
Submitted:
01 February 2025
Posted:
20 February 2025
You are already at the latest version
Abstract
Objective of the Study The aim of this study was to improve predictions regarding tumour aggressiveness and treatment outcomes in breast cancer. This condition affects over one million people globally each year, with prognosis depending on clinical and biological factors such as age, tumour size, nodal status, and histological grade. Methods and Results The research was based on published data highlighting abnormal expressions of miRNAs involved in the initiation and development of breast cancer, as well as negative mutations in the BRCA1 and BRCA2 genes. Approximately 15% of breast cancers are of the basal type, often identified as triple-negative breast cancers (TNBC). These types of cancer are characterized by the absence of estrogen and progesterone receptors, as well as HER2, including both basal-like cancers and some poorly differentiated luminal cancers. The BRCA1and BRCA2 genes are considered the most important genes in hereditary predisposition to breast cancer, along with genes such as PTEN and P53. Several studies have emphasized the role of aberrant miRNA expression in the initiation and progression of cancer. Breast cancer treatment varies depending on the stage and molecular characteristics of the disease, including chemotherapy, hormonal therapy, surgical interventions, and/or radiotherapy. An innovative treatment uses a modified miRNA sequence that naturally blocks cell division to target cancer cells specifically. Conclusions Identifying the genetic structure of malignant cells in breast cancer provides valuable scientific insights that can serve as improved predictors of tumour aggressiveness and cancer treatment outcomes.
Keywords:
Inflammatory breast cancer
; triple-negative breast cancers
; P53 gene
; isoform p53 protein
; miRNAs
Introduction
International statistics of breast cancer, (BC), show that persons with BRCA1 and BRCA2 mutations have a significantly higher risk of developing this disease in per cent at 45% to 65%, until by the age of 70 years, [1].
It is recommended that individuals with these mutations have a genetic consult. Other risk factors of BC include obesity, hormone therapy including progestin and estrogen, abuse of alcohol and sedentarism, [2].
The most severe forms of breast cancer occur when the tumour spreads in metastases to other parts of the body. The early diagnosis and new molecular treatments in breast cancer improved the outcomes of patients, [3].
Despite these advancements, tumour recurrence and metastasis remain the leading causes of mortality for many BC patients, posing significant challenges in reducing mortality rates, particularly in terminal cases. To improve disease-free survival rates, investigating biomarkers associated with BC cell metastasis is essential, [4].
The first study analyzing gene expression patterns in breast cancer identified at least four major molecular classes: luminal-like, basal-like, normal-like, and HER2-positive. Factors such as histological type, tumour grade, size, lymph node involvement, estrogen receptor status, and HER2 receptor status significantly influence prognosis and response to systemic therapies, [5].
Basal-like breast cancers account for approximately 15% of breast cancer cases and are often classified as triple-negative breast cancers (TNBCs). These cancers are characterized by the absence of estrogen, progesterone, and HER2 receptors and are frequently associated with younger patients and poor prognoses, [6].
Many studies, last time, showed the roles of different microRNAs (miRNAs) in the development and progression of BC. Additionally, the wild-type p53 protein, reported to be reduced by more than 50% in various cancers, has been identified as a potential genetic target for miRNAs of carcinogenic process, [7].
Methodology
The study was based on published data that demonstrated abnormal miRNA expressions involved in the initiation and development of cancer, as well as negative mutations in the BRCA1 and BRCA2 genes in breast cancer, [8].
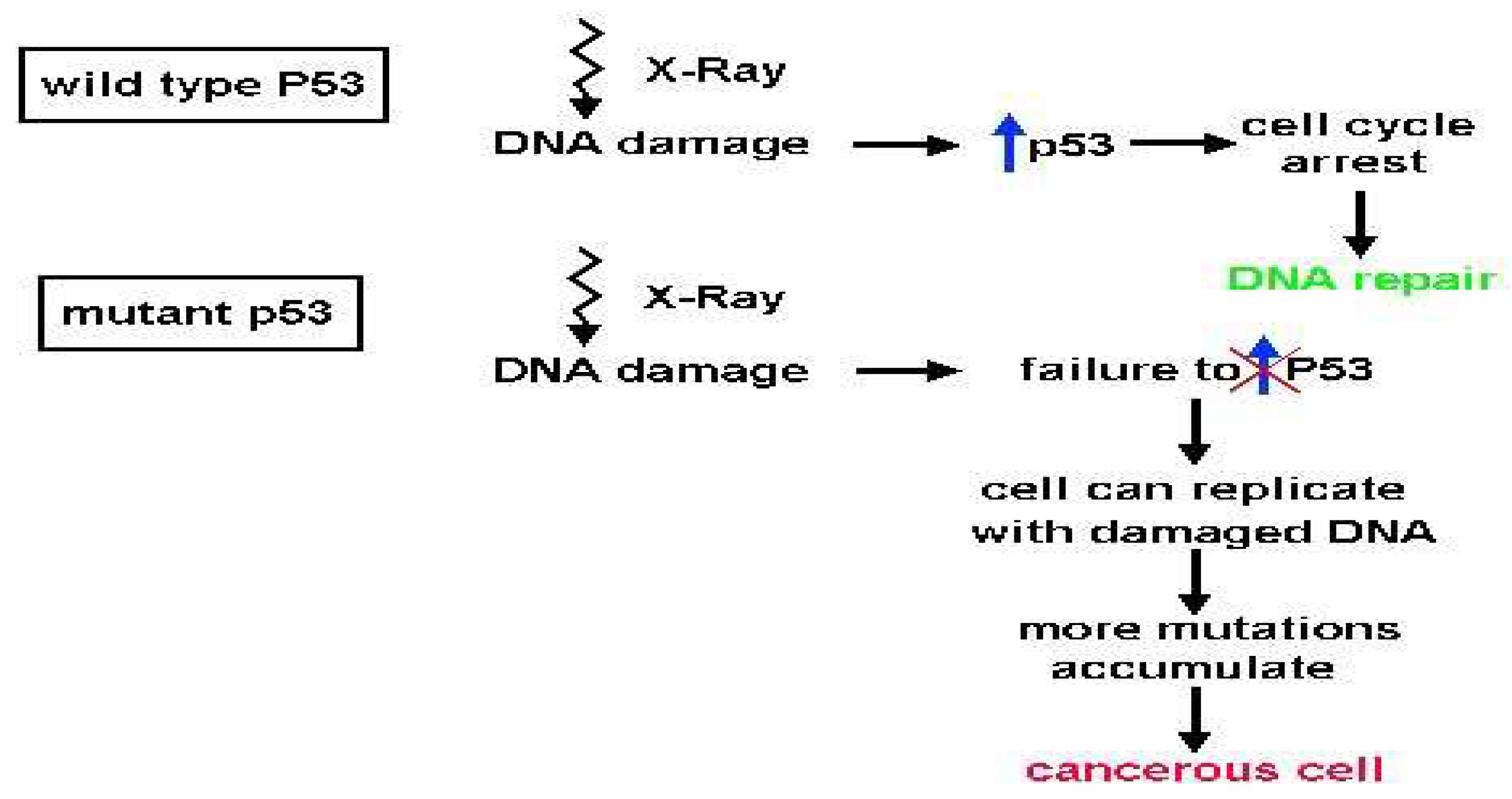
The BRCA1 and BRCA2 genes are considered the most important in terms of hereditary predisposition to breast cancer, besides genes such as the PTEN gene and P53 gene. Predisposition of P53 gene mutation appears in Fraumeni Syndrome and may also be associated with negative mutations in the BRCA1 and BRCA2 genes in BC, [9]. [Scheme 1].
