Submitted:
07 February 2025
Posted:
08 February 2025
You are already at the latest version
Abstract
Background/ Objectives
Brachymetatarsia is a rare congenital anomaly characterised by the shortening of one or more metatarsals, which can cause functional problems, pain and aesthetic difficulties. We present the case of a 17-year-old female patient with brachymetatatarsia of the 3rd and 4th radii of the right foot, refractory to conservative treatment and with persistent pain during standing. The aim of this study is to describe an innovative surgical approach using an autologous calcaneal graft for the treatment of this pathology.
Methods
After evaluating all available surgical options, it was decided to perform an au-tologous calcaneal implant at the base of metatarsals 3 and 4 to increase their length. In addition, radii 2 and 5 were shortened to restore a physiological metatarsal parabola and definitively eliminate metatarsalgia.
Results
The procedure achieved complete correction of the metatarsal parabola. The patient experienced complete resolution of metatarsal pain and satisfactory functional recovery. The autologous calcaneal graft provided adequate support due to its cortico-cancellous composition, high osteogenic capacity and low antigenicity, making it an optimal choice in foot and ankle surgery.
Conclusions
Autologous calcaneal grafting has proven to be an effective and safe surgical alternative for the correction of brachymetatarsia. Its use makes it possible not only to increase the length of the affected metatarsals but also to de-finitively resolve metatarsalgia, improving the quality of life of patients with this pathology. This case highlights the usefulness of autologous grafts in reconstructive procedures of the foot, due to their structural and biological advantages.
Keywords:
Brachymetatarsia
; Metatarsal lengthening
; Chronic metatarsalgia
; Structural bone graft
; Reconstructive foot surgery
; Biomechanical alterations
; Postoperative functional outcomes
1. Introduction
Brachymetatarsia is a congenital deformity characterised by abnormal shortening of one or more metatarsals due to premature closure of the growth plate [1]. This condition primarily affects the fourth metatarsal, followed by the first, with a marked predominance in females (14.8:1) and a bilateral prevalence in approximately 25.8 % of cases [2,3]. Although some patients remain asymptomatic, the deformity can cause transfer pain, metatarsalgia, calluses, soft tissue contractures and cosmetic concerns, especially during adolescence [4,5].
The diagnosis of brachymetatarsia is based on weight-bearing radiographs, where the affected metatarsal is found to be more than 5 mm proximal to the normal metatarsal parabola described by Lelievre [6]. In addition, it may be associated with secondary deformities such as claw or hammertoes, and, in severe cases, with significant functional impairment of the forefoot [7,8].
Conservative management, including the use of orthoses and specialised footwear, can be helpful in relieving pain and improving forefoot pressure distribution. However, these strategies do not correct the underlying deformity, and in symptomatic cases or those with significant cosmetic implications, surgery is used to restore metatarsal length and foot function [9,10].
Among the surgical options, bone lengthening can be performed using two main approaches: acute single-stage lengthening and gradual distraction. The former, which includes techniques such as the interposition of autologous or allogeneic bone grafts, is a faster option and has lower complication rates but is limited in the amount of lengthening that can be achieved [11,12]. On the other hand, gradual distraction allows greater bone elongation but requires prolonged use of external fixators and is associated with a higher risk of complications, such as infections, fractures and joint stiffness [13,14]. Bone grafts, particularly autologous bone grafts, have been shown to be effective in one-stage procedures for moderate deformities, providing stability and good cosmetic and functional results [15,16].
Despite advances in surgical techniques, there is no definitive consensus on the best option for treating brachymetatarsia. Treatment selection should be based on patient-specific characteristics, such as desired length, age, aesthetic expectations and risk of complications [17]. In this context, the present manuscript reports a clinical case of brachymetatarsia treated by single-stage lengthening with autologous bone grafting, highlighting the clinical and functional results obtained.
