
Submitted:
26 December 2024
Posted:
27 December 2024
You are already at the latest version
Abstract
Antimicrobial stewardship programs (ASPs) and diagnostic stewardship programs (DSPs) are es-sential strategies for effectively managing infectious diseases and tackling antimicrobial resistance (AMR). This narrative review highlights the necessity of a multidisciplinary approach, advocating for the involvement of diverse healthcare professionals to support comprehensive stewardship practices in pediatric care. Emphasizing the importance of setting-specific interventions across inpatient, outpatient, and emergency contexts, the review calls for enhanced education and col-laboration among healthcare providers and families. This analysis also underscores the cost-effectiveness of ASPs and explores metrics critical to evaluating their success in pediatrics, focusing on outcomes that go beyond antibiotic consumption to include metrics such as AMR rates. The manuscript further examines emerging opportunities and ongoing challenges in ASP implementation, outlining future research directions. Key priorities include large-scale studies to assess the long-term impacts of ASPs, cost-effectiveness evaluations of pediatric-specific diagnostic tools, and the potential for integrating artificial intelligence to support clinical decisions. Ad-dressing these areas will strengthen the effectiveness and sustainability of ASPs, ultimately con-tributing to global efforts against AMR and improving pediatric health outcomes.
Keywords:
antibiotics
; antimicrobial resistance
; antimicrobial stewardship programs
; pediatric infectious diseases
; point-of-care tests
; rapid diagnostic tests
1. Introduction
Programs focused on the appropriate use of antimicrobials and diagnostic tools are essential for managing infectious diseases effectively and efficiently [1]. Antimicrobial stewardship programs (ASPs) have become a cornerstone in the fight against antimicrobial resistance (AMR), a critical public health issue recognized globally also in the pediatric population [1,2,3].
One of the primary goals of pediatric ASPs is to reduce the inappropriate use of antibiotics, which remains a significant challenge [1]. Children are frequently prescribed antibiotics, especially in outpatient settings, and unnecessary use or not optimal doses are common [4,5,6], leading to potential adverse drug reactions and the emergence of resistant organisms, which can complicate future treatment options and lead to poorer health outcomes [7]. Moreover, the developing immune system and microbiota in children can be profoundly affected by antimicrobial exposure, with long-term health implications including allergies, asthma, and obesity [8,9,10,11].
In pediatrics, these programs should rely on the best available evidence, ideally from studies specifically conducted in children, considering the unique aspects related to age, growth, and physiology. However, despite significant strides made in adult healthcare, there is a relative paucity of literature and consensus on the best practices tailored for pediatric settings [12]. Indeed, the pediatric population presents unique challenges and opportunities for ASPs due to differences in pharmacokinetics, disease epidemiology, and the impact of antimicrobial use on developing microbiomes [4,13,14].
Successful implementation of pediatric ASPs requires a multidisciplinary approach, not only with collaboration between different healthcare workers but also engaging with patients and their families through education, helping in reducing unnecessary antibiotics use and increasing adherence [15]. This narrative review provides an overview of current knowledge on ASPs and diagnostic stewardship programs (DSPs) in pediatric settings based on existing literature, expert opinions, and case studies. We will focus on the definition of ASP and DSP, the different healthcare workers that should be involved, the different types of ASPs and DSPs, and their implementation in different pediatric settings, considering inpatient settings, outpatient settings, and the pediatric emergency departments (PEDs). Moreover, we will focus on the cost-efficacy of these programs and on the different metrics that should be used to evaluate the efficacy of the implementation of an ASP or DSP in pediatric care, considering not only antibiotic consumption but also other outcomes, such as, for example, antimicrobial resistance rate. Finally, we will focus on the different steps for the creation and implementation of these programs and on the challenges related to their implementation and sustainability.
2. What is a Antibiotic Stewardship Program (ASP) and a Diagnostic Stewardship Program (DSP)?
ASP can be defined as a comprehensive set of actions designed to promote the responsible use of antibiotics [16,17]. This involves selecting the appropriate drug, dose, timing, frequency, and route of administration based on knowledge of the antimicrobial spectrum and pharmacokinetic/pharmacodynamic data, ideally tailored to the specific clinical condition.
DSP encompasses activities that complement ASP by ensuring the appropriate use of diagnostic tests in clinical settings [18,19]. It aims to direct testing towards the appropriate patients, thereby improving the correct use of antibiotics. This includes selecting the most suitable microbiological tests for the clinical situation, executing these tests correctly, and choosing the right tests to assess the patient’s initial clinical conditions and response to treatment. Proper execution and evaluation of antibiotic sensitivity tests are fundamental for managing infectious diseases. Additionally, evaluating plasma (and potentially tissue) concentrations of drugs, when available, can further support the optimal management strategy.
ASPs and DSPs must be implemented in a coordinated and parallel manner, as they are closely interdependent.
3. Which healthcare workers should be involved in an ASP? The Antimicrobial Stewardship Team
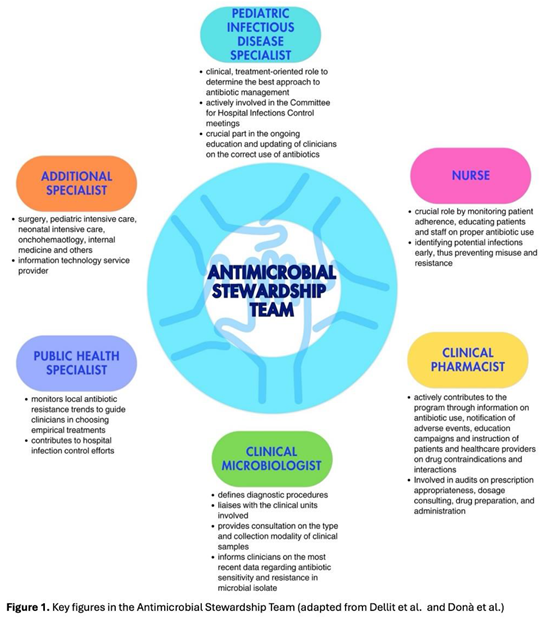
Every ASP requires a multidisciplinary team tasked with defining governmental policies for the responsible use of antibiotics, aligning with infection control protocols [20,21]. The Antimicrobial Stewardship Team (AST) in pediatric care should be led by a pediatric infectious disease specialist or, in absence, by a pediatrician with expertise in antibiotic therapy. This role is essential for ensuring that treatment recommendations and guidelines are grounded in the latest evidence in the field. Having a physician specializing in pediatric infectious diseases strengthens the program’s credibility. Direct engagement with prescribing physicians and the clinical governance committee is crucial: interaction with the former helps educate them on improved prescribing practices and fosters collaboration in discussing challenging cases or barriers faced during the program’s implementation; engagement with the latter is necessary to secure formal approval and financial support for the program’s execution [22].
Additionally, the team should also include at least one expert from each relevant field: a nurse, a clinical pharmacist, a clinical microbiologist, a public health specialist, and other physicians depending on the wards involved in the implementation. Each team member should have clearly defined roles [16,23]. Although nurses are not formal prescribers in most countries, they play a crucial role in antimicrobial communication and management, actively engaging in encouraging, reminding, and overseeing prescribers’ choices while questioning decisions when necessary. Their involvement has shown significant potential in optimizing antimicrobial use, especially in areas such as monitoring the choice of antimicrobial, timing, therapy duration, and dosing. Clinical pharmacists play an important role in promoting the rational use of antimicrobial drugs and educating physicians; their competency on new drugs available and on possible adverse events or possible interactions with other drugs play a crucial role, especially in complicated patients in more fragile settings. Clinical microbiologists are essential not only in the management of acute cases, during which they could provide crucial information regarding the type of the pathogen and the spectrum of resistance to target antibiotic therapy, but also in the choice of which antimicrobial should be limited or reassessed in a specific setting. Indeed, they should provide, on a regular basis, the epidemiology of the hospital, with the recent burden of antibiotic resistance in the different wards, to allow for updating recommendations on empirical antibiotic therapy [22]. The involvement of physicians from the ward where the program is implemented is essential to establish a bridge between the AST and the ward team, fostering cooperation and collaboration across both groups. This multidisciplinary nature of the AST ensures a comprehensive and integrated approach to optimal antibiotic treatment management (Figure 1).
