
Submitted:
20 January 2025
Posted:
21 January 2025
You are already at the latest version
Abstract
Objectives: Thermal ablation has emerged as an effective, nephron-sparing treatment for small renal masses (SRMs), particularly in patients with comorbidities. However, tumor recurrence remains a challenge, necessitating evidence-based approaches for salvage management. This review examines the outcomes of minimally invasive modalities for managing recurrence following primary ablation of SRMs.
Methods: A literature review was conducted using the Medline database, following PRISMA guidelines. Studies published between 1981 and 2024 were screened based on predefined PICO criteria. Inclusion focused on patients with tumor recurrence after primary ablation therapy who underwent minimally invasive salvage treatments including repeat ablation, laparoscopic/robotic partial or radical nephrectomy, or active surveillance. Data extracted included patient demographics, initial treatments, recurrence timelines, salvage modalities, and outcomes.
Results: Of 364 patients across 29 studies, 249 (68.4%) underwent re-ablation, 82 (22.5%) were treated with laparoscopic/robotic partial or radical nephrectomy, and 33 (9%) were managed with active surveillance. Among 249 patients with re-ablation, 179 (71.9%) showed no evidence of disease, 67 (26.9%) experienced recurrence, and outcomes were indeterminate in 3 (1.2%). Salvage minimally invasive partial or radical nephrectomy outcomes were available for 64 cases, with 63 (98.4%) showing no recurrence. In 33 patients under active surveillance, 4 died, 4 underwent surgery, and 25 remained under monitoring, though follow-up data were limited.
Conclusion: Minimally invasive salvage modalities, such as re-ablation and laparoscopic/robotic partial or radical nephrectomy, effectively manage tumor recurrence, achieving >70% and >98% oncological success, respectively, despite technical challenges. Future studies directly comparing these modalities are essential for establishing standardized protocols for salvage management.
Keywords:
renal cell carcinoma
; small renal mass
; recurrence
; ablation
; salvage nephrectomy
; active surveillance
; minimally invasive surgery
; laparoscopic
; robotic
1. Introduction
Kidney cancer, now the 12th most common malignancy worldwide, is on the rise, with an estimated 400,000 new cases and 175,000 deaths annually. Around 50% of new patients are diagnosed with stage I renal cell carcinoma (RCC) (T1a) as reports show an increasing percentage from 43% to 57% Between 1993 to 2004[1]. Small renal mass (SRM) is consistent with the definition of clinical stage I kidney tumors (cT1a) as incidentally detected, contrast-enhancing small-size (<4cm) solid or cystic lesions[2]. When approaching patients with SRM, nephron-sparing procedures should be prioritized. Ablative modalities have emerged as a viable alternative for managing cT1a solid renal masses, particularly those smaller than 3 cm, as recommended by the American Urological Association (AUA) guidelines[3]. These therapies demonstrate favorable efficacy and excellent safety profiles, contributing to their growing utilization. With advantages such as low postoperative morbidity and renal function preservation, ablative techniques are confidently employed by radiologists and urologists through percutaneous and laparoscopic approaches[4,5]. Common ablation modalities include cryoablation (CA), microwave ablation (MWA), radiofrequency ablation (RFA), high-intensity focused ultrasound (HIFU), and irreversible electroporation (IRE) [6,7].
Recurrence rates following ablative techniques vary ranging from 1-9% based on the method and approach employed [8]. Most recurrences are detected within the first five years after the procedure [9]. Given the higher recurrence rates associated with ablative therapies compared to partial or radical nephrectomy, it is crucial to establish a well-structured follow-up strategy and provide salvage modalities to address the treatment failures [3].
There is currently no consensus on the optimal treatment for management of tumor recurrence following ablative therapies. Re-ablation, partial or radical nephrectomy, and active surveillance remain the primary management strategies employed to address post-ablation tumor recurrence[10]. Re-ablation is commonly used due to its demonstrated efficacy and acceptable complication rates, particularly in older patients with higher comorbidities[11]. Despite technical difficulties posed by fibrosis from primary ablation treatments, laparoscopic /robotic partial and radical nephrectomy remain viable treatment options in selected cases[12].
This literature review aims to present the outcomes of various minimally invasive approaches for management of tumor recurrence following primary ablation of small renal masses. To our knowledge, this is the largest accumulated series of patients with recurrence after renal mass ablation who were managed with minimally invasive modalities (including active surveillance).
2. Material and Methods:
A systematic literature review was conducted using the Medline (PubMed) database, adhering to the 2020 Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) protocol for reporting[13]. Various combinations of the following keywords were used to identify relevant articles: salvage, therapy, recurrent, kidney, cancer, ablation, renal retreatment, mass, ablative, nephrectomy, MWA, RFA, HIFU, CA, partial, radical, robotic, percutaneous, laparoscopic, and minimally invasive surgery. The search results were filtered by species (human), publication type (article), language (English) and publication year (1981 to 2024).
Studies were selected based on the PICO criteria: [patient, intervention, comparator, outcome] [14].
- (P) Adults (> 18 years) with prior ablative therapy for renal cancer presenting with tumor recurrence during follow-up period.
- (I) Minimally invasive treatment for tumor recurrence after primary ablation, including re-ablation, laparoscopic or robotic partial or radical nephrectomy and active surveillance.
- (C) Comparisons between different re-treatment modalities regarding outcomes, follow-up, and other relevant factors.
- (O) Outcomes of interest included primary and secondary treatment success, retreatment outcomes (e.g. disease recurrence, metastasis, death, successful treatment or no evidence of disease (NED)), tumor types and stages, time to recurrence, follow-up duration, and patient characteristics like age and gender, if available.
Figure 1 illustrates the study selection process following the PRISMA protocol. The initial search identified 2,064 studies published between 1981 and 2024 using various keyword combinations. Sixty additional studies were included after reviewing the reference lists of relevant studies to identify further management strategies for recurrence after ablative therapies and their outcomes. Of these, 14 were excluded due to duplication. After screening titles and abstracts for our eligibility criteria, 1,945 articles were excluded. The full text of the remaining 165 articles were studied; additional 136 studies were excluded. These exclusions encompassed studies with open surgery approach for salvage treatments, review articles, editorial comments, editor letters, and conference abstracts. Moreover, 35 additional studies were excluded despite meeting our initial criteria, due to missed critical data, such as the procedure or patients’ outcomes[15,16,17,18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49]. A full-text review of the remaining studies resulted in the inclusion of 29 studies, which collectively evaluated 364 patients[12,50,51,52,53,54,55,56,57,58,59,60,61,62,63,64,65,66,67,68,69,70,71,72,73,74,75,76,77].
Demographic data, including the type of initial ablative therapy, the time interval between the first treatment and recurrence, patient age, the type of secondary retreatment management, tumor pathology and stage, re-treatment outcomes, and follow-up duration, were systematically collected. This data formed the basis of our analysis and enabled a comparative evaluation of minimally invasive approaches (including active surveillance) for managing tumor recurrence after primary ablation.
Two authors independently performed article screening, selection, and data extraction. The senior author supervised the process and resolved any disagreements. This approach ensures a transparent and reliable review process, minimizing potential biases and enhancing the credibility of our conclusions.
3. Results
As mentioned above, we extracted and analyzed the data of 364 patients from 29 studies. These patients underwent minimally invasive modalities (including active surveillance) for management of tumor recurrence following primary renal mass ablation (Table 1). Six studies focused exclusively on laparoscopic or robotic-assisted partial or radical nephrectomy as a secondary salvage approach; ten studies evaluated repeat ablation as the primary modality and thirteen studies investigated both minimally invasive nephrectomy (partial or radical) and repeat ablation for recurrence management. In eight studies, active surveillance was chosen as the management option for some patients while other options were selected for the rest of patients.
