
Submitted:
27 December 2024
Posted:
30 December 2024
You are already at the latest version
Abstract
Air pollution and health effects in communities near industrial areas are a matter of con-cern in Thailand. Elevated air pollution concentrations are associated with morbidity and mortality arising from the lower respiratory tract. In this study, we aimed to assess if liv-ing in a community near a new industrial estate in central Thailand was associated with an elevated incidence of lower respiratory tract illness (LRTI) among the elderly. We used data on hospital admissions from a primary hospital and sub-district health promoting hospitals in six sub-districts located within a radius of 5 kilometers from the industrial estate between 1st November 2023 and 31st March 2024, using a cross-sectional study de-sign. There were 1,311 elderly are living within a radius of 3 kilometers and 1,488 between 3 and 5 kilometers. We found a statistically significant increased risk of hospitalization for LRTI in the elderly living within a radius of less than 3 kilometers (odds ratio 3.43 [95%CI: 1.61- 7.36]), compared to those living in a radius between 3 and 5 kilometers. Our results provide strong support for the associations between hospitalization for LRTI and living distance from the new industrial estate.
Keywords:
hospitalization
; lower respiratory tract illness
; industrial emissions
; industrial estate
; chronic disease
1. Introduction
Exposure to air pollution is a global issue which directly affects respiratory health. In the Global Burden of Disease Study it was estimated that in 2019, exposure to air pollution was responsible for 695,000 deaths and 15.4 million disability adjusted life years (DALYs) due to chronic obstructive pulmonary disease (COPD) and 326,000 deaths and 19.5 million DALYs due to lower respiratory tract infections worldwide [1]. In Asia, between 2010 and 2017, approximately 21.4 million people died from chronic respiratory diseases, although with large differences in mortality between countries. In Thailand, the age-standardized crude mortality rate from chronic respiratory diseases in this period has been around 20 per 100,000 inhabitants per year [2].
Air pollution exposure has a direct impact on the increase in lower respiratory tract illness especially in communities near industrial activity[1]. Lower respiratory tract disease has been strongly associated with air pollution. An increase of 10 μg/m3 in the two-year average of PM2.5 has been associated with a 2.24% increase in the incidence of asthma [3]. NO2 has been associated with daily admissions for lung infections, asthma and COPD, and PM2.5 has been associated with COPD hospital admissions [1]. In China, each 10 µg/m3 increase in PM2.5 has been associated with a 3.51% (95%CI: 0.96-6.12%) increase in the risk of admission for acute lower respiratory infection admission. It has been shown that admissions for lower respiratory tract diseases increase as PM2.5 concentrations increase [4].
People living near the Industrial Estate Islamabad in the industrial sector of the Islamabad Capital Territory in Pakistan (i.e., within a radius of approximately 650 meters) had an increased risk of lower respiratory tract disease, including chronic bronchitis, phlegm and dyspnea [5]. Residents living near a Petrochemical Industrial Complex in seven countries—Argentina (La Plata), Brazil (Rio Grande do Norte), Taiwan (Miaoli, Jenwu, Linyuan, Chunghua, and Yunlin), Thailand (Rayong Province), Spain (Tarragona), Italy (Sardinia and Basilicata) and the United Kingdom (Teesside)—had a significantly higher incidence of cough, wheezing, bronchitis, rhinitis and asthma [6]. Prevalence rates of asthma and rhinoconjunctivitis were found to be 24% and 34%, respectively, among people living near gold mines and copper mines in Northern Chile at an average distance of 2.1 and 1.9 kilometers, respectively [7]. Higher levels of PM2.5 and NOX from industry emissions have also been associated with decreased lung function including a lower forced vital capacity (FVC) and a lower forced expiration volume in 1 s (FEV1) and have been associated with dry cough [8]. The ambient particulate matter pollution-related burden of LRTI and COPD were higher among countries with low and low-middle socio-demographic indices (SDIs), while countries with high-middle SDIs showed the highest burden of tracheal, bronchus, and lung cancer attributable to exposure to ambient particulate matter pollution [1]. People living in developing countries, including in Southeast Asia, are increasingly burdened with outdoor air pollution. This is partly an adverse result of the drive of the industrial sector to develop the economy in the country [9].
