
Submitted:
02 January 2025
Posted:
04 January 2025
You are already at the latest version
Abstract
Objectives: The objectives of this study were: to determine mean percentages of measles vaccination coverage with two, one and zero doses of vaccine and anti-measles herd immunity levels in World Health Organization (WHO) regions in 2023; to assess variations in measles vaccination coverage and anti-measles herd immunity-related indicators from 2019 to 2023; and to assess whether zero-dose measles vaccination coverage indicators were on track to achieve the Immunization Agenda 2030 objective. Methods: Mean percentages of vaccination coverage with two, one and zero doses of measles vaccine in WHO regions in 2023 were calculated using data from the WHO/UNICEF global and regional immunization information system. Results: In 2023, the global mean two-dose measles vaccination coverage was 65.3%, and mean two-dose vaccination coverage were lower than 95% in all WHO regions; the mean prevalence of measles protected individuals in the target vaccination population was 87.6%; and anti-measles herd immunity levels in the target vaccination population were sufficient to block the transmission of measles viruses with greater transmissibility (Ro ≥ 15) only in the Western Pacific and European WHO regions. The global mean two-dose measles vaccination coverage decreased by 3.7% from 2019 to 2023. In 2023, the mean zero-dose measles coverage and number of zero-dose measles children and were 36.7% and 40.6% greater than their values required to be on-track to achieve the 2030 objective. Conclusion: This study found that all measles vaccination coverage-related indicators worsened from 2019 to 2023, and the zero-dose measles vaccination coverage and number of zero-dose measles children in 2023 were not on track to achieve the AI2030 objective. Interventions to increase routine two-dose measles vaccination coverage should be developed in all WHO regions.
Keywords:
Measles vaccination
; measles elimination and eradication
; WHO regions
; two-dose measles coverage
; MCV1
; MCV2
; measles zero-dose coverage
; anti-measles herd immunity
; measles prevention strategies
1. Introduction
In 2020, the 73rd World Health Assembly endorsed the Immunization Agenda 2030 (IA2030), envisioning “a world where everyone, everywhere, at every age, fully benefits from vaccines for good health and well-being” [1]. In 2011, the Global Vaccine Action Plan was proposed to eliminate measles in at least five WHO regions by 2020 [2]. The IA2030 agenda has committed to eliminating measles in at least five of the six WHO regions by 2030 [1].
The elimination of measles from all WHO and UNICEF regions is feasible because humans are the only reservoir for measles, effective vaccines are available, highly sensitive and specific diagnostic tests are available, endemic measles transmission was interrupted in America in 2016 and 83 countries were verified as having eliminated measles in 2019 [2,3]. Unfortunately, measles cases and outbreaks occurred in all WHO regions and measles elimination was not sustained in any region during 2012−2023 [4,5,6,7,8]. The Americas region lost its elimination status in 2019 and no WHO region has been verified as having eliminated measles since 2019 [2,3,4,5]. In the Americas region, measles reemerged in Brazil and Venezuela in 2018 [4,5]. In the European region, a total of 9010 measles cases, 4259 hospitalizations, and 2 deaths due to measles were reported by European countries to the WHO’s centralized information system for infectious diseases (CISID) in 2023 [6,7,8].
The strategic plan proposed by the WHO considers that achieving and maintaining percentages of vaccination coverage of at least 95% with two doses of the measles containing vaccine (MCV) is a key intervention to achieve measles elimination and eradication [9,10,11,12]. Routine measles vaccination is based on two doses of measles-mumps-rubella (MMR) vaccine. Children receive their initial measles vaccine when they are 12–15 months old and the second dose when they are 3–15 years old [9,12,13,14,15]. The objective of this strategy is to protect vaccinated individuals and to achieve and maintain a proportion (or prevalence) of protected individuals sufficient to establish the necessary herd immunity to block measles transmission in the community [9,10,11,12]. It is assumed that the percentages of measles vaccination coverage proposed by the WHO can generate and maintain sufficient anti-measles herd immunity levels to block the transmission of measles viruses in the population [10,11,16].
A study carried out in 2019 [10] found mean percentages of two-dose measles vaccination coverage lower than 90% in all regions of the WHO: 38.8% in the African region; 71–73% in the Americas, Eastern Mediterranean, and Western Pacific regions; and 81–83% in the European and South-East Asia regions. These results were explained by the very low percentage −only 14.4%− of countries with ≥95% two-dose measles vaccination coverage worldwide, ranging from 2.1% in the African region to 14–27% in the other WHO regions [10]. In 2019, anti-measles herd immunity levels in the target vaccination population against measles viruses with Ro values of 18 were established in 32.5% of countries worldwide. However, herd immunity levels were not sufficient against measles viruses with Ro ≥ 10 in the African and Eastern Mediterranean regions, against measles viruses with Ro ≥ 11 in the Western Pacific region, and against measles virus with Ro ≥ 13 in the Americas, European, and South-East Asia regions [10].
The objectives of this study were: 1) to determine the vaccination coverage for two, one and zero doses of measles vaccine and anti-measles herd immunity levels in countries and WHO regions in 2023; 2) to assess variations in measles vaccination coverage and anti-measles herd immunity-related indicators in WHO regions from 2019 to 2023; and 3) to assess whether zero-dose and measles vaccination coverage indicators were on track to achieve the Immunization Agenda 2030 objective.
2. Methods
2.1. Mean Percentages of Routine Measles Vaccination Coverage in Regions of the WHO in 2023
The mean percentages of vaccination coverage for the first and second dose of measles-containing vaccine (MCV1, MCV2) were determined for different regions of the WHO using the information from the WHO/UNICEF global and regional immunization information system [17]. WHO considers six regions: African region, Americas region, Eastern Mediterranean region, European region, South-East Asia region and Western Pacific region (WPR) [2,17].
WHO and UNICEF estimate coverage with the first and second measles containing vaccine (MCV1 and MCV2) doses delivered by routine immunization services for all countries, using annual administrative estimates and vaccination coverage surveys [18]. Percentages of vaccination coverage for the MCV1 vaccine in different countries were estimated among children aged 1 year or among children aged 2 years, when the MCV1 was given to children aged ≥ 1 year [18]. Percentages of vaccination coverage for the MCV2 vaccine in different countries were estimated among children at the recommended age, according to national immunization schedules [18].
2.2. Mean Vaccination Coverage with Zero, One and Two Doses of Measles Vaccine in the WHO Regions in 2023
The mean percentages of vaccination coverage with zero, one and two doses of measles vaccine were determined in the world, WHO regions from the vaccination coverage with zero, one and two doses of measles vaccine in different countries [10]. The two-dose measles vaccination coverage (V2) was determined in each country from the vaccination coverage with the second dose of measles-containing vaccine (MCV2) in 2023 and the vaccination coverage with the first dose of measles-containing vaccine (MCV1) in 2021 (MCV2 x MCV1) [10]. This calculation was based on the recommendation that measles containing vaccines (measles-rubella-mumps or MMR vaccine) must be administered at 12–15 months (MCV1 vaccine) and 3 years of age (MCV2 vaccine) [1,13,15]. Consequently, individuals vaccinated with two doses of routine measles vaccine in 2023 must have received the MCV2 vaccine in 2023 and the MCV1 vaccine in 2021.
The vaccination coverage with one dose of measles vaccine (V1) in the target vaccination population was determined in each country from the two-dose vaccination coverage, MCV1 coverage and MCV2 coverage (V1 = (MCV1 – V2) + (MCV2 – V2)) [10]. The zero-dose vaccination coverage (V0) was determined from the one dose and two-dose measles vaccination coverage (V0 = 100 – V1 – V2) [10].
2.3. Anti-Measles Herd Immunity Levels in the Target Vaccination Population in the WHO Regions in 2023
Anti-measles herd immunity levels in the target vaccination populations were determined in countries of the world in 2023 from the vaccination coverage with one and two doses of measles vaccine in the target vaccination population, and the effectiveness for one a two doses of measles vaccine [10]. Anti-measles herd immunity levels in the target vaccination populations were determined in different WHO regions in 2023 from the country-based mean vaccination coverage with one and two doses of measles vaccine in the target vaccination population, and the effectiveness for one a two doses of measles vaccine [10]. In this study, values of effectiveness in preventing measles cases of 92% and 95% were assumed for one and two doses of measles vaccine [19].