All the patients included in this review had tumor recurrence after primary ablative therapy (n=364). As shown in Table 2, most of these patients had undergone CA (198 cases: 54.3%) and RFA (123 cases: 33.7%) as their primary method of ablation.
For management of tumor recurrence after primary ablation among the 364 patients included in this review, 249 patients (68.4%) underwent second ablation therapy, 82 cases (22.5%) were treated with laparoscopic/ robotic partial or radical nephrectomy, and 33 cases (9%) were managed with active surveillance (Table 3).
Of the 249 patients who underwent re-ablation for tumor recurrence, 179 (71.9%) had no evidence of disease (recurrence) during follow-up. Tumor recurrence was observed in 67 cases (26.9%), while the procedural outcomes could not be determined in 3 (1.2%) patients. Among 82 cases treated with laparoscopic/ robotic partial or radical nephrectomy, the outcomes for 18 cases (21.9%) were either unavailable or the patients were lost to follow-up. Among the remaining 64 patients with reported treatment outcome, only one patient experienced recurrence and succumbed to the disease, while 63 patients were successfully treated with no recurrence reported during follow up period.
Regarding the 33 patients managed with active surveillance, there were significant limitations in obtaining follow-up details and outcomes. Of the reported cases, four patients died during follow-up, four eventually underwent surgery, and 25 remained under active monitoring. Comprehensive information on secondary treatment outcomes is presented in Table 4.
4. Discussion
Since 2017, the AUA guidelines have recommended ablation therapy as an alternative option for managing cT1a solid renal masses (<4 cm in size) [78]. These SRMs are generally characterized by slow growth, low-grade histology, and a minimal tendency for metastasis [79]. While partial nephrectomy remains the standard of care for cT1a renal masses, thermal ablation and active surveillance are particularly viable options for managing the disease in older patients with significant comorbidities[78].
According to the current AUA guidelines, patients undergoing ablative procedures should have contrast-enhanced imaging both before and within six months after treatment if biopsy results indicate malignant or nondiagnostic tumors [78]. At most institutions, computed tomography (CT) or magnetic resonance imaging (MRI) is performed within the first-month after the ablation to detect residual tumors (i.e. failed ablation) and establish a baseline imaging of the ablation zone. Protocols for detecting recurrence after the negative initial follow-up imaging vary by institution. Typically, three to four imaging studies are performed during the first year, followed by imaging every 6 to 12 months in subsequent years [80]. For monitoring patients after primary ablation, AUA guidelines recommend a low-risk postoperative follow-up protocol that involves medical history reviews, physical examination, laboratory testing, abdominal and chest imaging at specified intervals (6, 12, 24, 36, 48, 60, 72–84, and 96–120 months) [3].
In our review, about 65% of recurrences were identified between 6 and 30 months after primary ablation. However, several studies documented recurrences that may occur as late as 54 months, highlighting the importance of long-term imaging to detect late recurrence after primary ablation. Stewart et al. demonstrated that adherence to the 2014 AUA guideline imaging recommendations for low-risk cases could miss at least 60% of recurrences if follow-up is limited to three years[81].
Interpreting findings on post-procedure CT and MRI scans requires expertise in recognizing the unique imaging features of the ablation zone. For instance, benign peri-ablation enhancement, commonly observed on post-procedure imaging, may persist for months before resolving. Additionally, homogenous contrast enhancement of the ablation zone immediately after RFA can mimic tumor recurrence [82,83]. One study reported that 1 in 5 patients (20%) treated with CA showed peripheral rim enhancement of the treatment zone at three months after the ablation, which decreased by approximately 5% per year during follow-up. By the end of the study, only 1.8% of their patients remained suspicious of having residual tumors [25].
Therefore, active surveillance can play a crucial role after renal ablation, enabling the monitoring of imaging findings and the distinguish between benign post-treatment phenomena and true tumor recurrence. To avoid overtreatment, Breda et al. proposed one-year surveillance as a safe management strategy for patients presenting with early enhancement on scans following CA or RFA [84].
There is currently no consensus on the optimal management modality for tumor recurrence following ablative therapies. Re-ablation, partial or radical nephrectomy, and active surveillance remain the primary management strategies for addressing post-ablation tumor recurrence[10]. All cases included in this review involved patients diagnosed with tumor recurrence after primary ablation who opted for active surveillance or a minimally invasive salvage modality such as re-ablation or laparoscopic/ robotic partial or radical nephrectomy. Higher comorbidity indices among patients undergoing primary ablation and concerns about adhesions and surgical complications may lead many clinicians to favor ablation for managing recurrent tumors after primary ablation.
In this review, of the 364 analyzed patients, 249 (68.4%) underwent salvage ablation, the majority (>90%) of these patients were followed for more than 20 months (range 10-132 months). Of the 249 patients who underwent re-ablation for tumor recurrence following primary ablation, 179 (71.8%) patients achieved successful second ablation, with no evidence of disease during follow-up. Sixty-seven patients (26.9%) experienced new recurrences following secondary ablation, while three were lost to follow-up.
The 71.8% success rate of second ablation observed in our review closely aligns with the 76% success rate (38 out of 50 cases) reported in a prior cohort study on the management of residual or recurrent disease following thermal ablation of renal cortical tumors[62]. Interestingly, four studies included in our review, documented outcomes of a third retreatment attempt in 12 patients with recurrences after the second ablation. Among these, two patients underwent successful salvage nephrectomy, seven patients achieved successful tertiary ablations, and three cases were observed after a failed tertiary ablation.
While the overall success rate of second ablation is promising, it is imperative to counsel patients on the chance of failure and the need for proceeding with partial/ radical nephrectomy. This approach ensures informed decision-making before treatment.
In case of nephrectomy after primary ablation, although partial nephrectomy as a nephron-sparing procedure is often prioritized, post-ablation fibrosis, adhesions, and associated complications may necessitate intraoperative conversion to radical nephrectomy. These patients should be counseled about the complexity of partial nephrectomy and the potential need for conversion to radical nephrectomy [37].
Notably, despite these concerns, 82 (22.5%) patients in the current series underwent successful laparoscopic/ robotic partial or radical nephrectomy, comprising 46 robotic partial nephrectomy (56.1%) and 36 robotic/ laparoscopic radical nephrectomy (43.9%). Most salvage nephrectomy cases (~77%) in this review were followed for at least 30–50 months. Among the 64 cases with reported outcomes, all but one patient (who died of cancer) were successfully treated with no evidence of disease during follow-up. For example, Martini et al., reported on 35 patients with tumor recurrence after primary ablation, all of them were managed with robotic partial nephrectomy, achieving successful outcomes with no instances of recurrence during their follow-up[12].
Overall, while salvage partial or radical nephrectomy in post-ablation settings might be associated with some technical challenges, it can be performed safely in carefully selected patients and yields excellent postoperative outcomes. Future studies directly comparing the outcomes of re-ablation versus minimally invasive nephrectomy are necessary to provide more robust evidence supporting the optimal salvage treatment modality in this setting.
