Submitted:
02 February 2025
Posted:
04 February 2025
You are already at the latest version
Abstract
Neurodevelopmental disorders (NDDs), such as autism spectrum disorder (ASD) and attention-deficit/hyperactivity disorder (ADHD), and mood disorders (MDs), including major depressive disorder and bipolar disorder, present significant global health challenges due to their high prevalence and profound impact on quality of life. Emerging evidence highlights overlapping neurobiological mechanisms between NDDs and MDs, including shared genetic susceptibilities, neurotransmitter dysregulation (e.g., dopaminergic and serotonergic pathways), neuroinflammation, and hypothalamic-pituitary-adrenal (HPA) axis dysfunction. Environmental factors, such as early-life adversity, further exacerbate these vulnerabilities, contributing to the complexity of their clinical presentation and comorbidity. Functional neuroimaging studies reveal altered connectivity in brain regions critical for emotional regulation and executive function, such as the prefrontal cortex and amygdala, across these disorders. Despite these advances, integrative diagnostic frameworks and targeted therapeutic strategies remain underexplored, limiting effective intervention. This review synthesizes current knowledge on the shared neurobiological underpinnings of NDDs and MDs, emphasizing the need for multidisciplinary research to develop unified approaches for diagnosis and treatment. Addressing these intersections can improve clinical outcomes and enhance the quality of life for individuals affected by these disorders.

Keywords:
neurodevelopmental disorders
; mood disorders
; biological mechanisms
; synaptic impairments
; attention-deficit/hyperactivity disorder
; autism spectrum disorder
; intellectual disability
; learning disorders
; communication disorders
Graphical abstract

Introduction
Neurodevelopmental disorders (NDDs), such as autism spectrum disorder (ASD), attention-deficit/hyperactivity disorder (ADHD), and mood disorders (MDs), including major depressive disorder (MDD) and bipolar disorder, represent significant public health challenges due to their high prevalence and profound impact. Globally, it is estimated that common mental disorders, such as anxiety and depression, affect 17.6% of the population within a 12-month period, with higher prevalence among women and individuals with lower socioeconomic status [1]. Among children and adolescents, NDDs have significant prevalence rates, with ADHD affecting approximately 8.5%, ASD about 2.9%, and specific learning disorders around 6.4%, often accompanied by psychiatric comorbidities like anxiety and depression [2,3]. Additionally, up to 18% of individuals with NDDs exhibit significant genetic alterations, often linked to developmental delays and ASD, emphasizing the need for early and integrated diagnostics [4] .
The relationship between NDDs and MDs is further complicated by overlapping clinical presentations. Symptoms such as emotional dysregulation, impaired executive function, and social difficulties are frequently observed across both groups of disorders. Studies have shown that individuals with ADHD often experience heightened emotional sensitivity and mood instability, which can mimic or overlap with depressive or bipolar symptoms [5]. Similarly, individuals with ASD frequently present with elevated levels of anxiety and depression, raising questions about whether these are comorbid conditions or manifestations of shared underlying mechanisms [6]. Functional impairments in emotional processing have been linked to atypical connectivity patterns in brain regions associated with emotional regulation, further underscoring the complexity of these overlapping symptoms [7].
Recent evidence indicates a significant overlap in the neurobiological mechanisms underlying NDDs and MDs. Shared pathways, such as alterations in dopaminergic and serotonergic systems, neuroinflammation, and genetic susceptibilities, highlight the complex interaction between these disorders. Studies suggest that the regulation of the dopamine D1 receptor can attenuate neuroinflammation, indicating a key role of this system in the progression of symptoms [8]. Additionally, functional variants associated with the serotonergic system, such as in the HTR1A gene, have been linked to an increased risk of motor and psychiatric complications, suggesting a robust genetic interaction between the dopaminergic and serotonergic systems [9]. Advances in neuroimaging studies demonstrate that brain regions such as the prefrontal cortex and amygdala show functional alterations that contribute to the perpetuation of symptoms in both disorders [10].
The role of environmental factors and their interaction with genetic predispositions also warrants attention. Adverse childhood experiences, such as trauma and neglect, have been shown to influence the onset and severity of both NDDs and MDs. For instance, exposure to emotional trauma during childhood has been significantly associated with an increased risk of MDs in the offspring of bipolar disorder patients [11]. Additionally, the interaction between genetic variations in the CRHR1 gene, a gene that encodes the corticotropin-releasing hormone receptor 1, and childhood trauma has been identified as a risk factor for suicidal behaviors in patients with affective disorders, reinforcing the connection between genetic predispositions and early environmental stressors [12]. These experiences can exacerbate underlying neurobiological vulnerabilities, such as dysregulation of the stress response mediated by the hypothalamic-pituitary-adrenal (HPA) axis. Early interventions become essential to mitigate the long-term impacts of these conditions, as childhood trauma exposure has been linked to epigenetic changes, such as the hypermethylation of the Nr3c1 gene, which encodes glucocorticoid receptor that regulates the stress response and is associated with the development of neuropsychiatric symptoms [13].
Despite significant advancements in the understanding of NDDs and MDs as individual entities, the interconnected neurobiological processes between these conditions remain underexplored. This lack of integrative research limits the development of unified diagnostic frameworks and effective therapeutic interventions. For instance, current diagnostic criteria often treat comorbidities as independent conditions, leading to fragmented care and less effective treatment strategies [5]. Moreover, disparities in diagnosis and management, such as those related to socioeconomic status or access to care, exacerbate the individuals’ challenges faced with these co-occurring disorders, as shown in a large-scale study in the United States [14]. Bridging these gaps requires a shift toward interdisciplinary research that combines psychiatry, neurology, and developmental neuroscience. Advances in genomics-informed multidisciplinary approaches have demonstrated promise, particularly in guiding personalized treatment plans and addressing the complexity of NDDs [15].
This article aims to review the shared neurobiological mechanisms of NDDs and MDs, focusing on specific disorders, including ASD, ADHD, and intellectual disabilities. By identifying common pathophysiological mechanisms, this work seeks to inform future research and clinical practices to improve outcomes for individuals affected by these complex and often co-occurring conditions.
Common neurobiological mechanisms between neurodevelopmental disorders and mood disorders
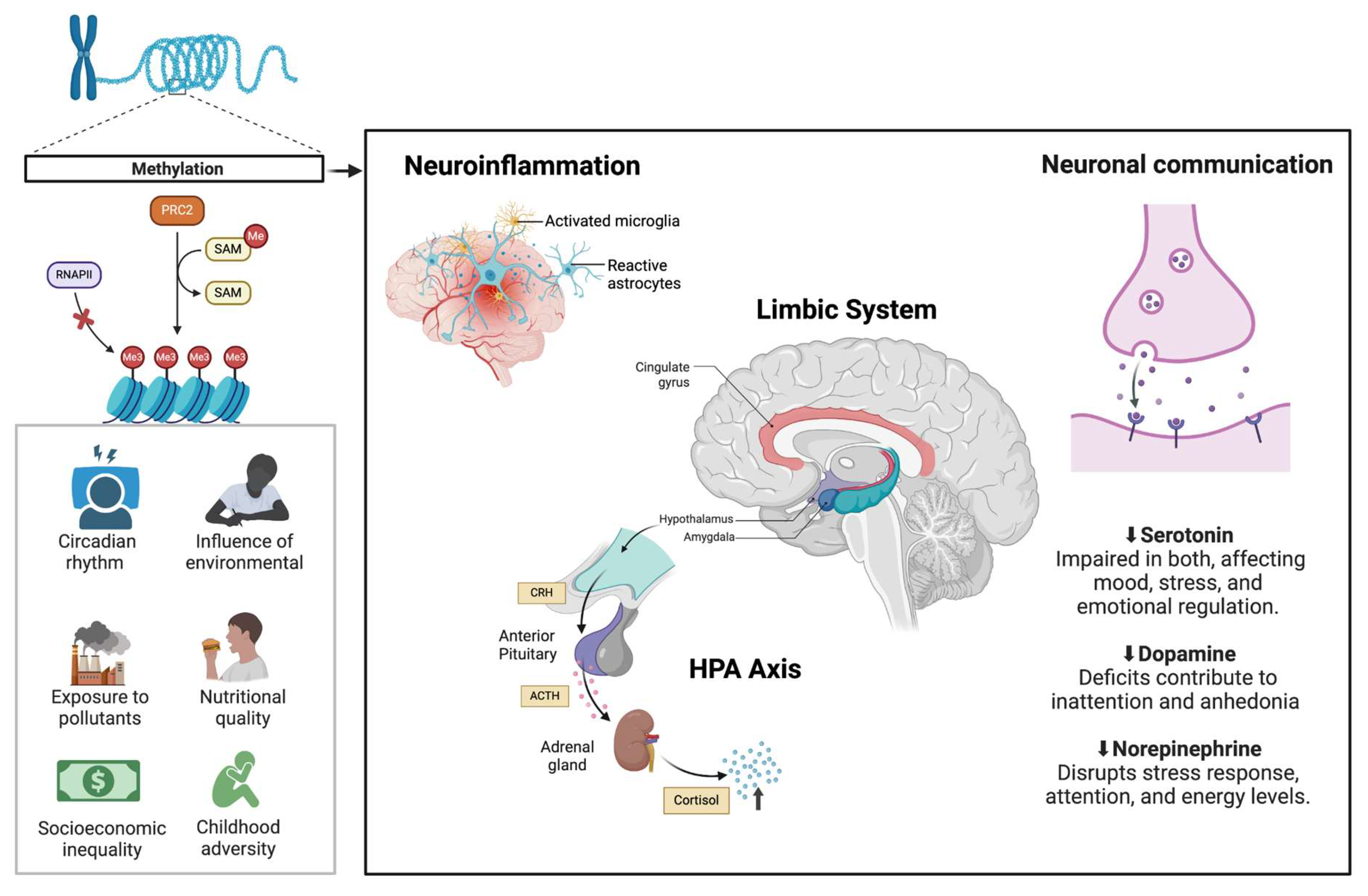
Figure 1. Common neurobiological pathways in NDDs and MDs.
