
Submitted:
28 February 2025
Posted:
02 March 2025
You are already at the latest version
Abstract
Background/Objectives: Romania remains endemic for measles due to suboptimal vaccine coverage rates. During the last three epidemics, the highest incidence of measles was recorded in children younger than 1 year, who should have been partially protected by maternal antibodies. A nationwide cross-sectional seroprevalence study was conducted on persons of fertile age to evaluate potential immunity gaps in the population. Methods: Between June and October 2020, 959 serum samples were col-lected from individuals aged 25-44 years (46.5% females) from all the geographic re-gions in Romania. Measles IgG antibodies were assessed using an enzyme-linked immune assay (DIA.PRO-Diagnostic Bioprobes Srl, Italy). Statistical analysis was performed in IBM SPSS Statistics 27.0, using Fisher’s exact and chi-squared tests to test for associations between seropositivity and demographic factors, with p < 0.05 con-sidered statistically significant. Results: The overall measles seroprevalence was 77%, without gender- or geographic region-related differences. Both the seropositivity rate and the measles antibodies titers increased with age, with the highest difference be-tween the oldest and the youngest age group (p=0.057), suggesting persistent im-munity after natural infection in older individuals or anamnestic responses in vac-cinated persons, caused by repeated exposures to the circulating virus. An additional confirmatory pilot study on 444 pregnant women confirmed the low level of measles seroprevalence (68.4%), with a significant upward trend in older ages (75% in those aged >40 years old vs. 65% in those aged 25-29 years, p=0.018 and mean reactivity of measles antibodies 3.05+/-1.75 in those aged > 40 years vs. 2.28+/-1.39 in those aged 25-29 years, p=0.037). Conclusions. This study signals critical immunity gaps in the population that contribute to the accumulation of susceptible individuals and recur-rent measles outbreaks. The absence of measles antibodies in women of childbearing age increases the newborn’s susceptibility to infection, with potentially severe com-plications.
Keywords:
seroprevalence
; measles
; Romania
; measles IgG Antibodies
; pregnant women
1. Introduction
Measles is one of the most contagious human diseases, with an estimated reproduction rate in a susceptible population (R0) of 9–18, surpassing all other viral diseases (e.g., chickenpox R0 = 5–7, polio R0 = 4–13) [1]. As such, a high vaccination coverage (>97% for both doses of measles vaccine and 95% measles immunity in children aged 1−9 years) is required to control virus transmission and to achieve the WHO elimination target [2,3,4]. Suboptimal vaccination coverage in specific regions and certain population groups, amplified by missed vaccine doses during the COVID-19 pandemic and by aggressive anti-vaccination campaigns, together with the increased population mobility, intensified by conflicts, war, climatic and economic displacements, have conducted to measles re-emergence worldwide [5].
In Europe, over 95,000 measles cases were reported in 2024 by the WHO Regional Office. A significant increase in measles cases has already been reported in 2023 [6] as a consequence of decreasing vaccine coverage rates during the COVID-19 pandemic, with six Central Eastern European countries experiencing significant epidemics: Kazakhstan, Azerbaijan, Kyrgyzstan, Romania, the Russian Federation, and Türkiye. Kazakhstan and Kyrgyzstan had the highest incidence in the age group 1-4 years. In comparison, the Russian Federation and Türkiye reported the most significant proportion of measles cases in adults aged 20 years and older [7]. Apart from Türkiye, all the previously affected areas remain endemic for measles in 2024: Kazakhstan (27 760 cases), Romania (21 738 cases), Azerbaijan (16 675 cases), Russian Federation (14 751 cases), Kyrgyzstan (12 587 cases) [8]. In the EU/EEA, Romania has the highest notification rate and the highest mortality rate, mostly in children less than 5 years old and unvaccinated [8]. These epidemics arise because of persistent cumulative immunity gaps in the population caused by suboptimal vaccination or waning immunity in countries with good immunization programs [9]. To detect these immunity gaps and to effectively control the spread of measles, seroepidemiological prevalence studies must be conducted as part of the verification process for disease elimination [10].
In Europe, the last seroprevalence study for measles virus infection was conducted between 1996-2004, by the European Seroepidemiology Network (ESEN 2), as part of a more extensive study on age-specific seroprevalence for eight vaccine-preventable diseases (measles, mumps, rubella, diphtheria, pertussis, varicella-zoster, hepatitis A, hepatitis B) [11]. The results showed that Romania was one of the seven countries considered at risk of measles epidemics due to high susceptibility in children [12]. Indeed, during the last 15 years, Romania has experienced three large-scale measles outbreaks: between 2011–2012 (12,234 confirmed cases and three deaths), between 2016 and 2020 (over 20 000 confirmed cases and 64 deaths) and between 2023-2024 (over 25 000 cases and 22 deaths, still ongoing) [13,14,15]. The susceptible population has been continuously amplified due to the suboptimal coverage rates with both doses of the measles-mumps-rubella vaccine registered during the last 10-15 years [16]. The most significant number of cases and deaths in all three epidemics have been recorded in children up to one year of age, who should have been partially protected by maternal antibodies transmitted trans-placentally and through breastfeeding. In this context, this study aimed to assess the seroprevalence of measles antibodies in Romania in persons of fertile ages to evaluate potential immunity gaps that leave newborns unprotected against measles and to inform specific targeted vaccination campaigns.
