
Submitted:
20 January 2025
Posted:
22 January 2025
You are already at the latest version
Abstract
Background/Objectives: This study aimed to compare the accuracy of digital measurements obtained from orthopantomographies (OPGs) or panoramic radiographs and lateral cephalograms in evaluating facial asymmetry in patients with different skeletal classes. The sample consisted of 128 Romanian patients (67 females, 61 males; median age 21 years) who sought orthodontic treatment. Methods: Lateral cephalograms and OPGs were obtained for each patient, and digital tracing was performed using the WEBCEPH program. Angular measurements (ANB, FMA, gonial angles) and linear measurements (ramus height, mandibular body length) were assessed on both imaging modalities. Results: Strong positive correlations were found between the gonial angle and ramus height measurements obtained from lateral cephalograms and OPGs (rs range: 0.800-0.946; p < 0.001). However, mandibular body length showed weaker correlations between the two methods. Significant sex differences were observed, with males exhibiting larger craniofacial measurements compared to females (p < 0.05). Conclusions: The findings suggest that OPGs can be reliably used to measure the gonial angle and ramus height, providing results comparable to lateral cephalograms. However, caution should be exercised when predicting horizontal measurements from OPGs. Standardization of the OPG recording process and further research with larger sample sizes are required to establish standard panoramic norms for OPG parameters in the assessment of facial asymmetry.
Keywords:
ANB
; artificial intelligence
; dentistry
; digital analysis
; FMA
; gonial angle
; mandibular body length
; orthodontics
; ramus height
; WEBCEPH
1. Introduction
The success of orthodontic therapy and dental care depends on a thorough patient assessment. A comprehensive evaluation of occlusion, soft tissue connections, and skeletal form is required for diagnosis and therapy planning, typically involving radiographs, dental casts, clinical examinations, and patient photos [1]. Among these, panoramic radiographs are an essential tool for orthodontic diagnosis and treatment planning, providing a broad view of the mandibular and maxillary arches, temporomandibular joints, and supporting tissues. Introduced by Professor Yrjo Paatero in 1961, panoramic radiographs are valued for their non-invasiveness, lower radiation exposure, affordability, and ability to display the entire dentition and surrounding anatomy [2].
Since Levandoski first analyzed panoramic radiographs in 1991, research on their quantitative accuracy has been limited, partly due to the inherent variability in magnification [3]. Despite these limitations, panoramic radiographs remain integral to orthodontic and dental diagnosis, aiding in the detection of mandibular asymmetry, dental anomalies, tooth eruption patterns, bone pathology, and cysts or tumors. They also play a critical role in monitoring orthodontic therapy, as highlighted by Graber's 1967 recommendation for their routine use [4].
Cephalometric radiographs, introduced by Broadbent in 1931, are equally vital for orthodontics [5]. They provide sagittal views of skeletal, dental, and soft tissue relationships, enabling quantitative analyses through precise landmark identification. However, landmark identification errors and superimposition challenges can limit their reliability in certain diagnostic scenarios, particularly in assessing facial asymmetry [6,7,8,9].
Facial asymmetry, while common to some degree in the general population, can have significant functional and aesthetic implications when severe. Its etiology includes congenital, acquired, and developmental factors [10,11,12]. Accurate diagnosis often involves supplemental imaging, intraoral and extraoral examinations, and advanced radiographic techniques like orthopantomograms (OPGs) and lateral cephalograms. OPGs, in particular, allow separate evaluation of right and left structures, mitigating the superimposition challenges of lateral cephalograms. However, questions remain about the validity of certain cephalometric measurements taken on OPGs, warranting further investigation [13,14].
Recent advancements in artificial intelligence (AI) have revolutionized medical imaging, including dental radiographs. AI-powered algorithms now assist in landmark identification and measurement analysis, potentially reducing human error and enabling less experienced practitioners to achieve consistent results. Despite its promise, AI implementation in orthodontics often requires manual input of measurements, introducing the possibility of missing or incomplete data [15].
The current study aims to evaluate the accuracy of digital orthopantomography imaging in determining gonial angles, ramus height, and mandibular body length compared to lateral cephalograms in patients presenting with various skeletal classes. By addressing the limitations of traditional methods and exploring the integration of modern technologies, this research seeks to enhance diagnostic precision and improve orthodontic treatment outcomes.
2. Materials and Methods
2.1. Ethical Considerations
The study was conducted on patients enrolled in the Discipline of Orthodontics I, Faculty of Dental Medicine, "Victor Babeș" University of Medicine and Pharmacy in Timișoara. Written informed consent was obtained from all participants, and ethical approval was granted by the Scientific Research Ethics Committee of the "Victor Babeș" University of Medicine and Pharmacy, Timișoara, Romania (CECS number 04/26.01.2024).
2.2. Study Design and Participants
This cross-sectional study included 128 Romanian patients who sought orthodontic treatment at the university’s clinic. Each patient underwent a comprehensive clinical assessment, including radiographs, pre-treatment study models, and clinical photographs. Inclusion criteria comprised individuals over a specified age, those with good oral hygiene, Romanian nationals, and patients willing to participate in the study. Exclusion criteria included prior orthodontic or orthognathic surgical interventions, history of craniofacial clefts, use of hormonal medications, endocrine disorders, neurological conditions, or maxillofacial trauma.
2.1. Procedure Methodology
2.1.1. Protocol and Measurements for Digital Lateral Cephalometry and Orthopantomographs
All patients' lateral cephalograms were obtained with their heads in their natural positions as a point of reference [16], and also orthopantomographies (OPGs) or panoramic radiographs were obtained with their heads in their natural positions.
During radiography exposure, patients were placed upright, shoulders relaxed, back straight, feet closed, head straight over the chin rest, biting on a bite block, tongue against the hard palate, and head with the median sagittal plane perpendicular to the ground and the Frankfort plane parallel to the floor. Patients were positioned in a natural head position for cephalometric radiographs, with the lips in relaxed contact, the teeth in central occlusion, and the gaze straight ahead. The patients were positioned with the Frankfort horizontal plane parallel to the floor and the external auditory meatus under mild pressure from the cephalostat's ear rods. The radiography images' crispness and quality were assessed.
Using a PaX-i3D Green (Vatech, Hwaseong, Republic of Korea) device, qualified radiography technicians took orthopantomographies (OPGs) or panoramic radiographs and lateral cephalograms.
WEBCEPH™ is an A.I.-web-based orthodontic and orthognathic platform.
We used the WEBCEPH program (version 2.0.0) for digital tracing. Before being imported into the WebCeph, each digital image from a lateral cephalometric radiograph and panoramic radiographs was downloaded and saved to a Lenovo IdeaPad 5 Pro computer. Once the radiological images were uploaded to the WebCeph application, the system instantly recognized each anatomical site for lateral cephalometric radiographs. Both the automated and semi-automatic WebCeph options were used to identify landmarks on the digital photos, also for lateral cephalometric radiographs. The size of the images for the lateral cephalogram was 2430x3016, with a width of 2430 pixels, a height of 3016 pixels, a horizontal and vertical resolution of 96 dpi, and a bit depth of 24, and for the panoramic radiographs, it was 3070x2376, with a width of 3070 pixels, a height of 2376 pixels, a horizontal and vertical resolution of 96 dpi, and a bit depth of 24.
A calibration of 10 mm was used for the lateral cephalograms and 65 px for the linear measurements that were performed on the panoramic radiographs. We used WebCeph to import the digital radiographs that were saved as JPEG files. We used a 14" screen to perform the automated analysis. The WebCeph® (Korean Intellectual Property Office, Seoul, Republic of Korea, WebCeph, 2.0.0 AssembleCircle Corp, Pangyoyeok-ro, Bundang-gu, Seongnam-si, Gyeonggi-do, Republic of Korea) software program for digital tracing was used to perform the cephalometric analysis and measure panoramic radiographs. Both the Korean and US Intellectual Property Offices have granted patents to WEBCEPHTM's AI inventions.
Before being imported into WebCeph, each digital image greyscale file was downloaded and stored on a Lenovo IdeaPad 5 Pro computer.
Three angular measurements were made on the lateral cephalograms: the ANB angle, the FMA angle (to classify the patients in their skeletal class), and the gonial angle; linear measurements such as the height of the mandibular ramus and the length of the mandibular body were also made. On the panoramic radiographs, we had two angular measurements, the gonial angles, and linear measurements such as the height of the ascending ramus: Sigmoid notch point-Antegonion (Snp-Ag) on the right and left sides and the length of the mandibular body: Gonion-Mandibular Midpoint (Go-M), the same for the right and left sides.
Exclusion criteria in this study: patients who have had surgical orthodontic treatment in the past, patients who have had orthodontic treatment in the past of any type, patients with a history of craniofacial clefts, patients with neurological disorders, endocrine disorders, or hormonal medication, and jaw trauma facial. Inclusion criteria were patients over seven years old, patients who wanted to participate in this study, patients with good dental hygiene, patients from Romania, and patients who presented themselves for orthodontic treatment.
Measurements were taken based on these landmarks, and planes are presented in Table 1 below.
The ANB angle measures the difference between the mandible and maxilla in the sagittal plane. Skeletal class I, or 2°, is the normal value. Higher values indicate Skeletal class II. Skeletal class III corresponds to lower and even negative values.
Nasion is the most anterior point on the frontonasal suture in the medio-sagittal plane and corresponds to the root of the nose. A point represents the most posterior point on the anterior nasal spine's curvature, situated below the SNA and in front of the root of the upper central incisor. The bone contour's most posterior point lies between the SNA and Pr. B point is the most posterior point on the profile of the mandibular alveolar process, between Id and Pog—an anatomical, bony, median point.
