percentage of early marriage, one of the risks of breast cancer in Indonesia, is relatively high at 11%. Delaying marriage may impose additional social and financial burdens on the family [32]. Our result stated that women who marry at a younger age had an increased chance of developing breast cancer. Previous studies suggest that the risk of developing breast cancer decreases by 17% for each additional year of delayed marriage [33,34].
Beyond systemic and socioeconomic barriers, cultural and personal factors also play a role. In Indonesia, breast cancer screening remains taboo for many women due to embarrassment or sensitivity regarding body exposure. In some cases, women must obtain their husband’s permission for check-ups at health facilities. Fear of pain during mammograms, apprehension about test results, and lack of awareness regarding the benefits of routine screening further discourage participation [27,29,35]. To increase screening practices, effective public health campaigns focusing on the causes, risks, and symptoms of breast cancer are essential to address these challenges [20]. Health promotion efforts should leverage diverse communication channels, including mass media and community-based interventions, to enhance awareness and engagement [36].
We also suggested the potential influence of genetics on breast cancer risk. A strong family history, particularly among first-degree relatives, significantly increases the risk [37]. In our study, the analysis reported that a history of paternal death due to cancer is associated with breast cancer risk, both before and after controlling for confounders, particularly in rural populations. While the underlying mechanism remains unclear, previous studies found that the history of paternal cancer was associated with an increased incidence of lobular breast cancer in descendants (OR 1.9; 95% CI 1.2-2.8), potentially due to genetic alleles in the father that predispose daughters to breast cancer [38].
A large sample size with very few missing datasets is an advantage of this study. However, limitations include potential recall bias from self-reported data and differences in case-control sample sizes when stratified by residence. Social desirability bias may result in overreporting data in some responses, although this is unlikely to have differentially affected the groups [39]. Furthermore, our study could not eliminate screening bias; women diagnosed with cancer may experience increased screening frequency due to symptoms, genetic predispositions, or physician recommendations.
5. Conclusions
In conclusion, the results of this study provide strong evidence for initiating a nationwide breast cancer screening program. Intensifying the BSE campaign and enhancing mammography infrastructure and resources, especially in rural areas, will facilitate seamless implementation and enhance early detection efforts. Further in-depth studies with larger sample sizes were necessary to explore the underlying reasons for the low uptake of screening practices and to develop targetted interventions for improving breast cancer prevention and early diagnosis in Indonesia.
Author Contributions
Conceptualization, P.R. and R.A.D.S.; methodology, P.R. and R.A.D.S.; validation, I.I..; formal analysis, P.N.L. and E.P.; investigation, P.N.L. and E.P..; resources, A.A.I.; writing—original draft preparation, R.A.D.S. and P.L..; writing—review and editing, R.A.D.S., P.L., I.I., E.W.; funding acquisition, R.A.D.S. All authors have read and agreed to the published version of the manuscript
Funding
This research is funded by the Directorate of Research and Development (https://research.ui.ac.id/research/), Universitas Indonesia under Hibah PUTI 2024 (Grant No. NOMOR: NKB-361/UN2.RST/HKP.05.00/2024).
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Institutional Review Board (or Ethics Committee) of Universitas YARSI with reference number: 024/KEP-UY/EA.10/I/2025. The surveys and procedures in IFLS, publicly available data, received approval from the following ethics committees: the Institutional Review Board (IRB) of RAND Corporation and the Universitas Gajah Mada, under ethical clearance number s0064-06-01-CR01. Additional information concerning ethical approval can be found at https://www.rand.org/labor/FLS/IFLS.html.
Informed Consent Statement
The IRB evaluated the written informed consent obtained from participants, which was addressed in the context. No identifiers have been incorporated into the manuscript.
Data Availability Statement
The datasets are available in the RAND Corporation’s website as the institute that conducted the survey and owned the IFLS data: https://www.rand.org/well-being/social-and-behavioral-policy/data/FLS/IFLS.html.
Acknowledgments
This research is funded by the Directorate of Research and Development, Universitas Indonesia, under Hibah PUTI 2022 (Grant No. NKB-361/UN2.RST/HKP.05.00/2024).
Conflicts of Interest
The authors declare no conflicts of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
Abbreviations
The following abbreviations are used in this manuscript:
| IARC | International Agency for Research on Center |
| IFLS | Indonesia Family Life Survey |
| BSE | Breast-Self Examination |
| LMIC | Low- and Middle-Income Countries |
| aOR | Adjusted Odds Ratio |
| CI | Confidence Interval |
References
- Bray F, Laversanne M, Sung H, Ferlay J, Siegel RL, Soerjomataram I, Jemal A. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA A Cancer J Clinicians [Internet]. 2024 May [cited 2024 Dec 14];74(3):229–63. [CrossRef]
- de Souza JA, Hunt B, Asirwa FC, Adebamowo C, Lopes G. Global Health Equity: Cancer Care Outcome Disparities in High-, Middle-, and Low-Income Countries. Journal of clinical oncology : official journal of the American Society of Clinical Oncology. 2016;34(1):6–13.