4. Different Types of ASP
ASP interventions can be classified as core strategies (i.e., pre-authorization of restricted antimicrobials and prospective audit and feedback) or minor interventions [16] or interventions before the prescriptions and after [24]. According to Infectious Diseases Society of America and The Society for Healthcare Epidemiology of America (IDSA/SHEA) guidelines, programs should decide whether to include one core strategy or a combination of both strategies based on the availability of facility-specific resources for consistent implementation, but some implementation is essential [25]. Each of these interventions has pros and cons (Figure 2).
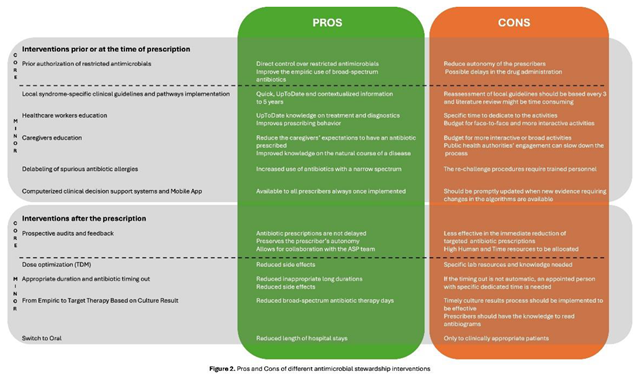
4.1. What Interventions Are Effective Prior to or at the Time of Prescription?
4.1.1. Core Strategy
a. Pre-authorization of restricted antimicrobials: A pharmacist or an ASP clinician must approve the prescription of a specific antimicrobial before the pharmacy releases it. This provides direct control over restricted antimicrobials and mostly improves the empiric use. The pitfalls of this strategy are the reduced autonomy of the prescribers and possible delays in the drug administration [16,26].
4.1.2. Minor Elements
a. Local syndrome-specific clinical guidelines and pathways implementation: Local clinical guidelines (LCG) or clinical pathways (CPs) targeted common syndromes (e.g., respiratory tract infections, urinary tract infections, skin infections, and surgical prophylaxis), are adapted from national or international evidence-based guidelines to fit specific healthcare settings, addressing local epidemiology, diagnostic capabilities, and drug availability [16,24]. According to recommendations from the World Health Organization (WHO) and the IDSA/SHEA regarding ASP implementation, local clinical guidelines should be accompanied by a strategy for implementation (i.e., health-care workers education or clinical pathways creation or audit and feedback [24,25]. Moreover, to guide clinical guidelines contextualization, tools such as weighted-incidence syndrome combination antibiograms (WISCA) should be adopted. Indeed, WISCA provides highly informative estimates on antibiotic coverage patterns weighted on the most prevalent pathogens overcoming the limitation of combination antibiograms [26,27,28].
b. Healthcare workers’ education: Face-to-face or online talks, workshops, clinical case simulations, and toolkits are fundamental for optimal patient care to ensure knowledge of the most updated management strategies [29,30,31]. Continuous education will ensure that the most up-to-date treatments, diagnostic tools, and strategies are acknowledged. Healthcare workers’ education offers different advantages for stewardship training and can improve effectively prescribing behavior, especially when paired with other interventions [32].
c. Computerized clinical decision support (CDS): Tools and mobile applications enhance ASP by personalizing antibiotic regimens based on patient-specific factors and providing instant access to guidelines and dosing calculators, thereby improving adherence to stewardship principles and preventing dosing errors in real-time [33].
d. Caregivers education: Caregivers should be informed about the correct use, administration, storage, and disposal of antimicrobials, including antibiotics, to become allies in combating AMR and improve children’s outcomes. Mass education campaigns informing the public, with messages about the ineffectiveness of antibiotics against viral infections such as respiratory syncytial virus (RSV) and influenza, can be implemented, as well as direct education from healthcare workers addressing specific syndromes. Having both approaches enhances overall public awareness of AMR and helps counter widespread misinformation and misconceptions about antibiotics. Interventions focusing on improving the quality of parent-healthcare provider communication have repeatedly evidenced the greatest impact on rates of inappropriate prescribing [34,35].
e. Guidelines for antibiotic allergy and delabeling of spurious antibiotic allergies: Antibiotics are the cause of 40% of IgE and non-IgE-mediated allergic reactions to drugs, and the most allergenic are the beta-lactams. Still, up to 95% of patients reporting a penicillin allergy can tolerate a rechallenge [36,37]. Performing dedicated antibiotic allergy history-taking, with or without dedicated skin testing to remove false antibiotic allergy labels, can be an effective strategy to prevent the unnecessary avoidance of effective antibiotics and the indiscriminate use of broad-spectrum antibiotics [38].
f. Antimicrobial order form: Generic antimicrobial order forms, where the prescriber specifies the drug and regimen, may be utilized for any anti-infective or solely for restricted antimicrobials. These forms require the clinician to provide an indication for the antimicrobial and may also request the anticipated duration of therapy. By using these forms, documentation and communication regarding antimicrobial therapy can be enhanced, and data collection for medication use evaluations becomes more streamlined [39]. When restricted agents are prescribed, these forms may require clinicians to confirm adherence to institution-specific criteria, supporting appropriate prescribing and simplifying the approval process.
4.2. What Interventions Are Effective After the Time of Prescription?
4.2.1. Core Strategy
a. Prospective audits and feedback (PAF): Feedback can be provided in real-time or on a defined timing basis and can be delivered directly via the prescription tool or face-to-face during consultation meetings with the AST. This is usually a persuasive intervention where the rationale behind the recommendations is provided to convince the prescriber to modify the antimicrobial prescription, but without imposing therapeutic choices (handshake stewardship). Different from the pre-authorization strategy, this intervention preserves the prescriber’s autonomy and allows for collaboration with the AST [40,41,42].
4.2.2. Minor Elements
a. Dose optimization: Therapeutic drug monitoring (TDM) ensures that antibiotic levels remain within therapeutic ranges, optimizing efficacy while minimizing toxicity; regular monitoring and dose adjustments are particularly important for antibiotics with narrow therapeutic windows [43,44].
b. Appropriate duration and antibiotic timing out: ending antibiotic therapy after an appropriate length of treatment is crucial, as extending the duration unnecessarily can increase adverse events without improving patient outcomes. Moreover, setting specified timing-out of antibiotic refill will help reassess the antibiotic duration [16].
c. From empiric to target therapy based on culture results and antibiotic monitoring by pharmacist: Empiric therapy is started based on clinical judgment and likely pathogens, but once culture results are available, therapy should be tailored to the specific pathogens, finding the best possible combination of antibiotics with the help of pharmacist when needed, enhancing treatment efficacy and reducing unnecessary broad-spectrum antibiotic use [16,24].
d. Switch to oral: Transitioning from intravenous to oral antibiotics when clinically appropriate (based on patient stability, ability to absorb oral medications, and availability of effective oral formulations) reduces hospital length of stay and healthcare costs [16].
By implementing a combination of these strategies, healthcare facilities can enhance their antimicrobial stewardship efforts, leading to better patient outcomes, reduced AMR, and overall improved public health.
5. The Different Types of ASP: Does the Same Program Fit All the Settings?
In pediatric settings, the implementation of ASPs varies across inpatients, outpatients, and PEDs, each with its unique challenges and strategies.
5.1. Inpatient Pediatric Care
In 2014, the Centers for Disease Control and Prevention (CDC) recommended that all hospitals implement ASPs and published the “Core Elements of Hospital ASPs,” which outlined the main features to ensure the success of an ASP [45]. A systematic review describing ASP implementation in hospitals in the USA and Europe showed that PAF, guidelines implementation, and more specific approaches based on laboratory testing and checklists were the most used interventions [46]. Indeed, a USA study suggested that a combination of PAF and pre-authorization could enable ASPs to maximize the strengths of each strategy [42], whereas a study conducted in UK, showed a great impact of behavioral interventions [47].
