
Submitted:
18 February 2025
Posted:
19 February 2025
You are already at the latest version
Abstract
Thyroid cancer is a very common endocrine system malignancy. Nevertheless, a dearth of precise markers makes it challenging to apply precision medicine to thyroid cancer. The limitations to standard diagnosis technique (fine needle aspiration biopsy) such as indeterminate cases and inaccuracies in distinguishing between different types of cancers lead to unnecessary surgeries and thus warrant development of more discriminatory biomarkers to improve the accuracy of the existing diagnostic and prognostic techniques. Moreover, individualized therapies for thyroid cancer are necessary to avoid overtreatment of indolent lesions and undertreatment of high-risk progressive disease. Since thyroid cancer metabolic signatures are associated with disease ag-gressiveness and responsiveness to therapy, metabolomics has been recently used for diagnostic and prognostic biomarkers discovery. This strategy enabled detection of several metabolites from tissue samples or biofluids to facilitate the classification of disease aggressiveness and to potentially assist in individualized therapies. In this review, we have summarized the utilization and potential of metabolomics in thyroid cancer.
Keywords:
Thyroid cancer
; metabolomics
; biomarkers
; mass spectrometry
; resistance
1. Introduction
Thyroid cancer is the most prevalent endocrine malignancy [1,2,3]. The occurrence of thyroid nodules is attributed to a combination of various factors such as genetics, environment, sex and age. Thyroid nodules mostly occur in females and the incidences rise with age [4,5]. The rising incidence in thyroid cancer has been attributed to a large extend to over-detection due to excessive imaging that has been observed in the early 2000s, and that has plateaued in recent years [6], when more conservative diagnostic criteria have been applied [7].
Thyroid cancer originates from either the follicular cells or the parafollicular cells of the thyroid gland. Follicular cells are mainly involved in the uptake of iodine and production of thyroid hormones, and lead to majority of thyroid carcinomas. On the other hand, parafollicular neuroendocrine cells are associated with the secretion of calcitonin that plays a role in calcium metabolism. Histologically, thyroid cancer is divided into four groups: papillary, follicular, anaplastic (all derived from follicular epithelial cells) and medullary (originating from parafollicular cells). Papillary thyroid cancer (PTC) accounts for about 85%, follicular thyroid cancer (FTC) almost 7-14%, medullary thyroid cancer (MTC) about 3% and anaplastic thyroid cancer (ATC) is approximately 2% of thyroid cancer incidences [8].
The most commonly used method to diagnose thyroid cancer is FNAB (fine-needle aspiration biopsy) and cytological analysis [9]. The Bethesda System classifies FNAB results into six categories: (I) nondiagnostic, (II) benign, (III) atypia of undetermined significance, (IV) follicular neoplasm, (V) suspicious for malignancy, and (VI) malignant [10,11]. However, about 30% of FNABs are unable to distinguish benign from malignant owing to their indeterminate character (Bethesda III/IV) [12]. This uncertainty leads to repetition and reevaluation of FNABs or application of molecular testing that increases the diagnostic accuracy [13,14]. Despite advancements in molecular testing, unnecessary thyroidectomies or lobectomies are still prevalent, having been reported in 56-68% of nodules with Bethesda III/ IV cytology and 21% with Bethesda V cytology [15,16]. Moreover, molecular tests commercially available in the U.S. (Afirma GSC, Thyroseq, and ThyGeNEXT/ ThyraMIR) are not widely used in Europe and Canada due to high costs and reimbursement issues [17,18,19]. Additionally, processing time for molecular testing of indeterminate thyroid nodules takes around 2-4 weeks [17]. Therefore, there is a dire need for more cost-effective and rapid diagnostic techniques.
The use of “OMICS” technologies, which is composed of transcriptomics, genomics, metabolomics and proteomics, is very attractive in the field of cancer. In particular, metabolomics is efficient in providing information of physiological condition of the biological specimen and its phenotype [20]. In general, this technology targets metabolites < 1500 Da molecular weight [21]. It has been found to be useful for investigating the metabolism of cancer cells and finding new diagnostic and prognostic markers [22]. A number of studies have already reported the identification of biomarkers for breast [23], prostate [24], kidney [25] and brain [26] cancer through metabolomic analysis. The use of metabolomics can help in the investigation of distinct phenotypes resulting from the environmental or genetic factors [27]. Metabolic pathways can be correlated with cancer biomarkers as cancer development and progression is associated with metabolic switches that could be reflected in metabolic profiles. Accumulating evidence has suggested marked changes in normal and malignant thyroid tissue samples with respect to the level of lipids and its metabolites [21,28,29,30,31,32]. Lipids have a significant role in cellular metabolism and growth and are therefore associated with oncogenic pathways [33,34].
This review summarizes the recent developments in the field of metabolomics utilization in thyroid cancer and outlines potential applications of this promising tool.
2. Search Strategy
We conducted a comprehensive literature review utilizing the PubMed search engine. Data were analyzed from full-length original articles, case studies and clinical reports between 1/1/1980 - 12/31/2024. Keywords included “thyroid cancer”, “thyroid carcinoma”, “metabolomics”, “targeted metabolomics”, “untargeted metabolomics”, “biomarkers”, “therapy resistance”, “mass spectroscopy” “MRI spectroscopy”, “metabolism”, “metabolites”. The search was restricted to manuscripts published in English, and primarily focused on articles based on their originality, relevance and clinical significance. The search strategy has been summarized in Figure 1.
3. Untargeted and Targeted Metabolomics
Although there are several studies utilizing transcriptomic, genomic and proteomic analysis in the area of thyroid cancer [35,36,37], metabolomics has not been extensively employed. Metabolomics can be classified into untargeted and targeted metabolomics [38], as outlined in Figure 2.
The two most important techniques used for the analysis in thyroid cancer are: Matrix Assisted Laser Desorption Ionization-Imaging Mass Spectrometry (MALDI-IMS) and High-Resolution Magic Angle Spinning Nuclear Magnetic Resonance (HR-MAS NMR) [39,40]. Marked differences were found between normal and tumor tissues in these studies. Owing to the diversity of metabolites with respect to their composition and physicochemical attributes, a unique analytical method is not available for the complete metabolome. Also, the various methods used differs with respect to their sensitivity and specificity [21].
NMR spectroscopy and mass spectroscopy, in combination with gas chromatography (GC) or liquid chromatography (LC), is frequently used to evaluate metabolic profiles of biological samples. The differences between these routinely used analytical techniques have been summarized in Figure 3. It is extremely important that the sample is adequately collected, stored and processed for the metabolomics analysis. Some samples, for example urine, can be directly evaluated. In some instances, urease is required to be added to the urine samples to get rid of urea which could interfere with the quality of GC assay [41,42]. In the GC/MS analysis, the method of derivatization plays a significant role in converting the polar metabolites into volatile compounds. On the other hand, NMR requires balancing the pH using phosphate buffer. Also, if the samples require further dilution, deuterium is required [43]. Deproteinization is essential for blood samples owing to the presence of abundant protein. The sample processing requires at least 100-500µl volume of biofluids.
In general, tissue processing is more complicated as it contains blood and is associated with tissue heterogeneity. Often, saline is utilized for washing the samples and techniques such as LCM (laser-capture microdissection) are employed prior to storage. Moreover, in order to obtain metabolites from tissues, an extraction buffer and homogenizer are needed [44]. Thereafter, the specimens are dried and appropriate solvent is added to them to proceed with LC/MS. In case of GC/MS, further chemically derivatization steps are required (Figure 3).
A crucial factor to consider for metabolomics assays is the use of suitable chemical solvents for the samples. Some solvents include: butanol/methanol (BUME), chloroform (methyl tert-butyl ether, MTBE) or methanol to be used for GC/MS as well as LC/MS. For NMR studies, trimethylsilylpropanoic acid (TSP) or 4, 4-dimethyl-4-silapentane-1-sulfonic acid (DSS) is conventionally used as reference standard for appropriate metabolite quantifications [45]. Once the data is collected, normalization and mean centering is conducted to process the data. Univariate, unsupervised multivariate statistics or supervised multivariate statistics can be used for the data analysis. There are several tools available such as Ingenuity Pathway Analysis (IPA, by Qiagen), Cytoscape and Metaboanalyst which can be utilized for quantification of data. The various steps involved in this assay are summarized in Figure 4. Untargeted metabolomics focus on global analysis of known as well as unknown metabolites and is thus unbiased. The data obtained can be further utilized for relative quantification and serve as diagnostic or prognostic tool.
On the other hand, targeted metabolomics can identify and analyze a limited number of pre-defined metabolites or confirm and validate the data obtained from unsupervised screening. For example, some of the metabolites that can be targeted have been consistently detected in malignancies, including thyroid cancer. Elevated lactate, and changes in the levels of leucine, choline, phenylalanine and tyrosine have been reported. The increased lactate can be attributed to the Warburg effect which suggests that cancer cells demonstrate upregulated glycolysis with high lactate secretion even under abundant oxygen conditions [46]. Lactate has an essential role in cell migration, angiogenesis and self-metabolism. It has also been reported as a potential biomarker in various cancers including breast, pancreatic, lung and thyroid cancer [47,48,49,50].
4. Metabolomics for Biomarker Discovery
Metabolomics has become a gateway for studying metabolic pathways, phenotypes and metabolic reprogramming in thyroid cancer. Significant alterations are documented in thyroid cancer metabolism of glucose, amino acids, and lipids, as well as mitochondrial respiration as compared with non-malignant thyroid tissue [51,52]. Thyroid cancer research can capitalize on these metabolic alterations as an avenue for identifying new biomarkers. Metabolomic studies in thyroid cancer have been commonly based on NMR techniques, specifically 1H-NMR metabolomics with an untargeted approach [53]. However, mass spectrometry has gained significance in recent work given the limitations of NMR, such as its lower sensitivity [52,54]. Given the enhanced sensitivity of mass spectrometry-based metabolomics, a broader range of metabolites can be detected, providing a more comprehensive understanding of metabolic alterations in thyroid cancer [53]. Other metabolomic techniques, such as Fourier-transform infrared spectroscopy, are also gaining attention in thyroid cancer research [55]. Razavi et al. conducted a systematic review and meta-analysis of NMR-based metabolomic studies, identifying forty differential metabolites associated with thyroid cancer (Table 1) [56]. These metabolites could serve as promising biomarkers for early diagnosis. In a subsequent study, Razavi et al. identified potential biomarkers for thyroid cancer, including the commonly downregulated metabolite, myo-inositol [57]. Myo-inositol may help differentiate malignant tissue from healthy tissue, offering a non-invasive diagnostic tool using biofluids such as plasma [57]. The diagnostic performance measured as area under the curve (AUC) of the metabolic profile, which included myo-inositol, was 85.3%, comparable to that of FNA (90%)[58,59]. In a recent study by Yu et al., a novel metabolic biomarker signature (17 biomarker panel) was identified to distinguish between PTC and benign thyroid nodule (BTN) (Table 1). Interestingly, the diagnostic accuracy of this test was 92.72% in the validation cohort, which is also comparable to standard FNAB. However, while FNAB is a gold standard, the 30% prevalence of cytologically indeterminate thyroid nodules suggests that metabolomics may complement FNAB. Moreover, when combined with ultrasound, it might strengthen the diagnostic accuracy even more [60]. In fact, metabolomics has been applied for indeterminate and/or nondiagnostic FNABs [55,61,62,63,64]. These studies demonstrate that metabolomics can effectively reclassify indeterminate FNAB specimen, with potential accuracy rates of up to 95%. Accurately classifying indeterminate nodules as malignant or benign is crucial for reducing the need for unnecessary diagnostic surgeries (Table 1).