2. Materials and Methods
Subjects. (1) A nationwide cross-sectional study of individuals of fertile age was conducted in persons 25-44 years old, the age groups in which the highest birth rate is recorded in Romania, according to the Eurostat data [17]. The sample size was calculated using a validated sampling strategy [18] to ensure regional and age group representativeness, considering the proportionality criterion by geographic regions, gender, and age groups. A sample size of 959 subjects was established as statistically significant using the following formula in EpiInfo 7 Program: n = [DEFF*Np(1-p)]/ [(d2/Z21-α/2*(N-1)+p*(1-p)] - where n represents the sample size, DEFF- the design effect for cluster surveys (1); N -the population size; p- the probability (50%); d -the error proportion (0.05), z -factor based on the confidence level (Z = 1.96 for a 95 percent confidence level) and 1-α -the level of confidence (95%). The 959 samples were selected and grouped into four age groups: 25-29 years, 30-34 years, 35-39 years, and 40-44 years, according to the demographic data published by the National Institute of Statistics [19]. The serum samples were collected between July and October 2020, within a seroprevalence study initially designed for COVID-19, and stored at -800C in the National Institute for Public Health (NIPH) laboratory. The study was performed on completely anonymized, randomly selected remaining samples, for which informed consent for research use was previously obtained from individual patients. The study was approved by the Ethics Commission of the NIPH (Nr. 10056/22.05.2023).
(2) Prospective pilot study on pregnant women. To further confirm the seroprevalence results, a prospective pilot study was conducted in 444 pregnant women aged 25-45 years, randomly selected from those routinely monitored during pregnancy in a tertiary hospital in Bucharest between 2022-2023.
Anti-measles IgG antibodies testing. For both studies, measles IgG antibodies were tested using an enzyme-linked immune assay (Measles Virus IgG, DIA.PRO-Diagnostic Bioprobes Srl, Italy), with results expressed as reactivity (a ratio between the 450 nm optical density of the sample and the cut-off). According to the manufacturer protocol, the results were considered negative if < 1 and positive if ≥ 1.
Statistical analysis was performed using IBM SPSS Statistics 27.0 for Windows utilizing the Percentage Difference Calculation Test (Z) and corresponding confidence intervals of 95% (95% CI), with p < 0.05 considered statistically significant. Stratified analysis of the measles seroprevalence by age groups and by regions vs national was performed in STATA /MP13.1 for Windows using the Percentage Difference Calculation Test (Z) and corresponding confidence intervals of 95% (95% CI), with p < 0.05 considered statistically significant.
3. Results
Measles seroprevalence in individuals of fertile age. The mean age of the 959 enrolled individuals was 35.2 +/- 0.18 years and 46.5 % (n = 446) were females. There was a balanced distribution of age groups, genders, and geographic regions (Table 1): 3.2. Evolution of vaccine coverage rates
The overall seroprevalence of IgG anti-measles antibodies was 77%, without significant gender differences (77.4% in females and 76.6% in males). The measles seroprevalence rate increases with age, with the highest rates of seropositivity (Table 2) achieved in the age group 40-44 years.
There are no statistically significant differences in the measles seroprevalence rates by geographic region, nor in the seroprevalence rates of different age groups from the different areas compared to the national seroprevalence (Table 3).
Analysis of measles antibodies reactivities. Using reactivities as a surrogate for measles antibody titers, we analyzed the mean values between the age groups included in the study. Using the Dunnett t-test (treat one group as a control and compare all other groups against it) and corresponding confidence intervals of 95%, with p < 0.05 considered statistically significant, the highest difference is registered between the youngest age group studied (25-29 years) and the oldest age group (40-44 years), with marginal statistical significance (Table 4). For the other age groups, there are no statistically significant differences in the reactivity values (Table 4).
For measles seropositive samples, the reactivities increase significantly with age (from a mean of 4.28 ± 0.32 in those aged 25-29 to 5.40 ± 0.28 in those aged 40-44, p=0.057). Figure 1.
Measles seroprevalence in pregnant women. The mean age of the enrolled pregnant women was 31.5±5.7 years, and the mean gestational age was 21.8±9.8 weeks. Only 68.4% of pregnant women had IgG measles antibodies, with a mean reactivity value of 2,595 ±1,438. There is no significant difference between the seropositive and seronegative women according to the mean age (31.8 ± 0.3 years vs 31.2 ± 0.3 years, p=0.22) or urban/rural residence (70.5% vs 67.7%, p=0.3). The seropositivity rate is significantly higher for women aged > 40 years (75% vs 65% in younger women, p=0.018). The mean reactivity of measles antibodies in pregnant women has a significant upward trend by age groups (from 2.28 ±1.39 in those aged 25-29 years to 3.05 ±1.75 in those aged > 40 years, p=0.037), Figure 2.
