
Submitted:
31 December 2024
Posted:
31 December 2024
You are already at the latest version
Abstract
Background/Objectives: Even today the interstitial lung disease (ILD) is diagnosed by chest high-resolution computed tomography (lung HR-CT). A large amount of data is available about the use-fulness of lung ultrasound (LUS) in ILD. The aim of this study is to evaluate the LUS capacity to discrim-inate different ILD patterns in systemic sclerosis (SSc) patients, such as UIP, NSIP with GGO, and NSIP with GGO and reticulations, and then the possibilityto identify the progressive fibrosing ILD. Methods: All SSc-patients with recent HRCT performed underwent LUS. Results: ILD was observed in 99 (63.5%) patients (25% with UIP pattern, and 75% with NSIP pattern (46 with GGO, 28 with GGO and reticula-tions). By ROC curve analysis, that higher accuracy, sensitivity, and specificity were found for pleural line irregularity (0.68, 95.8%, and 41.5%, p=0.004), pleural line thickness (0.72, 70.8%, and 73.2%, p=0.001), and subpleural cyst (0.68, 58.3%, and 78.9%, p=0.004) to detect UIP pattern. The best performance among LUS signs for NSIP with GGO pattern was observed for B-lines (accuracy: 0.73, sensitivity: 92.9% and specific-ity: 54.3, p=0.0001). LUS signs with higher accuracy, sensitivity, and specificity for NSIP with GGO and reticulations were pleural line irregularity (0.69, 96%, and 42.1%, p=0.002), pleural line thickness (0.69, 65.4%, 72.7%, p=0.002), and B-lines (0.72, 96.2%, 48.8%, p=0.0001). Furthermore, a total number of B-line > 10 maximises LUS performance with 92.3% sensitivity, and an accuracy of 0.83 (p=0.0001) to detect the NSIP pattern, particularly GGO. A sample-restricted analysis (66 SSc patients) evidenced the presence of progressive fibrosing ILD in 77%. By binary regression analysis, that the unique LUS sign associated with progressive fibrosing ILD was the presence of pleural line irregularity (OR: 3.6; 95% CI 1.08-11.9; p= 0.036). Conclusions: Our study demonstrated that the LUS presented a high capacity to discriminate the different patterns of SSc-ILD. Therefore, the hypothesis of using transthoracic LUS as a screening method for the evaluation of the presence of SSc-ILD and to establish the correct timing for the execution of chest HR-CT, in order to avoid patients from excessive exposure to ionising radiation is supported.
Keywords:
Interstitial lung disease
; usual interstitial pneumonia
; non-specific interstitial pneumonia
; lung ultrasound (LUS)
; B-lines
1. Introduction
Interstitial lung disease (ILD) is one of the most frequent clinical features in systemic sclerosis (SSc), estimated in 53% of patients with SSc with a diffuse cutaneous subset and in 35% of patients with a limited cutaneous subset. [1] Together with pulmonary arterial hypertension, despite advances in therapeutic management, it currently represents the most frequent cause of death in patients with SSc (28%). [2,3,4,5,6,7]
The gold-standard instrumental method for diagnosing and following SSc-ILD is chest high-resolution computed tomography (lung HR-CT). Given the subclinical onset and the need to diagnose SSc-ILD as early as possible, in order to try to slow down its progression through pharmacological therapy, lung HR-CT is recommended to be performed periodically. [8,9,10,11,12,13,14]
The most frequent lung CT pattern of ILD in SSc, above all in early phases of the disease, is the nonspecific interstitial pneumonia (NSIP) characterised by the presence of ground glass opacities (GGO) and reticulations, and less recurrent usual interstitial pneumonia (UIP), identified by honeycombing and traction bronchiectasis. [8,9,10,11,12,13,14,15]
In the last decade, however, the issues of high cost and the risk related to excessive exposure to ionising radiation, which every CT scan induces, and the increased risk of developing neoplasms (especially breast carcinomas) in patients with SSc [16], has induced the scientific community to search for new instrumental methods that are less harmful to the patient. Among these, transthoracic lung ultrasound (LUS) has assumed considerable importance, due to preliminary data supporting a positive association between LUS signs and CT findings [17,18,19,20,21,22,23,24,25]
This study aims to evaluate the LUS capacity to discriminate different ILD patterns in SSc patients, such as UIP, NSIP with GGO, and NSIP with GGO and reticulations. Furthermore, we wanted to evaluate the presence of any characteristic LUS signs to identify progressive fibrosing ILD.
2. Materials and Methods
One hundred fifty-six patients were consecutively recruited for this study, followed at the outpatient clinic of the Rheumatology Unit of Policlinico of Foggia and the Rheumatology Unit of Policlinico of Bari. All patients satisfied ACR/EULAR 2013 classification criteria for SSc. [26] The clinical examination at enrolled visit includes age, disease history, medications, visceral involvement, and laboratory test for reactants of the acute phase of inflammation (erythrocyte sedimentation rate, C-reactive protein), antinuclear antibodies (assessed by immunofluorescence) and extractable nuclear antigens antibodies (evaluated by immunoblotting), the presence of ILD and its pattern at CT lungs, the respiratory capacity by pulmonary function test, evaluation of the presence of main LUS signs of ILD, the assessment of nailfold capillaroscopy patterns. The extent and severity of skin thickening were evaluated by the modified Rodnan skin score.
Inclusion criteria were: age older than 18 years, the satisfaction of ACR/EULAR 2013 classification criteria for SSC; chest CT scan within three months before or three months after LUS evaluation; and availability of recent and complete pulmonary function test with FVC, DLCO and FEV1.
Exclusion criteria were: history or recent reactivation of chronic obstructive pulmonary disease, lung cancer, lung infection, heart failure, pulmonary oedema, pulmonary arterial hypertension, acute respiratory distress syndrome and diffuse alveolar haemorrhage and thoracic surgery.
