1. Introduction
Death by road traffic crashes (RTC) is a major public health challenge globally [
1,
2], in low- middle income countries (LMIC) and especially in Africa [
3]. In Ghana the situation is not any better with the Ashanti region recording the highest number of RTC fatalities [
4,
5]. Preventing RTC is the gold standard but when they do occur, minimizing the consequences of severe injuries by providing care to the injured significantly contributes to reduction in morbidity and mortality [
6,
7,
8,
9,
10]. Poor access to emergency medical services, prehospital care and medical imaging modalities needed for efficient diagnosis in health facilities contribute to preventable deaths that occur in the trauma setting, especially in Africa [
11,
12].
When injured RTC victims are admitted to the emergency room in a hospital, they are often unconscious, in shock, disoriented or intubated. Depending only on clinical examinations alone has been shown to be unreliable for ruling out traumatic injuries [
13,
14]. Diagnostic imaging techniques have proven to help in confirming the suspicions of the clinicians and helping guide treatment pathways resulting in reduced treatment costs and improved outcomes [
15]. Improvements in imaging technologies over the last few decades have enhanced the understanding and management of trauma patients and have proven to be essential to guide diagnosis thereby lessening the risk of mortality and morbidity [
16,
17,
18,
19].
The Advanced Trauma Life Support (ATLS) program of the American College of Surgeons (ACS) has globally influenced the protocols governing the care of severely injured patients and is based on the fundamental principle of rapid assessment and resuscitation of patients in the window of opportunity, widely known as the “Golden Hour” to lessen the risk of morbidity or mortality [
20]. The ATLS recommends diagnostic imaging for trauma patients during primary surveys for resuscitation, and during secondary surveys for definitive care. The adjuncts to primary survey for trauma patients include antero- posterior (AP) chest radiograph, pelvic radiograph and/or lateral cervical spine radiograph to check for fractures and other life- threatening injuries and abdominal sonography (known as FAST: Focused Assessment with Sonography in Trauma) to quickly detect free intra- peritoneal fluid which may indicate abdominal bleeding. These essential diagnostic examinations offer critical information to the clinicians to support resuscitative measures [
21]. The adjuncts to the secondary surveys include specialized diagnostic tests such as whole/ total body CT scan (using the computed tomography machine) to rule out cranio-cerebral, cervical or thoraco-abdominal injuries, or magnetic resonance imaging (MRI) scans if brain injuries are suspected [
13,
17,
20]. These essential diagnostic tests make imaging equipment vital to the initial assessment of RTC victims. Despite the apparent advantages diagnostic imaging offers to the clinician in the trauma environment, resource-limited settings have faced significant challenges in improving access to these necessary diagnostic equipment. Some of the barriers relate to the cost of the equipment, the lack of infrastructure needed to support their use (water, electricity, internet, access roads, etc.), poor maintenance regimes due to lack of trained biomedical engineers, insufficient radiologists, to mention a few [
22,
23,
24,
25].
The growing role of medical imaging in the management of trauma victims, along with the development of more sophisticated technologies, is supporting the clinician to better depict life-threatening diagnoses. Even though the need for imaging equipment for early and efficient diagnosis of RTC injuries has been well documented, there is paucity of knowledge regarding where they are located with respect to RTC, their functional state and how accessible they are to crash- prone areas (also known as blackspots) in Ghana.
This study covered four (4) imaging modalities; ultrasonography (US), radiography (x-ray), computed tomography (CT) and magnetic resonance imaging (MRI). The findings of this study will reveal the current situation in the Ashanti region and help policy makers decide on ways to improve the situation. For this study, an equipment is functional if it is operational, produces reliable and accurate images, is available for use when needed and safe to use by its operator [
26]. A summary of these modalities and their usefulness in the management of RTC injuries is presented in
Table 1.
This study is part of a larger one that sought to investigate accessibility of emergency medical services to road traffic injury victims within the Ashanti region. The objective of this current study was to investigate the availability and functionality of essential imaging equipment in health facilities for RTC injury management in the Ashanti region.
2. Methods
The Ashanti region is Ghana’s third largest out of the sixteen regions covering a land surface of 24,389 km2. Lying between longitudes 0.15W and 2.25W and latitudes 5.50N and 7.46N, the region has a population of 5.44 million persons making it the most populated region [
32]. Ashanti boasts of 658 health facilities with 53% being privately- owned, 33% being government- owned, 11% being quasi- governmental and 3% being faith- based facilities. The Ghana Health Service and the Ministry of Health have oversight responsibility of all government-owned facilities [
33].
This study was a cross-sectional one with a quantitative approach. Preliminary data on possible locations of the modalities in question were sourced from the Ashanti Regional Health Directorate of the Ghana Health Service and consolidated with work done by Bour et al. (2024) [
34]. The essential imaging modalities of interest were ultrasound (US), radiography (x-ray), computed tomography (CT) and magnetic resonance imaging (MRI) because they are recommended for the initial evaluation of trauma patients involved in high-energy vehicular crashes [
20]. A structured questionnaire adapted from the World Health Organization (WHO)’s Harmonized Health Facility Assessment (HHFA) tool [
35] was used to collect data on the facilities and equipment availability, functionality and maintenance status from the preselected facilities. The study questionnaire was administered by ABP and research assistants to appropriate personnel (administrators, radiologists and/ or biomedical engineers) at all 48 public, private and Christian Health Association of Ghana (CHAG)- owned facilities (hospitals and diagnostic centers) known to have at least one of the modalities of interest. Written consent was obtained from each participant at the facility. Information collected included details of the facilities, the presence and functional status of the equipment. Geolocation data of all the imaging equipment identified during the study were collected and mapped. The presence of ultrasound machines alone did not qualify a facility to be part of this study as most of such facilities were maternity or family clinics without emergency departments hence unsuitable as destination hospitals for RTC victims. The primary data were collected between March and April 2024. Secondary geospatial data of all crash-prone areas in the Ashanti region were sourced from Mesic et al. (2024). The type of facility at which the equipment was located was classified as either "health facility" (clinic or hospital) or "diagnostic center", which implies a location where diagnostic tests are performed, but where other care is not provided.