Anti-measles herd immunity levels in the target population vaccination against measles viruses with Ro values from 10 to 20 were assessed in countries and WHO regions. Herd immunity against measles viruses with Ro values equal to or lower than 10, 11, 12, 13, 14, 15, 16, 17, 18, 19 and 20 was considered established in a region when its country-based mean prevalence of individuals with vaccine-induced measles protection in the target population vaccination was higher than 90%, 90.9%, 91.7%, 92.3%, 93.3%, 93.7%, 94.4%, 94.1%, 94.7% and 95%, respectively [10,11].
Anti-measles herd immunity levels in different WHO regions were also assessed by determining the percentage of countries in each region with sufficient herd immunity against measles viruses with Ro from 10 to 20. Herd immunity considered established in a country against measles viruses with Ro values equal to or lower than 10, 12, 15, 18, 19, and 20 was when its prevalence of individuals with vaccine-induced measles protection in the target population vaccination was higher than 90%, 91.7%, 93.3%, 94.4%, 94.7% and 95%, respectively [10,11].
2.4. Assessment of Whether Zero-Dose Measles Vaccination Indicators in 2023 Were on Track to Achieve the Immunization Agenda 2030 Objective
In this study, tracks required from 2019 to 2030 to achieve a 50% reduction by 2030 were determined for three zero-dose measles coverage indicators: 1) estimated number of children who did not receive the first dose of measles containing vaccine (MCV1) [20]; 2) mean MCV1-based zero dose coverage; and 3) mean zero-dose coverage determined from two-dose measles vaccine coverage [10].
Immunization Agenda 2030 proposes a 50% reduction in the number of zero-dose children observed in 2019 by 2030 [20]. For operational purposes, WHO/UNICEF defines zero-dose children for measles vaccination as those who lack the MCV1 vaccine [20]. The track required from 2019 to 2030 to achieve the AI2030 objective of number of zero-dose children was determined by considering the WHO/UNICEF estimated number of children who did not receive the MCV1 vaccine in 2019 (22.2 million) [20], and a 50% lower number (9.65 million) in 2030. To assess whether the number of zero-dose children was on-track to achieve the 2030 goal, the estimated number of zero-dose children in 2023 was compared with the number required to be on-track.
The track required from 2019 to 2030 for mean MCV1-based zero-dose measles coverage to achieve a 50% reduction by 2030 was determined by considering the mean MCV1-based zero-dose coverage (12.4%) observed in 2019 [10] and a 50% lower coverage (6.2%) in 2030. This analysis can be considered similar to the analysis based on the number of zero-dose measles children because WHO/UNICEF estimates the number of zero-dose children from 100 − MCV1 coverage [4,20]. To assess whether the zero-dose measles coverage in 2023 was on-track to achieve the 2030 goal, the coverage in 2023 was compared with the coverage required to be on-track.
The track required to achieve a 50% reduction from 2019 to 2030 for zero-dose measles coverage (from two-dose and one-dose coverage) was determined by considering the mean zero-dose coverage obtained in 2019 (12.4%) [10] and a 50% lower level in 2030 (6.2%). To assess whether the mean zero-dose measles coverage in 2023 was on-track to achieve the 2030 goal, the coverage in 2023 was compared with the mean two-dose coverage required to be on-track.
2.5. Statistical Analysis
Microsoft Excel (Microsoft Corporation, Redmond, WA, USA) was used to calculate: 1) the mean percentage of vaccination coverage with the MCV1 and MCV2 vaccines in 2023 in different WHO regions; 2) the percentages of vaccination coverage with two, one and zero doses of measles vaccine in different countries of the world; 3) the mean percentages of vaccination coverage with two, one and zero doses of measles vaccine in regions of the WHO; 4) the prevalence of vaccine-induced measles protection in individuals in the target measles vaccination population in different countries of the world on 2023; and 5) the mean prevalence of vaccine-induced measles protected individuals in the target measles vaccination population in regions of the WHO. Microsoft Excel (Microsoft Corporation, Redmond, WA, USA) was used to assess the establishment of herd immunity against measles viruses in countries of the world and regions of the WHO in 2023.
3. Results
3.1. Mean Percentages of Routine Measles Vaccination Coverage in Countries of the World and Regions of the WHO in 2023
In the World, in 2023, the mean vaccination coverage for the first (MCV1) and second (MCV2) doses of measles vaccines were 85.2 and 77.1%, respectively (Table 1). The mean vaccination coverage for the first dose of measles vaccine was 83.3% in 2021 (Table 1). In 2023, the mean vaccination coverage for the first (MCV1) and second (MCV2) doses of measles vaccines were 85.2 and 77.1%, respectively (Table 1). The mean vaccination coverage for the first dose of measles vaccine was 83.3% in 2021 (Table 1).
In 2023, the mean percentages of vaccination coverage with the MCV1 and MCV2 vaccines were lower than 95% in all WHO regions, except the Western Pacific region (97%) for the MCV1 vaccine (Table 1). In 2021, the mean percentages of vaccination coverage with the MCV1 vaccine were lower than 95% in all WHO regions, except the South East Asia region (98%) and the Western Pacific region (97.5%) (Table 1).
3.2. Mean Percentages of Vaccination Coverage with Two, One and Zero Doses of Measles Vaccines in the World and Regions of the WHO in 2023
In the world, in 2023, the mean percentages of vaccination coverage with two, one and zero doses of measles vaccine were 65.3%, 27.8% and 6.9%, respectively (Table 2).
The global mean two-dose measles vaccination coverage found in this study (65.3%) was 31% lower than the 95% objective proposed by the WHO. The two-dose measles vaccination coverage was ≥ 95% in only 17 (8.7%) countries of the world, and it was ≥ 90% in 41 (21%) countries (Table 2).
In the WHO regions, the mean vaccination coverage with two doses of measles vaccine ranged from 48.1% in the African region to 93.2 in the Western Pacific region (Table 2). The mean vaccination coverage with one dose of measles vaccine ranged from 6.7% in the Western Pacific region to 46.5% in the Western Pacific region (Table 2). The mean vaccination coverage with zero doses of measles vaccine ranged from <1% in the Western Pacific, South-East Asia and European regions to 21.1% in the African region (Table 2).
The percentage of countries with ≥ 95% two-dose measles vaccination coverage ranged from 0% in the African region to 22.7% in the Eastern Mediterranean region (Table 2). The percentage of countries with ≥ 90% two-dose measles vaccination coverage ranged from 0% in the African region to 40.9% in the Eastern Mediterranean region (Table 2).
The percentage of countries where all children in the target vaccination population had received one or two doses of measles vaccine ranged from 0% in the African region to 22.7% in the Eastern Mediterranean region (Table 2).
3.3. Anti-Measles Herd Immunity Levels in Countries of the World and Regions of the WHO in 2023
In 2023, the global mean prevalence of individuals with vaccine-induced measles protection in the target measles vaccination population was 87.6% (Table 2). Based on the global mean prevalence of vaccine-induced measles protection in the target vaccination population, anti-measles herd immunity was not established in the world against measles viruses with Ro ≥ 10, because the mean prevalence of individuals with vaccine-induced measles protection (87.6%) was lower than the critical prevalence of 90% required against measles viruses with a Ro value of 10 (Table 2).
Anti-measles herd immunity was established in 129 (66.1%) countries of the world against measles viruses with Ro ≤ 10; in 81 (41.5%) countries against measles viruses with Ro ≤ 15; in 25 (12.8%) countries against measles viruses with Ro ≤ 19, and it was not established in any country against measles viruses with Ro ≥ 20 (Table 2).
The mean (per country) prevalence of measles protection ranged from 74% in African region to 94.1 in the European region and 94.6% in the Western Pacific region (Table 2). Based on the regional mean prevalence of vaccine-induced measles protection, anti-measles herd immunity levels in the target vaccination population were not sufficient to block the transmission of measles viruses with greater transmissibility (Ro ≥ 15) only in the Western Pacific and European WHO regions. Anti-measles herd immunity was established against measles viruses with Ro ≤ 18 (94.4% required) in the West Pacific region; against viruses with Ro ≤ 16 (93.7% required) in the European region; against viruses with Ro ≤ 14 (92.9% required) in the South-East Asia region; against viruses with Ro ≤ 12 (91.7% required) in the Americas region; and against viruses with Ro ≤ 11 (90.9% required in the Eastern Mediterranean region (Table 2). Anti-measles herd immunity was not stablished against measles viruses with Ro ≥ 19 because the required protection prevalence of 94.7% was greater than the mean prevalence achieved in any region (Table 2). In the African region, anti-measles herd immunity was not established against viruses with Ro ≥ 10 because its mean measles protection prevalence was lower than the required prevalence of 90% (Table 2).
