Submitted:
05 February 2026
Posted:
05 February 2026
You are already at the latest version
Abstract
Background: Malignant tumors pose a serious threat to human health; however, the etiologies of most cancers remain elusive, which highlights the limitations of the prevailing biological-reductionist and statistical paradigms in modern medicine. Methods: To address these gaps, this study developed a physics-informed conceptual model of the human organism from a life-environment systems perspective. This model emphasizes the high degree of order in living systems and centers on the functional role of the immune system, integrating biological, psychological, and environmental dimensions into a unified analytical framework. Results: The model provides a coherent explanation for tumorigenesis, framing it as a state of dysregulation in the internal environment that arises from persistent exogenous factors and compromised immune surveillance. It further predicts a comprehensive treatment framework targeting physiological disorder rectification, etiological factor intervention, and psychosocial support. Conclusion: This study advances immuno-oncology by elucidating the impact of psychosocial and behavioral factors on immunity from a holistic, systems-based perspective. The model bridges the gap between modern and traditional medical paradigms, offering a novel intellectual framework to refocus clinical practice on etiological diagnosis and integrated care, with the potential to improve cancer management.
Keywords:
immuno-oncology
; systems medicine
; physical biomedicine
; qualitative physics
; integrative oncology
; etiological diagnosis
; homeostasis
1. Introduction
Malignant tumors are currently one of the major global public health problems. According to the International Agency for Research on Cancer (IARC), one in five people worldwide will develop cancer during their lifetime, and approximately one in nine men, and one in 12 women, will die from cancer [1]. The prevention and treatment of cancer have become a major concern for the global medical community.
The disease-centric (allopathic) model has played a significant role in the early advancement of biomedicine. The invention of antibiotics, for instance, is a milestone in the history of medicine, as it reduces the mortality of infectious diseases and enormously promotes the development of modern medicine. The development of targeted chemotherapeutic agents has made precision therapy possible. These agents avoid the extensive destruction of normal cells caused by traditional chemotherapy, prolong patient survival, improve quality of life, and promote the transformation of cancer management into a chronic disease. However, several experts have discovered that the idea of adversarial therapy has certain limitations. Many oncological agents continue to induce hematological toxicity, and some therapeutic modalities themselves carry carcinogenic risks [2,3]. Additionally, the concept of precision treatment in biomedicine contradicts not only the biopsychosocial model (BPSM) proposed by Engel, but also the holistic principles of traditional medicine [4,5]. Consequently, interest in integrative medicine has been steadily increasing [6,7].
The biomedical system itself faces numerous challenges. First, humans are conscious beings possessing both natural and social attributes. Biomedicine is focused on the investigation of molecular pathways in order to uncover the mechanisms of cancer; however, the origins of life and consciousness remain important unsolved mysteries. Biological life is characterized by networks of unimaginable complexity. Without a comprehensive understanding of normal life phenomena, a complete explanation of pathology through biomedicine remains fundamentally limited. Additionally, although clinical diagnostics repeatedly emphasize the importance of etiological diagnoses, many internal diseases, including mental disorders, are currently diagnosed according to clinical symptoms, syndromes, and test results, rather than etiologies. To illustrate this notion, gastrointestinal hemorrhage can be diagnosed using symptoms, while nephrotic syndrome and Cushing’s diseases are diagnosed on syndromic presentation. Hypertension, diabetes, and arrhythmia are diagnosed using laboratory results, while some diseases, such as Hodgkin's lymphoma, are named after the physicians who first described them. Currently, the etiologies of the vast majority of chronic diseases remain unknown. Without a clear understanding of etiologies, achieving cures for chronic diseases remains an elusive goal.
Furthermore, pathophysiologists indicate that, during the process of disease occurrence and development, evidence-based medicine cannot distinguish between causes and effects. The traditional theory of polygenic diseases states that complex diseases are determined by a combination of genetic and environmental factors, emphasizing the important connection between genetic factors and diseases. Therefore, in biomedicine, much effort is devoted to genetic testing. However, statistical associations only indicate correlation, which does not prove causation [8]. From the perspective of etiological diagnoses, conclusions may differ. For example, genetic factors are highly correlated with skin color, and the incidence of skin cancer in individuals with medium to dark skin is much lower than in those with light skin. However, ultraviolet radiation can be a fundamental cause of skin cancer. Genetic factors increase tumor liability, but they are not the etiologies. Earlier genetic studies estimated the heritability of schizophrenia to be as high as 80%; however, analyses based on DNA data suggested that it is less than 3%, raising the question of "missing heritability." [9,10]
Natural selection has eliminated lineages with low environmental fitness. Genetic diseases of reproductive origin are relatively uncommon. Many de novo alterations in chromosome structure and number result in embryonic lethality. Monogenic diseases are uncommon, and digenic combinations are extremely rare [11]. Moreover, heritability in statistical models may include genetic and cultural transmission inheritance; however, psychological behavior is greatly influenced by the environment. It is difficult to fully distinguish between genetic and environmental influences. As a result, genes are sometimes falsely credited for the effects of the environment [9].
To address these limitations of biology and statistics in modern medicine, this study applied physical modeling to establish a conceptual model. The aim was to explain cancer from a novel perspective and to provide a new paradigm for its treatment.
2. Methods
Physical modeling is an important method in physics research. By abstracting away secondary factors and focusing on primary determinants, physical modeling simplifies complex real-world problems into more comprehensible scenarios. Modeling can help researchers gain a deeper understanding of the essence and governing laws of phenomena, predict and interpret experimental results, and guide engineering practice and technological innovation. In this study, a conceptual model of the human organism was established using physical modeling. The model regarded the human body as a whole, and ignored the complex intercellular signaling pathways by acknowledging the high orderliness of living organisms. Meanwhile, the model weakened the impact of biological classification of somatic cells by emphasizing the functional role of the immune system. Given the complexity of phenomena in the life and social sciences, observational data often lack the precision required for quantitative physical modeling. Consequently, this study prioritizes the development of a conceptual framework over a quantitative mathematical model at this stage.
3. Model Description and Implications
3.1. Model Assumptions and Related Concepts
(i) There are no verifiable genetic-material abnormalities of reproductive origin. This model primarily addresses non-genetic diseases.
(ii) Given a suitable (micro) environment, cells can replicate and differentiate correctly; likewise, the human body can develop normally in a suitable external environment.
(iii) Mutated, aged, and dead cells that arise spontaneously can be effectively eliminated by a normal immune system. In the context of this model, the immune system is regarded as a functional entity without distinguishing specific cellular subtypes.
(iv) The whole organism is highly ordered (i.e., in a healthy state) prior to the impact of adverse exogenous factors.
(v) Key concepts related to the model are summarized in Table 1.
