
Submitted:
10 February 2025
Posted:
11 February 2025
You are already at the latest version
Abstract
Adverse childhood experiences, such as abuse, are a risk factor for mental health and socio-emotional development in adulthood. Assessing these experiences in specific populations allows for the identification of patterns and the implementation of preventive interventions. Objective: To evaluate the psychometric properties of the abbreviated version of the Adverse Childhood Experiences Abuse Form (ACE-ASF) in Ecuadorian youth, aiming to ensure the validity, reliability, and consistency of the instrument in accurately measuring abuse dimensions in this Ecuadorian population. Methodology: An instrumental study was conducted on the psychometric properties of the 8-item ACE-ASF, applying it to a sample of 840 university students (52.1% women and 47.9% men). The evaluation focused on analyzing the factorial structure and internal consistency of the instrument in this sample. Results: The two-factor model showed satisfactory fit across all levels of invariance (configural, metric, scalar, and strict), with acceptable fit indices (CFI, TLI, GFI, RMSEA and SRMR). Internal consistency was adequate, as assessed by the Omega and Cronbach’s Alpha coefficients. Convergent and discriminant validity were confirmed using the AVE and HTMT indices, ensuring proper differentiation between the dimensions assessed. Conclusion: The ACE-ASF proved to be a valid and reliable instrument for assessing abuse experiences in Ecuadorian youth. Its two-factor structure reflects distinct yet related dimensions, providing a useful tool for identifying adverse childhood experiences in this population.
Keywords:
Psychometrics
; Child physical abuse
; Child sexual abuse
; validation
1. Introduction
Violence against children is a critical public health issue, affecting nearly one billion children annually [1,2,3]. Adverse Childhood Experiences (ACEs), including physical, emotional, and sexual abuse, as well as neglect, are linked to a range of long-term consequences that extend beyond childhood and into adulthood. These experiences significantly impact physical, mental, and reproductive health, contributing to chronic conditions such as cardiovascular disease, obesity, and diabetes [4,5,6]. Furthermore, ACEs affect cognitive and social development, resulting in poor academic performance, impaired emotional regulation, and difficulties in forming and maintaining healthy relationships during childhood [7,8]. Adolescents and young adults (over 18 years) who experienced ACEs are also more likely to face mental health challenges, including depression, anxiety, and post-traumatic stress disorder (PTSD) [9].
The neurobiological effects of ACEs are profound, disrupting brain development and affecting stress response systems, emotional regulation, and decision-making processes. These disruptions persist in adulthood, affecting emotional and cognitive functioning, which can impact various aspects of life, such as academic success, work performance, and interpersonal relationships [10]. Adolescents and young adults who have been exposed to childhood violence are also more likely to engage in high-risk behaviors such as smoking, alcohol and drug use, and risky sexual practices. These behaviors are strongly associated with the development of non-communicable diseases, cancer, and sexually transmitted infections in both adolescents and adults [11,12,13,14].
In addition to the individual health consequences, ACEs contribute to the perpetuation of cycles of violence, extending beyond childhood. Adolescents and young adults who experienced abuse during childhood are at higher risk of becoming victims or perpetrators of violence in later stages of life, continuing the intergenerational transmission of abuse [15,16,17,18]. These patterns underscore the critical need for early intervention strategies that focus not only on children but also on young adults who have experienced ACEs. Addressing these experiences in both childhood and adulthood can prevent the long-term effects of abuse, break the cycle of violence, and promote resilience and recovery in individuals. The development of culturally sensitive, evidence-based interventions that target both children and young adults is essential for mitigating the lasting impacts of ACEs and promoting healthier, more resilient individuals and communities.
1.1. Methodological Approaches to Studying Childhood Violence and Adverse Childhood Experiences
Research on childhood violence and Adverse Childhood Experiences (ACEs) has employed a range of methodological approaches aimed at understanding the prevalence, long-term impact, and diverse outcomes of abuse. Large-scale cross-sectional studies, such as the Violence Against Children Surveys (Centers for Disease Control and Prevention, 2015) and the Optimus Studies (UBS Optimus Foundation, 2015), primarily focus on assessing the incidence of childhood victimization, identifying perpetrators, and exploring a limited set of outcomes related to the immediate effects of abuse. These studies predominantly concentrate on children under 18 years of age, providing valuable data on the scope and nature of abuse in this age group [19,20].
In addition to these studies, repeated cross-sectional research, such as those conducted by the UK's National Society for the Prevention of Cruelty to Children (NSPCC), allows for the examination of trends in the prevalence of child abuse over time. By tracking these trends, researchers can identify whether rates of abuse are increasing, decreasing, or fluctuating, providing critical insights into the effectiveness of current prevention strategies and policy interventions [19,20]. This type of data is essential for recognizing shifts in societal and cultural attitudes toward child abuse and the evolving risk factors contributing to its occurrence.
Longitudinal studies, such as the LONGSCAN Consortium, are particularly valuable as they track cohorts of children over extended periods, sometimes decades, to understand the long-term evolution of abuse and its lasting effects on victims. These studies help to map how childhood violence can shape mental health outcomes, behavioral issues, and overall well-being, extending well into adolescence and even into young adulthood, often beyond the age of 18. The ability to track these individuals over time also allows for a deeper understanding of the cumulative impact of multiple ACEs on a person's life trajectory, including their adult health, socioeconomic status, and interpersonal relationships [21].
Moreover, multi-country health surveys, which incorporate child abuse assessments alongside other health-related topics, offer a global perspective on the prevalence and impact of childhood violence. These studies enable comparisons across various regions, revealing differences and similarities in how child abuse is experienced and addressed across cultures, healthcare systems, and legal frameworks [22,23,24]. Such comparative data are crucial for identifying universal patterns of abuse and understanding region-specific challenges, particularly in low- and middle-income countries where child protection services may be less developed.
Despite the valuable insights offered by these methodologies, significant challenges persist in validating and ensuring the reliability of measures used to assess child abuse, particularly in diverse cultural contexts. Different cultural perceptions of what constitutes abuse, as well as varying levels of willingness to report it, can introduce biases in data collection. For example, behaviors that are considered abusive in one culture may be viewed as acceptable or even necessary in another. This complicates the development of universally applicable definitions and instruments for assessing child abuse and ACEs, which in turn affects the accuracy of the data collected.
In addition, the methodologies used in child abuse research often face issues related to the underreporting of abuse, either due to fear of repercussions or due to a lack of awareness about what constitutes abuse. Ensuring that assessment tools are culturally sensitive, reliable, and valid across different populations is critical for producing accurate data. Furthermore, longitudinal studies that track individuals into adulthood are especially important in understanding how early experiences of violence and neglect contribute to ongoing mental health challenges, substance abuse, and patterns of re-victimization or perpetration of violence in later life.
The need for accurate and culturally sensitive tools is underscored by the growing interest in studying the psychometric properties of instruments like the Adverse Childhood Experiences Abuse Short Form (ACE-ASF) in specific populations, such as Ecuadorian youth. The ACE-ASF, designed to assess the extent of childhood abuse, requires thorough validation in local contexts to ensure its effectiveness and reliability. This process involves examining its internal consistency, construct validity, and applicability to the cultural and socio-economic environment of Ecuador, where unique challenges in child protection and reporting practices may affect the instrument’s performance. Addressing these limitations is crucial for enhancing the accuracy of childhood violence assessments and for informing the development of more effective intervention strategies. Improvements in measurement tools, better cultural adaptation of research instruments, and more inclusive data collection strategies are all necessary steps in improving the overall quality of research on childhood violence and ACEs. This will ultimately lead to more effective interventions that not only address immediate issues but also promote long-term healing and resilience among victims, as well as reduce the overall burden of abuse on society.
1.2. Adverse Childhood Experiences Questionnaire
The ACE is one of the most widely used instruments for evaluating childhood trauma and violence. It is designed to assess various domains of early-life adversities, including physical, emotional, and sexual abuse, neglect, and household dysfunction. These domains collectively capture the broad range of stressful and harmful experiences that can shape a child's psychological and physiological development, with lasting effects on health throughout the lifespan. By identifying these risk factors early, the ACE Questionnaire serves as a powerful tool for understanding the long-term consequences of childhood adversity and informs preventive and intervention strategies [25,26,27,28]. Initially developed for use in high-income countries, its application has expanded significantly in low- and middle-income countries, underscoring the universal nature of childhood trauma and the increasing recognition of its global prevalence [29]. This global expansion has prompted adaptations of the instrument to account for different socio-cultural contexts, enhancing its relevance for a diverse range of populations.
The ACE Questionnaire is grounded in a solid psychometric foundation, demonstrating a reliable three-factor structure that captures physical/emotional abuse, household dysfunction, and sexual victimization. These factors have been shown to correlate with various adverse health outcomes, including mental health disorders, substance abuse, and chronic diseases. The tool's construct validity is well-established, meaning it accurately measures what it intends to, and its internal consistency is strong, reflecting the robustness of the instrument in capturing various dimensions of early-life trauma. The reliability of the ACE Questionnaire makes it a valuable resource for both research and clinical purposes, as it consistently demonstrates its ability to predict negative health outcomes across diverse populations [30,31]. Its wide use in research has made it a cornerstone in the study of how childhood adversity impacts adult health and well-being.
Recognizing the need for a more culturally adaptable version, the World Health Organization (WHO) developed the ACE-International Questionnaire (ACE-IQ), a 43-item instrument tailored for use in diverse cultural settings, including low- and middle-income countries. The ACE-IQ was specifically designed to retain the core domains of the original ACE Questionnaire while incorporating relevant cultural nuances that might affect how childhood trauma is experienced and reported in different societies. This version has broadened the scope of ACE research, allowing for more inclusive assessments of childhood adversity across the globe [35]. The ACE-IQ has been implemented in various countries, including Kenya [36], Brazil [37], and Iraq [39], with preliminary studies supporting its usefulness in these diverse settings. However, there remains a need for further investigation into the psychometric properties of the ACE-IQ in these regions, as limited data on its reliability and validity persist. These gaps suggest the necessity of more cross-cultural research to ensure the instrument’s accuracy and to better understand its applicability in different cultural and socioeconomic contexts [41].
In addition to the full ACE and ACE-IQ versions, there is also the ACE Abuse Short Form (ACE-ASF), an abbreviated 8-item version that specifically targets abuse-related experiences. This shorter form is particularly useful for situations where time constraints or resource limitations may require a more focused assessment of abuse dimensions. The ACE-ASF is designed to be used with adolescents and adults, offering a more efficient means of gathering critical data on abuse while retaining the core elements of the original ACE Questionnaire. Though promising in its utility, the psychometric validation of the ACE-ASF across diverse populations and cultural settings remains incomplete. As a result, additional research is needed to explore its reliability, construct validity, and effectiveness in capturing the complexities of abuse experiences in different demographic groups. This is especially important in the case of Ecuadorian youth, where understanding the psychometric properties of the ACE-ASF is crucial for ensuring that the instrument accurately reflects the unique sociocultural dynamics and patterns of childhood abuse in the Ecuadorian context. Such validation will help ensure that the ACE-ASF is both a reliable and culturally sensitive tool for assessing childhood abuse in Ecuador, allowing for more effective interventions and support for youth affected by trauma [42].
