1. Introduction
Pre-operative imaging in autologous tissue transfers has developed in several ways to assess the patency of its vascular origin and the perforators. The inconsistency of the perforators among the patients is one of its drawbacks. Angiography is the standard method to detect the vascular pedicled. CT Angiography (CTA) and MR Angiography (MRA) are more favored these days due to their high resolution in visualizing the pedicled and surrounding anatomy. However, these procedures have a risk of allergy, high cost, and cannot be reproducible during intraoperative. [
1]. Recently, smartphone-based thermal imaging (SBTI) emerged to map the perforators with high sensitivity and specificity. The same device can be applied during intraoperative and post-operative monitoring [
2,
3].
In recent years, the superficial circumflex iliac artery (SCIA) flap has become popular as a modality of functional lymphedema reconstruction. The superficial lymphatic vessels attached to this flap can be transferred to the donor. The inconsistency of the two perforators in the SCIA flap can be confusing. The superficial vein can be used as a clue to design and harvest the flap with the superficial perforator to avoid lymph donor morbidity. Planning this flap is recommended using indocyanine green (ICG) lymphography [
4,
5]. However, ICG and its imaging device cannot be accommodated in some situations.
In this report, we present a functional lymphedema reconstruction treated by vascularized lymph node transfer. The donor was taken from the SCIP flap. We highlighted the use of SBTI and vein viewer as non-invasive imaging to assist in designing SCIP flaps by tracking superficial veins and perforators.
2. Case Reports
A 72-year-old woman was referred to our clinic due to edema in her right upper extremity. In the past two years, she experienced a worsened swelling from the hand to the brachial area. The swelling was followed by pain and heaviness, especially in the evening or after doing household chores. She also complained of episodes of lymphorrea three to four times a year. In 2014, the patient received a radical mastectomy of her right breast due to mammary carcinoma that was followed by radiation. She was diagnosed with hypertension and was treated with 5 mg of amlodipine in the same year.
During our examination, there was non-pitting edema from the right hand to the arm. We compare her right upper extremity in the midline with its contralateral in cm; hand: 20/19, wrist: 21/17, mid-forearm: 30/25, mid-arm: 35/30. Also, there was a scar on her right anterior torso due to mastectomy. The lymphoscintigraphy examination showed a total obstruction at her right upper extremity. We diagnosed the patient as secondary obstructive lymphedema stage 2 according to the International Society of Lymphology due to radical mastectomy and planned to do a functional lymphedema reconstruction with SCIA flap. Patient’s BMI was 30,8 kg/m2 with pedunculus abdomen. The clinical and scintigraphy picture are as follow
Figure 1.
Preoperative documentation of patient with difference of her bilateral upper extremities, mastectomy scar and lymphoscintigraphy.
Figure 1.
Preoperative documentation of patient with difference of her bilateral upper extremities, mastectomy scar and lymphoscintigraphy.
