
Submitted:
09 January 2025
Posted:
10 January 2025
You are already at the latest version
Abstract
Cancer pain is a common issue for patients, especially in advanced cancer stages and significantly affects quality of life (QoL), treatment tolerance, and overall treatment outcomes. Pain can arise from primary tumors, metastases, and as a result treatments like radiotherapy (RT). Effective pain management is crucial, especially with RT being a key method for alleviating cancer pain, particularly in cases of bone and soft tissue metastases. RT provides relief for 60-80% of patients by reducing tumor size and mitigating associated pain. Radiotherapy can also induce pain, especially radiation-induced neuropathic pain, which may require further treatment. Despite these potential side effects, RT remains an essential tool in managing cancer pain, though careful management of its toxicities is necessary to improve patient QoL and survival.
Keywords:
Pain
; neuropathic pain
; radiotherapy
; bone metastases
1. Introduction
Most cancer patients experience pain as part of their illness, especially those with advanced cancer where the goal of treatment is not complete recovery, but providing relief from symptoms, including pain. Cancer pain may be a result of a developing primary tumor or metastases in the lymph nodes, but predominately it occurs in patients experiencing distant metastases, particularly in the skeletal system [1]. It has long been established that pain has a negative impact on quality of life (QoL), decreases tolerance of treatment and can also affect treatment compliance [2]. The latter substantially influences the treatment results and the patients’ outcomes [3]. Moreover, cancer pain may appear during or after oncological therapy, including radiotherapy (RT). Therefore, appropriate pain management plays an important role in the overall outcome of anticancer therapy with regard to patient treatment tolerance and their QoL [4].
2. Radiotherapy as a Mainstream Procedure for the Treatment of Cancer Pain
Three main RT techniques are used for the management of cancer pain: Teleradiotherapy (or external beam radiation therapy, EBRT) is the most commonly used irradiation technique in oncological treatment. In EBRT the radiation source is placed at a certain distance from the tumor, and the patient, lying in a predetermined position, is exposed to a beam of ionizing radiation (either photon or electron) generated by a therapeutic device - a medical linear accelerator. The irradiation area includes not only the tumor, but also an appropriate margin of surrounding tissues due to the possibility of cancerous cells existing around the tumor that has been visualized in imaging studies (computed tomography, magnetic resonance imaging). A patient who is to undergo EBRT is prepared by selecting the appropriate immobilization and conducting a localization computed tomography scan to define the exact irradiation targets. Additionally, important points are marked on the patient’s skin, which are essential for reproducing the planned irradiation field [5].
- Brachytherapy (BRT) is a form of localized RT used to treat various types of cancer, which involves placing a radioactive source directly inside or very close to the tumor. This allows for high doses of radiation to be delivered directly to the cancerous tissue simultaneously minimizing radiation exposure to surrounding healthy tissues. The localized radiation can help shrink tumors, alleviate obstruction, and reduce inflammation, which can lead to significant pain relief [6]. This technique is particularly effective in cases where cancer causes localized pain due to soft tissue masses, for instance in head and neck cancers, prostate cancers, gynecological malignancies [7]. Sometimes BRT is used to treat painful bone metastases, particularly in areas like the spine, pelvis or other bones where radiation can be delivered precisely [8]. In cancers of the gastrointestinal tract, urinary tract, or reproductive organs, BRT can be used to treat obstruction-related pain, especially when tumors are pressing on other organs or nerves. Various radioactive isotopes are used in BRT, such as iridium-192 (192Ir), cesium-137 (137Cs), cobalt-60 (60Co), radium-226 (226Ra), or yttrium-90 (90Y), which are placed in close proximity to the tumor for a strictly defined period of time. The various types of BRT are described in Table 1.
Brachytherapy is considered an invasive radiotherapy technique and often requires collaboration with an anesthesiologist and a nursing assistant to monitor that the patient is appropriately anesthetized. During brachytherapy, a relatively high dose of radiation is delivered to a small volume of tissue surrounding the radiation source applicators, and the treatment effects experienced by the patient typically occur within a few days [14,15]. The main limitations of BRT are that its use is restricted to managing localized pain and tumors that are accessible for radiation delivery, thus BRT is a rarely used treatment option for painful bone metastases.
- 2.
- The mechanism of action in radioisotope therapy is radiation-induced destruction of cells, which is a technique that differs slightly from that of RT. In radioisotope therapy, the most commonly used elements are strontium-89 (89Sr), samarium-153 (153Sm), phosphorus-32 (32P), radium-223 and (alpharadium) [16,17,18], as described in Table 2. The most widely used strontium isotope is an analog of calcium and selectively accumulates in metastatic lesions in the bones [19,20]. The therapeutic action is based on the emission of beta radiation, which destroys cancer cells with minimal damage to the surrounding healthy tissues [21]. The most common indication for the use of radioactive strontium isotopes is multiple, painful bone metastases that cannot be irradiated with external sources (teletherapy) due to their extensive distribution. The effects of isotopic therapy last from 3 to 12 months, and the onset of action may not become apparent until several weeks after the treatment. Occasionally, before the therapeutic effect occurs, there may be a transient increase in pain symptoms, in which case the patient may require a temporary increase in analgesic doses [22,23]. Isotope treatment can be used in combination with RT, provided there is an appropriate time interval after prior monitoring of blood morphological parameters.
In RT, the probability of destroying all cancer cells increases as the number of target cells decreases. However, in RPT, fewer cells do not result in a higher tumor control probability because the radiation is not uniformly delivered. If the radiation comes from a radionuclide on the tumor cell surface, fewer cells mean less energy is deposited into the targeted cells. This is partly offset by higher concentrations in smaller cell clusters compared to larger tumors.
3. The Molecular Mechanism of Radiotherapy
The fundamental physical cellular process in RT is ionization, along with the phenomenon of water radiolysis and the formation of hydroxyl free radicals, which trigger a series of biological and chemical consequences in the irradiated cell. The cytotoxic, anti-inflammatory, and anti-edema effects of RT lead to a reduction in tumor size and swelling around the tumor, thereby alleviating pressure on nearby structures of the nervous system and decreasing cancer infiltration into affected tissue structures, which contributes to a reduction in the severity of cancer pain [37]. Radiotherapy also exerts a hemostatic effect by obliterating small venous and arterial vessels within the tumor. Moreover, RT can directly affect pain receptors (e.g., nerves), changing their sensitivity or reducing their activity [38].
The molecular effect of RT is a complex reaction which is supported by several mechanisms, which are shown in Figure 1. Firstly, RT by induction of apoptosis and necrosis in tumor cells inhibits inflammatory mediators within the tumor and surrounding tissues. After sustaining damage, tumor cells decrease the release of cytokines such as TNF-alpha, IL-1, IL-6 and other mediators that sensitize pain receptors [39,40]. Secondly, ionizing radiation can directly affect nerve endings and alter their sensitivity by inducing changes in ion channel activity (such as the TRPV1 receptor) on sensory neurons, reducing their ability to transmit pain signals [41]. Thirdly, RT modifies the tumor microenvironment by reducing tumor volume, which in turn decreases mechanical pressure on adjacent tissues, nerves, and blood vessels. Additionally, radiation-induced changes in blood flow and oxygenation in the tumor can result in reduced metabolic by-products that may irritate pain receptors [42]. Fourthly, RT can activate the body’s natural pain-relieving mechanisms through release of endorphins and other endogenous opioids in reaction to cellular stress and damage caused by radiation. Fifthly, RT modulates the local tumor immune response, leading to anti-inflammatory effects. Immune cells that infiltrate the tumor in response to radiation can release factors that not only target cancer cells, but also reduce pain-inducing inflammation [43,44].
In addition, it has been demonstrated that RT reduces the activity of the cyclic adenosine monophosphate-protein kinase A (cAMP-PKA) signaling pathway, which is involved in both inflammatory pain and neuropathic pain [45,46]. The proinflammatory cytokines (such as TNF-α and IL-1β are activated and released from the astrocytes and microglial cells) are activators of the cAMP-PKA pathway in primary afferent neurons [47]. Preliminary results in rat models suggest that RT may suppress bone cancer pain through inhibition of abnormal activation of the cAMP-PKA signaling pathway, suggesting a new mechanism for the RT of bone cancer pain [48]. Finally, it is worth adding that RT affects the level of mineralization and bone density recalcification, which is associated with relief from bone cancer pain [49,50].
4. Radiotherapy as a Painkiller
Radiotherapy is the mainstage treatment for alleviating cancer pain [51]. Pain relief after RT may be achieved as many as 60–80% of patients [52]. The ionizing radiation can reduce the tumor or cancerous tissue infiltrates, which can ultimately contribute to a decrease in the intensity of perceived pain [53]. Radiotherapy is an effective pain management procedure. The most common clinical indications for the use of RT in alleviating cancer pain include: bone metastases, especially in the spine where there is a risk of spinal cord compression syndrome, brain metastases, painful cancer infiltrates in soft tissues, and cancerous obstruction of the pancreas and esophagus, which hinders painless swallowing [54,55]. Indications for RT also include superior vena cava syndrome and tumors blocking the airways, which make breathing difficult and may cause dyspnea, either with accompanying pain or occurring without pain [56,57].
There are specific clinical situations, such as superior vena cava syndrome, that require rapid improvement in the overall clinical condition of the patient, where the immediate (within 48-72 hours) implementation of RT in the mediastinal area as initial treatment (e.g., in patients with non-small cell lung cancer) allows for effective reduction of the tumor mass in the mediastinum, thereby alleviating symptoms of dyspnea, chest pressure or pain [58]. The radiation protocol typically used for this indication involves administering a total dose of, for example, 20 Gy in 5 fractional doses or 30 Gy in 10 fractional doses. After a break of 3 to 4 weeks from irradiation, the response to treatment is assessed. If tumor regression occurs, there is the possibility of re-irradiation according to the previously mentioned scheme or radicalizing the treatment by decreasing the fractional doses and increasing the total dose [59,60].
A clinical situation that requires RT are brain metastases (BrM), which affect about one-third of cancer patients and are most commonly seen in the course of small cell lung cancer, breast cancer, melanoma, kidney cancer or rectal cancer [61,62]. Brain metastases are accompanied by swelling of the surrounding brain tissue, causing symptoms such as diffuse headaches, nausea, vomiting, weakness, or other neurological symptoms, and significantly worsen the patient’s survival prognosis [63,64]. In the case of a single BrM, especially when the primary lesion is controlled, surgical removal of the tumor can be considered, followed by irradiation, or treatment with stereotactic RT, which involves delivering single, high doses of ionizing radiation to a small volume of the tumor [65,66]. In the case of multiple BrM, when control of the primary cancer is not possible, whole brain radiotherapy (WBRT) is used in 5 or 10 fractions, depending on the patient’s overall condition, the type of cancer, and the further treatment planned [67,68]. Radiotherapy, for which the blood-brain barrier is not an obstacle, easily reaches the targeted areas of the brain, leading to a reduction in the volume of tumor lesions and peritumoral edema, thus resulting in a de-escalation of the symptoms experienced by the patient.
4.1. Radiotherapy as a Mainstage Procedure in Painful Metastatic Bone Cancer
Bone metastases (BoM) are associated with very advanced cancer and occur in approximately 60% of cancer patients [69,70]. They most commonly affect patients with advanced breast, prostate, lung, kidney, or thyroid cancer [71,72]. The most serious complication of BoM is that of pathological fractures, which can lead to nerve damage, vascular injury, loss of joint stability, and even compression of nerves or the spinal cord in cases of metastatic lesions located in the spine.
