
Submitted:
09 February 2025
Posted:
10 February 2025
You are already at the latest version
Abstract
Breast cancer is described as a nomadic growth and proliferation of cells that occurs in breast tissues. There are many tumors that are benign in the breast due to soft tissue, which are also considered non-cancerous. For example, fibrocystic changes aren't actually a cancer condition. Breast cancer is the commonest disease worldwide. This is becoming most common disease related to female mortality worldwide. Breast cancer is the deadliest disease in women. Most cancers can be cured through surgery. Clinical methods consider breast cancer to be a heterogeneous disease. The identification of expression profiles for genes has been categorized into two main groups. This group is dependent on estrogen receptors known as ER. The tumors in the breast are associated with ER expression that expresses hormone-related factors. In developed countries, the mortality threshold, especially due to breast cancer survivors, is very low. Like lung cancer in developed countries, leading cause of death is becoming breast cancer but not more so, it also causes female deaths in developing countries. There has been some encouragement in the mortality and incidence rates of breast cancer with stable new cases. There is also a decrease in the mortality rate in some high-income and developed areas. However, the opposite occurs in the developing regions of the world. There has also been a decrease in incidents and deaths in the United States and physical activity can affect hormonal concentration and energy balance.
Keywords:
Breast cancer
; Etiology
; Hormones
; Mortality rate
; heterogeneous disease
Introduction
Breast cancer is perceived as a significant malignant diseases found in women, and it is ranked as the second most common carcinoma worldwide. Among all types of cancer, breast cancer is the deadliest type in the world, accounting for 30% of new cancer cases in women. [1,2,3]. There has been a slight increase of approximately 0.3% each year in the prevalence rate of breast cancer [4], while the five-year survivability of patients of breast cancer is 90%. This rate is higher than the average of 67% for all cancer patients. [5,6,7]. Almost 5 to 10 percent of breast cancer cases can be credited to hereditary causes, such as mutations in two types of cancer genes in a family history. [8,9,10,11,12].
1.1. Structure of Breast
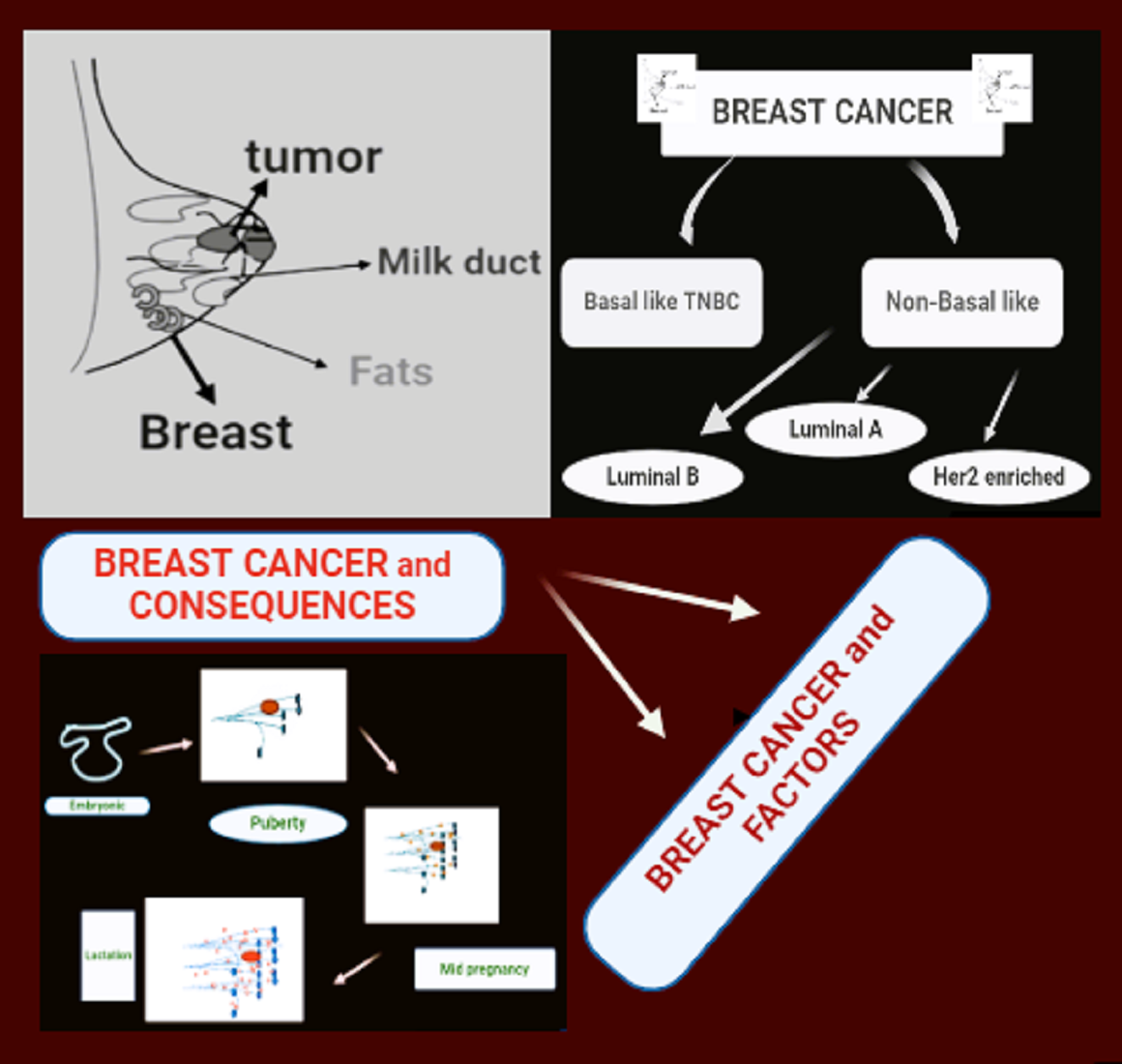
The breast is composed of two main types of tissues, which are stromal, also known as supportive tissues and glandular tissues [13,14]. The milk-producing glands, referred to as lobules, are present within the glandular tissues. There is also a passage for the flow of milk, which is referred to as ducts. Stromal tissues are composed of fibrous and adipose connective tissues present in the breast. The formation of the chest, including tissues, in the defensive system, known as lymphatic tissue. It will cleanse waste materials and cellular fluids [15,16,17,18] (Figure 1a, b).
Figure 1.
a, b. Structure of breast.

1.2. Kinds of Breast Tumors
Tumors come in various types that develop in different parts of the breast. There are many such tumors that occur due to soft tissue in the breast, which are also considered non-cancerous [19,20]. For example, fibrocystic changes aren't actually a cancer condition. It leads to the formation of cysts in women that produce fluid. Fibrosis in the breast is known as areas of lumpiness and tenderness or pain, which also involves the growth of tissue like lesions. The onset of breast cancer primarily occurs in those cells that are arranged in rows by ducts [21,22,23,24]. Some cells are in the process of forming, which are lined up in lobules. A small number begins in other tissues [25].
1.3. Death Rate Due to Breast Cancer
Breast cancer is generally found to be a diagnosable disease. This disease primarily causes death, particularly among women. This type of cancer accounts for 23 percent of the total cancer cases [26,27,28]. Approximately 14 percent of deaths worldwide are due to breast cancer. Breast cancer is primarily a disease that causes mortality in established countries and is becoming the second rising disease in developing countries. This disease is generally found among women worldwide. It will result in deaths and illnesses. It will rapidly increase over the years. Due to the influence of various significant factors in the emergence of the patient's condition, this cancer has been categorized as a multifaceted disease [29,30,31,32,33].
According to data and a report from the World Health Organization (WHO), it is anticipated that in the coming years, particularly by 2030, Breast cancer rates are rising globally [34,35]. The prevalence of this disease is very high from Eastern Africa to Western Europe. Japan has been excluded from this list; otherwise, the rate of breast cancer is higher in developed countries, while it is lower in developing countries [36]. In developed countries, the mortality threshold, especially due to breast cancer survivors, is very low. Like lung cancer in developed countries, breast cancer is additionally the driving cause of death, but not more, in developing countries [37,38,39].
There has been some encouragement in the mortality and incidence rates of breast cancer with the stable new cases. There is also a decrease in the mortality rate in higher-income and developed areas [40,41]. However, the situation has been quite the opposite in the developing regions of the world. It has been observed that since 1990, the rate of cancer has been stagnant, with a decrease of 3.5 percent each year from 2001 to 2004. The mortality rate due to breast cancer has decreased by 24 percent. This was done in comparison with two women, one of whom is young and the other has estrogen receptor-positive disease. There has also been a decrease in incidents and deaths in the United States [42,43,44,45,46].
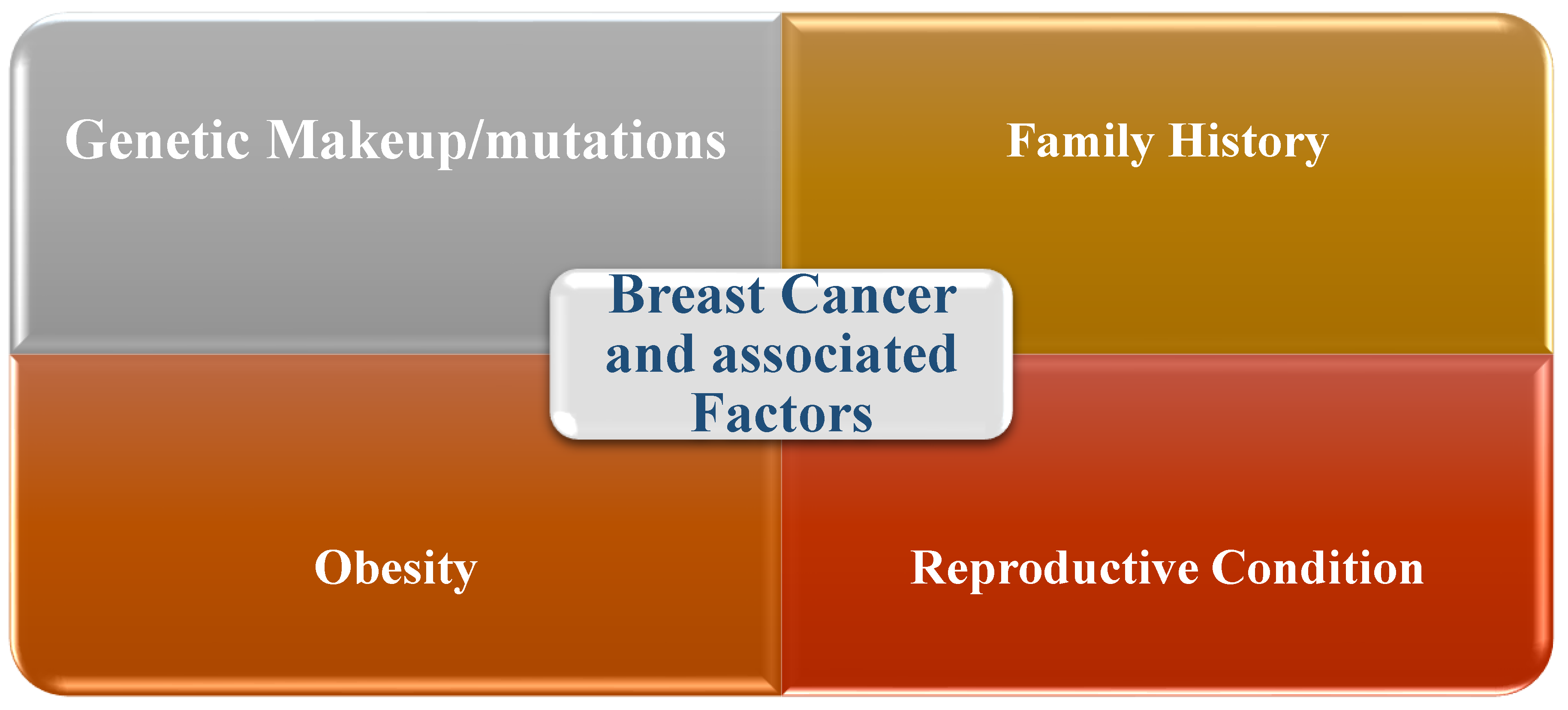
1.4. Risk Factors Associated with Breast Cancer
There are certain risk factors associated with a high level of risk for developing breast cancer. These will fall under the category of unmodifiable factors such as age, genetic predisposition, etc. [47,48,49]. The consumption of alcohol, as well as modifiable factors such as weight gain or obesity and low physical activity, are also present. Observational thinks about show that people who are exceptionally physically dynamic have a lower hazard of breast cancer compared to less dynamic ladies. These components moreover incorporate:
- Introductory evaluation and screening
- Late determination
- Financial and racial incongruities
- Hereditary and biological variables
Figure 1.
c Factors associated with breast cancer.
