
Submitted:
21 January 2025
Posted:
22 January 2025
You are already at the latest version
Abstract
Background / Aims: Previous studies suggested a link between Helicobacter pylori (H. pylori) infection and steatotic liver disease, now termed metabolic dysfunction-associated steatotic liver disease (MASLD). This study aimed to identify the association of active H. pylori infection and new concept of MASLD in a longitudinal cohort. Methods: We reviewed 1,497 health examinees who had two endoscopic biopsies for H. pylori activity, without hepatic steatosis at the baseline abdominal ultrasonography. Subjects were classified into four groups based on H. pylori activity. Multivariable Cox models were assessed the link between H. pylori activity status and incident MASLD. Results: Over a median follow-up of 31.1 months, 247 subjects (16.5%) developed MASLD. The groups were: H. pylori naïve (n = 57, 15.6%), de-novo (n = 31, 15.3%), eradicated (n = 32, 16.1%), and persistent (n = 127, 17.4%). The H. pylori persistent group had a higher risk of MASLD compared to naïve group (hazard ratio: 1.41; 95% confidence interval: 1.01 - 1.96; P-value = 0.045). The association between H. pylori activity status and incident MASLD was significant only with ongoing infection. Conclusions: Persistent H. pylori infection increases the risk of MASLD, indicating that active infection may contribute to MASLD development. Eradicating active H. pylori infection might help lower the incidence of MASLD.
Keywords:
Helicobacter pylori
; Metabolic dysfunction-associated steatotic liver disease
; Non-alcoholic fatty liver disease
; Cohort study
1. Introduction
Helicobacter pylori (H. pylori) is a bacterium that colonizes the gastric environment. It is one of the most common chronic bacterial infections in humans, with about two thirds of the world’s general population currently infected [1,2]. It is well established that H. pylori infection is related to the development of intra-gastric diseases including chronic gastritis, peptic ulcer, mucosa-associated lymphoid tissue lymphoma, and gastric adenocarcinoma [3]. Beyond its established local pathologies, several pathophysiologic mechanisms linked to H. pylori infection have been suggested, including chronic inflammation, alteration of gut microbiome, malabsorption of nutrients, and so on that can result in extra-gastric systematic manifestations [4]. Since the 1980s, studies have found that this infection is associated with extra-gastric manifestations such as metabolic syndrome, diabetes, coronary heart diseases, liver tumor, and steatotic liver disease, previously known as non-alcoholic fatty liver disease (NAFLD) [5,6,7,8].
Steatotic liver disease is characterized by hepatic steatosis. It is a leading cause of chronic liver disease with a high global prevalence [9]. In 2023, more than 200 experts in liver disease formalized to rename NAFLD to a metabolic dysfunction-associated steatotic liver disease (MASLD) [10]. MASLD is diagnosed when cardiometabolic risk factors coexisted and have been suggested to identify more significant fibrosis than NAFLD, though most of the NAFLD meet MASLD criteria [11,12,13].
Development of MASLD involves a multiple-hit mechanism of abnormal lipid metabolism, insulin resistance with environmental exposure, and genetic susceptibility [14]. Studies have suggested that dysbacteriosis of the intestinal flora including H. pylori can induce abnormal lipid metabolism in the liver, eventually leading to the development of steatotic liver disease [15,16]. Recently, studies including meta-analysis have revealed that H. pylori infection is associated with MASLD development and that H. pylori eradication could reduce the risk MASLD [17,18,19,20]. Controversially, there are continuous debates on this subject, with some studies suggesting that H. pylori is not associated with MASLD [21,22,23,24]. Previous studies had limitations in that study types were mostly cross-sectional, with diagnosis of H. pylori done by non-invasive tests which could not represent an active infection status. Therefore, this study aimed to identify the association of active H. pylori infection diagnosed by serial invasive tests and the risk of MASLD in a cohort of asymptomatic subjects with a longitudinal follow-up.
2. Materials and Methods
2.1. Database
This was a retrospective cohort study performed at Samsung Changwon Medical Center, South Korea. The flowchart for study selection is shown in Figure 1. We screened healthy adults aged 19 years or older in a health screening cohort who participated in a comprehensive health-screening exam at the center of Samsung Changwon Medical Center between January 2012 and December 2018. Since we aimed to find out the longitudinal effect of active H. pylori infection status on the development of MASLD, we included participants who underwent invasive diagnostic test of H. pylori twice on endoscopy with at least two abdominal ultrasounds taken (the second endoscopy was performed at least 1 year apart from the baseline). We excluded subjects who had hepatic steatosis on baseline ultrasound (n = 1,115) and possible specific etiology for steatotic liver disease such as history of chronic liver disease (positive serologic test for hepatitis B or C virus or cirrhosis) (n = 8), elevated alanine aminotransferase 80 U/I (n = 86), and alcohol intake 30 g/day for men and 20 g/day for women (n = 605). Finally, a total of 1,497 participants were included in the analysis. This study was conducted in accordance with the Declaration of Helsinki. The study protocol was approved by the Institutional Review Board (IRB) of Samsung Changwon Medical Center on August 20, 2023 (IRB approval No. SCMC 2023-08-005). The requirement to obtain informed patient consent was waived by the IRB because this study was retrospective by analyzing existing administrative and clinical data.
2.2. Data Collection and Variables
Clinical variables collected were demographic characteristics (including age, sex and body mass index (BMI)), detailed physical examination including systolic blood pressure (SBP), and a self-administered health questionnaire on smoking, alcohol consumption, physical activity, medication use, and medical history (including hypertension, diabetes mellitus, and dyslipidemia). Serum biochemical markers including fasting glucose, high-sensitivity C-reactive protein (hsCRP), lipid profile (such as total cholesterol (TC), triglycerides, low-density lipoprotein cholesterol (LDL), and high-density lipoprotein cholesterol (HDL)), and liver enzyme profile (such as aspartate aminotransferase (AST), alanine aminotransferase (ALT), and gamma-glutamyl transferase (GGT)) were measured after more than 12 hours of fasting and reviewed from electronic medical records.
BMI was calculated as weight in kilograms/height in square meters (kg/m2) and categorized as underweight (BMI < 18.5), normal (18.5 BMI < 24.9), overweight (25.0 BMI < 29.9) and obese (BMI 30.0). Smoking status was categorized as currently non-smoker, moderate smoker ( 1 pack/day), and heavy smoker ( 1 pack/day). Alcohol consumption was divided into mild ( 10 g/day) and modest ( 10 g/day). Regular exercise was determined when moderate to hard intense physical activity was performed three or more times per week. Dyslipidemia was defined when one or more of lipid profiles met the definition of criteria (HDL40 mg/dl or TG200 mg/dl or LDL160 mg/dl) or currently on dyslipidemia medication in a questionnaire [25].
2.3. H. Pylori Diagnosis and Definition of Active H. pylori Infection Status
During upper endoscopy exam, biopsies were done for the H. pylori special stain (Warthin-Starry stain) or rapid urease test (Pyloplus, ARJ Medical Inc, USA) on at least two sites of the stomach of greater curvature sides of the antrum and body. Tests were performed for participants who voluntarily wanted H. pylori test or were suspected to have active H. pylori gastritis such as diffuse redness, enlarged folds, mucosal edema, and nodularity [26].
As we wanted to know the impact of ongoing activity of H. pylori infection on incident of MASLD, participants were divided into 4 groups based on the result of serial invasive diagnostic tests: 1) H. pylori naïve group, when active H. pylori infection was not identified on the two continuous tests; 2) H. pylori de-novo group, when initial H. pylori negative infection state on the first exam turned up to be positive on the follow up study; 3) H. pylori eradicated group, when a positive infection state turned up to be negative; and 4) H. pylori persistent group, when sustained active H. pylori infection was detected during serial exams. A schematic diagram of the study design is shown in Figure 2.