Scheme 1.
Effects of isomorph p53 protein in the carcinogenesis process.
Angiogenesis is an essential factor in tumour growth and metastasis in various malignancies. Increasing evidence demonstrates that angiogenesis is regulated by microRNAs (miRNAs), which are small non-coding RNAs consisting of 19-25 nucleotides.
Results
Over the past 10 years, the roles of miRNAs have been extensively investigated across multiple types of human cancers. Evidence suggests that miRNAs regulate gene expression by targeting various molecules that influence the physiology and development of cancer cells, [10].
Depending on their functions in different tumour types, miRNAs are classified as either oncogenes or tumour suppressors Same expression of miRNAs can contribute to chemoresistance, radioresistance, and endocrine resistance in the treatment of BC, [11].
The P53 gene encodes a protein commonly referred to as the "guardian of the genome," which binds to DNA to regulate transcription, control the cell cycle, and induce apoptosis, among other functions. According to epidemiological studies, the risk of developing cancer in patients with P53 gene polymorphisms is as high as 90%. The product of the P53 gene, the p53 protein, is a phosphoprotein consisting of 393 amino acids and contains four functional domains, one of which activates transcription factors, [Scheme2].
Scheme 2.
P53 protein in active tetrameric form.
Numerous studies have demonstrated that aberrant miRNA expression is involved in the initiation and development of cancer. Additionally, the native p53 protein, which has been reported to be decreased by more than 50% in various cancers, could be used as a target gene of miR-214, [12].
Discussions
Recent studies have shown that miR-124 contributes to development and aggressive malignancy, in tumour spread, epithelial-mesenchymal transition (EMT), metastasis, and cellular resistance at chmiotherapy. Particularly in BC was found that the overexpression of miR-214 significantly enhanced cell invasion by down-regulating p53 expression, [13].
For instance, BC tissues have been shown to exhibit reduced expression of miR-124 compared with normal tissues. Thus, miRNAs are regarded as effective targets for further studies on the design of novel therapeutic strategies, [14].
Also, the type of miR-124 overexpression has been shown to contribute to an increase in the number of cells present in the G0/G1 phase cellular cycle and inhibits STAT3 production.This miR-124 is a key modulator of cholinergic anti-inflammatory effects and can inhibit the expression of TNF-, [15, 16], [Scheme 3].
Scheme 3.
PI3K/Akt triggers a signalling cascade that modulates tumour cell proliferation
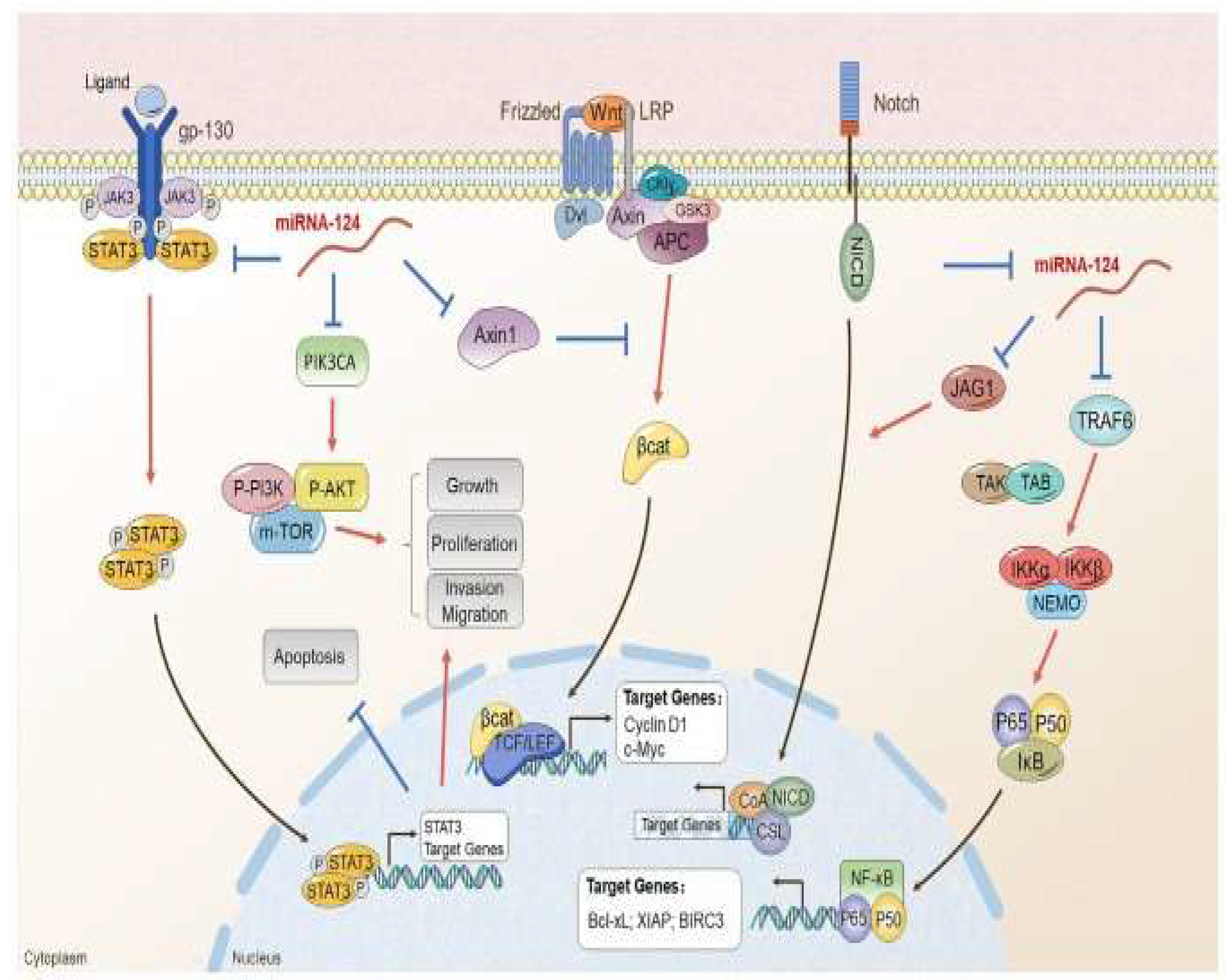
A target for cancer treatment must be the JAK/STAT signalling pathway which stimulates the molecular mutations in different cancer diseases.[18].