1.5. Treatment Approaches for Breast Cancer
Breast Cancer Overview
According to the Centers for Disease Control and Prevention (CDC), breast cancer is a disease caused by the uncontrolled multiplication of cells in the breast. The classification of breast cancer mainly depends on the type of cells that turn into cancer. Recent data estimated that about 2 million new cases were reported in 2020, and there has also been an increase in the rate of incidents over the past few years [62,63,64,65].
There are two main types of breast cancer: non-small cell cancer (non-invasive) and squamous cell cancer (invasive). Non-invasive breast cancer, like ductal carcinoma in situ (DCIS), is limited to the ducts and doesn't spread to the surrounding tissues. As opposed to, breast cancer can spread to neighboring tissues. Cancer is also a complex disease whose management varies depending on the presentation of surface markers such as hormone receptor (HR) and HER2. The commonest type of breast cancer is hormone receptor positive (HR+)/HER2 negative, accounting approximately 70% of patients and can be treated with hormonal medications such as tamoxifen. HER2-positive breast cancer is characterized by an overdose of HER2, which is responsible for 15 to 20% of cases, and can be treated with HER2-targeted therapies such as trastuzumab. Finally, triple-negative breast cancer (TNBC) has lower expression of ER, PR, and HER2 and tends to be aggressive, requiring chemotherapy as first-line treatment, while other treatments are being investigated [66,67,68].
Determining cancer risk is important for effective medical screening and prophylaxis. There are seven main risk factors associated with the development of breast cancer: gender, age, personal and family background, genetic predisposition medical history, pregnancy, external hormonal drug use, and genetic predisposition [69]. It is important to remember that the possibility of breast cancer increases with age, and those with breast cancer in a first-degree relative are 2-3 times more likely to develop the disease [70,71,72].
There is a 95% guarantee for breast cancer that these are carcinomas. Breast cancer grows from elements of epithelial cells. Breast cancer is divided into two types. They have been named in situ carcinoma and invasive carcinoma which has also been named infiltrative. In ductal or lobular epithelium, there's an increase in carcinoma. So it'll stay there. There won't be any attack on the basement membrane underneath it. But it's forming an extension beyond the epithelial boundaries [73,74,75]. The ability for metastasis won't be there anymore when there's both a malignant and local disease. Beyond the basement membrane extends lobular or ductal disease that is forming the epithelial border. Therefore, the disease is known as invasive or infiltrating ductal or lobular carcinoma. This raises the possibility of metastasis and death occurring in invasive disease [76,77].
Breast cancer is the deadly disease among women. Most cancers are cured through surgery [78]. Only 1/3 has cheating features, showing slow growth. But there is immediate metastasis. Early and recent treatments reduce the chances of developing tumors. But a repeat is certain. This will result in a higher mortality rate [79,80,81].
The seeds that are responsible for the behavior of breast cancer cells are grown in their origin. In the embryonic stage, lactating cells are affected by invasive and motile properties and cell movements. At the time of pregnancy, the circulatory formation of the mammary ducts and the alveoli occurs. These are enclosed as bilayered epithelial structures in the central lumen. Lumen cells are connected to each other by E-cadherin. It is needed for the survival of lactating cells. The luminal layer is surrounded by myoepithelial cells and enters each other through P-cadherin. P-cadherin maintained the development of preterm lactation. It is describing that myoepithelial cell junctions loosen up and trigger ductal branching. This is done by allowing luminal cells or basal progenitors that are over-allowance to basement membrane signals. Development of these bidirectional arrangements by connecting luminal and myoepithelial layers through desmosomal cadherin, desmocolin (DSC) and desmoglin (DSG). In normal mammary glands, H-cadherin is expressed. But in breast tumor cell lines, cadherin 11 and n-cadherin are expressed. There is an absence of expression patterns of these proteins in normal glands [82,83,84] (Figure 2)
3. Symptoms and Clinical Manifestations of Breast Cancer
The World Health Organization defines cancer as a broad group of diseases that occur in almost any organ or tissue in the body in which cells are abnormal. It can grow out of control, spread beyond normal, invade other parts of the body, and/or spread to other organs. . The underlying factors that promote tumor growth are called "cancer symptoms." include: (1) maintain proliferative signaling, (2) avoiding growth suppression, (3) activating invasion and metastasis, (4) enabling replicative immortalization, (5) promoting angiogenesis, (6) resisting cell death, (7) reprogramming energy metabolism, (8) inhibiting cell death and transformation, (9) tumor-promoting inflammation, (10) opening phenotypic plasticity, (11) irreversible plasticity, (12) promoting irreversible plasticity. Epigenetic reprogramming [85,86,87,88,89,90].
Some signs of breast cancer are considered classic symptoms. The first classic symptom is a lump in the breast or armpit. This will change its structure, cyclical changes, size, and skin conditions just like the monthly self-exams known as BSE. Common alert features of breast cancer include, for example, a lump that feels like a mass or swelling in the breast, lymph nodes in the armpit gets swell, blood discharge from the nipple, pain in the nipple, inversion of the nipple, scales or dimpling on the nipple skin, and persistent tenderness in the breast [91,92,93]. Lastly, there can be unusual pain or discomfort in the breast. In the metastatic stage, known as advanced, the underarm lymph nodes show more symptoms, such as bone pain, lung metastases causing shortness of breath, liver metastases leading to loss of appetite, and weight loss, headaches, nerve weakness, or pain [94,95].
In clinical ways, breast cancer is considered a heterogeneous disease. Profile identification for gene expression is divided into two basic groups. These groups depend on the estrogen receptor called the ER. Tumors in the breast are associated with ER expression of hormone-related factors. But tumors that are not related to hormones do not express ER. According to the origin of each cell type such as luminal or myoepithelial cell compartment, breast cancer classification is basal-like and non-basal-like. Basal likes are also considered "triple negatives". It accounts for about 10% of breast cancer. Its explanation is done by three hormonal receptors that are not present. These receptors are ER, human growth factor neuroreceptor (HER2), and the progesterone receptor known as PR. So, basal cytokeratin is highly expressed. There is also a difference in non-basal cancers. It is rich in luminal A, luminal B, and HER2 [96,97] (Figure 3).
There are many women around the world who are diagnosed by breast cancer. So, it will be found that breast cancer is numerically overlooked in other categories of health issues. It will also be considered an orphan disease. The reason for this is the lack of knowledge about this disease and the characteristics of tumors that distribute general care [98,99,100]. Recent policies have been made internationally for cancer, and plans have been given for new initiatives. But these are not related to breast cancer. Nutritional recommendations are also not considered. There is also a decrease in deaths in third world countries [101].
Today, it is a dangerous disease in women in Europe. Occurrence of breast cancer is increasing with age and patients tend to occur after menopause [102]. Diagnosis is a better option for breast cancer. Treatment of the disease may then be good for the survival of the patient. Survivors have improved over the years, but the risk of recurrence is probably for the rest of life. If the cancer returns after some time, it will cause more stress [103,104,105].
In comparison to initial organized diagnosis, recurrence is adjusted and more issues are perceived. This adjustment is reliable on the part of the woman for an indefinite period in the future and is more limited. There is a study that describes the intent of new diagnosis for cancer recurrence. It delineates the experience of women regarding psychological issues differently from the new diagnosis. The extent of recurrence through the early stages of breast cancer is directly illustrated in the psychological phase [106,107,108].
4. Breast Cancer and Physical Activities
Physical exercise is considered a potential intervention to improve the quality of life of women with breast cancer. Physical exercise has long been considered important in the treatment of many chronic disorders and has been successful in improving the quality of life and reducing all-cause mortality [109]. Anew studies suggest that moderate physical activity may also reduce and limited the risk of dying from breast cancer; thus, exercise may not only improve well-being but also survival. Breast cancer is considered the foremost common type of cancer within the world. More specifically, it refers to a type of cancer that occurs in the breast tissue (especially the lobules and ducts). [110] and includes various pathological conditions with many different characteristics at the molecular and cellular levels. These diseases have longer survival rates than other types of cancer. However, recurrence, metastatic spread and complications due to surgery can harm the physical and mental health of patients [111,112,113].
The coordination between physical activity and the reduction of chances of mortality due to breast cancer, as well as the lesser or less severe negative effects following treatment, is significant. Unfortunately, women diagnosed with breast cancer reduce their level of physical activity by up to 11 percent, with even greater reductions observed in patients undergoing chemotherapy (50 percent) and radiotherapy (24 percent). Since physical exercise is of utmost importance in improving physical functioning, such as cardiorespiratory fitness, muscle strength, and psychological fitness, and taking into account that a pronounced decrease in physical performance, negative changes in body composition (e.g., increased body mass) and an increased trend toward depression or anxiety are common side effects of cancer treatment, exercise after breast cancer therapy. The role of has become an important area of research [114,115,116,117,118].
Because approximately one-third of breast cancer patients receiving adjuvant chemotherapy experience cardiotoxicity, the role of exercise training in reducing cardiotoxic effects has been further investigated by physicians. Limited data are currently available to determine the best aerobic training regimen (including type, duration, and duration of exercise) to improve cardiovascular fitness and reduce morbidity and cancer risk [119]. For example, recent considers have appeared that aerobic exercise is effectual on anthracycline- and anti-HER2 monoclonal antibody-induced cardiotoxicity in women with breast cancer, improving diastolic function and cardiopulmonary function. [120].
The guidelines for physical activity for Americans have reduced the risks of recurrence and mortality by 50% due to breast cancer. Therefore, the evidence from epidemics supports that physical activity during leisure time and organized exercise before and after a diagnosis of breast cancer plays a role in reducing the risks of recurrence and mortality associated with breast cancer. Exercise can affect the systems of multiple organs and impact the overall body's homeostasis, and the integration of exercise with the brain's system has been studied to understand the molecular basis of exercise. In addition, exercise is thought to be beneficial in protecting the immune system and preventing cancer, as well as many biological processes occurring in the body. [121,122,123] (Figure 4).
5. The Natural Components Connecting Physical Movement and Breast Cancer
Sex steroid hormones increase the incidence and possibilities of breast cancer in women with elevated systemic levels of estrogen and androgen. In premenopausal ladies, physical movement is contrarily related with levels of the sex hormones estradiol and testosterone. [124]. Since sex hormones are primarily produced in adipose tissues in postmenopausal women, after adjusting for body mass index, physical activity was found to be associated with reduced levels of estrogen and estradiol, suggesting that weight loss and obesity may be associated with regulation of sex hormones and reduce cancer risk. [125,126,127].
The effects of sex hormones on body functioning suggest that physical activity, independent of weight and physical weakness, may protect against breast cancer by reducing sex hormones. [128].