3.2. Model Establishment
In ecology, the environment refers to everything surrounding a given biological unit, which may be a single entity or a collective. By analogy, if each somatic cell is considered an independent entity, then the human body constitutes a complex and highly ordered multicellular society. Additionally, there are many physiological barriers inside and outside the human body. These barriers isolate the internal environment from the external one, and protect vital organs from the impact of changes in the internal environment. Based on this notion of a collection of living cells, barriers, and the environment, the human body can be partitioned into several relatively independent regions to form the conceptual model shown in Figure 1.
When analyzing with this model, the following aspects should be noted: (i) Areas that communicate with the external environment, such as the lungs and intestine, or areas having barriers due to differences in cellular genotype, such as the testes and placenta, will be considered independent from the internal environment. (ii) Psychological research indicates that psychological phenomena arise from objective reality. Without external stimuli, the human brain does not generate psychological activity independently. Social reality has a decisive constraining effect on human psychology. Therefore, this model classifies the effects of psychological and behavioral factors as exogenous, an approach analogous to that adopted in certain pathophysiological frameworks.
4. Discussion
4.1. Model Analysis
4.1.1. Pathogenic Pathways of Exogenous Factors
Notably, many modifiable risk factors have been proven to cause cancer [12]. Based on known etiologies, the pathogenic pathways of exogenous factors are delineated in Figure 2A.
Barrier contact route: (i) Physicochemical factors: Coal tar, for instance, can directly cause cancer, while tobacco is the principal cause of lung cancer [1,13]. (ii) Biological factors: An example of this is an infection with Helicobacter pylori (Figure 2B). Chronic H. pylori infection is considered the principal cause of noncardia gastric cancer [1]. Chronic inflammation may induce genomic damage, which is closely related to the occurrence and development of tumors [14].
Non-barrier contact route: (i) Physicochemical factors: Many environmental physical factors exert significant adverse effects on the immune system. For example, the DNA and nuclear membrane of cells are the prime targets of ionizing radiation, especially in the thymus. Low-dose ionizing radiation may permanently impair immune fitness and thereby accelerate immune senescence [15]. (ii) Psychosocial factors: Adverse stimulation of the nervous system can cause changes in various systems throughout the whole body by affecting the thalamus, hypothalamus, and brainstem, leading to functional disorders of the body (Figure 2C). Acute and chronic stress can significantly alter the immune response [16,17]. (iii) Behavioral factors: Sedentary behavior, for instance, is associated with increased body fat and parallels the increased prevalence of multiple chronic diseases [18]. Night shift work also increases risk for many kinds of chronic diseases [19]. Malnutrition is the primary cause of human immune suppression, while overnutrition, such as obesity and high cholesterol, also exerts adverse effects on the immune system [20,21,22]. Although the consequences of adverse behavioral habits may partially overlap with adverse barrier contact (such as tobacco smoking leading to increased exposure to chemical carcinogens), this pathway primarily underscores the role of individual agency and choice.
4.1.2. Uncovering the Mysteries of the Tumor
As correlation alone does not establish causation, only those diseases with a proven causal link to abnormalities of reproductive origin are defined as typical genetic diseases in this study. Examples of such conditions include the trisomy 21 syndrome and Huntington's disease, which are caused by abnormalities in fertilized eggs. Research shows that immune responses decrease with aging, contributing to the increased incidence of chronic diseases [23]. However, aging does not necessarily imply disease, and tumors can occur at any age. In addition, immune immaturity in children should be considered in the context of exogenous pathogenic factors and is not, by itself, an etiology of childhood cancer; otherwise, it would contradict the premise (model assumptions) of this study. Furthermore, modern humans have a unique ability to control their living environments, and tumors are currently regarded as chronic diseases that can occur in any habitable location worldwide. Therefore, this study does not consider immune senescence due to aging, immune immaturity in children, or normal seasonal and geographical variations in the natural environment in its discussion of tumorigenesis and treatment.
According to the medical genetic theory, cancers are approximately divided into two types: inherited cancer-predisposing syndromes only involve several rare cancers, while non-syndromic tumors include most common tumors. The former are termed genetic tumors, while the latter—traditionally viewed as complex diseases—are designated non-genetic tumors and will be discussed later.
Tumors are characterized by abnormal cellular proliferation and are usually clonal (a feature commonly studied in oncology). Since normal immune surveillance eliminates abnormal cells, their persistence implies a concomitant failure of immune surveillance—a core tenet of tumor immunology (Figure 3A). Within this model, which abstracts away tissues and organs, the immune system is consequently defined solely as the collective of immune cells and molecules. Deficient immune surveillance implies abnormalities in the number or function of immune cells and/or molecules. Immune molecules are constituents of the internal environment; thus, abnormalities in these molecules indicates a dysregulated internal environment. As for immune cells, abnormalities may arise from sporadic mutations, radiation damage, or a disordered immune microenvironment. Given that: (i) The frequency of nuclear DNA mutations is generally low, and sporadic mutations are eliminated by surveillance mechanisms; (ii) the origin and differentiation sites of the principal immune cells (including the bone marrow, thymus, spleen, and lymph nodes) do not directly contact the external environment and can only be accessed through bodily fluids. It follows that, barring direct DNA damage, the emergence of numerous abnormal immune cells signifies dysregulation of the internal environment, irrespective of its detectability by current assays. Hematological malignancies, being intrinsically linked to immune dysfunction, exhibit distinctions from solid malignancies; however, the underlying driver of deranged cellular proliferation remains consistent. Moreover, through organism-environment interactions, radiation-generated abnormal or immune cells perturb the internal environment, which in turn induces further dysfunction in immune cells, creating a feedback loop. The carcinogenic effect of radiation typically manifests after a latent period of several years. This latency is likely attributable to the robust homeostasis of the normal internal environment, which temporarily constrains the proliferative expansion of abnormal cells and the pathological remodeling of the microenvironment. This dynamic process is illustrated in Figure 3B, and a parallel logic can be applied to the analysis of intracranial tumors.
Normal living organisms are highly ordered. They adapt to their environment, possess multiple internal mediating and reparative mechanisms, and feed on negative entropy [24]. This implies that, aside from the sporadic survival of abnormal cells during immunocompromised periods, normal living organisms (including individual cells) are unlikely to actively cause disease until they can no longer resist the universal increase in entropy or encounter cellular replicative senescence. If living organisms are proven to inevitably cause disease in the absence of these factors, such diseases would correspond to typical genetic diseases. The self-repairing ability of living organisms, which traditional medicine repeatedly emphasizes but modern medicine sometimes fails to acknowledge, also explains some rare self-healing phenomena [25,26] observed in complex diseases. These rare self-healing phenomena are similar to the reversal of reversible cell damage once the causative factor has been removed.