2. Case Report
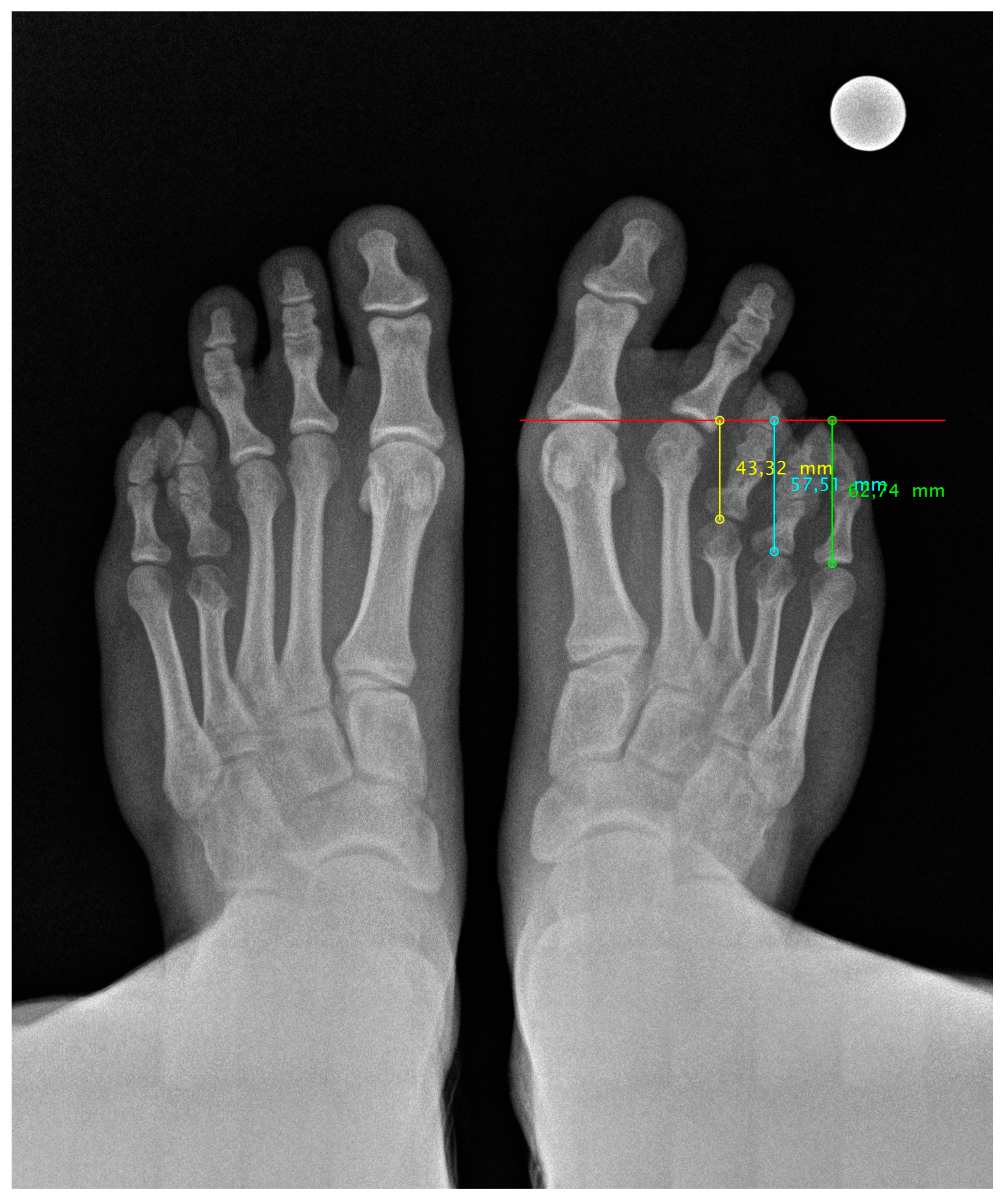
We present the case of a 17-year-old female patient who presented herself for consultation with severe pain in the central metatarsals of her right foot. This is a young patient with a medical history without systemic, cardiac, neurological or rheumatological diseases.
Clinical examination revealed a valgus foot with hyperkeratosis under the 3rd and 4th metatarsal heads. The patient has been wearing unloading plantar orthoses for 8 years. Conservative treatment has not achieved its objective and the patient is living with continuous pain EVA 8 caused by metatarsalgia at the age of 17 years.
Finally, the radiological study confirms a diaphyseal shortening of the 3rd and 4th radius of the right foot. Her left foot also shows diaphyseal shortening only of the 4th radius with no symptoms.
Figure 1.
Pre-surgical radiological image of both feet under load.
2.1. Surgical Procedure
The patient receives a spinal block with 0.75% bupivacaine, along with sedation administered by the anesthesiology team. A tourniquet is placed 10 cm below the fibular head with a pressure of 250 mm Hg.
First, an oblique incision is made on the lateral aspect of the calcaneus for the extraction of a 1.8cm x 1.1cm bone graft.