Tests confirming the presence of BoM include X-rays, computed tomography, bone scintigraphy, magnetic resonance imaging, and PET scans and other new molecular and hybrid imaging methods, including SPECT/CT, PET/CT, and whole-body MRI [73].
The most common sites for BoM include the thoracic spine, lumbar spine, sacrum, cervical spine, pelvis, ribs, and the humerus and femur [74]. Osteolytic BoM are associated with the destruction of trabecular and cortical bone due to the occlusion of medullary blood vessels by stimulated osteoclasts and are found in breast cancer, non-small cell lung cancer, thyroid cancer, and kidney cancer [75,76]. Osteoblastic BoM, which involve the overproduction of hard, brittle bone, typically occur in small cell lung cancer, prostate cancer, or breast cancer [77].
The most frequent symptom in patients with BoM is pain, reported by more than two-thirds of patients. This pain is more frequently associated with metastases to the spine, pelvis, or ribs than with long bones. It is often described as burning, stabbing, dull, nagging, or tearing. The pain intensifies during movement, physical activity, coughing, or sneezing. Notably, its intensity is lower or absent in the morning and increases throughout the day, peaking in the afternoon and evening, depending on the level of activity. Rest usually provides relief. In cases of BoM to the vertebral bodies, pain occurs while sitting or standing and subsides or decreases when lying down. However, if there is compression of the spinal cord, the pain sharply increases to severe levels when lying down, prompting patients to sleep in a semi-reclined or sitting position [78]. In patients with rib metastases, the pain worsens with deep breathing, and they tend to lie on the side affected by the metastases to immobilize the ribs during respiration.
Between 20 and 40% of cancer patients experience neuropathic pain which is associated with higher pain intensity, poorer quality of life, and higher intake of analgesics [79,80]. Neuropathic mechanisms play an important role in the pathophysiology of cancer-induced bone pain and may cause metastatic bone pain refractory to standard pain treatments. Up to one third of patients with bone metastases may suffer from neuropathic pain, which may be successfully treated with RT [81,82,83]. In many cases, patients with BoM live for many years, depending on the type of cancer, the number and volume of metastases, not only in the skeletal system but also in solid organs, the effectiveness of previous cancer treatments, the overall health of the patient, and the control of comorbidities [84].
One of the most effective methods for treating BoM is RT, which involves irradiating the selected metastatic focus. Radiotherapy is used in cases of:
- bone pain resulting from the presence of metastatic lesions, e.g., in the spine
- osteolytic metastases with significant bone loss that threaten fractures
- conditions following pathological bone fractures
Radiation induced pain relief in bone metastases is achieved by many mechanisms, which may include: ossification, diminishing osteoclast activity in the bone microenvironment, and killing cancer cells along with a reduction in osteolysis. After RT, partial pain relief is achieved in 50-80% of patients, with complete relief observed in about 30% of patients [87,88]. Typically, single, double, or five-fraction external beam irradiation is administered over one or two weeks. The effectiveness of these methods is comparable in terms of pain relief [89,90]. For the convenience of patients and their caregivers, single-dose radiotherapy is preferred for painful uncomplicated BoM, although there is often a need for re-irradiation [91]. The decision regarding the individual treatment plan is made by the radiation oncologist, taking into account the type of cancer, the overall health of the patient, the predicted survival time, the presence of metastases in other locations, the feasibility of multiple visits to the radiotherapy center, and the patient’s preferences. Multi-fraction irradiation schemes (short course radiation therapy, for example: 10 × 3 Gy or 5 × 4 Gy) are usually proposed for patients in better overall condition with a longer expected survival, after orthopedic surgical procedures, and in cases of spinal cord compression syndrome [92]. Patients with numerous painful BoM in worse overall health typically undergo single irradiation of the metastatic foci, but with a higher fractional dose (mostly 1x 8 Gy) [93]. Pain control persisting 3–6 months after RT is experienced by 35% of patients. In some patients, re-irradiation can be considered to prolong the pain relief effect after several weeks from the initial irradiation [94,95]. A limitation of the present review is that non-uniform primary end-points have been used in different studies (Table 3). Moreover, in the case of patients with neuropathic pain multi-fraction irradiation schedules may be preferred to a single fraction, as this leads to longer durability of pain control with a higher remineralization rate of the irradiated vertebrae [96,97]. Furthermore, in patients with low risk asymptomatic bone metastasis without gross osteolytic changes, especially female patients with pelvic, skull and spine metastasis, there is an indication for RT in order to prevent the development of severe bone pain [98].
In summary, the decision on RT fractionation should be supported by guidelines designated by the American Society for Radiation Oncology (ASTRO) Evidence-Based Guidelines or the European Society for Radiation Oncology (ESTRO) [99,100,101]. According to these recommendations it is considered that pain relief is equivalent after a single 8 Gy fraction, 20 Gy in 5 fractions, 24 Gy in 6 fractions, and 30 Gy in 10 fractions for patients with previously unirradiated painful bone metastases. A single fraction treatment in particular may be considered for patients with poor overall prognosis. Re-irradiation in the case of symptomatic peripheral bone metastases or in spine lesions should be used while adhering to normal tissue dosing constraints.
For patients with widespread involvement of the skeletal system, half-body irradiation may be considered, which typically alleviates pain in about 70% of patients for 2-3 months [110]. The upper, middle or lower half of the skeleton may be irradiated [111,112]. In some patients with stable, oligometastatic (up to 5 metastatic foci) cancer, stereotactic irradiation of single BoM, such as in the spine, may be considered [113,114]. The stereotactic radiotherapy technique, which delivers a high ablative biological dose in one to several fractions in a short treatment course, involves administering one, two or three high fractional doses of ionizing radiation to a precisely defined metastatic focus, guided by imaging studies with careful planning of the irradiated area based on magnetic resonance imaging (MRI) or positron emission tomography (PET). Recent studies show that the effects of this treatment last longer and usually do not require re-irradiation [115,116,117].
In patients with multiple BoM, where the use of teletherapy is challenging, isotopic therapy should be considered. In this case, particular indications pertain to metastatic foci in long bones (femur, tibia, bones of the hand) or in the spine and pelvis, which are most prone to pathological fractures. Isotopic treatment is indicated even with mild pain symptoms, as it reduces pain and strengthens the bones at the site of the metastases.
4.2. Radiotherapy as an Effective Analgesic Procedure in Advanced Head and Neck Cancer Patients
Patients with advanced head and neck cancer often suffer severe pain as a result of extensive soft tissue tumor infiltration, which is often difficult to alleviate pharmacologically. These patients frequently take high doses of strong painkillers without achieving satisfactory pain relief. Radiotherapy is used in the form of short course treatment both in order to treat extensive cancer infiltration and to relieve pain [118,119]. This RT procedure not only provides effective relief from cancer pain after just a few days, but may also reduce the need for pain medication, especially strong opioids [120].
4.3. Radiotherapy as an Effective Procedure in Inflammatory Joint Diseases
Cancers occur most often in older people with comorbidities, especially degenerative joint diseases such as osteoarthritis. However, RT for degenerative joint disease is not a first-line treatment and it is generally used when other options fail. It is important to note that RT in most cases is not a cure for the underlying degenerative condition but may help in managing symptoms. An interesting and important feature of RT with low-dose ionizing energy (single dose of 0.5 to 1 Gy and a total dose of 3 to 6 Gy) which has been recognized since the early 20th century is its analgesic effect in treating inflammatory and degenerative musculoskeletal diseases (MSDs) such as plantar fasciitis and epicondylitis humeri. The exact mechanism remains unclear, but it is believed that low-dose radiotherapy triggers a complex anti-inflammatory response, which is shown in figure1. The effects of anti-inflammatory radiation involve functional modulation of the adhesion of white blood cells to activated endothelial cells and regulation of the induction of nitric oxide synthase in activated macrophages [121,122]. This process most likely involves inhibiting leukocyte accumulation, transfer, and differentiation into macrophages, while also reducing the production of pro-inflammatory cytokines and nitric oxide, which regulate vascular permeability and help suppress the inflammatory cycle [123,124].
Moreover, it has been noticed that after low-dose RT, pro-inflammatory cytokines were generally slightly reduced, but IL-6 was significantly increased. IL-6 is a pro-inflammatory cytokine involved in various pathways, including bone metabolism. While it typically promotes bone resorption and inflammation, it can also have anti-resorptive effects by increasing osteoprotegerin, which inhibits osteoclastogenesis [125]. To sum up, RT is more effective in healing superficial soft tissue diseases or inhibiting cartilage degeneration in osteoarthritis whose therapeutic effect in the case of osteoarthritic lesions reaches up to 75% [126].
4.4. Pain Flares
A flare up of pain is a common side effect of radiopharmaceutical and hormonal therapies, with incidence rates for external beam RT ranging from 2% to 44% [127,128]. Hird et al. reported a 40% incidence of pain flares, mostly occurring within the first 5 days of treatment [129]. These flares may be linked to rapid release of inflammatory cytokines and dexamethasone, due to its anti-inflammatory effects, may help reduce or prevent them130. Chow et al. found that dexamethasone, compared to placebo, reduced pain flare incidence, nausea, and improved functional activity and appetite without serious side effects [131].
4.5. Factors Predicting RT Effectiveness
It is likely that the future direction of research in helping to alleviate cancer pain will be to identify predictors or markers for response to palliative RT in order to classify patients according to successful responses to RT. It is well known that performance status is one of the most important variables in predicting RT response. Moreover, breast or prostate cancer patients also have significantly better response after analgesic RT [132]. Furthermore, the presence of soft tissue expansion outside bone has been found to predict better RT response in patients with painful bone metastases. It has been shown that inflammation measured with CRP was not a predictor for RT response, but patients using corticosteroids had significantly lower response rates with painful bone metastases [133,134]. The latest research emphasizes that educational and organizational strategies are needed to reduce the proportion of patients with inadequate pain management. It is well known that the earlier RT is used in painful bone metastases, the higher its effectiveness [135]. Referring patients for palliative RT earlier may improve the probability of better pain responses and treatment outcomes. Finally, it is worth adding that the effectiveness of RT can be greatly improved by using new technologies to safely deliver higher doses of radiation while sparing healthy tissues as much as possible.
5. The Other Side of the Coin in the Effect of Radiotherapy
5.1. Pain as a Consequence of Radiotherapy
Radiotherapy not only kills cancer cells, but may also affect adjacent non-cancerous cells by releasing various cytokines and inflammatory mediators from damaged cancer cells. The inflammatory reaction can cause fibrosis, atrophy, and ulceration of the tissues, including vessels and nerves, and consequently nerve damage may result in increased pain [136]. In rare cases radiation-induced neuropathy may occur. The exact mechanism of this painful condition is still unclear. Radiation-induced neuropathic pain is often progressive, unresponsive to conservative treatment, and at times irreversible. The main mechanism of radiation-induced neuropathic pain, such as radiation-induced brachial plexopathy after radiotherapy for breast carcinoma is perineural fibrosis and ischemia, subsequently leading to myelin destruction and axonal injury [137].