- Lim YX, Lim ZL, Ho PJ, Li J. Breast Cancer in Asia: Incidence, Mortality, Early Detection, Mammography Programs, and Risk-Based Screening Initiatives. Cancers [Internet]. 2022 Aug 30 [cited 2024 Dec 24];14(17):4218. Available from: https://www.mdpi.com/2072-6694/14/17/4218.
- Fu M, Peng Z, Wu M, Lv D, Li Y, Lyu S. Current and future burden of breast cancer in Asia: A GLOBOCAN data analysis for 2022 and 2050. The Breast [Internet]. 2025 Feb [cited 2025 Mar 13];79:103835. Available from: https://linkinghub.elsevier.com/retrieve/pii/S0960977624001668. [CrossRef]
- The Global Cancer Observatory. The Global Cancer Observatory - Indonesia [Internet]. 2022. Available from: https://gco.iarc.who.int/media/globocan/factsheets/populations/360-indonesia-fact-sheet.pdf.
- Camacho R, Sepúlveda C, Neves D, Piñeros M, Villanueva M, Dangou JM, Fadhil I, Galea G, Garg R, Luciani S. Cancer control capacity in 50 low- and middle-income countries. Global Public Health [Internet]. 2015 Oct 21 [cited 2024 Aug 9];10(9):1017–31. [CrossRef]
- Diaz A, Kang J, Moore SP, Baade P, Langbecker D, Condon JR, Valery PC. Association between comorbidity and participation in breast and cervical cancer screening: A systematic review and meta-analysis. Cancer Epidemiology [Internet]. 2017 Apr [cited 2025 Mar 19];47:7–19. Available from: https://linkinghub.elsevier.com/retrieve/pii/S1877782116302533. [CrossRef]
- Orwat J, Caputo N, Key W, De Sa J. Comparing Rural and Urban Cervical and Breast Cancer Screening Rates in a Privately Insured Population. Social Work in Public Health [Internet]. 2017 Jul 4 [cited 2024 Dec 9];32(5):311–23. [CrossRef]
- Simo RT, Baiguerel EM, Nwabo Kamdje AH, Seke Etet PF, Ahmadou M, Nangue C, Telefo PB. Awareness of Breast Cancer Screening among the Medical and General Population of the North Region of Cameroon. Sahgal P, editor. International Journal of Breast Cancer [Internet]. 2021 Jul 27 [cited 2024 Jul 29];2021:1–7. Available from: https://www.hindawi.com/journals/ijbc/2021/6663195/. [CrossRef]
- Wahidin M, Febrianti R, Susanty F, Hasanah S. Twelve Years Implementation of Cervical and Breast Cancer Screening Program in Indonesia. Asian Pac J Cancer Prev [Internet]. 2022 Mar 1 [cited 2024 Jul 29];23(3):829–37. Available from: http://journal.waocp.org/article_90018.html. [CrossRef]
- Fei X, Wu J, Kong Z, Christakos G. Urban-Rural Disparity of Breast Cancer and Socioeconomic Risk Factors in China. Coleman WB, editor. PLoS ONE [Internet]. 2015 Feb 17 [cited 2024 Dec 9];10(2):e0117572. [CrossRef]
- Nelson HD, Darney BG, Ahrens K, Burgess A, Jungbauer RM, Cantor A, Atchison C, Eden KB, Goueth R, Fu R. Associations of Unintended Pregnancy With Maternal and Infant Health Outcomes: A Systematic Review and Meta-analysis. JAMA [Internet]. 2022 Nov 1 [cited 2022 Dec 9];328(17):1714. Available from: https://jamanetwork.com/journals/jama/fullarticle/2797874. [CrossRef]
- N. Hamajima, K. Hirose, K. Tajima, T. Rohan, C. M. Friedenreich, E. E. Calle, S. M. Gapstur, S. M. Gapstur, S. M. Gapstur, J. M. Liff, R. Talamini, N. Chantarakul, S. Koetsawang, D. Rachawat, Y. Marcou, E. Kakouri, S. W. Duffy, A. Morabia, L. Schuman, W. Stewart, M. Szklo, P. F. Coogan. Menarche, menopause, and breast cancer risk: individual participant meta-analysis, including 118 964 women with breast cancer from 117 epidemiological studies. The Lancet Oncology [Internet]. 2012 Nov [cited 2024 Aug 9];13(11):1141–51. Available from: https://linkinghub.elsevier.com/retrieve/pii/S1470204512704254.