4. Discussion
According to the results of the ESEN 2 seroprevalence study [11] in Romania, in 2002, the rate of measles seronegative adults was 1.4% for the age group 20-39 years and 0.3 % for those aged 40+ years). In the present study, we showed a marked increase, up to 23%, in the rate of measles seronegative individuals aged 25-45 years. All these individuals, except those aged 40-44 years, should have been vaccinated, as the measles vaccine was introduced in the national immunization program in 1979 in Romania. Although we did not have access to the vaccination records, the low measles seropositivity can be due to (a) lack of vaccination, (b) lack of seroconversion after vaccination due to primary vaccine failure [20], or breaches in the cold chain during vaccine transport or storage [21], (c) waning of measles antibodies [22]. A lower seroconversion rate after vaccination could be an explanation for individuals aged 30-39 years, representing the 1981-1990 birth cohorts, who should have received a single dose of measles vaccine administered at the age of 9-11 months, following the national vaccination schedule valid in Romania from 1979 till 1995. Vaccination at a younger age is less immunogenic, and measles vaccine efficacy in infants younger than 9 months was estimated to be 58% compared to 83% in those 9 months or older [23]. Several studies have also reported the waning of measles antibodies years after vaccination [24,25,26,27], and the antibody’s level after vaccination is often lower than that induced by natural measles virus infection [28,29]. Mathematical modeling has suggested that the waning of vaccine-induced immunity might be compatible with the recent trends in measles cases in England, with the rising number of breakthrough infections among individuals who have received two doses of the measles vaccine [30] and in Germany [31]. Nevertheless, in our cohort, the seropositivity rate and the measles antibody titers are lower in the youngest age group compared to the older age groups, making waning a less probable hypothesis. Instead, in our measles endemic setting, the higher titers of measles antibodies in older individuals suggest life-long immunity following measles infection (most probable for the age group 40-44 years, born before the introduction of measles vaccination) or multiple anamnestic responses in vaccinated individuals, with vaccine-induced antibodies boosted by repeated exposures to the circulating virus. Additionally, we did not detect gender-related differences in the measles seropositivity rate or antibody titers, although vaccine-induced immune responses might differ between males and females [32], supporting hybrid immunity or gained after natural infection. The low seroprevalence seen in this study in young individuals (both in the nationwide study on those of fertile age and in the pilot study on pregnant women) probably reflects the continuously decreasing vaccine coverage rates reported in Romania [16]. These individuals, aged 25-29 years, should have received a complete measles vaccination regimen, as they were born after the introduction 1995 of a second routine measles vaccine dose in the national immunization program. The lack of humoral immunity seen in an essential part of this study’s subjects does not signify a lack of measles protection, as an anamnestic response might be developed after viral exposure, and cellular immunity might still be present and efficient, as reported for agammaglobulinemia patients who can cure measles [22]. Indeed, during the current measles epidemic in Romania, only 10.6% of all cases have been reported in adults, of which 33.9% had an unknown vaccination status, and only 2.9% and 2.8%, respectively, were vaccinated with one and two doses. Nevertheless, the lack of protective antibodies in young, active individuals of both genders increases the risk of viral spread in the community, workplaces, nurseries, kindergartens, and schools. Frequent migration in and outside the country can amplify the transmission chains and explain the repeated measles outbreaks in Romania, fueled by the low vaccine coverage rates. Immunity gaps have been reported in other European countries [33,34,35,36], but at lower levels than the ones found in Romania, and measles outbreaks have been infrequent and with a limited number of cases. In addition, the absence of measles antibodies in women of fertile age means that there is no passive transplacental antibodies transfer during future pregnancies, leaving the newborn completely unprotected against measles during the first year of life before reaching the recommended vaccination age. The low rate of measles seropositivity found in the general population of fertile age is confirmed in the tested pregnant women and is further reflected by the high measles incidence in newborns aged 6 months or younger during the currently ongoing epidemic in Romania. As such, we suggest that the prenatal analysis package in Romania should also include testing for measles antibodies. This will allow vaccination of the seronegative women before conception or, in the case of already pregnant women, vaccination after delivery to ensure adequate protection for future pregnancies. Vaccination of seronegative future mothers will ensure a high level of antibodies during pregnancy and increase protection in newborns [37,38] who are at risk for severe measles complications [39]. As both vaccination-acquired maternal antibodies and passively transmitted antibody titers decline rapidly, an early vaccination of very young infants born from seronegative mothers might also be recommended during measles outbreaks [40,41]. A meta-analysis of the vaccine efficacy showed that vaccination before 9 months yields lower antibody titers compared to the regular administration at 9 or 12 months but that additional vaccine doses ensure a high seropositivity and cellular immunity, supporting early vaccination during outbreaks [23]. It is also tempting to speculate that once aware of the risk posed to the newborn by the absence of maternal antibodies; a mother will also acknowledge the need for all recommended childhood vaccinations, increasing vaccine acceptance and improving the national vaccine coverage rate. The materno-fetal passive transferred humoral immunity can also influence the dynamics of pathogen transmission in the community and the epidemic patterns, as suggested in a mathematical model [42].
