Submitted:
16 February 2025
Posted:
17 February 2025
You are already at the latest version
Abstract
Non-alcoholic fatty liver disease (NAFLD) has frequently been associated with obesity, type 2 diabetes (T2D) and dyslipidemia, all of which are shared by increased insulin resistance. It has become the most common liver disorder in Korea as well as in developed countries and, therefore, is associated with increased health burden of morbidity and mortality. It has an association with T2D, and T2D increases the risk of cirrhosis and related complications. NAFLD encompasses a disease continuum from simple steatosis to non-alcoholic steatohepatitis which is characterized by faster fibrosis progression. Although its liver-related complication is estimated to be, at most, 10%, it will be a leading cause of cirrhosis and hepatocellular carcinoma soon in Korea. Although the main causes of death in people with NAFLD are cardiovascular disease and extra-hepatic malignancy, advanced liver fibrosis is a key prognostic marker for liver-related outcomes, and can be assessed with combinations of non-invasive tests in the community. Numbers of components of metabolic syndrome involved could be another important prognostic information of NAFLD assessed easily in the routine care of the community. There is a few approved therapy for NAFLD, although several drugs including antioxidants attracts practitioners’ attention. Because of the modest effect of the present therapeutics, let alone complex pathophysiology and substantial heterogeneity of disease phenotypes, combination treatment is a viable option for many patients with NAFLD in the Korean community. Comprehensive approach taking healthy lifestyle and weight reduction into account remain a mainstay to the prevention and treatment of NAFLD.
Keywords:
non-alcoholic fatty liver disease
; metabolic syndrome
; diabetes
; liver fibrosis
; community
1. Introduction
As type 2 diabetes (T2D) increases the concentration of glucose in the blood of adult population, kidney and nerve damage as well as retinal complications will naturally ensue as its consequences. It can also cause serious cardiovascular complications (CVDs) such as peripheral vascular disease, stroke, angina, and /or myocardial infarction. In the long run, these all contributes to increase mortality and morbidity of diabetes patients and reduces their life expectancy. It was not until 1960, along with rapid modernization as well as social and economic growth with improved medical utilization patterns, the number of diabetes patients was found to increase explosively. From the epidemiological data implemented in Yonchon, Gyonggi-do in 1990, we now know 8 out of 100 adults in Korea have diabetes [1]. Consecutive follow up study, performed 2 years later at the same location proved that diabetes condition is expected to increase in the future [2]. Therefore, proper management plan in the community level should be employed knowing that diabetes is an important health issue in Korea.
Non-alcoholic fatty liver disease (NAFLD), which commonly co-associate with T2D, which has not been counted as an important bad companion yet, is also a chronic metabolic disease that reduces quality of life of the patients with T2D in the community [3]. NAFLD is the liver component of a cluster of conditions that are associated with metabolic syndrome (MS). NAFLD is known to have a bidirectional association with components of MS [4]. Although Koreans have a higher fraction of NAFLD patients who are lean, their illness has the same prognosis or worse than those who are obese. It is a disease with increased phlegm which is common in the community, especially in Korea [5]. Over the past four decades, NAFLD has become the most common chronic liver disorder (with a global prevalence of around 25% of the adult population) [4]. As around 10% of people with NAFLD develop liver-related complications, a crucial challenge is to identify those who are at the highest risk for these complications among the people affected by NAFLD. Due to its high prevalence, NAFLD is now the most rapidly increasing cause of liver-related morbidity and mortality and is emerging as an important cause of end-stage liver disease, hepatocellular carcinoma, and liver transplantation with higher medical costs [4,6,7,8]. Gradually, nonalcoholic steato-hepatitis (NASH) and cirrhosis have also emerged as causes for increased health care costs. Among community inhabitants of age 30s to 50s, the overall death rate due to chronic liver diseases, excluding hepatocellular carcinoma ranks 2nd to 4th in Korea [5]. Therefore, NAFLD is fathomed as a very important threat to the health of our people and regarded as emerging big health problems. The number of patients with NAFLD is very high, and so is the mortality rate due to its complications because of the expensive health costs. Despite the growing concern, NAFLD is underappreciated as an important chronic disease, and there are few national strategies or policies for NAFLD [5].
NAFLD is defined by the presence of steatosis in more than 5% of hepatocytes in association with metabolic risk factors (particularly, obesity and T2D) and in the absence of excessive alcohol consumption or other chronic liver diseases [7,9]. NAFLD is a diagnosis of exclusion and there is a debate about the limitations of this term. In 2020, an international panel of experts proposed the concept of metabolic dysfunction-associated fatty liver disease (MAFLD) to highlight the contribution of cardiometabolic risk factors to the development and progression of liver disease [10]. NAFLD encompasses a disease continuum that includes steatosis with or without mild inflammation and a necroinflammatory subtype (NASH), which is additionally characterized by the presence of hepatocellular injury (hepatocyte ballooning). However, the prime pathogenesis of disease can vary substantially among patients with NAFLD, which could be crucial hurdles to be managed appropriately in the community. Furthermore, disease progression and response to treatment are heterogeneous. Information about disease activity and, in particular, the extent of liver fibrosis is necessary to assess the severity of liver disease and provide prognostic information. Growing knowledge from metabolomics, genomics, and other areas will enable disease phenotyping and facilitate potential disease stratification in the future.
Diabetes and NAFLD is known to be the conditions often coexist in the community. Research on the cause and clinical significance of this correlation is rare. Generally, as the content of liver fat increases, the chances of lipid oxidation also increases accordingly. It has been known that in the circumstances of increased whole body lipid oxidation, the levels of endogenous glucose production increase and those of glucose disposal decrease [11]. Excess lipids might also induce glucose intolerance through an inhibitory effect on glucose storage [12]. According to one report of calorimetric experiment, in severe NAFLD patients, a more dramatic decrease in insulin-mediated suppression of whole-body lipid oxidation implicating deepened IR, which results in a less decrease in blood β-hydroxy butyrates (ketones) was observed [13]. Likewise, more marked decrease in insulin-mediated suppression of glycerol production was also found in severe NAFLD. Therefore, lesser degree of insulin-mediated suppression of glucose production as a whole occurs as the level of plasma nonesterified fatty acids (FA) increases, which might be fathomed as a primary driver of NAFLD.
In around half of people with cirrhosis, a devastating complication of NAFLD, therefore, abnormalities in glucose tolerance are observed. According to one report, 15-20% of liver cirrhosis newly develop diabetes over 5 years [5]. Detection of T2D among patients with NAFLD or NASH is important in part because improved glycemic control may improve NAFLD. Although there is no difference in the short-term prognosis between cirrhosis patients with and without diabetes, patients with diabetes have a more poor long-term prognosis. It is known that liver failure occurs frequently in patients with diabetes. Importantly, advanced liver fibrosis should be counted as a key prognostic marker for liver-related outcomes and can be assessed with combinations of non-invasive tests in the community. In the present review, we would first like to present a overviewing synopsis explaining pathogenesis, pathways of NAFLD progression, diagnostic modalities and assessing methods of disease severity, especially when combined with fibrosis. Then, we extend our discussion on viable prevention and management strategies in the community. Ultimately, we would like to appreciate NAFLD as an important chronic disease and suggest some strategies or policies to overcome it on a community level.
2. Pathogenesis in General
The principal mechanism for NAFLD development is overnutrition, which causes not only expansion of adipose tissue but also accumulation of ectopic fat in the liver. Meanwhile, macrophage infiltration of the visceral adipose tissue creates a proinflammatory state that promotes IR [14]. Inappropriate lipolysis under the influence of IR results in unabated delivery of fatty acids to the liver, which, along with increased de-novo lipogenesis (DNL), overwhelms its metabolic capacity. The imbalance in lipid metabolism leads to the formation of lipotoxic lipids that contribute to cellular stress (oxidative stress (OS) and endoplasmic reticulum (ER) stress), inflammasome activation and apoptotic cell death, and stimulation of inflammation, tissue regeneration, and fibrogenesis [7,15,16]. Inflammatory and profibrogenic macrophages are implicated in the progression of liver fibrosis and might also have a role in chronic inflammatory processes in other tissues as well [17] (Figure 1).
These pathogenic pathways of NAFLD are influenced by multiple metabolic, genetic, and microbiome-related factors that are not understood completely yet. NAFLD has a heritable component with variable penetrance estimates by 20–70% [7]. A single-nucleotide polymorphism (SNP) in the patatin-like phospholipase domain–containing 3 (PNPLA3) gene is the best characterized genetic variant associated with susceptibility to NAFLD, the importance of which have not yet been assessed properly in the Korean community. Moreover, all of known genetic variants account for a small proportion (10–20%) of overall heritability, although this proportion varies across populations. These genes might influence multiple traits such as those related with IR with divergent effects on NAFLD and cardiovascular comorbidities. Several genetic risk variants of NAFLD show a synergistic interaction with those of obesity. In addition, crosstalk between the liver and other organs (particularly, adipose tissue and the gut) via FGF19 and FGF21 might also contribute to metabolic dysregulation and inflammation in NAFLD [18,19,20,21,22] (Figure 1). Alterations in gut microbiota are seen in patients with NAFLD and some data suggest that there is a fecal-microbiome signature associated with advanced fibrosis [23,24]. However, confirmation of these bacterial signatures in different geographical regions controlling for environmental factors is required to determine their clinical significance and use for diagnostic purposes.