- Shete S, Deng Y, Shannon J, Faseru B, Middleton D, Iachan R, Bernardo B, Balkrishnan R, Kim SJ, Huang B, Millar MM, Fuemmler B, Jensen JD, Mendoza JA, Hu J, Lazovich D, Robertson L, Demark-Wahnefried W, Paskett ED, Rural Workgroup of the Population Health Assessment in Cancer Center Catchment Areas Initiative, Foulds A, Mrkva A, Bear T, Yuan JM, Ferketich A, Fisher J, Huerta T, McAlearney A, Gray D, Washington C, Fickle D, Aker H, Dickinson S, Lyu C, Kianersi S, Anderson H, Smith K, Ma D, Lillie H, Upshaw S, Dahman B, Wheeler D, Gal T, Ksinan A, Morris B, Miller C, Do E, Fugate-Laus K, Fallavollita W, Ginder G, Winn R, Loughran T, Fouad M, Bae S, Scarinci I, Baskin M, Daniel C, Hardy C, Farris P, Mori M, Zhang Z, McCrea-Robertson S, Greiner A, Doody D, Jensen R, Ellerbeck E, Chen R, Krebill H, Kurz D, Voges N, Batten G, Anderson R, Hauser L, Guterbock T, Desai R, Haaland B. Differences in Breast and Colorectal Cancer Screening Adherence Among Women Residing in Urban and Rural Communities in the United States. JAMA Netw Open [Internet]. 2021 Oct 4 [cited 2024 Dec 9];4(10):e2128000. Available from: https://jamanetwork.com/journals/jamanetworkopen/fullarticle/2784628. [CrossRef]
- Gabrielle LeBlanc, Inkoo Lee, Henry Carretta, Yi Luo, Debajyoti Sinha, George Rust1. Rural-Urban Differences in Breast Cancer Stage at Diagnosis. Women’s Health Report. 2022;3(1):207–14. [CrossRef]
- Theodoropoulos, Xie, Wang, Wen, Li. Rural-urban differences in breast and colorectal cancer screening among US women, 2014-2019. RRH [Internet]. 2022 Sep 11 [cited 2024 Dec 9]; Available from: https://www.rrh.org.au/journal/article/7339.
- Frankenberg E, Hamilton P, Polich S, Suriastini W, Thomas D. User’s Guide for the Indonesia Family Life Survey, Wave 2: Volume 2 [Internet]. RAND; 2000. Available from: https://sites.rand.org/labor/family/software_and_data/FLS/IFLS/IFLS2/doc/volume2.zip.
- Ministry of Health. Basic Health Research 2018 (Riskesdas 2018) [Internet]. 2019. Available from: https://repository.badankebijakan.kemkes.go.id/id/eprint/3514/.
- Ministry of Health. Pedoman Nasional Pelayanan Kedokteran Tata Laksana Kanker Payudara [Internet]. 2018. Available from: https://www.kemkes.go.id/id/pnpk-2018---tata-laksana-kanker-payudara.
- Osei-Afriyie S, Addae AK, Oppong S, Amu H, Ampofo E, Osei E. Breast cancer awareness, risk factors and screening practices among future health professionals in Ghana: A cross-sectional study. Laganà AS, editor. PLoS ONE [Internet]. 2021 Jun 24 [cited 2024 Jul 29];16(6):e0253373. [CrossRef]
- Pouryousef S, Pirzadeh Z, Keshavarzi S, Kargar Jahromi M, Rousta A. Breast Cancer Knowledge, Attitude, and Preventive Behaviors and Associated Factors in Women Visiting the Oncology Research and Treatment Center in Southern Fars (City of Gerash). Indian J Gynecol Oncolog [Internet]. 2024 Sep [cited 2024 Aug 13];22(3):98. [CrossRef]
- Løberg M, Lousdal ML, Bretthauer M, Kalager M. Benefits and harms of mammography screening. Breast Cancer Res [Internet]. 2015 Dec [cited 2024 Aug 16];17(1):63. [CrossRef]
- Canelo-Aybar C, Ferreira DS, Ballesteros M, Posso M, Montero N, Solà I, Saz-Parkinson Z, Lerda D, Rossi PG, Duffy SW, Follmann M, Gräwingholt A, Alonso-Coello P. Benefits and harms of breast cancer mammography screening for women at average risk of breast cancer: A systematic review for the European Commission Initiative on Breast Cancer. J Med Screen [Internet]. 2021 Dec [cited 2024 Aug 12];28(4):389–404. [CrossRef]
- Dietze E, Jones V, Seewaldt V. Breast Self-Examination: the Case for a Second Look. Curr Breast Cancer Rep [Internet]. 2020 Jun [cited 2024 Aug 16];12(2):118–24. [CrossRef]
- Coleman C. Early Detection and Screening for Breast Cancer. Seminars in Oncology Nursing [Internet]. 2017 May [cited 2024 Jul 29];33(2):141–55. Available from: https://linkinghub.elsevier.com/retrieve/pii/S0749208117300190.
