
Submitted:
18 February 2025
Posted:
19 February 2025
You are already at the latest version
Abstract
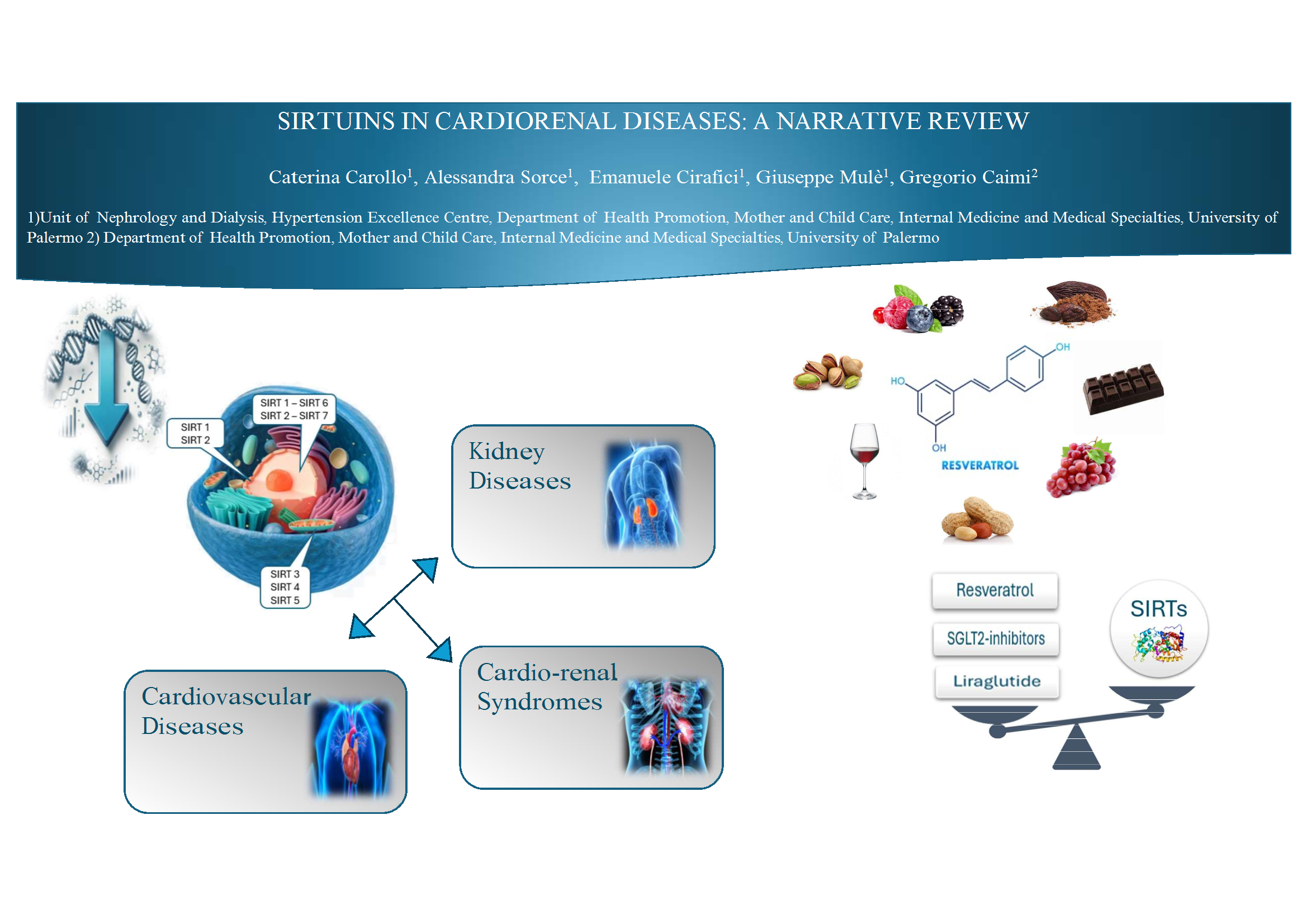
Aging is a very complex process and it has been linked with Sirtuins. Sirtuin enzymes are a family of deacetylases that are related with caloric restriction and aging by modulating energy metabolism, genomic stability and stress resistance. Up to now, seven sirtuins have been recognized. Our purpose is to clarify the role of sirtuins in Chronic Kidney Disease (CKD). Moreover, as heart and kidney diseases are strictly interrelated, we’re going to explore their role in heart diseases and cardio-renal cross-talk. A reciprocal relationship between CKD and aging seems to exist, since CKD may contribute to premature biological aging of different organ systems. SIRTs are involved in pathophysiology of renal diseases; their activation can delay the progression of several renal diseases. Cardiovascular diseases (CVDs) are the leading cause of global mortality and a major contributor to disability. Notably, an increasing number of studies linked SIRTs with different CVDs. SIRTs affect the production of mitochondrial reactive oxygen species (ROS) by modulating mitochondrial function. The imbalance of SIRTs levels may increase the vulnerability to CVDs. SIRTs are involved in pathophysiological mechanisms of HFpEF (heart failure with preserved ejection fraction) through different signalling pathways. Fibrosis is the linkage mechanism between heart and kidney in the development of cardio-renal diseases. Different natural SIRT1 agonists showed renoprotective effects and among these Resveratrol (RSV) and other phenolic compounds have been widely investigated with interesting and positive results. Future research is obviously needed to clarify the role of these molecules and their potential therapeutical role in heart and kidney diseases.
Keywords:
sirtuins
; SIRTs
; CKD
; CV disease
; Cardio-renal syndrome
; Resveratrol
; Aging
Introduction
In previous papers we described the emerging role of sirtuins in aging and aging-related diseases. [1,2] Aging is a very complex process in which genetic, environmental and cellular pathways are involved.
Sirtuin enzymes are a family of highly conserved protein deacetylases that are related with caloric restriction and aging by modulating energy metabolism, genomic stability and stress resistance. Sirtuins may promote different post translational modifications in many different proteins so they are actually known as deacylases [3]. Sirtuins’ activity depends on nicotinamide adenine dinucleotide (NAD). This is very important if we consider that NAD is a crucial cofactor for many mitochondrial metabolic processes that lead to energy production. Mitochondria are largely expressed in heart and kidneys. Mitochondrial ROS production leads to altered DNA and electron chain transport, thus impairing mitochondrial function. This dangerous chain could be counteracted by healthy mitochondria and selective autophagy of damaged ones thus explaining the beneficial effects of caloric restriction. [4]
Up to now, seven sirtuins have been recognized, listed from 1 to 7. Each of them shows a catalytic domain (present in all sirtuins) whilst different N- and C-ends give specific biological features to every sirtuin.