2.4. Definition of MASLD Development
The primary outcome was MASLD development during follow-up. Hepatic steatosis was defined by abdominal ultrasonography based on standard criteria such as diffuse increased echogenicity of liver parenchyma, deep attenuation, hepatorenal echo contrast and vessel blurring [27]. MASLD was diagnosed when at least one or more of the following five cardiometabolic risk factors were detected at the time of incident hepatic steatosis: (1) BMI 23 kg/m2 or waist circumference > 90 cm for males or 80 cm for females; (2) fasting serum glucose 100 mg/dL or 2-hour post-load glucose levels140mg/dl or HbA1c5.7 % or diagnosis of type 2 diabetes or treatment for type 2 diabetes; (3) blood pressure 130/85 mmHg or specific antihypertensive drug treatment; (4) plasma triglycerides 150mg/dl or lipid-lowering treatment; (5) plasma HDL 40 mg/dl for males or 50 mg/dl for females or lipid-lowering treatment.[11]
We excluded subjects with possible specific etiology for steatotic liver disease such as excessive alcohol consumption, chronic liver disease including viral hepatitis and elevated ALT over 2 folds of upper normal limit at baseline. Therefore, cases of newly found hepatic steatosis with cardiometabolic risk factor were considered incident MASLD.
2.5. Statistical Analysis
Continuous variables were compared using a Student’s t-test, and categorical variables were compared using one-way ANOVA, Kruskal Wallis test, or Pearson's chi-square test. Descriptive statistics were used to summarise participants’ baseline characteristics between groups and post hoc analysis was performed using Bonferroni's adjustment.
The primary endpoint was incident MASLD. Cox proportional hazard models were used. Multivariable models were analyzed after adjusting for age, sex (Model 1), and metabolic risk factors such as BMI, exercise, smoking, drinking, blood pressure, fasting glucose and presence of dyslipidemia (Model 2). Liver enzyme profiles of AST, ALT, GGT were further adjusted (Model 3). Statistical significance was considered when P- value was less than 0.05. All statistical analyses were performed using SAS software version 9.4 (SAS Institute, Cary, NC, USA) and IBM SPSS version 25.0 (SPSS Inc., IBM Corporation, Chicago, IL, USA).
3. Results
3.1. Basic Characteristics of the Study Cohort
Table 1 shows demographic and clinical characteristics of the 1,497 included participants. The mean age of the study population was 46.7 years. There were 956 (63.9%) males. According to the activity status of H. pylori infection, H. pylori naïve, H. pylori de-novo, H. pylori eradicated, and H. pylori persistent groups had 365, 203, 199, and 730 subjects, respectively. The median interval between two serial endoscopy exams was 23.1 months. There were statistically significant differences in age, regular exercise, systolic blood pressure and AST between groups. During follow-up, MASLD developed in 247 (16.5%) cases in the total study population (n = 1,497). The median follow-up period was 31.1 months (rage, 12 to 83.3 months). The percentage of incident MASLD was 15.6% in the H. pylori naïve group, 15.3% in the H. pylori de-novo, 16.1% in the H. pylori eradicated group and 17.4% in the H. pylori persistent group.
3.2. Factors Associated with MASLD Development
Compared to the H. pylori naïve group, the H. pylori persistent group showed a higher risk of MASLD development in univariable and multivariable Cox proportional hazard models (univariable hazard ratio [HR]: 1.48; 95% confidence interval [CI]: 1.08 - 2.02; P = 0.015; multivariable HR: 1.41; 95% CI: 1.01 - 1.96; P = 0.045). Other than H. pylori activity status, age, male sex, higher BMI, fasting glucose, ALT, GGT, and presence of dyslipidemia were also significant factors associated with MASLD development in multivariable analysis (Table 2). We used serial multivariable adjustment models to figure out the interaction between H. pylori activity status and such factors on the development of MASLD. The H. pylori persistent group showed a higher risk for MASLD development than the H. pylori naïve group in multivariable Model 1 and final multivariable Model 3, but not statistically significant in Model 2 (HR: 1.39; 95% CI: 1.00 - 1.92; p = 0.051) (Table 3). Figure 3 shows cumulative incidence of MASLD based on active H. pylori infection status.
3.3. Active H. pylori Infection Status and the Development of MASLD
We further analyzed the association between various H. pylori infection status and the MASLD development. Results are shown in Table 3. When the H. pylori persistent group was compared with rest of others, the association between persistent H. pylori infection and MASLD development was statistically significant in all multivariable analyses (Model 1, 2 and Model 3 (HR: 1.33; 95% CI: 1.02 - 1.73; P = 0.033)). Results of cumulative incidence of MASLD in the H. pylori persistent group and others are shown in Figure 4. When participants were divided by the last active H. pylori infection status (i.e., the presence of active H. pylori infection at the baseline regardless of previous infection), the association between the last active H. pylori infection and incident MASLD was attenuated after serial adjustments.
4. Discussion
In this cohort study, we found that participants with persistently active H. pylori infection were at a higher risk of MASLD than those with infection-naïve or other infection statuses. Other risk factors for incident MASLD included age, male gender, higher BMI, fasting glucose, ALT, and GGT.
We focused on the diagnosis of active H. pylori infection by serial invasive histologic biopsies and assumed that a more continuous exposure to an active H. pylori infection was associated with a higher risk of MASLD development. Serial biopsy results of infection status meant that active infection had persisted at least during the interval between two biopsies. We divided participants into four groups based on results of biopsies. The H. pylori persistent group was assumed to have the highest exposure to an active infection compared to the H. pylori de-novo or eradicated group with a modest exposure and the H. pylori naïve group with the lowest exposure. Our findings indicated that a continuous exposure to active H. pylori infection might contribute to MASLD pathogenesis. To the best of our knowledge, this was the first longitudinal study that evaluated the association between H. pylori infection and the risk of MASLD based on H. pylori activities diagnosed by serial invasive biopsies.
Many studies including high-quality meta-analyses have demonstrated an association between MASLD and H. pylori infection. Although heterogeneity existed according to sample size, study method, and the method of diagnosing H. pylori infection, meta-analyses studies have shown high odds ratios of MASLD ranging from 1.19 to 1.27 in H. pylori positive patients compared to H. pylori negative patients [19,28,29,30]. However, some unmet needs existed in previous studies because most studies had a cross-sectional, or case control design and non-invasive tests were mostly used to evaluate H. pylori infection. A prospective cohort study with a large study population of 17,028 South Korean adults followed for over 81,130 person-years has found a higher incidence of MASLD in H. pylori-seropositive patients.[17] As authors mentioned in study limitations, seropositivity for H. pylori diagnosis was evaluated in their study, which had a limited effectiveness because diagnostic accuracy might be low. In addition, their study included all patients with past, eradicated, and present H. pylori infection. Therefore, it could not accurately distinguish active infection. One retrospective study of 64 obese patients undergoing bariatric surgery has demonstrated that active H. pylori infection is independently associated with biopsy-proven non-alcoholic steatohepatitis and fibrosis [31]. A few non-longitudinal studies have used invasive histologic tests to confirm the diagnosis of H. pylori infection [32,33].