3. Molecular Pathways of NAFLD Progression
In around 15% of NAFLD patients, simple steatosis can evolve into NASH, a mixture of inflammation, hepatocellular injury, and fibrosis, often culminating in cirrhosis and even hepatocellular cancer [25]. Although the precise molecular mechanism underlying NAFLD progression is not completely understood, its pathogenesis on the whole has been assumed by the ‘double-hit hypothesis’ [26]. The first hit includes lipid accumulation in the liver, followed by a second hit in which proinflammatory mediators induce inflammation, hepatocellular injury, and fibrosis. Nowadays, a more complex model assumed by ‘multiple parallel hits hypothesis’ suggest that FAs and their metabolites might be truly lipotoxic and they might contribute to NAFLD progression [27,28]. It is certain that in NAFLD patients, IR leads to hepatic steatosis via multiple mechanisms [29]. Not only DNL is increased, but FAs are also taken up into liver excessively from the serum. Furthermore, a decrease in mitochondrial FA oxidation and secretion of very-low-density lipoproteins (VLDL) has been reported. It turns out that triglyceride (TG) accumulation in the cytoplasm of hepatocytes, as the hallmark of NAFLD, arises from an imbalance between lipid acquisition (FA uptake and DNL) and removal (mitochondrial FA oxidation and export) and accompanies multiple pathophysiological mechanisms in NASH [26].
The first process called DNL includes de novo synthesis of FAs through a continuing process of polymerization in the hepatocyte in which glucose is converted to acetyl-CoA by glycolysis and the oxidation of pyruvate in the beginning. Then, acetyl-CoA carboxylase (ACC1) converts acetyl-CoA into malonyl-CoA. Finally, FA synthase (FAS) catalyzes the formation of palmitic acid from malonyl-CoA and acetyl-CoA. Depending on the metabolic needs, FAs are then processed to TGs and stored or rapidly metabolized. On the whole, the rate of DNL is regulated primarily at the transcriptional level. Several nuclear transcription factors such as liver X receptor α (LXRα), sterol regulatory element-binding protein 1c (SREBP1c), carbohydrate-responsive element-binding protein (ChREBP), farnesoid X receptor (FXR), and several enzymes (ACC1, FAS, and steroyl CoA desaturase 1 (SCD1)) are involved. After the ingestion of meals, as plasma glucose and insulin levels rise, activation of lipogenesis through the activation of ChREBP and SREBP1c is promoted, respectively [26]. In humans, NAFLD has been associated with increased hepatic expression of several genes involved in DNL [26,30].
Oxidation of FAs occurs in the mitochondria, peroxisomes and the ER. It facilitates the degradation of activated FAs to acetyl-CoA. Activated long chain fatty acids (LCFAs) are shuttled across the membrane via carnitine palmitoyltransferase-1 (CPT1). Malonyl-CoA, an important intermediate of DNL, is an inhibitor of CPT1. In FA overload condition such as NAFLD and diabetes as well, cytochrome P450 (CYP4A)-dependent ω-oxidation of LCFAs occurs in the ER and induces ROS and lipid peroxidation. During the process of β-oxidation, electrons are indirectly donated to the electron transport chain (ETC) to drive ATP synthesis. Acetyl-CoA can be further processed via the tricarboxylic acid (TCA) cycle, or in the case of FA abundance, be converted into ketones. PPARα and insulin signaling are involved in the regulation of FA oxidation and the formation of ketones. In the liver, PPARα plays a pivotal role in FA metabolism by upregulating the expression of numerous genes involved in mitochondrial and peroxisome FA oxidation [30,31]. Therefore, activation of PPARα might prevent and decrease hepatic fat storage.
4. Diagnosis and Assessment of Disease Severity
NAFLD is frequently diagnosed by imaging, although it can be implicated from clinical risk scores such as fatty liver index (FLI) or identified histologically. In routine practice, the most commonly used test is abdominal ultrasonography (US) [32,33]. However, abdominal US has two important limitations: insensitivity and misdiagnosis. Advanced fibrosis can coarsen hepatic echotexture and blur vascular pattern and may lead to misdiagnosis. The sensitivity of US is low when steatosis is mild (< 30%). Instead, MRI-based measurements of hepatic steatosis can detect as little as 5% fat and are sensitive to dynamic change, but are often used in the research setting rather than in routine clinical practice in the community.
Detection of T2D among patients with NAFLD or NASH is important because improved glycemic control may improve NAFLD. NAFLD patients with T2D is associated with a more than 2 times increased risk of advanced fibrosis, cirrhosis-related complications, and liver disease mortality [7]. Obesity, dyslipidemia and hypertension are also associated with an increased risk of severe liver disease, although the effect sizes are smaller than for T2D [34,35]. Therefore, numbers of components of MS involved should be counted at first visit and could be used as an important prognostic information of NAFLD assessed easily in the routine care of NAFLD (Figure 2). Patients with NAFLD who are older than 65 years also have a higher prevalence of advanced fibrosis. A variant of the PNPLA3 gene encoding adiponutrin may be associated with NAFLD histological severity and development of hepatocellular carcinoma as well as liver-related and all-cause mortality. Recently, the PNPLA3 genotypes in addition to diabetes status were found to identify patients at a higher risk of cirrhosis among those at an indeterminate risk of NAFLD in two Caucasian cohorts [36], the clinical role of which has not been reproduced in a Korean biopsy-proven NAFLD cohort [37].
5. Non-Invasive Tests of Disease Severity
Liver enzymes (alanine aminotransferase (ALT) and aspartate aminotransferase (AST)) may be a first-step to assess and monitor patients with liver diseases. However, serum liver enzyme concentrations can be normal in more than half of patients with NAFLD, and correlate poorly with the histological severity [38]. Traditionally, liver biopsy was used to characterize and quantify histological features of steatosis, inflammation, hepatocyte ballooning, and fibrosis. However, this invasive procedure is not suitable for widespread use to assess progression or response to therapy in the community. In addition to its risk and cost, liver biopsy is prone to sampling bias. Moreover, subjective variability in histological assessment is also documented. As fibrosis has consistently emerged as the most crucial histologic feature predicting clinical events, instead, researchers have developed several non-invasive tests estimating fibrosis. Simple fibrosis scores, such as the NAFLD fibrosis score (NFS), Fibrosis-4 (FIB-4) index and AST-to-platelet ratio index (APRI) composed of demographic, clinical, and routine laboratory parameters have been developed and are ready to be applied in the community. These are inexpensive to use and can be applied easily in the Korean community [39,40]. Although the overall sensitivity of these scores is assumed not to be high, they have high negative predictive values to exclude advanced liver fibrosis. Patients with low fibrosis scores are also at a low risk of developing liver-related complications.
Another way to estimate liver fibrosis in patients with NAFLD is to measure liver stiffness by US-based and MR elastography [41]. Transient elastography (Fibro-scan) has been most extensively evaluated, is widely available, and therefore, can be used in the community. It is also possible to estimate hepatic steatosis by controlled attenuation parameter measurement at the same time. The liver stiffness measurement (LSM) also correlates with future risk of hepatocellular carcinoma and cirrhotic complications.
In the community, we may start with inexpensive simple fibrosis scores (NFS or FIB-4) as a first step to identify individuals at low risk of advanced fibrosis who can be managed in the community. Numbers of components of MS involved could be another prognostic marker of NAFLD assessed easily in the routine care in the community. Individuals with high risk of advanced fibrosis require additional assessment with Fibro-scan, or might require referral to university hospitals (secondary care) for investigation of liver disease or management of advanced fibrosis. Patients without advanced fibrosis at initial assessment might require ongoing monitoring to identify progressive liver disease and retesting 3 years after initial assessment (Figure 2) [42].
6. Comorbid Conditions
Although the risk of liver disease progression is extensive, the main cause of death in patients with NAFLD is CVDs, followed by extrahepatic malignancy such as colorectal or breast cancer [7,25]. These might be resulted from increased cardiometabolic risk factors that are shared in NAFLD and CVDs. However, it is not known to what extent NAFLD has a direct causative role in the development of CVDs. In addition to the characteristic proatherogenic lipid profile, the bidirectional relationship between NAFLD and some MS features (T2D and hypertension) is one mechanism by which NAFLD might augment cardiovascular risk [43,44]. Patients with NAFLD have a 1.9 times higher risk of incident cancers than the general population, particularly cancers involving the liver, gastrointestinal tract and uterus [45]. It might be driven by the association of NAFLD with visceral adiposity and chronic low-grade inflammation, but this mechanism has not yet been determined.
7. Prevention & Management of NAFLD
Along with new strategies in the diagnosis, risk stratification, and management of NAFLD, a few studies have succeeded in evaluating primary prevention of NAFLD, which can be organized and managed easily in the community. It turns out that improved diet quality [46] and sustained physical activity [47] reduced the risk of developing NAFLD, even among individuals with high genetic risk. As a first start, clinicians can manage to implement comprehensive programs to promote and coordinate lifestyle interventions with dietary modification and exercise, accompanied by management of metabolic comorbidities. The team approaches to fulfil these activities can be easily organized and accessed in the community level via the holistic medicine pursuing multidisciplinay approach. Having various non-invasive tests to diagnose NAFLD and liver fibrosis at hand, to screen for NAFLD and NAFLD with fibrosis can be amenable, particularly when patients participate in secondary prevention programs for T2D or MS. However, data are inconsistent, partly reflecting the paucity of available effective therapeutic interventional measures [48]. Irrespective of the possibilities of over-diagnosing NAFLD, once NAFLD is diagnosed applying simple clinical indices or abdominal US in the community, practitioners recommend risk stratification by assessing for the presence of advanced fibrosis or cirrhosis, and the evaluation of cardiovascular risk and comorbid illnesses (Figure 2).
