
Submitted:
15 June 2023
Posted:
15 June 2023
You are already at the latest version
Abstract
Accurate data on susceptibility rates against measles in general population of Greece are scarce. Many studies estimate the vaccination coverage but none has calculated the nationwide immunity rate, involving all age groups, against measles virus. The purpose of our study was to determine the immunity status to measles, especially after the latest outbreak in 2017-2018. In total, 3,972 leftover blood samples were collected from a nationwide laboratory network using a geograph-ically stratified sampling strategy and were tested for the presence of measles specific IgG anti-bodies. The overall crude seroprevalence was calculated 89.6% and the adjusted 89.8% (95% CI: 88.8% - 90.8%). There was no statistically significant difference in seropositivity among sexes (p=0.783). Higher immunity rates and antibody titer were found in older age groups ≥ 41 years old (94.9%, 95% CI: 93.7% - 95.9%, and 730.0 IU/l) in comparison to younger individuals 1-40 years old (83.4%, 95% CI: 81.6% - 85.7%, and 616.5 IU/l). ). Comparing the seroprevalence among Nomenclature of Territorial Units for Statistics (NUTS 2), a statistically significant difference was estimated among them (<0.001). The two regions where higher measles incidence was observed during the 2017-2018 outbreak, Eastern Macedonia and Thrace and Western Greece, were among the four regions with the lower seropositivity (84.6%, 95% CI: 79.9% -89.4% and 85.9%, 95% CI: 81.4% - 90.4%, respectively). Our study showed a measles immunity gap that affects younger age groups and makes a new measles outbreak likely. Enforcement of vaccination campaigns and ad-dressing vaccine hesitancy could bridge it and achieve the required target for herd immunity.
Keywords:
measles
; seroprevalence
; immunity
; anti-measles IgG antibodies
; Greece
1. Introduction
The adoption of childhood vaccinations during the second half of the 20th century has been one of the most successful and cost-effective public health policies [1,2]. The wide implementation of vaccination programs leading to the control of several infectious diseases, as in the case of measles [3]. Measles is a highly contagious, serious disease caused by a virus belonging in the paramyxovirus family and it is normally passed through direct contact and through the air [4]. It is documented that major epidemics occurred approximately every 2–3 years and measles caused an estimated 2.6 million deaths each year before the introduction of measles vaccine and widespread vaccination [4].
In 1961 the vaccine was hailed as 100% effective and the first measles vaccine was licensed for public use in 1963 [5]. An improved version of the measles vaccine was created in 1968 - a “weaker” version, passed the virus through chick embryo cells 40 times to weaken it - and in 1971, followed by a combined developed vaccine against measles, mumps and rubella, known as MMR vaccine [5]. In 2018, about 86% of the world's children received one dose of measles vaccine by their first birthday through routine health services – up from 72% in 2000 – and during 2000 - 2018, measles vaccination prevented an estimated 23.2 million deaths [4].
Because measles has such a high infectivity rate, the threshold for community protection is also very high, requiring at least 95% immunity among the population to prevent epidemics [6]. Despite of the availability of the safe and cost-effective vaccine, an observed failure to maintain very high rates of immunization – result of many causes - brings measles outbreaks [7]. In 2018, 353,236 measles cases reported to World Health Organization (WHO) and there were more than 140,000 measles deaths globally, mostly among children under the age of five [4]. Global measles deaths continued to climb prior to the COVID-19 pandemic. In 2019, the highest number of reported cases in the last 23 years was recorded, 873,022 cases, and there were over 207,000 measles deaths globally [5].
In Greece, around 1975 the measles vaccine started being given to boys and girls aged 1 year, while it was introduced in the National Immunization Programme as mandatory in 1981 [8,9]. Throughout the last two decades, the incidence of measles in Greece has presented a constant decline. However, sporadic clusters or even outbreaks are still recorded. The three last post-honeymoon outbreaks in Greece occurred in 2005-2006, 2010–2011, and the most extensive in 2017-2018 [10,11,12]. During the last epidemic in 2017-2018, 3,259 cases were reported through the mandatory notification system in effect for measles, and 2,104 (64.5%) of them were under the age of 14 years, including 833 children (25.5%) aged 1-4 years old [9,12,13]. The majority of cases concerned largely under-vaccinated groups of Roma population (almost 60%), young adults aged 25-44 years old, and health workers with no or incomplete history of vaccination [14]. The highest incidence was observed in the region of Western Greece and Eastern Macedonia – Thrace [9].
The European Centre for Disease Prevention and Control (ECDC) classifies Greece in countries with >95% vaccination coverage with one dose of a measles-containing vaccine while vaccination coverage with second dose is estimated ≤89% [15,16,17]. A significant heterogeneity in vaccination coverage is observed between different population samples. A recent study conducted in 2020-2021 estimated that MMR coverage among undergraduate Health Science students is about 96.1%, while a national survey conducted in 2017 found very low vaccination coverage on Roma children based on vaccination document; 47.9% of them were vaccinated with one MMR dose and only 7.6% with two doses [18,19].
A number of studies have been conducted in order to estimate the measles vaccine coverage, but only a few measured antibodies in serum samples in specific populations and not at national level [18,19,20,21,22]. The aim of our study was to calculate the Greek population’s immunity levels by measuring specific IgG anti-measles antibodies in serum samples representative of all Greek regions and age groups and assess whether seropositivity levels were associated with the incidence of measles in different regions.
2. Materials and Methods
2.1. Study Design and Participants
Blood samples were collected by using the leftover sampling methodology (residual sera from the general population) after the epidemic of 2017-2018 in Greece [23]. We applied a geographically stratified sampling strategy based on regional units (Nomenclature of Territorial Units for Statistics (NUTS) level 3) to produce a representative sample, taking into consideration age (1–24, 25-54, 55-64,65-79 ≥ 80 years) and sex distribution. The required sample size was determined to be 246 blood samples from each of the 13 NUTS level 2 regions, using a margin of error of ±5%, a confidence level of 95%, an 80% expected frequency and 10,718,565 people (estimated population of Greece-1/1/2020). The sample size that was calculated using Epi info. However, the number of actual samples collected differed from the pre-determined number of samples above.
The leftover blood samples were collected from a nationwide laboratory network, including both public hospital and private laboratories. The samples were derived from individuals who visited the laboratories for a screening routine, check-up, chronic disease follow-up or other medical reasons. The geographical distribution of the collected leftover samples is shown in the Figure 1. Age, sex, residence and the date of blood sampling were recorded for each sample.
2.2. Laboratory Analysis
Samples were collected and stored at −80 °C at the Laboratory of Hygiene and Epidemiology, Medical School in Larissa, Greece. The presence of anti-Measles IgG antibodies was evaluated using a commercially available kit (SERION ELISA classic Masern/Measles Virus Ig) for enzyme linked immunosorbent assay (ELISA) according to the manufacturer’s recommendations. Absorbance was read at 405 nm and IgG antibody concentration was calculated using a standard curve. According to the manufacturer’s instructions titres were interpreted as negative (<150 IU/l), border-line (equivocal) (150-200 IU/l) and positive (>200IU/l).