From this analysis, the model yields a central deduction: adverse exogenous factors, via distinct pathways and mechanisms (Figure 2, A to C), induce disorders in the internal environment—either locally or systemically—or cause cellular damage that secondarily disrupts the internal environment, ultimately leading to immune abnormalities. The emergence and persistence of tumor cells can result from sporadic mutations or exposure to carcinogens, coupled with concurrent immune abnormalities. To sum up, the survival of somatic mutations in non-genetic malignant tumors results from immune deficiency. When aging and immune immaturity are not considered, and the essential attribute of normal life points towards order and repair, the states of non-genetic tumor result from the toxic effects of adverse exogenous factors. They represent a state of mutual adaptation among abnormal clones, immune cells, and the dysregulated internal environment, which is similar to biological evolution and adaptation occurring at the cellular level. This inference aligns with the evolutionary theory of cancer [14].
4.1.3. Difference Between Benign and Malignant Tumors
A tumor can be analogized to an aberrant, ectopic organ or system within the body (Figure 3A). The fundamental distinction between benign and malignant tumors lies in the pathological influence the abnormal mass exerts on the internal environment or the organism as a whole. Consequently, key determinants of cancer risk collectively include: the number of abnormal cells, their proliferation rate, anatomical location, secretory capacity, and encapsulation status. Furthermore, the degree of tumor differentiation often reflects the severity of dysregulation in the local or systemic internal environment and is therefore strongly associated with clinical prognosis.
4.1.4. Convergence with Traditional Medicine
Since both abnormal and immune cells adapt to a dysregulated internal environment, restoring homeostasis may arrest the proliferation of malignant clones while gradually restore immune competence. This rationale provides a scientific foundation for traditional Chinese medicine principles such as promoting "equilibrium," "harmonizing yin and yang," and enabling patients to "survival with cancer." [27]
4.2. Model Prediction: Cancer Treatment Framework
In the following section, pathogenic pathways of exogenous factors (Figure 2A) are integrated with the established disease model (Figure 3A) to propose a treatment framework for non-genetic malignant tumors (excluding intracranial tumors). This framework primarily addresses three aspects: (i) management of the resultant pathophysiological state, (ii) identification and intervention against the underlying etiological factors, and (iii) psychosocial support implemented both before and after diagnosis as a preventive and adjuvant measure.
4.2.1. Management of the Resultant Pathophysiological State
Human medicine has developed considerable expertise in the following areas: (i) Elimination of abnormal clones: This is a well-established strength of modern medicine, such as removing solid masses using surgery, inducing remission of hematological malignancies and using targeted drugs with minimal side effects for highly malignant tumors. However, given that the mysteries of life are not yet fully understood, the goal of tumor removal should be balanced with preserving organ function whenever possible. (ii) Homeostatic reconstitution: Studies have shown that a major obstacle in the immunotherapy used against solid tumors is the immunosuppressive environment [28]. Therefore, intervention strategies for the internal environment must become an important part of treatment. These should include, but are not limited to, the regulation of whole-body balance using traditional medicine (such as traditional Chinese medicine, Ayurvedic medicine, and Unani medicine [29,30,31]), plasma exchange, lymphoplasmapheresis, and semi-whole blood exchange [32,33,34] (Ongoing clinical trial: NCT06177561). It is noteworthy that semi-whole blood exchange is an emerging technology in transfusion medicine. It has shown considerable potential in treating many traditionally complex diseases and has recently been associated with remarkable clinical outcomes [35,36,37]. These findings, however, represent preliminary clinical observations of an emerging technology; robust evidence from large-scale trials is still required. (iii) Immune reconstitution: Patients can expect natural recovery after homeostasis has been restored. Additionally, hematopoietic stem cell transplantation (HSCT) is considered an approach to rebuilding immunity, primarily used in hematological malignancies. It is not routinely recommended for most solid tumors; however, it should also be noted that, without interfering with homeostasis (even in cases where the conditioning regimens for HSCT may temporarily destabilize physiological balance) and underlying etiologies, numerous studies show that HSCT in breast cancer improves progression-free-survival (PFS) and may represent a viable clinical option for select patients with specific biological characteristics [38]. (iv) Supportive care for physiological resilience: This essential component includes targeted management of cancer- and treatment-related symptoms, coupled with evidence-based nutritional support [39]. The goal is to optimize the host's internal environment, enhance tolerance to therapies, and facilitate overall recovery.
4.2.2. Identification and Intervention Against the Underlying Etiological Factors
Although many cancers are currently considered incurable diseases in modern medicine, they are also considered preventable. However, some complex diseases may have multiple etiologies, and it may be difficult for physicians to predict patient behavior. Patients may conceal certain preferences, some etiologies may not be effectively identified by either doctors or patients, and some etiologies may even stem from social customs. Furthermore, sometimes patients understand the possible adverse effects of their lifestyle choices, but do not wish to implement changes. One such example is the smoking rate, which remains high despite the label "Smoking may lead to lung cancer" being clearly printed on cigarette packs. Another example includes lack of sleep and consumption of unhealthy foods. While most people know these habits are unhealthy, many remain unwilling to change their lifestyles. Curing cancer is, therefore, a more complex endeavor than can be addressed by medical interventions alone. In addition, immune deficiency of the patients with a same type of cancer may result from different etiologies. If the focus remains solely on correcting physiological disorders without addressing the underlying specific etiologies, disease relapse is highly likely. The challenges described above require clinical oncologists to collaborate with multidisciplinary clinical experts to strengthen the etiological diagnoses for each cancer patient, especially in terms of psychological and behavioral factors, and to precisely tailor therapies based on the underlying specific etiologies: (i) Interventions for physicochemical and biological factors: These include treatment of chronic infectious lesions, and avoidance of chemical carcinogens and radioactive sources [40,41,42]; (ii) Interventions for psychological and behavioral factors: These include cognitive adjustment, behavioral (habit) adjustment, and maintenance of a healthy lifestyle, such as maintaining a healthy weight by following a healthy diet; avoiding smoking and alcohol consumption; engaging in appropriate physical activity; adhering to a regular and restorative sleep schedule; managing prolonged mental stress; and establishing harmonious interpersonal relationships and social support networks [43,44,45,46,47,48,49,50].
