1. Introduction
Chronic pain is a health problem that takes a high toll at the personal and social level, both in terms of what patients suffer and the ensuing economic costs [
1]. Due to its complexity, it requires an interdisciplinary, personalized, and comprehensive approach that considers emotional functioning [
2]. Since its introduction over two decades ago, the Initiative on Methods, Measurement, and Pain Assessment in Clinical Trials (IMMPACT) has helped shape improved pain assessment standards. IMMPACT recommends the Profile of Mood States (POMS) be applied to assess emotional functioning during pain as this assessment tool is relatively short, useful in non-psychiatric populations, and relevant to the main negative emotions related to pain [
3].
The POMS was originally designed to assess the mood states of psychiatric patients [
4]. It consists of 65 adjectives describing six mood dimensions: Tension-Anxiety, Depression-Dejection, Anger-Hostility, Vigor-Activity, Fatigue-Inertia, and Confusion-Bewilderment. The items that constitute Friendliness were excluded due to their lack of discriminatory validity with the Vigor-Activity scale. Using the remaining 58 items, an overall mood disturbance score can be calculated by totaling the scores of all subscales except Vigor-Activity. The initial study achieved good psychometric properties in samples from outpatient drug trials, psychotherapy, or a combination of psychotherapy and drug treatments, with an internal consistency (alpha) of between 0.84 and 0.95, a test-retest reliability between 0.65 and 0.74, and a concurrent validity with MMPI scales between -0.58 and 0.69.
The same researchers who recommended the use of the POMS as a measure of emotional functioning in pain within IMMPACT noted a few psychometric shortcomings, the most cited being the Depression subscale [
3]. Some thus proposed that the Beck Depression Inventory (BDI) be used as a complementary measure [
5]. Although the POMS has been used in patients with chronic pain [
6,
7,
8,
9], to our knowledge, only one study has tested the factor structure of the POMS in these patients to date. The authors of this study not only found it impossible to confirm the POMS but were also unable to propose a new exploratory structure [
10]. Their conclusion was that the POMS was not a valid instrument for assessing emotional functioning in patients with chronic pain; among other alternatives, they proposed testing shortened versions of the POMS for this population [
10].
Though several abbreviated versions of the POMS have been published, they do not appear to be widely used in research (POMS-B [
11], V-POMS [
12], POMS-SF [
13]). The most common, the Shortened Version of the Profile of Mood States (SV-POMS), was developed to reduce the number of items for critically ill patients [
14]. In a study involving 83 cancer patients, the original six factors were confirmed, the number of items was reduced from 58 to 37, and good internal consistency coefficients were maintained (between .80 and .91). Studies in healthy adult and cancer patient samples support the reliability of this abbreviated version (between .73 and .96) [
15,
16,
17,
18]. In the literature review conducted as part of this study, only two studies were found on the construct validity of the SV-POMS, neither of which examined patients with chronic pain. In one, Baker et al. [
15] fully confirmed the SV-POMS factor structure in 437 cancer patients (χ2 = 1697, df = 614, p < 0.001; RMR = .07; AGFI = 0.77; CFI = 0.88; RMSEA = 0.06); in the second, Kim et al. [
19] validated the factor structure and invariance for gender groups of the Depression subscale only, with the exception of one item, "Blue," in 9170 cancer survivors.
Consequently, the aim of this study was to confirm the factor structure and test the internal consistency of the SV-POMS as a measure of emotional functioning in a sample of chronic pain patients. The study was expected to show an optimal fit of the original six-factor structure (Tension-Anxiety, Depression-Dejection, Anger-Hostility, Vigor-Activity, Fatigue-Inertia, and Confusion-Bewilderment) and adequate reliability coefficients.
2. Materials and Methods
2.1. Participants
As it was not possible to confirm the full POMS factor structure, this study involves a reanalysis of data previously utilized [
10]. This sample was comprised of chronic pain patients (n = 588) from Seville (Andalusia, Spain) who were about to undergo psychological treatment at one of three locations: primary care health centers (n = 472), a fibromyalgia association (n = 75), and a community center (n = 41). The sociodemographic characteristics and clinical data of the samples are presented on
Table 1 and
Table 2 respectively.
2.2. Measures
Participants had completed a Spanish version of the full 65-item POMS [
20] (see
Appendix A). Each item is an adjective that participants must score on a 5-point Likert scale (0 to 4). In the English version, the instructions are as follows: Read each word/statement below, decide how you have been feeling, in respect to the word/statement, in the past week and today, and select the appropriate statement "Not at All,” "A Little,” "Moderately,” “Quite a Lot,” or "Extremely" to indicate your feeling.
To confirm the SV-POMS structure, the original 37 items were included in the statistical analyses [
14,
16,
17]: Tension-Anxiety, six items (“tense,” “on edge,” “uneasy,” “restless,” “nervous,” “anxious”); Depression-Dejection, eight items (“unhappy,” “sad,” “blue,” “hopeless,” “discouraged,” “miserable,” “helpless,” “worthless”); Anger-Hostility, seven items (“angry,” “peeved,” “grouchy,” “annoyed,” “resentful,” “bitter,” “furious”); Vigor-Activity, six items (“lively,” “active,” “energetic,” “cheerful,” “full of life,” “vigorous”); Fatigue-Inertia, five items (“worn out,” “listless,” “fatigued,” “exhausted,” “sluggish,” “bushed,” “weary”); and, Confusion-Bewilderment, five items (“confused,” “unable to concentrate,” “bewildered,” “forgetful,” “uncertain about things”). The score for each subscale is obtained by totaling the scores of all items and then dividing the sum by the number of items, with a minimum of 0 and a maximum of 4. The Total Mood Disturbance score is obtained by adding the scores of all subscales except Vigor-Activity and dividing by the number of subscales (six). The possible range is from -4 to 4 and the higher the score, the higher the Total Mood Disturbance. Participants were also asked to score other measures recommended by the IMMPACT initiative [
21] (see
Table 2): pain chronicity, pain intensity, pain duration, pain interference, and pain frequency.