- Icanervilia A, Choridah L, Van Asselt A, Vervoort J, Postma M, Rengganis A, Kardinah K. Early Detection of Breast Cancer in Indonesia: Barriers Identified in a Qualitative Study. Asian Pac J Cancer Prev [Internet]. 2023 Aug 1 [cited 2024 Jul 29];24(8):2749–55. Available from: https://journal.waocp.org/article_90754.html. [CrossRef]
- Majidi A, Majidi S, Salimzadeh S, Khazaee-Pool M, Sadjadi A, Salimzadeh H, Delavari A. Cancer Screening Awareness and Practice in a Middle Income Country; A Systematic Review from Iran. Asian Pac J Cancer Prev [Internet]. 2017 Dec [cited 2024 Jul 29];18(12). [CrossRef]
- Hassan LM, Mahmoud N, Miller AB, Iraj H, Mohsen M, Majid J, Reza SM, Mojgan M. Evaluation of effect of self-examination and physical examination on breast cancer. The Breast [Internet]. 2015 Aug [cited 2024 Aug 13];24(4):487–90. Available from: https://linkinghub.elsevier.com/retrieve/pii/S0960977615001058. [CrossRef]
- Choridah L, Icanervilia AV, De Wit MJM, Van Asselt ADI, Kurniawan WT, Fahmi YI, Rengganis AA. Knowledge and Acceptance Towards Mammography as Breast Cancer Screening Tool Among Yogyakarta Women and Health Care Providers (Mammography Screening in Indonesia). J Canc Educ [Internet]. 2021 Jun [cited 2024 Aug 16];36(3):532–7. [CrossRef]
- Tran L, Tran P. US urban–rural disparities in breast cancer-screening practices at the national, regional, and state level, 2012–2016. Cancer Causes Control [Internet]. 2019 Oct [cited 2024 Dec 9];30(10):1045–55. [CrossRef]
- Ida Bagus Gede Putra Pratama. Diagnostic Reference Level (DRL) dan Status Terkini di Indonesia [Internet]. Nuclear Energy Regulatory Agency; 2020. Available from: https://bapeten.go.id/upload/14/192c8353e1-drl-dan-status-terkini-di-indonesia.pdf.
- Wibowo HR, Ratnaningsih M, Goodwin NJ, Ulum DF, Minnick E. One household, two worlds: Differences of perception towards child marriage among adolescent children and adults in Indonesia. The Lancet Regional Health - Western Pacific [Internet]. 2021 Mar [cited 2024 Dec 25];8:100103. Available from: https://linkinghub.elsevier.com/retrieve/pii/S2666606521000122. [CrossRef]
- Lai T, Huang Y, Xiong J. Changes in behavior patterns or demographic structure? Re-estimating the impact of higher education on the average age of the first marriage. Front Psychol [Internet]. 2023 Jan 27 [cited 2024 Dec 22];14:1085293. [CrossRef]
- Jahani MA, Ghasemi B, Soltani SA, Naderi M, Nikbakht HA, Hashemi SN, Yazdani Charati J, Mahmoudi G. The relationship between demographic factors and known risk factors with breast cancer in women aged 30-69. Annals of Medicine & Surgery [Internet]. 2024 May 3 [cited 2024 Dec 22]. [CrossRef]
- Anastasi N, Lusher J. The impact of breast cancer awareness interventions on breast screening uptake among women in the United Kingdom: A systematic review. J Health Psychol [Internet]. 2019 Jan [cited 2024 Jul 29];24(1):113–24. [CrossRef]
- The Lancet Oncology. Awareness campaigns and cancer screening. The Lancet Oncology [Internet]. 2022 Jul [cited 2024 Jul 29];23(7):829. Available from: https://linkinghub.elsevier.com/retrieve/pii/S1470204522003400.