- -
- -
- -
- mobility of pleural line, in particular, the presence of sliding sing;
- -
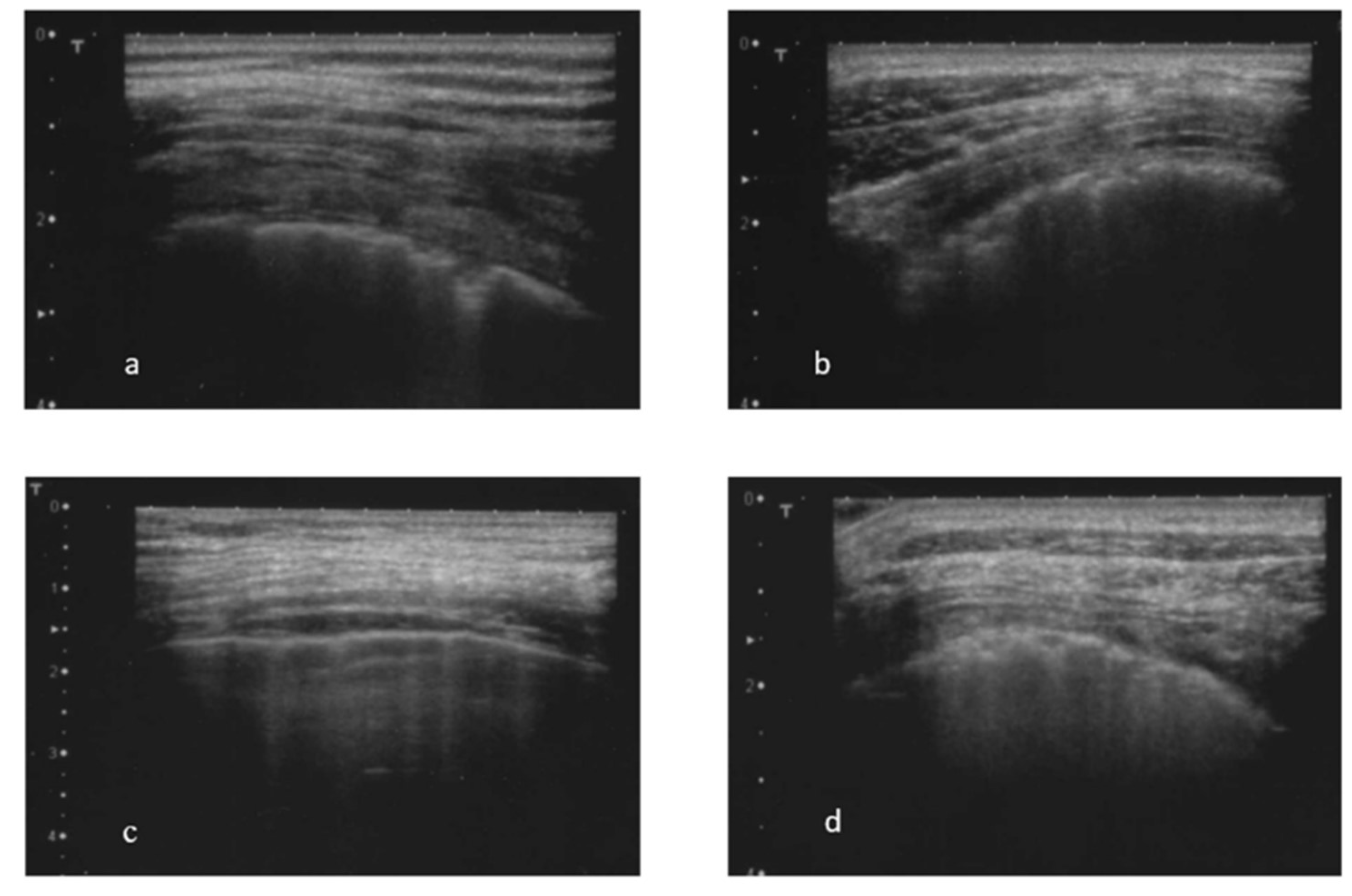
- the presence and the total number of B-lines (abnormal in the presence of 3 or more B-lines in at least two consecutive scans or the presence of at least 5 B-lines in the entire intercostal space examined) (Figure 1 c) [30; 32]. The total number of B-lines was given by the sum of all the B-lines found in the different fields examined;
- -
- the presence of almost one subpleural cyst (Figure 1 d), defined as hypo-echoic lesions that interrupt the pleural line;
- -
- the presence of the pleural effusion.
Statistical Analysis.
The results were expressed as means (m) ± standard deviation (sd); categorical variables were expressed as numbers (percentage). The normality of the distribution of the study variables was verified with the Kolmogorov-Smirnov test.
Statistical differences between the two groups were analyzed with the t-student for unpaired data. Multiple comparisons of continuous variables were analyzed with analysis of variance (ANOVA) followed by the Bonferroni test.
Pearson χ2 and Fisher’s exact test, followed by Z-test, were used to compare categorical variables and percentages.
The ROC curve was used to compare the diagnostic performance of each US sign with lung CT patterns of ILD as NSIP with GGO, NSIP with GGO and reticulations, and UIP, assessing the area under the curve (AUC). The AUC values of 0.50–0.59, 0.60–0.69, 0.70–0.79, and ≥0.80 are defined as none, poor, acceptable, and excellent accuracy, respectively
Binary logistic regression was used to evaluate predictors of progressive fibrosing ILD.
Statistical significance was defined as a value of p≤0.05.
Statistical analysis was performed with IBM SPSS Statistics 26.
Ethics Approval.
Our study was approved by the local Ethics Committee (115/C.E.. All participants gave their informed consent to participate in this study and undergo a computed tomography scan.
3. Results
One hundred and fifty-six Caucasian patients diagnosed with SSC (mean age 59.0 ± 12.4 years; and mean disease duration 32 ± 10.8 years) satisfied the inclusion criteria. The ILD at lung CT was detected in 99 (63.5%) studied patients, of which 25 (25%) with UIP pattern, and 74 (75%) with NSIP pattern (46 with GGO alone, and 28 with GGO and reticulations).
The comparison between the study groups of the main demographic and clinical characteristics is shown in Table 1. A higher presence of anti-Scl-70 antibodies was found in patients with ILD (any CT patterns) compared with no-ILD patients. Lower values of FVC at pulmonary function tests are detected in UIP (84.8 ± 18.3) and NSIP with GGO and reticulations (84 ± 19.4) groups. As regards other specific CT lung abnormalities, a higher rate of micro-nodules was found in NSIP with GGO group (56.5%). More extensive and severe ILD, assessed by Warrick Score, was recognized in UIP (10.2 ± 4) and NSIP with GGO and reticulations (10.8 ± 1.7) groups (Table 1).
3.2. Figures, and Tables
Figure 2.
Graphical representation of ROC curve analysis of different LUS signs for detecting a) UIP CT ILD-pattern; b) NSIP with GGO CT ILD-pattern; c) NSIP with GGO and reticulation CT ILD pattern. *p≤0.05.
Figure 2.
Graphical representation of ROC curve analysis of different LUS signs for detecting a) UIP CT ILD-pattern; b) NSIP with GGO CT ILD-pattern; c) NSIP with GGO and reticulation CT ILD pattern. *p≤0.05.