Environmental factors influence DNA methylation, where PRC2 (Polycomb Repressive Complex 2) regulates gene expression by adding Me (methyl groups) via SAM (S-adenosylmethionine), inhibiting RNAPII (RNA Polymerase II) and altering neural function. These changes contribute to neuroinflammation (activated microglia, reactive astrocytes) and HPA axis (Hypothalamic-Pituitary-Adrenal) dysfunction, increasing CRH (Corticotropin-Releasing Hormone), ACTH (Adrenocorticotropic Hormone), and cortisol release. Alterations in the limbic system, including the cingulate gyrus, amygdala, and hypothalamus, impact emotional regulation. Neurotransmitter dysregulation, with reduced serotonin, dopamine, and norepinephrine, impairs mood, attention, and stress response, reinforcing the shared pathophysiology of NDDs and MDs.
Figure 1.
illustrates some common neurobiological mechanisms between neurodevelopmental disorders and mood disorders.
Figure 1.
illustrates some common neurobiological mechanisms between neurodevelopmental disorders and mood disorders.
From the early years of life, NDDs, such as ASDs and ADHDs, significantly impact cognitive and behavioral trajectories, supported by robust genetic and neurobiological foundations. These conditions often overlap with MDs, such as MDD and bipolar disorder, characterized by persistent emotional changes and dysfunctions in neurotransmitter systems [16]. Studies show that NDDs and MDs exhibit common alterations in neural circuits, such as the limbic system and the prefrontal cortex, critical areas for emotional and behavioral regulation [17]. Environmental factors, such as early stress, can also exacerbate manifestations in both categories [18].
Evidence suggests that NDD and MD are not distinct categories but share complex neurobiological foundations. Alterations in mechanisms such as synaptic plasticity, neurotransmitter metabolism, and neural connectivity contribute to developing symptoms in both conditions. Identifying these common points is essential for advancing clinical understanding, as MD symptoms often mask or exacerbate NDD manifestations [19]. For instance, genetic studies highlight the overlap of variants affecting brain development and neurogenesis genes, indicating biological connections between these disorders [18].
Identifying shared neurobiological mechanisms between NDD and MD is crucial to enhancing diagnostic precision and therapeutic interventions. Both types of disorders exhibit alterations in the HPA axis, which regulates stress responses, and dysfunctions in neurotransmitters such as dopamine and serotonin, directly influencing emotional and behavioral processes [17,18]. Studies suggest these changes can be observed in functional brain imaging, revealing abnormal connectivity patterns in NDD and MD [16]. Moreover, neuroinflammation, mediated by immune system alterations, is a common mechanism that aggravates symptoms in both conditions [19].
The overlap of these mechanisms has significant clinical implications. For example, identifying common biological markers can guide the development of targeted therapies that address multiple symptoms simultaneously, such as neurotransmitter modulators or interventions to regulate the HPA axis [18]. Additionally, personalized treatment strategies based on shared mechanisms can prevent the progression of comorbidity and improve patients' quality of life [17].
This neurobiological overlap is also reflected in diagnostic and therapeutic challenges. For example, MD symptoms can hinder the identification of core ASD characteristics. Recent studies highlight the importance of careful differentiation between these conditions to avoid misdiagnoses. According to Wittkopf et al. [20], a comprehensive evaluation that includes emotional and behavioral dimensions is crucial, as proper clinical management depends on accurately identifying the disorders involved.
MDs, such as MDD and bipolar disorder, are characterized by persistent emotional state changes, ranging from episodes of deep sadness to extreme euphoria. These disorders have a complex neurobiological basis, influenced by genetic factors, neurotransmitter alterations, and dysfunctions in brain circuits. Studies show that imbalances in serotonin, dopamine, and norepinephrine systems play central roles in developing and maintaining MD symptoms, directly affecting mood regulation and stress response [16]. Additionally, alterations in the prefrontal cortex, responsible for decision-making and emotional control, and the limbic system, such as the amygdala and hippocampus, are strongly associated with dysfunctional emotional patterns [17].
Genetic factors also significantly contribute to the predisposition to MDs. Polymorphisms in genes related to serotonin transporters and dopamine receptors are frequently identified in individuals with depression and bipolar disorder [18]. These genetic changes, combined with environmental factors such as childhood trauma, can modify synaptic plasticity and neurogenesis, resulting in vulnerabilities to developing these disorders [19].
One main point of convergence between NDDs and MDDs is genetic overlap. Studies reveal that variants in genes associated with brain development regulation, such as those involved in synaptic plasticity and neurotransmitter transport, are shared between NDDs and MDs [16]. These genetic similarities suggest that both disorders may derive from underlying neurobiological processes related to neural development.
Structural and functional brain changes are also commonly observed. For example, reduced hippocampal volume and dysfunctions in prefrontal cortex connectivity with subcortical areas are reported in individuals with NDD and MD [18]. These changes affect emotional and behavioral regulation, contributing to shared symptoms such as impulsivity, emotional dysfunction, and attention deficits.
Another common mechanism is the dysfunction of the HPA axis, which regulates the stress response. HPA axis alterations lead to abnormal cortisol levels, which can negatively impact brain plasticity and exacerbate symptoms of both disorders [17]. Moreover, chronic stress and neuroinflammation, associated with immune system imbalances, are frequently observed in individuals with NDD and MD, suggesting a link between stress responses and shared pathological mechanisms [19].
Autism spectrum disorder
ASD is a neurodevelopmental condition characterized by persistent deficits in social communication and interaction, as well as restricted and repetitive patterns of behavior, interests, or activities. According to the fifth edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-5), the diagnosis of ASD is based on manifestations observed in two main domains: (1) deficits in social reciprocity and nonverbal communication and (2) stereotyped behaviors, restricted interests, and adherence to inflexible routines [21]. The diagnostic complexity of ASD arises from its broad phenotypic variability, with varying degrees of severity and associated manifestations, including psychiatric comorbidities and cognitive alterations. This variability is linked to genetic and environmental factors influencing neurodevelopment from the earliest stages of life [22].
The main signs and symptoms of ASD include deficits in social communication and restrictive and repetitive behaviors, which vary in severity and functional impact among individuals. Difficulties in social communication manifest as challenges in initiating or maintaining interactions, understanding implicit rules of reciprocity, and adjusting behavior to different social contexts. Individuals with ASD often show limited use of gestures and facial expressions, hindering the conveyance of intentions and emotions and compromising the formation of interpersonal relationships [22]. Furthermore, emotional regulation and the presence of alexithymia-difficulty in identifying and expressing emotions—have been identified as critical factors for understanding the emotional impact of ASD, especially in high-functioning cases [23].