Different studies demonstrated the efficacy of ASPs in pediatric settings, both in high and low and middle-income countries (HICs and LMICs). The quasi-experimental study by Newland et al. demonstrated the effectiveness of PAF in reducing antibiotic use, showing a monthly reduction in overall antibiotic days of therapy (DOT) and length of therapy (LOT) by 7% and 8% per 1,000 patient-days, respectively (p=0.045) [48]. The impact was even more pronounced for specific antibiotics—ceftriaxone/cefotaxime, vancomycin, ceftazidime, and meropenem—where DOT and LOT decreased by 17% and 18% per 1,000 patient-days, respectively (p<0.001), compared to hospitals without ASPs [48]. Similar results were obtained by Hersh et al. that compared nine hospitals with ASP and 22 hospitals without ASP, showing an average monthly decline of 5.7% in DOT and of 8.2% in DOT of specific antibiotics (vancomycin, carbapenems, linezolid) in the hospital with ASP [49]. Furthermore, an Italian study demonstrated the efficacy of an ASP intervention conducted through observation, education, audit and feedback, and the provision of an electronic app to support antibiotic prescription based on local susceptibility data [49]. The study reported a significant decrease in antibiotic consumption (-452.49 DOT/1000 patient days, p<0.001) after the introduction of a mobile app, with a clear inversion of the Access to Watch ratio (from 0.7 to 1.7), without an increase in length of hospital stay, admission to pediatric intensive care unit and in-hospital mortality [50]. However, simpler interventions, such as the implementation of CPs, have also proven effective in reducing both antibiotic prescribing rates and the duration of antibiotic therapy. For instance, a study by Rossin et al. demonstrated a reduction in broad-spectrum antibiotic prescriptions (from 100.0% to 38.5%) and a shortened hospital stay (from 13.5 days to 7.0 days) for children admitted with lower respiratory tract infections (LRTIs) following the introduction of a specific CP for managing community-acquired pneumonia (CAP) [51].
Similar results were obtained also in studies conducted in LMICs [52,53]. The study published by Rahbarimanesh et al. showed a reduction in the use of meropenem and vancomycin in a Children’s Hospital in Pakistan after the introduction of a specific ASP [53], whereas the study published by Opondo et al. reported that in hospitals with ASP interventions, the risk of antibiotic prescriptions for non-bloody diarrhea was 70% lower than in hospital without ASP interventions [52].
The efficacy of ASP has also been evaluated in special settings, such as pediatric and neonatal intensive care units or oncology units. The study published by Wattier et al., conducted in a Pediatric Oncology and Stem Cell Transplantation Service in the USA, showed a reduction in tobramycin and ciprofloxacin use after the update of internal guidelines on the management of fever in neutropenia [54]. Similar results were reported in the study of Haque et al. conducted in a pediatric intensive care unit in Pakistan, which showed a 64% reduction in antibiotic use after ASP implementation [55].
5.2. Primary Care Setting
In 2016, the CDC published the Core Elements of Outpatient Stewardship [45]. Despite these recommendations, the best methods for conducting ASPs in the outpatient setting are currently unknown, and the uptake of outpatient ASP has remained low [56,57]. Implementing ASPs in the outpatient setting faces more challenges than in the inpatient setting, such as lack of funding, difficulties in identifying a clinician leader, obtaining antibiotic prescription data to identify high-impact targets, tracking process improvements and clinical outcomes, and sustaining improvements over time [58,59,60,61]. Additionally, antibiotic use is influenced by various factors, including parents’ beliefs and behaviors, their understanding of antibiotics, prior experiences, and adherence and disposal instructions [58]. In England, the largest reduction in antibiotic use was reported with structural-level interventions attributed to policy and commissioning interventions, such as primary care financial incentives [47].
Different studies showed the efficacy of ASP in outpatient settings, both in HICs and LMICs. An Italian study conducted at a regional level reported a significant impact of a multifaceted ASP, including guidelines, e-learning, and prescription reports, in improving the rate and quality of prescriptions in primary care settings [59]. The study reported a substantial reduction in the annual prescription rate per 100 patients (9.33 to 3.39; p = 0.009), with a reduction in prescription rates of amoxicillin-clavulanate (50.25 to 14.21; p = 0.001) and third-generation cephalosporins (28.43 to 5.43; p < 0.01) [59]. Similar results were obtained in a randomized controlled trial conducted in primary care pediatricians in the USA with a personalized audit and feedback intervention. The prescription of broad-spectrum antibiotics decreased from 26.8% to 14.3%, with an absolute difference of 12.5%, among primary care pediatricians in the intervention arm, compared with an absolute difference of only 5.8% in the control arm [59]. Considering specific infectious diseases, off-guideline prescriptions for children with CAP decreased from 15.7% to 4.2% in the intervention arm, compared to the control arm, in which the decrease was from 17.11% to 16.3% [60]. Unfortunately, the results of this trial were not sustainable over time. Indeed, twelve months after the start of the study, the PAF was stopped, showing in the six months after a new increase in antibiotic prescriptions. These results underlined the difficulties in sustaining results over time and the importance of the intervention, especially education intervention, for the effectiveness of the program [61]. Similar results were obtained in a randomized controlled trial conducted in 25 township hospitals in China, randomly allocated to the intervention group (12 centers) and to the control group (13 centers) [24]. The antibiotic prescription rate decreased from 82% to 40% in the intervention group and from 75% to 70% in the control group, determining an adjusted absolute risk reduction in antibiotic prescribing of -29% (95%CI -42 to -16, p<0.0002) [62].
5.3. Pediatric Emergency Departments
Antibiotic overprescribing in PEDs is influenced by clinician–caregiver dynamics and diagnostic uncertainties [63,64]. PEDs may be considered a hybrid setting, merging elements of both inpatient and outpatient stewardships with specific challenges related to logistical and provider-level barriers as well as intrinsic obstacles to the ED environment [65]. A recent systematic review reported that ASP implementation in PEDs in the USA and Europe focused mainly on multiple interventions, such as clinical practice guidelines (CPG) or CPs combined with education, but also on single interventions and other types of ASPs such as validated clinical prediction models for pneumonia [64]. Other potential strategies that could be implemented to improve antibiotic prescribing include utilizing the CDS tool and PAF, establishing follow-up procedures, implementing safety netting systems, and delivering comprehensive training, and supervision [64]. The impact of CPs on the management of acute otitis media and pharyngitis in an Italian PED has been demonstrated in the study published by Donà et al., which reported a reduction in broad-spectrum antibiotic prescriptions after the implementation of CPs (from 53.2% to 32.4%, p<0.001 for acute otitis media, from 46.6% to 6.6%, p<0.001 for pharyngitis) [32]. The same results were obtained by implementing the same CPs in other Italian PEDs, with a statistically significant reduction in broad-spectrum antibiotics used by 29.5-55.2% and by 80% respectively for acute otitis media and pharyngitis [27]. Nevertheless, as reported by Gerber in the outpatient settings [61], the results were not sustainable over time in all the centers involved. Indeed, only two centers combined the introduction of CPs with educational talks and recall lessons over time, whereas the third center did not associate recall educational lessons and was not able to sustain the results. This study highlighted the importance of education in the achievement and sustainability of results. Similar results were reported in another study conducted in the USA, showing an increase in the percentage of prescriptions with the recommended agent at the appropriate dose and duration, from a mean of 32.7% to 52.4%, after the introduction of an ASP characterized by a combination of tracking and reporting, education and expertise, action for policy and practice and commitment [48].
6. Different Types of Diagnostic Stewardship
In pediatric settings, DSP are tailored to the unique features of young patients, such as the need for non-invasive or micro-invasive techniques and the ability to perform tests on small samples, particularly capillary blood samples [66,67].
Various diagnostic tests, including biomarker tests, point-of-care tests (POCTs), multiplex polymerase chain reaction (PCR) panels can be integrated into clinical practice [68,69].
Biomarker testing, such as C-reactive protein (CRP) and procalcitonin (PCT), is a valuable tool for distinguishing bacterial infections from viral ones and optimizing antibiotic prescriptions [70], although there are no predefined cut-offs for these biomarkers to distinguish between viral and bacterial. The study published by Barbieri et al. showed that the implementation of CP for the management of LRTIs, including the use of CRP and PCT with pre-defined cut-offs, reduced antibiotic prescriptions from 36.2% to 12.5% (p = 0.036) in patients hospitalized for bronchiolitis [71]. The use of PCT has also been studied to shorten the antibiotic length of therapy. A recent meta-analysis showed that PCT-guided antibiotic therapy was associated with a significantly shorter length of antibiotic therapy compared with the control group (weighted mean difference, WMD, −2.22 days; 95% CI, −3.41 to −1.03; p <0.001) with a significantly lower rate of adverse events compared with the control group (relative risk, RR, 0.25, 95%CI 0.11-0.58) [72]. Some studies have shown that PCT levels correlate with bacterial infections, particularly in neonatal and pediatric intensive care settings, enabling clinicians to make more informed decisions regarding the initiation or discontinuation of antibiotics. The study published by Milcent et al. in 2016 showed that PCT has higher accuracy in identifying invasive bacterial infection (IBI) in neonates and infants with less than 90 days of age compared to CRP; indeed the AUC ROC curve for the detection of IBI for PCT was higher than that for CRP concentration (AUC, 0.91; 95%CI 0.83-0.99; vs AUC, 0.77; 95%CI, 0.65-0.89; p = .002) [70]. Instead, no difference in accuracy was observed in the identification of severe bacterial infection between PCT and CRP [70]. The use of PCT in PICU to reduce antibiotic consumption was studied by Katz et al. [24]. Antibiotic days of therapy were not significantly different between the procalcitonin arm (median 6.6, interquartile range [IQR], 3.1-10.9) and the usual care arm (7.6, IQR 3-11.8), although more antimicrobial stewardship was made in the procalcitonin arm compared to the control arm, with a higher adherence to the algorithm-based antibiotic recommendations in the procalcitonin arm (70%) [73]. Despite the usefulness reported in some studies, other authors recommended against the use of PCT alone due to the great variability in specificity across different cut-offs [74].