Numerous ponders have appeared that elevated plasma insulin levels are coupled with cancer and increase the risk of acquiring cancer. Insulin resistance and insulin-like growth factors (IGFs) may raise the cancer risk by increasing estrogen levels. Exercise reduces insulin resistance and insulin sensitivity, increases glucose uptake, total IGF-1, and IGF-binding proteins. [129,130,131]. In addition, fasting insulin levels decreased in breast cancer patients due to weight loss after exercise intervention, and this is thought to contribute to improved breast cancer screening. Sex steroid hormones such as estrogen and androgen increase the risk of developing and spreading breast cancer in women with breast cancer. Physical activity in premenopausal women is associated with levels of the sex hormones estradiol and testosterone. This suggests that weight loss and obesity may be associated with regulating female hormones and reducing cancer risk in patients. (Table 2) [132,133,134,135,136].
Physical activity is generally anti-inflammatory and may reduce the risk of disease in healthy individuals without a diagnosis of cancer. The influence of physical activity on IL-6, TNF-α, and CRP levels are variable and limited. Adipose tissue contains multiple cell types found in mammary glands and secretes adiponectin, leptin, resistin, and other cytokines. Physical activity has also been shown to regulate circulating adipokines. Leptin promotes breast cancer growth, migration, and metastasis through its proinflammatory effects, while adiponectin is an anti-inflammatory hormone that interacts negatively with fat. Low adiponectin is associated with higher body weight and more fat, and the adiponectin: leptin ratio is an important determinant of the effect of adipokines on breast cancer risk. Physical activity has been shown to directly affect body fat, resulting in increased serum adiponectin levels and decreased serum leptin levels. [137,138].
Physical activity can modulate cytokines and adipokines. However, a small reduction in cancer risk has been associated with reducing obesity and losing weight. Myocaine and stress hormones release various actin proteins, such as IL-6, myonectin, myostatin, and irisin, into the skeletal muscles, our largest organ, during exercise, and circulating actin levels are adjusted by the exercise [139].
An approach to characterize muscle tissue to recognize the molecular basis of exercise performance. Clinical studies have shown that increasing irisin levels through physical activity can prevent cancer by activating caspases and inhibiting NF-κB activity. The stress hormone catecholamines are an important factor in the prevention of breast cancer. Exercise rapidly increases plasma epinephrine and norepinephrine. Cortisol levels vary with the duration and intensity of exercise. Exercise can regulate tumor growth by activating the catecholamines hippo signaling pathway. [140,141,142].
However, the role of stress hormones as an important component of exercise has not been directly studied in cancer patients and may have implications for cancer prevention [143]. Many circulating factors such as hormones, inflammatory markers, and actin can be regulated by physical activity and exercise. Many metabolites in plasma play a role in body functions and may play an important role in cancer prevention [144,145,146].
Various ponders have appeared that plasma metabolites are related with cancer chance and may serve as biomarkers for early cancer discovery. Oxidative stress and reactive oxygen species are associated with many diseases, including cancer development and progression. Interestingly, intense exercise creates a prooxidative environment [147,148]. However, regular exercise can increase the ability to withstand oxidative environments by increasing antioxidant defenses. In this context, the persistent physiological effects of oxidative stress may help prevent breast cancer progression and metastasis. [149,150,151].
Recent studies have revealed that expression of microRNAs is regulated by physical activity and exercise in healthy individuals and patients with various diseases.. Due to their significant role in regulating cell growth, microRNAs may serve as important regulators and potential biomarkers of movement and response. Some microRNAs associated with breast cancer, such as miR-21 and let-7a, have been altered through exercise, indicating that microRNAs may mediate the relationship between exercise and cancer. [152,153].
Functional molecules such as proteins, lipids, mRNA and microRNA, as well as different soluble mediators, can act as a source of communication between tissues during physical exercise, leading to biological effects. Physical exercise causes the rapid release of exosomes into the circulation, and their production plays an important role in the overall coordination of the body by providing actin. Therefore, ectopic cysts can ameliorate the negative effects of exercise and affect breast development. [154,155].
Physical activity has a significant effect on the level and function of the immune system, as do natural antibiotics, which are the most potent anti-infective agents in circulation. IL-6 increased the activation of killer cells in spontaneously mutated mice, leading to reduced tumor initiation and progression [156]. Additionally, the tumor microenvironment can regulate inflammatory processes by using myelosuppressive cells, exercise, and weight loss as preventive strategies, thus controlling tumor growth and metastasis. Finally, Evidence suggests that gut microbiota may play a role in the development of many cancers and may influence treatment and that the microbiome may play a role in the maintenance of some deadly diseases, including breast cancer. Exercise may reduce obesity-induced inflammatory diseases and alter the structure and metabolites of the gut microbiota. Therefore, physical interventions may alter the gut microbial community composition associated with disease. Generally, physical activity and the changes that happen in the body during it can help in preventing breast cancer and improving overall survival outcomes. [157,158,159].
6. Discussion
Physical activity may prevent breast cancer, especially in young premenopausal and postmenopausal women. Both recreational and occupational activities reduce the overall risk. [160]. There is a significant relationship between recreational activities and cancer risk, and this relationship is mediated by nutrition and exercise. Protective effects of physical activity have been shown in premenopausal and postmenopausal women, and retrospective analyses also suggest that physical activity has a protective effect.
Recent studies have shown that there is a link between physical activity and cancer, and that it has a protective effect on the body against cancer. It is stated that physical activity reduces the risk of developing 13 types of cancer. The relationship between exercise and reduced cancer risk is especially strong in women with early-stage breast cancer. [161,162,163,164].
The risk of breast cancer is influenced by endogenous hormones. Physical activity can provide a way to fundamentally prevent breast cancer through its effect on ovarian hormones. This effect is shown through changes in age during menstruation and the number and nature of menstrual cycles, which are factors related to the risk of breast cancer itself [165].
Studies on animals show that the risk of breast cancer is lower with exercise at the onset of tumors, but not necessarily during tumor promotion. Epidemiological studies indicate that overall, women who are more physically active have a lower risk of breast cancer, while experimental studies on the effects of exercise in women suggest that exercise can affect the characteristics of the menstrual cycle. Studies show that physical activity reduces the hazards of cancer. It can prevent cancer growth and metastasis, beat the after-effects of cancer treatment, increase patients' endurance to treatment, and improve patients' well-being. By deeply understanding the effects of physical training on the development and progression of malignant tumors, metabolic pathways, and immune responses, we can understand the relationship between exercise and cancer prevention, and then develop personalized treatments for patients. Besides the positive effects of exercise, it's also helpful in treating other diseases and differentiating some cancers. [166,167,168].
Despite this, women have faced obstacles in experimental studies and epidemiological studies of physical activity and breast cancer risk due to several methodological limitations [169]. Major problems in epidemiological studies include inadequate and inadequate measurement of women's physical activity throughout their lives and inadequate control of potential confounding factors. Experimental studies examining the effects of physical activity on female fertility have not fully assessed the effects of exercise and changes in the menstrual cycle. Physical exercise, when combined with surgery, chemotherapy, radiation therapy, immunotherapy, and other cancer treatments, can inhibit the growth of cancer cells. It fights cancer by improving the proliferation of cancer cells, increasing blood perfusion, promoting angiogenesis, and activating the body's immune system. Exercise may improve cancer risk and survival, especially for breast, colon and prostate cancer. Exercise affects cancer metabolic reprogramming through improvements in blood perfusion, angiogenesis, and cancer hypoxia. [170,171,172].
7. Conclusion
There are a lot of risk factors involved in the development of breast cancer. The data available shows that women are at risk of breast cancer recurrence. In developed countries, women are dying from breast cancer. The lethality of breast cancer also contributes to mortality. The significant links between lifetime and current physical activity and the risk of death from all causes will be associated with death related to breast cancer. Physical activity after diagnosis will reduce the risk of death. Further studies are discovering new mechanisms through which physical activity increases the survival of breast cancer survivors.
Future Perspective:
Exercise can motivate people to make lifestyle changes, improve aerobic fitness and physical activity, manage fatigue, and improve quality of life. In addition to non-drug prevention and prevention, exercise can help reduce the risk of cancer. Moreover, physical activity plays a role in the treatment of all types of cancer. For instance, it can lessen treatment-related toxicity and side effects, and enhance the effects of other treatments. So, it's important to not just look into the effects of physical exercise on all aspects of cancer, but also to figure out the type, amount, and intensity of exercise that matters. Patients should develop an exercise program tailored to the specific needs of their cancer treatment and follow physical therapy instructions. Long-term exercise follow-up in people with cancer can improve muscle strength, physical fitness, physical capacity, and exercise tolerance.
References
- Arnold, M.; Morgan, E.; Rumgay, H.; Mafra, A.; Singh, D.; Laversanne, M.; Soerjomataram, I. Current and future burden of breast cancer: Global statistics for 2020 and 2040. The Breast. 2022, 66, 15–23. [Google Scholar] [CrossRef] [PubMed]
- Mattiuzzi, C.; Lippi, G. Current cancer epidemiology. Journal of epidemiology and global health. 2019, 9, 217–222. [Google Scholar] [CrossRef] [PubMed]
- Lin, H.Y.; Park, JY. Epidemiology of Cancer. In Anesthesia for Oncological Surgery. Cham: Springer International Publishing 2024, 11-16.
- Giaquinto, AN.; Sung, H.; Miller, KD.; Kramer, JL.; Newman, LA.; Minihan, A.; Siegel, RL. Breast cancer statistics, 2022. CA: a cancer journal for clinicians. 2022, 72, 524–541. [Google Scholar] [CrossRef]
- Giaquinto, AN.; Sung, H.; Newman, LA.; Freedman, RA.; Smith, RA.; Star, J.; Siegel, RL. Breast cancer statistics 2024. CA: a cancer journal for clinicians. 2024, 74, 477–495. [Google Scholar] [CrossRef]
- Ali-Gombe, M.; Mustapha, MI.; Folasire, A.; Ntekim, A. , Campbell, OB. Pattern of survival of breast cancer patients in a tertiary hospital in South West Nigeria. Ecancermedicalscience. 2021, 15. [Google Scholar] [CrossRef]
- Ilic, L.; Simon, J.; Hackl, M.; Haidinger, G. Time Trends in Male Breast Cancer Incidence, Mortality, and Survival in Austria (1983–2017). Clinical Epidemiology. 2024, 57–69. [Google Scholar] [CrossRef]
- Liu, L.; Hao, X.; Song, Z.; Zhi, X.; Zhang, S.; Zhang, J. Correlation between family history and characteristics of breast cancer. Scientific reports. 2021, 11, 6360. [Google Scholar] [CrossRef]
- Sokolova, A.; Johnstone, KJ.; McCart Reed, AE.; Simpson, PT.; Lakhani, SR. Hereditary breast cancer: syndromes, tumour pathology and molecular testing. Histopathology. 2023, 82, 70–82. [Google Scholar] [CrossRef]
- Hong, R.; Xu, B. Breast cancer: an up-to-date review and future perspectives. Cancer communications. 2022, 42, 913–936. [Google Scholar] [CrossRef]
- Fakhri, N.; Chad, MA.; Lahkim, M.; Houari, A.; Dehbi, H.; Belmouden, A.; El Kadmiri, N. Risk factors for breast cancer in women: an update review. Medical Oncology. 2022, 39, 197. [Google Scholar] [CrossRef]
- Wang, X.; Zou, C.; Zhang, Y.; Li, X.; Wang, C.; Ke, F.; Zhang, Y. Prediction of BRCA gene mutation in breast cancer based on deep learning and histopathology images. Frontiers in Genetics. 2021, 12, 661109. [Google Scholar] [CrossRef] [PubMed]
- Biswas, SK.; Banerjee, S.; Baker, GW.; Kuo, CY.; Chowdhury, I. (2022). The mammary gland: basic structure and molecular signaling during development. International Journal of Molecular Sciences. 2022, 23, 3883. [Google Scholar] [CrossRef] [PubMed]
- Ferreira, T.; Gama, A.; Seixas, F.; Faustino-Rocha, AI.; Lopes, C.; Gaspar, VM.; Oliveira, PA. Mammary glands of women, female dogs and female rats: similarities and differences to be considered in breast cancer research. Veterinary Sciences. 2023, 10, 379. [Google Scholar] [CrossRef] [PubMed]
- Kumar, V. Age related histomorphological and histochemical studies on mammary gland of goat (Doctoral dissertation, Guru Angad Dev Veterinary and Animal Sciences University), 2022.