Another type of miRNA, miR-124 has been shown to have a beneficial role that can inhibit the migration and proliferation of certain cancer cell types and can be used in therapeutic strategies of BC,[19].
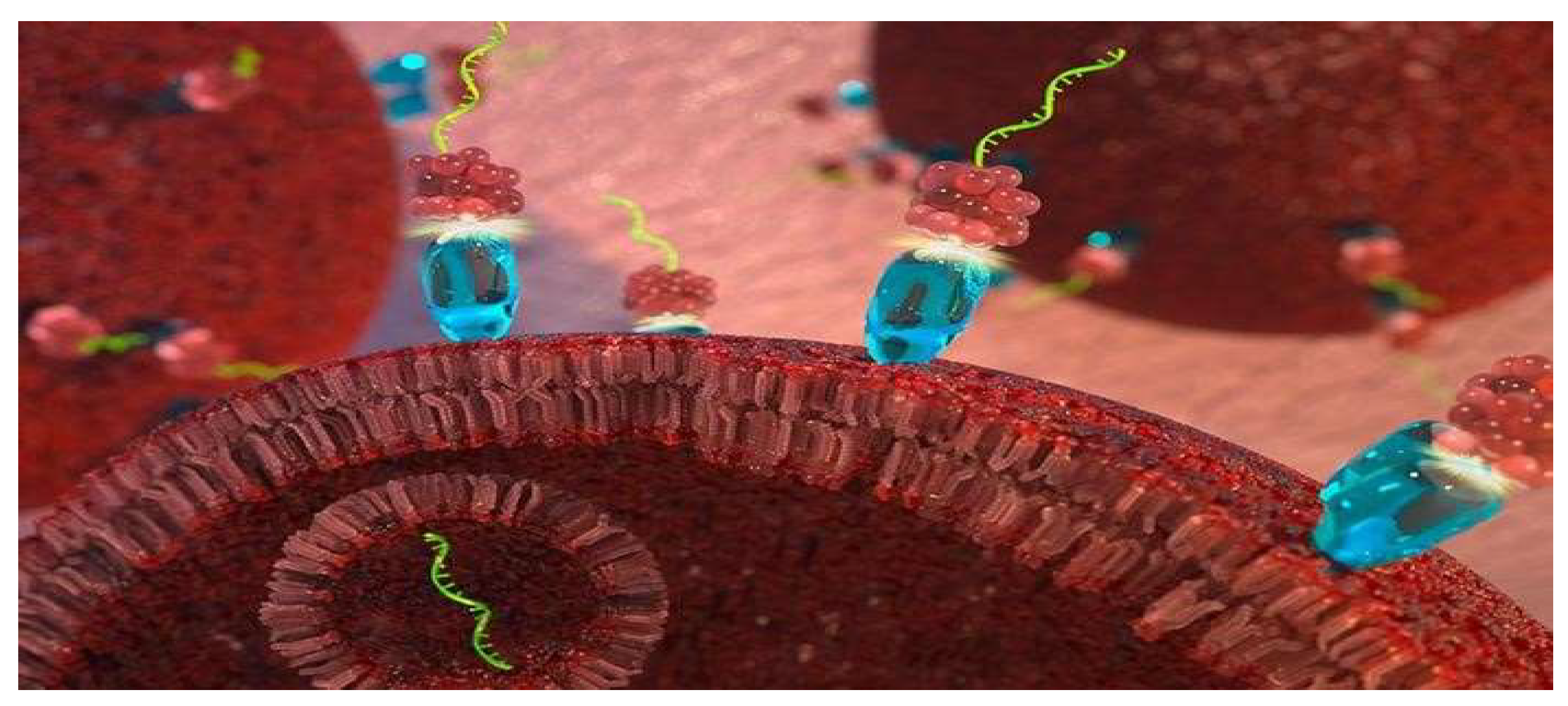
While the concept of reintroducing microRNA-34a into cancer cells may appear straightforward, researchers have faced numerous challenges in developing an effective therapy.It is well known that the membranes of cells in the human body have receptors that bind to folic acid and draw this vitamin into cells. So as so, the researchers attached a folate molecule vitamin with microRNA-34afor this to be inset in nucleus cells, [20], [Scheme 4].
Scheme 4.
A novel therapy targets cancer cells using a modified strand of microRNA that naturally inhibits cell division.
Scheme 4.
A novel therapy targets cancer cells using a modified strand of microRNA that naturally inhibits cell division.
