Submitted:
16 February 2025
Posted:
18 February 2025
You are already at the latest version
Abstract
Background: Understanding vaccine attitudes, knowledge, and perceptions is critical for improving vaccine uptake, particularly among vulnerable populations such as pregnant women. This study aimed to test and adapt the World Health Organization (WHO) Behavioural and Social Drivers (BeSD) tools and the Vaccination Attitudes Examination (VAX) Scale for assessing maternal and childhood vaccine attitudes in the South African context. Methods: We conducted a mixed-methods pilot study among pregnant women attending antenatal care at two public hospitals in Cape Town, South Africa, between September 2023 and January 2024. Quantitative data were collected using a self-administered questionnaire on tablets, incorporating the adapted BeSD and VAX tools, while qualitative data were gathered through semi-structured interviews. Additionally, the quantitative questionnaire contained the General Vaccine Attitude Survey questions developed from the compendium of survey questions created by the World Health Organization Strategic Advisory Group of Experts on Immunization (WHO SAGE) Working Group on Vaccine Hesitancy. Adaptations to the tools were informed by participant feedback and pretesting. Results: Eighty pregnant women agreed to participate in the quantitative survey, one participant dropped out of the study and seven completed follow-up qualitative interviews. The tools were well received, with participants reporting ease of use and understanding. Minor linguistic adjustments improved clarity, and participants identified healthcare providers as key influencers of vaccine decision-making. Knowledge gaps regarding maternal vaccination and concerns about vaccine safety during pregnancy were prominent. The mixed-methods approach provided complementary insights into the tools' applicability and participants' attitudes. Conclusions: This pilot study demonstrated that the WHO BeSD tools and VAX Scale, with minor adaptations, are feasible and acceptable for use in South Africa. These findings support their application in larger studies to explore maternal vaccine confidence and decision-making. Addressing knowledge gaps and leveraging trusted sources of information are critical to enhancing vaccine uptake in similar settings.
Keywords:
maternal vaccines
; routine childhood vaccination
; vaccine attitudes
; WHO BeSD Framework
; VAX Scale
; pilot study
; South Africa
1. Introduction
Infectious diseases are associated with high morbidity and mortality among pregnant women, their fetuses, and infants. During pregnancy and in the first few months of life, mothers and babies experience a naturally lowered immune response, making them more susceptible to various infectious diseases [1,2,3].
In recent years, maternal immunization has gained significant attention from the scientific community. Numerous observational studies have consistently shown that vaccinating women during pregnancy is not only safe but also highly effective as a public health intervention. This strategy provides protection not just for the expectant mother, but also for her developing baby in the early months of life [4,5,6,7,8].
The effectiveness of any vaccination program is related to how well the at-risk population understands the benefits of vaccines and how they work. Insufficient information or misinformation can lead to lower vaccine acceptance among vulnerable groups, such as pregnant women. Understanding their attitudes, experiences, and any concerns or barriers they face is essential, as these factors can significantly influence their decisions regarding vaccination during pregnancy [1,4,9,10,11]. Additionally, vaccine uptake relies not only on the vaccines’ availability and accessibility; other important factors are significant, particularly mothers’ knowledge and attitudes toward maternal and routine childhood vaccines. Personal factors, such as maternal knowledge and attitudes toward vaccination, can greatly influence whether mothers vaccinate themselves and have their children vaccinated, even when services are available and accessible [12,13,14,15]. Understanding how personal beliefs and experiences influence vaccine decision-making among pregnant women is crucial for enhancing vaccine acceptance and coverage in both routine and outbreak contexts. However, most studies have primarily been conducted in high-income countries, resulting in limited data and application of these tools among pregnant women in low- and middle-income countries (LMICs), particularly in African countries [16]. The limited data and research on maternal vaccination in LMICs, especially in African countries, impede the development of context-specific interventions to improve vaccine acceptance. Addressing this gap is crucial for designing effective strategies that can increase vaccination coverage among pregnant women and ensure the successful implementation of recommended vaccines in routine care. Therefore, this study will for the first time test the feasibility of the General Attitudes Toward Vaccine Survey questions developed by the WHO SAGE working group on vaccine hesitancy [17]; the Vaccination Attitudes Examination (VAX) Scale [18]; and the WHO Behavioural and Social Drivers of Vaccination (BeSD) COVID-19 and Childhood Vaccination survey tools [19] among pregnant women in Cape Town, South Africa. Besides, we aimed to assess if these tools are deemed understandable and acceptable by the study participants.
2. Materials and Methods
2.1. Study Design and Setting
In preparation for a prospective mixed-methods cohort study, a pilot study was conducted to assess the feasibility, acceptability, and usability of the adapted tools.
We conducted a mixed-method cross-sectional pilot study in the Cape Metro West Region in Cape Town, South Africa to test and adapt the General Attitudes Toward Vaccine Survey questions developed by the WHO SAGE working group on vaccine hesitancy [17]; the Vaccination Attitudes Examination (VAX) Scale [18]; and the WHO Behavioural and Social Drivers of Vaccination (BeSD) COVID-19 and Childhood Vaccination survey tools [19]. The cross-sectional sample population was randomly drawn from pregnant women attending their routine antenatal visits at secondary and tertiary public hospitals between September 2023 and January 2024.
2.2. Study Population and Recruitment
Pregnant women aged 18 and above presenting to antenatal clinics at these health facilities were invited to participate in the study regardless of the pregnancy trimester. Pregnant women under 18, who were not South African citizens or residents of the city of Cape Town, and who did not speak English, IsiXhosa, or Afrikaans were excluded from the study. In addition, pregnant women who were unable to provide consent forms were excluded.
A trained research assistant approached pregnant women while they were waiting for their appointments at the antenatal clinics, screened participants for eligibility, provided them with an information sheet, and informed them that their participation was voluntary. They were also told that they could withdraw from the study at any time and that their decision on whether to participate would not affect the care they received at the clinic. Pregnant women who agreed to participate signed a written informed consent form.
Given the pilot nature of this study, a sample size calculation was not performed; however, we considered 10% (n=81) of the estimated sample size for the prospective mixed-methods cohort study (n=810).
2.3. Adaptation of Tools and Instruments
In 2018, the WHO introduced the BeSD framework and tools to assist policymakers, healthcare managers, and researchers in conducting a comprehensive analysis of the factors influencing vaccine acceptance and uptake [20]. Using these tools, programs can assess vaccine uptake, track trends over time, and systematically gather data to design, implement, and evaluate targeted interventions aimed at reducing hesitancy and improving vaccination rates.
The Vaccination Attitudes Examination (VAX) Scale is a tool designed to evaluate general attitudes toward vaccines. Its development focused on identifying anti-vaccination attitudes that are predictive of vaccination behavior [18]. Four key attitudes were identified: (1) mistrust of vaccine benefit, (2) worries over unforeseen future effects, (3) concerns about commercial profiteering and (4) preference for natural immunity. These four factors cover a broad range of anti-vaccination sentiments, making the VAX scale highly effective in identifying individuals who are resistant to vaccination [21].
The BeSD framework and tools focus on measurable factors at the individual level, specifically related to vaccination. It is organized into four domains. The "thinking-and-feeling" domain examines individuals' perceptions of the risks posed by diseases and their confidence in the vaccine, including their trust in its safety and benefits. The "social processes" domain explores the influence of social norms on vaccination, such as recommendations from healthcare providers. The "motivation" domain centers on individuals' intention to get vaccinated, while the "practical issues" domain addresses their experiences with the vaccination process [20]. The full framework includes multiple questions for each domain, whereas a simplified version uses a single priority question per domain.