In general, while the ACE and its adaptations have become indispensable tools for identifying the impact of childhood adversity, there is still much work to be done in refining and validating these instruments across a variety of cultural and socio-economic contexts. The ongoing expansion of ACE research into low- and middle-income countries and the development of tools like the ACE-IQ and ACE-ASF represent significant strides toward understanding and mitigating the long-term effects of childhood trauma. Nevertheless, continuous research and psychometric testing are necessary to further improve the global applicability, reliability, and validity of these essential instruments, ensuring that they can serve as effective tools for prevention, early intervention, and support for individuals affected by childhood violence. The psychometric properties of the ACE-ASF, particularly in the context of Ecuadorian youth, should be a focal point of future research to ensure its relevance and efficacy in identifying childhood abuse and guiding necessary interventions.
1.3. Study Objective
The primary objective of this study is to analyze the psychometric properties of the abbreviated version of the Adverse Childhood Experiences Questionnaire (ACE-ASF) in Ecuadorian youth, with a particular focus on ensuring its reliability, validity, and measurement invariance. This evaluation aims to confirm that the instrument is suitable for accurately measuring the dimensions of abuse within this specific population, ensuring that it consistently captures the intended constructs.
The first objective is to analyze the reliability of the ACE-ASF in the Ecuadorian youth population, to ensure the stability of the instrument. This analysis aims to determine whether the questionnaire maintains a high level of internal consistency when measuring adverse experiences, which is essential for its application in future research. The second objective is to analyze the structural validity of the ACE-ASF through Confirmatory Factor Analysis (CFA), with the aim of evaluating whether the dimensions of the questionnaire, such as physical-emotional abuse and sexual abuse, are grouped according to the expected theoretical structure, ensuring that the model is valid and suitable for the Ecuadorian youth population. The third objective is to evaluate the convergent and discriminant validity of the ACE-ASF, to verify that the abuse dimensions are measured accurately and distinctly, ensuring that each category of the questionnaire adequately captures the different types of adverse experiences. Finally, the fourth objective is to examine the invariance of the ACE-ASF model by sex, with the aim of ensuring that the instrument is equally applicable and valid for both men and women, avoiding gender-related biases among participants.
The hypotheses are as follows: the first hypothesis is that the ACE-ASF presents high reliability in the Ecuadorian youth population, evidenced by a significant level of internal consistency in measuring adverse experiences. The second hypothesis is that the structure of the ACE-ASF adequately fits the underlying theory, with the dimensions of physical-emotional abuse and sexual abuse grouping coherently according to the proposed theoretical model, as demonstrated by the Confirmatory Factor Analysis (CFA). The third hypothesis is that the dimensions of physical-emotional abuse and sexual abuse in the ACE-ASF show significant convergent and discriminant validity, ensuring that each category of the questionnaire accurately and distinctly measures the different types of adverse experiences. Finally, the fourth hypothesis is that the ACE-ASF model is invariant by sex, meaning the instrument is equally applicable and valid for both men and women, without gender-related biases
2. Materials and Methods
2.1. Research Design
Instrumental research was conducted in two phases, following the current standards for the validation of educational and psychological tests [43], as well as the guidelines for the adaptation and translation of existing tests [44,45,46,47]. In the first phase, linguistic adaptation of the original test was carried out [42] through an iterative translation process performed by experts [48]. In the second phase, evidence of reliability and validity of the instrument.
2.2. Participants
The sample included a total of 840 participants selected by means of a non-probabilistic convenience sample [49]. In terms of sex, the majority of participants identified themselves as women (52.1%, n = 438), while 47.9% (n = 402). In terms of ethnicity, the vast majority of participants (90.2%, n = 758) identified as mestizo. Other ethnicities were represented to a lesser extent: 6.3% of the participants (n = 53) identified themselves as Afro-Ecuadorian, 1.5% as white (n = 13), 1.2% as Montubio (n = 10) and 0.7% as Indigenous (n = 6). Regarding the age of the participants, the analysis yielded a mean of 20.61 years with a standard deviation of 2.52, and a median of 21 years, which suggests a slight concentration of ages around this value.
2.3. Measures
2.3.1. Ad-hoc sociodemographic survey
An ad hoc sociodemographic data survey was administered to collect the age, sex and ethnicity of the participants.
2.3.2. Adverse Childhood Experiences Abuse Short Form (ACE-ASF)
The form consists of 8 Likert-type items. In the exploratory factor analysis in the research of Meinck et al. [42] established a two-factor structure: physical/emotional abuse and sexual abuse. In the confirmatory factor analysis, they stated that this model fit the data well [χ²(gl) = 60.526(19); RMSEA = 0.036; CFI/TLI = 0.990/0.986]. Metric invariance between sexes was supported. Internal consistency was good (α = .83) for the sexual abuse scale and low (α = .57) for the physical/emotional abuse scale [42].
2.4. Procedure
The study was conducted following the ethical guidelines of the Helsinki Declaration. The research was approved by the Human Research Ethics Committee of the Pontificia Universidad Católica del Ecuador under Protocol No PV-14-2022. Data collection was performed through the application of face-to-face surveys, where participants completed the self-report form using pencil and paper.
After obtaining the necessary permissions from the educational institutions, the participants were invited to take part in the study. They were informed of the purpose and importance of the research, emphasizing the voluntary nature of their participation. In addition, they were informed of their right to withdraw or change their mind at any time during the process. Each participant signed an informed consent form, ensuring that they understood and accepted the terms of their participation.
The responses obtained were transcribed into the OpenClinic data management system, where they were analyzed in several aspects: (a) sociodemographic characteristics, (b) perception of conflict resolution style by dimensions, (c) conflict resolution style according to sex, and (d) confirmatory factor analysis. First, descriptive analyses were carried out for each item and for the general dimensions of childhood grandparenting. Measures of central tendency (mean and median) and dispersion (standard deviation) were calculated for each item, as well as skewness and kurtosis to evaluate the distribution of responses. These analyses revealed patterns of responses among the young people and allowed the identification of items with high skewness and kurtosis, indicating less common adverse experiences in the sample.
2.5. Statistical analysis
The analyses were performed using R version 4.4.3 [50] and JASP version 0.19.3. Regarding the first objective, to analyze the reliability of the ACE-ASF in the Ecuadorian youth population, item descriptive statistics such as mean, standard deviation, skewness, and kurtosis were calculated. Normality was assessed using the Shapiro-Wilk test [51,52,53]. Additionally, reliability estimates [54,55], such as Guttman’s Lambda 2 (λ2) and Lambda 6 (λ6), as well as the Greatest Lower Bound (GLB), were used to measure the internal consistency of the questionnaire, considering total variance, covariances between items, and residual errors. The Average Interitem Correlation (AIC) was also calculated to assess the average correlation between items. Descriptive measures, including mean, standard deviation, and 95% confidence intervals for each reliability estimate, were reported to evaluate the precision and stability of the results.
Regarding the second objective, to analyze the structural validity of the ACE-ASF through Confirmatory Factor Analysis (CFA), the factor structure of the questionnaire was examined using the Lavaan statistical package [56]. Since the data did not meet the assumption of multivariate normality [57,58], the diagonally weighted least squares estimator (DWLS) was applied [59]. Fit indices were evaluated using a comparative fit index (CFI) of .95 and a standardized root mean square residual (SRMR) of .08, which were established as the optimal model fit criteria [60,61,62]. Reliability of the factors was further assessed using Cronbach's alpha and McDonald's omega coefficients [63].
Regarding the third objective, to evaluate the convergent and discriminant validity of the ACE-ASF, two key indicators were used: the Average Variance Extracted (AVE) and the Heterotrait-Monotrait Ratio (HTMT). These indicators provide evidence of scale validity, with reference values of AVE ≥ .500 and HTMT ≤ .950 [64]. The statistical analyses included Composite Reliability (CR > 0.70) and Variance Inflation Factor (VIF < 10) [65]. Additionally, Spearman’s correlation coefficient [66] was applied to examine the relationship between the factors of physical-emotional abuse (summation of items A1–A4) and sexual abuse (summation of items A5–A8). This analysis ensured that the dimensions of the questionnaire were measured accurately and distinctly, confirming the validity of each category in capturing different types of adverse experiences.
To address the fourth objective, to examine the invariance of the ACE-ASF model by sex, configural, metric, scalar, and strict invariance models were tested [58,61,62]. This analysis ensured that the questionnaire is equally applicable and valid for both men and women, avoiding gender-related biases among participants.
Finally, a network analysis [67,68,69,70] was conducted to explore the relationships and centrality of items within the questionnaire. Measures of centrality (betweenness, closeness, strength, and expected influence) and clustering methods (Barrat, Onnela, WS, and Zhang) were employed to provide additional insights into the questionnaire’s structure and the interconnections between its components. These analyses contribute to a comprehensive understanding of the ACE-ASF’s psychometric properties, ensuring its reliability, validity, and applicability for the Ecuadorian youth population.
3. Results
Table 1 presented the descriptive data for the items and dimensions of the Adverse Childhood Experiences Abuse Short Form (ACE-ASF) in Ecuadorian youth (n = 840). Overall, the individual items showed notable variability, with medians ranging from 2 to 3 and means ranging from 2.07 (A8) to 3.283 (A1). Items A1 and A3 showed distributions closer to symmetry, with lower skewness and kurtosis values, while items A5 to A8, related to sexual abuse experiences, displayed higher levels of skewness and kurtosis, especially item A8, which had a skewness of 2.259 and a kurtosis of 8.944. In all cases, the Shapiro-Wilk test was significant (p < .001), suggesting that none of the distributions followed a normal pattern.
Regarding the grouped dimensions, dimension F1 (physical and emotional abuse, sum of A1 to A4) had a median of 10 and a mean of 11.308, with a moderately symmetric distribution (skewness = 0.542) and kurtosis close to zero (-0.258), indicating a more uniform distribution. On the other hand, dimension F2 (sexual abuse, sum of A5 to A8) had a median of 8 and a mean of 8.523, with a more asymmetric and leptokurtic distribution (skewness = 1.821 and kurtosis = 6.902), showing a concentration of values at the lower end. Both dimensions showed significance in the normality test (p < .001), confirming distribution patterns that did not follow a normal curve.
In the original model, the fit was excellent, with a χ² value of 19.587, 19 degrees of freedom, and a χ²/df ratio of 1.031 (p = 0.420), indicating that the model fit the data well. The fit indices were optimal, with CFI, TLI, and GFI values of 0.999, and an RMSEA of 0.006, with a confidence interval ranging from 0.000 to 0.031.
To assess sex invariance, the configural, metric, scalar, and strict models were tested. In each model, the fit indices remained high (CFI, TLI, and GFI = 0.999), and the RMSEA remained at 0.000, with confidence intervals between 0.000 and 0.023, reflecting stable fit across different levels of invariance. The configural invariance test yielded a χ² value of 27.058 with 38 degrees of freedom (p = 0.907), while the strict model showed a χ² value of 49.101 with 58 degrees of freedom (p = 0.791), indicating that the model is invariant with respect to sex at the configural, metric, scalar, and strict levels.