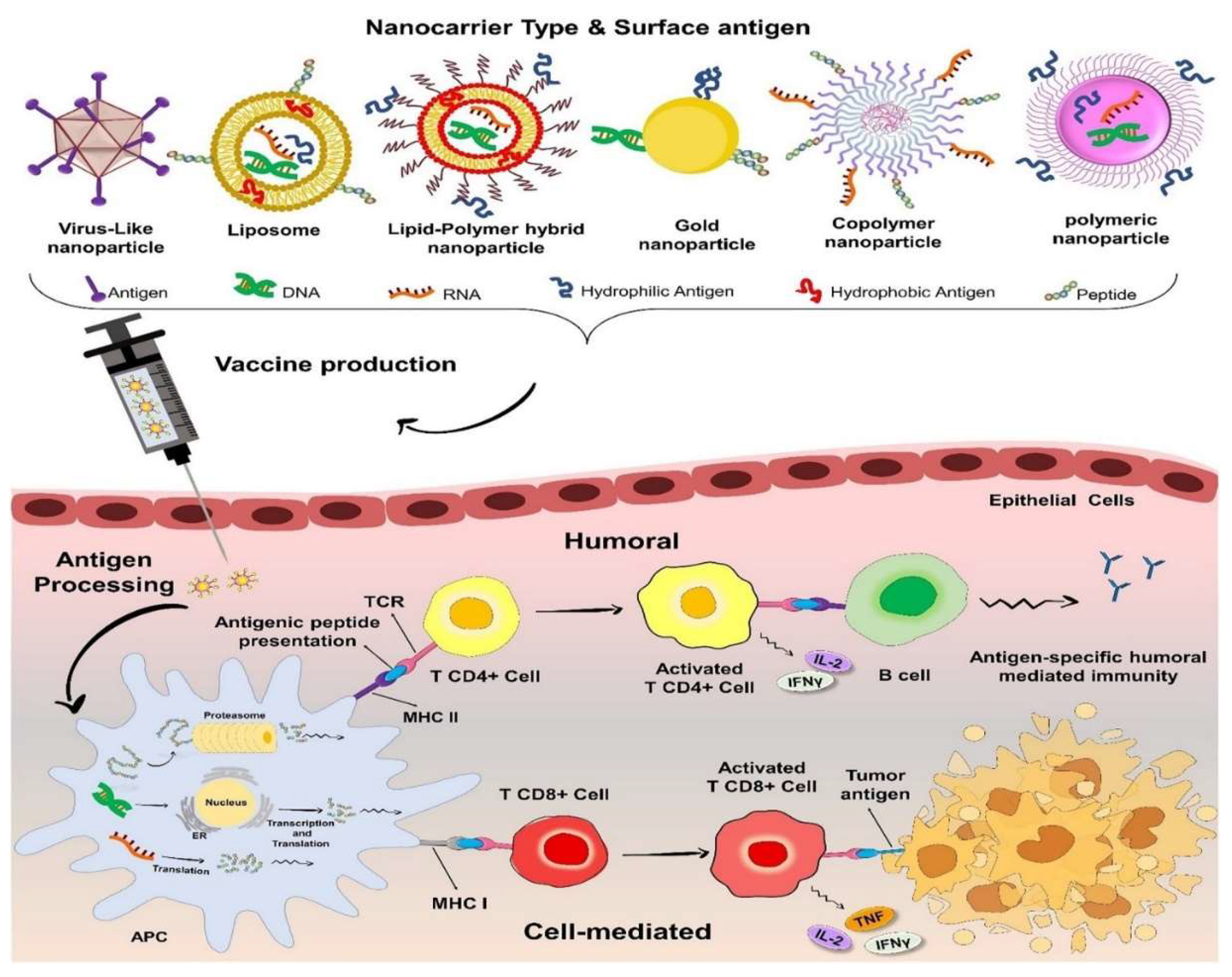
Active immunotherapies also create a protective effect against neoplastic tissue by readjusting the immune system to a state of antitumor surveillance. In tumour cells, antigen (Ag) expression differs from that of healthy cells. The differentiation of CD4+ and CD8+ T-cell responses is initiated by specialized antigen-presenting cells (APCs), such as dendritic cells (DCs). Ultimately, CD8+ T cells localize to tumour tissue, and target, and destroy cancer cells.However, due to its low antigenicity, immunotherapy is not recommended for ER+ breast cancer. Research findings indicate that various factors contribute to the reduced antigenicity of ER+ BC, which is linked to decreased production of tumour neoantigens (neo-Ag). In recent years, significant research has also focused on anti-HER2 vaccines, [21], [Scheme 5].
Scheme 5.
Anti-HER2 vaccines stimulate the differentiation of CD4+ and CD8+ T cells through specialized antigen-presenting cells (APCs), such as dendritic cells (DCs), ultimately enabling CD8+ T cells to target tumour tissue.
Scheme 5.
Anti-HER2 vaccines stimulate the differentiation of CD4+ and CD8+ T cells through specialized antigen-presenting cells (APCs), such as dendritic cells (DCs), ultimately enabling CD8+ T cells to target tumour tissue.