Although various factors impact vaccine decision-making, the BeSD framework is regarded as an effective tool for researchers, healthcare managers, and policymakers to better understand the motivations behind vaccination intentions and uptake. Its focus on measurable drivers allows it to guide decisions related to program implementation, monitoring, and evaluation [20].
The General Attitudes Toward Vaccine Survey questions developed from the compendium of survey questions created by the WHO SAGE working group on vaccine hesitancy [17] and have been previously adapted to maternal vaccines [22,23].
The quantitative questionnaire covers participants’ demographics and obstetric history, the VAX scale [18], the BeSD of COVID-19 vaccination tools and the BeSD priority indicators for routine childhood vaccines, based on the WHO BeSD vaccination framework [20], and the General Attitudes Toward Vaccine Survey questions [20].
For the qualitative component, we developed an interview guide to assess participants’ understanding including attitudes and beliefs, and to test their ability to engage with the interview guide content using the following BeSD domains: “thinking and feeling”; “social processes”; “motivation”, and “pragmatic issues” [20].
At the start of the study, the English version of the quantitative questionnaire and the interview guide were used. After making the required changes, all study documents were translated into IsiXhosa and Afrikaans and then back-translated into English, as these are the three official languages in Western Cape, South Africa [24]. They were tested, and the necessary adjustments were applied. Participants were given the choice of language to complete the questionnaire or conduct the interview. We adapted the survey tools as follows:
- ▪
- For the General Attitudes towards Maternal Vaccines, we applied minor changes to the questions for clarity as follows: “Vaccines given during pregnancy are important for my health,” “All recommended vaccines for pregnant women offered by the government program in my community are beneficial,” and “Recommended vaccines for pregnant women are effective.”
- ▪
- For the VAX scale, a five-point Likert scale “Strongly Disagree”, “Disagree”, “Neutral”, “Agree”, “Strongly Agree” was used instead of a six-point Likert scale, “Strongly Disagree”, “Disagree”, “Somewhat disagree”, “Somewhat agree”, “Agree”, “Strongly Agree”.
- ▪
- For the BeSD COVID-19 tool, the “Reasons for low ease of access,” “Service satisfaction,” and “Service quality” constructs were not included, as the focus of the study was on knowledge and attitudes. Most of the questions were adapted for use among pregnant women. For instance, “How concerned are you about getting COVID-19 during pregnancy?”, “Do you want to get a COVID-19 vaccine during pregnancy?”, and “How safe do you think a COVID-19 vaccine is for you as a pregnant woman?” Minor changes to the multiple-choice options were applied to a few questions, such as “Have you ever been contacted about being due for a COVID-19 vaccine?” (answer options: Yes, before pregnancy; Yes, during this pregnancy; No), etc. We also added the following questions: “Has a health worker recommended you get a COVID-19 vaccine before pregnancy?” as participants might have received a health worker recommendation before pregnancy. We added a question about the reason for receiving the COVID-19 vaccine before pregnancy, a question on whether COVID-19 has been discussed with the participant during the current pregnancy, and a question on what will make the participant confident in accepting the COVID-19 vaccine during pregnancy.
- ▪
- We added "Yes or No" questions about trust in COVID-19 and routine childhood vaccines to compare participants' trust in the different vaccines.
- ▪
- For the interview guide, the following BeSD constructs were explored for both COVID-19 and childhood vaccines: “What people feel and think,” “Motivation,” and “Social processes.”
- ▪
-
Questions about the following topics were added to the interview guide:
- ◦
- Questions about the participants’ knowledge and attitudes towards vaccines in general and vaccination during pregnancy.
- ◦
- Questions regarding COVID-19 vaccine decision-making before pregnancy to compare the participants' attitudes before and during pregnancy.
- ◦
- At the time of the study, the National Department of Health in South Africa was planning to switch from Tetanus-reduced diphtheria (Td), which had been administered during antenatal care, to Tetanus, reduced-strength diphtheria, and acellular pertussis (Tdap) starting in January 2024 [25]. Therefore, we also discussed whether they would accept the Tdap vaccine after being informed about it.
2.4. Data Collection Procedures
Quantitative data was collected through a self-administered structured questionnaire on RedCap [26,27]. The questionnaire had four sections: Section One relates to data on demographics and pregnancy; Section Two concerns participants’ attitudes towards vaccination in general; Section Three contains the WHO BeSD tool for COVID-19 vaccination, and Section Four contains the BeSD tool for childhood vaccination priority indicators. Participants completed the quantitative survey while they were waiting for their appointment with their healthcare providers in the waiting area.
We conducted semi-structured interviews using the adapted guide with the participants who agreed to participate in the qualitative component on the same day they completed the quantitative survey after they had seen their healthcare providers in a private room in the health facility that had been provided to the research staff.
2.5. Data Analysis
The analysis of both quantitative and qualitative data was approached through an integrated mixed-methods perspective, where the two parts complemented each other to address the study objectives. Quantitative data were analyzed using Stata software version 18.0 (Stata Corp., College Station, TX), with descriptive statistics employed to summarize demographic characteristics. Continuous variables were reported as means and standard deviations, while categorical variables were presented as proportions and percentages. For qualitative data, thematic analysis was applied, starting with verbatim transcription of interviews. Using Nvivo software, codes were developed to cluster concepts within the data [28]. After identifying recurring codes, they were grouped into subcodes or categories, and themes were derived by connecting across participants and categories. This integrated approach allowed for a comprehensive understanding of the study's findings, where the quantitative data provided statistical insights, and the qualitative analysis revealed deeper contextual and thematic insights, together offering a richer interpretation of the study objectives.
2.6. Ethics
The Human Research Ethics Committee (HREC) at the Faculty of Health Sciences, University of Cape Town (HREC REF 011/2023), approved this study. The research assistant provided the participants with an information sheet and informed them that their participation was voluntary. They were also told that they could withdraw from the study at any time and that their decision on whether to participate would not affect the care they received at the clinic. Pregnant women who agreed to participate signed a written informed consent form. Participants who agreed to participate in the semi-structured interviews signed an additional consent form.
3. Results
A total of 103 participants were approached and invited to fill out the study questionnaire. Of these, 80 pregnant women agreed to participate and signed the consent form. Participants filled out the self-administered surveys in the waiting area while waiting for their appointment with their healthcare provider. During the study, only one participant dropped out. The response rate was 77% (79/103). Of the 79 participants who completed the questionnaire, 10 were further invited to participate in the qualitative component. Three participants declined, and seven agreed and participated in the interviews, signing the relevant consent form (Figure 1). Interviews were conducted after the participants' appointments, before they left the hospital, in a private room provided by the antenatal staff.
3.1. Demographic Characteristics of the Study Population
The mean age of the participants was 31 ± 6 years. Most pregnant women fell into the Black African (n = 47, 60%), Colored (n = 29, 38%) categories. We determined maternal socio-economic status based on household income and the majority were in the low-income category (n = 76, 96%) and had a secondary education level (n = 52, 66%). The mean gestational age was 15 ± 8 weeks, 62% (n=47) of the participants had high-risk pregnancies, and 14% (n=11) were HIV positive as shown in Table 1.
Filling out the questionnaire took an average of 11 minutes (range: 8-13 minutes). Interviews were conducted after the participants' appointments, before they left the hospital, in a private room provided by the antenatal staff. The interviews lasted between 20 to 40 minutes.