In our previous papers [1,2] we examined the role of sirtuins in influencing the factors that worsen physiological aging such as glucose metabolism, DNA stability and cancer, neurodegenerative processes, COPD.
Now our aim is to clarify the role of sirtuins as pathophysiological agents and therapeutical targets in Chronic Kidney Disease (CKD). Moreover, as heart and kidney diseases are strictly interrelated, we’re going to explore their role in heart diseases and cardio-renal cross-talk.
Sirtuins in Kidney Diseases
By 2021, a joint statement from the American Society of Nephrology, European Renal Association, and International Society of Nephrology indicated that more than 850 million people suffer from some form of kidney disease. CKD affects between 8% and 16% of the population worldwide. It is defined by a glomerular filtration rate (GFR) of less than 60 mL/min/1.73 m2, albuminuria of at least 30 mg per 24 hours, or markers of kidney damage (eg, hematuria or structural abnormalities such as polycystic or dysplastic kidneys) persisting for more than 3 months [5].
CKD is associated with a great increase in morbidity and mortality and a decrease in health related quality of life. The severity of these complications is generally proportional to the decline in renal function and it is most evident in patients with end-stage renal disease (ESRD) [6]. Moreover, CKD causes very important economic consequences. In 2023, in USA there was a 40% increase, from $54.9B to $76.8B in expenditures for individuals with CKD [7].
The risk of CKD increases with age and elderly patients are overrepresented in dialysis population [8]. Moreover, a reciprocal relationship between CKD and aging seems to exist, since CKD may contribute to premature biological aging of different organ systems [9]. This may result in the occurrence of usually geriatric complications in relatively young patients with ESRD [10].
Each of the seven sirtuins plays a role in this complex relationship.
Sirt1 is widely expressed in renal tubular cells and podocytes [11], SIRT2 is mainly expressed in proximal epithelial renal tubular cells [12]. SIRT1 and SIRT2 are located both in nucleus and cytoplasm. SIRT3, Sirt 4 and SIRT5 are demonstrated in mitochondria [13] of proximal epithelial tubular cells [14,15]), SIRT 6 and SIRT7 can be found almost exclusively in nucleus (SIRT7 in proximal tubules and collecting tubules [16].
Previous studies confirmed that SIRTs are involved in pathophysiology of renal diseases [17]; their activation can delay the progression of several renal diseases, including diabetic kidney disease (DKD), acute kidney injury (AKI), and hypertensive nephropathy.
One of the most common causes of CKD is diabetes. Diabetic kidney disease (DKD) is defined by the presence of CKD in a person with diabetes [5] and it is considered as the leading cause of end-stage renal disease (ESRD) in developed and developing countries [18]. The mostly involved sirtuins in the pathophysiology of DKD are: SIRT1, SIRT3 and SIRT6. [19,20]. Previous studies have shown that levels of these sirtuins are decreased in patients with diabetes and DKD: metabolism of glucose and fatty acids produces NADH with consequent impaired NAD+/NADH ratio and low expression of sirtuins. In murine models, a correlation was found between low levels of SIRT1, SIRT3 and SIRT6 and increased proteinuria, fibrosis and podocyte damage resulting in kidney injury [21]. SIRT1 knockout mice exhibited worsening of diabetic kidney modifications and acute kidney injury [22,23].
Consistent with its dual localization, Sirt1 can acts on different targets both in nucleus and cytoplasm. In DKD mice Sirt1 reduces oxidative stress injury, while overexpression of Sirt7 reduces inflammation and improves renal function [24,25].
Sirt1 regulates autophagy and delays the progression of AKI by deacetylating of the autophagy regulator Beclin1 [26].
Sirtuin family regulates mesangial cell proliferation and hypertrophy, podocytes apoptosis, oxidative stress, fibrosis, proximal tubular glucose metabolism, and renal tubular injury in patients with DKD.
SIRT4 has been shown to play a crucial role in insulin secretion and glucose homeostasis, as demonstrated by the development of glucose intolerance and insulin resistance in SIRT4-deficient mice [27].
SIRTs are also involved in obesity-related kidney disease. In adipose tissue SIRT1 suppresses adipocyte differentiation, lipid accumulation and inflammation by inhibiting PPAR and NF-κβ [28,29]. Moreover it regulates adiponectin gene expression and this is worthy of attention because adiponectin promotes functional recovery after podocyte ablation. [30]
SIRT5 was initially described as an urea cycle regulating agent through the direct activation of carbamoyl phosphate synthetase 1 [31]. Subsequent studies have revealed that it also exhibits demalonylase and desuccinylase activities, through which it controls ketogenesis [32,33].
Sirt 3, by improving mitochondrial functions, plays a role against acute kidney injury. Lack of Sirt3 further exacerbates the pathological damage of AKI, while its overexpression alleviates mitochondrial damage in AKI [34].
In hypertensive renal disease, an increase in the number of DNA double-strand breaks (DSBs) is accompanied by a decrease in Sirt6 expression [35]. Sirt 1 also regulates blood pressure by targeting endothelial nitric oxide synthase and Angiotensin II Type 1 receptors: a defective eNOS due to endothelial dysfunction contributes to kidney and cardiovascular disease [36]. Sirt 1 expression also protects from oxidative stress and vascular calcification in CKD [37,38]. The same sirtuin also regulates the activity and expression of hypoxia-inducible factor-2α (HIF-2α), which is responsible for the hypoxic induction of erythropoietin by renal cells [39].
Regulation of the activity of sirtuins has been shown to delay renal disease progression in both cellular and animal models [40] and this should depend on their influence on fibrosis onset. SIRT1 has protective effects against fibrosis [41], Sirt2 contributes to the activation and proliferation of renal fibroblasts, therefore its blocking attenuates the development of renal fibrosis and may have therapeutic potential for the treatment of CKD [42]. Sirt3 is closely associated with the remission of renal fibrosis through deacetylation of mitochondrial proteins [43]. Sirt 6 is expressed in the kidney and its deficiency in murine models is related with renal hypertrophy and glomerular enlargement. Sirt 6 deletion induces podocyte injury and cellular loss with consequent proteinuria. Progressively, SIRT 6 deficiency causes renal fibrosis [44]. in podocytes and proximal epithelial tubular cells. [45,46] Overexpression of Sirt6 delays the progression of renal interstitial fibrosis in CKD through targeting HIPK-2 [47].