Many theories have been suggested about the relationship between H. pylori and MASLD, although more detailed studies are needed. Possible contributions of H. pylori infection to MASLD development include chronic inflammation, altered gut microbiota, increased intestinal permeability, increased insulin resistance, dyslipidemia, and metabolic syndrome, and so on [34,35,36]. Pro-inflammatory cytokines increased by H. pylori infection can generate low grade systemic inflammation. When the gastrointestinal epithelium is disrupted by H. pylori, infection related metabolites are absorbed through portal flow to the liver [37]. Finally, toll-like receptors can activate the inflammatory process and lead to hepatic steatosis [38]. H. pylori infection has also been suggested to be associated with metabolic syndrome by several possible potential mechanisms in meta-analysis and systematic reviews [8,39,40]. Metabolic syndrome and MASLD are also strongly associated in both directions [41]. In this study, statistically significant association between H. pylori infection and MASLD was attenuated when metabolic variables were adjusted in Model 2 analysis. This might be due to a confounding effect of H. pylori, metabolic dysregulation, and MASLD development. From these findings, potential pathogenetic mechanisms between H. pylori infection and metabolic dysregulation may be hypothesized, eventually resulting in the development of MASLD.
Although this study is strengthened by a cohort study design and diagnostic methods of active H. pylori based on serial invasive endoscopic biopsies, we should acknowledge that our present study has several limitations. First, the retrospective design of this study inherits potential selection, measurement, and recall biases. We included participants who had no specific symptoms based on a questionnaire. However, possible symptomatic participants such as those with gastroesophageal reflux and so on are more likely to undergo endoscopic exams. Given that obesity is strongly associated with gastroesophageal reflux and MASLD, participants who underwent endoscopy were more likely to have higher BMI than those without undergoing an upper endoscopy. By this selection, the association between H. pylori and MASLD might have been inflated. Second, hepatic steatosis was defined by abdominal ultrasonography known to have a wide range of sensitivity and specificity [42]. Finally, the study population consisted of mostly healthy Asian individuals in a single center.
5. Conclusions
We report that a persistently active H. pylori infection is associated with a higher risk of MASLD development. An active H. pylori infection might contribute to the development of MASLD through multiple pathogenic mechanisms. H. pylori eradication therapy for asymptomatic healthy individuals with an active infection might have a benefit by reducing the risk of MASLD. Validation studies including other populations in multiple centers are needed to make our findings more generalizable. Furthermore, randomized controlled trials are needed to evaluate if bacterial elimination can have a consistent therapeutic effect on MASLD regression and eventually reduce related comorbidities.
Author Contributions
Study concept and design: JYK and OJL; Acquisition, analysis, or interpretation of data: JYK and NGK; Writing and drafting of the manuscript: JYK; Critical revision of the manuscript for important intellectual content: BSK, JHC, HIK and OJL; Statistical analysis: NGK and MJ. All authors have read and approved the final manuscript.
Funding
This research received no external funding.
Informed Consent Statement
Informed consent was waived by the board.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Acknowledgments
We would like to show our greatest appreciation to all professors of the Sungkyunkwan University School of Medicine and Gyeongsang National University College of Medicine who provided helpful comments and suggestions.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Coelho, L.G.V.; Marinho, J.R.; Genta, R.; Ribeiro, L.T.; Passos, M.; Zaterka, S.; Assumpcao, P.P.; Barbosa, A.J.A.; Barbuti, R.; Braga, L.L.; et al. Ivth Brazilian Consensus Conference on Helicobacter Pylori Infection. Arq Gastroenterol 2018, 55, 97–121. [Google Scholar] [CrossRef]
- Everhart, J.E. Recent developments in the epidemiology of Helicobacter pylori. Gastroenterol Clin North Am 2000, 29, 559–578. [Google Scholar] [CrossRef] [PubMed]
- Leja, M.; Grinberga-Derica, I.; Bilgilier, C.; Steininger, C. Review: Epidemiology of Helicobacter pylori infection. Helicobacter 2019, 24 Suppl 1, e12635. [Google Scholar] [CrossRef]
- Santos, M.L.C.; de Brito, B.B.; da Silva, F.A.F.; Sampaio, M.M.; Marques, H.S.; Oliveira, E.S.N.; de Magalhaes Queiroz, D.M.; de Melo, F.F. Helicobacter pylori infection: Beyond gastric manifestations. World J Gastroenterol 2020, 26, 4076–4093. [Google Scholar] [CrossRef] [PubMed]
- Mladenova, I.; Durazzo, M. Transmission of Helicobacter pylori. Minerva Gastroenterol Dietol 2018, 64, 251–254. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; Wang, F.; Shi, S. Helicobacter pylori Infection Increase the Risk of Myocardial Infarction: A Meta-Analysis of 26 Studies Involving more than 20,000 Participants. Helicobacter 2015, 20, 176–183. [Google Scholar] [CrossRef]
- Wang, F.; Liu, J.; Lv, Z. Association of Helicobacter pylori infection with diabetes mellitus and diabetic nephropathy: a meta-analysis of 39 studies involving more than 20,000 participants. Scand J Infect Dis 2013, 45, 930–938. [Google Scholar] [CrossRef] [PubMed]
- Gunji, T.; Matsuhashi, N.; Sato, H.; Fujibayashi, K.; Okumura, M.; Sasabe, N.; Urabe, A. Helicobacter pylori infection is significantly associated with metabolic syndrome in the Japanese population. Am J Gastroenterol 2008, 103, 3005–3010. [Google Scholar] [CrossRef]
- Younossi, Z.M.; Koenig, A.B.; Abdelatif, D.; Fazel, Y.; Henry, L.; Wymer, M. Global epidemiology of nonalcoholic fatty liver disease-Meta-analytic assessment of prevalence, incidence, and outcomes. Hepatology 2016, 64, 73–84. [Google Scholar] [CrossRef]
- Rinella, M.E.; Lazarus, J.V.; Ratziu, V.; Francque, S.M.; Sanyal, A.J.; Kanwal, F.; Romero, D.; Abdelmalek, M.F.; Anstee, Q.M.; Arab, J.P.; et al. A multisociety Delphi consensus statement on new fatty liver disease nomenclature. Hepatology 2023, 78, 1966–1986. [Google Scholar] [CrossRef]
- Rinella, M.E.; Lazarus, J.V.; Ratziu, V.; Francque, S.M.; Sanyal, A.J.; Kanwal, F.; Romero, D.; Abdelmalek, M.F.; Anstee, Q.M.; Arab, J.P.; et al. A multisociety Delphi consensus statement on new fatty liver disease nomenclature. Ann Hepatol 2024, 29, 101133. [Google Scholar] [CrossRef] [PubMed]
- Rinella, M.E.; Sookoian, S. From NAFLD to MASLD: updated naming and diagnosis criteria for fatty liver disease. J Lipid Res 2024, 65, 100485. [Google Scholar] [CrossRef]
- Hagström, H.; Vessby, J.; Ekstedt, M.; Shang, Y. 99% of patients with NAFLD meet MASLD criteria and natural history is therefore identical. J Hepatol 2024, 80, e76–e77. [Google Scholar] [CrossRef] [PubMed]
- Buzzetti, E.; Pinzani, M.; Tsochatzis, E.A. The multiple-hit pathogenesis of non-alcoholic fatty liver disease (NAFLD). Metabolism 2016, 65, 1038–1048. [Google Scholar] [CrossRef] [PubMed]