The Eastern Mediterranean, Europe, South-East Asia and Western Pacific regions had the best country-based anti-measles herd immunity profiles, while the African region had the worst profile (Table 2). In the Eastern Mediterranean region, herd immunity was established in 15 (68.2%) countries against measles with Ro ≤ 10, in 11 (50%) countries against measles viruses with Ro ≤ 15, and in 7 (31.8%) countries against measles viruses with Ro ≤ 19 (Table 2). By contrast, in the African region, herd immunity was established in 19 (40.4%) countries against measles with Ro ≤ 10, in 5 (10.6%) country against measles with Ro ≤ 15, and in any (0%) country against measles viruses with Ro > 15 (Table 2).
3.4. Variation for Routine Measles Vaccination-Related indicators in Countries of the World and Regions of the WHO from 2019 to 2023
The study found that five measles vaccination coverage-related indicators worsened and one indicator improved from 2019 to 2023 (Table 3).
The mean global two-dose measles vaccination coverage decreased by 3.7% and the mean global zero-dose measles vaccination coverage increased by 7.8% from 2019 to 2023 (Table 3).
The percentage of countries with two-dose measles vaccination coverage ≥ 95% and ≥ 90% decreased by 39.6% and 18.6%, respectively, from 2019 to 2023 (Table 3). The percentage of countries where all children had received at least dose of measles vaccine decreased by 24.8% from 2019 to 2023 (Table 3). The mean global one-dose vaccination coverage improved by 7.8% from 2019 to 2023 (Table 3).
The global mean two-dose measles vaccination coverage decreased from 2019 to 2023 in the South-East Asia, Eastern Mediterranean and Americas regions, while it improved in the other regions (Table 3). The variation for this indicator ranged from −35% in the South-East Asia region to 30.9% in the Western Pacific region (Table 3).
The mean zero-dose measles vaccination coverage decreased from 2019 to 2023 in all WHO regions except in the African region (Table 3). The variation for this indicator ranged from −96.5% in the Western Pacific region to 24.9% in the African region (Table 3).
The percentage of countries with two-dose measles vaccination coverage ≥ 95% decreased between 2019 and 2023 in all WHO regions (Table 3). The variation for this indicator ranged from −4.6% in the Eastern Mediterranean region to −100% in the African region (Table 3).
The percentage of countries with two-dose measles vaccination coverage ≥ 90% decreased between 2019 and 2023 in all WHO regions, except in the Eastern Mediterranean and South-East Asia regions (Table 3). The variation for this indicator between 2019 and 2023 ranged from 7.3% in the Eastern Mediterranean region to −100% in the African region (Table 3).
The percentage of countries without children with zero-dose children for measles vaccination decreased from 2019 to 2023 in all WHO regions, except in the Europe and Western Pacific regions (Table 3). The variation for this indicator between 2019 and 2023 ranged from 0% in the Europe and Western Pacific regions to −100% in the African region (Table 3).
3.5. Variation for Anti-Measles herd Immunity-Related Indicators in Countries of the World and Regions of the WHO from 2019 to 2023
The study found that all anti-measles herd immunity-related indicators assessed in this study decreased in the world from 2019 and 2023 (Table 3). The global mean prevalence of individuals in the target vaccination population with vaccine-induced measles immunity decreased by 0.6% from 2019 to 2023 (Table 3). The percentage of countries with herd immunity against measles viruses with transmissibility levels (Ro values) equal to or lower than 10, 12, 15, 18 and 19 decreased from 2019 to 2023 by 6.4%, 7.7%, 19.4%, 28.9% and 100%, respectively (Table 3). The percentage of countries with herd immunity against measles viruses with transmissibility levels equal to or higher than 20 found in 2023 (0%) did not vary from 2019 (Table 3).
The mean prevalence of individuals in the target vaccination population with vaccine-induced measles immunity increased in the Western Pacific, Eastern Mediterranean, European and Americas regions, while it decreased in the Africa and South-Esat Asia regions between 2019 and 2023 (Table 3). The variation for this indicator between 2019 and 2023 ranged from 6.5% in the Western Mediterranean region to −4.6% in the African region (Table 3).
The indicator percentage of countries with herd immunity against measles viruses with Ro values from 10 to 20 worsened in all WHO regions from 2019 to 2023 (Table 3). In the African, Americas and European regions, the percentage of countries with herd immunity against measles viruses with Ro values from 10 to 19 decreased from 2019 to 2023, with 7.4−100% decreases in the African region, 15−67% decreases in the Americas region, and 2−22% decreases in the European region (Table 3). In the Western Pacific region, the percentage of countries with herd immunity against measles viruses with Ro values from 10 to 18 decreased by 11−18% from 2019 to 2023, while it did not vary against viruses with Ro value of 19 (Table 4). In the Eastern Mediterranean region, the percentage of countries with herd immunity against measles viruses with Ro values from 18 to 18 increased by 11−19% and it decreased by 4.5% against viruses with Ro values from 12 to 15 (Table 3). In the South-East Asia region, the percentage of countries with herd immunity against measles viruses with Ro values from 10 to12 decreased by 11−12%, increased by 16.7% against viruses with Ro values of 15, decreased by 33% against viruses with Ro values of 18 and did not vary against viruses with Ro values of 19 (Table 3).
3.6. Assessment of Whether Zero-Dose Measles Vaccination Indicators in 2023 Were on Track to Achieve the IA2030 Objective Reduction by 2030
In 2023, the three indicators of zero-dose measles coverage assessed in this study were not on track to achieve a 50% reduction in their 2019 values by 2030. The number of zero-dose measles children estimated by the WHO/UNICEF, the mean MCV1-based zero-dose coverage and the two-dose measles coverage were 40.6%, 46,5% and 36.7% greater than their values required to be on-track to achieve the 2030 objective (Figure 1, Figure 2).
The number of zero-dose measles children estimated by WHO/UNICEF in 2023 (22.2 million) [20] was not on track to achieve the 2030 objective of 9.65 million (Figure 1). To be on-track, the number of zero-dose measles children should be reduced by 877,273 per year from 2019 to 2030 (Figure 1). The number of zero-dose measles children estimated in 2023 was 40.6% greater than the number required (15.8 million) to be on-track. The number of zero-dose measles children estimated by WHO/UNICEF for 2020 (22.3 million), 2021 (24.7 million) and 2022 (21.9 million) [4,20,21] were also out of track to achieve the IA2030 objective (Figure 1)
In 2023, the mean zero-dose measles vaccination coverage determined from the mean MCV1 coverage (14.8%) was not on track to achieve the 2030 objective of 6.2% (Figure 2). To be on-track, the MCV1-based zero-dose coverage should be reduced by 0.56% per year from 2019 to 2030. In 2023, the mean MCV1-based zero-dose coverage was 46.5% greater than the coverage required (10.1%) to be on track to achieve the 2030 objective (Figure 2). The mean MCV1-based zero-dose coverage in 2020, 2021 and 2022 were also out-off track (Figure 2).
In 2023, the mean zero-dose measles vaccination coverage determined from the coverage for two and one doses of measles vaccine (6.9%) was not on track to achieve the 2030 objective of 3.2% (Figure 2). To be on-track, the zero-dose coverage should be reduced by 0.29% per year from 2019 to 2030. In 2023, the mean zero-dose coverage was 36.7% greater than the coverage required (5.2%) to be on track to achieve 2030 (Figure 2). The mean zero-dose coverage in 2020, 2021 and 2022 were also out-off track (Figure 2).
4. Discussion
This study found four key results for 2023: 1) the global means for two-dose, one-dose and zero-dose measles vaccination coverage were 65.3%, 27.8% and 6.9%, respectively; 2) mean percentages of two-dose measles vaccination coverage were lower than ≥ 95% in all WHO regions; 3) the mean prevalence of measles protected individuals in the target vaccination population was 87.6%; and 4) anti-measles herd immunity levels in the target vaccination population was sufficient to block the transmission of measles viruses with greater transmissibility (Ro ≥15) only in the Western Pacific and European WHO regions.
In addition, this study found that measles vaccination coverage and anti-measles herd immunity-related indicators worsened from 2019 to 2023. The mean measles vaccination coverage increased by 7.8%. The percentage of countries with two-dose measles vaccination coverage ≥ 95% decreased by 39.6%. The mean prevalence of measles- protected individuals in the target vaccination population decreased by 0.6%. The mean MCV1 coverage and the number of zero-dose measles vaccine children in 2023 were not on track to achieve the AI2030 objective of zero-dose measles vaccination coverage.