The FMA angle allows us to see the skeletal typology in a vertical orientation. The mandibular plane and the Frankfurt plane comprise this angle. The typical value is 25 ± 3°. The growth type is normodivergent when the value falls within normal bounds. The growth type is hyperdivergent when the value exceeds 28°. Hypodivergent growth occurs when the value is less than 22°.
Frankfurt Plane made up of Po-O (Porion–Orbital); Porion is the highest (external) point on the bony border of the external auditory canal—an anatomical point, bony, bilateral. Orbital is the lowest point on the lower edge of the bony orbit. Anatomical point: bone, bilateral.
Mandibular Plane is composed of Go-Me (Gonion-Menton); a tangent between the two sites of greatest convexity on the inferior border of the mandible that forms the lower border of the mandibular body. Gonion is the most posterior, lateral, and inferior point on the external face of the angle of the mandible. Menton is the lowest point on the chin symphysis [22].
The term "gonial angle" refers to the angle that forms when a tangent touches the posterior border of the ramus at two points: the angle region (Broca) and the condyle. It has also been used to describe the posterior inferior angle region of the mandible (Brodie). In humans, the gonial angle can range from 100 to 148 degrees. Its mean angle is lowest among early Caucasians, Australians, and American Indians, and it is highest among Caucasians, Chinese, Eskimos, and Negroes. The mean angle of females is 3 to 5 degrees greater than that of males across all racial groups. According to cross-sectional studies, the gonial angle grows larger from the earliest stages of embryogenesis until birth and then continuously shrinks from birth until old age. The rate of decline is approximately half as high until adulthood, and it only decreases by a few degrees from maturity to old age. The decline is greatest before the age of six. Complete tooth loss may cause the gonial angle to become more obtuse once more, reversing the normal aging changes [23].
The mean value of Gonial Angle is 122.81±10.68. Ramus height (minus condyle and coronoid process): measured from point Snp to Ag point, the mean value is 46.22 ± 6.34, the separation between the antegonion point and the sigmoid notch point (without including the condyle and coronoid). Mandibular body length: measured from point Go to point M, the mean value is 88.52±9.35, from the gonion point to the mandibular midpoint. Sigmoid notch point (SNP): the deepest point on the sigmoid/mandibular notch. Antegonion (Ag): the highest point of the concavity or notch on the ramus's lower border where it connects to the mandibular body. Mandibular midpoint (M): by projecting the mental spine onto the lower mandibular boundary parallel to the ANS vertical plane, one can determine the mandibular midpoint (M) [21].
2.1.2. Reliability Analysis
To ensure measurement reliability, intra-rater consistency was assessed. A single examiner performed all measurements, and a randomly selected 20% of the dataset was re-analyzed after a two-week interval. The intraclass correlation coefficient (ICC) was computed, with values greater than 0.75 considered indicative of good reliability.
In the same way that they would position a patient's head in a cephalostat, radiologists positioned the skulls in three dimensions. The center axis of the skull should run parallel to the lateral film, which should appropriately cover the bilateral structures on the mandibular inferior border (Figure 1).
Figure 1 below shows the angle that we drew for this study. In figure (a) we have the FMA angle (FH plane and the mandibular plane), in figure (b) we have the ANB angle (Nasion-Apoint and the Nasion-Bpoint plane), and in figure (c) we have the gonial angle (the mandibular plane and the ramus plane's built point of junction), all drawn on a lateral cephalogram.
The Figure 2 below shows the angular measurements that were made in the WebCeph digital program. We measured the ANB angle, the FMA angle, and also measured the gonial angle. The gonial angle will be measured bilaterally on orthopantomography, as we will see below. In figure (a) we have represented the view mode line analysis, and in figure (b) we have represented the chart and the mean values, standard deviation, resultant values, severity (which is indicated by the symbol "*"; one "*" indicates the least degree of severity, and more "*" indicates a greater degree of severity), polygonal charts, and their interpretations are all shown in detail.
In Figure 3 below, we also measured ramus height and mandibular body length. In view mode, in figure (a), line analysis is presented, and in figure (b), it is represented by a chart. A detailed display of the mean values, standard deviation, resultant values, severity (represented by the symbol "*"; one "*" denotes the least degree of severity, and more "*" denotes a greater degree of severity), polygonal charts, and their interpretations is provided.
Figure 4 follows in which, (a), we showed how we calibrated the panoramic radiographs for the linear measurements at 65 pixels, taking the reference and the vertical ruler next to it. Since the technique used to obtain panoramic radiographs greatly distorts the horizontal length, it can be difficult to quantify the horizontal dimension accurately. Measurements taken vertically are generally more accurate than those taken horizontally because the vertical dimension is less susceptible to this kind of distortion. In general, panoramic radiographs are sufficiently distorted, and it is challenging to offer a uniform pixel conversion value since different radiography machines provide varying image sizes.
In figure (b) we measured ramus height from Snp-Ag (sigmoid notch point and antegonion) and mandibular body length Go-M (mandibular midpoint and gonion). These measurements were performed bilaterally for both the right and left sides. In figures (c) and (d) we showed how we drew digitally.
In Figure 5 we present the angular measurements we performed in this study; we measured the gonial angles bilaterally, on both sides, the results being very similar to the results we obtained by performing these measurements on the lateral cephalograms.
In order to measure, a line tangent to the mandibular lower border and another line tangent to the distal border of the ascending ramus and the condyle on either side were drawn.
3. Results
Our sample, comprising 128 individuals, provides an analysis of several mandibular and craniofacial parameters with a balanced gender distribution, with 52% female (n=67) and 48% male (n=61) participants. The median age of the cohort is 21 years, with an interquartile range (IQR) of 16 to 29 years, indicating a relatively young study population.
The functional mandibular angle (FMA) exhibits a median value of 22, with an IQR of 17 to 25, reflecting the range of mandibular growth and development among the participants. The gonial angle assessed using cephalometric methods presents a median of 121 degrees (IQR: 116–127), which suggests a consistent anatomical configuration across the cohort. Measurements of the mandibular ramus height using cephalometry imaging reveal a median value of 44 mm (IQR: 41–48 mm), indicating minimal variation in vertical ramus dimensions. The mandibular body length assessed via cephalometric methods has a median value of 70 mm, with an IQR of 65 to 76 mm, demonstrating uniformity in horizontal mandibular development. Orthopantomography (OPG) assessments of the gonial angle on the right and left sides yield medians of 121 degrees (IQR: 116–127) and 122 degrees (IQR: 117–127), respectively, confirming symmetry in angular measurements. Similarly, mandibular ramus height measurements using OPG on the right and left sides show medians of 44.0 mm (IQR: 40.0–47.0 mm) and 43 mm (IQR: 40–48 mm), with negligible side-to-side differences.
The mandibular body width measured through OPG is consistent across sides, with the right side presenting a median of 71 mm (IQR: 67–76 mm) and the left side having a median of 71 mm (IQR: 67–75 mm). These findings underscore the symmetrical and proportional mandibular architecture within the study population (Table 2).
Table 3 presents a comparison of craniofacial measurements between female and male participants, analyzing differences across variables such as age, gonial angles, mandibular ramus height, and mandibular body dimensions. A total of 128 participants were included, with 67 females and 61 males.
The median age of the male group (23.0 years; IQR: 15.7–30.7) was slightly higher than that of the female group (21.0 years; IQR: 17.0–26.0), but this difference was not statistically significant (P = 0.42). Similarly, the FMA angle showed comparable distributions between females (median: 21.0°; IQR: 16.0–25.0) and males (median: 22.0°; IQR: 18.7–26.0), with no significant difference (P = 0.50).
Significant differences were observed in gonial angles measured on lateral cephalograms and panoramic radiographs. The Gonial Angle (lateral ceph) was higher in males (median: 123.4°; IQR: 118.5–128.9) compared to females (median: 120.4°; IQR: 115.4–125.2), with a significant P-value of 0.01. The gonial angle on the right side measured on OPG was also larger in males (median: 123.0°; IQR: 117.0–129.0) than in females (median: 120.0°; IQR: 114.9–125.8), with P = 0.01. However, no significant difference was noted for the left gonial angle (P = 0.20).
Mandibular ramus height measurements revealed consistent differences, with males exhibiting significantly greater heights than females across all methods and sides. For instance, mandibular ramus height (lateral ceph) was 46.9 mm (IQR: 42.0–52.1) in males, compared to 41.9 mm (IQR: 38.5–45.0) in females (P < 0.01). The same trend was observed in right and left ramus heights measured on OPG, with males showing significantly higher values (P < 0.01 for both).
Mandibular body dimensions also demonstrated significant sex differences. Males had longer mandibular bodies measured on lateral cephalometric radiographs (median: 73.0 mm; IQR: 66.7–77.3) compared to females (median: 69.8 mm; IQR: 64.7–73.9), with P = 0.01. Similarly, mandibular body widths on both the right and left sides measured on OPG were larger in males than females, with significant P-values of <0.01 and 0.02, respectively.
For the gonial angle on Lateral Ceph, the median gonial angle remains consistent across all age groups. The variability is moderate, and the whiskers show no extreme deviation from the central tendency. Some outliers are observed in the 0-18 and 19-30 groups (Figure 6).
For the height of mandibular ramus on Lateral Ceph, the median height remains consistent across the age groups (0-18, 19-30, 31+). The variability within each group, as represented by the interquartile range, is relatively small. A few outliers are observed, particularly in the younger (0-18) and middle (19-30) age groups (Figure 7 ).