2.3. Procedures
This study was carried out in accordance with the recommendations of the Ethics Committee of the South Seville Health District (Andalusian Health Service). All participants voluntarily consented in writing in accordance with the Helsinki Declaration.
Since the study involved psychological interventions, the inclusion criteria were the following: (a) to be age 18 or older; (b) to have a chronic pain diagnosis by a Spanish healthcare practitioner; (c) to have visited primary care due to difficulties with chronic pain during the recruitment period (present maladaptive adjustment to pain); (d) to not be in the middle of an employment dispute or waiting for approval on a disability pension; (e) to not have a primary psychopathological disorder; (f) to not be in psychiatric or psychological treatment (but could be taking painkillers, anxiolytics, or antidepressants) (g) to be able to follow group intervention sessions, thus excluding conditions such as deafness, blindness, or dementia; (h) to be willing to sign an agreement to attend the sessions (group and/or individual); and (i) to not be hospitalized.
Groups of eight to ten people collectively self-administered the questionnaires under the supervision of two graduate students in clinical psychology who also provided support. For this study, only the pretest measurements were considered.
2.4. Data Analysis
SPSS 29 was used to store and analyze the data for internal consistency reliability coefficient and average discrimination index before factor structure analysis. The reliability coefficient was calculated using McDonald’s omega (ω). Values > .80 were considered strong reliability evidence; and .65 – .80, acceptable reliability evidence [
22]. Regarding the average discrimination index, values greater than 0.40 were considered excellent; between 0.30 and 0.40, good; 0.20 to 0.30, adequate; and values less than 0.20, inadequate [
23].
PRELIS and LISREL 12.4.4 were used to calculate the polychoric correlation matrix [
24,
25], check the bivariate normal distribution (an assumption required for the use of polychoric correlations), and complete the confirmatory factor analysis (CFA). Pairwise deletion was used to address missing data. The bivariate normal distribution assumption was verified by calculating the chi-square test (χ2), considering the percentage of pairs of correlations that led to a rejection of the null hypothesis. Assuming a 95% confidence level, the Bonferroni correction was applied: the α value used for statistical decision was calculated with the formula α /c, α = .05 subsequent to a 95% confidence level; and c = number of contrasts = (number of items x number of items – 1)/2. χ2 tends to reject the null hypothesis with large sample sizes. For this reason, the root mean square error of approximation (RMSEA) was also obtained. Values under .1 were considered an insignificant effect on the parameter estimate [
26].
The original 37-item second-order factor SV-POMS structure [
14] was tested using CFA [
27]. Estimates were obtained using unweighted least squares, adequate for polychoric correlations and ordinal variables with asymmetrical distribution [
25,
26,
27,
28]. The lambda parameter of the first item in each factor was set to one to deal with the model identification problem and limit the range of latent variables on the measurement scale.
The standardized factor loadings were then obtained. Lambdas with absolute values over .30 were deemed adequate. Furthermore, the following indices were calculated to check the model fit, yielding appropriate results when (a) χ2 test, p > .05; (b) the value of the expected cross-validation index (ECVI) was closer to the saturated model than to the independence model (a lower value implies a better fit) [
29]; (c) a root mean square error of approximation (RMSEA) [
26] of less than .05 was considered a good fit, between .08 and .10 a reasonable fit, and greater than .10 unfit [
30]; and (d) goodness of fit index (GFI); (e) adjusted goodness of fit index (AGFI) (Hooper et al., 2008); (f) comparative fit index (CFI) [
31]; (g) normed fit index (NFI); and (h) non-normed fit index (NNFI) [
32] above .80 indicating an appropriate fit [
33].
3. Results
3.1. Reliability
All but one factor presented excellent reliability coefficients (Tension-Anxiety, ω = .89; Depression-Dejection, ω = .87; Anger-Hostility, ω = .91; Vigor-Activity, ω = .85; Fatigue-Inertia, ω = .81), the exception being Confusion-Bewilderment (ω = .77) which was acceptable. The global reliability coefficient also was excellent (ω = .95).
3.2. Discrimination Index
All item results were excellent, ranging from .417 to .761, except for “Active,” “Full of life,” “Miserable,” and “Energetic,” which were good (ranging from .031 to .361), and “Vigorous,” which was adequate (.206). Average discrimination indices yielded excellent results for Tension-Anxiety (D = .65), Depression-Dejection (D = .62), Anger-Hostility, (D = .67), Fatigue-Inertia (D = .58), Confusion-Bewilderment (D = .55), and the global score (D = .61). Only Vigor-Activity yielded a good result (D = .35).