When determining the optimal treatment for tumor recurrence following primary ablation, a thorough assessment of the patient’s overall health, comorbidities, tumor characteristics, and procedural considerations is paramount. Robotic partial nephrectomy, when performed by highly experienced surgeons, seems the preferred minimally invasive nephron sparing approach, offering a high rate of disease control. However, re-ablation is a less invasive procedure with an acceptable success rate and can be offered to older patients with significant comorbidities. Radical nephrectomy can be reserved for patients with tumors exhibiting adverse features and/or high nephrometry scores. Moreover, active surveillance plays a pivotal role in evaluating both patient status and tumor dynamics, facilitating timely and judicious intervention when clinically warranted. Surveillance is particularly advantageous for patients with small renal masses and substantial comorbidities, where the potential risks of immediate intervention may surpass its benefits. Moreover, active surveillance aids clinicians in differentiating benign imaging findings from true tumor recurrence, thereby optimizing patient management and reducing unnecessary procedures.
Our review study has several limitations. The scarcity of studies specifically reporting on patients with local recurrence following primary ablation required extensive efforts to identify and analyze matching cases in the literature. A significant number of studies had to be excluded due to insufficient outcome data or the inability to extract relevant case outcomes from pooled datasets. Furthermore, the available data sometimes lacked granularity; some of the studies only provided the number of cases and their outcomes without critical information, such as tumor size, which limited our ability to perform detailed analyses. Variability in physician expertise and the method of ablation procedures may also have contributed to heterogeneity in the reported outcomes. Despite these limitations this review collected a large series of patients underwent various salvage minimally invasive treatment modalities after failed primary ablation.
5. Conclusions
This review highlights the outcomes of various minimally invasive management strategies for tumor recurrence following primary ablation of small renal masses, including repeat ablation, laparoscopic/ robotic partial and radical nephrectomy, and active surveillance. Our findings underscore the efficacy of second thermal ablation as a salvage treatment, achieving disease control in more than 70% of patients, while minimally invasive partial or radical nephrectomy demonstrated excellent oncological control (>98%) in carefully selected patients despite technical challenges. Active surveillance can also be considered as a viable option for tumors with indolent features in patients with comorbidities. Surveillance is also a non-invasive approach to distinguish benign post-treatment changes from true recurrence. The variability in timing of recurrence following primary ablation (e.g., the chance of recurrence beyond 30 months) highlights the critical importance of long-term follow-up after ablation to optimize patient outcomes. Longitudinal studies comparing nephrectomy versus re-ablation with extended follow-up are essential to further define the role of these strategies and establish standardized protocols for managing tumor recurrence after primary ablation.
References
- Kane, C.J.; Mallin, K.; Ritchey, J.; Cooperberg, M.R.; Carroll, P.R. Renal cell cancer stage migration: analysis of the National Cancer Data Base. Cancer 2008, 113, 78–83. [Google Scholar] [CrossRef] [PubMed]
- Maroni, P.; Moss, J. Nephron-sparing surgery. Semin Intervent Radiol 2014, 31, 104–106. [Google Scholar] [CrossRef]
- Campbell, S.C.; Uzzo, R.G.; Karam, J.A.; et al. Renal Mass and Localized Renal Cancer: Evaluation, Management, and Follow-up: AUA Guideline: Part II. Journal of Urology 2021, 206, 209. [Google Scholar] [CrossRef] [PubMed]
- Abbosh, P.H.; Bhayani, S.B. Thermoablation of Renal Masses: The Urologist's Perspective. Semin Intervent Radiol 2011, 28, 361–366. [Google Scholar] [CrossRef]
- Mouli, S.K.; McDevitt, J.L.; Su, Y.K.; Ragin, A.B.; Gao, Y.; Nemcek, A.A., Jr.; Lewandowski, R.J.; Salem, R.; Sato, K.T. Analysis of the RENAL and mRENAL Scores and the Relative Importance of Their Components in the Prediction of Complications and Local Progression after Percutaneous Renal Cryoablation. J Vasc Interv Radiol 2017, 28, 860–867. [Google Scholar] [CrossRef] [PubMed]
- Klingler, H.C.; Susani, M.; Seip, R.; Mauermann, J.; Sanghvi, N.; Marberger, M.J. A novel approach to energy ablative therapy of small renal tumours: laparoscopic high-intensity focused ultrasound. Eur Urol 2008, 53, 810–816. [Google Scholar] [CrossRef] [PubMed]
- Wagstaff, P.; Ingels, A.; Zondervan, P.; de la Rosette, J.J.; Laguna, M.P. Thermal ablation in renal cell carcinoma management: a comprehensive review. Curr Opin Urol 2014, 24, 474–482. [Google Scholar] [CrossRef] [PubMed]
- Aveta, A.; Iossa, V.; Spena, G.; Conforti, P.; Pagano, G.; Dinacci, F.; Verze, P.; Manfredi, C.; Ferro, M.; Lasorsa, F.; et al. Ablative Treatments for Small Renal Masses and Management of Recurrences: A Comprehensive Review. Life (Basel) 2024, 14. [Google Scholar] [CrossRef]
- Adamy, A.; Chong, K.T.; Chade, D.; Costaras, J.; Russo, G.; Kaag, M.G.; Bernstein, M.; Motzer, R.J.; Russo, P. Clinical characteristics and outcomes of patients with recurrence 5 years after nephrectomy for localized renal cell carcinoma. J Urol 2011, 185, 433–438. [Google Scholar] [CrossRef]
- Cross, B.W.; Parker, D.C.; Cookson, M.S. Salvage Surgery After Renal Mass Ablation. Urol Clin North Am 2017, 44, 305–312. [Google Scholar] [CrossRef] [PubMed]
- Singer, E.A.; Bratslavsky, G. Management of locally recurrent kidney cancer. Curr Urol Rep 2010, 11, 15–21. [Google Scholar] [CrossRef] [PubMed]
- Martini, A.; Turri, F.; Barod, R.; Rocco, B.; Capitanio, U.; Briganti, A.; Montorsi, F.; Mottrie, A.; Challacombe, B.; Lagerveld, B.W.; et al. Salvage Robot-assisted Renal Surgery for Local Recurrence After Surgical Resection or Renal Mass Ablation: Classification, Techniques, and Clinical Outcomes. Eur Urol 2021, 80, 730–737. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Eriksen, M.B.; Frandsen, T.F. The impact of patient, intervention, comparison, outcome (PICO) as a search strategy tool on literature search quality: a systematic review. J Med Libr Assoc 2018, 106, 420–431. [Google Scholar] [CrossRef] [PubMed]