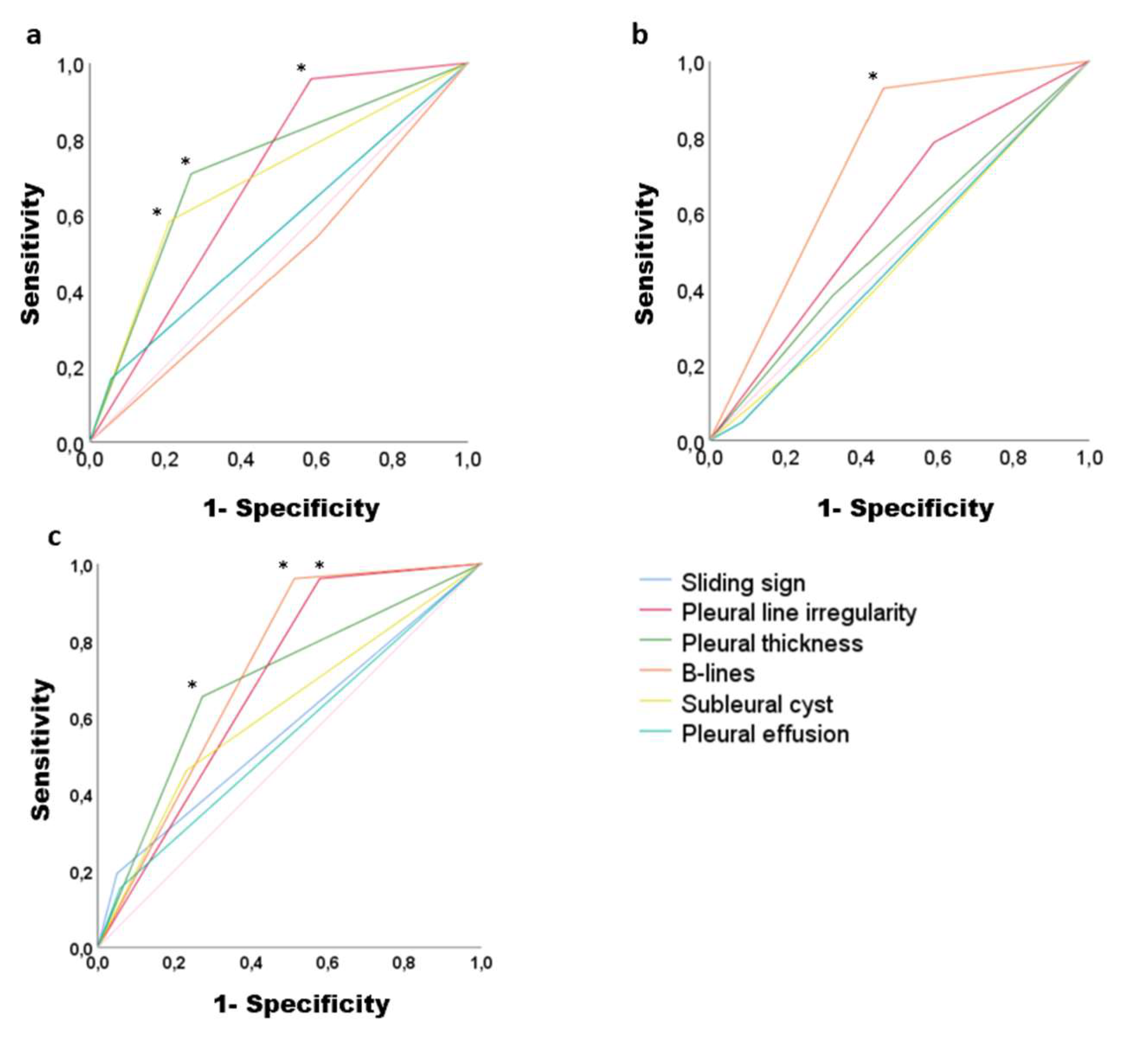

Table 1.
Comparison among study groups of the main demographic, clinical and instrumental characteristics.
Table 1.
Comparison among study groups of the main demographic, clinical and instrumental characteristics.
| No-ILD | UIP | NSIP with GGO | NSIP with GGO and reticulations | p-value | |
|---|---|---|---|---|---|
| N (%) | 57 (36,5%) | 25 (16%) | 46 (29,5%) | 28 (18%) | |
| F/M | 55 (96%) / 2 (3%) | 23 (92%) / 2 (8%) | 43 (93%) / 3 (6%) | 27 (96%) / 1 (4%) | 0.788 |
| Age (years) | 57.5 ± 14.4 | 60.4 ± 11.0 | 58.2 ± 11.5 | 62.2 ± 10.1 | 0.370 |
| Disease duration (years) | 9.7 ± 6.9 | 10.9 ± 5.9 | 7.4 ± 5.9 | 7.8 ± 7.7 | 0.479 |
| BMI | 25.9 ± 4.1 | 25.2 ± 6.1 | 25.2 ± 4.3 | 26.1 ± 4.5 | 0.170 |
| ESR (mm/h) | 19.3 ± 14.8 | 17.6 ± 14 | 17.7 ± 13.1 | 24.5 ± 14.4 | 0.242 |
| CRP (mg/l) | 4.8 ± 4.8 | 5.0 ± 1.1 | 7.5 ± 1.3 | 9.6 ± 1.8 | 0.238 |
| ENA | |||||
| Anti CENP-B | 42 (74%) | 3 (12%) | 6 (13%) | 6 (23%) | 0.0001^ |
| Anti Scl-70 | 10 (17,5%) | 19 (76%) | 36 (78%) | 17 (65%) | 0.0001” |
| Nailfold Videocapillaroscopy | |||||
| Early scleroderma pattern | 16 (32%) | 4 (20%) | 16 (40%) | 4 (17%) | 0.440 |
| Active scleroderma pattern | 24 (45%) | 8 (40%) | 15 (37%) | 12 (52%) | 0.786 |
| Late scleroderma pattern | 13 (24%) | 8 (40%) | 9 (22,5%) | 7 (30%) | 0.443 |
| Cutaneous subsets | |||||
| Limited | 49 (86%) | 20 (80%) | 34 (74%) | 25 (89%) | 0.292 |
| Diffuse | 8 (14%) | 5 (20%) | 12 (26%) | 3 (11%) | 0.296 |
| Presence of LUS abnormalities | |||||
| Sliding sign | 0 (0%) | 5 (20%) | 2 (4%) | 5 (18,5%) | 0.002 § |
| Pleural line irregularity | 15 (26%) | 24 (96%) | 35 (76%) | 27 (96%) | 0.0001^ |
| Pleural thickness | 2 (3,5%) | 18 (72%) | 16 (36%) | 18 (64%) | 0.0001° |
| B-lines | 10 (17,5%) | 14 (56%) | 43 (93,5%) | 27 (96%) | 0.0001# |
| B-lines number | 3.5 ± 16.1 | 29.0 ± 10.2 | 69.5 ± 10.7 | 56.6 ± 11.8 | 0.0001# |
| Subpleural cystis | 5 (9%) | 14 (58%) | 10 (24%) | 13 (48%) | 0.0001@ |
| Pleural effusion | 2 (3,5%) | 4 (16%) | 2 (4%) | 4 (14%) | 0.103 |
| PFT | |||||
| FVC% baseline | 108.1 ± 14.4 | 84.8 ± 18.3 | 99.5 ± 15.4 | 84 ± 19.4 | 0.0001& |
| DLCO% baseline | 77.1 ± 16.9 | 77.2 ± 17 | 77.7 ± 18 | 69.1 ± 18.5 | 0.627 |
| TLC% baseline | 101.6 ± 12.9 | 75.2 ± 11 | 92.9 ± 16.2 | 91.8 ± 33 | 0.059 |
| Other lung CT abnormalities | |||||
| Micro nodules | 6 (13%) | 8 (32%) | 26 (56.5%) | 9 (32%) | 0.0001* |
| Warrick Score | 0.0 ± 0.0 | 10.2 ± 4.0 | 8 ± 3.4 | 10.8 ± 1.7 | 0.0001$ |
1 BMI: body mass index; CRP: C-reactive proteins; CT: computed tomography; ENA: Extractable Nuclear Antigen; ESR: erythrocyte sedimentation rate; F: female; GGO: ground glass; ILD: interstitial lung disease; M: male; LUS: lung ultrasound; NSIP: non-specific interstitial pneumonia; PFT: pulmonary function tests; UIP: usual interstitial pneumonia. *NSIP with GGO vs UIP p≤0,05; NSIP with GGO vs No-ILD p≤0,05; NSIP with GGO and reticulations vs No-ILD p≤0,05; UIP vs No-ILD p≤0,05, § UIP vs No-ILD p≤0,05; NSIP with GGO and reticulations vs No-ILD p≤0,05, ^ NSIP with GGO vs No-ILD p≤0,05; UIP vs No-ILD p≤0,05; NSIP with GGO and reticulations vs No-ILD p≤0,05, “ No-ILD vs NSIP with GGO p≤0,05; No-ILD vs UIP p≤0,05; No-ILD vs NSIP with GGO and reticulations p≤0,05, ° UIP vs NSIP with GGO p≤0,05; NSIP with GGO vs No-ILD p≤0,05; NSIP with GGO and reticulations vs No-ILD p≤0,05; UIP vs No-ILD p≤0,05, # UIP vs No-ILD p≤0,05; NSIP with GGO vs No-ILD p≤0,05; NSIP with GGO and reticulations vs No-ILD p≤0,05; NSIP with GGO vs UIP p≤0,05; NSIP with GGO and reticulations vs UIP p≤0,05, @ UIP vs No-ILD p≤0,05; UIP vs NSIP with GGO p≤0,05; NSIP with GGO and reticulations vs No-ILD p≤0,05, & UIP vs No-ILD p≤0,05; NSIP with GGO vs No-ILD p≤0,05; NSIP with GGO and reticulations vs No-ILD p≤0,05; UIP vs NSIP with GGO p≤0,05; NSIP with GGO and reticulations vs GGO p≤0,05, $ UIP vs No-ILD p≤0,05; NSIP with GGO vs No-ILD p≤0,05; NSIP with GGO and reticulations vs No-ILD p≤0,05; NSIP with GGO vs NSIP with GGO and reticulations p≤0,05.