3.2. Participant Feedback and Usability of Tools
The questionnaire took an average of 11 minutes to complete (range: 8-13 minutes). The antenatal staff provided a private room for the interviews, which were conducted after the participants' appointments before they left the hospital. The interviews lasted 20 to 40 minutes.
The first twenty participants completed the English version of the questionnaire. A few of them did not understand the word “con” in the VAX scale, so we changed it to “scam.” The participants found the adapted survey questions clear overall and did not encounter any difficulties in answering the questions.
Participants found filling out the survey on the tablet easy and did not experience any difficulties, especially because all questions were either "Yes or No" or multiple-choice type questions.
The questionnaire was then translated into IsiXhosa and Afrikaans and back-translated into English. The remaining 60 participants were allowed to fill out the questionnaire in their preferred language. Only three participants chose the IsiXhosa version, and two chose the Afrikaans version.
Three participants did not complete the full questionnaire. Thus, to ensure the completeness of the questionnaire, we had changed the setting of the survey on RedCap and participants could not submit the survey if there were unanswered questions.
Overall, participants found the survey easily understandable and filled it out without any difficulties. They provided minor comments on the translated versions, and we made the necessary changes.
The final version of the survey is provided in Supplementary Document S1.
3.3. Findings on General Attitudes Toward Vaccination
Findings from the VAX scale indicated that 64.5% (n = 49) of the participants rely on vaccines to stop infectious diseases, and 62.7% (n = 47) feel protected after being vaccinated. Fifty-nine point nine percent (n = 42) believe that most vaccines appear to be safe, though there may be problems that have not yet been discovered, and 46% (n = 35) believe that vaccines can cause unforeseen problems in children. Furthermore, 66% (n = 50) of the study participants reported that they worry about the unknown effects of vaccines in the future. Results of the VAX scale are presented in Table 2.
Two themes emerged when we discussed vaccines in general with pregnant women. Theme one relates to knowledge and beliefs about vaccines. Most of the participants had heard about vaccines, but they expressed having basic knowledge and stated that they didn’t know much about vaccination.
“I don't know anything about them. I just know that they protect you from the viruses.” Participant #1.
“ It helps to prevent you from getting sick….Or If you get it, you won't get it so bad…That's all I know.” Participant #6.
Two participants shared their beliefs on the influence of religion on their views on vaccination. One participant mentioned that her religion doesn’t believe in vaccines, but her religious views or religious leaders do not influence her stance on vaccination, as she believes vaccines prevent her from getting ill. However, another participant said that her religious views do influence her beliefs about vaccines and that she considers what her religious leaders tell her and their advice.
“In my religion, we don't believe in vaccines and vitamins…I would take it still because I believe it prevents you from getting sick.” Participant #6.
“I would say yes, because like in some religions would say like, do not take the vaccine then we can always pray about it. Because when you, when you're sick, there's only one person that can heal you. And it's, it's our lord. So, I would say I would consider, their opinion…I've got a pastor. So, he sends me to church. And he would always tell us like, you can go, but it's your own decision. Decision to make. But you must also know that this is stuff that is here to test us. To see if you, if your faith is gonna be strong. So, you can have your vaccine. It's not a problem, but you can also just pray. And ask God, to protect you and your family.” Participant #7.
Theme two is about vaccination decision-making process including opinion leaders or significant persons who influence the participants’ intent to vaccinate, adding to their information-seeking behaviour. All participants stated that the doctor’s opinion influences the most their intent to vaccinate.
“Because usually I listen to what the doctor says. Like I'm a hypertension person. If he tells me, you must take your tablets at 7 a.m. I usually do that on time. So, when it comes to my health it's gonna be better for me. My blood pressure will stay normal. Because I take it every day at the same time. So, I would say the doctor's opinion in vaccination.” Participant #1.
“If it's recommended to me by a doctor, then I will take it. But if it's not by a doctor, then I will not”. Participant #3.
In contrast, when participants were asked whether their friends' or family’s views and opinions on vaccines influenced their attitudes and intent to vaccinate, participants expressed differing views.
“…If they are against it that's their problem. I will still go for it.” Participant #6.
“I would say my family's opinion, yeah, would also make me not take it.” Participant #2.
Participant #4 said that her decision would depend on the disease and the side effects of the vaccine: “ The reason is going to depend on what kind of disease is going to come and then I must know that vaccine is not going to make my life, maybe is not, I'm not going to be sick after doing this vaccine.”
Besides, Participant #5 touched on her information-seeking behavior while deciding whether to get vaccinated: “…I will look for information on Google and the clinic. Then I'll ask the nurse or a doctor. I will show her what I researched about it, and I will ask her. If it's like that or if it's not like that. Then I would believe the doctor.”
3.4. Knowledge and Attitudes Toward Maternal Vaccination
Fifty-one percent (n = 38) of pregnant women agreed that all recommended vaccines for pregnant women offered by the government program in their community are beneficial, and 53% (n = 40) agree that the recommended vaccines for pregnant women are effective. However, 61% (n = 46) are concerned about the serious side effects of vaccines. Participants' general attitudes towards maternal vaccines are presented in Table 3.
Two themes emerged when discussing vaccination during pregnancy with participants. Theme three was Knowledge of Vaccination During Pregnancy. All study participants stated that they were unaware of vaccinations recommended for pregnant women.
“I don't know anything.” Participant #2.
“I don't know much about it; to be honest, I haven't really seen people getting vaccinated during pregnancy. I think there might not be enough information about it. Because I'm six months in now. This is the first time I heard about getting vaccinated while pregnant. Because when you're pregnant, they just tell you, don't do this, don't do that. You can't take this medication; you can't take that. So, you just stay away from everything. So, I don't think there's enough information about it.” Participant #5.
Theme four was the vaccine decision-making process during pregnancy. We discussed with pregnant women how they would decide whether to get vaccinated during pregnancy if recommended vaccines were available.
“If it's recommended by the doctor, then I would take it.” Participant #7
Two participants said they would get the Tdap vaccine to protect their babies.
“I will get it for the safety of my baby. ” Participant #3
“I will take it because I want to protect the baby.” Participant #4
However, Participant #6 stated that she would not accept any vaccines during pregnancy: “I don't believe in taking anything when pregnant.”
In addition, we explored COVID-19 vaccine acceptance among pregnant women. We asked them how they would decide whether to get vaccinated against COVID-19 during pregnancy if it were recommended. Only two participants said they would take the vaccine if recommended by their doctor to protect their baby. Most participants were hesitant about getting vaccinated against COVID-19 during pregnancy because they wanted to be sure the vaccine was safe for both them and their babies.
“I need to know that if I take this COVID vaccine right now, while I'm pregnant, it's going to be safe, I'm not going to be sick, and it's not going to cause a problem in my body.” Participant #4
3.5. Knowledge and Attitudes Toward Routine Childhood Vaccines
Routine childhood vaccination BeSD priority indicators are presented in Table 4. Seventy-three point four percent (n = 58) of the participants think that childhood vaccines are very important for their child’s health, 59.5% (n = 47) want to vaccinate their child with all recommended vaccines in South Africa, and 31.7% (n = 25) want their child to get some of these vaccines.
Three themes emerged when discussing childhood vaccination with participants. Theme five was knowledge and the trusted sources of information regarding childhood vaccination. All participants had heard about routine childhood vaccines and immunization schedules for babies. They understood that childhood vaccines protect infants and young children from infectious diseases.
Their most trusted sources of information on childhood vaccination were doctors, nurses, and healthcare providers at clinics.