- Josefson, C. C.; Orr, TJ.; Hood, WR.; Skibiel, AL. Hormones and lactation in mammals. In Hormones and Reproduction of Vertebrates. 2024, 137–167. [Google Scholar]
- Ingthorsson, S.; Traustadottir, GA.; Gudjonsson, T. Breast Morphogenesis: From Normal Development to Cancer. A Guide to Breast Cancer Research: From Cellular Heterogeneity and Molecular Mechanisms to Therapy.
- Gomes, PRL. ; Motta-Teixeira, LC.; Gallo, CC.; do Carmo Buonfiglio, D.; de Camargo, LS.; Quintela, T.; Cipolla-Neto, J. Maternal pineal melatonin in gestation and lactation physiology, and in fetal development and programming. General and comparative endocrinology. 2021, 300, 113633. [Google Scholar] [CrossRef]
- Lawrence, RA. Physiology of lactation. In Breastfeeding. 2022, 58–92. [Google Scholar]
- Agre, AM.; Upade, AC.; Yadav, MA.; Kumbhar, SB. A Review on Breasr Cancer and Its Management. World J. Pharm. Res. 2021, 10, 408–437. [Google Scholar]
- Mohammed, AA. Benign breast disorders in female. Revista de Senología y Patología Mamaria. 2022, 35, 42–48. [Google Scholar] [CrossRef]
- Gupta, M.; Goyal, N. Applied anatomy of breast cancer. In Breast Cancer: Comprehensive Management. 2022, 23-35.
- Briem, E.; Ingthorsson, S.; Traustadottir, GA.; Hilmarsdottir, B.; Gudjonsson, T. Application of the D492 cell lines to explore breast morphogenesis, EMT and cancer progression in 3D culture. Journal of mammary gland biology and neoplasia, 2019, 24, 139–147. [Google Scholar] [CrossRef]
- Beňačka, R.; Szabóová, D.; Guľašová, Z.; Hertelyová, Z.; Radoňák, J. Classic and new markers in diagnostics and classification of breast cancer. Cancers. 2022, 14, 5444. [Google Scholar] [CrossRef]
- Ramos, R.; Swedlund, B.; Ganesan, AK.; Morsut, L.; Maini, PK.; Monuki, ES.; Plikus, MV. Parsing patterns: Emerging roles of tissue self-organization in health and disease. Cell. 2024, 187, 3165–3186. [Google Scholar] [CrossRef] [PubMed]
- Sosinsky, AZ.; Rich-Edwards, JW.; Wiley, A.; Wright, K.; Spagnolo, PA.; Joffe, H. Enrollment of female participants in United States drug and device phase 1–3 clinical trials between 2016 and 2019. Contemporary Clinical Trials. 2022, 115, 106718. [Google Scholar] [CrossRef] [PubMed]
- Wang, W.; Yan, Y.; Guo, Z.; Hou, H.; Garcia, M.; Tan, X.; Suboptimal Health Study Consortium and European Association for Predictive, Preventive and Personalised Medicine. All around suboptimal health—a joint position paper of the Suboptimal Health Study Consortium and European Association for Predictive, Preventive and Personalised Medicine. EPMA Journal. 2021, 12, 403–433. [Google Scholar] [CrossRef]
- Ruiz, JM.; O'Neill, RM.; Juster, RP.; Irgens, MS. Dimensions of diversity and influences on health disparities. In APA handbook of health psychology, Volume 1: Foundations and context of health psychology. 2025, 51-70.
- Huang, J.; Chan, PS.; Lok, V.; Chen, X.; Ding, H.; Jin, Y.; Wong, MC. Global incidence and mortality of breast cancer: a trend analysis. Aging (Albany NY). 2021, 13, 5748. [Google Scholar] [CrossRef]
- Lei, S.; Zheng, R.; Zhang, S.; Wang, S.; Chen, R.; Sun, K.; Wei, W. Global patterns of breast cancer incidence and mortality: A population-based cancer registry data analysis from 2000 to 2020. Cancer Communications. 2021, 41, 1183–1194. [Google Scholar] [CrossRef]
- Wilkinson, L.; Gathani, T. Understanding breast cancer as a global health concern. The British journal of radiology. 2022, 95, 20211033. [Google Scholar] [CrossRef]
- Lima, SM.; Kehm, RD.; Terry, MB. Global breast cancer incidence and mortality trends by region, age-groups, and fertility patterns. EClinicalMedicine. 2021, 38. [Google Scholar] [CrossRef]
- Sopik, V. International variation in breast cancer incidence and mortality in young women. Breast Cancer Research and Treatment. 2021, 186, 497–507. [Google Scholar] [CrossRef]
- Zhang, S.; Jin, Z.; Bao, L.; Shu, P. The global burden of breast cancer in women from 1990 to 2030: assessment and projection based on the global burden of disease study 2019. Frontiers in Oncology. 2024, 14, 1364397. [Google Scholar] [CrossRef]
- Soerjomataram, I.; Bray, F. Planning for tomorrow: global cancer incidence and the role of prevention 2020–2070. Nature reviews Clinical oncology. 2021, 18, 663–672. [Google Scholar] [CrossRef]
- Fuentes, JDB. ; Morgan, E.; de Luna Aguilar, A.; Mafra, A.; Shah, R.; Giusti, F.; Soerjomataram, I. Global stage distribution of breast cancer at diagnosis: a systematic review and meta-analysis. JAMA oncology. 2024, 10, 71–78. [Google Scholar] [CrossRef] [PubMed]
- Duggan, C.; Trapani, D.; Ilbawi, AM.; Fidarova, E.; Laversanne, M.; Curigliano, G.; Anderson, BO. National health system characteristics, breast cancer stage at diagnosis, and breast cancer mortality: a population-based analysis. The Lancet Oncology. 2021, 22, 1632–1642. [Google Scholar] [CrossRef] [PubMed]
- Thandra, KC.; Barsouk, A.; Saginala, K.; Aluru, JS.; Barsouk, A. Epidemiology of lung cancer. Contemporary Oncology/Współczesna Onkologia. 2021, 25, 45–52. [Google Scholar] [CrossRef] [PubMed]
- Tanoue, LT. Women and lung cancer. Clinics in Chest Medicine. 2021, 42, 467–482. [Google Scholar] [CrossRef]
- Wojtyla, C.; Bertuccio, P.; Wojtyla, A.; La Vecchia, C. European trends in breast cancer mortality, 1980–2017 and predictions to 2025. European Journal of Cancer. 2021, 152, 4–17. [Google Scholar] [CrossRef]
- Nogueira, MC.; Guerra, MR.; Bustamante-Teixeira, MT.; e Silva, GA.; Tomazelli, J.; Pereira, DDA. ; Malta, DC. Mortality due to cervical and breast cancer in health regions of Brazil: impact of public policies on cancer care. Public Health. 2024, 236, 239–246. [Google Scholar] [CrossRef]
- Siegel, RL.; Kratzer, TB.; Giaquinto, AN.; Sung, H.; Jemal, A. Cancer statistics, 2025. CA: A Cancer Journal for Clinicians.
- Siegel, RL.; Miller, KD.; Wagle, NS.; Jemal, A. Cancer statistics, 2023. CA: a cancer journal for clinicians. 2023, 73, 17–48. [Google Scholar] [CrossRef]
- Giaquinto, AN.; Miller, KD.; Tossas, KY.; Winn, RA.; Jemal, A.; Siegel, RL. Cancer statistics for African American/black people 2022. CA: a cancer journal for clinicians. 2022, 72, 202–229. [Google Scholar] [CrossRef]
- Qing, T.; Karn, T.; Rozenblit, M.; Foldi, J.; Marczyk, M.; Shan, NL.; Pusztai, L. Molecular differences between younger versus older ER-positive and HER2-negative breast cancers. NPJ Breast Cancer. 2022, 8, 119. [Google Scholar] [CrossRef]
- Yoon, KH.; Park, Y.; Kang, E.; Kim, EK.; Kim, JH.; Kim, SH.; Shin, HC. Effect of estrogen receptor expression level and hormonal therapy on prognosis of early breast cancer. Cancer Research and Treatment: Official Journal of Korean Cancer Association. 2022, 54, 1081–1090. [Google Scholar] [CrossRef]
- McCarthy, AM.; Friebel-Klingner, T.; Ehsan, S.; He, W.; Welch, M.; Chen, J.; Armstrong, K. Relationship of established risk factors with breast cancer subtypes. Cancer medicine. 2021, 10, 6456–6467. [Google Scholar] [CrossRef] [PubMed]
- Daly, AA.; Rolph, R.; Cutress, RI.; Copson, ER. A review of modifiable risk factors in young women for the prevention of breast cancer. Breast Cancer: Targets and Therapy.