Radiotherapy may produce various types of post-RT chronic pain syndromes, including peripheral nerve entrapment, radiculopathy, myelopathy, noncardiac chest pain, pelvic pain, osteonecrosis, and other soft-tissue damage after exposure to RT [138]. The neuropathic pain may be successfully treated with oral pharmacotherapy, systemic drug infusion with lidocaine or with spinal cord stimulation [139,140], but radiation-induced neuropathic pain is often unresponsive to conservative treatment. Systemic lidocaine treatment is worth applying in patients with intractable radiation-induced neuropathic pain, even if it is a centrally sensitized state, as a rescue-treatment modality. The main mechanism of action of systemically administered lidocaine is blocking peripheral and central voltage-gated sodium channels, and increasing spinal inhibitory glycinergic neurotransmission mediated by N-methyl-d-aspartate receptors. The systemic lidocaine treatment may reduce opioid consumption and relieve pain in patients with intractable radiation-induced neuropathic pain [141,142,143].The various pain mechanisms occurring after RT are presented in Figure 2.
5.2. Painful Complications After RT
The most common side effects of RT to the spine may include temporary worsening of back pain, sore throat, heartburn, and nausea, depending on the level of the spine being treated. After RT patients may experience temporary fatigue and because ionizing radiation penetrates through the skin, it may cause the treated area to look and feel sunburned – a condition called radiation dermatitis. Most of these are transient early reactions and do not require treatment. However, RT may also cause late consequences. Radiation fibrosis syndrome is a general term describing a myriad of clinical conditions associated with RT, typically caused by an increased accumulation of thrombin in tissue, which may lead to progressive fibrotic tissue sclerosis. Radiation fibrosis syndrome may present during RT or years after treatment and can affect any tissue type, including skin, muscles, tendons, viscera, and nerves. Its effects can have significant functional implications, such as pain, loss of sensation, and weakness [144]. A comparatively rare phenomenon is radiation mononeuritis described as radiation-induced injury at the nerve root or plexus [145]. Late mononeuropathy is a relatively rare complication, but should be considered in patients presenting with neuropathy after RT146. Other complications following RT which cause pain include: osteoradionecrosis (ORN) in head and neck cancer patients, and soft tissue necrosis specifically manifesting as ulceration and cavitation [147]. Early ORN is related to higher radiation doses (>70 Gy), late ORN is multifactorial, involving radiation-related cellular injury and impaired osteoblast function, as well as vascular damage resulting in a chronically hypoxic microenvironment [148,149].
Radiation can also cause damage to the bones of the spine, which may result in a reduction in the patient’s height or change in the shape (curvature) of the spine [150]. In a study with rats it was observed that two weeks after irradiation the three-dimensional bone structure model became coarse, and the trabecular structure continued to thin and disrupt after irradiation, while significant changes in the bone mineral density were not noticed [151]. In vitro studies show that high-dose radiotherapy (RT) significantly damages the viability and function of bone cells, including osteoclasts, osteoblasts, and osteocytes. In vivo animal models reveal that high-dose RT causes morphological changes, inhibits bone repair, and increases bone fragility. Clinical data indicate a rising risk of bone damage, such as fractures over time following high-dose RT [152,153]. Most importantly, osteopenia and osteoporosis increase the risk to bones after RT and are significant problems among cancer patients. Numerous clinical studies have shown that osteoporosis is also a risk factor for developing sacral insufficiency fractures and vertebral body fractures after RT [154,155]. Table 4 summarizes these two sides of RT as a double-edged sword in association with cancer pain.
6. Conclusions
Radiation therapy remains a key cancer treatment, especially for cancer pain. As clinical outcomes improve, minimizing radiation-related toxicities has become a priority. Radiotherapy works in conjunction with pharmacological, radioisotope or molecular therapy, thereby increasing the analgesic effect to enhance therapeutic efficacy, not only in cancer, but also in chronic inflammatory joint diseases. Moreover, RT despite its documented analgesic effects, may also induce or intensify pain in certain clinical situations, as described above. Most of these side effects generally dissipate over time. To sum up, RT in addition to its analgesic effects, can cause serious, undesirable side effects in terms of pain induction, which can make it something of a double-edged sword in cancer treatment. Many of these side effects present difficult challenges to patients and their recognition and treatment can significantly improve patients’ health, long-term survival and QoL.
Author Contributions
Conceptualization: M.Z. Wojtukiewicz and M. Konopka-Filippow, Methodology: M. Konopka-Filippow and M.Z. Wojtukiewicz, Writing: M. Konopka-Filippow, Writing – Review & Editing: B. Politynska, A. M. Wojtukiewicz, M. Konopka-Filippow Visualization: M. Konopka-Filippow, Supervision: M.Z. Wojtukiewicz.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Agarawal J.P., Swangsilpa T., van der Linden Y., Rades D., Jeremic B., Hoskin P.J. The Role of External Beam Radiotherapy in the Management of Bone Metastases. Clin. Oncol. 2006,8,747–760. [CrossRef]
- Lin J, Hsieh RK, Chen JS, Lee KD, Rau KM, Shao YY, Sung YC, Yeh SP, Chang CS, Liu TC, Wu MF, Lee MY, Yu MS, Yen CJ, Lai PY, Hwang WL, Chiou TJ. Satisfaction with pain management and impact of pain on quality of life in cancer patients. Asia Pac J Clin Oncol. 2020,16,2:e91-e98. [CrossRef] [PubMed]
- Sierko E, Hempel D, Zuzda K, Wojtukiewicz MZ. Personalized Radiation Therapy in Cancer Pain Management. Cancers (Basel). 2019,11,3,:390. [CrossRef] [PubMed] [PubMed Central]
- Chow E., Zeng L., Salvo N., Dennis K., Tsao M., Lutz S. Update on the Systematic Review of Palliative Radiotherapy Trials for Bone Metastases. Clin. Oncol. 2012,24,112–124. [CrossRef]
- Baskar R, Lee KA, Yeo R, Yeoh KW. Cancer and radiation therapy: current advances and future directions. Int J Med Sci. 2012,9,3,193-9. [CrossRef] [PubMed] [PubMed Central]
- Jooya A, Talla K, Wei R, Huang F, Dennis K, Gaudet M. Systematic review of brachytherapy for symptom palliation. Brachytherapy. 2022, 6,912-932. [CrossRef] [PubMed]
- Becerra-Bolaños Á, Jiménez-Gil M, Federico M, Domínguez-Díaz Y, Valencia L, Rodríguez-Pérez A. Pain in High-Dose-Rate Brachytherapy for Cervical Cancer: A Retrospective Cohort Study. J Pers Med. 2023, 13, 8,1187. [CrossRef] [PubMed] [PubMed Central]
- Mao G, Theodore N. Spinal brachytherapy. Neuro Oncol. 2022, 24,S62-S68. [CrossRef] [PubMed] [PubMed Central]
- Bossi A, Foulon S, Maldonado X, Sargos P, MacDermott R, Kelly P, Fléchon A, Tombal B, Supiot S, Berthold D, Ronchin P, Kacso G, Salem N, Calabro F, Berdah JF, Hasbini A, Silva M, Boustani J, Ribault H, Fizazi K; PEACE-1 investigators. Efficacy and safety of prostate radiotherapy in de novo metastatic castration-sensitive prostate cancer (PEACE-1): a multicentre, open-label, randomised, phase 3 study with a 2 × 2 factorial design. Lancet. 2024, 404, 10467,:2065-2076. [CrossRef] [PubMed]
- Krzysztofiak T, Kamińska-Winciorek G, Pilśniak A, Wojcieszek P. High dose rate brachytherapy in nonmelanoma skin cancer-Systematic review. Dermatol Ther. 2022, 9,e15675. [CrossRef] [PubMed]
- Cao Q., Wang H., Meng N., Jiang Y., Jiang P., Gao Y., Tian S., Liu C., Yang R., Wang J., et al. CT- guidance interstitial 125Iodine seed brachytherapy as a salvage therapy for recurrent spinal primary tumors. Radiat. Oncol. 2014, 9,301. [CrossRef]
- Qian J., Bao Z., Zou J., Yang H. Effect of pedicle fixation combined with 125I seed implantation for metastatic thoracolumbar tumors. J. Pain Res. 2016 ,9,271–278.
- Nag S, Hu KS. Intraoperative high-dose-rate brachytherapy. Surg Oncol Clin N Am. 2003, 4,1079-97. [CrossRef] [PubMed]
- He J, Mai Q, Yang F, Zhuang W, Gou Q, Zhou Z, Xu R, Chen X, Mo Z. Feasibility and Clinical Value of CT-Guided 125I Brachytherapy for Pain Palliation in Patients With Breast Cancer and Bone Metastases After External Beam Radiotherapy Failure. Front Oncol. 2021, 11,627158. [CrossRef] [PubMed] [PubMed Central]
- Zuckerman S.L., Lim J., Yamada Y., Bilsky M.H., Laufer I. Brachytherapy in Spinal Tumors: A Systematic Review. World Neurosurg. 2018, 118, e235–e244. [CrossRef]
- Parker C., Heinrich D., O’Sullivan J.M., Fossa S., Chodacki A., Demkow T., Cross A., Bolstad B., Garcia- Vargas J., Sartor O. Sartor Overall survival benefit of radium-223 chloride (Alpharadin) in the treatment of patients with symptomatic bone metastases in Castration-resistant Prostate Cancer (CRPC): A phase III randomized trial (ALSYMPCA) Eur. J. Cancer. 2011, 47,3. [CrossRef]
- Choi J.Y. Treatment of Bone Metastasis with Bone-Targeting Radiopharmaceuticals. Nucl. Med. Mol. Imaging. 2018,52,200–207. [CrossRef]
- Ma Y.-B., Yan W.-L., Dai J.-C., Xu F., Yuan Q., Shi H.-H. Strontium-89: A desirable therapeutic for bone metastases of prostate cancer. Zhonghua Nan Ke Xue. 2008,14,819–822.
- Ogawa K., Washiyama K. Bone Target Radiotracers for Palliative Therapy of Bone Metastases. Curr. Med. Chem. 2012, 19,3290–3300. [CrossRef]
- Finlay I.G., Mason M.D., Shelley M. Radioisotopes for the palliation of metastatic bone cancer: A systematic review. Lancet Oncol. 2005, 6,392–400. [CrossRef]
- Fettich J., Padhy A., Nair N., Morales R., Tanumihardja M., Riccabonna G., Nair G. Comparative clinical efficacy and safety of Phosphorus-32 and Strontium-89 in the palliative treatment of metastatic bone pain: Results of an IAEA Coordinated Research Project. World J. Nucl. Med. 2003 ,34,226–231.
- Parker C., Nilsson S., Heinrich D., Helle S.I., O’Sullivan J.M., Fosså S.D., Chodacki A., Wiechno P.,Logue J., Seke M., et al. Alpha Emitter Radium-223 and Survival in Metastatic Prostate Cancer. N. Engl.J. Med. 2013, 369,213–223. [CrossRef]
- Dolezal J., Vizda J., Odrazka K. Prospective evaluation of samarium-153-EDTMP radionuclide treatment for bone metastases in patients with hormone-refractory prostate cancer. Urol. Int. 2007, 78,50–57. [CrossRef]
- Dafermou A., Colamussi P., Giganti M., Cittanti C., Bestagno M., Piffanelli A. A multicentre observational study of radionuclide therapy in patients with painful bone metastases of prostate cancer. Eur. J. Nucl. Med. 2001, 28,788–798. [CrossRef]
- Baczyk M., Milecki P., Baczyk E., Sowiński J. The effectivness of strontium 89 in palliative therapy of painful prostate cancer bone metastases. Ortop. Traumatol. Rehabil. 2003, 5,364–368.