From a biological perspective, ASD is associated with complex and multifactorial alterations involving genetic and neurological mechanisms. Genome-wide association Studies (GWAS) have identified genetic variants in genes related to synaptogenesis, neuronal plasticity, and the regulation of neural development, such as SH3 and multiple ankyrin repeat domains 3 (SHANK3), neurexin 1(NRXN1), and chromodomain helicase DNA binding protein 8 (CHD8) [24]. These genetic mutations affect communication between neurons and may impair functional connectivity between different brain regions, particularly in areas associated with socialization and cognition.
Additionally, changes in white and gray matter volume and functional and structural connectivity are frequently observed in individuals with ASD. Functional neuroimaging analyses indicate hyperconnectivity in local circuits and hypoconnectivity in long-distance networks, particularly those involving the prefrontal cortex, superior temporal cortex, and amygdala [25]. These findings suggest an imbalance in neural network integration, contributing to the disorder's behavioral and cognitive characteristics.
Restrictive and repetitive behaviors constitute another central aspect of ASD, including the repetition of words or phrases (echolalia), stereotyped motor movements, and inflexible adherence to routines or patterns. Individuals with ASD may also exhibit intense and unusual interests, such as fixation on numbers or specific objects [21,22]. Sensory alterations, such as hypersensitivity or hyposensitivity to environmental stimuli, are common and can exacerbate repetitive behaviors, impacting social interaction and environmental adaptation [22].
Psychiatric comorbidities are common in ASD and include ADHD, anxiety, obsessive-compulsive disorders (OCDs), and MDs. The presence of these conditions often complicates diagnostic differentiation, as highlighted by Wittkopf et al. [20], who emphasized the importance of carefully evaluating overlapping symptoms to distinguish ASD from mood or anxiety disorders. Emotional challenges, such as difficulties in regulating emotions and irritability, exacerbate the adaptive and social challenges faced by individuals with ASD and their families.
Standardized tools, such as the Autism Diagnostic Observation Schedule (ADOS-2) and the Autism Diagnostic Interview-Revised (ADI-R), are widely used to assess the severity and specific manifestations of ASD. The ADOS-2 evaluates difficulties in social interaction and repetitive behavioral patterns, while the ADI-R allows retrospective analysis of early childhood [22]. This integrative approach is essential for addressing the heterogeneity of ASD, providing a more accurate diagnosis and targeted interventions.
The broad phenotypic variability of ASD, which includes differences in intelligence quotient (IQ), adaptive skills, and emotional problems, poses a challenge in both clinical practice and research [22]. Normative models have been proposed to identify homogeneous subgroups, facilitating the personalization of interventions. This perspective makes therapeutic strategies more practical, focusing on adaptive and functional outcomes [22,23].
Attention-deficit/hyperactivity disorder
ADHD is a neurodevelopmental disorder that has been extensively studied due to its significant impact on individuals' lives. It is characterized by a persistent pattern of inattention and/or hyperactivity-impulsivity, which interferes with the individual's functioning and development. According to the criteria established by the DSM-5, symptoms must be present for at least six months, be inappropriate for the individual's developmental level, and cause significant impairment in two or more settings, such as school, home, or work environments. ADHD is classified into three main subtypes: predominantly inattentive, predominantly hyperactive/impulsive, and combined type, which encompasses characteristics of the previous subtypes. Each subtype presents distinct manifestations, although they often overlap, forming a complex spectrum of symptoms [26].
Among the symptoms related to inattention, difficulties in organizing tasks and activities, frequent memory lapses, and a tendency to lose necessary everyday objects are observed. Hyperactivity symptoms are evident in behaviors such as constant restlessness and difficulty remaining seated for extended periods. Impulsivity manifests in hasty actions, such as interrupting conversations and difficulty waiting one's turn in group situations. When not adequately managed, these behaviors can lead to additional problems in social interactions, academic performance, and family life [27].
The etiology of ADHD is multifactorial, involving genetic, neurobiological, and environmental factors. Studies point to alterations in the prefrontal cortex and the dopaminergic system as central to the executive control difficulties observed in the disorder. These alterations also contribute to the higher prevalence of comorbidities, such as mood and anxiety disorders, frequently reported in individuals with ADHD and ASD [27].
Among psychiatric comorbidities, MDs, such as depression and anxiety, are significantly prevalent in both ADHD and ASD. Individuals with these conditions often exhibit symptoms of irritability, emotional regulation difficulties, and a pronounced vulnerability to stress. This vulnerability is a key characteristic that contributes to the worsening of their clinical conditions, underscoring the urgent need to address this issue. Studies demonstrate that the association between ASD and MDs reflects a complex interaction between neurobiological alterations, HPA axis dysfunctions, and environmental factors [27,28].
Moreover, the risk of depression and suicidal behaviors in individuals with ASD, especially in high-functioning cases, highlights the need for specific and targeted interventions. According to Ruggieri [28], factors such as social isolation, communication difficulties, and emotional overload are among the main elements contributing to the increased risk of suicide in this population. This scenario reinforces the urgency of implementing comprehensive preventive strategies that integrate psychological support, pharmacological interventions, and initiatives focused on social inclusion, aiming to minimize the impact of comorbidities.
In the context of ADHD, pharmacological therapy, particularly the use of stimulants like methylphenidate, plays an essential role in managing core symptoms such as inattention and hyperactivity. Additionally, this type of intervention can bring complementary benefits by helping with emotional regulation, a difficulty often shared between individuals with ADHD and ASD [27].
Finally, the integrated management of ADHD, ASD, and psychiatric comorbidities requires a multidisciplinary approach combining medical interventions, psychotherapies, and educational support. In addition to improving clinical outcomes, strategies that promote social inclusion and address associated risks, such as suicide, are essential to enhance patients' quality of life and emotional well-being [28].
Intellectual disability
Intellectual disability (ID), previously referred to as mental retardation, is a condition that affects approximately 1-3% of the global population, originating before the age of 18 [29]. Defined by deficits in intellectual functioning (e.g., reasoning, problem-solving, planning) and adaptive behavior (e.g., social, conceptual, and practical skills), ID imposes challenges in personal independence and social responsibility [30].
The diagnosis of ID is guided by criteria outlined in the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, Text Revision (DSM-5-TR). These criteria emphasize three core elements: deficits in intellectual functioning, measured through standardized IQ tests, typically with scores below 70; deficits in adaptive behavior, evaluated across conceptual, social, and practical domains; and onset during the developmental period, distinguishing ID from acquired disabilities in adulthood [26].
The etiologies of ID are diverse and can be broadly categorized as genetic, environmental, and multifactorial. Genetic factors include chromosomal abnormalities, such as Down syndrome and Fragile X syndrome, and single-gene mutations, such as Rett syndrome, which are among the most studied genetic causes [31]. Recent advances in whole-genome sequencing have expanded the identification of pathogenic variants associated with ID [32]. Environmental factors include prenatal exposures, such as maternal infections (e.g., rubella, cytomegalovirus) and substance use (e.g., alcohol, drugs), as well as perinatal complications like hypoxia [33]. The interaction of genetic predisposition and environmental factors, including socioeconomic conditions, nutrition, and access to healthcare, also contribute to ID development [34].
Research has uncovered intriguing connections between ID and MDs, suggesting a potential neurobiological link between these conditions. Individuals with ID have a higher prevalence of MDs, such as depression and anxiety, compared to the general population [35,36]. For example, individuals with specific genetic syndromes associated with ID, such as Fragile X syndrome and Down syndrome, have an increased risk of developing MDs [37,38,39]. Neuroimaging studies have also revealed differences in brain structure and function in individuals with ID, which may contribute to the increased vulnerability to MDs [40].
Additionally, environmental factors, such as social isolation, limited access to resources, socioeconomic status, job satisfaction, and stressful life events, may compound the challenges faced by individuals with ID, further increasing their risk of developing MDs [41,42]. Biopsychosocial factors associated with depression and anxiety in older adults with ID include treatable and modifiable factors like mood stabilizer medications and aggressive challenging behavior [43].