3.3. Bivariate Normal Distribution
Given that 37 items were included, 666 correlations were obtained (37 x 36 /2). Based on Χ2, the bivariate normality assumption was met in 93.8% of the occasions (625 correlations), comparing their significance with p = .05 / 666 = .00007 after applying the Bonferroni correction. Moreover, the RMSEA was less than .1 in 99.9% of the cases (663 correlations).
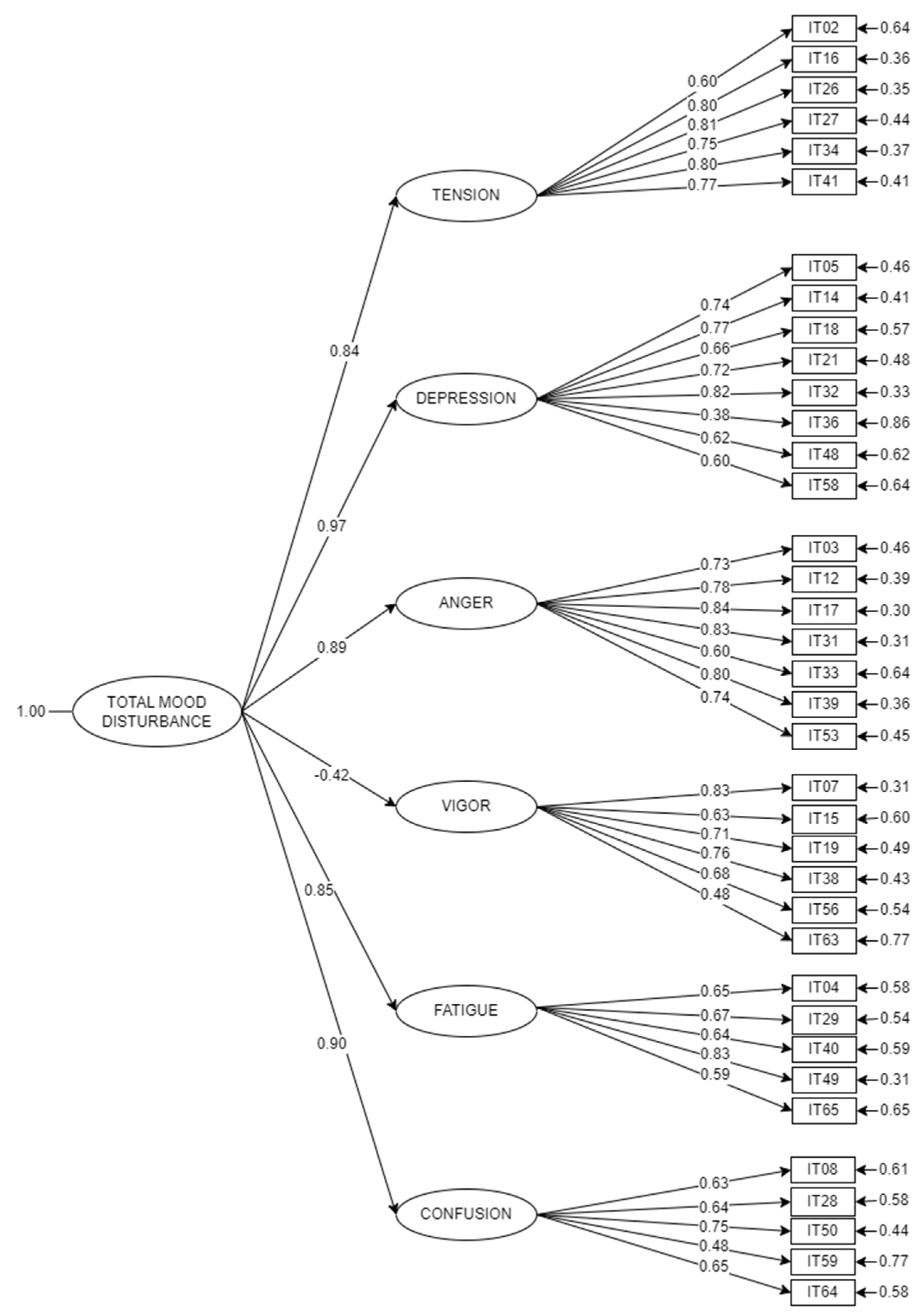
3.4. Factor Loadings
Figure 1 presents the model, including the standardized factor loadings. Lambdas ranged from .38 to .84 and gammas, from -.42 (Vigor-Activity) to .97 (Depression-Dejection), five of which were over .84.
3.5. Fit Indices
There was no adjustment with X2(624) = 2402.113, p < .0001, possibly due to the large sample size. The other indices showed an adequate fit of the proposed model as follows: ECVI = 4.361 (saturated ECVI = 2.395; independent ECVI = 21.855); RMSEA = .070, 90% CI [.067, .072]; GFI = .974; AGFI = .971; CFI = .853; NFI = .812; and NNFI = .843.
3.6. Descriptives
Means and standard deviations were 2.39 (0.98) for Tension-Anxiety, 1.67 (0.93) for Depression-Dejection, 1.73 (1.03) for Anger-Hostility, 1.60 (0.85) for Vigor-Activity, 2.41 (0.94) for Fatigue-Inertia, 1.90 (0.97) for Confusion-Bewilderment, and 1.42 (0.75) for Total Mood Disturbance.
The Spanish SV-POMS is available in paper and pencil format and in Excel format in
Appendix B and Supplemental content S1, respectively. Both can be used to obtain direct scores and percentiles.