5. Conclusions
The results of this nationwide measles seroprevalence study reveal that an important proportion of individuals of fertile age in Romania are seronegative for measles antibodies, a fact further confirmed in a pilot study in pregnant women. Given the virus’s circulation in the community and the low vaccination coverage rate in the general population, this implies an increased risk of measles for newborns. To close these immunization gaps in the community, active immunization of seronegative women before or after pregnancy and early vaccination of susceptible infants must be deployed.
Author Contributions
Conceptualization, SR and AS; methodology, AS, ML, FLF, CS, AP, SR; data acquisition and analysis: AS, ML, II, CS, validation, SR, FLF, CC and AP.; formal analysis, AS, SR.; resources, SR; writing—original draft preparation, AS, SR.; writing—review and editing SR, CC, AP supervision, CC, SR.; funding acquisition SR, AP. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
All data presented are available upon request from first author (AS).
Acknowledgments
The publication of this paper was supported by Carol Davila University of Medicine and Pharmacy through the program “Publish not Perish”.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Guerra FM, Bolotin S, Lim G, Heffernan J, Deeks SL, Li Y, Crowcroft NS. The basic reproduction number (R0) of measles: a systematic review. Lancet Infect Dis. 2017 Dec;17(12):e420-e428. Epub 2017 Jul 27. PMID: 28757186. [CrossRef]
- Plans-Rubió, P. Are the Objectives Proposed by the WHO for Routine Measles Vaccination Coverage and Population Measles Immunity Sufficient to Achieve Measles Elimination from Europe? Vaccines 2020, 8, 218. [CrossRef]
- Immunization Agenda 2030: A Global Strategy to Leave No One Behind https://www.who.int/teams/immunization-vaccines-and-biologicals/strategies/ia2030, accessed July 5, 2024.
- European Immunization Agenda 2030. Copenhagen:WHO Regional Office for Europe; 2021. Licence: CC BY-NC-SA 3.0 IGO. ISBN: 978-92-890-5605-2.
- Calderón et al., The Influence of Antivaccination Movements on the Re-emergence of Measles, J Pure Appl Microbiol, 2019, 13(1), 127-132, 5302. [CrossRef]
- European Centre for Diseases Control, Measles on the rise in the EU/EEA: considerations for public health response, 16 February 2024 https://www.ecdc.europa.eu/sites/default/files/documents/measles-eu-threat-assessment-brief-february-2024.pdf, accessed June 27, 2024.
- Muscat M, Ben Mamou M, Reynen-de Kat C, Jankovic D, Hagan J, Singh S, Datta SS. Progress and Challenges in Measles and Rubella Elimination in the WHO European Region. Vaccines (Basel). 2024 Jun 20;12(6):696. PMID: 38932424; PMCID: PMC11209032. [CrossRef]
- European Centre for Diseases Control, Weekly Communicable Disease Threats Report, Week 41, 5 - 11 October 2024 https://www.ecdc.europa.eu/sites/default/files/documents/communicable-disease-threats-report-week-41-2024.pdf accessed October 15, 2024.
- Hayman DTS. Measles vaccination in an increasingly immunized and developed world. Hum Vaccin Immunother. 2019;15(1):28-33. Epub 2018 Sep 19. PMID: 30156949; PMCID: PMC6363159. [CrossRef]
- Manual for the Laboratory-based Surveillance of Measles, Rubella, and Congenital Rubella Syndrome. Laboratory testing for determination of population immune status https://www.who.int/publications/m/item/chapter-9-manual-for-the-laboratory-based-surveillance-of-measles-rubella-and-congenital-rubella-syndrome, accessed December 20, 2024.
- Kafatos G, Andrews N, McConway KJ, Anastassopoulou C, Barbara C, De Ory F, Johansen K, Mossong J, Prosenc K, Vranckx R, Nardone A, Pebody R, Farrington P. Estimating seroprevalence of vaccine-preventable infections: is it worth standardizing the serological outcomes to adjust for different assays and laboratories? Epidemiol Infect. 2015 Aug;143(11):2269-78. Epub 2014 Nov 25. PMID: 25420586; PMCID: PMC9151055. [CrossRef]
- Andrews N, Tischer A, Siedler A, Pebody RG, Barbara C, Cotter S, Duks A, Gacheva N, Bohumir K, Johansen K, Mossong J, Ory Fd, Prosenc K, Sláciková M, Theeten H, Zarvou M, Pistol A, Bartha K, Cohen D, Backhouse J, Griskevicius A. Towards elimination: measles susceptibility in Australia and 17 European countries. Bull World Health Organ. 2008 Mar;86(3):197-204. PMID: 18368206; PMCID: PMC2647410. [CrossRef]
- National Center for Disease Control. Evolution analysis of communicable diseases under surveillance, Annual reports: https://insp.gov.ro/centrul-national-de-supraveghere-si-control-al-bolilor-transmisibile-cnscbt/rapoarte-anuale/ Romanian, accessed November 12, 2024.