Thailand is one of those countries in Southeast Asia in which the industrial sector is developing rapidly towards becoming the heart of the Thai economy. An industrial estate (or park) is an area that is shared by many producers that partly share the same infrastructure and facilities. Industrial estates have become important contributors to the industrial development of the country [10]. Currently, there are 66 locations in all regions of Thailand with various types of industries. They form an important industrial production base in the Association of Southeast Asian Nations (ASEAN), but at the same time air quality and community health are negatively affected, especially in factory areas. NO2 concentration in the industrial area of Rayong have shown to be 10.4 - 34.0 µg/m3, which was significantly higher than in urban and background areas [11]. The average PM2. 5 concentrations were 38.8 ± 25.2 µg/m3 in wet season and 52.7 ± 33.9 µg/m3 in dry season [12]. In Nakhon Ratchasrima the mean value of the 24-hr average PM2.5 concentration in the industrial area was 34.7 µg/m3, significantly higher than in the urban [13]. Communities surrounding Map Ta Phut Industrial Estate in Rayong Province face air pollution problems and have a higher incidence of respiratory diseases due to air pollution [12,14]. Residents living near industrial areas suffer from respiratory diseases due to air pollution. Children living near industrial areas in Rayong, Thailand, particularly with high levels of pollutants are at risk of chronic bronchitis, bronchial asthma, dyspnea and wheezing, persistent cough and persistent phlegm. There is a higher prevalence in communities near industrial areas than in distant communities. Children in schools within 1 kilometer of a petrochemical industry area have shown to have a substantially higher risk of experiencing respiratory symptoms (OR 3.41 [1.70-6.85]) than those in schools between 5 and 10 km from this industry [15]. Air pollution concentrations in the central and surrounding areas in the past 10 years (2013-2022) are likely to improve. But there are still some pollutants that still exceed the standard, especially PM2.5 and NO2. which NO2. from November to March in 2022 found the highest 1-hour average at each measurement point in the range of 21-189 ppb, average 63 ppb. The annual average was in the range of 2-30 ppb, average 10 ppb, found to exceed standard in 2 areas in the central with the highest number of industrial factories[16]. And the highest PM2.5 concentration 24-hour average range between 22-156 µg/m3. In 2023 PM2.5 in Bangkok and its vicinity: the overall image of the area tended to become more severe. The PM2.5 had an average of 31 μg/m3 and there were 97 days that PM2.5 level exceeded the standard[17].
The world population aged 60 years and older is expected to double in the next 35 years. Caring for this elderly population has become an important global healthcare issue. In 2016, more than 1 million people aged 70 years and older died from infections of the lower respiratory tract, with increasing age being the largest factor that increases morbidity and death rates. Advanced age is associated with reduced physiological reserves and an aging immune system [18]. In 2024, Thailand is a country of aged society. In 2023, there were 13.64 million people aged over 60 years (19.5%) [18]. However, there have been no studies on air pollution and its effects on the health of the elderly living in areas near relatively new industries in Thailand. Therefore, in the present study, we aimed to study the effect of a new industrial estate in central Thailand, established less than ten years ago, on air pollution and the health of the elderly population living nearby. We measured the concentrations of PM2.5 and NO2 and evaluated the association between hospitalization of elderly for LRTI and living in communities near this new industrial estate. The results of this study will lead to the determination of measures to prevent and control air pollution and its impact on the health of surrounding communities so that the same problems do not repeat themselves near industrial estates that have been established for a long time. It will also make industry leaders who have factory expansion plans aware of the need for adequate air pollution control measures.
2. Materials and Methods
2.1. Study Area: Communities Near a New Industrial Estate
The study area includes 6 sub-districts in the central region of Thailand. We selected the sub-districts according to distance from a new industrial estate, i.e. areas located within a radius of 5 kilometers around the estate. Communities were divided into those located “near” (0-3 km) and those located “far” (>3-5 km) from the fence the new industrial estate.
2.2. Measurements of Air Pollutants
We measured PM2.5 and NO2 concentrations in the communities within 3 kilometers and those between 3 and 5 kilometers from the new industrial estate. We measured in 4 areas from 17-25 January 2024, continuously 24 hours a day, covering working days and weekends. Measurements were done according to the US EPA standard, using a low-volume PM2.5 air sampler and an NOx Chemiluminescence Analyzer.
2.3. Hospitalization Data
To evaluate the association between, on the one hand, the incidence of hospital admissions due to LRTI among elderly and, on the other hand, living near the industrial estate, LRTI data were obtained from 43 health database files of each of six sub-district health promoting hospitals and one district hospital in the period from 1st November 2023 to 31st March 2024. Using the International Classification of Diseases, Revision 10 (ICD-10), all healthcare contacts due to acute or chronic lower respiratory symptoms by individuals residing in the selected sub-districts were identified. ICD-10 J20-22 codes were used to identify acute LRTI and ICD-10 J40-47 codes to identify chronic LRTI.
We included 2,799 elderly from the six sub-districts in this study. We collected the following data on these elderly from the medical files: reason for hospitalization (lower respiratory tract illness or not), gender, age, body mass index, education level, current occupation, smoking status, history of drinking alcohol, and chronic diseases (diabetes, hypertension, dyslipidemia, etc.).
Because not all covariables were available for all sub-districts (especially smoking data was lacking for 3 sub-districts), we divided the data analysis into two parts: in part one we analyzed the entire elderly population in the study area (2,799 elderly from the six sub-districts), and in part two we analyzed only the data of the sub-districts for which all variables were available. The selected sub-districts for part two were representative of the nearby as well as the remote area population (1,347 elderly from three sub-districts).
2.4. Statistical Data Analysis
We investigated the associations between hospitalization for LRTI and distance from a new industrial estate, using a cross-sectional analytical study design. We used univariable logistic regression analysis to explore unadjusted associations between hospitalization for LRTI and various factors. The data are presented with crude odds ratios, 95% confidence intervals of the crude odds ratios and p-values. Results with p-values < 0.25 were selected for the initial multivariable model.