It is certain that those patients with T2D have a high prevalence of NAFLD (40–70%), and are more likely to develop advanced fibrosis, cirrhosis, and hepatocellular carcinoma [49]. Multi-morbidity and polypharmacy are commonly found in patients with T2D and NAFLD in several community hospitals of Korea, highlighting a need for multidisciplinary management to address the complicated health care needs [50]. In university diabetes clinics, the prevalence of advanced fibrosis among patients with NAFLD is around 2 ~ 4 times higher than in the community [51,52]. Because of the increasing need to assess NAFLD and liver fibrosis that should be incorporated into the routine care of patients with T2D, the American Diabetes Association now recommends that “Patients with T2D and elevated liver enzymes (ALT) or fatty liver on US should be evaluated for the presence of NASH and liver fibrosis [53].” However, since ALT measurements are inaccurate and are within the normal range in most people with T2D and NAFLD, many patients with clinically significant liver disease will not be diagnosed. Alternatively, we can rephrase them into a better recommendation implicating that “Patients with T2D with elevated FLI or fatty liver on US should be evaluated for the presence of NASH and liver fibrosis applying simple fibrosis scores.”
8. Management of NAFLD in the Community
Although the liver related burden of NASH is substantial and increasing, CVDs and malignancy are the leading causes of death in people with NAFLD [4,43,44,45,51]. Therefore, management of NASH deserves to stick to a holistic approach that strives to minimize CV risk and to reduce inducers of steatosis and systemic inflammation. Central obesity is an important driver of disease through the promotion of IR and proinflammatory signaling. Although the nutrient content and proportion of the fat in diet is important, weight loss inducing more than 5–7% of present body weight reduces hepatic fat content and NASH, while weight loss in excess of 10% brings about even fibrosis reduction in a large proportion of people, irrespective of method of weight loss [54]. However, sustained weight loss is challenging because it requires a transformation of behavior patterns. It is difficult to adhere to calorie restriction (CR), the most crucial step for weight loss, because calorie intake must be carefully monitored every day. Ultimate success requires substantial commitment in addition to clear and solid recommendations and support from the treatment team, which might be organized at the community level. Important hurdles to weight loss such as medical comorbidities, low education levels, and little access to healthy food should be considered when developing a treatment plan. While CR is a conventional recommendation to help people with NAFLD achieve their weight reduction goals, another optional approach that limits the timing of food intake has recently been introduced. Time-restricted eating may be an attractive alternative to CR for weight loss in patients with T2D as well as in NAFLD and can be utilized easily in the community [55,56]. Alternatively, despite surgical risk, bariatric surgery in NAFLD patients with severe obesity can lead to substantial (15–25%), durable weight reduction and improvement in liver histological features of NASH and fibrosis [57]. Weight loss improves NAFLD and all of cardio-metabolic comorbidities, which then favorably affects cardiovascular and malignancy related risk. There is an independent contribution of NASH to cardiovascular and cancer risk but we do not know yet if liver targeted treatment interventions will reduce them.
9. Optimizing Management with Existing Therapeutics
Irrespective of numerous researches and activities to treat NAFLD, there is only one FDA approved therapy for NASH until now. A combination of conservative treatment (lifestyle adjustments, increasing physical activity and smoking/ alcohol cessation) appears to be beneficial. Intriguingly, several drugs that are available for other indications have been studied for NAFLD treatment (Table 1). Similar to the experiences with several hepatotonics, ursodeoxycholic acid, ω-3 fatty acids and metformin have not shown any histological benefit. Metformin, an important diabetic treatment medicine relieving IR has no effect on NASH disease activity [58]. Vitamin E and pioglitazone have been endorsed by current guidelines as possible treatment in patients with NASH [59,60,62,63]. The benefits of vitamin E for NASH have been proved in several studies of patients without diabetes or cirrhosis. In a trial of patients with T2D and NASH, combination therapy of vitamin E with pioglitazone achieved improvement of NASH without worsening of fibrosis [62]. Nonetheless, vitamin E can only be used taking potential adverse effects (increased risk of bleeding and adverse cardiovascular outcomes in higher doses) into account. Although statins have no discernible histological benefit on NASH, they should be used for cardiovascular risk reduction.
Thiazolidinediones (TZDs), to which pioglitazone belong, activate PPARγ in adipose tissue and has been proposed to promote differentiation of adipocytes and storage of fat in adipose tissue, protecting peripheral tissues from lipotoxicity [73]. Fortunately, all TZDs are highly effective in improving NAFLD outcomes. Multiple trials in NASH patients with and without diabetes have shown that pioglitazone improves NASH activity with a some improvement in fibrosis [73,74]. Weight gain and the risk of bone loss are side effects. Accordingly, it appears unlikely that either vitamin E or pioglitazone will be studied in phase 3 studies. Alternatively, other drugs that modulate PPAR-γ and complementary mechanisms are being developed. GLP-1 receptor agonists [65,66,75,76] and SGLT2 inhibitors [66,77,78], antidiabetic medications that are cardioprotective and renoprotective are currently being studied in several trials to assess their efficacy in NASH resolution and improvement in fibrosis. These drugs have additional benefit of inducing weight loss. Several GLP-1 receptor agonists are being evaluated for the treatment of NASH with some success. In a phase 2 trial, s.c. semaglutide 0.4 mg daily proved NASH resolution without worsening of fibrosis [64]. Although it is difficult to discern if this effect is independent of weight loss, it shows the highest rate of NASH resolution ever reported in NASH therapeutic trials [77,78]. Interestingly, in a recent Korean study of T2D with NAFLD, SGLT2 inhibitors shows a higher NAFLD regression and lower adverse liver-related outcomes compared with other oral anti-diabetic drugs including TZDs [79].
10. Emerging Therapeutics of NASH
Numerous drugs of NASH treatment with different mechanisms of action, aiming to target lipid metabolism, inflammatory, or fibrotic pathways, are in development [80] (Figure 1). Trials utilizing potent FXR agonist has proven favorable results [67,81,82]. A trial of obeticholic acid [81] was implemented as the first phase 3 trial to prove an improvement in fibrosis without worsening of NASH, confirming the findings of the previous phase 2 trial [67,82]. However, the magnitude of response was modest, suggesting that combination therapy will be required to treat the majority of patients adequately. Although obeticholic acid failed to achieve complete NASH resolution, it did improve individual histological features. However, pruritus and increase in LDL concentration are side effects of obeticholic acid. Recently, the selective thyroid hormone receptor β (THR-β) agonists are found to be effective in the treatment of NAFLD [69,70], and approved by FDA. In addition, irrespective of multiple failures caused by disease heterogeneity, several other drugs are in advanced stages of development for NASH [68,71,72]. However, future treatment will require combination therapy since the modest effect and potential side effects in higher doses of these drugs. Several combination trials are also now underway. The ATLAS trial showed an improvement in fibrosis with cilofexor (a FXR agonist) and firsocostat (a ACC inhibitor) in patients with NASH and fibrosis [83]. Patients receiving this combination were more likely to have better improvement in the NAFLD activity score than those receiving monotherapy. Given the modest difference, more effective combinations will be needed.
11. MiRNA Targeting for NAFLD
NAFLD is associated with thorough reprogramming of hepatic metabolism. Research indicates that various metabolic pathways deregulated in NAFLD converge in the aberrant accumulation of lipids into hepatocytes. In recent years, microRNAs (miRs) have been proposed to halt the development and progression of NAFLD as alterations of epigenetic mechanisms may contribute to these hepatic metabolic changes [84]. As elevated glucose levels can lead to increased DNL, miR-dependent alterations of hepatic glycolysis, gluconeogenesis and glycogen metabolism are key pathological mechanisms contributing to NAFLD development. In addition, deregulated cellular processes, such as autophagy or ER stress and the UPR were also implicated in steatosis and shown to be under the control of several miRs. However, to develop an efficient miR-based therapeutic strategy, targeting common key transcription factors involved in hepatic glucose and lipid metabolism would be important to have a broader systemic effect on NAFLD [85]. MiR-192 and miR-29, which are both deregulated in the liver of patients with NAFLD, were reported to target SREBP1, while ChREBP is regulated by miR-1322 in hepatocytes. LXR, which can regulate the activity of both SREBP1 and ChREBP, was also found to be targeted by several miRs (miR-1, miR-155, miR-206 and miR-613). PPARγ, a lipogenic transcription factor, was found to be regulated by miR-27a, miR-34a, miR-128 and miR130. In addition, PPARγ is also involved in hepatic stellate cells activation repression, thereby negatively regulating hepatic fibrosis. MiR-696 and miR-130a are targeting its cofactor, PGC1α, while miR-16 and miR-100 are acting on its repressor, NCOR. Another strategy to alleviate steatosis in the liver is to activate lipid oxidation by derepressing expression of PPARα. PPARα was shown to be targeted by miR-9, miR-10b, miR-21, miR-33 and miR-199a. However, as all these transcription factors or cofactors are provisional potential targets to be regulated, which have been examined only in some cell lines and/ or in animal models, their real influence in NAFLD development and progression in man have not yet been determined.