Learning disorders
Learning disorders (LDs) are neurobiological conditions that affect 3% to 10% of children and significantly affect the capacity to acquire, retain, and apply information, influencing their academic performance and everyday skills [44]. These conditions encompass a range of disorders, including dyslexia, dyscalculia, and ADHD, each with distinct but overlapping characteristics. Dyslexia, for instance, primarily impairs reading and language-related abilities, while dyscalculia affects mathematical reasoning and number comprehension [45]. ADHD, on the other hand, is characterized by difficulties in maintaining attention, regulating impulses, and managing hyperactivity, which can indirectly impact learning [46].
The etiology of LDs is complex and multifaceted, involving an interplay of genetic, neurological, and environmental factors. Studies identified heritable components linked to specific genes that influence brain function and structure [47,48]. Neurological factors also contribute, with differences in brain regions such as the prefrontal cortex, hippocampus, and parietal lobes observed in individuals with LDs. These differences affect neural connectivity, processing speed, and executive functioning, which are essential for learning and memory [49,50].
Environmental influences, including prenatal exposure to toxins, nutritional deficiencies, and adverse childhood experiences, further compound the risk of developing LDs through epigenetic mechanisms [51]. Educational and social environments can mitigate or exacerbate individuals' challenges with these conditions [52].
Increasing evidence points to a potential relationship between LDs and MDs, suggesting that the two may be linked at a neurobiological level. For example, individuals with LDs often experience co-occurring mental health challenges, including higher rates of depression and anxiety compared to the general population [53,54].
Recent research has identified specific neural networks and brain regions that are typically altered in individuals with LDs, such as changes in the activity and connectivity of brain areas involved in language processing, attention, and executive function [55]. Interestingly, similar neurobiological alterations have also been observed in individuals with MDs, suggesting that there may be overlapping neural pathways and mechanisms that contribute to both types of disorders [53,55].
One potential explanation for the relationship between LDs and MDs is the impact of academic and social challenges on an individual's psychological well-being. Learning difficulties often lead to low self-esteem, frustration, and feelings of inadequacy, particularly in environments where academic performance is heavily emphasized [54]. Social exclusion is another contributing factor; children with ADHD or dyslexia, for instance, may experience bullying or isolation, which can heighten anxiety and depression. This social-emotional stress can further impair cognitive functioning, creating a vicious cycle that exacerbates both learning and MDs [57].
The interplay between stress and LDs is also explained by neurobiological mechanisms, particularly dysregulation of the HPA axis. Chronic stress associated with unmet academic expectations has been shown to impair hippocampal function, critical for memory and learning, and to increase susceptibility to MDs [58]. Furthermore, comorbid MDs, such as depression, can worsen cognitive impairments, creating significant challenges for academic achievement and overall quality of life [59].
Communication disorders
Communication disorders (CDs), such as stuttering, speech sound disorders, aphasia, and social communication disorders, encompass a broad spectrum of difficulties in speech, language, and communication [60]. These challenges can profoundly affect an individual's ability to express themselves and engage in social interactions, often contributing to the development and manifestation of MDs, such as depression and anxiety [61].
The intricate relationship between CDs and MDs has been the subject of intense scientific scrutiny. Neuropsychiatry researchers have sought to unravel the complex neurobiological mechanisms that underlie the compelling connections between these two critical domains of human functioning [62].
Research suggests that the neurobiological mechanisms driving this connection involve processes related to language processing, social cognition, and emotional regulation. For instance, individuals with aphasia may experience frustration and isolation due to their inability to communicate effectively, which can increase their risk of depression [63]. Similarly, children with social communication disorder often face difficulties in peer relationships, which may lead to anxiety over time [64].
A research has highlighted the significant role of synaptic plasticity in the pathogenesis of MDs. Disruptions in the functional and structural connections of the neural circuits that underlie mood regulation have been implicated as a key driver of depressive symptomatology. Various risk factors, including stress-induced physiological changes, can cause these disruptions. Communication disorders have also been linked to alterations in neural connectivity and synaptic function, suggesting a potential shared neurobiological basis between these two conditions [62].
The neurobiology of severe mood and anxiety disorders has been extensively studied, revealing the involvement of multiple neurotransmitter systems and neural networks in regulating mood, emotion, and behavior. The frontal lobe, particularly the prefrontal cortex, has been identified as a key region in these processes. Responsible for executive functions such as decision-making, impulse control, and social behavior modulation, the prefrontal cortex is often impaired in individuals with CDs, which frequently co-occur with mood and anxiety disorders [60].
In addition to these mechanisms, recent studies have pointed to the role of cortical excitability and dopaminergic pathways in the relationship between communication disorders and MDs. Altered excitability, particularly in the motor cortex and language areas, may contribute to speech production and perception difficulties, exacerbating emotional distress and frustration. Furthermore, the dopaminergic system, important in motivation and reward processing, is dysregulated in both CDss and MDs. This dysregulation may impair the individual’s ability to experience positive reinforcement, thus reinforcing feelings of helplessness and anxiety [65,66].
Moreover, emerging research has identified inflammatory processes as an essential factor in the pathophysiology of both MDs and communication difficulties. Chronic inflammation has been implicated in the dysregulation of neurotransmitter systems, such as serotonin and glutamate, which are critical for mood regulation and cognitive functions like language processing. Elevated levels of inflammatory cytokines may disrupt neural communication, particularly in brain regions responsible for speech and emotional regulation [67,68,69].
Diagnostic and therapeutic implications
Advances in diagnostic methodologies have significantly enhanced our understanding of NDDs and MDs. Innovative genetic techniques, such as next-generation sequencing (NGS), have emerged as pivotal tools for identifying genetic variants associated with NDDs and improving diagnostic precision. For instance, studies using targeted gene panels and exome sequencing have demonstrated diagnostic yields of up to 25% in patients with syndromic or nonsyndromic NDDs, underscoring the importance of these technologies in personalized medicine [70,71]. These methods also facilitate early detection, enabling timely therapeutic interventions and better management outcomes.
Integrating neuroimaging technologies, such as functional magnetic resonance imaging (fMRI), has further elucidated the shared neural pathways involved in NDDs and MDs. Research highlights the role of altered connectivity in regions like the prefrontal cortex and amygdala in both conditions, paving the way for novel therapeutic approaches targeting these networks [72]. Moreover, diffusion tensor imaging (DTI) has shed light on white matter abnormalities in NDDs and MDs, emphasizing the importance of understanding brain network dynamics to develop precision diagnostics [73].
In the therapeutic domain, advancements in pharmacological strategies include medications targeting specific neurotransmitter systems. For example, aripiprazole and risperidone have been shown to alleviate symptoms of irritability and aggression in children with ASD [74]. Moreover, selective serotonin reuptake inhibitors (SSRIs) and dopamine receptor modulators are increasingly employed to address overlapping symptoms in MDs and NDDs, demonstrating efficacy in both conditions when appropriately tailored [8]. Research into glutamatergic systems and their modulation through agents such as memantine further illustrates the expanding scope of pharmacological interventions [75].
On the behavioral front, evidence-based interventions like cognitive-behavioral therapy (CBT) and applied behavior analysis (ABA) continue to demonstrate efficacy. CBT has been particularly effective in managing comorbid anxiety and depression in individuals with NDDs, while ABA remains a cornerstone for addressing social and communication deficits in ASD [76]. Additionally, newer approaches incorporating digital health tools, such as mobile applications and wearable devices, are being integrated into therapy regimens to track progress and personalize interventions [77].
Personalized treatment plans informed by genetic and environmental risk profiles are becoming central to targeted interventions. For example, variations in the CRHR1 gene associated with stress-response dysregulation have guided therapies addressing MDs linked to early life trauma [12]. Similarly, pharmacogenomic approaches have helped optimize drug responses, reducing adverse effects and enhancing treatment efficacy in complex cases [78].
Despite these advancements, significant gaps remain in translating diagnostic insights into clinical practice. Barriers such as delayed diagnoses, lack of access to genetic counseling, and socioeconomic disparities hinder the practical application of these advancements [79]. Furthermore, the lack of integration across disciplines like psychiatry, neurology, and genetics often results in fragmented care, underscoring the need for more cohesive diagnostic and therapeutic strategies [80].