The results of reliability and validity (convergent and discriminant) for the sex invariance of the Adverse Childhood Experiences Abuse Short Form in Ecuadorian youth. Regarding reliability, consistent values of McDonald's omega (ω) and Cronbach's alpha (α) were observed for both factors and across both sexes at the configural, metric, scalar, and strict levels. In the male group, Factor 1 (Physical and Emotional Abuse) showed moderate to high reliability with ω and α values ranging slightly from 0.842 to 0.857, while Factor 2 (Sexual Abuse) maintained high reliability with ω ranging from 0.771 to 0.801. In the female group, Factor 1 had higher reliability values than in males, with ω ranging from 0.804 to 0.890, and Factor 2 exhibited high reliability with ω ranging from 0.880 to 0.907.
In terms of validity, AVE (convergent validity) and HTMT (discriminant validity) values confirmed the adequacy of the model for both factors in each group. At the configural level, Factor 1 had an AVE of 0.588 for males and 0.524 for females, while Factor 2 showed an AVE of 0.227 and 0.458, respectively. At the metric, scalar, and strict levels, these values remained stable, suggesting that both convergent and discriminant validity were satisfactory for both factors and sexes. Thus, the results indicated that the model is valid and reliable for assessing childhood adverse experiences in an invariant manner across males and females.
Table 2 provided the standardized factor loadings, as well as the reliability and validity values for the original model of the Adverse Childhood Experiences Abuse Short Form in a sample of Ecuadorian youth. In Factor 1 (Physical and Emotional Abuse), the factor loadings for indicators A1 to A4 ranged from 0.705 to 0.832, showing high internal consistency for this factor, with an omega (ω) value of 0.830 and a Cronbach's alpha (α) of 0.823. The overall reliability for this factor was also high, with a total ω of 0.872 and a total α of 0.812, indicating adequate cohesion among the items of this factor. The convergent validity (AVE) for Factor 1 was 0.553, confirming that the indicators effectively measured the construct of physical and emotional abuse.
In Factor 2 (Sexual Abuse), the factor loadings for items A5 to A8 were similarly strong, with values ranging from 0.654 to 0.858, particularly highlighting item A5 with a loading of 0.858. This factor achieved acceptable reliability, with ω of 0.861 and α of 0.867. The reliability and validity values indicated that Factor 2 remained internally consistent, with an AVE of 0.637, supporting the convergent validity of the factor. Furthermore, the HTMT index of 0.367 reflected adequate discriminant validity between the two factors. These results collectively suggested that the original model is reliable and valid for assessing childhood adverse experiences within the physical-emotional and sexual abuse factors in the studied sample.
Composite Reliability (CR) and the Variance Inflation Factor (VIF) are key indicators for assessing the quality of a measurement model. In your study, the CR values for factors F1 and F2 are 0.83 and 0.85, respectively, indicating high internal consistency of the items, exceeding the accepted threshold of 0.70. This suggests that the items within each factor reliably measure the same construct. On the other hand, the VIF values for F1 and F2 are 1.42 and 1.56, respectively, indicating low multicollinearity among the items, as they fall below the critical threshold of 10. Taken together, these results strengthen the validity and reliability of the measurement model used to evaluate adverse childhood experiences in Ecuadorian youth.
Figure 1 displayed the structural model of the Adverse Childhood Experiences Abuse Short Form, consisting of two factors: F1 (Physical and Emotional Abuse) and F2 (Sexual Abuse). Factor F1 included items A1, A2, A3, and A4, with standardized factor loadings of 0.71, 0.70, 0.83, and 0.70, respectively, with A3 showing the highest association with this factor. Factor F2 comprised items A5, A6, A7, and A8, with loadings of 0.86, 0.80, 0.82, and 0.65, where item A5 showed the highest association with the sexual abuse factor. Additionally, an HTMT index of 0.37 was observed between factors F1 and F2, indicating a moderate correlation between physical/emotional abuse and sexual abuse. The standardized estimates and the HTMT index were presented with two decimal places for greater precision.
A significant correlation of 0.299 (p < .001) was found between Factor 1 (Physical and Emotional Abuse) and Factor 2 (Sexual Abuse), indicating a positive, although moderate, relationship between both types of abuse. This correlation suggests that, in this sample, youth who reported experiences of physical and emotional abuse were also moderately likely to have experienced childhood sexual abuse.
Figure 2 presented a detailed analysis of the network structure, centrality, and clusters of the items in the Adverse Childhood Experiences Abuse Short Form (ACE-ASF) questionnaire applied to Ecuadorian youth.
In the central panel, the network of interactions between the items (A1–A8) was represented. Each node corresponded to an item from the questionnaire, while the lines connecting them (edges) indicated the magnitude and direction of their relationships. The thickness and color of the lines reflected the intensity of these connections; for example, the interactions between A6 and A7 stood out for their greater strength, represented by thicker and more intensely colored lines. This pattern suggested that these items were strongly related, possibly measuring very similar or complementary aspects within the adverse experience.
The left and right panels presented the results of the centrality metrics of the items, such as betweenness, closeness, strength, and expected influence. These metrics identified which items were most relevant within the network. For example, A7 and A6 showed high values across several centrality metrics, indicating that these items were key nodes within the network and played an important role in connecting other items. In contrast, items such as A1 and A4 showed lower values, suggesting that they played a more peripheral role in the questionnaire's structure.
Finally, the cluster analysis identified groupings of items that shared similarities in their relationships. The clusters reflected groups of items that likely assessed specific dimensions of adverse experiences. This analysis facilitated the interpretation of the questionnaire by highlighting patterns of relationships among the items, which could be useful for designing more targeted interventions or simplifying the instrument in future applications. In conclusion, the results highlighted the importance of certain items, such as A6 and A7, in the assessment of adverse experiences, as well as the internal organization of the instrument. This analysis significantly contributed to validating and optimizing the ACE-ASF in the Ecuadorian context.
Figure 3 presented the networks, centrality measures, and clustering analysis of Adverse Childhood Experiences (ACE-ASF) in Ecuadorian youth, differentiated by sex (male and female). In the lower part of the figure, four centrality measures for the items (betweenness, closeness, strength, and expected influence) and four clustering methods (Barrat, Onnela, WS, and Zhang) were analyzed, comparing the results by sex. Regarding the centrality measures, "betweenness" showed differences in how certain items acted as intermediaries in male and female networks. Closeness indicated the proximity of the nodes to the rest of the network, with variations depending on gender. Strength reflected the intensity of the connections, showing that females presented weaker relationships compared to males. Finally, expected influence measured the overall influence of each node in the network, where some items had greater influence in males.
Regarding the clustering methods, each technique (Barrat, Onnela, WS, and Zhang) identified unique patterns in how the items clustered within the male and female networks. These analyses evidenced clear differences in the structural organization of adverse experiences by sex, reflecting particular dynamics in how these experiences were processed or experienced. In summary, the figure highlighted significant differences in the characteristics and structures of adverse experience networks between males and females. These differences suggested important implications for the design of gender-specific interventions and future research in the Ecuadorian context.
The network analysis of the Adverse Childhood Experiences Short Form (ACE-ASF) among Ecuadorian youth revealed a dense structure with eight nodes and 23 edges, indicating a sparsity of 17.9% (Supplement Table 1). Centrality measures showed that A3 and A5 were key nodes, with high betweenness, closeness, and strength, while A7 had high expected influence (Supplement Table 2). Clustering analysis revealed A6’s strong presence in subgroups, whereas A2 and A4 had weaker connections (Supplement Table 3). The weight matrix highlighted notable connections like A3-A4 (0.488) and A7-A8 (0.794), alongside weaker relationships such as A5-A8 (-0.189) (Supplement Table 4). The analysis also revealed gender differences: for both men and women, the network had eight nodes and 18 edges, resulting in a sparsity of 0.357 (Supplement Table 5). Centrality measures indicated that A3 was central for both sexes, but more dominant in men. A5 and A7’s importance varied by sex (Supplement Table 6). Clustering measures differed by gender, with A4 exhibiting high clustering in men and A6 in women (Supplement Table 7). The weight matrix revealed that the strongest link in men was between A3 and A4 (0.484), while in women, it was between A7 and A8 (0.7), suggesting that the connections between adverse experiences may differ based on gender (Supplement Table 8).
The analysis of physical and emotional violence, as well as sexual violence, revealed gender differences in the reported scores. Women had a slightly higher mean score for physical and emotional violence (M = 11.500, SD = 3.427) compared to men (M = 11.100, SD = 3.625), and a more pronounced difference in sexual violence (M = 8.868, SD = 2.630) compared to men (M = 8.147, SD = 1.623). The median scores were similar for sexual violence across genders (Med = 8), while for physical and emotional violence, women scored higher (Med = 11) than men (Med = 10). The dispersion of data was lower for sexual violence among men, as indicated by its lower coefficient of variation (0.199). The Mann-Whitney U test showed that the difference in physical and emotional violence was marginally significant (U = 81,225.000, p = 0.051), whereas the difference in sexual violence was highly significant (U = 74,258.500, p < .001), with women scoring higher. The effect size, represented by the rank-biserial correlation, was small for physical and emotional violence (r = 0.077, SE = 0.040) but larger for sexual violence (r = 0.157, SE = 0.040), suggesting that gender differences were more pronounced in the latter dimension.
4. Discussion
The main objective of the research was to analyze the psychometric properties of the abbreviated version of the Adverse Childhood Experiences Questionnaire (ACE-ASF) in Ecuadorian youth, with a particular focus on ensuring its reliability, validity, and measurement invariance.
4.1. Reliability
The findings confirm that the ACE-ASF exhibits a high level of internal consistency in the Ecuadorian youth population, supporting its reliability as a tool for measuring adverse experiences. The Cronbach's alpha coefficients (α = 0.823 for Factor 1: Physical and Emotional Abuse; α = 0.867 for Factor 2: Sexual Abuse) reflect a strong association between the items and the constructs being evaluated. These results align with previous studies, such as those by Chegeni et al. [71] in Iran and Meinck et al. [42] in Romania, which also identified a bifactorial structure in the ACE-ASF. However, it is worth noting that the Romanian study reported lower reliability for the first factor (α = 0.57).
Additionally, the inclusion of Composite Reliability (CR) in this research represents a significant advancement in the psychometric evaluation of the ACE-ASF, allowing for the measurement of the internal consistency of the model from a more comprehensive perspective. Unlike other traditional indicators, such as Cronbach's alpha [63], CR takes into account the factor loadings of the items, providing a more accurate estimate of the reliability of the construct. The results obtained in this study show CR values greater than 0.70, confirming that the scale demonstrates high internal coherence [55]. This finding not only validates the applicability of the ACE-ASF in the Ecuadorian context but also establishes a solid foundation for its use in future studies on adverse childhood experiences.
4.2. Validity
The results of the present study confirm the validity of the original two-factor structure of the Adverse Childhood Experiences Abuse Short Form (ACE-ASF) proposed by Meinck et al. [42] in a sample of Ecuadorian youth. The original model demonstrated excellent fit, evidenced by a non-significant chi-square (Χ² = 19.587, p = 0.420), a high comparative fit index (CFI = .999), a low root mean square error of approximation (RMSEA = 0.006, CI: 0.000–0.031), and a standardized root mean square residual (SRMR = 0.041). These results are consistent with previous research supporting the robustness of this factorial structure in diverse cultural contexts. The findings reinforce the applicability of the ACE-ASF for assessing childhood abuse experiences in Ecuadorian youth and provide a reliable foundation for its use in future research focused on this population.