All the imaging modalities were geospatially mapped with ESRI’s ArcGIS Pro software version 3.3.2, after which geolocations of all 104 blackspots were superimposed on the data set. A proximity tool (Near Analysis) was conducted to determine the travel distance between blackspots and each of the modalities available, assuming 100% functionality and repeated exclusively with actual functional units. The output of the solver was exported into Microsoft Excel spreadsheet version 16.92 (Microsoft Corporation, Redmond, Washington, USA) for analysis and visualization.
Another tool, the Closest-facility solver was used to find the number of blackspots closest to health facilities with CT installed base, assuming 100% functionality; the same analysis was conducted with only actual functional units and the differences in access were examined. The analysis was based on imaging modality types, ownership, age from year of installation, type of maintenance cover and functional status. Comparative analysis of ownership/ functionality and maintenance cover type/ modality were performed.
This study was approved by the Ghana Health Service Ethics Review Committee (GHS-ERC:024/10/23), the Komfo Anokye Teaching Hospital Institutional Review Board (KATH.IRB/AP/014/24) and the Ethical Committee for Basic and Applied Science of the College of Basic and Applied Science, University of Ghana (ECBAS 006/23-24).
3. Results
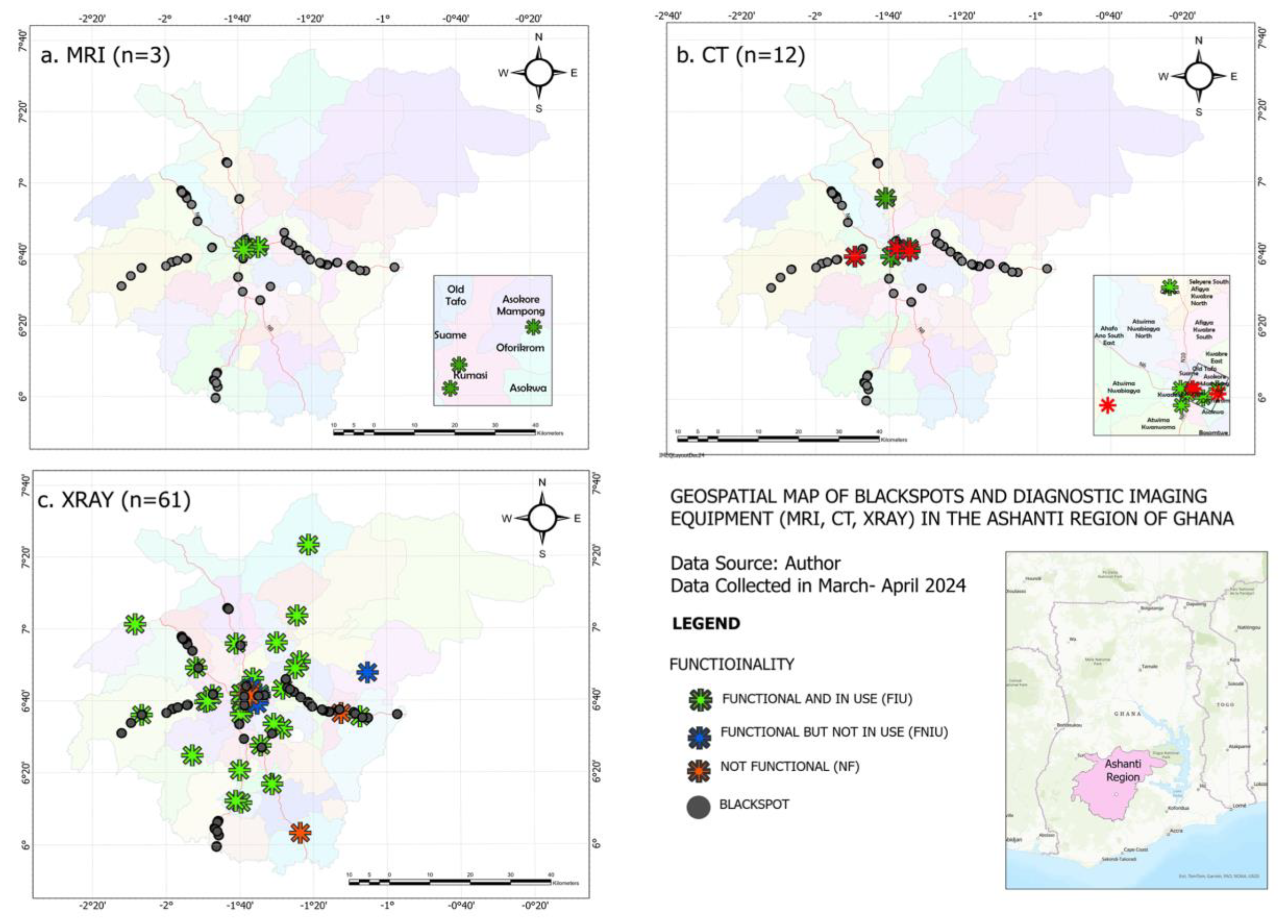
Figure 1 shows the geographical spread of the imaging modalities with respect to injury blackspots in the Ashanti region.
All of the MRI machines were concentrated in the center of the region. Two (16.67%) CT machines were geographically located outside the central part of the region, one of which was not functional. X-ray machines were sufficiently spread around most of the blackspots in the region.
Forty-eight (48) facilities were visited and a response rate of 93.8% was achieved of which 84.4% (n=38) were health facilities and 15.6% (n=7) were diagnostic centers. From
Table 2, two of the three MRIs in the region were in the health facilities; 1 in a public and the other in a private hospital. At the time of data collection, all three were functional and in use with an average age of almost 10 years. No faith-based facility owned an MRI machine.
The CTs that were found in this study were primarily in health facilities (60%) and in the private sector. Majority (66.7%) were found to be functional and in use with an average age of 6.5 years.