Mass spectrometry imaging (MSI) of metabolites offers another approach for thyroid cancer diagnostics. While non-invasive analysis of metabolites can provide insightful quantifications, MSI allows spatial mapping of metabolites. As tumors exhibit significant heterogeneity, metabolite spatial mapping gives a more complete picture of metabolic plasticity beyond their sole concentration [65,66]. In thyroid cancer, MSI has had many recent applications. MALDI-MSI has shown to be capable of identifying PTC from benign tissue through lipid profiling of formalin-fixed tissue [67]. Lipid profiling revealed that phosphatidylcholines, sphingomyelins, and phosphatidic acids were more abundant in malignant tissue versus benign. A study utilizing desorption electrospray ionization mass spectrometry (DESI-MS) imaging provides a potential method for analyzing FNAB samples to reduce the number of unnecessary diagnostic surgeries [68]. The metabolic profiles of the FNAB samples were obtained from DESI-MS and classified malignant PTC from benign tissue with an AUC of 0.98, higher than that of FNAB. Another recent study using MALDI imaging found that N-glycan abundance was much higher in normal thyroid tissue compared to that of cancer tissue [69]. Mao et al. used air flow-assisted desorption electrospray ionization mass spectrometry imaging (AFAIDESI-MSI) to distinguish benign follicular thyroid adenoma (FTA) from malignant carcinoma based on metabolic signature, finding both phospholipids and fatty acids to be more abundant in FTA than FTC [70]. Given this information, they also found the metabolic enzymes fatty acid synthase (FASN) and calcium-independent phospholipase A2 (iPLA2) to be significantly upregulated in FTA. These metabolic alterations had a diagnostic AUC of 73.6%, with potential of classifying borderline follicular tumors. Overall, mass spectrometry imaging enhances thyroid cancer diagnostics by providing spatial metabolic profiling that improves understanding of tumor heterogeneity.
Recent studies have also focused on developing thyroid cancer metabolic profiles using biofluids. This is a minimally invasive approach as compared to FNA and/or surgery to collect a biospecimen. The study by Berinde et al. supports the potential of using metabolic biomarkers to discriminate between papillary thyroid cancer (PTC), benign nodules, and healthy subjects [73]. Through HPLC-QTOF-ESI+-MS technology, they identified 17 metabolites, including lipid and selenium-related molecules, that had discriminatory value of 0.97 for differentiation between PTC and healthy control patients [73]. Another study by Berinde et al. investigated the urinary biomarkers to differentiate PTC and benign nodules from healthy controls [74]. They identified ten classes of metabolites, mostly lipid-related, that served as diagnostic biomarkers with an accuracy of 65-73%. This suboptimal accuracy suggests that urinalysis might be subject to a significant bias from several confounding excreting metabolites, preventing its use as a sole diagnostic tool.
Analyzing breath metabolites is another non-invasive approach for early diagnosis of thyroid cancer [75]. Biomarkers were identified in both end-tidal and mixed expiratory breath, with area under the curve (AUC) values greater than 90% for effectively distinguishing between PTC and healthy control groups. Potential classes of breath biomarkers identified in the study by Li et al. included alkanes, esters, ketones, and fluorine/chlorine organic compounds.
Additionally, Razavi et al. used 1H NMR spectroscopy to profile metabolites of PTC plasma samples [59]. Their profiling identified increased levels of leucine and lysine, along with decreased levels of pyruvate and tyrosine in patients with PTC compared to healthy individuals [59]. Although the diagnostic accuracy was 85%, the sample size was relatively small, and the study requires further validation.
Zhang et al. also identified ten amino acid metabolites in saliva that were able to differentiate PTC from healthy controls [76]. These metabolites used as individual biomarkers had AUC values ranging from 67.8-83.3%. However, when alanine, valine, proline, and phenylalanine were combined into a diagnostic panel, the AUC improved to 93.6%, suggesting that combining multiple biomarkers will increase accuracy of early diagnosis. Both urinary and serum metabolites were investigated by Chen et al., and they identified six metabolites with potential of diagnosing PTC (AUC = 95.2% in samples from both females and males) [77]. To further validate this study and incorporate PTC staging into the metabolite analysis, a larger sample size is necessary, as biofluids were collected from only 124 untreated PTC patients, 76 untreated BTN patients, and 116 healthy controls, respectively.
Importantly, when identifying these biomarkers, it’s crucial to consider how they are influenced by confounding physiological factors. For example, iodine is closely linked to thyroid function and may affect different biomarkers of thyroid cancer [78]. Liu et al. found that iodine nutrition affects the diagnostic accuracy of several serum metabolites [78]. In addition, environmental chemical disruptors can play a significant role in the interpretation of metabolomics data. Wang et al. studied how exposure to per- and polyfluoroalkyl substances (PFAS) affects the serum metabolome and thyroid cancer risk [79]. Their study suggested that PFAS exposure may disrupt several free fatty acid metabolites involved with thyroid cancer pathogenesis [79]. Similarly, Song et al. examined the impact of polybrominated diphenyl ethers (PBDEs) on the metabolic signature of PTC [80]. Their findings highlighted octopamine and 5-hydroxyindole as potential diagnostic biomarkers for PTC [80].
To summarize, these findings suggest that metabolic biomarkers, such as those found in biofluids, and combined with novel imaging techniques may significantly add to the armamentarium of thyroid cancer diagnosis and might serve as minimally invasive and affordable ways to diagnose thyroid cancer [81].
5. Metabolomics in Disease Subtyping
Recent studies have also focused on using metabolomic profiling to further phenotype thyroid cancer. Wojakowska et al. showed that metabolic signature of classic PTC is different compared with follicular variant PTC, as it is characterized by upregulated citric acid and downregulated gluconic acid [82]. This data may suggest that the main oncogenic drivers of classic PTC such as BRAFV600E are associated with different metabolic profiles than RAS-driven tumors that usually present a follicular pattern of growth [83]. Qu et al. aimed to characterize PTC patients based on risk of recurrence [84]. Their multi-omic strategy included metabolomic profiling of 503 metabolites from 102 tumor and 37 paired normal tissue samples [84]. Patients with high risk of recurrence had upregulated levels of triglycerides, free fatty acids, histamine, and kynurenine. Additionally, upregulation of metabolites in amino acid biosynthesis and glycolysis were found in patients with high recurrence risk. These findings corroborate with pre-clinical and clinical studies showing that molecular alterations in similar metabolic pathways were associated with poor PTC outcomes[85,86,87,88,89,90].
Lee et al. used liquid chromatography-mass spectrometry (LC-MS) to perform metabolic profiling of 17 thyroid tumor-normal tissue pairs [91]. Their data showed an increase of serine and related metabolites in undifferentiated thyroid cancer, highlighting the role of the serine/glycine pathway in thyroid cancer cell proliferation/de-differentiation [84]. Similarly, Huang et al. performed metabolite set enrichment analysis in thyroid cancer, identifying enriched pathways such as arachidonic acid and cysteine/methionine metabolism which are both associated with the ferroptosis pathway [92]. Furthermore, they found that the enzyme longevity assurance homologue 2 (LASS2) in association with transferrin receptor (TFRC) can suppress metastasis in thyroid cancer by regulating ferroptosis, a critical pathway involved in tumor growth and proliferation [92].
Metastatic disease in thyroid cancer is associated with a poorer prognosis, and early detection of metastatic potential or identifying metabolic pathways that could be targeted to eradicate metastatic disease are of outmost importance. Xu et al. found 31 differential metabolites in serum from patients with lymph node metastasis compared to those without metastatic disease, including elevated levels of L-proline, L-tryptophan, and 5-hydroxylysine, and decreased levels of deoxycholic acid, erucic acid, and glycerophosphocholine [93]. Another study identified increased lactate associated with lymph node metastasis [94]. Shen et al. explored the metabolic signature of PTC with distant metastasis, revealing 31 differential serum metabolites linked to glucose, amino acids, lipids, gut microbes, and vitamin metabolism [95]. Similarly, another study found six altered metabolites associated with metastatic thyroid cancer, including ascorbic acid, guanidinoacetic acid, betaine, pyruvate, phenylacetic acid, and adenosine [96]. While these studies were limited by small sample sizes, they offer promising avenues to understanding and targeting metabolic shifts occurring in metastatic disease and potentially testing it as biomarkers of early metastatic disease. They may also potentially serve to capture the metabolic reprogramming in response to targeted therapy. By analyzing changes in metabolites, this technique provides a real-time picture of a drug’s anti-tumor effects at the metabolic level. Unlike traditional methods that focus on tumor imaging and biomarkers measurements (such as thyroid cancer-specific thyroglobulin or calcitonin), metabolomics can monitor treatment response through the analysis of metabolic reprogramming. For example, a study by Ouyang et al. showed how metabolomics can be used to evaluate the therapeutic benefits of metformin in thyroid cancer [97]. By integrating metabolomics with transcriptomics, they identified significant molecular changes associated with treatment. Specifically, they observed altered metabolites of glutathione metabolism and the TCA cycle, and inhibited glycolysis. A study by Thakur et al. also revealed downregulated oxidative phosphorylation in response to metformin treatment [98]These findings all point to the ability of metabolomics to assess metabolic shifts associated with treatment.
Since resistance to targeted therapies is the main reason of thyroid cancer-specific mortality, we next focus on the role of metabolic profiling in unresponsiveness to standard treatment.
6. Metabolomics for Overcoming Therapy Resistance
Resistance to radioiodine therapy continues to be a major cause of thyroid cancer mortality. Timely identification of radioiodine resistance in patients is crucial for selecting the appropriate alternative treatment options, such as tyrosine kinase inhibitors (TKIs). Zheng et al. used LC-MS to identify metabolic differences between RAI-resistant and non-resistant thyroid cancer patients [99]. Their analysis revealed differences in metabolites of the phenylalanine and tyrosine pathways, which could serve as biomarkers for predicting RAI resistance [99]. However, these biomarkers have not been tested prospectively, to validate its utility in clinical practice. In a similar study, Wang et al. found that ketone body metabolism was significantly altered in RAI-resistant differentiated thyroid cancer (DTC) patients [100]. Specifically, upregulation of acetoacetate in non-RAI-resistant patients enhanced 131I uptake and increased sodium/iodide symporter (NIS) and thyroid stimulating hormone receptor (TSHR) levels [100]. This key finding suggests potential therapeutic applications of inducing ketogenesis to overcome RAI-resistance in DTC. Untargeted metabolomics performed by Yu et al. revealed that polyfluoroalkyl substance (PFAS) exposure may be associated with resistance to radioiodine (RAI) therapy [101]. The authors identified enrichment of perfluorodecanoic and perfluorononanoic acids in RAI-refractory DTC patients, which was associated with thyroid cancer progression and reduced expression of sodium-iodide symporter (NIS), that is necessary for RAI uptake [101].