“I know that they should get it since the period of being small and that it helps them with their immune system and growing up.” Participant #1
“It's important that the baby must get the vaccine. Because babies must not be getting the illness and get sick and sick.” Participant #4
“Trusted sources of information are my doctor and nurses, that's all.” Participant #6
Theme six was the intention to vaccinate and the reasons. All participants stated that they planned to vaccinate their children and shared their motivations.
“Because I want her to be protected.” Participant #2
“Because I want him must get healthy, not getting sick. Getting coughing, I don't want to, I don't want to lose him.” Participant #4
“Definitely. Because that is just my belief. Because I was raised that way, my mother made sure I was up to date. My siblings were up to date with our vaccines. I've already chosen for my son, my first baby, to have all these vaccines.” Participant #5
Theme seven was the experience of vaccinating a child under five, one participant shared her experience of vaccinating her child, how she made the decision, and what she felt immediately after vaccinating her baby:
“I have discussed it with no one. I just decided to do it...When my child was vaccinated, I felt relieved. Really relieved!”. Participant #5
3.6. COVID-19 Vaccination Knowledge and Perceptions
COVID-19 vaccination BeSD priority indicators are presented in Table 4. Fifty-four point four percent (n = 43) of the study participants think that getting COVID-19 during pregnancy is “A little important” or “Not at all important.” Sixty-eight point four percent (n = 54) do not want to get the COVID-19 vaccine during the current pregnancy, and only one participant was willing to get vaccinated against COVID-19 during pregnancy.
Three themes emerged regarding COVID-19 disease and COVID-19 vaccines prior to getting pregnant. Theme eight focuses on participants’ perceived risk and concerns about contracting COVID-19. Most participants were worried about getting COVID-19, which they considered a severe disease.
“I was scared of getting COVID because I heard that COVID is dangerous, it's killing people. Yeah. I was very scared. “Participant #4.
“The very first time I was obviously very worried. Because I didn't know much about it. I didn't know what it was like. When we got COVID the first time, it was just off the road, shutdown happened. So, we didn't, there wasn't a lot of information out there. And I was very worried. Because my husband was very, very sick. We also had my son; my son was only a year or two at the time. And then uhm, the second time I got COVID, I had COVID and all these fevers. My son was very sick.” Participant #5.
Participant #7 had different views and experiences with COVID-19. She was not worried, and when she and her family had COVID-19, it was mild, similar to the flu:
”Everyone in the house had COVID. Yeah, so and we didn't even know it was COVID. And I went for a COVID test. When the test came back, I was fine you know. But it showed now we had COVID. But other than that, I wasn't scared. I was just relaxed, I didn't panic… Maybe it was self-esteem, because I said to myself, it was just the flu. So, I wasn't scared. Nobody panicked. We were normal in the house. Everyone had it. So, it was normal for us. It was just like the flu.”
Theme nine was on views and beliefs on COVID-19 vaccines. Participants shared different views on COVID-19 vaccines. For instance, one believes that COVID-19 vaccines are important because they prevent infection. Besides, another participant believes that COVID-19 vaccines are safe, and she has confidence in COVID-19 vaccines and the government.
“Yeah, it's important, because it makes us safe”. Participant #4.
“I think it's very safe. Like I said, I don't think people would put in the time and the effort. And all that money to then produce a product that is not good and not safe. I don't think the government would do that to the people. And I don't think it would be promoted on such a large scale. If It's a good potential to be harmful.” Participant #5.
Although Participant #7 was initially worried because COVID-19 vaccines were new, she later believed they were safe as she had not heard of anyone dying from the vaccine: “With this new vaccine, I'm worried about safety... I think it is safe because I haven't heard anyone died of it.”
However, Participant #6 had negative views on COVID-19 vaccines, influenced by what she had heard from family and friends.
“I've heard a lot of stuff; I heard that it gives you the flu. I have heard it from family, friends and like, they were complaining. Those who took the vaccine were complaining about, the pain they got in their arms. I don't know if it is true because I never had it…I heard nothing positive.”
Theme nine was the decision-making process for whether to get vaccinated or not against COVID-19 before the current pregnancy. The decision-making process regarding COVID-19 vaccination before the current pregnancy varied among participants. Participant #2 took the COVID-19 vaccine to protect herself from getting the disease: “I just wanted to be protected from getting the Corona.”
Participant #5 had a bad experience with COVID-19 and decided to get vaccinated after doing her research once the vaccine became available.
“Because of how ill we were in the beginning. When we got COVID the first time. And then obviously, when the vaccine came out, we did our research. Is it safe? Is it good for us to take the vaccine? And it was then when I got COVID the second time around, it wasn't that bad. I haven't been sick even since it has been a few years now. Since I’ve had the vaccine.”
However, Participant #3 chose not to get vaccinated due to concerns about side effects based on stories she had heard.: “I was very concerned. There were too many stories, like negative things people said on the internet, or friends of mine said very bad things, so I just decided not to do it.”
4. Discussion
The pilot testing of the quantitative self-administered survey and qualitative interviews was successfully conducted among pregnant women attending antenatal care in Cape Town. The survey methodology, the use of tablets, and logistics were effective. Pregnant women found the survey easy to complete, and the timing while waiting for their appointment was adequate. Conducting the interviews after their appointment with the healthcare provider was also convenient for them.
A key consideration is that data collection was conducted by a PhD student and a research assistant who were not part of the hospital staff. This made participants feel more comfortable and relaxed when sharing their opinions, particularly during qualitative interviews, as they were speaking with someone who was not a healthcare worker at the hospital they were attending, which may reduce the social desirability and interviewer bias.
This pilot study tested and adapted the WHO BeSD tools, the General Attitudes Toward Vaccine Survey questions developed by the WHO SAGE working group on vaccine hesitancy, and the VAX Scale for use among pregnant women in Cape Town, South Africa. These tools have been used to explore maternal vaccine decision-making in countries like Kenya [22,23] Australia [30], and Poland [31] where pregnant women believed that a pregnant woman would be protected if vaccinated [22,23]. Mistrust of Vaccine Benefit, Concerns about Commercial Profiteering, and Preference for Natural Immunity constructs of the VAX scale were associated with vaccine uptake during pregnancy [31]. Additionally, pregnant women reported that they were concerned that the COVID-19 vaccine could cause harm to the unborn baby [30].
Despite the significant burden of vaccine-preventable diseases and critical gaps in vaccine delivery and uptake in LMICs [32], nuanced explorations of the knowledge, acceptance, and attitudes of pregnant women towards vaccines using these tools are undertaken or reported. This potentially undermines appropriate reforms to existing policy and practice. Our findings provide initial evidence of the tools' usability and acceptability among pregnant women in South Africa while identifying areas for refinement to ensure their suitability for broader application in settings with similar contexts.
4.1. Key Findings and Appraisal
The tools were well-received by participants, who reported ease of use and understanding, particularly when using tablets for the quantitative survey. This is consistent with findings from other studies that demonstrate the feasibility of self-administered, tablet-based surveys in low-resource settings for capturing maternal health data efficiently [33,34,35]. Importantly, the adapted tools were sensitive enough to capture nuanced attitudes toward maternal and routine childhood vaccination, as well as participants' perceptions of COVID-19 vaccines.