- Schoeler, M.; Caesar, R. Dietary lipids, gut microbiota and lipid metabolism. Rev Endocr Metab Disord 2019, 20, 461–472. [Google Scholar] [CrossRef]
- Leung, C.; Rivera, L.; Furness, J.B.; Angus, P.W. The role of the gut microbiota in NAFLD. Nat Rev Gastroenterol Hepatol 2016, 13, 412–425. [Google Scholar] [CrossRef] [PubMed]
- Kim, T.J.; Sinn, D.H.; Min, Y.W.; Son, H.J.; Kim, J.J.; Chang, Y.; Baek, S.Y.; Ahn, S.H.; Lee, H.; Ryu, S. A cohort study on Helicobacter pylori infection associated with nonalcoholic fatty liver disease. J Gastroenterol 2017, 52, 1201–1210. [Google Scholar] [CrossRef] [PubMed]
- Yu, Y.Y.; Tong, Y.L.; Wu, L.Y.; Yu, X.Y. Helicobacter pylori infection eradication for nonalcoholic fatty liver disease: a randomized controlled trial. Sci Rep 2022, 12, 19530. [Google Scholar] [CrossRef]
- Liu, R.; Liu, Q.; He, Y.; Shi, W.; Xu, Q.; Yuan, Q.; Lin, Q.; Li, B.; Ye, L.; Min, Y.; et al. Association between Helicobacter pylori infection and nonalcoholic fatty liver: A meta-analysis. Medicine (Baltimore) 2019, 98, e17781. [Google Scholar] [CrossRef]
- Mantovani, A.; Lando, M.G.; Borella, N.; Scoccia, E.; Pecoraro, B.; Gobbi, F.; Bisoffi, Z.; Valenti, L.; Tilg, H.; Byrne, C.D.; et al. Relationship between Helicobacter pylori infection and risk of metabolic dysfunction-associated steatotic liver disease: An updated meta-analysis. Liver Int 2024, 44, 1513–1525. [Google Scholar] [CrossRef] [PubMed]
- Okushin, K.; Takahashi, Y.; Yamamichi, N.; Shimamoto, T.; Enooku, K.; Fujinaga, H.; Tsutsumi, T.; Shintani, Y.; Sakaguchi, Y.; Ono, S.; et al. Helicobacter pylori infection is not associated with fatty liver disease including non-alcoholic fatty liver disease: a large-scale cross-sectional study in Japan. BMC Gastroenterol 2015, 15, 25. [Google Scholar] [CrossRef]
- Baeg, M.K.; Yoon, S.K.; Ko, S.H.; Noh, Y.S.; Lee, I.S.; Choi, M.G. Helicobacter pylori infection is not associated with nonalcoholic fatty liver disease. World J Gastroenterol 2016, 22, 2592–2600. [Google Scholar] [CrossRef] [PubMed]
- Fan, N.; Peng, L.; Xia, Z.; Zhang, L.; Wang, Y.; Peng, Y. Helicobacter pylori Infection Is Not Associated with Non-alcoholic Fatty Liver Disease: A Cross-Sectional Study in China. Front Microbiol 2018, 9, 73. [Google Scholar] [CrossRef]
- Wernly, S.; Wernly, B.; Semmler, G.; Völkerer, A.; Rezar, R.; Semmler, L.; Stickel, F.; Aigner, E.; Niederseer, D.; Datz, C. Non-alcoholic fatty liver disease is not independently associated with Helicobacter pylori in a central European screening cohort. Minerva Med 2022, 113, 936–949. [Google Scholar] [CrossRef] [PubMed]
- Jin, E.S.; Shim, J.S.; Kim, S.E.; Bae, J.H.; Kang, S.; Won, J.C.; Shin, M.J.; Jin, H.Y.; Moon, J.; Lee, H.; et al. Dyslipidemia Fact Sheet in South Korea, 2022. Diabetes Metab J 2023, 47, 632–642. [Google Scholar] [CrossRef] [PubMed]
- Seo, J.-y.; Ahn, J.Y. Endoscopic Features According to Helicobacter pylori Infection Status. The Korean Journal of Medicine 2023, 98, 117–124. [Google Scholar] [CrossRef]
- Ferraioli, G.; Soares Monteiro, L.B. Ultrasound-based techniques for the diagnosis of liver steatosis. World J Gastroenterol 2019, 25, 6053–6062. [Google Scholar] [CrossRef]
- Heydari, K.; Yousefi, M.; Alizadeh-Navaei, R.; Lotfi, P.; Sheydaee, F.; Raei, M.; Vahdatinia, A.; Hessami, A.; Rafati, S.; Moosazadeh, M.; et al. Helicobacter pylori Infection and Non-alcoholic Fatty Liver Disease: A Systematic Review and Meta-Analysis. Turk J Gastroenterol 2022, 33, 171–181. [Google Scholar] [CrossRef] [PubMed]
- Zhou, B.G.; Yang, H.J.; Xu, W.; Wang, K.; Guo, P.; Ai, Y.W. Association between Helicobacter pylori infection and nonalcoholic fatty liver disease: A systematic review and meta-analysis of observational studies. Helicobacter 2019, 24, e12576. [Google Scholar] [CrossRef] [PubMed]
- Mantovani, A.; Turino, T.; Altomari, A.; Lonardo, A.; Zoppini, G.; Valenti, L.; Tilg, H.; Byrne, C.D.; Targher, G. Association between Helicobacter pylori infection and risk of nonalcoholic fatty liver disease: An updated meta-analysis. Metabolism 2019, 96, 56–65. [Google Scholar] [CrossRef] [PubMed]
- Doulberis, M.; Srivastava, S.; Polyzos, S.A.; Kountouras, J.; Papaefthymiou, A.; Klukowska-Rotzler, J.; Blank, A.; Exadaktylos, A.K.; Srivastava, D.S. Active Helicobacter pylori Infection is Independently Associated with Nonalcoholic Steatohepatitis in Morbidly Obese Patients. J Clin Med 2020, 9. [Google Scholar] [CrossRef]
- Yu, L.Y.; Hu, K.C.; Liu, C.J.; Hung, C.L.; Bair, M.J.; Chen, M.J.; Wang, H.Y.; Wu, M.S.; Shih, S.C.; Liu, C.C. Helicobacter pylori infection combined with non-alcoholic fatty liver disease increase the risk of atherosclerosis: Focus in carotid artery plaque. Medicine (Baltimore) 2019, 98, e14672. [Google Scholar] [CrossRef]
- Lecube, A.; Valladares, S.; López-Cano, C.; Gutiérrez, L.; Ciudin, A.; Fort, J.M.; Reñé, J.M.; Matias-Guiu, X.; de Torres, I.; Bueno, M.; et al. The Role of Morbid Obesity in the Promotion of Metabolic Disruptions and Non-Alcoholic Steatohepatitis by Helicobacter Pylori. PLoS One 2016, 11, e0166741. [Google Scholar] [CrossRef] [PubMed]
- Miele, L.; Valenza, V.; La Torre, G.; Montalto, M.; Cammarota, G.; Ricci, R.; Mascianà, R.; Forgione, A.; Gabrieli, M.L.; Perotti, G.; et al. Increased intestinal permeability and tight junction alterations in nonalcoholic fatty liver disease. Hepatology 2009, 49, 1877–1887. [Google Scholar] [CrossRef]
- Sabaté, J.M.; Jouët, P.; Harnois, F.; Mechler, C.; Msika, S.; Grossin, M.; Coffin, B. High prevalence of small intestinal bacterial overgrowth in patients with morbid obesity: a contributor to severe hepatic steatosis. Obes Surg 2008, 18, 371–377. [Google Scholar] [CrossRef] [PubMed]
- Polyzos, S.A.; Kountouras, J.; Zavos, C.; Deretzi, G. The association between Helicobacter pylori infection and insulin resistance: a systematic review. Helicobacter 2011, 16, 79–88. [Google Scholar] [CrossRef] [PubMed]
- Waluga, M.; Kukla, M.; Żorniak, M.; Bacik, A.; Kotulski, R. From the stomach to other organs: Helicobacter pylori and the liver. World J Hepatol 2015, 7, 2136–2146. [Google Scholar] [CrossRef] [PubMed]
- Polyzos, S.A.; Kountouras, J. Novel Advances in the Association Between Helicobacter pylori Infection, Metabolic Syndrome, and Related Morbidity. Helicobacter 2015, 20, 405–409. [Google Scholar] [CrossRef] [PubMed]
- Shin, D.W.; Kwon, H.T.; Kang, J.M.; Park, J.H.; Choi, H.C.; Park, M.S.; Park, S.M.; Son, K.Y.; Cho, B. Association between metabolic syndrome and Helicobacter pylori infection diagnosed by histologic status and serological status. J Clin Gastroenterol 2012, 46, 840–845. [Google Scholar] [CrossRef] [PubMed]
- Upala, S.; Jaruvongvanich, V.; Riangwiwat, T.; Jaruvongvanich, S.; Sanguankeo, A. Association between Helicobacter pylori infection and metabolic syndrome: a systematic review and meta-analysis. J Dig Dis 2016, 17, 433–440. [Google Scholar] [CrossRef]
- Powell, E.E.; Wong, V.W.; Rinella, M. Non-alcoholic fatty liver disease. Lancet 2021, 397, 2212–2224. [Google Scholar] [CrossRef] [PubMed]
- Hernaez, R.; Lazo, M.; Bonekamp, S.; Kamel, I.; Brancati, F.L.; Guallar, E.; Clark, J.M. Diagnostic accuracy and reliability of ultrasonography for the detection of fatty liver: a meta-analysis. Hepatology 2011, 54, 1082–1090. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Flowchart of participant enrollment. H. pylori, Helicobacter pylori; USG, ultrasonography.