The global mean (per country) two-dose routine measles vaccination coverage found in this study in 2023 was lower than the 95% vaccination coverage objective proposed by the WHO, and was 3.7% lower than in 2019 (65.3% vs. 67.8%). The low worldwide mean two-dose measles vaccination coverage can be explained by very low percentages of two-dose routine measles vaccination coverage in countries in the African (mean 48%) and South-East Asia (mean 53%) regions of the WHO, while the mean two-dose percentages of vaccination coverage in other WHO regions ranged from 65% to 93%.
In addition, the study found that the percentage of countries with two-dose measles vaccination coverage ≥ 95% in 2023 was only 8.7% worldwide, with 0% of countries in the African region, 3−10% of countries in the Americas, European and South-East Asia regions and 15−23% of countries in the Western Pacific and Eastern Mediterranean regions of the WHO. These results showed that achieving ≥95% two-dose measles vaccination coverage is a priority objective for vaccination programs in all countries and WHO regions.
This study found that the global mean (per country) prevalence of individuals with anti-measles immune protection in the target vaccination population in 2023 (87.6%) was not sufficient to block the transmission of measles viruses with a transmissibility of 10 because it was lower than the 90% prevalence required to establish herd immunity. Nevertheless, the situation differed greatly among the WHO regions. In the European and Western Pacific regions, the mean prevalence of protected individuals was sufficient to establish herd immunity against measles viruses with low, moderate and high transmissibility (Ro ≤ 16−18). In the South East Asia region, the mean prevalence was sufficient to establish herd immunity against measles viruses with moderate transmissibility (Ro ≤ 14). In the Eastern Mediterranean and Americas regions, the mean prevalence was sufficient to establish herd immunity against measles viruses with low transmissibility (Ro ≤ 11−12). The situation in the African region was critical, as its mean prevalence was not sufficient to establish herd immunity against measles viruses with low, moderate or high transmissibility (Ro ≥ 10).
The global mean zero-dose measles vaccination coverage found in this study in 2023 was 6.9%, and it increased by 7.8% from 2019 to 2023. The worldwide mean zero-dose measles coverage found in 2023 can be explained by the high mean zero-dose coverage in countries in the African region (21.1%), which contrasted with the <3% mean zero-dose coverage in the other WHO regions. The 7.8% increase in this indicator between 2019 and 2023 can be explained by the 24.9% increase in the African region. In fact, the mean zero-dose measles coverage improved in all WHO regions from 2019 to 2023, except in the African region.
In addition, the study found that the percentage of countries with 0% zero-dose measles vaccination was only 9.7% worldwide. In these countries all children had received at least one dose of measles vaccine and the percentage of zero-dose children was 0%. The percentage of countries with 0% zero-dose children in the world in 2023 depended greatly on the situation in the African region, because any of its countries had 0% zero-dose children in 2023. In the other WHO regions, the percentage of countries with 0% zero-dose measles vaccine children ranged from 5.7% to 18%. These results showed that achieving 0% zero-dose children for measles vaccination should be a priority objective for vaccination programs in all countries and WHO regions.
Measles meets criteria for disease eradication, but the results found this study for 2023 showed that routine measles vaccination programs had not recovered from COVID-19 pandemic disruptions, and progress toward measles elimination in most countries and in all WHO regions has slowed. A similar result was found by WHO/UNICEF [20], and inadequate progress toward measles eradication were found in prior evaluations carried out in 2016 [22], 2019 [10], 2021 [21] and 2022 [4]. The midterm evaluation of the Global Measles Strategic Plan 2012–2020 carried out in 2016 [22] considered that progress toward measles eradication was inadequate in 2016 due to a lack of political will as well as country ownership, reflected in insufficient resources.
The IA2030 agenda has committed to eliminating measles in at least five of the six WHO regions by 2030 and one of the key IA2030 objectives is to reduce the number of measles zero-dose children registered in 2019 by 50% in 2030 [1,20]. However, this study found that the three indicators of zero-dose measles coverage assessed were not on track for achieving a 50% reduction from 2019 to 2030. In 2023, the number of zero-dose measles children estimated by the WHO/UNICEF, the mean MCV1-based zero-dose coverage and the two-dose measles coverage were 40.6%, 46,5% and 36.7% greater than their values required to be on-track to achieve the 2030 objective.
The strategic plan proposed by the WHO to achieve measles elimination and eradication includes two key vaccination measures: 1) to achieve and maintain ≥ 95% routine measles vaccination coverage with two doses of measles vaccine; and 2) to implement supplementary immunization activities (SIA) to population groups to reach individuals susceptible to measles [2,3]. However, achieving and maintaining a routine vaccination coverage with two doses of measles vaccine ≥ 95% must have a higher priority in all countries and WHO regions for three reasons. Firstly, achieving and maintaining a routine measles vaccination coverage≥ 95% can generate sufficient population immunity to establish anti-measles herd immunity in the community [10,11,23]. Secondly, it is a critical strategy in the path toward measles elimination because it could be achieved only in countries with strong measles vaccination programs and strong primary health care services [20,24]. Thirdly, the strategy to increase measles vaccination coverage with SIAs has limitations that makes it not sufficient for achieving and maintaining measles elimination [10,11,25].
In each country and WHO region, a routine measles vaccination coverage with two doses of measles vaccine coverage of at least 95% should be achieved in every birth cohort and in different areas and communities to ensure sufficient population immunity to establish anti-measles herd immunity against measles viruses [1−3,10,11,25]. Based on the results of this study, three measles prevention strategies should be developed depending on the two-dose routine measles vaccination coverage and anti-measles vaccine-induced herd immunity levels achieved in 2023. In the European and Western Pacific regions, the main objective should be to increase their 86−93% mean two-dose measles vaccination coverage to ≥95% to avoid cases and outbreaks generated by viruses imported from endemic countries.
In the Eastern Mediterranean, Americas, and South East Asia regions the main objective should be to increase their 53−72% mean two-dose measles vaccination coverage to ≥95% and to increase anti-measles herd immunity levels to block transmission of measles viruses with greater transmissibility.
In the African region, great efforts and international support are necessary to increase the two-dose measles vaccination coverage in the African region from 48% to ≥95%, reduce the number of zero-dose measles vaccine children and increase anti-measles herd immunity levels. This study found that insufficient global mean levels for measles vaccination-related and anti-measles herd immunity-related indicators depended greatly on the situation in the African region. Therefore, the global measles eradication objective depends greatly on improving the measles situation in the African region.
The following interventions can be used to increase routine two-dose measles vaccination coverage to ≥95% and to increase anti-measles herd immunity levels in all countries and WHO regions: 1) implement advanced vaccination programs [26,27]; 2) increase routine two-dose measles vaccination coverage from 95% to 97% [11]; 3) develop measles screening and vaccination programs to reach susceptible individuals and populations with low measles immunity levels [10,11,25,28,29]; 4) develop supplementary vaccination activities [20,30,31]; 4) implement interventions to increase measles vaccination access and vaccines provision [32]; 5) implement interventions to reduce measles vaccination hesitancy [33,34,35,36]; 6) implement interventions to increase healthcare provider engagement [37]; and 7) implement compulsory measles vaccination [38,39].
Advanced immunization information systems could be developed to detect unvaccinated individuals and to detect areas and population groups with low routine vaccination rates [26,27]. However, they would not be able to detect areas and population groups with low anti-measles herd immunity levels due to primary vaccine failure and waning vaccine-induced immunity [40].
Screening and vaccination programs can be developed to reach susceptible individuals and populations with low measles immunity levels. Currently, screening and vaccination programs are not implemented in European countries due to their logistic and economic challenges. However, they can achieve and maintain anti-measles herd immunity levels against measles viruses with greater transmissibility [10,11,25,28]. Seroprevalence studies in representative samples of the population, areas and population groups can be developed to guide screening and vaccination programs to achieve and maintain measles elimination in different countries and WHO regions [25].