POCTs are diagnostic tests conducted at the time and place of patient care. These tests provide quick results, aiding timely decision-making, especially in outpatient and emergency settings [75,76,77]. One of the most common POCTs used in pediatric settings is the urinary dipstick, a valuable tool to identify children with a suspected urinary tract infection (UTI), avoiding antibiotic prescription in those without suspected UTI [76].
In children, CRP-POCT reduced antibiotic prescribing when CRP cut-off guidance was provided, with no difference in clinical recovery, resolution of symptoms, or hospital admissions compared to usual care [75]. For respiratory tract infections, POCTs like rapid streptococcal antigen and influenza tests can significantly reduce unnecessary antibiotic prescriptions, although strong evidence is still needed for children. Indeed, streptococcal tests potentially reduce antibiotic use by 25% [78], especially when associated with educational lectures, as reported by the study which observed a decrease of more than 50% in antibiotic prescription for children with sore throat after the introduction of rapid streptococcal test [78]. Instead, more studies are needed regarding the use of rapid viral testing since some studies did not find changes in antibiotic prescriptions in the group of children evaluated with rapid viral testing. For example, the study published by Thibeault et al. showed no difference in antibiotic prescription rate in children with positive rapid test results for RSV compared to children with negative tests [79].
Multiplex PCR (mPCR) panels can simultaneously detect multiple pathogens (e.g., viruses, bacteria, fungi) from a single sample [80]. This tool is particularly useful in diagnosing respiratory and gastrointestinal infections in children, where symptoms of viral and bacterial infections often overlap. It is also beneficial in diagnosing conditions like meningoencephalitis and sepsis. Compared to standard methods, mPCR panels provide quick identification of the causative pathogen and can lead to targeted antimicrobial therapy, reducing the use of broad-spectrum antibiotics [80]. Children admitted with respiratory symptoms and tested with a syndromic panel were less likely to receive empiric antibiotics (odds ratio 0.45, p < 0.001; 95% CI 0.39-0.52) and had a shorter duration of empiric broad-spectrum antibiotics (6.4 vs. 32.9 hours; p < 0.001) [81]. However, other studies failed to demonstrate this reduction. The study published by del Rosal et al., evaluating the use of mPCR respiratory panel in children with suspected viral pneumonia, showed no statistically significant differences in total antibiotics consumption (83% vs 86%) or antibiotics given for ≥72 h (58% vs. 66%) compared to an historical cohort [68]. A reduction in antibiotic prescriptions at discharge was observed in the intervention group (41% vs 72%, p=0.001) [68]. These results are similar to those reported by Rao et al. in their randomized controlled trial, which reported that the use of rapid respiratory pathogen testing did not change antibiotic prescriptions rate compared to usual practice (RR 1.1; 95%CI 0.9-1.4) [82].
The use of mPCR has been shown to be effective also for other pediatric infectious diseases. In cases of acute diarrhea, the use of multiplex PCR panels reduced inappropriate antibiotic use from 42.9% to 25.8% [83], while the use of mPCR panels for central nervous system fluid analysis may reduce the duration of therapy and the hospital length of stay in children admitted for presumptive meningitis or encephalitis [84].
7. The Different Types of Diagnostic Stewardship: Does the Same Program Fit All the Settings?
7.1. Inpatient Pediatric Care
Hospitalized children often require immediate and effective antimicrobial therapy, making DSPs crucial in this setting. As part of hospital ASPs, molecular assays for rapid identification of pathogens in bloodstream infections (BSIs) have proven effective in minimizing the duration of empirical therapy and reducing the time to targeted antibiotic therapy in life-threatening neonatal and pediatric infections, encouraging de-escalation of antibiotics when appropriate and improving patient outcomes [67,85]. A study on the adult population reported a shorter median time until pathogen detection in the T2 group compared to the usual care (4.5 h vs 60 h, p<0.001) as well as the time until targeted therapy (antibiotic with the narrowest spectrum and maximal effectiveness, 6.4 h vs 42.2 h, p = 0.043 [86]. Moreover, commercially available molecular methods to detect antibiotic resistance genes within hours are promising tools to rapidly optimize treatment and aid in infection control by identifying clusters of resistant strains. Studies on the adult population showed encouraging results. A randomized controlled trial compared the blood culture testing with standard-of-care (SOC) culture and antimicrobial susceptibility testing with rapid organism identification and phenotypic antimicrobial susceptibility testing using the Accelerate Pheno System (RAPID) [87]. Although no difference in patients outcome between the two groups was observed, the median time to first antibiotic modification for overall antibiotics for gram negative antibiotics and for antibiotic escalation for antimicrobial-resistant BSIs was faster in the RAPID arm vs the SOC arm (8.6, IQR 2.6-27.6, vs 14.9, IQR 3.3-41.1, hours, p=0.02, 17.3, IQR 4.9-72, vs 42.1, IQR 10.1-72, hours, p<0.001, 18.4, IQR 5.8–72, vs 61.7, IQR 30.4–72 hours; p=0.01, respectively) [87]. However, considering their high costs, they should be reserved for specific settings, such as critically ill and immunocompromised patients.
For central nervous system infections, the FilmArray Meningitis/Encephalitis Panel can detect a broad range of pathogens directly in cerebrospinal fluid with a turnaround time of about one hour [88], allowing for more targeted use of antimicrobials, particularly in young patients or specific population such as immunocompromised individuals. The study published by Kadambari et al., comparing a group of children that underwent lumbar puncture for suspected central nervous system infection before and after the introduction of FilmArray, showed a shorter duration of antibiotic in the intervention group, especially in the case of enterovirus meningitis (median: 4 vs. 5 days) and human parechovirus meningitis (median: 4 vs. 4.5 days) but also in the case of culture/FilmArray-negative cerebrospinal fluid (median: 4 vs. 6 days) [89].
However, the risk of over-testing can lead to overdiagnosis, unnecessary antimicrobial treatments, and excessive costs. Inadequate specimen collection and storage can also reduce test accuracy. Therefore, robust microbiology support with pediatric-specific expertise, evidence-based CPs for diagnosing common pediatric infections, and educational programs for clinicians and nursing staff are critical to obtaining accurate sample collection, timely processing, and proper interpretation of results to ensure appropriate diagnosis and achieving a consistent and cost-effective reduction of antibiotic consumption alongside ASP [90].
7.2. Primary Care Settings
In the primary care setting, POCTs are valuable tools to differentiate between viral and bacterial pathogens beyond clinical symptoms. Training pediatricians on the appropriate use of diagnostic tests, such as pharyngeal swabs or rapid viral tests, improves diagnosis accuracy, reduces unnecessary antibiotic use, and encourages “watch and wait” approaches before starting antibiotics. However, barriers to the widespread use of POCTs at primary healthcare levels exist, likely due to insufficient healthcare worker training or limited economic resources [91].
A recent meta-analysis showed that streptococcal rapid tests and influenza rapid tests are the most used POCTs in primary care [92]. Many studies reported a significant reduction in antibiotic consumption following the introduction of the streptococcal rapid tests. Conversely, a significant increase in oseltamivir prescribing with POCTs was observed in 60.0% of the analyzed studies. Implementing community-level education campaigns on accurate diagnosis and appropriate antibiotic use helps build public understanding and support for ASP initiatives.