The ACE-ASF demonstrated adequate convergent and discriminant validity, evidenced by the clear and precise differentiation between the dimensions of physical-emotional abuse and sexual abuse. The standardized factor loadings ranged from 0.707 to 0.832 for Factor 1 and from 0.654 to 0.858 for Factor 2, confirming the instrument's capacity to measure specific constructs. These results are consistent with international research that has employed similar tools, such as the ACE-IQ, to assess adverse experiences in diverse cultural contexts [36-39, 72]. Studies like that of Xu et al. [73] also emphasize the importance of refined scoring methodologies, which could benefit both the ACE-ASF and the ACE-IQ, particularly in epidemiological and clinical research.
Additionally, the analysis of the Variance Inflation Factor (VIF) was incorporated to assess multicollinearity between the items of the scale, ensuring that there is no excessive redundancy that could affect the interpretation of the results [65]. The VIF values obtained in this research were below the critical threshold of 10, indicating acceptable levels of independence between the items and strengthening the validity of the model. This indicator is crucial in the validation of the ACE-ASF, as it ensures that the observed relationships between the variables are genuine and not the result of artificially inflated correlations. Thus, a more solid and reliable structure is ensured, establishing a methodological standard for future psychometric research.
4.3. Measurement Invariance
The tests for invariance by sex also support the robustness and generalizability of the ACE-ASF. The results showed that the configural, metric, scalar, and strict models maintained excellent fit indices, with CFI values consistently at .999, RMSEA values at 0.000, and SRMR below 0.06. This invariance confirms that the ACE-ASF measures the underlying constructs equivalently for both men and women, ensuring that comparisons between sexes are meaningful and free from bias. These findings not only validate the use of the ACE-ASF in Ecuador but also set a precedent for its application in sex-based analyses in similar sociocultural contexts, thereby expanding its relevance and utility in the study of adverse childhood experiences globally.
The ACE-ASF model was found to be invariant by gender, ensuring that measurements are equivalent for both males and females. This finding is crucial for the instrument's applicability across diverse subgroups within the Ecuadorian population, particularly in research and clinical contexts. While international studies like that of Meinck et al. [42] did not explicitly report gender invariance analyses, research such as that by Casas-Muñoz et al. [74] in Mexico underscores the relevance of such analyses for identifying differential patterns in exposure to adverse experiences.
4.4. Comparisons with the ACE-IQ
In contrast to the ACE-ASF's specific focus on abuse dimensions, the ACE-IQ offers a broader perspective by considering a variety of childhood adversities. Studies conducted in countries such as Kenya, Brazil, Saudi Arabia, and Iraq [36,37,38,39] have demonstrated its utility, though they also highlight limitations in its psychometric validation, particularly in low-income settings [72]. The results from Ecuador with the ACE-ASF are comparable to those of these studies, particularly in identifying correlations between adverse experiences and mental health, such as depression and PTSD [36,37,38,39]. For example, the ACE-ASF in Ecuador revealed moderate correlations between abuse dimensions (r = 0.299, p < 0.001).
In contrast, the ACE-IQ, with its broader scope, provides insights into a wider range of adverse experiences, but its psychometric properties in specific cultural or low-income contexts may limit the robustness of its findings compared to the ACE-ASF [73]. The ACE-ASF, while narrower in focus, offers more specific and validated insights into the relationship between abuse and mental health in the Ecuadorian youth population. This highlights the importance of selecting the appropriate tool depending on the research context and the specific dimensions of adversity being studied.
5. Conclusions
The Ecuadorian experience with the ACE-ASF underscores the need for cultural adaptations to maximize the validity and reliability of these tools. Specifically, cultural biases and stigmatization associated with the sexual abuse dimension (F2) presented significant challenges in data collection. This finding aligns with studies such as that of Chen et al. [75], which highlighted the influence of scoring methodologies and cultural barriers on the interpretation of results. Both the ACE-ASF and the ACE-IQ are valuable tools for assessing adverse experiences in diverse cultural contexts. In Ecuador, the ACE-ASF demonstrated its utility by providing reliable and culturally sensitive measurements of physical-emotional and sexual abuse. At the same time, international studies on the ACE-IQ highlight its capacity to assess a broader spectrum of childhood adversities. Integrating both perspectives can enrich our understanding of adverse experiences and their impact on mental health, facilitating the design of targeted and culturally adapted interventions.
The Adverse Childhood Experiences Abuse Short Form (ACE-ASF) is a suitable and reliable tool for assessing childhood adversities in Ecuadorian youth. The identified factorial structure, consisting of two dimensions (Physical and Emotional Abuse and Sexual Abuse), aligns with previous findings in international contexts, such as those reported in Iran and Romania. Reliability analyses showed satisfactory values, and sex invariance confirmed the model’s applicability for both males and females, allowing for equitable comparisons between genders. However, the high skewness and kurtosis observed in the items related to sexual abuse highlight the influence of cultural and social factors that may limit the reporting of such experiences, emphasizing the importance of considering the context when interpreting the results.
This study presents certain limitations that should be taken into account when interpreting the findings. First, the sample used was specific and non-probabilistic, which limits the generalization of the results to other regions or populations in the country. Additionally, the use of self-report questionnaires may be subject to biases such as selective recall or social desirability, especially regarding sensitive topics like sexual abuse, which could affect the accuracy of the collected data. Furthermore, the cross-sectional design of the study prevents the establishment of causal relationships between adverse experiences and their potential impacts on psychological well-being. Additionally, sociodemographic variables such as socioeconomic status or ethnicity were not included, which could influence responses and enrich the analysis.
Future research should address these limitations by expanding the sample to include different regions of Ecuador and diverse population groups, such as children, adolescents, and older adults. Additionally, it would be valuable to explore how cultural and social factors influence the perception and reporting of adverse experiences, particularly those related to sexual abuse, to adapt the instrument in a way that is more sensitive to local contexts. Longitudinal studies would allow for a deeper understanding of the trajectories of adverse experiences and their long-term effects on mental health, interpersonal relationships, and psychological development.
It would also be pertinent to include variables such as resilience, social support, and mental health to analyze how these dimensions moderate or mediate the effects of adverse experiences. Comparing the results obtained in Ecuador with those from other Latin American countries could help identify cultural similarities and differences, strengthening the cross-cultural validity of the ACE-ASF. Finally, based on these findings, it would be important to design prevention and intervention programs aimed at mitigating the negative effects of adverse childhood experiences, promoting the psychological and social well-being of affected individuals. This comprehensive approach would contribute not only to the development of more robust instruments but also to the implementation of more effective policies and practices in the field of mental health.
For future research, we recommend conducting a Systematic Review and Meta-analysis on the reliability and validation of the psychometric properties of the Adverse Childhood Experiences Abuse Short Form (ACE-ASF) in university populations [76]. Such a study would provide a comprehensive evaluation of the instrument's reliability across various studies and contexts, shedding light on its consistency and applicability in higher education settings. Additionally, investigating the prevalence of adverse childhood experiences [77] could provide valuable insights into how these experiences manifest across different populations and cultural contexts, contributing to a deeper understanding of their impact on human development.
Furthermore, a promising direction for future research would be to explore factorial invariance [78,79,80] within the ACE-ASF. This type of analysis is essential for determining whether the measurement model remains stable across diverse groups, such as gender, age, or cultural contexts. Establishing invariance ensures that the instrument measures adverse childhood experiences equivalently across different subgroups, thus enhancing the generalizability of the findings.
Author Contributions
Contribution to the conception and design: A.R.; Contribution to data collection: A.R., L.B.-B., H.S., J.H.D. and F.J.R.-D.; Contribution to data analysis and interpretation: A.R., J.V.Q.-C., and L.B.-B.; Drafting and/or revising the article: A.R., L.B.-B., F.J.R.-D. and J.V.Q.-C.; Approval of the final version for publication: A.R., L.B.-B., J.H.D. and F.J.R.-D.; Obtaining authorization for the scale: J.H.D. All authors have read and agreed to the published version of the manuscript.
Funding
This research was financed by the Universidad Politécnica Salesiana Sede Cuenca, Ecuador.
Institutional Review Board Statement
All procedures conducted in this study involving human participants adhered to the ethical standards established by the ethics committee. This study was approved by the Human Research Ethics Committee of the Pontifical Catholic University of Ecuador (code 046-UIO-2022). This research is derived from the research project entitled “Prevalence and risk factors of dating violence among Ecuadorian adolescents and university students and evaluation of the effectiveness of psychological intervention with virtual reality in reducing anxiety, depression and post-traumatic stress derived from violence”, under the direction of Dr. Andres Ramirez, with the support of the Research Group in Psychology (GIPSI-SIB) of the Salesian Polytechnic University (Universidad Politécnica Salesiana), Cuenca, Ecuador.
Informed Consent Statement
Informed consent was obtained from all subjects involved in this study.
Data Availability Statement
The data supporting this research are publicly available and can be obtained by emailing the first author of this article.
Acknowledgments
The authors would like to thank the Universidad Politécnica Salesiana, Ecuador, and especially to Juan Cárdenas Tapia.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| ACE | Adverse Childhood Experiences Questionnaire |
| ACE-ASF | Adverse Childhood Experiences Abuse Short Form |
| AVE | Average Variance Extracted |
| HTMT | Heterotrait-Monotrait Ratio |
| CR | Composite Reliability |
| VIF | Variance Inflation Factor |
| CFI | Comparative ft index |
| TLI: | Tucker-Lewis Index |
| GFI | Goodness of Fit Index |
| RMSEA | Root Mean Square Error of Approximation |
| SRMR | Standardized Root Mean Square Residual |
Appendix A
Appendix A.1
The reliability analysis of the Adverse Childhood Experiences Abuse Short Form (ACE-ASF) applied to Ecuadorian youth (n = 840) showed robust results (Table A1). For the total scale (items A1-A8), the Lambda 2 coefficient (λ2) had an estimated value of 0.835, while Lambda 6 (λ6) reached 0.867, and the Greatest Lower Bound (GLB) was 0.906. These indicators suggested high internal consistency for the complete scale. The average inter-item correlation (AIC) was reported as 0.376, with a total mean score of 19.831 (SD = 4.741). Additionally, the 95% confidence intervals indicated stable estimates, with lower bounds of 0.813, 0.844, and 0.890, respectively, and upper bounds of 0.854, 0.887, and 0.921. When analyzing specific dimensions, the first dimension (F1, physical and emotional abuse, items A1-A4) obtained an estimated λ2 of 0.826, a λ6 of 0.788, and a GLB of 0.860, with an AIC of 0.540. The average scores for this dimension were 11.308 (SD = 3.527), indicating high internal consistency. The 95% confidence intervals were also narrow, ranging from 0.803 to 0.845 for λ2, 0.763 to 0.811 for λ6, and 0.837 to 0.880 for GLB. In the second dimension (F2, sexual abuse, items A5-A8), the reliability estimates were even higher. The λ2 had an estimated value of 0.869, λ6 reached 0.853, and GLB was 0.914, with an AIC of 0.633. The average scores for this dimension were 8.523 (SD = 2.234). The confidence intervals for λ2 ranged from 0.834 to 0.898, for λ6 from 0.814 to 0.888, and for GLB from 0.885 to 0.937, demonstrating the stability of these measures. In conclusion, the results supported the reliability of the ACE-ASF instrument for assessing adverse childhood experiences in the Ecuadorian population, both for the total scale and its specific dimensions.