For the length of the mandibular body on Lateral Ceph, the median length appears stable across the three age groups. The 19-30 age group shows a slightly wider interquartile range compared to the others. Outliers are present in all age groups, with a higher concentration in the 19-30 group (Figure 8).
Table 4 presents the correlation matrix for mandibular ramus height measurements from Lateral Ceph and orthopantomography (OPG) methods. Spearman's correlation coefficient indicates the strength of the monotonic relationship between the variables. High positive correlations were found between the measurements. For instance, the correlation between Ramus Height Lateral Ceph and Ramus Height Right OPG was 0.901, with a 95% confidence interval ranging from 0.863 to 0.930, and the relationship was statistically significant (p < 0.001). Similarly, the correlation between Ramus Height Lateral Ceph and Ramus Height Left OPG was 0.844, also statistically significant (p < 0.001). The correlation between the right and left OPG ramus height measurements was 0.800, with a confidence interval of 0.725 to 0.855, and was also statistically significant (p < 0.001). The high correlations suggest strong consistency and agreement between the cephalometry and OPG methods for measuring mandibular ramus height.
Table 5 summarizes the correlation between gonial angle measurements using cephalometric imaging (lateral ceph) and orthopantomography or panoramic radiograph (OPG) methods (right and left). Spearman's rho (rs) was used to evaluate monotonic relationships, and results are presented with degrees of freedom and significance levels.
Strong positive correlations were observed between Gonial Angle Lateral Ceph and both OPG measurements. For instance, the correlation between Gonial Angle Lateral Ceph and Gonial Angle Right OPG was 0.946 (p < 0.001), indicating a near-perfect monotonic relationship. Similarly, the correlation between Gonial Angle Lateral Ceph and Gonial Angle Left OPG was 0.858 (p < 0.001). The correlation between the right and left OPG measurements was also strong, with rs = 0.811 (p < 0.001).
Males demonstrated consistently larger craniofacial measurements, including gonial angles, ramus heights, and mandibular body dimensions, compared to females. These findings highlight the anatomical differences between sexes, which are critical for individualized orthodontic and surgical planning. Variables such as age and FMA angle did not show significant differences between sexes, suggesting that other factors primarily drive the observed differences in craniofacial measurements.
4. Discussion
This study aimed to evaluate the accuracy of digital orthopantomography (OPG) or panoramic radiography in determining angular and linear craniofacial measurements compared to lateral cephalograms, focusing on their applicability in diagnosing facial asymmetry and skeletal patterns. The findings demonstrated that while angular measurements on OPGs, such as the gonial angle, exhibit strong correlations with lateral cephalometric counterparts, linear vertical measurements like mandibular body length showed weaker correlations.
The gonial angle measurements on OPGs showed strong positive correlations with lateral cephalograms (rs = 0.946, p < 0.001 for the right side; rs = 0.858, p < 0.001 for the left side). These results align with prior research by Shahabi et al. [2] and Larheim and Svanaes [24], confirming the reliability of OPGs for angular assessments. This consistency highlights the utility of OPGs in evaluating angular relationships of the mandible, especially in diagnosing facial asymmetry. Similarly, mandibular ramus height measurements on OPGs also correlated strongly with lateral cephalograms (rs = 0.901, p < 0.001), supporting the findings of Ongkosuwito et al. [25] that vertical measurements on OPGs are generally accurate under optimal conditions.
However, mandibular body length showed weaker correlations between the two modalities, emphasizing the limitations of OPGs for horizontal measurements. This discrepancy can be attributed to the inherent magnification and distortion in panoramic imaging, as noted by Tronje et al. [26], where horizontal dimensions are particularly susceptible to non-linear distortion.
Our findings align with earlier studies suggesting that panoramic radiographs can be a reliable adjunct for angular and vertical measurements, provided the patient is appropriately positioned. For instance, Mattila et al. [27] reported that gonial angles on OPGs closely matched those measured on dry skulls. Conversely, studies like those by Nohadani and Ruf [28] highlighted the limitations of OPGs for longitudinal evaluation of vertical facial dimensions, consistent with our results for mandibular body length.
While Akcam et al. [29] and Kurt et al. [30] emphasized the utility of OPGs for assessing skeletal patterns and mandibular asymmetry, they also cautioned against over-reliance on OPGs for precise quantitative assessments of horizontal parameters. This study corroborates these findings, particularly for mandibular body length, which exhibited weaker agreement between the two imaging modalities.
The strong correlation between angular measurements on OPGs and lateral cephalograms underscores the potential of OPGs as a preliminary diagnostic tool in orthodontics. OPGs provide the advantage of visualizing the right and left sides separately without the superimposition challenges inherent in lateral cephalograms. This makes them particularly useful in assessing facial asymmetry and angular relationships in clinical practice.
However, caution is warranted when interpreting linear measurements from OPGs. As noted, the prediction percentages for horizontal and vertical measurements remain low due to nonlinear distortion and inconsistent magnification factors [14,26]. Thus, while OPGs are valuable for initial screening, lateral cephalograms remain the gold standard for precise cephalometric analysis.
5. Limitations and Future Directions
Despite the promising findings, this study has several limitations. First, the sample size, while robust, was restricted to Romanian patients, potentially limiting the generalizability of the results. Second, variability in patient positioning during OPG acquisition, despite standardized protocols, may have influenced the accuracy of certain measurements. Additionally, the study focused solely on two-dimensional imaging modalities, excluding emerging three-dimensional technologies like cone-beam computed tomography (CBCT), which offer superior accuracy for craniofacial assessments.
Future research should aim to standardize OPG acquisition protocols further, minimizing variability caused by patient positioning and equipment settings. Larger, multicenter studies involving diverse populations are needed to establish normative values for panoramic metrics and validate their consistency across different imaging systems. Additionally, integrating artificial intelligence algorithms to enhance landmark detection and measurement accuracy on OPGs may help address current limitations [15,17]. Comparative studies involving CBCT should also be conducted to explore its potential as a complementary or alternative diagnostic tool to OPGs and lateral cephalograms.
6. Conclusions
This study highlights the utility of OPGs for angular and vertical mandibular measurements, offering a reliable, non-invasive, and cost-effective option for initial orthodontic assessments. However, their limitations for horizontal measurements necessitate careful interpretation and the complementary use of lateral cephalograms when precision is paramount. Standardizing OPG protocols and leveraging advancements in imaging technologies are essential steps toward enhancing their diagnostic potential. While OPGs cannot replace lateral cephalograms entirely, they remain a valuable adjunct in orthodontic diagnostics, particularly for assessing asymmetry and angular parameters.
Author Contributions
Conceptualization: A.-A.S., C.-A.S.; methodology: A.C.M.; validation: A.C.M., R.N., A.P., and C.-A.S.; formal analysis: A.C.M., A.-A.S., L.V., and A.A.H.; investigation: A.-A.S., A.A.H., L.V., and A.C.M.; resources: C.-A.S.; data curation: A.-A.S.; writing—original draft preparation: A.-A.S.; writing—review and editing: C.-A.S., A.-A.S.; visualization: R.N. and A.P.; supervision: C.-A.S.; project administration: C.-A.S. All authors have read and agreed to the published version of the manuscript.
Funding
We would like to acknowledge VICTOR BABES UNIVERSITY OF MEDICINE AND PHARMACY TIMIȘOARA for their support in covering the costs of publication for this research paper.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Institutional Ethics Committee of University of Medicine and Pharmacy Victor Babes Timisoara, Romania (CECS Nr. 04/26.01.2024).
Informed Consent Statement
All subjects involved in the study gave their informed consent.