Beyond RAI resistance, metabolomics can provide insights into RAI-therapy induced radiotoxicity. Two studies by Lu et al. examined the effects of 131I treatment on gut metabolites in DTC patients [102,103]. LC-MS/MS untargeted metabolomics found downregulated pathways of linoleic acid, arachidonic acid, and tryptophan metabolism after 131I therapy [102]. These radiation-sensitive pathways are suspected to play a crucial role in protecting against radiation toxicity, which could have long-term implications in DTC patients. Despite the downregulation of arachidonic acid-related metabolites and pathways post-131I therapy, arachidonic acid supplementation in mice reduced radiotoxicity, offering potential for mitigating side effects of radiation therapy [103]. These findings highlight the importance of metabolomic profiling in understanding radiotoxicity and suggest potential therapeutic strategies for minimizing side effects.
Since RAI-resistant thyroid cancer requires therapy with targeted TKIs, understanding resistance to such therapy is of vital importance. Resistance to single agent chemotherapeutics remains a major challenge in managing aggressive thyroid cancer. Metabolomics has proven useful for identifying metabolic alterations associated with therapy resistance. A recent study by Kumari et al. utilizing the technique of unsupervised metabolomics revealed that thyroid cancer cell lines resistant to standard care TKI Lenvatinib clustered separately from non-resistant cell lines, suggesting a distinct metabolic profile [104]. Xu et al. investigated the synergistic effects of BRAF and PIM1 inhibitors on BRAFV600E-positive PTC cell lines [105]. PIM1 is an oncogenic serine/threonine kinase involved in the cell cycle, drug resistance, cell survival, and cell proliferation. Expression of PIM1 is upregulated in BRAFV600E-mutated thyroid cancer, which could possibly serve as an escape mechanism to BRAF inhibitors. The metabolomic data revealed that the combination therapy limited the availability of essential amino acids (phenylalanine, arginine, and glutamate) for cell growth and proliferation, while also downregulating nucleotide synthesis pathways [105]. Liu et al. integrated metabolomics and transcriptomics to uncover mechanisms contributing to thyroid cancer resistance to anlotinib that has been used in clinical trials for metastatic progressive thyroid cancer [106]. Combined “omics” analysis revealed high expression of glutamate in anlotinib-resistant thyroid cancer cell lines [106]. Additionally, eight genes closely related to glutamate involvement in disease pathways were differentially expressed [106]. Of these genes, LPAR1 (Lysophosphatidic acid receptor 1) is suspected to be a potentially important target for overcoming resistance to anlotinib [106]. LPAR1 plays a role in cell proliferation, migration, and survival by mediating with signaling pathways involved with tumor growth [107].
These findings emphasize the ability of metabolomics to detect metabolic shifts in resistant clones and identify targets for therapies aimed at overcoming drug resistance in thyroid cancer. Therefore, it is important to develop models investigating the signal detected by metabolomics studies in the appropriate in vitro and in vivo models, to understand a potential causal relationships and associations with thyroid cancer.
7. Models for Metabolomic Studies
Model development is essential for advancing metabolite-based approaches for screening thyroid cancer biomarkers. Kuang et al. developed a machine learning model with potential of screening for thyroid cancer using metabolite biomarkers [108]. Their machine learning model identified PTC-related metabolites with an accuracy of 87.3%. The combination of machine learning and artificial intelligence with metabolite biomarkers holds great promise for rapid screening and accurate diagnosis of thyroid cancer [108].
Cell culture models allow for controlled and reproducible studies of the metabolic behavior of thyroid cancer [72]. Metabolic alterations have been documented using cell lines from multiple subtypes of thyroid cancer [72]. In the oncocytic thyroid cancer cell line XTC.UC1, metabolomics analysis revealed that glycolytic intermediates were utilized not only for upregulated glycolysis, but also lipid metabolism and serine synthesis [109]. Since this diversion of metabolites was not observed in non-oncocytic models, it’s suspected that the defective mitochondria-rich oncocytic cancer cells may be compensating for their defected mitochondrial oxidative phosphorylation [109]. In fact, Kumari et al. described how oncocytic thyroid cancer is characterized by genetic alterations leading to decreased oxidative phosphorylation and increased glycolysis [110]. Another study utilized PTC-derived cell lines to investigate the cytotoxic effects of Vitamin C, revealing that it induces oxidative stress and alters glycolysis and the TCA cycle, leading to cancer cell death and suggesting potential treatment strategies [111]. Additionally, Chen et al. proposed a method involving gold-doped zirconium-based metal-organic framework (ZrMOF/Au) nanostructures for the metabolic profiling of thyroid cancer [112]. Cristiani et al. also developed a 3D thyroid organoid model from human primary thyrocytes for investigation of thyroid metabolism[113]. Their study revealed that thyroid metabolism-related genes, such as TPO, TSHR, PAX8, TTF-1, NIS, IYD, and TG, maintained functionality in the 3D organoids, whereas 2D cultures lost phenotype over time. While thyroid cancer patient-derived organoids have been established [114,115], further advancements are needed to translate these models for use in metabolomic studies.
Together, these efforts highlight the growing potential of different metabolomic approaches for thyroid cancer.
8. Metabolomics: Bridging other Omics
Metabolomic studies tend to be much more powerful when coupled with genomics, transcriptomics, and proteomics. Dhuli et al. reviewed how the integration of “OMICS” sciences has improved the diagnosis, prognosis, and treatment of thyroid cancer [116]. In particular, they found that major advancements in precision medicine have stemmed from combined efforts of “OMICS” disciplines. For example, genomics and transcriptomics have uncovered critical mutations driving thyroid cancer, whereas proteomics and metabolomics have identified biomarkers enhancing the accuracy of thyroid cancer diagnostics and prognostics.
Molecular markers discovered through multi-omics approaches enable development of personalized therapies, such NTRK or ALK fusions improving overall prognosis for thyroid cancer patients [117]. Another comprehensive analysis displays the complexity of each thyroid cancer subtype and underscores the translational benefits of a multi-omics approach for improving patient risk stratification and identifying targeted therapies [118]. Gulfidan et al. investigated PTC prognostic biomarkers through a meta-analysis of four transcriptome datasets, revealing key genes, proteins, metabolites, and regulatory molecules [119]. Their multi-omic data led to the identification of potential therapies that may be useful in treating PTC, including meclizine, rottlerin, and tretinoin, to name just a few. Overall, the integration of omics disciplines provides a powerful framework for revealing molecular alterations in thyroid cancer, advancing personalized treatment, and improving patient outcomes.
The most important applications of metabolomics in cancer research include distinguishing between tumor subtypes, environmental risk factors, individualized therapies, biomarker identification and cancer pathophysiology, and have been summarized in Figure 5.
9. Conclusions and Future Directions
In summary, current application of metabolomics is limited to research studies, but there is a potential for its utilization for diagnostic purposes, treatment monitoring and prognostication (Figure 5). However, to translate these research findings to standard clinical practice, verifying the reproducibility and preciseness of the identified biomarkers in larger diverse populations is required. Standard operating procedures for metabolomics’ wider application in thyroid cancer are needed and involve multiple steps including standardized sample collection, processing and streamlined analysis. It would be imperative to develop models that include clinical, pathological, molecular and metabolomics data to optimize the diagnostic procedures, discriminate between indolent and aggressive thyroid cancers, and guide individualized therapies. Developing a comprehensive framework for metabolomics can facilitate personalized treatment for thyroid cancer patients, that could lead to improved outcomes. In addition, targeting metabolic pathways is an emerging strategy to overcome resistance towards the standard treatment options and warrants further investigation in preclinical models and clinical trials.
Author Contributions
Conceptualization, S.K. and J.K.-G.; Methodology, Software, Validation, Formal Analysis, Investigation, Resources, Data Curation, S.K. and J.K.-G; Writing—Original Draft Preparation, Writing—Review & Editing, Visualization, S.K., A.M. and J.K.-G.; Supervision, J.K.-G; Project Administration, J.K.-G.; Funding Acquisition, J.K.-G. All authors have read and agreed to the published version of the manuscript.
Funding
This work was funded by the Intramural Program of the National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK), National Institutes of Health (NIH), Bethesda, Maryland (NIDDK Intramural Program ZIE DK 04705313).
Acknowledgments
We thank Dr. Lee Weinstein for critical review of the paper.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
| TCA | Tricarboxylic acid |
| FDG-PET | 18F-deoxyglucose Positron Emission Tomography |
| OXPHOS | Oxidative phosphorylation |
| MS | Mass Spectrometry |
| NMR | Nuclear Magnetic Resonance |
| FNAB | Fine-needle aspiration biopsy |
| LC-MS | Liquid chromatography coupled to mass spectrometry |
| GC-MS | Gas chromatography coupled to mass spectrometry |
| LCM | Laser-capture microdissection |
| AUS | Atypia of undetermined significance |
| FLUS | Follicular lesion of undetermined significance |
| FN | Follicular neoplasm |
| SMC | Suspicious for malignant cells |
| MALDI-IMS | Matrix Assisted Laser Desorption Ionization-Imaging Mass Spectrometry |
| HR-MAS NMR | High-Resolution Magic Angle Spinning Nuclear Magnetic Resonance |
| LASS2 | Longevity assurance homologue 2 |
| BUME | Butanol/methanol |
| MTBE | Methyl tert-butyl ether |
| NIS | Sodium/iodide symporter |
| TSHR | Thyroid stimulating hormone receptor |
| DTC | Differentiated thyroid cancer |
| PTC | Papillary thyroid cancer |
| FTC | Follicular thyroid cancer |
| MTC | Medullary thyroid cancer |
| ATC | Anaplastic thyroid cancer |
| TSP | Trimethylsilylpropanoic acid |
| DSS | 4,4-dimethyl-4-silapentane-1-sulfonic acid |
| TKI | Tyrosine kinase inhibitors |
References
- Sipos, J.; Mazzaferri, E. Thyroid Cancer Epidemiology and Prognostic Variables. Clin. Oncol. 2010, 22, 395–404. [Google Scholar] [CrossRef] [PubMed]
- Sherman, S.I. Thyroid carcinoma. Lancet 2003, 361, 501–11. [Google Scholar] [CrossRef] [PubMed]
- Kondo, T.; Ezzat, S.; Asa, S.L. Pathogenetic mechanisms in thyroid follicular-cell neoplasia. Nat. Rev. Cancer 2006, 6, 292–306. [Google Scholar] [CrossRef] [PubMed]
- Knudsen, N.; Laurberg, P.; Perrild, H.; Bülow, I.; Ovesen, L.; Jørgensen, T. Risk Factors for Goiter and Thyroid Nodules. Thyroid® 2002, 12, 879–888. [Google Scholar] [CrossRef]
- Albi, E. , et al., Radiation and Thyroid Cancer. Int J Mol Sci. 2017, 18. [Google Scholar] [CrossRef]
- Society, A.C. , Cancer Facts & Figures 2025. 2025.