- Brewer HR, Jones ME, Schoemaker MJ, Ashworth A, Swerdlow AJ. Family history and risk of breast cancer: an analysis accounting for family structure. Breast Cancer Res Treat [Internet]. 2017 Aug [cited 2024 Aug 12];165(1):193–200. [CrossRef]
- Ellberg C, Olsson H. Breast cancer patients with lobular cancer more commonly have a father than a mother diagnosed with cancer. BMC Cancer [Internet]. 2011 Dec [cited 2024 Aug 13];11(1):497. [CrossRef]
- Cronin KA, Miglioretti DL, Krapcho M, Yu B, Geller BM, Carney PA, Onega T, Feuer EJ, Breen N, Ballard-Barbash R. Bias Associated With Self-Report of Prior Screening Mammography. Cancer Epidemiology, Biomarkers & Prevention [Internet]. 2009 Jun 1 [cited 2024 Dec 14];18(6):1699–705. Available from: https://aacrjournals.org/cebp/article/18/6/1699/66967/Bias-Associated-With-Self-Report-of-Prior.
Figure 1.
STROBE Flow Diagram of Case-Control Studies.
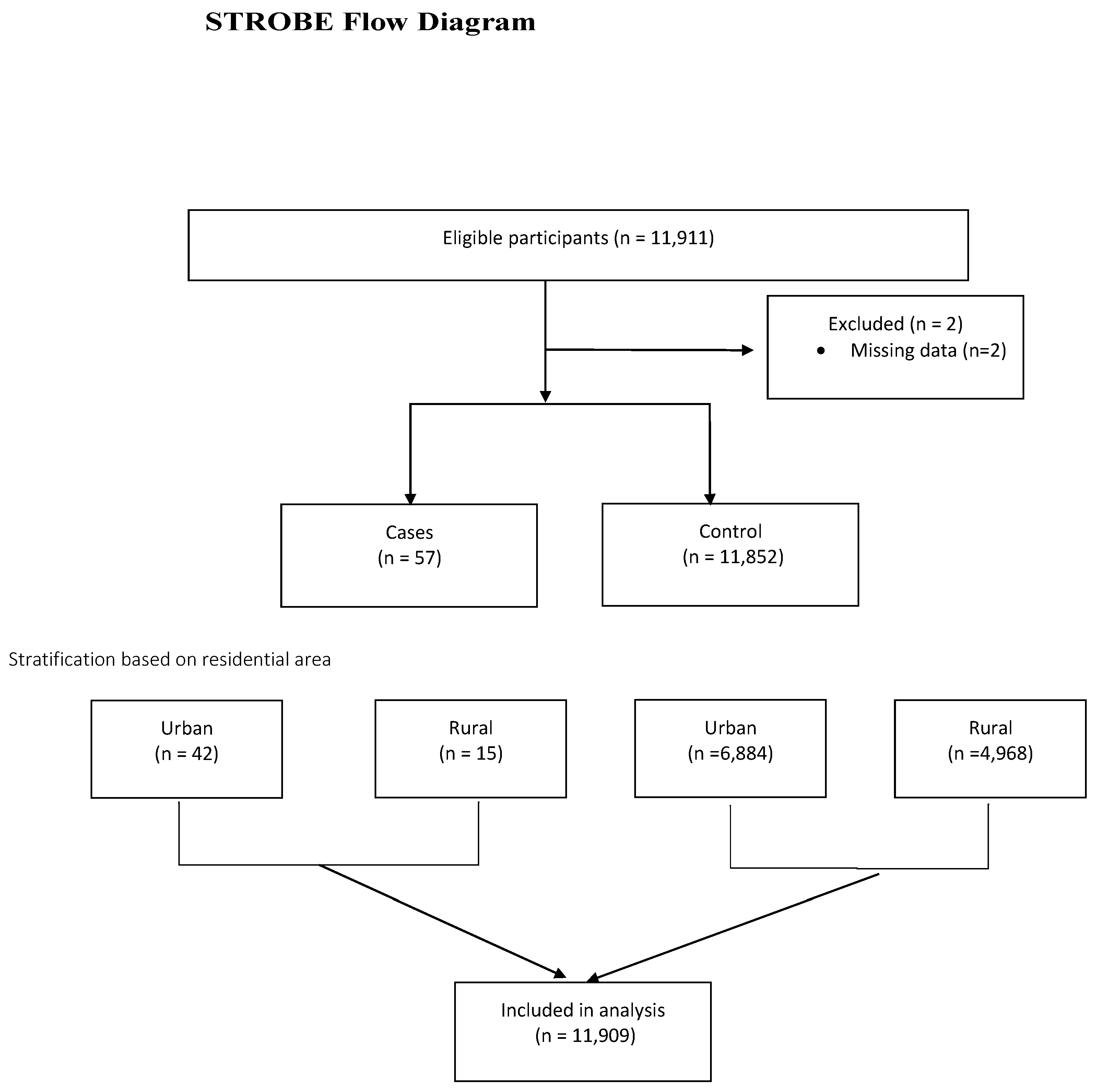

Table 1.