4.2.3. Psychosocial Support Implemented Both Before and After Diagnosis
Beyond biological interventions, psychosocial factors play a critical role in cancer care. In the family and sociocultural models employed in abnormal psychology, psychological disturbances are not merely disorders residing within the individual, but can also represent reactions to dysfunction within the family system or broader societal malaise. Therefore, in addition to patient evaluation, we also need to evaluate the patient’s family and even society as a whole using the following approaches: (i) Intervention for cancer patients and their families: These include dealing with cancer-related mental disorders, avoiding post-traumatic stress disorder, and mitigating the financial and time toxicity arising from cancer treatment and healthcare system engagement[51,52,53,54]; (ii) Societal-level interventions: These include optimizing the medical system, eliminating cancer-related fear and discrimination, developing robust support networks and psychosocial oncology services, promoting healthy lifestyles, preventing infectious diseases, pursuing environmental protection, and fostering societal goals that encompass both material and spiritual well-being [55,56,57,58,59,60,61].
In the future, precise etiological diagnosis and tailored intervention for each cancer patient should become a primary objective not only for direct care providers (e.g., physicians, clinical psychologists, nutritionists) but also for public health policymakers, patients, families, and sociologists.
5. Conclusion
In this study, multidisciplinary knowledge was utilized to construct a conceptual model suitable for the human body. The model meets the requirements of both reductionism in modern medicine and holism in traditional medicine.
This model was then used to provide a coherent explanation for fundamental questions in tumorigenesis. Suggestions were also provided for a cancer treatment framework with value including: (i) management of the resultant pathophysiological state, (ii) identification and intervention against the underlying etiological factors, and (iii) psychosocial support implemented both before and after diagnosis. Distinguished from existing frameworks like the evolutionary theory of cancer and the biopsychosocial model (BPSM), the proposed model uniquely integrates a physics-informed, holistic perspective. It centers on two core tenets: the inherent high orderliness of living systems and the pivotal functional role of the immune system in tumor formation and treatment. Furthermore, it explicitly links psychosocial and behavioral factors to immune regulation. By transcending the limitations of over-categorization in biological thought, this approach provides a coherent framework capable of bridging therapeutic concepts from both modern and traditional medicine. As a conceptual framework, the model prioritizes qualitative logical reasoning over quantitative mathematical formulation at this stage. Nevertheless, its graphical representation provides a robust and sufficient basis for analyzing overarching patterns of cancer occurrence and for deriving principled clinical treatment frameworks. Ultimately, the translational value and clinical efficacy of this integrative approach must be, and await, rigorous empirical validation.
Despite these considerations, under reasonable assumptions, the model exhibits logical rigor and internal consistency. Its predictions are empirically verifiable and align not only with modern medical research but also with traditional medical concepts. Additionally, the predictive and systematic treatment modalities derived from this model are fully consistent with BPSM. It is particularly noteworthy that the predictive cancer treatment framework in this study incorporates recent developments in clinical hemato-immunology (including many emerging techniques in blood transfusion, such as lymphoplasmapheresis combined with HSCT or semi-whole blood exchange) to the cancer treatment plan in BPSM, which can rapidly restore homeostasis in the internal environment and rebuild immunity. These advances hold significant potential for enhancing the prospects of cancer cure. Although large-scale clinical trials to validate the entire cancer treatment framework may require considerable time, this practical constraint does not reflect a deficiency in the model itself. The proposed model offers a novel intellectual framework to refocus clinical attention on etiological diagnosis of cancers, and may facilitate the integration of the medical treatment concepts from both modern and traditional medicine to advance cancer management worldwide—pending rigorous clinical validation.
Acknowledgments
The author would like to thank LetPub (www.letpub.com.cn) for linguistic assistance and pre-submission expert review.
Conflicts of Interest statement
The author has no competing interests to declare.
Abbreviations
IARC, International Agency for Research on Cancer; BPSM, biopsychosocial model; HSCT, hematopoietic stem cell transplantation; PFS, progression-free-survival.
References
- Bray F, Laversanne M, Sung H, et al. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2024;74(3):229-263. [CrossRef]
- Rejeski K, Subklewe M, Locke FL. Recognizing, defining, and managing CAR-T hematologic toxicities. Hematology Am Soc Hematol Educ Program. 2023;2023(1):198-208. [CrossRef]
- Duncan CN, Bledsoe JR, Grzywacz B, et al. Hematologic Cancer after Gene Therapy for Cerebral Adrenoleukodystrophy. N Engl J Med. 2024;391(14):1287-1301. [CrossRef]
- Engel GL. The need for a new medical model: a challenge for biomedicine. Science. 1977;196(4286):129-136. [CrossRef]
- Ahmad W, Sofi G, Alam MA, et al. Understanding Holism in the light of principle underlying practice of Unani Medicine. Rev Environ Health. 2022;37(2):189-199. [CrossRef]
- Fan D. Holistic Integrative Medicine Declaration. Front Med. 2024;18(5):938-940. [CrossRef]
- Světlák M. Integrative medicine in oncology - between science, ideology, and pragmatism. Klin Onkol. 2025;38(4):264-269. [CrossRef]
- Savage N. Why artificial intelligence needs to understand consequences. Nature. 2023. [CrossRef]
- Conley D, Fletcher J. The Genome Factor: What the Social Genomics Revolution Reveals about Ourselves, Our History, and the Future. Princeton: Princeton University Press 2017.
- Maher B. Personal genomes: The case of the missing heritability. Nature. 2008;456(7218):18-21. [CrossRef]
- Neuhofer CM, Prokisch H. Digenic Inheritance in Rare Disorders and Mitochondrial Disease-Crossing the Frontier to a More Comprehensive Understanding of Etiology. Int J Mol Sci. 2024;25(9). [CrossRef]
- Islami F, Marlow EC, Thomson B, et al. Proportion and number of cancer cases and deaths attributable to potentially modifiable risk factors in the United States, 2019. CA Cancer J Clin. 2024;74(5):405-432. [CrossRef]
- Lipsick J. A History of Cancer Research: Carcinogens and Mutagens. Cold Spring Harb Perspect Med. 2021;11(3). [CrossRef]
- Liu W, Deng Y, Li Z, et al. Cancer Evo-Dev: A Theory of Inflammation-Induced Oncogenesis. Front Immunol. 2021;12:768098. [CrossRef]
- Lumniczky K, Impens N, Armengol G, et al. Low dose ionizing radiation effects on the immune system. Environ Int. 2021;149:106212. [CrossRef]
- Dragoş D, Tănăsescu MD. The effect of stress on the defense systems. J Med Life. 2010;3(1):10-18.