- Zhou, Q.; Zhang, L.-Y.; Xie, C.; Zhang, M.-L.; Wang, Y.-J.; Liu, G.-H. Metabolomics as a potential method for predicting thyroid malignancy in children and adolescents. Pediatr. Surg. Int. 2019, 36, 145–153. [Google Scholar] [CrossRef]
- Zaballos, M.A.; Santisteban, P. Key signaling pathways in thyroid cancer. J. Endocrinol. 2017, 235, R43–R61. [Google Scholar] [CrossRef]
- Cibas, E.S.; Ali, S.Z. The Bethesda System for Reporting Thyroid Cytopathology. Thyroid 2009, 19, 1159–65. [Google Scholar] [CrossRef]
- Yang, J.; Schnadig, V.; Logrono, R.; Wasserman, P.G. Fine-needle aspiration of thyroid nodules: A study of 4703 patients with histologic and clinical correlations. Cancer 2007, 111, 306–315. [Google Scholar] [CrossRef]
- Ali, S.Z. , et al. , The 2023 Bethesda System for reporting thyroid cytopathology. Journal of the American Society of Cytopathology 2023, 12, 319–325. [Google Scholar]
- Yassa, L.; Cibas, E.S.; Benson, C.B.; Frates, M.C.; Doubilet, P.M.; Gawande, A.A.; Moore, F.D., Jr.; Kim, B.W.; Nosé, V.; Marqusee, E.; et al. Long-term assessment of a multidisciplinary approach to thyroid nodule diagnostic evaluation. Cancer 2007, 111, 508–516. [Google Scholar] [CrossRef] [PubMed]
- Pacini, F. , et al, Erratum: European consensus for the management of patients with differentiated thyroid carcinoma of the follicular epithelium. European Journal of Endocrinology 2006, 155, 385–385. [Google Scholar]
- Bongiovanni, M.; Spitale, A.; Faquin, W.C.; Mazzucchelli, L.; Baloch, Z.W. The Bethesda System for Reporting Thyroid Cytopathology: A Meta-Analysis. Acta Cytol. 2012, 56, 333–339. [Google Scholar] [CrossRef]
- Ho, A.S.; Sarti, E.E.; Jain, K.S.; Wang, H.; Nixon, I.J.; Shaha, A.R.; Shah, J.P.; Kraus, D.H.; Ghossein, R.; Fish, S.A.; et al. Malignancy Rate in Thyroid Nodules Classified as Bethesda Category III (AUS/FLUS). Thyroid® 2014, 24, 832–839. [Google Scholar] [CrossRef]
- Mavromati, M.; Saiji, E.; Demarchi, M.S.; Lenoir, V.; Seipel, A.; Kuczma, P.; Jornayvaz, F.R.; Becker, M.; Fernandez, E.; De Vito, C.; et al. Unnecessary thyroid surgery rate for suspicious nodule in the absence of molecular testing. Eur. Thyroid. J. 2023, 12. [Google Scholar] [CrossRef]
- Hannoush, Z.C.; Ruiz-Cordero, R.; Jara, M.; Kargi, A.Y. Current State of Molecular Cytology in Thyroid Nodules: Platforms and Their Diagnostic and Theranostic Utility. J. Clin. Med. 2024, 13, 1759. [Google Scholar] [CrossRef]
- Durante, C.; Hegedüs, L.; Czarniecka, A.; Paschke, R.; Russ, G.; Schmitt, F.; Soares, P.; Solymosi, T.; Papini, E. 2023 European Thyroid Association Clinical Practice Guidelines for thyroid nodule management. Eur. Thyroid. J. 2023, 12. [Google Scholar] [CrossRef]
- MacKay, C.; Turner, B.; Clarke, S.; Wallace, T.; Rigby, M.H. Cost-Effectiveness Analysis of Molecular Testing for Indeterminate Thyroid Nodules in Nova Scotia. J. Otolaryngol.-Head Neck Surg. 2024, 53. [Google Scholar] [CrossRef]
- Nicholson, J.K.; Lindon, J.C.; Holmes, E. ‘Metabonomics’: Understanding the metabolic responses of living systems to pathophysiological stimuli via multivariate statistical analysis of biological NMR spectroscopic data. Xenobiotica 1999, 29, 1181–1189. [Google Scholar] [CrossRef]
- Wojakowska, A.; Chekan, M.; Widlak, P.; Pietrowska, M. Application of Metabolomics in Thyroid Cancer Research. Int. J. Endocrinol. 2015, 2015, 1–13. [Google Scholar] [CrossRef]
- Spratlin, J.L.; Serkova, N.J.; Eckhardt, S.G. Clinical Applications of Metabolomics in Oncology: A Review. Clin. Cancer Res. 2009, 15, 431–440. [Google Scholar] [CrossRef] [PubMed]
- Denkert, C.; Bucher, E.; Hilvo, M.; Salek, R.; Orešič, M.; Griffin, J.; Brockmöller, S.; Klauschen, F.; Loibl, S.; Barupal, D.K.; et al. Metabolomics of human breast cancer: new approaches for tumor typing and biomarker discovery. Genome Med. 2012, 4, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Thysell, E.; Surowiec, I.; Hörnberg, E.; Crnalic, S.; Widmark, A.; Johansson, A.I.; Stattin, P.; Bergh, A.; Moritz, T.; Antti, H.; et al. Metabolomic Characterization of Human Prostate Cancer Bone Metastases Reveals Increased Levels of Cholesterol. PLOS ONE 2010, 5, e14175. [Google Scholar] [CrossRef]
- Kind, T. , et al. , A comprehensive urinary metabolomic approach for identifying kidney cancerr. Anal Biochem, 2007, 363, 185–95. [Google Scholar]
- Howe, F.; Barton, S.; Cudlip, S.; Stubbs, M.; Saunders, D.; Murphy, M.; Wilkins, P.; Opstad, K.; Doyle, V.; McLean, M.; et al. Metabolic profiles of human brain tumors using quantitative in vivo 1H magnetic resonance spectroscopy. Magn. Reson. Med. 2003, 49, 223–232. [Google Scholar] [CrossRef]
- Claudino, W.M.; Goncalves, P.H.; di Leo, A.; Philip, P.A.; Sarkar, F.H. Metabolomics in cancer: A bench-to-bedside intersection. Crit. Rev. Oncol. 2012, 84, 1–7. [Google Scholar] [CrossRef]
- Miccoli, P.; Torregrossa, L.; Shintu, L.; Magalhaes, A.; Chandran, J.; Tintaru, A.; Ugolini, C.; Minuto, M.N.; Miccoli, M.; Basolo, F.; et al. Metabolomics approach to thyroid nodules: A high-resolution magic-angle spinning nuclear magnetic resonance–based study. Surgery 2012, 152, 1118–1124. [Google Scholar] [CrossRef]
- Grogan, R.H.; Mitmaker, E.J.; Clark, O.H. The Evolution of Biomarkers in Thyroid Cancer—From Mass Screening to a Personalized Biosignature. Cancers 2010, 2, 885–912. [Google Scholar] [CrossRef]
- Guo, L.; Wang, C.; Chi, C.; Wang, X.; Liu, S.; Zhao, W.; Ke, C.; Xu, G.; Li, E. Exhaled breath volatile biomarker analysis for thyroid cancer. Transl. Res. 2015, 166, 188–195. [Google Scholar] [CrossRef]
- Shang, X.; Zhong, X.; Tian, X. Metabolomics of papillary thyroid carcinoma tissues: potential biomarkers for diagnosis and promising targets for therapy. Tumor Biol. 2016, 37, 11163–11175. [Google Scholar] [CrossRef]
- Chen, M.; Shen, M.; Li, Y.; Liu, C.; Zhou, K.; Hu, W.; Xu, B.; Xia, Y.; Tang, W. GC-MS-based metabolomic analysis of human papillary thyroid carcinoma tissue. Int. J. Mol. Med. 2015, 36, 1607–1614. [Google Scholar] [CrossRef] [PubMed]
- Wenk, M.R. The emerging field of lipidomics. Nat. Rev. Drug Discov. 2005, 4, 594–610. [Google Scholar] [CrossRef]
- Bandu, R.; Mok, H.J.; Kim, K.P. Phospholipids as cancer biomarkers: Mass spectrometry-based analysis. Mass Spectrom. Rev. 2016, 37, 107–138. [Google Scholar] [CrossRef]
- Xing, M.; Haugen, B.R.; Schlumberger, M. Progress in molecular-based management of differentiated thyroid cancer. Lancet 2013, 381, 1058–1069. [Google Scholar] [CrossRef] [PubMed]
- Krause, K.; Jeßnitzer, B.; Fuhrer, D.; Führer-Sakel, D. Proteomics in Thyroid Tumor Research. J. Clin. Endocrinol. Metab. 2009, 94, 2717–2724. [Google Scholar] [CrossRef]
- Carpi, A.; Mechanick, J.I.; Saussez, S.; Nicolini, A. Thyroid tumor marker genomics and proteomics: Diagnostic and clinical implications. J. Cell. Physiol. 2010, 224, 612–619. [Google Scholar] [CrossRef]
- Schrimpe-Rutledge, A.C.; Codreanu, S.G.; Sherrod, S.D.; McLean, J.A. Untargeted Metabolomics Strategies—Challenges and Emerging Directions. J. Am. Soc. Mass Spectrom. 2016, 27, 1897–1905. [Google Scholar] [CrossRef]