Data Availability Statement
All data regarding this manuscript can be requested from the corresponding author at alexandru.motofelea@umft.ro.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Tashkandi, N.E.; Alnaqa, N.H.; Al-Saif, N.M.; Allam, E. Accuracy of Gonial Angle Measurements Using Panoramic Imaging versus Lateral Cephalograms in Adults with Different Mandibular Divergence Patterns. J. Multidiscip. Healthc. 2024, 1923–1929. [Google Scholar] [CrossRef]
- Shahabi, M.; Ramazanzadeh, B.A.; Mokhber, N. Comparison between the external gonial angle in panoramic radiographs and lateral cephalograms of adult patients with Class I malocclusion. J. Oral Sci. 2009, 51, 425–429. [Google Scholar] [CrossRef] [PubMed]
- Choi, J.Y.; Oh, S.H.; Kim, S.H.; Ahn, H.W.; Kang, Y.G.; Choi, Y.S.; Nelson, G. Effectiveness of 2D Radiographs in Detecting CBCT-Based Incidental Findings in Orthodontic Patients. Sci. Rep. 2021, 11, 9280. [Google Scholar] [CrossRef] [PubMed]
- Farman, A.G. Panoramic Radiographic Assessment in Orthodontics. In Panoramic Radiology: Seminars on Maxillofacial Imaging and Interpretation; Langlais, R.P., Langland, O.E., Eds.; Springer: Berlin, Heidelberg, 2007; pp. 83–89. [Google Scholar]
- Broadbent, B.H. A New X-Ray Technique and Its Application to Orthodontia. Angle Orthod. 1931, 1(2), 45–66. [Google Scholar]
- Hwang, S.A.; Lee, J.S.; Hwang, H.S.; Lee, K.M. Benefits of Lateral Cephalogram During Landmark Identification on Posteroanterior Cephalograms. Korean J. Orthod. 2019, 49(1), 32–40. [Google Scholar] [CrossRef] [PubMed]
- El-Mangoury, N.H.; Shaheen, S.I.; Mostafa, Y.A. Landmark Identification in Computerized Posteroanterior Cephalometrics. Am. J. Orthod. Dentofac. Orthop. 1987, 91(1), 57–61. [Google Scholar] [CrossRef]
- Major, P.W.; Johnson, D.E.; Hesse, K.L.; Glover, K.E. Landmark Identification Error in Posterior Anterior Cephalometrics. Angle Orthod. 1994, 64(6), 447–454. [Google Scholar] [PubMed]
- Athanasiou, A.E.; Miethke, R.R.; Van Der Meij, A.J.W. Random Errors in Localization of Landmarks in Postero-Anterior Cephalograms. Br. J. Orthod. 1999, 26(4), 273–284. [Google Scholar] [CrossRef]
- Haraguchi, S.; Iguchi, Y.; Takada, K. Asymmetry of the Face in Orthodontic Patients. Angle Orthod. 2008, 78(3), 421–426. [Google Scholar] [CrossRef]
- Chia, M.S.; Naini, F.B.; Gill, D.S. The Aetiology, Diagnosis, and Management of Mandibular Asymmetry. Orthod. Update 2008, 1(2), 44–52. [Google Scholar] [CrossRef]
- Cheong, Y.W.; Lo, L.J. Facial Asymmetry: Etiology, Evaluation, and Management. Chang Gung Med. J. 2011, 34(4), 341–351. [Google Scholar] [PubMed]
- Gupta, S.; Jain, S. Orthopantomographic Analysis for Assessment of Mandibular Asymmetry. J. Indian Orthod. Soc. 2012, 46(1), 33–37. [Google Scholar] [CrossRef]
- Kumar, S.S.; Thailavathy, V.; Srinivasan, D.; Loganathan, D.; Yamini, J. Comparison of Orthopantomogram and Lateral Cephalogram for Mandibular Measurements. J. Pharm. Bioallied Sci. 2017, 9 (Suppl. 1), S92–S95. [Google Scholar] [PubMed]
- Kim, Y.-H.; Park, J.-B.; Chang, M.-S.; Ryu, J.-J.; Lim, W.H.; Jung, S.-K. Influence of the Depth of the Convolutional Neural Networks on an Artificial Intelligence Model for Diagnosis of Orthognathic Surgery. J. Pers. Med. 2021, 11, 356. [Google Scholar] [CrossRef] [PubMed]
- Ahn, J.H.; Bae, K.H.; Park, Y.J.; Hong, R.K.; Nam, J.H.; Kim, M.J. Assessment of Antero-Posterior Skeletal Relationships in Adult Korean Patients in the Natural Head Position and Centric Relation. Korean J. Orthod. 2010, 40(6), 421–431. [Google Scholar] [CrossRef]