2.3. Statistical Analysis
Initially, we determined an unweighted relative frequency of all positive participants characteristics (age, sex and area of residence): this is the crude seroprevalence. The weighted proportions of positive tests in the countrywide sample were based on the sex and age distribution of the Greek population, according to the 2020 estimated population [24]. The 95% confidence interval (CI) for weighted data were estimated using Clopper-Pearson exact binomial interval. The titer of antibodies was described using mean and standard deviation (StD). The 95% CI for the mean was estimated using normal distribution. Chi-square (χ2), Mann-Whitney U test and Kruskal Wallis test were used to assess differences in seropositivity and titer of antibodies as appropriate. To compare the relative incidence of measles between Regions, we used binary logistic regression models. These models were adjusted for age and sex. We calculated the adjusted seroprevalence of the four regions with the lowest seropositivity and we used it as the reference group. For all analyses, a 5% significance level was set. All statistical analyses were performed using Statistical Package for the Social Sciences software version 29.0 (SPSS Inc., Chicago, IL, USA).
2.4. Ethical Statement
The current study was approved by the Ethics Committee of the Faculty of Medicine, University of Thessaly (No. 186). A written consent form was signed by all of the participants and the serum samples were anonymized and encrypted during the study.
3. Results
In total 3,972 samples were collected and analysed from all regions in Greece. Data on sex, age and place of residence were available for 94.4%, 97.4% and 97.9% of total sample respectively. Figure 1 displays the geographic distribution of collected leftover samples. A total of 1,330 samples were collected from the Attica region, followed by 648 from Central Macedonia, 256 from Thessaly, 234 from Western Greece, 229 from Peloponnese, 227 from Central Greece, 225 from Eastern Macedonia and Thrace, 288 from Crete, 105 from Epirus, 100 from South Aegean, 97 from Western Macedonia, 72 from North Aegean, and 76 from the Ionian Islands.
According to Table 1, the crude seroprevalence for the population is 89.6% and the adjusted seroprevalence is 89.8 (95%, CI 88.8% - 90.8%). There is no statistically significant difference in seroprevalence between both sexes (p=0.783), between large urban areas and the rest of the country (p=0.991) or between the islands and the mainland (p=0.523). However, there is a difference in seroprevalence between different age groups (p<0.001). The proportion of positive samples increased with age, as we observed the highest adjusted seroprevalence in age groups 55-64 (95.6%, 95% CI: 93.7-97.4%), 65-79 (94.9%, 95% CI: 93%-96.7%) and 80+ (95.4%, 95% CI:92.3%-98.6%). Additionally, we found adjusted seroprevalence to be significantly higher for individuals over 41 years old (94,9%, 95%CI: 93.7% - 95.9%) compared to those aged under 40 (83.4%. 95% CI: 81.6% - 85.7%) (p<0.001).
Regarding antibody titers, we also found a significant difference between sexes (p=0.003). There is a statistically significant difference in the medians of antibody titer between the age groups (p<0.001) with the lowest titer of 632.1 IU/l being observed in individuals aged 25-54 and the highest titer of 749.6 IU/l in 65-79. The median titers demonstrated no difference when we compared large urban areas to the rest of the country and the islands to the mainland.
Additionally, when comparing the study’s found seronegativity with the targets set for each age group by WHO [25], children aged 1-4 (21.1%), 10-14 (6.6%) and individuals 15-40 years old (11.8%) did not meet them (Figure 2).
In Figure 3, we can see that the highest proportion of seronegative samples is observed in age group 1-4 (21.1%) and the lowest in individuals >41 years old (3.9%).The highest antibody titers, however, were found in age group 1-4 years old (738.5 IU/l) and the lowest in age group 15-40 years old (605.1 IU/l). The last age group also demonstrated the highest proportion of border samples (3.2%). Finally, seropositivity peaked in age group >41 years old (95%) but was lowest in children aged 1-4 (78.9%).
According to Table 2 and Figure 4, when analyzing the presence of measles antibodies in different Regions of Greece (NUTS 2), Eastern Macedonia and Thrace (84.6%, 95% CI 79.9%-89.4%) and Western Macedonia (85.2%, 95% CI: 78.1%-92.3%) had the lowest seroprevalence. The lowest antibody titers were recorded in Eastern Macedonia and Thrace 610.7 IU/l and Western Greece 636.9 IU/l. On the contrary, the highest seroprevalence was observed in the North Aegean Regions (95.7%, 95% CI: 91.0% - 100%), and Peloponnese (95.6%, 95% CI: 92.6% - 98.7%). However, the highest antibody titers were found in South Aegean (730.9 IU/l) and in Central Macedonia (705.1 IU/l).
According to Table 2, the four Regions with the lowest seropositivity were Western Macedonia, Eastern Macedonia and Thrace, Western Greece and Ionian Islands and the seropositivity of these Regions was 85.4% (95% CI 82.6%-88.2%). Figure 5 depicts the pairwise comparisons of seropositivity between these four to the remaining Regions. Peloponnese, Central Macedonia, North and South Aegean had statistically significantly higher seropositivity than the four Regions with the lowest seroprevalence while in Thessaly, Crete, Epirus, Central Greece, and Attica, a higher seropositivity was calculated but without statistically signifigant difference.
4. Discussion
The aim of our study was to estimate the seroprevalence of measles in the general population in Greece. We found that almost 90% of individuals had serologic proof of immunity against measles virus in our study population, which reflects that about 10% were susceptible to measles. Considering that at least 95% vaccination coverage with two doses of measles-containing vaccine is the widely accepted target for controlling the spread of measles virus adopted by WHO, there is an immunity gap against measles in the Greek population [6,26]. This specific target rate is important in order to protect infants, who are vulnerable to complications of measles and too young to receive the first dose of vaccine [27]. This observed deviation from herd immunity allows the circulation and spread of the virus and makes the appearance of clusters or even outbreaks among susceptible individuals possible.
A typical example that picturizes the danger posed by low immunity level is the measles epidemic which took place in 2017-2018 as part of an outbreak in Europe [28]. In Greece, it began in May 2017 and continued until the end of 2018, with the majority of cases occurring in 2018. A total of 968 measles cases were confirmed in 2017, and 2,291 in 2018. The outbreak affected multiple regions in Greece, with the highest incidence reported in Western Greece and Eastern Macedonia and Thrace [9,13]. The seroprevalence in these regions was estimated in our study among the lowest in the country. This could be one explanation among others that answers the question why the epidemic affected more these specific regions and, on the other hand, indicates that despite the virus circulation, herd immunity could be hardly achieved through natural infection. It should be noted that two more regions were identified with similar levels of low seropositivity. Observing that the last 20 years a post-honeymoon measles outbreak occurs every 5-7 years in Greece, we should be vigilant, especially in the areas with the low seroprevalence, as in 2023-2024 may be a year of reintroduction and spread of measles virus.
The last outbreak mainly occurred among susceptible population, such as Roma (60.5%), children younger than 14 years old - even infants are included – and young adults 25-44 years old, unvaccinated or incompletely vaccinated healthcare workers, and people of foreign origin (10%). In 2017, a study performed on 251 Roma children calculated that only 42.9-47.9% of them had been vaccinated with at least one dose of MMR, 18.8-21% had it by the age of 24 months old, while only 6.8-7.6% were recorded as vaccinated with two doses [19]. This study indicates that Roma is an under vaccinated and vulnerable population and explains the high proportion of cases in this community.