Moreover, Sirt3 inhibits renal calcium oxalate crystal formation by promoting macrophage M2 polarisation via the deacetylation of FOXO1 [48] and protects from hyperlipidemia-related renal injury [49].
In animal models of autosomal-dominant polycystic kidney disease (ADPKD), Sirtuin 1 inhibition delays cyst formation. In ADPKD patients compared to healthy subjects Kurtgoz and coworkers found that urine SIRT1 levels were significantly lower. Also serum SIRT1 levels of ADPKD patients were higher than control cases, but the difference wasn’t statistically significant. These findings suggest an impaired SIRT1 metabolism in ADPKD patients which might play a role in cysts development [50].
SIRT2 is involved in cilia pathophysiology and centrosome function that on their turns are involved in polycystic kidney disease and in ciliopathy-associated disease progression [51]. Moreover, by inhibiting caspase-3 and ROS generation, it affects apoptosis and oxidative stress [52].
In murine models of caloric restriction, Kume and coworkers [53] demonstrated a beneficial mitochondria autophagy: in their model Sirt 1 can deacetylate different substrates, including the transcription factor Forkhead box O3a (FOXO3a) that, on its turn, promotes, under hypoxic conditions, the expression of Bnip3, a gene that allows autophagy and p27, a cyclin-dependent kinase inhibitor that exerts antiapoptotic effects in the kidney.
The preminent mitochondrial localization of sirtuins is interesting: mitochondria are deeply involved in renal physiology and pathophysiology and their dysfunction is actually recognized as a key factor for renal diseases, both inherited and acquired. Mitochondrial dysfunction might cause both glomerular and tubular diseases. Cystic renal diseases have also been associated with mitochondria by different Authors and a close relationship between mitochondrial dysfunction and CKD progression is also demonstrated. [54]
Sirtuins and Cardiovascular Diseases
Cardiovascular diseases (CVDs), principally ischemic heart disease (IHD) and stroke, are the leading cause of global mortality and a major contributor to disability. The total number of cardiovascular events almost doubled from 1990 to 2019 [54]. Notably, an increasing number of studies linked SIRTs with different CVDs. SIRTs affect the production of mitochondrial reactive oxygen species (ROS) by modulating mitochondrial function and increasing endothelial dysfunction, leading to an increased progression of atherosclerotic lesions [55]. The imbalance of SIRTs levels may increase the vulnerability to CVDs, including heart failure (HF), atherosclerosis, ischaemic heart disease, hypertrophic heart disease and metabolic disease.
It seems that SIRT1 protects the heart from hypertrophic stimulation, oxidative stress damage, ROS accumulation and apoptotic damage. It also could avoid ischemic/reperfusion (I/R) injury, as well as SIRT 3 and SIRT 6 [56,57,58]; SIRT3 exerts a cardioprotective role by protecting mitochondrial function; evidences suggest that activation of SIRT6 may be a therapeutic tool to treat atherosclerosis.
The role of SIRTs in atherosclerosis is relatively clear, with main effects in regulating LDL cholesterol levels, macrophages, foam cells, and endothelial function through various factors and signaling pathways; SIRT 1, SIRT3 and SIRT 6 are the sirtuins involved in protecting against atherosclerosis and cardiac hypertrophy [59,60,61]. They also exhibit a protecting role towards diabetic cardiomyopathy. Unfortunately, not all SIRTs activities are beneficial. For example, SIRT2 is destructive in I/R injury (its downregulation is protective against I/R injury [62]) and SIRT4 is detrimental towards heart hypertrophy and fibrosis [63].
SIRTs are involved in pathophysiological mechanisms of HFpEF (heart failure with preserved ejection fraction) [64]. As summarized by European Society of Cardiology [65], it is the most significant subtype of HF, and it is primarily characterized by left ventricular diastolic dysfunction (LVDD).
SIRT family has recently been found to be associated with HFpEF development through different signaling pathways such as the eEF2K/eEF2 pathway, the SIRT1/transmembrane BAX inhibitor motif, the Sirt3/MnSOD pathway, and the AMPK/PGC-1α pathway, causing endoplasmic reticulum stress, apoptosis, mitophagy, oxidative stress, and mitochondrial dysfunction [66]. SIRT4, SIRT5, and SIRT7, instead, are downregulated in HF.
Sirtuins and Cardio-Renal Diseases
It is well known that fibrosis is also involved in the onset of HF and it is also recognized as the linkage mechanism between heart and kidney in the development of cardio-renal diseases. Fibrosis arises from the proliferation of fibroblasts and their differentiation to myofibroblasts and subsequent deposition of extracellular matrix (ECM). Another important factor involved in heart and kidney fibrosis is endothelial-to-mesenchymal transition (EndMT) [67,68] that seems to be an important mechanism leading to glomerular sclerosis in DKD [69]. Several studies shown that TGF-β, through activation of several signaling pathways (TGF/Smad, Erk, Akt), is the main stimulator and modulator of EndMT [70]. According to previous studies, SIRT1 and SIRT3 (both decreased in TGF-β - induced EndMT) seem to be TGF-β inhibiting factors [71,72] so their upregulation could be a chance to attenuate both cardiac and renal fibrosis thus mitigating cardio-renal syndromes, in which fibrosis plays an important role [73].
Resveratrol and Sirtuins Agonists in Cardio-Renal Diseases
After this brief dissertation, it is clear how sirtuins deserve our attention for their deep involvement in metabolic and pathophysiological ways of kidney and heart disease so these enzymes could be hypothesized as therapeutical targets. Different natural SIRT1 agonists showed renoprotective effects in animal models [74] and among these Resveratrol (RSV) and other phenolic compounds have been widely investigated with interesting and positive results.
Polyphenols, a diverse group of phytochemicals found in various fruits, vegetables, teas, and wines, have garnered significant attention in recent years for their potential health benefits, particularly in the context of cardiorenal diseases. These compounds have been shown to exhibit antioxidant, anti-inflammatory, and vasodilatory effects, which may be beneficial for cardiovascular and renal health.
