Submitted:
11 January 2025
Posted:
14 January 2025
You are already at the latest version
Abstract
Perinatal parvoviral infection in puppies leads to necrotizing myocarditis, resulting in either high mortality or gradual heart damage. We believe that canine parvovirus 2 (CPV-2) myocardial infection is not being fully recognized as a cause of myocarditis, cardiac injury, and fibrosis repair in young dogs, despite the significant reduction in the epidemic of canine parvoviral myocarditis due to extensive vaccination. This study analyzed formalin-fixed, paraffin-embedded tissues obtained from 40 canine cases aged less than two years, spanning the period from 2019 to 2021. The objective was to test for the presence of CPV 2. Cardiac necrosis, inflammation, or fibrosis were observed in the diagnosed cases, but the age-matched controls did not have any cardiac abnormalities and tested positive for CPV. The presence of myocardial CPV-2 was detected in young dogs with mild myocarditis, suggesting that the period of vulnerability to myocarditis in the heart may be greater than what has been previously documented. CPV-2 was found in dogs who had extensive myocardial fibrosis, indicating that CPV-2 had caused previous injury to the heart muscle. Although vaccinations are common, these findings indicate that CPV-2 continues to be a major contributor to cardiac injury in dogs.
Keywords:
1. Introduction
2. Materials and Methods
3. Results
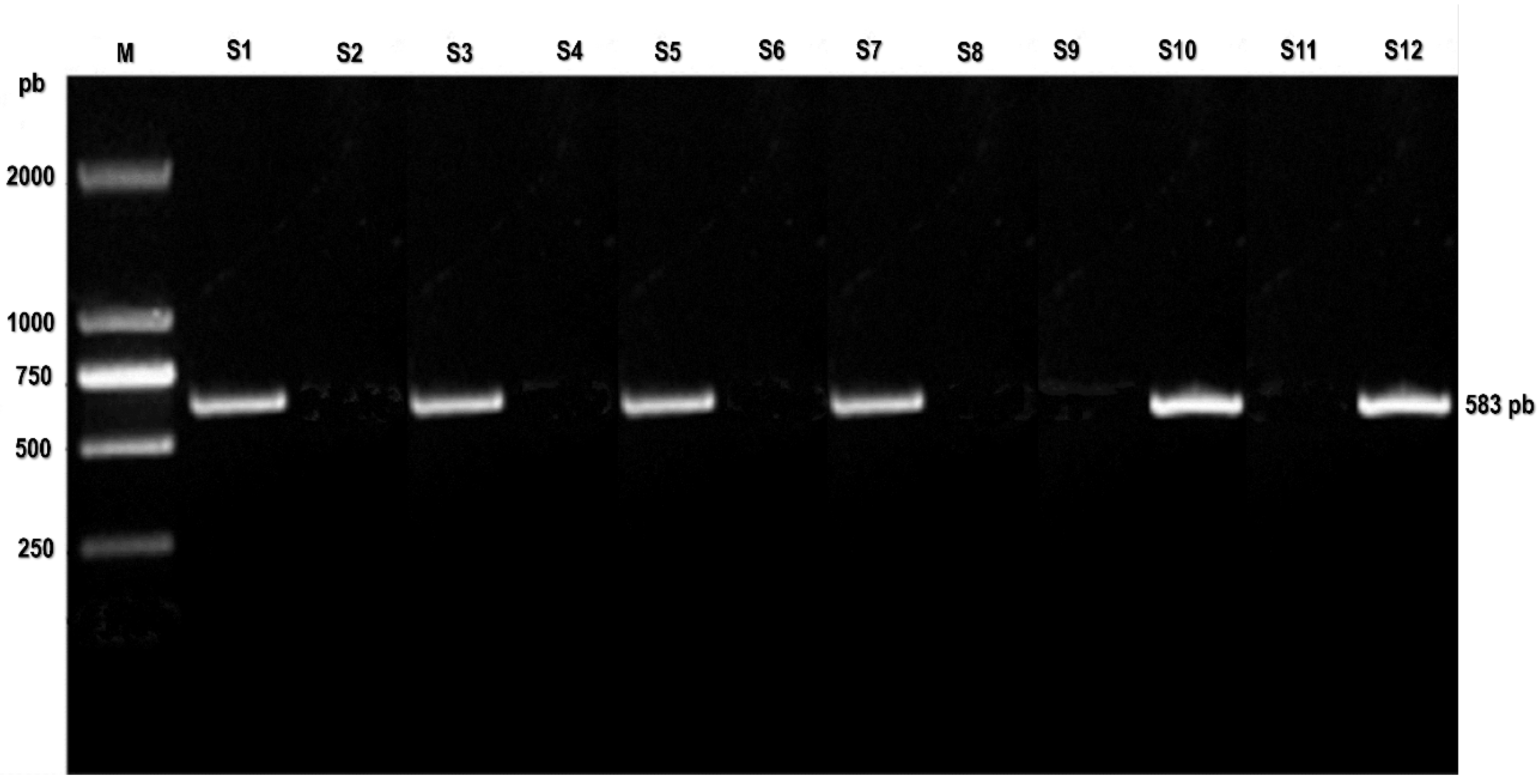
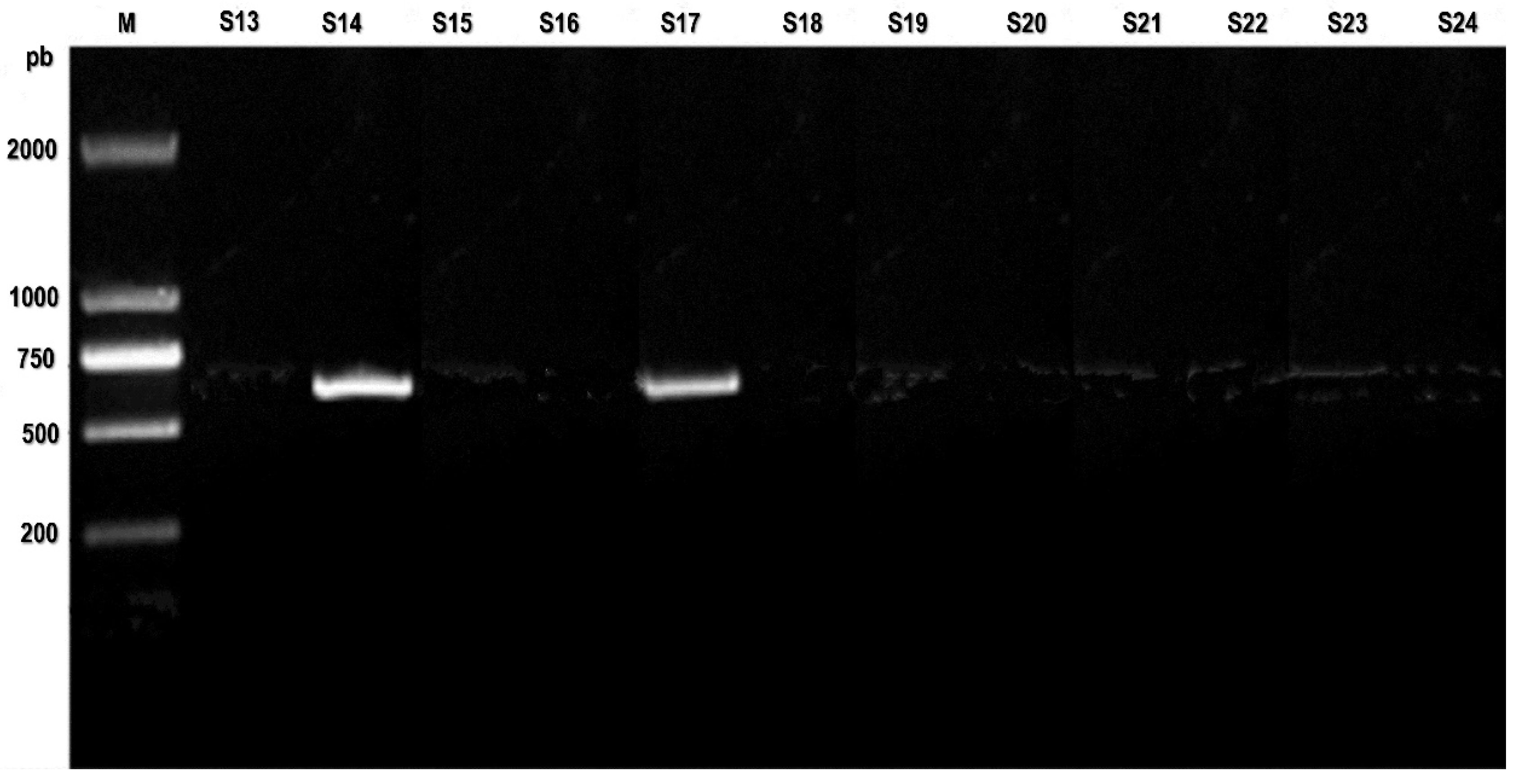
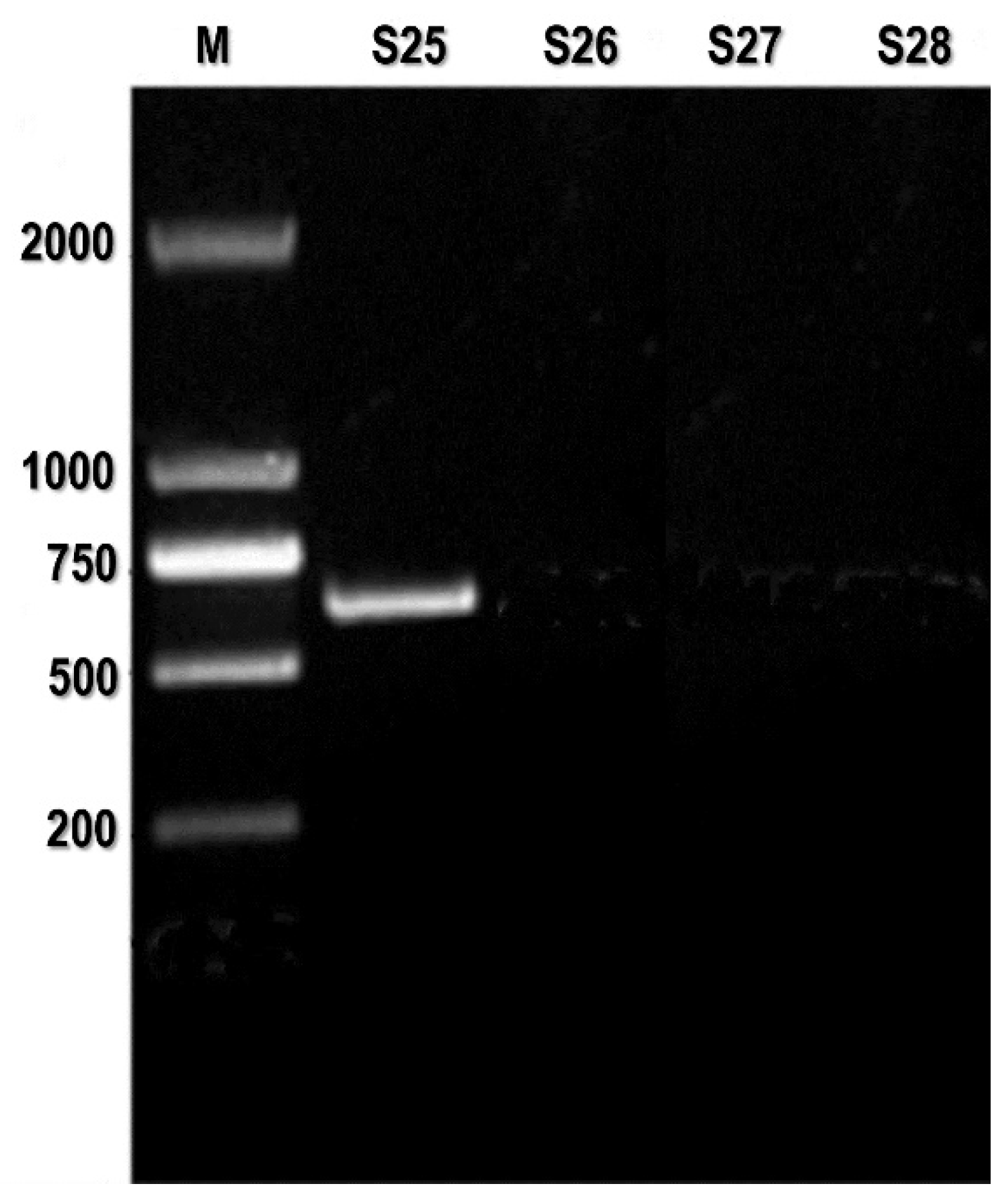
3.1. PCR
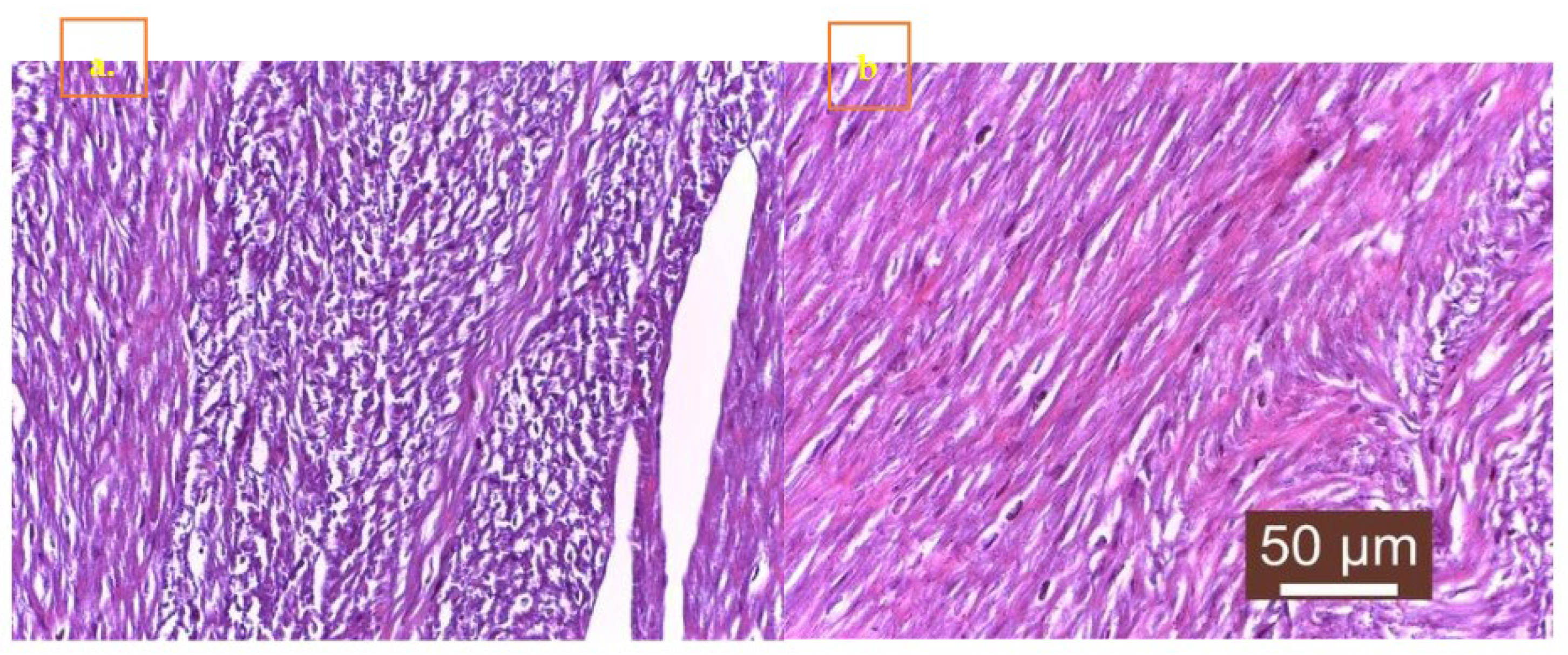
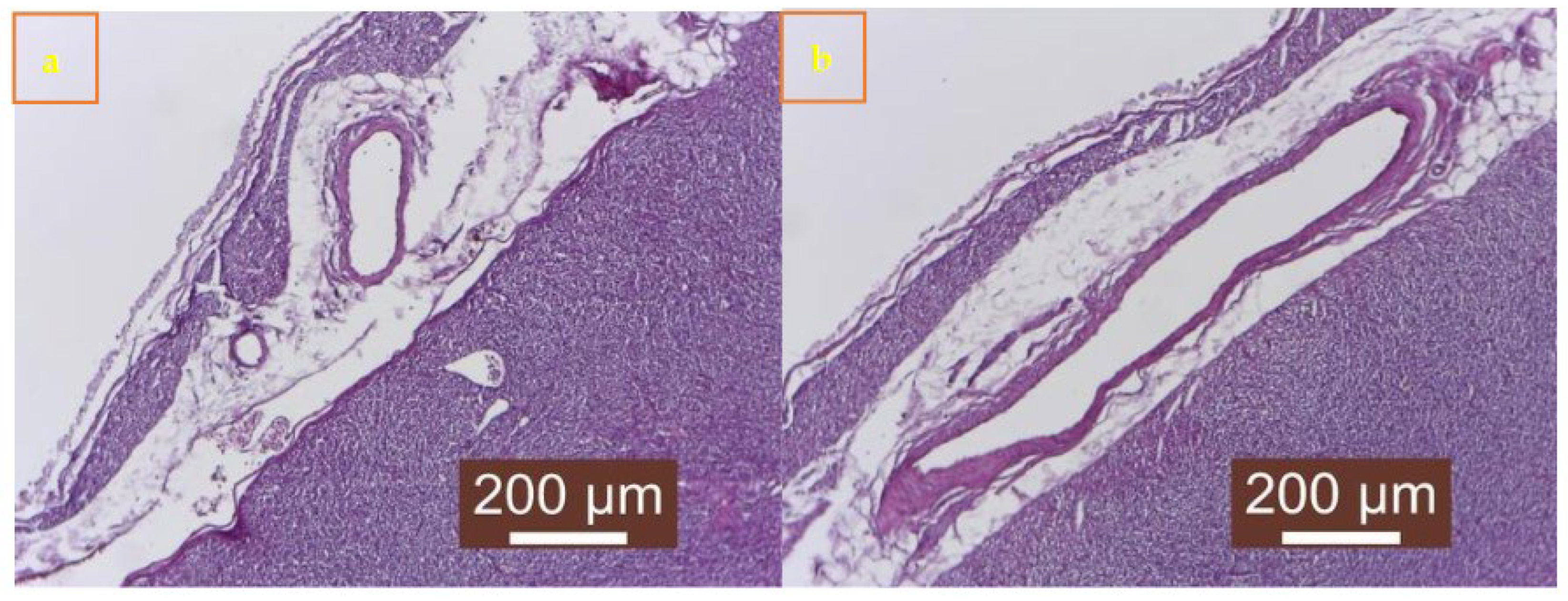
3.2. Histopathologic Findings
4. Discussions
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ford J, McEndaffer L, Renshaw R, Molesan A, Kelly K. Parvovirus Infection Is Associated with Myocarditis and Myocardial Fibrosis in Young Dogs. Vet Pathol. 2017; 54(6), 964-971. [CrossRef]