Table A1.
Reliability Statistics of the Adverse Childhood Experiences Abuse Short Form (ACE-ASF) in Ecuadorian Youth (n = 840).
Table A1.
Reliability Statistics of the Adverse Childhood Experiences Abuse Short Form (ACE-ASF) in Ecuadorian Youth (n = 840).
| Estimate | λ2 | λ6 | GLB | AIC | Mean | SD | |
| Total | Point estimate | 0.835 | 0.867 | 0.906 | 0.376 | 19.831 | 4.741 |
| (A1 - A8) | 95% CI lower bound | 0.813 | 0.844 | 0.890 | 0.332 | 19.510 | 4.524 |
| 95% CI upper bound | 0.854 | 0.887 | 0.921 | 0.416 | 20.152 | 4.979 | |
| F1 | Point estimate | 0.826 | 0.788 | 0.860 | 0.540 | 11.308 | 3.527 |
| (A1 - A4) | 95% CI lower bound | 0.803 | 0.763 | 0.837 | 0.501 | 11.070 | 3.366 |
| 95% CI upper bound | 0.845 | 0.811 | 0.880 | 0.573 | 11.547 | 3.704 | |
| F1 | Point estimate | 0.869 | 0.853 | 0.914 | 0.633 | 8.523 | 2.234 |
| (A5 - A8) | 95% CI lower bound | 0.834 | 0.814 | 0.885 | 0.565 | 8.372 | 2.132 |
| 95% CI upper bound | 0.898 | 0.888 | 0.937 | 0.697 | 8.674 | 2.346 |
Note.F1 = Physical and Emotional Abuse, F2 = Sexual Abuse, λ2 = Guttman's λ2, λ6 = Guttman's λ6, GLB = Greatest Lower Bound, AIC = Average interitem correlation. .
Appendix A.2
The results of the factor analysis indicated that both the Kaiser-Meyer-Olkin (KMO) index and Bartlett's test of sphericity were satisfactory in all cases, suggesting the adequacy of the data for conducting a factor analysis (Table A2). Regarding the KMO index, the observed values for each item (A1 to A8) were above 0.7, indicating a good sample adequacy. In the general analysis, the KMO was 0.808, reflecting an appropriate suitability for the analysis. Specifically, the KMO values for men and women were very similar, with men achieving a value of 0.792 and women 0.810, further supporting the robustness of the analysis for both genders.
The R², which measures the variance explained by each item, ranged from 0.317 to 0.797, with items A5, A6, and A7 showing the highest explained variance. Bartlett's test of sphericity, which tests the null hypothesis that the correlation matrix is an identity matrix, was significant for all three groups (General, Men, and Women), with p-values < 0.001. This suggests that the correlations between items were strong enough to justify the use of a factor analysis. In conclusion, the results showed that the data were appropriate for conducting a factor analysis, with KMO indices and Bartlett's test of sphericity supporting the validity of the analyses for both the general group and the subgroups of men and women.
Table A2.
Kaiser-Meyer-Olkin and Bartlett's Test Results for Factor Analysis by Group.
| General | Man | Woman | ||||
| KMO | R² | KMO | R² | KMO | R² | |
| A1 | 0.818 | 0.499 | 0.816 | 0.513 | 0.813 | 0.483 |
| A2 | 0.865 | 0.496 | 0.841 | 0.504 | 0.872 | 0.474 |
| A3 | 0.771 | 0.692 | 0.773 | 0.709 | 0.775 | 0.684 |
| A4 | 0.830 | 0.497 | 0.821 | 0.515 | 0.845 | 0.484 |
| A5 | 0.815 | 0.736 | 0.802 | 0.537 | 0.811 | 0.782 |
| A6 | 0.834 | 0.648 | 0.795 | 0.453 | 0.833 | 0.719 |
| A7 | 0.788 | 0.666 | 0.751 | 0.559 | 0.798 | 0.797 |
| A8 | 0.768 | 0.427 | 0.736 | 0.317 | 0.771 | 0.590 |
| Overall | 0.808 | 0.792 | 0.810 | |||
| Bartlett's test of sphericity | ||||||
| Χ² | 3.099.719 | 1.242.090 | 1.729.997 | |||
| df | 28 | 28 | 28 | |||
| p | < .001 | < .001 | < .001 | |||
Note.KMO = Kaiser-Meyer-Olkin test, R² = R-Squared.
References
- Ferrara, P.; Cammisa, I.; Zona, M.; Corsello, G.; Giardino, I.; Vural, M.; Pettoello-Mantovani, M. The global issue of violence toward children in the context of war. J. Pediatr. 2024, 269. [Google Scholar] [CrossRef]
- Hillis, S.; Mercy, J.; Amobi, A.; Kress, H. Global prevalence of past-year violence against children: A systematic review and minimum estimates. Pediatrics 2016, 137. [Google Scholar] [CrossRef]
- Thomas, S.P. Preventing violence against children and youth. Issues Ment. Health Nurs. 2024, 45, 363–364. [Google Scholar] [CrossRef] [PubMed]
- Ali, S.; Pasha, S.A.; Cox, A.; Youssef, E. Examining the short and long-term impacts of child sexual abuse: a review study. SN Soc. Sci. 2024, 4, 56. [Google Scholar] [CrossRef]
- Güler, A.; Maas, M.K.; Mark, K.P.; Kussainov, N.; Schill, K.; Coker, A.L. The impacts of lifetime violence on women's current sexual health. Women's Health Rep. 2024, 5, 56–64. [Google Scholar] [CrossRef]
- Swift, A.; Berry, M.; Fernandez-Pineda, M.; Haberstroh, A. An Integrative Review of Adverse Childhood Experiences and Reproductive Traumas of Infertility and Pregnancy Loss. J. Midwifery Women's Health 2024, 69, 258–278. [Google Scholar] [CrossRef] [PubMed]
- Bhutta, Z.A.; Bhavnani, S.; Betancourt, T.S.; Tomlinson, M.; Patel, V. Adverse childhood experiences and lifelong health. Nat. Med. 2023, 29, 1639–1648. [Google Scholar] [CrossRef]
- Qu, G.; Shu, L.; Liu, H.; Ma, S.; Han, T.; Zhang, H.; Huang, C.; Wang, J.; Yang, L.; Sun, Y. Association Between Adverse Childhood Experiences and Academic Performance Among Children and Adolescents: A Global Meta-Analysis. Trauma Violence Abuse. 2024, 25, 3332–3345. [Google Scholar] [CrossRef]
- Horino, M.; Abu-Rmeileh, N.M.E.; Yang, W.; Albaik, S.; Al-Khatib, L.; Seita, A. Exploring the link between adverse childhood experiences and mental and physical health conditions in pregnant Palestine refugee women in Jordan. Public Health 2023, 220, 179–186. [Google Scholar] [CrossRef]
- Jewkes, R.; Dunkle, K.; Nduna, M.; Jama, P.N.; Puren, A. Associations between childhood adversity and depression: Substance abuse and HIV and HSV2 incident infections in rural South African youth. Child Abuse Negl. 2010, 34, 833–841. [Google Scholar] [CrossRef]
- Meinck, F.; Woollett, N.; Franchino-Olsen, H.; Silima, M.; Thurston, C.; Fouché, A.; Christofides, N. Interrupting the intergenerational cycle of violence: protocol for a three-generational longitudinal mixed-methods study in South Africa (INTERRUPT_VIOLENCE). BMC Public Health 2023, 23, 395. [Google Scholar] [CrossRef]
- Miller, G.E.; Chen, E.; Parker, K.J. Psychological stress in childhood and susceptibility to the chronic diseases of aging: Moving toward a model of behavioral and biological mechanisms. Psychol. Bull. 2011, 137, 959–997. [Google Scholar] [CrossRef] [PubMed]
- Ramiro, L.S.; Madrid, B.J.; Brown, D.W. Adverse childhood experiences (ACE) and health-risk behaviors among adults in a developing country setting. Child Abuse Negl. 2010, 34, 842–855. [Google Scholar] [CrossRef] [PubMed]
- Sansone, A.; Limoncin, E.; Colonnello, E.; Mollaioli, D.; Ciocca, G.; Corona, G.; Jannini, E.A. Harm reduction in sexual medicine: How to manage patients with sexual dysfunction caused by substance use. Sexual Med. Rev. 2024, 12, 422–429. [Google Scholar]
- Butler, N.; Quigg, Z.; Bellis, M.A. Cycles of violence in England and Wales: the contribution of childhood abuse to risk of violence revictimisation in adulthood. BMC Med. 2020, 18, 1–13. [Google Scholar] [CrossRef]
- Herrenkohl, T.I.; Fedina, L.; Roberto, K.A.; Raquet, K.L.; Hu, R.X.; Rousson, A.N.; Mason, W.A. Child Maltreatment, Youth Violence, Intimate Partner Violence, and Elder Mistreatment: A Review and Theoretical Analysis of Research on Violence Across the Life Course. Trauma Violence Abus. 2022, 23, 314–328. [Google Scholar] [CrossRef]
- Marshall, C.; Langevin, R.; Cabecinha-Alati, S. Victim-to-victim intergenerational cycles of child maltreatment: A systematic scoping review of theoretical frameworks. Int. J. Child Adolesc. Resil. 2022, 9, 95–115. [Google Scholar] [CrossRef]
- Shields, M.; Tonmyr, L.; Hovdestad, W.E.; Gonzalez, A.; MacMillan, H. Exposure to family violence from childhood to adulthood. BMC Public Health 2020, 20, 1–15. [Google Scholar] [CrossRef]
- May-Chahal, C.; Cawson, P. Measuring Child Maltreatment in the United Kingdom: A Study of the Prevalence of Child Abuse and Neglect. Child Abuse & Neglect 2005, 29, 969–984. [Google Scholar] [CrossRef]
- May-Chahal, C.; Bertotti, T.; Di Blasio, P.A.C.M.; Cerezo, M.A.; Gerard, M.; Grevot, A.; Al-Hamad, A. Child Maltreatment in the Family: A European Perspective. European Journal of Social Work 2006, 9, 3–20. [Google Scholar] [CrossRef]
- Fry, D.; McCoy, A.; Swales, D. The Consequences of Maltreatment on Children’s Lives: A Systematic Review of Data From the East Asia and Pacific Region. Trauma, Violence, & Abuse 2012, 13, 209–233. [Google Scholar] [CrossRef]
- Meinck, F.; Steinert, J.; Sethi, D.; Gilbert, R.; Bellis, M.; Alink, L.; Baban, A. Measuring and Monitoring National Prevalence of Child Maltreatment: A Practical Handbook; World Health Organization: Geneva, Switzerland, 2016; Available online: https://ora.ox.ac.uk/objects/uuid:d119ecfc-cd5e-45bc-8cde-13fabdfa982a/files/m580e1cc881179236acc5ba604fd6def9.