- Bodewes, FTH. ; Van Asselt, AA.; Dorrius, MD.; Greuter, MJW.; De Bock, GH. Mammographic breast density and the risk of breast cancer: A systematic review and meta-analysis. The Breast. 2022, 66, 62–68. [Google Scholar] [CrossRef] [PubMed]
- Sarmiento, DD.; Tumas, N.; Pereyra, SA.; Scruzzi, GF.; Pou, SA. Social determinants of breast cancer screening: a multilevel analysis of proximal and distal factors related to the practice of mammography. Cancer Epidemiology, Biomarkers & Prevention. 2024, 33, 1651–1658. [Google Scholar]
- Czwikla, J.; Urbschat, I.; Kieschke, J.; Schüssler, F.; Langner, I.; Hoffmann, F. Assessing and explaining geographic variations in mammography screening participation and breast cancer incidence. Frontiers in Oncology. 2019, 9, 909. [Google Scholar] [CrossRef]
- Tan, HS.; Plichta, JK.; Kong, A.; Tan, CW.; Hwang, S.; Sultana, R.; Habib, AS. Risk factors for persistent pain after breast cancer surgery: a multicentre prospective cohort study. Anaesthesia. 2023, 78, 432–441. [Google Scholar] [CrossRef]
- Klein, I.; Kalichman, L.; Chen, N.; Susmallian, S. A comprehensive approach to risk factors for upper arm morbidities following breast cancer treatment: a prospective study. BMC cancer. 2021, 21, 1–10. [Google Scholar] [CrossRef]
- Waks, AG.; Winer, EP. Breast cancer treatment: a review. Jama. 2019, 321, 288–300. [Google Scholar] [CrossRef]
- Davies, E.; Hiscox, S. New therapeutic approaches in breast cancer. Maturitas. 2011, 68, 121–128. [Google Scholar] [CrossRef]
- Trayes, KP.; Cokenakes, SE. Breast cancer treatment. American family physician. 2021, 104, 171–178. [Google Scholar]
- Riis, M. Modern surgical treatment of breast cancer. Annals of medicine and surgery. 2020, 56, 95–107. [Google Scholar] [CrossRef]
- Shah, C.; Bauer-Nilsen, K.; McNulty, RH.; Vicini, F. Novel radiation therapy approaches for breast cancer treatment. In Seminars in Oncology. 2020, 47, 209–216. [Google Scholar] [CrossRef] [PubMed]
- Anampa, J.; Makower, D.; Sparano, JA. Progress in adjuvant chemotherapy for breast cancer: an overview. BMC medicine. 2015, 13, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Denduluri, N.; Somerfield, MR.; Chavez-MacGregor, M.; Comander, AH.; Dayao, Z.; Eisen, A.; Giordano, SH. Selection of optimal adjuvant chemotherapy and targeted therapy for early breast cancer: ASCO guideline update. Journal of Clinical Oncology. 2021, 39, 685–693. [Google Scholar] [CrossRef] [PubMed]
- Ficarra, S.; Thomas, E.; Bianco, A.; Gentile, A.; Thaller, P.; Grassadonio, F.; Hofmann, H. Impact of exercise interventions on physical fitness in breast cancer patients and survivors: a systematic review. Breast Cancer. 2022, 29, 402–418. [Google Scholar] [CrossRef]
- Figueroa, JD.; Gray, E.; Pashayan, N.; Deandrea, S.; Karch, A.; Vale, DB.; Breast Screening Working Group. The impact of the Covid-19 pandemic on breast cancer early detection and screening. Preventive medicine. 2021, 151, 106585. [Google Scholar] [CrossRef]
- Smolarz, B.; Nowak, AZ.; Romanowicz, H. Breast cancer—epidemiology, classification, pathogenesis and treatment (review of literature). Cancers. 2022, 14, 2569. [Google Scholar] [CrossRef]
- Goff, SL.; Danforth, DN. The role of immune cells in breast tissue and immunotherapy for the treatment of breast cancer. Clinical breast cancer. 2021, 21, e63–e73. [Google Scholar] [CrossRef]
- Łukasiewicz, S.; Czeczelewski, M.; Forma, A.; Baj, J.; Sitarz, R.; Stanisławek, A. Breast cancer—epidemiology, risk factors, classification, prognostic markers, and current treatment strategies—an updated review. Cancers. 2021, 13, 4287. [Google Scholar] [CrossRef]
- Schegoleva, AA.; Khozyainova, AA.; Fedorov, AA.; Gerashchenko, TS.; Rodionov, EO.; Topolnitsky, EB.; Denisov, EV. Prognosis of different types of non-small cell lung cancer progression: current state and perspectives. Cell Physiol Biochem. 2021, 55, 29–48. [Google Scholar]
- Orrantia-Borunda, E.; Anchondo-Nuñez, P.; Acuña-Aguilar, LE.; Gómez-Valles, FO.; Ramírez-Valdespino, CA. Subtypes of breast cancer. Breast Cancer. 2022.
- Zapletal, O.; Žatecký, J.; Gabrielová, L.; Selingerová, I.; Holánek, M.; Burkoň, P.; Coufal, O. Axillary Overtreatment in Patients with Breast Cancer After Neoadjuvant Chemotherapy in the Current Era of Targeted Axillary Dissection. Cancers. 2025, 17, 178. [Google Scholar] [CrossRef] [PubMed]
- Kanth, P.; Inadomi, JM. Screening and prevention of colorectal cancer. Bmj. 2021, 374. [Google Scholar] [CrossRef] [PubMed]
- Monticciolo, DL.; Malak, SF.; Friedewald, SM.; Eby, PR.; Newell, MS.; Moy, L.; Smetherman, D. Breast cancer screening recommendations inclusive of all women at average risk: update from the ACR and Society of Breast Imaging. Journal of the American College of Radiology. 2021, 18, 1280–1288. [Google Scholar] [CrossRef] [PubMed]
- Cathcart-Rake, EJ.; Ruddy, KJ.; Bleyer, A.; Johnson, RH. Breast cancer in adolescent and young adult women under the age of 40 years. JCO oncology practice. 2021, 17, 305–313. [Google Scholar] [CrossRef]
- Kashyap, D.; Pal, D.; Sharma, R.; Garg, VK.; Goel, N.; Koundal, D.; Belay, A. [Retracted] Global Increase in Breast Cancer Incidence: Risk Factors and Preventive Measures. BioMed research international. 2022, (1), 9605439. [Google Scholar] [CrossRef]
- Stavrou, M.; Constantinidou, A. Tumor associated macrophages in breast cancer progression: implications and clinical relevance. Frontiers in Immunology. 2024, 15, 1441820. [Google Scholar] [CrossRef]
- Bhardwaj, P.; Brown, KA. Obese adipose tissue as a driver of breast cancer growth and development: update and emerging evidence. Frontiers in Oncology. 2021, 11, 638918. [Google Scholar] [CrossRef]
- McCart Reed, AE.; Kalinowski, L.; Simpson, PT.; Lakhani, SR. Invasive lobular carcinoma of the breast: the increasing importance of this special subtype. Breast Cancer Research. 2021, 23, 1–16. [Google Scholar] [CrossRef]
- Yang, X. Surviving Late-Stage Cancers by Practicing Guan Yin Citta Dharma Door. Health Science Journal. 2024, 18, 1–12. [Google Scholar]
- Baum, NH.; Mobley, D.; Key, RG. Prostate Cancer: Expert Advice for Helping Your Loved One.2023.
- Shang, C.; Xu, D. Epidemiology of Breast Cancer. Oncologie (Tech Science Press). 2022, 24. [Google Scholar] [CrossRef]
- Bulska-Będkowska, W.; Czajka-Francuz, P.; Jurek-Cisoń, S.; Owczarek, AJ.; Francuz, T.; Chudek, J. The predictive role of serum levels of soluble cell adhesion molecules (sCAMs) in the therapy of advanced breast cancer—A single-centre study. Medicina. 2022, 58, 153. [Google Scholar] [CrossRef] [PubMed]
- San Juan, BP.; Hediyeh-Zadeh, S.; Rangel, L.; Milioli, HH.; Rodriguez, V.; Bunkum, A.; Chaffer, CL. Targeting phenotypic plasticity prevents metastasis and the development of chemotherapy-resistant disease. MedRxiv. 2022, 2022–03. [Google Scholar]
- Guang, Y.; Wan, F.; He, W.; Zhang, W.; Gan, C.; Dong, P.; Zhang, Y. A model for predicting lymph node metastasis of thyroid carcinoma: a multimodality convolutional neural network study. Quantitative Imaging in Medicine and Surgery. 2023, 13, 8370. [Google Scholar] [CrossRef] [PubMed]
- Moral, R.; Escrich, E. Influence of olive oil and its components on breast cancer: Molecular mechanisms. Molecules. 2022, 27, 477. [Google Scholar] [CrossRef]
- Narain, R.; Muncie-Vasic, JM.; Weaver, VM. Forcing the code: tension modulates signaling to drive morphogenesis and malignancy. Genes & Development. 2025, 39, 163–181. [Google Scholar]
- Vickers, R.; Porter, W. Immune Cell Contribution to Mammary Gland Development. Journal of Mammary Gland Biology and Neoplasia. 2024, 29, 16. [Google Scholar] [CrossRef]
- So, WK.; Law, BM.; Ng, MS.; He, X.; Chan, DN.; Chan, CW.; McCarthy, AL. Symptom clusters experienced by breast cancer patients at various treatment stages: a systematic review. Cancer Medicine. 2021, 10, 2531–2565. [Google Scholar] [CrossRef]
- Lehman, CD.; Lamb, LR.; D'Alessandro, HA. Mitigating the impact of coronavirus disease (COVID-19) vaccinations on patients undergoing breast imaging examinations: a pragmatic approach. American Journal of Roentgenology. 2021, 217, 584–586. [Google Scholar] [CrossRef]
- Fortin, J.; Leblanc, M.; Elgbeili, G.; Cordova, MJ.; Marin, MF.; Brunet, A. The mental health impacts of receiving a breast cancer diagnosis: A meta-analysis. British Journal of Cancer. 2021, 125, 1582–1592. [Google Scholar] [CrossRef]
- Ilkhomovna, KD. Manifestations of post-mastectomy syndrome, pathology of the brachial neurovascular bundle in clinical manifestations. Innovative Society: Problems, Analysis and Development Prospects (Spain).
- Harada, TL.; Uematsu, T.; Nakashima, K.; Kawabata, T.; Nishimura, S.; Takahashi, K.; Sugino, T. Evaluation of breast edema findings at T2-weighted breast MRI is useful for diagnosing occult inflammatory breast cancer and can predict prognosis after neoadjuvant chemotherapy. Radiology. 2021, 299, 53–62. [Google Scholar] [CrossRef]
- Toledo, G.; Ochoa, CY.; Farias, AJ. Religion and spirituality: their role in the psychosocial adjustment to breast cancer and subsequent symptom management of adjuvant endocrine therapy. Supportive Care in Cancer. 2021, 29, 3017–3024. [Google Scholar] [CrossRef] [PubMed]
- Shetty, MK. Imaging of the Symptomatic Breast. In Breast & Gynecological Diseases: Role of Imaging in the Management. 2021, 27-79.
- Barba, D.; León-Sosa, A.; Lugo, P.; Suquillo, D.; Torres, F.; Surre, F.; Caicedo, A. Breast cancer, screening and diagnostic tools: All you need to know. Critical reviews in oncology/hematology. 2021, 157, 103174. [Google Scholar] [CrossRef] [PubMed]
- Seif Abd Elalem, SG.; Kamel, HH.; Abd Elrahim, AH.; Osman, HA. Early Symptoms of Breast Cancer among Postmenopausal Women In El–Minia Oncology Center. Minia Scientific Nursing Journal. 2023, 14, 8–20. [Google Scholar] [CrossRef]
- Cudjoe, D. Facilitators to Earlier Presentation among Women Diagnosed with Early Stage Breast Cancer Disease; a Systematic Narrative Review of Literature. 2024.
- Shaikh, K.; Krishnan, S.; Thanki, R.; Shaikh, K.; Krishnan, S.; Thanki, R. Types, diagnosis, and treatment of breast cancer. Artificial intelligence in breast cancer early detection and diagnosis. 2021, 21–35. [Google Scholar]
- Fumagalli, C.; Barberis, M. Breast cancer heterogeneity. Diagnostics. 2021, 11, 1555. [Google Scholar] [CrossRef]
- Guo, L.; Kong, D.; Liu, J.; Zhan, L.; Luo, L.; Zheng, W.; Sun, S. Breast cancer heterogeneity and its implication in personalized precision therapy. Experimental hematology & oncology. 2023, 12, 3. [Google Scholar]
- Gutierrez, C.; Owens, A.; Medeiros, L.; Dabydeen, D.; Sritharan, N.; Phatak, P.; Kandlikar, SG. Breast cancer detection using enhanced IRI-numerical engine and inverse heat transfer modeling: model description and clinical validation. Scientific Reports. 2024, 14, 3316. [Google Scholar] [CrossRef]
- Tu, N.; Henderson, M.; Sundararajan, M.; Salas, M. Discrepancies in ICD-9/ICD-10-based codes used to identify three common diseases in cancer patients in real-world settings and their implications for disease classification in breast cancer patients and patients without cancer: a literature review and descriptive study. Frontiers in Oncology. 2023, 13, 1016389. [Google Scholar]
- Hsu, PY. Liou, CF. Impact of patient resourcefulness on cancer patients’ pain management and medical opioid use: A cross-sectional study. European Journal of Oncology Nursing. 2025, 74, 102771. [Google Scholar] [CrossRef]
- Soerjomataram, I.; Bray, F. Planning for tomorrow: global cancer incidence and the role of prevention 2020–2070. Nature reviews Clinical oncology. 2021, 18, 663–672. [Google Scholar] [CrossRef]
- Cechanovičiūtė, V.; Cechanovičienė, I. (2022). Overview of the epidemiology, risk factors, clinical features, diagnostics and prevention of breast cancer. Medicinos mokslai. Medical sciences. Kėdainiai: VšĮ" Lietuvos sveikatos mokslinių tyrimų centras".