- Dines B, Kellihan H, Allen C, Loynachan A, Bochsler P and Newbury S. Case report: Long-term survival in puppies assessed with echocardiography, electrocardiography and cardiac troponin I after acute death in littermates due to parvoviral myocarditis. Front. Vet. Sci. 2023, 10:1229756. [CrossRef]
- Horecka, K.; Porter, S.; Amirian, E.S.; Jefferson, E. A Decade of Treatment of Canine Parvovirus in an Animal Shelter: A Retrospective Study. Animals 2020, 10, 939. [CrossRef]
- Mylonakis, M.; Kalli, I.; Rallis, T. Canine parvoviral enteritis: An update on the clinical diagnosis, treatment, and prevention. Vet. Med. Res. Rep. 2016, 7, 91–100.
- Khatri, R.; Poonam, M.H.; Minakshi, P.C. Epidemiology, Pathogenesis, Diagnosis and Treatment of Canine Parvovirus Disease in Dogs: A Mini Review. J. Veter-Sci. Med Diagn. 2017, 6, 06.
- Behdenna A, Lembo T, Calatayud O, et al. Transmission ecology of canine parvovirus in a multi-host, multi-pathogen system. Proc Biol Sci. 2019, 286(1899):20182772. [CrossRef]
- Decaro, N.; Buonavoglia, C.; Barrs, V.R. Canine parvovirus vaccination and immunisation failures: Are we far from disease eradication? Vet. Microbiol. 2020, 247, 108760.
- Eregowda CG, De UK, Singh M, et al. Assessment of certain biomarkers for predicting survival in response to treatment in dogs naturally infected with canine parvovirus. Microb Pathog. 2020, 149:104485.