Table 2.
ROC curve analysis. Sensitivity, specificity, and accuracy of different lung ultrasound signs for detecting specific ILD CT lung patterns (UIP, NSIP with GGO, NSIP with GGO and reticulations).
Table 2.
ROC curve analysis. Sensitivity, specificity, and accuracy of different lung ultrasound signs for detecting specific ILD CT lung patterns (UIP, NSIP with GGO, NSIP with GGO and reticulations).
| Sensitivity | Specificity | Accuracy | p-value | |
|---|---|---|---|---|
| UIP CT lungs pattern | ||||
| Sliding sign | 16.7% | 95% | 0.55 (0.42-0.68) | 0.396 |
| Pleural line irregularity | 95.8% | 41.5% | 0.68 (0.58-0.78) | 0.004 |
| Pleural thickness | 70.8% | 73.2% | 0.72 (0.60-0.83) | 0.001 |
| B-lines | 54.2% | 39.8% | 0.47 (0.34-0.59) | 0.643 |
| Subpleural cyst | 58.3% | 78.9% | 0.68 (0.56-0.81) | 0.004 |
| Pleural effusion | 16,7% | 95% | 0.55 (0.42-0.68) | 0.396 |
| NSIP with GGO CT lungs pattern | ||||
| Sliding sign | 48% | 91.4% | 0.48 (0.37-0.58) | 0.719 |
| Pleural line irregularity | 78.6% | 41% | 0.59 (0.49-0.69) | 0.065 |
| Pleural thickness | 38.1% | 67.6% | 0.52 (0.42-0.63) | 0.589 |
| B-lines | 92.9% | 54.3% | 0.73 (0.65-0.81) | 0.0001 |
| Subpleural cysts | 23.8% | 71.4% | 0.47 (0.37-0.57) | 0.653 |
| Pleural effusion | 4.8% | 91.4% | 0.48 (0.37-0.58) | 0.719 |
| NSIP with GGO and reticulation CT lungs pattern | ||||
| Sliding sign | 19% | 95% | 0.57 (0.44-0.70) | 0.254 |
| Pleural line irregularity | 96.2% | 42.1% | 0.69 (0.59-0.78) | 0.002 |
| Pleural thickness | 65.4% | 72.7% | 0.69 (0.57-0.80) | 0.002 |
| B-lines | 96.2% | 48.8% | 0.72 (0.63-0.81) | 0.0001 |
| Subpleural cyst | 47.2% | 76.9% | 0.61 (0.49-0.74) | 0.066 |
| Pleural effusion | 15.4% | 42% | 0.54 (0.42-0.67) | 0.443 |
CT: computed tomography; GGO: ground glass; ILD: interstitial lung disease; LUS: lung ultrasound; NSIP: non-specific interstitial pneumonia; UIP: usual interstitial pneumonia.
4. Discussion
A large number of studies are available on the use of LUS in ILD, although a consensus has never been reached on its real clinical value, the coding and scoring system [14]. Our study adds to the other published works, introducing considerations regarding how LUS can differentiate specific lung HR-CT patterns such as NSIP, and UIP. Indeed, the present study highlights that transthoracic LUS is a enough sensitive and specific technique in evaluating the presence of typical SSc-ILD tomographic patterns and is also sufficiently accurate in discriminating its different and characteristic phases. The finding of B-lines on LUS was found to be significantly associated with the presence of active inflammatory phases of SSc-ILD, characterized by GGO, as observed in the NSIP pattern. [33,34,35,36] and that the finding of irregularities of the pleural line, of thickening of the pleural line and subpleural cysts is, instead, significantly associated with the presence of honeycombing and traction bronchiectasis, as in UIP pattern, and therefore of the fibrosis phase. So, principally, the presence or the absence of B-lines significantly differentiates the NSIP pattern from the UIP pattern.