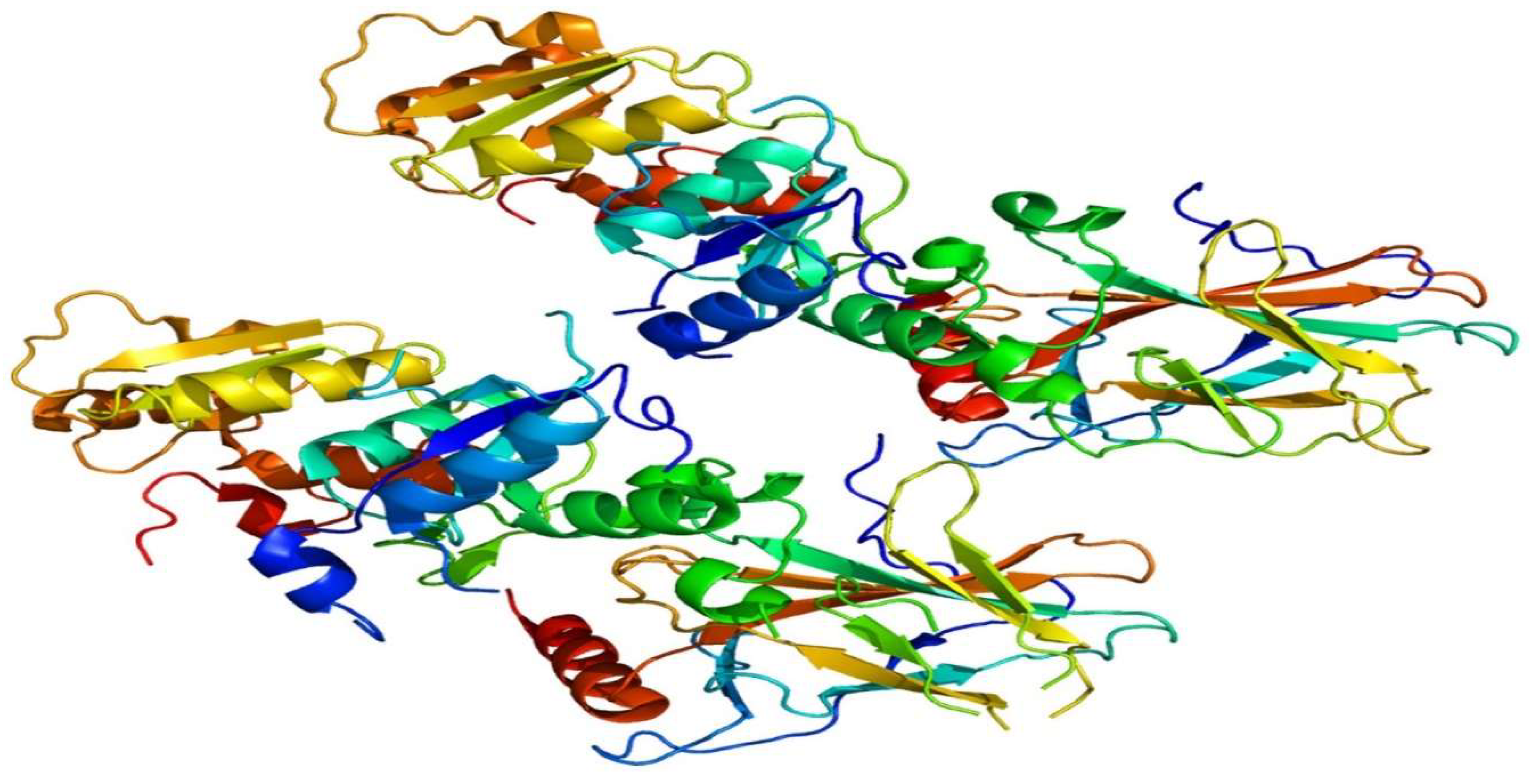
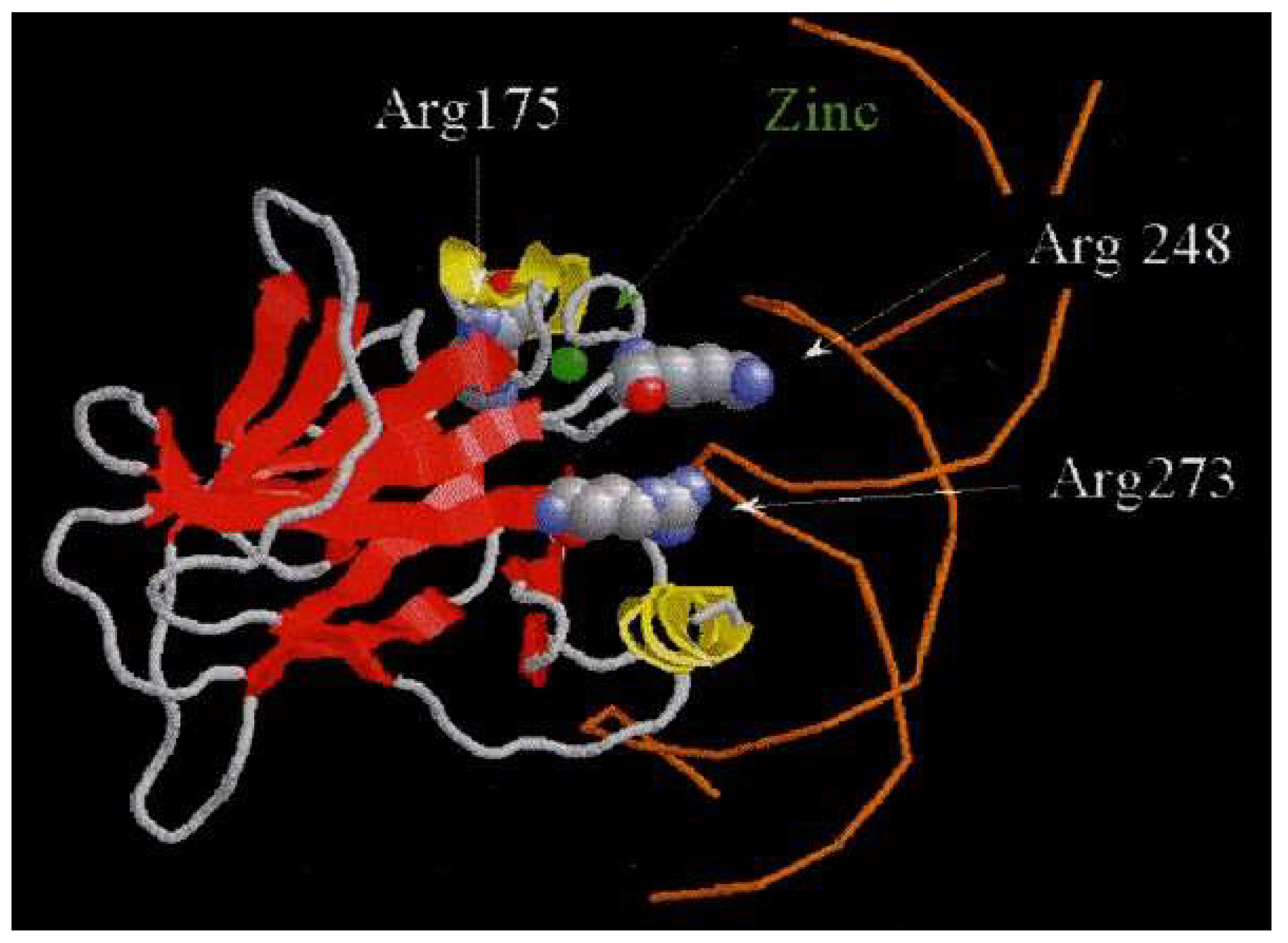
The last clinical studies of advanced BC, after the conventional oncologic treatment,have shown that the presence of P53 gene mutations was associated with lower survival rates of patients but the activation of the non-mutant P53 gene,presented in another form of BC,led to a complete inhibition of tumour growth by inhibiting the cytoplasmic oncogenic MDM2 protein., [22, 23, 24], [Figure 1].