Family-based interventions and community support systems have also gained prominence in therapeutic frameworks. Studies suggest empowering caregivers through psychoeducation and resource access significantly enhances treatment adherence and outcomes [81]. Moreover, policy-level changes, such as improving healthcare access and funding for genetic testing, remain essential for bridging gaps in care and ensuring equitable access to these advanced diagnostic and therapeutic options.
Final considerations
The relationship between IDs, LDs, and CDs with MDs highlights complex interactions that contribute to the challenges individuals face in both cognitive and emotional domains.
Research has shown that individuals with ID exhibit higher rates of MDs, such as depression and anxiety, compared to the general population [80]. Genetic factors, such as chromosomal abnormalities and gene mutations, along with environmental influences like prenatal exposure to infections or substances, contribute to the development of ID. Neuroimaging studies further support the theory that structural and functional brain differences in individuals with ID might predispose them to MDs. Moreover, social factors such as isolation and lack of resources may amplify the risks of developing MDs in individuals with ID, creating a cycle of exacerbating cognitive and emotional difficulties.
Similarly, LDs, including dyslexia, ADHD, and dyscalculia, are linked with MDs due to neurobiological alterations that affect brain areas involved in attention, language processing, and executive function. These disorders share overlapping neural pathways with MDs, which are often further complicated by the social-emotional stress individuals experience. Academic struggles and the frustration stemming from them can significantly impact self-esteem, potentially leading to depression and anxiety. Additionally, chronic stress has been shown to affect hippocampal function, thereby impairing cognitive performance and increasing susceptibility to MDs. Both, ASD and ADHD are also frequently associated with mood disturbances, mainly due to the challenges in social interactions, emotional regulation, and executive functioning that these individuals face.
In communication disorders, such as aphasia and social communication disorder, the inability to effectively communicate can lead to frustration, social isolation, and emotional distress, which are significant risk factors for depression and anxiety. The neurobiological mechanisms underlying these disorders involve alterations in neural connectivity and synaptic plasticity, which are also implicated in mood regulation.. Recent studies have highlighted the role of neurotransmitter systems, such as the dopaminergic system, in the overlap between mood and communication disorders, with dysregulation potentially leading to impaired emotional processing and exacerbation of feelings of helplessness. Moreover, inflammatory processes implicated in MDs and communication difficulties may disrupt neurotransmitter systems critical for mood and language processing, suggesting a shared pathophysiological basis for these disorders.
Some neurobiological features common to NDDs and MDs relate to synaptic structure and impairments in local connections and between brain regions involved in MDs and NDDs. These biological processes and mechanisms often underlie genetic polymorphisms or mutations, which direct changes in proteins involved in synaptic structure and connection.
An example of a gene that appears to have structural and functional involvement in circuits related to MDs and NDDs is the protocadherin 17 gene (PCDH17), which encodes a protein of the cadherin family. A study observed a relationship between the PCDH17 and MDs, cognition, and personality. A single-nucleotide polymorphism (SNP) of PCDH17, related to increased transcription, was associated with changes in morphology and reduced density of dendritic spines, reduced amygdala volume, increased MDs, cognitive impairments, and emotional instability [83].
As previously reported, knowledge of genetic characteristics, such as polymorphisms, in addition to the local interaction and between underlying brain structures, both NDDs and MDs, is crucial for advancing the understanding of these disorders and, consequently, for proposing and discovering more effective and common therapeutic strategies for them.
From another angle, the complex interactions between NDDs and MDs highlight the necessity of an integrated approach to treatment. Considering both these conditions' cognitive and emotional dimensions is essential to provide a holistic and effective intervention. By addressing the underlying neurobiological, social, and emotional factors, individuals can have better support in navigating these challenges and improve their overall well-being and quality of life.
Author Contributions
Conceptualization, A.G.B., Z.M.I.; writing—original draft preparation, A.G.B., B.V.S., M.M.; writing-review and editing, M.D.B., Z.M.I. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Data sharing is not applicable to this article as no new data were created or analyzed in this study.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Steel, Z.; Marnane, C.; Iranpour, C.; Chey, T.; Jackson, J.W.; Patel, V.; Silove, D. The Global Prevalence of Common Mental Disorders: A Systematic Review and Meta-Analysis 1980–2013. Int. J. Epidemiol. 2014, 43, 476–493. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.; Zhao, S.; Zhang, M.; Xiang, M.; Zhao, J.; Chen, S.; Wang, H.; Han, L.; Ran, J. Prevalence of Neurodevelopmental Disorders among US Children and Adolescents in 2019 and 2020. Front. Psychol. 2022, 13, 997648. [Google Scholar] [CrossRef] [PubMed]
- Bădescu, G.M.; Fîlfan, M.; Sandu, R.E.; Surugiu, R.; Ciobanu, O.; Popa-Wagner, A. Molecular Mechanisms Underlying Neurodevelopmental Disorders, ADHD and Autism. Romanian J. Morphol. Embryol. Rev. Roum. Morphol. Embryol. 2016, 57, 361–366. [Google Scholar]
- Gillentine, M.A.; Wang, T.; Eichler, E.E. Estimating the Prevalence of De Novo Monogenic Neurodevelopmental Disorders from Large Cohort Studies. Biomedicines 2022, 10, 2865. [Google Scholar] [CrossRef] [PubMed]
- Halvorsen, M.; Mathiassen, B.; Myrbakk, E.; Brøndbo, P.H.; Sætrum, A.; Steinsvik, O.O.; Martinussen, M. Neurodevelopmental Correlates of Behavioural and Emotional Problems in a Neuropaediatric Sample. Res. Dev. Disabil. 2019, 85, 217–228. [Google Scholar] [CrossRef]
- Sesso, G.; Cristofani, C.; Berloffa, S.; Cristofani, P.; Fantozzi, P.; Inguaggiato, E.; Narzisi, A.; Pfanner, C.; Ricci, F.; Tacchi, A.; et al. Autism Spectrum Disorder and Disruptive Behavior Disorders Comorbidities Delineate Clinical Phenotypes in Attention-Deficit Hyperactivity Disorder: Novel Insights from the Assessment of Psychopathological and Neuropsychological Profiles. J. Clin. Med. 2020, 9, 3839. [Google Scholar] [CrossRef] [PubMed]
- Safar, K.; Vandewouw, M.M.; Pang, E.W.; De Villa, K.; Crosbie, J.; Schachar, R.; Iaboni, A.; Georgiades, S.; Nicolson, R.; Kelley, E.; et al. Shared and Distinct Patterns of Functional Connectivity to Emotional Faces in Autism Spectrum Disorder and Attention-Deficit/Hyperactivity Disorder Children. Front. Psychol. 2022, 13, 826527. [Google Scholar] [CrossRef]
- Wang, T.; Nowrangi, D.; Yu, L.; Lu, T.; Tang, J.; Han, B.; Ding, Y.; Fu, F.; Zhang, J.H. Activation of Dopamine D1 Receptor Decreased NLRP3-Mediated Inflammation in Intracerebral Hemorrhage Mice. J. Neuroinflammation 2018, 15. [Google Scholar] [CrossRef] [PubMed]
- Redenšek, S.; Blagus, T.; Trošt, M.; Dolžan, V. Serotonin-Related Functional Genetic Variants Affect the Occurrence of Psychiatric and Motor Adverse Events of Dopaminergic Treatment in Parkinson’s Disease: A Retrospective Cohort Study. J. Pers. Med. 2022, 12, 266. [Google Scholar] [CrossRef]
- Pizzagalli, D.A.; Berretta, S.; Wooten, D.; Goer, F.; Pilobello, K.T.; Kumar, P.; Murray, L.; Beltzer, M.; Boyer-Boiteau, A.; Alpert, N.; et al. Assessment of Striatal Dopamine Transporter Binding in Individuals With Major Depressive Disorder: In Vivo Positron Emission Tomography and Postmortem Evidence. JAMA Psychiatry 2019, 76, 854. [Google Scholar] [CrossRef] [PubMed]
- Koenders, M.A.; Mesman, E.; Giltay, E.J.; Elzinga, B.M.; Hillegers, M.H.J. Traumatic Experiences, Family Functioning, and Mood Disorder Development in Bipolar Offspring. Br. J. Clin. Psychol. 2020, 59, 277–289. [Google Scholar] [CrossRef] [PubMed]
- Sanabrais-Jiménez, M.A.; Sotelo-Ramirez, C.E.; Ordoñez-Martinez, B.; Jiménez-Pavón, J.; Ahumada-Curiel, G.; Piana-Diaz, S.; Flores-Flores, G.; Flores-Ramos, M.; Jiménez-Anguiano, A.; Camarena, B. Effect of CRHR1 and CRHR2 Gene Polymorphisms and Childhood Trauma in Suicide Attempt. J. Neural Transm. 2019, 126, 637–644. [Google Scholar] [CrossRef]
- Vester, A.I.; Hermetz, K.; Burt, A.; Everson, T.; Marsit, C.J.; Caudle, W.M. Combined Neurodevelopmental Exposure to Deltamethrin and Corticosterone Is Associated with Nr3c1 Hypermethylation in the Midbrain of Male Mice. Neurotoxicol. Teratol. 2020, 80, 106887. [Google Scholar] [CrossRef] [PubMed]
- Straub, L.; Bateman, B.T.; Hernandez-Diaz, S.; York, C.; Lester, B.; Wisner, K.L.; McDougle, C.J.; Pennell, P.B.; Gray, K.J.; Zhu, Y.; et al. Neurodevelopmental Disorders Among Publicly or Privately Insured Children in the United States. JAMA Psychiatry 2022, 79, 232. [Google Scholar] [CrossRef] [PubMed]
- Besterman, A.D.; Adams, D.J.; Wong, N.R.; Schneider, B.N.; Mehta, S.; DiStefano, C.; Wilson, R.B.; Martinez-Agosto, J.A.; Jeste, S.S. Genomics-Informed Neuropsychiatric Care for Neurodevelopmental Disorders: Results from A Multidisciplinary Clinic 2024.