4. Discussion
Our aim was to confirm the SV-POMS factor structure and internal consistency in a sample of patients with chronic pain. Since this measure had not yet been validated for chronic pain, cancer patients comprised the samples of the selected reference studies [
14,
15,
16,
17,
18,
19].
The average discrimination indices were excellent for all factors except Vigor-Activity, which was good, while the overall discrimination indices were excellent for all items except “Active,” “Full of life,” “Miserable” and “Energetic,” which were good, and “Vigorous” which was adequate. Although these findings far from sufficed and no other studies could be found for the purposes of comparison, it is striking that four of the five adjectives that did not yield excellent discrimination indices corresponded to Vigor-Activity. This could perhaps be attributed to the fact that the sample was comprised of patients who have been suffering from pain for fifteen years on average, making it more difficult for them to identify with adjectives related to that factor. Furthermore, 65% of the patients had no schooling or had only attended elementary school, so they might have had problems understanding non-colloquial terms such as miserable, vigorous, or even energetic.
The second-order factor structure was fully confirmed, this is, Total Mood Disturbance composed of Depression-Dejection, reversed Vigor-Activity, Anger-Hostility, Tension-Anxiety, Confusion-Bewilderment, and Fatigue-Inertia. Factor loadings for every factor, every item, and all fit indices were adequate, in line with what was obtained by Baker et al. [
15], the only study on SV-POMS to conduct a CFA. Kim and Smith [
19] confirmed the factor structure of the Depression-Dejection subscale minus one item, "Blue,” which resulted in moderate differential item functioning for gender groups.
Regarding internal consistency, our results confirm excellent reliability coefficients for the SV-POMS global score and for every subscale, except for Confusion-Bewilderment, which was acceptable. This finding of slightly lower reliability of the Confusion-Bewilderment subscale was supported by all except two of the studies examined [
15,
16,
17,
18]. The exceptions were the original study by Schacham [
14], where the reliability of all subscales except Tension-Anxiety were excellent, and the study by Kim & Smith [
19], whose analysis focused solely on the Depression-Dejection subscale. Although the coefficients were more than sufficient, the Confusion-Bewilderment factor could be greatly influenced by the sample used. Its reliability was already lower in the full original version [
4], and was not confirmed in either the full or abbreviated version validated with healthy samples [
34]. Therefore, if the proponents of the full version of the POMS recommended using the BDI due to the lower reliability of the Depression-Dejection subscale [
3], our results on the SV-POMS suggest, as did DiLorenzo et al. [
17], that the Confusion-Bewilderment subscale should not be used in isolation.
At this point, it seems relevant to note the two traditions in mood measurement [
35]. One focuses on affective valence, where positive and negative affect are generally distinguished; the other, which includes the SV-POMS, centers on the emotional content. Achieving good discriminative validity is much more difficult when measuring specific mood states than affective valence, which make the results herein even more valuable. These results support the hypothesis that the superior construct and discriminative validity of the shortened POMS versions in comparison to the full version are probably due to the selection of the psychometrically soundest items [
14,
15,
16,
17,
18].
Consequently, the SV-POMS was found here to be a valid and reliable measure of emotional functioning in chronic pain. The main clinical significance of the study is to use psychometric data to support a reasonably brief instrument, which allows for measuring the six most relevant mood states in patients with chronic pain, facilitating its use by health professionals. Additionally, considering that only one validation was found in a language other than English (French) [
18], it is important that this SV-POMS validation was done in Spanish, the mother tongue of about 500 million people.
The primary limitation of this study was representativeness since the samples came from public primary care and community centers. This resulted in a very specific participant profile: mostly middle-aged women with low educational attainment, low-medium socioeconomic status, and a diagnosis of fibromyalgia with high chronicity. The results may not be generalizable due to three main factors: lack of ethnic and cultural diversity in the sample (100% Spanish Caucasians), low educational attainment (two-thirds had only attended elementary school, and some had no schooling at all), and the prevalence of a single diagnosis (fibromyalgia, which accounted for 59% of the sample).
Future lines of research on the SV-POMS as a measure of emotional functioning in chronic pain patients should focus on confirming its psychometric properties in larger and more heterogeneous samples, expanding validation studies to other types of internal and external validity, and increasing the number of adaptations to other languages.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org, Suppl S1: Spanish Short Version of the Profile of Mood States (SV-POMS) for Excel.
Author Contributions
CMLJ and FJCG developed the original idea and design of the study and acquired data. SSC and SCM were mainly responsible for the study methodology and performed data analysis. All authors interpreted and discussed the results, drafted the article, commented on it and revised it for important intellectual content, gave the final approval of the version to be published, and took responsibility for the integrity of the work as a whole.