- Donadel M, Stanescu A, Pistol A, Stewart B, Butu C, Jankovic D, Paunescu B, Zimmerman L. Risk factors for measles deaths among children during a Nationwide measles outbreak - Romania, 2016-2018. BMC Infect Dis. 2021 Mar 19;21(1):279. PMID: 33740895; PMCID: PMC7976682. [CrossRef]
- National Institute of Public Health. National Centre for Communicable Diseases Surveillance and Control, Monthly reports. Romanian. Available from: https://insp.gov.ro/informari-lunare/, accessed November 12, 2024.
- Stanescu A, Ruta SM, Cernescu C, Pistol A. Suboptimal MMR Vaccination Coverages-A Constant Challenge for Measles Elimination in Romania. Vaccines (Basel). 2024 Jan 22;12(1):107. PMID: 38276679; PMCID: PMC10819452. [CrossRef]
- Eurostat, the statistical office of the European Union, reference metadata, Fertility. https://ec.europa.eu/eurostat/cache/metadata/en/demo_fer_esms.htm, accessed June 10, 2024.
- Steven K. Thompson, Sampling. Third Edition, 2012. Wiley Series in Probability and Statistics ISBN: 978-0-470-40231-3).
- National Institute of Statistics. Romanian. http://statistici.insse.ro:8077/tempo-online/#/pages/tables/insse-table, accessed June 10, 2024.
- Wiedermann, U., Garner-Spitzer, E. & Wagner, A. Primary vaccine failure to routine vaccines: why and what to do? Hum. Vaccin. Immunother. 12, 239–243 (2016). [CrossRef]
- Pambudi N.A., Sarifudin A., Gandidi I.M., Romadhon R. Vaccine cold chain management and cold storage technology to address the challenges of vaccination programs Energy Rep., 8 (2022), pp. 955-972. [CrossRef]
- Griffin DE, The Immune Response in Measles: Virus Control, Clearance and Protective Immunity, Viruses 2016, 8(10), 282. [CrossRef]
- Nic Lochlainn LM, de Gier B, van der Maas N, Strebel PM, Goodman T, van Binnendijk RS, de Melker HE, Hahné SJM. Immunogenicity, effectiveness, and safety of measles vaccination in infants younger than 9 months: a systematic review and meta-analysis. Lancet Infect Dis. 2019 Nov;19(11):1235-1245. Epub 2019 Sep 20. PMID: 31548079; PMCID: PMC6838664. [CrossRef]
- Gonçalves G, Frade J, Nunes C, Mesquita JR, Nascimento MS. Persistence of measles antibodies, following changes in the recommended age for the second dose of MMR-vaccine in Portugal. Vaccine. 2015 Sep 22;33(39):5057-63. [CrossRef]
- Kang HJ, Han YW, Kim SJ, Kim YJ, Kim AR, Kim JA, Jung HD, Eom HE, Park O, Kim SS. An increasing, potentially measles-susceptible population over time after vaccination in Korea. Vaccine. 2017 Jul 24;35(33):4126-4132. Epub 2017 Jun 29. PMID: 28669617. [CrossRef]
- Ghafoori F, Mokhtari-Azad T, Foroushani AR, Farahmand M, Shadab A, Salimi V. Assessing seropositivity of MMR antibodies in individuals aged 2-22: evaluating routine vaccination effectiveness after the 2003 mass campaign-a study from Iran’s National Measles Laboratory. BMC Infect Dis. 2024 Jul 12;24(1):696. PMID: 38997625; PMCID: PMC11245767. [CrossRef]
- Williamson KM, Faddy H, Nicholson S, Stambos V, Hoad V, Butler M, Housen T, Merritt T, Durrheim DN. A Cross-Sectional Study of Measles-Specific Antibody Levels in Australian Blood Donors-Implications for Measles Post-Elimination Countries. Vaccines (Basel). 2024 Jul 22;12(7):818. PMID: 39066455; PMCID: PMC11281562. [CrossRef]
- Franconeri L, Antona D, Cauchemez S, Lévy-Bruhl D, Paireau J. Two-dose measles vaccine effectiveness remains high over time: A French observational study, 2017-2019. Vaccine. 2023 Sep 7;41(39):5797-5804. Epub 2023 Aug 14. PMID: 37586955. [CrossRef]
- Plotkin S. A. et. al., Plotkin’s vaccines, 7th Edition, Elsevier, 2018.