After obtaining and preparing the calcaneal bone graft, we made a longitudinal incision in the 3rd and 4th intermetatarsal space to perform a base osteotomy. Once the osteotomy had been performed, we placed calcaneal bone autograft at the base of the 3rd and 4th metatarsal.
Subsequently, analysing the length achieved in the 3rd and 4th metatarsal, it was decided to perform a distal shortening osteotomy in the 2nd and 5th metatarsal.
The fragments are fixed with four 1.6 mm K-wires placed from the distal phalanx to the base of the lesser radii.
Sutures were performed using 2/0 synthetic absorbable sutures for the closure of the capsules of the first MTP and lesser rays, 3/0 sutures for the closure of the fascia and 4/0 BiosynTM monofilament sutures for continuous skin closure in all incisions.
2.2. Postsurgical Procedure and Evolution
The patient underwent post-surgical immobilisation with a plaster cast. It was at week 8, after radiographic review, when the K-wire fixation of the 2nd, 4th and 5th radii was removed. At week 10, K-wire fixation of the 3rd radius was removed and partial loading began with the use of a Walker boot for 4 weeks.
After 16 weeks, the patient had no pain or limitations and started to wear physiological footwear. At 6 months, she began to practice running and the metatarsal adequately accepted the ground reaction force.
3. Results
Post-surgical radiological images show a good position and alignment of the metatarsal parabola. We can observe the favourable evolution of the bone consolidation of the shortening osteotomies and the correct integration of the bone autoimplant. Also visible is the bone defect at the level of the lateral aspect of the calcaneus after removal of the autogenous graft. This will be filled with new bone over the next few months until a calcaneus with normal morphology is achieved.
Anteroposterior and lateral radiographs were taken at 6, 12, 18 and 24 months post-surgery (Figure 2). The radiological study shows correct bone consolidation, good alignment of the metatarsal parabola, as well as the remodelling process that the calcaneus is undergoing after removal of the autotransplant.
There is a significant change in the aesthetic change of the foot (Figure 3). An appreciable longitudinal difference is maintained, but accompanied by a magnificent alignment, although the aesthetic aspect has never been important, but rather the functional aspect. Our patient, after two years of follow-up, maintains a good quality of life without pain, and that is what is important.
Figure 2.
Radiological image 24 months post-surgery of both feet in loading. Improvement of the metatarsal parabola harmony can be seen.
Figure 2.
Radiological image 24 months post-surgery of both feet in loading. Improvement of the metatarsal parabola harmony can be seen.
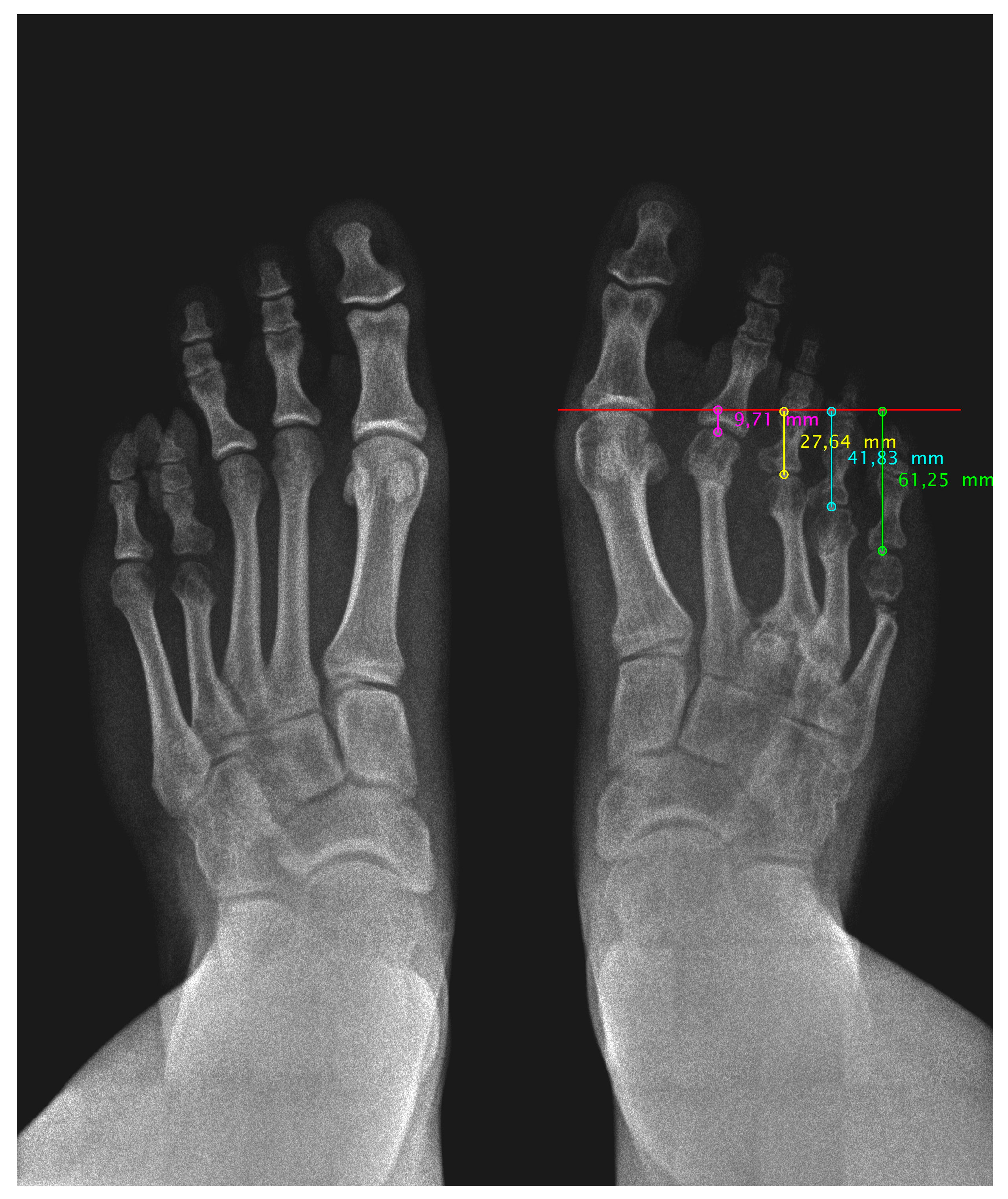
Figure 3.
Image of the patient's foot, showing before and after surgery creating digital harmony and improved load distribution.