Figure 1.
Flowchart of participant enrollment. H. pylori, Helicobacter pylori; USG, ultrasonography.
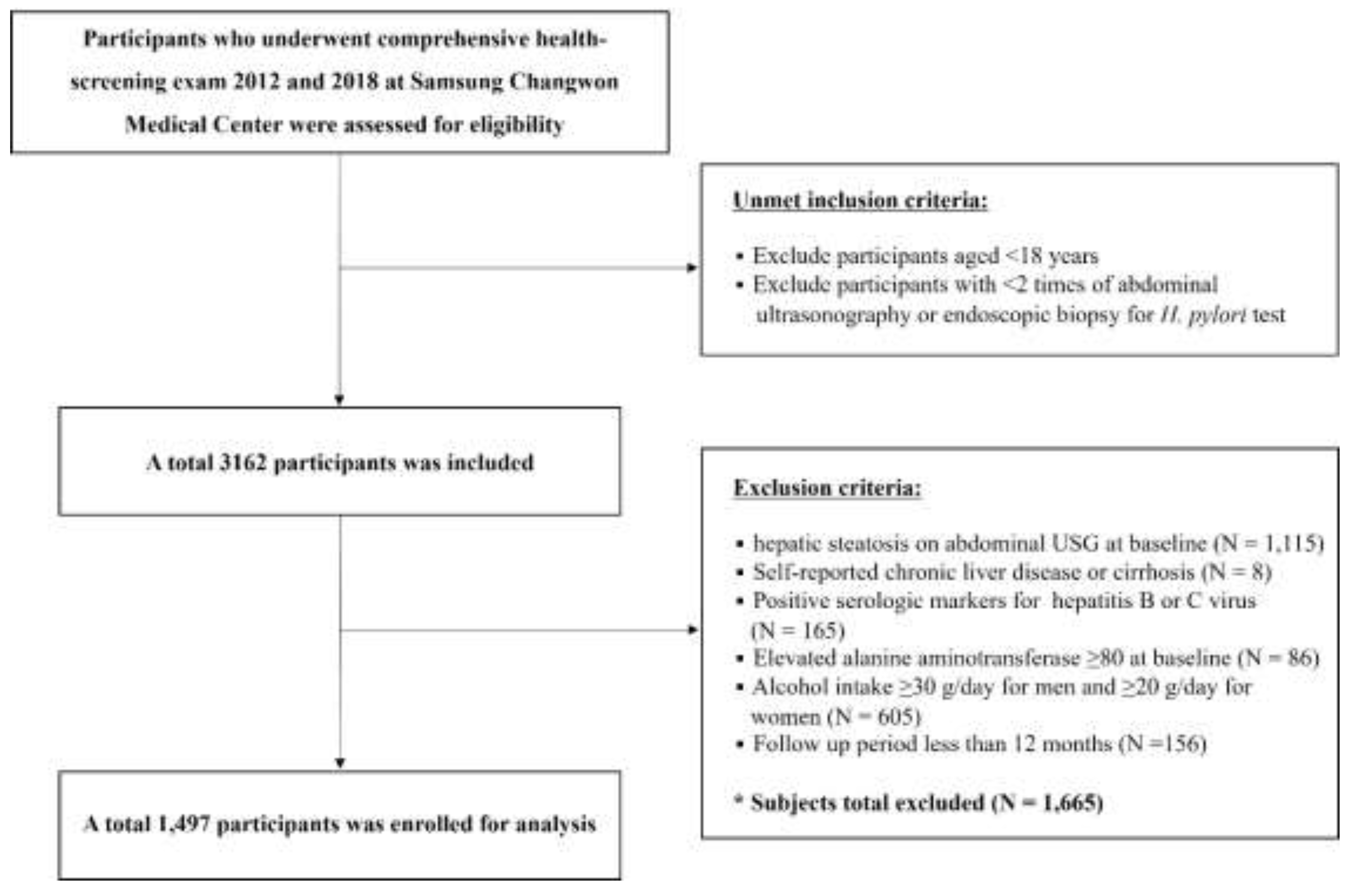
Figure 2.
Schematic diagram of the study design. H. pylori, Helicobacter pylori; USG, ultrasonography; CMRF, cardiometabolic risk factor.
Figure 2.
Schematic diagram of the study design. H. pylori, Helicobacter pylori; USG, ultrasonography; CMRF, cardiometabolic risk factor.