- Robert A, Suffel AM, Kucharski AJ. Long-term waning of vaccine-induced immunity to measles in England: a mathematical modelling study. Lancet Public Health. 2024 Oct;9(10):e766-e775. Epub 2024 Sep 26. PMID: 39342948. [CrossRef]
- Bitzegeio J, Majowicz S, Matysiak-Klose D, Sagebiel D, Werber D. Estimating age-specific vaccine effectiveness using data from a large measles outbreak in Berlin, Germany, 2014/15: evidence for waning immunity. Euro Surveill. 2019 Apr;24(17):1800529. PMID: 31039834; PMCID: PMC6628761. [CrossRef]
- Klein, S.L.; Flanagan, K.L. Sex differences in immune responses. Nat. Rev. Immunol. 2016, 16. [CrossRef]
- Nasika A, Bogogiannidou Z, Mouchtouri VA, Dadouli K, Kyritsi MA, Vontas A, Voulgaridi I, Tsinaris Z, Kola K, Matziri A, Lianos AG, Kalala F, Petinaki E, Speletas M, Hadjichristodoulou C. Measles Immunity Status of Greek Population after the Outbreak in 2017-2018: Results from a Seroprevalence National Survey. Vaccines (Basel). 2023;11(7):1220. [CrossRef]
- Marchi S, Remarque EJ, Viviani S, Rizzo C, Monteverde Spencer GT, Coluccio R, Montomoli E, Trombetta CM. Measles immunity over two decades in two large Italian Regions: How far is the elimination goal? Vaccine. 2021 Sep 24;39(40):5928-5933. Epub 2021 Aug 26. PMID: 34456073. [CrossRef]
- Grassi T, Bagordo F, Rota MC, Dettori M, Baldovin T, Napolitano F, Panico A, Massaro E, Marchi S, Furfaro G, Immordino P, Savio M, Gabutti G; Sero-epidemiological Study Group. Seroprevalence of measles antibodies in the Italian general population in 2019-2020. Vaccine. 2024 Sep 17;42(22):126012. [CrossRef]
- Bugdaycı Yalcın BN, Sasmaz CT. Measles Seroprevalence and Related Factors in Women Aged 15-49 Years Old, in Mersin, Turkey. Iran J Public Health. 2023 Mar;52(3):593-602. PMID: 37124900; PMCID: PMC10135515. [CrossRef]
- Gieles NC, Mutsaerts EAML, Kwatra G, Bont L, Cutland CL, Jones S, Moultrie A, Madhi SA, Nunes MC. Measles seroprevalence in pregnant women in Soweto, South Africa: a nested cohort study. Clin Microbiol Infect. 2020 Apr;26(4):515.e1-515.e4. Epub 2019 Nov 13. PMID: 31730905. [CrossRef]
- Janaszek,W.;Slusarczyk, J. Immunity against measles in populations of women and infants in Poland. [CrossRef]
- Ben-Chetrit E, Oster Y, Jarjou’i A, Megged O, Lachish T, Cohen MJ, Stein-Zamir C, Ivgi H, Rivkin M, Milgrom Y, Averbuch D, Korem M, Wolf DG, Wiener-Well Y. Measles-related hospitalizations and associated complications in Jerusalem, 2018-2019. Clin Microbiol Infect. 2020 May;26(5):637-642. [CrossRef]
- Principi N, Esposito S. Early vaccination: a provisional measure to prevent measles in infants. Lancet Infect Dis. 2019;19(11):1157-1158. [CrossRef]
- Mathew JL, Wagner AL, Ratho RK, Patel PN, Suri V, Bharti B, Carlson BF, Dutta S, Singh MP, Boulton ML. Maternally transmitted anti-measles antibodies, and susceptibility to disease among infants in Chandigarh, India: A prospective birth cohort study. PLoS One. 2023 Oct 3;18(10):0287110. [CrossRef]
- Moghadas, S. M.; Alexander, M. E.; Sahai, B.M. Waning herd immunity: A challenge for eradication of measles, Journal of Mathematics, Vol.38, Nr. 5, 2008.
Figure 1.
Mean reactivity of measles antibody by age groups.
