
Submitted:
04 February 2025
Posted:
06 February 2025
You are already at the latest version
Abstract
Background/Objectives: Hypofractionated radiation therapy (Hypo-RT) schedules may offer radiobiological, patient convenience, and healthcare resource advantages over standard fractionated radiation therapy (S-RT) for glioblastoma (GBM). Additionally, simulated integrated boost (SIB) Hypo-RT is proven to be an effective and safe treatment. We report on our experience regarding progression-free survival (PFS), overall survival (OS), and RT-related toxicities in GBM patients treated with Hypo-RT and S-RT. Methods: Patients with IDH-wildtype GBM received either Hypo-RT (40.05-52.5 Gy/15 fractions) or S-RT (60-70 Gy/30 fractions). Volumetric modulated arc therapy was performed for all patients. Concomitant temozolomide (75 mg/m²/day) and adjuvant chemotherapy (TMZ 150-200 mg/m² for 5 days every 28 days) were administered. OS and PFS were estimated using the Kaplan-Meier method. Results: Ninety-five patients were treated (Hypo-RT: 52, S-RT: 43). With a median follow-up of 25 months (range 9-63), the median age was 65 and 54 years for the Hypo-RT and S-RT groups, respectively. All patients tolerated the treatment well; no significant adverse effects were observed in either group. No acute or late neurological side effects of grade ≥ 2 were reported during RT. Grade 3-4 hematologic toxicity occurred in five cases, all of which interrupted concomitant TMZ (all occurring in the S-RT arm). The time to progression for the S-RT and Hypo-RT groups was 13.7 and 11.1 months, respectively (p=0.243). Regarding OS, the S-RT group had a median OS of 28.8 months compared to 17.5 months in the Hypo-RT group (p=0.007). Conclusions: Although further investigations are ongoing, a statistically significant difference exists in OS between Hypo-RT and S-RT. Hypo-RT could potentially become the standard of care not only for elderly patients but also for those with poor prognosis. Additional investigation with more data is necessary in this context to determine the best standard approach.
Keywords:
radiotherapy
; glioblastoma
; hypofractionated
; normofractionated
1. Introduction
Glioblastoma (GBM) is the most significative malignant primitive brain tumor of the central nervous system, with a percentage around 50% and a poor prognosis with a 5-year overall survival (OS) of about 6.8% [1,2].
The new WHO classification of 2021 introduced significant changes regarding the molecular profile, with the inclusion of differentiations for the “new” GBM entities (only IDH/IDH3 wild type) [3]. The standard treatment for patients with a confirmed diagnosis of GBM involved radical surgery and, subsequently, conventional radiation therapy (RT) up to a dose of 60 Gy, along with concomitant and adjuvant chemotherapy using Temozolomide [4]. In the study by Stupp, mature data showed that with a longer follow-up of 45.9 months, the 2-, 3-, and 4-year overall survival (OS) rates were 11.2%, 4.3%, and 3.8% in the RT alone group versus 27.3%, 16.7%, and 12.9% in the RT plus TMZ group [5].
Recently, in older individuals or those with a poor prognosis (≥ 60-65 years), hypofractionated radiotherapy (Hypo-RT) combined with TMZ is the post-operative treatment that should be considered [6,7,8].
Malmstrom et al. [6] published a randomized Phase III trial in 2012 with three comparison arms: TMZ alone versus standard RT (60Gy in 30 fractions) versus hypo-RT (34Gy in 10 fractions) for patients older than 60. Another Phase III trial by Roa et al. compared two different Hypo-RT schedules (40Gy in 15 fractions and 25Gy in 5 fractions) without concurrent TMZ in patients over 65 years [8]. The authors concluded that hypo-RT should be considered a standard treatment option for elderly patients aged 65 to 70 years. However, the total dose used in these latter Phase III trials was lower than that of the Stupp protocol.
Given the high rates of local recurrence in GBM, typically occurring within 1.5-2 cm from the original tumor edges, along with the fatalities caused by this recurrence, the treatment approach should aim to enhance local control [9,10,11].
To enhance local control, postoperative RT modalities (including intensity-modulated radiotherapy with more precise target coverage that spares surrounding healthy tissue), total dosage, and new fractionation schedules have been assessed for these patients. Several hypo-RT studies in high-grade gliomas have shown promising results concerning efficacy and toxicity, utilizing a biologically effective dose (BED) comparable to standard RT [12,13,14,15,16,17].
Given this background, the current retrospective analysis aimed to compare the toxicity profile and outcomes in patients affected by GBM treated with hypo-RT versus standard RT plus concomitant/adjuvant TMZ.
2. Materials and Methods
2.1. Patients
Inclusion criteria included individuals newly diagnosed with histologically confirmed GBM, aged over 18 years, with a Karnofsky performance scale (KPS) greater than 50, and possessing adequate bone marrow, renal, and liver function. All patients underwent debulking surgery. For cases of unresectable tumors, a biopsy was conducted for diagnosis. The study defined subtotal resection as the removal of less than 100% but more than 50% of the tumor. Patients who met any of the following criteria were excluded from the study: prior brain radiotherapy, brainstem tumors, age under 18 years, and KPS below 50. Each patient signed a specific consent form that was approved by the Institutional Review Board. All procedures were conducted in accordance with the Helsinki Declaration of 1975. Besides advanced age, several factors can contribute to poor prognosis in patients with brain tumors. These factors include low Karnofsky Performance Status (KPS), high Recursive Partitioning Analysis (RPA) class, neurological symptoms resulting from surgical interventions or mass effect, high tumor burden, unresectable or multifocal lesions, significant comorbidity, and potential low treatment compliance due to the rapidly progressive nature of the disease. The study’s endpoints were the evaluation of progression-free survival (PFS), overall survival (OS), and acute and late toxicity.
2.2. Radiotherapy
According to previous reports, patients must lie supine during treatment [17,18]. It was essential to align their post-surgery MRI scans with the treatment plan precisely. Various organs at risk (OARs) were identified and assessed. The gross tumor volume (GTV) was determined using T1-weighted MRI scans with gadolinium contrast. The GTV included the surgical cavity along with any residual contrast-enhanced lesion, or the entire lesion if a biopsy was the only procedure performed. The clinical target volume (CTV1) for the Simultaneous Integrated Boost (SIB) was defined as the GTV without margins or plus 1-3 mm. Meanwhile, the clinical target volume for the lower-dose volume (CTV2) was determined by adding a 10-15 mm margin to the CTV1 while respecting the anatomical barriers and OARs. To establish PTV1 and PTV2, a CTV expansion of 2-3 mm was applied. The total radiation dose was determined based on various factors such as the patient’s age, residual disease presence, and whether they were regarded as having a poor prognosis. For patients not expected to have a poor prognosis, a dose of 60 Gy was administered over 30 fractions (standard S-RT), with the option of a boost up to 70 Gy for residual disease. Conversely, for patients deemed to have a poor prognosis, a dose of 40.05 Gy was administered over 15 fractions, with the option of a boost up to 52.5 Gy (hypo-RT). The prescribed dose of 52.5 Gy in 3 weeks corresponds to a biological effective dose (BED) similar to standard RT. The BED10 values for the prescribed dose and standard RT were 70.88 Gy and 72 Gy, respectively [12,14,17]. Flattening filter-free (FFF) and volumetric modulated arc therapy (VMAT) plans were created using TrueBeam™ (Varian Medical Systems) with two or more partial arcs, either coplanar or non-coplanar. All treatment plans were optimized for PTV, ensuring that over 98% of the PTV received at least 95% of the prescribed dose.