Quantitative results revealed moderate levels of vaccine confidence, with notable concerns about vaccine safety during pregnancy. Qualitative data underscored the critical role of healthcare providers as trusted sources of information, corroborating existing literature that identifies healthcare provider recommendations as pivotal in maternal vaccine decision-making [16,32]. However, knowledge gaps regarding specific vaccines recommended during pregnancy were evident, emphasizing the need for targeted educational interventions. For instance, pregnant women participating in the interviews indicated that they were not aware of any vaccines recommended during pregnancy. However, the National Integrated Maternal and Perinatal Care Guidelines for South Africa provides comprehensive guidelines on vaccines recommended for pregnant women [36]. These vaccines including Td, Influenza, and COVID-19 are administered to all pregnant women at no cost at public health facilities. Very recently, the National Department of Health switched from Td to Tdap to enhance protection against pertussis [25]. Further additions to existing guidelines include recommendations on COVID-19 vaccines [37,38]. Unfortunately, a low level of awareness among pregnant women regarding these vaccine recommendations negatively impacts demand generation and uptake. Further to this, gaps in service delivery, such as stockouts of COVID-19 or flu vaccines create barriers to acceptance and uptake [39,40].
Lastly, our findings demonstrate the utility of the VAX Scale and BeSD tools in eliciting pregnant women's perceptions of vaccine safety and effectiveness, but some adaptations were required to enhance their cultural and contextual relevance. For example, minor linguistic changes improved comprehension of key terms like "con," which was revised to "scam." Such modifications highlight the importance of pretesting tools to ensure clarity and accuracy in diverse settings.
4.2. Strengths and Limitations of This Pilot Study
This study represents the first attempt to adapt and test these globally recognized tools for assessing vaccine attitudes among pregnant women in South Africa, filling a critical gap in the literature. The integration of quantitative and qualitative methodologies using a mixed-methods design allowed for a comprehensive evaluation of the tools' performance and enriched the understanding of maternal vaccine confidence in the local context.
We also share practical insights with participant feedback on the tools' usability and logistics offering valuable guidance for future research, such as leveraging waiting times at healthcare facilities for data collection. Further to this, while interviewing a sub-population of the survey participants provided crucial findings, we observed that prior participation in the survey may have influenced interviewees' responses. We therefore propose interviewing a separate group of pregnant women with no prior knowledge of the survey questions to enhance insights on these focal areas.
As a pilot study, the sample size was limited, which may affect the generalizability of the findings. However, the primary goal was to refine the tools rather than draw definitive conclusions. In addition, while the tools were translated into multiple languages, most participants completed the survey in English, limiting insights into the effectiveness of the IsiXhosa and Afrikaans versions. Lastly, this study was conducted in public antenatal clinics, and the findings may not reflect the experiences of pregnant women accessing private healthcare.
4.3. Implications for Future Research
The results suggest that the WHO BeSD Framework and tools in addition to the VAX Scale, and the adapted General Vaccine Attitude Survey questionnaire that has been developed from the compendium of survey questions by the SAGE Working Group on Vaccine Hesitancy with minor adaptations, are fit for purpose in the South African context. Future studies should apply these tools in larger and more diverse populations to validate their utility and explore the broader determinants of vaccine acceptance. Additionally, efforts should be made to address the knowledge gaps identified in this pilot, particularly through healthcare provider-driven educational interventions.
5. Conclusions
This pilot study demonstrates the feasibility and acceptability of using the WHO BeSD tools and framework, the General Attitudes Toward Vaccine Survey questions developed by the WHO SAGE working group on vaccine hesitancy, and the VAX Scale to assess vaccine confidence among pregnant women in South Africa. These findings pave the way for their use in larger-scale studies and contribute to the global understanding of maternal vaccine attitudes. Addressing maternal knowledge gaps and leveraging healthcare provider influence will be crucial in designing effective interventions to promote vaccine confidence and uptake in this and similar settings.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org.
Author Contributions
Conceptualization, I.A and E.A.-D.; methodology, I.A., E.A.-D., and JNG.; formal analysis, I.A., JNG and E.A.-D.; investigation, I.A, JNG and E.A.-D.; resources, I.A., E.A.-D., and RM.; data curation, I.A., and JNG.; writing—original draft preparation, I.A.; writing—review and editing, I.A., JNG, E.A.-D., B.M.K., and R.M.; visualization, I.A., and E.A.-D.; supervision, E.A.-D., B.M.K., and R.M.; project administration, I.A. Final approval of the version to be published, E.A.-D., JNG, B.M.K., and R.M.; agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved, I.A., E.A.-D., B.M.K., and R.M. All authors have read and agreed to the published version of the manuscript.
Funding
This research received funding from the University of Cape Town, the Faculty Research Committee at the Faculty of Health Sciences, and the Department of Pediatrics and Child Health.
Institutional Review Board Statement
This study was approved by the Human Research Ethics Committee (HREC) at the Faculty of Health Sciences, University of Cape Town (HREC REF 011/2023).
Informed Consent Statement
Written Informed consent was obtained from all the participants involved in the study. An additional written informed consent form was obtained from participants who participated in the qualitative component of the study.
Acknowledgments
We would like to acknowledge the Wellcome Trust for supporting Dr. Imen Ayouni’s PhD scholarship under the Wellcome Trust grant (Reference 222300/Z/20/Z awarded to B. M. K. and R. M.).
Conflicts of Interest