12. Therapeutic Potential of a New Antioxidant Protein Delivery in NAFLD
Though diabetes and/ or NAFLD progression commonly associate with increased OS, only vitamin E, an important antioxidant, but not other antioxidants have been shown to improve the histology of NAFLD. These inconsistent effects of antioxidants might be resulted from diverse factors such as difficulty in maintaining a consistent circulating antioxidant level, inadequate tissue distribution, and lack of suitable exogenous antioxidants. Therapeutic antioxidants should be given in appropriate cellular concentration enough to tackle newly generating ROS levels without significant toxicity [86]. Therefore, a different way of delivering medicines having antioxidant properties has been studied [87]. If antioxidant in general are to improve the pathophysiology in various stages of NAFLD, steady delivery at required concentrations into the cells or into the cellular compartment where generates ROS would be most important. A strategy to induce an endogenous and nonspecific antioxidant or to deliver it in a more efficient way could be a more attractive approach. As NAFLD progression might be resulted from OS in mitochondria, ER and others (especially in hepatocyte as well as stellate cells) due to lipotoxicity, hypoxia and AGE accumulation, endogenous nonspecific antioxidant treatment may improve tissue repair in various stages of NAFLD. Therefore, nonspecific antioxidants such as metallothionein (MT), SOD and catalase have been exploited to combat increased ROS in various tissues applying intracellular delivery [86,87,88,89,90]. Taking advantage of the recently developed cell-penetrating peptide technologies, each of these antioxidants and their combination inhibited various OS and had the potential to protect cells and tissues against NAFLD progression as well as diabetes and its complications due to its anti-apoptotic and anti-oxidant effects either in vitro or in vivo [90]. Tat-MT and Tat-SOD given in combination intraperitoneally at regular interval were protective against various injuries and protected against steatosis as well as inflammatory condition in OLETF rats (unpublished data). This result is reminiscent of similar delay in development of NASH by vitamin E.
13. Challenges and Prospects
Although progress has been made during the past decades in investigating the natural history and underlying biology of NAFLD, there are still many areas of challenges and obstacles. NAFLD at large and NASH in particular are poorly understood and recognized by health care professionals working in the community, especially in Korea. Implementation of appropriate strategies to identify and manage at-risk patients of NAFLD with advanced fibrosis will ask for timely action by clinicians in community care, diabetes clinics, and other specialists who treat patients with metabolic risk factors. There is an increasing need for the awareness of a multi-pronged public health approaches to cope with increased NAFLD risk factors in rapidly modernizing community. When we consider liver fibrosis, a key prognostic marker for liver-related outcomes can be assessed with combinations of non-invasive tests in the routine care of the patients in the community, these challenges can be overcome irrespective of the obesogenic environment. In addition, there should be several obstacles to develop highly effective therapeutic measures of intervention. One of the most important challenges in the community hospital is a long-term necessity of liver biopsy for diagnosis and follow-up. Although reliable biomarkers that can accurately diagnose and stage NAFLD across the entire disease spectrum does not yet exist, a diagnostic biomarker, in conjunction with a prognostic biomarker, would allow the identification of high-risk individuals on whom resources should be concentrated. A second challenge is the substantial heterogeneity of NAFLD and the current limited understanding of disease phenotypes. The ability to phenotype patients would permit more accurate prognostication, selection of appropriate therapy, and prediction of treatment response than is currently possible. Lastly, the refinement of therapeutic strategies into thoughtful combination approaches, tailored to the patient’s individual disease inducers, are needed for increased response rates and a change in our attitude to screening. Finally, regardless of the progress that has been, or will be, made in diagnostic tests and drug treatments, healthy lifestyle and weight reduction remains crucial for the prevention and treatment of NAFLD, as obesity is the main driver of this common liver disease and its associated metabolic comorbidities.
References
- Park Y, Lee HK, Koh C-S, Min HK, Yoo KY, Kim YI, Shin YS: Prevalence of diabetes mellitus and IGT in Yonchon County, Korea. Diabetes Care 18: 534-538, 1995.
- Shin CS, Lee HK, Koh C-S, Kim YI, Shin YS, Yoo KY, Paik HY, Park Y, Yang BG: Risk factors for the development of NIDDM in Yonchon County, Korea. 1: Diabetes Care 20(12), 1842.
- Younossi, Z.M.; Koenig, A.B.; Abdelatif, D.; Fazel, Y.; Henry, L.; Wymer, M. Global epidemiology of nonalcoholic fatty liver disease—meta-analytic assessment of prevalence, incidence, and outcomes. Hepatology 2016; 64: 73–84.
- Younossi Z, Anstee QM, Marietti M, Hardy T, Henry L, Eslam M, George J, Bugianesi E: Global burden of NAFLD and NASH: trends, predictions, risk factors and prevention. Nat Rev Gastroenterol Hepatol 2018; 15: 11–20.
- Park Y, Kim TW: Liver cirrhosis and diabetes mellitus. Taehan Kan Hakhoe Chi 8(1): 22-34, 2002.
- Paik, J.M.; Golabi, P.; Younossi, Y.; Mishra, A.; Younossi, Z.M. Changes in the global burden of chronic liver diseases from 2012 to 2017: the growing impact of NAFLD. Hepatology 2020; 72: 1605–16.
- Powell, E.E.; Wong, V.W.-S.; Rinella M:, N.A.F.L.D. Lancet 2021; 397:, 2212–24.
- Estes, C.; Razavi, H.; Loomba, R.; Younossi, Z.; Sanyal, A.J. Modeling the epidemic of nonalcoholic fatty liver disease demonstrates an exponential increase in burden of disease. Hepatology 2018; 67: 123–33.
- Cusi K, Isaacs S, Barb D, Basu R, Caprio S, Garvey WT, Kashyap S, Mechanick JI, Mouzaki M, Nadolsky K, Rinella ME, Vos MB, Younossi Z: American association of clinical endocrinology clinical practice guideline for the diagnosis and management of non-alcoholic fatty liver disease in primary care and endocrinology clinical settings: Co-sponsored by the American association for the study of liver diseases (AASLD). Endocr Pract 2022; 28(5):528-562.
- Eslam M, Newsome PN, Sarin SK, Anstee QM, Targher G, Romero-Gomez M, Zelber-Sagi S, Wong VW, Dufour JF, Schattenberg JM, Kawaguchi T, Arrese M, Valenti L, Shiha G, Tiribelli C, Yki-Järvinen H, Fan JG, Grønbæk H, Yilmaz Y, Cortez-Pinto H, Oliveira CP, Bedossa P, Adams LA, Zheng MH, Fouad Y, Chan WK, Mendez-Sanchez N, Ahn SH, Castera L, Bugianesi E, Ratziu V, George J: A new definition for metabolic dysfunction-associated fatty liver disease: an international expert consensus statement. J Hepatol 2020; 73: 202–09.
- Hue, L.; Taegtmeyer, H. The Randle cycle revisited: a new head for an old hat. Am J Physiol Endocrinol Metab 2009; 297: E578-91.
- García-Ruiz, C.; Baulies, A.; Mari, M.; García-Rovés, P.M.; Fernandez-Checa, J.C. Mitochondrial dysfunction in non-alcoholic fatty liver disease and insulin resistance: cause or consequence? Free Radic Res. 2013; 47: 854-68.
- Smith, G.I.; Shankaran, M.; Yoshino, M.; Schweitzer, G.G.; Chondronikola, M.; Beals, J.W.; Okunade, A.L.; Patterson, B.W.; Nyangau, E.; Field, T.; Sirlin, C.B.; Talukdar, S.; Hellerstein, M.K.; Klein, S. Insulin resistance drives hepatic de novo lipogenesis in nonalcoholic fatty liver disease. J Clin Invest 2020; 130: 1453-1460.
- Barrow, F.; Khan, S.; Wang, H. ; Revelo XS: The emerging role of B cells in the pathogenesis of, N.A.F.L.D. Hepatology 2021; 74: 2277-2286.
- Friedman, S.L.; Neuschwander-Tetri, B.A.; Rinella, M.; Sanyal, A.J. Mechanisms of NAFLD development and therapeutic strategies. Nat Med 2018; 24: 908–22.
- Sanyal, A.J. Past, present and future perspectives in nonalcoholic fatty liver disease. Nat Rev Gastroenterol Hepatol.
- Lefere, S.; Tacke, F. Macrophages in obesity and non-alcoholic fatty liver disease: crosstalk with metabolism. JHEP Rep.
- Azzu, V.; Vacca, M.; Virtue, S.; Allison, M.; Vidal-Puig, A. Adipose tissue liver cross talk in the control of whole-body metabolism: implications in nonalcoholic fatty liver disease. Gastroenterology 2020; 158: 1899–912.
- Aron-Wisnewsky, J.; Warmbrunn, M.V.; Nieuwdorp, M.; Clément, K. Nonalcoholic fatty liver disease: modulating gut microbiota to improve severity? Gastroenterology 2020; 158: 1881–98.