- Sciuto R., Festa A., Pasqualoni R., Semprebene A., Rea S., Bergomi S., Maini C.L. Metastatic bone pain palliation with 89-Sr and 186-Re-HEDP in breast cancer patients. Breast Cancer Res. Treat. 2001, 66,101–109. [CrossRef]
- Zenda S., Nakagami Y., Toshima M., Arahira S., Kawashima M., Matsumoto Y., Kinoshita H., Satake M., Akimoto T. Strontium-89 (Sr-89) chloride in the treatment of various cancer patients with multiple bone metastases. Int. J. Clin. Oncol. 2014, 19,739–743. [CrossRef]
- Laing A.H., Ackery D.M., Bayly R.J., Buchanan R.B., Lewington V.J., McEwan A.J.B., Macleod P.M., Zivanovic M.A. Strontium-89 chloride for pain palliation in prostatic skeletal malignancy. Br. J. Radiol. 1991, 64,817–822. [CrossRef]
- Sartor O., Reid R.H., Hoskin P.J., Quick D.P., Ell P.J., Coleman R.E., Kotler J.A., Freeman L.M., Olivier P. Samarium-153-lexidronam complex for treatment of painful bone metastases in hormone-refractory prostate cancer. Urology 2004, 63, 940–945. [CrossRef]
- Serafini A.N., Houston S.J., Resche I., Quick D.P., Grund F.M., Ell P.J., Bertrand A., Ahmann F.R., Orihuela E., Reid R.H., et al. Palliation of pain associated with metastatic bone cancer using samarium- 153 lexidronam: A double-blind placebo-controlled clinical trial. J. Clin. Oncol. 1998, 16, 1574–1581. [CrossRef]
- Parker C., Heinrich D., O’Sullivan J.M., Fossa S., Chodacki A., Demkow T., Cross A., Bolstad B., Garcia- Vargas J., Sartor O. Sartor Overall survival benefit of radium-223 chloride (Alpharadin) in the treatment of patients with symptomatic bone metastases in Castration-resistant Prostate Cancer (CRPC): A phase III randomized trial (ALSYMPCA) Eur. J. Cancer. 2011, 47,3. [CrossRef]
- Parker C., Nilsson S., Heinrich D., Helle S.I., O’Sullivan J.M., Fosså S.D., Chodacki A., Wiechno P.,Logue J., Seke M., et al. Alpha Emitter Radium-223 and Survival in Metastatic Prostate Cancer. N. Engl.J. Med. 2013, 369,213–223. [CrossRef]
- Han S.H., de Klerk J.M.H., Tan S., van het Schip A.D., Derksen B.H., van Dijk A., Kruitwagen C.L.J.J., Blijham G.H., van Rijk P.P., Zonnenberg B.A. The PLACORHEN study: A double-blind, placebo- controlled, randomized radionuclide study with (186) Re-etidronate in hormone-resistant prostate cancer patients with painful bone metastases. Placebo Controlled Rhenium Study. J. Nucl. Med. 2002, 43, 1150–1156.
- Han S.H., Zonneberg B.A., de Klerk J.M., Quirijnen J.M., van het Schip A.D., van Dijk A., Blijham G.H., van Rijk P.P. 186Re-etidronate in breast cancer patients with metastatic bone pain. J. Nucl. Med.1999, 40, 639–642.
- Palmedo H., Guhlke S., Bender H., Sartor J., Schoeneich G., Risse J., Grünwald F., Knapp F.F., Biersack H.J. Dose escalation study with rhenium-188 hydroxyethylidene diphosphonate in prostate cancer patients with osseous metastases. Eur. J. Nucl. Med. 2000, 27,123–130. [CrossRef]
- Liepe K., Hliscs R., Kropp J., Gruning T., Runge R., Koch R., Knapp F.F.J., Franke W.G. Rhenium-188- HEDP in the palliative treatment of bone metastases. Cancer Biother. Radiopharm. 2000, 15, 261–265. [CrossRef]
- Goblirsch, M.J.; Zwolak, P.P.; Clohisy, D.R. Biology of Bone Cancer Pain. Clin. Cancer Res. 2006, 12, 6231s–6235s. [Google Scholar] [CrossRef] [PubMed]
- Goblirsch, M.; Mathews, W.; Lynch, C.; Alaei, P.; Gerbi, B.J.; Mantyh, P.W.; Clohisy, D.R. Radiation treatment decreases bone cancer pain, osteolysis and tumor size. Radiat. Res. 2004, 161, 228–234. [Google Scholar] [CrossRef] [PubMed]
- MacLeod K, Laird BJA, Carragher NO, Hoskin P, Fallon MT, Sande TA. Predicting Response to Radiotherapy in Cancer-Induced Bone Pain: Cytokines as a Potential Biomarker? Clin Oncol (R Coll Radiol). 2020 ,32,10 ,e203-e208. [CrossRef] [PubMed]
- Lou, Y.; Chen, Y.; Yuan, Y.; Wang, R.; Shan, H. Study on the Correlation between Pain and Cytokine Expression in the Peripheral Blood of Patients with Bone Metastasis of Malignant Cancer Treated Using External Radiation Therapy. Pain Res Manag. 2022, 2022,1119014. [CrossRef] [PubMed] [PubMed Central]
- Cun-Jin S, Jian-Hao X, Xu L, Feng-Lun Z, Jie P, Ai-Ming S, Duan-Min H, Yun-Li Y, Tong L, Yu-Song Z. X- ray induces mechanical and heat allodynia in mouse via TRPA1 and TRPV1 activation. Mol Pain. 2019, 1744806919849201. [CrossRef] [PubMed] [PubMed Central]
- Habberstad R, Aass N, Mollnes TE, Damås JK, Brunelli C, Rossi R, Garcia-Alonso E, Kaasa S, Klepstad P. Inflammatory Markers and Radiotherapy Response in Patients With Painful Bone Metastases. J Pain Symptom Manage. 2022, 64,4,330-339. [CrossRef] [PubMed]
- Bertho A, Iturri L, Prezado Y. Radiation-induced immune response in novel radiotherapy approaches FLASH and spatially fractionated radiotherapies. Int Rev Cell Mol Biol. 2023 ,376:37-68. [CrossRef] [PubMed]
- Dutt S, Ahmed MM, Loo BW Jr, Strober S. Novel Radiation Therapy Paradigms and Immunomodulation: Heresies and Hope. Semin Radiat Oncol. 2020, 30,2,194-200. [CrossRef] [PubMed] [PubMed Central]
- Song XJ, Wang ZB, Gan Q, Walters ET. cAMP and cGMP contribute to sensory neuron hyperexcitability and hyperalgesia in rats with dorsal root ganglia compression. J Neurophysiol. 2006, 95,1,479-92. [CrossRef] [PubMed]
- Zheng JH, Walters ET, Song XJ. Dissociation of dorsal root ganglion neurons induces hyperexcitability that is maintained by increased responsiveness to cAMP and cGMP. J Neurophysiol. 2007, 97,1,15-25. [CrossRef] [PubMed]
- Liu S, Liu YP, Song WB, Song XJ. EphrinB-EphB receptor signaling contributes to bone cancer pain via Toll-like receptor and proinflammatory cytokines in rat spinal cord. Pain 2013, 154,12,2823- 2835. [CrossRef] [PubMed]
- Zhu G, Dong Y, He X, Zhao P, Yang A, Zhou R, Ma J, Xie Z, Song XJ. Radiotherapy Suppresses Bone Cancer Pain through Inhibiting Activation of cAMP Signaling in Rat Dorsal Root Ganglion and Spinal Cord. Mediators Inflamm. 2016, 5093095. [CrossRef] [PubMed] [PubMed Central]
- Koswig S, Budach V. Remineralisation und Schmerzlinderung von Knochenmetastasen nach unterschiedlich fraktionierter Strahlentherapie (10 mal 3 Gy vs. 1 mal 8 Gy). Eine prospektive Studie [Remineralization and pain relief in bone metastases after after different radiotherapy fractions (10 times 3 Gy vs. 1 time 8 Gy). A prospective study]. Strahlenther Onkol. 1999, 175,10,500-8. German. [CrossRef] [PubMed]
- Sprave, T.; Verma, V.; Förster, R.; Schlampp, I.; Hees, K.; Bruckner, T.; Bostel, T.; El Shafie, R.A.; Welzel, T.; Nicolay, N.H.; et al. Bone density and pain response following intensity-modulated radiotherapy versus three-dimensional conformal radiotherapy for vertebral metastases—Secondary results of a randomized trial. Radiat. Oncol. 2018, 13, 212. [Google Scholar] [CrossRef] [PubMed]
- Wei R.L., Mattes M.D., Yu J., Thrasher A., Shu H.-K., Paganetti H., De Los Santos J., Koontz B., Abraham C., Balboni T. Attitudes of radiation oncologists toward palliative and supportive care in the United States: Report on national membership survey by the American Society for Radiation Oncology (ASTRO) Pract. Radiat. Oncol. 2017,7,113–119. [CrossRef]
- Murakami S, Kitani A, Kubota T, Uezono Y. Increased pain after palliative radiotherapy: not only due to cancer progression. Ann Palliat Med. 2024, 13, 18-21. [CrossRef] [PubMed]
- Brozović G, Lesar N, Janev D, Bošnjak T, Muhaxhiri B. CANCER PAIN AND THERAPY. Acta Clin Croat. 2022, 61,103-108. [CrossRef] [PubMed] [PubMed Central]
- Ng S.P., Koay E.J. Current and emerging radiotherapy strategies for pancreatic adenocarcinoma: stereotactic, intensity modulated and particle radiotherapy. Ann. Pancreat. Cancer. 2018,1,22. [CrossRef]
- Ryan J.F., Rosati L.M., Groot V.P., Le D.T., Zheng L., Laheru D.A., Shin E.J., Jackson J., Moore J., Narang A.K., et al. Stereotactic body radiation therapy for palliative management of pancreatic adenocarcinoma in elderly and medically inoperable patients. Oncotarget. 2018, 9,16427–16436. [CrossRef]
- Arscott WT, Emmett J, Ghiam AF, Jones JA. Palliative Radiotherapy: Inpatients, Outpatients, and the Changing Role of Supportive Care in Radiation Oncology. Hematol Oncol Clin North Am. 2020;34(1):253-277.