The authors declare no conflict of interest.
References
- Healy, C.M.; Rench, M.A.; Montesinos, D.P.; Ng, N.; Swaim, L.S. Knowledge and attitiudes of pregnant women and their providers towards recommendations for immunization during pregnancy. Vaccine 2015, 33, 5445–5451. [Google Scholar] [CrossRef]
- Creanga, A.A.; Johnson, T.F.; Graitcer, S.B.; Hartman, L.K.; Al-Samarrai, T.; Schwarz, A.G.; Chu, S.Y.P.; Sackoff, J.E.; Jamieson, D.J.; Fine, A.D.; et al. Severity of 2009 Pandemic Influenza A (H1N1) Virus Infection in Pregnant Women. Obstet. Gynecol. 2010, 115, 717–726. [Google Scholar] [CrossRef]
- Jamieson, D.J.; A Honein, M.; A Rasmussen, S.; Williams, J.L.; Swerdlow, D.L.; Biggerstaff, M.S.; Lindstrom, S.; Louie, J.K.; Christ, C.M.; Bohm, S.R.; et al. H1N1 2009 influenza virus infection during pregnancy in the USA. Lancet 2009, 374, 451–458. [Google Scholar] [CrossRef]
- D'Alessandro, A.; Napolitano, F.; D'Ambrosio, A.; Angelillo, I.F. Vaccination knowledge and acceptability among pregnant women in Italy. Hum. Vaccines Immunother. 2018, 14, 1573–1579. [Google Scholar] [CrossRef]
- Baxter, R.; Bartlett j Fireman, B.; Lewis, E.; Klein, N.P. Effectiveness of Vaccination During Pregnancy to Prevent Infant Pertussis. Pediatrics 2017, 139, 1–8. [Google Scholar] [CrossRef]
- Nunes, M.C.; Cutland, C.L.; Jones, S.; Downs, S.; Weinberg, A.; Ortiz, J.R.; Neuzil, K.M.; Simões, E.A.F.; Klugman, K.P.; A Madhi, S. Efficacy of Maternal Influenza Vaccination Against All-Cause Lower Respiratory Tract Infection Hospitalizations in Young Infants: Results From a Randomized Controlled Trial. Clin. Infect. Dis. 2017, 65, 1066–1071. [Google Scholar] [CrossRef]
- Skoff, T.H.; Blain, A.E.; Watt, J.; Scherzinger, K.; McMahon, M.; Zansky, S.M.; et al. Impact of the US Maternal Tetanus, Diphtheria, and Acellular Pertussis Vaccination Program on Preventing Pertussis in Infants <2 Months of Age: A Case-Control Evaluation. Clinical Infectious Diseases 2017, 65, 1977–1983. [Google Scholar] [PubMed]
- Zerbo, O.; Modaressi, S.; Chan, B.; Goddard, K.; Lewis, N.; Bok, K.; Fireman, B.; Klein, N.P.; Baxter, R. No association between influenza vaccination during pregnancy and adverse birth outcomes. Vaccine 2017, 35, 3186–3190. [Google Scholar] [CrossRef]
- Donaldson, B.; Jain, P.; Holder, B.S.; Lindsey, B.; Regan, L.; Kampmann, B. What determines uptake of pertussis vaccine in pregnancy? A cross sectional survey in an ethnically diverse population of pregnant women in London. Vaccine 2015, 33, 5822–5828. [Google Scholar] [CrossRef]
- Ditsungnoen, D.; Greenbaum, A.; Praphasiri, P.; Dawood, F.S.; Thompson, M.G.; Yoocharoen, P.; Lindblade, K.A.; Olsen, S.J.; Muangchana, C. Knowledge, attitudes and beliefs related to seasonal influenza vaccine among pregnant women in Thailand. Vaccine 2016, 34, 2141–2146. [Google Scholar] [CrossRef]
- MacDougall, D.M.; Halperin, B.A.; Langley, J.M.; McNeil, S.A.; MacKinnon-Cameron, D.; Li, L.; Halperin, S.A. Knowledge, attitudes, beliefs, and behaviors of pregnant women approached to participate in a Tdap maternal immunization randomized, controlled trial. Hum. Vaccines Immunother. 2016, 12, 879–885. [Google Scholar] [CrossRef]
- Manjunath, U.; Pareek, R.P. Maternal knowledge and perceptions aboutthe routine immunization programme--a study in a semiurban area in Rajasthan. Indian J. Med. Sci. 2003, 57, 158–163. [Google Scholar]
- Adedire, E.B.; Ajumobi, O.; Bolu, O.; Nguku, P.; Ajayi, I. Maternal knowledge, attitude, and perception about childhood routine immunization program in Atakumosa-west Local Government Area, Osun State, Southwestern Nigeria. Pan. Afr. Med. J. 2021, 40, 8. [Google Scholar]
- Luman, E.T.; McCauley, M.M.M.; Shefer, A.; Chu, S.Y. Maternal Characteristics Associated With Vaccination of Young Children. Pediatrics 2003, 111, 1215–1218. [Google Scholar] [CrossRef]
- Fatiregun, A.A.; Okoro, A.O. Maternal determinants of complete child immunization among children aged 12–23 months in a southern district of Nigeria. Vaccine 2012, 30, 730–736. [Google Scholar] [CrossRef]
- Kilich, E.; Dada, S.; Francis, M.R.; Tazare, J.; Chico, R.M.; Paterson, P.; Larson, H.J. Factors that influence vaccination decision-making among pregnant women: A systematic review and meta-analysis. PLOS ONE 2020, 15, e0234827. [Google Scholar] [CrossRef] [PubMed]
- Larson, H.J.; Jarrett, C.; Schulz, W.S.; Chaudhuri, M.; Zhou, Y.; Dubé, E.; Schuster, M.; MacDonald, N.E.; Wilson, R.; The SAGE Working Group on Vaccine Hesitancy. Measuring vaccine hesitancy: The development of a survey tool. Vaccine 2015, 33, 4165–4175. [Google Scholar] [CrossRef]
- Martin, L.R.; Petrie, K.J. Understanding the Dimensions of Anti-Vaccination Attitudes: the Vaccination Attitudes Examination (VAX) Scale. Ann. Behav. Med. 2017, 51, 652–660. [Google Scholar] [CrossRef] [PubMed]
- World Health O. Behavioural and social drivers of vaccination: tools and practical guidance for achieving high uptake 2022. Available online: https://www.who.int/publications/i/item/9789240049680 (accessed on 6 January 2025).
- Hub VD. BEHAVIORAL AND SOCIAL DRIVERS OF VACCINATION (BeSD). Available online: https://demandhub.org/behavioral-and-social-drivers-of-vaccination-besd/ (accessed on 12 February 2025).
- Roberts, H.A.; Clark, D.A.; Kalina, C.; Sherman, C.; Brislin, S.; Heitzeg, M.M.; Hicks, B.M. To vax or not to vax: Predictors of anti-vax attitudes and COVID-19 vaccine hesitancy prior to widespread vaccine availability. PLOS ONE 2022, 17, e0264019. [Google Scholar] [CrossRef]
- Otieno, N.A.; Nyawanda, B.; Otiato, F.; Adero, M.; Wairimu, W.N.; Atito, R.; Wilson, A.D.; Gonzalez-Casanova, I.; Malik, F.A.; Verani, J.R.; et al. Knowledge and attitudes towards influenza and influenza vaccination among pregnant women in Kenya. Vaccine 2020, 38, 6832–6838. [Google Scholar] [CrossRef] [PubMed]
- Otieno, N.A.; Otiato, F.; Nyawanda, B.; Adero, M.; Wairimu, W.N.; Ouma, D.; Atito, R.; Wilson, A.; Gonzalez-Casanova, I.; Malik, F.A.; et al. Drivers and barriers of vaccine acceptance among pregnant women in Kenya. Hum. Vaccines Immunother. 2020, 16, 2429–2437. [Google Scholar] [CrossRef] [PubMed]
- Government WC. The Western Cape Language Policy. Available online: https://d7.westerncape.gov.za/general-publication/western-cape-language-policy (accessed on 27 January 2025).
- National Department of Health RoSA. Tetanus, reduced-strength diphtheria and acellular pertussis (Tdap), Knowledge Hub Webinar 2023. Available online: https://knowledgehub.health.gov.za/system/files/2023-11/KH%20webinar%20Session%202%20Tdap%20-%20final.pdf (accessed on 14 January 2024).