- Beksac, A.T.; Carbonara, U.; Abou Zeinab, M.; Meagher, M.; Hemal, S.; Tafuri, A.; Tuderti, G.; Antonelli, A.; Autorino, R.; Simone, G.; et al. Redo Robotic Partial Nephrectomy for Recurrent Renal Tumors: A Multi-Institutional Analysis. J Endourol 2022, 36, 1296–1301. [Google Scholar] [CrossRef] [PubMed]
- Bersang, A.B.; Søndergaard Mosholt, K.S.; Verner Jensen, C.; Germer, U.; Holm, M.; Røder, M.A. Safety and oncological outcome following radiofrequency ablation of small renal masses in a single center. Scand J Urol 2021, 55, 203–208. [Google Scholar] [CrossRef] [PubMed]
- Bertolo, R.; Garisto, J.; Armanyous, S.; Agudelo, J.; Lioudis, M.; Kaouk, J. Perioperative, oncological and functional outcomes after robotic partial nephrectomy vs. cryoablation in the elderly: A propensity score matched analysis. Urologic Oncology: Seminars and Original Investigations 2019, 37, e299–e294. [Google Scholar] [CrossRef] [PubMed]
- Bianchi, L.; Chessa, F.; Piazza, P.; Ercolino, A.; Mottaran, A.; Recenti, D.; Serra, C.; Gaudiano, C.; Cappelli, A.; Modestino, F.; et al. Percutaneous ablation or minimally invasive partial nephrectomy for cT1a renal masses? A propensity score-matched analysis. Int J Urol 2022, 29, 222–228. [Google Scholar] [CrossRef] [PubMed]
- Chan, P.; Vélasco, S.; Vesselle, G.; Boucebci, S.; Herpe, G.; Debaene, B.; Ingrand, P.; Irani, J.; Tasu, J.P. Percutaneous microwave ablation of renal cancers under CT guidance: safety and efficacy with a 2-year follow-up. Clin Radiol 2017, 72, 786–792. [Google Scholar] [CrossRef]
- Clark, T.W.; Malkowicz, B.; Stavropoulos, S.W.; Sanchez, R.; Soulen, M.C.; Itkin, M.; Patel, A.; Mondschein, J.I.; Wein, A.J. Radiofrequency ablation of small renal cell carcinomas using multitined expandable electrodes: preliminary experience. J Vasc Interv Radiol 2006, 17, 513–519. [Google Scholar] [CrossRef] [PubMed]
- De Filippo, M.; Ziglioli, F.; Russo, U.; Pagano, P.; Brunese, L.; Bertelli, E.; Pagnini, F.; Maestroni, U. Radiofrequency ablation (RFA) of T1a renal cancer with externally cooled multitined expandable electrodes. Radiol Med 2020, 125, 790–797. [Google Scholar] [CrossRef] [PubMed]
- Fraisse, G.; Colleter, L.; Peyronnet, B.; Khene, Z.E.; Mandoorah, Q.; Soorojebally, Y.; Bourgi, A.; De La Taille, A.; Roupret, M.; De Kerviler, E.; et al. Peri-operative and local control outcomes of robot-assisted partial nephrectomy vs percutaneous cryoablation for renal masses: comparison after matching on radiological stage and renal score. BJU Int 2019, 123, 632–638. [Google Scholar] [CrossRef] [PubMed]
- Guan, W.; Bai, J.; Liu, J.; Wang, S.; Zhuang, Q.; Ye, Z.; Hu, Z. Microwave ablation versus partial nephrectomy for small renal tumors: intermediate-term results. J Surg Oncol 2012, 106, 316–321. [Google Scholar] [CrossRef]
- Guillotreau, J.; Haber, G.-P.; Autorino, R.; Miocinovic, R.; Hillyer, S.; Hernandez, A.; Laydner, H.; Yakoubi, R.; Isac, W.; Long, J.-A.; et al. Robotic Partial Nephrectomy Versus Laparoscopic Cryoablation for the Small Renal Mass. European Urology 2012, 61, 899–904. [Google Scholar] [CrossRef] [PubMed]
- Hegarty, N.J.; Gill, I.S.; Desai, M.M.; Remer, E.M.; O'Malley, C.M.; Kaouk, J.H. Probe-ablative nephron-sparing surgery: cryoablation versus radiofrequency ablation. Urology 2006, 68, 7–13. [Google Scholar] [CrossRef] [PubMed]
- Jasinski, M.; Bielinska, M.; Siekiera, J.; Kamecki, K.; Salagierski, M. Ultrasound-Guided Percutaneous Thermal Ablation of Renal Cancers—In Search for the Ideal Tumour. Cancers 2023, 15, 518. [Google Scholar] [CrossRef]
- Jiménez, J.A.; Zhang, Z.; Zhao, J.; Abouassaly, R.; Fergany, A.; Gong, M.; Kaouk, J.; Krishnamurthi, V.; Stein, R.; Stephenson, A.; et al. Surgical Salvage of Thermal Ablation Failures for Renal Cell Carcinoma. J Urol 2016, 195, 594–600. [Google Scholar] [CrossRef] [PubMed]
- Karam, J.A.; Wood, C.G.; Compton, Z.R.; Rao, P.; Vikram, R.; Ahrar, K.; Matin, S.F. Salvage surgery after energy ablation for renal masses. BJU International 2015, 115, 74–80. [Google Scholar] [CrossRef] [PubMed]
- Konstantinidis, C.; Trilla, E.; Serres, X.; Montealegre, C.; Lorente, D.; Castellón, R.; Morote, J. Association among the R.E.N.A.L. nephrometry score and clinical outcomes in patients with small renal masses treated with percutaneous contrast enhanced ultrasound radiofrequency ablation. Cent European J Urol 2019, 72, 92–99. [Google Scholar] [CrossRef]
- Kowalczyk, K.J.; Hooper, H.B.; Linehan, W.M.; Pinto, P.A.; Wood, B.J.; Bratslavsky, G. Partial nephrectomy after previous radio frequency ablation: the National Cancer Institute experience. J Urol 2009, 182, 2158–2163. [Google Scholar] [CrossRef] [PubMed]
- Levinson, A.W.; Su, L.M.; Agarwal, D.; Sroka, M.; Jarrett, T.W.; Kavoussi, L.R.; Solomon, S.B. Long-term oncological and overall outcomes of percutaneous radio frequency ablation in high risk surgical patients with a solitary small renal mass. J Urol 2008, 180, 499–504. [Google Scholar] [CrossRef]
- Ma, Y.; Bedir, S.; Cadeddu, J.A.; Gahan, J.C. Long-term outcomes in healthy adults after radiofrequency ablation of T1a renal tumours. BJU Int 2014, 113, 51–55. [Google Scholar] [CrossRef] [PubMed]
- Margue, G.; Michiels, C.; Allenet, C.; Dupitout, L.; Ricard, S.; Jambon, E.; Blanc, P.; Alezra, E.; Estrade, V.; Capon, G.; et al. Feasibility of salvage robotic partial nephrectomy after ablative treatment failure (UroCCR-62 study). Minerva Urol Nephrol 2022, 74, 209–215. [Google Scholar] [CrossRef]
- Matin, S.F.; Ahrar, K.; Cadeddu, J.A.; Gervais, D.A.; McGovern, F.J.; Zagoria, R.J.; Uzzo, R.G.; Haaga, J.; Resnick, M.I.; Kaouk, J.; et al. Residual and recurrent disease following renal energy ablative therapy: a multi-institutional study. J Urol 2006, 176, 1973–1977. [Google Scholar] [CrossRef]
- Mayo-Smith, W.W.; Dupuy, D.E.; Parikh, P.M.; Pezzullo, J.A.; Cronan, J.J. Imaging-guided percutaneous radiofrequency ablation of solid renal masses: techniques and outcomes of 38 treatment sessions in 32 consecutive patients. AJR Am J Roentgenol 2003, 180, 1503–1508. [Google Scholar] [CrossRef] [PubMed]
- McDougal, W.S.; Gervais, D.A.; McGovern, F.J.; Mueller, P.R. Long-term followup of patients with renal cell carcinoma treated with radio frequency ablation with curative intent. J Urol 2005, 174, 61–63. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, C.T.; Lane, B.R.; Kaouk, J.H.; Hegarty, N.; Gill, I.S.; Novick, A.C.; Campbell, S.C. Surgical Salvage of Renal Cell Carcinoma Recurrence After Thermal Ablative Therapy. The Journal of Urology 2008, 180, 104–109. [Google Scholar] [CrossRef]