The presence of LUS signs, such as the presence of irregularities of the pleural line, thickening of the pleural line, the presence of subpleural cysts, reduced mobility of the pleural line and the presence of B-lines, in patients with pulmonary fibrosis, was first described in 1997 [37] Other studies have evaluated the presence of these same LUS signs in ILD secondary to sarcoidosis, rheumatoid arthritis, SSc, mixed connective tissue disease, Sjogren’s syndrome and primary biliary cirrhosis, demonstrating their presence also in these secondary forms of ILD [30], and highlighting, in particular, that the presence of B-lines distributed throughout the lung area is associated with more severe pulmonary fibrosis. [38] Concerning the LUS evaluation of ILD in connective tissue diseases, in previous studies, it has been observed that the greater number of B-lines could identify SSc-ILD [30; 38-39]; and, in particular, that the number of B-lines correlates with the tomographic Warrick Score, an index of severity of SSc-ILD [20]. Furthermore, the high sensitivity of B-lines in evaluating the presence of SSc-ILD has been described both in patients with a diagnosis of very early SSc [40] and those with a diagnosis of SSc. [32]
The high frequency and sensitivity, found in the present study, between the presence of B-lines and the tomographic pattern of NSIP with GGO, characteristic of active inflammatory processes
[41], could be attributed to the presence of inflammatory infiltrate that would determine a variation in acoustic impedance of the lung parenchyma, creating the air-water interface necessary for the generation of B-lines, as demonstrated in previous studies [42,43,44].
Concerning the cut-off of B-lines, the limit of >10 B-lines found to be sufficiently effective for recognising ILD, confirms what was previously found for ILD-SSc. [45,46]; but in our study we found a high sensitivity for the NSIP pattern, especially for the GGO-only pattern but also for the GGO and reticulations pattern. These findings have not been specifically evaluated in previous studies. However, few data support the presence of B-lines in both GGO and honeycombing patterns [14,47]. Still, no study has ever investigated the possible association between specific CT patterns, such as UIP and NSIP, and LUS signs. These results could indicate a greater sensitivity for the more inflammatory phases, which presuppose the presence of a greater inflammatory infiltrate with a subsequent increase in acoustic impedance.
In a previous study, a low specificity (55%) of B-lines was highlighted for SSc-ILD, despite a high sensitivity (100%); this finding was attributed to the probable presence of pulmonary oedema [32]; similar data was observed in our study, for both NSIP with GGO and NSIP with GGO and reticulations, but patients with pulmonary oedema, or other heart and lung diseases were excluded, so there could be other reasons yet to understand.
Regarding the tomographic pattern of UIP, a high sensitivity of LUS signs was observed, such as thickening of the pleural line, the presence of irregularities of the pleural line and the presence of subpleural cysts. This finding could be due to the presence of structural subversion of the lung parenchyma (complete loss of the typical acinar structure of the lung) observed in cases of stabilized pulmonary fibrosis, characterized tomographically by the presence of honeycombing. [48]
No data are available on the use of LUS in progressive fibrosing ILD; for the first time in this study, we observed a strict association between this ILD pattern and the presence of pleural line irregularities. Probably the subversion of the parenchymal structure could explain the irregularities of the pleural line visible with LUS. Observational studies with larger patient samples would serve to confirm this finding.
In the group of patients enrolled in this study, the percentage of SSc-ILD (63%) is in line with what has been described in other studies [1,49]; and the ENA specificity found most frequently in these patients is anti-Scl-70, as observed previously [50].
Therefore, LUS, due to its versatility, ease of handling and low maintenance costs, could assume considerable clinical importance for evaluating SSc-ILD. Furthermore, the ease of interpretation of LUS images and the rapid execution times (minimum duration < 10 minutes [32] and maximum 23 minutes [46]) make LUS an efficient instrumental method from a clinical point of view.
The accuracy and completeness of the information provided by the tomographic images, currently not obtainable by other methods, still make the chest HR-CT the gold-standard instrumental technique for diagnosing SSc-ILD. Although, probably, LUS will probably not replace the chest HR-CT for the diagnosis of SSc-ILD, at least, at the moment, it could be considered a guide to establish the most appropriate timing to perform the chest HR-CT, minimising the risk of exposure to ionising radiation [32]. In recent decades, this latter risk and the need to contain the costs related to the diagnosis and clinical management of patients has led the scientific community to identify new imaging techniques and new predictors of disease. [17,18,19,20,21,22,23,24,25,51,52,53,54,55,56] A LUS score with a weighted score for each LUS sign would be desirable to improve the diagnostic ability of LUS for different HR-CT patterns of ILD. The clinical utility of recognizing early and without excessive exposure to ionizing radiation, the different patterns of ILD-SSc, could have important implications in the therapeutic management of patients with SSc. Probably with the advent of artificial intelligence software, it will probably be possible to design multifactorial scores that will meet the needs of clinicians.
There are some limitations to our study such as the distance between two consecutive B-lines was not reported. This parameter has been shown to correlate with the Warrick score in patients diagnosed with pulmonary fibrosis [57], but its evaluation was not considered useful for the purposes of our study. It would have been, furthermore, interesting to compare the ultrasound data of patients with SSc-ILD with healthy subjects and other groups of patients with pathologies complicated with ILD. However, in other studies conducted on this topic, the same LUS signs highlighted in this study were also found for other forms of ILD. [30,39,58]. We did not use the scoring system of LUS, as it has not yet been validated. As regards the progressive fibrosing ILD, it would have been useful to evaluate the LUS in an observational study, almost in two study-time points, in conjunction with the lung HR-CT, instead, we only have one LUS detection in conjunction with the last lung HR-CT performed.
5. Conclusions
The present study, comparing two instrumental methods, such as transthoracic LUS and lung HR-CT, demonstrates that there is a satisfying association between these two methods in evaluating the presence of specific patterns of ILD. In particular, LUS has shown high sensitivity in distinguishing different tomographic ILD patterns, such as UIP, with pleural line irregularities, pleural line thickness and the presence of subpleural cells; NSIP with GGO, characterised by B-lines; and NSIP with GGO and reticulations, characterised by pleural thickness, pleural irregularities, and B-lines. Therefore, the hypothesis of using transthoracic LUS as a screening method for the evaluation of the presence of SSc-ILD and to establish, therefore, the correct timing for the execution of chest HR-CT, in order to avoid patients from excessive exposure to ionising radiation is supported.