- Harris, P.A.; Taylor, R.; Thielke, R.; Payne, J.; Gonzalez, N.; Conde, J.G. Research electronic data capture (REDCap)—A metadata-driven methodology and workflow process for providing translational research informatics support. J. Biomed. Inform. 2009, 42, 377–381. [Google Scholar] [CrossRef] [PubMed]
- Harris, P.A.; Taylor, R.; Minor, B.L.; Elliott, V.; Fernandez, M.; O'Neal, L.; McLeod, L.; Delacqua, G.; Delacqua, F.; Kirby, J.; et al. The REDCap consortium: Building an international community of software platform partners. J. Biomed. Inform. 2019, 95, 103208. [Google Scholar] [CrossRef]
- Mortelmans, D. Analyzing Qualitative Data Using NVivo. In The Palgrave Handbook of Methods for Media Policy Research; Van den Bulck, H., Puppis, M., Donders, K., Van Audenhove, L., Eds.; Springer International Publishing: Cham, 2019; pp. 435–450. [Google Scholar]
- Jansen, J.W.C. (Ed.) Fault lines: a primer on race, science and society; African Sun Media: Stellenbosch, 2020. [Google Scholar]
- Rikard-Bell, M.; Elhindi, J.; Lam, J.; Seeho, S.; Black, K.; Melov, S.; Jenkins, G.; McNab, J.; Wiley, K.; Pasupathy, D. COVID-19 vaccine acceptance among pregnant women and the reasons for hesitancy: A multi-centre cross-sectional survey. Aust. New Zealand J. Obstet. Gynaecol. 2022, 63, 335–343. [Google Scholar] [CrossRef]
- Kiersnowska, I.; Kalita-Kurzyńska, K.; Piekutowska-Kowal, W.; Baranowska, J.; Krzych-Fałta, E. Attitudes towards Maternal Immunisation of Polish Mothers: A Cross-Sectional, Non-Representative Study. Vaccines 2024, 12, 1143. [Google Scholar] [CrossRef]
- Davies, A.; Mullin, S.; Chapman, S.; Barnard, K.; Bakhbakhi, D.; Ion, R.; Neuberger, F.; Standing, J.; Merriel, A.; Fraser, A.; et al. Interventions to enhance medication adherence in pregnancy- a systematic review. BMC Pregnancy Childbirth 2023, 23, 1–21. [Google Scholar] [CrossRef]
- Manyazewal, T.; Woldeamanuel, Y.; Blumberg, H.M.; Fekadu, A.; Marconi, V.C. The potential use of digital health technologies in the African context: a systematic review of evidence from Ethiopia. npj Digit. Med. 2021, 4, 1–13. [Google Scholar] [CrossRef]
- Lee, S.; Lee, Y.-J.; Kim, S.; Choi, W.; Jeong, Y.; Rhim, N.J.; et al. Perceptions on Data Quality, Use, and Management Following the Adoption of Tablet-Based Electronic Health Records: Results from a Pre–Post Survey with District Health Officers in Ghana. Journal of Multidisciplinary Healthcare 2022, 15, 1457–1468. [Google Scholar] [CrossRef] [PubMed]
- Kong, S.Y.J.; Acharya, A.; Basnet, O.; Haaland, S.H.; Gurung, R.; Gomo, Ø.; Ahlsson, F.; Meinich-Bache, Ø.; Axelin, A.; Basula, Y.N.; et al. Mothers’ acceptability of using novel technology with video and audio recording during newborn resuscitation: A cross-sectional survey. PLOS Digit. Heal. 2024, 3, e0000471. [Google Scholar] [CrossRef]
- Department of Health SA. NATIONAL INTEGRATED MATERNAL AND PERINATAL CARE GUIDELINES FOR SOUTH AFRICA 2024. Fifth edition. Available online: https://knowledgehub.health.gov.za/system/files/elibdownloads/2024-10/Integrated%20Maternal%20and%20Perinatal%20Care%20Guideline_23_10_2024_0.pdf (accessed on 27 January 2025).
- Ashkir, S.; Khaliq, O.P.; Hunter, M.; Moodley, J. Maternal vaccination: A narrative review. South. Afr. J. Infect. Dis. 2022, 37, 6. [Google Scholar] [CrossRef]
- The National Institute for Communicable Diseases (NICD) SA. Vaccination of pregnant and breastfeeding women (August update) 2021. Available online: https://www.nicd.ac.za/vaccination-of-pregnant-and-breastfeeding-women-august-update/ (accessed on 27 January 2025).
- Wei, C.R.; Kamande, S.; Lang’at, G.C. Vaccine inequity: a threat to Africa’s recovery from COVID-19. Trop. Med. Heal. 2023, 51, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Davies, B.; Olivier, J.; Amponsah-Dacosta, E. Health Systems Determinants of Delivery and Uptake of Maternal Vaccines in Low- and Middle-Income Countries: A Qualitative Systematic Review. Vaccines 2023, 11, 869. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Enrollment flow chart.
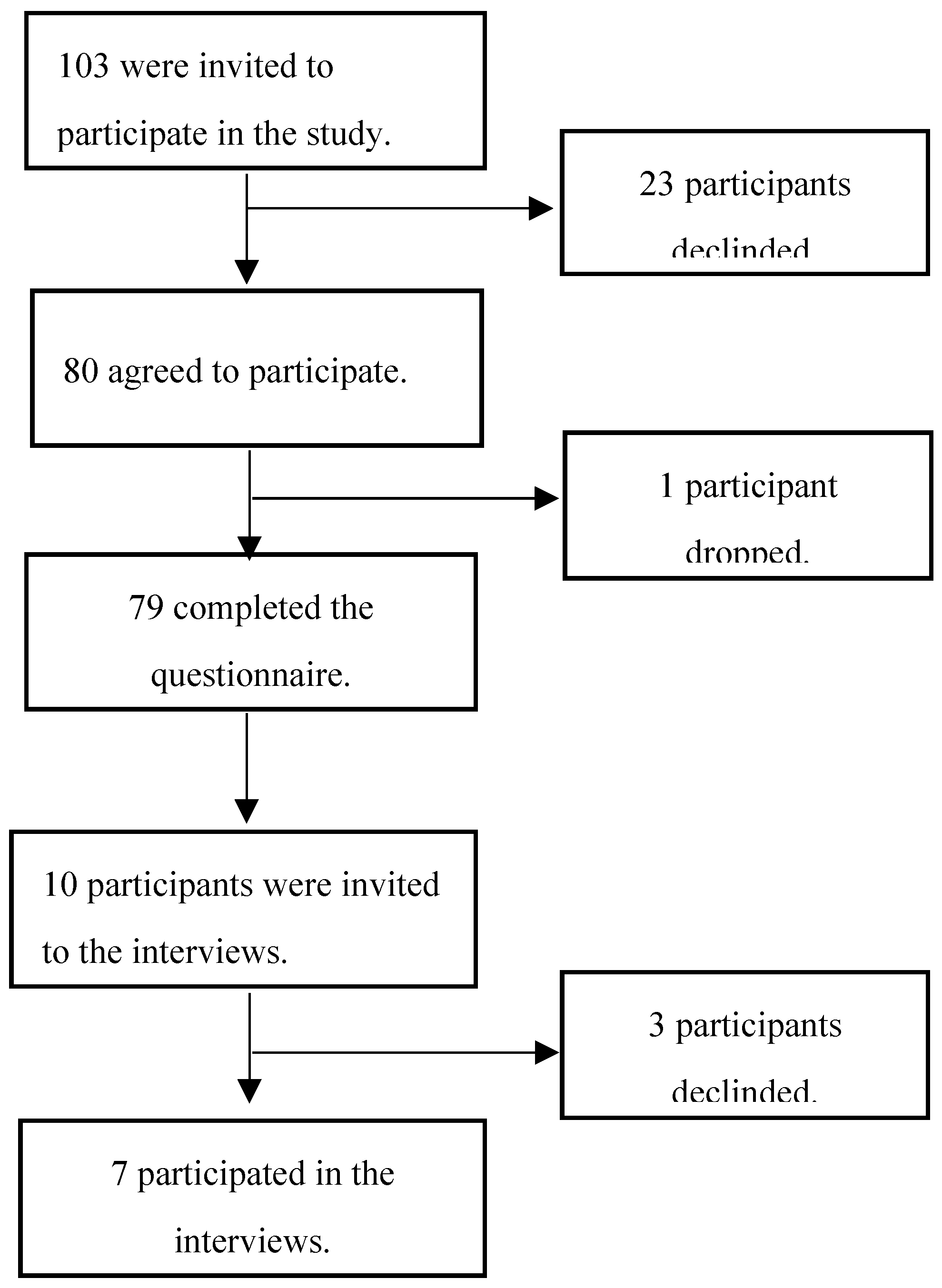

Table 1.