- Steele, B.; Neelakantan, L.; Jochim, J.; Davies, L.M.; Boyes, M.; Franchino-Olsen, H.; Dunne, M.; Meinck, F. Measuring Violence Against Children: A COSMIN Systematic Review of the Psychometric and Administrative Properties of Adult Retrospective Self-report Instruments on Child Abuse and Neglect. Trauma, Violence, & Abuse 2024, 25, 183–196. [Google Scholar] [CrossRef]
- Meinck, F.; Murray, A.L.; Dunne, M.P.; Schmidt, P.; Nikolaidis, G.; Petroulaki, K.; Browne, K. Measuring Violence Against Children: The Adequacy of the International Society for the Prevention of Child Abuse and Neglect (ISPCAN) Child Abuse Screening Tool-Child Version in 9 Balkan Countries. Child Abuse & Neglect 2020, 108, 104636. [Google Scholar] [CrossRef]
- Felitti, V.J.; Anda, R.F.; Nordenberg, D.; Williamson, D.F.; et al. Adverse Childhood Experiences and Health Outcomes in Adults: The ACE Study. Journal of Family and Consumer Sciences 1998, 90, 31. Available online: https://www.proquest.com/scholarly-journals/adverse-childhood-experiences-health-outcomes/docview/218184173/se-2.
- Hulme, P.A. Psychometric Evaluation and Comparison of Three Retrospective, Multi-Item Measures of Childhood Sexual Abuse. Child Abuse & Neglect 2007, 31, 853–869. [Google Scholar] [CrossRef]
- Liebschutz, J.M.; Buchanan-Howland, K.; Chen, C.A.; Frank, D.A.; Richardson, M.A.; Heeren, T.C.; Cabral, H.J.; Rose-Jacobs, R. Childhood Trauma Questionnaire (CTQ) Correlations with Prospective Violence Assessment in a Longitudinal Cohort. Psychological Assessment 2018, 30, 841–845. [Google Scholar] [CrossRef]
- Midei, A.J.; Matthews, K.A.; Chang, Y.-F.; Bromberger, J.T. Childhood Physical Abuse Is Associated with Incident Metabolic Syndrome in Mid-Life Women. Health Psychology 2013, 32, 121–127. [Google Scholar] [CrossRef]
- Mikton, C.; Power, M.; Raleva, M.; Makoae, M.; Al Eissa, M.; Cheah, I.; et al. The Assessment of the Readiness of Five Countries to Implement Child Maltreatment Prevention Programs on a Large Scale. Child Abuse & Neglect 2013, 37, 1237–1251. [Google Scholar] [CrossRef]
- Ford, D.C.; Merrick, M.T.; Parks, S.E.; Breiding, M.J.; Gilbert, L.K.; Edwards, V.J.; Dhingra, S.S.; Barile, J.P.; Thompson, W.W. Examination of the Factorial Structure of Adverse Childhood Experiences and Recommendations for Three Subscale Scores. Psychology of Violence 2014, 4, 432–444. [Google Scholar] [CrossRef]
- Ford, K.; Bellis, M.A.; Hughes, K.; Barton, E.R.; Newbury, A. Adverse Childhood Experiences: A Retrospective Study to Understand Their Associations with Lifetime Mental Health Diagnosis, Self-Harm or Suicide Attempt, and Current Low Mental Wellbeing in a Male Welsh Prison Population. Health & Justice 2020, 8, 13. [Google Scholar] [CrossRef]
- Holden, G.W.; Gower, T.; Chmielewski, M. Methodological Considerations in ACEs Research. In Adverse Childhood Experiences; Academic Press: San Diego, CA, USA, 2020. [Google Scholar] [CrossRef]
- Wingenfeld, K.; Schäfer, I.; Terfehr, K.; Grabski, H.; Driessen, M.; Grabe, H.; Löwe, B.; Spitzer, C. The Reliable, Valid and Economic Assessment of Early Traumatization: First Psychometric Characteristics of the German Version of the Adverse Childhood Experiences Questionnaire (ACE). Psychotherapie, Psychosomatik, Medizinische Psychologie 2011, 61, e10–e14. [Google Scholar] [CrossRef] [PubMed]
- Kovács-Tóth, B.; Oláh, B.; Kuritárné Szabó, I.; Fekete, Z. Psychometric Properties of the Adverse Childhood Experiences Questionnaire 10 Item Version (ACE-10) Among Hungarian Adolescents. Frontiers in Psychology 2023, 14, 1161620. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Adverse Childhood Experiences International Questionnaire. In Adverse Childhood Experiences International Questionnaire (ACE-IQ); World Health Organization: Geneva, Switzerland, 2018; Available online: https://www.who.int/violence_injury_prevention/violence/activities/adverse_childhood_experiences/en/.
- Goodman, M.L.; Raimer-Goodman, L.; Chen, C.X.; Grouls, A.; Gitari, S.; Keiser, P.H. Testing and Testing Positive: Childhood Adversities and Later Life HIV Status Among Kenyan Women and Their Partners. Journal of Public Health 2017, 39, 720–729. [Google Scholar] [CrossRef] [PubMed]
- Soares, A.L.G.; Howe, L.D.; Matijasevich, A.; Wehrmeister, F.C.; Menezes, A.M.; Gonçalves, H. Adverse Childhood Experiences: Prevalence and Related Factors in Adolescents of a Brazilian Birth Cohort. Child Abuse & Neglect 2016, 51, 21–30. [Google Scholar] [CrossRef]
- Almuneef, M.; Qayad, M.; Aleissa, M.; Albuhairan, F. Adverse Childhood Experiences, Chronic Diseases, and Risky Health Behaviors in Saudi Arabian Adults: A Pilot Study. Child Abuse & Neglect 2014, 38, 1787–1793. [Google Scholar] [CrossRef]
- Al-Shawi, A.F.; Lafta, R.K. Effect of Adverse Childhood Experiences on Physical Health in Adulthood: Results of a Study Conducted in Baghdad City. Journal of Family and Community Medicine 2015, 22, 78–84. [Google Scholar] [CrossRef]
- Tran, Q.A.; Dunne, M.P.; Vo, T.V.; Luu, N.H. Adverse Childhood Experiences and the Health of University Students in Eight Provinces of Vietnam. Asia Pacific Journal of Public Health 2015, 27, 26S–32S. [Google Scholar] [CrossRef]
- Pace, C.S.; Muzi, S.; Rogier, G.; Meinero, L.L.; Marcenaro, S. The Adverse Childhood Experiences–International Questionnaire (ACE-IQ) in Community Samples Around the World: A Systematic Review (Part I). Child Abuse & Neglect 2022, 129, 105640. [Google Scholar] [CrossRef]
- Meinck, F.; Cosma, A.P.; Mikton, C.; Baban, A. Psychometric Properties of the Adverse Childhood Experiences Abuse Short Form (ACE-ASF) Among Romanian High School Students. Child Abuse & Neglect 2017, 72, 326–337. [Google Scholar] [CrossRef]
- Arias, A.; Sireci, S. Validez y Validación para Pruebas Educativas y Psicológicas: Teoría y Recomendaciones. Rev. Iberoam. Psicol. 2021, 14, 11–22. [Google Scholar] [CrossRef]
- Muñiz, J.; Elosua, P.; Hambleton, R.K. Directrices para la traducción y adaptación de los tests: Segunda edición. Psicothema 2013, 25, 151–157. [Google Scholar] [CrossRef]
- Cruchinho, P.; López-Franco, M.D.; Capelas, M.L.; Almeida, S.; Bennett, P.M.; Miranda da Silva, M.; Gaspar, F. Translation, Cross-Cultural Adaptation, and Validation of Measurement Instruments: A Practical Guideline for Novice Researchers. J. Multidiscip. Healthc. 2024, 17, 2701–2728. [Google Scholar] [CrossRef]
- Moore, G.; Campbell, M.; Copeland, L.; Craig, P.; Movsisyan, A.; Hoddinott, P.; Evans, R. Adapting Interventions to New Contexts—The ADAPT Guidance. BMJ 2021, 374, n1679. [Google Scholar] [CrossRef]
- Brauer, K.; Ranger, J.; Ziegler, M. Confirmatory Factor Analyses in Psychological Test Adaptation and Development: A Nontechnical Discussion of the WLSMV Estimator. Psychol. Test Adapt. Dev. 2023, 4, 4–12. [Google Scholar] [CrossRef]
- Elosua, P.; Mujika, J.; Almeida, L.S.; Hermosilla, D. Judgmental-Analytical Procedures for Adapting Tests: Adaptation to Spanish of the Reasoning Tests Battery. Rev. Latinoam. Psicol. 2014, 46, 117–126. [Google Scholar] [CrossRef]
- Teodoro Dantas Sartori, J. Determining the Confidence Interval for Non-Probabilistic Surveys: Method Proposal and Validation. Commun. Stat.-Theory Methods 2024, 1–9. [Google Scholar] [CrossRef]
- R Core Team. R: A language and environment for statistical computing. (Version 4.1) [Computer software]. 2022. Retrieved from (R packages retrieved from CRAN snapshot 2023-04-07).
- Shapiro, S.S.; Wilk, M.B. An analysis of variance test for normality (complete samples). Biometrika 1965, 52, 591–611. [Google Scholar] [CrossRef]
- Monter-Pozos, A.; González-Estrada, E. On Testing the Skew Normal Distribution by Using Shapiro–Wilk Test. J. Comput. Appl. Math. 2024, 440, 115649. [Google Scholar] [CrossRef]
- Demir, S. Comparison of Normality Tests in Terms of Sample Sizes under Different Skewness and Kurtosis Coefficients. Int. J. Assess. Tools Educ. 2022, 9, 397–409. [Google Scholar] [CrossRef]
- Malkewitz, C.P.; Schwall, P.; Meesters, C.; Hardt, J. Estimating reliability: A comparison of Cronbach's α, McDonald's ωt and the greatest lower bound. Soc. Sci. Human. Open 2023, 7, 100368. [Google Scholar] [CrossRef]
- Pfadt, J.M.; Sijtsma, K. Statistical Properties of Lower Bounds and Factor Analysis Methods for Reliability Estimation. In: Wiberg, M.; Molenaar, D.; González, J.; Kim, J.S.; Hwang, H. (Eds.) Quantitative Psychology. IMPS 2021. Springer Proc. Math. Stat. 2022, 393, 57–71. [CrossRef]
- Rosseel, Y.; Loh, W.W. A structural after measurement approach to structural equation modeling. Psychol. Methods 2024, 29, 561–588. [Google Scholar] [CrossRef]
- DiStefano, C.; Shi, D.; Morgan, G.B. Collapsing categories is often more advantageous than modeling sparse data: Investigations in the CFA framework. Struct. Equ. Modeling 2021, 28, 237–249. [Google Scholar] [CrossRef]
- Shi, D.; DiStefano, C.; Zheng, X.; Liu, R.; Jiang, Z. Fitting latent growth models with small sample sizes and non-normal missing data. Int. J. Behav. Dev. 2021, 45, 179–192. [Google Scholar] [CrossRef]
- Du, H.; Bentler, P.M. Distributionally weighted least squares in structural equation modeling. Psychol. Methods 2022, 27, 519–540. [Google Scholar] [CrossRef]
- Cho, G.; Hwang, H.; Sarstedt, M.; Ringle, C.M. Cutoff criteria for overall model fit indexes in generalized structured component analysis. J. Mark. Anal. 2020, 8, 189–202. [Google Scholar] [CrossRef]
- Hu, L.; Bentler, P.M. Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Struct. Equ. Model. 1999, 6, 1–55. [Google Scholar] [CrossRef]
- Shi, D.; Maydeu-Olivares, A. The Effect of Estimation Methods on SEM Fit Indices. Educ. Psychol. Meas. 2020, 80, 421–445. [Google Scholar] [CrossRef]
- Revelle, W. Psych: Procedures for psychological, psychometric, and personality research [R package]. 2019.