Supplementary immunization activities (SIAs) can be developed to reach populations and areas with low percentages of vaccination coverage. SIAs based on catch-up and follow-up vaccination campaigns are currently implemented in countries with inadequate first and/or second measles vaccine doses coverage [20]. In 2022, 115 million people received measles vaccines through SIAs in 44 countries [4]. Catch-up SIAs include children aged 9 months−14 years and follow-up SIAs include children aged 9−59 months. SIAs are implemented to provide a second vaccination opportunity to an entire cohort with low measles vaccination coverage, and to protect children who are susceptible to measles due to primary MCV1 failure [2,20]. However, the strategy to increase measles vaccination coverage with SIAs has important economic and logistic limitations that makes it not sufficient for achieving and maintain measles elimination, such as that they are not able to detect and vaccinate all susceptible children [10,11,25]. A recent study [41] assessing the quality and results achieved with SIAs implemented since 2020, found a mean SIA coverage among previously measles zero-dose children was 58.3%, although only 23% of the 66 countries with a national-level SIA had a post-campaign coverage survey report available and 50% of the reports included the coverage achieved among previously measles zero-dose children [41]. The analysis of a high-quality anonymized database from a SIA carried out in Somalia in 2022 found that 94.6% of the children included in SIAs had been previously vaccinated with either one or 2+ measles doses, 5.4% of the children had received previously zero-doses of measles vaccine, and the SIA coverage was 92% among previously vaccinated children and only 37.2% among zero-dose children [41].
Parents attitudes and beliefs toward measles vaccination are of great importance in influencing measles vaccination [42,43]. Parents hesitancy to vaccinate their children can be attributed to concerns about vaccine efficacy and safety, measles susceptibility, measles severity, vaccine accessibility and mistrust in experts [33−35]. Health education activities and national vaccination information campaigns can be developed to fight against measles vaccination hesitancy to reduce misinformation about measles vaccine efficacy and safety and to improve trust in vaccines, health providers and vaccination programs. In the United States of America, National Immunization Awareness Month is an annual observance held in August to highlight the importance of vaccination for people of all ages [36]. These interventions can help raise awareness about the importance of vaccination and encourage people to talk to a healthcare provider they trust about staying up to date on their vaccinations.
Delaying measles elimination in countries and WHO regions makes it more difficult to achieve and maintain measles elimination and eradication in the world [44]. The widening measles vaccination coverage and measles immunity gaps among countries and WHO regions found in this study for the 2019−2023 period shows that the risk of measles outbreaks has increased in all countries and the probability of re-establishing measles transmission in countries where measles had eliminated is now greater than in 2019.
This study has several limitations. Firstly, the analysis carried out in this study used the information on routine vaccination of the WHO/UNICEF global and regional immunization systems. This information is subject to potential bias due to misreporting of percentages of routine vaccination coverage. However, the information reported by the WHO/UNICEF global and regional immunization systems is validated periodically by the World Health Organization [17,18,45]. Secondly, herd immunity levels in different countries of the world and WHO regions were assessed by comparing the prevalence of individuals with vaccine-induced protection and the critical prevalence blocking the transmission of measles viruses in the population. This method requires to assume homogeneous mixing of individuals within the population and homogeneous distribution of protected individuals within the population [10]. Thirdly, anti-measles herd immunity levels in different countries of the world and WHO regions were assessed against measles viruses with Ro values from 10 to ≥ 20. Anti-measles herd immunity levels would be greater against measles viruses with Ro values lower than 10. However, Ro values from 10 to 20 have been found in studies assessing the transmissibility of measles viruses [10,46].
5. Conclusions
The study found that worldwide percentages of two-dose measles vaccination coverage were lower than ≥ 95% and anti-measles herd immunity levels in the target vaccination population were not sufficient to block the transmission of measles viruses with greater transmissibility (Ro ≥ 15) only in the Western Pacific and European WHO regions. All measles vaccination coverage-related and anti-measles herd immunity-related indicators worsened from 2019 to 2023. The zero-dose measles coverage and number of zero-dose measles children found in 2023 were not on track to achieve the AI2030 objective. Interventions to increase routine two-dose measles vaccination coverage should be developed in all WHO regions to meet the goal of eradicating measles worldwide.
Funding
This research received no external funding.
Institutional Review Board Statement
The study did not require ethical approval.
Data Availability Statement
The original contributions presented in this study are included in the article/supplementary material. Further inquiries can be directed to the corresponding author.
Acknowledgments
Mean percentages of measles routine vaccination coverage in regions of the WHO were calculated using the information of the WHO on “WHO/UNICEF estimates of routine vaccines”: https://www.who.int/news-room/questions-and-answers/item/who-unicef-estimates-of-national-immunization-coverage.
Conflicts of Interest
The author declares no conflicts of interest.
References
- World Health Organization (WHO). Global Vaccine Action Plan; WHO: Geneve, Switzerland, 2020. Available online: https://www.who.int/publications/i/item/global-vaccine-action-plan-2011-2020 (accessed on 15 October 2024).
- WHO/UNICEF. Immunization Agenda 2030. A global strategy to leave no one behind. 5389. Available online: https://cdn.who.int/media/docs/default-source/immunization/strategy/ia2030/ia2030-draft-4-wha_b8850379-1fce-4847-bfd1-5d2c9d9e32f8.pdf?sfvrsn=5389656e_69&download=true (accessed on 15 October 2024).
- World Health Organization (WHO). Global Vaccine Action Plan: Monitoring, Evaluation and Accountability; Secretariat Annual Report 2020; WHO: Geneve, Switzerland, 2020; Available online: https://www.who.int/publications/i/item/global-vaccine-action-plan-monitoring-evaluationaccountability-secretariat-annual-report-2020.
- Minta, A.A.; Ferrari, M.; Antoni, S.; Portnoy, A.; Sbarra, A.; Lambert, B.; Hatcher, C.; Hsu, C.H.; Ho, L.L.; Steulet, C.; Gacic-Dobo, M.; Rota, P.A.; Mulders, M.N.; Bose, A.S.; Caro, W.P.; O’Connor, P.; Crowcroft, N.S. Progress Toward Measles Elimination - Worldwide, 2000-2022. MMWR Morb. Mortal. Wkly. Rep. 2023, 72, 1262–1268. [Google Scholar] [CrossRef] [PubMed]
- O’Connor, P.; Masresha, B.; Pastor, D.; Musa, N.; Hagan, J.; Khanal, S.; Lee, C.-W.; Crowcroft, N. Global Status Report for the Verification of Measles and Rubella Elimination, 2022. Vaccines 2024, 12, 947. [Google Scholar] [CrossRef] [PubMed]
- WHO; Centralized Information System for Infectious Diseases (CISID). Measles-number of cases, 2015–2023. Available online: http://data.euro.who.int/cisid/?TabID=523870 (accessed on 7 October 2024).
- WHO; Centralized Information System for Infectious Diseases (CISID). Measles-Number of hospitalizations. 2023. Available online: http://data.euro.who.int/cisid/?TabID=523869 (accessed on 7 September 2024).
- WHO; Centralized Information System for Infectious Diseases (CISID). Measles-Number of deaths. 2023. Available online: http://data.euro.who.int/cisid/?TabID=523871 (accessed on 7 October 2024).
- World Health Organization (WHO). Strategic Plan. for Measles and Congenital Rubella Infection in the WHO European Region; WHO Regional Office for Europe: Copenhagen, Denmark, 2003. [Google Scholar]
- Plans-Rubió, P. Vaccination Coverage for Routine Vaccines and Herd Immunity Levels against Measles and Pertussis in the World in 2019. Vaccines 2021, 9, 256. [Google Scholar] [CrossRef]
- Plans-Rubió, P. Are the Objectives Proposed by the WHO for Routine Measles Vaccination Coverage and Population Measles Immunity Sufficient to Achieve Measles Elimination from Europe? Vaccines 2020, 8, 218. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization (WHO). Strategic plan for measles and congenital rubella infection in the WHO European Region; WHO Regional Office for Europe: Copenhagen, Denmark, 2003. Available online: https://iris.who.int/handle/10665/107526 (accessed on 7 October 2024).
- European Centre for Disease Prevention and Control (ECDC). Measles: Recommended Vaccination. Available online: https://vaccine-schedule.ecdc.europa.eu/Scheduler/ByDisease?SelectedDiseaseId=8&SelectedCountryIdByDisease=-1 (accessed on 2 December 2024).
- Vanderslott, S.; Dathui, S.; Spooner, F.; Roser, M. Our World in Data. Vaccination. Available online: https://ourworldindata.org/vaccination (accessed on 2 December 2024).
- Rosenthal SR, Clements CJ. Two-dose measles vaccination schedules. Bull. World Health Organ 1993, 71, 421–428.