2.3. Chemotherapy
Patients received concomitant TMZ at a daily dose of 75 mg per square meter of body surface area for 21 consecutive days, seven days a week, starting on Day 1 and continuing until the last day of RT. Blood counts were monitored weekly throughout the treatment. Additionally, patients were administered 2-4 mg/day of dexamethasone along with a proton pump inhibitor during RT, while antiepileptic and antiemetic medications were provided as needed. Patients underwent 6-12 cycles of adjuvant TMZ (150-200 mg/m²/day, five days every 28 days), beginning four weeks after completing RT or until disease progression [4,5,17].
2.4. Follow-Up
After radiation therapy, clinical evaluations and MRI were conducted within 45 to 60 days. For the first two years, additional evaluations occurred every 2 to 3 months or as needed. During each visit, the patient’s neurological status and the severity of any complications were assessed according to the National Cancer Institute Common Toxicity Criteria (NCI-CTC Version 4). In the absence of disease progression, adverse neurological events were deemed a consequence of the treatment. The RANO response criteria were applied to evaluate the disease status [19]. The assessment included both acute and late toxicity, as well as PFS and OS, as outcome variables. The categorical variables of acute and late toxicity were defined according to the NCI-CTC scale. Using a binary classification, the study noted whether or not radio-necrosis was present.
2.5. Statistical Analysis
The PFS was calculated from the date of surgery to the last follow-up date or the time of progression. Similarly, OS was measured from the surgery date to the last follow-up date or death from any cause. The Kaplan-Meier method was utilized to assess PFS and OS. A log-rank test was performed to compare various subgroups in univariate analysis. Multivariate analysis was carried out using the Cox regression model to identify independent prognostic factors. A two-sided p-value of 0.05 or less was deemed statistically significant. The following prognostic factors were analyzed: sex, age (<65 vs. ≥65), type of surgery (surgery vs. biopsy), resection (complete vs. incomplete), the interval between surgery and RT (> or < 55 days), protocol RT (S-RT vs. Hypo-RT), adjuvant TMZ (> or < 6 cycles), and O6-methylguanine-DNA-methyltransferase (MGMT) promoter methylation status (methylated vs. not methylated). Data management and statistical analysis were performed using the open-source R platform (version 3.5.2).
3. Results
3.1. patients
From October 2019 to January 2024, 95 GBM patients were treated, including 43 with the standard approach (30 fractions) and 52 with hypo-RT (15 fractions). Table 1 presents the clinical characteristics of the study population. The median age was 62 years (range 24–82). A complete resection was performed in 28 patients (29.5%), significantly more in the standard RT arm (p 0.01). Biopsy alone was conducted in 6 of 43 cases (14%) in the standard RT arm, while 19 of 52 patients (37%) in the hypo-RT arm underwent the same. The median time from the surgical procedure to RT was 54 days (range 41–75), with no statistical difference between the two arms (p=0.19). Compliance with RT plus TMZ was 100%, although five patients discontinued TMZ due to platelet counts below 50,000; all patients were in the S-RT arm. At the 25-month median follow-up, 49 patients (51.6%) were alive, and 68 (71.6%) experienced disease progression. The median OS was 25 months (95% CI 9.8–na), with a 1-year OS of 85% (95% CI 31–73%); the median PFS was 12 months (95% CI 5.8–11.9). As for toxicity, no acute or late neurological side effects greater than Grade 2 were reported. Grade 3–4 hematologic toxicity occurred in 5 cases during RT, but only TMZ was interrupted. Adjuvant TMZ was given to all patients (median six cycles, range 4–17).
Of the 68 cases of disease progression, 39 (41%) underwent re-irradiation followed by second-line systemic therapy (regorafenib or fotemustine). Six patients received second-line chemotherapy alone, while the remaining patients were assessed for best supportive care. The most commonly chosen chemotherapy was regorafenib [20,21], which was also administered alongside re-irradiation.
3.2. Prognostic Factors for OS and PFS
The univariate and multivariate prognostic factors influencing overall survival (OS) for the entire population are presented in Table 2. Consequently, younger age (HR: 2.06; CI 1.05-4.03, p = 0.03), adjuvant TMZ of fewer than six cycles (HR: 0.35; CI 0.18-0.65; p = 0.001), and a time from surgery to RT of less than 55 days (HR: 0.27; CI 0.13-0.46; p = 0.0003) emerged as significant adverse prognostic factors for survival. S-RT and MGMT methylation positively impacted univariate analysis (p = 0.004). Evaluating PFS, adjuvant TMZ of fewer than six cycles (p = 0.0005; p = 0.00002 in both the univariate and multivariate analyses) and a time from surgery to RT of less than 55 days (p = 0.004 in multivariate analysis) were identified as significant adverse prognostic factors.
3.3. S-RT Versus Hypo-RT
Table 1 presents a descriptive analysis of the characteristics of study patients from both groups. The characteristics in both study arms were comparable, except for age (p<0.001) and type of surgery (p=0.01). In the Hypo-RT group, the most common surgical interventions were incomplete resection and biopsy (44% and 37%, respectively), while in the S-RT group, 42% of patients underwent complete resection. Progression-free survival (PFS) was similar in both groups: the time to progression was 13.7 months for S-RT and 11.1 months for Hypo-RT (p=0.243), with 1-year and 2-year PFS rates of 46.7% and 28.5% for Hypo-RT, and 60.5% and 28.5% for S-RT (Figure 1). Likewise, OS showed a significant difference for the S-RT arm: the median OS was 28.8 months for S-RT compared to 17.5 months for the Hypo-RT group (p=0.007; Figure 2). The 1-year and 2-year OS rates were 95.3% and 64% for S-RT, and 72.5% and 43.3% for Hypo-RT. The univariate and multivariate prognostic factors influencing OS are shown in Table 3. Consequently, younger age (HR:2.85; CI: 1.26-6.44, p = 0.01), a time between surgery and RT of less than 55 days (HR:0.22; CI: 0.09-0.54, p = 0.0008) for Hypo-RT, and adjuvant TMZ of fewer than 6 cycles (p=0.002; p = 0.001) for both groups were significant adverse prognostic factors for survival. In evaluating PFS, the same factors were determined as significant adverse prognostic factors in the univariate and multivariate analyses, as shown in Table 4.