RSV has been proven to be useful in treating different chronic diseases through enhancing mitochondrial quality [75] which is altered in several chronic diseases, such as Alzheimer’s disease (AD), Parkinson’s disease (PD), cardiovascular disease, obesity, cancer and various forms of CKD (including DKD, IgA kidney disease, membranous nephropathy and polycystic kidney disease) [76]. RSV seems to be able to regulate mitochondrial dynamics, mitophagy, endogenous mitochondrial apoptosis, oxidative stress, mitochondrial membrane homeostasis, and respiratory chain function and mitochondrial quality control thus contributing to delay the onset of the above mentioned chronic diseases [75]. SIRT1 activated by RSV attenuates ISO-induced cardiac dysfunction and fibrosis by regulating EndMT in vivo [77]. SIRT1 overexpression suppressed the development of TGF-β1-induced EndMT in vitro. In this study it was also shown that P-Smad2/3 expression was increased in ISO-induced cardiac fibrosis, but was attenuated by RSV-activated SIRT1 (perhaps due to SIRT1’s ability to inhibit the nuclear translocation of Smad2/3).
Also in CKD patients, Resveratrol exerts beneficial, promising effects by modulating SIRT1 levels, oxidative stress and inflammation.
Pharmacologycal agents, such as SRT1720, a SIRT 1 activator, showed renal antifibrotic effects by reducing oxidative stress. [78]
Physical exercise (both as single sessions and training) activates SIRT1 which, on its turn, activates mitochondrial oxidative function. [79]
Sirtuins agonists (represented by NAD+), have gradually emerged as new treatments for heart failure. By modulating metabolism, maintaining redox homeostasis, and regulating immune responses, Sirtuins improve heart failure symptoms and prognosis.
More recently, Liraglutide, a novel antidiabetic agent, showed to influence SIRT1 expression in stroke patients and this finding confirms that sirtuins are worthy of investigation to ameliorate treatment and prognosis of CKD patients, independently of the cause of primary kidney disease. [80]
SGLT2 inhibitors have been demonstrated to upregulate SIRT3 expression. SGLT2 inhibition suppressed epithelial to mesenchymal transition and fibrogenesis in kidney proximal tubules; this effect of SGLT2 inhibition was associated with its ability to restore SIRT3 expression and glycolysis [81]. This interesting pharmacological activity could be a potential therapeutical target to prevent cardiac remodeling. Moreover, SGLT2 inhibitors activate SIRT1/PGC-1α/FGF21 pathway through their ability to induce a fasting-like metabolic and transcriptional paradigm [82]. The cardioprotective effects of SGLT2 inhibitors may also be related to this particular signaling [83].
Conclusions and Future Directions
Future research is obviously needed to clarify the role of these molecules and to enhance their potential therapeutical role in heart and kidney diseases. But, on our opinion, this topic is worthy of more attention because Resveratrol or other Sirtuins agonists’ administration could become an useful and safe tool in cardiorenal diseases.
In diabetic rats, the intergenerational treatment with oral resveratrol improved the functions of the heart, kidney, and brain. The more interesting finding is that resveratrol treatment increases the second and third generations' resistance to neurobehavioral changes, diabetes, and -associated cardio-renal dysfunction. [84].
It is really interesting to hypothesize similar studies in humans to prove the efficacy and safety of this natural compound.
A systematic review and meta-analysis analyzed multiple studies on polyphenol intake and kidney health. The review concluded that higher dietary polyphenol intake was associated with a lower risk of chronic kidney disease (CKD) and improved renal function markers among the general population [85] This aligns with findings from another study [86] which demonstrated that higher consumption of flavonoid-rich foods was inversely related to the incidence of CKD in older adults.
In addition to their effects on blood pressure and kidney function, the anti-inflammatory properties of polyphenols have been shown to play a crucial role in protecting against the progression of cardiorenal diseases. A recent study [87] explored the impact of berry polyphenols on inflammatory markers in patients with chronic heart failure. The findings suggested that berry supplementation led to a significant reduction in inflammatory cytokines and improved cardiac function, highlighting the protective role of polyphenols in cardiovascular health [88]
In summary, emerging research underlines the potential of polyphenols as a promising dietary intervention for the prevention and management of cardiorenal diseases. Their beneficial effects on blood pressure, kidney function, lipid profiles, and inflammation make them a valuable area of study for improving cardiovascular and renal health outcomes. Continued exploration of polyphenol-rich diets in diverse populations will further elucidate their role in promoting cardiorenal health.
References
- Carollo, C.; Urso, C.; Lo Presti, R.; Caimi, G. Sirtuins and Chronic Obstructive Pulmonary Disease. Food and Nutrition Sciences 2018, 9, 1254–1260. [Google Scholar] [CrossRef]
- Carollo, C.; Firenze, A.; Caimi, G. Sirtuins and Aging: Is there a Role for Resveratrol? International Journal of Advanced Nutritional and Health Science 2016, 4, 203–211. [Google Scholar] [CrossRef]
- Michishita, E.; Park, J.Y.; Burneskis, J.M.; Barrett, J.C.; Horikawa, I. Evolutionarily conserved and non conserved cellular localizations and functions of human SIRT proteins. Mol Biol Cell 2005, 16, 4623–4635. [Google Scholar] [CrossRef] [PubMed]
- Balaban, R.S.; Nemoto, S.; Finkel, T. Mitochondria, oxidants, and aging. Cell 2005, 120, 483–495. [Google Scholar] [CrossRef] [PubMed]
- Kidney Disease: Improving Global Outcomes (KDIGO) CKD Work Group 2024. Kidney International 2024, 105 (Suppl. 4S), S117–S314. [CrossRef]
- Abdel Kader, K. Symptoms with or because of Kidney Failure? Clin J Am Soc Nephrol. 2022, 17, 475–477. [Google Scholar] [CrossRef]
- US Renal Data System 2023.