Almost 60% of x-ray machines were found in the public sector with CHAG and private facilities constituting 11.5% and 29.5% ownership respectively. A significant majority (82%) of x-ray units were found to be functional and in use with an average age of 7.8 years. (
Table 1)
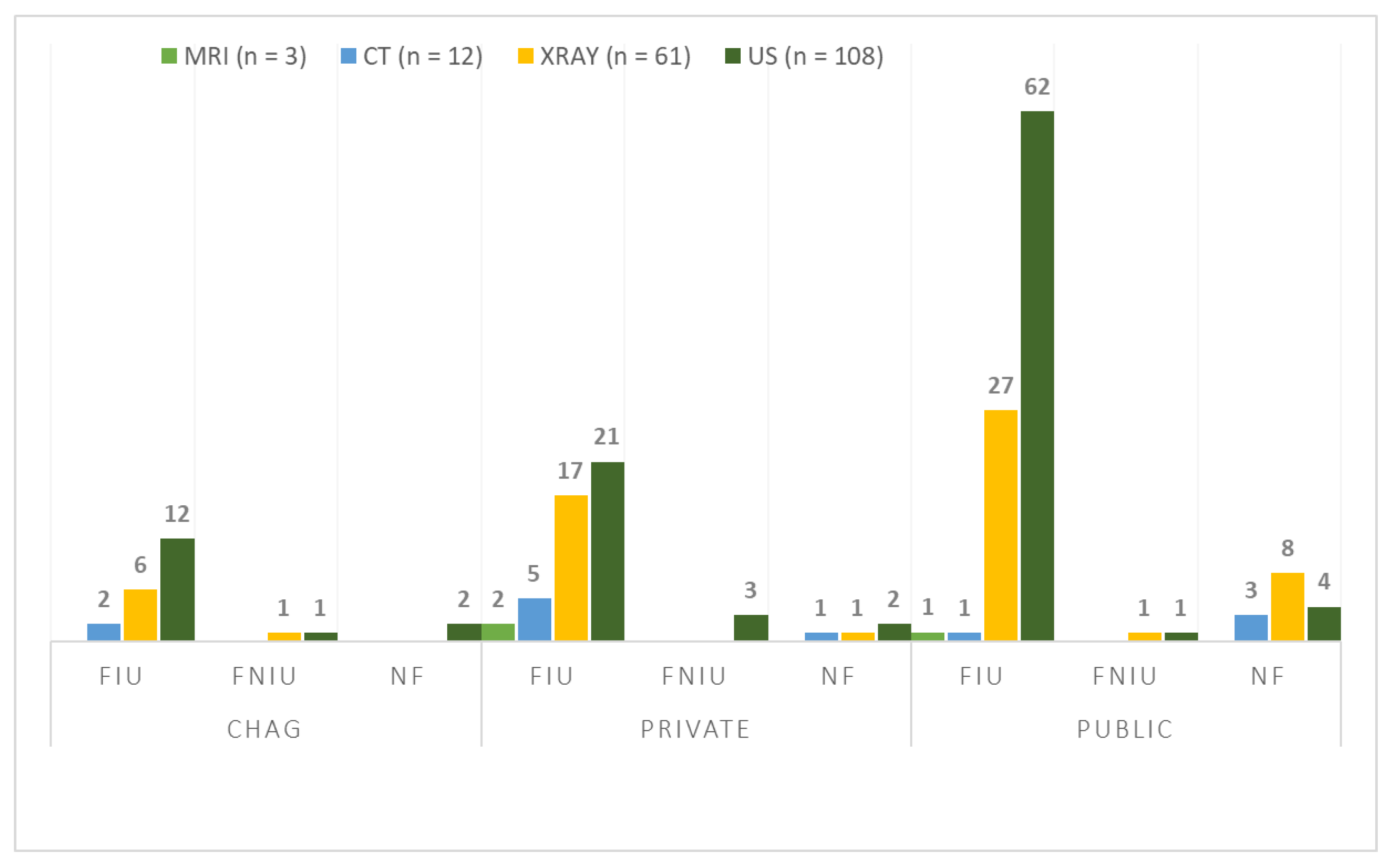
Figure 2 shows the functional status of the modalities with respect to ownership while
Table 2 lists the reasons for non- functionality. There were more non-functional CT machines in the public sector while majority of x-ray machines in the public, private and faith-based facilities were functional and in use.
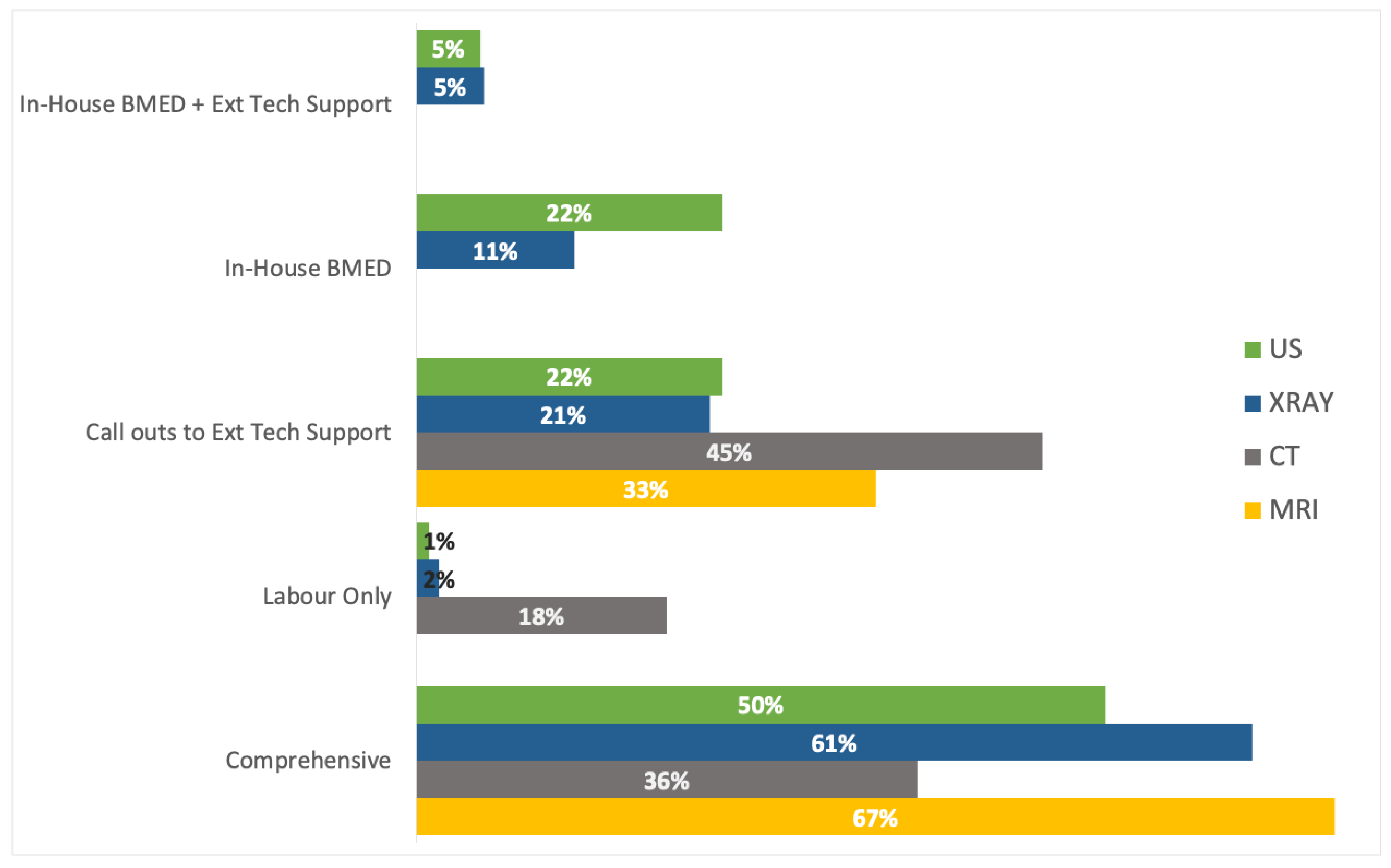
Figure 3 shows the proportion of the imaging modalities that had some maintenance cover. MRIs were mostly covered under comprehensive service contracts while CTs were mainly not covered at all (45%) or had a labour-only cover (18%). A third of CTs were however found to be covered comprehensively. Over half of x-ray machines (56%) were covered comprehensively with a significant number of facilities reporting callouts to external technical teams for support. The two modalities that in-house biomedical engineering teams had technical expertise to maintain were the ultrasound and x-ray machines.
Table 3 reveals the impact of non-functionality on access to imaging services by RTC victims. It shows the geographical proximity (by travel distance) of the three diagnostic imaging modalities. The distance from a blackspot to a health facility where an x-ray machine was available and definitive care could be given to victims was found to be about 9km assuming that all the x-ray machines were functional in those hospitals. The same analysis carried out excluding the non-functional equipment found a non-significant change in distance of about 20meters. However, the same analyses conducted on CT machines revealed a statistically significant travel distance increment of nearly three (3) kilometers of travel. Due to the statistically significant impact of non-functionality on CT access, the study went further to investigate the distribution of blackspots around health facilities that had a CT installed (
Table 4).
The results of geospatial closest-facility analysis for CT machines are shown in
Table 4. Seven (7) of the eight (8) health facilities with CT machines were found to be close to all the 104 blackspots identified in the Ashanti region however, three (3) health facilities- HFCT-02, HFCT-08 and HFCT-10- were closest to a combined majority (80%) of the known crash-prone areas. Repeating this analysis exclusively on health facilities with only functional CTs revealed a redistribution of blackspots to four (4) facilities only, with three (3) of them being close to 99% of all the blackspots.
Table 4.
How much longer will RTC victims travel to from crash sites to hospitals with diagnostic imaging equipment due to broken down equipment?
Table 4.