- Rai, S.; Griffiths, K.R.; Breukelaar, I.A.; Barreiros, A.R.; Boyce, P.; Hazell, P.; Foster, S.L.; Malhi, G.S.; Harris, A.W.F.; Korgaonkar, M.S. Common and Differential Neural Mechanisms Underlying Mood Disorders. Bipolar Disord. 2022, 24, 795–805. [Google Scholar] [CrossRef] [PubMed]
- Deng, Q.; Hu, L.; Ding, Y.-Q.; Lang, B. Editorial: The Commonality in Converged Pathways and Mechanisms Underpinning Neurodevelopmental and Psychiatric Disorders. Front. Mol. Neurosci. 2023, 16, 1349631. [Google Scholar] [CrossRef] [PubMed]
- Marcolongo-Pereira, C.; Castro, F.C.D.A.Q.; Barcelos, R.M.; Chiepe, K.C.M.B.; Rossoni Junior, J.V.; Ambrosio, R.P.; Chiarelli-Neto, O.; Pesarico, A.P. Neurobiological Mechanisms of Mood Disorders: Stress Vulnerability and Resilience. Front. Behav. Neurosci. 2022, 16, 1006836. [Google Scholar] [CrossRef] [PubMed]
- De Marco, R.L.; Daniel, M.B.N.; Calvo, E.N.; Araldi, B.L. Tea e Neuroplasticidade: Identificação e Intervenção Precoce / Asd and Neuroplasticity: Identification and Early Intervention. Braz. J. Dev. 2021, 7, 104534–104552. [Google Scholar] [CrossRef]
- Wittkopf, S.; Stroth, S.; Langmann, A.; Wolff, N.; Roessner, V.; Roepke, S.; Poustka, L.; Kamp-Becker, I. Differentiation of Autism Spectrum Disorder and Mood or Anxiety Disorder. Autism 2022, 26, 1056–1069. [Google Scholar] [CrossRef]
- Lord, C.; Brugha, T.S.; Charman, T.; Cusack, J.; Dumas, G.; Frazier, T.; Jones, E.J.H.; Jones, R.M.; Pickles, A.; State, M.W.; et al. Autism Spectrum Disorder. Nat. Rev. Dis. Primer 2020, 6, 5. [Google Scholar] [CrossRef]
- Portolese, J.; Gomes, C.S.; Daguano Gastaldi, V.; Paula, C.S.; Caetano, S.C.; Bordini, D.; Brunoni, D.; Mari, J.D.J.; Vêncio, R.Z.N.; Brentani, H. A Normative Model Representing Autistic Individuals Amidst Autism Spectrum Phenotypic Heterogeneity. Brain Sci. 2024, 14, 1254. [Google Scholar] [CrossRef]
- Morie, K.P.; Jackson, S.; Zhai, Z.W.; Potenza, M.N.; Dritschel, B. Mood Disorders in High-Functioning Autism: The Importance of Alexithymia and Emotional Regulation. J. Autism Dev. Disord. 2019, 49, 2935–2945. [Google Scholar] [CrossRef] [PubMed]
- Sanders, S.J.; He, X.; Willsey, A.J.; Ercan-Sencicek, A.G.; Samocha, K.E.; Cicek, A.E.; Murtha, M.T.; Bal, V.H.; Bishop, S.L.; Dong, S.; et al. Insights into Autism Spectrum Disorder Genomic Architecture and Biology from 71 Risk Loci. Neuron 2015, 87, 1215–1233. [Google Scholar] [CrossRef] [PubMed]
- Hahamy, A.; Behrmann, M.; Malach, R. The Idiosyncratic Brain: Distortion of Spontaneous Connectivity Patterns in Autism Spectrum Disorder. Nat. Neurosci. 2015, 18, 302–309. [Google Scholar] [CrossRef] [PubMed]
- American Psychiatric Association Publishing. Diagnostic and Statistical Manual of Mental Disorders: DSM-5.; Fifth edition. Special edition, 2017.; CBS Publishers & Distributors: New Delhi, 2017; ISBN 978-93-86217-96-7.
- Oakley, B.; Loth, E.; Murphy, D.G. Autism and Mood Disorders. Int. Rev. Psychiatry 2021, 33, 280–299. [Google Scholar] [CrossRef]
- Ruggieri, V. [Autism, depression and risk of suicide]. Medicina (Mex.) 2020, 80 Suppl 2, 12–16. [Google Scholar]
- Olusanya, B.O.; Smythe, T.; Ogbo, F.A.; Nair, M.K.C.; Scher, M.; Davis, A.C. Global Prevalence of Developmental Disabilities in Children and Adolescents: A Systematic Umbrella Review. Front. Public Health 2023, 11, 1122009. [Google Scholar] [CrossRef]
- Sappok, T.; Hassiotis, A.; Bertelli, M.; Dziobek, I.; Sterkenburg, P. Developmental Delays in Socio-Emotional Brain Functions in Persons with an Intellectual Disability: Impact on Treatment and Support. Int. J. Environ. Res. Public. Health 2022, 19, 13109. [Google Scholar] [CrossRef] [PubMed]
- Ilyas, M.; Mir, A.; Efthymiou, S.; Houlden, H. The Genetics of Intellectual Disability: Advancing Technology and Gene Editing. F1000Research 2020, 9, 22. [Google Scholar] [CrossRef] [PubMed]
- Lindstrand, A.; Eisfeldt, J.; Pettersson, M.; Carvalho, C.M.B.; Kvarnung, M.; Grigelioniene, G.; Anderlid, B.-M.; Bjerin, O.; Gustavsson, P.; Hammarsjö, A.; et al. From Cytogenetics to Cytogenomics: Whole-Genome Sequencing as a First-Line Test Comprehensively Captures the Diverse Spectrum of Disease-Causing Genetic Variation Underlying Intellectual Disability. Genome Med. 2019, 11, 68. [Google Scholar] [CrossRef] [PubMed]
- Leonard, H.; Montgomery, A.; Wolff, B.; Strumpher, E.; Masi, A.; Woolfenden, S.; Williams, K.; Eapen, V.; Finlay-Jones, A.; Whitehouse, A.; et al. A Systematic Review of the Biological, Social, and Environmental Determinants of Intellectual Disability in Children and Adolescents. Front. Psychiatry 2022, 13, 926681. [Google Scholar] [CrossRef] [PubMed]
- Tchoua, P.P.; Clarke, E.; Wasser, H.; Agrawal, S.; Scothorn, R.; Thompson, K.; Schenkelberg, M.; Willis, E.A. The Interaction between Social Determinants of Health, Health Behaviors, and Child’s Intellectual Developmental Diagnosis 2024.