- Zefferino R, Di Gioia S, Conese M. Molecular links between endocrine, nervous and immune system during chronic stress. Brain Behav. 2021;11(2):e01960. [CrossRef]
- Henson J, De Craemer M, Yates T. Sedentary behaviour and disease risk. BMC Public Health. 2023;23(1):2048. [CrossRef]
- Korf HW, Bittner N, Caspers S, et al. Impact of artificial light at night and night shift work on brain functions and metabolism. Gen Comp Endocrinol. 2025:114822. [CrossRef]
- Morales F, Montserrat-de la Paz S, Leon MJ, et al. Effects of Malnutrition on the Immune System and Infection and the Role of Nutritional Strategies Regarding Improvements in Children's Health Status: A Literature Review. Nutrients. 2023;16(1). [CrossRef]
- Fang X, Henao-Mejia J, Henrickson SE. Obesity and immune status in children. Curr Opin Pediatr. 2020;32(6):805-815. [CrossRef]
- Saad EE, Michel R, Borahay MA. Cholesterol and Immune Microenvironment: Path Towards Tumorigenesis. Curr Nutr Rep. 2024;13(3):557-565. [CrossRef]
- Fulop T, Witkowski JM, Pawelec G, et al. On the immunological theory of aging. Interdiscip Top Gerontol. 2014;39:163-176. [CrossRef]
- Schrödinger E. What is Life? the Physical Aspect of the Living Cell. Cambridge: Cambridge University Press 1944.
- Lau KL, Ferozepurwalla Z. Spontaneous regression of head and neck squamous cell carcinoma: a systematic review and meta-analysis of case reports. J Laryngol Otol. 2024;138(11):1054-1060. [CrossRef]
- Li S, Yu FH, Yanfen S. A Case of Spontaneous Remission of Non-Hodgkin's Lymphoma in the Lung. Clin Case Rep. 2025;13(3):e70265. [CrossRef]
- Fu R, Li J, Yu H, et al. The Yin and Yang of traditional Chinese and Western medicine. Med Res Rev. 2021;41(6):3182-3200. [CrossRef]
- Dagar G, Gupta A, Masoodi T, et al. Harnessing the potential of CAR-T cell therapy: progress, challenges, and future directions in hematological and solid tumor treatments. J Transl Med. 2023;21(1):449. [CrossRef]
- Hung YL, Leung SS, Chiu SP, et al. Perceptions about traditional Chinese medicine use among Chinese breast cancer survivors: A qualitative study. Cancer Med. 2023;12(2):1997-2007. [CrossRef]
- Deshmukh V, Chiplunkar S, Sardeshmukh S, et al. Selective Adjuvant Ayurvedic Treatment Modulates Immune Response and Oxidative Stress in a Patient with Carcinoma of the Pyriform Fossa, Undergoing Radiotherapy: A Case Study. Complement Med Res. 2024;31(6):577-591. [CrossRef]
- Pandey L, Pasricha R, Joseph D, et al. Use of complementary and alternative medicine among patients with cancer in a sub-Himalayan state in India: An exploratory study. J Ayurveda Integr Med. 2021;12(1):126-130. [CrossRef]
- Rony R, Shokrani A, Malhi NK, et al. Therapeutic Plasma Exchange: Current and Emerging Applications to Mitigate Cellular Signaling in Disease. Biomolecules. 2025;15(7). [CrossRef]
- Zheng B, Li A, Chen Y. Effetive Observation of the Lymphocyte Clearance and Plasmapheresis to the Multiple Myeloma [Article in Chinese]. Cancer Research on Prevention and Treatment. 2004;31(8):501-503.
- Li B. Innovative application of blood transfusion therapy in clinical difficult, critical and rare diseases [Article in Chinese]. China Medical News. 2022;37(23):13. [CrossRef]
- The First Affiliated Hospital of Guangxi Medical University, 2025: https://www.gxmuyfy.cn/news/newsyljs/29957.html.
- Zhejiang Provincial People's Hospital Bijie Hospital, 2025: http://m.bjhospital.net/newscenter_lcyx/2025/7ax193by.html.
- Gansu Provincial Central Hospital, 2025: https://www.mdweekly.com.cn/m/article/detail?id=56389.
- Greco R, Ruggeri A, McLornan DP, et al. Indications for haematopoietic cell transplantation and CAR-T for haematological diseases, solid tumors and immune disorders: 2025 EBMT practice recommendations. Bone Marrow Transplant. 2025. [CrossRef]
- Wang G, Pan S. Synergistic Effects of Psychological Resilience Training and Nutritional Support on Postoperative Recovery, Nutritional Reconstitution, Sleep Quality, and Long-Term Survival in Gastric Cancer: A Randomized Controlled Trial. Ann Surg Oncol. 2025. [CrossRef]
- Ford AC, Yuan Y, Moayyedi P. Helicobacter pylori eradication therapy to prevent gastric cancer: systematic review and meta-analysis. Gut. 2020;69(12):2113-2121. [CrossRef]
- Abate HM, Bujnowski D, Jowell A, et al. Ubiquitous Environmental Exposures and Risk of Hepatocellular Carcinoma: A Narrative Review. Dig Dis Sci. 2025. [CrossRef]
- Talapko J, Talapko D, Katalinić D, et al. Health Effects of Ionizing Radiation on the Human Body. Medicina (Kaunas). 2024;60(4). [CrossRef]
- Paslaru AM, Plesea-Condratovici A, Moroianu LA, et al. Mind over Malignancy: A Systematic Review and Meta-Analysis of Psychological Distress, Coping, and Therapeutic Interventions in Oncology. Medicina (Kaunas). 2025;61(6). [CrossRef]