Despite the costs related to the POCTs, similar good results were achieved also in developing countries. The use of a digital clinical decision support algorithm combined with CRP test, hemoglobin test, pulse oximeter and mentorship has proven effective in reducing antibiotic prescription in primary care facilities in Tanzania, with an adjusted difference of -46.4% (95% CI -57.6 to -35.2), without an increase in treatment failure (adjuster relative risk 0.97, 95% CI 0.85-1.10) [93]. Another study conducted among primary health facilities in Burkina Faso evaluated the impact of POCTs for respiratory pathogens (RSV, influenza, Streptococcus pyogenes, Streptococcus pneumoniae), for malaria and for other infections (dengue, typhoid fever, and urine dipstick), showing a reduction in antibiotic prescription (risk difference (RD) -16.8%, 95%CI -21.7% to -12.0%, p<0.010), with a greater decrease in patients without malaria (RD: −46.0%; −54.7% to −37.4%; P < .001), and in those with a respiratory diagnosis (RD: −38.2%; −43.8% to −32.6%; P < .001) [94].
7.3. Pediatric Emergency Departments (PEDs)
PED is a dynamic environment where rapid decision-making is essential. Antimicrobial treatment is typically empiric, often without microbiological results or feedback on the patient’s course. The use of POCTs has proven effective for ASP in PED, significantly decreasing antibiotic use after their introduction into clinical practice [77]. Indeed, the study published by Tan et al. showed that a positive rapid viral test was associated with fewer antibiotic prescriptions compared to children without a test performed (aOR 0.6, 95% CI 0.5-0.) [77]. However, the implementation of these tests alone is often insufficient to modify antimicrobial prescription trends. The introduction of POCTs should be accompanied by educational interventions and the establishment of diagnostic and therapeutic CPs to ensure the rational use of antibiotics [77].
8. How Should the Effectiveness of an ASP and DSP Be Evaluated? The Different Metrics in Pediatric Settings
Measuring performance indicators are essential to evaluate the effectiveness of ASPs. Standardized measures are challenging to assess and vary among studies in different settings. Most of the studies evaluated antibiotic use [1]. The DOTs per 1,000 patient-days is preferred over defined daily doses (DDDs) per 1,000 patient-days in the hospitalized pediatric population because DDD does not accurately describe antimicrobial use in pediatric settings due to age- and weight-based dosing in children [95]. DOT is defined by counting each antimicrobial administered on a hospital day (i.e., a 5-day course of 3 antibiotics results in 15 DOTs) [25].
LOT per 1,000 patient-days provides an overview of the number of days patients receive antimicrobial therapy, irrespective of the number of antibiotics prescribed, and could be an additional metric to describe overall antimicrobial prescribing behaviors in hospital settings [96]. The DOT/LOT ratio measures the number of antibiotics prescribed to each patient. Notably, unlike DDD per 1,000 patient-days, DOTs and LOT can only be obtained via medical records [96].
These metrics fail to describe prescribing appropriateness including antibiotic dose accuracy, the spectrum of activity (i.e., a broad-spectrum antibiotic like a carbapenem usually counts for half the DOTs compared to a narrow-spectrum combination course), and reasons for prescribing [25,96]. To better characterize antibiotic prescriptions, the WHO developed the AWaRe Classification [24]. This is a valuable framework for antibiotic stewardship, as it simplifies prescribing by categorizing antibiotics into Access, Watch, and Reserve groups based on resistance potential and clinical necessity. “Access” antibiotics are those antibiotics that could be prescribed freely and should always be available, such as amoxicillin, amoxicillin-clavulanate, first-generation cephalosporins, “Watch” antibiotics are those that should be prescribed with caution due to a broader spectrum of activity and a higher risk of developing antibiotic resistance, such as second- and third-generation cephalosporins, macrolides, carbapenems, fluoroquinolones, and “Reserve” antibiotics are 29 newer-generation and more expensive antibiotics, which are the last option for multidrug-resistant (MDR) infections, such as linezolid, daptomycin, ceftazidime-avibactam or meropenem vaborbactam [97,98]. A unique feature of the system is its inclusion of unclassified antibiotics, which often consist of fixed combinations and serve as a point of interest for developing country-specific stewardship strategies. This unclassified group spans both narrower-spectrum and broader-spectrum antibiotics, reflecting varied use patterns that underscore the need for clearer guidance on their categorization. In countries with high use of unclassified antibiotics, reclassifying these agents under AWaRe categories may shift access-to-watch ratios, potentially complicating trends and stewardship approaches for these medications. Although tools like the access-to-watch ratio and amoxicillin index provide intuitive methods for evaluating antibiotic use, they have limits. For instance, these tools may overlook narrower-spectrum antibiotics in certain regions, and they lack the ability to directly address the antibiotic spectrum, highlighting an area where AWaRe could be refined to support more detailed stewardship efforts [99].
To better assess prescribing appropriateness, antimicrobial use measures should be adjusted by case mix and ward [100]. Other qualitative indicators applied should evaluate adherence to guidelines (i.e., the proportion of children on antibiotic therapy without indication; surgical prophylaxis beyond 24 hours; time to switch from empiric to targeted antibiotic treatment when etiology has been assessed, or from intravenous to oral treatment when indicated).
Gathering antibiotic data is essential for evaluating the effectiveness of a stewardship intervention. Although daily data collection is ideal, it is often labor-intensive and consumes significant human resources, especially when electronic data are not available. Point prevalence surveys (PPSs) have become a valuable tool for efficiently capturing antibiotic prescription information with reduced effort [101].
In the outpatient pediatric setting, the ASP most used indicator is the number of antibiotic prescriptions per 1,000 children per year [102]. More useful metrics include the prescription rate for Watch antibiotics classes and the amoxicillin/amoxicillin-clavulanic acid ratio. Amoxicillin currently remains the first-line antibiotic recommended worldwide for most of the pediatric respiratory infections, accounting for more than 70% of pediatric visits. Therefore, an increase in the amoxicillin to amoxicillin-clavulanic acid ratio is a marker of effective pediatric ASPs in the community.
Microbiological outcomes, such as the rate of MRSA and ESBL or carbapenem-resistant Enterobacterales in invasive infections, are often proposed. In particular, the UKHSA propose as AMR local indicators to monitor Escherichia coli resistance testing every three months to 3rd generation cephalosporins, carbapenem, ciprofloxacin, gentamicin, piperacillin/tazobactam for blood samples and to trimethoprim, and nitrofurantoin for urine samples [103]. Moreover, it is recommended to produce indicators for each hospital and for each local health unit. Indeed, different studies showed a reduction in AMR after the introduction of ASPs. For example, in the study published by Sarma et al. in 2015, after the introduction of fluoroquinolone restrictions, a decline in the percentage of ciprofloxacin-resistant extended-spectrum beta-lactamase (ESBL) producing urinary E. coli isolates was observed in both hospitals (RR: 0.473; 95% CI 0.315-0.712) and community settings (0.098; 95% CI 0.062-0.157) [104]. Another study published by Lawes et al., focusing on the restriction of the use of cephalosporins, co-amoxiclav, clindamycin, fluoroquinolones, and macrolides, showed a decrease in the methicillin-resistant Staphylococcus aureus (MRSA) prevalence density by 54% in hospitals and 37% in the community [105]. Other studies reported a decline in macrolide-resistance rates in Gram-positive cocci following a reduction in macrolide prescriptions in the community [106,107]. However, a lack of decreasing prevalence of MDR pathogens may not reflect ASP failure. Indeed, AMR is a complex event that probably requires time to reverse after a decrease in antimicrobial pressure.
The rate of Clostridioides difficile infections (CDIs) as ASP measure should be used cautiously in the pediatric setting due to the high carriage rate in the first years of life, differently from the adult setting [108]. However, the hospital-acquired CDIs rate should be monitored, particularly among immunocompromised patients beyond two years of age, as it is a good marker of poor strategies to contain healthcare-associated infections other than antimicrobial prescriptions [109]. Again, the UKHSA recommends producing CDIs rates every twelve months for each hospital and for each local health unit for both community-acquired and hospital-acquired infections [103]. Moreover, other indicators recommended to monitor are hospital and community bacteremia rates caused by E. coli, Klebsiella spp., MRSA, MSSA and Pseudomonas aeruginosa.
Clinical outcome measures are more difficult to obtain in children. Mortality is very rare in children and, like intensive care admission, could be a multifactorial event often associated with underlying clinical conditions. Metrics that are considered reliable and feasible in pediatric hospital settings include the length of hospital stay (LOS) and the 30-day readmission rate. Recently, the 30-day clinical failure rate has been more frequently reported to evaluate clinical outcomes, particularly in studies assessing shortened antibiotic courses for subacute (such as osteomyelitis) or non-invasive infections [60].