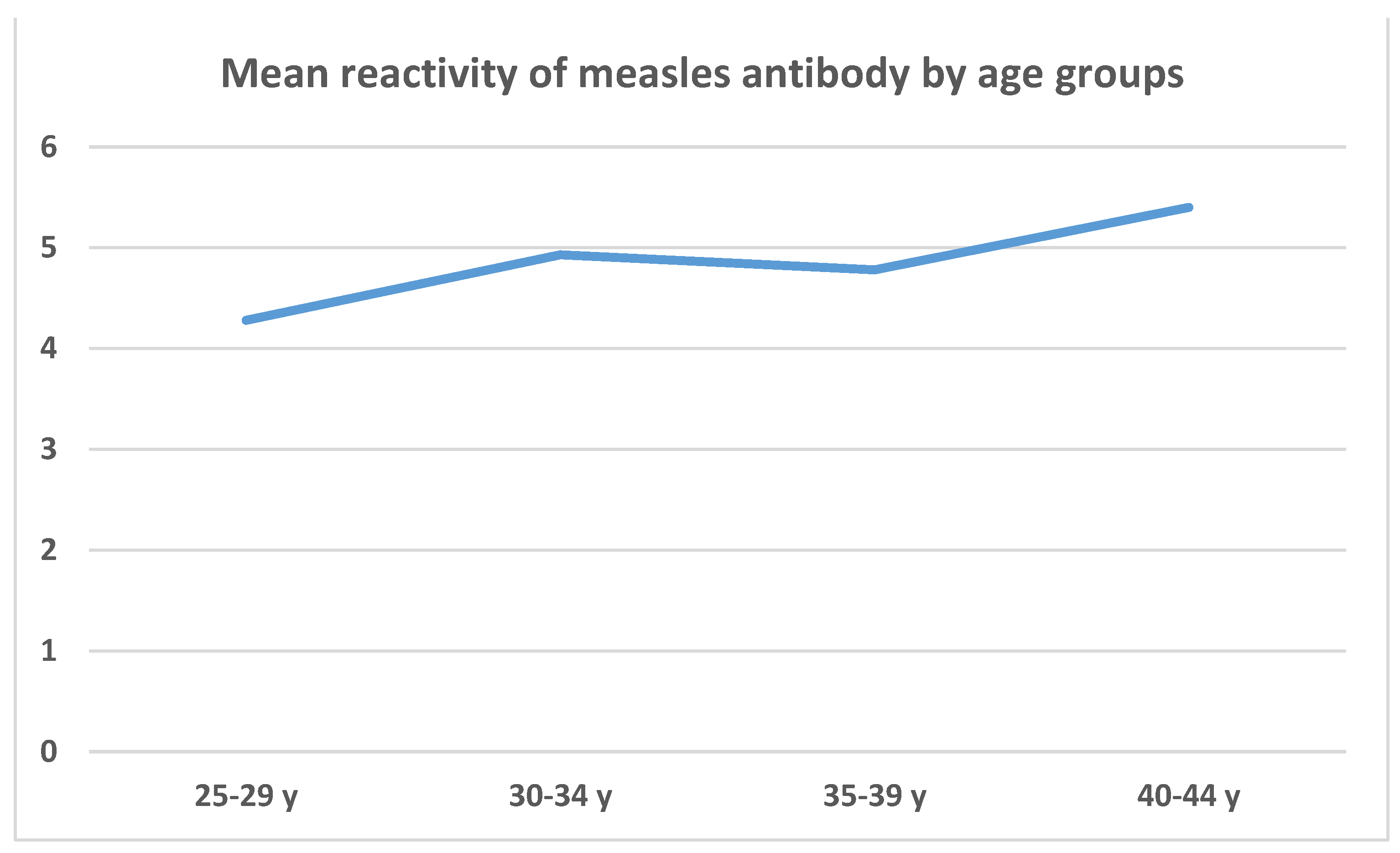
Figure 2.
Seropositivity rate and mean reactivity of measles antibodies in pregnant women.
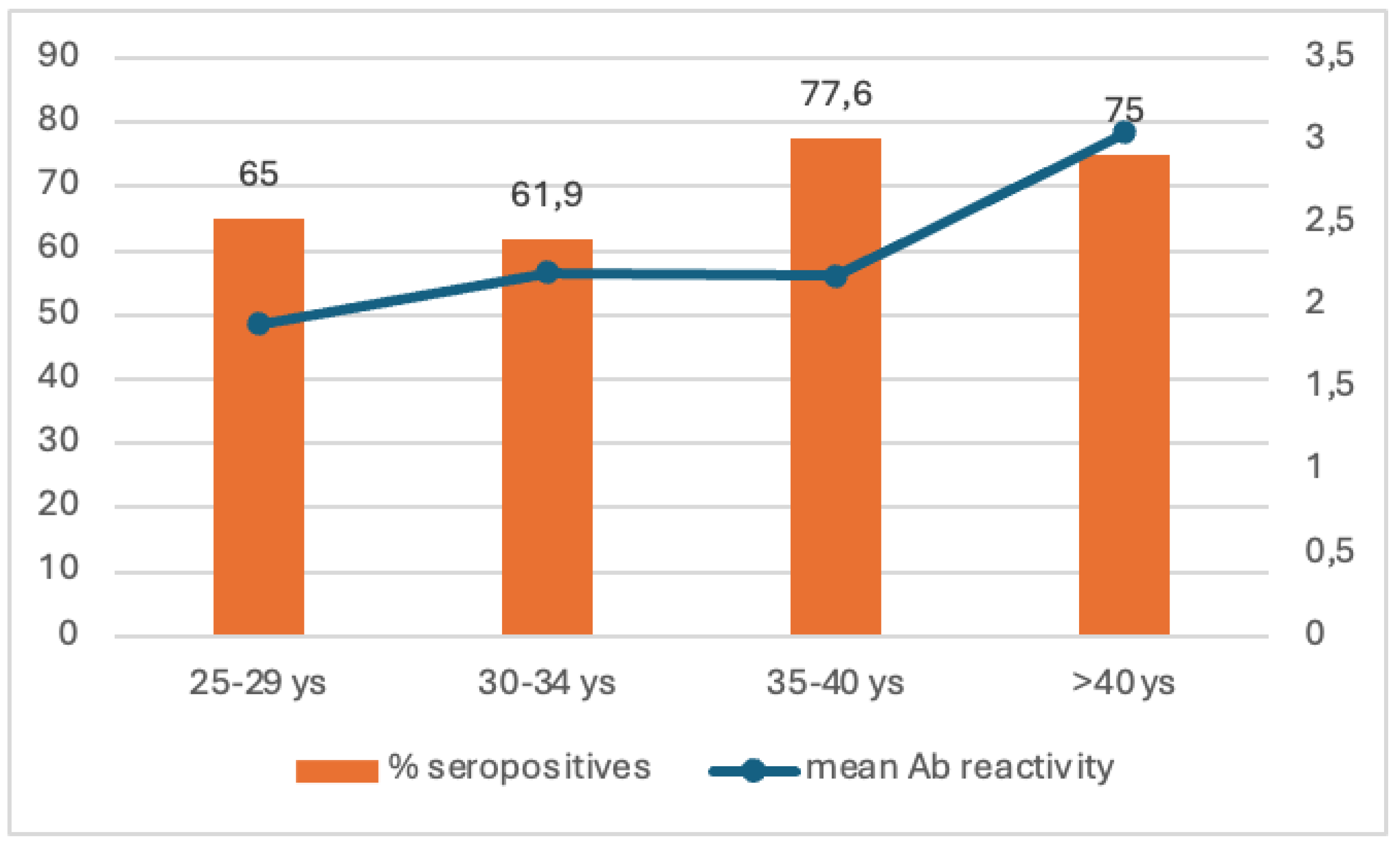

Table 1.
Age group and gender distribution of people selected in the study.
| Age group | Females N=446 |
Males N=513 |
Total number N=959 |
|---|---|---|---|
| 25-29 years | 90 | 103 | 193 |
| 30-34 years | 112 | 129 | 241 |
| 35-40 years | 112 | 131 | 243 |
| 40-44 years | 132 | 150 | 282 |
Table 2.
Comparative analysis of seroprevalence of IgG anti-measles antibodies values by age groups and gender.
Table 2.
Comparative analysis of seroprevalence of IgG anti-measles antibodies values by age groups and gender.
| Seroprevalence of IgG anti measles antibodies | ||||
|---|---|---|---|---|
| Total N=959 |
Females N=446 |
Males N=513 |
||
| Age group | N(%) of positives |
N(%) of positives |
N(%) of positives |
p |
| 25-29 y | 128 (66.3%) | 55 (61.1%) | 73 (70.9%) | 0.153 |
| 30-34 y | 176 (73%) | 88 (78.6%) | 88 (68.2%) | 0.708 |
| 35-39 y | 199 (81,9%) | 90 (80.4%) | 109 (83.2%) | 0.565 |
| 40-44 y | 235 (83.3%) | 112 (84.8%) | 123 (82%) | 0.521 |
|
Total positives |
738 (77%) |
345 (77.4%) | 393 (76.6%) | 0.796 |
Table 3.
Comparative analysis of measles seroprevalence values by regions and age groups.
| Region | Age group | |||||||