How much longer will RTC victims travel to from crash sites to hospitals with diagnostic imaging equipment due to broken down equipment?
| |
Distance measurement in kilometres |
| |
Distance to ALL hospital- based machines
n (SD) |
Distance to ONLY functional hospital- based machines
n (SD) |
Change in av. distance |
p- valueb
|
| X-rayc
|
8.68 (5.15) |
8.70 (5.12) |
+0.02 |
0.068a
|
| CTd
|
26.82 (19.04) |
29.63 (19.41) |
+2.82 |
0.000a
|
| MRIe
|
35.43 |
35.43 |
0.00 |
NA |
Table 5.
How does non-functionality of CT machines affect the distribution of blackspots around health facilities?
Table 5.
How does non-functionality of CT machines affect the distribution of blackspots around health facilities?
| Health Facility Code |
Number of Blackspots closesta to Facility assuming all CTs were functional |
Number of Blackspots closest to functional CTs only |
Percentage change in number of Blackspots |
# of slices of CT |
Age of CT |
Type of maintenance cover |
| HFCT-01 |
6 |
44 |
633% |
16 |
11 |
Comprehensive |
| HFCT-02 |
27 |
- |
|
16 |
2 |
Comprehensive |
| HFCT-04 |
10 |
36 |
260% |
16 |
7 |
Comprehensive |
| HFCT-05 |
4 |
- |
|
128 |
12 |
Call outs to external team |
| HFCT-06 |
1 |
5 |
400% |
32 |
2 |
Call outs to external team |
| HFCT-08 |
38 |
- |
|
6 |
5 |
Labour only |
| HFCT-10 |
18 |
19 |
56% |
32 |
1 |
|
| TOTAL |
104 |
104 |
|
|
|
|
4. Discussion
This study aimed to analyze accessibility of essential diagnostic imaging equipment to RTC victims to support efficient diagnoses of their injuries. As part of a larger study on the efficiency of emergency medical services, we investigated the availability and functionality of MRI, CT, x-ray and ultrasound machines in health facilities in Ashanti region, the region with the highest number of road crash fatalities in Ghana.
4.1. MRI
Figure 1a shows the sparsity of MRI technology in the Ashanti region of Ghana. The World Health Organization (WHO) determines accessibility by calculating number of scanners per million people (pmp). This study found that the Ashanti region’s three MRI machines equated to a density of 0.55 pmp which is lower than South Africa’s 3 pmp [
36], similar to Zimbabwe’s 0.5 pmp [
37] but higher than Ghana’s overall 0.08 pmp [
34] and Sub- Saharan Africa (SSA)’s 0.04 pmp [
38]. Even though this could be considered as good density for a geographical region, the data revealed that there really is only one MRI in the public sector to support diagnostics and is installed in the only public tertiary facility. While the ATLS recommends MRI scans for severely injured patients, the Royal College of Radiologists emphasize that MRI is rarely indicated in the acute trauma setting except in some specific cases such as epidural hematoma or when brain or spinal injuries are suspected [
40]. Longer image acquisition times and the need for patient stability hemodynamically before MRI scanning require that other forms of diagnostic tests, such as CT scans, and treatments be done before an MRI [
14].