- Guo, S.; Qiu, L.; Wang, Y.; Qin, X.; Liu, H.; He, M.; Zhang, Y.; Li, Z.; Chen, X. Tissue imaging and serum lipidomic profiling for screening potential biomarkers of thyroid tumors by matrix-assisted laser desorption/ionization-Fourier transform ion cyclotron resonance mass spectrometry. Anal. Bioanal. Chem. 2014, 406, 4357–4370. [Google Scholar] [CrossRef]
- Deja, S.; Dawiskiba, T.; Balcerzak, W.; Orczyk-Pawiłowicz, M.; Głód, M.; Pawełka, D.; Młynarz, P. Follicular Adenomas Exhibit a Unique Metabolic Profile. 1H NMR Studies of Thyroid Lesions. PLOS ONE 2013, 8, e84637. [Google Scholar] [CrossRef]
- Scalbert, A.; Brennan, L.; Fiehn, O.; Hankemeier, T.; Kristal, B.S.; van Ommen, B.; Pujos-Guillot, E.; Verheij, E.; Wishart, D.; Wopereis, S. Mass-spectrometry-based metabolomics: limitations and recommendations for future progress with particular focus on nutrition research. Metabolomics 2009, 5, 435–458. [Google Scholar] [CrossRef]
- Beger, R.D. A Review of Applications of Metabolomics in Cancer. Metabolites 2013, 3, 552–574. [Google Scholar] [CrossRef] [PubMed]
- Brennan, L. NMR-based metabolomics: From sample preparation to applications in nutrition research. Prog. Nucl. Magn. Reson. Spectrosc. 2014, 83, 42–49. [Google Scholar] [CrossRef] [PubMed]
- Griffin, J.L.; Kauppinen, R.A. Tumour Metabolomics in Animal Models of Human Cancer. J. Proteome Res. 2006, 6, 498–505. [Google Scholar] [CrossRef]
- Felli, I.C.; Brutscher, B. Recent Advances in Solution NMR: Fast Methods and Heteronuclear Direct Detection. Chemphyschem 2009, 10, 1356–1368. [Google Scholar] [CrossRef]
- Warburg, O. On the Origin of Cancer Cells. Science 1956, 123, 309–314. [Google Scholar] [CrossRef]
- Suman, S.; Sharma, R.K.; Kumar, V.; Sinha, N.; Shukla, Y. Metabolic fingerprinting in breast cancer stages through 1H NMR spectroscopy-based metabolomic analysis of plasma. 2018, 160, 38–45. [Google Scholar] [CrossRef]
- Michálková, L. , et al., Diagnosis of pancreatic cancer via(1)H NMR metabolomics of human plasma. Analyst 2018, 143, 5974–5978. [Google Scholar] [CrossRef]
- An, Y.J.; Cho, H.R.; Kim, T.M.; Keam, B.; Kim, J.W.; Wen, H.; Park, C.-K.; Lee, S.-H.; Im, S.-A.; Kim, J.E.; et al. An NMR metabolomics approach for the diagnosis of leptomeningeal carcinomatosis in lung adenocarcinoma cancer patients. Int. J. Cancer 2014, 136, 162–171. [Google Scholar] [CrossRef]
- San-Millán, I.; Brooks, G.A. Reexamining cancer metabolism: lactate production for carcinogenesis could be the purpose and explanation of the Warburg Effect. Carcinog. 2016, 38, 119–133. [Google Scholar] [CrossRef]
- Nagayama, Y.; Hamada, K. Reprogramming of Cellular Metabolism and Its Therapeutic Applications in Thyroid Cancer. Metabolites 2022, 12, 1214. [Google Scholar] [CrossRef]
- Abooshahab, R.; Gholami, M.; Sanoie, M.; Azizi, F.; Hedayati, M. Advances in metabolomics of thyroid cancer diagnosis and metabolic regulation. Endocrine 2019, 65, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Abooshahab, R.; Ardalani, H.; Zarkesh, M.; Hooshmand, K.; Bakhshi, A.; Dass, C.R.; Hedayati, M. Metabolomics—A Tool to Find Metabolism of Endocrine Cancer. Metabolites 2022, 12, 1154. [Google Scholar] [CrossRef] [PubMed]
- Coelho, M.; Raposo, L.; Goodfellow, B.J.; Atzori, L.; Jones, J.; Manadas, B. The Potential of Metabolomics in the Diagnosis of Thyroid Cancer. Int. J. Mol. Sci. 2020, 21, 5272. [Google Scholar] [CrossRef] [PubMed]
- Neto, V.; Esteves-Ferreira, S.; Inácio, I.; Alves, M.; Dantas, R.; Almeida, I.; Guimarães, J.; Azevedo, T.; Nunes, A. Metabolic Profile Characterization of Different Thyroid Nodules Using FTIR Spectroscopy: A Review. Metabolites 2022, 12, 53. [Google Scholar] [CrossRef]
- Razavi, S.A.; Khorsand, B.; Salehipour, P.; Hedayati, M. Metabolite signature of human malignant thyroid tissue: A systematic review and meta-analysis. Cancer Med. 2024, 13, e7184. [Google Scholar] [CrossRef]
- Razavi, S.A.; Kalari, M.; Haghzad, T.; Haddadi, F.; Nasiri, S.; Hedayati, M. Exploring the potential of myo-inositol in thyroid disease management: focus on thyroid cancer diagnosis and therapy. Front. Endocrinol. 2024, 15, 1418956. [Google Scholar] [CrossRef]
- Lan, L.; Luo, Y.; Zhou, M.; Huo, L.; Chen, H.; Zuo, Q.; Deng, W. Comparison of Diagnostic Accuracy of Thyroid Cancer With Ultrasound-Guided Fine-Needle Aspiration and Core-Needle Biopsy: A Systematic Review and Meta-Analysis. Front. Endocrinol. 2020, 11, 44. [Google Scholar] [CrossRef]
- Razavi, S.A.; Mahmanzar, M.; Gh. , B.F.N.M.; Zamani, Z.; Nasiri, S.; Hedayati, M. Plasma metabolites analysis of patients with papillary thyroid cancer: A preliminary untargeted 1H NMR-based metabolomics. J. Pharm. Biomed. Anal. 2023, 241, 115946. [Google Scholar] [CrossRef]
- Yu, S.; Liu, C.; Hou, Y.; Li, J.; Guo, Z.; Chen, X.; Zhang, L.; Peng, S.; Hong, S.; Xu, L.; et al. Integrative metabolomic characterization identifies plasma metabolomic signature in the diagnosis of papillary thyroid cancer. Oncogene 2022, 41, 2422–2430. [Google Scholar] [CrossRef]
- D’andréa, G.; Jing, L.; Peyrottes, I.; Guigonis, J.-M.; Graslin, F.; Lindenthal, S.; Sanglier, J.; Gimenez, I.; Haudebourg, J.; Vandersteen, C.; et al. Pilot Study on the Use of Untargeted Metabolomic Fingerprinting of Liquid-Cytology Fluids as a Diagnostic Tool of Malignancy for Thyroid Nodules. Metabolites 2023, 13, 782. [Google Scholar] [CrossRef]
- Rezig, L.; Servadio, A.; Torregrossa, L.; Miccoli, P.; Basolo, F.; Shintu, L.; Caldarelli, S. Diagnosis of post-surgical fine-needle aspiration biopsies of thyroid lesions with indeterminate cytology using HRMAS NMR-based metabolomics. Metabolomics 2018, 14, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Ryoo, I.; Kwon, H.; Kim, S.C.; Jung, S.C.; A Yeom, J.; Shin, H.S.; Cho, H.R.; Yun, T.J.; Choi, S.H.; Sohn, C.-H.; et al. Metabolomic analysis of percutaneous fine-needle aspiration specimens of thyroid nodules: Potential application for the preoperative diagnosis of thyroid cancer. Sci. Rep. 2016, 6, 30075. [Google Scholar] [CrossRef] [PubMed]
- Torregrossa, L.; Shintu, L.; Chandran, J.N.; Tintaru, A.; Ugolini, C.; Magalhães, A.; Basolo, F.; Miccoli, P.; Caldarelli, S. Toward the Reliable Diagnosis of Indeterminate Thyroid Lesions: A HRMAS NMR-Based Metabolomics Case of Study. J. Proteome Res. 2012, 11, 3317–3325. [Google Scholar] [CrossRef] [PubMed]
- Planque, M.; Igelmann, S.; Campos, A.M.F.; Fendt, S.-M. Spatial metabolomics principles and application to cancer research. Curr. Opin. Chem. Biol. 2023, 76, 102362. [Google Scholar] [CrossRef]
- Min, X.; Zhao, Y.; Yu, M.; Zhang, W.; Jiang, X.; Guo, K.; Wang, X.; Huang, J.; Li, T.; Sun, L.; et al. Spatially resolved metabolomics: From metabolite mapping to function visualising. Clin. Transl. Med. 2024, 14, e70031. [Google Scholar] [CrossRef]
- Wojakowska, A. , et al., Discrimination of papillary thyroid cancer from non-cancerous thyroid tissue based on lipid profiling by mass spectrometry imaging. Endokrynol Pol 2018, 69, 2–8. [Google Scholar] [CrossRef]