Multivariable logistic regression analysis was used to investigate the associations between hospitalization for LRTI and distance from the new industrial estate, adjusted for various factors. The analysis was done separately for the entire population and for the subgroup for which all variables were available. The suitability of the model was evaluated using quality of fit. We set the significance level at 0.05. The final model is presented with adjusted odds ratios, 95% confidence intervals of the adjusted odds ratios and p-values.
2.5. Ethics Statement
This study has been reviewed by the Khon Kaen University Ethics Committee for Human Research based on the Declaration of Helsinki and The ICH Good Clinical Practice Guidelines, date of approval is 7th November 2023.
3. Results
3.1. Study Area and Measured Air Pollutants
3.2. Descriptive Statistics of the Study Population
A total of 2,799 elderly (54.38% female) lived in the study area with more than half aged between 60 and 69 years (59.16%), 68.66% with normal BMI, 46.84% living within 3 kilometers of the new industrial estate and 75.46% living downwind of it (when considering north-east to be the prevailing wind direction for this time of the year) (Table 2). The incidence rate of hospitalization for LRTI over the 5-month study period was 2.36%. For the sub-districts for which the complete dataset was available, we found that 77.43% of the elderly had at least one chronic disease, while 6.98% had high blood pressure and 6.09% had diabetes. Most of them were currently not working (anymore) (95.55%) and most had completed only primary school (95.32%). Only 10.10% were current or former cigarette smokers.
3.3. The Association Between the Incidence of LRTI Among Elderly and Living in Communities Near the New Industrial Estate
In the univariable analysis, we found that the elderly living in communities near the industrial estate (0 – 3 km) had higher rates of hospitalization for LRTI (OR 2.15, 95%CI: 1.15-4.06) than those living further away (3 – 5 km) from the estate (Table 3). In the multivariable analysis, we adjusted for various potential confounders: gender, age, BMI, education, smoking and diabetes. The multivariable analysis confirmed the higher rates of hospitalization for LRTI in the elderly living near the industrial estate (OR 3.43; 95%CI: 1.61-7.36, p-value: 0.001).
Also other factors were associated with increased rates of hospitalization in the multivariable model. Being underweight (BMI < 18.50 kg/m2; OR 5.39; 95%CI: 2.00-14.50, p-value: 0.001) or overweight (BMI ≥ 23.00 kg/m2; OR 1.89; 95%CI: 0.85-4.15, p-value: 0.112) led to higher rates of hospitalization. In addition, there was an increased rate of hospitalization for LRTI among the elderly with diabetes (OR 33.89; 95%CI: 15.01-76.05, p-value: <0.001). Compared with those between 60 and 69 years old, subjects aged 70 – 79 (OR 1.33; 95%CI: 0.57- 3.07, p-value: 0.508) and those over 80 years of age (OR 2.50; 95%CI: 1.02- 6.10, p-value: 0.045) had higher rates of hospitalization for LRTI.
4. Discussion
Our study is the first to examine air pollution concentrations in communities near an industrial estate that is no more than 10 years old, and to assess air pollution and its health impact on the elderly. Elderly are a vulnerable group in this new residential environment in which former agricultural communities have transformed into communities near industrial estates. We expect that there will be more communities like this due to economic expansion in many countries around the world.
Previous studies have suggested that communities within a radius of 5 kilometers from industrial zones should be monitoring for air pollution and its health effects. We measured the air concentration of PM2.5 in the area closest to a new industrial estate (0 – 3 kilometers) and an area further away. Both areas were similar in that the PM2.5 concentration was higher than the WHO air quality guidelines (< 37.5 µg/m3). There was no significant difference in PM2.5 concentration between the two areas. Weather conditions could have affected the measured concentrations of PM2.5 [19,20,21].
We found a statistically significant increase in the risk of hospitalization for LRTI in the elderly living within a radius of 3 kilometers (OR 3.43 (95%CI: 1.61-7.36). This is consistent with several previous studies that found an increased risk of respiratory diseases associated with residential proximity to industrial zones. Adults living in communities less than 650 meters away from the Industrial Estate Islamabad in Pakistan had a significant increase in chronic bronchitis, phlegm, wheezing and dyspnea [5]. In Northern Chile, communities near gold mines and copper mines had a high prevalence of asthma [7]. A study in 7 countries—Argentina (La Plata), Brazil (Rio Grande do Norte), Taiwan (Miaoli, Jenwu, Linyuan, Chunghua, and Yunlin), Thailand (Rayong Province), Spain (Tarragona), Italy (Sardinia and Basilicata), and the United Kingdom (Teesside)—found that the incidence of bronchitis, asthma, cough, wheezing and rhinitis were associated with living near a petrochemical industrial complex [6]. Exposure to industrial air pollution in residencies less than 5 km from industrial areas has been associated with respiratory symptoms, phlegm, cough [9,21] and lower lung function parameters (FEV1, FVC) [8]. Among adults living within a 5 km radius of an industrial area in Malaysia 34.5% experienced coughing and 25.5% chest tightness [9]. In New York State, a study found strong associations between living within 5 km of a biorefinery facility and respiratory emergency department visit rates related to (exacerbations of) emphysema, asthma, chronic bronchitis and chronic airway obstruction [22].