The average travel distance from a blackspot to an MRI machine in the Ashanti region could be attributed to the fact that most of the crash- prone areas are in the peri-urban and rural areas, whereas the MRI machines are concentrated in the central urban part of the region. The pressure on these services requires that these machines be functional always and available to render service, as was found to be the case in the region.
All 3 MRI machines, with an average age of approximately 10 years, were functional and in use and were mainly under comprehensive maintenance contract. Complexities involved in maintaining this capital- intensive technology has forced owners to utilize the services of external contractors which end up being costly over the long term. None of them were maintained by the in-house biomedical engineering team. This may be due to expertise residing with private medical equipment distributors, a finding which corroborates what was found in a survey of MRI machines in Africa [
39]. In addition to this, the extremely high cost of the equipment, poor infrastructure (unreliable electricity, water, poor internet connectivity, expensive setup costs, and so on) including a dearth in radiographers and radiologists to support the utilization of this technology have been identified as barriers to MRI access [
38].
4.2. CT
Figure 1b shows the geographic spread of all 12 CT machines. Similar to findings from Kenya [
40], majority of the CT machines were found in the central and urban part of the region, with 2 on the outskirts, one of which was non-functional. The number of CT units translates to 2.21pmp, less than South Africa’s 5.0 pmp [
36] and Kenya’s 3.9 pmp [
40] but greater than Ghana’s national total of 1.46 pmp [
34], Zimbabwe’s 1.5 pmp [
37], Zambia’s 0.79 pmp, Uganda’s 0.6 pmp and Tanzania’s 0.42pmp [
41].
Despite the higher availability, majority of the units are in the private sector which is similar to what these other countries reported. This could be due to the high cost of ownership of a CT machine, considering factors such as infrastructure, maintenance, spare parts, training, and so on, an investment which is relatively easier to make in the private sector than public, especially in LMICs. Majority of the CT units were functional and in use (
Figure 2) which could be attributed to the comprehensive maintenance cover most of them had, a service being delivered by contracted private companies.
Furthermore, the study assessed spatial distance access to CT machines in health facilities.
The average distance from the 104 blackspots to a health facility with a CT machine was found to be an average of 27km, assuming all the eight CTs were functional. However, when restricting the analysis to only the four functional units and the average travel distance increased by 2.83km (p<0.000) highlighting the impact of non-functionality on RTC patient access. This delay in reaching care could worsen outcomes for severely injured RTC victims as increase in transport time is linked to reduced survival odds [
42]. These findings emphasize the urgent need for improved maintenance of CT machines to enhance trauma care.
Analyzing access to CT machines from blackspots from another perspective, this study sought to find out the health facilities with CT machines which were closest to blackspots and found that, assuming all units were functional 7 out of the 8 hospital-based CT machines were close to all 104 blackspots with 4 of them close to majority (89%) of the blackspots (
Table 3). When the non- functional hospital-based units (n=3) were isolated from the analysis, the study saw significant redistribution of blackspots to four hospitals with functional units. This analysis reveals the great impact of non-functionality on the options of suitable health facilities where severely injured RTC victims could be taken to within the region. This could imply therefore that these four hospitals would be under pressure from RTC injuries bearing in mind that these blackspots are crash-prone areas where severe injuries are known to occur frequently. Of particular note are the two hospital HFCT-02 and HFCT-08 which were close to more than half (n= 65) of the blackspots but whose CT machines were non-functional thereby contributing to the redistribution of pressure on to the four hospitals with functional units.
Some of the reasons for non-functionality were faulty tube, faulty parts and damaged UPS (
Table 2). None of these units was maintained by in-house biomedical engineering departments, a situation which could be an indicator of the lack of technical training provided to biomedical engineers in hospitals that own CT machines. Several studies have discussed the challenges of technically sustaining expensive diagnostic imaging equipment and one of the barriers, in addition to the high investment cost, is the lack of training of local biomedical engineers to carry out planned preventive maintenance. Most hospitals have no choice but to rely on expensive distributors/ agents to provide this technical service at a high cost which causes significant periods of non-functionality (downtime). With an average age of 6.5 years which is relatively low, one would have expected the functional units to be more.
4.3. X-Ray
Figure 1 shows a generous distribution of x-ray around the blackspots in the Ashanti region. Indeed the distribution was so uniform that the average travel time from a blackspot to a hospital-based x-ray device was found to be about 8km, which is considered as near [
42] a far cry from the 26km and 35km for CT and MRI machines respectively. Radiography has been identified by the ATLS as one of the recommended critical primary survey diagnostic tests conducted to confirm, among other things, the presence or absence of fractures in the extremities of severely injured RTC victims. So important is this that the WHO’s Guidelines for Trauma Care also recommends x-ray scans during the initial assessments carried out for all serious trauma victims. The Ashanti region can boast of an x-ray availability index of 11.21 units pmp, which is higher than Tanzania’s 9 pmp but significantly lower than Zimbabwe’s 26 pmp [
37] and South Africa’s 34.8 pmp [
36]. Interestingly, majority (82%) of these devices were found to be functional and in use (
Table 1), which could be attributable to the type of maintenance cover, as maintenance is the core reason for the high rates of non-functional medical equipment in LMICs. It is noteworthy that the x-ray modality was the only one which in-house biomedical engineering teams felt confident in supporting technically as can be seen in
Figure 3.
The impact of this high functionality is shown in the statistically non-significant (p = 0.068 at 95% confidence interval) average change in distance measure from blackspots to all x-ray machines (assuming 100% functionality) and from blackspots to only functional x-ray machines (82%). It was interesting to note also that majority of the x-ray were in the public sector and majority of the functional ones were also found in the public sector, a situation which is at variance to the other modalities, majority of which were in the private sector. Indeed, this could imply that majority of the health facilities with x-ray units which can quickly reveal life-threatening chest and pelvic injuries in trauma patients are more accessible to the general public because they are near most blackspots and are functional.