- Olweny, E.O.; Park, S.K.; Tan, Y.K.; Best, S.L.; Trimmer, C.; Cadeddu, J.A. Radiofrequency ablation versus partial nephrectomy in patients with solitary clinical T1a renal cell carcinoma: comparable oncologic outcomes at a minimum of 5 years of follow-up. Eur Urol 2012, 61, 1156–1161. [Google Scholar] [CrossRef] [PubMed]
- Panhelleux, M.; Balssa, L.; David, A.; Thiery-Vuillemin, A.; Kleinclauss, F.; Frontczak, A. Evaluation of local control after percutaneous microwave ablation versus partial nephrectomy: A propensity score matched study. The French Journal of Urology 2024, 34, 102534. [Google Scholar] [CrossRef] [PubMed]
- Ryoo, H.; Kang, M.; Sung, H.H.; Jeon, H.G.; Jeong, B.C.; Jeon, S.S.; Lee, H.M.; Park, B.K.; Seo, S.I. A Comparison of Functional and Oncologic Outcomes between Partial Nephrectomy and Radiofrequency Ablation in Patients with Chronic Kidney Disease after Propensity Score Matching. Diagnostics (Basel) 2022, 12. [Google Scholar] [CrossRef]
- Salagierski, M.; Salagierski, M.; Salagierska-Barwińska, A.; Sosnowski, M. Percutaneous ultrasound-guided radiofrequency ablation for kidney tumors in patients with surgical risk. Int J Urol 2006, 13, 1375–1379. [Google Scholar] [CrossRef] [PubMed]
- Singh, R.K.; Gideon, M.; Rajendran, R.; Mathew, G.; Nair, K. Advancing Treatment Frontiers: Radiofrequency Ablation for Small Renal Mass-Intermediate-Term Results. J Kidney Cancer VHL 2023, 10, 1–6. [Google Scholar] [CrossRef]
- Takaki, H.; Soga, N.; Kanda, H.; Nakatsuka, A.; Uraki, J.; Fujimori, M.; Yamanaka, T.; Hasegawa, T.; Arima, K.; Sugimura, Y.; et al. Radiofrequency ablation versus radical nephrectomy: clinical outcomes for stage T1b renal cell carcinoma. Radiology 2014, 270, 292–299. [Google Scholar] [CrossRef]
- Uribe, P.S.; Costabile, R.A.; Peterson, A.C. Progression of renal tumors after laparoscopic radiofrequency ablation. Urology 2006, 68, 968–971. [Google Scholar] [CrossRef] [PubMed]
- Varkarakis, I.M.; Allaf, M.E.; Inagaki, T.; Bhayani, S.B.; Chan, D.Y.; Su, L.M.; Jarrett, T.W.; Kavoussi, L.R.; Solomon, S.B. Percutaneous radio frequency ablation of renal masses: results at a 2-year mean followup. J Urol 2005, 174, 456–460. [Google Scholar] [CrossRef]
- Wasnik, A.P.; Higgins, E.J.; Fox, G.A.; Caoili, E.M.; Davenport, M.S. Yield of Routine Image-Guided Biopsy of Renal Mass Thermal Ablation Zones: 11-Year Experience. Academic Radiology 2019, 26, 232–238. [Google Scholar] [CrossRef] [PubMed]
- Wessendorf, J.; König, A.; Heers, H.; Mahnken, A.H. Repeat Percutaneous Radiofrequency Ablation of T1 Renal Cell Carcinomas is Safe in Patients with Von Hippel-Lindau Disease. Cardiovasc Intervent Radiol 2021, 44, 2022–2025. [Google Scholar] [CrossRef]
- Zagoria, R.J.; Traver, M.A.; Werle, D.M.; Perini, M.; Hayasaka, S.; Clark, P.E. Oncologic efficacy of CT-guided percutaneous radiofrequency ablation of renal cell carcinomas. AJR Am J Roentgenol 2007, 189, 429–436. [Google Scholar] [CrossRef] [PubMed]
- Zargar, H.; Samarasekera, D.; Khalifeh, A.; Remer, E.M.; O'Malley, C.; Akca, O.; Autorino, R.; Kaouk, J.H. Laparoscopic vs percutaneous cryoablation for the small renal mass: 15-year experience at a single center. Urology 2015, 85, 850–855. [Google Scholar] [CrossRef] [PubMed]
- Attawettayanon, W.; Kazama, A.; Yasuda, Y.; Zhang, J.J.H.; Shah, S.; Rathi, N.; Munoz-Lopez, C.; Lewis, K.; Li, J.; Beksac, A.T.; et al. Thermal Ablation Versus Partial Nephrectomy for cT1 Renal Mass in a Solitary Kidney: A Matched Cohort Comparative Analysis. Ann Surg Oncol 2024, 31, 2133–2143. [Google Scholar] [CrossRef]
- Breen, D.J.; Bryant, T.J.; Abbas, A.; Shepherd, B.; McGill, N.; Anderson, J.A.; Lockyer, R.C.; Hayes, M.C.; George, S.L. Percutaneous cryoablation of renal tumours: outcomes from 171 tumours in 147 patients. BJU Int 2013, 112, 758–765. [Google Scholar] [CrossRef] [PubMed]
- Caputo, P.A.; Zargar, H.; Ramirez, D.; Andrade, H.S.; Akca, O.; Gao, T.; Kaouk, J.H. Cryoablation versus Partial Nephrectomy for Clinical T1b Renal Tumors: A Matched Group Comparative Analysis. European Urology 2017, 71, 111–117. [Google Scholar] [CrossRef] [PubMed]
- Chang, X.; Liu, T.; Zhang, F.; Ji, C.; Zhao, X.; Wang, W.; Guo, H. Radiofrequency ablation versus partial nephrectomy for clinical T1a renal-cell carcinoma: long-term clinical and oncologic outcomes based on a propensity score analysis. Journal of Endourology 2015, 29, 518–525. [Google Scholar] [CrossRef] [PubMed]
- Duffey, B.; Nguyen, V.; Lund, E.; Koopmeiners, J.S.; Hulbert, J.; Anderson, J.K. Third Prize: Intermediate-Term Outcomes After Renal Cryoablation: Results of a Multi-Institutional Study. Journal of Endourology 2011, 26, 15–20. [Google Scholar] [CrossRef] [PubMed]
- Emara, A.M.; Kommu, S.S.; Hindley, R.G.; Barber, N.J. Robot-assisted partial nephrectomy vs laparoscopic cryoablation for the small renal mass: redefining the minimally invasive ‘gold standard’. BJU international 2014, 113, 92–99. [Google Scholar] [CrossRef]
- Feng, C.L.; Franco, A.; Ditonno, F.; Manfredi, C.; Chow, A.K.; Autorino, R. Robotic salvage partial nephrectomy following surgical and ablative therapies. Int Braz J Urol 2024, 50, 373–374. [Google Scholar] [CrossRef] [PubMed]
- Ferakis, N.; Bouropoulos, C.; Granitsas, T.; Mylona, S.; Poulias, I. Long-Term Results After Computed-Tomography–Guided Percutaneous Radiofrequency Ablation for Small Renal Tumors. Journal of Endourology 2010, 24, 1909–1913. [Google Scholar] [CrossRef] [PubMed]
- Gupta, A.; Raman, J.D.; Leveillee, R.J.; Wingo, M.S.; Zeltser, I.S.; Lotan, Y.; Trimmer, C.; Stern, J.M.; Cadeddu, J.A. General anesthesia and contrast-enhanced computed tomography to optimize renal percutaneous radiofrequency ablation: multi-institutional intermediate-term results. J Endourol 2009, 23, 1099–1105. [Google Scholar] [CrossRef]
- Ji, C.; Zhao, X.; Zhang, S.; Liu, G.; Li, X.; Zhang, G.; Minervini, A.; Guo, H. Laparoscopic radiofrequency ablation versus partial nephrectomy for cT1a renal tumors: Long-term outcome of 179 patients. Urologia Internationalis 2016, 96, 345–353. [Google Scholar] [CrossRef]
- Klatte, T.; Mauermann, J.; Heinz-Peer, G.; Waldert, M.; Weibl, P.; Klingler, H.C.; Remzi, M. Perioperative, oncologic, and functional outcomes of laparoscopic renal cryoablation and open partial nephrectomy: a matched pair analysis. Journal of endourology 2011, 25, 991–997. [Google Scholar] [CrossRef] [PubMed]
- Liu, N.; Huang, D.; Cheng, X.; Chong, Y.; Wang, W.; Gan, W.; Guo, H. Percutaneous radiofrequency ablation for renal cell carcinoma vs. partial nephrectomy: Comparison of long-term oncologic outcomes in both clear cell and non-clear cell of the most common subtype. Urologic Oncology: Seminars and Original Investigations 2017, 35, e531–e530. [Google Scholar] [CrossRef] [PubMed]