- Castro-Espin C, Agudo A. The Role of Diet in Prognosis among Cancer Survivors: A Systematic Review and Meta-Analysis of Dietary Patterns and Diet Interventions. Nutrients. 2022;14(2). [CrossRef]
- Marino P, Mininni M, Deiana G, et al. Healthy Lifestyle and Cancer Risk: Modifiable Risk Factors to Prevent Cancer. Nutrients. 2024;16(6). [CrossRef]
- Zhu C, Ma H, He A, et al. Exercise in cancer prevention and anticancer therapy: Efficacy, molecular mechanisms and clinical information. Cancer Lett. 2022;544:215814. [CrossRef]
- Han C, Li N, Wang X, et al. Sleep disorders in cancer: interactions and intrinsic links. Front Oncol. 2025;15:1535442. [CrossRef]
- Liu Y, Tian S, Ning B, et al. Stress and cancer: The mechanisms of immune dysregulation and management. Front Immunol. 2022;13:1032294. [CrossRef]
- Nisiraiou A, Bozas A, Kyrou D, et al. Post-Traumatic Growth in Adult Cancer Survivors: A Scoping Review of Psychological Factors, Predictors, and Interventions. Int J Psychol. 2025;60(5):e70097. [CrossRef]
- Sezgin MG, Bektas H. Strength in Shared Experiences: A Meta-Synthesis of Qualitative Studies on Peer Support in Haematologic Cancer. Semin Oncol Nurs. 2025:151961. [CrossRef]
- Osmani V, Hörner L, Klug SJ, et al. Prevalence and risk of psychological distress, anxiety and depression in adolescent and young adult (AYA) cancer survivors: A systematic review and meta-analysis. Cancer Med. 2023;12(17):18354-18367. [CrossRef]
- Buciuc AG, Espinel Z, Weber M, et al. Post-Traumatic Stress and Stressor-Related Disorders in Hematological Malignancies: A Review. J Clin Med. 2025;14(17). [CrossRef]
- Kadambi S, Wang Y, Job A, et al. Financial Toxicity in Older Adults With Cancer and Their Caregivers. JCO Oncol Pract. 2025;21(1):92-99. [CrossRef]
- Jing J, Li M, Rui Y, et al. The weight of time: experience of time toxicity among advanced cancer patients and their family caregivers-a qualitative study. Support Care Cancer. 2025;33(10):862. [CrossRef]
- Niraula S. Rethinking prestige and dependency in global oncology. Cancer. 2025;131(18):e70087. [CrossRef]
- Maas A, Westerweel A, Maurice-Stam H, et al. The Prevalence and Associated Factors of Cancer-Related Worries in Adult Survivors of Childhood Cancer: A Systematic Review. Psychooncology. 2025;34(2):e70101. [CrossRef]
- Zhao H, Zhang XW, Li X. Lifestyle factors in hepatocellular carcinoma: From pathogenesis to prognosis. World J Clin Oncol. 2025;16(7):107723. [CrossRef]
- Hu Y, Zhu Y, Lu NH. The management of Helicobacter pylori infection and prevention and control of gastric cancer in China. Front Cell Infect Microbiol. 2022;12:1049279. [CrossRef]
- Leite Dias BR, Vidal Nogueira LM, Leal Ataíde Rodrigues I, et al. Lung cancer associated with natural vegetation cover: spatial analysis in the state of Pará, eastern Brazil. Geospat Health. 2025;20(2). [CrossRef]
- Ruzindana K, Anorlu RI. Global disparities in gynecologic cancer outcomes: A call for action. Int J Gynaecol Obstet. 2025;171 Suppl 1(Suppl 1):210-220. [CrossRef]
- Gonçalves CJ, Almeida AS. The Role of a Spiritual Approach in Patients With Cancer: A Systematic Review. Cureus. 2025;17(8):e89783. [CrossRef]
Figure 1.
A conceptual model of the human body from a life-environment systems perspective. The model conceptualizes the body as a bounded system containing cells and extracellular matrix. Within it, peripheral cells, the central nervous system (CNS), and the thymus are envisioned as distinct entities inhabiting a shared internal environment. The digestive tract is represented as a penetrating tube, whereas the respiratory and urogenital tracts are blind-ended tubes. Owing to the blood-brain and blood-thymus barriers, the CNS and thymus maintain distinct microenvironments (the thymus is modeled analogously to the CNS; annotations omitted for clarity). Blue arrows indicate potential neural connections. (A) Three-dimensional schematic. (B) Two-dimensional schematic.
Figure 1.
A conceptual model of the human body from a life-environment systems perspective. The model conceptualizes the body as a bounded system containing cells and extracellular matrix. Within it, peripheral cells, the central nervous system (CNS), and the thymus are envisioned as distinct entities inhabiting a shared internal environment. The digestive tract is represented as a penetrating tube, whereas the respiratory and urogenital tracts are blind-ended tubes. Owing to the blood-brain and blood-thymus barriers, the CNS and thymus maintain distinct microenvironments (the thymus is modeled analogously to the CNS; annotations omitted for clarity). Blue arrows indicate potential neural connections. (A) Three-dimensional schematic. (B) Two-dimensional schematic.
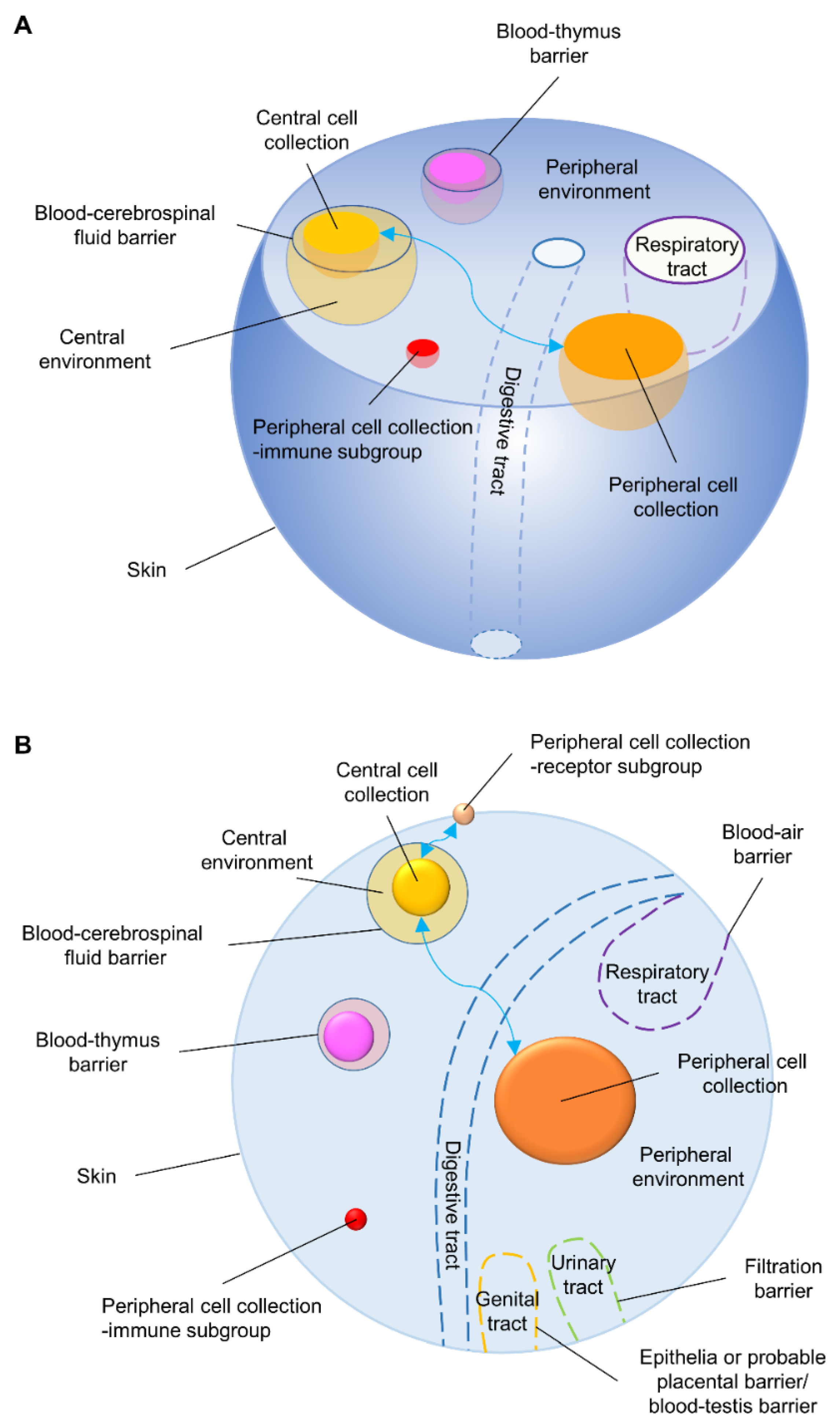
Figure 2.