The finding of a large number of seronegative people was reinforced in another study carried out before the epidemic in 2017-2018 [21]. They collected and tested 611 serum samples during June 2014-January 2016 from Northern Greece, while the age of participants ranged from 10 days to 82 years old. Seroprevalence was found to be 82.07%. However, newborns and infants not eligible for vaccination were included and this could explain the low level of seroprevalence that was found. If excluding the 0-15 months babies as the majority of them are under vaccination age threshold according to our national vaccination schedule, a seropositivity almost 87.4% is calculated, further approaching our results. Either way, these levels of seropositivity are below those required for herd immunity and could explain the measles epidemic that followed. In our study, we excluded the children under 1 year old.
But even after the outbreak, the population immunity did not reach the desired level for measles elimination. A serosurvey calculating measles antibodies among multi-transfused patients with hemoglobinopathies conducted in Greece, following the last measles outbreak, showed that 89.3% of patients were found positive [22]. However, the group of frequently transfused patients does not appropriately represent the general population.
In another serosurvey performed in 2018-2019 on Greek soldiers aged from 18.3 to 29.9 years old, the immunity rate against measles was calculated 80%, much lower than our result. It is also worth mentioning that, via their vaccination certifications, 94.3% of the participants were fully vaccinated against measles and almost half of them in a timely manner [20]. The significant difference found between recorded immunization and observed seropositivity could bear clinical and epidemiological consequences and therefore, highlights the importance for serosurveys. Based only on vaccination certification, it is possible to underestimate the risk of measles outbreaks.
According to a vaccination coverage study published in 2017, 97.3% of Greek preschool children aged 2–3 years were immunized with one dose of MMR [17]. However, a second dose is recommended for all children, which is essential to immunize the approximately 15% of them who do not develop protective immunity after their first dose [5]. A vaccination coverage >95% was also found via Child Vaccination Booklet in another published study conducted in the academic year 2020–2021 on health science undergraduate students, aged 18–30 years old [18]. However, studies based on vaccination certifications of specific social groups may overestimate the immunity levels and gives the false impression of an ideal seroepidemiological status. As already mentioned before, the ECDC ranks Greece among countries with vaccination coverage against measles of ≤89% in the general population [15].
We have to consider that the collection of our serum samples was conducted during a period preceding or overlapping the first years of COVID-19 pandemic. An immunity gap had already been documented. There is an undeniable risk that the gap has now widened further as it is commonly accepted that access to health facilities and hence vaccination - especially for minorities - was neglected during the pandemic. According to WHO, in 2021, a record high of nearly 40 million children missed a measles vaccine dose: 25 million children missed their first dose and an additional 14.7 million children missed their second dose [29]. The suboptimal vaccination coverage, in conjunction with the lifting of public health measures, magnifies the threat of a measles outbreak with a higher number of cases, subsequent complications, and even deaths.
In our study individuals younger than 40 years did not meet the WHO threshold to ensure herd immunity. This finding raises questions about the effectiveness of vaccination policy and enforcement considering they were born after 1981, the year when vaccination against the virus became mandatory. This may be due to a variety factors such as: 1) unequal access to health facilities for minorities, 2) vaccine hesitancy especially after the publication of the non-evidenced, incorrect causal association between MMR vaccine and autism spectrum disorders, 3) primary vaccination failure - due to failures in vaccine attenuation, vaccination regimens, or administration - and 4) secondary vaccination failure - waning vaccine-induced immunity meaning a decrease of circulating IgG antibodies some years after vaccination [30,31]. An inverse relationship has been documented; as the years pass since the second dose of measles vaccination, the proportion of vaccinated persons who converse to seronegative increases [32]. We should not forget that mothers may be included in young adults’ group. Lower levels of maternal antibodies may pose a major problem for infants and lead to a gap of protection until the children can get vaccinated.
Another equally important reason for low seropositivity among younger age groups could be the delay on the administration of the second dose [32]. As mentioned earlier in a survey conducted in the Greek Air Force, even though the overwhelming majority of the recruits were fully vaccinated, the half of them received the second dose of vaccine late [20]. The untimely vaccination is also documented by another study performed in Greece’s second largest city; a 21% delay rate for the MMR vaccine was recorded [33]. This delay may have a negative impact on induced immunity. An inverse correlation between antibody titers and the time elapsed between the two vaccinations has been proven [34]. The proportion of individuals with equivocal or negative titres was higher the longer the time period since last vaccination had been [34].
Opposed to younger age groups, adults over 40 years have reached the desired threshold set by WHO. This finding could be explained taking into consideration that these individuals had been naturally immunized against the virus mainly during childhood. A significant number of serosurveys performed in Europe have arrived to similar conclusions and it is supported that naturally acquired immunity can be preserved for longer time period [32,35,36,37]. Besides longer-term humoral immunity, a higher antibody titer is observed in the same age group, a result compatible with natural infection [35].
In our study, we also calculated samples with borderline antibody titer. It is documented that individuals whose titers are classified as equivocal often have sufficient anti-measles antibodies with neutralizing capacity [32]. Even in this optimistic scenario, the proportion of people with immunity is estimated at around 92%, below the target rate for disease elimination.
We found no statistically significant difference in seroprevalence against measles between females and males and to our knowledge, sex differences regarding immunization coverage have not been suggested with the exception of one study which showed significantly higher vaccination coverage in females [18].
Among seropositive individuals, as it was said before, a significant difference was observed between younger than 40 years old and older individuals. This finding could also possibly demonstrates the most effective immunity through natural infection [35]. Comparing the level of antibodies titer among the two sexes, males seems to present higher titer but it is not statistically significant and it comes in contrast with the general acceptance that females typically develop higher immune responses to viral infections and vaccine [38]. However, comparing the titer among sexes per age group, males present statistically significantly higher titer in younger age group “25-54”, finding supported also by other study [39]. In any case, both sexes show high antibody titres in all age groups, making them immune to measles.
Our study presents some limitations. The leftover sampling methodology could be considered one of them, as non-random convenient sampling may affect the representativeness of samples collected. Furthermore, we did not have the exact information about age, sex or place of residence for a small number of samples. Thus, these samples were excluded during statistical adjustment. Finally, there was no possibility of distinguishing between vaccination-induced immunity and natural infection during laboratory analysis and there was no access to vaccination records.
However, our study is superior on many other points. To our knowledge, this is the first national seroprevalence study on measles involving the general population; all age groups and both sexes. The majority of studies estimate the immunity level for measles in Greece based on vaccination booklets. However, vaccination coverage studies may not accurately reflect immunity on the grounds that they do not account for primary and secondary vaccination failure or the case of natural infection. Few serosurveys have been carried out in Greece and there are focused only on specific groups; such as air force recruits or patients with hemoglobinopathies [20,22]. There is only one serosurvey estimating measles immunity in every age group but is limited to northern Greece and was conducted on 2017, during the measles outbreak without reflecting the possible impact of the outbreak on the immunity of the population [21].
5. Conclusions
Measles is a vaccine-preventable disease targeted for elimination in most WHO regions. Greece is considered by the European Regional Verification Commission for Measles and Rubella to have eliminated endemic transmission of measles in 2020 [40]. Unfortunately, the seroprevalence we found is lower than the one required for herd immunity. As the virus has not been eliminated worldwide, the threat of its reintroduction and subsequent outbreak is imminent. With a view to increase the immunity level, vaccination campaigns must be urgently launched, aiming to raise awareness about the benefits of vaccines and address the issues of vaccine hesitancy and misinformation. Enforcement of immunization activities among minorities with poor access to health services, such as Roma populations and asylum seekers, and better surveillance strategies should be also encouraged [40].