- Zubair, M.; Wang, S.; Ali, N. Advanced approaches to breast cancer classification and diagnosis. Frontiers in Pharmacology. 2021, 2021. 11, 632079. [Google Scholar] [CrossRef]
- Stephan, P.; Stephan, T.; Kannan, R.; Abraham, A. A hybrid artificial bee colony with whale optimization algorithm for improved breast cancer diagnosis. Neural Computing and Applications. 2021, 33, 13667–13691. [Google Scholar] [CrossRef]
- Barrios, CH. Global challenges in breast cancer detection and treatment. The Breast. 2022, 62, S3–S6. [Google Scholar] [CrossRef] [PubMed]
- Xiong, W.; Huang, M.; Leung, XY.; Li, Y. The healing impact of travel on the mental health of breast cancer patients. Tourism Management. 2025, 106, 104997. [Google Scholar] [CrossRef]
- Tsai, W.; Wang, JHY. Fatalism and psychological distress among Chinese American Breast Cancer Survivors: mediating role of perceived self-control and fear of cancer recurrence. International journal of behavioral medicine. 2023, 30, 705–713. [Google Scholar] [CrossRef]
- Park, JH.; Jung, YS.; Kim, JY.; Bae, SH. Determinants of quality of life in women immediately following the completion of primary treatment of breast cancer: A cross-sectional study. PloS one. 2021, 16, e0258447. [Google Scholar] [CrossRef]
- Cannioto, RA.; Hutson, A.; Dighe, S.; McCann, W.; McCann, SE.; Zirpoli, GR.; Ambrosone, CB. Physical activity before, during, and after chemotherapy for high-risk breast cancer: relationships with survival. JNCI: Journal of the National Cancer Institute. 2021, 113, 54–63. [Google Scholar] [CrossRef]
- Saleem, I.; Said, MS.; Islam, M.; Nadeem, H.; Khan, AH.; Hashmi, AM. Clinical evaluation of patients suffering from breast cancer and determination of evolving treatment therapies and better strategies related to breast cancer. International Journal of Natural Medicine and Health Sciences. 2023, 2, 17–24. [Google Scholar]
- Emery, J.; Butow, P.; Lai-Kwon, J.; Nekhlyudov, L.; Rynderman, M.; Jefford, M. Management of common clinical problems experienced by survivors of cancer. The Lancet. 2022, 399, 1537–1550. [Google Scholar] [CrossRef]
- DiCaprio, MR.; Murtaza, H.; Palmer, B.; Evangelist, M. Narrative review of the epidemiology, economic burden, and societal impact of metastatic bone disease. Annals of Joint. 2022, 7. [Google Scholar] [CrossRef]
- Bergerot, C.; Bergerot, PG.; Maués, J.; Segarra-Vazquez, B.; Mano, MS.; Tarantino, P. Is cancer back?—psychological issues faced by survivors of breast cancer. Annals of Palliative Medicine. 2024, 13, 1229234–1221234. [Google Scholar] [CrossRef] [PubMed]
- Inam, F.; Bergin, RJ.; Mizrahi, D.; Dunstan, DW.; Moore, M.; Maxwell-Davis, N.; Swain, CT. Diverse strategies are needed to support physical activity engagement in women who have had breast cancer. Supportive Care in Cancer. 2023, 31, 648. [Google Scholar] [CrossRef] [PubMed]
- Natalucci, V.; Villarini, M.; Emili, R.; Acito, M.; Vallorani, L.; Barbieri, E.; Villarini, A. Special attention to physical activity in breast cancer patients during the first wave of COVID-19 pandemic in Italy: the DianaWeb cohort. Journal of personalized medicine. 2021, 11, 381. [Google Scholar] [CrossRef] [PubMed]
- Magno, S.; Rossi, MM.; Filippone, A.; Rossi, C.; Guarino, D.; Maggiore, C.; Masetti, R. Screening for Physical Activity Levels in Non-Metastatic Breast Cancer Patients Undergoing Surgery: An Observational Study. Integrative Cancer Therapies. 2022, 21, 15347354221140327. [Google Scholar] [CrossRef]
- Rock, CL.; Thomson, CA.; Sullivan, KR.; Howe, CL.; Kushi, LH.; Caan, BJ.; McCullough, ML. American Cancer Society nutrition and physical activity guideline for cancer survivors. CA: a cancer journal for clinicians. 2022, 72, 230–262. [Google Scholar] [CrossRef]
- Albini, A.; La Vecchia, C.; Magnoni, F.; Garrone, O.; Morelli, D.; Janssens, JP.; Corso, G. Physical activity and exercise health benefits: cancer prevention, interception, and survival. European Journal of Cancer Prevention. 2025, 34, 24–39. [Google Scholar] [CrossRef]
- Jacquinot, Q.; Meneveau, N.; Falcoz, A.; Bouhaddi, M.; Roux, P.; Degano, B.; Mougin, F. Cardiotoxicity is mitigated after a supervised exercise program in HER2-positive breast cancer undergoing adjuvant trastuzumab. Frontiers in Cardiovascular Medicine. 2022, 9, 1000846. [Google Scholar] [CrossRef]
- Brown, LJ.; Meredith, T.; Yu, J.; Patel, A.; Neal, B.; Arnott, C.; Lim, E. Heart failure therapies for the prevention of HER2-monoclonal antibody-mediated cardiotoxicity: a systematic review and meta-analysis of randomized trials. Cancers. 2021, 13, 5527. [Google Scholar] [CrossRef]
- Travers, G.; Kippelen, P.; Trangmar, SJ.; González-Alonso, J. Physiological function during exercise and environmental stress in humans—an integrative view of body systems and homeostasis. Cells. 2022, 11, 383. [Google Scholar] [CrossRef]
- Qiu, Y.; Fernández-García, B.; Lehmann, HI.; Li, G.; Kroemer, G.; López-Otín, C.; Xiao, J. Exercise sustains the hallmarks of health. Journal of sport and health science. 2023, 12, 8–35. [Google Scholar] [CrossRef]
- Zagalaz-Anula, N.; Mora-Rubio, MJ.; Obrero-Gaitán, E.; Del-Pino-Casado, R. Recreational physical activity reduces breast cancer recurrence in female survivors of breast cancer: A meta-analysis. European Journal of Oncology Nursing. 2022, 59, 102162. [Google Scholar] [CrossRef] [PubMed]
- Zeng, H.; Yang, Z.; Li, J.; Wen, Y.; Wu, Z.; Zheng, Y.; He, J. Associations between female lung cancer risk and sex steroid hormones: a systematic review and meta-analysis of the worldwide epidemiological evidence on endogenous and exogenous sex steroid hormones. BMC cancer. 2021, 21, 690. [Google Scholar] [CrossRef] [PubMed]
- Mohanty, SS.; Mohanty, PK. Obesity as potential breast cancer risk factor for postmenopausal women. Genes & diseases. 2021, 8, 117–123. [Google Scholar]
- Steiner, BM.; Berry, DC. The regulation of adipose tissue health by estrogens. Frontiers in Endocrinology. 2022, 13, 889923. [Google Scholar] [CrossRef]
- Hetemäki, N.; Robciuc, A.; Vihma, V.; Haanpää, M.; Hämäläinen, E.; Tikkanen, MJ.; Savolainen-Peltonen, H. Adipose tissue sex steroids in postmenopausal women with and without menopausal hormone therapy. The Journal of Clinical Endocrinology & Metabolism.
- Iwase, T.; Wang, X.; Shrimanker, TV.; Kolonin, MG.; Ueno, NT. Body composition and breast cancer risk and treatment: mechanisms and impact. Breast cancer research and treatment. 2021, 186, 273–283. [Google Scholar] [CrossRef]
- Bleach, R.; Sherlock, M.; O’Reilly, MW.; McIlroy, M. Growth hormone/insulin growth factor axis in sex steroid associated disorders and related cancers. Frontiers in Cell and Developmental Biology. 2021, 9, 630503. [Google Scholar] [CrossRef]
- Merritt, MA.; Strickler, HD.; Hutson, AD.; Einstein, MH.; Rohan, TE.; Xue, X.; Gunter, MJ. Sex hormones, insulin, and insulin-like growth factors in recurrence of high-stage endometrial cancer. Cancer Epidemiology, Biomarkers & Prevention. 2021, 30, 719–726. [Google Scholar]
- Gharahdaghi, N.; Phillips, BE.; Szewczyk, NJ.; Smith, K.; Wilkinson, DJ.; Atherton, PJ. Links between testosterone, oestrogen, and the growth hormone/insulin-like growth factor axis and resistance exercise muscle adaptations. Frontiers in physiology. 2021, 11, 621226. [Google Scholar] [CrossRef]
- D’alonzo, NJ.; Qiu, L.; Sears, DD.; Chinchilli, V.; Brown, JC.; Sarwer, DB.; Sturgeon, KM. WISER survivor trial: combined effect of exercise and weight loss interventions on insulin and insulin resistance in breast cancer survivors. Nutrients. 2021, 13, 3108. [Google Scholar] [CrossRef]
- Dieli-Conwright, CM.; Harrigan, M.; Cartmel, B.; Chagpar, A.; Bai, Y.; Li, FY.; Irwin, ML. Impact of a randomized weight loss trial on breast tissue markers in breast cancer survivors. NPJ Breast Cancer. 2022, 8, 29. [Google Scholar] [CrossRef]
- Sturgeon, K. M.; Brown, JC.; Sears, DD.; Sarwer, DB.; Schmitz, KH. WISER survivor trial: combined effect of exercise and weight loss interventions on inflammation in breast cancer survivors. Medicine and science in sports and exercise. 2023, 55, 209. [Google Scholar] [CrossRef] [PubMed]
- Harvie, M.; Pegington, M.; Howell, SJ.; Bundred, N.; Foden, P.; Adams, J.; Howell, A. Randomised controlled trial of intermittent vs continuous energy restriction during chemotherapy for early breast cancer. British Journal of Cancer. 2022, 126, 1157–1167. [Google Scholar] [CrossRef] [PubMed]
- Lin, D.; Sturgeon, KM.; Gordon, BR.; Brown, JC.; Sears, DD.; Sarwer, DB.; Schmitz, KH. WISER survivor trial: combined effect of exercise and weight loss interventions on adiponectin and leptin levels in breast cancer survivors with overweight or obesity. Nutrients. 2023, 15, 3453. [Google Scholar] [CrossRef]
- Babaei, P.; Hoseini, R. Exercise training modulates adipokine dysregulations in metabolic syndrome. Sports Medicine and Health Science. 2022, 4, 18–28. [Google Scholar] [CrossRef]