4. Discussion
GBM encompasses heterogeneous tumor groups that differ by site of origin, histopathological characteristics, tumor microenvironment, and genetics. It is often resistant to various treatments, including radiotherapy, chemotherapy, and targeted therapy, with overall survival rates spanning from a few months to several years, making it invariably lethal. The standard treatment for this tumor thus far includes surgical resection, postoperative radiotherapy with concomitant temozolomide, followed by adjuvant therapy. This treatment protocol provides a median OS of 14.6 months, while the percentage of patients surviving for two years rises from 10.4% to 26.5% [4,5]. The standard treatment consists of 60 Gy delivered in 30 fractions over six weeks, with each fraction being 2 Gy administered using three-dimensional conformal fractionated radiation therapy. Glioblastoma multiforme (GBM) is characterized by a rapid doubling time. Utilizing prolonged RT schedules may enhance cell repopulation, which contributes to up to 10% of patients experiencing disease [22,23,24]. GBM tumors are known to have relatively high resistance to radiation therapy, responding similarly to late-responding neural tissue. This means their reaction to radiation may be delayed and take longer to manifest. Approximately 50% of GBM tumors carry a mutated P53 tumor suppressor gene. These tumors have been observed to behave like late-reacting tissues when subjected to conventional high-dose radiation therapy, demonstrating a significant level of resistance and aggressiveness. Consequently, they may benefit from hypo-RT protocols. In the current scenario, hypo-RT offers several advantages, such as enhancing the effectiveness of killing cancer cells by administering a higher dose per treatment session over a shorter period. Moreover, it may help to minimize the negative impact of accelerated tumor cell regrowth by reducing the overall duration of radiation therapy. Numerous studies analyzing three weeks of RT have demonstrated safety and efficacy, reporting a median survival of up to 20 months [12,14,17,25,26,27]. Although many studies of hypo-RT in GBM utilized suboptimal radiation doses, they reported efficacy comparable to CFRT, particularly in high-risk patients. However, the therapeutic potential of HFRT schedules remains under investigation. In a prior report, poor prognosis GBM patients were treated with hypo-RT combined with simultaneous integrated boost (52.5Gy in 15 fractions). The data is encouraging; the median OS was 13 months.
Given this background, the current analysis aimed to retrospectively evaluate all GBM patients treated with RT (standard or hypo-RT) in our department. In this study, the total dose for Hypo-RT was 52.5 Gy over 3 weeks, yielding a biological effective dose (BED) similar to standard RT (BED10 of 70.88 Gy compared to 72 Gy, respectively).
A total of ninety-five patients underwent RT and were included in this study, which revealed a median OS and PFS of 25 and 12 months, respectively. PFS was comparable in both groups, with 13.7 months for S-RT and 11.1 months for Hypo-RT. Similarly, OS demonstrated a significant difference in the S-RT arm, where the median OS was 28.8 months for S-RT, compared to 17.5 months in the Hypo-RT group (p=0.007). One-year and two-year OS rates were 95.3% and 64% for S-RT, and 72.5% and 43.3% for Hypo-RT.
It is important to reach a consensus on the appropriate dose of HFRT to be used in studies. In a pilot study by Terasaki et al., a median survival of 15.6 months was achieved using a dose of 45 Gy in 15 fractions alongside concurrent and adjuvant TMZ [28]. Navarria et al. evaluated a total dose of 60 Gy in 15 fractions in a phase II trial involving 97 patients. They reported a median OS of 16 months and a 2-year OS of 30.5% [26]. Considering the sample size and the retrospective nature of this analysis, the current data align with those reported by Navarria et al. [26].
Indeed, when the total dose was reduced, negative survival outcomes were recorded. For instance, in the study published by Ryan et al., a median OS of 9 months with a 2-year OS of 9% was reported. In this study, 93 patients were randomized to receive either 60/30 fractions or 45/15 fractions. [27].
Regarding side effects, published data indicate an increased incidence of grade III-IV radionecrosis (3 to 20%) when high-dose per fraction and therapeutically effective doses are used [26]. In the present analysis, toxicity data align with those from other experiences; in fact, only grade I-II toxicity was noted. Additionally, five patients discontinued concomitant TMZ in the standard arm due to a reduction in PTL [26,27].
However, despite the biological effective dose being similar in both groups, we observed better survival in the standard arm. This is likely due to the differing populations; specifically, those in the standard arm were younger (only 14% were over 65 years old compared to 50% in the hypo-RT arm) and had a complete surgical resection (42% versus 19%). This suggests that younger patients achieved better results with the standard approach and that the extent of surgical resection is a significant prognostic factor affecting survival, as expected.
In both univariate and multivariate analyses, age, MGMT status, time from surgery to RT, and more than six cycles of TMZ are critical prognostic factors for survival. Although most treated patients underwent extensive surgical resection (29.5% with complete resection and 44% with partial resection), there was no significant perioperative morbidity, and adjuvant treatments commenced between 6 and 8 weeks (median 55 days). A meta-analysis of 16 Radiation Therapy Oncology Group (RTOG) randomized controlled trials has shown that PFS is not adversely affected by a delay in starting RT, provided it begins within six weeks after surgery [28,29]. Consequently, current treatment recommendations advise initiating RT within six weeks after surgery. However, recent data indicated that delaying the initiation of adjuvant RT by six weeks or more did not significantly impact either PFS or OS [30,31,32,33,34].
Our study observed an increase in survival when RT started more than 55 days after surgery, particularly in patients in the hypo-RT arm (Table 3 and Table 4). The explanation for this result likely relates to the characteristics of the patients; in fact, it may be that there is a bias between the study groups, with patients who were in poorer condition at presentation being treated earlier. Among the patients who began RT within 55 days post-surgery, about 60% received hypo-RT and were in worse condition at presentation.
However, the reported median OS (25 months from surgery for the entire population may serve as a surrogate for data regarding gap surgery-RT), increasing the likelihood of a brief delay in administering RT without negatively impacting OS and PFS results.
In our cohort regarding chemotherapy, adjuvant TMZ was successfully administered to 100% of patients, with 50% receiving more than six cycles. It continues to be an important prognostic factor for survival in both univariate and multivariate analyses.