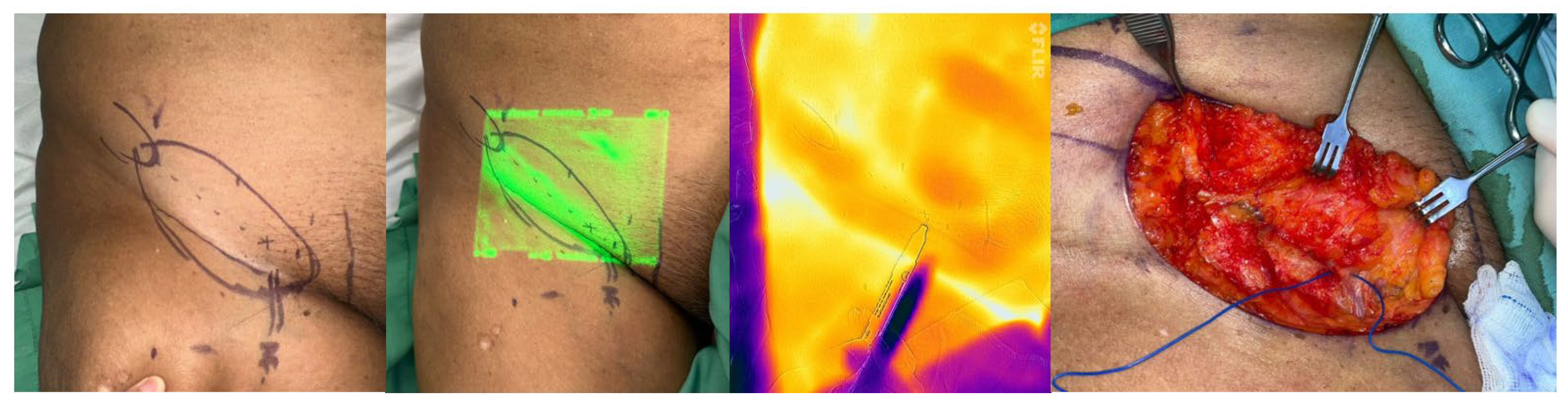
By retracting her abdomen to cranial, a line of flap axis was drawn from the anterior superior iliac spine (ASIS) to pubic tubercle. Pre-operative mapping was done with a vein viewer Vision2 to locate the superficial vein. A FLIR-ONE thermal cam image was used to locate the hot zone of perforators that needed to be incorporated into the design. Finally, an 11 cm x 4.5 cm flap was made. The flap was harvested from the distal and inferior above the fascia along the superficial vein to find the perforator. Then, the superior border of the flap was incised to have a complete dissection of the superficial circumflex iliac artery and vein. Two lymph nodes that were attached to the vessel were dissected, and their attachment was confirmed under the microscope. There were another couple of lymph nodes that were preserved to hinder donor site morbidity.
Figure 2.
(left) The design. (middle left) Connecting dots are drawings of superficial vein that confirm with vein viewer. (midle right) The course of the hot zone was mapped by FLIR ONE. (right) The finding of the perforator and superficial vein.
Figure 2.
(left) The design. (middle left) Connecting dots are drawings of superficial vein that confirm with vein viewer. (midle right) The course of the hot zone was mapped by FLIR ONE. (right) The finding of the perforator and superficial vein.
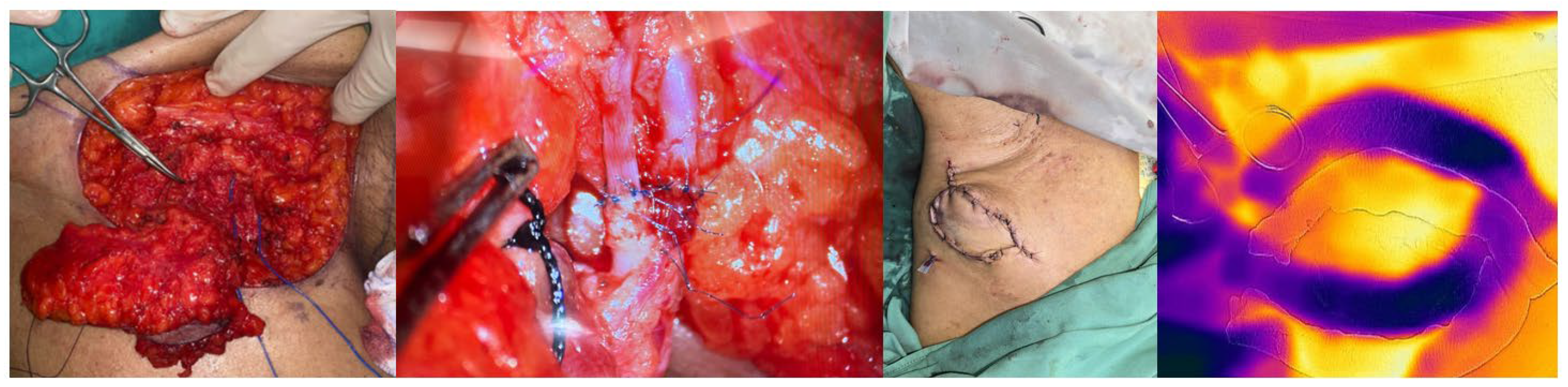
An incision was made in the old mastectomy scar, and the branch of the thoracodorsal artery and vein were dissected near the axilla as the recipient site. SCIA flap was transferred to the recipient. End-to-end anastomosis of the artery and vein was performed using 10.0 monofilament. Assessment of patency by Acland maneuvers was done under a microscope. The distal half of the skin was de-epithelized and buried at the anterior thorax, leaving a 7x4.5 cm skin island for flap monitoring. FLIR-ONE once again captured an image of the flap with a gauze border to assess its flow and as a baseline for monitoring. The donor site was closed primary. The patient was discharged from the hospital 5 days after the procedure.