- DeHoog, R.J. , et al., Preoperative metabolic classification of thyroid nodules using mass spectrometry imaging of fine-needle aspiration biopsies. Proc Natl Acad Sci U S A 2019, 116, 21401–21408. [Google Scholar] [CrossRef]
- Wallace, E.N.; West, C.A.; McDowell, C.T.; Lu, X.; Bruner, E.; Mehta, A.S.; Aoki-Kinoshita, K.F.; Angel, P.M.; Drake, R.R. An N-glycome tissue atlas of 15 human normal and cancer tissue types determined by MALDI-imaging mass spectrometry. Sci. Rep. 2024, 14, 1–15. [Google Scholar] [CrossRef]
- Mao, X.; Huang, L.; Li, T.; Abliz, Z.; He, J.; Chen, J. Identification of Diagnostic Metabolic Signatures in Thyroid Tumors Using Mass Spectrometry Imaging. Molecules 2023, 28, 5791. [Google Scholar] [CrossRef]
- Khatami, F.; Payab, M.; Sarvari, M.; Gilany, K.; Larijani, B.; Arjmand, B.; Tavangar, S.M. Oncometabolites as biomarkers in thyroid cancer: a systematic review. Cancer Manag. Res. 2019, 11, 1829–1841. [Google Scholar] [CrossRef]
- Abooshahab, R.; Razavi, F.; Ghorbani, F.; Hooshmand, K.; Zarkesh, M.; Hedayati, M. Thyroid cancer cell metabolism: A glance into cell culture system-based metabolomics approaches. Exp. Cell Res. 2024, 435, 113936. [Google Scholar] [CrossRef]
- Berinde, G.M.; Socaciu, A.I.; Socaciu, M.A.; Petre, G.E.; Socaciu, C.; Piciu, D. Metabolic Profiles and Blood Biomarkers to Discriminate between Benign Thyroid Nodules and Papillary Carcinoma, Based on UHPLC-QTOF-ESI+-MS Analysis. Int. J. Mol. Sci. 2024, 25, 3495. [Google Scholar] [CrossRef] [PubMed]
- Berinde, G.M.; Socaciu, A.I.; Socaciu, M.A.; Petre, G.E.; Rajnoveanu, A.G.; Barsan, M.; Socaciu, C.; Piciu, D. In Search of Relevant Urinary Biomarkers for Thyroid Papillary Carcinoma and Benign Thyroid Nodule Differentiation, Targeting Metabolic Profiles and Pathways via UHPLC-QTOF-ESI+-MS Analysis. Diagnostics 2024, 14, 2421. [Google Scholar] [CrossRef] [PubMed]
- Li, L.; Wen, X.; Li, X.; Yan, Y.; Wang, J.; Zhao, X.; Tian, Y.; Ling, R.; Duan, Y. Identifying potential breath biomarkers for early diagnosis of papillary thyroid cancer based on solid-phase microextraction gas chromatography-high resolution mass spectrometry with metabolomics. Metabolomics 2024, 20, 1–13. [Google Scholar] [CrossRef]
- Zhang, J.; Wen, X.; Li, Y.; Li, X.; Qian, C.; Tian, Y.; Ling, R.; Duan, Y. Diagnostic approach to thyroid cancer based on amino acid metabolomics in saliva by ultra-performance liquid chromatography with high resolution mass spectrometry. Talanta 2021, 235, 122729. [Google Scholar] [CrossRef]
- Chen, J.; Hu, Q.; Hou, H.; Wang, S.; Zhang, Y.; Luo, Y.; Chen, H.; Deng, H.; Zhu, H.; Zhang, L.; et al. Metabolite analysis-aided diagnosis of papillary thyroid cancer. Endocrine-Related Cancer 2019, 26, 829–841. [Google Scholar] [CrossRef]
- Liu, Z.; Zhang, W.; Wang, C.; Wang, X.; Luo, J.; He, Y.; Zhang, Y.; Chen, S.; Zhou, Q.; Sun, D.; et al. Study on identification of diagnostic biomarkers in serum for papillary thyroid cancer in different iodine nutrition regions. Biomarkers 2024, 1–10. [Google Scholar] [CrossRef]
- Wang, F.; Lin, Y.; Qin, L.; Zeng, X.; Jiang, H.; Liang, Y.; Wen, S.; Li, X.; Huang, S.; Li, C.; et al. Serum metabolome associated with novel and legacy per- and polyfluoroalkyl substances exposure and thyroid cancer risk: A multi-module integrated analysis based on machine learning. Environ. Int. 2024, 195, 109203. [Google Scholar] [CrossRef]
- Song, J.; Liu, Y.; Peng, J.; Jiang, Y.; Lin, X.; Zhang, J. Identification of serum metabolites associated with polybrominated diphenyl ethers (PBDEs) exposure in papillary thyroid carcinoma: a case–control study. Environ. Geochem. Heal. 2024, 46, 1–14. [Google Scholar] [CrossRef]
- Zhao, M.; Li, R.; Miao, C.; Miccoli, P.; Lu, J. Non-invasive diagnosis of papillary thyroid microcarcinoma using a novel metabolomics analysis of urine. Endocrine 2024, 1–12. [Google Scholar] [CrossRef]
- Wojakowska, A.; Chekan, M.; Marczak, Ł.; Polanski, K.; Lange, D.; Pietrowska, M.; Widlak, P. Detection of metabolites discriminating subtypes of thyroid cancer: Molecular profiling of FFPE samples using the GC/MS approach. Mol. Cell. Endocrinol. 2015, 417, 149–157. [Google Scholar] [CrossRef] [PubMed]
- Baloch, Z.W.; Asa, S.L.; Barletta, J.A.; Ghossein, R.A.; Juhlin, C.C.; Jung, C.K.; LiVolsi, V.A.; Papotti, M.G.; Sobrinho-Simões, M.; Tallini, G.; et al. Overview of the 2022 WHO Classification of Thyroid Neoplasms. Endocr. Pathol. 2022, 33, 27–63. [Google Scholar] [CrossRef] [PubMed]
- Qu, N.; Chen, D.; Ma, B.; Zhang, L.; Wang, Q.; Wang, Y.; Wang, H.; Ni, Z.; Wang, W.; Liao, T.; et al. Integrated proteogenomic and metabolomic characterization of papillary thyroid cancer with different recurrence risks. Nat. Commun. 2024, 15, 1–18. [Google Scholar] [CrossRef]
- Chai, Y.J.; Yi, J.W.; Oh, S.W.; A Kim, Y.; Yi, K.H.; Kim, J.H.; Lee, K.E. Upregulation of SLC2 (GLUT) family genes is related to poor survival outcomes in papillary thyroid carcinoma: Analysis of data from The Cancer Genome Atlas. Surgery 2017, 161, 188–194. [Google Scholar] [CrossRef]
- Wen, S.; i Luo, Y.; Wu, W.; Zhang, T.; Yang, Y.; Ji, Q.; Wu, Y.; Shi, R.; Ma, B.; Xu, M.; et al. Identification of lipid metabolism-related genes as prognostic indicators in papillary thyroid cancer. Acta Biochim. et Biophys. Sin. 2021, 53, 1579–1589. [Google Scholar] [CrossRef]
- Ban, E.J.; Kim, D.; Kim, J.K.; Kang, S.-W.; Lee, J.; Jeong, J.J.; Nam, K.-H.; Chung, W.Y.; Kim, K. Lactate Dehydrogenase A as a Potential New Biomarker for Thyroid Cancer. Endocrinol. Metab. 2021, 36, 96–105. [Google Scholar] [CrossRef]
- Wang, Z.; Wang, F. Construction and evaluation of a prognosis prediction model for thyroid carcinoma based on lipid metabolism-related genes. 2022, 43, 323–332. [Google Scholar]
- Enomoto, K.; Hotomi, M. Amino Acid Transporters as Potential Therapeutic Targets in Thyroid Cancer. Endocrinol. Metab. 2020, 35, 227–236. [Google Scholar] [CrossRef]
- Huang, J.; Sun, W.; Wang, Z.; Lv, C.; Zhang, T.; Zhang, D.; Dong, W.; Shao, L.; He, L.; Ji, X.; et al. FTO suppresses glycolysis and growth of papillary thyroid cancer via decreasing stability of APOE mRNA in an N6-methyladenosine-dependent manner. J. Exp. Clin. Cancer Res. 2022, 41, 1–18. [Google Scholar] [CrossRef]
- Lee, S.E.; Park, S.; Yi, S.; Choi, N.R.; Lim, M.A.; Chang, J.W.; Won, H.-R.; Kim, J.R.; Ko, H.M.; Chung, E.-J.; et al. Unraveling the role of the mitochondrial one-carbon pathway in undifferentiated thyroid cancer by multi-omics analyses. Nat. Commun. 2024, 15, 1–17. [Google Scholar] [CrossRef]
- Huang, Y.; Du, J.; Li, D.; He, W.; Liu, Z.; Liu, L.; Yang, X.; Cheng, X.; Chen, R.; Yang, Y. LASS2 suppresses metastasis in multiple cancers by regulating the ferroptosis signalling pathway through interaction with TFRC. Cancer Cell Int. 2024, 24, 1–19. [Google Scholar] [CrossRef] [PubMed]
- Xu, B.; Gao, W.; Xu, T.; Liu, C.; Wu, D.; Tang, W. A UPLC Q-Exactive Orbitrap Mass Spectrometry-Based Metabolomic Study of Serum and Tumor Tissue in Patients with Papillary Thyroid Cancer. Toxics 2022, 11, 44. [Google Scholar] [CrossRef] [PubMed]