- Nitta, K.; Okada, K.; Yanai, M.; Takahashi, S. Aging and chronic kidney disease. Kidney Blood Press Res. 2013, 38, 109–120. [Google Scholar] [CrossRef]
- Stenvinkel, P.; Larsson, T.E. Chronic kidney disease: A clinical model of premature aging. Am J Kidney Dis. 2013, 62, 339–351. [Google Scholar] [CrossRef]
- Kooman, J.P.; van der Sande, F.M.; Leunissen, K.M. Kidney disease and aging: A reciprocal relation. Exp Gerontol. 2017, 87, 156–159. [Google Scholar] [CrossRef]
- Morigi, M.; Perico, L.; Benigni, A. Sirtuins in Renal Health and Disease. J Am Soc Nephrol 2018, 29, 1799–1809. [Google Scholar] [CrossRef]
- Jung, Y.J.; Lee, A.S.; Nguyen-Thanh, T.; Kim, D.; Kang, K.P.; Lee, S.; et al. SIRT2 Regulates LPS-Induced Renal Tubular CXCL2 and CCL2 Expression. J Am Soc Nephrol 2015, 26, 1549–1560. [Google Scholar] [CrossRef] [PubMed]
- Michishita, E.; Park, J.Y.; Burneskis, J.M.; Barrett, J.C.; Horikawa, I. Evolutionarily conserved and nonconserved cellular localizations and functions of human SIRT proteins. Mol Biol Cell. 2005, 16, 4623–4635. [Google Scholar] [CrossRef]
- Koyama, T.; Kume, S.; Koya, D.; Araki, S.; Isshiki, K.; Chin-Kanasaki, M.; et al. SIRT3 Attenuates Palmitate-Induced ROS Production and Inflammation in Proximal Tubular Cells. Free Radic Biol Med 2011, 51, 1258–1267. [Google Scholar] [CrossRef]
- Chiba, T.; Peasley, K.D.; Cargill, K.R.; Maringer K v Bharathi, S.S.; Mukherjee, E.; et al. Sirtuin 5 Regulates Proximal Tubule Fatty Acid Oxidation to Protect Against AKI. J Am Soc Nephrol 2019, 30, 2384–2398. [Google Scholar] [CrossRef] [PubMed]
- Miyasato, Y.; Yoshizawa, T.; Sato, Y.; Nakagawa, T.; Miyasato, Y.; Kakizoe, Y.; et al. Sirtuin 7 Deficiency Ameliorates Cisplatin-Induced Acute Kidney Injury Through Regulation of the Inflammatory Response. Sci Rep 2018, 8, 5927. [Google Scholar] [CrossRef]
- Kitada, M.; Kume, S.; Koya, D. Role of sirtuins in kidney disease. Curr Opin Nephrol Hypertens. 2014, 23, 75–79. [Google Scholar] [CrossRef] [PubMed]
- Chung, W.K.; Erion, K.; Florez, J.C.; Hattersley, A.T.; Hivert, M.F.; Lee, C.G.; McCarthy, M.I.; Nolan, J.J.; Norris, J.M.; Pearson, E.R.; Philipson, L.; McElvaine, A.T.; Cefalu, W.T.; Rich, S.S.; Franks, P.W. Precision Medicine in Diabetes: A Consensus Report From the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD). Diabetes Care. 2020, 43, 1617–1635. [Google Scholar] [CrossRef]
- Zhong, Y.; Lee, K.; He, J.C. SIRT1 is a potential drug target for treatment of diabetic kidney disease. Frontiers in Endocrinology 2018, 9, 624. [Google Scholar] [CrossRef]
- Dong YJLiu, N.; Xiao, Z.; Sun, T.; Wu, S.H.; Sun, W.X.; Xu, Z.G.; Yuan, H. Renal protective effect of Sirtuin 1. J Diabetes Res. 2014, 2014, 843786. [Google Scholar]
- Bian, C.; Ren, H. Sirtuin Family and Diabetic Kidney Disease. Front Endocrinol 2022, 13, 901066. [Google Scholar] [CrossRef]
- Hasegawa, K.; Wakino, S.; Simic, P.; Sakamaki, Y.; Minakuchi, H.; Fujimura, K.; Hosoya, K.; Komatsu, M.; Kaneko, Y.; Kanda, T.; Kubota, E.; Tokuyama, H.; Hayashi, K.; Guarente, L.; Itoh, H. Renal tubular SIRT1 attenuates diabetic albuminuria by epigenetically suppressing Claudin-1 overexpression in podocytes. Nat Med 2013, 19, 1496–1504. [Google Scholar] [CrossRef] [PubMed]
- Gao, R.; Chen, J.; Hu, Y.; Li, Z.; Wang, S.; Shetty, S.; Fu, J. SIRT1 Deletion leads to enhanced inflammation and aggravates endotoxin -induced acute kidney injury. PLoS ONE, 2014, 9, e98909. [Google Scholar] [CrossRef] [PubMed]
- Li, S.; Lin, Z.; Xiao, H.; Xu, Z.; Li, C.; Zeng, J.; Xie, X.; Deng, L.; Huang, H. Fyn deficiency inhibits oxidative stress by decreasing c-Cbl-mediated ubiquitination of Sirt1 to attenuate diabetic renal fibrosis. Metabolism 2023, 139, 155378. [Google Scholar] [CrossRef]
- Li, X.; Liu, J.; Lu, L.; Huang, T.; Hou, W.; Wang, F.; Yu, L.; Wu, F.; Qi, J.; Chen, X.; et al. Sirt7 associates with ELK1 to participate in hyperglycemia memory and diabetic Nephropathy via modulation of DAPK3 expression and endothelial inflammation. Transl Res. 2022, 247, 99–116. [Google Scholar] [CrossRef] [PubMed]
- Deng, Z.; Sun, M.; Wu, J.; Fang, H.; Cai, S.; An, S.; Huang, Q.; Chen, Z.; Wu, C.; Zhou, Z.; et al. SIRT1 attenuates sepsis-induced acute kidney injury via Beclin1 deacetylation-mediated autophagy activation. Cell Death Dis. 2021, 12, 217. [Google Scholar] [CrossRef] [PubMed]
- Anderson, K.A.; Huynh, F.K.; Fisher-Wellman, K.; Stuart, J.D.; Peterson, B.S.; Douros, J.D. SIRT4 Is a lysine deacylase that controls leucine metabolism and insulin secretion. Cell Metab 2017, 25, 838–855.e15. [Google Scholar] [CrossRef]
- Picard, F.; Kurtev, M.; Chung, N.; Topark-Ngarm, A.; senawong, T.; Machado De Oliveira, R.; et al. SIRT1 promotes fat mobilization in white adipocytes by repressing PPAR gamma. Nature 2004, 429, 771–776. [Google Scholar] [CrossRef]