Funding
This research was funded by the Fondo Nacional de Desarrollo Científico y Tecnológico FONDECYT Regular, ANID, Chilean government [1190945]; the ERDF government program for Andalusia 2014-2020, Spain [US-1263096]; the VI Research and Transfer Plan-VI-PPITUS, Universidad de Sevilla, Spain [VIPP PRECOMPETI 2020/1333]; Andalusian Plan for Research, Development and Innovation (PAIDI 2020), Government of Andalusia, Spain [ref. PY20-01122]; and the PID2020-115486GB-I00 grant funded by the Ministerio de Ciencia e Innovación (MCIN/AEI/ 10.13039/501100011033), Spanish government.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Ethics Committee of the Southern Seville Health District (Andalusian Health Service), approval number 12032012.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Acknowledgments
We would like to express our gratitude to coordinator José Sánchez Blanco and the healthcare professionals at Southern Seville Primary Care for enlisting the patients for this study: Bienvenida Baena Ramírez, Carlos López Pérez, Daniel Benítez Merelo, Juan José Luna Cano, María Dolores Lario Fernández, Pablo Guzmán Pueyo, Paloma Caro Bejarano, Roberto Moreno Borrego, and Rocío del Pino Gómez. We also thank the Association for Fibromyalgia Patients (APEFIR) of Los Palacios in Seville for their invaluable support. The graduate students who were on hand for assistance during the self-administration of the questionnaires include Abraham Rafael Lomeña Calero, Candela García Fernández, Carmen María Gómez Guerrero, Cristina Naranjo García, Elia María Ruiz García, Felisa Losada Durán, Francisco Aboza García, Germán Cortizo Sabalete, Gumersinda Naranjo, Inmaculada Concepción Pérez Barea, Inmaculada Villajos López, Jesús Funuyet Salas, Lidia Cotes García, Manuel Berlanga de Ávila, María Amparo Espinosa Bermúdez, María del Carmen González Ortega, Marta Lavado Zambrano, Miguel Cruz Cortés, Milagros Buero Gallego, Mónica Pérez Rodríguez, Pedro Bendala Rodríguez, Rafael García Alonso, Sara Martín Gandullo, Saúl Corzo Camacho, Sergio Cruz Cantueso, and María del Mar Rodríguez Navas. Their help was invaluable. We would also like to thank the following undergraduate students who helped with data processing: Álvaro Ojeda Martín, Ana León Collantes, Andrea Pilar Donoso, Blanca del Rocío Tataje Medrano, Carmen López Rodríguez, Esther Arzúa Meléndez, Irene Martínez Cuevas, Laura Andrade Fernández, María Ángeles Vizcaíno Leal, María del Carmen Jiménez Sánchez, María del Rocío Álvarez Morales, María Rocío Varilla Román, and Raquel Padilla Moó. We are also grateful to Wendy Gosselin (American Translation Association member #275293) for revising the English language version of the manuscript. Finally, we are indebted to all the patients who participated in our study, despite being in poor health, for their cooperation.
Conflicts of Interest
The authors declare no conflicts of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
Abbreviations
The following abbreviations are used in this manuscript:
| IMMPACT |
Initiative on Methods, Measurement, and Pain Assessment in Clinical Trials |
| CFA |
Confirmatory Factor Analysis |
| POMS |
Profile of Mood States |
| SV-POMS |
Shortened Version of the Profile of Mood States |
| ECVI |
Expected Cross-Validation Index |
| RMSEA |
Root Mean Square Error of Approximation |
| GFI |
Goodness of Fit Index |
| AGFI |
Adjusted Goodness of Fit Index |
| CFI |
Comparative Fit Index |
| NFI |
Normed Fit Index |
| NNFI |
Non-Normed Fit Index |
| MMPI |
Minnesota Multiphasic Personality Inventory |
| BDI |
Beck Depression Inventory |
Appendix A
Perfil de Estados de Ánimo (POMS). Versión Española de Arce, Andrade & Seoane (2000) del Original de McNair, Lorr & Droppleman (1971)