- Alam, M.K.; Alfawzan, A.A. Dental Characteristics of Different Types of Cleft and Non-cleft Individuals. Front. Cell Dev. Biol. 2020, 8, 789. [Google Scholar] [CrossRef] [PubMed]
- Alam, M.K.; Alfawzan, A.A. Evaluation of Sella Turcica Bridging and Morphology in Different Types of Cleft Patients. Front. Cell Dev. Biol. 2020, 8, 656. [Google Scholar] [CrossRef]
- Xiong, X.; Zhang, Q.; Liu, Y. Correlations between Mandibular Ramus Height and Occlusal Planes in Han Chinese Individuals with Normal Occlusion: A Cross-Sectional Study. APOS Trends Orthod. 2021, 11(3), 261–266. [Google Scholar] [CrossRef]
- Radhakrishnan, P.D.; Varma, N.K.S.; Ajith, V.V. Dilemma of Gonial Angle Measurement: Panoramic Radiograph or Lateral Cephalogram. Imaging Sci. Dent. 2017, 47(2), 93–97. [Google Scholar] [CrossRef]
- Al-Gunaid, T.H.; Bukhari, A.K.; El Khateeb, S.M.; Yamaki, M. Relationship of Mandibular Ramus Dimensions to Lower Third Molar Impaction. Eur. J. Dent. 2019, 13, 213–221. [Google Scholar] [CrossRef]
- Szuhanek, C.; Schiller, A.; Grigore, A.; Popa, L. Ghid Ortodonție; Editura Victor Babeș: 2019.
- Jensen, E.; Palling, M. The Gonial Angle: A Survey. Am. J. Orthod. 1954, 40, 120–133. [Google Scholar] [CrossRef]
- Larheim, T.A.; Svanaes, D.B. Reproducibility of Rotational Panoramic Radiography: Mandibular Linear Dimensions and Angles. Am. J. Orthod. Dentofacial Orthop. 1986, 90, 45–51. [Google Scholar] [CrossRef]
- Ongkosuwito, E.M.; Dieleman, M.M.; Kuijpers-Jagtman, A.M.; Mulder, P.G.; van Neck, J.W. Linear Mandibular Measurements: Comparison between Orthopantomograms and Lateral Cephalograms. Cleft Palate Craniofac. J. 2009, 46, 147–153. [Google Scholar] [CrossRef]
- Tronje, G.; Welander, U.; McDavid, W.D.; Morris, C.R. Image Distortion in Rotational Panoramic Radiography: IV. Object Morphology; Outer Contours. Acta Radiol. Diagn. 1981, 22, 689–696. [Google Scholar] [CrossRef] [PubMed]
- Mattila, K.; Altonen, M.; Haavikko, K. Determination of the Gonial Angle from the Orthopantomogram. Angle Orthod. 1977, 47, 107–110. [Google Scholar] [PubMed]
- Nohadani, N.; Ruf, S. Assessment of Vertical Facial and Dentoalveolar Changes Using Panoramic Radiography. Eur. J. Orthod. 2008, 30, 262–268. [Google Scholar] [CrossRef] [PubMed]
- Akcam, M.O.; Altiok, T.; Ozdiler, E. Panoramic radiographs: A tool for investigating skeletal pattern. Am. J. Orthod. Dentofacial Orthop. 2003, 123, 175–181. [Google Scholar] [CrossRef]
- Kurt, G.; Uysal, T.; Sisman, Y.; Ramoglu, S.I. Mandibular Asymmetry in Class II Subdivision Malocclusion. Angle Orthod. 2008, 78, 32–37. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
(a) ANB angle, (b) FMA angle, and (c) gonial angle.
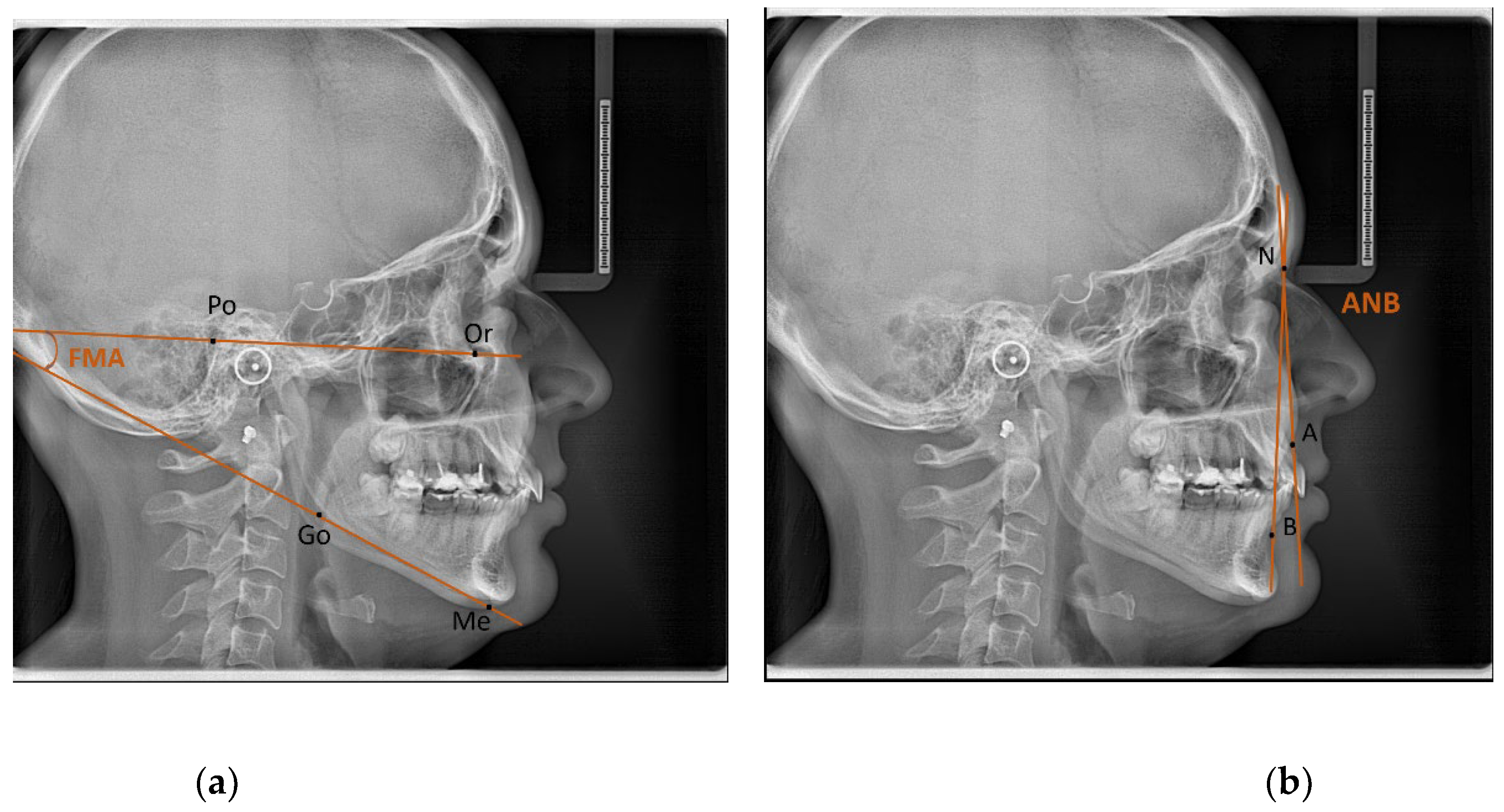
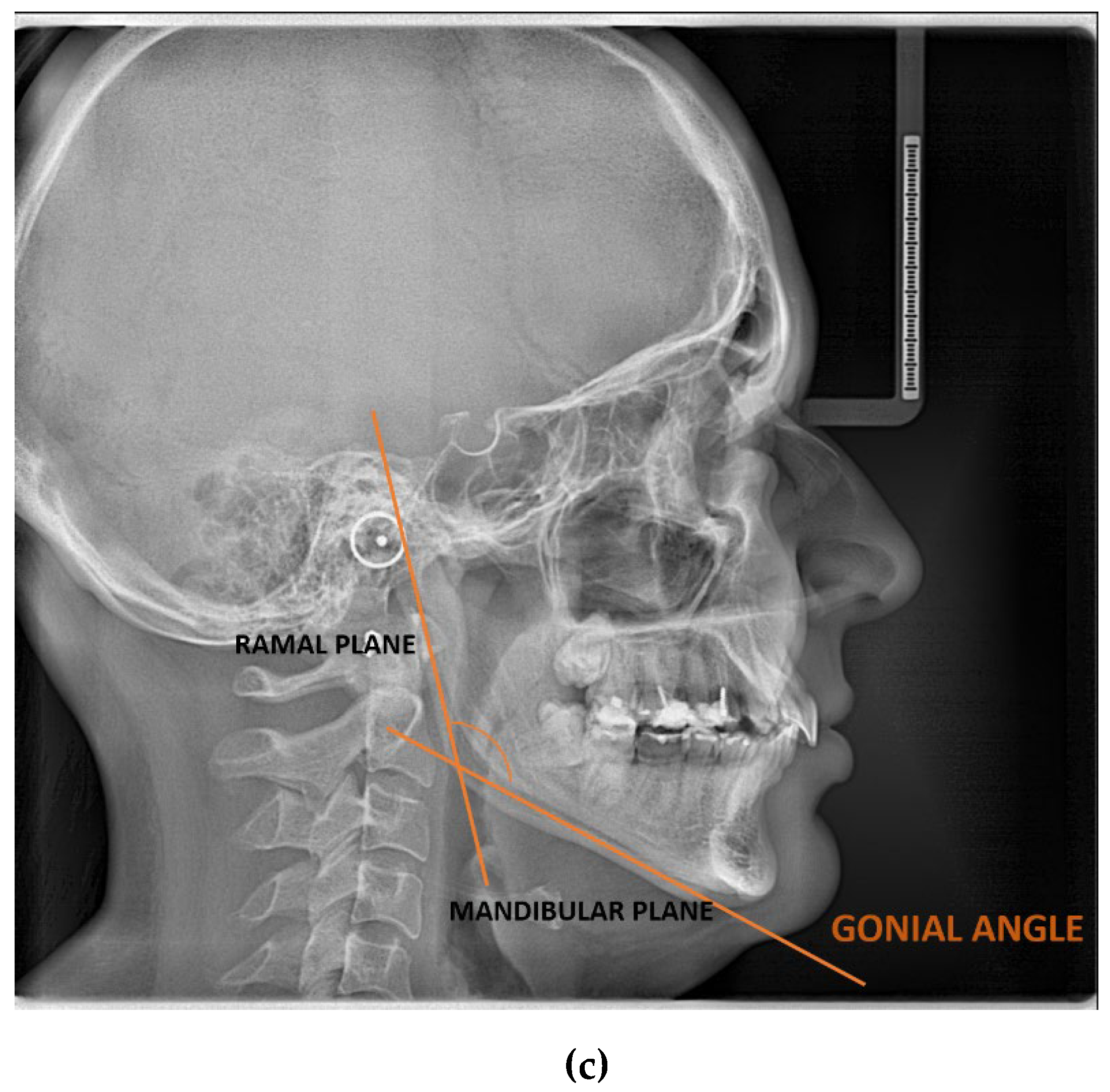
Figure 2.
The WebCeph digital program in which we measured the ANB angle, the FMA angle, and the gonial angle. (a) image view mode by line analysis and image (b) by a chart.
Figure 2.
The WebCeph digital program in which we measured the ANB angle, the FMA angle, and the gonial angle. (a) image view mode by line analysis and image (b) by a chart.
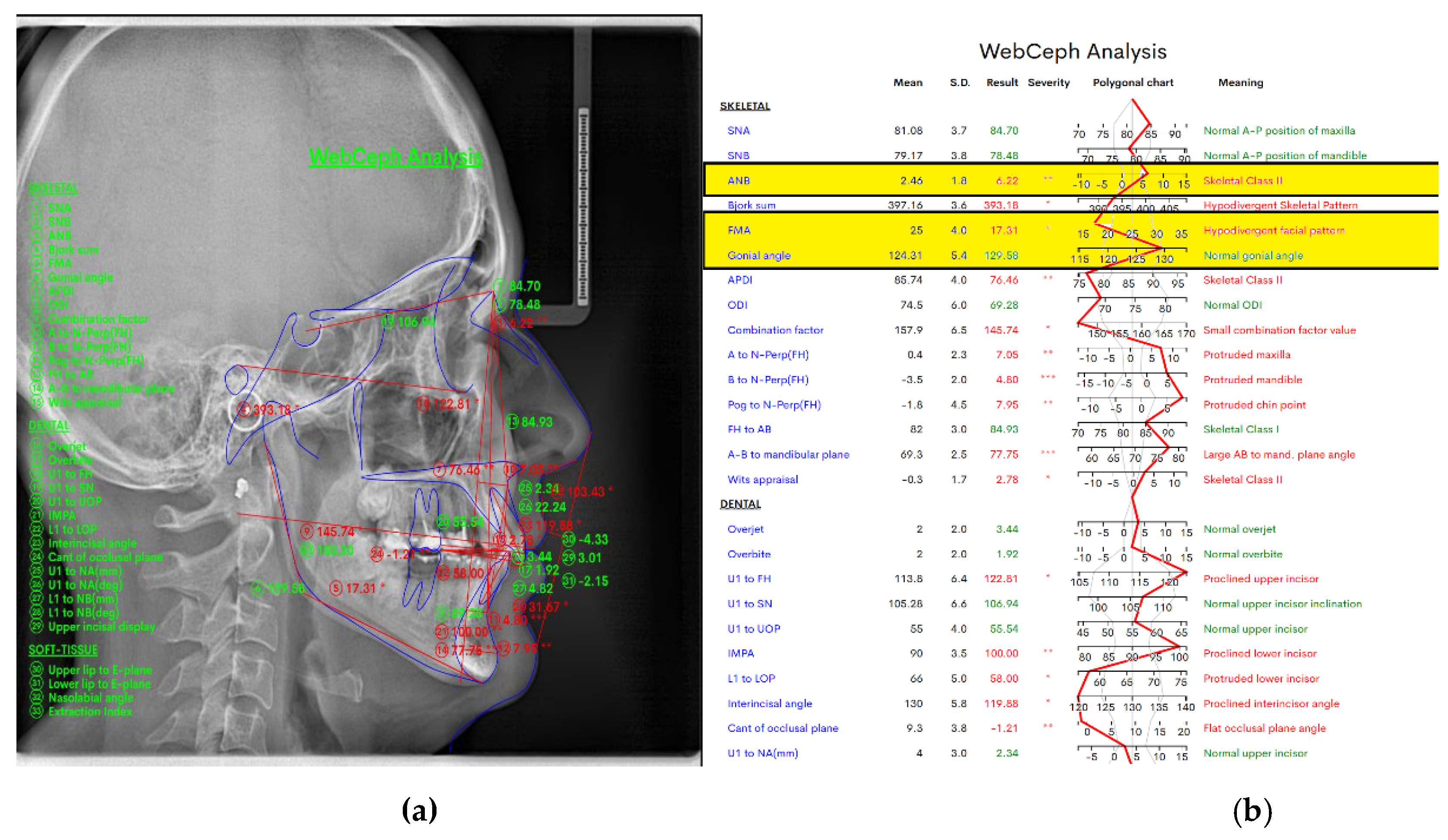
Figure 3.
In the WebCeph digital program, we measured ramus height and mandibular body length (a) in figure view mode by line analysis and image (b) by a chart.
Figure 3.
In the WebCeph digital program, we measured ramus height and mandibular body length (a) in figure view mode by line analysis and image (b) by a chart.