- Gillum, M.P.; Kotas, M.E.; Erion, D.M.; Kursawe, R.; Chatterjee, P.; Nead, K.T.; et al. SIRT1 regulates adipose tissue inflammation. Diabetes 2011, 60, 3100–3102. [Google Scholar] [CrossRef]
- Rutkowski, J.M.; Wang, Z.V.; Park, A.S.; Zhang, J.; Zhang, D.; Hu, M.C.; et al. Adiponectin promotes functional recovey after podocyte ablation. JASN 2013, 24, 268–282. [Google Scholar] [CrossRef]
- Nakagawa, T.; Lomb, D.J.; Haigis, M.C.; Guarente, L. SIRT5 deacetylates carbamoyl phosphate synthetase 1 and regulates the urea cycle. Cell 2009, 137, 560–570. [Google Scholar] [CrossRef]
- Rardin, M.J.; He, W.; Nishida, Y.; Newman, J.C.; Carrico, C.; Danielson, S.R. SIRT5 regulates the mitochondrial lysine succinylome and metabolic networks. Cell Metab 2013, 18, 920–933. [Google Scholar] [CrossRef]
- Du, J.; Zhou, Y.; Su, X.; Yu, J.J.; Khan, S.; Jiang, H. Sirt5 is a NAD-dependent protein lysine demalonylase and desuccinylase. Science 2011, 334, 806–809. [Google Scholar] [CrossRef] [PubMed]
- Jian, Y.; Yang, Y.; Cheng, L.; Yang, X.; Liu, H.; Li, W.; Wan, Y.; Yang, D. Sirt3 mitigates LPS-induced mitochondrial damage in renal tubular epithelial cells by deacetylating YME1L1. Cell Prolif. 2023, 56, e13362. [Google Scholar] [CrossRef] [PubMed]
- Zhong, Y.; Lee, K.; He, J.C. SIRT1 Is a Potential Drug Target for Treatment of Diabetic Kidney Disease. Front Endocrinol 2018, 9, 624. [Google Scholar] [CrossRef]
- Yu, W.; Fu Yc Chen, C.J.; Wang, X.; Wang, W. SIRT1, a novel target to prevent atherosclerosis. J Cell Biochem 2009, 108, 10–13. [Google Scholar] [CrossRef]
- Yan, J.; Wang, J.; He, J.C.; Zhong, Y. Sirtuin 1 in Chronic Kidney Disease and Therapeutic Potential of Targeting Sirtuin 1. Front Endocrinol 2022, 13, 917773. [Google Scholar] [CrossRef] [PubMed]
- Takemura, A.; Iijima, K.; Ota, H.; Son, B.K.; Ito, Y.; Ogawa, S.; et al. Sirtuin 1 Retards Hyperphosphatemia-Induced Calcification of Vascular Smooth Muscle Cells. Arterioscler Thromb Vasc Biol 2011, 31, 2054–2062. [Google Scholar] [CrossRef] [PubMed]
- Dioum, E.M.; Chen, R.; Alexander, M.S.; Zhang, Q.; Hogg, R.T.; Gerard, R.D.; et al. : Regulation of hypoxia-inducible factor 2alpha signaling by the stress-responsive deacetylase sirtuin 1. Science 2009, 324, 1289–1293. [Google Scholar] [CrossRef]
- Jin, Q.; Ma, F.; Liu, T. Sirtuins in kidney diseases: Potential mechanism and therapeutic targets. Cell Commun Signal 2024, 22, 114. [Google Scholar] [CrossRef]
- Vasko, R.; Xavier, S.; Chen, J.; Lin, C.H.; Ratliff, B.; Rabadi, M.; et al. Endothelial Sirtuin 1 Deficiency Perpetrates Nephrosclerosis Through Downregulation of Matrix Metalloproteinase-14: Relevance to Fibrosis of Vascular Senescence. J Am Soc Nephrol JASN 2014, 25, 276–291. [Google Scholar] [CrossRef]
- Ponnusamy, M.; Zhou, X.; Yan, Y.; Tang, J.; Tolbert, E.; Zhao, T.C.; Gong, R.; Zhuang, S. Blocking sirtuin 1 and 2 inhibits renal interstitial fibroblast activation and attenuates renal interstitial fibrosis in obstructive Nephropathy. J Pharmacol Exp Ther. 2014, 350, 243–256. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Wen, P.; Luo, J.; Ding, H.; Cao, H.; He, W.; Zen, K.; Zhou, Y.; Yang, J.; Jiang, L. Sirtuin 3 regulates mitochondrial protein acetylation and metabolism in tubular epithelial cells during renal fibrosis. Cell Death Dis. 2021, 12, 847. [Google Scholar] [CrossRef]
- Huang, W.; Liu, H.; Zhu, S.; Woodson, M.; Liu, R.; Tilton, R.G.; Miller, J.D.; Zhang, W. Sirt6 deficiency results in progression of glomerular injury in the kidney. Aging 2017, 9, 1069–1081. [Google Scholar] [CrossRef] [PubMed]
- Huang, W.; Liu, H.; Zhu, S.; Woodson, M.; Liu, R.; Tilton, R.G.; et al. Sirt6 Deficiency Results in Progression of Glomerular Injury in the Kidney. Aging 2017, 9, 1069–1083. [Google Scholar] [CrossRef] [PubMed]
- Cai, J.; Liu, Z.; Huang, X.; Shu, S.; Hu, X.; Zheng, M.; et al. The Deacetylase Sirtuin 6 Protects Against Kidney Fibrosis by Epigenetically Blocking β-Catenin Target Gene Expression. Kidney Int 2020, 97, 106–118. [Google Scholar] [CrossRef]
- Li, X.; Li, W.; Zhang, Z.; Wang, W.; Huang, H. SIRT6 overexpression retards renal interstitial fibrosis through targeting HIPK2 in chronic Kidney Disease. Front Pharmacol. 2022, 13, 1007168. [Google Scholar] [CrossRef]
- Xi, J.; Chen, Y.; Jing, J.; Zhang, Y.; Liang, C.; Hao, Z.; Zhang, L. Sirtuin 3 suppresses the formation of renal calcium oxalate crystals through promoting M2 polarization of macrophages. J Cell Physiol. 2019, 234, 11463–11473. [Google Scholar] [CrossRef]
- Chen, H.-H.; Zhang, Y.-X.; Lv, J.-L.; Liu, Y.-Y.; Guo, J.-Y.; Zhao, L.; Nan, Y.-X.; Wu, Q.-J.; Zhao, Y.-H. Role of sirtuins in metabolic disease-related renal injury. Biomedicine & Pharmacotherapy 2023, 161. [Google Scholar]