Observational studies should be performed to confirm LUS findings to characterize the pattern of progressive fibrosing ILD.
Author Contributions
C.R. and A.C. designed the study, wrote, and critically revised the final draft of the manuscript, and approved the submitted version. C.R. performed the statistical analysis and interpreted the data. G.B, R.B., V.R., F.C., M.F., F.I., C.M.I.Q., D.L., A.T. and F.P.C. collected the data and revised the final draft of the manuscript. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding
Institutional Review Board Statement
This study was approved by the local ethics committee (Ethics Review Board of Policlinico of Foggia, protocol number 115/C.E., and all patients were informed about the nature and aim of the study and gave and signed their consent to participate in this study.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data presented in this study are available on request from the corresponding author.
Acknowledgments
Special thanks to Dr. C. Bonali for his contribution.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| BMI | body mass index |
| CRP | C-reactive proteins |
| ESR | erythrocyte sedimentation rate |
| GGO | Ground glass opacities |
| LUS | Lung ultrasound |
| ILD | Interstitial lung disease |
| Lung HR-CT | chest high-resolution computed tomography |
| NSIP | Non-specific interstitial pneumonia |
| PFT | pulmonary function tests |
| ROC | Receiver operating characteristic |
| SSc | Systemic sclerosis |
| UIP | Usual interstitial pneumonia |
References
- Walker UA, Tyndall A, Czirjak L, Denton C, Farge-Bancel D, Kowal-Bielecka O, et al. Clinical risk assessment of organ manifestations in systemic sclerosis: a report from the EULAR Scleroderma Trials And Research group database. Ann Rheum Dis. 2007, 66, 754–763. [Google Scholar] [CrossRef] [PubMed]
- Steen VD, Medsger TA. Changes in causes of death in systemic sclerosis, 1972–2002. Ann Rheum Dis. 2007, 66, 940–944.
- Distler, O.; Assassi, S.; Cottin, V.; Cutolo, M.; Danoff, S.K.; Denton, C.P.; Distler, J.H.; Hoffmann-Vold, A.-M.; Johnson, S.R.; Ladner, U.M.; et al. Predictors of progression in systemic sclerosis patients with interstitial lung disease. Eur. Respir. J. 2020, 55, 1902026. [Google Scholar] [CrossRef] [PubMed]
- Elhai, M.; Meune, C.; Avouac, J.; Kahan, A.; Allanore, Y. Trends in mortality in patients with systemic sclerosis over 40 years: A systematic review and meta-analysis of cohort studies. Rheumatology 2012, 51, 1017–1026. [Google Scholar] [CrossRef] [PubMed]
- Tyndall, A.J.; Bannert, B.; Vonk, M.; Airò, P.; Cozzi, F.; Carreira, P.E.; Bancel, D.F.; Allanore, Y.; Müller-Ladner, U.; Distler, O.; et al. Causes and risk factors for death in systemic sclerosis: A study from the EULAR Scleroderma Trials and Research (EUSTAR) database. Ann. Rheum. Dis. 2010, 69, 1809–1815. [Google Scholar] [CrossRef] [PubMed]
- Volkmann, E.R.; Tashkin, D.P.; Sim, M.; Li, N.; Goldmuntz, E.; Keyes-Elstein, L.; Pinckney, A.; Furst, D.E.; Clements, P.J.; Khanna, D.; et al. Short-term progression of interstitial lung disease in systemic sclerosis predicts long-term survival in two independent clinical trial cohorts. Ann. Rheum. Dis. 2018, 78, 122–130. [Google Scholar] [CrossRef] [PubMed]
- Diot E, Boissinot E, Asquier E, Guilmot JL, Lemarie E, Valat C, et al. Relationship between abnormalities on high-resolution CT and pulmonary function in systemic sclerosis. Chest. 1998, 114, 1623–1629. [Google Scholar] [CrossRef] [PubMed]
- Wells A, Hansell D, Rubens M, King A, Cramer D, Black C, et al. Fibrosing alveolitis in systemic sclerosis. Indices of lung function in relation to extent of disease on computed tomography. Arthritis Rheum. 1997, 40, 1229–1236. [Google Scholar]
- Orlandi, M.; Landini, N.; Sambataro, G.; Nardi, C.; Tofani, L.; Bruni, C.; Randone, S.B.; Blagojevic, J.; Melchiorre, D.; Hughes, M.; et al. The role of chest CT in deciphering interstitial lung involvement: Systemic sclerosis versus COVID-19. Rheumatology 2021, 28, 615. [Google Scholar]
- Clukers, J.; Lukers, J.; Lanclus, M.; Belmans, D.; van Holsbeke, C.; de Backer, W.; Vummidi, D.; Cronin, P.; Lavon, B.R.; de Backer, J.; et al. Interstitial lung disease in systemic sclerosis quantification of disease classification and progression with high-resolution computed tomography: An observational study. J. Scleroderma Relat. Disord. 2021, 6, 154–164. [Google Scholar] [CrossRef] [PubMed]
- Desai, S.R.; Veeraraghavan, S.; Hansell, D.M.; Nikolakopolou, A.; Goh, N.S.; Nicholson, A.G.; Colby, T.V.; Denton, C.P.; Black, C.M.; Du Bois, R.M.; et al. CT features of lung disease in patients with systemic sclerosis: Comparison with idiopathic pulmonary fibrosis and non-specific interstitial pneumonia. Radiology 2004, 232, 560–567. [Google Scholar] [CrossRef] [PubMed]
- Launay, D.; Remy-Jardin, M.; Michon-Pasturel, U.; Mastora, I.; Hachulla, E.; Lambert, M.; Delannoy, V.; Queyrel, V.; Duhamel, A.; Matran, R.; et al. High resolution computed tomography in fibrosing alveolitis associated with systemic sclerosis. J. Rheumatol. 2006, 33, 1789–1801. [Google Scholar] [PubMed]
- Ruaro, B.; Baratella, E.; Confalonieri, P.; Wade, B.; Marrocchio, C.; Geri, P.; Busca, A.; Pozzan, R.; Andrisano, A.G.; Cova, M.A.; et al. High-Resolution Computed Tomography: Lights and Shadows in Improving Care for SSc-ILD Patients. Diagnostics 2021, 11, 1960. [Google Scholar] [CrossRef]
- Soldano, S.; Trombetta, A.C.; Contini, P.; Tomatis, V.; Ruaro, B.; Brizzolara, R.; Montagna, P.; Sulli, A.; Paolino, S.; Pizzorni, C.; et al. Increase in circulating cells coexpressing M1 and M2 macrophage surface markers in patients with systemic sclerosis. Ann. Rheum. Dis. 2018, 77, 1842–1845. [Google Scholar] [CrossRef] [PubMed]