9. What is the Cost-Effectiveness of an ASP and a DSP?
Different ASPs and DSPs strategies can directly and indirectly affect healthcare expenses, and the planning and implementation of each intervention incur costs. Therefore, the cost-benefit balance of ASPs should be considered in experimental models testing different approaches. Models of economic evaluation include [110]:
- cost-minimization analysis: two alternative programs or treatments are compared to ascertain the less expensive;
- cost-benefit analysis: the costs associated with an ASP strategy should be compared to the potential benefits, including both financial metrics and intangible benefits that encompass health gains, lives saved, and the reduction of adverse events following antimicrobial use (e.g., CDIs);
- cost-effectiveness analysis: the cost difference between two interventions (or compared to standard care) divided by the difference in their effects, defined as incremental cost-effectiveness ratio (ICER). It represents the average incremental cost associated with one additional unit of effect (e.g., the incremental cost per percentage point reduction in antibiotic prescription rate). This is the simplest measure of economic analysis, though it may not account for confounding factors such as hospital occupancy rates, price variations, and cost differences among different producers. This type of analysis should be normalized using consumption metrics such as DDD, DOT, and LOT [110].
Most studies published in pediatric settings focus on antibiotic cost savings before and after an ASP implementation, typically reporting only short-term evaluations. In the study published by Zhang et al., the implementation of multifaceted ASP in the outpatient setting has been associated with a 29% absolute risk reduction in antibiotic prescribing in children with upper respiratory tract infection, with an incremental cost-effectiveness ratio of only $0.03 per percentage point reduction in antibiotic prescribing [111]. Another study, published by Velasco-Arnaiz, reported that the hospital expenditure on antibacterials and antifungal drugs decreased by a total of 64,406 euros in 2017 and 137,574 euros in 2018 as compared with the 2015-2016 mean expenditure for an absolute savings of 201,980 euros after the introduction of a post prescription review with feedback-based antimicrobial stewardship program in a European children’s hospital [41]. Reduction in costs after the implementation of DSP is still debated. The study published by Lubell et al. regarding the use CRP POCT in the management of respiratory tract infection in children in primary care settings in Vietnam did not show a reduction in healthcare costs. Indeed, although the use of this POCT reduced the consumption of antibiotics, the cost of the test itself was higher than the potential savings from reduced prescriptions observed in the study [24]. However, the authors reported that with higher adherence to the test results, their use would be cost-beneficial [112].
Cost-analysis can vary in complexity even for the same variable. For instance, the direct costs of antimicrobial treatment can be categorized into three levels: the first level includes only drug acquisition costs, the second level incorporates the first level along with costs related to preparation, dispensing, and administration, as well as expenses related to antibiotic-related adverse events and clinical failure, and the third level further adds daily hospital stay costs [113,114].
Indirect costs are frequently overlooked, as well as long-term effects such as cost savings related to the reduction of AMR are not estimated. Furthermore, there is a high variability in costs attributed to the same intervention and to AMR (if estimated) in both inpatient and outpatient settings, which could influence the analysis. A systematic review and meta-analysis published in 2023 estimated that infections caused by MDR bacteria, in comparison with non-MDR ones, have higher management costs, estimated up to 29,000 USD per episode [115]. This higher cost could be related to the higher length of stay and the higher odds ratios of mortality for resistant infection and mortality [115]. Table 1 reports a detailed list of costs and potential benefits of ASPs according to healthcare setting [116].
Additional elements that impact economic outcomes include the type of healthcare system financing and the care setting where the program is implemented. For instance, in hospital settings, costs primarily involve the work time of healthcare professionals and the implementation of diagnostic techniques, while benefits can be easily estimated by comparing expenditures on antimicrobial acquisition before and after the intervention. In the study published by Turner et al., the implementation of an ASP consisting of physician-group engagement and pharmacist PAF in a freestanding children’s hospital in the USA showed a reduction in the average monthly drug-acquisition costs [117]. Although pharmacy and physician clinicians were asked to perform additional tasks for the ASP, these tasks were integrated into the clinical practice, resulting in no additional cost. Therefore, the study showed a cost saving of approximately $67,000/year over the 2-year postintervention period [117]. Conversely, in outpatient settings, costs often rely on general practitioners or primary care providers. Furthermore, regional variations in healthcare systems (such as public financing, insurance-based, or out-of-pocket models) also contribute to differences in economic outcomes. Table 2 summarizes a framework for establishing costs accountable for AMR in a one health perspective.
10. Which Are the Most Important Phases to Successfully Implement an ASP?
Implementing an ASP requires careful adaptation to specific settings, as no fixed model or consensus on the best approach exists [24] (Srinivasan, 2017; Mendelson et al., 2020). The process can be divided into three phases (Figure 3).
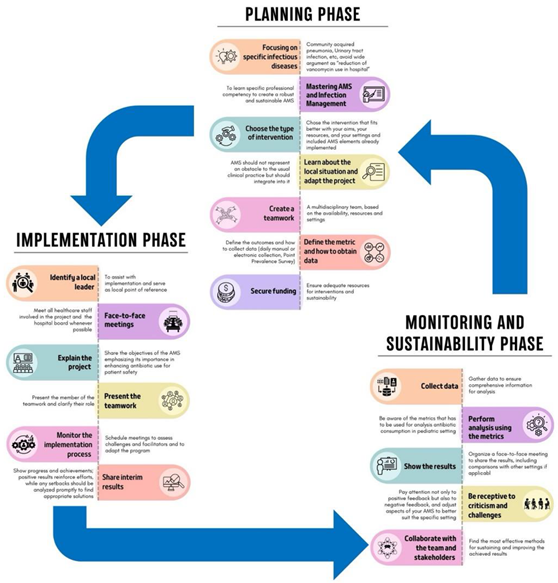
10.1. Planning Phase
This is a critical phase for establishing a robust program. To have more precise interventions, it is essential to focus on specific pediatric infectious diseases, such as CAP or UTIs, rather than broad objectives, like reducing unnecessary vancomycin use [118,119]. Specific professional competencies in ASP and infection management are needed, and the interventions chosen should align with your goals, the literature search, and available resources and settings. Some interventions are costly and may not be feasible everywhere. For example, a PAF intervention might be challenging in a PED but more suitable in an intensive care unit with adequate resources. Moreover, compliance with national and local guidelines is essential unless strong evidence supports alternative approaches. The creation of teamwork and the definition of the roles are essential steps. Furthermore, it is important to pre-establish the outcomes that should be evaluated, identify the best data collection methods, and evaluate if all the data needed for the analysis are available. This phase, as well as all the other phases, can be costly, both financially and in terms of human resources, so finding funds and dedicated personnel is mandatory [118,119].
10.2. Implementation Phase
This phase involves executing the planned strategies. To better engage local staff, it is essential to identify a local leader to assist with implementation and serve as the local reference point. This leader should motivate team members, foster a positive work environment, and facilitate communication among healthcare personnel [120].
Moreover, face-to-face meetings with healthcare staff and the hospital board are crucial for fostering a collaborative environment and securing funding. During these meetings, it is essential to clearly explain the project and its reasons.
Monitoring the implementation process through scheduled meetings is essential to assess difficulties encountered and allow adjustments to the program if needed. Moreover, it allows for the sharing of interim results, the demonstration of achievements, and the encouragement of continuous improvements. Indeed, real-time feedback reinforces efforts and allows for promptly addressing any setbacks [118,119].
10.3. Monitoring and Sustainability Phase
The final phase evaluates the results and ensures the ASP’s long-term success. Collecting data for monitoring, whether manually, electronically, or through PPSs, ensures comprehensive information for thorough analysis that should be conducted using appropriate metrics [118,119]. To maintain transparency and engagement, the results should be presented to stakeholders through face-to-face meetings, including comparisons with other settings. Furthermore, it is important to be receptive to criticism and challenges to adjust aspects of the ASP to suit the specific setting better. Attention to both positive and negative feedback and assessing challenges during implementation helps enhance the ASP [118,119].
In this phase, it is also important to collaborate with the team and stakeholders to determine the most effective methods for sustaining and improving achieved results [71].