- Gay, N.J. The theory of measles elimination: implications for the design of elimination strategies. J Infect Dis 2004, 189 (Suppl 1), S27. [Google Scholar]
- UNICEF. WHO/UNICEF Estimates of Routine Vaccination Coverage. 2023. Available online: https://data.unicef.org/topic/child-health/immunization/ (accessed on 9 September 2024).
- Burton, A.; Monasch, R.; Lautenbach, B.; Gacic-Dobo, M.; Maryanne, N.; Karimov, R.; Wolfson, L.; Jones, G.; Birmingham, M. WHO and UNICEF estimates of national infant immunization coverage: Methods and processes. Bull. World Health Organ. 2009, 87, 535–541. [Google Scholar] [CrossRef] [PubMed]
- Demicheli, V.; Rivetti, A.; Debalini, M.G.; Di Pietrantonj, C. Vaccines for Measles, Mumps and Rubella in Children (Review). The Cochrane Library 2012, Issue 2. Available online: https://www.princeton.edu/~{}sswang/demicheli_pietrantonj12_cochrane_ report_MMR-risks.pdf (accessed on 22 July 2024).
- WHO-UNICEF. Progress and challenges with achieving universal immunization coverage. 9141. Available online: https://cdn.who.int/media/docs/default-source/immunization/wuenic-progress-and-challenges.pdf?sfvrsn=b5eb9141_12&download=true.
- Minta, A.A.; Ferrari, M.; Antoni, S.; Portnoy, A.; Sbarra, A.; Lambert, B.; Hauryski, S.; Hatcher, C.; Nedelec, Y.; Datta, D.; Ho, L.L.; Steulet, C.; Gacic-Dobo, M.; Rota, P.A.; Mulders, M.N.; Bose, A.S.; Perea, W.A.; O’Connor, P. Progress Toward Regional Measles Elimination - Worldwide, 2000-2021. MMWR Morb. Mortal. Wkly. Rep 2022, 71, 1489–1495. [Google Scholar] [CrossRef]
- Orenstein, W., A.; Cairns, L.; Hinman, A.; Nkowane, B.; Olivé, J.M.; Reingold, A.L. Measles and Rubella Global Strategic Plan 2012-2020 midterm review report: Background and summary. Vaccine 2018, 36 Suppl 1, A35–A42. [Google Scholar] [CrossRef]
- World Health Organization (WHO). Measles vaccines: position paper − Aprl 2017. Wkly. Epidemiol. Rep. 2017, 92, 205–227. [Google Scholar]
- Winter, A.K.; Moss, W.J. Possible Paths to Measles Eradication: Conceptual Frameworks, Strategies, and Tactics. Vaccines 2024, 12, 814. [Google Scholar] [CrossRef]
- Plans, P. New preventive strategy to eliminate measles, mumps and rubella from Europe based on the serological assessment of herd immunity levels is the population. Eur. J. Clin. Microbiol. Infect. Dis. 2013, 32, 961–996. [Google Scholar] [CrossRef]
- Pavia, G.; Branda, F.; Ciccozzi, A.; Romano, C.; Locci, C.; Azzena, I.; Pascale, N.; Marascio, N.; Quirino, A.; Matera, G.; Giovanetti, M.; Casu, M.; Sanna, D.; Ceccarelli, G.; Ciccozzi, M.; Scarpa, F. Integrating digital health solutions with immunization strategies: Improving immunization coverage and monitoring in the post-COVID-19 era. Vaccines 2024, 12, 847. [Google Scholar] [CrossRef]
- Stockwell, M.S.; Fiks, A.G. Utilizing health information technology to improve vaccine communication and coverage. Hum. Vaccin. Immunother. 2013, 9, 1802–1811. [Google Scholar] [CrossRef] [PubMed]
- Rabil, M.J.; Tunc, S.; Bish, D.R.; Bish, E.K. Benefits of integrated screening and vaccination for infection control. PLoS One 2022, 17, e0267388. [Google Scholar] [CrossRef] [PubMed]
- Rachlin, A.; Hampton, L.M.; Rota, P.A.; Mulders, M.N.; Papania, M.; Goodson, J.L.; Krause, L.K.; Hanson, M.; Osborn, J.; Kelly-Cirino, C.; et al. Use of Measles and Rubella Rapid Diagnostic Tests to Improve Case Detection and Targeting of vaccinations. Vaccines 2024, 12, 823. [Google Scholar] [CrossRef] [PubMed]
- Mokdad, A.H.; Gagnier, M.C.; Colson, K.E.; Dansereau, E.; Zuniga-Brenes, P.; Rios-Zertuche, D.; Haakenstad, A.; Johanns, C.K.; Palmisano, E.B.; Hernandez, B.; et al. Missed opportunities for measles, mumps, and rubella (MMR) immunization in Mesoamerica: Potential impact on coverage and days at risk. PLoS ONE 2015, 10, e0139680. [Google Scholar] [CrossRef]
- Ropero Alvarez, A.M.; Jane Kurtis, H.; Vulanovic, L.; Hasan, H.; Ruiz, C.; Thrush, E. The evolution of Vaccination Week in the Americas. Rev. Panam. Salud Publica 2017, 41, e150. [Google Scholar] [CrossRef]
- Szilagyi, P.G.; Schaffer, S.; Shone, L.; Barth, R.; Humiston, S.G.; Sandler, M.; Rodewald, L.E. Reducing geographical, racial, and ethnic disparities in childhood immunization rates by using reminder/recall interventions in urban primary care practices. Pediatrics 2002, 110, e58. [Google Scholar] [CrossRef]
- Kaufman, J.; Rak, A.; Vasiliadis, S.; Brar, N.; Atif, E.; White, J.; Danchin, M.; Durrheim, D.N. The Case for Assessing the Drivers of Measles Vaccine Uptake. Vaccines 2024, 12, 692. [Google Scholar] [CrossRef]
- Higgins, D.M.; O’Leary, S.T. A World without Measles and Rubella: Addressing the Challenge of Vaccine Hesitancy. Vaccines 2024, 12, 694. [Google Scholar] [CrossRef] [PubMed]
- Wilder-Smith, A.B.; Qureshi, K. Resurgence of measles in Europe: A systematic review on parental attitudes and beliefs of measles vaccine. J. Epidemiol. Glob. Health 2020, 10, 46–58. [Google Scholar] [CrossRef] [PubMed]
- Center for Disease Control (CDC). National Immunization Awareness Month. Available online: https://www.cdc.gov/vaccines/events/niam/index.html (accessed on 3 November 2024).
- Poland CM, Ratishvili T. Vaccine hesitancy and health care providers: Using the preferred cognitive styles and decision- making model and empathy tool to make progress. Vaccine X 2022, 11, 100174. [CrossRef]
- Salmon, D.A.; Teret, S.P.; Macintyre, C.R.; Salisbury, D.; Burgess, M.A.; Halsey, N.A. Compulsory vaccination and conscientious or philosophical exemptions: Past, present, and future. Lancet 2006, 367, 436–442. [Google Scholar] [CrossRef]
- Haverkate, M.; D’Ancona, F.; Giambi, C.; Lopalco, P.L.; Cozza, V.; Appelgren, E. Mandatory and recommended vaccination in the EU, Iceland and Norway: Results of the VENICE 2010 survey on the ways of implementing national vaccination programmes. EuroSurveill. 2010, 17, p. 20183. Available online: http://www.eurosurveillance.org/ViewArticle.aspx?Articleld=20183 (accessed on 29 November 2024).
- Pannuti, C.S.; Morello, R.J.; De Moraes, J.C.; Curti, S.P.; Afonso, A.M.S.; Camargo, M.C.C.; De Souza, V.A.U.F. Identification of primary and secondary measles vaccine failures by measurement of immunoglobulin G avidity in measles cases during the 1997 São Paulo Epidemic. Clin. Diagn. Lab. Immunol. 2004, 11, 119–122. [Google Scholar] [CrossRef]
- Danovaro-Holliday, M.C.; Koh, M.; Steulet, C.; Rhoda, D.A.; Trimner, M.K. Lessons from Recent Measles Post-Campaign Coverage Surveys Worldwide. Vaccines 2024, 12, 1257. [Google Scholar] [CrossRef] [PubMed]
- O’Leary ST, Opel DJ, Cataldi JR, Hackell JM; Committee on Infectious Diseases; Committee on Practice and Ambulatory Medicine; Committee on Bioethics. Strategies for Improving Vaccine Communication and Uptake. Pediatrics. 2024, 153, e2023065483. [CrossRef]
- European Centre for Disease Prevention and Control (ECDC). Catalogue of interventions addressing vaccine hesitancy; ECDC: Stockholm, Sweden, 2017. [Google Scholar]
- Crowcroft, N.S.; Minta, A.A.; Bolotin, S.; Cernuschi, T.; Ariyarajah, A.; Antoni, S.; Mulders, M.N.; Bose, A.S.; O’Connor, P.M. The Problem with Delaying Measles Elimination. Vaccines 2024, 12, 813. [Google Scholar] [CrossRef]
- WHO-UNICEF. WHO UNICEF immunization coverage estimates 2023 revision (released 15 July 2024). Available online: https://www.who.int/publications/m/item/WUENIC_notes (accessed on 29 November 2024).