- Somm E, Jornayvaz FR: Fibroblast Growth Factor 15/19: From Basic Functions to Therapeutic Perspectives. Endocr Rev 2018; 39: 960–989.
- Asrih, M.; Altirriba, J.; Rohner-Jeanrenaud, F.; Jornayvaz, F.R. Ketogenic Diet Impairs FGF21 Signaling and Promotes Differential Inflammatory Responses in the Liver and White Adipose Tissue. PLoS ONE, 2015; 10: e0126364. [Google Scholar]
- Author’s unpublished observation.
- Loomba R, Seguritan V, Li W, Long T, Klitgord N, Bhatt A, Dulai PS, Caussy C, Bettencourt R, Highlander SK, Jones MB, Sirlin CB, Schnabl B, Brinkac L, Schork N, Chen CH, Brenner DA, Biggs W, Yooseph S, Venter JC, Nelson KE: Gut microbiome-based metagenomic signature for non-invasive detection of advanced fibrosis in human nonalcoholic fatty liver disease. Cell Metab, 2017; 25: 1054–62.e5.
- Caussy C, Tripathi A, Humphrey G, Bassirian S, Singh S, Faulkner C, Bettencourt R, Rizo E, Richards L, Xu ZZ, Downes MR, Evans RM, Brenner DA, Sirlin CB, Knight R, Loomba R: A gut microbiome signature for cirrhosis due to nonalcoholic fatty liver disease. Nat Commun, 2019; 10: 1406.
- Inciardi RM, Mantovani A, Targher G: Non-alcoholic fatty liver disease as an emerging risk factor for heart failure. Curr Heart Fail Rep. 2023; 20(4):308-319.
- Badmus OO, Hillhouse SA, Anderson CD, Hinds TD, Stec DE: Molecular mechanisms of metabolic associated fatty liver disease (MAFLD): functional analysis of lipid metabolism pathways. Clin Sci (Lond). 2022; 136(18):1347-1366.
- Buzzetti E, Pinzani M, Tsochatzis EA: The multiple-hit pathogenesis of non-alcoholic fatty liver disease (NAFLD). Metabolism 2016; 65: 1038–1048.
- Parthasarathy G, Revelo X, Malhi H: Pathogenesis of Nonalcoholic Steatohepatitis: An Overview. Hepatol Commun, 2020; 4: 478–492.
- Ferguson D, Finck BN: Emerging therapeutic approaches for the treatment of NAFLD and type 2 diabetes mellitus. Nat Rev Endocrinol. 2021; 17(8):484-495.
- Samuel, V.T.; Shulman, G.I. Nonalcoholic fatty liver disease as a nexus of metabolic and hepatic diseases. Cell Metab, 2018;27:22–41. [Google Scholar]
- Qiu YY, Zhang J, Zeng FY, Zhu YZ: Roles of the peroxisome proliferator-activated receptors (PPARs) in the pathogenesis of nonalcoholic fatty liver disease (NAFLD). Pharmacol Res 2023; 192:106786.
- Bril F, Ortiz-Lopez C, Lomonaco R, Orsak B, Freckleton M, Chintapalli K, Hardies J, Lai S, Solano F, Tio F, Cusi K: Clinical value of liver ultrasound for the diagnosis of nonalcoholic fatty liver disease in overweight and obese patients. Liver Int, 2015; 35: 2139–46.
- Wong, V.W.; Adams, L.A.; de Lédinghen, V.; Wong, G.L.; Sookoian, S. Noninvasive biomarkers in NAFLD and NASH—current progress and future promise. Nat Rev Gastroenterol Hepatol, 2018; 15: 461–78. [Google Scholar]
- Jarvis H, Craig D, Barker R, Spiers G, Stow D, Anstee QM, Hanratty B: Metabolic risk factors and incident advanced liver disease in non-alcoholic fatty liver disease (NAFLD): a systematic review and meta-analysis of population-based observational studies. PLoS Med, 2020; 17: e1003100.
- Pitisuttithum P, Chan WK, Piyachaturawat P, Imajo K, Nakajima A, Seki Y, Kasama K, Kakizaki S, Fan JG, Song MJ, Yoon SK, Dan YY, Lesmana L, Ho KY, Goh KL, Wong VWS, Treeprasertsuk S: Predictors of advanced fibrosis in elderly patients with biopsy-confirmed nonalcoholic fatty liver disease: the GOASIA study. BMC Gastroenterol, 2020; 20: 88.
- Chen VL, Oliveri A, Miller MJ, et al. PNPLA3 Genotype and Diabetes Identify Patients With Nonalcoholic Fatty Liver Disease at High Risk of Incident Cirrhosis. Gastroenterology, 2023;164:966-977.e17.
- Koo, B.K.; Lee, D.H.; Park, J.H.; Kim, W. Heterogeneity in the risk of incident liver cirrhosis driven byPNPLA3genotype and diabetes among different populations. Hepatobiliary Surg Nutr, 2024;13(1):115-118. [Google Scholar]
- Wong VW, Wong GL, Tsang SW, Hui AY, Chan AW, Choi PC, Chim AM, Chu S, Chan FK, Sung JJ, Chan HL: Metabolic and histological features of non-alcoholic fatty liver disease patients with different serum alanine aminotransferase levels. Aliment Pharmacol Ther, 2009; 29: 387–396.
- Mahady SE, Macaskill P, Craig JC, Wong GLH, Chu WCW, Chan HLY, George J, Wong VWS: Diagnostic accuracy of noninvasive fibrosis scores in a population of individuals with a low prevalence of fibrosis. Clin Gastroenterol Hepatol, 2017; 15: 1453–60.e1.
- Hagström, H.; Talbäck, M.; Andreasson, A.; Walldius, G.; Hammar, N. Ability of noninvasive scoring systems to identify individuals in the population at risk for severe liver disease. Gastroenterology, 2020; 158: 200–14. [Google Scholar]
- Eddowes PJ, Sasso M, Allison M, Tsochatzis E, Anstee QM, Sheridan D, Guha IN, Cobbold JF, Deeks JJ, Paradis V, Bedossa P, Newsome PN: Accuracy of FibroScan controlled attenuation parameter and liver stiffness measurement in assessing steatosis and fibrosis in patients with nonalcoholic fatty liver disease. Gastroenterology, 2019; 156: 1717–30.
- Tsochatzis EA, Newsome PN: Non-alcoholic fatty liver disease and the interface between primary and secondary care. Lancet Gastroenterol Hepatol, 2018; 3: 509–17.
- Lee YH, Cho Y, Lee BW, Park CY, Lee DH, Cha BS, Rhee EJ: Nonalcoholic fatty liver disease in diabetes. Part I: epidemiology and diagnosis. Diabetes Metab J, 2019;43:31-45.
- Lucero D, Miksztowicz V, Gualano G, Longo C, Landeira G, Álvarez E, Zago V, Brites F, Berg G, Fassio E, Schreier L: Nonalcoholic fatty liver disease associated with metabolic syndrome: Influence of liver fibrosis stages on characteristics of very low-density lipoproteins. Clin Chim Acta. 2017; 473:1-8.
- Allen AM, Hicks SB, Mara KC, Larson JJ, Therneau TM: The risk of incident extrahepatic cancers is higher in non-alcoholic fatty liver disease than obesity - a longitudinal cohort study. J Hepatol, 2019; 71: 1229–36.
- Ma J, Hennein R, Liu C, Long MT, Hoffmann U, Jacques PF, Lichtenstein AH, Hu FB, Levy D: Improved diet quality associates with reduction in liver fat, particularly in individuals with high genetic risk scores for nonalcoholic fatty liver disease. Gastroenterology, 2018; 155: 107–17.
- Gerage AM, Ritti-Dias RM, Balagopal PB, Conceição RD, Umpierre D, Santos RD, Cucato GG, Bittencourt MS: Physical activity levels and hepatic steatosis: a longitudinal follow-up study in adults. J Gastroenterol Hepatol, 2018; 33: 741–46.
- Chalasani N, Younossi Z, Lavine JE, Charlton M, Cusi K, Rinella M, Harrison SA, Brunt EM, Sanyal AJ: The diagnosis and management of nonalcoholic fatty liver disease: practice guidance from the American Association for the Study of Liver Diseases. Hepatology, 2018; 67: 328–57.
- Anstee, Q.M.; Targher, G.; Day, C.P. Progression of NAFLD to diabetes mellitus, cardiovascular disease or cirrhosis. Nat Rev Gastroenterol Hepatol, 2013; 10: 330–44. [Google Scholar]
- Patel PJ, Hayward KL, Rudra R, Horsfall LU, Hossain F, Williams S, Johnson T, Brown NN, Saad N, Clouston AD, Stuart KA, Valery PC, Irvine KM, Russell AW, Powell EE: Multimorbidity and polypharmacy in diabetic patients with NAFLD: implications for disease severity and management. Medicine (Baltimore), 2017; 96: e6761.
- Lee BW, Lee YH, Park CY, Rhee EJ, Lee WY, Kim NH, Choi KM, Park KG, Choi YK, Cha BS, Lee DH; Korean Diabetes Association (KDA) Fatty Liver Research Group: Non-alcoholic fatty liver disease in patients with type 2 diabetes mellitus: a position statement of the fatty liver research group of the Korean diabetes association. Diabetes Metab J, 2020; 44: 382–401.