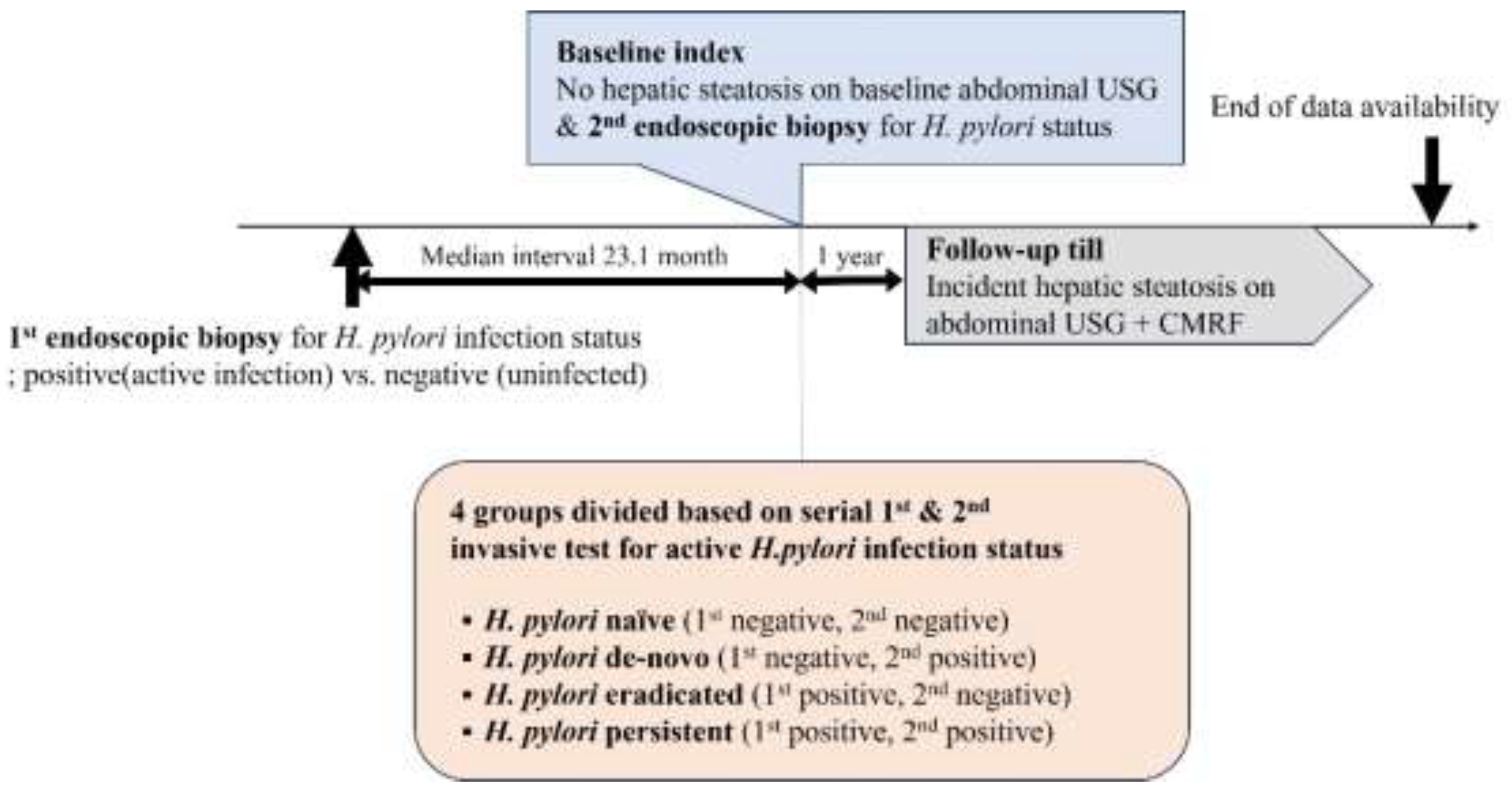
Figure 3.
(A) Cumulative incidence for MASLD by active H. pylori infection status divided by 4 groups. (B) Cumulative incidence for MASLD by H. pylori naïve and persistent infection (p-value = 0.016, log rank test). MASLD, metabolic dysfunction-associated steatotic liver disease; H. pylori, Helicobacter pylori.
Figure 3.
(A) Cumulative incidence for MASLD by active H. pylori infection status divided by 4 groups. (B) Cumulative incidence for MASLD by H. pylori naïve and persistent infection (p-value = 0.016, log rank test). MASLD, metabolic dysfunction-associated steatotic liver disease; H. pylori, Helicobacter pylori.
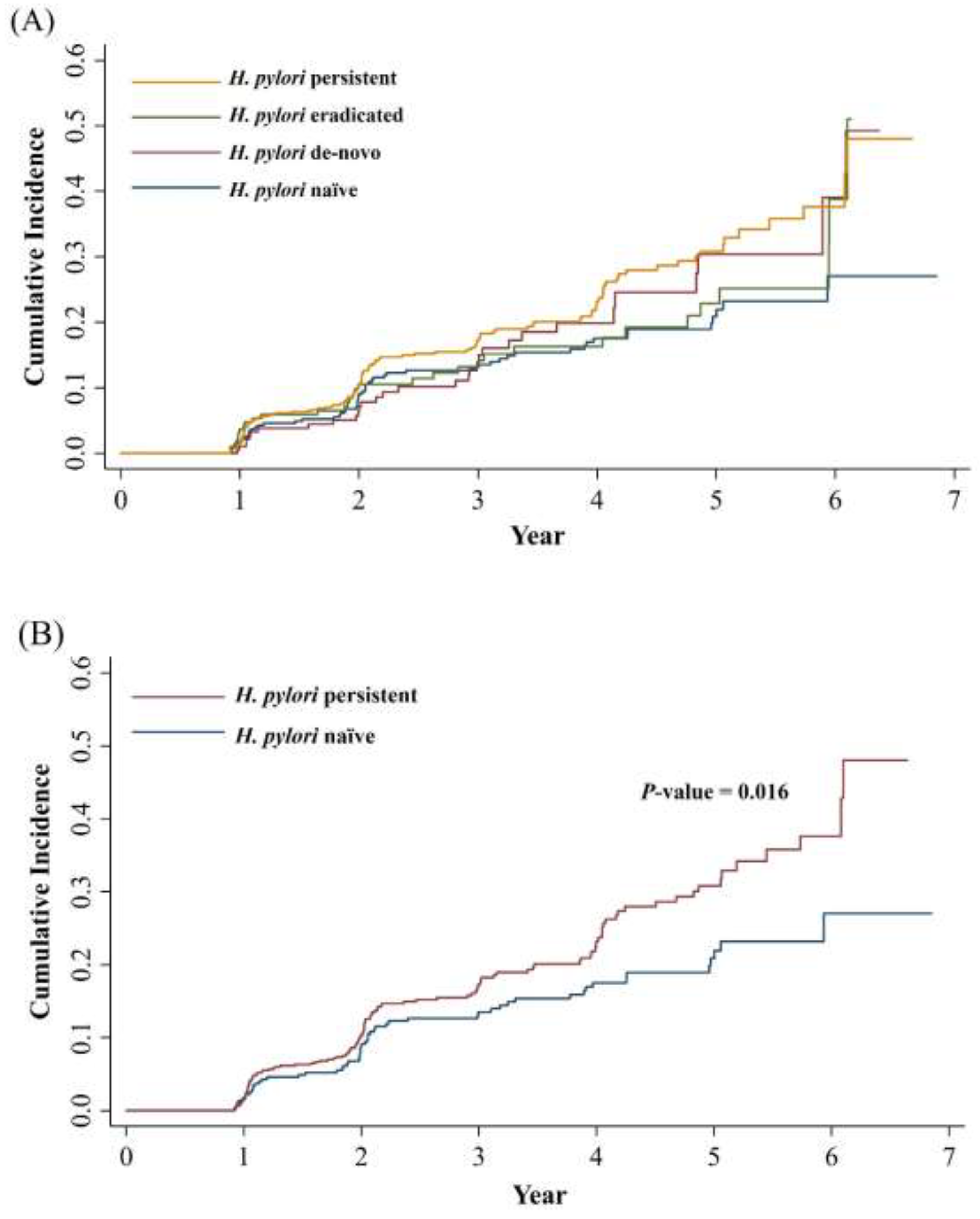
Figure 4.
Cumulative incidence for MASLD by H. pylori persistent infection and others. MASLD, metabolic dysfunction-associated steatotic liver disease; H. pylori, Helicobacter pylori.
Figure 4.
Cumulative incidence for MASLD by H. pylori persistent infection and others. MASLD, metabolic dysfunction-associated steatotic liver disease; H. pylori, Helicobacter pylori.