Figure 1.
Three-dimensional representation of the p53 protein structure in its isomorphic form, obtained through X-ray imaging. In hereditary cancer clinics, five mutations of the P53 gene have been identified.
Figure 1.
Three-dimensional representation of the p53 protein structure in its isomorphic form, obtained through X-ray imaging. In hereditary cancer clinics, five mutations of the P53 gene have been identified.
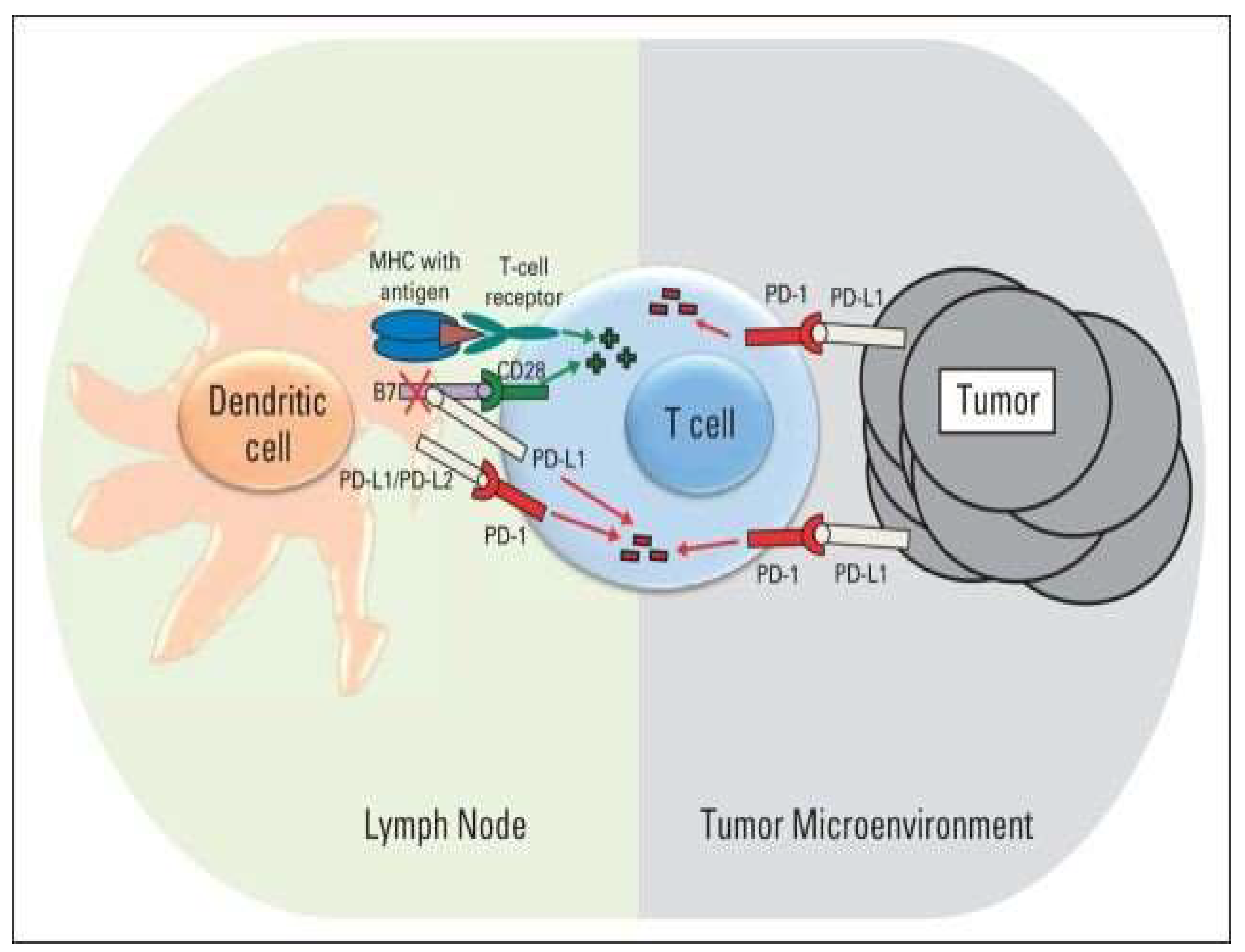
In clinical trials, antibodies specific to the p53 isoform protein, combined with peptides derived from p53, have been used to evaluate immune responses in cancer patients with P53 gene mutations. Short-term in vitro stimulation with p53-transfected dendritic cells showed that over 40% of breast cancer patients exhibited reactivation of CD4+ and CD8+ T cells. Numerous laboratory studies and clinical trials are currently underway, investigating anti-CTLA-4 antibodies and immune checkpoints such as PD-1/PD-L1, which could improve the outlook for patients with various types of malignancies, [25, 26],[Scheme 6].
Scheme 6.