- Cusi, K. A diabetologist’s perspective of non-alcoholic steatohepatitis (NASH): knowledge gaps and future directions. Liver Int, 2020; 40 (suppl 1): 82–88. [Google Scholar]
- American Diabetes Association. 4. Comprehensive medical evaluation and assessment of comorbidities: standards of medical care in diabetes—2019. Diabetes Care 2019; 42 (suppl 1): S34–45.
- Vilar-Gomez E, Martinez-Perez Y, Calzadilla-Bertot L, Torres-Gonzalez A, Gra-Oramas B, Gonzalez-Fabian L, Friedman SL, Diago M, Romero-Gomez M: Weight loss through lifestyle modification significantly reduces features of nonalcoholic steatohepatitis. Gastroenterology, 2015; 149: 367–78.e5.
- Pavlou V, Cienfuegos S, Lin S, Ezpeleta M, Ready K, Corapi S, Wu J, Lopez J, Gabel K, Tussing-Humphreys L, Oddo VM, Alexandria SJ, Sanchez J, Unterman T, Chow LS, Vidmar AP, Varady KA, Effect of time-restricted eating on weight loss in adults with type 2 diabetes. A randomized clinical trial. JAMA Netw Open, 2023;6(10):e2339337.
- Wilkinson MJ, Manoogian ENC, Zadourian A, Lo H, Fakhouri S, Shoghi A, Wang X, Fleischer JG, Navlakha S, Panda S, Taub PR: Ten-hour time-restricted eating reduces weight, blood pressure, and atherogenic lipids in patients with metabolic syndrome. Cell Metab. 2020;31(1):92-104.e5.
- Lassailly G, Caiazzo R, Ntandja-Wandji L-C, Gnemmi V, Baud G, Verkindt H, Ningarhari M, Louvet A, Leteurtre E, Raverdy V, Dharancy S, Pattou F, Mathurin P: Bariatric surgery provides long-term resolution of nonalcoholic steatohepatitis and regression of fibrosis. Gastroenterology, 2020; 159: 1290–301.e5.
- Musso G, Cassader M, Rosina F, Gambino R: Impact of current treatments on liver disease, glucose metabolism and cardiovascular risk in non-alcoholic fatty liver disease (NAFLD): a systematic review and meta-analysis of randomised trials. Diabetologia, 2012; 55: 885-904.
- Sanyal AJ, Chalasani N, Kowdley KV, McCullough A, Diehl AM, Bass NM, Neuschwander-Tetri BA, Lavine JE, Tonascia J, Unalp A, Van Natta M, Clark J, Brunt EM, Kleiner DE, Hoofnagle JH, Robuck PR; NASH CRN: Pioglitazone, vitamin E, or placebo for nonalcoholic steatohepatitis. N Engl J Med, 2010; 362: 1675–85.
- Cusi K, Orsak B, Bril F, Lomonaco R, Hecht J, Ortiz-Lopez C, Tio F, Hardies J, Darland C, Musi N, Webb A, Portillo-Sanchez P: Long-term pioglitazone treatment for patients with nonalcoholic steatohepatitis and prediabetes or type 2 diabetes mellitus: a randomized trial. Ann Intern Med, 2016; 165: 305–15.
- Athyros VG, Mikhailidis DP, Didangelos TP, Giouleme OI, Liberopoulos EN, Karagiannis A, Kakafika AI, Tziomalos K, Burroughs AK, Elisaf MS: Effect of multifactorial treatment on non-alcoholic fatty liver disease in metabolic syndrome: a randomised study. Curr Med Res Opin, 2006; 22: 873-83.
- Vilar-Gomez E, Vuppalanchi R, Gawrieh S, Ghabril M, Saxena R, Cummings OW, Chalasani N: Vitamin E improves transplant-free survival and hepatic decompensation among patients with nonalcoholic steatohepatitis and advanced fibrosis. Hepatology, 2020; 71: 495–509.
- Bril F, Biernacki DM, Kalavalapalli S, Lomonaco R, Subbarayan SK, Lai J, Tio F, Suman A, Orsak BK, Hecht J, Cusi K: Role of vitamin E for nonalcoholic steatohepatitis in patients with type 2 diabetes: a randomized controlled trial. Diabetes Care, 2019; 42: 1481–88.
- Armstrong MJ, Gaunt P, Aithal GP, Barton D, Hull D, Parker R, Hazlehurst JM, Guo K; LEAN trial team; Abouda G, Aldersley MA, Stocken D, Gough SC, Tomlinson JW, Brown RM, Hübscher SG, Newsome PN: Liraglutide safety and efficacy in patients with non-alcoholic steatohepatitis (LEAN): a multicentre, double-blind, randomised, placebo-controlled phase 2 study. Lancet, 2016; 387: 679–90.
- Newsome PN, Buchholtz K, Cusi K, Linder M, Okanoue T, Ratziu V, Sanyal AJ, Sejling AS, Harrison SA; NN9931-4296 Investigators: A placebo-controlled trial of subcutaneous semaglutide in nonalcoholic steatohepatitis. N Engl J Med, 2021; 384: 1113–24.
- Eriksson JW, Lundkvist P, Jansson PA, Johansson L, Kvarnström M, Moris L, Miliotis T, Forsberg GB, Risérus U, Lind L, Oscarsson J: Effects of dapagliflozin and n-3 carboxylic acids on non-alcoholic fatty liver disease in people with type 2 diabetes: a double-blind randomised placebo-controlled study. Diabetologia, 2018; 61: 1923-1934.
- Neuschwander-Tetri BA, Loomba R, Sanyal AJ, Lavine JE, Van Natta ML, Abdelmalek MF, Chalasani N, Dasarathy S, Diehl AM, Hameed B, Kowdley KV, McCullough A, Terrault N, Clark JM, Tonascia J, Brunt EM, Kleiner DE, Doo E; NASH Clinical Research Network: Farnesoid X nuclear receptor ligand obeticholic acid for non-cirrhotic, non-alcoholic steatohepatitis (FLINT): a multicentre, randomised, placebo-controlled trial. Lancet, 2015; 385: 956–65.
- Gawrieh S, Noureddin M, Loo N, Mohseni R, Awasty V, Cusi K, Kowdley KV, Lai M, Schiff E, Parmar D, Patel P, Chalasani N: Saroglitazar, a PPAR-α/γ Agonist, for Treatment of NAFLD: A Randomized Controlled Double-Blind Phase 2 Trial. Hepatology, 2021; 74:1809-1824.
- Harrison SA, Bashir MR, Guy CD, Zhou R, Moylan CA, Frias JP, Alkhouri N, Bansal MB, Baum S, Neuschwander-Tetri BA, Taub R, Moussa SE: Resmetirom (MGL-3196) for the treatment of non-alcoholic steatohepatitis: a multicentre, randomised, double-blind, placebo-controlled, phase 2 trial. Lancet, 2019; 394: 2012–24.
- Harrison SA, Bedossa P, Guy CD, Schattenberg JM, Loomba R, Taub R, Labriola D, Moussa SE, Neff GW, Rinella ME, Anstee QM, Abdelmalek MF, Younossi Z, Baum SJ, Francque S, Charlton MR, Newsome PN, Lanthier N, Schiefke I, Mangia A, Pericàs JM, Patil R, Sanyal AJ, Noureddin M, Bansal MB, Alkhouri N, Castera L, Rudraraju M, Ratziu V; MAESTRO-NASH Investigators: A Phase 3, Randomized, Controlled Trial of Resmetirom in NASH with Liver Fibrosis. N Engl J Med. 2024; 390:497-509.
- Harrison SA, Neff G, Guy CD, Bashir MR, Paredes AH, Frias JP, Younes Z, Trotter JF, Gunn NT, Moussa SE, Kohli A, Nelson K, Gottwald M, Chang WCG, Yan AZ, DePaoli AM, Ling L, Lieu HD: Efficacy and Safety of Aldafermin, an Engineered FGF19 Analog, in a Randomized, Double-Blind, Placebo-Controlled Trial of Patients With Nonalcoholic Steatohepatitis. Gastroenterology, 2021; 160: 219-231.e1.
- Loomba, R.; Sanyal, A.J.; Kowdley, K.V.; Bhatt, D.L.; Alkhouri, N.; Frias, J.P.; Bedossa, P.; Harrison, S.A.; Lazas, D.; Barish, R.; Gottwald, M.D.; Feng, S.; Agollah, G.D.; Hartsfield, C.L.; Mansbach, H.; Margalit, M. ; Abdelmalek MF: Randomized controlled trial of the FGF21 analogue Pegozafermin in, N.A.S.H. N Engl J Med 2023; 389: 998-1008.
- Celi, F.S.; Shuldiner, A.R. The role of peroxisome proliferator-activated receptor gamma in diabetes and obesity. Curr Diab Rep, 2002;2(2):179-185. [Google Scholar]
- Belfort R, Harrison SA, Brown K, Darland C, Finch J, Hardies J, Balas B, Gastaldelli A, Tio F, Pulcini J, Berria R, Ma JZ, Dwivedi S, Havranek R, Fincke C, DeFronzo R, Bannayan GA, Schenker S, Cusi K: A placebo-controlled trial of pioglitazone in subjects with nonalcoholic steatohepatitis. N Engl J Med, 2006; 355: 2297–307.