Author Contributions
Conceptualization, V.A.M, M.S. and C.H.; methodology, C.H.; validation, A.N.; formal analysis, K.D.; resources, M.A.K., A.V., I.V., Z.T., A.G.L., K.K., A.M., O.F., O.K. and F.K.; data curation, A.N.; writing—original draft preparation, A.N. and Z.B.; writing—review and editing, A.N., Z.B. and C.H.; visualization, K.D.; supervision, V.A.M, E.P., M.S. and C.H.; project administration, A.N. and C.H. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki and was approved by the by the ethical committee of the Faculty of Medicine,University of Thessaly, Greece (No. 168, 15.11.2021).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data are not publicly available as they contain sensitive information at individual level.
Acknowledgments
The authors highly appreciate the continuous support for this project offered by the laboratories that participated in the study.
Conflicts of Interest
The authors declare no conflict of interest.
References
- van Panhuis, W.G.; Grefenstette, J.; Jung, S.Y.; Chok, N.S.; Cross, A.; Eng, H.; Lee, B.Y.; Zadorozhny, V.; Brown, S.; Cummings, D.; et al. Contagious Diseases in the United States from 1888 to the Present. New England Journal of Medicine 2013, 369, 2152–2158. [Google Scholar] [CrossRef] [PubMed]
- Zhou, F.; Shefer, A.; Wenger, J.; Messonnier, M.; Wang, L.Y.; Lopez, A.; Moore, M.; Murphy, T. V.; Cortese, M.; Rodewald, L. Economic Evaluation of the Routine Childhood Immunization Program in the United States, 2009. Pediatrics 2014, 133, 577–585. [Google Scholar] [CrossRef] [PubMed]
- Benefits from Immunization During the Vaccines for Children Program Era — United States, 1994–2013. Available online: https://www.cdc.gov/mmwr/preview/mmwrhtml/mm6316a4.htm (accessed on 12 April 2023).
- Measles. Available online: https://www.who.int/news-room/fact-sheets/detail/measles?gclid=CjwKCAiA9NGfBhBvEiwAq5vSy0LoZb6eUZCrIeVfmg9FcNW4VdNHQ59bwBZj0A0edN3FVE1Nbgfu4xoCFIUQAvD_BwE (accessed on 12 April 2023).
- History of Measles Vaccination. Available online: https://www.who.int/news-room/spotlight/history-of-vaccination/history-of-measles-vaccination?topicsurvey=ht7j2q)&gclid=Cj0KCQiAutyfBhCMARIsAMgcRJRuqLNP-QtuKj1VVPoeHCzxgEtm-NsexSb7H-bJSaOWKg9qUQV3EDUaAnF3EALw_wcB (accessed on 12 April 2023).
- Moss, W.J.; Shendale, S.; Lindstrand, A.; O’Brien, K.L.; Turner, N.; Goodman, T.; Kretsinger, K. Feasibility Assessment of Measles and Rubella Eradication. Vaccine 2021, 39, 3544–3559. [Google Scholar] [CrossRef] [PubMed]
- Wilder-Smith, A.B.; Qureshi, K. Resurgence of Measles in Europe: A Systematic Review on Parental Attitudes and Beliefs of Measles Vaccine. J Epidemiol Glob Health 2020, 10, 46. [Google Scholar] [CrossRef] [PubMed]
- Panagiotopoulos, T.; Antoniadou, I.; Valassi-Adam, E.; Berger, A. Increase in Congenital Rubella Occurrence after Immunisation in Greece: Retrospective Survey and Systematic Review. BMJ : British Medical Journal 1999, 319, 1462. [Google Scholar] [CrossRef] [PubMed]
- Σημεία, Σ. Τμήμα Επιδημιολογικής Επιτήρησης Και Παρέμβασης ΕΠΙΔHΜΙOΛOΓΙΚA ΔΕΔOΜΕΝA ΓΙA ΤHΝ ΙΛAΡA ΣΤHΝ ΕΛΛAΔA 2018 (ΣΥΣΤHΜA ΥΠOΧΡΕΩΤΙΚHΣ ΔHΛΩΣHΣ ΝOΣHΜAΤΩΝ).
- Ιλαρά - Εθνικός Oργανισμός Δημόσιας Υγείας. Available online: https://eody.gov.gr/disease/ilara/ (accessed on 12 April 2023).
- Gianniki, M.; Siahanidou, T.; Botsa, E.; Michos, A. Measles Epidemic in Pediatric Population in Greece during 2017–2018: Epidemiological, Clinical Characteristics and Outcomes. PLoS One 2021, 16. [Google Scholar] [CrossRef] [PubMed]
- Measles Reported Cases and Incidence. Available online: https://immunizationdata.who.int/pages/incidence/measles.html?CODE=GRC&YEAR= (accessed on 12 April 2023).
- Σμιμα Επιδθμιολογικισ Επιτιρθςθσ Και Παρζμβαςθσ ΕΠΙΔHΜΙOΛOΓΙΚA ΔΕΔOΜΕΝA ΓΙA ΣHΝ ΙΛAΡA ΣHΝ ΕΛΛAΔA.
- Τμήμα Επιδημιολογικής Επιτήρησης Και Παρέμβασης ΕΠΙΔHΜΙOΛOΓΙΚA ΔΕΔOΜΕΝA ΓΙA ΤHΝ ΙΛAΡA ΣΤHΝ ΕΛΛAΔA.
- Vaccination Coverage for Second Dose of a Measles-Containing Vaccine, EU/EEA, 2018. Available online: https://www.ecdc.europa.eu/en/publications-data/vaccination-coverage-second-dose-measles-containing-vaccine-eueea-2018 (accessed on 12 April 2023).
- Vaccination Coverage for the First Doses of Measles and Rubella Containing Vaccine by Country, EU/EEA, 2018. Available online: https://www.ecdc.europa.eu/en/publications-data/vaccination-coverage-first-doses-measles-and-rubella-containing-vaccine-country-0 (accessed on 12 April 2023).
- Georgakopoulou, T.; Menegas, D.; Katsioulis, A.; Theodoridou, M.; Kremastinou, J.; Hadjichristodoulou, C. A Cross-Sectional Vaccination Coverage Study in Preschool Children Attending Nurseries-Kindergartens: Implications on Economic Crisis Effect. Hum Vaccin Immunother 2017, 13, 190–197. [Google Scholar] [CrossRef] [PubMed]
- Andrie, E.K.; Sakellari, E.; Barbouni, A.; Tsitsika, A.K.; Lagiou, A. Vaccination Coverage during Childhood and Adolescence among Undergraduate Health Science Students in Greece. Children 2022, Vol. 9, Page 1553 2022, 9, 1553. [Google Scholar] [CrossRef] [PubMed]
- Papamichail, D.; Petraki, I.; Arkoudis, C.; Terzidis, A.; Smyrnakis, E.; Benos, A.; Panagiotopoulos, T. Low Vaccination Coverage of Greek Roma Children amid Economic Crisis: National Survey Using Stratified Cluster Sampling. The European Journal of Public Health 2017, 27, 318. [Google Scholar] [CrossRef] [PubMed]
- Maltezou, H.C.; Karantoni, H.; Petrikkos, P.; Georgota, P.; Katerelos, P.; Liona, A.; Tsagarakis, S.; Theodoridou, M.; Hatzigeorgiou, D. Vaccination Coverage and Immunity Levels against Vaccine-Preventable Diseases in Male Air Force Recruits in Greece. Vaccine 2020, 38, 1181–1185. [Google Scholar] [CrossRef] [PubMed]
- Gioula, G.; Exindari, M.; Melidou, A.; Minti, F.; Sidiropoulou, E.; Dionisopoulou, S.; Kiriazi, M.; Tsintarakis, E.; Malisiovas, N. Seroprevalence of measles in Northern Greece Acta Microbiologica Hellenica 2017 62(3):145-150. 1.