Characteristic of respondents.
| Variables |
Urban (n=6926) | Rural (n=4983) |
|---|---|---|
| Mean+SD (min-max) | Mean+SD (min-max) | |
| Age (2007; years) | 35.86+14.11 (15-94) | 36.92+15.13 (15-88) |
| Age at menarche (years) | 13.88+1.61 (12-41) | 14.05+1.77 (12-64) |
| Age at marriage (years) | 22.08+5.45 (15-70) | 20.97+5.46 (15-55) |
| Menopausal age (years) | 47.17+4.47 (25-58) | 46.45+4.81 (27-57) |
Table 2.
Association between screening practices, individual and sociodemographic characteristics, and breast cancer in urban and rural areas.
Table 2.
Association between screening practices, individual and sociodemographic characteristics, and breast cancer in urban and rural areas.
| Risk factors | Urban (n=6926) | Rural (n=4983) | ||||||
|---|---|---|---|---|---|---|---|---|
| Case | Control | Case | Control | |||||
| n (%) | n (%) | p-value | OR (95%CI) | n (%) | n (%) | p-value | OR (95%CI) | |
| Breast self-examination | ||||||||
| Ever | 19 (48.7) | 1375 (20.9) | 0.000* | 3.6 (1.916;6.763) | 7 (50.0) | 429 (9.2) | 0.000* | 9.923 (3.464;28.423) |
| Never | 20 (51.3) | 5210 (79.1) | 7 (50.0) | 4257 (90.8) | ||||
| Have heard about mammograms | ||||||||
| Yes | 14 (35.0) | 611 (9.2) | 0.000* | 5.304 (2.755;10.120) | 3 (20.0) | 198 (4.2) | 0.024* | 5.697 (1.595;20.350) |
| No | 26 (65.0) | 6018 (90.8) | 12 (80.0) | 4512 (95.8) | ||||
| Have a mammogram test in the last 12 months | ||||||||
| Perform | 6 (42.9) | 11 (1.8) | 0.000* | 40.909 (12.139;137.866) | 0 (0.0) | 2 (1.0) | 1.000 | NA |
| Not perform | 8 (57.1) | 600 (98.2) | 3 (100) | 196 (99.0) | ||||
| Have health insurance | ||||||||
| Yes | 17 (40.5) | 1910 (27.7) | 0.096+ | 1.771 (0.954;3.287) | 5 (33.3) | 1009 (20.3) | 0.206 | 1.962 (0.669;5.752) |
| No | 25 (59.5) | 4974 (72.3) | 10 (66.7) | 3959 (79.7) | ||||
| Age | ||||||||
| > 40 years | 12 (28.6) | 2445 (35.5) | 0.438 | 0.726 (0.371;1.421) | 7 (46.7) | 1908 (38.4) | 0.696 | 1.403 (0.508;3.876) |
| < 40 years | 30 (71.4) | 4439 (64.5) | 8 (53.3) | 3060 (61.6) | ||||
| Age at menarche | ||||||||
| < 14 years | 19 (61.3) | 2312 (45.5) | 0.114 | 1.898 (0.920;3.919) | 5 (38.5) | 1509 (40.1) | 1.000 | 0.934 (0.305;2.859) |
| > 14 years | 12 (38.7) | 2772 (54.5) | 8 (61.5) | 2254 (59.9) | ||||
| Age at marriage | ||||||||
| < 19 years | 25 (75.8) | 3089 (55.2) | 0.018* | 2.536 (1.142;5.633) | 8 (61.5) | 1564 (36.9) | 0.084+ | 2.738 (0.894;8.383) |
| > 19 years | 8 (24.2) | 2507 (44.8) | 5 (38.5) | 2676 (63.1) | ||||
| Marital status | ||||||||
| Not married | 4 (9.5) | 448 (6.5) | 0.351 | 1.512 (0.537;4.256) | 1 (6.7) | 169 (3.4) | 0.406 | 2.028 (0.265;15.514) |
| Married | 38 (90.5) | 6436 (93.5) | 14 (93.3) | 4799 (96.6) | ||||
| Occupation status | ||||||||
| Unemployment | 20 (47.6) | 2565 (37.3) | 0.221 | 1.531 (0.834;2.810) | 3 (20.0) | 1592 (32.0) | 0.413 | 0.530 (0.149;1.881) |
| Employment | 22 (52.4) | 4319 (62.7) | 12 (80.0) | 3376 (68.0) | ||||
| Education level | ||||||||
| High school or higher education | 26 (61.9) | 3047 (44.3) | 0.032* | 2.046 (1.096;3.821) | 6 (40.0) | 1087 (21.9) | 0.113 | 2.380 (0.845;6.702) |