- Seo, J.W.; Han, K.; Lee, J.; Kim, E.-K.; Moon, H.J.; Yoon, J.H.; Park, V.Y.; Baek, H.-M.; Kwak, J.Y. Application of metabolomics in prediction of lymph node metastasis in papillary thyroid carcinoma. PLOS ONE 2018, 13, e0193883. [Google Scholar] [CrossRef]
- Shen, C.; Zhang, Y.; Liu, Y.; Yin, S.; Zhang, X.; Wei, W.; Sun, Z.; Song, H.; Qiu, Z.; Wang, C.; et al. A distinct serum metabolic signature of distant metastatic papillary thyroid carcinoma. Clin. Endocrinol. 2017, 87, 844–852. [Google Scholar] [CrossRef] [PubMed]
- Cararo Lopes, E. , et al. , Integrated metabolic and genetic analysis reveals distinct features of human differentiated thyroid cancer. Clin Transl Med. 2023, 13, e1298. [Google Scholar]
- Ouyang, J.; Feng, Y.; Zhang, Y.; Liu, Y.; Li, S.; Wang, J.; Tan, L.; Zou, L. Integration of metabolomics and transcriptomics reveals metformin suppresses thyroid cancer progression via inhibiting glycolysis and restraining DNA replication. Biomed. Pharmacother. 2023, 168, 115659. [Google Scholar] [CrossRef]
- Thakur, S.; Daley, B.; Gaskins, K.; Vasko, V.V.; Boufraqech, M.; Patel, D.; Sourbier, C.; Reece, J.; Cheng, S.-Y.; Kebebew, E.; et al. Metformin Targets Mitochondrial Glycerophosphate Dehydrogenase to Control Rate of Oxidative Phosphorylation and Growth of Thyroid Cancer In Vitro and In Vivo. Clin. Cancer Res. 2018, 24, 4030–4043. [Google Scholar] [CrossRef]
- Zheng, W.; Tang, X.; Dong, J.; Feng, J.; Chen, M.; Zhu, X. Metabolomic screening of radioiodine refractory thyroid cancer patients and the underlying chemical mechanism of iodine resistance. Sci. Rep. 2024, 14, 1–13. [Google Scholar] [CrossRef]
- Wang, J.; Xu, Q.; Xuan, Z.; Mao, Y.; Tang, X.; Yang, K.; Song, F.; Zhu, X. Metabolomics reveals the implication of acetoacetate and ketogenic diet therapy in radioiodine-refractory differentiated thyroid carcinoma. Oncol. 2024, 29, e1120–e1131. [Google Scholar] [CrossRef]
- Yu, Y.; Ning, K.; Liu, X.; Liang, Y.; Jiao, Z.; Zou, B.; Cai, T.; Yang, Z.; Chen, W.; Wu, T.; et al. Per- and polyfluoroalkyl substances (PFAS) exposure is associated with radioiodine therapy resistance and dedifferentiation of differentiated thyroid cancer. Environ. Pollut. 2025, 367, 125629. [Google Scholar] [CrossRef]
- Lu, G.; Gao, D.; Liu, Y.; Yu, X.; Jiang, W.; Lv, Z. Early and long-term responses of intestinal microbiota and metabolites to 131I treatment in differentiated thyroid cancer patients. BMC Med. 2024, 22, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Lu, G.; Gao, D.; Jiang, W.; Yu, X.; Tong, J.; Liu, X.; Qiao, T.; Wang, R.; Zhang, M.; Wang, S.; et al. Disrupted gut microecology after high-dose 131I therapy and radioprotective effects of arachidonic acid supplementation. Eur. J. Nucl. Med. 2024, 51, 2395–2408. [Google Scholar] [CrossRef] [PubMed]
- Kumari, S.; Thakur, S.; Cardenas, S.; Makarewicz, A.; Klubo-Gwiezdzinska, J. Metabolic Reprogramming Contributes to Resistance Towards Lenvatinib in Thyroid Cancer. VideoEndocrinology 2024, 11, 54–56. [Google Scholar] [CrossRef]
- Xu, Q.; Wang, J.; Mao, Y.; Xuan, Z.; Yang, K.; Tang, X.; Zhu, X. Combined BRAF and PIM1 inhibitory therapy for papillary thyroid carcinoma based on BRAFV600E regulation of PIM1: Synergistic effect and metabolic mechanisms. Neoplasia 2024, 52, 100996. [Google Scholar] [CrossRef]
- Liu, B.; Peng, Y.; Su, Y.; Diao, C.; Qian, J.; Zhan, X.; Cheng, R. Transcriptome and metabolome sequencing identifies glutamate and LPAR1 as potential factors of anlotinib resistance in thyroid cancer. Anti-Cancer Drugs 2024, 35, 741–751. [Google Scholar] [CrossRef]
- Lin, Y.H. C. Lin, and C.C. Chen, Lysophosphatidic Acid Receptor Antagonists and Cancer: The Current Trends, Clinical Implications, and Trials. Cells 2021, 10. [Google Scholar] [CrossRef]
- Kuang, A.; Kouznetsova, V.L.; Kesari, S.; Tsigelny, I.F. Diagnostics of Thyroid Cancer Using Machine Learning and Metabolomics. Metabolites 2023, 14, 11. [Google Scholar] [CrossRef]
- Kurashige, T.; Shimamura, M.; Hamada, K.; Matsuse, M.; Mitsutake, N.; Nagayama, Y. Characterization of metabolic reprogramming by metabolomics in the oncocytic thyroid cancer cell line XTC.UC1. Sci. Rep. 2023, 13, 1–11. [Google Scholar] [CrossRef]
- Kumari, S.; Adewale, R.; Klubo-Gwiezdzinska, J. The Molecular Landscape of Hürthle Cell Thyroid Cancer Is Associated with Altered Mitochondrial Function—A Comprehensive Review. Cells 2020, 9, 1570. [Google Scholar] [CrossRef]
- Tronci, L.; Serreli, G.; Piras, C.; Frau, D.V.; Dettori, T.; Deiana, M.; Murgia, F.; Santoru, M.L.; Spada, M.; Leoni, V.P.; et al. Vitamin C Cytotoxicity and Its Effects in Redox Homeostasis and Energetic Metabolism in Papillary Thyroid Carcinoma Cell Lines. Antioxidants 2021, 10, 809. [Google Scholar] [CrossRef]
- Chen, J.; Yu, X.; Qu, Y.; Wang, X.; Wang, Y.; Jia, K.; Du, Q.; Han, J.; Liu, H.; Zhang, X.; et al. High-Performance Metabolic Profiling of High-Risk Thyroid Nodules by ZrMOF Hybrids. ACS Nano 2024, 18, 21336–21346. [Google Scholar] [CrossRef] [PubMed]
- Cristiani, S.; Bertolini, A.; Carnicelli, V.; Contu, L.; Vitelli, V.; Saba, A.; Saponaro, F.; Chiellini, G.; Sabbatini, A.R.M.; Giambelluca, M.A.; et al. Development and primary characterization of a human thyroid organoid in vitro model for thyroid metabolism investigation. Mol. Cell. Endocrinol. 2024, 594, 112377. [Google Scholar] [CrossRef] [PubMed]
- Yang, H.; Liang, Q.; Zhang, J.; Liu, J.; Wei, H.; Chen, H.; Wei, W.; Chen, D.; Zhao, Y. Establishment of papillary thyroid cancer organoid lines from clinical specimens. Front. Endocrinol. 2023, 14, 1140888. [Google Scholar] [CrossRef] [PubMed]
- Chen, D.; Tan, Y.; Li, Z.; Li, W.; Yu, L.; Chen, W.; Liu, Y.; Liu, L.; Guo, L.; Huang, W.; et al. Organoid Cultures Derived From Patients With Papillary Thyroid Cancer. J. Clin. Endocrinol. Metab. 2021, 106, 1410–1426. [Google Scholar] [CrossRef]
- Dhuli, K.; Medori, M.C.; Donato, K.; E Maltese, P.; Tanzi, B.; Tezzele, S.; Mareso, C.; Miertus, J.; Generali, D.; A Donofrio, C.; et al. Omics sciences and precision medicine in thyroid cancer. . 2023, 174, 11–20. [Google Scholar] [CrossRef]
- Al-Jundi, M.; Thakur, S.; Gubbi, S.; Klubo-Gwiezdzinska, J. Novel Targeted Therapies for Metastatic Thyroid Cancer—A Comprehensive Review. Cancers 2020, 12, 2104. [Google Scholar] [CrossRef]
- Boufraqech, M.; Nilubol, N. Multi-omics Signatures and Translational Potential to Improve Thyroid Cancer Patient Outcome. Cancers 2019, 11, 1988. [Google Scholar] [CrossRef]
- Gulfidan, G.; Soylu, M.; Demirel, D.; Erdonmez, H.B.C.; Beklen, H.; Sarica, P.O.; Arga, K.Y.; Turanli, B. Systems biomarkers for papillary thyroid cancer prognosis and treatment through multi-omics networks. Arch. Biochem. Biophys. 2021, 715, 109085. [Google Scholar] [CrossRef]
Figure 1.
Strategy utilized for literature search and screening process.
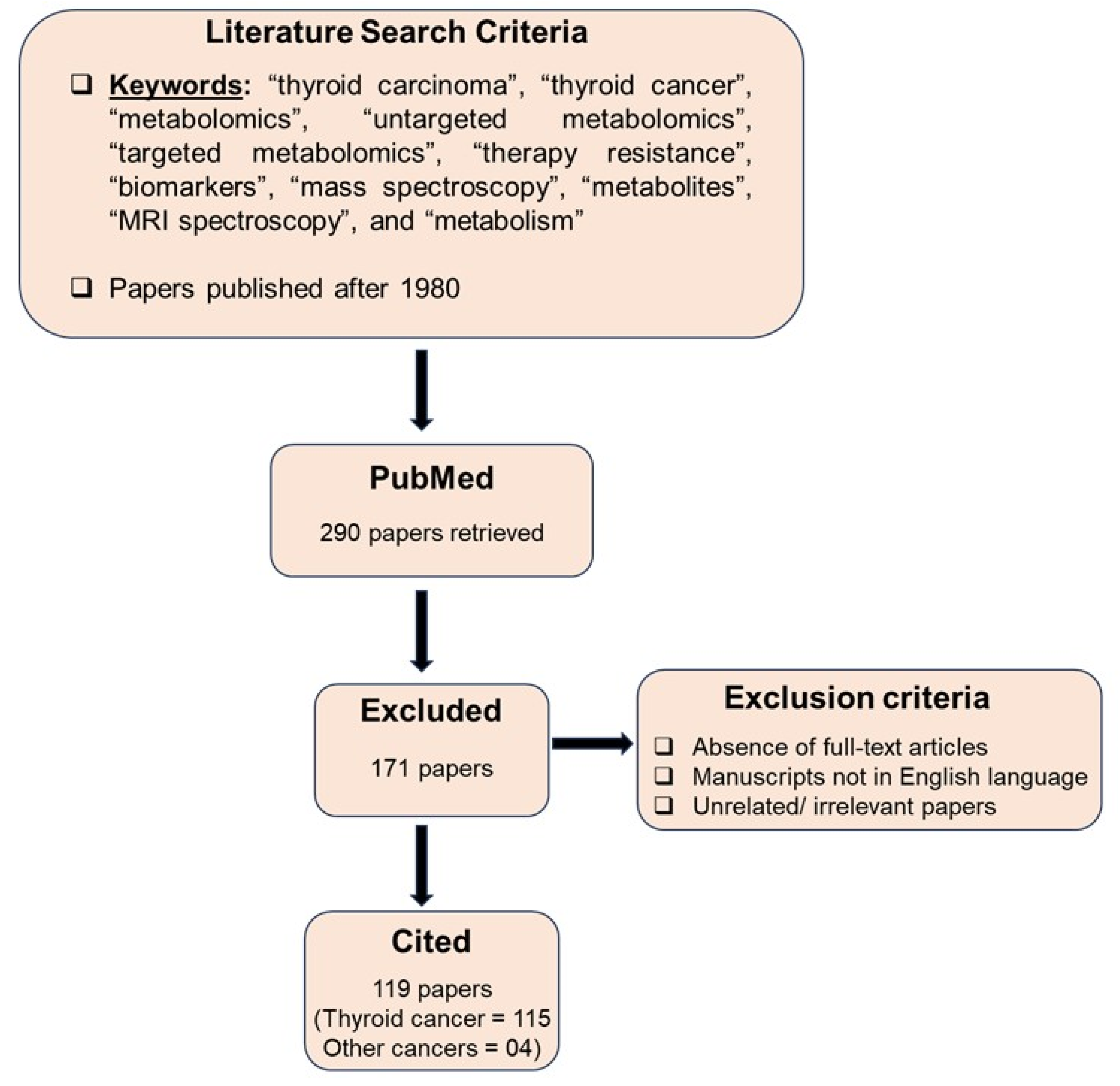
Figure 2.
Difference between untargeted and targeted metabolomics. (Biorender software was utilized for preparing the figure.).
Figure 2.
Difference between untargeted and targeted metabolomics. (Biorender software was utilized for preparing the figure.).
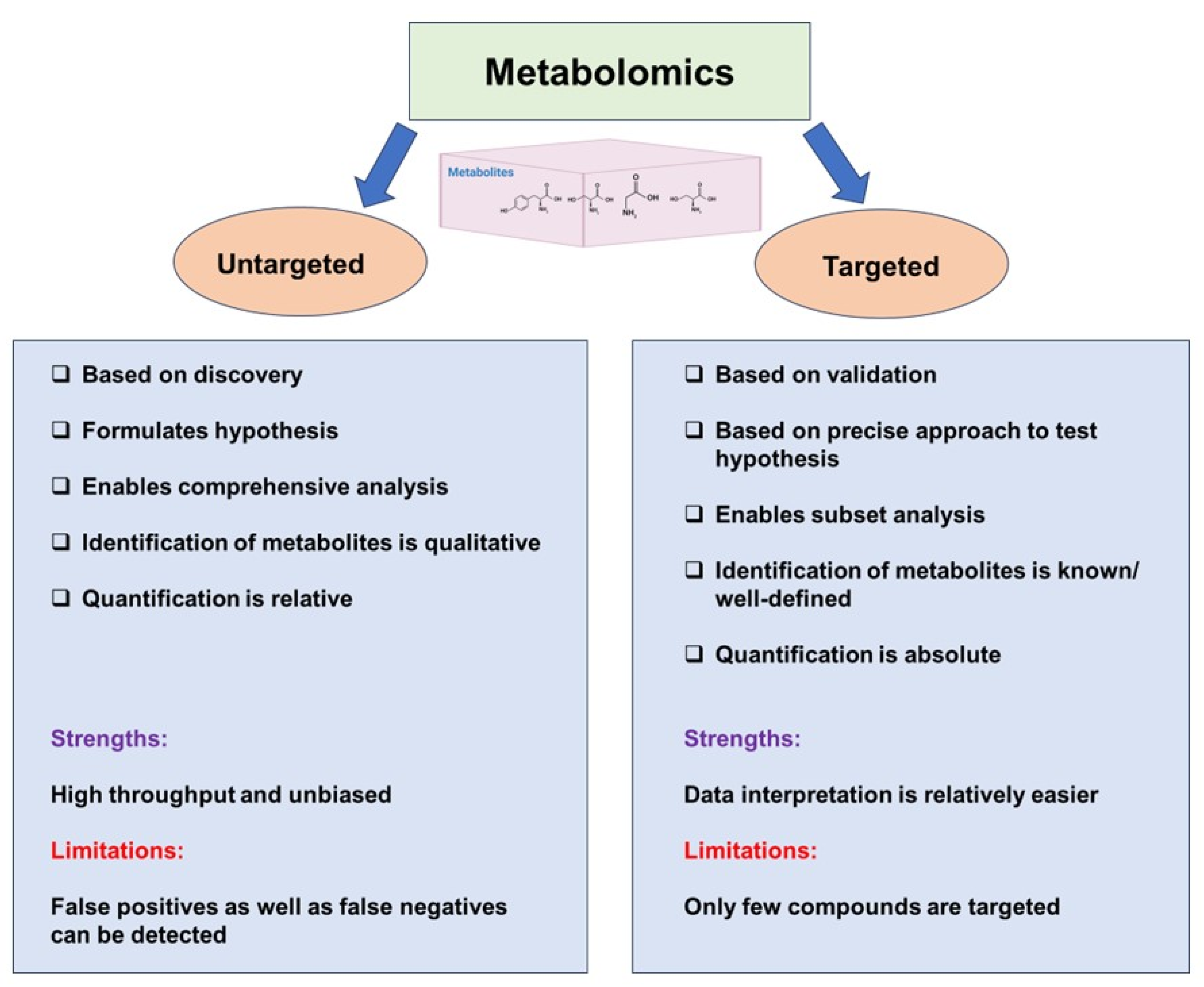
Figure 3.