La lista de palabras que aparece a continuación describe sentimientos que tienen las personas. Después de leer cada palabra fíjese en las cinco opciones posibles y elija la que mejor describa cómo se ha sentido usted últimamente rodeándola con un círculo según la siguiente escala: 0 = Nada; 1 = Poco; 2 = Moderadamente; 3 = Bastante; 4 = Muchísimo
| 1 |
Amistoso/a |
0 |
1 |
2 |
3 |
4 |
|
33 |
Resentido/a |
0 |
1 |
2 |
3 |
4 |
| 2 |
Tenso/a |
0 |
1 |
2 |
3 |
4 |
|
34 |
Nervioso/a |
0 |
1 |
2 |
3 |
4 |
| 3 |
Enfadado/a |
0 |
1 |
2 |
3 |
4 |
|
35 |
Solo/a |
0 |
1 |
2 |
3 |
4 |
| 4 |
Rendido/a |
0 |
1 |
2 |
3 |
4 |
|
36 |
Desdichado/a |
0 |
1 |
2 |
3 |
4 |
| 5 |
Infeliz |
0 |
1 |
2 |
3 |
4 |
|
37 |
Aturdido/a |
0 |
1 |
2 |
3 |
4 |
| 6 |
Sensato/a |
0 |
1 |
2 |
3 |
4 |
|
38 |
De buen humor |
0 |
1 |
2 |
3 |
4 |
| 7 |
Animado/a |
0 |
1 |
2 |
3 |
4 |
|
39 |
Amargado/a |
0 |
1 |
2 |
3 |
4 |
| 8 |
Confuso/a |
0 |
1 |
2 |
3 |
4 |
|
40 |
Exhausto/a |
0 |
1 |
2 |
3 |
4 |
| 9 |
Arrepentido/a |
0 |
1 |
2 |
3 |
4 |
|
41 |
Ansioso/a |
0 |
1 |
2 |
3 |
4 |
| 10 |
Agitado/a |
0 |
1 |
2 |
3 |
4 |
|
42 |
Listo/a para pelear |
0 |
1 |
2 |
3 |
4 |
| 11 |
Desatento/a |
0 |
1 |
2 |
3 |
4 |
|
43 |
Afable/a |
0 |
1 |
2 |
3 |
4 |
| 12 |
Enojado/a |
0 |
1 |
2 |
3 |
4 |
|
44 |
Abatido/a |
0 |
1 |
2 |
3 |
4 |
| 13 |
Considerado/a |
0 |
1 |
2 |
3 |
4 |
|
45 |
Desesperado/a |
0 |
1 |
2 |
3 |
4 |
| 14 |
Triste |
0 |
1 |
2 |
3 |
4 |
|
46 |
Perezoso/a |
0 |
1 |
2 |
3 |
4 |
| 15 |
Activo/a |
0 |
1 |
2 |
3 |
4 |
|
47 |
Rebelde |
0 |
1 |
2 |
3 |
4 |
| 16 |
Con nervios |
0 |
1 |
2 |
3 |
4 |
|
48 |
Indefenso |
0 |
1 |
2 |
3 |
4 |
| 17 |
Malhumorado/a |
0 |
1 |
2 |
3 |
4 |
|
49 |
Cansado |
0 |
1 |
2 |
3 |
4 |
| 18 |
Melancólico/a |
0 |
1 |
2 |
3 |
4 |
|
50 |
Desconcertado/a |
0 |
1 |
2 |
3 |
4 |
| 19 |
Enérgico/a |
0 |
1 |
2 |
3 |
4 |
|
51 |
Alerta |
0 |
1 |
2 |
3 |
4 |
| 20 |
Descontrolado/a |
0 |
1 |
2 |
3 |
4 |
|
52 |
Engañado/a |
0 |
1 |
2 |
3 |
4 |
| 21 |
Desesperanzado/a |
0 |
1 |
2 |
3 |
4 |
|
53 |
Furioso/a |
0 |
1 |
2 |
3 |
4 |
| 22 |
Relajado/a |
0 |
1 |
2 |
3 |
4 |
|
54 |
Eficiente |
0 |
1 |
2 |
3 |
4 |
| 23 |
No merecedor/a |
0 |
1 |
2 |
3 |
4 |
|
55 |
Confiado/a |
0 |
1 |
2 |
3 |
4 |
| 24 |
Rencoroso/a |
0 |
1 |
2 |
3 |
4 |
|
56 |
Dinámico/a |
0 |
1 |
2 |
3 |
4 |
| 25 |
Comprensivo/a |
0 |
1 |
2 |
3 |
4 |
|
57 |
Con mal genio |
0 |
1 |
2 |
3 |
4 |
| 26 |
Intranquilo/a |
0 |
1 |
2 |
3 |
4 |
|
58 |
Inútil |
0 |
1 |
2 |
3 |
4 |
| 27 |
Inquieto/a |
0 |
1 |
2 |
3 |
4 |
|
59 |
Olvidadizo/a |
0 |
1 |
2 |
3 |
4 |
| 28 |
Desconcentrado/a |
0 |
1 |
2 |
3 |
4 |
|
60 |
Despreocupado/a |
0 |
1 |
2 |
3 |
4 |
| 29 |
Fatigado/a |
0 |
1 |
2 |
3 |
4 |
|
61 |
Aterrorizado/a |
0 |
1 |
2 |
3 |
4 |
| 30 |
Servicial |
0 |
1 |
2 |
3 |
4 |
|
62 |
Culpable |
0 |
1 |
2 |
3 |
4 |
| 31 |
Irritado/a |
0 |
1 |
2 |
3 |
4 |
|
63 |
Vigoroso/a |
0 |
1 |
2 |
3 |
4 |
| 32 |
Desanimado/a |
0 |
1 |
2 |
3 |
4 |
|
64 |
Inseguro/a |
0 |
1 |
2 |
3 |
4 |
| |
|
|
|
|
|
|
|
65 |
Agotado/a |
|
|
|
|
|
Appendix B
Perfil de Estados de Ánimo Versión Abreviada en Español (POMS-SV, Shacham, 1983)
La lista de palabras que aparece a continuación describe sentimientos que tienen las personas. Después de leer cada palabra fíjese en las cinco opciones posibles y elija la que mejor describa cómo se ha sentido usted últimamente rodeándola con un círculo según la siguiente escala: 0 = Nada; 1 = Poco; 2 = Moderadamente; 3 = Bastante; 4 = Muchísimo
| 1 |
Tenso/a |
0 |
1 |
2 |
3 |
4 |
|
19 |
Irritado/a |
0 |
1 |
2 |
3 |
4 |
| 2 |
Enfadado/a |
0 |
1 |
2 |
3 |
4 |
|
20 |
Desanimado/a |
0 |
1 |
2 |
3 |
4 |
| 3 |
Rendido/a |
0 |
1 |
2 |
3 |
4 |
|
21 |
Resentido/a |
0 |
1 |
2 |
3 |
4 |
| 4 |
Infeliz |
0 |
1 |
2 |
3 |
4 |
|
22 |
Nervioso/a |
0 |
1 |
2 |
3 |
4 |
| 5 |
Animado/a |
0 |
1 |
2 |
3 |
4 |
|
23 |
Desdichado/a |
0 |
1 |
2 |
3 |
4 |
| 6 |
Confuso/a |
0 |
1 |
2 |
3 |
4 |
|
24 |