- Mendez-Gutierrez, A.; Aguilera, CM.; Osuna-Prieto, FJ.; Martinez-Tellez, B.; Rico Prados, MC.; Acosta, FM.; Sanchez-Delgado, G. Exercise-induced changes on exerkines that might influence brown adipose tissue metabolism in young sedentary adults. European Journal of Sport Science. 2023, 23, 625–636. [Google Scholar] [CrossRef]
- Anderson, A. S.; Renehan, AG.; Saxton, JM.; Bell, J.; Cade, J.; Cross, AJ.; Martin, RM. Cancer prevention through weight control—where are we in 2020? British Journal of Cancer. 2021, 124, 1049–1056. [Google Scholar] [CrossRef]
- Sadier, N. S.; El Hajjar, F.; Al Sabouri, AAK. ; Abou-Abbas, L.; Siomava, N.; Almutary, AG.; Tambuwala, MM. Irisin: An unveiled bridge between physical exercise and a healthy brain. Life Sciences. 2024, 339, 122393. [Google Scholar] [CrossRef]
- Okechukwu, CE.; Okechukwu, CE.; Agag, A.; Naushad, N.; Abbas, S.; Deb, AA. Hypothesized biological mechanisms by which exercise-induced irisin mitigates tumor proliferation and improves cancer treatment outcomes. MGM Journal of Medical Sciences. 2021, 8, 452–458. [Google Scholar] [CrossRef]
- Waseem, R.; Shamsi, A.; Mohammad, T.; Hassan, MI.; Kazim, SN.; Chaudhary, AA.; Islam, A. FNDC5/irisin: physiology and pathophysiology. Molecules. 2022, 27, 1118. [Google Scholar] [CrossRef]
- Thomas, R.; Kenfield, SA.; Yanagisawa, Y.; Newton, RU. Why exercise has a crucial role in cancer prevention, risk reduction and improved outcomes. British medical bulletin. 2021, 139, 100–119. [Google Scholar] [CrossRef]
- You, M.; Xie, Z.; Zhang, N.; Zhang, Y.; Xiao, D.; Liu, S.; Tao, Y. Signaling pathways in cancer metabolism: mechanisms and therapeutic targets. Signal Transduction and Targeted Therapy. 2023, 8, 196. [Google Scholar] [CrossRef] [PubMed]
- Akbar, N.; Khan, NA.; Muhammad, JS. Siddiqui, R. The role of gut microbiome in cancer genesis and cancer prevention. Health Sciences Review. 2022, 2, 100010. [Google Scholar] [CrossRef]
- Chen, L.; Zhernakova, DV.; Kurilshikov, A.; Andreu-Sánchez, S.; Wang, D.; Augustijn, HE.; Fu, J. Influence of the microbiome, diet and genetics on inter-individual variation in the human plasma metabolome. Nature medicine. 2022, 28, 2333–2343. [Google Scholar] [CrossRef] [PubMed]
- Jelic, MD.; Mandic, AD.; Maricic, SM.; Srdjenovic, BU. Oxidative stress and its role in cancer. Journal of cancer research and therapeutics. 2021, 2021. 17, 22–28. [Google Scholar] [CrossRef]
- Sahoo, BM.; Banik, BK.; Borah, P.; Jain, A. Reactive oxygen species (ROS): key components in cancer therapies. Anti-Cancer Agents in Medicinal Chemistry (Formerly Current Medicinal Chemistry-Anti-Cancer Agents). 2022, 22, 215–222. [Google Scholar] [CrossRef]
- Raza, A.; Salehi, H.; Rahman, MA.; Zahid, Z.; Madadkar Haghjou, M.; Najafi-Kakavand, S.; .Zhuang, W. Plant hormones and neurotransmitter interactions mediate antioxidant defenses under induced oxidative stress in plants. Frontiers in Plant Science. 2022, 13, 961872. [Google Scholar] [CrossRef]
- Oke, OE.; Akosile, OA.; Oni, AI.; Opowoye, IO.; Ishola, C. A.; Adebiyi, JO.; Abioja, MO. Oxidative stress in poultry production. Poultry Science. 2024, 104003. [Google Scholar] [CrossRef]
- Kaur, H.; Hussain, SJ.; Kaur, G.; Poor, P.; Alamri, S.; Siddiqui, MH.; Khan, MIR. Salicylic acid improves nitrogen fixation, growth, yield and antioxidant defence mechanisms in chickpea genotypes under salt stress. Journal of Plant Growth Regulation. 2022, 41, 2034–2047. [Google Scholar] [CrossRef]
- Li, S.; Lei, Z.; Sun, T. The role of microRNAs in neurodegenerative diseases: a review. Cell Biology and Toxicology. 2023, 39, 53–83. [Google Scholar] [CrossRef]
- Alwani, A.; Andreasik, A.; Szatanek, R.; Siedlar, M.; Baj-Krzyworzeka, M. The role of miRNA in regulating the fate of monocytes in health and cancer. Biomolecules. 2022, 12, 100. [Google Scholar] [CrossRef]
- Dos Santos, JAC. ; Veras, ASC.; Batista, VRG.; Tavares, MEA.; Correia, RR.; Suggett, CB.; Teixeira, GR. Physical exercise and the functions of microRNAs. Life sciences. 2022, 304, 120723. [Google Scholar]
- Khoury, R.; Nagy, C. Running from stress: a perspective on the potential benefits of exercise-induced small extracellular vesicles for individuals with major depressive disorder. Frontiers in Molecular Biosciences. 2023, 10, 1154872. [Google Scholar] [CrossRef] [PubMed]
- Saeidi, A.; Tayebi, SM.; To-Aj, O.; Karimi, N.; Kamankesh, S.; Niazi, S.; Zouhal, H. Physical Activity, Natural Products, and Minerals in the SARS-CoV-2 Pandemic: An Update. Annals of applied sport science. 2021, 9. [Google Scholar] [CrossRef]
- Aya, V.; Flórez, A.; Perez, L.; Ramírez, JD. Association between physical activity and changes in intestinal microbiota composition: A systematic review. PLoS One. 2021, 16, e0247039. [Google Scholar] [CrossRef]
- Zhou, M.; Johnston, LJ.; Wu, C.; Ma, X. Gut microbiota and its metabolites: Bridge of dietary nutrients and obesity-related diseases. Critical reviews in food science and nutrition. 2023, 63, 3236–3253. [Google Scholar] [CrossRef]
- Rahman, MM.; Islam, MR.; Shohag, S.; Ahasan, MT.; Sarkar, N.; Khan, H.; Rauf, A. Microbiome in cancer: Role in carcinogenesis and impact in therapeutic strategies. Biomedicine & Pharmacotherapy. 2022, 149, 112898. [Google Scholar]
- Molina-Molina, E.; Furtado, GE.; Jones, JG.; Portincasa, P.; Vieira-Pedrosa, A.; Teixeira, AM.; Sardão, VA. The advantages of physical exercise as a preventive strategy against NAFLD in postmenopausal women. European Journal of Clinical Investigation. 2022, 52, e13731. [Google Scholar] [CrossRef]
- Kutac, P.; Buzga, M.; Elavsky, S.; Bunc, V.; Jandacka, D.; Krajcigr, M. The Effect of Regular Physical Activity on Muscle and Adipose Tissue in Premenopausal Women. Applied Sciences. 2021, 11, 8655. [Google Scholar] [CrossRef]
- Fenech, MF.; Bull, CF.; Van Klinken, BJW. Protective effects of micronutrient supplements, phytochemicals and phytochemical-rich beverages and foods against DNA damage in humans: a systematic review of randomized controlled trials and prospective studies. Advances in Nutrition. 2023, 14, 1337–1358. [Google Scholar] [CrossRef]
- Pistelli, M.; Natalucci, V.; Scortichini, L.; Agostinelli, V.; Lenci, E.; Crocetti, S.; Berardi, R. The impact of lifestyle interventions in high-risk early breast cancer patients: a modeling approach from a single institution experience. Cancers. 2021, 13, 5539. [Google Scholar] [CrossRef]
- Dimauro, I.; Grazioli, E.; Antinozzi, C.; Duranti, G.; Arminio, A.; Mancini, A.; Di Luigi, L. Estrogen-receptor-positive breast cancer in postmenopausal women: the role of body composition and physical exercise. International journal of environmental research and public health. 2021, 18, 9834. [Google Scholar] [CrossRef] [PubMed]
- Obeagu, EI.; Obeagu, GU. Breastfeeding’s protective role in alleviating breast cancer burden: A comprehensive review. Annals of Medicine and Surgery. 2024, 86, 2805–2811. [Google Scholar] [CrossRef] [PubMed]
- García-Chico, C.; López-Ortiz, S.; Peñín-Grandes, S.; Pinto-Fraga, J.; Valenzuela, PL.; Emanuele, E.; Santos-Lozano, A. Physical exercise and the hallmarks of breast cancer: a narrative review. Cancers. 2023, 15, 324. [Google Scholar] [CrossRef] [PubMed]
- Negrini, KA.; Lin, D.; Shah, D.; Wu, H.; Wehrung, KM.; Thompson, HJ.; Sturgeon, KM. Role of Oncostatin M in Exercise-Induced Breast Cancer Prevention. Cancers. 2024, 16, 2716. [Google Scholar] [CrossRef]
- Romero-Parra, N.; Cupeiro, R.; Alfaro-Magallanes, VM.; Rael, B.; Rubio-Arias, JÁ. ; Peinado, AB.; IronFEMME Study Group. Exercise-induced muscle damage during the menstrual cycle: a systematic review and meta-analysis. The Journal of Strength & Conditioning Research. 2021, 35, 549–561. [Google Scholar]
- Dixon-Suen, SC.; Lewis, SJ.; Martin, RM.; English, DR.; Boyle, T.; Giles, GG.; Zheng, W. Physical activity, sedentary time and breast cancer risk: a Mendelian randomisation study. British journal of sports medicine. 2022, 56, 1157–1170. [Google Scholar] [CrossRef]
- Darling, AM.; Wang, D.; Perumal, N.; Liu, E.; Wang, M.; Ahmed, T.; GWG Pooling Project Consortium. Risk factors for inadequate and excessive gestational weight gain in 25 low-and middle-income countries: An individual-level participant meta-analysis. PLoS medicine. 2023, 20, e1004236. [Google Scholar] [CrossRef]
- Tennfjord, MK.; Gabrielsen, R.; Tellum, T. Effect of physical activity and exercise on endometriosis-associated symptoms: a systematic review. BMC women's health. 2021, 21, 1–10. [Google Scholar] [CrossRef]
- Butt, MS.; Saleem, J.; Zakar, R.; Aiman, S.; Khan, MZ.; Fischer, F. Benefits of physical activity on reproductive health functions among polycystic ovarian syndrome women: a systematic review. BMC Public Health. 2023, 23, 882. [Google Scholar] [CrossRef]
- Wang, Q.; Zhou, W. Roles and molecular mechanisms of physical exercise in cancer prevention and treatment. Journal of sport and health science. 2021, 10, 201–210. [Google Scholar] [CrossRef]
Figure 2.
Embryonic and adult development of mammary gland.