11. Future Perspectives
Core strategies like prospective audits, feedback, and pre-authorization have shown effectiveness in ASP but are often resource-intensive [123]. In pediatric outpatient settings — where most antibiotic prescriptions occur [123] — stewardship efforts face additional challenges due to limited resources, lack of structured frameworks, and insufficient organizational support, unlike in inpatient settings [124]. As a result, interventions are often guideline-based, while more comprehensive strategies are rarely implemented. To address these challenges, key strategies have been highlighted. The first is commitment, urging prescribers to engage actively in responsible antibiotic use. Next, action for policy and practice focuses on adopting specific policies or interventions aimed at improving antibiotic prescribing. Tracking and reporting involve the continuous monitoring of prescriptions, coupled with feedback through audits, to help prescribers assess and refine their practices. Lastly, education and expertise should extend beyond healthcare providers to include patients and caregivers, ensuring a comprehensive approach to improving antibiotic use and understanding [125,126]. Parents play a critical role in pediatric ASPs, as they are often the primary influencers in their child’s healthcare decisions. Their expectations and knowledge about antibiotics can significantly affect prescribing behaviors, either promoting or discouraging the use of antibiotics [58]. Educating parents about the appropriate use of antibiotics and the risks associated with resistance is crucial to minimizing unnecessary prescriptions. Despite its significance, the involvement of parents in stewardship efforts remains underexplored. Further research is needed to identify effective strategies for parental engagement, evaluate the impact of educational interventions, and develop methods to integrate parents as active partners in stewardship. Understanding these elements is essential for creating comprehensive ASPs that address both provider and parental factors influencing antibiotic use in pediatric care.
Additionally, POCTs, mPCR, septic biomarkers, and reliable microbiological cultures play a critical role in timely treatment and reducing unnecessary antibiotic use in both pediatric outpatient and inpatient care [127]. However, assessing the financial and logistical aspects of implementing POTCs in pediatric care is essential to gauge their long-term viability and impact within healthcare systems. Key considerations in implementing POCTs extend beyond initial costs and logistical planning. Proper training for healthcare professionals is crucial not only to use POCTs effectively but also to interpret the results accurately, as misinterpretation could lead to inappropriate treatment decisions. Ensuring widespread availability across diverse clinical settings, particularly in resource-limited areas, requires coordinated infrastructure and sustained funding. Integrating POCTs within existing healthcare workflows further supports their effectiveness, maximizing their potential impact on patient outcomes and ASP effort [127]. Further research is needed to evaluate how these diagnostic tools can be seamlessly incorporated into daily clinical workflows and to optimize their use for sustainable, effective pediatric care.
Furthermore, in specialized pediatric fields such as neonatal or pediatric intensive care units and hemato-oncological wards, the complexity of care is compounded by the need to manage infections caused by MDR organisms. While novel antimicrobials are more readily available for adult populations, children often face limited access due to ethical concerns surrounding drug trials in pediatric patients, as well as the complexities involved in conducting such trials [128]. The lack of specific pediatric data can result in suboptimal dosing strategies, as the pharmacokinetics and pharmacodynamics of drugs in children differ significantly from adults, necessitating tailored approaches. Moreover, in these settings, critically ill children are especially vulnerable, making it difficult to distinguish infections from other inflammatory conditions. This ambiguity complicates decisions on de-escalating or discontinuing antibiotics, leading to higher antibiotic usage compared to general pediatric wards [129]. Implementing targeted interventions to refine empiric antibiotic therapies can reduce inappropriate broad-spectrum antibiotic use. Updating internal guidelines with the latest evidence and applying the WISCA method to identify optimal empiric treatments are promising strategies to improve antibiotic prescribing for these fragile patients [28].
One critical area in the management of these complex cases is TDM. It is essential for ensuring that the dosage of antimicrobials is optimized to maximize efficacy while minimizing toxicity [130]. Pediatric patients, especially neonates and those critically-ill, often require precise dosing adjustments due to factors such as varying body sizes, organ immaturity, and complex underlying health conditions that influence drug absorption, metabolism, and excretion. Additionally, many antimicrobials used to treat MDR organisms have a narrow therapeutic window, underscoring the importance of TDM. TDM is essential for preventing underdosing, which can result in treatment failure, and overdosing, which may lead to severe adverse effects, thereby ensuring optimal therapeutic outcomes and patient safety. TDM-guided expert clinical pharmacological advice programs have proven effective in tailoring and optimizing treatment dosage, with more than 40% of recommended dosing adjustments both in adults and pediatric setting [131].
Establishing ASPs in LMICs involves a distinct set of challenges. Infectious diseases continue to be the leading cause of mortality among children under the age of five, and AMR rates in these regions are notably high [132]. Restricted access to microbiology services and antibiotic susceptibility testing frequently leads to extensive reliance on broad-spectrum antibiotics [133]. Additionally, healthcare resources in developing countries are frequently limited, with professionals who may not always have specialized training. Guidelines targeted for establishing ASPs in LMICs are essential and should focus on different areas compared to those for HICs, such as for example ensuring access to diagnostic testing, providing education on AMR and antibiotic prescription practice, establishing national and international agencies to regulate, monitor and audit drug production, distribution, and dispensing practices [133].
Data collection is crucial yet challenging. Electronic daily data collection provides a clear, representative view of antibiotic usage and highlights changes in prescription patterns post-intervention. However, since many centers lack electronic data systems, manual collection is often required. To lessen the burden on healthcare staff, PPS, conducted at various times throughout the year, offers a practical alternative for gathering antibiotic prescription data efficiently [134].
The use of varied metrics and the absence of internationally validated measures for pediatric patients complicate comparisons across similar studies in different settings. While DDDs have been applied in pediatric research, uncertainty about their suitability remains. The AWaRe classification is a step forward toward standardized metrics in pediatric settings; however, the large number of antibiotics in the unclassified category poses challenges, particularly in countries with high usage rates of these antibiotics [9].
One major challenge in implementing pediatric ASPs is the need to revise regulatory frameworks and develop specific recommendations that account for global healthcare diversity. Existing guidelines, largely designed for the USA healthcare system [16], must be adapted to suit the varying structures in different settings in other countries. National ASPs have already been established in some countries outside the USA. For example, since 2013 UK developed and adopted a variety of interventions to improve ASP, with the aim of reducing antibiotic consumption, especially broad-spectrum ONES, in both primary and secondary care [135].
Although ASPs consistently enhance clinical practices and patient outcomes, their return on investment is often indirect and not immediately visible [135]. Developing a comprehensive business plan is crucial for the success of an ASP; however, integrating stewardship responsibilities into the roles of existing staff can serve as a more cost-effective strategy. This approach maximizes the use of current resources while still supporting the goals of the program, allowing institutions to implement ASPs without incurring significant additional costs. However, for long-term success, developing a comprehensive business plan that ensures sustainable financial backing for both personnel and infrastructure is essential.
Despite considerable advancements in pediatric ASPs over the past decade, significant knowledge gaps remain in pediatric care, highlighting the need for ongoing research to refine and enhance these programs. Future efforts must prioritize large-scale, longitudinal studies to evaluate the long-term impact of ASPs on AMR trends, clinical outcomes, and overall patient safety. These studies should incorporate standardized metrics, allowing for comparability across diverse healthcare settings and regions. Such a comprehensive approach would enable the identification of global patterns in ASP effectiveness, helping to establish benchmarks for success and revealing context-specific challenges that require targeted interventions.
Investigating the economic impact of ASPs, particularly in resource-limited settings, is crucial for understanding how these initiatives can be sustainably scaled and maintained. Such data would provide valuable insights to guide policy decisions, advocating for increased investment in healthcare infrastructure and training to support pediatric ASPs. Overcoming financial and infrastructural barriers through innovative approaches like telehealth and artificial intelligence (AI) is essential for extending the reach and effectiveness of ASPs globally, ensuring their successful implementation across diverse healthcare environments [3]. The potential applications of AI in medicine are vast. Importantly, AI solutions are designed to complement, not replace, physicians and healthcare professionals, serving as valuable tools to improve and support clinical practice [3]. AI could play a pivotal role in the fight against AMR. Machine learning (ML) algorithms could predict trends in AMR and treatment responses, suggest specific therapeutic agents, and identify genetic markers related to antibiotic resistance by analyzing large genomic datasets [136]. For example, Feretzakis et al. developed an ML-based model using antimicrobial susceptibility data from a tertiary hospital in Greece. This model predicts antibiotic susceptibility based on sample source, infection site, Gram stain results, and past susceptibility data, achieving 72.6% accuracy [137]. AI and ML could also be useful in monitoring antibiotic prescribing. Indeed, antimicrobial prescribing requires frequent adjustments as clinical data evolve, but manual review is challenging due to limited resources and extensive information. Hospitals increasingly use automated decision support systems, though many rely on static rule sets that generate excessive, unhelpful alerts. To address this, ML-based systems incorporating feedback to continuously improve and effectively support key decisions may be helpful [138]. AI could also be applied in drug development to streamline the discovery of new antibiotics and optimize drug administration [139] and in expanding knowledge, particularly among students and residents, by enhancing understanding of antibiotic prescribing practices [140]. However, a gap remains between promising AI models and their integration into clinical settings. Further research is needed to assess the impact of AI and ML on ASP, as well as to fully explore the capabilities these technologies may offer [141].