We found significant evidence of an increased risk of hospitalization for LRTI among elderly with diabetes (OR 33.98; 95%CI: 15.01-76.05). This is consistent with a study in Japan that found significant associations between diabetes and mortality from respiratory infection [12]. Also, significant associations have been found between diabetes and mortality from respiratory infection among both men and women (HR 1.39; 95%CI, 1.10–1.76 and HR 2.30; 95%CI, 1.71–3.11, respectively) [19]. It was also found that being either underweight (< 18.50 kg/m2) or overweight (≥ 23.00 kg/m2) was associated with hospitalization for LRTI in the elderly. For the underweight elderly we found an OR of 5.39 (95%CI: 2.00- 14.50) and for the overweight an OR of 1.89 (95%CI: 0.85- 4.15) compared with the normal-weight elderly. Also, increasing age is an important factor that increases morbidity and mortality. It is associated with reduced physiological reserves and an aging immune system. Worldwide, in 2016, more than 1 million people aged 70 years or over died from lower respiratory tract infections [23]. In the USA, it was found that increasing age is associated with the incidence of emphysema to the extent of 0.11 and 0.06 for every 2 μg/m3 -unit increase in PM2.5 and 10 ppb NOx [20]. Increasing age is associated with respiratory disease, characterized by increased inflammation and decreased lung function, including asthma and COPD [24]. The results from our study support age as an important risk factor for hospitalization due to LRTI. For those older than 80 years, we found an OR of 2.50 (95%CI: 1.02- 6.10) compared to those aged 60 to 69 years.
We found an association between having had higher education and having been hospitalized for LRTI (OR 3.06 [95%CI: 0.95-9.91]). We assume that this association results from the fact that education increases access to health services. Education leads to better job opportunities and higher income, making it easier to access healthcare services [25,26]. Smoking is an important risk factor for severe LRTI. Also, our study confirmed that cigarette smoking increased the risk of hospitalization for LRTI in the elderly [OR 1.41 [95%CI: 0.40-5.01]). Previous studies have found that current smokers were twice as likely to have asthma and that there is an increased risk of respiratory disease in smokers who have chronic disease [15,22,27,28,29].
A major strength of our study is that we were able to describe both air pollution and health effects. Firstly, we measured PM2.5 and NO2 in the community (Table 1). Secondly, we analyzed the association between distance between communities and the new industrial estate. The results of our study strongly support the proposition that nearby areas are more at risk. Nevertheless, because PM2.5 and NO2 concentrations were similar in all measured areas, we were unable to identify the causal exposures that led to the elevated risk of hospitalization due to LRTI in the elderly living near the industrial estate. It is likely that industrial emissions which we did not measure could explain the associations that we found in this study.
5. Conclusions
We found that the concentration of PM2.5 in areas close to the industrial area within 0-3 kilometers was not different from the area next to it. However, it was found that elderly living near industrial areas were more affected by their health. It was found that elderly people who live near industrial areas have a higher incidence of hospitalization due to LRTI than elderly who live next to them. In addition, having diabetes mellitus, body mass index less than normal and education level is also associated with risk of hospitalization due to LRTI.
Elderly people who live near industries are a high-risk group that requires screening and health monitoring especially lower respiratory system diseases. Especially during the dusty season, from November to March, it is crucial for local health service units to monitor dust concentration levels in the air. This is important for vulnerable populations, such as elderly individuals with diabetes or those with an abnormal body mass index (BMI). Given their increased susceptibility to respiratory issues, these groups should also undergo regular screening for lower respiratory tract diseases, which can be exacerbated by air pollution. A limitation of our study is the incompleteness of the secondary data from 43 health databases on many variables, such as occupational history, length of living in the community, family history of chronic disease, day of admission and date of discharge from the hospital and the precise symptoms of lower respiratory tract illness. A future study should, in addition to collecting primary data on air samples, also collect primary data on the health effects of the elderly. This will provide information about symptoms and important factors that affect lower respiratory tract illnesses.
Author Contributions
Conceptualization, Ronsmans S., Pirawan W.; methodology, Ronsmans S., Pirawan W.; formal analysis, Pirawan W. and Ronsmans S.; investigation, Pirawan W.; resources, Pirawan W.; data curation, Pirawan W.; writing—original draft preparation, Pirawan W., Ronsmans S; writing—review and editing, Ronsmans S, Chananya J., Yuparat L., Vanoirbeek J. and Wipharat, Ph.; visualization, Pirawan W., Ronsmans S.; supervision, Ronsmans S; Chananya J.; funding acquisition, Chananya J., Pirawan W. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by National Research Council of Thailand (NRCT)
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Ethics Committee of Khon Kaen University (protocol code HE662222 and date of approval, 7th November 2023), for studies involving humans.
Informed Consent Statement
This project has been considered by the Human Ethics Committee of Khon Kaen University and has been classified as a human research project that is eligible for expedited review. Because the risk is very low by using secondary data from health databases that are already stored in the regular care system. The identity of the volunteer cannot be determined.
Data Availability Statement
No new data were created in this study. Data sharing is not applicable to this article.