- Guerra, F.; Bolotin, S.; Lim, G.; Heffernan, J.; Deeks, S.L.; Li, Y.; Crowcroft, N.S. The basic reproduction number (Ro) of measles: A systematic review. Lancet Infect. Dis. 2017, 17, e420–e428. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Number of zero-dose measles children (MCV1 vaccine) estimated from 2019 and 2023 and number measles required from 2019 to 2030 to achieve the IA 2030 objective (9.65 million).
Figure 1.
Number of zero-dose measles children (MCV1 vaccine) estimated from 2019 and 2023 and number measles required from 2019 to 2030 to achieve the IA 2030 objective (9.65 million).
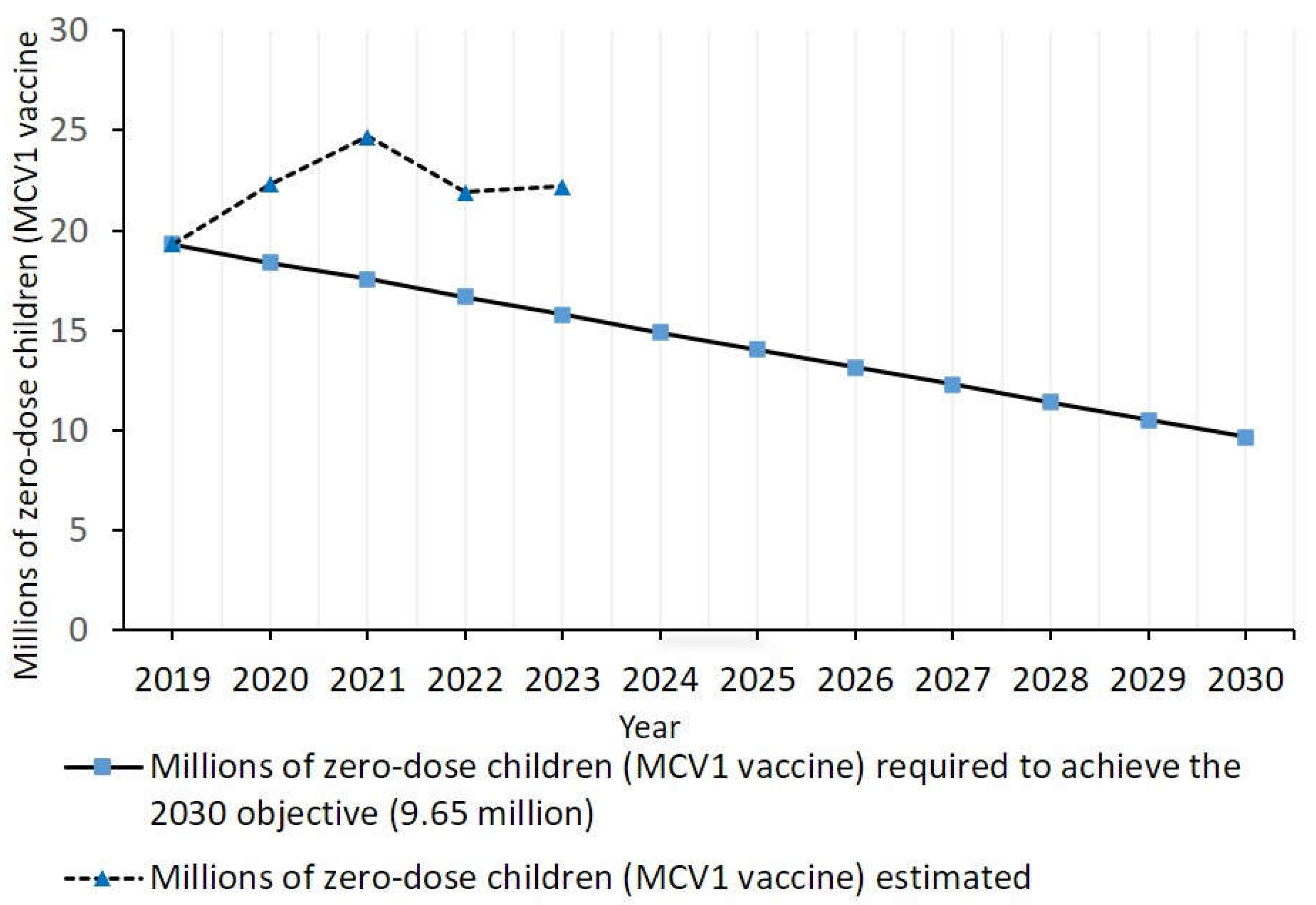
Figure 2.
Track to achieve a 50% reduction from 2019 to 2030 for mean MCV1-based zero-dose measles vaccination coverage, and MCV1-based zero-dose coverage observed from 2019 to 2023. Track to achieve a 50% reduction from 2019 to 2030 for mean zero-dose measles vaccination coverage determined from two and one doses of measles vaccination, and zero-dose coverage observed in this study for 2023 .
Figure 2.
Track to achieve a 50% reduction from 2019 to 2030 for mean MCV1-based zero-dose measles vaccination coverage, and MCV1-based zero-dose coverage observed from 2019 to 2023. Track to achieve a 50% reduction from 2019 to 2030 for mean zero-dose measles vaccination coverage determined from two and one doses of measles vaccination, and zero-dose coverage observed in this study for 2023 .
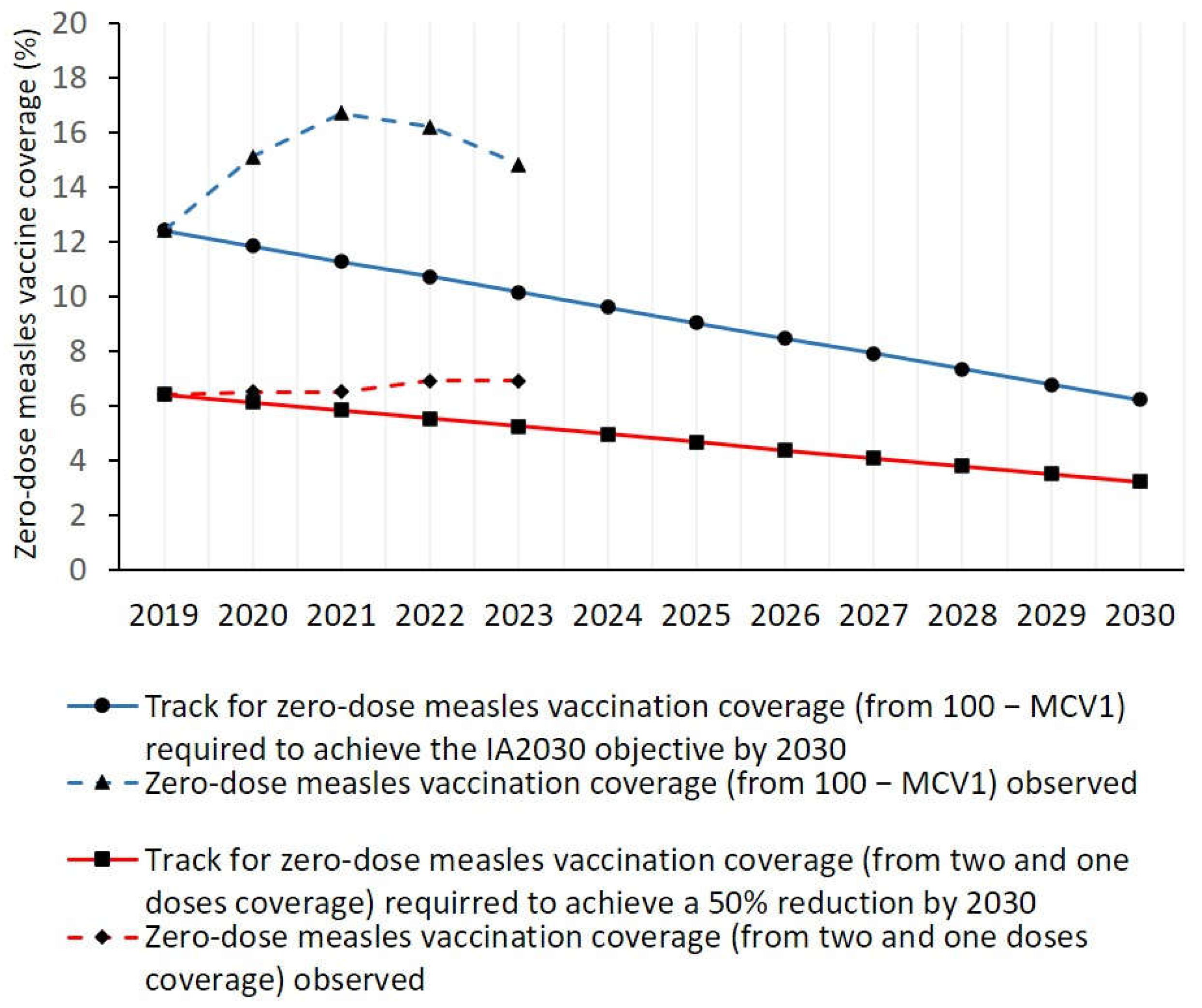

Table 1.