4.4. Ultrasound
The near ubiquitous ultrasound machine plays a critical role during the primary survey of the trauma patient via the Focused Assessment with Sonography for Trauma (FAST) which was introduced to support trauma assessment, diagnosis and management several decades ago [
20]. In a survey conducted across 62 LMIC on ultrasound utilization, it was discovered that 43% of respondents used the ultrasound machine (FAST) in the trauma setting [
43]. Due to its portability, low cost, non- invasiveness and relative ease of use, the ultrasound machine is commonly known as the ‘surgeon’s stethoscope of trauma’ acting as a practical tool to quickly detect free fluid in the pericardial space, pleural cavity and abdomen [
14,
18]. It is valuable for ruling in an injury but not ruling it out.
Unlike the x-ray and CT machines, the ultrasound machine does not emit any radiation so does not need to be registered by Ghana’s Nuclear Regulatory Authority before use [
34]; its portability makes it difficult to track and build a national database for [
34].
Even though this study recognizes the critical role of the ultrasound machine in the diagnosis of trauma injuries, data collected were not specific to this modality as the availability of the ultrasound machine alone was not enough to classify a health facility as suitable to receive RTC victims. Indeed, most of the ultrasound- alone facilities were maternity clinics or family practices without emergency departments. The ultrasound data therefore presented in this study were those found in hospitals that had one or more of the other modalities in question. For this study majority of ultrasound machines were in the public sector, in health facilities and functional. This study also found that local in-house biomedical engineers were adequately trained to provide preventive and corrective maintenance on ultrasound machines in the health facilities in the Ashanti region; this could account for the high rate of functionality of this modality.
4.5. Clinical Implication
The findings from this study underscore the very important roles of ultrasound and x-ray in the efficient diagnosis of injuries in trauma patients. It reveals that the Ashanti region has a good spatial distribution of these modalities with respect to blackspots, they are largely found in hospitals and not diagnostic centers, functional and in use, and maintained adequately well by in-house biomedical engineering teams in partnership with external firms. The predominance of x-ray and ultrasound modalities in the public sector suggests a deliberate attempt at maximizing coverage and accessibility for patients seeing that public hospitals are the first points of contact for RTC victims. This distribution could ensure that essential x-ray and ultrasound services are available to the broader segment of the population, especially those who may not have access to private healthcare facilities. The ability of in-house biomedical engineering teams to maintain them ensures the sustainability of the technology for its lifetime thereby reducing downtime and service disruptions.
Same can, however, not be said for the availability and functionality of MRI and CT. These limitations present challenges in providing a comprehensive scope of diagnostic imaging services, potentially leading to suboptimal outcomes especially for severely injured trauma patients. While x-ray provide sufficient insights into the bone structure and chest injuries, ultrasounds show the presence or absence of free fluids especially in the abdomen area while CT provides detailed assessment of potential internal injuries in soft tissues and organs, and when neurological or spinal injuries are suspected in the trauma patient, MRI scans are indicated. Despite concerns regarding substantial radiation exposure during diagnostic imaging, especially during CT scans [
27], improvements in all these imaging techniques that have occurred in the last few decades have significantly contributed to the understanding and efficient management of trauma patients’ injuries. A lack of the full complement of these diagnostic services may result in misdiagnosis, delayed treatments and ultimately poor patient outcomes.
5. Conclusions
This study highlights the critical gaps in diagnostic imaging availability and functionality in the Ashanti region, particularly for CT and MRI. Although X-ray and ultrasound modalities are well-distributed, their diagnostic scope is limited. Addressing these gaps requires a multi-pronged approach. In the short term, the Ministry of Health could prioritize the repair and maintenance of the non- functional CT machines in the 3 health facilities to improve access.
In the medium term, hospitals could establish partnerships with private diagnostic imaging centers within the region could also help provide interim solutions, although patients would have to be stabilized first before visiting private diagnostic centers for CT and MRI scans. Diagnostic centers that are close to hospitals without CT machines could have arrangements to prioritize the facilities’ patients and even send reports electronically to clinicians in the hospitals in an efficient manner.
It is also recommended that the proposed 500- bed Afari Military Hospital [
44] and 100- bed Obuasi Trauma Hospital currently under construction in the Ashanti region, both of which have diagnostics centers with modalities including MRI, CT and x-ray machines, among others [
45], be completed and operationalized to improve access to care.
Finally, there has to be a long- term strategic effort to invest in additional CT machines, especially in the high- risk, crash- prone areas and also build capacity in local biomedical engineers in the maintenance of all the imaging modalities, especially CT and MRI machines. From this study, it was noted that only x-ray and ultrasound technologies were the ones maintained by inhouse biomedical engineering teams. Building hospital in-house capacity can help reduce total reliance on private distributor companies whose services are usually expensive which contributes to the high cost of ownership.
5.1. Limitations
This study focused on ultrasound, x-ray, CT and MRI machines. There are other modalities which are useful in the diagnosis of trauma patients such as mobile x-ray units, fluoroscopy and C- Arms. Future studies on the availability and functionality of these modalities could provide a bigger picture on the state of diagnostic imaging equipment in the region.
5.2. Future Studies
Future studies could investigate the proportions of trauma victims that actually present at the emergency departments of these hospitals that have been identified to be close to RTC in the Ashanti region. An analysis of the diagnoses that were given and the types of imaging scans that were recommended to the trauma patients would lend some insights into the patient pathway. Also the trauma patients referred to the private diagnostic centers for scans could be studied to assess the demand of diagnostic imaging services within the region. Finally, future studies could investigate the cost-effectiveness of the different imaging modalities in trauma care and explore innovative solutions to improve access in resource- limited settings such as Ghana.
Author Contributions
Conceptualization, A.B.P, E.T, A.G, E.E.K, C.M and P.D.; methodology, A.B.P, C.M and P.D; validation, A.B.P, B.B, E.T, E.E.K, A.G, C.M and P.D; formal analysis, A.B.P; investigation, A.B.P; resources, C.M and P.D; data curation, A.B.P; writing—original draft preparation, A.B.P; writing—review and editing, A.B.P, B.B, E.T, E.E.K, A.G, C.M and P.D; visualization, A.B.P; supervision, E.T, E.E.K and A.G; funding acquisition, C.M and P.D.