Figure 3.
Image of the patient's foot, showing before and after surgery creating digital harmony and improved load distribution.

4. Discussion
Surgical treatment of brachymetatarsia is primarily aimed at restoring the length of the affected metatarsal to improve the function and aesthetics of the foot. The most commonly used techniques include one-stage lengthening, usually involving bone grafting, and gradual distraction by osteogenesis. Both options have advantages and limitations that have been extensively described in the literature.
4.1. One-Stage Elongation
One-stage lengthening is often performed by the interposition of autologous, allogeneic or synthetic bone grafts. This technique allows correction of moderate deformities with an average length gain of 14.4 mm [18]. However, the technique has limitations related to soft tissue tension, which restricts lengthening to less than 15 mm in most cases to avoid complications such as ischaemia or skin necrosis [19,20].
Giannini et al. achieved good results using homologous bone grafts in 41 feet, with an average gain of 13 mm and complete bone healing in all cases, with no significant complications [19]. Waizy et al. reported the use of autologous fibula grafts fixed with locking plates in eight patients, obtaining an average elongation of 9.01 mm without postoperative complications [21]. However, the use of autologous grafts is associated with donor site morbidity, whereas allogeneic grafts have lower osteogenic capacity and a higher risk of resorption [22].
4.2. Gradual Distraction
The gradual distraction technique, performed with external fixators, is an alternative that allows elongations greater than 15 mm due to its ability to lengthen both bone and soft tissues progressively. Recent studies show an average gain of 17.2 mm and an elongation rate of 37 % [23]. However, this technique is associated with a higher incidence of complications (36.5 %) compared to one-stage lengthening (21.1 %), with infections, fractures and joint subluxations being the most frequent [24,25].
The healing rate in gradual distraction (61.4 days/cm) is significantly higher than in one-stage procedures, reflecting a longer recovery time for patients [26]. In addition, the use of circular devices has demonstrated a reduction in the incidence of joint misalignments and subluxations compared with monolateral fixators, although their use remains limited [27,28,29].
4.3. Alternative and Combined Techniques
Z-osteotomy is a technique that allows lengthening without the need for bone grafting, which reduces morbidity at the donor site. However, it is limited to minor elongations and is not applicable in all cases [30]. On the other hand, some authors have combined gradual distraction with bone graft interposition to optimise results and reduce the duration of the distraction procedure, obtaining good results without significant complications [31].