- Fairchild A., Harris K., Barnes E., Wong R., Lutz S., Bezjak A., Cheung P., Chow E. Palliative thoracic radiotherapy for lung cancer: A systematic review. J. Clin. Oncol. 2008, 26, 4001–4011. [CrossRef]
- Lutz ST. Palliative radiotherapy: history, recent advances, and future directions. Ann Palliat Med. 2019, 8, 3,240-245. [CrossRef] [PubMed]
- Zhu X, Zhang B, Zhang S, Xia X, Sun S, Wu D. Stereotactic body radiotherapy for superior vena cava syndrome. Rep Pract Oncol Radiother. 2011,27,4,756-757. [CrossRef] [PubMed] [PubMed Central]
- Williams GR, Manjunath SH, Butala AA, Jones JA. Palliative Radiotherapy for Advanced Cancers: Indications and Outcomes. Surg Oncol Clin N Am. 2021, 3,3, 563-580. [CrossRef] [PubMed]
- Matsui JK, Perlow HK, Upadhyay R, McCalla A, Raval RR, Thomas EM, Blakaj DM, Beyer SJ, Palmer JD. Advances in Radiotherapy for Brain Metastases. Surg Oncol Clin N Am. 2023, 323,56,9-586. [CrossRef] [PubMed]
- Antoni D, Mesny E, El Kabbaj O, Josset S, Noël G, Biau J, Feuvret L, Latorzeff I. Role of radiotherapy in the management of brain oligometastases. Cancer Radiother. 2024, 28,1,103-110. [CrossRef] [PubMed]
- Cho S, Chu MK. Headache in Brain Tumors. Neurol Clin. 2024, 42,2,487-496. [CrossRef] [PubMed]
- Cuneo A, Murinova N. Headache Management in Individuals with Brain Tumor. Semin Neurol. 2024, 44,1,74-89. [CrossRef] [PubMed]
- Gondi V, Bauman G, Bradfield L, Burri SH, Cabrera AR, Cunningham DA, Eaton BR, Hattangadi-Gluth JA, Kim MM, Kotecha R, Kraemer L, Li J, Nagpal S, Rusthoven CG, Suh JH, Tomé WA, Wang TJC, Zimmer AS, Ziu M, Brown PD. Radiation Therapy for Brain Metastases: An ASTRO Clinical Practice Guideline. Pract Radiat Oncol. 2022, 12,4,265-282. [CrossRef] [PubMed]
- Gagliardi F, De Domenico P, Snider S, Nizzola MG, Mortini P. Efficacy of neoadjuvant stereotactic radiotherapy in brain metastases from solid cancer: a systematic review of literature and meta- analysis. Neurosurg Rev. 2023, 46,1,130. [CrossRef] [PubMed]
- Bodensohn R, Kaempfel AL, Boulesteix AL, Orzelek AM, Corradini S, Fleischmann DF, Forbrig R, Garny S, Hadi I, Hofmaier J, Minniti G, Mansmann U, Pazos Escudero M, Thon N, Belka C, Niyazi M. Stereotactic radiosurgery versus whole-brain radiotherapy in patients with 4-10 brain metastases: A nonrandomized controlled trial. Radiother Oncol. 2023, 186,109744. [CrossRef] [PubMed]
- Ono T, Nemoto K. Re-Whole Brain Radiotherapy May Be One of the Treatment Choices for Symptomatic Brain Metastases Patients. Cancers (Basel). 2022, 4,21,5293. [CrossRef] [PubMed] [PubMed Central]
- Coleman RE, Croucher PI, Padhani AR, Clézardin P, Chow E, Fallon M, Guise T, Colangeli S, Capanna R, Costa L. Bone metastases. Nat Rev Dis Primers. 2020, 6,1,83. [CrossRef] [PubMed]
- Arcangeli G., Pinnarò P., Rambone R., Giannarelli D., Benassi M. A phase III randomized study on the sequencing of radiotherapy and chemotherapy in the conservative management of early-stage breast cancer. Int. J. Radiat. Oncol. Biol. Phys. 2006, 64,61–167. [CrossRef]
- Migliorini F, Maffulli N, Trivellas A, Eschweiler J, Tingart M, Driessen A. Bone metastases: a comprehensive review of the literature. Mol Biol Rep. 2020, 47,8,6337-6345. [CrossRef] [PubMed]
- Harstell W.F., Santosh Y. Palliation of bone metastases. In: Halperin E., Perez C., Brady L., editors. Principles and Practice of Radiat. Oncol. 2013, 1, 1778–1791.
- Cook GJR, Goh V. Molecular Imaging of Bone Metastases and Their Response to Therapy. J Nucl Med. 2020, 61,6,799-806. [CrossRef] [PubMed]
- Kakhki VR, Anvari K, Sadeghi R, Mahmoudian AS, Torabian-Kakhki M. Pattern and distribution of bone metastases in common malignant tumors. Nucl Med Rev Cent East Eur. 2013, 16,2,66-9. [CrossRef] [PubMed]
- Clézardin P, Coleman R, Puppo M, Ottewell P, Bonnelye E, Paycha F, Confavreux CB, Holen I. Bone metastasis: mechanisms, therapies, and biomarkers. Physiol Rev. 2021, 101,3,797-855. [CrossRef] [PubMed]
- Käkönen SM, Mundy GR. Mechanisms of osteolytic bone metastases in breast carcinoma. Cancer 2003, 1,97,834-9. [CrossRef] [PubMed]
- Guise TA, Mohammad KS, Clines G, Stebbins EG, Wong DH, Higgins LS, Vessella R, Corey E, Padalecki S, Suva L, Chirgwin JM. Basic mechanisms responsible for osteolytic and osteoblastic bone metastases. Clin Cancer Res. 2006 Oct 15;12(20 Pt 2):6213s-6216s. [CrossRef] [PubMed]
- Challapalli A, Aziz S, Khoo V, Kumar A, Olson R, Ashford RU, Gabbar OA, Rai B, Bahl A. Spine and Non- spine Bone Metastases - Current Controversies and Future Direction. Clin Oncol (R Coll Radiol). 2020, 32,11,728-744. [CrossRef] [PubMed]
- Bouhassira, D.; Luporsi, E.; Krakowski, I. Prevalence and incidence of chronic pain with or without neuropathic characteristics in patients with cancer. Pain 2017, 158, 1118–1125. [Google Scholar] [CrossRef] [PubMed]
- Zinboonyahgoon, N.; Luansritisakul, C. Neuropathic pain feature in cancer-induced bone pain: Does it matter? A prospective observational study. Korean J. Pain 2023, 36, 253–267. [Google Scholar] [CrossRef] [PubMed]
- Roos DE. Radiotherapy for neuropathic pain due to bone metastases. Ann Palliat Med. 2015, 4,220-4. [CrossRef] [PubMed]
- Gouveia AG, Chan DCW, Hoskin PJ, Marta GN, Trippa F, Maranzano E, Chow E, Silva MF. Advances in radiotherapy in bone metastases in the context of new target therapies and ablative alternatives: A critical review. Radiother Oncol. 2021, 163,55-67. [CrossRef] [PubMed]
- Mestdagh F, Steyaert A, Lavand'homme P. Cancer Pain Management: A Narrative Review of Current Concepts, Strategies, and Techniques. Curr Oncol. 2023, 30,7,6838-6858. [CrossRef] [PubMed] [PubMed Central]
- Takei D, Tagami K. Management of cancer pain due to bone metastasis. J Bone Miner Metab. 2023 ,41,3,327-336. [CrossRef] [PubMed]
- Lutz S., Berk L., Chang E., Chow E., Hahn C., Hoskin P., Howell D., Konski A., Kachnic L., Lo S., et al. Palliative radiotherapy for bone metastases: An ASTRO evidence-based guideline. Int. J. Radiat. Oncol. Biol. Phys. 2011, 79,965–976. [CrossRef]
- Tseng YD. Radiation Therapy for Painful Bone Metastases: Fractionation, Recalcification, and Symptom Control. Semin Radiat Oncol. 2023, 2,139-147. [CrossRef] [PubMed]
- Lam T.C., Tseng Y. Defining the radiation oncologist’s role in palliative care and radiotherapy. Ann. Palliat. Med. 2018, 7,1002. [CrossRef]
- Sierko E, Hempel D, Zuzda K, Wojtukiewicz MZ. Personalized Radiation Therapy in Cancer Pain Management. Cancers (Basel). 2019, 11,3,390. [CrossRef] [PubMed] [PubMed Central]
- Koswig S., Budach V. Remineralization and pain relief in bone metastases after after different radiotherapy fractions (10 times 3 Gy vs. 1 time 8 Gy). A prospective study. Strahlenther. Onkol. 1999, 175,500–508. [CrossRef]
- Foro Arnalot P., Fontanals A.V., Galcerán J.C., Lynd F., Latiesas X.S., de Dios N.R., Castillejo A.R., Bassols M.L., Galán J.L., Conejo I.M., et al. Randomized clinical trial with two palliative radiotherapy regimens in painful bone metastases: 30 Gy in 10 fractions compared with 8 Gy in single fraction. Radiother. Oncol. 2008, 89,150–155. [CrossRef]
- Nongkynrih A., Dhull A.K., Kaushal V., Atri R., Dhankhar R., Kamboj K. Comparison of Single Versus Multifraction Radiotherapy in Palliation of Painful Bone Metastases. World J. Oncol. 2018, 9,91–95. [CrossRef]
- Bianchi SP, Faccenda V, Pacifico P, Parma G, Saufi S, Ferrario F, Belmonte M, Sala L, De Ponti E, Panizza D, Arcangeli S. Short-term pain control after palliative radiotherapy for uncomplicated bone metastases: a prospective cohort study. Med Oncol. 2023, 41,1,13. [CrossRef] [PubMed]
- Kachnic L., Berk L. Palliative Single-Fraction Radiation Therapy: How Much More Evidence Is Needed? JNCI. 2005, 97,786–788. [CrossRef]
- Chow E., Zeng L., Salvo N., Dennis K., Tsao M., Lutz S. Update on the Systematic Review of Palliative Radiotherapy Trials for Bone Metastases. Clin. Oncol. 2012;24:112–124. [CrossRef]
- Chow E., van der Linden Y.M., Roos D., Hartsell W.F., Hoskin P., Wu J.S.Y., Brundage M.D., Nabid A., Tissing-Tan C.J.A., Oei B., et al. Single versus multiple fractions of repeat radiation for painful bone metastases: A randomised, controlled, non-inferiority trial. Lancet Oncol. 2014, 15,164–171. [CrossRef]
- Roos D.E., Turner S.L., O’Brien P.C., Smith J.G., Spry N.A., Burmeister B.H., Hoskin P.J., Ball D.L. Randomized trial of 8 Gy in 1 versus 20 Gy in 5 fractions of radiotherapy for neuropathic pain due to bone metastases (Trans-Tasman Radiation Oncology Group, TROG 96.05) Radiother. Oncol. 2005,75,54–63. [CrossRef]
- Saito T., Tomitaka E., Toya R., Matsuyama T., Ninomura S., Watakabe T., Oya N. A neuropathic pain component as a predictor of improvement in pain interference after radiotherapy for painful tumors: A secondary analysis of a prospective observational study. Clin. Transl. Radiat. Oncol. 2018, 12,34–39. [CrossRef]
- Saito AI, Hirai T, Inoue T, Hojo N, Kawai S, Kato Y, Ito K, Kato M, Ozawa Y, Shinjo H, Toda K, Yoshimura RI. Time to Pain Relapse After Palliative Radiotherapy for Bone Metastasis: A Prospective Multi-institutional Study. Anticancer Res. 2023, 43,2,865-873. [CrossRef] [PubMed]
- Lutz S., Balboni T., Jones J., Lo S., Petit J., Rich S.E., Wong R., Hahn C. Palliative radiation therapy for bone metastases: Update of an ASTRO Evidence-Based Guideline. Pract. Radiat. Oncol. 2017, 7,4–12. [CrossRef]
- van der Velden J, Willmann J, Spałek M, Oldenburger E, Brown S, Kazmierska J, Andratschke N, Menten J, van der Linden Y, Hoskin P. ESTRO ACROP guidelines for external beam radiotherapy of patients with uncomplicated bone metastases. Radiother Oncol. 2022, 173,197-206. [CrossRef] [PubMed]
- Oldenburger E, Brown S, Willmann J, van der Velden JM, Spałek M, van der Linden YM, Kazmierska J, Menten J, Andratschke N, Hoskin P. ESTRO ACROP guidelines for external beam radiotherapy of patients with complicated bone metastases. Radiother Oncol. 2022, 173,240-253. [CrossRef] [PubMed]
- Steenland E, Leer JW, van Houwelingen H, Post WJ, van den Hout WB, Kievit J, de Haes H, Martijn H, Oei B, Vonk E, van der Steen-Banasik E, Wiggenraad RG, Hoogenhout J, Wárlám-Rodenhuis C, van Tienhoven G, Wanders R, Pomp J, van Reijn M, van Mierlo I, Rutten E. The effect of a single fraction compared to multiple fractions on painful bone metastases: a global analysis of the Dutch Bone Metastasis Study. Radiother Oncol. 1999, 2,101-9. doi: 10.1016/s0167-8140(99)00110-3. Erratum in: Radiother Oncol 1999 Nov;53(2):167. Leer, J [corrected to Leer, JW]; van Mierlo ,T [corrected to van Mierlo, I]. PMID: 10577695.