Acknowledgments
This project received information on the health of the elderly from the Provincial Public Health Office, District Hospital, Sub-district Health Promoting Hospitals and received support for collecting PM2.5 and NO2 samples from Sub-district health promotion hospitals, schools, and temples in the target areas in the central region, Thailand. The National Research Council of Thailand and the Department of Disease Control, Ministry of Public Health supported with a research scholarship. The researchers would like to thank them very much for their support in this research.
Conflicts of Interest
The authors declare no conflicts of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
References
- Wu, Y.; Song, P.; Lin, S.; Peng, L.; Li, Y.; Deng, Y.; Deng, X.; Lou, W.; Yang, S.; Zheng, Y.; Xiang, D.; Hu, J.; Zhu, Y.; Wang, M.; Zhai, Z.; Zhang, D.; Dai, Z.; Gao, J. Global Burden of Respiratory Diseases Attributable to Ambient Particulate Matter Pollution: Findings From the Global Burden of Disease Study 2019. Frontiers of Public Health 2021, 9, 740800. [Google Scholar] [CrossRef]
- Baptista, E. A.; Dey, S.; Pal, S. Chronic respiratory disease mortality and its associated factors in selected Asian countries: evidence from panel error correction model. BMC Public Health 2021, 21, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Requia, W. J.; Adams, M. D.; Koutrakis, P. Association of PM2.5 with diabetes, asthma, and high blood pressure incidence in Canada: A spatiotemporal analysis of the impacts of the energy generation and fuel sales. Science of the Total Environment 2017, 584-585, 1077–1083. [Google Scholar] [CrossRef] [PubMed]
- Luong, L. T. M.; Dang, T. N.; Thanh Huong, N. T.; Phung, D.; Tran, L. K.; Van Dung, D.; Thai, P. K. Particulate air pollution in Ho Chi Minh city and risk of hospital admission for acute lower respiratory infection (ALRI) among young children. Environmental Pollution 2019, 257, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Bano, R.; Khayyam, U. Industrial air pollution and self-reported respiratory and irritant health effects on adjacent residents: a case study of Islamabad Industrial Estate (IEI). Air Quality, Atmosphere & Health 2021, 14, 1709–1722. [Google Scholar]
- Chang, W.-W.; Boonhat, H.; Lin, R.-T. Incidence of Respiratory Symptoms for Residents Living Near a Petrochemical Industrial Complex: A Meta-Analysis. International Journal of Environmental Research and Public Health 2020, 17, 1–16. [Google Scholar] [CrossRef]
- Herrera, R.; Radon, K.; von Ehrenstein, O. S.; Cifuentes, S.; Muñoz, D. M.; Berger, U. Proximity to mining industry and respiratory diseases in children in a community in Northern Chile: A crosssectional study. Herrera et al. Environmental Health 2016, 15, 1–10. [Google Scholar] [CrossRef]
- Baptista, E. A.; Dey, S.; Pal, S. The effect of industry-related air pollution on lung function and respiratory symptoms in school children. Environmental Health 2018, 17, 1–10. [Google Scholar]
- Isa, K. N. M.; Som, N. A. N. M.; Jalaludin, J.; Hashim, N. H. Effects of Residential Proximity to Industrial Zone on Respiratory Symptoms among Residents in Parit Raja, Batu Pahat. Malaysian Journal of Medicine and Health Sciences 2024, 20, 168–174. [Google Scholar]