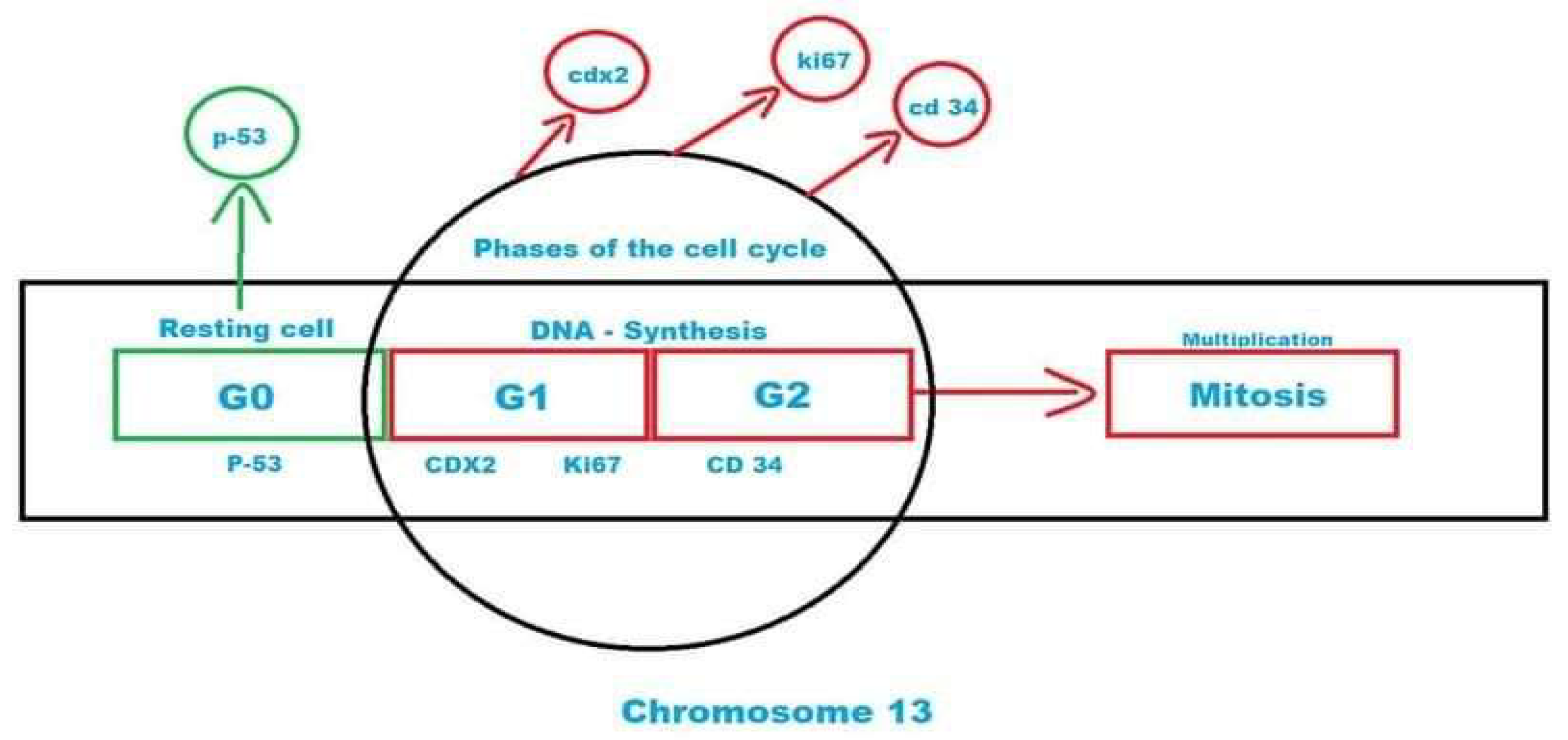
The Ki67 protein has a half-life of approximately 1–1.5 hours. It is present during all active phases of the cell cycle (G1, S, G2, and M), but is absent in resting cells (G0). In the later phases of mitosis (during anaphase and telophase), Ki67 levels decrease sharply, [Figure 3].
Scheme 6.
The Ki67 protein has a half-life of approximately 1–1.5 hours. It is present during all active phases of the cell cycle (G1, S, G2, and M), but is absent in resting cells (G0). In the later phases of mitosis (during anaphase and telophase), Ki67 levels decrease sharply, [Figure 3].
CRISPR/Cas9, as an effective genomic engineering tool, now has a vital role in treating various diseases.The efficacy of cancer therapy is increased by the use of CRISPR/Cas9 gene editing technologies, [27, 28].
For example, the CRISPR technology can be used for miR-124 editing reduction Also, in last studies demonstrated that the hormonal therapy applied inBC can be often combined with CDK4/6 inhibitor therapy with very good response in disease evolution, [29, 30].
Clinically, the index of proliferative studies of different types of cancer, indexpKi67 protein has been shown to be higher in malignant tissues with poorly differentiated tumour cells compared to normal tissues. A past cutoff of 20%was established for classifying cancer tumours as high proliferative., [31], [ Scheme 7].
Scheme 7.
Ki67 as a positive or negative marker in a tumour biopsy can be an oversimplification of its role as an indicator of tumour aggressiveness.
Scheme 7.
Ki67 as a positive or negative marker in a tumour biopsy can be an oversimplification of its role as an indicator of tumour aggressiveness.
Studies on Ki67 have indicated that it undergoes proteasome-mediated degradation during the G1 phase and upon cell-cycle exit. Additionally, the depletion of Cadherin1 (Cdh1), an activator of the Anaphase Promoting Complex (APC/C), has been linked to altered Ki67 regulation, [32].
5. Conclusions
Genetic research used to identify the genomics of malignant cells provides valuable scientific insights and offers improved predictors of tumour aggressiveness and cancer treatment outcomes. Additionally, the results of these researches are likely to play an increasing role in guiding personalized oncological treatments.
References
- Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2018; 68:394–424.
- Arnold, M. , Morgan, E., Rumgay, H., Mafra, A., Singh, D. et al. Current and future burden of breast cancer: Global statistics for 2020 and 2040. The Breast 2022; 66: 15–23.
- Dai X, Xiang L, Li T, Bai Z. Cancer Hallmarks, Biomarkers and Breast Cancer Molecular Subtypes. J Cancer. 2016;7(10):1281-1294. [CrossRef]
- Zaimy MA, Saffarzadeh N, Mohammadi A, Pourghadamyari H, Izadi P, Sarli A, Moghaddam LK, Paschepari SR, Azizi H, Torkamandi S, Tavakkoly-Bazzaz J. New methods in the diagnosis of cancer and gene therapy of cancer based on nanoparticles. Cancer Gene Ther. 2017; 24:233–243.