- Marso SP, Bain SC, Consoli A, Eliaschewitz FG, Jódar E, Leiter LA, Lingvay I, Rosenstock J, Seufert J, Warren ML, Woo V, Hansen O, Holst AG, Pettersson J, Vilsbøll T; SUSTAIN-6 Investigators: Semaglutide and cardiovascular outcomes in patients with type 2 diabetes. N Engl J Med, 2016; 375: 1834–44.
- O’Neil PM, Birkenfeld AL, McGowan B, Mosenzon O, Pedersen SD, Wharton S, Carson CG, Jepsen CH, Kabisch M, Wilding JPH: Efficacy and safety of s\emaglutide compared with liraglutide and placebo for weight loss in patients with obesity: a randomised, double-blind, placebo and active controlled, dose-ranging, phase 2 trial. Lancet, 2018; 392: 637–49.
- Hsiang JC, Wong VW. SGLT2 inhibitors in liver patients. Clin Gastroenterol Hepatol, 2020; 18: 2168–72.e2.
- Zinman B, Wanner C, Lachin JM, Fitchett D, Bluhmki E, Hantel S, Mattheus M, Devins T, Johansen OE, Woerle HJ, Broedl UC, Inzucchi SE; EMPA-REG OUTCOME Investigators: Empagliflozin, cardiovascular outcomes, and mortality in type 2 diabetes. N Engl J Med, 2015; 373: 2117–28.
- Jang H, Kim Y, Lee DH, Joo SK, Koo BK, Lim S, Lee W, Kim W: Outcomes of various classes of oral antidiabetic drugs on nonalcoholic fatty liver disease. JAMA Intern Med. Published online , 2024.
- Neuschwander-Tetri, B.A. Therapeutic landscape for NAFLD in 2020. Gastroenterology 2020; 158: 1984–98.e3.
- Younossi ZM, Ratziu V, Loomba R, Rinella M, Anstee QM, Goodman Z, Bedossa P, Geier A, Beckebaum S, Newsome PN, Sheridan D, Sheikh MY, Trotter J, Knapple W, Lawitz E, Abdelmalek MF, Kowdley KV, Montano-Loza AJ, Boursier J, Mathurin P, Bugianesi E, Mazzella G, Olveira A, Cortez-Pinto H, Graupera I, Orr D, Gluud LL, Dufour JF, Shapiro D, Campagna J, Zaru L, MacConell L, Shringarpure R, Harrison S, Sanyal AJ; REGENERATE Study Investigators: Obeticholic acid for the treatment of non-alcoholic steatohepatitis: interim analysis from a multicentre, randomised, placebo-controlled phase 3 trial. Lancet, 2019; 394: 2184–96.
- Pockros PJ, Fuchs M, Freilich B, Schiff E, Kohli A, Lawitz EJ, Hellstern PA, Owens-Grillo J, Van Biene C, Shringarpure R, MacConell L, Shapiro D, Cohen DE: CONTROL: a randomized phase 2 study of obeticholic acid and atorvastatin on lipoproteins in nonalcoholic steatohepatitis patients. Liver Int, 2019; 39: 2082–93.
- Loomba R, Noureddin M, Kowdley KV, Kohli A, Sheikh A, Neff G, Bhandari BR, Gunn N, Caldwell SH, Goodman Z, Wapinski I, Resnick M, Beck AH, Ding D, Jia C, Chuang JC, Huss RS, Chung C, Subramanian GM, Myers RP, Patel K, Borg BB, Ghalib R, Kabler H, Poulos J, Younes Z, Elkhashab M, Hassanein T, Iyer R, Ruane P, Shiffman ML, Strasser S, Wong VW, Alkhouri N; for the ATLAS Investigators: Combination therapies including cilofexor and firsocostat for bridging fibrosis and cirrhosis attributable to NASH. Hepatology, 2021; 73: 625–43.
- Hochreuter MY, Dall M, Treebak JT, Barrès R: MicroRNAs in non-alcoholic fatty liver disease: Progress and perspectives, Mol Metab 2022; 65:101581. Epub 2022 Aug 23.
- 2: M, Sobolewski C, Dolicka D, de Sousa MC, Foti M: miRNAs and NAFLD: from pathophysiology to therapy, Gut 2019;68, 2019.
- Park L, Min D, Kim H, Chung HY, Lee CH, Park IS, Kim Y, Park Y: TAT-enhanced delivery of metallothionein can partially prevent the development of diabetes. Free Radic Biol Med, 2011;51(9):1666-74.
- Min, D.; Kim, H.; Park, L.; Kim, T.H.; Hwang, S.; Kim, M.J.; Jang, S. ; Park Y: Amelioration of diabetic neuropathy by TAT-mediated enhanced delivery of metallothionein, S.O.D. Endocrinology 2012;153(1):81-91.
- Park L, Min D, Kim H, Park J, Choi S, Park Y: The combination of metallothionein and superoxide dismutase protects pancreatic β cells from oxidative damage. Diab Metab Res Rev, 2011; 27(8):802-8.
- Park Y, Kim H, Park L, Min D, Park J, Choi S, Park MH: Effective delivery of endogenous antioxidants ameliorates diabetic nephropathy. PLOS One, 2015;10(6): e0130815.
- Park Y, Cai L: Reappraisal of metallothionein; Clinical applications in patients with diabetes mellitus. J Diabetes, 2018;10(3): 213-231.
Figure 1.
Schematic presentation of pathogenesis of NAFLD and possible mechanisms of action of available treatment strategies. The imbalance in lipid metabolism due to overnutrition leads to the formation of lipotoxic lipids that contribute to oxidative and endoplasmic reticulum stress, inflammasome activation and apoptotic cell death, and stimulation of inflammation, tissue regeneration, and fibrogenesis. The pathogenic pathways of NAFLD influenced by metabolic, genetic, and microbiome-related factors were also depicted. The crosstalk between the liver and other organs (particularly, adipose tissue and the gut) via FGF19 and FGF21 might also contribute to metabolic dysregulation and inflammation in NAFLD.
Figure 1.
Schematic presentation of pathogenesis of NAFLD and possible mechanisms of action of available treatment strategies. The imbalance in lipid metabolism due to overnutrition leads to the formation of lipotoxic lipids that contribute to oxidative and endoplasmic reticulum stress, inflammasome activation and apoptotic cell death, and stimulation of inflammation, tissue regeneration, and fibrogenesis. The pathogenic pathways of NAFLD influenced by metabolic, genetic, and microbiome-related factors were also depicted. The crosstalk between the liver and other organs (particularly, adipose tissue and the gut) via FGF19 and FGF21 might also contribute to metabolic dysregulation and inflammation in NAFLD.
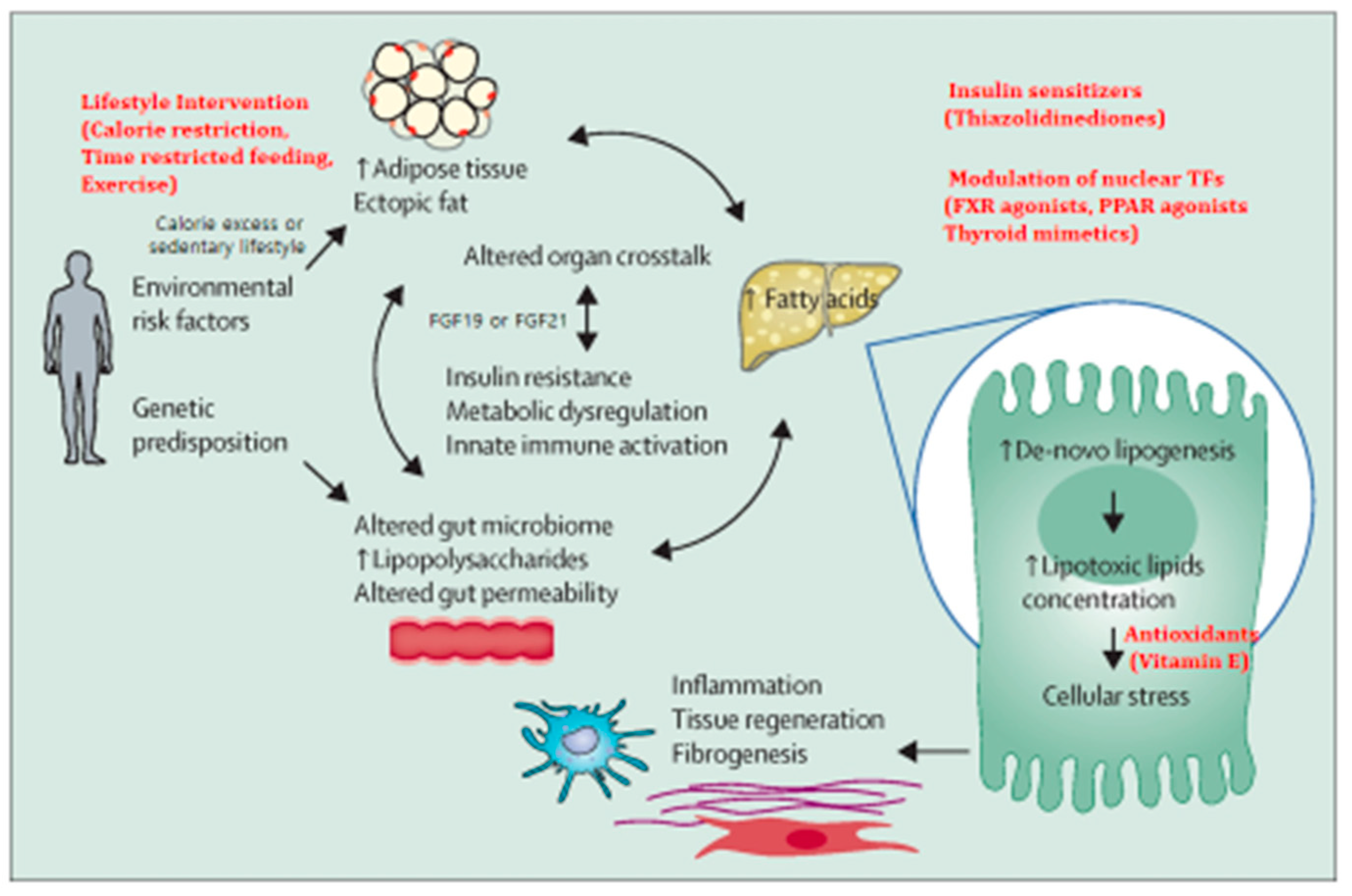
Figure 2.