4.4. Limitations
This study has several important limitations. First, most of the studies reviewed are retrospective in design and lack randomised controlled trials, which limits the robustness of the conclusions. In addition, heterogeneity in surgical techniques and functional assessment tools makes direct comparison of results difficult. Small sample sizes and limited follow-up in some studies also restrict the ability to assess long-term complications. Finally, our results are based solely on a subjective assessment proposed by the authors, which could introduce biases in the interpretation of the data.
4. Conclusions
Gradual distraction, especially when combined with techniques such as osteotomy or metatarsal reaming, appears to be the safest option for cases requiring significant lengthening, either more than 40% of the original metatarsal length or more than 15mm. This technique allows progressive control of lengthening, reduces the risk of neurovascular complications and facilitates soft tissue adaptation. In addition, the use of a K-wire after removal of the distraction device helps to stabilise the metatarsal, ensuring correct alignment.
In our case, we chose to avoid excessive lengthening and prioritised a single-stage technique, using a calcaneal allograft in combination with reduction of the adjacent metatarsals. Although this approach required additional surgical procedures, we felt that it offered our patient a more controlled postoperative period, with lower risks of infection and associated complications. Despite the need to maintain a period of unsupported immobilisation for eight weeks, the results were satisfactory in terms of function and aesthetics.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org, Supplementary file1: CARE Checklist of Information to Include When Writing a Case Report.
Author Contributions
Conceptualisation, M.O-R. and L.M.G-F.; methodology, A.F-G.; validation, M.P.C.; investigation, M.O-R. and A.F-G.; resources, L.M.G-F.; writing - original draft preparation, A.F-G and M.O-R.; writing - review and editing, L.M.G-F and A.F-G .; visualisation, A.F-G .; supervision, M.P.C and A.C.M.; project administration, L.M.G-F .; all the authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding
Institutional Review Board Statement
Ethical review and approval were waived for this study as it is a retrospective case report that did not involve experimental interventions or the collection of additional data beyond standard clinical practice. Written informed consent was obtained from the patient for the publication of this case report and accompanying images.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Data sharing is not applicable. No new data were created or analyzed in this study.
Acknowledgments
The authors thank the surgical team and the human staff of the Viamed Santa Angela de la Cruz Hospital in Seville.
Conflicts of Interest
The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript, or in the decision to publish the results.
References
- Arceri A, Mazzotti A, Zielli SO, Artioli E, Viroli G, Traversari M, et al. What's the evidence on surgical treatment for congenital brachymetatarsia: A systematic review and meta-analysis. J Orthop. 2024;49:107-16.
- Fusini F, Alessandro M, Rava A, Kristijan Z, Felli L, Colò G. Aetiology, diagnosis, and treatment of brachymetatarsia: a narrative review. Musculoskelet Surg. 2021;105:11-9.
- Woo SH, Bang CY, Ahn HC, Kim SJ, Choi JY. Anatomical reconstruction of the fourth brachymetatarsia with one-stage iliac bone and cartilage cap grafting. J Plast Reconstr Aesthet Surg. 2017;70(5):666-72. [CrossRef]
- Kim HS, Lee YS, Jung JH, Shim JS. Complications of distraction osteogenesis in brachymetatarsia: Comparison between the first and fourth brachymetatarsia. Foot Ankle Surg. 2017;25(2):113-8. [CrossRef]
- Davidson RS. Metatarsal lengthening for congenital deformities of the foot. Clin Podiatr Med Surg. 2001;18(4):685-95.
- Peña-Martínez VM, Palacios-Barajas D, Blanco-Rivera JC, Arnaud-Franco Á, Elizondo-Rodríguez JA, Acosta-Olivo C, et al. Results of external fixation and metatarsophalangeal joint fixation with K-wire in brachymetatarsia. Foot Ankle Int. 2018;39(8):942-8. [CrossRef]
- Shecaira AP, Fernandes RMP. Brachymetatarsia: one-stage versus two-stage procedures. Foot Ankle Clin. 2019;24(4):677-87.
- Lamm BM, Gourdine-Shaw MC. Problems, obstacles, and complications of metatarsal lengthening for the treatment of brachymetatarsia. Clin Podiatr Med Surg. 2010;27(4):561-82. [CrossRef]
- Giannini S, Faldini C, Pagkrati S, Luciani D, Leardini A, Marcacci M. One-stage metatarsal lengthening by allograft interposition: a novel approach for congenital brachymetatarsia. Clin Orthop Relat Res. 2010;468:1933-42. [CrossRef]
- Fuiano M, Mosca M, Caravelli S, Di Liddo M, Grassi A, Massimi S, et al. Callus distraction with external fixator for the treatment of congenital brachymetatarsia. Foot Ankle Surg. 2020;26(6):693-8. [CrossRef]
- Urano Y, Kobayashi A. Bone-lengthening for shortness of the fourth toe. J Bone Joint Surg Am. 1978;60(1):91-3. [CrossRef]
- Schimizzi A, Brage M. Brachymetatarsia. Foot Ankle Clin N Am. 2004;9(3):555-70.