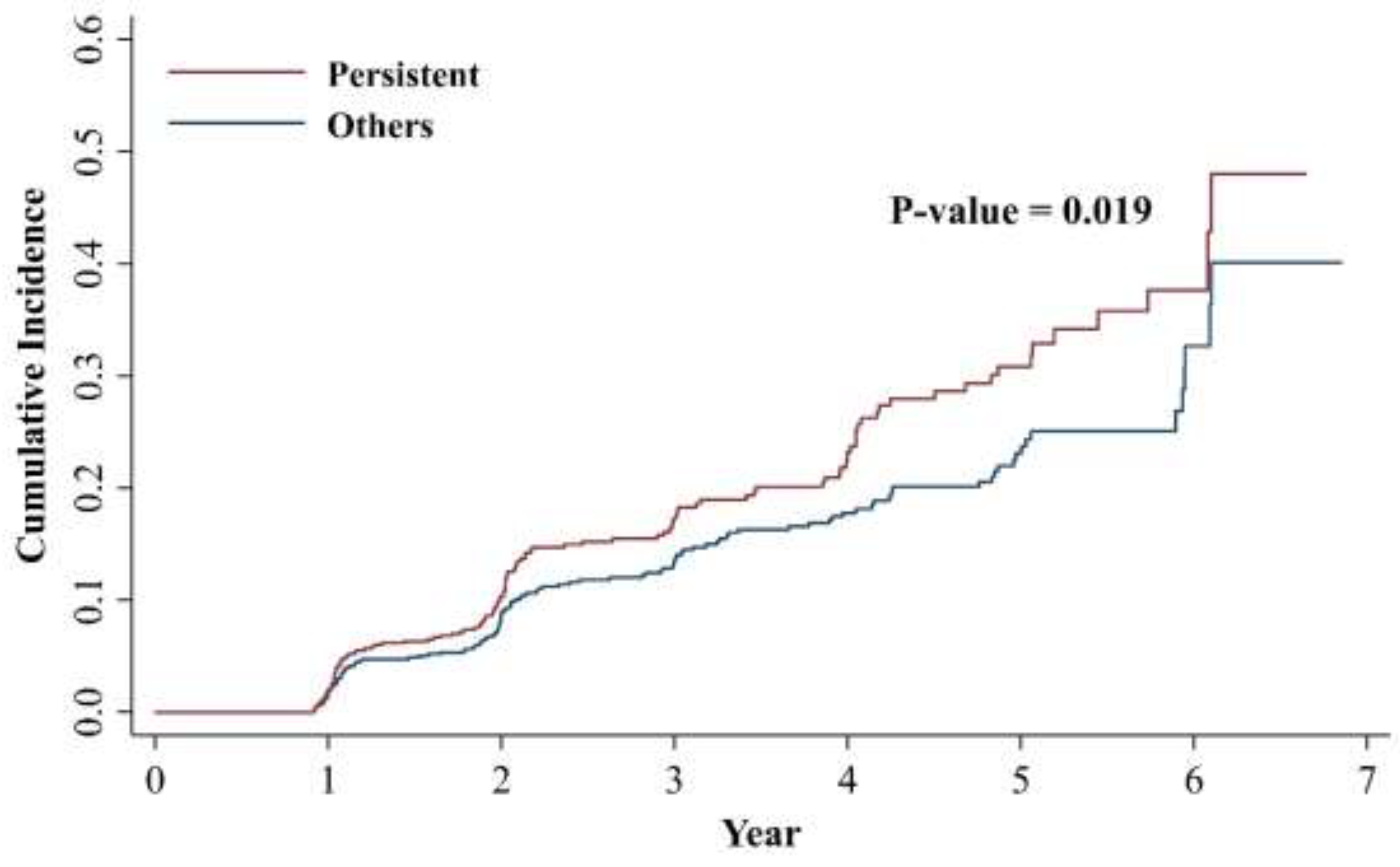

Table 1.
Baseline characteristics of the study population.
| Total (n = 1,497) |
H. pylori naïve (n = 365) |
H. pylori de-novo (n = 203) |
H. pylori eradicated (n = 199) |
H. pylori persistent (n = 730) |
p-value | |
|---|---|---|---|---|---|---|
| Age (years) | 46.71 ± 7.17 | 48.85 ± 7.67 | 47.83 ± 7.14 | 46.72 ± 7.29 | 45.32 ± 6.56 | <0.001 |
| Male (%) | 956 (63.9) | 218 (59.7) | 133 (65.5) | 133 (66.8) | 472 (64.7) | 0.272 |
| Body mass index (kg/m2) | 23.14 ± 2.55 | 23.02 ± 2.42 | 23.18 ± 2.58 | 23.14 ± 2.40 | 23.20 ± 2.65 | 0.740 |
| <18.5 | 44 (2.94) | 10 (2.74) | 5 (2.46) | 5 (2.51) | 24 (3.29) | |
| 18.5-24.9 | 1110 (74.15) | 278 (76.16) | 145 (71.43) | 150 (75.38) | 537 (73.56) | |
| 25-29.9 | 305 (20.37) | 66 (18.08) | 46 (22.66) | 43 (21.61) | 150 (20.55) | |
| ≥30 | 17 (1.14) | 6 (1.64) | 1 (0.49) | 0 (0.00) | 10 (1.37) | |
| Smoking | 0.296 | |||||
| Never smoker | 533 (35.60) | 125 (34.25) | 68 (33.50) | 77 (38.69) | 263 (36.03) | |
| Current(<1pack/day) | 428 (28.59) | 97 (26.58) | 59 (29.06) | 56 (28.14) | 216 (29.59) | |
| Current(≥1pack/day) | 268 (17.90) | 59 (16.16) | 38 (18.72) | 37 (18.59) | 134 (18.36) | |
| Alcohol | 0.085 | |||||
| Mild (10g/day) | 442 (29.53) | 116 (31.78) | 53 (26.11) | 55 (27.64) | 218 (29.86) | |
| Modest (10g/day) | 690 (46.09) | 151 (41.37) | 89 (43.84) | 103 (51.76) | 347 (47.53) | |
| Regular exercise | 229 (19.97) | 74 (20.27) | 34 (16.75) | 44 (22.11) | 147 (20.14) | 0.021 |
| hsCRP (mg/dl) | 1.02 ± 3.29 | 0.96 ± 2.28 | 1.47 ± 5.72 | 1.02 ± 2.19 | 0.93 ± 3.04 | 0.222 |
| SBP (mmHg) | 116.66 ± 11.38 | 116.31 ± 11.65 | 118.79 ± 11.58 | 117.94 ± 10.98 | 115.90 ± 11.22 | 0.005 |
| Fasting glucose (mg/dl) | 89.46 ± 14.74 | 89.46 ± 11.69 | 89.58 ± 21.77 | 89.97 ± 18.96 | 89.28 ± 12.22 | 0.950 |
| AST (U/I) | 22.11 ± 8.37 | 23.30 ± 9.16 | 22.34 ± 8.73 | 22.98 ± 9.46 | 21.21 ± 7.41 | <0.001 |
| ALT (U/I) | 20.29 ± 10.37 | 20.61 ± 10.46 | 20.79 ± 10.40 | 20.87 ± 10.96 | 19.83 ± 10.14 | 0.411 |
| GGT (U/I) | 26.55 ± 28.65 | 24.57 ± 22.89 | 27.71 ± 28.58 | 24.68 ± 21.93 | 27.74 ± 32.58 | 0.247 |
| Dyslipidemia (%) | 27.5 | 26.8 | 29.1 | 25.1 | 28.1 | 0.798 |
| HOMA-IR | 0.94 ± 0.61 | 0.92 ± 0.57 | 0.92 ± 0.66 | 0.95 ± 0.59 | 0.95 ± 0.62 | 0.925 |
| MASLD (%) | 247 (16.5) | 57 (15.6) | 31 (15.3) | 32 (16.1) | 127 (17.4) | |
| Follow up (month) | 31.1 (12, 83.3) | 39.0 (12, 83.3) | 33.8 (12, 77.5) | 31.9 (12, 74.6) | 25.5 (12, 80.8) | |
| Interval between serial biopsy (months) | 23.1 (5.0, 77.5) | 21.6 (5.0, 73.1) | 24.6 (7.4, 70.3) | 22.4 (5.2, 73.7) | 23.2 (5.8, 77.5) |
Values are presented as mean±standard deviation, median (min, max) or number (%) by descriptive analysis, frequency analysis. H. pylori, Helicobacter pylori; hsCRP, high-sensitivity C-reactive protein: SBP, systolic blood pressure: AST, aspartate aminotransferase; ALT, alanine aminotransferase; GGT, gamma-glutamyltransferase; HOMA-IR, homeostasis model assessment of insulin resistance; MASLD, metabolic dysfunction-associated steatotic liver disease. Dyslipidemia: HDL≤40 mg/dl or TG≥200 mg/dl or LDL≥160 mg/dl or use of dyslipidemia medication.