- Manganas, C.; Sophia, K.; Myria, D.; Aikaterini, P.; Maria, X. Journal of Prevention and Infection Control Seroprevalence for Measles Antibodies among Multi-Transfused Patients with Hemoglobinopathies: The Experience of a Thalassemia and Sickle Cell Department in Seroprevalence for Measles Antibodies among Multi-Transfused Pa-Tients with Hemoglobinopathies: The Experience of a Thalassemia and Sickle Cell Department in Greece. 2022,. [CrossRef]
- Nardone, A.; Miller, E. Serological Surveillance of Rubella in Europe: European Sero-Epidemiology Network (ESEN2). Euro Surveill 2004, 9, 5–7. [Google Scholar] [CrossRef] [PubMed]
- Statistics - ELSTAT. Available online: https://www.statistics.gr/en/statistics/-/publication/SPO18/- (accessed on 13 April 2023).
- Copenhagen The Expanded Programme on Immunization in the European Region of WHO Measles A Strategic Framework for the Elimination of Measles in the European Region.
- Ask the Experts: Measles, Mumps, and Rubella (MMR) Vaccines. Available online: https://www.immunize.org/askexperts/experts_mmr.asp (accessed on 13 April 2023).
- Measles in the EU/EEA: Current Outbreaks, Latest Data and Trends – January 2018. Available online: https://www.ecdc.europa.eu/en/news-events/measles-eueea-current-outbreaks-latest-data-and-trends-january-2018 (accessed on 13 April 2023).
- Georgakopoulou, T.; Horefti, E.; Vernardaki, A.; Pogka, V.; Gkolfinopoulou, K.; Triantafyllou, E.; Tsiodras, S.; Theodoridou, M.; Mentis, A.; Panagiotopoulos, T. Ongoing Measles Outbreak in Greece Related to the Recent European-Wide Epidemic. Epidemiol Infect 2018, 146, 1692–1698. [Google Scholar] [CrossRef]
- Nearly 40 Million Children Are Dangerously Susceptible to Growing Measles Threat. Available online: https://www.who.int/news/item/23-11-2022-nearly-40-million-children-are-dangerously-susceptible-to-growing-measles-threat (accessed on 13 April 2023).
- MMR Vaccines and Autism. Available online: https://www.who.int/groups/global-advisory-committee-on-vaccine-safety/topics/mmr-vaccines-and-autism (accessed on 13 April 2023).
- Tafuri, S.; Bianchi, F.P.; Stefanizzi, P.; De Nitto, S.; Maria, A.; Larocca, V.; Germinario, C.; Tafuri, S. The Journal of Infectious Diseases Long-Term Immunogenicity of Measles Vaccine: An Italian Retrospective Cohort Study. The Journal of Infectious Diseases ® 2020, 221, 721–729. [Google Scholar] [CrossRef]
- Poethko-Müller, C.; Mankertz, A. Sero-Epidemiology of Measles-Specific IgG Antibodies and Predictive Factors for Low or Missing Titres in a German Population-Based Cross-Sectional Study in Children and Adolescents (KiGGS). Vaccine 2011, 29, 7949–7959. [Google Scholar] [CrossRef] [PubMed]
- Tasika, E.; Farmaki, E.; Roilides, E.; Antachopoulos, C. Implementation of the Greek National Immunization Program among Nursery Attendees in the Urban Area of Thessaloniki. Hippokratia 2019, 23, 147. [Google Scholar] [PubMed]
- Anichini, G.; Gandolfo, C.; Fabrizi, S.; Miceli, G.B.; Terrosi, C.; Savellini, G.G.; Prathyumnan, S.; Orsi, D.; Battista, G.; Cusi, M.G. Seroprevalence to Measles Virus after Vaccination or Natural Infection in an Adult Population, in Italy. Vaccines 2020, Vol. 8, Page 66 2020, 8, 66. [Google Scholar] [CrossRef] [PubMed]
- Bianchi, F.P.; Mascipinto, S.; Stefanizzi, P.; De Nitto, S.; Germinario, C.; Tafuri, S. Long-Term Immunogenicity after Measles Vaccine vs. Wild Infection: An Italian Retrospective Cohort Study. https://doi.org/10.1080/21645515.2020.1871296 2021, 17, 2078–2084. [CrossRef]
- Ristić, M.; Milošević, V.; Medić, S.; Malbaša, J.D.; Rajčević, S.; Boban, J.; Petrović, V. Sero-Epidemiological Study in Prediction of the Risk Groups for Measles Outbreaks in Vojvodina, Serbia. PLoS One 2019, 14, e0216219. [Google Scholar] [CrossRef] [PubMed]
- Smetana, J.; Chlibek, R.; Hanovcova, I.; Sosovickova, R.; Smetanova, L.; Gal, P.; Dite, P. Decreasing Seroprevalence of Measles Antibodies after Vaccination – Possible Gap in Measles Protection in Adults in the Czech Republic. PLoS One 2017, 12, 170257. [Google Scholar] [CrossRef] [PubMed]
- Ruggieri, A.; Anticoli, S.; D’ambrosio, A.; Giordani, L.; Viora, M. Monographic Section The Influence of Sex and Gender on Immunity, Infection and Vaccination. Ann Ist Super Sanità 2016, 52, 198–204. [Google Scholar] [CrossRef] [PubMed]
- Mikhail Kostinov, P.; Pavel Zhuravlev, I.; Nikolay Filatov, N.; Aristitsa Kostinova, M.; Valentina Polishchuk, B.; Anna Shmitko, D.; Cyrill Mashilov, V.; Anna Vlasenko, E.; Alexey Ryzhov, A.; Anton Kostinov, M. Gender Differences in the Level of Antibodies to Measles Virus in Adults. Vaccines (Basel) 2021, 9. [Google Scholar] [CrossRef]
- Tenth Meeting of the European Regional Verification Commission for Measles and Rubella Elimination; 2022.
Figure 1.
Geographical distribution of samples collected for serosurvey.

Figure 2.
Seronegativity per age group compared to respective WHO target.