- Jager, M.C., Tomlinson, J.E., Lopez-Astacio, R.A. et al. Small but mighty: old and new parvoviruses of veterinary significance. Virol J 18, 210 (2021). [CrossRef]
- Gallinella G. New insights into parvovirus research. Viruses. 2019, 11(11):1053.
- Dik, I.; Mustafa Emin, O.Z.; Avci, O.; Simsek, A. Determination of Canine Parvovirus Variants in Puppies by Molecular and Phylogenetic Analysis. Pak. Vet. J. 2022, 42, 171.
- Hao, X.; Li, Y.; Xiao, X.; Chen, B.; Zhou, P.; Li, S. The Changes in Canine Parvovirus Variants over the Years. Int. J. Mol. Sci. 2022, 23, 11540. [CrossRef]
- Hao, X.; He, Y.; Wang, C.; Xiao, W.; Liu, R.; Xiao, X.; Zhou, P.; Li, S. The increasing prevalence of CPV-2c in domestic dogs in China. PeerJ 2020, 8, e9869.
- Qi, S.; Zhao, J.; Guo, D.; Sun, D. A Mini-Review on the Epidemiology of Canine Parvovirus in China. Front. Vet. Sci. 2020, 7, 5.
- Temizkan, M.C.; Sevinc Temizkan, S. Canine Parvovirus in Turkey: First Whole-Genome Sequences, Strain Distribution, and Prevalence. Viruses 2023, 15, 957. [CrossRef]
- Zhuang, Q.Y.; Qiu, Y.; Pan, Z.H.; Wang, S.C.; Wang, B.; Wu, W.K.; Yu, J.M.; Yi, Y.; Sun, F.L.; Wang, K.C. Genome sequence characterization of canine parvoviruses prevalent in the Sichuan province of China. Transbound. Emerg. Dis. 2019, 66, 897–907. [CrossRef]
- Hoang, M.; Wu, H.Y.; Lien, Y.X.; Chiou, M.T.; Lin, C.N. A SimpleProbe((R)) real-time PCR assay for differentiating the canine parvovirus type 2 genotype. J. Clin. Lab. Anal. 2019, 33, e22654.
- Schirò G, Mira F, Decaro N, et al. Persistence of DNA from canine parvovirus modified-live virus in canine tissues. Vet Res Commun. 2023, 47(2):567-574. [CrossRef]
- Mokhtari, Azam, Farmani, Naghmeh, & Rajabi, Milad. Detection of Canine Parvovirus by PCR and its association with some of risk factors. Revista MVZ Córdoba. 2018, 23(2), 6607-6616.
- Navarro C, Detection of Canine Parvovirus in Dogs by Means Polymerase Chain Reaction. 2020 - 7(6). AJBSR.
- Latimer HB. Variability in body and organ weights in the newborn dog and cat compared with that in the adult. Anat Rec. 1967, 157:449– 56. [CrossRef]
- Sime TA, Powell LL, Schildt JC, Olson EJ. Parvoviral myocarditis in a 5-week-old Dachshund: parvoviral myocarditis in a puppy. J Vet Emerg Crit Care. 2015, 25:765–9.
- Reichart D, Magnussen C, Zeller T, Blankenberg S. Dilated cardiomyopathy: from epidemiologic to genetic phenotypes. J Intern Med. 2019, 286:362–72.
- Doyle E. Canine parvovirus and other canine enteropathogens. In:Lila M, Janeczko S, Hurley KF, editors. Infectious Disease Management in Animal Shelters, 2nd ed. Hoboken, NJ: Wiley-Blackwell, 2021, p. 321–36.
- Spindel, M.E.; Krecic, M.R.; Slater, M.R.; Vigil, N. Evaluation of a Community’s Risk for Canine Parvovirus and Distemper Using Antibody Testing and GIS Mapping of Animal Shelter Intakes. J. Appl. Anim. Welf. Sci. 2018, 00, 1–13. [CrossRef]
- Langhorn R, Willesen JL. Cardiac troponins in dogs and cats. J Vet Intern Med. 2016, 30:36–50.
- Lakhdhir S, Viall A, Alloway E, Keene B, Baumgartner K, Ward J. Clinical presentation, cardiovascular findings, etiology, and outcome of myocarditis in dogs: 64 cases with presumptive antemortem diagnosis (26 confirmed postmortem) and 137 cases with postmortem diagnosis only (2004–2017). J Vet Cardiol. 2020, 30:44–56.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).