- Ozkan Kurtgoz, P.; Karakose, S.; Cetinkaya, C.D.; et al. Evaluation of sirtuin 1 (SIRT1) levels in autosomal dominant polycystic kidney disease. Int Urol Nephrol 2022, 54, 131–135. [Google Scholar] [CrossRef]
- Zhou, X.; Fan, L.X.; Sweeney, W.E.; Denu, J.M.; Avner, E.D.; Li, x. Sirtuin 1 inhibition delays cyst formation in autosomal-dominant polycystic kidney disease. J Clin Invest 2013, 123, 3084–3098. [Google Scholar] [CrossRef]
- Nie, H.; Hong, Y.; Lu, X.; Zhang, J.; Chen, H.; Li, Y.; et al. SIRT2 mediates oxidative stress-induced apoptosis of differentiated PC12 cells. Neuroreport 2014, 25, 838–842. [Google Scholar] [CrossRef] [PubMed]
- Kume, S.; Uzu, T.; Horiike, K.; Chin-Kanasaki, M.; Isshiki, K.; Araki, S.; Sugimoto, T.; Haneda, M.; Kashiwagi, A.; Koya, D. Calorie restriction enhances cell adaption to hypoxia through SIRT1-dependent mitochondrial autophagy in mouse aged kidney. J Clin Invest 2010, 120, 1043–1055. [Google Scholar] [CrossRef] [PubMed]
- Guo, Y.; Che, R.; Wang, P.; Zhang, A. Mitochondrial dysfunction in the pathophysiology of renal diseases. Am J Physiol Renal Physiol. 2024, 326, F768–F779. [Google Scholar] [CrossRef] [PubMed]
- Roth, G.A.; Mensah, G.A.; Johnson, C.O.; et al. Global burden of cardiovascular diseases and risk factors, 1990-2019: Update from the GBD 2019 study. J. Am. Coll. Cardiol. 2020, 76, 2982–3021. [Google Scholar] [CrossRef]
- Hsu, C.P.; Zhai, P.; Yamamoto, T.; Maejima, Y.; Matsushima, S.; Hariharan, N.; Shao, D.; Takagi, H.; Oka, S.; Sadoshima, J. Silent information regulator 1 protects the heart from ischemia/reperfusion. Circulation 2010, 122, 2170–2182. [Google Scholar] [CrossRef]
- Porter, G.A.; Urciuoli, W.R.; Brookes, P.S.; Nadtochiy, S.M. SIRT3 deficiency exacerbates ischemia-reperfusion injury: Implication for aged hearts. Am J Physiol Heart Circ Physiol 2014, 306, H1602–H1609. [Google Scholar] [CrossRef]
- Wang, X.X.; Wang, X.L.; Tong, M.M.; et al. SIRT6 protects cardiomyocytes against ischemia/reperfusion injury by augmenting FoxO3α-dependent antioxidant defense mechanisms. Basic Res. Cardiol. 2016, 111, 13. [Google Scholar] [CrossRef]
- Alcendor, R.R.; Gao, S.; Zhai, P.; Zablocki, D.; Holle, E.; Yu, X.; Tian, B.; Wagner, T.; Vatner, S.F.; Sadoshima, J. Sirt1 regulates aging and resistance to oxidative stress in the heart. Circ Res 2007, 100, 1512–1521. [Google Scholar] [CrossRef]
- Sundaresan, N.R.; Gupta, M.; Kim, G.; Rajamohan, S.B.; Isbatan, A.; Gupta, M.P. Sirt3 blocks the cardiac hypertrophic response by augmenting Foxo3a-dependent antioxidant defense mechanisms in mice. J Clin Invest 2009, 119, 2758–2771. [Google Scholar] [CrossRef]
- Sundaresan, N.R.; Vasudevan, P.; Zhong, L.; Kim, G.; Samant, S.; Parekh, V.; Pillai, V.B.; Ravindra, P.V.; Gupta, M.; Jeevanandam, V.; Cunningham, J.M.; Deng, C.X.; Lombard, D.B.; Mostoslavsky, R.; Gupta, M.P. The sirtuin SIRT6 blocks IGF-Akt signaling and development of cardiac hypertrophy by targeting c-Jun. Nat Med 2012, 18, 1643–1650. [Google Scholar] [CrossRef]
- Lynn, E.G.; McLeod, C.J.; Gordon, J.P.; Bao, J.; Sack, M.N. SIRT2 is a negative regulator of anoxia-reoxygenation tolerance via regulation of 14-3-3 zeta and BAD in H9c2 cells. FEBS Lett 2008, 582, 2857–2862. [Google Scholar] [CrossRef]
- Liu, Y.-P.; Wen, R.; Liu, C.-F.; Zhang, T.-N.; Yang, N. Cellular and molecular biology of sirtuins in cardiovascular disease. Biomedicine & Pharmacotherapy 2023, 164, 114931. [Google Scholar]
- Lu, Y.; Li, Y.; Xie, Y.; Bu, J.; Yuan, R.; Zhang, X. Exploring Sirtuins: New Frontiers in Managing Heart Failure with Preserved Ejection Fraction. International Journal of Molecular Sciences. 2024, 25, 7740. [Google Scholar] [CrossRef] [PubMed]
- McDonagh, T.A.; Metra, M.; Adamo, M.; Gardner, R.S.; Baumbach, A.; Böhm, M.; Burri, H.; Butler, J.; Čelutkienė, J.; Chioncel, O.; et al. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: Developed by the Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC) with the special contribution of the Heart Failure Association (HFA) of the ESC. Rev. Esp. Cardiol. (Engl. Ed.) 2022, 75, 523. [Google Scholar] [PubMed]
- Wu, Q.-J.; Zhang, T.-N.; Chen, H.-H.; Yu, X.-F.; Lv, J.-L.; Liu, Y.-Y.; Liu, Y.-S.; Zheng, G.; Zhao, J.-Q.; Wei, Y.-F.; et al. The sirtuin family in health and disease. Signal Transduct. Target. Ther. 2022, 7, 402. [Google Scholar] [PubMed]
- Zeisberg, E.M.; Tarnavski, O.; Zeisberg, M.; Dorfman, A.L.; McMullen, J.R.; Gustafsson, E.; Chandraker, A.; Yuan, X.; Pu, W.T.; Roberts, A.B.; Neilson, E.G.; Sayegh, M.H.; Izumo, S.; Kalluri, R. Endothelial-to-mesenchymal transition contributes to cardiac fibrosis. Nat Med 2007, 13, 952–961. [Google Scholar] [CrossRef]
- Zeisberg, E.M.; Potenta, S.E.; Sugimoto, H.; Zeisberg, M.; Kalluri, R. Fibroblasts in kidney fibrosis emerge via endothelial-to-mesenchymal transition. J Am Soc Nephrol 2008, 19, 2282–2287. [Google Scholar] [CrossRef]