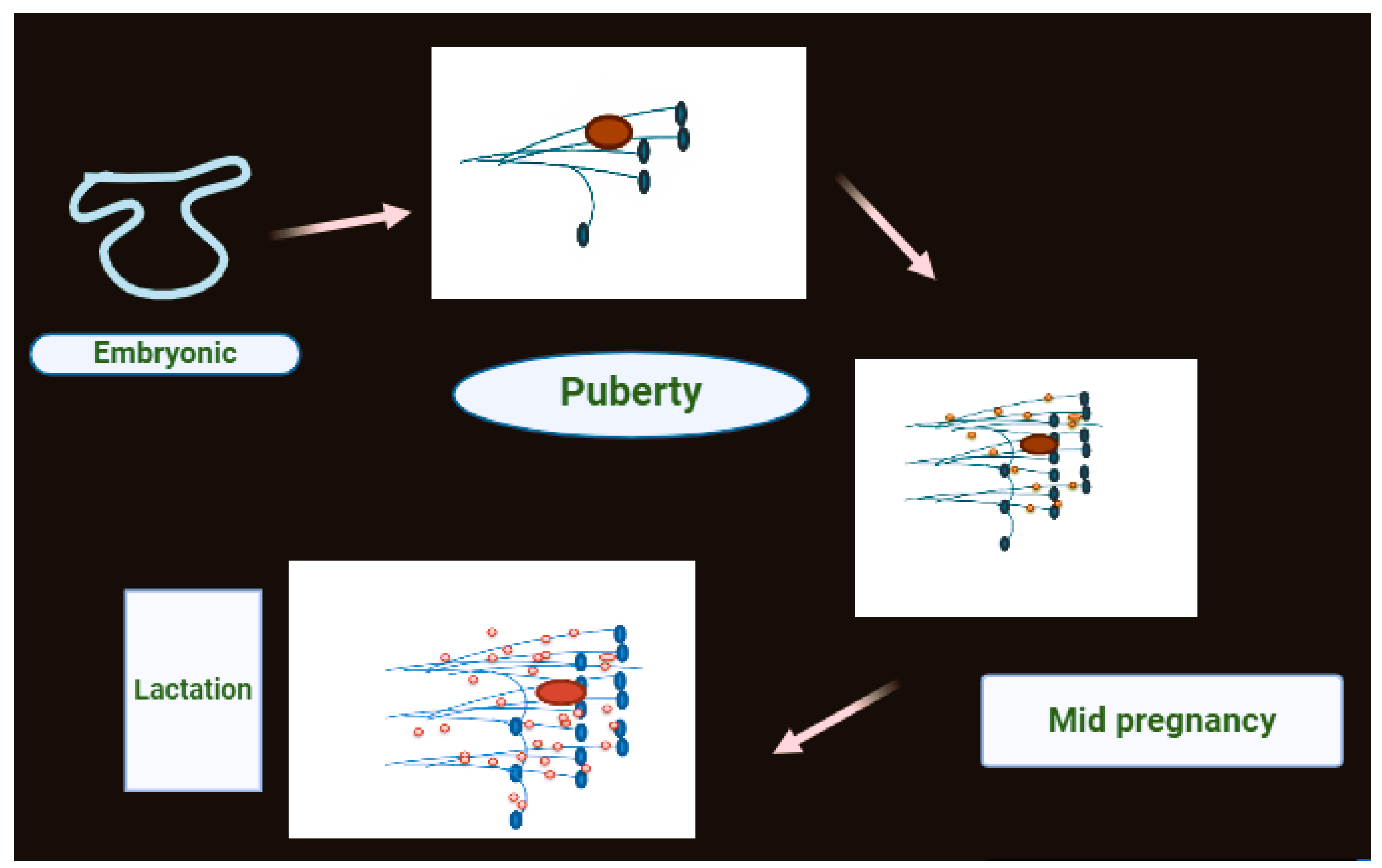
Figure 3.
Breast cancer sub-types and relative prevalence.
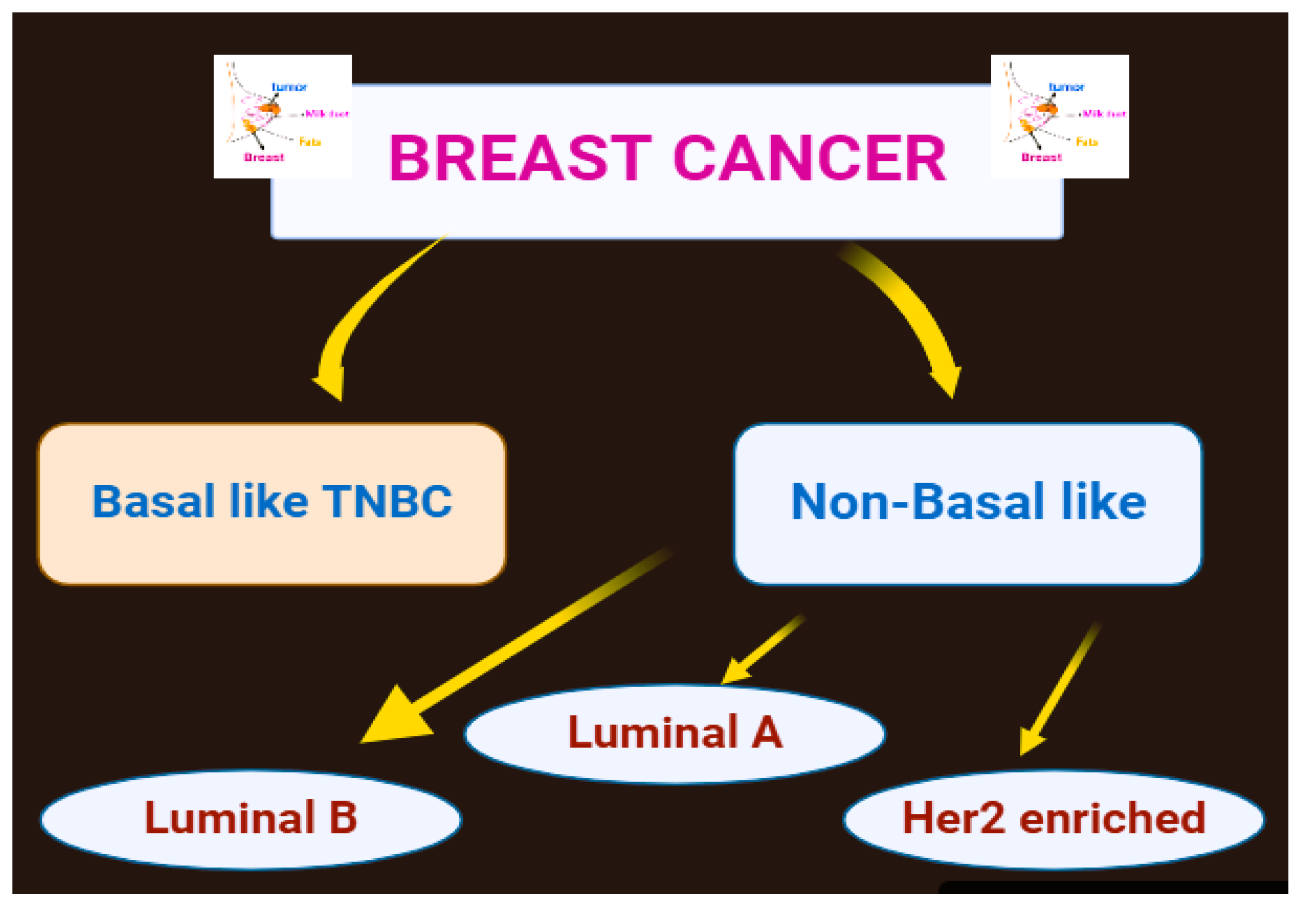
Figure 4.
Physical activity affects the systemic factors linked with the outcomes of breast cancer.
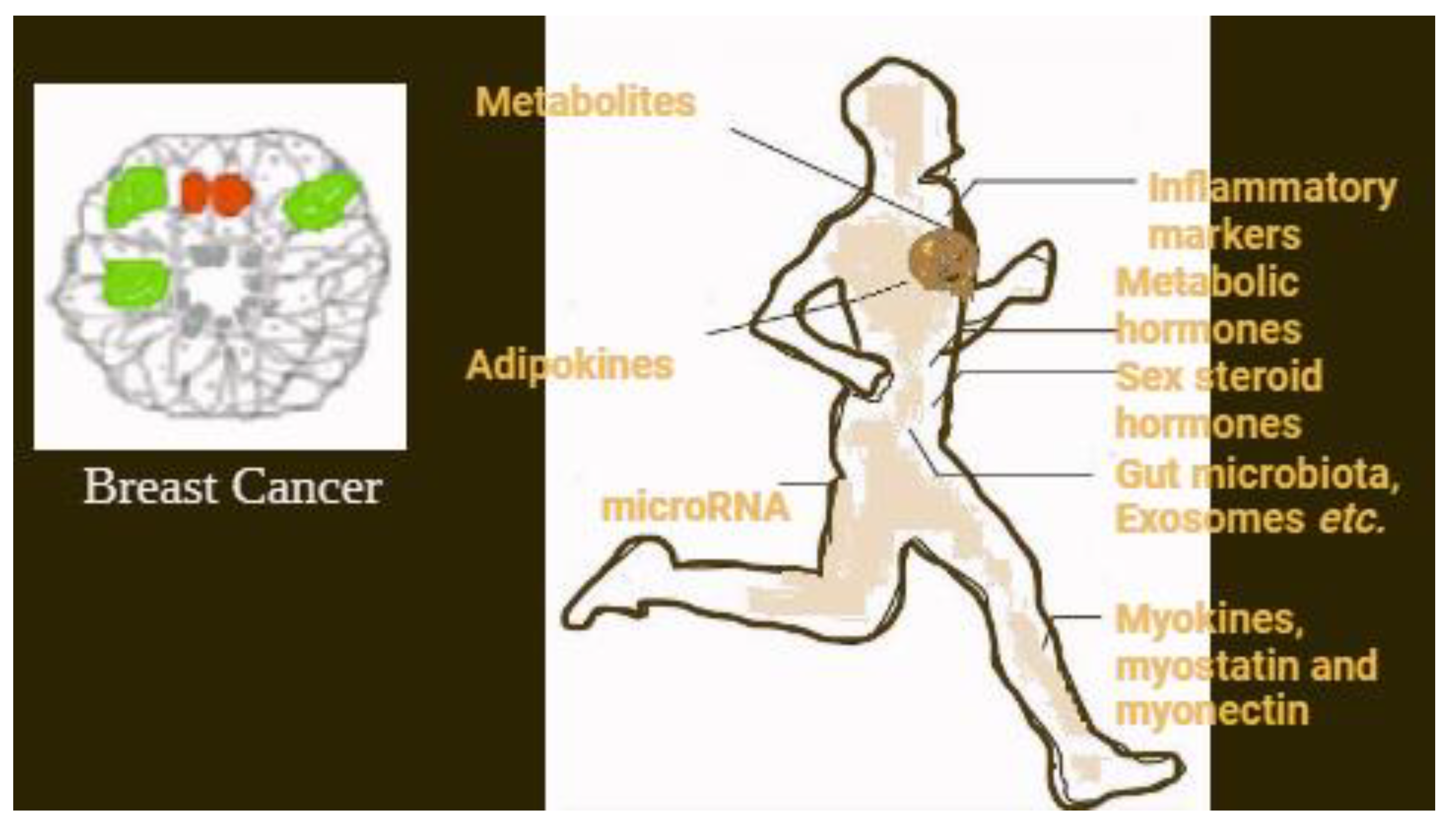

Table 1.
Approaches to treat breast cancer.
| Approaches | Procedure |
|---|---|
| Surgical Resection | At the outset of breast cancer, surgical removal of the tumor is possible. The earlier the tumor is removed, the higher the survival rate. |
| Radiotherapy | High-energy radiation are used to destroy cancer cells, which is often used to get rid of leftover cancer tissues after surgery. |
| Adjuvant Chemotherapy | Chemotherapy is done after surgery to target any remaining cancer cells and prevent the cancer from coming back. |
| Neoadjuvant Chemotherapy | Chemotherapy is administered before surgery to shrink the tumor so that it can be removed during surgery. |
| Hormonal Therapies | In cancer treatment, they are used as hormone receptor blockers to help block hormones (such as estrogen) that promote tumor growth. |
| Monoclonal Antibodies | Using antibodies for targeted therapy, like trastuzumab (Herceptin), is especially effective against HER2 positive breast cancer. |
| Immunotherapy | This viewpoint makes a difference boost the body's resistant framework to battle cancer and appears guarantee in forceful sorts of breast cancer. |
| Small Molecular Inhibitors | They target particular molecular pathways included in cancer cell development and survival, giving more successful and less poisonous medications than chemotherapy. |
| Physical activity | There are many theories that explain how the body reduces the risk of cancer. This includes a lower risk for estrogen and androgens. There are also some factors related to insulin, adipokines, etc. Similar mechanisms might work in the survival of breast cancer. This will overall reduce mortality and recurrence related to the disease. |
Table 2.
Mediators effected by physical activity in breast cancer.
| Sex steroid hormones | Estrogen, Testosterone and androgens |
| Metabolic hormones | Insulin, Insulin-like growth factor, Leptin, |
| Inflammatory markers | C-reactive proteins, Tumor necrosis factor, Inter leukins |
| Stress hormones | Cortisol, Epinephrine, Nor Epinephrine |
| Adipokines | Resistin, Adiponectin |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