- Loloi, J.; Shingleton, W.B.; Nakada, S.Y.; Zagoria, R.J.; Landman, J.; Lee, B.R.; Matin, S.F.; Ahrar, K.; Leveillee, R.J.; Cadeddu, J.A.; et al. Management of Residual or Recurrent Disease Following Thermal Ablation of Renal Cortical Tumors. J Kidney Cancer VHL 2020, 7, 1–5. [Google Scholar] [CrossRef]
- Long, J.-A.; Bernhard, J.-C.; Bigot, P.; Lanchon, C.; Paparel, P.; Rioux-Leclercq, N.; Albiges, L.; Bodin, T.; Nouhaud, F.-X.; Boissier, R.; et al. Partial nephrectomy versus ablative therapy for the treatment of renal tumors in an imperative setting. World Journal of Urology 2017, 35, 649–656. [Google Scholar] [CrossRef] [PubMed]
- Lorber, G.; Glamore, M.; Doshi, M.; Jorda, M.; Morillo-Burgos, G.; Leveillee, R.J. Long-term oncologic outcomes following radiofrequency ablation with real-time temperature monitoring for T1a renal cell cancer. Urol Oncol 2014, 32, 1017–1023. [Google Scholar] [CrossRef]
- Matsumoto, E.D.; Johnson, D.B.; Ogan, K.; Trimmer, C.; Sagalowsky, A.; Margulis, V.; Cadeddu, J.A. Short-term efficacy of temperature-based radiofrequency ablation of small renal tumors. Urology 2005, 65, 877–881. [Google Scholar] [CrossRef] [PubMed]
- Murray, C.A.; Welch, B.T.; Schmit, G.D.; Schmitz, J.J.; Weisbrod, A.J.; Callstrom, M.R.; Welch, T.L.; Thompson, R.H.; Kurup, A.N.; Boorjian, S.A.; et al. Safety and Efficacy of Percutaneous Image-guided Cryoablation of Completely Endophytic Renal Masses. Urology 2019, 133, 151–156. [Google Scholar] [CrossRef]
- Okhunov, Z.; Chamberlin, J.; Moreira, D.M.; George, A.; Babaian, K.; Shah, P.; Youssef, R.; Kaler, K.S.; Lobko, II; Kavoussi, L. ; et al. Salvage Percutaneous Cryoablation for Locally Recurrent Renal-Cell Carcinoma After Primary Cryoablation. J Endourol 2016, 30, 632–637. [Google Scholar] [CrossRef] [PubMed]
- Pandolfo, S.D.; Loizzo, D.; Beksac, A.T.; Derweesh, I.; Celia, A.; Bianchi, L.; Elbich, J.; Costa, G.; Carbonara, U.; Lucarelli, G.; et al. Percutaneous thermal ablation for cT1 renal mass in solitary kidney: A multicenter trifecta comparative analysis versus robot-assisted partial nephrectomy. Eur J Surg Oncol 2023, 49, 486–490. [Google Scholar] [CrossRef] [PubMed]
- Patel, S.R.; Francois, S.; Bhamber, T.; Evans, H.; Gaston, K.; Riggs, S.B.; Teigland, C.; Clark, P.E.; Roy, O.P. Safety and effectiveness of percutaneous renal cryoablation with conscious sedation. Arab J Urol 2020, 18, 163–168. [Google Scholar] [CrossRef] [PubMed]
- Psutka, S.P.; Feldman, A.S.; McDougal, W.S.; McGovern, F.J.; Mueller, P.; Gervais, D.A. Long-term oncologic outcomes after radiofrequency ablation for T1 renal cell carcinoma. Eur Urol 2013, 63, 486–492. [Google Scholar] [CrossRef]
- Rembeyo, G.; Correas, J.M.; Jantzen, R.; Audenet, F.; Dariane, C.; Delavaud, C.; Mejean, A.; Timsit, M.O. Percutaneous Ablation Versus Robotic Partial Nephrectomy in the Treatment of cT1b Renal Tumors: Oncologic and Functional Outcomes of a Propensity Score-weighted Analysis. Clin Genitourin Cancer 2020, 18, 138–147. [Google Scholar] [CrossRef]
- Stern, J.M.; Svatek, R.; Park, S.; Hermann, M.; Lotan, Y.; Sagalowsky, A.I.; Cadeddu, J.A. Intermediate comparison of partial nephrectomy and radiofrequency ablation for clinical T1a renal tumours. BJU Int 2007, 100, 287–290. [Google Scholar] [CrossRef] [PubMed]
- Sundelin, M.O.; Lagerveld, B.; Ismail, M.; Keeley Fx, Jr.; Nielsen, T.K. Repeated Cryoablation as Treatment Modality After Failure of Primary Renal Cryoablation: A European Registry for Renal Cryoablation Multinational Analysis. J Endourol 2019, 33, 909–913. [Google Scholar] [CrossRef] [PubMed]
- Tracy, C.R.; Raman, J.D.; Donnally, C.; Trimmer, C.K.; Cadeddu, J.A. Durable oncologic outcomes after radiofrequency ablation: experience from treating 243 small renal masses over 7.5 years. Cancer 2010, 116, 3135–3142. [Google Scholar] [CrossRef]
- Yanagisawa, T.; Miki, J.; Shimizu, K.; Motohashi, K.; Enoki, K.; Egawa, S. Residue and recurrence in percutaneous cryoablation for cT1 renal tumor: Clinical utility and feasibility of salvage cryoablation with iodized oil marking. Int J Urol 2022, 29, 472–474. [Google Scholar] [CrossRef] [PubMed]
- Yang, B.; Autorino, R.; Remer, E.M.; Laydner, H.K.; Hillyer, S.; Altunrende, F.; White, M.A.; Khanna, R.; Stein, R.J.; Haber, G.-P.; et al. Probe ablation as salvage therapy for renal tumors in von Hippel-Lindau patients: The Cleveland Clinic experience with 3 years follow-up. Urologic Oncology: Seminars and Original Investigations 2013, 31, 686–692. [Google Scholar] [CrossRef]
- Zhou, J.; Wu, X.; Zhang, J.; Huang, J.; Chen, Y. Mid-to-long term oncologic and functional outcomes of zero ischemia laparoscopic microwave ablation-assisted tumor enucleation for renal cell carcinoma: a single-center experience. Transl Cancer Res 2021, 10, 2328–2336. [Google Scholar] [CrossRef] [PubMed]
- Campell, S.C.; Clark, P.E.; Chang, S.S.; et al. Renal Mass and Localized Renal Cancer: Evaluation, Management, and Follow-Up: AUA Guideline Part I. Journal of Urology 2021, 206, 199. [Google Scholar] [CrossRef] [PubMed]
- Sánchez-Martín, F.M.; Millán-Rodríguez, F.; Urdaneta-Pignalosa, G.; Rubio-Briones, J.; Villavicencio-Mavrich, H. Small renal masses: incidental diagnosis, clinical symptoms, and prognostic factors. Adv Urol 2008, 2008, 310694. [Google Scholar] [CrossRef]
- Kawamoto, S.; Solomon, S.B.; Bluemke, D.A.; Fishman, E.K. Computed tomography and magnetic resonance imaging appearance of renal neoplasms after radiofrequency ablation and cryoablation. Semin Ultrasound CT MR 2009, 30, 67–77. [Google Scholar] [CrossRef]
- Stewart, S.B.; Thompson, R.H.; Psutka, S.P.; Cheville, J.C.; Lohse, C.M.; Boorjian, S.A.; Leibovich, B.C. Evaluation of the National Comprehensive Cancer Network and American Urological Association renal cell carcinoma surveillance guidelines. J Clin Oncol 2014, 32, 4059–4065. [Google Scholar] [CrossRef] [PubMed]
- Iannuccilli, J.D.; Grand, D.J.; Dupuy, D.E.; Mayo-Smith, W.W. Percutaneous ablation for small renal masses-imaging follow-up. Semin Intervent Radiol 2014, 31, 50–63. [Google Scholar] [CrossRef]
- Javadi, S.; Ahrar, J.U.; Ninan, E.; Gupta, S.; Matin, S.F.; Ahrar, K. Characterization of contrast enhancement in the ablation zone immediately after radiofrequency ablation of renal tumors. J Vasc Interv Radiol 2010, 21, 690–695. [Google Scholar] [CrossRef]
- Breda, A.; Anterasian, C.; Belldegrun, A. Management and outcomes of tumor recurrence after focal ablation renal therapy. J Endourol 2010, 24, 749–752. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) flow chart.