- Koswig S, Buchali A, Böhmer D, Schlenger L, Budach V. Palliative Strahlentherapie von Knochenmetastasen. Eine retrospective Analyse von 176 Patienten [Palliative radiotherapy of bone metastases. A retrospective analysis of 176 patients]. Strahlenther Onkol. 1999, 175,10,509-14. German. [CrossRef] [PubMed]
- Roos DE, Turner SL, O'Brien PC, Smith JG, Spry NA, Burmeister BH, Hoskin PJ, Ball DL; Trans-Tasman Radiation Oncology Group, TROG 96.05. Randomized trial of 8 Gy in 1 versus 20 Gy in 5 fractions of radiotherapy for neuropathic pain due to bone metastases (Trans-Tasman Radiation Oncology Group, TROG 96.05). Radiother Oncol. 2005, 75,1,54-63. [CrossRef] [PubMed]
- Hartsell WF, Scott CB, Bruner DW, Scarantino CW, Ivker RA, Roach M 3rd, Suh JH, Demas WF, Movsas B, Petersen IA, Konski AA, Cleeland CS, Janjan NA, DeSilvio M. Randomized trial of short- versus long-course radiotherapy for palliation of painful bone metastases. J Natl Cancer Inst. 2005, 97,11,798-804. [CrossRef] [PubMed]
- Foro Arnalot P, Fontanals AV, Galcerán JC, Lynd F, Latiesas XS, de Dios NR, Castillejo AR, Bassols ML, Galán JL, Conejo IM, López MA. Randomized clinical trial with two palliative radiotherapy regimens in painful bone metastases: 30 Gy in 10 fractions compared with 8 Gy in single fraction. Radiother Oncol. 2008, 89,2,150-5. [CrossRef] [PubMed]
- Nongkynrih A, Dhull AK, Kaushal V, Atri R, Dhankhar R, Kamboj K. Comparison of Single Versus Multifraction Radiotherapy in Palliation of Painful Bone Metastases. World J Oncol. 2018, 9,3,91-95. [CrossRef] [PubMed] [PubMed Central]
- Nguyen QN, Chun SG, Chow E, Komaki R, Liao Z, Zacharia R, Szeto BK, Welsh JW, Hahn SM, Fuller CD, Moon BS, Bird JE, Satcher R, Lin PP, Jeter M, O'Reilly MS, Lewis VO. Single-Fraction Stereotactic vs Conventional Multifraction Radiotherapy for Pain Relief in Patients With Predominantly Nonspine Bone Metastases: A Randomized Phase 2 Trial. JAMA Oncol. 2019, 5,6,872-878. doi: 10.1001/jamaoncol.2019.0192. Erratum in: JAMA Oncol. 2021 Oct 1;7(10):1581. doi: 10.1001/jamaoncol.2021.3081. PMID: 31021390; PMCID: PMC6487911.
- Nguyen EK, Ruschin M, Zhang B, Soliman H, Myrehaug S, Detsky J, Chen H, Sahgal A, Tseng CL. Stereotactic body radiotherapy for spine metastases: a review of 24 Gy in 2 daily fractions. J Neurooncol. 2023, 163,1, 15-27. [CrossRef] [PubMed]
- Bilski M, Konat-Bąska K, Mastroleo F, Hoskin P, Alicja Jereczek-Fossa B, Marvaso G, Korga M, Klas J, Zych K, Bijak P, Kukiełka A, Fijuth J, Kuncman Ł. Half body irradiation (HBI) for bone metastases in the modern radiotherapy technique era - A systematic review. Clin Transl Radiat Oncol. 2024, 49,100845. [CrossRef] [PubMed] [PubMed Central]
- Delinikolas P., Patatoukas G., Kouloulias V., Dilvoi M., Plousi A., Efstathopoulos E., Platoni K. A novel Hemi-Body Irradiation technique using electron beams (HBIe−) Phys. Medica. 2018, 46,16–24. [CrossRef]
- Pal S., Dutta S., Adhikary S., Bhattacharya B., Ghosh B., Patra N. Hemi body irradiation: An economical way of palliation of pain in bone metastasis in advanced cancer. South Asian J. Cancer. 2014, 3,28. [CrossRef]
- Ryu S, Deshmukh S, Timmerman RD, Movsas B, Gerszten P, Yin FF, Dicker A, Abraham CD, Zhong J, Shiao SL, Tuli R, Desai A, Mell LK, Iyengar P, Hitchcock YJ, Allen AM, Burton S, Brown D, Sharp HJ, Dunlap NE, Siddiqui MS, Chen TH, Pugh SL, Kachnic LA. Stereotactic Radiosurgery vs Conventional Radiotherapy for Localized Vertebral Metastases of the Spine: Phase 3 Results of NRG Oncology/RTOG 0631 Randomized Clinical Trial. JAMA Oncol. 2023, 9,6,800-807. [CrossRef] [PubMed] [PubMed Central]
- Nguyen EK, Ruschin M, Zhang B, Soliman H, Myrehaug S, Detsky J, Chen H, Sahgal A, Tseng CL. Stereotactic body radiotherapy for spine metastases: a review of 24 Gy in 2 daily fractions. J Neurooncol. 2023, 163,1,15-27. [CrossRef] [PubMed]
- Palma D.A., Salama J.K., Lo S.S., Senan S., Treasure T., Govindan R., Weichselbaum R. The oligometastatic state-separating truth from wishful thinking. Nat. Rev. Clin. Oncol. 2014, 11,549–557. [CrossRef]
- Osborn V.W., Lee A., Yamada Y. Stereotactic Body Radiation Therapy for Spinal Malignancies. Technol. Cancer Res. Treat. 2018, 17. [CrossRef]
- Bindels BJJ, Mercier C, Gal R, Verlaan JJ, Verhoeff JJC, Dirix P, Ost P, Kasperts N, van der Linden YM, Verkooijen HM, van der Velden JM. Stereotactic Body and Conventional Radiotherapy for Painful Bone Metastases: A Systematic Review and Meta-Analysis. JAMA Netw Open. 2024, 7,2,e2355409. [CrossRef] [PubMed] [PubMed Central]
- Shahid Iqbal M, Kelly C, Kovarik J, Goranov B, Shaikh G, Morgan D, Dobrowsky W, Paleri V. Palliative radiotherapy for locally advanced non-metastatic head and neck cancer: A systematic review. Radiother Oncol. 2018, 126,3,558-567. [CrossRef] [PubMed]
- Zingeta GT, Worku YT, Awol M, Woldetsadik ES, Assefa M, Chama TZ, Feyisa JD, Bedada HF, Adem MI, Mengesha T, Wong R. Outcome of Hypofractionated Palliative Radiotherapy Regimens for Patients With Advanced Head and Neck Cancer in Tikur Anbessa Hospital, Ethiopia: A Prospective Cohort Study. JCO Glob Oncol. 2024, 10,e2300253. [CrossRef] [PubMed] [PubMed Central]
- Schaller AKCS, Peterson A, Bäckryd E. Pain management in patients undergoing radiation therapy for head and neck cancer - a descriptive study. Scand J Pain. 2020, 21,2,256-265. [CrossRef] [PubMed]
- Trott KR, Kamprad F. Radiobiological mechanisms of anti-inflammatory radiotherapy. Radiother Oncol. 1999, 51,3,197-203. [CrossRef] [PubMed]
- Arenas M, Sabater S, Hernández V, Rovirosa A, Lara PC, Biete A, Panés J. Anti-inflammatory effects of low-dose radiotherapy. Indications, dose, and radiobiological mechanisms involved. Strahlenther Onkol. 2012, 188,11,975-81. [CrossRef] [PubMed]
- Rühle A, Tkotsch E, Mravlag R, Haehl E, Spohn SKB, Zamboglou C, Huber PE, Debus J, Grosu AL, Sprave T, Nicolay NH. Low-dose radiotherapy for painful osteoarthritis of the elderly: A multicenter analysis of 970 patients with 1185 treated sites. Strahlenther Onkol. 2021, 197,10, 895-902. [CrossRef] [PubMed] [PubMed Central]
- Abdelmaqsoud A, Vorotniak N, Strauß D, Hentschel B. The analgesic effect of low-dose radiotherapy in treating benign musculoskeletal painful disorders using different energies: A retrospective cohort study. JRP 2023, 22,e78. [CrossRef]
- Weissmann T, Rückert M, Zhou JG, Seeling M, Lettmaier S, Donaubauer AJ, Nimmerjahn F, Ott OJ, Hecht M, Putz F, Fietkau R, Frey B, Gaipl US, Deloch L. Low-Dose Radiotherapy Leads to a Systemic Anti-Inflammatory Shift in the Pre-Clinical K/BxN Serum Transfer Model and Reduces Osteoarthritic Pain in Patients. Front Immunol. 2022, 12,777792. [CrossRef] [PubMed] [PubMed Central]
- Javadinia, S A, Nazeminezhad, N, Ghahramani-Asl, R et al. Low-dose radiation therapy for osteoarthritis and enthesopathies: a review of current data. Int J Radiat Biol 2021, 97,10,1352–1367. [CrossRef]
- Loblaw DA, Wu JS, Kirkbride P, et al. Pain flare in patients with bone metastases after palliative radiotherapy--a nested randomized control trial. Support. Care Cancer 2007,15,451-5.
- Chow E, Ling A, Davis L, et al. Pain flare following external beam radiotherapy and meaningful change in pain scores in the treatment of bone metastases. Radiother Oncol 2005, 75:64-9. [CrossRef]
- Hird A, Chow E, Zhang L, et al. Determining the incidence of pain flare following palliative radiotherapy for symptomatic bone metastases: results from three canadian cancer centers. Int J Radiat Oncol Biol Phys 2009, 75,193-7.
- Loblaw, D.A.; Wu, J.S.; Kirkbride, P.; Panzarella, T.; Smith, K.; Aslanidis, J.; Warde, P. Pain flare in patients with bone metastases after palliative radiotherapy—A nested randomized control trial. Support. Care Cancer 2007, 15, 451–455. [Google Scholar] [CrossRef] [PubMed]
- Chow E, Meyer RM, Ding K, et al. Dexamethasone in the prophylaxis of radiation-induced pain flare after palliative radiotherapy for bone metastases: a double-blind, randomised placebo-controlled, phase 3 trial. Lancet Oncol 2015, 16,1463-72.
- van der Velden JM, Peters M, Verlaan JJ, Versteeg AL, Zhang L, Tsao M, Danjoux C, Barnes E, van Vulpen M, Chow E, Verkooijen HM. Development and Internal Validation of a Clinical Risk Score to Predict Pain Response After Palliative Radiation Therapy in Patients With Bone Metastases. Int J Radiat Oncol Biol Phys. 2017, 99,4,859-866. doi: 10.1016/j.ijrobp.2017.07.029. Epub 2017 Jul 31.Erratum in: Int J Radiat Oncol Biol Phys. 2019 Aug 1;104(5):1186. doi: 10.1016/j.ijrobp.2019.05.016. PMID: 29063851.