| Less than high school | 16 (38.1) | 3837 (55.7) | 9 (60.0) | 3881 (78.1) | ||||
| Tobacco smoking | ||||||||
| Yes | 1 (2.4) | 169 (2.5) | 1.000 | 0.969 (0.133;7.087) | 1 (6.7) | 199 (4.0) | 0.460 | 1.712 (0.224;13.082) |
| No | 41 (97.6) | 6715 (97.5) | 14 (93.3) | 4769 (96.0) | ||||
| Consumption of meat | ||||||||
| 1-7 days/week | 32 (76.2) | 4694 (68.2) | 0.345 | 1.493 (0.733;3.042) | 11 (73.3) | 2518 (50.7) | 0.135 | 2.676 (0.851;8.414) |
| 0 day/week | 10 (23.8) | 2190 (31.8) | 4 (26.7) | 2450 (49.3) | ||||
| Consumption of fruit and vegetable | ||||||||
| < 7 days/week | 15 (37.5) | 2534 (38.2) | 1.000 | 0.969 (0.510;1.842) | 5 (33.3) | 2021 (42.9) | 0.626 | 0.665 (0.227;1.949) |
| >7 days/week | 25 (62.5) | 4094 (61.8) | 10 (66.7) | 2689 (57.1) | ||||
| Consumption of instant food and soda drink | ||||||||
| > 7 days/week | 1 (2.5) | 468 (7.1) | 0.526 | 0.337 (0.046;2.462) | 1 (6.7) | 370 (7.9) | 1.000 | 0.838 (0.110;6.389) |
| <7 days/week | 39 (97.5) | 6160 (92.9) | 14 (93.3) | 4340 (92.1) | ||||
| Body mass index | ||||||||
| > 25 kg/m2 | 15 (35.7) | 3301 (48.0) | 0.151 | 0.602 (0.320;1.133) | 6 (40.0) | 1947 (39.2) | 1.000 | 1.033 (0.367;2.907) |
| < 25 kg/m2 | 27 (64.3) | 3575 (52.0) | 9 (60.0) | 3017 (60.8) | ||||
| Number of births | ||||||||
| > 1 child | 13 (31.7) | 2956 (44.3) | 0.145 | 0.585 (0.302;1.131) | 8 (53.3) | 2252 (47.4) | 0.839 | 1.270 (0.460;3.507) |
| No child | 28 (68.3) | 3722 (55.7) | 7 (46.7) | 2502 (52.6) | ||||
| History of breastfeeding | ||||||||
| Never | 0 (0) | 82 (4.6) | 1.000 | NA | 0 (0.0) | 76 (6.0) | 1.000 | NA |
| Ever | 10 (100) | 1684 (95.4) | 4 (100) | 1183 (94.0) | ||||
| History of stillbirth | ||||||||
| Yes | 0 (0.0) | 87 (1.3) | 1.000 | NA | 0 (0.0) | 85 (1.8) | 1.000 | NA |
| No | 41 (100) | 6591 (98.7) | 15 (100) | 4669 (98.2) | ||||
| History of miscarriage | ||||||||
| Yes | 2 (4.9) | 444 (6.6) | 1.000 | 0.720 (0.173;2.992) | 1 (6.7) | 302 (6.4) | 1.000 | 1.053 (0.138;8.034) |
| No | 39 (95.1) | 6234 (93.4) | 14 (93.3) | 4452 (93.6) | ||||
| History of abortion | ||||||||
| Ever | 0 (0.0) | 47 (1.1) | 1.000 | NA | 0 (0.0) | 18 (0.6) | 1.000 | NA |
| Never | 28 (100) | 4344 (98.9) | 8 (100) | 3140 (99.4) | ||||
| Menopausal status | ||||||||
| Yes | 1 (2.4) | 136 (2.0) | 0.569 | 1.210 (0.165;8.862) | 1 (6.7) | 98 (2.0) | 0.260 | 3.550 (0.462;27.260) |
| No | 41 (97.6) | 6748 (98.0) | 14 (93.3) | 4870 (98.0) | ||||
| Oral contraception | ||||||||
| Ever | 15 (53.6) | 2241 (51.0) | 0.938 | 1.107 (0.526;2.332) | 4 (50.0) | 1474 (46.7) | 1.000 | 1.142 (0.285;4.576) |
| Never | 13 (46.4) | 2150 (49.0) | 4 (50.0) | 1684 (53.3) | ||||
| Injection contraception | ||||||||
| Ever | 18 (64.3) | 3187 (72.6) | 0.443 | 0.680 (0.313;1.477) | 4 (50.0) | 2402 (76.1) | 1.000 | 0.315 (0.079;1.261) |
| Never | 10 (35.7) | 1204 (27.4) | 4 (50.0) | 756 (23.9) | ||||
| Implant contraception | ||||||||
| Ever | 1 (3.6) | 292 (6.6) | 1.000 | 0.520 (0.070;3.840) | 0 (0.0) | 399 (12.6) | 0.607 | NA |
| Never | 27 (96.4) | 4099 (93.4) | 8 (100) | 2759 (87.4) | ||||
| Father died from cancer | ||||||||