Table 2.
Factors associated with MASLD development.
| Univariable analysis | Multivariable analysis | |||||
|---|---|---|---|---|---|---|
| HR (95% CI) | p-value | HR (95% CI) | p-value | |||
| Age | 1.02 (1.00, 1.04) | 0.019 | 1.02 (1.00, 1.04) | 0.033 | ||
| Male sex | 3.00 (2.14, 4.21) | <0.001 | 1.89 (1.18, 3.01) | 0.008 | ||
| Body mass index (kg/m2) | ||||||
| <18.5 | - | - | ||||
| 18.5-24.9 | reference | Reference | ||||
| 25-29.9 | 2.87 (2.20, 3.74) | <0.001 | 1.99 (1.49, 2.66) | <0.001 | ||
| ≥30 | 6.70 (3.52, 12.75) | <0.001 | 6.48 (3.31, 12.69) | <0.001 | ||
| Smoking | ||||||
| Never smoker | reference | Reference | ||||
| Current(<1pack/day) | 2.50 (1.76, 3.56) | <0.001 | 1.40 (0.92, 2.13) | 0.115 | ||
| Current(≥1pack/day) | 2.47 (1.67, 3.65) | <0.001 | 1.17 (0.75, 1.84) | 0.487 | ||
| Alcohol | ||||||
| Mild (10g/day) | reference | Reference | ||||
| Modest (10g/day) | 1.64 (1.19, 2.26) | 0.002 | 0.91 (0.64, 1.29) | 0.598 | ||
| Regular exercise | 0.84 (0.61, 1.17) | 0.315 | 0.83 (0.59, 1.17) | 0.288 | ||
| hsCRP (mg/dl) | 1.02 (1.00, 1.05) | 0.074 | ||||
| SBP (mmHg) | 1.02 (1.01, 1.03) | 0.001 | 1.00 (0.99, 1.01) | 0.726 | ||
| Fasting glucose (mg/dl) | 1.01 (1.01, 1.02) | <0.001 | 1.01 (1.00, 1.01) | 0.022 | ||
| AST (U/I) | 1.02 (1.01, 1.04) | <0.001 | 0.99 (0.97, 1.01) | 0.406 | ||
| ALT (U/I) | 1.04 (1.03, 1.05) | <0.001 | 1.02 (1.01, 1.04) | 0.004 | ||
| GGT (U/I) | 1.01 (1.01, 1.01) | <0.001 | 1.01 (1.00, 1.01) | 0.003 | ||
| Dyslipidemia (%) | 2.23 (1.73, 2.86) | <0.001 | 1.51 (1.15, 1.97) | 0.003 | ||
| H. pylori activity status | ||||||
| H. pylori naïve | reference | Reference | ||||
| H. pylori de-novo | 1.21 (0.78, 1.88) | 0.388 | 1.04 (0.65, 1.65) | 0.884 | ||
| H. pylori Eradicated | 1.18 (0.77, 1.82) | 0.446 | 1.18 (0.75, 1.85) | 0.472 | ||
| H. pylori Persistent | 1.48 (1.08, 2.02) | 0.015 | 1.41 (1.01, 1.96) | 0.045 | ||
p-values were calculated using the Cox proportional hazard model. MASLD, metabolic dysfunction-associated steatotic liver disease; HR, hazard ratio; CI, confidence interval; H. pylori, Helicobacter pylori; hsCRP, high-sensitivity C-reactive protein; SBP, systolic blood pressure; AST, aspartate aminotransferase; ALT, alanine aminotransferase; GGT, gamma-glutamyltransferase. Dyslipidemia: HDL≤40 mg/dl or TG≥200 mg/dl or LDL≥160 mg/dl or use of dyslipidemia medication.
Table 3.
Active H. pylori infection status and the development of MASLD.
| Model 0 | Model 1 | Model 2 | Model 3 | |||||
|---|---|---|---|---|---|---|---|---|
| HR (95% CI) | p-value | HR (95% CI) | p-value | HR (95% CI) | p-value | HR (95% CI) | p-value | |
| Active H. pylori infection status divided by 4 groups | ||||||||
| Naïve (-/-) | Reference | Reference | Reference | reference | ||||
| De-novo (-/+) | 1.21 (0.78, 1.88) | 0.388 | 1.13 (0.73, 1.76) | 0.573 | 1.11 (0.70, 1.76) | 0.659 | 1.04 (0.65, 1.65) | 0.884 |
| Eradicated (+/-) | 1.18 (0.77, 1.82) | 0.446 | 1.16 (0.75, 1.79) | 0.516 | 1.13 (0.72, 1.76) | 0.596 | 1.18 (0.75, 1.85) | 0.472 |
| Persistent (+/+) | 1.48 (1.08, 2.02) | 0.015 | 1.48 (1.07, 2.04) | 0.017 | 1.39 (1.00, 1.92) | 0.051 | 1.41 (1.01, 1.96) | 0.045 |
| Last active H. pylori infection (Baseline H. pylori activity) | ||||||||
| H. pylori (-) | Reference | Reference | Reference | reference | ||||
| H. pylori (+) | 1.34 (1.03, 1.74) | 0.029 | 1.32 (1.02, 1.73) | 0.038 | 1.27 (0.97, 1.66) | 0.086 | 1.24 (0.94, 1.63) | 0.122 |
| Persistently active H. pylori infection | ||||||||
| Others | Reference | Reference | Reference | reference | ||||
| Persistent | 1.35 (1.05, 1.73) | 0.019 | 1.38 (1.07, 1.78) | 0.014 | 1.31 (1.01, 1.69) | 0.043 | 1.33 (1.02, 1.73) | 0.033 |
p-values were calculated using the Cox proportional hazard model. Model 1: Adjusted for age, sex. Model 2: Model 1 plus adjustment for BMI, exercise, smoking, alcohol drinking, SBP, fasting glucose, dyslipidemia. Model 3: Model 2 plus adjustment for AST, ALT, GGT. H. pylori, Helicobacter pylori; MASLD, metabolic dysfunction-associated steatotic liver disease; HR, hazard ratio; CI, confidence interval; BMI, body mass index; SBP, systolic blood pressure; AST, aspartate aminotransferase; ALT, alanine aminotransferase; GGT, gamma-glutamyltransferase.. Dyslipidemia: HDL≤40 mg/dl or TG≥200 mg/dl or LDL≥160 mg/dl or use of dyslipidemia medication.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