The same data were recently reported in an updated systematic review and meta-analysis of extended adjuvant temozolomide [35]. Gupta et al. demonstrated that extended adjuvant TMZ (12 cycles) was linked to a statistically significant reduction in the risk of progression (HR = 0.72, 95% CI: 0.60-0.87; p = 0.007) and death (HR = 0.71, 95% CI: 0.57-0.90; p = 0.004) compared to the standard adjuvant six cycles of TMZ [35]. However, the survival benefit of 12 cycles was confined to data synthesized from retrospective, nonrandomized comparative studies, which showed no statistically significant difference in outcomes when only pooling data from RCTs.
Another issue for GBM to improve survival is the second-line therapy during recurrence. In the current population, salvage treatment at progression was administered to approximately 50% of patients: 41% received radiation therapy, and 45% received second-line chemotherapy, with 50% in the S-RT group compared to 40% in the hypo-RT group. These results are consistent with those reported in the literature [26] and may help explain the increase in OS. Across the entire population, the potential for reirradiation has demonstrated its prognostic significance in univariate analysis.
5. Conclusions
Despite the limitations of this study—such as its retrospective nature, nonrandomized design, and sample size—the results suggest that Hypo-RT is a feasible and safe approach, demonstrating no excessive treatment interruptions and acceptable toxicity, along with reasonable outcome rates. There are still open questions regarding dose escalation and the optimal schedule. Nevertheless, a phase III trial could determine the potential for incorporating Hypo-RT as the new standard of care for newly diagnosed GBM, not only for frail or older individuals.
Author Contributions
FCDG conceptualization, writing - original draft, formal analysis; IB methodology and investigation; VD conceptualization, data curation, formal analysis; PG methodology, data curation, formal analysis; FG conceptualization, methodology, formal analysis; TT project administration; MPS, AS, MC, RC, DG, IV, LL resources and investigation; VF, GS, MAG, CR, SF, LG supervision and validation; AF conceptualization, writing - review and editing, supervision and validation.
Funding
“This research received no external funding”.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Institutional Review Board (Title: Registro della Radioterapia avanzata in ambito oncologico e non: Advanced Radioterapy study ARTs) of General Regional Hospital F. Miulli (protocol code ARTs).” for studies involving humans.
Informed Consent Statement
“Informed consent was obtained from all subjects involved in the study.” “Written informed consent has been obtained from the patient(s) to publish this paper”.
Data Availability Statement
Data were available to the corresponding author.
Conflicts of Interest
“The authors declare no conflicts of interest.”.
References
- Schaff LR, Mellinghoff IK. Glioblastoma and Other Primary Brain Malignancies in Adults: A Review (2023). JAMA. Feb 21;329(7):574-587.
- Wen PY, Weller M, Lee EQ, Alexander BM, Barnholtz-Sloan JS, Barthel FP, Batchelor TT, Bindra RS, Chang SM, Chiocca EA, Cloughesy TF, DeGroot JF, Galanis E, Gilbert MR, Hegi ME, Horbinski C, Huang RY, Lassman AB, Le Rhun E, Lim M, Mehta MP, Mellinghoff IK, Minniti G, Nathanson D, Platten M, Preusser M, Roth P, Sanson M, Schiff D, Short SC, Taphoorn MJB, Tonn JC, Tsang J, Verhaak RGW, von Deimling A, Wick W, Zadeh G, Reardon DA, Aldape KD, van den Bent MJ (2020). Glioblastoma in adults: a Society for Neuro-Oncology (SNO) and European Society of Neuro-Oncology (EANO) consensus review on current management and future directions Neuro-Oncology 22(8), 1073–1113, 1073. [CrossRef]
- Park YW, Vollmuth P, Foltyn-Dumitru M, Sahm F, Choi KS, Park JE, Ahn SS, Chang JH, Kim SH (2023). The 2021 WHO Classification of Tumors of the Central Nervous System: clinical implications. J Magn Reson Imaging. 58(6):1680-1702.
- Stupp R, Hegi ME, Mason WP, van den Bent MJ, Taphoorn MJ, Janzer RC, Ludwin SK, Allgeier A, Fisher B, Belanger K, Hau P, Brandes AA, Gijtenbeek J, Marosi C, Vecht CJ, Mokhtari K, Wesseling P, Villa S, Eisenhauer E, Gorlia T, Weller M, Lacombe D, Cairncross JG, Mirimanoff RO (2009). Effects of radiotherapy with concomitant and adjuvant temozolomide versus radiotherapy alone on survival in glioblastoma in a randomized phase III study: 5-year analysis of the EORTC-NCIC trial. Lancet Oncol; 10(5):459–466.
- Stupp R, Hegi ME, Mason WP, van den Bent MJ, Taphoorn MJ, Janzer RC, Ludwin SK, Allgeier A, Fisher B, Belanger K, Hau P, Brandes AA, Gijtenbeek J, Marosi C, Vecht CJ, Mokhtari K, Wesseling P, Villa S, Eisenhauer E, Gorlia T, Weller M, Lacombe D, Cairncross JG, Mirimanoff RO; European Organisation for Research and Treatment of Cancer Brain Tumour and Radiation Oncology Groups; National Cancer Institute of Canada Clinical Trials Group (2009). Effects of radiotherapy with concomitant and adjuvant temozolomide versus radiotherapy alone on survival in glioblastoma in a randomized phase III study: 5-year analysis of the EORTC-NCIC trial. Lancet Oncol;10(5):459-66. [CrossRef]
- Malmström, A.; Grønberg, B.H.; Marosi, C.; Stupp, R.; Frappaz, D.; Schultz, H.; Abacioglu, U.; Tavelin, B.; Lhermitte, B.; Hegi, M.E.; et al. (2012). Temozolomide versus standard 6-week radiotherapy versus hypofractionated radiotherapy in patients older than 60 years with glioblastoma: The Nordic randomized, phase 3 trial. Lancet Oncol; 13, 916–926.
- Perry JR, Laperriere N, O’Callaghan CJ, Brandes AA, Menten J, Phillips C, Fay M, Nishikawa R, Cairncross JG, Roa W, Osoba D, Rossiter JP, Sahgal A, Hirte H, Laigle-Donadey F, Franceschi E, Chinot O, Golfinopoulos V, Fariselli L, Wick A, Feuvret L, Back M, Tills M, Winch C, Baumert BG, Wick W, Ding K, Mason WP; Trial Investigators (2017). Short-Course Radiation plus Temozolomide in Elderly Patients with Glioblastoma. N Engl J Med;376(11):1027-1037. [CrossRef]
- Roa, W.; Kepka, L.; Kumar, N.; Sinaika, V.; Matiello, J.; Lomidze, D.; Hentati, D.; Guedes de Castro, D.; Dyttus-Cebulok, K.; Drodge, S.; et al. (2015). International Atomic Energy Agency Randomized Phase III Study of Radiation Therapy in Elderly and/or Frail Patients With Newly Diagnosed Glioblastoma Multiforme. J. Clin. Oncol. 33, 4145–4150.