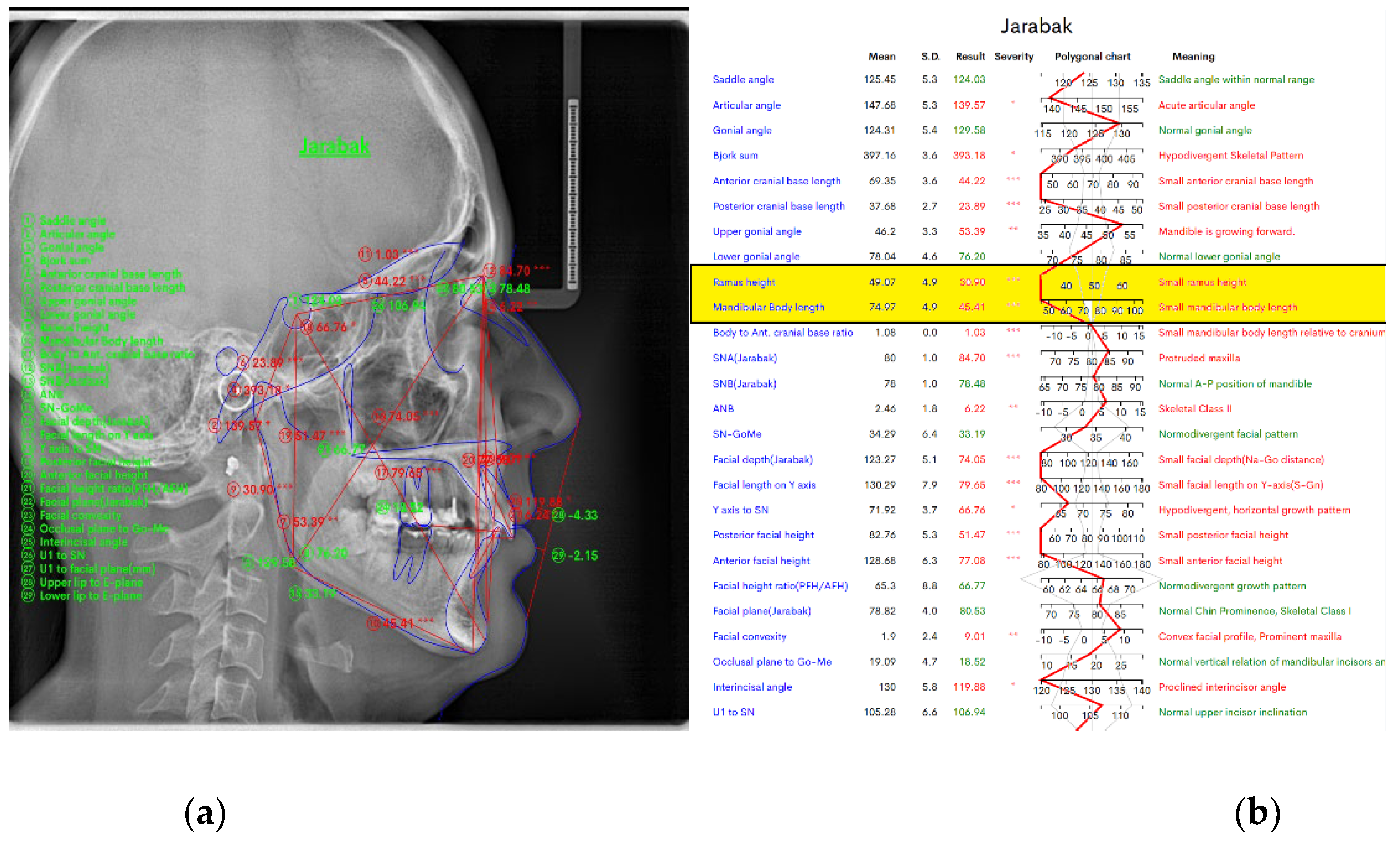
Figure 4.
The WebCeph digital program in which image (a) the calibration for the linear measurements performed, image (b) it represents the linear measurements performed: ramus height and mandibular body length. Figure (c) ramus height and (d) mandibular body length show exactly as we drew.
Figure 4.
The WebCeph digital program in which image (a) the calibration for the linear measurements performed, image (b) it represents the linear measurements performed: ramus height and mandibular body length. Figure (c) ramus height and (d) mandibular body length show exactly as we drew.
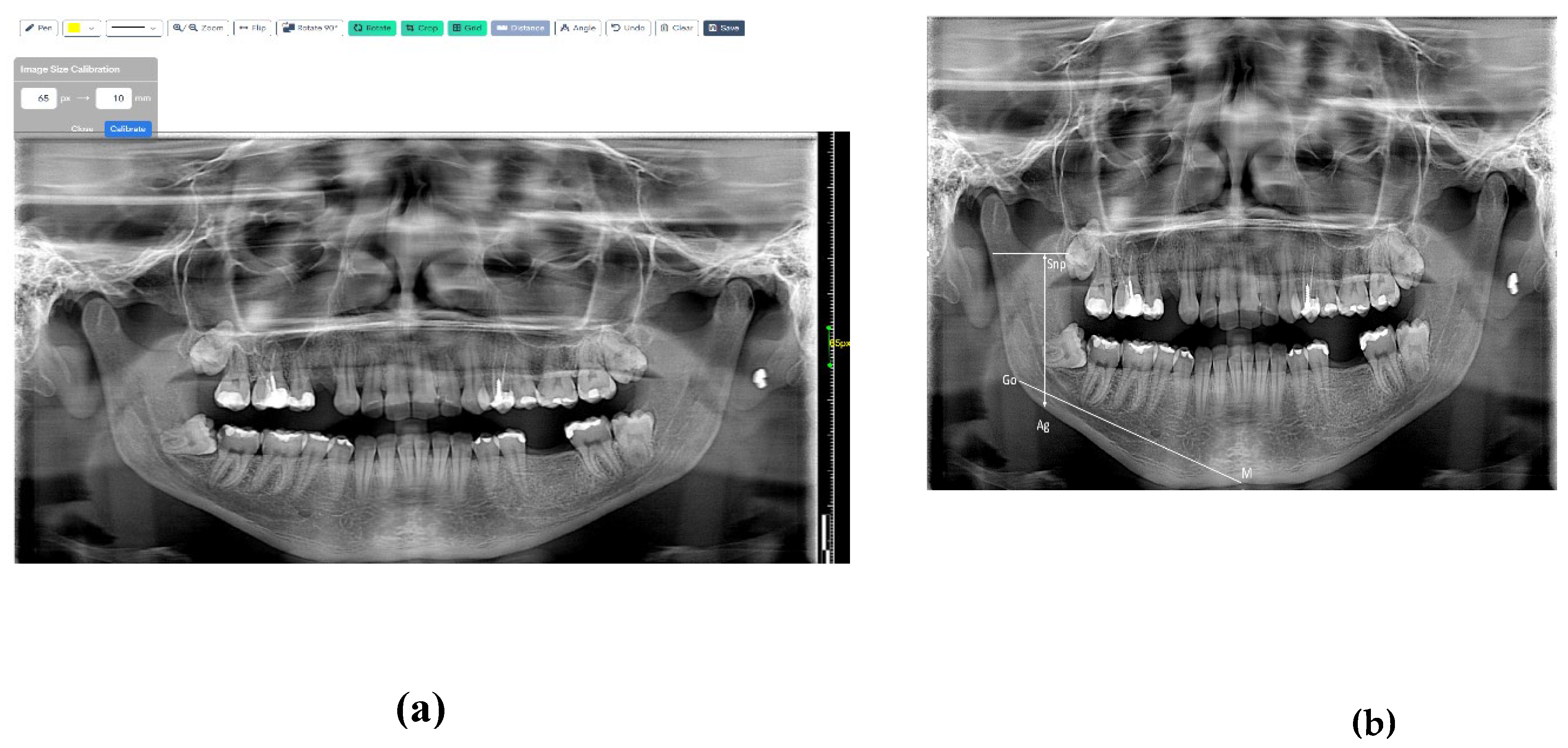
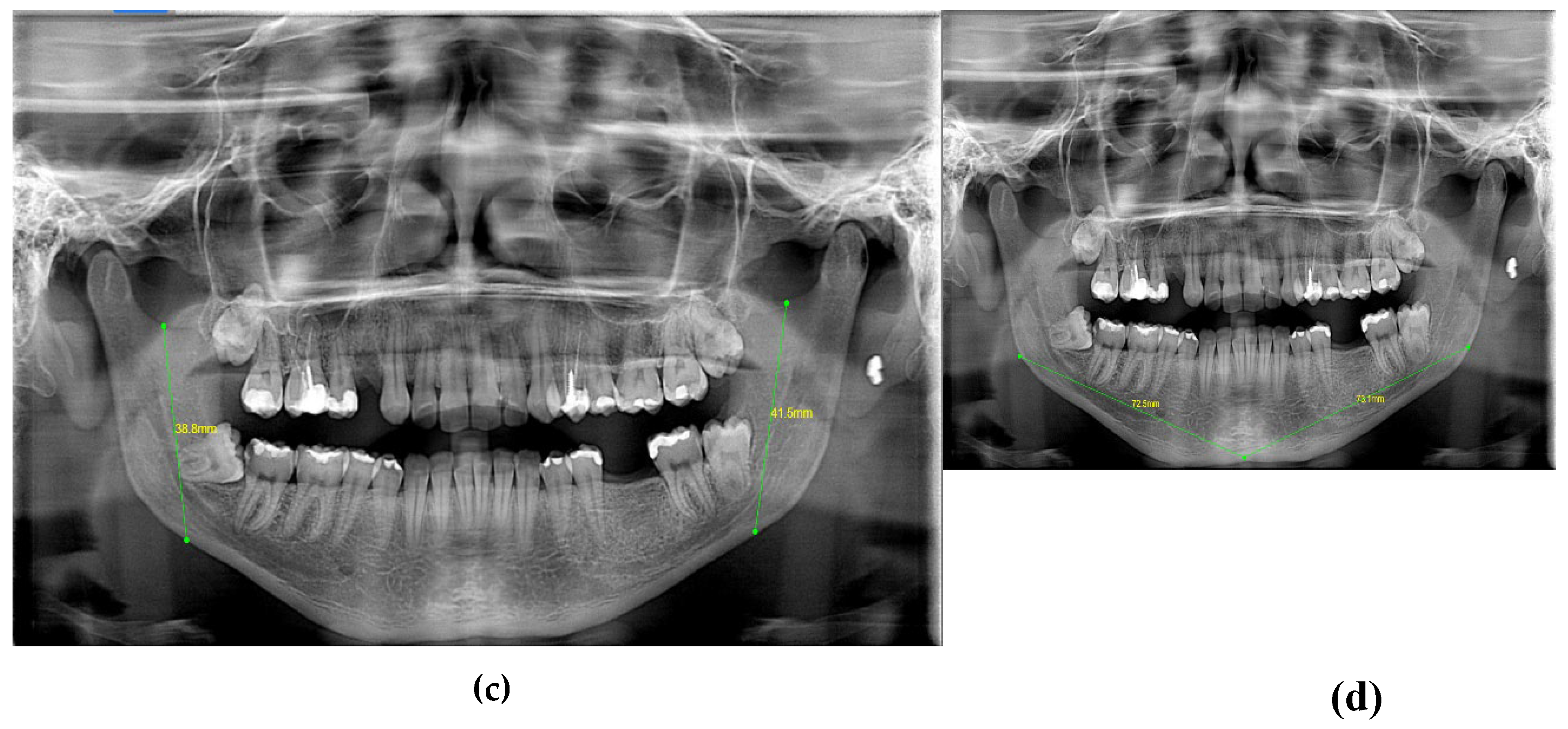
Figure 5.