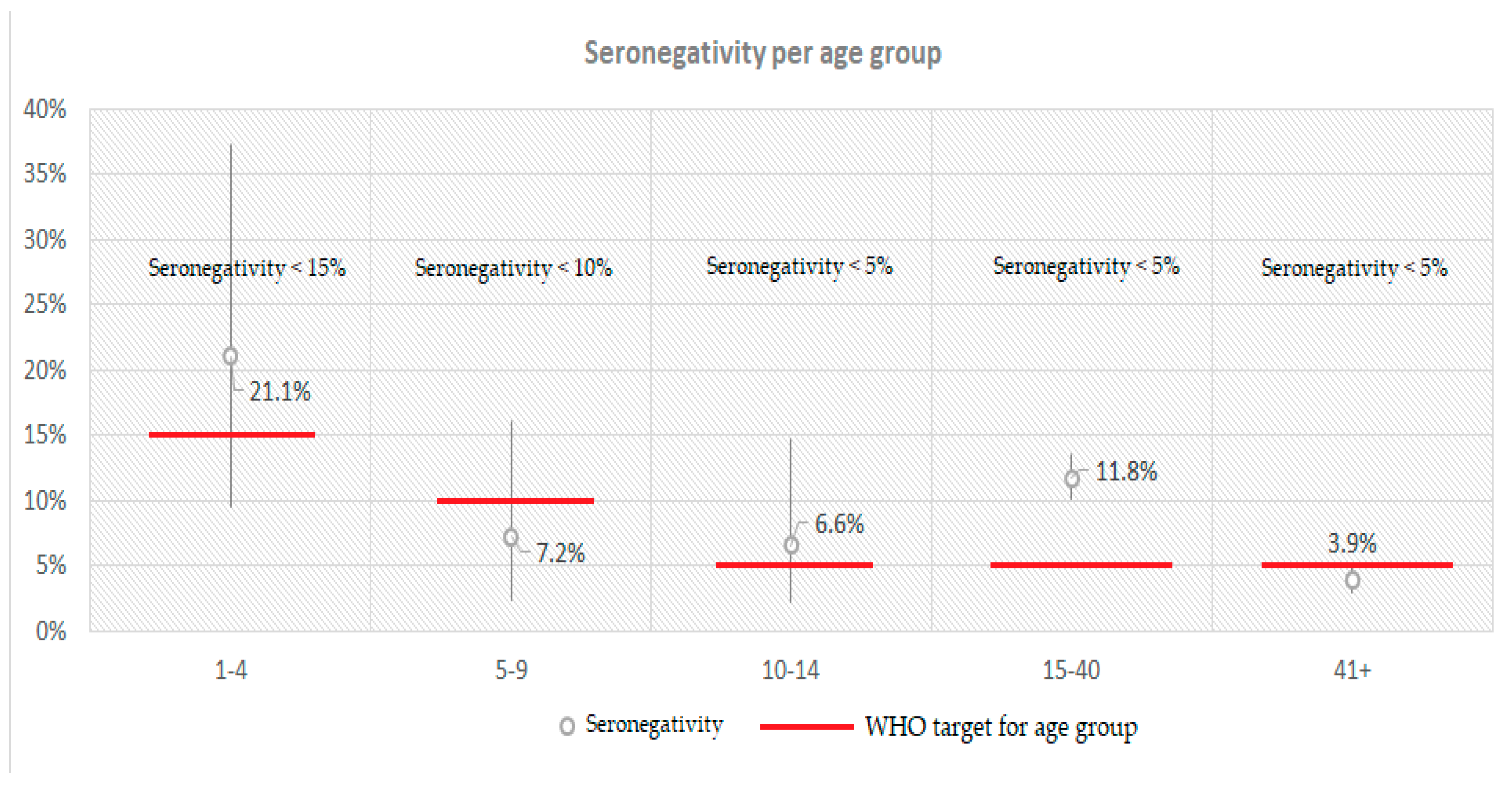
Figure 3.
The percentage (%) of positive, negative and border samples and the course of titer of anti-measles IgG antibodies per age group.
Figure 3.
The percentage (%) of positive, negative and border samples and the course of titer of anti-measles IgG antibodies per age group.
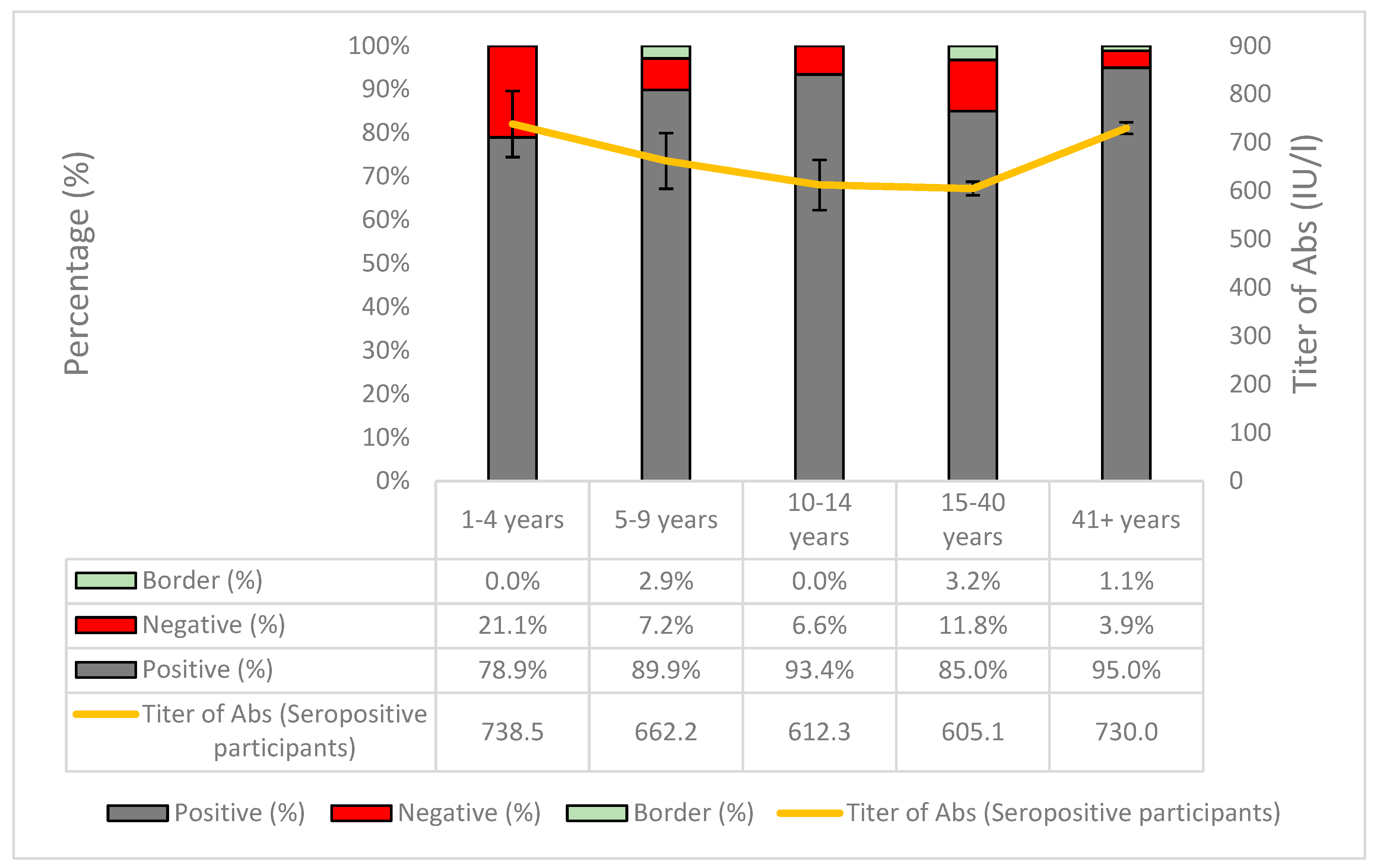
Figure 4.