- Balducci, M.; Apicella, G.; Manfrida, S.; Mangiola, A.; Fiorentino, A.; Azario, L.; D’Agostino, G.R.; Frascino, V.; Dinapoli, N.; Mantini, G.; et al. (2010). Single- Arm Phase II Study of Conformal Radiation Therapy and Temozolomide plus fractionated Stereotactic Conformal Boost in High grade Gliomas. Strahlentherapie und Onkologie; 186, 558–564.
- Niyazi M, Andratschke N, Bendszus M, Chalmers AJ, Erridge SC, Galldiks N, Lagerwaard FJ, Navarria P, Munck Af Rosenschöld P, Ricardi U, van den Bent MJ, Weller M, Belka C, Minniti G (2023). ESTRO-EANO guideline on target delineation and radiotherapy details for glioblastoma Radiother Oncol;184:109663. [CrossRef]
- Lee, S.W.; Fraass, B.A.; Marsh, L.H.; Herbort, K.; Gebarski, S.S.; Martel, M.K.; Radany, E.H.; Lichter, A.S.; Sandler, H. M (1999). Patterns of failure following high-dose 3-D conformal radiotherapy for high-grade astrocytomas: A quantitative dosimetric study. Int. J. Radiat. Oncol. Biol. Phys, 43, 79–88.
- Scoccianti, S.; Krengli, M.; Marrazzo, L.; Magrini, S.M.; Detti, B.; Fusco, V.; Pirtoli, L.; Doino, D.; Fiorentino, A.; Masini, L.; et al. (2018). Hypofractionated radiotherapy with simultaneous integrated boost (SIB) plus temozolomide in good prognosis patients with glioblastoma: A multicenter phase II study by the Brain Study Group of the Italian Association of Radiation Oncology (AIRO). Radiol. Med; 123, 48–62.
- Jablonska, P.A.; Diez-Valle, R.; Pérez-Larraya, J.G.; Moreno-Jiménez, M.; Idoate, M.Á.; Arbea, L.; Tejada, S.; Garcia de Eulate, M.R.; Ramos, L.; Arbizu, J.; et al. (2019). Hypofractionated radiation therapy and temozolomide in patients with glioblastoma and poor prognostic factors. A prospective, single-institution experience. PLoS ONE;14, e0217881.
- Navarria, P.; Pessina, F.; Cozzi, L.; Tomatis, S.; Reggiori, G.; Simonelli, M.; Santoro, A.; Clerici, E.; Franzese, C.; Carta, G.; et al. (2019). Phase II study of hypofractionated radiation therapy in elderly patients with newly diagnosed glioblastoma with poor prognosis. Tumori; 105, 47–54.
- Minniti, G.; Scaringi, C.; Lanzetta, G.; Terrenato, I.; Esposito, V.; Arcella, A.; Pace, A.; Giangaspero, F.; Bozzao, A.; Enrici, R. M (2015). Standard (60 Gy) or short-course (40 Gy) irradiation plus concomitant and adjuvant temozolomide for elderly patients with glioblastoma: A propensity-matched analysis. Int. J. Radiat. Oncol. Biol. Phys; 91, 109–115.
- Pedretti, S.; Masini, L.; Turco, E.; Triggiani, L.; Krengli, M.; Meduri, B.; Pirtoli, L.; Borghetti, P.; Pegurri, L.; Riva, N.; et al. (2019). Hypofractionated radiation therapy versus chemotherapy with temozolomide in patients affected by RPA class V and VI glioblastoma: A randomized phase II trial. J. Neurooncol; 143, 447–455.
- Gregucci F, Surgo A, Bonaparte I, Laera L, Ciliberti MP, Carbonara R, Gentile MA, Giraldi D, Calbi R, Caliandro M, Sasso N, D’Oria S, Somma C, Martinelli G, Surico G, Lombardi G, Fiorentino A (2021). Poor-Prognosis Patients Affected by Glioblastoma: Retrospective Study of Hypofractionated Radiotherapy with Simultaneous Integrated Boost and Concurrent/Adjuvant Temozolomide. J Pers Med; 11(11):1145. [CrossRef]
- Gregucci F, Bonaparte I, Surgo A, Caliandro M, Carbonara R, Ciliberti MP, Aga A, Berloco F, De Masi M, De Pascali C, Fragnoli F, Indellicati C, Parabita R, Sanfrancesco G, Branà L, Ciocia A, Curci D, Guida P, Fiorentino A (2021). Brain Linac-Based Radiation Therapy: “Test Drive” of New Immobilization Solution and Surface Guided Radiation Therapy. J Pers Med;11(12):1351. [CrossRef]
- Therasse, P.; Arbuck, S.G.; Eisenhauer, E.A.; Wanders, J.; Kaplan, R.S.; Rubinstein, L.; Verweij, J.; Van Glabbeke, M.; van Oosterom, A.T.; Christian, M.C.; et al. (2000). New guidelines to evaluate the response to treatment in solid tumors. European Organization for Research and Treatment of Cancer, National Cancer Institute of the United States, National Cancer Institute of Canada. J. Natl. Cancer Inst, 92, 205–216.
- Gregucci F, Di Guglielmo FC, Surgo A, Carbonara R, Laera L, Ciliberti MP, Gentile MA, Calbi R, Caliandro M, Sasso N, Davi’ V, Bonaparte I, Fanelli V, Giraldi D, Tortora R, Internò V, Giuliani F, Surico G, Signorelli F, Lombardi G, Fiorentino A (2023). Reirradiation with radiosurgery or stereotactic fractionated radiotherapy in association with regorafenib in recurrent glioblastoma Strahlenther Onkol. [CrossRef]
- Gregucci F, Surgo A, Carbonara R, Laera L, Ciliberti MP, Gentile MA, Caliandro M, Sasso N, Bonaparte I, Fanelli V, Tortora R, Paulicelli E, Surico G, Lombardi G, Signorelli F, Fiorentino A (2022). Radiosurgery and Stereotactic Brain Radiotherapy with Systemic Therapy in Recurrent High-Grade Gliomas: Is It Feasible? Therapeutic Strategies in Recurrent High-Grade Gliomas. J Pers Med;12(8):1336. [CrossRef]
- Reddy K, Damek D, Gaspar LE, et al. (2012). Phase II trial of hypofractionated IMRT withtemozolomide for patients with newly diagnosed glioblastoma multiforme. IntJ Radiat Oncol Biol Phys;84(3):655–660.17.
- Chen C, Damek D, Gaspar LE, et al. (2011). Phase I trial of hypofractionated intensity-modulated radiotherapy with temozolomide chemotherapy for patients with newly diagnosed glioblastoma multiforme. Int J Radiat Oncol Biol Phys;81(4):1066–1074.18.