Funding
Please add: This research was funded by the Fogarty International Center of the US National Institutes of Health, grant number D43-TW007267. The APC was funded by Fogarty International Center of the US National Institutes of Health.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Ethics Review Committee of the GHANA HEALTH SERVICE (protocol code GHS-ERC:024/10/23 on the 22nd December 2023), the Institutional Review Board of the KOMFO ANOKYE TEACHING HOSPITAL (protocol code KATH.IRB/AP/014/24 on the 22nd March 2024) and the Ethical Committee for Basic and Applied Science of the COLLEGE OF BASIC AND APPLIED SCIENCE OF THE UNIVERSITY OF GHANA (protocol code 006/23-24 on the 20th of November 2023) for studies involving humans.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors on request.
Acknowledgments
This study was funded by a grant (D43-TW007267) from the Fogarty International Center of the US National Institutes of Health. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Conflicts of Interest
The authors declare no conflicts of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
Abbreviations
The following abbreviations are used in this manuscript:
| AP |
Anterior- Posterior |
| ACS |
American College of Surgeons |
| ATLS |
Advanced Trauma Life Support |
| CHAG |
Christian Health Association of Ghana |
| CT |
Computed Tomography |
| ESRI |
Environmental Systems Research Institute |
| FAST |
Focused Assessment with Sonography in Trauma |
| FIU |
Functional and in use |
| FNIU |
Functional but not in use |
| HHFA |
Harmonized Health Facility Assessment |
| LMIC |
Low Middle-Income Country |
| MRI |
Magnetic Resonance Imaging |
| NF |
Non- functional |
| RTC |
Road Traffic Crash |
| UPS |
Uninterruptible Power Supply |
| US |
Ultrasound |
| WHO |
World Health Organization |
References
- World Health Organization., Save LIVES : a road safety technical package. World Health Organization, 2017.
- World Health Organization (WHO), Global Status Report on Road Safety, 1st ed. Geneva, 2018. Available online: https://www.who.int/publications/i/item/9789241565684.
- World Health Organization (WHO), Guidelines for essential trauma care, 1st ed. Gene: World Health Organisation, 2004.
- Ackaah, W., Larbi J., and Larley J., ‘Road Traffic Crashes in Ghana Statistics 2022’, Kumasi, Feb. 2024.
- Tawiah and E. Konadu- Boakye, ‘Nation spends $230m on injuries - Dr Ofori-Boadu discloses - Graphic Online’, Daily Graphic Online. Accessed: Sep. 07, 2022. Available online: https://www.graphic.com.gh/news/general-news/nation-spends-230m-on-injuries-dr-ofori-boadu-discloses.html.
- M. El Sayed, ‘Developing emergency and trauma systems internationally: What is really needed for better outcomes?’, J Emerg Trauma Shock, vol. 10, no. 3, pp. 91–92, Jul. 2017. [CrossRef]
- M. K. Harmsen, G. F. Giannakopoulos, P. R. Moerbeek, E. P. Jansma, H. J. Bonjer, and F. W. Bloemers, ‘The influence of prehospital time on trauma patients outcome: A systematic review’, Injury, vol. 46, no. 4, pp. 602–609, Apr. 2015. [CrossRef]
- S. L. Hsieh et al., ‘Association between the time to definitive care and trauma patient outcomes: every minute in the golden hour matters’, European Journal of Trauma and Emergency Surgery, 2021. [CrossRef]
- P. T. Pons and V. J. Markovchick, ‘Eight minutes or less: does the ambulance response time guideline impact trauma patient outcome’, J Emerg Med, vol. 23, pp. 43–48, 2002. [CrossRef]
- M. Cheng et al., ‘A systems management framework for medical device safety and optimal outcomes’, in Clinical Engineering Handbook, 2nd ed., J. F. Dyro, Ed., Elsevier, 2020, ch. 49, pp. 321–328. [CrossRef]
- World Bank, ‘The State of Emergency Medical Services in Sub-Saharan Africa.’, Washington, DC, 2021.
- N. K. Mould-Millman et al., ‘The state of Emergency Medical Services (EMS) systems in Africa’, Prehosp Disaster Med, vol. 32, no. 3, pp. 273–283, Jun. 2017. [CrossRef]
- D. Barron, ‘Polytrauma imaging – the role of integrated imaging’, Orthop Trauma, vol. 25, no. 2, pp. 83–90, Apr. 2011. [CrossRef]
- P.-A. Poletti, A. Platon, and C. D. Becker, ‘Role of Imaging in the Management of Trauma Victims’, in Emergency Radiology, 1st ed., Berlin, Heidelberg: Springer Berlin Heidelberg, 2002, ch. 1, pp. 3–23. [CrossRef]
- Crumley et al., ‘The impact of computed radiography and teleradiology on patients’ diagnosis and treatment in Mweso, the Democratic Republic of Congo’, PLoS One, vol. 15, no. 1, p. e0227773, Jan. 2020. [CrossRef]
- Victorian Department of Health, ‘Imaging in Trauma-Key Messages | Trauma Victoria’, Major Trauma Guidelines and Education. Accessed: Jun. 16, 2023. Available online: https://trauma.reach.vic.gov.au/guidelines/imaging-in-trauma/key-messages.
- H. Vela, C. I. Wertz, K. L. Onstott, and J. R. Wertz, ‘Trauma imaging: A literature review’, Radiol Technol, vol. 88, no. 3, pp. 263–276, 2017, Accessed: Jul. 02, 2023. Available online: https://www.scopus.com/record/display.uri?eid=2-s2.0-85015321421&origin=inward.
- Kumar, H. Agarwal, A. Gupta, S. Sagar, N. Banerjee, and S. Kumar, ‘Imaging Modalities in Trauma and Emergency—a Review’, Apr. 01, 2021, Springer. [CrossRef]
- K. Willett, ‘Imaging in trauma in limited-resource settings: A literature review’, African Journal of Emergency Medicine, vol. 9, pp. S21–S27, 2019. [CrossRef]
- ‘Student Course Manual ATLS ® Advanced Trauma Life Support ® FB:Cardiologia Siglo XXI’, 2018.