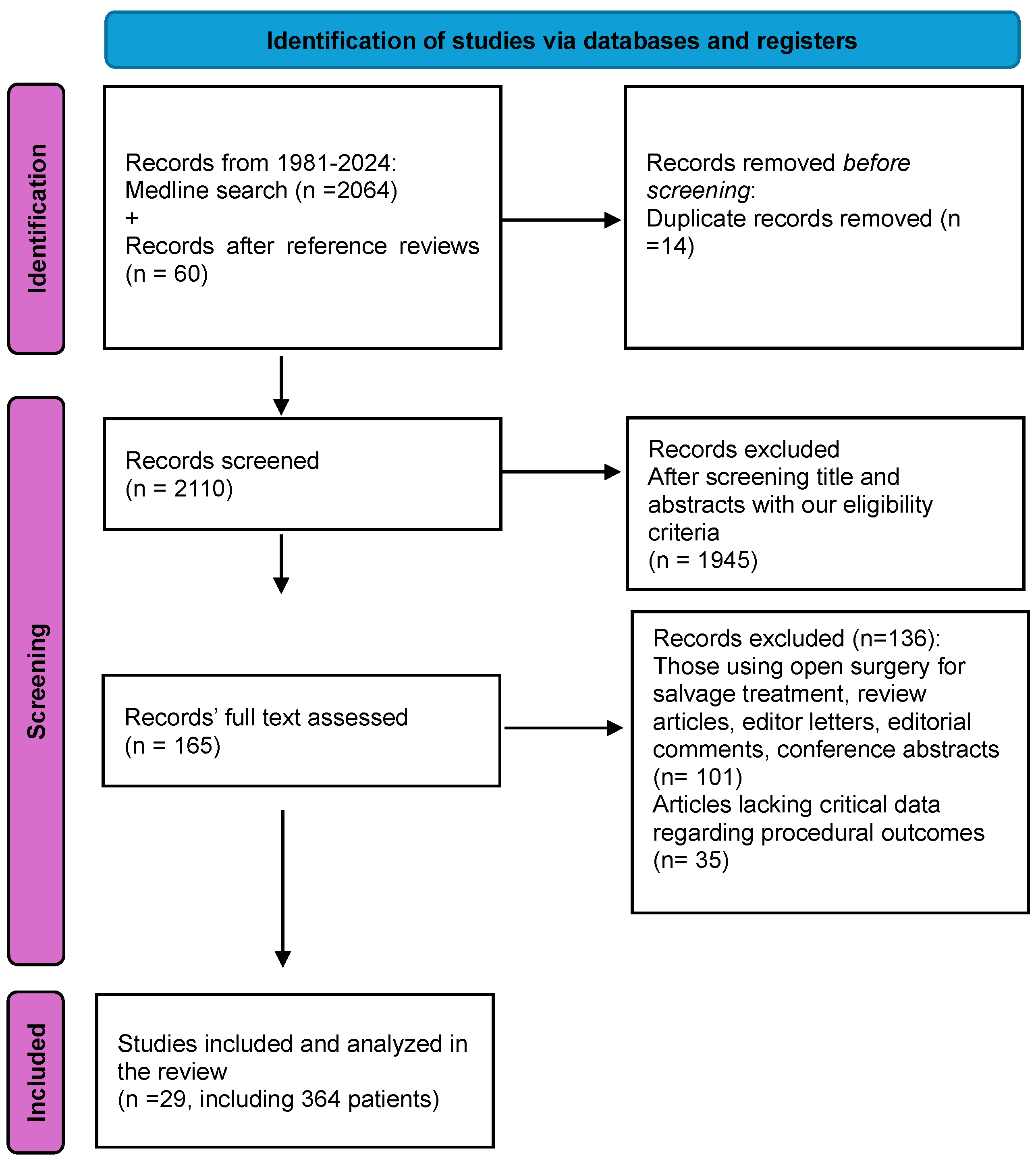

Table 1.
Summary of studies (n=29) addressing a minimally invasive approach for management of failures after primary ablation of small renal mass. Some of the studies presented multiple modalities. NED: No Evidence of Disease, RFA: Radiofrequency Ablation, CA: Cryoablation, Rec: Recurrence, PN: Partial nephrectomy, RN: Radical nephrectomy, L: Laparoscopic, R: Robotic, RCC: Renal cell carcinoma, ccRCC: Clear cell renal cell carcinoma, chRCC: Chromophobe renal cell carcinoma, pRCC: Papillary renal cell carcinoma, RO: Renal oncocytoma.
Table 1.
Summary of studies (n=29) addressing a minimally invasive approach for management of failures after primary ablation of small renal mass. Some of the studies presented multiple modalities. NED: No Evidence of Disease, RFA: Radiofrequency Ablation, CA: Cryoablation, Rec: Recurrence, PN: Partial nephrectomy, RN: Radical nephrectomy, L: Laparoscopic, R: Robotic, RCC: Renal cell carcinoma, ccRCC: Clear cell renal cell carcinoma, chRCC: Chromophobe renal cell carcinoma, pRCC: Papillary renal cell carcinoma, RO: Renal oncocytoma.