- Lu TYT, Hill CL, Pontifex EK, Roberts-Thomson PJ. Breast cancer and systemic sclerosis: a clinical description of 21 patients in a population-based cohort study. Rheumatol Int. 2008, 28, 895–899. [Google Scholar] [CrossRef] [PubMed]
- Demizio, D.J.; Bernstein, E. Detection and classification of systemic sclerosis-related interstitial lung disease: A review. Curr. Opin. Rheumatol. 2019, 31, 553–560. [Google Scholar] [CrossRef] [PubMed]
- Delle Sedie, A.; Doveri, M.; Frassi, F.; Gargani, L.; D’Errico, G.; Pepe, P.; Bazzichi, L.; Riente, L.; Caramella, D.; Bombardieri, S. Ultrasound Lung Comets in Systemic Sclerosis: A Useful Tool to Detect Lung Interstitial Fibrosis. Clin. Exp. Rheumatol. 2010, 28, S54. [Google Scholar]
- Wang, Y.; Gargani, L.; Barskova, T.; Furst, D.E.; Cerinic, M.M. Usefulness of lung ultrasound B-lines in connective tissue disease-associated interstitial lung disease: A literature review. Arthritis Res. Ther. 2017, 19, 206. [Google Scholar] [CrossRef]
- Gargani, L.; Doveri, M.; D’Errico, L.; Frassi, F.; Bazzichi, M.L.; Delle Sedie, A.; Scali, M.C.; Monti, S.; Mondillo, S.; Bombardieri, S.; et al. Ultrasound Lung Comets in Systemic Sclerosis: A Chest Sonography Hallmark of Pulmonary Interstitial Fibrosis. Rheumatology 2009, 48, 1382–1387. [Google Scholar] [CrossRef] [PubMed]
- Vicente-Rabaneda, E.F.; Bong, D.A.; Castañeda, S.; Möller, I. Use of ultrasound to diagnose and monitor interstitial lung disease in rheumatic diseases. Clin. Rheumatol. 2021, 40, 3547–3564. [Google Scholar] [CrossRef] [PubMed]
- Fairchild, R.; Chung, M.; Yang, D.; Sharpless, L.; Li, S.; Chung, L. Development and Assessment of Novel Lung Ultrasound Interpretation Criteria for the Detection of Interstitial Lung Disease in Systemic Sclerosis. Arthritis Care Res. 2021, 73, 1338–1342. [Google Scholar] [CrossRef] [PubMed]
- Hoffmann-Vold, A.M.; Molberg, Ø. Detection, screening, and classification of interstitial lung disease in patients with systemic sclerosis. Curr. Opin. Rheumatol. 2020, 32, 497–504. [Google Scholar] [CrossRef] [PubMed]
- Trombetta, A.C.; Smith, V.; Gotelli, E.; Ghio, M.; Paolino, S.; Pizzorni, C.; Vanhaecke, A.; Ruaro, B.; Sulli, A.; Cutolo, M. Vitamin D deficiency and clinical correlations in systemic sclerosis patients: A retrospective analysis for possible future developments. PLoS ONE 2017, 12, e0179062. [Google Scholar] [CrossRef] [PubMed]
- Volpicelli, G. Lung Ultrasound B-Lines in Interstitial Lung Disease. Chest 2020, 158, 1323–1324. [Google Scholar] [CrossRef] [PubMed]
- van den Hoogen F, Khanna D, Fransen J, Johnson SR, Baron M, Tyndall A, et al. 2013 classification criteria for systemic sclerosis: an American college of rheumatology/European league against rheumatism collaborative initiative. Ann Rheum Dis. 2013, 72, 1747–1755. [Google Scholar] [CrossRef] [PubMed]
- Goh NS, Desai SR, Veeraraghavan S, Hansell DM, Copley SJ, Maher TM, et al. Interstitial lung disease in systemic sclerosis: a simple staging system. Am J Respir Crit Care Med. 2008, 177, 1248–1254. [Google Scholar] [CrossRef] [PubMed]
- Raghu G, Remy-Jardin M, Richeldi L, Thomson CC, Inoue Y, Johkoh T, et al. Idiopathic Pulmonary Fibrosis (an Update) and Progressive Pulmonary Fibrosis in Adults: An Official ATS/ERS/JRS/ALAT Clinical Practice Guideline. Am J Respir Crit Care Med. 2022, 205, e18–e47. [Google Scholar] [CrossRef] [PubMed]
- Volpicelli G, Elbarbary M, Blaivas M et al. International evidence-based recommendations for point-of-care lung ultrasound. Intensive Care Med 2012, 38, 577–591. [Google Scholar] [CrossRef]
- Sperandeo M, Varriale A, Sperandeo G, Filabozzi P, Piattelli ML, Carnevale V, et al. Transthoracic ultrasound in the evaluation of pulmonary fibrosis: our experience. Ultrasound Med Biol. 2009, 35, 723–729. [Google Scholar] [CrossRef]
- Moazedi-Fuerst F, Zechner P, Tripolt N, Kielhauser S, Brickmann K, Scheidl S, et al. Pulmonary echography in systemic sclerosis. Clin Rheumatol. 2012, 31, 1621–1625. [Google Scholar] [CrossRef]
- Barskova T, Gargani L, Guiducci S, Randone SB, Bruni C, Carnesecchi G, et al. Lung ultrasound for the screening of interstitial lung disease in very early systemic sclerosis. Ann Rheum Dis. 2013, 72, 390–395. [Google Scholar] [CrossRef] [PubMed]
- Lee J, Im J, Ahn J, Kim Y, Han M. Fibrosing alveolitis: prognostic implication of ground-glass attenuation at high-resolution CT. Radiology. 1992, 184, 451–454. [Google Scholar] [CrossRef]
- Muller N, Staples CA, Miller RR, Vedal S, Thurlbeck WM, Ostrow DN. Disease activity in idiopathic pulmonary fibrosis: CT and pathologic correlation. Radiology. 1987, 165, 731–734. [Google Scholar] [CrossRef] [PubMed]
- Shahin AA, Sabri YY, Mostafa HA, Sabry EY, Hamid MA, Gamal H, et al. Pulmonary function tests, high-resolution computerized tomography, α1-antitrypsin measurement, and early detection of pulmonary involvement in patients with systemic sclerosis. Rheumatol Int. 2001, 20, 95–100. [Google Scholar] [CrossRef] [PubMed]
- Terriff BA, Kwan SY, Chan-Yeung M, Müller N. Fibrosing alveolitis: chest radiography and CT as predictors of clinical and functional impairment at follow-up in 26 patients. Radiology. 1992, 184, 445–449. [Google Scholar] [CrossRef]
- Lichtenstein D, Meziere G, Biderman P, Gepner A, Barre O. The comet-tail artifact: an ultrasound sign of alveolar-interstitial syndrome. Am J Respir Crit Care Med. 1997, 156, 1640–1646. [Google Scholar] [CrossRef] [PubMed]