Demographic characteristics of the sample study (n=79).
| Characteristic | n | % |
|---|---|---|
| Age (years) | ||
| Mean (SD) | 31 ± 6 | - |
| Gestational age (weeks) | ||
| Mean (SD) | 15 ± 8 | - |
| Pregnancy risk status | ||
| High risk | 47 | 62 |
| Low risk | 29 | 38 |
| Race* | ||
| Black African | 47 | 59.4 |
| Colored | 29 | 36.7 |
| White | 1 | 1.3 |
| Indian | 1 | 1.3 |
| Asian | 1 | 1.3 |
| Educational level | ||
| Primary | 2 | 2.5 |
| Secondary | 52 | 65.8 |
| Post-secondary certificate | 6 | 7.6 |
| Tertiary | 19 | 24.1 |
| Employment | ||
| Employed | 55 | 70 |
| Unemployed | 24 | 30 |
| Household income | ||
| Low | 76 | 96 |
| Middle | 3 | 4 |
| HIV status | ||
| HIV positive | 11 | 13.9 |
| HIV negative | 68 | 86.1 |
SD = Standard deviation. * This refers to (i) self-identified race (ii) these categories stemmed from the Apartheid Era and are officially used to describe South Africans [29].
Table 2.
Participants' attitudes towards vaccination in general (n=76).
| No | Statement | Strongly Disagree | Disagree | Neutral | Agree | Strongly Agree |
|---|---|---|---|---|---|---|
| 1 | I feel safe after being vaccinated. | 13 (17.1%) | 5 (6.7%) | 18 (23.7%) | 20 (26.7%) | 22 (29.0%) |
| 2 | I can rely on vaccines to stop serious infectious diseases. | 8 (10.5%) | 7 (9.2%) | 12 (15.8%) | 24 (31.6%) | 25 (32.9%) |
| 3 | I feel protected after getting vaccinated. | 7 (9.3%) | 5 (6.7%) | 16 (21.3%) | 27 (36.0%) | 20 (26.7%) |
| 4 | Although most vaccines appear to be safe, there may be problems that we haven't yet discovered. | 14 (18.4%) | 3 (4.0%) | 14 (18.4%) | 19 (25.0%) | 26 (34.2%) |
| 5 | Vaccines can cause unforeseen problems in children. | 14 (18.4%) | 8 (10.5%) | 19 (25%) | 24 (31.6%) | 11 (14.5%) |
| 6 | I worry about the unknown effects of vaccines in the future. | 7 (9.2%) | 7 (9.2%) | 12 (15.8%) | 24 (31.6%) | 26 (34.2%) |
| 7 | Vaccines make a lot of money for pharmaceutical companies but don't do much for regular people. | 15 (19.7%) | 10 (13.2%) | 24 (31.6%) | 14 (18.4%) | 13 (17.1%) |
| 8 | Authorities promote vaccination for financial gain, not for people's health. | 21 (27.6%) | 12 (15.8%) | 22 (29.0%) | 11 (14.5%) | 10 (13.2%) |
| 9 | Vaccination programs are a big scam. | 23 (30.3%) | 11 (14.5%) | 21 (27.6%) | 15 (19.7%) | 6 (7.9%) |
| 10 | Natural immunity lasts longer than a vaccination. | 11 (14.5%) | 10 (13.2%) | 29 (38.2%) | 15 (19.7%) | 11 (14.5%) |
| 11 | Natural exposure to viruses and germs gives the safest protection. | 12 (15.8%) | 11 (14.5%) | 29 (38.2%) | 14 (18.4%) | 10 (13.2%) |
| 12 | Being exposed to diseases naturally is safer for the immune system than being exposed through vaccination. | 13 (17.1%) | 11 (11.8%) | 31 (40.8%) | 13 (17.1%) | 10 (13.2%) |
Table 3.
Participants attitudes towards vaccination during pregnancy (n=75).
| No | Statement | Agree | Neutral/ No opinion | Disagree |
|---|---|---|---|---|
| 1 | Vaccines given in pregnancy are important for my health. | 37 (49.3%) | 26 (34.6%) | 12 (16.0%) |
| 2 | All recommended vaccines for pregnant women offered by the government program in my community are beneficial. | 38 (50.7%) | 25 (33.3%) | 12 (16.0%) |
| 3 | Recommended vaccines for pregnant women are effective. | 40 (53.3%) | 27 (36.0%) | 8 (10.7%) |
| 4 | New vaccines carry more risks than older vaccines. | 11 (14.7%) | 44 (58.7%) | 20 (26.7%) |
| 5 | Getting vaccines is a good way to protect myself from disease. | 51 (68.0%) | 15 (20.0%) | 9 (12.0%) |
| 6 | I am concerned about serious adverse effects of vaccines. | 46 (61.3%) | 18 (24.0%) | 11 (14.7%) |
| 7 | I do not need vaccines for diseases that are not common anymore. | 22 (29.3%) | 32 (42.7%) | 21 (28.0%) |
Table 4.
COVID-19 and routine childhood vaccination BeSD priority indicators (n=79).
| Statement | Response options | n | % |
|---|---|---|---|
|
- How important do you think getting a COVID-19 vaccine during pregnancy is for your health? |
|||
| Not at all important | 27 | 34.2 | |
| A little important | 16 | 20.3 | |
| Moderately important | 16 | 20.3 | |
| Very important | 20 | 25.3 | |
|
- Do you want to get a COVID-19 vaccine during pregnancy? |
|||
| No, you do not want to | 54 | 68.4 | |
| Yes you want to | 1 | 1.3 | |
| You are not sure | 3 | 11.4 | |
| No, I don't want to because I am already vaccinated | 15 | 19.0 | |
|
- Do you think most of your close family and friends want you to get a COVID-19 vaccine while you are pregnant? |
|||
| Yes | 18 | 22.8 | |
| No | 61 | 77.2 | |
| - Do you know where to go to get a COVID-19 vaccine for yourself? | |||
| Yes | 59 | 74.7 | |
| No | 20 | 25.3 | |
| - How easy is it to pay for COVID-19 vaccination? When you think about the cost, please consider any payments to the clinic, the cost of getting there and the cost of taking time away from work? | |||
| Not at all easy | 9 | 11.4 | |
| A little easy | 18 | 22.8 | |
| Moderately easy | 13 | 16.5 | |
| Very easy |
39 | 49.4 | |
| - How important do you think routine childhood vaccines (immunization) are for your child's health? | |||
| Not at all important | 7 | 8.9 | |
| A little important | 7 | 8.9 | |
| Moderately important | 7 | 8.9 | |
| Very important | 58 | 73.4 | |
| - Do you think most of your close family and friends want you to get your child vaccinated? | |||
| Yes | 56 | 70.9 | |
| No | 23 | 29.1 | |
| - South Africa has an immunization schedule of recommended vaccines for children. Do you want your child to get none of these vaccines (immunization), some of these vaccines (immunization), or all of these vaccines (immunization)? | |||
| None | 7 | 8.9 | |
| Some | 25 | 31.7 | |
| All | 47 | 59.5 | |
|
- Do you know where to go to get your child vaccinated? |
|||
| Yes | 67 | 84.8 | |
| No |
12 | 15.2 | |
|
- How easy is it to pay for your child vaccination? When you think about the cost, please consider any payments to the clinic, the cost of getting there, plus the cost of taking time away from work? (Think of any related cost even if the vaccines will be given for free at the clinic that you will go to get your child vaccinated) |
|||
| Not at all easy | 15 | 19.0 | |
| A little easy | 24 | 30.4 | |
| Moderately easy | 16 | 20.2 | |
| Very easy | 24 | 30.4 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