- Walker MD, Strike TA, Sheline GE (1979). An analysis of dose-effect relationshipin the radiotherapy of malignant gliomas. Int J Radiat Oncol Biol Phys;5(10):1725–1731.
- Iuchi T, Hatano K, Kodama T, et al. (2014). Phase 2 trial of hypofractionated high-dose intensity modulated radiation therapy with concurrent and adjuvant temozolomide for newly diagnosed glioblastoma. Int J Radiat Oncol Biol Phys;88(4):793–800.21.
- Navarria P, Pessina F, Tomatis S, et al. (2017). Are three weeks hypofractionated radia-tion therapy (HFRT) comparable to six weeks for newly diagnosed glioblastomapatients? Results of a phase II study. Oncotarget;8(40):67696–67708.
- Rayan A, Abdel-Kareem S, Hasan H, Zahran AM, Gamal DA. (2020). Hypofractionated radiation therapy with temozolomide versus standard chemoradiation in patients with glioblastoma multiforme (GBM): A prospective, single institution experience. Reports of Practical Oncology and Radiotherapy 25 (2020) 890– 898. 2020.
- Terasaki M, Eto T, Nakashima S, et al. (2011). A pilot study of hypofractionated radiation therapy with temozolomide for adults with glioblastoma multiforme. JNeurooncol;102(2):247–253.
- Blumenthal DT, Won M, Mehta MP, Curran WJ, Souhami L, Michalski JM, Rogers CL, Corn BW (2009). Short delay in initiation of radiotherapy may not affect outcome of patients with glioblastoma: a secondary analysis from the radiation therapy oncology group database. J. Clin. Oncol. 27, 733–9. [CrossRef]
- Blumenthal, D. T. , Won, M., Mehta, M. P., Gilbert, M. R. & Corn, B. W (2018). Short delay in initiation of radiotherapy for patients with glioblastoma- effect of concurrent chemotherapy: a secondary analysis from the NRG Oncology/Radiation Therapy Oncology Group (RTOG) database. Neuro Oncol. 20. [CrossRef]
- Mallick S, Kunhiparambath H, Gupta S, Benson R, Sharma S, Laviraj MA et al. (2018) Hypofractionated accelerated radiotherapy (HART) with concurrent and adjuvant temozolomide in newly diagnosed glioblastoma: a phase II randomized trial (HART-GBM trial). J Neurooncol 140(1) :75–82.
- Louvel G, Metellus P, Noel G, Peeters S, Guyotat J, Duntze J et al. (2016) Delaying standard combined chemoradiotherapy after surgical resection does not impact survival in newly diagnosed glioblastoma patients. Radiother Oncol 118(1):9–15.
- Lv L, Eda V, Callegaro-Filho S, Koch Lde D, Pontes Lde O, Weltman B (2016) E et al. Minimizing the uncertainties regarding the effects of delaying radiotherapy for Glioblastoma: a systematic review and meta-analysis. Radiother Oncol 118(1):1–8.
- Zur I, Tzuk-Shina T, Guriel M, Eran A, Kaidar-Person O (2020). Survival impact of the time gap between surgery and chemo-radiotherapy in Glioblastoma patients. Sci Rep;10(1):9595. [CrossRef]
Figure 1.
Progression-free survival for S-RT (A 30) and Hypo-RT (B 15).
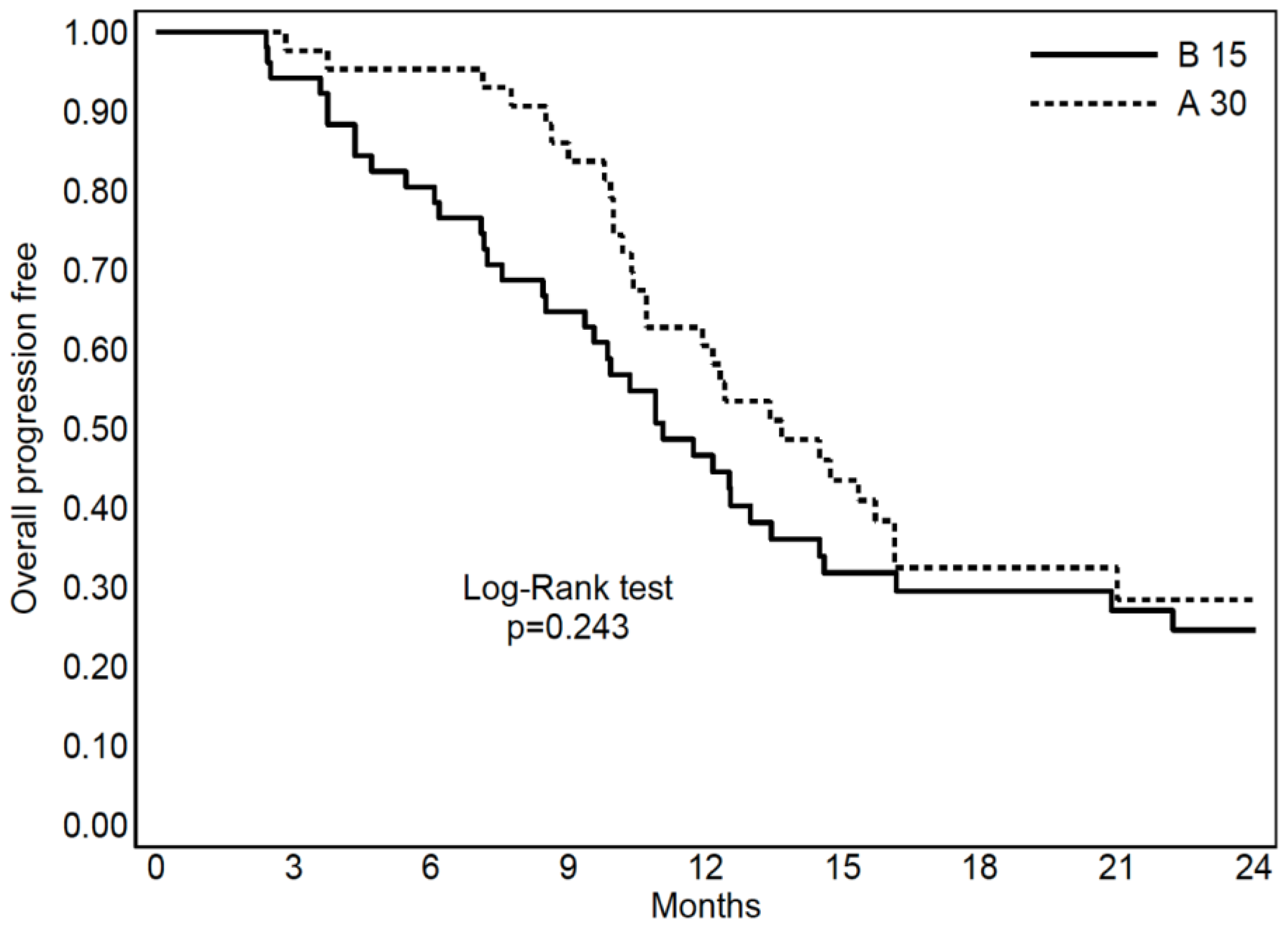
Figure 2.