- Yamsrual, S.; Sasaki, N.; Tsusaka, T. W.; Winijkul, E. Assessment of local perception on eco-industrial estate performances after 17 years of implementation in Thailand. Environmental Development 2019, 32, 1–22. [Google Scholar] [CrossRef]
- Sillapapiromsuk, S.; Koontoop, G.; Bootdee, S. Health Risk Assessment of Ambient Nitrogen Dioxide Concentrations in Urban and Industrial Area in Rayong Province, Thailand. TRENDS IN SCIENCES 2022, 19, 1–13. [Google Scholar] [CrossRef]
- Muenmee, S.; Bootdee, S. Health risk assessment of exposure PM2.5 from industrial area in Pluak Daeng district, Rayong province. Naresuan Phayao J 2021, 14, 95–110. [Google Scholar]
- Thongsaeng, P.; Karuchit, S.; Pongkiatkul, P. Concentration and chemical composition of PM2.5 in Nakhon Ratchasima city. Engineering Journal of Research and Development 2018, 30. [Google Scholar]
- Phantu, S.; Kaenbubpha, K.; Ployprom, N.; Bootdee, S. Health Risk Assessment of PM2.5 exposure in Dry season from Map Ta Phut Town Municility in Rayong Province. Journal of Science and Technology Nakhon Sawan Rajabhat University 2022, 14. [Google Scholar]
- Asa, P.; Jinsart, W. Effects of Air Pollution Related Respiratory Symptoms in Schoolchildren in Industrial Areas Rayong, Thailand. EnvironmentAsia 2016, 9, 116–123. [Google Scholar]
- Department, P. C. The state of air and noise pollution in Thailand. 2021. [Google Scholar]
- Department, P. C. Thailand state of pollution report 2023. 2024. [Google Scholar]
- Thailand, N. S. o. Summary of the performance of the elderly in Thailand 2023. 2024. [Google Scholar]
- Jawjit, S.; Pibul, P.; Muenrach, N.; Kuakul, A. Risk Assessment of PM10 Exposure of Stone Crushing Plant Nearby and Further Communities in Nakhon Si Thammarat. Journal of Science and Technology 2018, 27. [Google Scholar]
- Tantipanjaporn, T.; Srisakultiew, N.; Sukhantho, B. Health Risk Assessment of Inhalation Exposure to Respirable Dust among Workers in a Rice Mill in Kamphaeng Phet Province. Srinagarind Med J 2019, 34, 482–489. [Google Scholar]
- Qing, C.; Hehua, Z.; Yuhong, Z. Ambient air pollution and daily hospital admissions for respiratory system–related diseases in a heavy polluted city in Northeast China. Environmental Science and Pollution Research 2020, 27, 10055–10064. [Google Scholar]
- Eun, K. L.; Xiaobo, X. R.; Wangjian, Z.; Beth, J. F.; Haider, A. K.; Xuesong, Z.; Shao, L. Residential Proximity to Biorefinery Sources of Air Pollution and Respiratory Diseases in New York State. Environmental Science and Technology 2021, 55, 10035–10045. [Google Scholar]
- Watson, A.; Wilkinson, T. M. A. Respiratory viral infections in the elderly. Therapeutic Advances in Respiratory Disease 2021, 15, 1–17. [Google Scholar] [CrossRef]
- Wang, M.; Muraki, I.; Liu, K.; Shirai, K.; Tamakoshi, A.; Hu, Y.; Iso, H. Diabetes and Mortality From Respiratory Diseases: The Japan Collaborative Cohort Study. Journal of Epidemiology 2020, 30, 457–463. [Google Scholar] [CrossRef] [PubMed]
- George, C.; Ducatman, A. M.; Conway, B. N. Increased risk of respiratory diseases in adults withType 1 and Type 2 diabetes. Diabetes Research and Clinical Practice 2018, 142, 46–55. [Google Scholar] [CrossRef] [PubMed]