Consecutive assessment of severity of NAFLD in the community. Inexpensive simple fibrosis scores (NAFLD fibrosis score or FIB-4) can be counted as a first step to identify individuals at low risk of advanced fibrosis, who can be managed in the community. Individuals with high risk scores require additional assessment with Fibro-scan, or might require referral to university hospitals (secondary care) for investigation or management of advanced fibrosis. Patients without advanced fibrosis at initial assessment might require ongoing monitoring to identify progressive liver disease and retesting 3–5 years after initial assessment.
Figure 2.
Consecutive assessment of severity of NAFLD in the community. Inexpensive simple fibrosis scores (NAFLD fibrosis score or FIB-4) can be counted as a first step to identify individuals at low risk of advanced fibrosis, who can be managed in the community. Individuals with high risk scores require additional assessment with Fibro-scan, or might require referral to university hospitals (secondary care) for investigation or management of advanced fibrosis. Patients without advanced fibrosis at initial assessment might require ongoing monitoring to identify progressive liver disease and retesting 3–5 years after initial assessment.
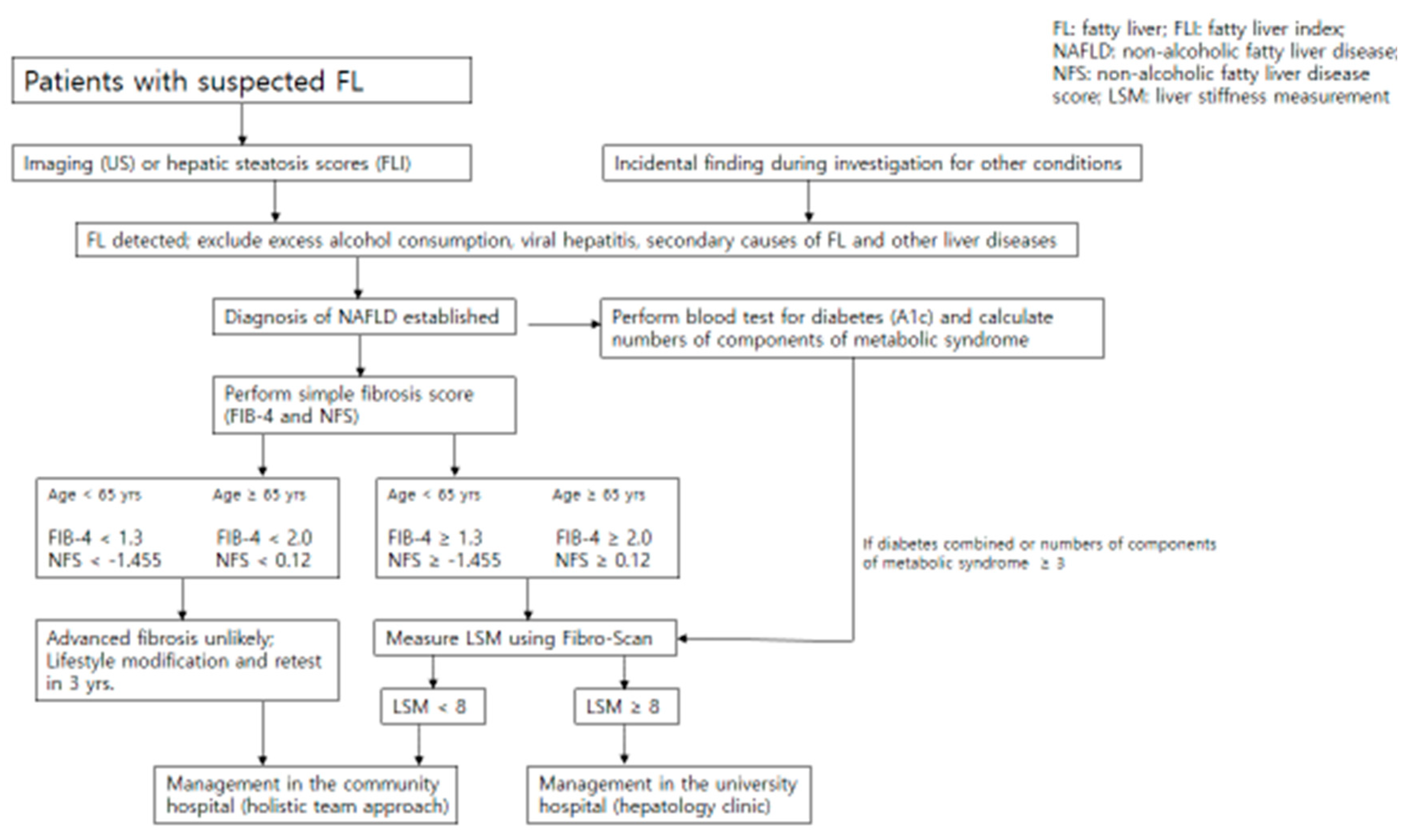

Table 1.
Comparison of landmark studies of different ways of management of NAFLD.
| Treatment modality | Specific treatment | Subjects | Effect | Quality of evidences followed | Adverse reactions | References |
|---|---|---|---|---|---|---|
| Lifestyle-induced weight loss | Weight reduction ≥ 7% | NAFLD (NASH) | Improve disease severity | Several small to moderate RCTs | None | [54] |
| Bariatric surgery | Roux-Y Gastric Bypass | NASH | Resolve NAFLD/NASH and regress fibrosis | Several small to moderate RCTs | Not completely safe due to surgery | [57] |
| Metformin | Metformin | NASH | Improve ALT, did not improve NASH histology | None, because of clear information |
Hypoglycemia, lactic acidosis | [58] |
| Thiazolidinedione | Pioglitazone | NASH (most are non-diabetics) | Improve NAFLD activity score, resolve NASH in some patients | Edema, bone loss | [59] | |
| Pioglitazone | NASH (prediabetes, or T2D) | Improve steatosis, inflammation and fibrosis progression, but did not improve fibrosis | Several small to moderate phase 2 RCTs | Edema, bone loss | [58,60] | |
| Statins | Simvastatin | NASH | Not improve steatosis, fibrosis, necroinflammation | None, because of clear information |
[58,61] | |
| Antioxidants | Vitamin E (800IU/D, 2 yrs) |
NASH | Improve NAFLD acitivity score, resolve definite NASH in some patients | Several small to moderate RCTs | Bleeding, adverse CV outcomes in higher doses | [59,62,63] |
| GLP-1 agonists | Semaglutide 0.4mg/D 72wks |
NASH | Improves hepatic steatosis, necroinflammation | Several small to moderate RCTs | Safe and effective (except nausea, anorexia, constipation) | [64,65] |
| SGLT2 inhibitors | Dapagliflozin 10mg/D 12wks |
NAFLD c T2D | Improves hepatic steatosis, necroinflammation, and liver enzymes | Several small RCTs with non-invasive tests | hypoglycemia, ketoacidosis, urinary tract and genital infections | [66] |
| FXR agonists | Obeticholic acid 25mg/D 72wks | NASH | Improve histology of NASH | Improve liver fibrosis in a phase III RCT | severe adverse reactions (pruritus, LDL increase) limit long-term use | [67] |
| PPARα agonists | Saroglitazar 4mg/D 16wks | NASH | improve dyslipidemia; reduce fat and triglyceride in the liver | Safe and effective | [68] | |
| THRβ agonist | Resmetirom 80mg/D 36wks | NASH | Reduce liver fat content | FDA approved | Safe and effective, but further studies are needed |
[69,70] |
| FGF19 analog | NGM282 1 or 3 mg/D 12wks | NASH | improve histological features and fibrosis score of NASH | Well-tolerated in a phase IIb study | Cholesterol increase, nausea, vomiting, diarrhea. | [71] |
| FGF21 analog | Pegozafermin s.c. weeky of biweekly |
NASH | improve histological features and fibrosis score of NASH | Well-tolerated in a phase Ib/IIa study | Safe and effective | [72] |
Abbreviations; NAFLD: nonalcoholic fatty liver disease; NASH: nonalcoholic steatohepatitis; RCT: randomized controlled trial; ALT: alanine aminotransferase; T2D: type 2 diabetes; CV: cardiovascular.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