- Fabregat C, Almendros S, Navarro-Martin A, Gonzalez J. Pain Flare-Effect Prophylaxis With Corticosteroids on Bone Radiotherapy Treatment: A Systematic Review. Pain Pract. 2020, 20,1,101-109. [CrossRef] [PubMed]
- Habberstad R, Frøseth TCS, Aass N, Bjerkeset E, Abramova T, Garcia-Alonso E, Caputo M, Rossi R, Boland JW, Brunelli C, Lund JÅ, Kaasa S, Klepstad P. Clinical Predictors for Analgesic Response to Radiotherapy in Patients with Painful Bone Metastases. J Pain Symptom Manage. 2021, 62,4,681- 690. [CrossRef] [PubMed]
- Donati CM, Maggiore CM, Maltoni M, Rossi R, Nardi E, Zamagni A, Siepe G, Mammini F, Cellini F, Di Rito A, Portaluri M, De Tommaso C, Santacaterina A, Tamburella C, Di Franco R, Parisi S, Cossa S, Fusco V, Bianculli A, Ziccarelli P, Ziccarelli L, Genovesi D, Caravatta L, Deodato F, Macchia G, Fiorica F, Napoli G, Buwenge M, Morganti AG. Adequacy of Pain Management in Patients Referred for Radiation Therapy: A Subanalysis of the Multicenter ARISE-1 Study. Cancers (Basel). 2023, 16,1,109. [CrossRef] [PubMed] [PubMed Central]
- Delanian S, Lefaix JL, Pradat PF. Radiation-induced neuropathy in cancer survivors. Radiother Oncol. 2012;105(3):273–282. [CrossRef]
- Fathers E, Thrush D, Huson SM, Norman A. Radiation-induced brachial plexopathy in women treated for carcinoma of the breast. Clin Rehabil. 2002, 16,2,160–165. [CrossRef]
- Andreyev HJ, Wotherspoon A, Denham JW, Hauer-Jensen M. Defining pelvic-radiation disease for the survivorship era. Lancet Oncol. 2010, 11,4,310–312. [CrossRef]
- Elahi F, Callahan D, Greenlee J, Dann TL. Pudendal entrapment neuropathy: a rare complication of pelvic radiation therapy. Pain Physician. 2013, 16,6,E793–E797.
- WHO Guidelines for the Pharmacological and Radiotherapeutic Management of Cancer Pain in Adults and Adolescents. Geneva: WHO 2018. [PubMed]
- Doo AR, Shin YS, Yoo S, Park JK. Radiation-induced neuropathic pain successfully treated with systemic lidocaine administration. J Pain Res. 2018, 11,545-548. [CrossRef] [PubMed] [PubMed Central]
- Moisset X. Neuropathic pain: Evidence based recommendations. Presse Med. 2024, 53,2,104232. [CrossRef] [PubMed]
- Tsai JH, Liu IT, Su PF, Huang YT, Chiu GL, Chen YY, Lai WS, Lin PC. Lidocaine transdermal patches reduced pain intensity in neuropathic cancer patients already receiving opioid treatment. BMC Palliat Care. 2023, 22,1,4. [CrossRef] [PubMed] [PubMed Central]
- Stubblefield MD: Cancer Rehabilitation: Principles and Practice, 2nd ed. New York, Demos Medical 2018.
- Pradat PF, Bouche P, Delanian S. Sciatic nerve moneuropathy: an unusual late effect of radiotherapy. Muscle Nerve. 2009, 40,5,872-4. [CrossRef] [PubMed]
- Zhu Y, Tsai W, Sokolof J. Sciatic Neuropathy After Radiation Treatment. Am J Phys Med Rehabil. 2021, 100,12,e198-e199. [CrossRef] [PubMed]
- Carr CM, Benson JC, DeLone DR, Diehn FE, Kim DK, Ma D, Nagelschneider AA, Madhavan AA, Johnson DR. Manifestations of radiation toxicity in the head, neck, and spine: An image-based review. Neuroradiol J. 2022, 4,427-436. [CrossRef] [PubMed] [PubMed Central]
- Chopra S, Kamdar D, Tulunay Ugur OE, et al. Factors predictive of severity of osteoradionecrosis of the mandible. Head & Neck 2011, 33,1600–1605. [CrossRef]
- Alhilali L, Reynolds AR, Fakhran S. Osteoradionecrosis after radiation therapy for head and neck cancer: differentiation from recurrent disease with CT and PET/CT imaging. Am J Neuroradiology 2014, 35,1405–1411. [CrossRef]
- Ito K, Nakajima Y, Ogawa H, Taguchi K. Fracture risk following stereotactic body radiotherapy for long bone metastases. Jpn J Clin Oncol. 2022, 52,1,47-52. [CrossRef] [PubMed]
- Igarashi T, Demura S, Kato S, Shinmura K, Yokogawa N, Yonezawa N, Shimizu T, Oku N, Murakami H, Tsuchiya H. Effects of Radiation on the Bone Strength of Spinal Vertebrae in Rats. Spine (Phila Pa 1976). 2022, 47,12,E514-E520. [CrossRef] [PubMed]
- Berk L. The effects of high-dose radiation therapy on bone: a scoping review. Radiat Oncol J. 2024, 42,2,95-103. [CrossRef] [PubMed] [PubMed Central]
- Yaprak G, Gemici C, Temizkan S, Ozdemir S, Dogan BC, Seseogullari OO. Osteoporosis development and vertebral fractures after abdominal irradiation in patients with gastric cancer. BMC Cancer. 2018, 11,18,1,972. [CrossRef] [PubMed] [PubMed Central]
- Berk L. The effects of high-dose radiation therapy on bone: a scoping review. Radiat Oncol J. 2024, 42,2,95-103. [CrossRef] [PubMed] [PubMed Central]
- Choi YJ. Cancer treatment-induced bone loss. Korean J Intern Med. 2024, 39,5,731-745. [CrossRef] [PubMed] [PubMed Central]
- Adlakha P, Maheshwari G, Dhanawat A, Sinwer R, Singhal M, Jakhar SL, Sharma N, Kumar HS. Comparison of two schedules of hypo-fractionated radiotherapy in locally advanced head-and-neck cancers. J Cancer Res Ther. 2022, 18,S151-S156. [CrossRef] [PubMed]
- Grewal AS, Jones J, Lin A. Palliative Radiation Therapy for Head and Neck Cancers. Int J Radiat Oncol Biol Phys. 2019, 1,105,2,254-266. [CrossRef] [PubMed]
- Gewandter JS, Walker J, Heckler CE, Morrow GR, Ryan JL. Characterization of skin reactions and pain reported by patients receiving radiation therapy for cancer at different sites. J Support Oncol. 2013, 11,4,183-9. [CrossRef] [PubMed] [PubMed Central]
- Park J, Lee JE. Comparison between 1-week and 2-week palliative radiotherapy courses for superior vena cava syndrome. Radiat Oncol J. 2023, 41,3,178-185. [CrossRef] [PubMed] [PubMed Central]
- Xu J, Yang G, An W, Wang W, Li F, Meng Y, Wang X. Correlations between the severity of radiation-induced oral mucositis and salivary epidermal growth factor as well as inflammatory cytokines in patients with head and neck cancer. Head Neck. 2023, 45,5,1122-1129. [CrossRef] [PubMed]
- Young J, Rattan D, Cheung A, Lazarakis S, McGilvray S. Pain management for persistent pain post radiotherapy in head and neck cancers: systematic review. Scand J Pain. 2023, 15,24,1. [CrossRef] [PubMed]
- Lam E, Wong G, Zhang L, Drost L, Karam I, Yee C, McCurdy-Franks E, Razvi Y, Ariello K, Wan BA, Nolen A, Wang K, DeAngelis C, Chow E. Self-reported pain in breast cancer patients receiving adjuvant radiotherapy. Support Care Cancer. 2021, 29,1,155-167. [CrossRef] [PubMed]
- Wan BA, Pidduck W, Zhang L, Nolen A, Yee C, Wang K, Chow S, Chan S, Drost L, Soliman H, Leung E, Sousa P, Lewis D, DeAngelis C, Taylor P, Chow E. Patient-Reported Pain in Patients with Breast Cancer Who Receive Radiotherapy. Pain Manag Nurs. 2021, 22,3,402-407. [CrossRef] [PubMed]
- Buwenge M, Macchia G, Arcelli A, Frakulli R, Fuccio L, Guerri S, Grassi E, Cammelli S, Cellini F, Morganti AG. Stereotactic radiotherapy of pancreatic cancer: a systematic review on pain relief. J Pain Res. 2018, 4,11,2169-2178. [CrossRef] [PubMed] [PubMed Central]
- Friedes C, Butala AA. Palliative radiotherapy for pancreatic cancer. Ann Palliat Med. 2024, 13,1,1-4. doi: 10.21037/apm-23-560. [CrossRef] [PubMed]
- Biran A, Bolnykh I, Rimmer B, Cunliffe A, Durrant L, Hancock J, Ludlow H, Pedley I, Rees C, Sharp L. A Systematic Review of Population-Based Studies of Chronic Bowel Symptoms in Cancer Survivors following Pelvic Radiotherapy. Cancers (Basel). 2023, 15,16,4037. [CrossRef] [PubMed] [PubMed Central]
- Bisson E, Piton L, Durand B, Sarrade T, Huguet F. Palliative pelvic radiotherapy for symptomatic frail or metastatic patients with rectal adenocarcinoma: A systematic review. Dig Liver Dis. 2024, 9,S1590-8658(24)00890-9. [CrossRef] [PubMed]
- Dhanachai M, Theerapancharoen V, Laothamatas J, Pongpech S, Kraiphibul P, Chanwitayanuchit T, Pochanugool L, Dangprasert S, Sarnvivad P, Sinpornchai V, Kuonsongtum V, Pirabul R, Yongvithisatid P. Early neurological complications after stereotactic radiosurgery/radiotherapy. J Med Assoc Thai. 2001, 84,12,1729-37. [PubMed]
- Zaki P, Barbour A, Zaki MM, Tseng YD, Amin AG, Venur V, McGranahan T, Vellayappan B, Palmer JD, Chao ST, Yang JT, Foote M, Redmond KJ, Chang EL, Sahgal A, Lo SS, Schaub SK. Emergent radiotherapy for spinal cord compression/impingement-a narrative review. Ann Palliat Med. 2023, 12,6, 1447-1462. [CrossRef] [PubMed]
- Gojsevic M, Shariati S, Chan AW, Bonomo P, Zhang E, Kennedy SKF, Rajeswaran T, Rades D, Vassiliou V, Soliman H, Lee SF, Wong HCY, Rembielak A, Oldenburger E, Akkila S, Azevedo L, Chow E; EORTC Quality of Life Group. Quality of life in patients with malignant spinal cord compression: a systematic review. Support Care Cancer. 2023, 31,12,736. [CrossRef] [PubMed]
- Vistad I, Cvancarova M, Kristensen GB, Fosså SD. A study of chronic pelvic pain after radiotherapy in survivors of locally advanced cervical cancer. J Cancer Surviv. 2011, 5,2,208-16. [CrossRef] [PubMed] [PubMed Central]
- Robijns J, Censabella S, Bollen H, Claes S, Van Bever L, Becker J, Pannekoeke L, Bulens P, Van de Werf E. Vaginal mucositis in patients with gynaecological cancer undergoing (chemo-)radiotherapy: a retrospective analysis. J Obstet Gynaecol. 2022, 42,6,2156-2163. [CrossRef] [PubMed]
Figure 1.