Figure 3.
(left) SCIP flap complex (middle left) end-to-end anastomosis with the branch of thoracodorsal artery and vein (middle right) the 7x4.5 cm skin island (right) post-op monitoring with FLIR ONE.
Figure 3.
(left) SCIP flap complex (middle left) end-to-end anastomosis with the branch of thoracodorsal artery and vein (middle right) the 7x4.5 cm skin island (right) post-op monitoring with FLIR ONE.
Two months after the first procedure, the patient’s skin paddle was removed, preserving the vital subcutaneous tissue. The surrounding skin was dissected to close the wound. The patient was followed after six months of the first procedure. She has no complaints of heaviness, edema, lymphorrea, or pain. Her wound heals perfectly. The measurements in cm compared to the contralateral side were as follows: hand: 19/19, wrist: 17/17, mid-forearm: 25/25, mid-arm: 33/31
Figure 4.
(Left) bilateral upper extremity discrepancy. (right) Follow up wound after six months.
Figure 4.
(Left) bilateral upper extremity discrepancy. (right) Follow up wound after six months.
3. Discussion
SCIA flap was introduced by Koshima et al. in 2004, and then it became popular as a reconstruction modality in different body parts, variable size, and utility [
4,
6]. This flap also carries lymph channels in its subdermal tissue and connects with groups of lymph nodes in the superficial epigastric. Thus, the flap is ideal for corrective physiological lymphedema reconstruction, either as lymph-interposition-flap transfer or as a lymphatic system transfer procedure [
5].
Planning an SCIA flap can be done with CTA, MRA, or color-coded duplex sonography. Nowadays, high-frequency sonography is preferred because it is noninvasive and accurate [
7]. For lymphedema surgery, injection of ICG is added lateral to the flap to map the lymph vessels and nodes [
8,
9]. Although it is accurate, dye injection is at risk of allergic reaction. The device to capture the image is also expensive, and the procedure is time-consuming [
1,
2]. Our healthcare system did not cover its use. Therefore, prior to the surgery, we simulated the work of Yoshimatsu et al. in performing LYST, which might benefit our patient [
9].
STBI has become our primary choice in perforator flaps and free flaps procedures due to its price and convenience. Although Altiparmak et al. stated that the SCIA perforators are stable, we still incorporate the STBI to confirm its location [
4]. Its high sensitivity and specificity in mapping the perforator and flap monitoring make us prefer to do it in our center, as is shown in this case [
3]. The hot zone of the perforator was marked to ensure its location in mapping, confirming intra operative, and during monitoring to assess perfusion of the flap [
10,
11,
12].
Vein viewer or vein finder was one of the simple tools to map superficial venous networks using near-infrared light waves captured by deoxyhaemoglobin. It penetrates up to 15 mm from the skin surface, creating better visualization. Initially, the application of a vein finder is during phlebotomy or vein cannulation. With this tool, the subcutaneous vein pattern can be drawn. Clinically, the wavelength of certain vein viewers cannot penetrate in some patients with dark skin color, high body mass index, and skin marks [
13,
14,
15,
16]. Locating superficial vein can be an advantage in designing and elevating this flap [
4,
7].