Mean percentages of vaccination coverage for the MCV1 and MCV2 vaccines in 2023 and the MCV1 vaccine in 2021 in the world and WHO regions.
Table 1.
Mean percentages of vaccination coverage for the MCV1 and MCV2 vaccines in 2023 and the MCV1 vaccine in 2021 in the world and WHO regions.
| MCV1 vaccine 2023 |
MCV2 Vaccine 2023 |
MCV1 vaccine 2021 |
n | |
| % | % | % | ||
| World | 85.2 | 77.1 | 83.3 | 195 |
| African region (AFR) | 71.5 | 62.0 | 65.0 | 47 |
| Americas region (AMR) | 93.0 | 83.0 | 87.5 | 35 |
| Eastern Mediterranean region (EMR) | 91.5 | 86.5 | 80.0 | 22 |
| European region (EUR) | 90.5 | 92.5 | 93.0 | 53 |
| South East Asia region (SEAR) | 62.5 | 54.5 | 98.0 | 11 |
| Western Pacific region (WPR) | 97.0 | 95.5 | 97.5 | 27 |
n: number of countries with vaccine in national routine vaccination programs; MCV1: first dose of measles-containing vaccine; MCV2: second dose of measles-containing vaccine.
Table 2.
Mean vaccination coverage with two, one and zero doses of measles vaccines, mean prevalence of individuals in the target vaccination population with vaccine-induced measles protection, percentage of countries with anti-measles herd immunity established in the target population vaccination, and percentage of countries with other measles vaccination indicators in regions of the WHO in 2023.
Table 2.
Mean vaccination coverage with two, one and zero doses of measles vaccines, mean prevalence of individuals in the target vaccination population with vaccine-induced measles protection, percentage of countries with anti-measles herd immunity established in the target population vaccination, and percentage of countries with other measles vaccination indicators in regions of the WHO in 2023.
| World | African region | Americas region | Eastern Mediterranean region |
European region | South-East Asia region | Western Pacific region |
|
|---|---|---|---|---|---|---|---|
| No. of countries | 195 | 47 | 35 | 22 | 53 | 11 | 27 |
| Routine measles vaccination-related indicators | |||||||
| Mean vaccination coverage (%) with two, one and zero doses of measles vaccine | |||||||
| 2 doses | 65.3 | 48.1 | 72.5 | 69.1 | 86.0 | 53.0 | 93.2 |
| 1 dose | 27.8 | 30.7 | 25.5 | 28.2 | 13.5 | 46.5 | 6.7 |
| 0 doses | 6.9 | 21.1 | 2.0 | 2.6 | 0.5 | 0.5 | 0.2 |
| Percentage of countries with two-dose measles vaccination coverage ≥ 95% and ≥ 90% | |||||||
| ≥ 95% | 8.7 | 0 | 2.9 | 22.7 | 9.4 | 18.2 | 14.8 |
| ≥ 90% | 21.0 | 0 | 8.6 | 40.9 | 30.2 | 36.4 | 33.3 |
| Percentage of countries where all children had received one or two doses of measles vaccine (0% of zero-dose children) | |||||||
| 9.7 | 0 | 5.7 | 22.7 | 9.4 | 18.2 | 18.5 | |
| Anti-measles herd immunity-related indicators | |||||||
| Mean prevalence (%) of individuals in the target vaccination population with vaccine-induced measles immunity | |||||||
| Measles immunity | 87.6 | 74.0 | 92.3 | 91.6 | 94.1 | 93.1 | 94.6 |
| Percentage of countries with herd immunity against measles viruses with Ro from 10 to ≥ 20 | |||||||
| Ro ≤ 10 | 66.1 | 40.4 | 62.9 | 68.2 | 92.4 | 72.7 | 59.3 |
| Ro ≤ 12 | 59.0 | 27.6 | 54.3 | 59.1 | 88.7 | 63.6 | 59.3 |
| Ro ≤ 15 | 41.5 | 10.6 | 25.7 | 50.0 | 66.0 | 63.6 | 51.8 |
| Ro ≤ 18 | 23.1 | 0 | 8.6 | 45.4 | 35.8 | 36.4 | 33.3 |
| Ro ≤ 19 | 0 | 0 | 5.7 | 31.8 | 13.2 | 27.3 | 22.2 |
| Ro ≥ 20 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
Table 3.
Variation for measles vaccination and anti-measles herd immunity indicators in different regions of the WHO between 2019 and 2023.
Table 3.
Variation for measles vaccination and anti-measles herd immunity indicators in different regions of the WHO between 2019 and 2023.
| World | African region | Americas region | Eastern Mediterranean region |
European region | South-East Asia region | Western Pacific region |
|
|---|---|---|---|---|---|---|---|
| No. of countries | 195 | 47 | 35 | 22 | 53 | 11 | 27 |
| Routine measles vaccination-related indicators | |||||||
| Mean vaccination coverage (%) with two. one and zero doses of measles vaccine | |||||||
| 2 doses | -3.7 | 24.0 | -1.0 | -3.2 | 2.5 | -35.0 | 30.9 |
| 1 dose | 7.8 | -30.7 | 5.8 | 27.6 | -11.2 | 171.9 | -71.0 |
| 0 doses | 7.8 | 24.9 | -25.9 | -60.0 | -44.4 | -64.3 | -96.5 |
| Percentage of countries with two-dose measles vaccination coverage ≥ 95% and ≥ 90% | |||||||
| ≥ 95% | -39.6 | -100.0 | -79.7 | -4.6 | -37.7 | -33.3 | -33.3 |
| ≥ 90% | -18.6 | -100.0 | -62.4 | 7.3 | -15.6 | 0.0 | -10.0 |
| Percentage of countries where all children had received one or two doses of measles vaccine (0% of zero-dose children) | |||||||
| -24.8 | -100.0 | -60.1 | -20.6 | 0.0 | -33.3 | 0.0 | |
| Anti-measles herd immunity-related indicators | |||||||
| Mean prevalence (%) of individuals in the target vaccination population with vaccine-induced measles immunity | |||||||
| Measles immunity | -0.6 | -4.6 | 0.5 | 3.9 | 0.4 | -0.1 | 6.5 |
| Percentage of countries with herd immunity against measles viruses with Ro from 10 to ≥ 20 | |||||||
| Ro ≤ 10 | -6.4 | 0.0 | -15.3 | 2.2 | -2.0 | -11.1 | -15.8 |
| Ro ≤ 12 | -7.7 | -7.4 | -17.4 | -4.5 | -2.1 | -12.5 | -11.1 |
| Ro ≤ 15 | -19.4 | -28.9 | -43.8 | -4.6 | -18.6 | 16.7 | -17.8 |
| Ro ≤ 18 | -28.9 | -100.0 | -62.4 | 19.2 | -13.7 | -33.2 | -18.2 |
| Ro ≤ 19 | -100.0 | -100.0 | -66.7 | 11.2 | -22.4 | 0.0 | 0.0 |
| Ro ≥ 20 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