Overall Survival for S-RT (A 30) and Hypo-RT (B 15).
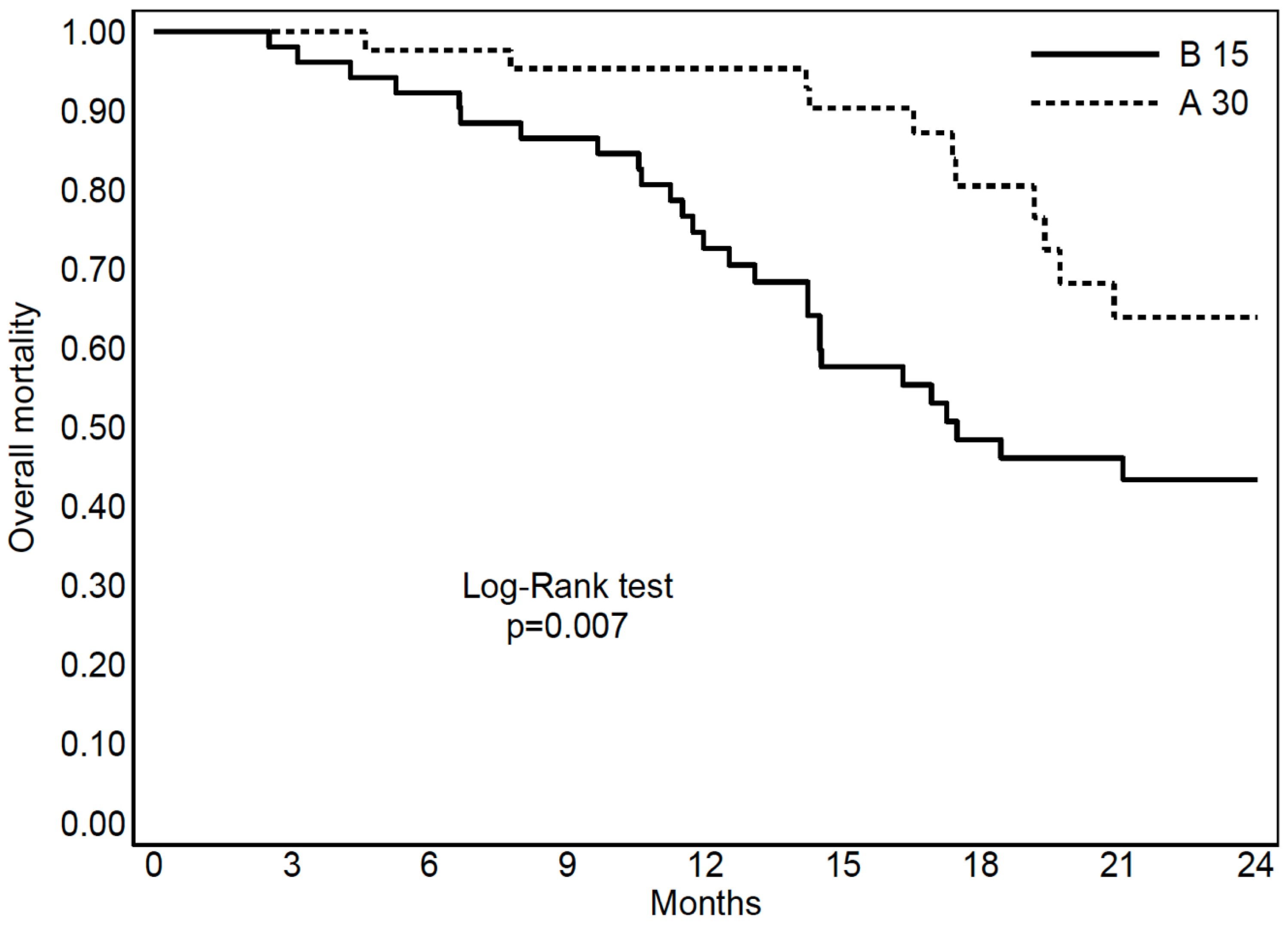

Table 1.
Patients’ characteristics of both arms.
| Table 1 | S-RT | Hypo-RT | P value | |
|---|---|---|---|---|
| Number of patients | ||||
| 43 | 52 | |||
| Gender | ||||
| Male | 24 (56%) | 35 (67%) | 0.25 | |
| Female | 19 (44%) | 17 (33%) | ||
| Age | ||||
| Median (IQR) [years] | 54 (24-74) | 65 (37-82) | <0.001 | |
| < 60 [years] | 28 (65%) | 13 (25%) | ||
| 60-65 [years] | 9 (21%) | 14 (25%) | ||
| > 65 [years] | 6 (14%) | 25 (50%) | ||
| MGMT methylation | ||||
| Methylated | 12 (28%) | 11 (21%) | 0.37 | |
| Unmethylated | 7 (16%) | 5 (10%) | ||
| Not Available | 24 (56%) | 36 (69%) | ||
| Surgery at diagnosis | ||||
| Complete | 18 (42%) | 10 (19%) | 0.01 | |
| Incomplete | 19 (44%) | 23 (44%) | ||
| Unresectable (Biopsy) | 6 (14%) | 19 (37%) | ||
| Median time between surgery and adjuvant therapy | ||||
| Median (IQR) [days] | 55 (46-75) | 53 (41-64) | 0.192 | |
| Adjuvant RT (total dose) | ||||
| 60 Gy in 30 fractions | 31 (72%) | - | <0.001 | |
| >60 Gy in 30 fractions | 12 (28%) | - | ||
| 40.5 Gy in 15 fractions | - | 17 (33%) | ||
| >40.5 Gy in 15 fractions | - | 35 (67%) | ||
| Adjuvant TMZ (cycles) | ||||
| Median (IQR) | 6 (5-17) | 6 (4-14) | 0.108 | |
| Reirradiation | ||||
| Yes | 21 (49%) | 18 (35%) | 0.167 | |
| Not | 22 (51%) | 34 (65%) | ||
| Second line systemic therapy | ||||
| Yes | 24 (56%) | 21 (40%) | 0.312 | |
| Not | 10 (23%) | 15 (29%) | ||
| Not Available | 9 (21%) | 16 (31%) | ||
| Type of second line systemic therapy | ||||
| Regorafenib | 11 (48%) | 10 (48%) | 0.365 | |
| Fotemustine | 3 (12%) | 2 (10%) | ||
| Bevacizumab | 4 (15%) | 1 (5%) | ||
| Not Available | 6 (25%) | 8 (37%) | ||
| Follow-up | ||||
| Median (range) [months] | 25 (18-36) | 31 (22-43) | 0.107 | |
Table 2.