- Cheung, G.W.; Wang, C. Current Approaches for Assessing Convergent and Discriminant Validity with SEM: Issues and Solutions. Acad. Manag. Proc. 2017, 2017, 12706. [Google Scholar] [CrossRef]
- Kalnins, A.; Praitis Hill, K. The VIF Score. What Is It Good For? Absolutely Nothing. Organizational Research Methods 2025, 28, 58–75. [Google Scholar] [CrossRef]
- De Winter, J.C.; Gosling, S.D.; Potter, J. Comparing the Pearson and Spearman correlation coefficients across distributions and sample sizes: A tutorial using simulations and empirical data. Psychol. Methods 2016, 21, 273. Available online: https://psycnet.apa.org/buy/2016-25478-001. [CrossRef]
- Christodoulou, A.; Michaelides, M.; Karekla, M. Network analysis: A new psychometric approach to examine the underlying ACT model components. J. Contextual Behav. Sci. 2019, 12, 285–289. [Google Scholar] [CrossRef]
- Borsboom, D.; Deserno, M.K.; Rhemtulla, M.; et al. Network analysis of multivariate data in psychological science. Nat. Rev. Methods Primers 2021, 1, 58. [Google Scholar] [CrossRef]
- Epskamp, S.; Maris, G.; Waldorp, L.J.; Borsboom, D. Network psychometrics. In The Wiley Handbook of Psychometric Testing: A Multidisciplinary Reference on Survey, Scale and Test Development; 2018; pp. 953–986. [CrossRef]
- Hevey, D. Network analysis: A brief overview and tutorial. Health Psychol. Behav. Med. 2018, 6, 301–328. [Google Scholar] [CrossRef]
- Chegeni, M.; Haghdoost, A.; Shahrbabaki, M.E.; Shahrbabaki, P.M.; Nakhaee, N. Validity and reliability of the Persian version of the Adverse Childhood Experiences Abuse Short Form. J. Educ. Health Promot. 2020, 9, 140. [Google Scholar] [CrossRef]
- Kidman, R.; Smith, D.; Piccolo, L.R.; Kohler, H.P. Psychometric evaluation of the Adverse Childhood Experience International Questionnaire (ACE-IQ) in Malawian adolescents. Child Abuse Negl. 2019, 92, 139–145. [Google Scholar] [CrossRef]
- Xu, L.; Liu, X.; Wang, J. Comparing the ACE-IQ and CTQ-SF in Chinese university students: Reliability and predictive validity for PTSD and depression. Trauma Violence Abuse 2023, 24, 193–208. [Google Scholar] [CrossRef]
- Muñoz, A.C.; Rojano, Á.E.V.; Caballero, A.R.; Solé, E.P.; Álvarez, M.G. Associations between mental health problems and Adverse Childhood Experiences (ACEs) in indigenous and non-indigenous Mexican adolescents. Child Abuse Negl. 2024, 147, 106595. [Google Scholar] [CrossRef]
- Chen, W.; Yu, Z.; Wang, L.; Gross, D. Examining Childhood Adversities in Chinese Health Science Students Using the Simplified Chinese Version of the Adverse Childhood Experiences-International Questionnaire (SC-ACE-IQ). Advers. Resil. Sci. 2022, 3, 335–346. [Google Scholar] [CrossRef]
- Burgos-Benavides, L.; Cano-Lozano, M.C.; Ramírez, A.; Rodríguez-Díaz, F.J. Instruments of Child-to-Parent Violence: Systematic Review and Meta-Analysis. Healthcare 2023, 11, 3192. [Google Scholar] [CrossRef]
- Burgos-Benavides, L.; Cano-Lozano, M.C.; Ramírez, A.; Contreras, L.; Rodríguez-Díaz, F.J. To What Extent is Child-to-Parent Violence Known in Latin America? A Systematic Review and Meta-analysis. Rev. Iberoam. Psicol. Salud 2024, 15, 80–95. [Google Scholar] [CrossRef]
- Burgos-Benavides, L.; Cano-Lozano, M.C.; Ramírez, A.; León, S.P.; Medina-Maldonado, V.; Rodríguez-Díaz, F.J. Assessment of Adolescents in Child-to-Parent Violence: Invariance, Prevalence, and Reasons. Children 2024, 11, 845. [Google Scholar] [CrossRef]
- Millsap, R.E.; Olivera-Aguilar, M. Investigating measurement invariance using confirmatory factor analysis. In Handbook of Structural Equation Modeling; Hoyle, R.H., Ed.; The Guilford Press: New York, NY, USA, 2012; pp. 380–392. Available online: https://psycnet.apa.org/record/2012-16551-023.
- Ramírez, A.; Medina-Maldonado, V.; Burgos-Benavides, L.; Alfaro-Urquiola, A.L.; Sinchi, H.; Herrero Díez, J.; Rodríguez-Diaz, F.J. Validation of the Psychometric Properties of the Conflict Resolution Styles Inventory in the University Population. Soc. Sci. 2024, 13, 615. [Google Scholar] [CrossRef]
Figure 1.
Model of the Adverse Childhood Experiences Abuse Short Form (ACE-ASF). Note. F1 = Physical and Emotional Abuse, F2 = Sexual Abuse, Standardized estimates and correlation between factors. The Python code can be viewed at the following link: https://n9.cl/5x9ld.
Figure 1.
Model of the Adverse Childhood Experiences Abuse Short Form (ACE-ASF). Note. F1 = Physical and Emotional Abuse, F2 = Sexual Abuse, Standardized estimates and correlation between factors. The Python code can be viewed at the following link: https://n9.cl/5x9ld.

Figure 2.
Network, Centrality and Clustering of the Adverse Childhood Experiences Abuse Short Form (ACE-ASF) in Ecuadorian youth.
Figure 2.
Network, Centrality and Clustering of the Adverse Childhood Experiences Abuse Short Form (ACE-ASF) in Ecuadorian youth.
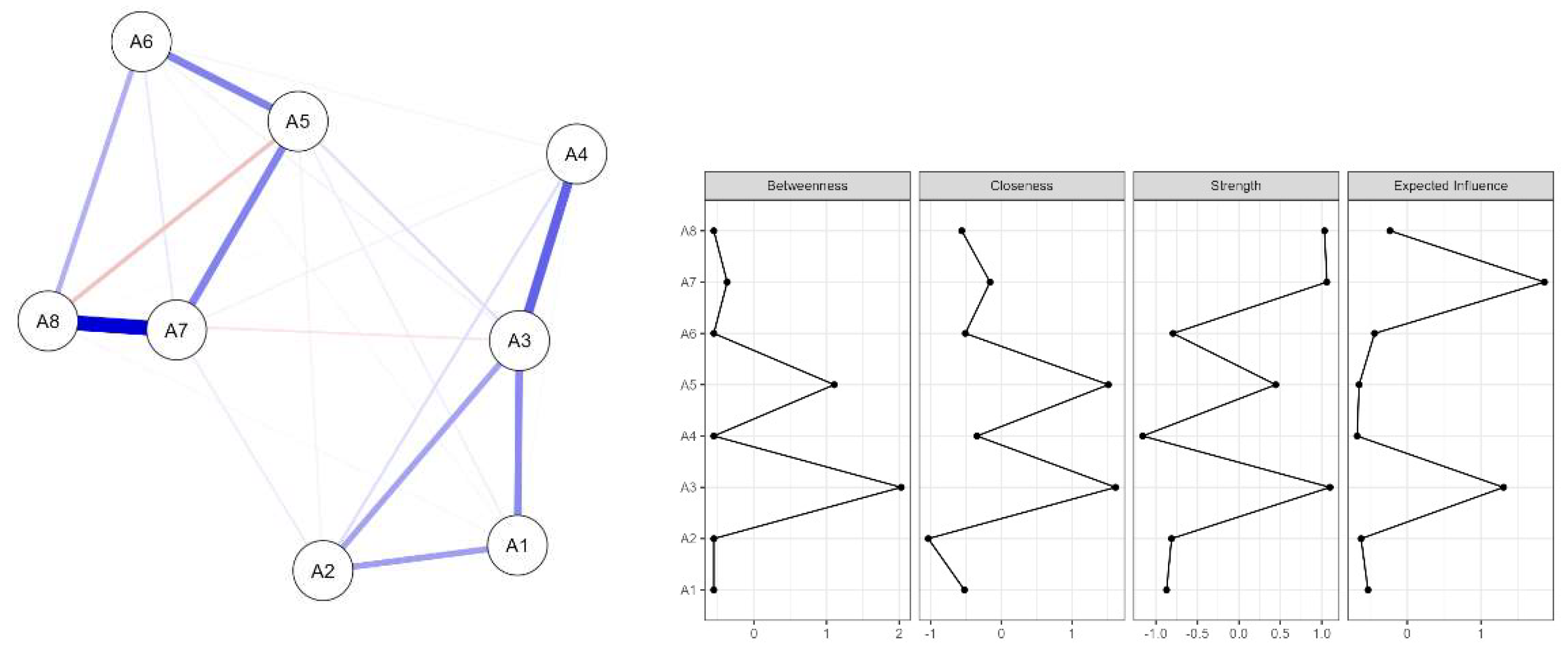
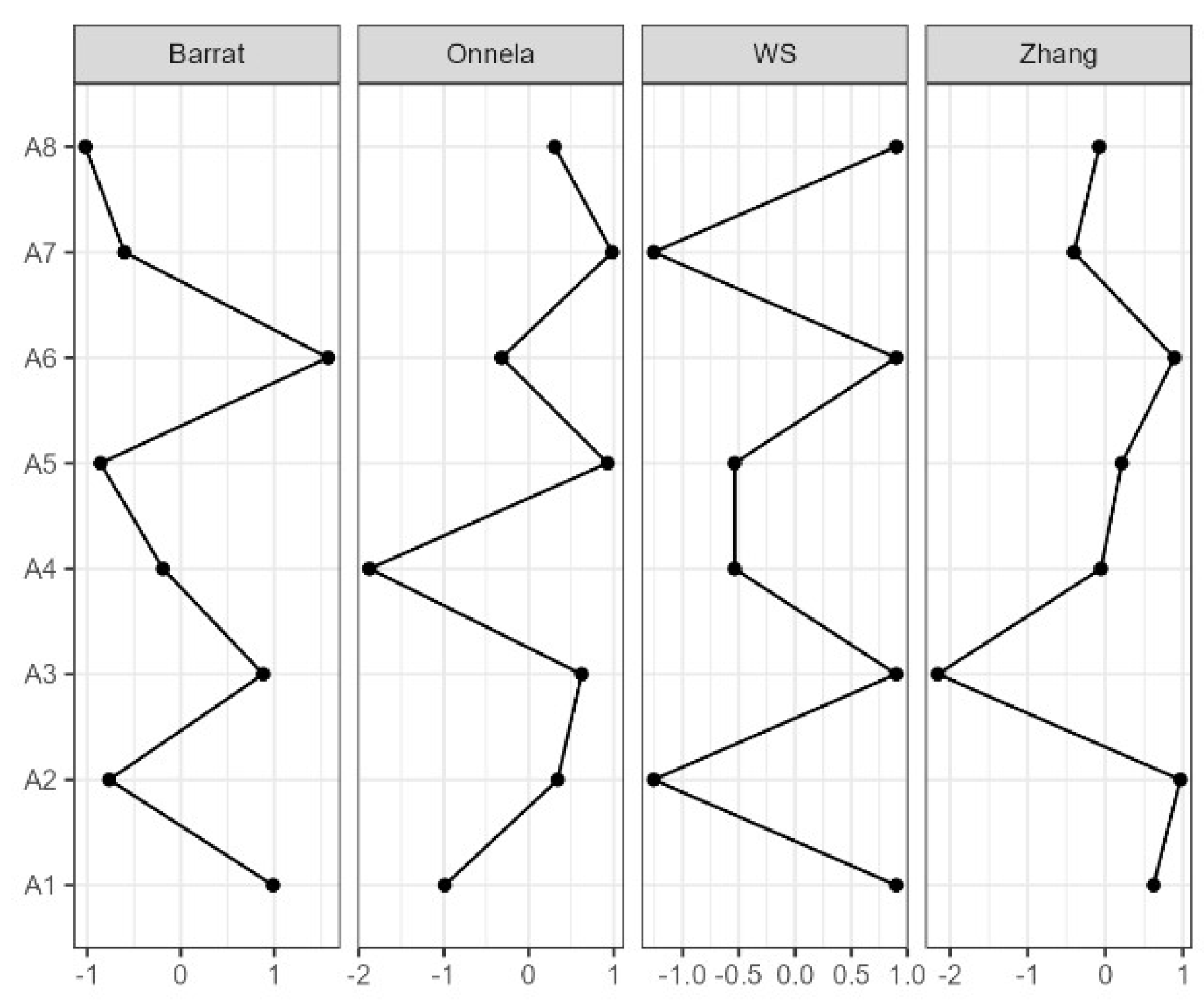
Figure 3.