- Eaton, C.; Tarver, J.; Shirazi, A.; Pearson, E.; Walker, L.; Bird, M.; Oliver, C.; Waite, J. A Systematic Review of the Behaviours Associated with Depression in People with Severe–Profound Intellectual Disability. J. Intellect. Disabil. Res. 2021, 65, 211–229. [Google Scholar] [CrossRef]
- Albuquerque, J.P. Diagnostic Issues in Other Mental Disorders Co-Morbid With Intellectual Disability. Eur. Psychiatry 2023, 66, S22–S23. [Google Scholar] [CrossRef]
- Adams, R.L.; Baird, A.; Smith, J.; Williams, N.; Van Den Bree, M.B.M.; Linden, D.E.J.; Owen, M.J.; Hall, J.; Linden, S.C. Psychopathology in Adults with Copy Number Variants. Psychol. Med. 2023, 53, 3142–3149. [Google Scholar] [CrossRef]
- Lightbody, A.A.; Bartholomay, K.L.; Jordan, T.L.; Lee, C.H.; Miller, J.G.; Reiss, A.L. Anxiety, Depression, and Social Skills in Girls with Fragile X Syndrome: Understanding the Cycle to Improve Outcomes. J. Dev. Behav. Pediatr. 2022, 43, e565–e572. [Google Scholar] [CrossRef] [PubMed]
- Rivelli, A.; Fitzpatrick, V.; Chaudhari, S.; Chicoine, L.; Jia, G.; Rzhetsky, A.; Chicoine, B. Prevalence of Mental Health Conditions Among 6078 Individuals With Down Syndrome in the United States. J. Patient-Centered Res. Rev. 2022, 9, 58–63. [Google Scholar] [CrossRef] [PubMed]
- Barua, P.D.; Vicnesh, J.; Gururajan, R.; Oh, S.L.; Palmer, E.; Azizan, M.M.; Kadri, N.A.; Acharya, U.R. Artificial Intelligence Enabled Personalised Assistive Tools to Enhance Education of Children with Neurodevelopmental Disorders—A Review. Int. J. Environ. Res. Public. Health 2022, 19, 1192. [Google Scholar] [CrossRef] [PubMed]
- Clark, L.M.; Kelley, M.L. Risk Factors for Dual Disorders in Individuals with Intellectual Disabilities. In Handbook of Dual Diagnosis; Matson, J.L., Ed.; Autism and Child Psychopathology Series; Springer International Publishing: Cham, 2020; pp. 119–139 ISBN 978-3-030-46834-7.
- Dow, M.; Long, B.; Lund, B. Reference and Instructional Services to Postsecondary Education Students with Intellectual Disabilities. Coll. Res. Libr. 2021, 82. [Google Scholar] [CrossRef]
- Bosch, O.J.; Nair, H.P.; Ahern, T.H.; Neumann, I.D.; Young, L.J. The CRF System Mediates Increased Passive Stress-Coping Behavior Following the Loss of a Bonded Partner in a Monogamous Rodent. Neuropsychopharmacology 2009, 34, 1406–1415. [Google Scholar] [CrossRef]
- Gupta, N.; Goyal, N.; Sharma, E. Learning Disability Certification in India: Quo Vadis. J. Indian Assoc. Child Adolesc. Ment. Health 2022, 18, 267–269. [Google Scholar] [CrossRef]
- López-Resa, P.; Moraleda-Sepúlveda, E. Working Memory Capacity and Text Comprehension Performance in Children with Dyslexia and Dyscalculia: A Pilot Study. Front. Psychol. 2023, 14, 1191304. [Google Scholar] [CrossRef] [PubMed]
- Español-Martín, G.; Pagerols, M.; Prat, R.; Rivas, C.; Ramos-Quiroga, J.A.; Casas, M.; Bosch, R. The Impact of Attention-Deficit/Hyperactivity Disorder and Specific Learning Disorders on Academic Performance in Spanish Children from a Low-Middle- and a High-Income Population. Front. Psychiatry 2023, 14, 1136994. [Google Scholar] [CrossRef] [PubMed]
- Higazi, A.M.; Kamel, H.M.; Abdel-Naeem, E.A.; Abdullah, N.M.; Mahrous, D.M.; Osman, A.M. Expression Analysis of Selected Genes Involved in Tryptophan Metabolic Pathways in Egyptian Children with Autism Spectrum Disorder and Learning Disabilities. Sci. Rep. 2021, 11, 6931. [Google Scholar] [CrossRef] [PubMed]
- Kubota, T. Biological Understanding of Neurodevelopmental Disorders Based on Epigenetics, a New Genetic Concept in Education. In Learning Disabilities - Neurobiology, Assessment, Clinical Features and Treatments; Misciagna, S., Ed.; IntechOpen, 2022 ISBN 978-1-83968-587-3.
- Avigan, P.D.; Cammack, K.; Shapiro, M.L. Flexible Spatial Learning Requires Both the Dorsal and Ventral Hippocampus and Their Functional Interactions with the Prefrontal Cortex. Hippocampus 2020, 30, 733–744. [Google Scholar] [CrossRef]
- Qu, J.; Hu, L.; Liu, X.; Dong, J.; Yang, R.; Mei, L. The Contributions of the Left Hippocampus and Bilateral Inferior Parietal Lobule to Form-meaning Associative Learning. Psychophysiology 2021, 58, e13834. [Google Scholar] [CrossRef] [PubMed]
- Kundakovic, M.; Jaric, I. The Epigenetic Link between Prenatal Adverse Environments and Neurodevelopmental Disorders. Genes 2017, 8, 104. [Google Scholar] [CrossRef] [PubMed]
- Ugalde, L.; Santiago-Garabieta, M.; Villarejo-Carballido, B.; Puigvert, L. Impact of Interactive Learning Environments on Learning and Cognitive Development of Children With Special Educational Needs: A Literature Review. Front. Psychol. 2021, 12, 674033. [Google Scholar] [CrossRef] [PubMed]
- Kokot, S.J. A Neurodevelopmental Approach for Helping Gifted Learners with Diagnosed Dyslexia and Attention Deficit/Hyperactivity Disorder (AD/HD). Afr. Educ. Rev. 2005, 2, 130–146. [Google Scholar] [CrossRef]
- Colomer, C.; Berenguer, C.; Roselló, B.; Baixauli, I.; Miranda, A. The Impact of Inattention, Hyperactivity/Impulsivity Symptoms, and Executive Functions on Learning Behaviors of Children with ADHD. Front. Psychol. 2017, 08. [Google Scholar] [CrossRef] [PubMed]
- Moreau, D.; Waldie, K.E. Developmental Learning Disorders: From Generic Interventions to Individualized Remediation. Front. Psychol. 2016, 6. [Google Scholar] [CrossRef]
- Mohammed, A.M.; Bahar, H.F. ; Karbala Governorate Education Directorate Ministry Of Education, Iraq MOOD DISORDER IN STUDENTS WITH LEARNING DISABILITIES. Am. J. Soc. Sci. Educ. Innov. 2024, 6, 31–49. [Google Scholar] [CrossRef]
- McEwen, B.S.; Gianaros, P.J. Stress- and Allostasis-Induced Brain Plasticity. Annu. Rev. Med. 2011, 62, 431–445. [Google Scholar] [CrossRef] [PubMed]
- Lupien, S.J.; McEwen, B.S.; Gunnar, M.R.; Heim, C. Effects of Stress throughout the Lifespan on the Brain, Behaviour and Cognition. Nat. Rev. Neurosci. 2009, 10, 434–445. [Google Scholar] [CrossRef] [PubMed]
- Maksyutynska, K.; Stogios, N.; Prasad, F.; Gill, J.; Hamza, Z.; De, R.; Smith, E.; Horta, A.; Goldstein, B.I.; Korczak, D.; et al. Neurocognitive Correlates of Metabolic Dysregulation in Individuals with Mood Disorders: A Systematic Review and Meta-Analysis. Psychol. Med. 2024, 54, 1245–1271. [Google Scholar] [CrossRef]
- Cai, H.; Dong, J.; Mei, L.; Feng, G.; Li, L.; Wang, G.; Yan, H. Functional and Structural Abnormalities of the Speech Disorders: A Multimodal Activation Likelihood Estimation Meta-Analysis. Cereb. Cortex 2024, 34, bhae075. [Google Scholar] [CrossRef] [PubMed]
- Pascoe, M.I.; Forbes, K.; De La Roche, L.; Derby, B.; Psaradellis, E.; Anagnostou, E.; Nicolson, R.; Georgiades, S.; Kelley, E. Exploring the Association between Social Skills Struggles and Social Communication Difficulties and Depression in Youth with Autism Spectrum Disorder. Autism Res. 2023, 16, 2160–2171. [Google Scholar] [CrossRef]
- Mann, J.J.; Currier, D.; Quiroz, J.A.; Manji, H.K. Neurobiology of Severe Mood and Anxiety Disorders. In Basic Neurochemistry; Elsevier, 2012; pp. 1021–1036 ISBN 978-0-12-374947-5.