Pathways of adverse exogenous factors affecting human physiology. (A) General pathways (postnatal stage): Adverse exogenous factors (physical, chemical, biological, psychosocial) can disrupt local or systemic homeostasis via neurohumoral pathways. A key feature is the bidirectional interaction between local lesions and the whole-body state, each influencing the other’s progression. (B) Example: Chronic bacterial infection ( H. pylori ): (i) Oral entry into the digestive tract. (ii) Colonization of gastric mucosal epithelium, altering the local microenvironment to establish chronic infection. (iii) Subsequent local-systemic interaction propagating dysregulation. (C) Example: Psychosocial stress: (i) An external catalyst triggers an emotional response. (ii) This response, mediated via the autonomic nervous system (sympathetic/parasympathetic), hypothalamic-pituitary-adrenal axis, and related pathways, affects endocrine/immune cells and the internal environment through neurohumoral signaling. (iii) The resulting dysregulation interfaces with emerging abnormal cells.
Figure 2.
Pathways of adverse exogenous factors affecting human physiology. (A) General pathways (postnatal stage): Adverse exogenous factors (physical, chemical, biological, psychosocial) can disrupt local or systemic homeostasis via neurohumoral pathways. A key feature is the bidirectional interaction between local lesions and the whole-body state, each influencing the other’s progression. (B) Example: Chronic bacterial infection ( H. pylori ): (i) Oral entry into the digestive tract. (ii) Colonization of gastric mucosal epithelium, altering the local microenvironment to establish chronic infection. (iii) Subsequent local-systemic interaction propagating dysregulation. (C) Example: Psychosocial stress: (i) An external catalyst triggers an emotional response. (ii) This response, mediated via the autonomic nervous system (sympathetic/parasympathetic), hypothalamic-pituitary-adrenal axis, and related pathways, affects endocrine/immune cells and the internal environment through neurohumoral signaling. (iii) The resulting dysregulation interfaces with emerging abnormal cells.
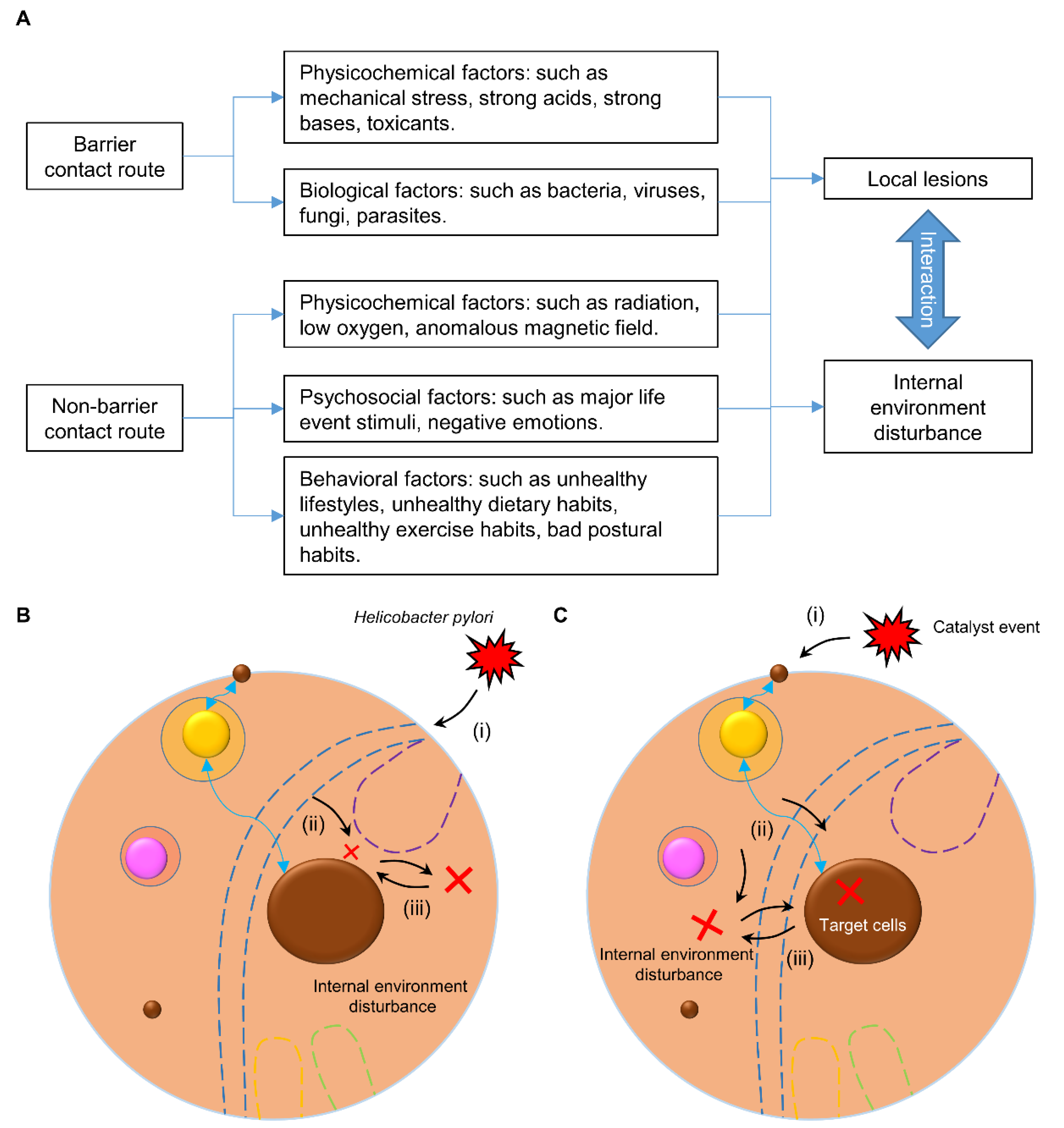
Figure 3.
The established and initial state of non-genetic tumors. (A) Pathological triad: The tumor, as an abnormal cell mass, co-exists with and is sustained by impaired immune surveillance and a dysregulated internal environment. These three components interact reciprocally, establishing a self-sustaining disease state. (B) Initial establishment: This panel illustrates the initial establishment of the pathological triad shown in (A) (highlighted in orange). The minus symbol (-) indicates a component in an abnormal condition.