Network, Centrality and Clustering of the Adverse Childhood Abuse Experiences Short Form (ACE-ASF) in Ecuadorian youth as a function of sex.
Figure 3.
Network, Centrality and Clustering of the Adverse Childhood Abuse Experiences Short Form (ACE-ASF) in Ecuadorian youth as a function of sex.
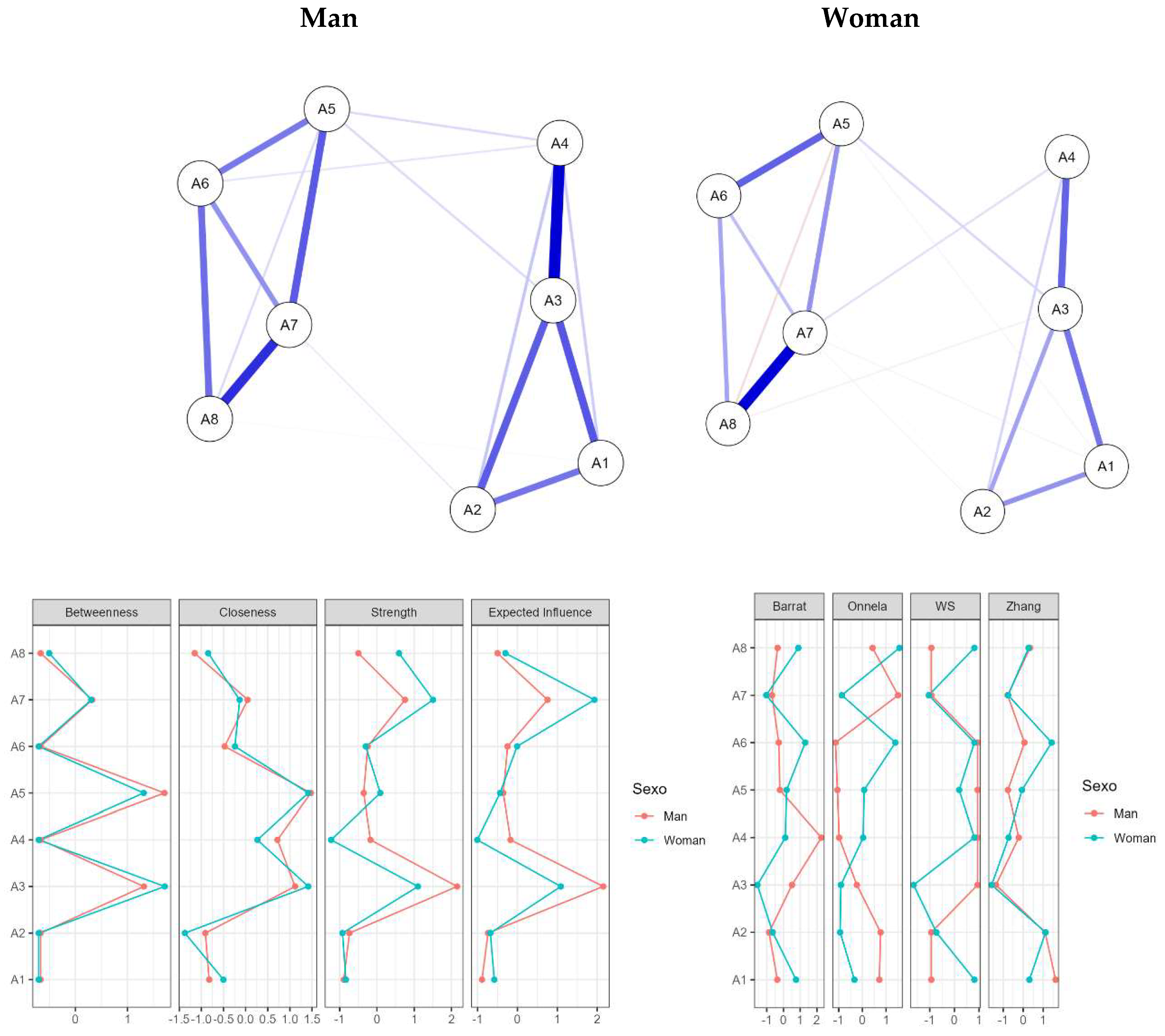
Table 1.
Descriptions of the items and dimensions of the Adverse Childhood Experiences Abuse Short Form (ACE-ASF) in Ecuadorian youth (n = 840).
Table 1.
Descriptions of the items and dimensions of the Adverse Childhood Experiences Abuse Short Form (ACE-ASF) in Ecuadorian youth (n = 840).
| Median | Mean | SD | Skewness | Kurtosis | p | Q1 | Q3 | |
|---|---|---|---|---|---|---|---|---|
| A1 | 3 | 3.283 | 1.219 | -0.159 | -1.133 | < .001 | 2 | 4 |
| A2 | 2 | 2.512 | 0.980 | 1.109 | 0.503 | < .001 | 2 | 3 |
| A3 | 3 | 3.025 | 1.162 | 0.285 | -1.050 | < .001 | 2 | 4 |
| A4 | 2 | 2.491 | 0.988 | 1.119 | 0.469 | < .001 | 2 | 3 |
| A5 | 2 | 2.242 | 0.775 | 1.601 | 3.213 | < .001 | 2 | 2 |
| A6 | 2 | 2.117 | 0.646 | 1.769 | 5.340 | < .001 | 2 | 2 |
| A7 | 2 | 2.096 | 0.609 | 2.106 | 7.914 | < .001 | 2 | 2 |
| A8 | 2 | 2.070 | 0.595 | 2.259 | 8.944 | < .001 | 2 | 2 |
Note:SD= Std. Deviation, p = P-value of Shapiro-Wilk, Q1=25th percentile, and Q3= 75th percentile.
Table 2.
Loadings, reliability and validity of the original Model of the Adverse Childhood Experiences Abuse Short Form (ACE-ASF) in Ecuadorian youth.
Table 2.
Loadings, reliability and validity of the original Model of the Adverse Childhood Experiences Abuse Short Form (ACE-ASF) in Ecuadorian youth.
| Factor | Indicator | Std. Est. (all) | α | ω | CR | VIF | ω Total | α Total | F1 | F2 |
|---|---|---|---|---|---|---|---|---|---|---|
| F1 | A1 | 0.707 | 0.823 | 0.83 | 0.83 | 1.42 | 0.872 | 0.812 | 0.553* | |
| A2 | 0.705 | |||||||||
| A3 | 0.832 | |||||||||
| A4 | 0.705 | |||||||||
| F2 | A5 | 0.858 | 0.867 | 0.861 | 0.85 | 1.56 | 0.367** | 0.637* | ||
| A6 | 0.805 | |||||||||
| A7 | 0.816 | |||||||||
| A8 | 0.654 |
Note. F1 = Physical and Emotional Abuse, F2 = Sexual Abuse, * = AVE (Convergent Validity), Bold ** = HTMT (Discriminant Validity), ω = McDonald's Omega, α = Cronbach's alpha, CF = Composite Reliability and VIF =Variance Inflation Factor.
Table 3.
Differences in the Dimensions of the Adverse Childhood Experiences Abuse Short Form (ACE-ASF) by Sex.
Table 3.
Differences in the Dimensions of the Adverse Childhood Experiences Abuse Short Form (ACE-ASF) by Sex.
| Physical and Emotional | Sexual | |||
|---|---|---|---|---|
| Man | Woman | Man | Woman | |
| n | 402 | 438 | 402 | 438 |
| Mean (M) | 11.100 | 11.500 | 8.147 | 8.868 |
| Std. Deviation | 3.625 | 3.427 | 1.623 | 2.630 |
| Median (Med) | 10 | 11 | 8 | 8 |
| IQR | 6 | 5 | 0 | 1 |
| Minimum | 4 | 4 | 4 | 4 |
| Maximum | 20 | 20 | 18 | 20 |
| 25th percentile | 8 | 9 | 8 | 8 |
| 50th percentile | 10 | 11 | 8 | 8 |
| 75th percentile | 14 | 14 | 8 | 9 |
| SE | 0.181 | 0.164 | 0.081 | 0.126 |
| Coefficient of variation | 0.327 | 0.298 | 0.199 | 0.297 |
| Mean Rank | 403.552 | 436.055 | 386.223 | 451.960 |
| Sum Rank | 162.228.000 | 190.992.000 | 155.261.500 | 197.958.500 |
| U | 81.225.000 | 74.258.500 | ||
| p | 0.051 | < .001 | ||
| VS-MPR* | 2.430 | 10.461.152 | ||
| Rank-Biserial Correlation (r) | 0.077 | 0.157 | ||
| SE Rank-Biserial Correlation | 0.040 | 0.040 | ||
Note:U = Mann-Whitney U.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