- Targhetta R, Chavagneux R, Balmes P, Lemerre C, Mauboussin JM, Bourgeois JM, et al. Sonographic lung surface evaluation in pulmonary sarcoidosis: preliminary results. J Ultrasound Med. 1994, 13, 381–388. [Google Scholar] [CrossRef] [PubMed]
- Reissig A, Kroegel C. Transthoracic Sonography of Diffuse Parenchymal Lung Disease The Role of Comet Tail Artifacts. J Ultrasound Med. 2003, 22, 173–180. [Google Scholar] [CrossRef] [PubMed]
- Avouac J, Fransen J, Walker U, Riccieri V, Smith V, Muller C, et al. Preliminary criteria for the very early diagnosis of systemic sclerosis: results of a Delphi Consensus Study from EULAR Scleroderma Trials and Research Group. Ann Rheum Dis. 2011, 70, 476–481. [Google Scholar] [CrossRef]
- Warrick JH, Bhalla M, Schabel SI, Silver RM. High resolution computed tomography in early scleroderma lung disease. J Rheumatol. 1991, 18, 1520–1528. [Google Scholar]
- Jambrik Z, Monti S, Coppola V, Agricola E, Mottola G, Miniati M, et al. Usefulness of ultrasound lung comets as a nonradiologic sign of extravascular lung water. Am J Cardiol. 2004, 93, 1265–1270. [Google Scholar] [CrossRef] [PubMed]
- Doveri M, Frassi F, Consensi A, Vesprini E, Gargani L, Tafuri M, et al. Ultrasound lung comets: new echographic sign of lung interstitial fibrosis in systemic sclerosis. Reumatismo. 2008, 60, 180–184. [Google Scholar]
- Picano E, Frassi F, Agricola E, Gligorova S, Gargani L, Mottola G. Ultrasound lung comets: a clinically useful sign of extravascular lung water. J Am Soc Echocardiogr. 2006, 19, 356–363. [Google Scholar] [CrossRef]
- Gargani L, Romei C, Bruni C, Lepri G, El-Aoufy, Orlandi M, et al. Lung ultrasound B-lines in systemic sclerosis: cut-off values and methodological indications for interstitial lung disease screening. Rheumatology 2022, 61, SI56–SI64. [Google Scholar] [CrossRef] [PubMed]
- Tardella M, Di Carlo M, Carotti M et al. Ultrasound B-lines in the evaluation of interstitial lung disease in patients with systemic sclerosis: cut-off point definition for the presence of significant pulmonary fibrosis. Medicine (Baltimore) 2018, 97, e0566. [Google Scholar] [CrossRef]
- Lacedonia D, Scioscia G, Giardinelli A, Quarato CMI, Sassani EV, Foschino Barbaro MP, et al. The Role of Transthoracic Ultrasound in the Study of Interstitial Lung Diseases: High-Resolution Computed Tomography Versus Ultrasound Patterns: Our Preliminary Experience. Diagnostics (Basel). 2021, 11, 439. [Google Scholar] [CrossRef] [PubMed]
- Hansell DM, Bankier AA, MacMahon H, McLoud TC, Muller NL, Remy J. Fleischner Society: glossary of terms for thoracic imaging 1. Radiology. 2008, 246, 697–722. [Google Scholar] [CrossRef]
- Bussone G, Mouthon L. Interstitial lung disease in systemic sclerosis. Autoimmun Rev. 2011, 10, 248–255. [Google Scholar] [CrossRef] [PubMed]
- Greidinger EL, Flaherty KT, White B, Rosen A, Wigley FM, Wise RA. African-American race and antibodies to topoisomerase I are associated with increased severity of scleroderma lung disease. Chest. 1998, 114, 801–807. [Google Scholar] [CrossRef] [PubMed]
- Assasi S, Sharif R, Lasky RE, McNearney TA, Estrada-Y-Martin RM, Draeger H, et al. Predictors of interstitial lung disease in early systemic sclerosis: a prospective longitudinal study of the GENISOS cohort. Arthritis Res Ther. 2010, 12, R166. [Google Scholar] [CrossRef] [PubMed]
- Wu W, Jordan S, Becker MO, Dobrota R, Maurer B, Fretheim H, et al. Prediction of progression of interstitial lung disease in patients with systemic sclerosis: the SPAR model. Ann Rheum Dis. 2018, 77, 1326–1332. [Google Scholar] [CrossRef] [PubMed]
- Le Goullec N, Duhamel A, Perez T, Hachulla AL, Sobanski V, Faivre JB, et al Predictors of lung function test severity and outcome in systemic sclerosis-associated interstitial lung disease . PLoS One.
- Landini N, Orlandi M, Bruni C, Carlesi E, Nardi C, et al. Computed tomography predictors of mortality or disease progression in systemic sclerosis – interstitial lung disease: a systemic review. Front Med (Lausanne) 2022, 8, 807982. [Google Scholar]
- Rotondo C, Urso L, Praino E, Cacciapaglia F, Corrado A, Cantatore FP, Iannone F. Thoracic lymphoadenopathy as possible predictor of the onset of interstitial lung disease associated to systemic sclerosis. J Scleroderma Relat Disord. 2020, 5, 210–218. [Google Scholar] [CrossRef]
- Hoffmann-Vold A, Maher TM, Philpot EE, Ashrafzadeh A, Barake R, Barsotti S, et al. The identification and management of interstitial lung disease in systemic sclerosis: evidence-based European consensus statements. Lancet Rheumatol. 2020, 2, e71–e83. [Google Scholar] [CrossRef] [PubMed]
- Hasan AA, Makhlouf HA, et al. B-lines: Transthoracic chest ultrasound signs useful in assessment of interstitial lung diseases. Ann Thorac Med. 2014, 9, 99. [Google Scholar] [CrossRef] [PubMed]
- Tardella M, Gutierrez M, Salaffi F, Carotti M, Ariani A, Bertolazzi C, et al. Ultrasound in the assessment of pulmonary fibrosis in connective tissue disorders: correlation with high-resolution computed tomography. J Rheumatol. 2012, 39, 1641–1647. [Google Scholar] [CrossRef]
Figure 1.
Echograms: signs detected by transthoracic lung ultrasound (linear probe between 7-10 MHz). a) thickening and irregularity of the pleural line; b) thickening and irregularity of the pleural line; c) B-lines; d) subpleural cysts.
Figure 1.
Echograms: signs detected by transthoracic lung ultrasound (linear probe between 7-10 MHz). a) thickening and irregularity of the pleural line; b) thickening and irregularity of the pleural line; c) B-lines; d) subpleural cysts.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