Adjusted seropositivity per Region (NUTS level 2).
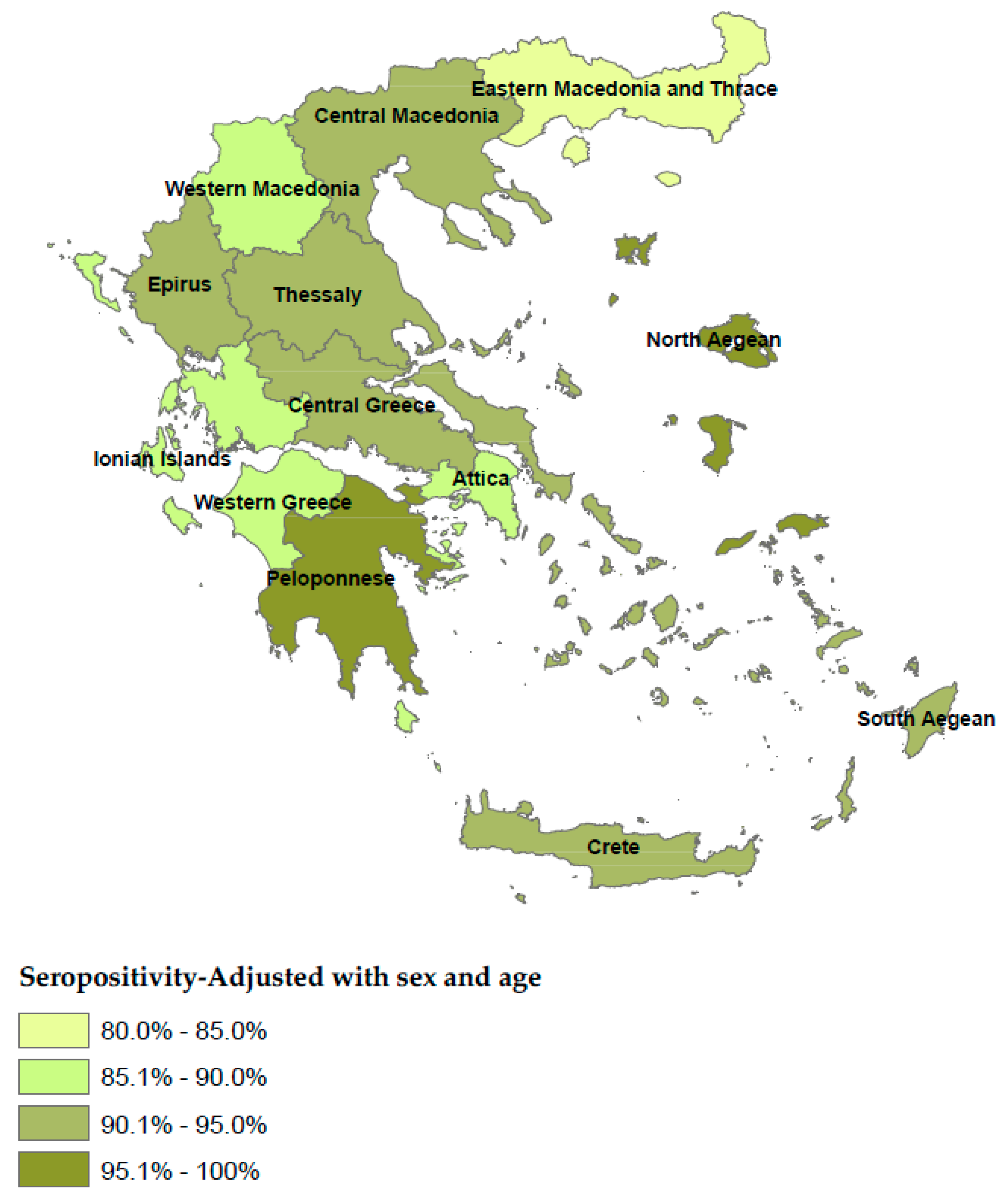
Figure 5.
Pairwise comparisons of seropositivity between the four Regions with the lowest seropositivity and the remaining Regions. * P-values are derived from binary logistic regression models with IgG positive (1/0) as the outcome variable, adjusted for age and sex. Error bars show 95% confidence intervals.
Figure 5.
Pairwise comparisons of seropositivity between the four Regions with the lowest seropositivity and the remaining Regions. * P-values are derived from binary logistic regression models with IgG positive (1/0) as the outcome variable, adjusted for age and sex. Error bars show 95% confidence intervals.
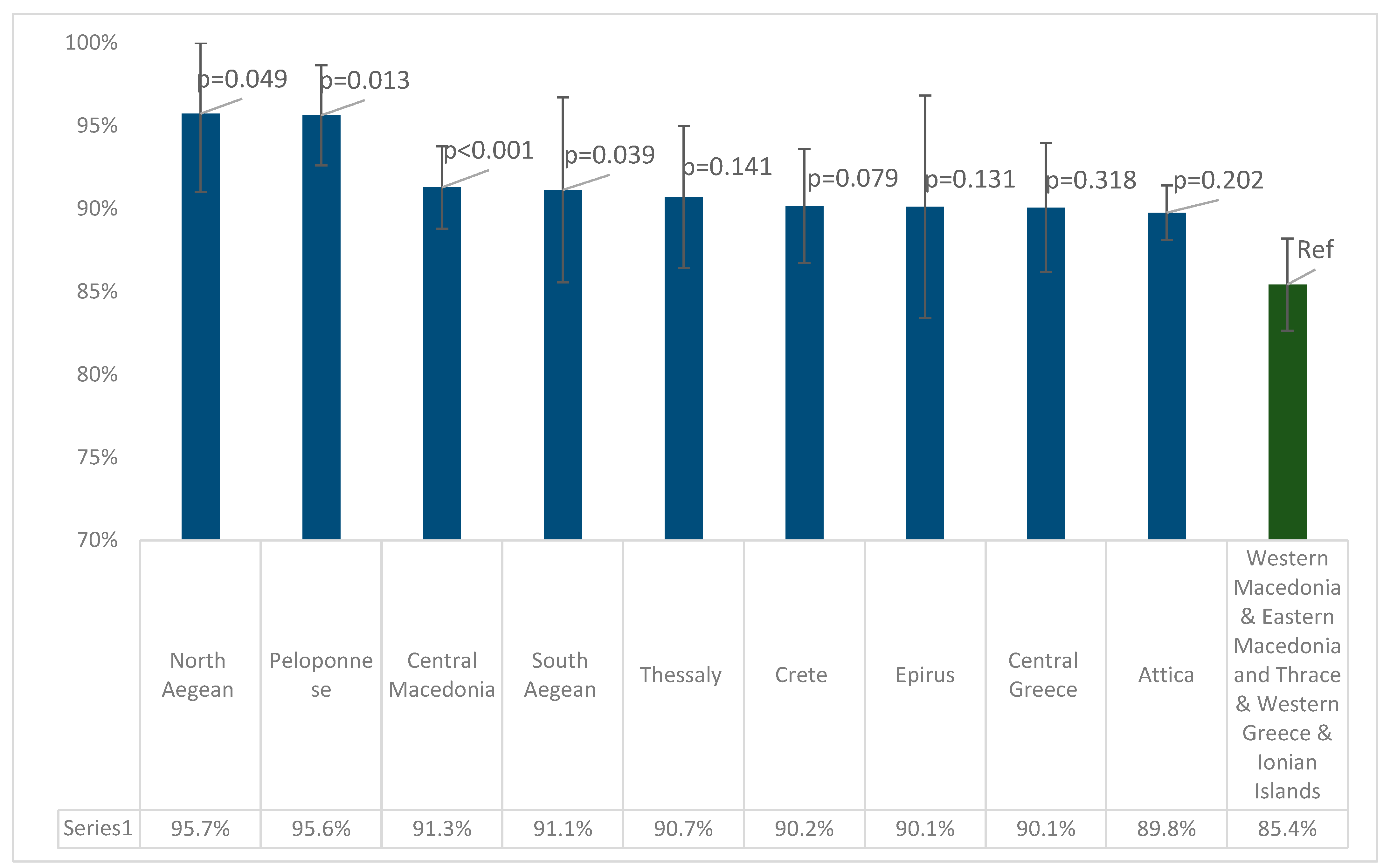

Table 1.