The groin area has few connections between the superficial and deep lymphatic systems. Therefore, harvesting the superficial lymph network will not affect the deep network [
17]. The SCIA flap was harvested as part of the LYST procedure for functional reconstruction, as there was no visualized lymphatic vessel in the pre-operative examination [
9]. In the publication by Campos et al., there is also a lymph network in the superficial subcutaneous layer that can be use in the lymphedema treatment [
5]. A dissection above the Scarpa fascia, or in other publications stated as “deep fat saving elevation,” will include the superficial vein [
8,
18,
19]. Therefore, we feel it is essential to locate the superficial vein.
There was a range of difficulty in the harvesting of SCIA flaps in obese patients [
4]. The handheld Doppler may not be optimal in this kind of patient because we relied on the assistant to expose the groin area [
1]. Color-coded sonography may be useful in our patient, but again, it is operator-dependent [
1,
20]. The use of SBTI and portable vein viewer are much more convenience in our setting due to their size and easy to use on the mapping and confirming intra-operative. STBI is also much more convenient for monitoring.
The LYST procedure performed in our patient has given many benefits for the patient. The patient was experiencing no more episodes of lymphorrea with a rapid decline of circumferential measurements.
4. Conclusions
STBI and vein viewer can be a good combination in design and harvesting SCIA flap in obese patient for LYST procedure in place where no ICG tools available.
Acknowledgments
The write.rs would like to thank dr. Irra R. Widarda for the thorough discussion and simulation before the procedure and dr. Teguh Marfen Djajakusumah for lending the FLIR ONE thermal camera.
Abbreviations
CTA: Computed Tomography Angiography
ICG: indocyanine green
LYST: lymphatic system transfer
MRA: Magnetic Resonance Angiography
SCIA: superficial circumflex inguinal artery
SBTI: smartphone-based thermal image
References
- Nassar AH, Maselli AM, Manstein S, Shiah E, Slatnick BL, Dowlatshahi AS, et al. Comparison of Various Modalities Utilized for Preoperative Planning in Microsurgical Reconstructive Surgery. J Reconstr Microsurg. 2022;38(3):170–80. [CrossRef]
- Van Dieren L, Oubari H, Callens L, Berkane Y, Quisenaerts T, Saget F, et al. Smartphone-based thermography in flap surgery: A systematic review and meta-analysis of perforator identification. Heliyon [Internet]. 2024;10(6):e26806. Available from: . [CrossRef]
- Raheman FJ, Rojoa DM, Patel NG. Performance of infrared thermography and thermal stress test in perforator mapping and flap monitoring: A meta-analysis of diagnostic accuracy. J Plast Reconstr Aesthetic Surg [Internet]. 2021;74(9):2013–25. Available from: . [CrossRef]
- Altiparmak M, Cha HG, Hong JP, Suh HP. Superficial Circumflex Iliac Artery Perforator Flap as a Workhorse Flap: Systematic Review and Meta-analysis. J Reconstr Microsurg. 2020;36(8):600–5. [CrossRef]
- Sánchez JLC, Suominen S, Pons G, Al-Sakkaf AM, Lusetti IL, Sirota M, et al. Lymphatic patterns in the superficial circumflex iliac artery perforator flap. J Reconstr Microsurg. 2024; [CrossRef]
- Franchi A, Andrea F, Perozzo G, Tiengo C, Walber J, Parisato A, et al. SCIP / SIEA and PAP : The New Workhorse Flaps in Soft Tissue Reconstruction for All Body Regions. 2025;