- Kao, S.-K.; Chan, C.-T. Increased Risk of Depression and Associated Symptoms in Poststroke Aphasia. Sci. Rep. 2024, 14, 21352. [Google Scholar] [CrossRef] [PubMed]
- Wren, Y.; Pagnamenta, E.; Orchard, F.; Peters, T.J.; Emond, A.; Northstone, K.; Miller, L.L.; Roulstone, S. Social, Emotional and Behavioural Difficulties Associated with Persistent Speech Disorder in Children: A Prospective Population Study. JCPP Adv. 2023, 3, e12126. [Google Scholar] [CrossRef] [PubMed]
- Fries, G.R.; Saldana, V.A.; Finnstein, J.; Rein, T. Molecular Pathways of Major Depressive Disorder Converge on the Synapse. Mol. Psychiatry 2023, 28, 284–297. [Google Scholar] [CrossRef]
- Li, Y.; Zhao, Y.; Lu, Y.; Lu, X.; Hu, Y.; Li, Q.; Shuai, M.; Li, R. Autism Spectrum Disorder-like Behavior Induced in Rat Offspring by Perinatal Exposure to Di-(2-Ethylhexyl) Phthalate. Environ. Sci. Pollut. Res. 2022, 29, 52083–52097. [Google Scholar] [CrossRef]
- Poletti, S.; Mazza, M.G.; Benedetti, F. Inflammatory Mediators in Major Depression and Bipolar Disorder. Transl. Psychiatry 2024, 14, 247. [Google Scholar] [CrossRef] [PubMed]
- Dall, M.; Fellinger, J.; Holzinger, D. The Link between Social Communication and Mental Health from Childhood to Young Adulthood: A Systematic Review. Front. Psychiatry 2022, 13, 944815. [Google Scholar] [CrossRef] [PubMed]
- Cantwell, D.P. Psychiatric Disorder in Children With Speech and Language Retardation: A Critical Review. Arch. Gen. Psychiatry 1977, 34, 583. [Google Scholar] [CrossRef]
- Mellone, S.; Puricelli, C.; Vurchio, D.; Ronzani, S.; Favini, S.; Maruzzi, A.; Peruzzi, C.; Papa, A.; Spano, A.; Sirchia, F.; et al. The Usefulness of a Targeted Next Generation Sequencing Gene Panel in Providing Molecular Diagnosis to Patients With a Broad Spectrum of Neurodevelopmental Disorders. Front. Genet. 2022, 13, 875182. [Google Scholar] [CrossRef] [PubMed]
- Postma, J.K.; Harrison, M.; Kutcher, S.; Webster, R.J.; Cloutier, M.; Bourque, D.K.; Yu, A.C.; Carter, M.T. The Diagnostic Yield of Genetic and Metabolic Investigations in Syndromic and Nonsyndromic Patients with Autism Spectrum Disorder, Global Developmental Delay, or Intellectual Disability from a Dedicated Neurodevelopmental Disorders Genetics Clinic. Am. J. Med. Genet. A. 2024, 194, e63791. [Google Scholar] [CrossRef] [PubMed]
- Dajani, D.R.; Burrows, C.A.; Odriozola, P.; Baez, A.; Nebel, M.B.; Mostofsky, S.H.; Uddin, L.Q. Investigating Functional Brain Network Integrity Using a Traditional and Novel Diagnostic System for Neurodevelopmental Disorders 2018.
- Mohajer, B.; Masoudi, M.; Ashrafi, A.; Mohammadi, E.; Bayani Ershadi, A.S.; Aarabi, M.H.; Uban, K.A. Structural White Matter Alterations in Male Adults with High Functioning Autism Spectrum Disorder and Concurrent Depressive Symptoms; a Diffusion Tensor Imaging Study. J. Affect. Disord. 2019, 259, 40–46. [Google Scholar] [CrossRef] [PubMed]
- Iffland, M.; Livingstone, N.; Jorgensen, M.; Hazell, P.; Gillies, D. Pharmacological Intervention for Irritability, Aggression, and Self-Injury in Autism Spectrum Disorder (ASD). Cochrane Database Syst. Rev. 2023, 10, CD011769. [Google Scholar] [CrossRef]
- Canitano, R.; Scandurra, V. Glutamatergic Agents in Autism Spectrum Disorders: Current Trends. Res. Autism Spectr. Disord. 2014, 8, 255–265. [Google Scholar] [CrossRef]
- Yu, Q.; Li, E.; Li, L.; Liang, W. Efficacy of Interventions Based on Applied Behavior Analysis for Autism Spectrum Disorder: A Meta-Analysis. Psychiatry Investig. 2020, 17, 432–443. [Google Scholar] [CrossRef] [PubMed]
- Arabian, H.; Abdulbaki Alshirbaji, T.; Schmid, R.; Wagner-Hartl, V.; Chase, J.G.; Moeller, K. Harnessing Wearable Devices for Emotional Intelligence: Therapeutic Applications in Digital Health. Sensors 2023, 23, 8092. [Google Scholar] [CrossRef]
- Gill, P.S.; Elchynski, A.L.; Porter-Gill, P.A.; Goodson, B.G.; Scott, M.A.; Lipinski, D.; Seay, A.; Kehn, C.; Balmakund, T.; Schaefer, G.B. Multidisciplinary Consulting Team for Complicated Cases of Neurodevelopmental and Neurobehavioral Disorders: Assessing the Opportunities and Challenges of Integrating Pharmacogenomics into a Team Setting. J. Pers. Med. 2022, 12, 599. [Google Scholar] [CrossRef]
- Simon, J.; Hyde, C.; Saravanapandian, V.; Wilson, R.; Distefano, C.; Besterman, A.; Jeste, S. The Diagnostic Journey of Genetically Defined Neurodevelopmental Disorders. J. Neurodev. Disord. 2022, 14, 27. [Google Scholar] [CrossRef] [PubMed]
- Finucane, B.M.; Ledbetter, D.H.; Vorstman, J.A. Diagnostic Genetic Testing for Neurodevelopmental Psychiatric Disorders: Closing the Gap between Recommendation and Clinical Implementation. Curr. Opin. Genet. Dev. 2021, 68, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Loader, S.J.; Brouwers, N.; Burke, L.M. Neurodevelopmental Therapy Adherence in Australian Parent-Child Dyads: The Impact of Parental Stress. Educ. Dev. Psychol. 2019, 36, 22–26. [Google Scholar] [CrossRef]
- Hamamah, S.; Aghazarian, A.; Nazaryan, A.; Hajnal, A.; Covasa, M. Role of Microbiota-Gut-Brain Axis in Regulating Dopaminergic Signaling. Biomedicines 2022, 10, 436. [Google Scholar] [CrossRef]
- Chang, H.; Hoshina, N.; Zhang, C.; Ma, Y.; Cao, H.; Wang, Y.; Wu, D.; Bergen, S.E.; Landén, M.; Hultman, C.M.; et al. The Protocadherin 17 Gene Affects Cognition, Personality, Amygdala Structure and Function, Synapse Development and Risk of Major Mood Disorders. Mol. Psychiatry 2018, 23, 400–412. [Google Scholar] [CrossRef] [PubMed]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