| 25-29 y | 30-34 y | 35-39 y | 40-44 y | |||||
| National | 66.3% | p | 73.0% | p | 81.9% | p | 83.3% | p |
| North West vs | 51.5% | 0.101 | 64.3% | 0.331 | 78.9% | 0.657 | 94.6% | 0.073 |
| Center vs | 76.9% | 0.413 | 84.2% | 0.285 | 85.7% | 0.718 | 80.0% | 0.703 |
| South vs | 66.7% | 0.967 | 84.8% | 0.09 | 81.0% | 0.889 | 82.4% | 0.874 |
| South East vs | 56.5% | 0.35 | 61.3% | 0.173 | 75.0% | 0.376 | 81.1% | 0.737 |
| South West vs | 69.0% | 0.773 | 63.0% | 0.169 | 79.6% | 0.705 | 87.5% | 0.433 |
| West vs | 84.6% | 0.05 | 82.8% | 0.255 | 84.8% | 0.682 | 75.0% | 0.242 |
| Bucharest-Ilfov vs | 73.3% | 0.579 | 71.4% | 0.75 | 95.5% | 0.958 | 83.3% | 0.355 |
| North East vs | 63.0% | 0.734 | 76.2% | 0.874 | 82.4% | 0.103 | 76.0% | 1 |
Table 4.
Comparative analysis of the measles reactivity rates between the age groups.
| Age group compared | Age group to be compared with | Mean measles reactivity differences between age groups | p |
|---|---|---|---|
| 25-29 y | 30-34 y | -0.656 | 0.870 (-2.293; 0.979) |
| 35-39 y | -0.505 | 0.772 (-1.591; 0.580) | |
| 40-44 y | -1.127 | 0.057 (-2.275; 0.020) | |
| 30-34 y | 35-39 y | 0.151 | 1.000 (-1.386; 1.689) |
| 40-44 y | -0.470 | 0.966 (-2.052; 1.112) | |
| 35-39 y | 40-44 y | -0.621 | 0.471 (-1.621; 0.377) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