- Schiltz D, Lenhard J, Klein S, Anker A, Lonic D, Heidekrueger PI, et al. Do-it-yourself preoperative high-resolution ultrasound-guided flap design of the superficial circumflex iliac artery perforator flap (Scip). J Clin Med. 2021;10(11). [CrossRef]
- Yoshimatsu H, Visconti G, Karakawa R, Hayashi A. Lymphatic System Transfer for Lymphedema Treatment: Transferring the Lymph Nodes with Their Lymphatic Vessels. Plast Reconstr Surg - Glob Open. 2020;8(4):1–4. [CrossRef]
- Yoshimatsu H, Cho MJ, Karakawa R, Okada A, Hayashi A, Fuse Y, et al. The role of lymphatic system transfer (LYST) for treatment of lymphedema: A long-term outcome study of SCIP flap incorporating the lymph nodes and the afferent lymphatic vessels. J Plast Reconstr Aesthetic Surg [Internet]. 2025;101:15–22. Available from: . [CrossRef]
- Hallock GG. Dynamic infrared thermography and smartphone thermal imaging as an adjunct for preoperative, intraoperative, and postoperative perforator free flap monitoring. Plast Aesthetic Res. 2019;6. [CrossRef]
- Yassin AM, Kanapathy M, Khater AME, El-Sabbagh AH, Shouman O, Nikkhah D, et al. Uses of Smartphone Thermal Imaging in Perforator Flaps as a Versatile Intraoperative Tool: The Microsurgeon’s Third Eye. JPRAS Open. 2023;38:98–108. [CrossRef]
- Fiedler LS, Lippert BM, Adrian L, Meyer T. Perfusion in Pedicled Skin Flaps: Initial Insights from Smartphone-Based Thermal Imaging Protocol. J Pers Med. 2024;14(7). [CrossRef]
- Francisco MD, Chen WF, Pan CT, Lin MC, Wen ZH, Liao CF, et al. Competitive real-time near infrared (Nir) vein finder imaging device to improve peripheral subcutaneous vein selection in venipuncture for clinical laboratory testing. Micromachines. 2021;12(4). [CrossRef]
- Caglar S, Buyukyilmaz F, Bakoglu I, Inal S, Salihoglu O. Efficacy of Vein Visualization Devices for Peripheral Intravenous Catheter Placement in Preterm Infants: A Randomized Clinical Trial. J Perinat Neonatal Nurs. 2019;33(1):61–7.
- Pan CT, Francisco MD, Yen CK, Wang SY, Shiue YL. Vein Pattern Locating Technology for Cannulation : A Review of the Low-Cost Vein Finder Prototypes. Sensors (Switzerland). 2019;19(16):1–17.
- Rothbart A, Yu P, Müller-Lobeck L, Spies CD, Wernecke KD, Nachtigall I. Peripheral intravenous cannulation with support of infrared laser vein viewing system in a pre-operation setting in pediatric patients Anesthesiology. BMC Res Notes. 2015;8(1):4–9.
- Hosomi K, Banda CH, Shiraishi M, Mitsui K, Ishiura R, Danno K, et al. Vascularized lymph node transfer with efferent lymphatico-lymphatic anastomosis for treatment of upper extremity lymphedema. Plast Aesthetic Res. 2023;10. [CrossRef]
- Myung Y, Yim S, Kim B kyu. A comparison of axial circumference between superficial circumflex iliac artery perforator flap and other workhorse flaps in dorsal foot reconstruction. J Plast Surg Hand Surg [Internet]. 2017;51(6):381–6. Available from:. [CrossRef]
- Fuse Y, Yoshimatsu H, Karakawa R, Yano T. Deep Fat Saving Elevation of the Superficial Circumflex Iliac Artery Perforator Flap. Med. 2022;58(5). [CrossRef]
- Zhu W, Yang Y, Jiang J, Zhu Q, Qi J, Qin B, et al. Value of the combination of a smartphone-compatible infrared camera and a hand-held doppler ultrasound in preoperative localization of perforators in flaps. Heliyon. 2023;9(6). [CrossRef]
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).