De buen humor |
0 |
1 |
2 |
3 |
4 |
| 7 |
Enojado/a |
0 |
1 |
2 |
3 |
4 |
|
25 |
Amargado/a |
0 |
1 |
2 |
3 |
4 |
| 8 |
Triste |
0 |
1 |
2 |
3 |
4 |
|
26 |
Exhausto/a |
0 |
1 |
2 |
3 |
4 |
| 9 |
Activo/a |
0 |
1 |
2 |
3 |
4 |
|
27 |
Ansioso/a |
0 |
1 |
2 |
3 |
4 |
| 10 |
Con nervios |
0 |
1 |
2 |
3 |
4 |
|
28 |
Indefenso/a |
0 |
1 |
2 |
3 |
4 |
| 11 |
Malhumorado/a |
0 |
1 |
2 |
3 |
4 |
|
29 |
Cansado/a |
0 |
1 |
2 |
3 |
4 |
| 12 |
Melancólico/a |
0 |
1 |
2 |
3 |
4 |
|
30 |
Desconcertado/a |
0 |
1 |
2 |
3 |
4 |
| 13 |
Enérgico/a |
0 |
1 |
2 |
3 |
4 |
|
31 |
Furioso/a |
0 |
1 |
2 |
3 |
4 |
| 14 |
Desesperanzado/a |
0 |
1 |
2 |
3 |
4 |
|
32 |
Dinámico/a |
0 |
1 |
2 |
3 |
4 |
| 15 |
Intranquilo/a |
0 |
1 |
2 |
3 |
4 |
|
33 |
Inútil |
0 |
1 |
2 |
3 |
4 |
| 16 |
Inquieto/a |
0 |
1 |
2 |
3 |
4 |
|
34 |
Olvidadizo/a |
0 |
1 |
2 |
3 |
4 |
| 17 |
Desconcentrado/a |
0 |
1 |
2 |
3 |
4 |
|
35 |
Vigoroso/a |
0 |
1 |
2 |
3 |
4 |
| 18 |
Fatigado/a |
0 |
1 |
2 |
3 |
4 |
|
36 |
Inseguro/a |
0 |
1 |
2 |
3 |
4 |
| |
|
0 |
1 |
2 |
3 |
4 |
|
37 |
Agotado/a |
0 |
1 |
2 |
3 |
4 |
References
- Cohen SP, Vase L, Hooten WM. Chronic pain: an update on burden, best practices, and new advances. The Lancet [Internet]. 2021 May 29;397(10289):2082–97. Available from: https://linkinghub.elsevier.com/retrieve/pii/S0140673621003937.
- McCracken LM. Personalized pain management: Is it time for process-based therapy for particular people with chronic pain? European Journal of Pain [Internet]. 2023 Oct 24;27(9):1044–55. Available from: https://onlinelibrary.wiley.com/doi/10.1002/ejp.2091.
- Kerns RD. Assessment of emotional functioning in pain treatment outcome research. In: IMMPACT-II Initiative on Methods, Measurement, and Pain Assessment in Clinical Trials [Internet]. Washington, D.C.; 2003. Available from: http://www.immpact.org/meetings/Immpact2/participants2.html.
- McNair DM, Lorr M, Droppleman LF. Profile of Mood States. San Diego, CA: Educational and Industrial Testing Service; 1971.
- Beck A, Ward CH, Mendelson M, Mock J, Erbaugh J. An Inventory for Measuring Depression. Arch Gen Psychiatry [Internet]. 1961 Jun 1;4(6):561–71. [CrossRef]
- Casini I, Fatighenti E, Giannantoni A, Massai L, Pieretti S, Ceccarelli I, et al. Food-Specific IgG4 Antibody-Guided Exclusion Diet Improves Conditions of Patients with Chronic Pain. Pain Ther. 2022;11(3):873–906.
- Edwards SA, Martin SL, Rainey T, Whitaker G, Greenwood DC, Jones A, et al. Influence of acute fasting on pain tolerance in healthy subjects: a randomised crossover study. FRONTIERS IN PAIN RESEARCH. 2023;4.
- Hergenroeder A, Quinn TD, Perdomo SJ, Kline CE, Gibbs BB. Effect of a 6-month sedentary behavior reduction intervention on well-being and workplace health in desk workers with low back pain. WORK-A JOURNAL OF PREVENTION ASSESSMENT & REHABILITATION. 2022;71(4):1145–55.
- Yamada K, Fujii T, Kubota Y, Wakaizumi K, Oka H, Matsudaira K. Negative effect of anger on chronic pain intensity is modified by multiple mood states other than anger: A large population-based cross-sectional study in Japan. Mod Rheumatol. 2022;32(3):650–7.
- López-Jiménez CM, Cano-García FJ, Sanduvete-Chaves S, Chacón-Moscoso S. Profile of Mood States Factor Structure Does Not Accurately Account for Patients with Chronic Pain. Pain Medicine [Internet]. 2021 Nov 1;22(11):2604–14. [CrossRef]
- Heuchert JP, McNair DM. Profile of mood states, POMS-2. North Tonawanda: Multi-Health Systems Inc. 2012.
- Wicherts JM, Vorst HCM. Modelpassing van de Verkorte Profile of Mood States en meetinvariantie over mannen en vrouwen TT - Model fit of the Dutch Shortened Profile of Mood States and measurement invariance over gender. Ned Tijdschr Psychol [Internet]. 2004 Feb;59(1):12–21. Available from: https://search.proquest.com/docview/620402801?accountid=14744.