The WebCeph digital program—two lines were drawn: one tangent to the lower border of the mandible and the other to the distal border of the ascending ramus and the condyle on either side.
Figure 5.
The WebCeph digital program—two lines were drawn: one tangent to the lower border of the mandible and the other to the distal border of the ascending ramus and the condyle on either side.

Figure 6.
Age-Wise Comparison of Gonial Angle Lateral Ceph.
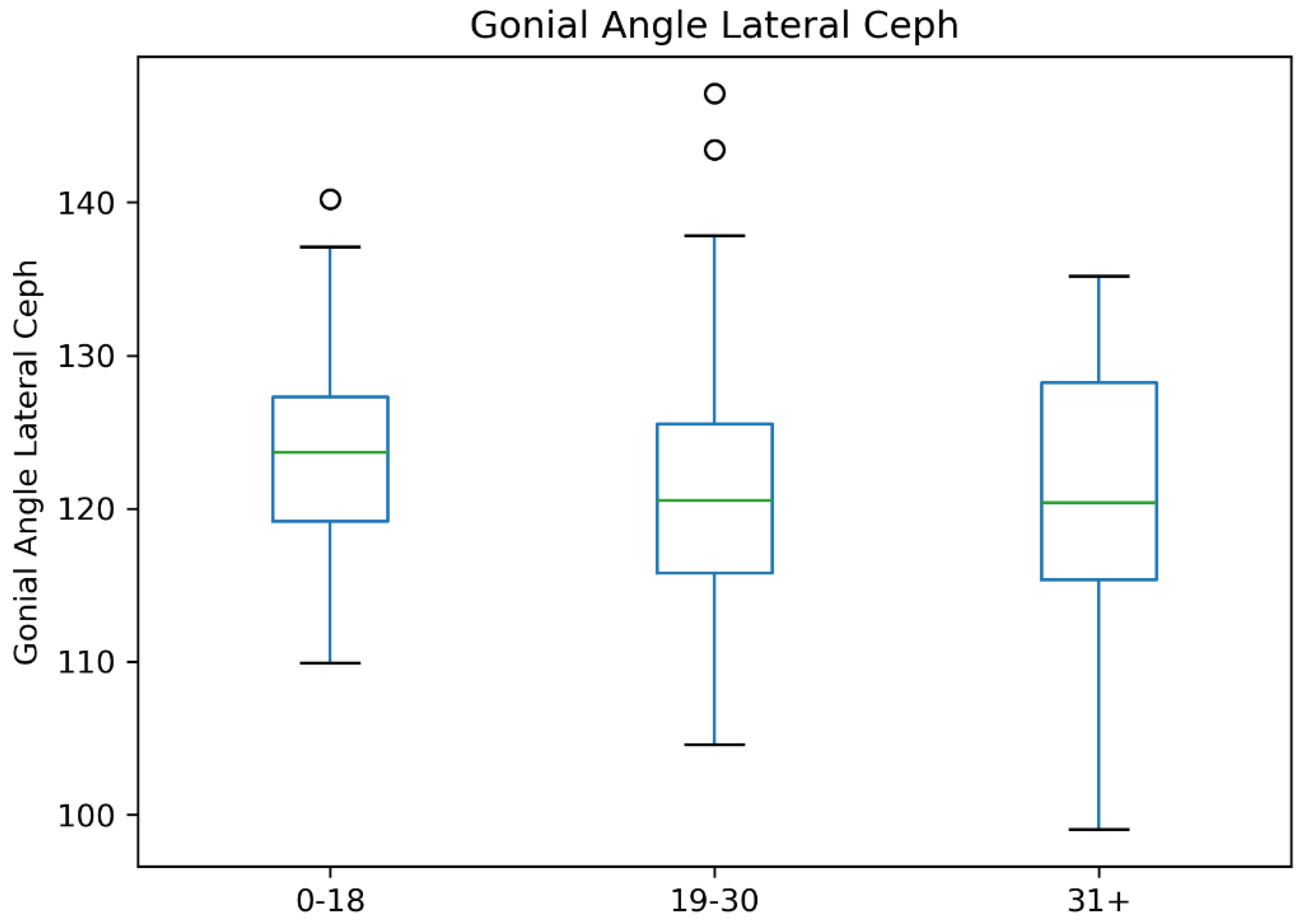
Figure 7.
Comparison of Mandibular Ramus Height Across Age Groups.
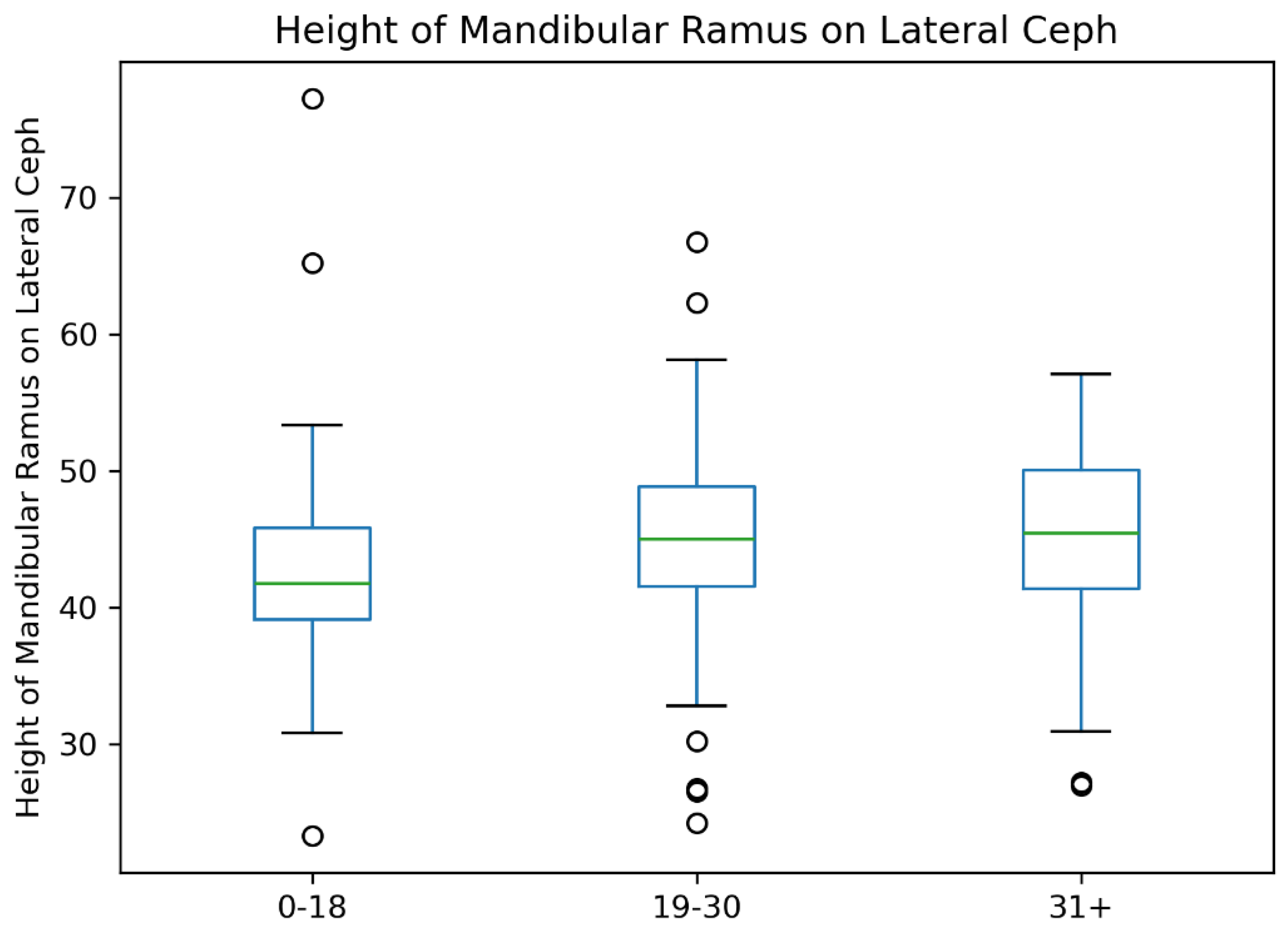
Figure 8.