- Kizu, A.; Medici, D.; Kalluri, R. Endothelial-mesenchymal transition as a novel mechanism for generating myofibroblasts during diabetic nephropathy. Am J Pathol 2009, 175, 1371–1373. [Google Scholar] [CrossRef]
- Pardali, E.; Sanchez-Duffhues, G.; Gomez-Puerto, M.C.; Ten Dijke, P. TGF-beta-Induced endothelial-mesenchymal transition in fibrotic diseases. Int. J. Mol. Sci. 2017, 18. [Google Scholar]
- Li, Z.; Wang, F.; Zha, S.; Cao, Q.; Sheng, J.; Chen, S. SIRT1 inhibits TGF-β-induced endothelial-mesenchymal transition in human endothelial cells with Smad4 deacetylation. J Cell Physiol 2018, 233, 9007–9014. [Google Scholar] [CrossRef]
- Lin, J.R.; Zheng, Y.J.; Zhang, Z.B.; Shen, W.L.; Li, X.D.; Wei, T.; Ruan, C.C.; Chen, X.H.; Zhu, D.L.; Gao, P.J. Suppression of Endothelial-to-Mesenchymal Transition by SIRT (Sirtuin) 3 Alleviated the Development of Hypertensive Renal Injury. Hypertension 2018, 72, 350–360. [Google Scholar] [CrossRef]
- Delgado-Valero, B.; Cachofeiro, V.; Martínez-Martínez, E. Fibrosis, the Bad Actor in Cardiorenal Syndromes: Mechanisms Involved. Cells 2021, 10, 1824. [Google Scholar] [CrossRef] [PubMed]
- Iside, C. Sirtuin 1 activation by natural phytochemicals: An overview. Front Pharmacol 2020, 11, 1225. [Google Scholar] [CrossRef]
- Tao, W.; Zhang, H.; Jiang, X.; Chen, N. Resveratrol combats chronic diseases through enhancing mitochondrial quality. Food Science and Human Wellness 2024, 13, 597–610. [Google Scholar] [CrossRef]
- Bhatia, D.; Capili, A.; Choi, M.E. Mitochondrial dysfunction in kidney injury, inflammation, and disease: Potential therapeutic approaches. Kidney Res Clin Pract. 2020, 39, 244–258. [Google Scholar] [CrossRef]
- Liu, Z.-H.; Zhang, Y.; Wang, X.; Fan, X.-F.; Zhang, Y.; Li, X.; Gong, Y.-S.; Han, L.-P. SIRT1 activation attenuates cardiac fibrosis by endothelial-to-mesenchymal transition. Biomedicine & Pharmacotherapy 2019, 118. [Google Scholar]
- Ren, Y.; Du, C.; Shi, Y.; Wei, J.; Wu, H.; Cui, H. . The Sirt 1 activator, SRT1720, attenuates renal fibrosis by inhibiting CTGF and oxidative stress. Int J Mol Med 2017, 39, 1317–1324. [Google Scholar] [CrossRef]
- Vargas-Ortiz, K.; Pérez-Vázquez, V.; Macías-Cervantes, M.H. Exercise and Sirtuins: A Way to Mitochondrial Health in Skeletal Muscle. Int J Mol Sci. 2019, 20, 2717. [Google Scholar] [CrossRef] [PubMed]
- Jeon, J.Y.; Choi, S.E.; Ha, E.S.; Lee, H.B.; Kim, T.H.; Han, S.J.; Kim, H.J.; Kim, D.J.; Kang, Y.; Lee, K.W. Role of liraglutide in brain repair promotion through Sirt1-mediated mitochondrial improvement in stroke. Int J Mol Med. 2019, 44, 1161–1171. [Google Scholar]
- Li, J.; Liu, H.; Takagi, S.; Nitta, K.; Kitada, M.; Srivastava, S.P.; Takagaki, Y.; Kanasaki, K.; Koya, D. Renal protective effects of empagliflozin via inhibition of EMT and aberrant glycolysis in proximal tubules. JCI Insight. 2020, 5, e129034. [Google Scholar] [CrossRef]
- Osataphan, S.; Macchi, C.; Singhal, G.; Chimene-Weiss, J.; Sales, V.; Kozuka, C.; Dreyfuss, J.M.; Pan, H.; Tangcharoenpaisan, Y.; Morningstar, J. SGLT2 inhibition reprograms systemic metabolism via FGF21-dependent and -independent mechanisms. JCI Insight. 2019, 4, e123130. [Google Scholar] [CrossRef] [PubMed]
- Packer, M. Cardioprotective effects of sirtuin-1 and its downstream effectors: Potential role in mediating the heart failure benefits of SGLT2 (Sodium-Glucose Cotransporter 2) inhibitors. Circ Heart Fail. 2020, 13, e007197. [Google Scholar] [CrossRef] [PubMed]
- Sharma, A.; Mukherjee, M.; Kumar, A.; Sharma, G.; Tabassum, F.; Akhtar, S.; Imam, M.T.; Saeed Almalki, Z.S. Preliminary investigation on impact of intergenerational treatment of resveratrol endorses the development of 'super-pups'. Life Sci 2023, 314, 121322. [Google Scholar] [CrossRef]
- Mirmiran, P.; Yuzbashian, E.; Rahbarinejad, P.; Asghari, G.; Azizi, F. Dietary Intakes of Total Polyphenol and Its Subclasses in Association with the Incidence of Chronic Kidney Diseases: A Prospective Population-based Cohort Study. Res. Sq. 2021. [Google Scholar] [CrossRef]
- Liu, P.; Peng, W.; Hu, F.; Li, G. Association between dietary intake of flavonoid and chronic kidney disease in US adults: Evidence from NHANES 2007-2008, 2009-2010, and 2017-2018. PLoS ONE 2024, 19, e0309026. [Google Scholar] [CrossRef]
- Arisi, T.O.P.; da Silva, D.S.; Stein, E.; Weschenfelder, C.; de Oliveira, P.C.; Marcadenti, A.; Lehnen, A.M.; Waclawovsky, G. Effects of cocoa consumption on cardiometabolic risk markers: Protocol for a systematic review and meta-analysis of randomized controlled trials. Nutrients 2024, 16, 1919. [Google Scholar] [CrossRef]
- Najjar, R.S.; Turner, C.G.; Wong, B.J.; Feresin, R.G. Berry-Derived Polyphenols in Cardiovascular Pathologies: Mechanisms of Disease and the Role of Diet and Sex. Nutrients 2021, 13, 387. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