Various biological effects of low-dose-radiotherapy (LDRT) on tissue in chronic inflammatory joint diseases.
Figure 1.
Various biological effects of low-dose-radiotherapy (LDRT) on tissue in chronic inflammatory joint diseases.
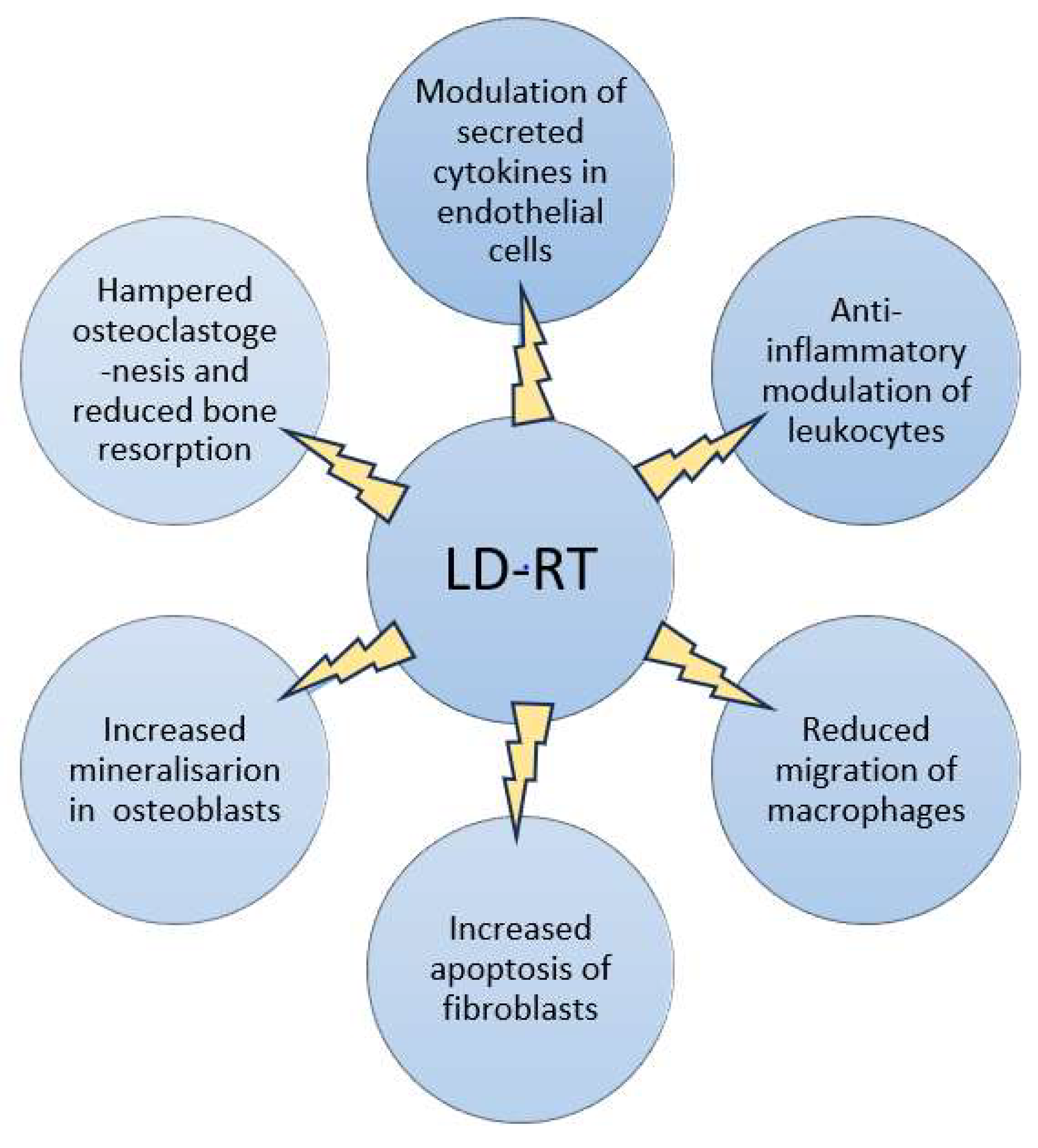
Figure 2.
The Patho-mechanisms of pain induced by radiotherapy (RT).
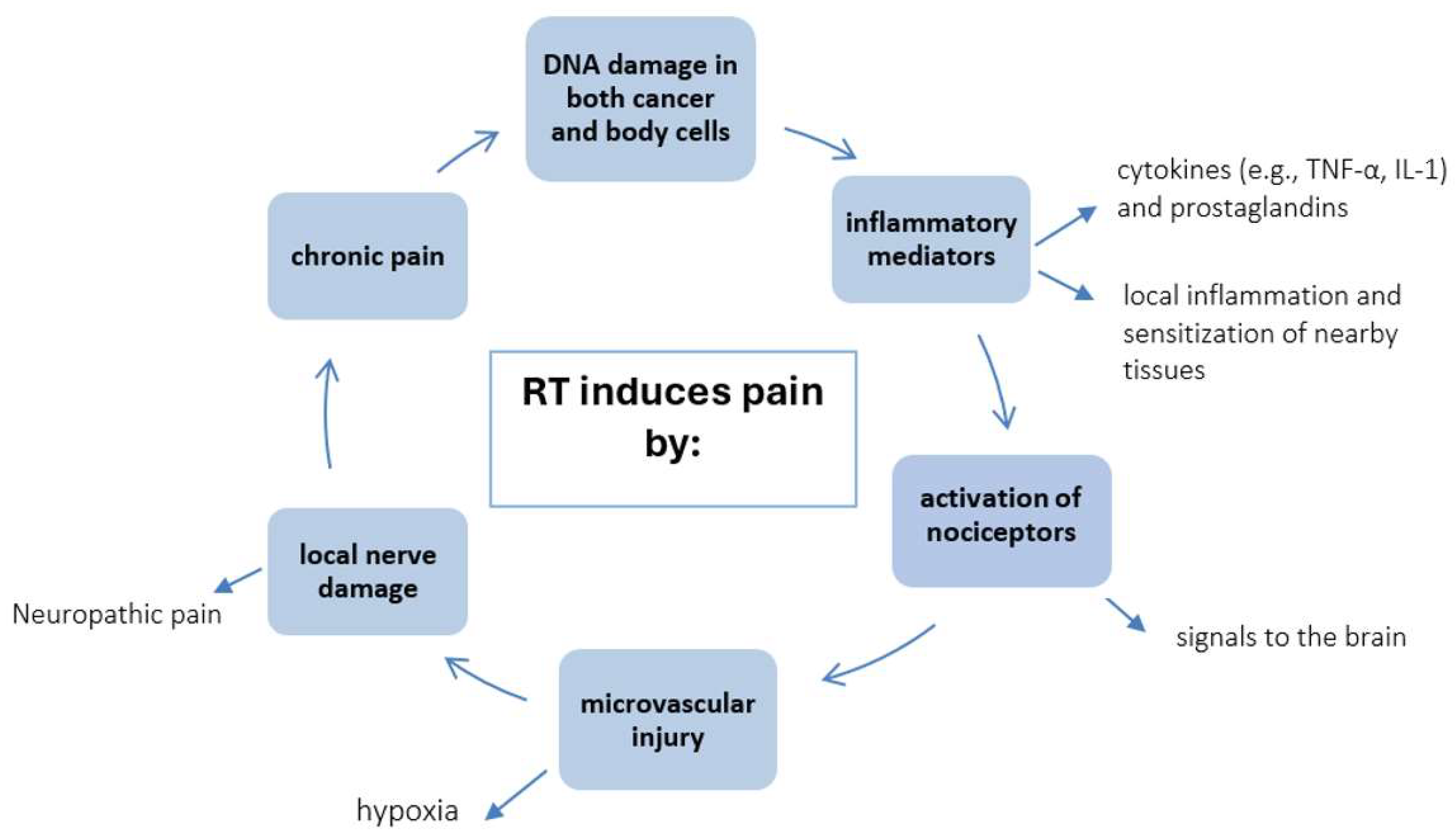

Table 1.
Types of brachytherapy categorized according to the methods used for placement of the applicator.
Table 1.
Types of brachytherapy categorized according to the methods used for placement of the applicator.
| Type of brachytherapy | Location of applicator |
| interstitial | the applicator is placed inside the tumor e.g., prostate cancer [9] |
| surface | a contact applicator used in the treatment of skin cancers [10] |
| intracavitary | the radiation source is placed within body cavities, e.g., in the uterus, oral cavity cancers or spinal canal cancers [11] |
| intraluminal | an applicator is inserted into the lumen of a cancer-infiltrated bronchus, e.g., irradiation of an intrabronchial lesion leads to its reduction and improved bronchial patency, thereby decreasing dyspnea and cancer pain [12] |
| intraoperative | an applicator is placed in the post operative cavity, e.g., following removal of a breast tumor [13] |
Table 2.
Radionuclides used in cancer pain relief.
| Radionuclide | Cancer | Indicate | Pain relief effect | Pain-free period |
| Strontium-89 Chloride | Prostate [24,25] breast26, lung, head and neck, colorectal [27] |
Bone pain | 63–88% | 6 weeks – 6 months |
| Samarium-153- EDTMP | lung, prostate [28,29] breast, osteosarcoma30 |
Bone pain | 62–78% | 3–8 months |
| Radium-223- Dichloride | Prostate [31,32] | Castration resistant prostate bone pain |
41-72% | Up to 16 weeks |
| Rhenium-186- HEDP | Prostate [33], breast [34] | Bone pain | 38% and 82% | 5–12 months |
| Rhenium-188- HEDP | Prostate [35,36] | progressive hormone- resistant prostate carcinoma and bone pain |
64-76% | 6 weeks |
Table 3.
Clinical studies demonstrating the analgesic effect of irradiation painful bone metastases depending on various dose and radiotherapy fractionation.
Table 3.
Clinical studies demonstrating the analgesic effect of irradiation painful bone metastases depending on various dose and radiotherapy fractionation.
| Study | RT scheme |
Complete pain response |
Partial pain response |
| Steenland et al., 1999 [102] |
1 × 8 Gy 6 × 4 Gy |
72% 69% |
37% 33% |
| Koswing et al., 1999 [103] |
1 × 8 Gy 10 × 3 Gy |
79% 82% |
31% 33% |
| Roos et al., 2005 [104] | 1 × 8 Gy 10 × 3 Gy |
61% 53% |
15% 18% |
| Hartsell et al., 2005 [105] |
1 × 8 Gy 10 × 3 Gy |
65% 66% |
15% 18% |
| Foro Arnalot et al., 2008 [106] |
1 × 8 Gy 10 × 3 Gy |
75% 86% |
15% 13% |
| Nongkynrih et al., 2018 [107] | 1 × 8 Gy 5 × 4 Gy 10 × 3 Gy |
80% 75% 85% |
20% 20% 20% |
| Nguygen et al., 2019 [108] |
1 x 12Gy-16 Gy 10 x 3 Gy |
55% 34% |
52% 19% |
| Ryu et al., 2023 [112] | 1 x 16-18 Gy 1x 8 Gy |
60% 41% |
- |
| Nguygen et al., 2023 [109] | 2x 12 Gy | 83-94% | - |
Table 4.
Radiotherapy (RT) as both a painkiller and a pain factor in various clinical situations.
| Radiotherapy as a double-edged sword - examples | |
| Painkiller in: | Pain Factor: |
|
|
|
|
|
|
|
|
|
|
|
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