- Do, J.; Park, C.-H.; Lee, Y.-T.; Yoon, K. J. Association between underweight and pulmonary function in 282,135 healthy adults: A cross-sectional study in Korean population. Scientific Reports 2019, 9, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Farihah Mohmad Shamsuddin, A.; Jalaludin, J.; Haslina Hashim, N. Exposure to industrial air pollution and its association with respiratory symptoms among children in Parit Raja, Batu Pahat. Earth and Environmental Science 2022, 1013, 1–11. [Google Scholar] [CrossRef]
- Chen, T.; Chen, F.; Wang, K.; Ma, X.; Wei, X.; Wang, W.; Huang, P.; Yang, D.; Xia, Z.; Zhao, Z. Acute respiratory response to individual particle exposure (PM(1.0), PM(2.5) and PM(10)) in the elderly with and without chronic respiratory diseases. Environmental pollution (Barking, Essex : 1987) 2021, 271, 116329. [Google Scholar] [CrossRef]
- Wang, M.; Fang, H. The effect of health education on knowledge and behavior toward respiratory infectious diseases among students in Gansu, China: a quasi-natural experiment. BMC Public Health 2020, 20, 1–13. [Google Scholar] [CrossRef]
Figure 1.
Map showing the new industrial estate in central Thailand, the six surrounding sub-districts, the location of the hospitals and the incidence rate of hospitalization for LRTI in the elderly population.
Figure 1.
Map showing the new industrial estate in central Thailand, the six surrounding sub-districts, the location of the hospitals and the incidence rate of hospitalization for LRTI in the elderly population.
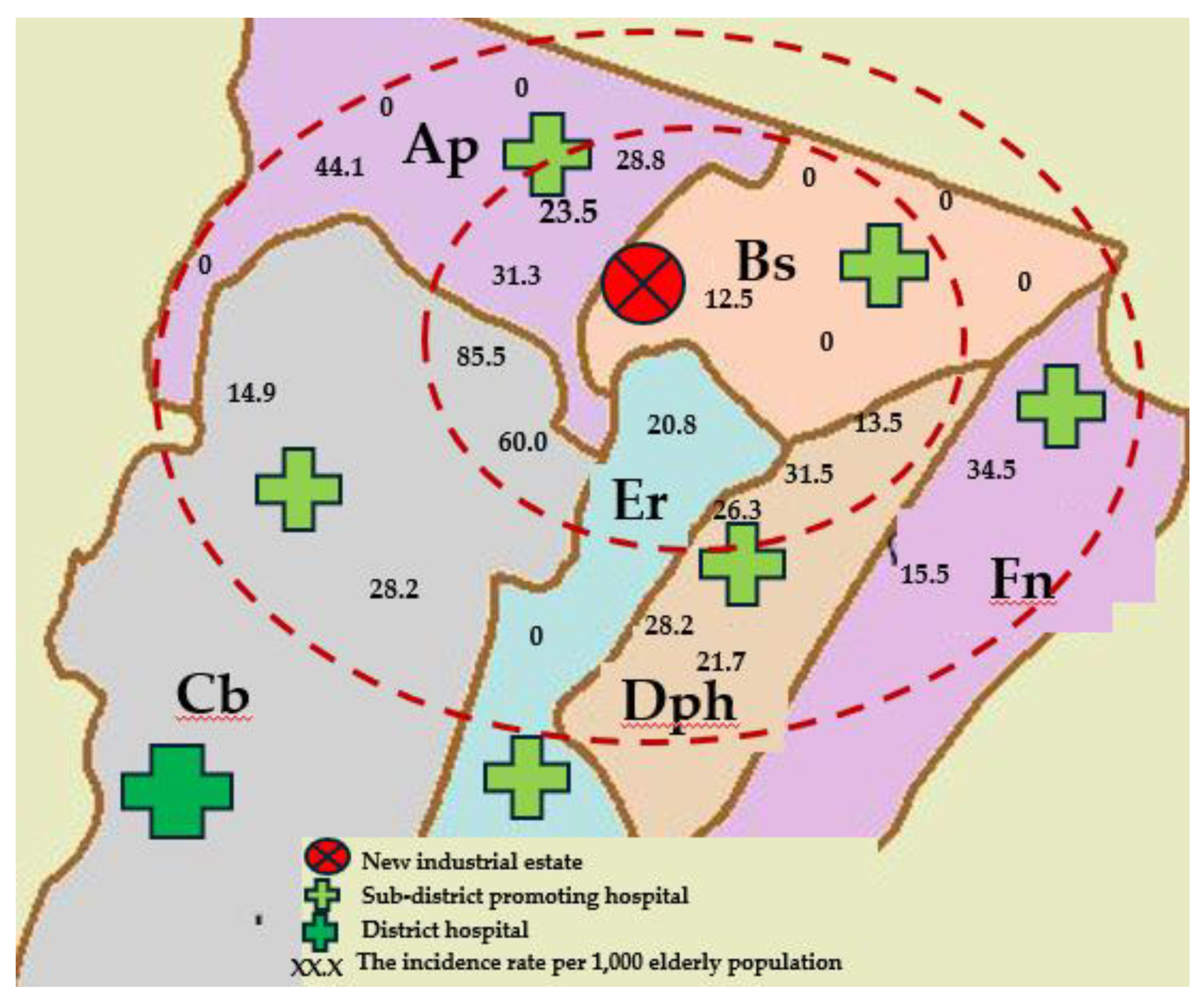

Table 1.
Descriptive statistics of PM2.5 and NO2 concentrations (18-25th January 2024).
| PM2.5 | NO2 | |||||||
| Distance | Min | Median | Mean (SD) | Max | Min | Median | Mean (SD) | Max |
| Near (0-3 km) | ||||||||
| Ap | 23.1 | 34.3 | 32.5 (6.8) | 41.4 | 0.004 | 0.005 | 0.005 (0.0002) | 0.005 |
| Bs | 17.5 | 41.6 | 38.8 (10.1) | 49.4 | 0.012 | 0.013 | 0.013 (0.0003) | 0.013 |
| Far (>3-5 km) | ||||||||
| Cb | 29.9 | 34.6 | 38.3 (7.6) | 50.9 | 0.004 | 0.004 | 0.004 (0.0005) | 0.005 |
| Dph | 32.6 | 41.3 | 44.6 (10.7) | 58.5 | 0.002 | 0.002 | 0.002 (0.0004) | 0.003 |
SD: Standard Deviation.
Table 2.
Baseline characteristics of the study population.
| Factors | Entire region (n = 2,799) | Subregion (n = 1,347) | |||
|---|---|---|---|---|---|
| Number | Percentage (%) | Number | Percentage (%) | ||
| LRTI | |||||
| No | 2,733 | 97.64 | 1,305 | 96.88 | |
| Yes | 66 | 2.36 | 42 | 3.12 | |
| Gender | |||||
| Female | 1,522 | 54.38 | 745 | 55.31 | |
| Male | 1,277 | 45.62 | 602 | 44.69 | |
| Age (years) | |||||
| 60-69 | 1,656 | 59.16 | 776 | 57.61 | |
| 70-79 | 721 | 25.76 | 344 | 25.54 | |
| ≥ 80 | 422 | 15.08 | 227 | 16.85 | |
| Mean (±SD) | 69.48 (± 8.36) | 69.71 (± 8.43) | |||
| Median (Min:Max) | 67 (60: 113) | 68 (60:97) | |||
| BMI (kg/m2) | |||||
| Normal weight (18.50-22.99 kg/m2) | 1187 | 68.66 | 660 | 49.00 | |
| Underweight (<18.50 kg/m2) | 152 | 10.66 | 124 | 9.20 | |
| Overweight (≥ 23.00 kg/m2) | 460 | 20.66 | 563 | 41.80 | |
| Mean (±SD) | 22.84 (±2.84) | 22.73 (±3.61) | |||
| Median (Min:Max) | 23.11 (10.59:41.87) | 22.35 (10.59:41.87) | |||
| Chronic disease | |||||
| N/A | 1,428 | 51.02 | 0 | 0 | |
| Any chronic disease | 1,043 | 37.26 | 1,043 | 77.43 | |
| Hypertension | 104 | 3.72 | 94 | 6.98 | |
| Diabetes | 89 | 3.18 | 82 | 6.09 | |
| Education level | |||||