Crude, adjusted seroprevalence and titer of anti-measles antibodies.
| Positive (N) | Negative (N) | Boarder (N) | Total | Crude Seroprevalence | Adjusted Seroprevalence* | 95% CI | Sig.** | Antibody Titer of Seropositive Participants | 95% CI | Sig. | ||||
| Overall | 3558 | 327 | 87 | 3972 | 89.6% | 89.8% | 88.8% | 90.8% | - | 672.9 | 662.7 | 683.1 | - | |
| Sex | Male | 1382 | 132 | 27 | 1541 | 89.7% | 89.2% | 87.6% | 90.8% | 0.783C | 692.9 | 674.0 | 711.8 | 0.003M-W |
| Female | 1974 | 180 | 54 | 2208 | 89.4% | 89.8% | 88.5% | 91.1% | 656.9 | 645.9 | 667.9 | |||
| Age groups | 1-24 | 810 | 110 | 35 | 955 | 84.8% | 84.4% | 81.9% | 86.8% | <0.001C | 640.5 | 609.4 | 671.6 | <0.001K-W |
| 25-54 | 1420 | 160 | 39 | 1619 | 87.7% | 87.6% | 85.9% | 89.3% | 632.1 | 619.0 | 645.3 | |||
| 55-64 | 555 | 25 | 4 | 584 | 95.0% | 95.6% | 93.7% | 97.4% | 744.2 | 723.7 | 764.6 | |||
| 65-79 | 486 | 17 | 6 | 509 | 95.5% | 94.9% | 93.0% | 96.7% | 749.6 | 730.2 | 769.0 | |||
| 80+ | 168 | 6 | 2 | 176 | 95.5% | 95.4% | 92.3% | 98.6% | 722.4 | 687.3 | 757.4 | |||
| Age groups | 1-40 | 1149 | 165 | 54 | 1368 | 84.0% | 83.4% | 81.6% | 85.7% | <0.001C | 616.5 | 593.4 | 639.6 | <0.001M-W |
| ≥41 | 1513 | 62 | 18 | 1593 | 95.0% | 94.9% | 93.7% | 95.9% | 730.0 | 718.0 | 742.1 | |||
| Large urban areas (>500,000) | 1532 | 152 | 27 | 1711 | 89.5% | 90.3% | 84.4% | 94.1% | 0.991C | 681.3 | 663.7 | 698.8 | 0.163-W | |
| Rest of country | 1949 | 170 | 58 | 2177 | 89.5% | 89.0% | 84.4% | 92.1% | 665.6 | 653.4 | 677.8 | |||
| Islands | 487 | 39 | 11 | 537 | 90.7% | 90.7% | 80.5% | 95.4% | 0.523C | 665.2 | 642.7 | 687.7 | 0.899-W | |
| Mainland | 2994 | 283 | 74 | 3351 | 89.3% | 89.2% | 85.3% | 92.4% | 673.7 | 662.2 | 685.2 | |||
* Adjusted seroprevalence was calculated using sera from participants for whom sex and age data were available; ** Comparison between positive and non-positive results. CI: Confidence Interval; C: Chi-Square-test; M-W: Mann-Whitney U test; K-W: Kruskal-Wallis test.
Table 2.
Crude, adjusted seroprevalence and titer of antibodies per Region.
| Region (NUTS Level 2) | Positive (N) | Negative (N) | Boarder (N) | Total | Crude Seroprevalence | Adjusted Seroprevalence | 95% CI | Sig.** | Antibody Titer of Seropositive Participants | 95% CI | Sig. | ||
| Attica | 1188 | 132 | 10 | 1330 | 89.3% | 89.8%* | 88.1% | 91.4% | <0.001C | 672.8 | 651.5 | 694.0 | <0.001K-W |
| Central Greece | 204 | 19 | 4 | 227 | 89.9% | 90.1% | 86.2% | 93.6% | 693.1 | 658.5 | 727.7 | ||
| Thessaly | 231 | 19 | 6 | 256 | 90.2% | 90.7%* | 86.4% | 95.0% | 642.9 | 608.4 | 677.4 | ||
| Western Greece | 200 | 22 | 12 | 234 | 85.5% | 85.9%* | 81.4% | 90.4% | 636.9 | 605.3 | 668.5 | ||
| Epirus | 97 | 4 | 5 | 106 | 91.5% | 90.5%* | 83.9% | 97.0% | 692.5 | 570.0 | 814.9 | ||
| Crete | 261 | 23 | 5 | 289 | 90.3% | 90.2% | 86.7% | 93.6% | 641.5 | 611.4 | 671.6 | ||
| Central Macedonia | 586 | 38 | 24 | 648 | 90.4% | 91.3%* | 88.8% | 93.8% | 705.1 | 685.2 | 725.1 | ||
| Ionian Islands | 64 | 10 | 2 | 76 | 84.2% | 85.8% | 78.0% | 93.6% | 686.1 | 627.3 | 745.0 | ||
| North Aegean | 68 | 3 | 1 | 72 | 94.4% | 95.7%* | 91.0% | 100% | 645.7 | 584.9 | 706.5 | ||
| South Aegean | 94 | 3 | 3 | 100 | 94.0% | 91.1% | 85.6% | 96.7% | 730.9 | 676.9 | 784.8 | ||
| Peloponnese | 220 | 9 | 0 | 229 | 96.1% | 95.6%* | 92.6% | 98.7% | 695.3 | 661.2 | 729.4 | ||
| Western Macedonia | 80 | 14 | 3 | 97 | 82.5% | 85.2% | 78.1% | 92.3% | 652.5 | 602.8 | 702.2 | ||
| Eastern Macedonia and Thrace | 189 | 27 | 10 | 226 | 83.6% | 84.6%* | 79.9% | 89.4% | 610.7 | 576.1 | 645.3 | ||
* Adjusted seroprevalence was calculated using sera from participants for whom sex, age, residence data were available; ** Comparison between positive and non-positive results. CI: Confidence Interval; C: Chi-Square-test; K-W: Kruskal-Wallis test.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