Figure 3.
The established and initial state of non-genetic tumors. (A) Pathological triad: The tumor, as an abnormal cell mass, co-exists with and is sustained by impaired immune surveillance and a dysregulated internal environment. These three components interact reciprocally, establishing a self-sustaining disease state. (B) Initial establishment: This panel illustrates the initial establishment of the pathological triad shown in (A) (highlighted in orange). The minus symbol (-) indicates a component in an abnormal condition.
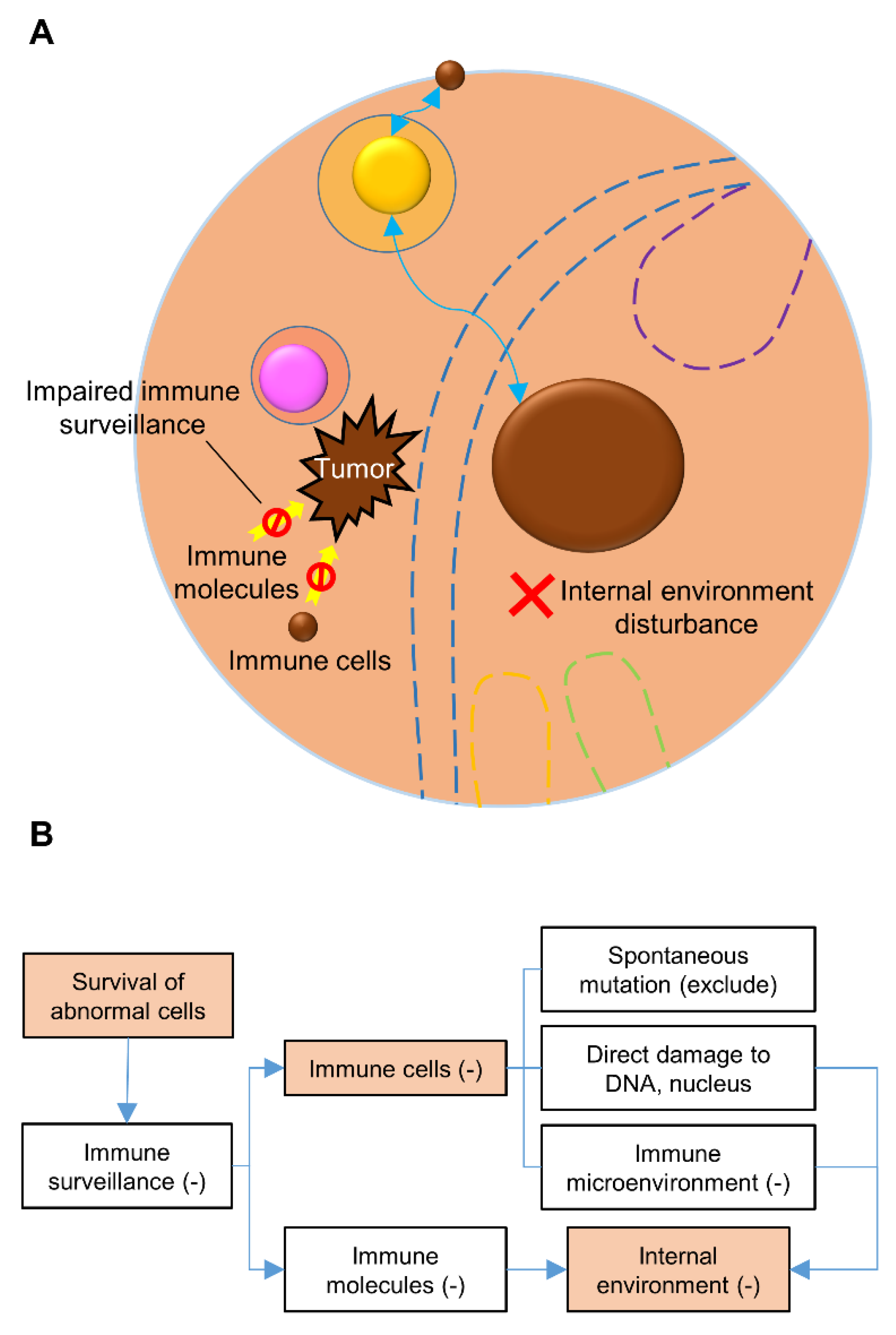

Table 1.
Key concepts and definitions for the physics-informed conceptual model.
| Concept | Definition |
| Protective barrier | Abbreviated as Category 1 barrier. Refers to barriers primarily located at the body surface that isolate the organism from the external environment or protect gametes/zygotes. Examples include the skin, blood-air barrier, mucous-HCO3− barrier, filtration barrier, placental barrier, and blood-testis barrier. |
| Internal barrier | Abbreviated as Category 2 barrier. Refers to barriers located within the body that protect vital organs from fluctuations in the internal environment. The principal examples are the blood-brain barrier and the blood-thymus barrier. |
| Collection of peripheral cells | Refers to the assembly of living cells situated between Category 1 and Category 2 barriers, encompassing both the cells that constitute the barriers and the cells they enclose. |
| Peripheral environment | Commonly referred to as the internal environment. It comprises all extracellular substances located between Category 1 and Category 2 barriers, including fluid components (e.g., plasma, interstitial fluid, lymph) and solid components (e.g., the fibrous elements and the ground substance of the extracellular matrix). |
| Collection of central cells | Refers to the assembly of living cells residing inside the blood-cerebrospinal fluid barrier, excluding the cells that form the barrier structure itself. |
| Central environment | Comprises all extracellular substances located inside the blood-cerebrospinal fluid barrier. |
| Collection of immune cells | Functional designation. Refers to the assembly of living cells within a given environment whose primary roles involve immune defense, surveillance, and homeostasis. This includes, but is not limited to, cell types such as granulocytes, lymphocytes, and monocytes/macrophages. Given the functional complexity and plasticity of the immune system, this model employs an inclusive, function-oriented definition. |
| Collection of immune molecules | Functional designation. Refers to the assembly of soluble mediators within a given environment whose primary functions involve immune signaling, regulation, and effector activities. Examples include immunoglobulins, complement proteins, cytokines, and chemokines; this list is not exhaustive. |
| Collection of receptor cells | Functional designation. Refers to the assembly of living cells within a given environment whose primary function is to detect and transduce external or internal stimuli into biological signals. This includes specialized sensory cells (e.g., photoreceptors, mechanoreceptors) and broader cell populations expressing pattern recognition or signal-receiving molecules; this list is also not exhaustive. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