Comparison of the various analytical techniques employed for metabolomics.
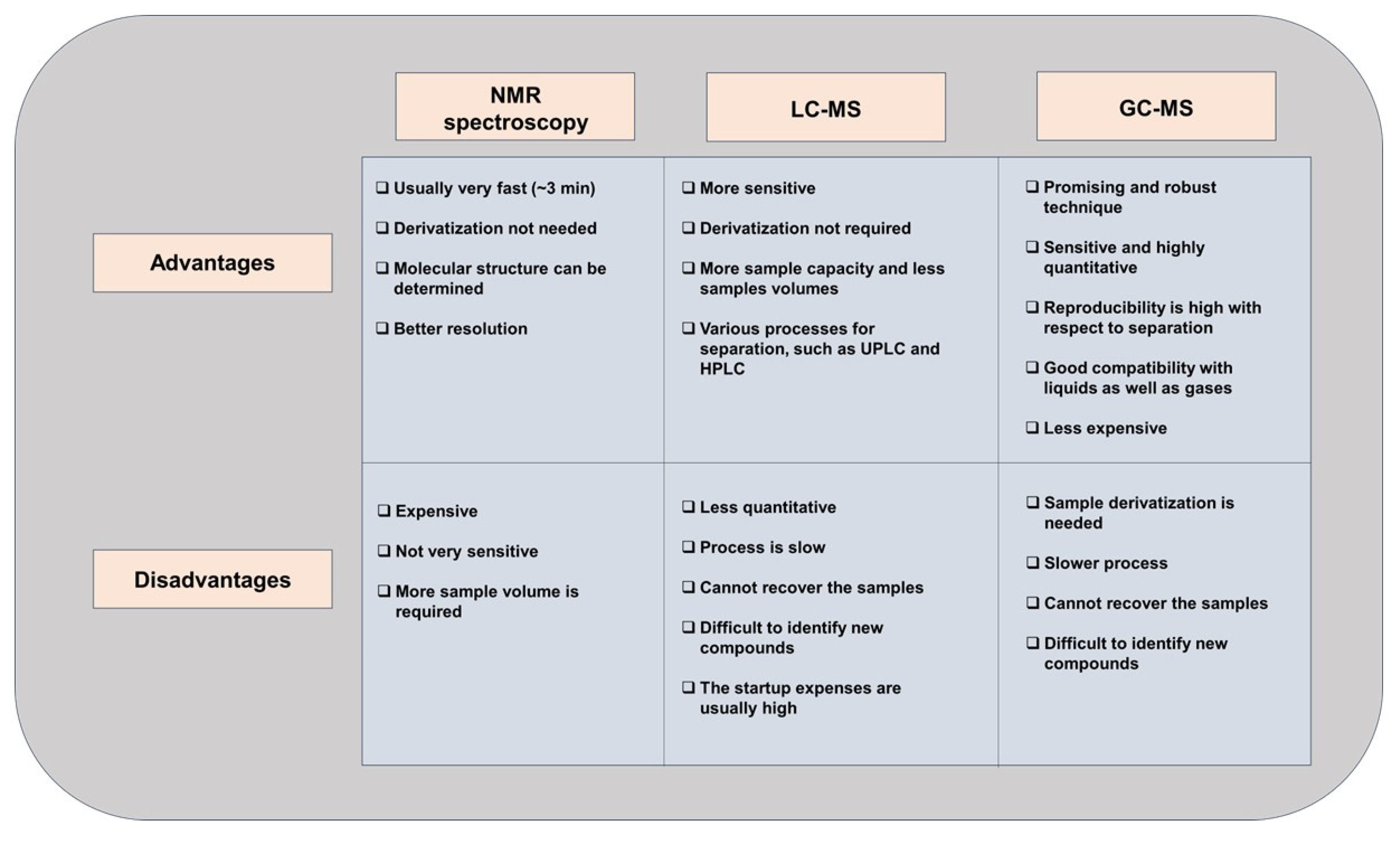
Figure 4.
Experimental procedure for metabolomics analysis. (The figure was prepared using Biorender software).
Figure 4.
Experimental procedure for metabolomics analysis. (The figure was prepared using Biorender software).
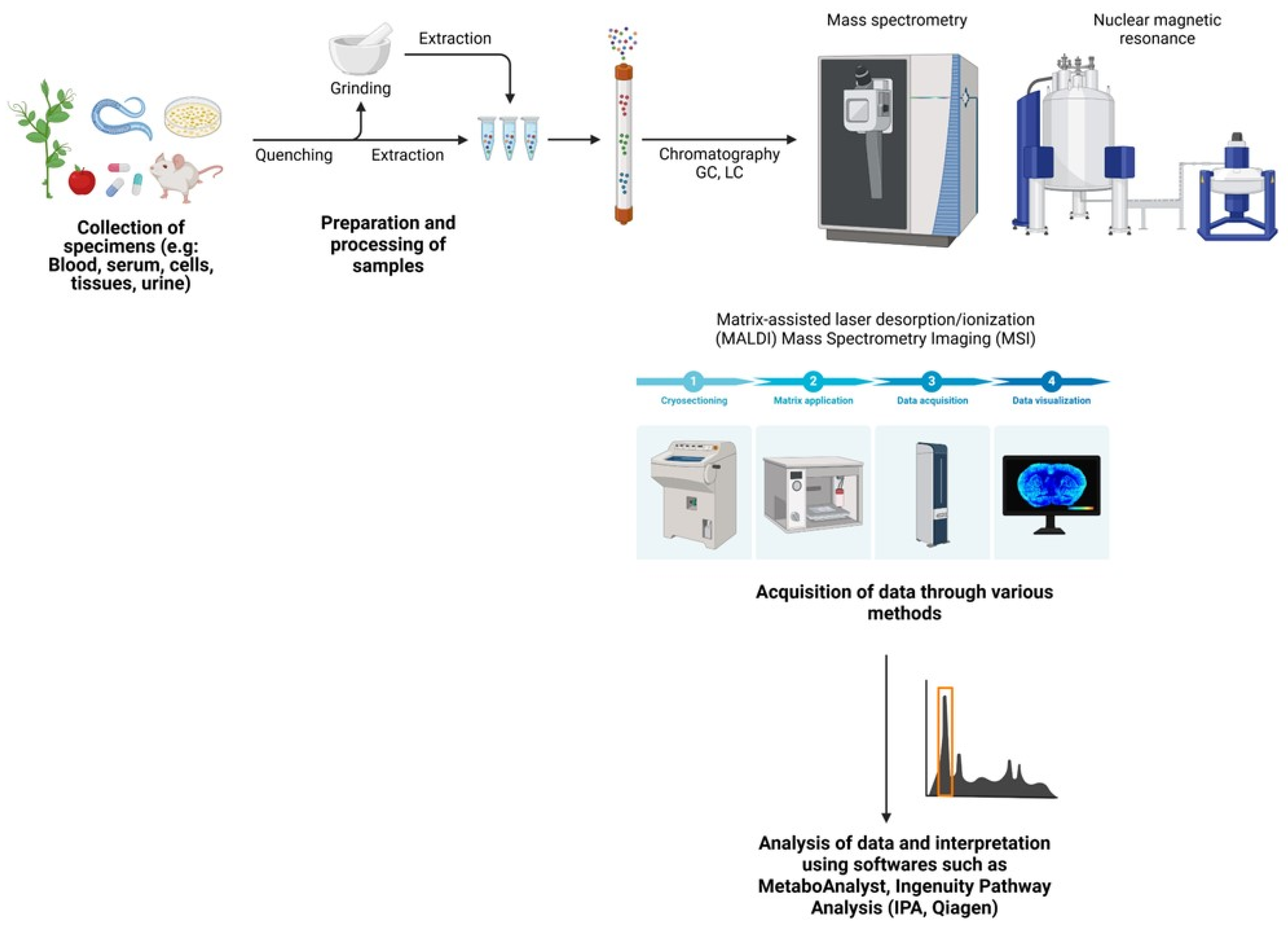
Figure 5.
The most important applications of metabolomics in the field of cancer research.

Table 1.
Emerging Trends in Metabolomics Thyroid Cancer Research.
| Reference | Review Design | Biospecimen used | Significantly Altered Metabolites |
|---|---|---|---|
| Khatami et al., 2019 [71] |
Systematic review of 31 metabolomic studies (15 targeted and 16 untargeted) investigating metabolite biomarkers of TC. All metabolomic techniques included in search criteria. | Plasma, serum, urine, or FNA specimens. Malignant TC vs. control (healthy, benign nodules, goiter) |
Citrate ↓ Lactate ↑ |
| Abooshahab et al., 2022 [53] |
Systematic review of metabolomics in endocrine cancers. 35 articles published from 2010-2022 on thyroid cancer metabolomics. Techniques included NMR (15 papers), GC/MS (8 papers), and LC/MS (12 papers). | Tissue, serum/plasma, urine, FNA samples Malignant vs. benign tumors |
Lactate ↑ Choline ↓ Mono- and disaccharides, and TCA intermediates altered |
| Coelho et al., 2020 [54] |
Review includes 45 original studies on TC metabolomic biomarkers. NMR (21 papers), MS (19 papers), other techniques (5 papers). Spatial metabolomics applied in several listed studies. | Tissue, plasma, serum, urine, feces, breath TC vs. healthy/benign controls |
Choline ↑ Lactate ↑ Tyrosine ↑ |
| Abooshahab et al., 2024 [72] |
Review of metabolomic studies on TC cell lines. 7 papers identified. MS (6 papers) and NMR (1 paper). | TC cell lines | Various alterations in glycolysis and TCA cycle metabolites |
| Neto et al., 2022 [55] |
Review of studies using FTIR spectroscopy to characterize normal vs. tumor samples. 13 papers met the criteria. | Thyroid tissue and cytology samples | Lipids ↓ Carbohydrates ↓ Lipid metabolism ↑ |
| Razavi et al., 2024 [56] |
Systematic review and meta-analysis of NMR-based metabolomic studies. 12 studies met the search criteria. | Tissue and FNAB specimens. Malignant vs. benign. |
Lactate ↑ Alanine ↑ Citrate ↓ |
| Nagayama et al., 2022 [51] |
Summarize the recent findings of metabolic reprogramming in TC as well as recent reports of metabolism-targeted therapies. | Thyroid tissue and cytology samples | Glucose metabolism ↑ Amino acid metab. ↑ Lipid metabolism ↑ |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