| Study |
Mean Age (year) |
Tumor Size (cm) |
Tumor histology |
Time to recurrence(month) |
Secondary treatment modality (no of cases) |
Outcome |
Follow up (Month) |
| Gupta et al. 2009 [1] | 55.5 | 2 | RCC | 5.5 | RFA (2) | 2 NED | 20.3 |
| Ferakis et al. 2010[2] | 62.3 | 4.46 | - | 32 | RFA (3) | NED | 58.66 |
| Liu et al. 2017[3] | - | > 4 | ccRCC | - | RFA (5) | 4 NED 1 Rec |
77 |
| Lorber et al. 2014[4] | - | 2.7 | 2 ccRCC 1 RCC |
86 | RFA (3) | NED | 65.6 |
| Matsumoto et al. 2005[5] |
 - - |
1 | RCC | < 6 | RFA (1) | Rec | 18 |
| Ji et al. 2016[6] | 72 | 3.2 |
ccRCC | 20 | RFA (1) | NED | 48 |
| Psutka et al. 2013[7] | - | < 7 | RCC | 30 | RFA (6) | 5 NED 1 Rec |
45 |
| Sternet et al. 2007[8] | - | < 4 | ccRCC | 18 | RFA (1) | NED | 12 |
| Long et al. 2017[9] | - | - | RCC | 13.1 | RFA (13) CA (2) |
14 NED 1 Rec |
38 |
| Tracy et al. 2010[10] | - | - | RCC | 9.66 | RFA (2) CA (1) |
2 NED 1 Rec |
- |
| Caputo et al. 2017[11] | - | - | - | - | CA (2) | 1 NED 1 Rec |
30.1 |
| Emara et al. 2014[12] | - | - | - | CA (2) | NED | 31.3 | |
| Murray et al. 2019[13] | - | < 4 | 5 RCC 1 RO |
- | CA (6) | 5 NED 1 Rec |
53 |
| Okhunov et al. 2016[14] | 64.8 | 2.4 | 14 ccRCC 3 pRCC 4 chRCC |
32 | CA (20) | 17 NED 3 Rec |
30 |
| Patel et al. 2020[15] | 74 | < 4 | - | - | CA (5) | NED | 42.7 |
| Yanagisawa et al 2022[16] | 74 | < 7 | 20 ccRCC 2 pRCC |
- | CA (22) | 20 NED 2 Rec |
33 |
| Rembey et al. 2020[17] | - | - | - | 13 | CA (6) | NED | 29 |
| Sundelin et.al 2019[18] | 66.5 | 3 | 55 ccRCC 5 pRCC 7 chRCC 5 not specified |
11.44 | CA (72) | 31 NED 38 Rec 3 Lost in F/U |
23 |
| Breen et al. 2013 [19] | 67 | - | RCC | 12 | Ablation (1) | NED | 18 |
| Pandolfo et al. 2023[20] | - | - | - | - | Ablation (8) | NED | 45 |
| Yang et al. 2013[21] | - | 3.36 | RCC | 12.33 | Ablation (3) | NED | 70.6 |
| Attawettayanon et al. 2024[22] | 64.8 | 2.3 | - | 28 | Ablation (12) | 7 NED 5 Rec |
53 |
| RN (2) | Unknown | ||||||
| Loloi et al. 2020[23] | - | 3.1 | 51 ccRCC 13 pRCC 2 chRCC 3 Benign 8 non-diagnostics |
13.7 | Ablation (50) | 38 NED 12 Rec |
28 |
| - | PN (5) RN (8) |
Unknown | |||||
| Long et al. 2017[9] | - | - | RCC | 13.1 | PN (1) RN (2)) |
NED | 38 |
| Patel et al. 2020[15] | 74 | < 4 | - | - | PN (1) RN (3) |
NED | 42.7 |
| Rembey et al. 2020[17] | - | - | - | 13 | RPN (1) RRN (2) |
NED | 29 |
| Duffey et al 2012[24] | - | - | RCC | 24.5 | RPN (2) LRN (1) |
1 P.N NED 2 Unknown |
70 |
| Martini et al 2021[25] | 78 | < 4 | RCC | 26 | RPN (35) | NED | 43 |
| Feng et al 2024[26] | 59 | 2.5 | RCC | - | RPN (1) | NED | 24 |
| Ferakis et al. 2010[2] | 58 | 5.1 | pRCC | 12 | RN (1) | NED | 78 |
| Gupta et al. 2009 [1] | 58 | 2.65 | ccRCC | 16.5 | RN (2) | NED | 20.3 |
|
Zhou et al. 2021[27] |
74 | 3.4 | RCC | <24 | RN (2) | NED | 9.5 |
| Caputo et al. 2017[11] | - | - | - | - | LRN (1) | NED | 30.1 |
| Lorber et al. 2014[4] | - | 4 | ccRCC | 42 | LRN (1) | NED | 65.6 |
| Yanagisawa et al 2022[16] | 74 | <7 | - | - | RRN (1) | Unknown | 33 |
| Chang et al 2015[28] | - | - | RCC | - | LRN (2) | NED | 67.6 |
| Sternet et al. 2007[8] | - | < 4 | ccRCC | 24 | LRN (1) | NED | 12 |
| Klatte et al 2011[29] | - | 2.5 | ccRCC | 14 | LRN (4) | NED | - |
| Ji et al. 2016[6] | 58.5 | 3.5 | ccRCC | 15 | LRN (2) | 1 NED 1 Death |
78 |
| Tracy et al. 2010[10] | - | - | RCC | 12 | LRN (1) | NED | 36 |
Table 2.
The primary ablative therapy approaches for the management of small renal mass in 364 patients who experienced recurrence during follow up period. CA: Cryoablation, RFA: Radiofrequency ablation, MWA: Microwave ablation, HIFU: High-intensity focused ultrasound
Table 2.
The primary ablative therapy approaches for the management of small renal mass in 364 patients who experienced recurrence during follow up period. CA: Cryoablation, RFA: Radiofrequency ablation, MWA: Microwave ablation, HIFU: High-intensity focused ultrasound
| Primary Ablation Approach | Number (%) of patients |
| CA | 198 (54.3%) |
| RFA | 123 (33.7%) |
| HIFU | 19 (5%) |
| MVA | 2(0.5%) |
| Not specified | 23(6%) |
| Total | 364 |
Table 3.
Secondary treatment modalities for management of failures after primary ablation of small renal mass in 364 patients. CA: Cryoablation, RFA: Radiofrequency ablation.
Table 3.
Secondary treatment modalities for management of failures after primary ablation of small renal mass in 364 patients. CA: Cryoablation, RFA: Radiofrequency ablation.
| Secondary treatment | Number (%) Of Cases | |
| Re-ablation | 249 (68.4%) | RFA: 37 (14.9%) CA:138 (55.4%) Not specified: 74 (29.7%) |
| Laparoscopic/ Robotic partial or radical nephrectomy | 82 (22.5%) | Partial Nephrectomy: 46 (56.1%) Radical Nephrectomy: 36 (43.9%) |
| Active Surveillance | 33 (9%) | |
| Total | 364 | |
Table 4.
Outcomes of various secondary treatment modalities for management of tumor recurrence after primary ablation (n=364). NED: No Evidence of Disease, CA: Cryoablation, RFA: Radiofrequency ablation.
Table 4.
Outcomes of various secondary treatment modalities for management of tumor recurrence after primary ablation (n=364). NED: No Evidence of Disease, CA: Cryoablation, RFA: Radiofrequency ablation.
| Re-ablation n=249 | |
| RFA | NED: 33 Recurrence: 4 |
| CA | NED: 89 Recurrence: 46 Unknown:3 |
| Not specified | NED: 57 Recurrence: 17 |
| Total | NED: 179 (71.9%) Recurrence: 67 (26.9%) Unknown: 3 |
| Laparoscopic/ robotic partial or radical nephrectomy n=82 | |
| Robotic partial nephrectomy (n=46) | NED:40 Unknown :6 |
| Robotic/ laparoscopic radical nephrectomy (n=36) | NED:23 Recurrence: 1 Unknown: 12 |
| Total | NED: 63 Recurrence: 1 Unknown: 18 |
| Active surveillance n=33 | |
| Surveillance | Surgery: 4 Death: 4 Surveillance: 25 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