- R. M. Bell, B. E. Krantz, and J. A. Weigelt, ‘ATLS: A Foundation for Trauma Training’, Ann Emerg Med, vol. 34, no. 2, pp. 233–237, Aug. 1999. [CrossRef]
- N. Aderinto, ‘Diagnosing the disparities: an analysis of the current state of medical imaging in Africa and strategies for improvement: a correspondence’, International Journal of Surgery: Global Health, vol. 6, no. 3, pp. e138–e138, May 2023. [CrossRef]
- Driban et al., ‘Failure to receive prescribed imaging is associated with increased early mortality after injury in Cameroon’, PLOS Global Public Health, vol. 3, no. 8, p. e0001951, Aug. 2023. [CrossRef]
- S. Geethanath and J. T. Vaughan, ‘Accessible magnetic resonance imaging: A review’, Journal of Magnetic Resonance Imaging, vol. 49, no. 7, Jun. 2019. [CrossRef]
- G. Frija et al., ‘How to improve access to medical imaging in low-and middle-income countries ?-NC-ND license (http://creativecommons.org/licenses/by-nc-nd/4.0/) Keywords: Access to imaging Low-and middle-income countries Centre of reference International commission on medical imaging’, EClinicalMedicine, vol. 38, p. 101034, Jul. 2021. [CrossRef]
- E. Geta, D. Terefa, and A. Desisa, ‘Efficiency of medical equipment utiliization and its associated factors at public referral hospitals in East Wollega Zone, Oromia Regional State, Ethiopia’, Medical Devices: Evidence and Research, pp. 36–46, Dec. 2023.
- M. Hui, J. H. MacGregor, H. C. Tien, and J. B. Kortbeek, ‘Radiation dose from initial trauma assessment and resuscitation: review of the literature’, Canadian Journal of Surgery, vol. 52, no. 2, p. 147, 2009, Accessed: Jan. 29, 2025. Available online: https://pmc.ncbi.nlm.nih.gov/articles/PMC2663507/.
- R. S. Khandpur, Handbook of Biomedical Instrumentation, 3rd ed., vol. 1. New Delhi: McGraw Hill Education (India) Private Limited, 2014.
- J. D. Bronzino, The Biomedical Engineering Handbook, 3rd ed. Connecticut: Taylor and Francis, 2006.
- J. F. Dyro, Clinical Engineering Handbook, 1st ed. New York, NY: Elsevier, 2004. [CrossRef]
- P. B. Thippeswamy and R. B. Rajasekaran, ‘Imaging in polytrauma – Principles and current concepts’, J Clin Orthop Trauma, vol. 16, p. 113, May 2021. [CrossRef]
- Ghana Statistical Service (GSS), ‘2021 Population and Housing Census: Press Release of Provisional Results’, Accra, Sep. 2021. Accessed: Jun. 17, 2023. Available online: https://statsghana.gov.gh/gssmain/fileUpload/pressrelease/2021%20PHC%20Provisional%20Results%20Press%20Release.pdf.
- GHS, ‘Profile of GHS – Ghana Health Service’. Accessed: Nov. 04, 2024. [Online]. Available online: https://ghs.gov.gh/profile-of-ghs/.
- K. Bour et al., ‘National inventory of authorized diagnostic imaging equipment in Ghana: data as of September 2020’, Pan African Medical Journal, vol. 41, Jan. 2022. [CrossRef]
- ‘HHFA_questionnaire_combined_core_AllGroups27JAN23_Final_clean[1]’.
- J. M. Kabongo, S. Nel, and R. D. Pitcher, ‘Analysis of licensed South African diagnostic imaging equipment’, PAMJ. 2015; 22:57, vol. 22, no. 57, 2015. [CrossRef]
- T. Maboreke, J. Banhwa, and R. D. Pitcher, ‘An audit of licensed Zimbabwean radiology equipment resources as a measure of healthcare access and equity’, Pan African Medical Journal, Jan. 2019. [CrossRef]
- S. Geethanath and J. T. Vaughan, ‘Accessible magnetic resonance imaging: A review’, Jun. 01, 2019, John Wiley and Sons Inc. [CrossRef]
- U. C. Anazodo et al., ‘A framework for advancing sustainable magnetic resonance imaging access in Africa’, NMR Biomed, vol. 36, no. 3, Mar. 2023. [CrossRef]
- M. Gathuru, G. D. O. Elias, and R. D. Pitcher, ‘Analysis of registered radiological equipment in Kenya’, PAMJ. 2021; 40:205, vol. 40, no. 205, p. 205, Dec. 2021. [CrossRef]
- P. S. Ngoya, W. E. Muhogora, and R. D. Pitcher, ‘Defining the diagnostic divide: an analysis of registered radiological equipment resources in a low-income African country’, PAMJ. 2016; 25:99, vol. 25, no. 99, Oct. 2016. [CrossRef]
- J. Nicholl, J. West, S. Goodacre, and J. Turner, ‘The relationship between distance to hospital and patient mortality in emergencies: An observational study’, Emergency Medicine Journal, vol. 24, no. 9, pp. 665–668, Sep. 2007. [CrossRef]
- S. Ginsburg, Z. Liddy, P. T. Khazaneh, S. May, and F. Pervaiz, ‘A survey of barriers and facilitators to ultrasound use in low- and middle-income countries’, Sci Rep, vol. 13, no. 1, Dec. 2023. [CrossRef]
- ‘Afari Military Hospital to be ready March - Graphic Online’. Accessed: Feb. 18, 2025. Available online: https://www.graphic.com.gh/news/general-news/ghana-news-afari-military-hospital-to-be-ready-march.html.
- 100-bed Obuasi Trauma Hospital takes off …after President Akufo-Addo cuts sod - Ghanaian Times’. Accessed: Feb. 10, 2025. Available online: https://ghanaiantimes.com.gh/100-bed-obuasi-trauma-hospital-takes-off-after-president-akufo-addo-cuts-sod/.
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).