- Chen KM, Snyder M, Krichbaum K. Translation and equivalence: The Profile of Mood States Short Form in English and Chinese. Int J Nurs Stud [Internet]. 2002 Aug;39(6):619–24. Available from: https://search.proquest.com/docview/619921481?accountid=14744.
- Shacham S. A Shortened Version of the Profile of Mood States. J Pers Assess [Internet]. 1983;47(3):305–6. Available from: http://www.tandfonline.com/doi/abs/10.1207/s15327752jpa4703_14.
- Baker F, Denniston M, Zabora J, Polland A, Dudley WN. A POMS short form for cancer patients: Psychometric and structural evaluation. Psychooncology. 2002;11(4):273–81.
- Curran SL, Andrykowski MA, Studts JL. Short Form of the Profile of Mood States (POMS-SF): Psychometric information. Psychol Assess [Internet]. 1995 Mar;7(1):80–3. Available from: https://search.proquest.com/docview/618655884?accountid=14744.
- Dilorenzo TA, Bovbjerg DH, Montgomery GH, Valdimarsdottir H, Jacobsen PB. The application of a shortened version of the profile of mood states in a sample of breast cancer chemotherapy patients. Br J Health Psychol [Internet]. 1999 Nov 16;4(4):315–25. Available from: https://bpspsychub.onlinelibrary.wiley.com/doi/10.1348/135910799168669.
- Fillion L, Gagnon P. French Adaptation of the Shortened Version of the Profile of Mood States. Psychol Rep [Internet]. 1999 Feb;84(1):188. Available from: http://asp.ammonsscientific.com/find.php?resource=PR0.84.1.188.
- Kim J, Smith T. Exploring measurement invariance by gender in the profile of mood states depression subscale among cancer survivors. Qual Life Res [Internet]. 2017 Jan;26(1):171–5. Available from: https://search.proquest.com/docview/1845056348?accountid=14744.
- Andrade E, Arce C, Seaone G. Adaptación al español del cuestionario Perfil de los Estados de Ánimo en una muestra de deportistas [Adaptation of the Profile of Mood States into Spanish with a sample of athletes]. Psicothema. 2002;14(4):708–13.
- Dworkin RH, Turk DC, Farrar JT, Haythornthwaite JA, Jensen MP, Katz NP, et al. Core outcome measures for chronic pain clinical trials: IMMPACT recommendations. Pain. 2005;113(1–2):9–19.
- Kalkbrenner MT. Alpha, Omega, and H Internal Consistency Reliability Estimates: Reviewing These Options and When to Use Them. Counseling Outcome Research and Evaluation. 2023;14(1).
- Barbero MI. Psicometría II. Métodos de elaboración de escalas [Psychometrics II. Methods to develop scales]. Madrid: Uned. 1993.
- Holgado-Tello FP, Chacón-Moscoso S, Barbero-García I, Vila-Abad E. Polychoric versus Pearson correlations in exploratory and confirmatory factor analysis of ordinal variables. Quality & Quantity: International Journal of Methodology [Internet]. 2010 Jan;44(1):153–66. Available from: https://search.proquest.com/docview/742973733?accountid=14744.
- Morata-Ramírez M de los Á, Holgado-Tello FP. Construct validity of Likert scales through confirmatory factor analysis: A simulation study comparing different methods of estimation based on Pearson and polychoric correlations. Int’l J Soc Sci Stud. 2013;1:54.
- Hooper D, Coughlan J, Mullen MR. Structural equation modelling: Guidelines for determining model fit. Electronic journal of business research methods. 2008;6(1):53–60.
- Bagozzi RP, Yi Y. Specification, evaluation, and interpretation of structural equation models. J Acad Mark Sci [Internet]. 2012 Jan;40(1):8–34. Available from: https://search.proquest.com/docview/923957517?accountid=14744.
- Jöreskog KG. Factor analysis by MINRES. To the memory of Harry Harman and Henry Kaiser. 2003.
- Browne MW, Cudeck R. Single sample cross-validation indices for covariance structures. Multivariate Behav Res [Internet]. 1989 Oct;24(4):445–55. Available from: https://search.proquest.com/docview/617747593?accountid=14744.
- Browne MW, Cudeck R. Alternative ways of assessing model fit. In: Sage focus editions. Sage publications; 1993. p. 136–136.
- Byrne BM. Structural equation modeling with LISREL, PRELIS, and SIMPLIS. [Б. и.] London; 1998.
- Hoe SL. Issues and procedures in adopting structural equation modeling technique. Journal of applied quantitative methods. 2008;3(1):76–83.
- Bendayan R, Blanca MJ, Fernández-Baena JF, Escobar M, Trianes MV. New empirical evidence on the validity of the Satisfaction with Life Scale in early adolescents. European Journal of Psychological Assessment [Internet]. 2013;29(1):36–43. Available from: https://search.proquest.com/docview/1284066109?accountid=14744.
- Bourgeois A, LeUnes A, Meyers M. Full-scale and short-form of the Profile of Mood States: A factor analytic comparison. J Sport Behav. 2010;33(4):355–76.
- Watson D, Vaidya JG. Mood Measurement: Current Status and Future Directions. In: Handbook of Psychology, Second Edition. 2012. p. 351–75.
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).