Mandibular Body Length Distribution by Age Groups.
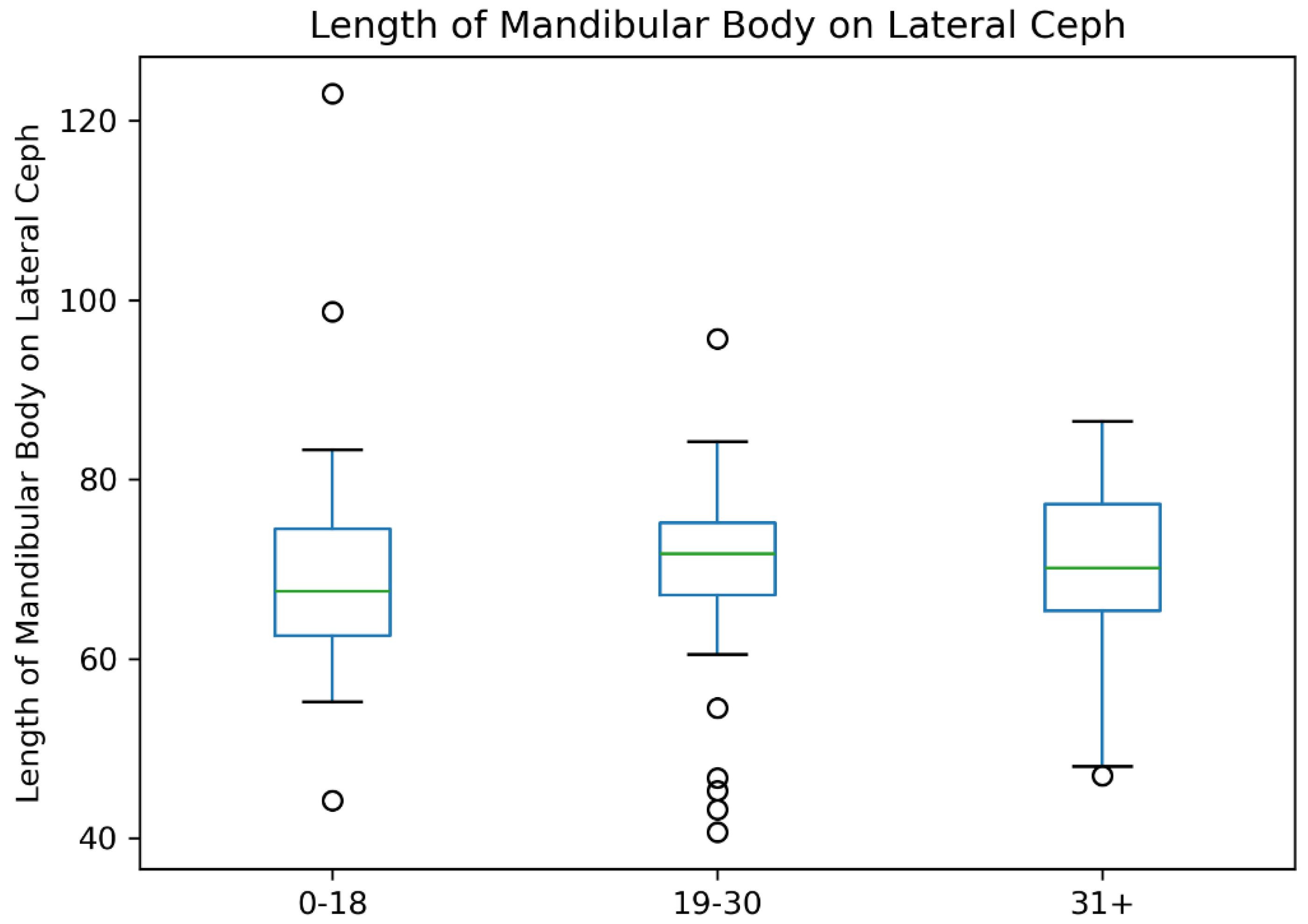

Table 1.
Measurement and landmark list.
| S. No. | Measurement | Description |
|---|---|---|
| 1 | ANB (°) | Angle between the Nasion-A point and the Nasion-B point plane [19]. |
| 2 | FMA (°) | Angle formed by the FH plane and the mandibular plane [19]. |
| 3 | GONIAL ANGLE (°) | At lateral cephalograms, it was determined at the junction of the mandibular and ramus planes. A line tangent to the lower border of the mandible and another line tangent to the distal border of the ascending ramus and the condyle on either side were drawn in order to measure the gonial angle in the panoramic radiographs [20]. The mandibular plane and the ramus plane’s built point of junction. |
| 4 | RAMUS HEIGHT | (mm) The distance between Ag and Snp [21]. |
| 5 | MANDIBULAR BODY LENGTH | (mm) The distance between point Go and point M [21]. |
FH plane-Frankfort plane, Ag-antegonion, Snp-sigmoid notch point, Go-Gonion, M-mandibular midpoint.
Table 2.
Patients baseline characteristics.
| Characteristic | N = 128 |
|---|---|
| Sex | |
| Female (F) | 67 (52%) |
| Male (M) | 61 (48%) |
| Age | 21 (16, 29) |
| FMA | 22 (17, 25) |
| Gonial Angle (Lateral Ceph) | 121 (116, 127) |
| Mandibular Ramus Height (Lateral Ceph) | 44 (41, 48) |
| Mandibular Body Length (Lateral Ceph) | 70 (65, 76) |
| Gonial Angle Right (OPG) | 121 (116, 127) |
| Gonial Angle Left (OPG) | 122 (117, 127) |
| Mandibular Ramus Height Right (OPG) | 44.0 (40.0, 47.0) |
| Mandibular Ramus Height Left (OPG) | 43 (40, 48) |
| Mandibular Body Width Right (OPG) | 71 (67, 76) |
| Mandibular Body Width Left (OPG) | 71 (67, 75) |
Table 3.
Comparison of Craniofacial Measurements Between Female and Male Participants.
| Variable | N | Female (F) (N = 67) (Median, Q1, Q3) | Male (M) (N = 61) (Median, Q1, Q3) | P-Value |
|---|---|---|---|---|
| Age (years) | 128 | 21.0 (17.0, 26.0) | 23.0 (15.7, 30.7) | 0.42 |
| FMA (°) | 121 | 21.0 (16.0, 25.0) | 22.0 (18.7, 26.0) | 0.5 |
| Gonial Angle (Lateral Ceph) (°) | 128 | 120.4 (115.4, 125.2) | 123.4 (118.5, 128.9) | 0.01 |
| Mandibular Ramus Height (Lateral Ceph) (mm) | 128 | 41.9 (38.5, 45.0) | 46.9 (42.0, 52.1) | <0.01 |
| Mandibular Body Length (Lateral Ceph) (mm) | 128 | 69.8 (64.7, 73.9) | 73.0 (66.7, 77.3) | 0.01 |
| Gonial Angle Right (OPG) (°) | 128 | 120.0 (114.9, 125.8) | 123.0 (117.0, 129.0) | 0.01 |
| Gonial Angle Left (OPG) (°) | 128 | 123.0 (116.2, 125.0) | 122.0 (117.0, 129.0) | 0.2 |
| Mandibular Ramus Height Right (OPG) (mm) | 126 | 42.0 (39.0, 45.0) | 46.0 (42.7, 50.0) | <0.01 |
| Mandibular Ramus Height Left (OPG) (mm) | 126 | 42.0 (38.0, 44.3) | 47.0 (42.0, 51.0) | <0.01 |
| Mandibular Body Width Right (OPG) (mm) | 128 | 69.5 (66.3, 74.0) | 73.7 (69.1, 77.2) | <0.01 |
| Mandibular Body Width Left (OPG) (mm) | 127 | 70.0 (66.0, 74.1) | 72.0 (69.0, 76.3) | 0.02 |
Data are presented as median (Q1, Q3). Measurements are in degrees (°) for angular values and millimeters (mm) for linear dimensions. Statistical significance was determined using the Wilcoxon test.
Table 4.
Correlation Matrix for Mandibular Ramus Heights.
| Variable | Ramus Height Lateral Ceph | Ramus Height Right OPG | Ramus Height Left OPG |
|---|---|---|---|
| Ramus Height Lateral Ceph | — | ||
| Spearman’s rho | — | 0.901 (95% CI: 0.863, 0.930) | 0.844 (95% CI: 0.785, 0.888) |
| p-value | — | <0.001 *** | <0.001 *** |
| Ramus Height Right OPG | — | ||
| Spearman’s rho | — | 0.800 (95% CI: 0.725, 0.855) | |
| p-value | — | <0.001 *** | |
| Ramus Height Left OPG | — |
Note: * p < .05, ** p < .01, *** p < .001.
Table 5.
Correlation Matrix for Gonial Angles.
| Variable | Gonial Angle Lateral Ceph | Gonial Angle Right OPG | Gonial Angle Left OPG |
|---|---|---|---|
| Gonial Angle (Lateral Ceph) | — | ||
| Spearman's rho | — | 0.946 *** | 0.858 *** |
| Degrees of Freedom (DF) | — | 126 | 126 |
| p-value | — | <0.001 | <0.001 |
| Gonial Angle Right (OPG) | — | ||
| Spearman's rho | — | 0.811 *** | |
| Degrees of Freedom (df) | — | 126 | |
| p-value | — | <0.001 | |
| Gonial Angle Left (OPG) | — |
Note: * p < .05, ** p < .01, *** p < .001.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