The univariate and multivariate prognostic factors influencing survival for the entire population.
Table 2.
The univariate and multivariate prognostic factors influencing survival for the entire population.
| Table 2 Variable |
Univariate | Multivariate | |||||
|---|---|---|---|---|---|---|---|
| HR | 95%CI | P | HR | 95%CI | P | ||
| Age (≥ 65 years) | |||||||
| 1.48 | 0.79-2.76 | 0.21 | 2.06 | 1.05-4.03 | 0.03 | ||
| MGMT methylation (YES) | |||||||
| 0.40 | 0.17-0.95 | 0.03 | - | - | - | ||
| Surgery type (Incomplete) | |||||||
| 1.17 | 0.60-2.29 | 0.63 | - | - | - | ||
| Surgery-RT time (≥ 55 days) | |||||||
| 0.38 | 0.19-0.73 | 0.003 | 0.27 | 0.13-0.56 | 0.0003 | ||
| Adjuvant RT (30 fx) | |||||||
| 0.55 | 0.29-0.99 | 0.05 | - | - | - | ||
| Adjuvant TMZ (≥ 6 cycles) | |||||||
| 0.42 | 0.23-0.78 | 0.005 | 0.35 | 0.18-0.65 | 0.001 | ||
| Reirradiation (YES) | |||||||
| 1.84 | 1.01-3.37 | 0.04 | - | - | - | ||
| Second line systemic therapy (YES) | |||||||
| 1.27 | 0.69-2.31 | 0.42 | - | - | - | ||
Table 3.
The univariate and multivariate prognostic factors influencing survival for S-RT and Hypo-RT.
Table 3.
The univariate and multivariate prognostic factors influencing survival for S-RT and Hypo-RT.
| Table 3: Variable |
Univariate | Multivariate | ||||||
|---|---|---|---|---|---|---|---|---|
| HR | 95%CI | P | HR | 95%CI | P | |||
| Age | ||||||||
| (≥ 60 years) | S-RT | 0.87 | 0.23-3.25 | 0.84 | - | - | - | |
| (≥ 65 years) | Hypo-RT | 1.62 | 0.78-3.36 | 0.18 | 2.85 | 1.26-6.44 | 0.01 | |
| MGMT methylation | ||||||||
| (YES) | S-RT | 0.49 | 0.11-2.23 | 0.35 | - | - | - | |
| (YES) | Hypo-RT | 0.38 | 0.13-1.1 | 0.07 | - | - | - | |
| Surgery type | ||||||||
| (Incomplete) | S-RT | 1.16 | 0.38-3.47 | 0.78 | - | - | - | |
| (Incomplete) | Hypo-RT | 0.93 | 0.38-2.29 | 0.88 | - | - | - | |
| Surgery-RT time | ||||||||
| (≥ 55 days) | S-RT | 0.64 | 0.21-2.01 | 0.44 | - | - | - | |
| (≥ 55 days) | Hypo-RT | 0.31 | 0.13-0.73 | 0.007 | 0.22 | 0.09-0.54 | 0.0008 | |
| Adjuvant RT | ||||||||
| (≥ 60 Gy) | S-RT | 0.28 | 0.9-1.86 | 0.2 | - | - | - | |
| (≥ 40.5Gy) | Hypo-RT | 1.08 | 0.49-2.39 | 0.84 | - | - | - | |
| Adjuvant TMZ | ||||||||
| (≥ 6 cycles) | S-RT | 0.48 | 0.13-1.69 | 0.25 | 0.14 | 0.02-0.73 | 0.01 | |
| (≥ 6 cycles) | Hypo-RT | 0.40 | 0.19-0.84 | 0.01 | 0.30 | 0.14-0.66 | 0.002 | |
| Reirradiation | ||||||||
| (YES) | S-RT | 2.79 | 0.77-10.09 | 0.11 | - | - | - | |
| (YES) | Hypo-RT | 1.82 | 0.89-3.73 | 0.10 | - | - | - | |
| Second line systemic therapy | ||||||||
| (YES) | S-RT | 1.91 | 0.59-6.14 | 0.27 | - | - | - | |
| (YES) | Hypo-RT | 1.19 | 0.58-2.45 | 0.61 | - | - | - | |
Table 4.
The univariate and multivariate prognostic factors influencing progression for S-RT and Hypo-RT.
Table 4.
The univariate and multivariate prognostic factors influencing progression for S-RT and Hypo-RT.
| Table 4 Variable |
Univariate | Multivariate | |||||
|---|---|---|---|---|---|---|---|
| HR | 95%CI | P | HR | 95%CI | P | ||
| Age | |||||||
| (≥ 60 years) | S-RT | 0.834 | 0.39-1.77 | 0.63 | - | - | - |
| (≥ 65 years) | Hypo-RT | 1.44 | 0.76-2.75 | 0.25 | 2.15 | 1.07-4.31 | 0.03 |
| MGMT methylation | |||||||
| (YES) | S-RT | 1.02 | 0.45-2.31 | 0.95 | - | - | - |
| (YES) | Hypo-RT | 0.51 | 0.22-1.17 | 0.11 | - | - | - |
| Surgery type | |||||||
| (Incomplete) | S-RT | 0.75 | 0.37-1.52 | 0.42 | - | - | - |
| (Incomplete) | Hypo-RT | 1.09 | 0.47-2.48 | 0.83 | - | - | - |
| Surgery-RT time | |||||||
| (≥ 55 days) | S-RT | 1.19 | 0.58-2.42 | 0.63 | - | - | - |
| (≥ 55 days) | Hypo-RT | 0.43 | 0.21-0.86 | 0.01 | 0.30 | 0.14-0.63 | 0.001 |
| Adjuvant RT | |||||||
| (≥ 60 Gy) | S-RT | 0.61 | 0.28-1.26 | 0.17 | - | - | - |
| (≥ 40.5Gy) | Hypo-RT | 1.22 | 0.60-2.47 | 0.57 | - | - | - |
| Adjuvant TMZ | |||||||
| (≥ 6 cycles) | S-RT | 0.47 | 0.22-0.98 | 0.04 | 0.26 | 0.12-0.62 | 0.002 |
| (≥ 6 cycles) | Hypo-RT | 0.38 | 0.20-0.74 | 0.004 | 0.31 | 0.15-0.60 | 0.0006 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