- Hung SK, Yang HJ, Lee MS. et al. Molecular subtypes of breast cancer predicting clinical benefits of radiotherapy after breast-conserving surgery: a propensity-score-matched cohort study. Breast Cancer Res 2023; (25); 149. [CrossRef]
- Dogra A, Mehta A, Doval DC. Are Basal-Like and Non-Basal-Like Triple-Negative Breast Cancers Really Different? J Oncol. 2020:4061063. [CrossRef]
- 7 Ismail A, El-Mahdy HA, Abuldsoud A et al. Beneficial and detrimental aspects of miRNAs as chief players in breast cancer: A comprehensive review. International Journal of Biological Macromolecules 2023; 224: 1541-1565.
- Si W, Shen J, Zheng H. et al. The role and mechanisms of action of microRNAs in cancer drug resistance. Clin Epigenetics. 2019; 11; 25. [CrossRef]
- Li JP, Zhang XM, Zhang Z, Zheng LH, Jindal S, Liu YJ. Association of p53 expression with poor prognosis in patients with triple-negative breast invasive ductal carcinoma. Medicine (Baltimore). 2019;98(18): e15449.
- Liu Y, Yang Y, Wang X, Yin S, Liang B, Zhang Y, Fan M, Fu Z, Shen C, Han Y, Chen B, Zhang Q. Function of microRNA-124 in the pathogenesis of cancer (Review). Int J Oncol. 2024 Jan;64(1):6. [CrossRef]
- Si, W. , Shen, J., Zheng, H. et al. The role and mechanisms of action of microRNAs in cancer drug resistance. Clin Epigenetics. 2019; 11; 25. [CrossRef]
- Amin MMJ, Trevelyan CJ, Turner NA. MicroRNA-214 in Health and Disease. Cells. 2021;10(12):3274. [CrossRef]
- Liu Y, Yang Y, Wang X, Yin S, Liang B, Zhang Y, Fan M, Fu Z, Shen C, Han Y, Chen B, Zhang Q. Function of microRNA-124 in the pathogenesis of cancer (Review). Int J Oncol. 2024;64(1):6. [CrossRef]
- Sarah, DG. Early Data for a Novel MiRNA Therapy Yield Promising Results. Oncology Times 2023; 45(23):p 17; http://doi/10.1097/01.COT.0000997480.29005.09.
- 15.. H, Torkamandi S, Tavakkoly-Bazzaz J. New methods in the diagnosis of cancer and gene therapy of cancer-based on nanoparticles. Cancer Gene Ther. 2017; 24:233–243.
- Vineis P, Wild CP. Global cancer patterns: Causes and prevention. Lancet. 2014; 383:549–557.
- Varna M, Bousquet G, Plassa LF, Bertheau P, Janin A. TP53 status and response to treatment in breast cancers. J Biomed Biotechnol.2011:284584. [CrossRef]
- Fatemeh-Davodabadi et al, Breast cancer vaccines: New insights into immunomodulatory and nano-therapeutic approach. Journal of Controlled Release. 2022; 349(4). https://www.researchgate.net/.
- Jia X, Wang X, Guo X, Ji J, Lou G, Zhao J, Zhou W, Guo M, Zhang M, Li C, Tai S, Yu S. MicroRNA-124: An emerging therapeutic target in cancer. Cancer Med. 2019 Sep;8(12):5638-5650. http://doi/10.1002/cam4.2489.
- Sarah, DG. Early Data for a Novel MiRNA Therapy Yield Promising Results. Oncology Times. 2023; 45(23): p 17; http://doi/10.1097/01.
- Sahar MA, Paish M, Powe DG et al. Tumor-Infiltrating CD8÷ Lymphocytes Predict Clinical Outcome in Breast Cancer Journal of Clinical Oncology 2011; (29)15. [CrossRef]
- Phillips KA, Nichol K, Ozcelik H, Knight J, Done SJ, Goodwin PJ et al. Frequency of p53 Mutations in Breast Carcinomas from Ashkenazi Jewish Carriers of BRCA1 Mutations, JNCI: Journal of the National Cancer Institute. 1999; (91)5;3: 69–473. [CrossRef]
- Jabir FA, Hoidy WH. No Evaluation of Serum P53 Levels in Iraqi Female Breast Cancer Patients. Asian Pac J Cancer Prev. 2017;18(9):2551-2553. doi. [CrossRef]
- Guptaa A, Shahb K, Ozac MJ, Behld T. Reactivation of the p53 gene by MDM2 inhibitors: A novel therapy for cancer treatment. Biomedicine & Pharmacotherapy. 2019; 109: 484–94.
- Pereira JA, Lanzar Z, Clark JT, et al. PD-1 and CTLA-4 exert additive control of effector regulatory T cells at homeostasis. Front. Immunol. 2023; 14: 20-23. [CrossRef]
- Paukena KE, Torchiac JA, Chaudhric A, Sharpea AH, Freeman GJ. Emerging concepts in PD-1 checkpoint biology. Seminars in Immunology. 2021: 101480. In Press,. [CrossRef]
- Ghosh C, Luong G, Sun Y. A snapshot of the PD-1/PD-L1 pathway. J Cancer. 2021;12(9):2735-46. [CrossRef]
- Torsin LI, Petrescu GED, Sabo AA, Chen B, Brehar FM, Dragomir MP et al. Editing and Chemical Modifications on Non-Coding RNAs in Cancer: A New Tale with Clinical Significance. Int. J. Mol. Sci. 2021; 22: 581. [CrossRef]
- Park M, Kim D, Ko S, Kim A, Mo K, Yoon H. Breast Cancer Metastasis: Mechanisms and Therapeutic Implications. Int J Mol Sci. 2022;23(12):6806. [CrossRef]
- Patanaphan V, Salazar OM, Risco R. Breast cancer: metastatic patterns and their prognosis. South Med J. 1988; 81(9):1109-1112.
- Romero Q, Bendahl PO, Fernö M, et al. A novel model for Ki67 assessment in breast cancer. Diagn Pathol. 2014; 9: 118. [CrossRef]
- Sobecki M, Mrouj K, Camasses A, et al. The cell proliferation antigen Ki-67 organises heterochromatin. Elife. 2016;5: e13722. [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