| N/A | 1,428 | 51.02 | 0 | 0 | |
| Primary school | 1,305 | 46.62 | 1,284 | 95.32 | |
| Higher than Primary school | 66 | 2.07 | 63 | 4.68 | |
| Occupation | |||||
| N/A | 1,428 | 51.02 | 0 | 0 | |
| None | 1,287 | 46.38 | 1,287 | 95.55 | |
| Farmer | 36 | 1.29 | 36 | 2.67 | |
| Laborer | 26 | 0.93 | 12 | 0.89 | |
| Other | 4 | 0.14 | 10 | 0.74 | |
| Smoking cigarettes | |||||
| N/A | 1,428 | 51.02 | 0 | 0 | |
| No | 1,235 | 44.12 | 1,211 | 89.90 | |
| Yes (current or previous) | 136 | 4.86 | 136 | 10.10 | |
| Drinking alcohol | |||||
| N/A | 1,428 | 51.02 | 0 | 0 | |
| No | 1,235 | 44.12 | 1,066 | 79.14 | |
| Yes (current or previous) | 136 | 4.86 | 281 | 20.86 | |
| PM2.5 average concentration (µg/m3 ) | |||||
| Low (<37.5 µg/m3) | 698 | 24.95 | 0 | 0 | |
| High (≥ 37.5 µg/m3) | 2,101 | 75.05 | 1,347 | 100 | |
| NO2 average concentration (ppm) | |||||
| Low (< 0.17 ppm) | 2,799 | 100 | 1,347 | 100 | |
| High (≥ 0.17 ppm) | 0 | 0 | 0 | 0 | |
| Wind direction | |||||
| Upwind | 687 | 24.54 | 285 | 21.16 | |
| Downwind | 2,112 | 75.46 | 1,062 | 78.84 | |
| Distance from home to the new estate | |||||
| Far (>3-5 km) | 1,488 | 53.16 | 760 | 56.42 | |
| Near (0-3 km) | 1,311 | 46.84 | 587 | 43.58 | |
Table 3.
Univariable and multivariable analysis of the associations between hospitalization for lower respiratory tract illness (LRTI) and distance from a new industrial estate, adjusted for various factors, for a subregion (n = 1,347) .
Table 3.
Univariable and multivariable analysis of the associations between hospitalization for lower respiratory tract illness (LRTI) and distance from a new industrial estate, adjusted for various factors, for a subregion (n = 1,347) .
| Factors | Number | LRTI | Univariable analysis | Multivariable analysis | |||||
|---|---|---|---|---|---|---|---|---|---|
| n | n | (%) | OR | 95% CI | p-value | ORadj | 95% CI | p-value | |
| Overall | 1,347 | 42 | 3.12 | ||||||
| Distance | 0.017 | 0.001 | |||||||
| Far (> 3-5 km) | 760 | 16 | 2.11 | 1 | 1 | ||||
| Near (0-3 km) | 587 | 26 | 4.43 | 2.15 | 1.15-4.06 | 3.43 | 1.61- 7.36 | ||
| Gender | 0.100 | 0.173 | |||||||
| Female | 745 | 18 | 2.42 | 1 | 1 | ||||
| Male | 602 | 24 | 3.99 | 1.67 | 0.90- 3.12 | 1.80 | 0.89-3.67 | ||
| Age (Years) | 0.296 | 0.021 | |||||||
| 60-69 | 776 | 21 | 2.71 | 1 | 1 | ||||
| 70-79 | 344 | 10 | 2.91 | 1.08 | 0.50-2.31 | 0.850 | 1.33 | 0.57- 3.07 | |
| ≥80 | 227 | 11 | 4.85 | 1.83 | 0.87- 3.86 | 0.112 | 2.50 | 1.02- 6.10 | |
| BMI | 0.001 | 0.280 | |||||||
| Normal weight | 660 | 12 | 1.82 | 1 | 1 | ||||
| Underweight | 124 | 11 | 8.87 | 5.25 | 2.26-12.20 | <0.001 | 5.39 | 2.00- 14.50 | |
| Overweight | 563 | 19 | 3.37 | 1.88 | 0.90-3.92 | 0.089 | 1.89 | 0.85- 4.15 | |
| Education | 0.055 | 0.001 | |||||||
| Primary | 1,284 | 95.32 | 2.88 | 1 | 1 | ||||
| Higher than primary | 63 | 4.68 | 7.94 | 2.90 | 1.10-7.66 | 3.06 | 0 .95-9.91 | ||
| Smoking cigarettes | 0.899 | 0.648 | |||||||
| No | 1,211 | 89.90 | 3.14 | 1 | 1 | ||||
| Yes (current or former) | 136 | 10.10 | 2.94 | 0.94 | 0 .33-2.66 | 1.41 | 0.40-5.01 | ||
| Diabetes | <0.001 | <0.001 | |||||||
| No | 1,265 | 93.91 | 1.74 | 1 | 1 | ||||
| Yes | 82 | 6.09 | 24.39 | 18.22 | 9.45-5.16 | 33.89 | 15.01-76.05 | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