- Lee KB, Park HW, Chung JY, Moon ES, Jung ST, Seon JK. Comparison of outcomes of distraction osteogenesis for first and fourth brachymetatarsia. J Bone Joint Surg Am. 2010;92(16):2709-18. [CrossRef]
- Toporowski G, Thiesen R, Gosheger G, et al. Callus distraction for brachymetatarsia: a comparison between an internal device and the external fixator. Foot Ankle Surg. 2022;28:1220-8. [CrossRef]
- Barbier D, Neretin A, Journeau P, Popkov D. Gradual metatarsal lengthening by external fixation: a new classification of complications and a stable technique to minimize severe complications. Foot Ankle Int. 2015;36:1369-77.
- Kim HS, Lee YS, Jung JH, Shim JS. Complications of distraction osteogenesis in brachymetatarsia: comparison between the first and fourth brachymetatarsia. Foot Ankle Surg. 2019;25:113-8. [CrossRef]
- Hung WC, Chen CH, Lin CH, et al. Subacute two-stage metatarsal lengthening with gradual distraction for brachymetatarsia. Foot Ankle Surg. 2023;29:86-9.
- Song HR, Oh CW, Kyung HS, et al. Fourth brachymetatarsia treated with distraction osteogenesis. Foot Ankle Int. 2003;24:706-11. [CrossRef]
- Steedman JT, Peterson HA. Brachymetatarsia of the first metatarsal treated by surgical lengthening. J Pediatr Orthop. 1992;12:780-5.
- Lee WC, Yoo JH, Moon JS. Lengthening of fourth brachymetatarsia by three different surgical techniques. J Bone Joint Surg Br. 2009;91:1472-7. [CrossRef]
- Marcinko DE, Rappaport MJ, Gordon S. Post-traumatic brachymetatarsia. J Foot Surg. 1984;23:451-3.
- Shim JS, Park SJ. Treatment of brachymetatarsia by distraction osteogenesis. J Pediatr Orthop. 2006;26:250-4. [CrossRef]
- Choi IH, Chung MS, Baek GH, et al. Metatarsal lengthening in congenital brachymetatarsia: one-stage lengthening versus lengthening by callotasis. J Pediatr Orthop. 1999;19:660-4.
- Waizy H, Polzer H, Schikora N, et al. One-stage metatarsal interposition lengthening with an autologous fibula graft for treatment of brachymetatarsia. Foot Ankle Spec. 2019;12:330-5.
- Jones MD, Pinegar DM, Rincker SA. Callus distraction versus single-stage lengthening with bone graft for treatment of brachymetatarsia: a systematic review. J Foot Ankle Surg. 2015;54:927-31. [CrossRef]
- Steedman JT, Peterson HA. Brachymetatarsia of the first metatarsal treated by surgical lengthening. J Pediatr Orthop. 1992;12:780-5.
- Hung WC, Chen CH, Lin CH, et al. Subacute two-stage metatarsal lengthening with gradual distraction for brachymetatarsia. Foot Ankle Surg. 2023;29:86-9.
- Lamm BM, Gourdine-Shaw MC. Problems, obstacles, and complications of metatarsal lengthening for the treatment of brachymetatarsia. Clin Podiatr Med Surg. 2010;27(4):561-82. [CrossRef]
- Jones MD, Pinegar DM, Rincker SA. Callus distraction versus single-stage lengthening with bone graft for treatment of brachymetatarsia: a systematic review. J Foot Ankle Surg. 2015;54:927-31. [CrossRef]
- Waizy H, Polzer H, Schikora N, et al. One-stage metatarsal interposition lengthening with an autologous fibula graft for treatment of brachymetatarsia. Foot Ankle Spec. 2019;12:330-5.
- Choi IH, Chung MS, Baek GH, et al. Metatarsal lengthening in congenital brachymetatarsia: one-stage lengthening versus lengthening by callotasis. J Pediatr Orthop. 1999;19:660-4. [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