| Yes | 1 (2.4) | 97 (1.4) | 0.451 | 1.707 (0.232;12.532) | 2 (13.3) | 38 (0.8) | 0.006* | 19.955 (4.353;91.472) |
| No | 41 (97.6) | 6787 (98.6) | 13 (86.7) | 4929 (99.2) | ||||
| Mother died from cancer | ||||||||
| Yes | 1 (2.4) | 96 (1.4) | 0.448 | 1.725 (0.235;12.666) | 0 (0) | 61 (1.2) | 1.000 | NA |
| No | 41 (97.6) | 6788 (98.6) | 15 (100) | 4906 (98.8) | ||||
| Healthcare accessibility (distance) | ||||||||
| > 5 km | 3 (18.8) | 300 (21.5) | 1.000 | 0.843 (0.239;2.978) | 3 (75.0) | 414 (48.1) | 0.357 | 3.239 (0.336;31.263) |
| < 5 km | 13 (81.3) | 1096 (78.5) | 1 (25.0) | 447 (51.9) | ||||
| Healthcare accessibility (time) | ||||||||
| >10 minutes | 6 (54.5) | 526 (40.0) | 0.364 | 1.802 (0.547;5.936) | 2 (50.0) | 447 (48.4) | 1.000 | 1.065 (0.149;7.592) |
| < 10 minutes | 5 (45.5) | 790 (60.0) | 2 (50.0) | 476 (51.6) | ||||
| Healthcare accessibility (price) | ||||||||
| IDR >16,500 | 0 (0.0) | 156 (10.7) | 0.392 | NA | 3 (75.0) | 444 (49.0) | 0.366 | 3.122 (0.323;30.122) |
| IDR < 16,500 | 15 (100) | 1301 (89.3) | 1 (25.0) | 462 (51.0) | ||||
| Socio-economic status (monthly household expenditure) | ||||||||
| Quintile 1 | 5 (11.9) | 1342 (19.5) | 0.026* | 3.160 (1.145;8.720) | 5 (33.3) | 1576 (31.7) | 0.133 | 2.747 (0.735;10.271) |
| Quintile 2 | 5 (11.9) | 1420 (20.6) | 0.020* | 3.344 (1.212;9.226) | 1 (6.7) | 1233 (24.8) | 0.034* | 10.745 (1.198;96.387) |
| Quintile 3 | 6 (14.3) | 1436 (20.9) | 0.033* | 2.818 (1.090;7.284) | 1 (6.7) | 946 (19.0) | 0.060+ | 8.244 (0.919;73.968) |
| Quintile 4 | 11 (26.2) | 1411 (20.5) | 0.301 | 1.510 (0.691;3.300) | 4 (26.7) | 754 (15.2) | 0.484 | 1.643 (0.409;6.600) |
| Quintile 5 | 15 (35.7) | 1274 (18.5) | 4 (26.7) | 459 (9.2) | ||||
Table 3.
Final multivariable determinants of breast cancer in urban and rural areas.
| Variables | Breast cancer | ||
|---|---|---|---|
| p-value | aOR | 95% CI | |
| Urban areasa | |||
| Have a mammogram test in the last 12 months | |||
| Not perform | Ref | 1 | |
| Perform | 0.000* | 48.038 | 10.327;83.453 |
| Breast self-examination | |||
| Never | Ref | 1 | |
| Ever | 0.046* | 10.223 | 1.037;50.809 |
| Age at marriage | |||
| >19 years | Ref | 1 | |
| <19 years | 0.052+ | 4.814 | 1.925;6.049 |
| Rural areasb | |||
| Breast self-examination | |||
| Never | Ref | 1 | |
| Ever | 0.000* | 11.102 | 3.324;37.077 |
| Age at marriage | |||
| >19 years | Ref | 1 | |
| <19 years | 0.010* | 5.345 | 1.498;19.071 |
| Father died from cancer | |||
| No | Ref | 1 | |
| Yes | 0.000* | 30.632 | 6.038;60.406 |
aOR, adjusted odds ratio; CI, confidence interval. a Initial model includes breast self-examination, heard about the mammogram, mammogram test, age at menarche, age at marriage, number of births, ownership of insurance, education level, occupation status, socio-economic status, and body mass index. b Initial model includes breast self-examination, heard about the mammogram, age at marriage, ownership of insurance, education level, meat consumption, socioeconomic status, and father died from cancer. *p-value < 0.05; +p-value < 0.10.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