On the other side, telehealth can help address staffing shortages in remote or underserved areas by enabling healthcare providers to offer timely guidance and support, thereby bridging critical gaps in care [142]. Access to technology is also helpful for delivering real-time, localized data on antibiotic use, with tools that facilitate detailed analysis and provide direct feedback, including alerts for broad-spectrum antibiotic use, automatic stop orders, and the transition from intravenous to oral therapies [143]. Integrating telehealth and AI into pediatric care holds promise for optimizing antibiotic prescribing, enhancing adherence to clinical guidelines, and supporting timely adjustments in therapy, including de-escalation.
Addressing these priorities will be key to advancing more effective and sustainable ASPs, ultimately reducing the global burden of AMR and improving health outcomes in pediatric populations.
12. Conclusions
This narrative review underscores the critical role of ASPs in pediatric care, emphasizing the need to adapt social and behavioral dynamics to foster collaboration among families, primary care providers, and hospital-based teams [114]. Despite some challenges, ASPs have consistently improved clinical practices and patient outcomes, even though financial benefits may not always be immediately apparent [121]. A multidisciplinary approach is vital for the success [23]. However, a significant challenge remains the shortage of healthcare workers with specialized training, particularly in low-resource settings. Research highlights that limited training opportunities and a lack of dedicated personnel for stewardship efforts undermine the effectiveness of ASPs [23]. Investing in the education and development of specialized professionals is essential to overcoming these barriers and ensuring that ASPs are tailored to the unique needs of pediatric patients.
Scope statement
This article, written by the key-opinion leaders in pediatric infectious diseases in Italy, provides a comprehensive review of the current state of Antimicrobial Stewardship Programs (ASPs) and Diagnostic Stewardship Programs (DSPs) in pediatric healthcare settings. It addresses the critical need for these programs to combat antimicrobial resistance (AMR) and improve antibiotic use in children, recognizing the unique challenges in pediatric care. It includes an analysis of various ASP strategies, such as pre-authorization, prospective audits and feedback, as well as the role of point of care tests (POCTs)and biomarkers in reducing unnecessary antibiotic prescriptions. The manuscript highlights the importance of a multidisciplinary approach involving pediatricians, pharmacists, microbiologists, and public health professionals to effectively manage antibiotic use across inpatient, outpatient, and emergency settings. The manuscript discusses economic evaluations, showing that ASPs, despite requiring initial investments, offer long-term cost savings. The article also identifies gaps in research, particularly in pediatric specific diagnostic tools and the integration of artificial intelligence into clinical decision-making. By addressing these issues, the article aims to contribute to the global effort to enhance the effectiveness and sustainability of ASPs, ultimately improving pediatric health outcomes and helping to mitigate the threat of AMR.
Author Contributions
DD and SE: conception and design of the work; DD, EB, GB, CL, SB, EC, CC, LG, LL ALV, MM, CM, MDL, SM, SE: writing the first draft of the manuscript; DD, EB, GB, CL, SB, EC, CC, LG, LL ALV, MM, CM, MDL, SM, SE: revised the final document. All authors read and approved the final manuscript.
Funding
None to declare.
Acknowledgements
Elisa Barbieri position is currently supported by the European Union - Next Generation EU under the National Recovery and Resilience Plan (NRRP) (project INF-ACT - One Health Basic and Translational Research Actions addressing Unmet Needs on Emerging Infectious Diseases).
Competing interests
The authors declare that they have no competing interests.
References
- Principi, N., and Esposito, S. (2016). Antimicrobial stewardship in paediatrics. BMC Infect Dis 16. [CrossRef]
- Tersigni, C., Montagnani, C., D’Argenio, P., Duse, M., Esposito, S., Hsia, Y., et al. (2019). Antibiotic prescriptions in Italian hospitalised children after serial point prevalence surveys (or pointless prevalence surveys): Has anything actually changed over the years? Ital J Pediatr 45. [CrossRef]
- Fanelli, U., Chiné, V., Pappalardo, M., Gismondi, P., and Esposito, S. (2020a). Improving the Quality of Hospital Antibiotic Use: Impact on Multidrug-Resistant Bacterial Infections in Children. Front Pharmacol 11. [CrossRef]
- De Luca, M., Donà, D., Montagnani, C., Vecchio, A. Lo, Romanengo, M., Tagliabue, C., et al. (2016). Antibiotic prescriptions and prophylaxis in Italian children. Is it time to change? Data from the ARPEC project. PLoS One 11. [CrossRef]
- Versporten, A., Bielicki, J., Drapier, N., Sharland, M., Goossens, H., Calle, G. M., et al. (2016). The worldwide antibiotic resistance and prescribing in european children (ARPEC) point prevalence survey: Developing hospital-quality indicators of antibiotic prescribing for children. Journal of Antimicrobial Chemotherapy 71, 1106–1117. [CrossRef]
- Barbieri, E., Di Chiara, C., Costenaro, P., Cantarutti, A., Giaquinto, C., Hsia, Y., et al. (2022). Antibiotic prescribing patterns in paediatric primary care in italy: Findings from 2012–2018. Antibiotics 11. [CrossRef]
- Cook, A., Sharland, M., Yau, Y., Bielicki, J., Grimwood, K., Cross, J., et al. (2022). Improving empiric antibiotic prescribing in pediatric bloodstream infections: a potential application of weighted-incidence syndromic combination antibiograms (WISCA). Expert Rev Anti Infect Ther 20, 445–456. [CrossRef]
- Frati, F., Salvatori, C., Incorvaia, C., Bellucci, A., Di Cara, G., Marcucci, F., et al. (2019). The role of the microbiome in asthma: The gut–lung axis. Int J Mol Sci 20. [CrossRef]
- Hsia, Y., Lee, B. R., Versporten, A., Yang, Y., Bielicki, J., Jackson, C., et al. (2019a). Use of the WHO Access, Watch, and Reserve classification to define patterns of hospital antibiotic use (AWaRe): an analysis of paediatric survey data from 56 countries. Lancet Glob Health 7, e861–e871. [CrossRef]
- Ballarini, S., Rossi, G. A., Principi, N., and Esposito, S. (2021). Dysbiosis in pediatrics is associated with respiratory infections: Is there a place for bacterial-derived products? Microorganisms 9, 1–19. [CrossRef]
- Bossù, G., Di Sario, R., Argentiero, A., and Esposito, S. (2021). Antimicrobial prophylaxis and modifications of the gut microbiota in children with cancer. Antibiotics 10, 1–15. [CrossRef]
- Newland, J. G., and Hersh, A. L. (2010). Purpose and design of antimicrobial stewardship programs in pediatrics. Pediatric Infectious Disease Journal 29, 862–863. [CrossRef]
- Tamma, P. D., Cosgrove, S. E., and Maragakis, L. L. (2012). Combination therapy for treatment of infections with gram-negative bacteria. Clin Microbiol Rev 25, 450–470. [CrossRef]
- Fanelli, U., Pappalardo, M., Chinè, V., Gismondi, P., Neglia, C., Argentiero, A., et al. (2020b). Role of artificial intelligence in fighting antimicrobial resistance in pediatrics. Antibiotics 9, 1–12. [CrossRef]
- Johnson, C., Nordby, A., Brage Hudson, D., Struwe, L., and Ruppert, R. (2023). Quality improvement: Antimicrobial stewardship in pediatric primary care. J Pediatr Nurs 70, 54–60. [CrossRef]
- Dellit, T. H., Owens, R. C., Mcgowan, J. E., Gerding, D. N., Weinstein, R. A., Burke, J. P., et al. (2007). Infectious Diseases Society of America and the Society for Healthcare Epidemiology of America Guidelines for Developing an Institutional Program to Enhance Antimicrobial Stewardship. Clinical Infectious Diseases 44, 159–77. Available at: https://academic.oup.com/cid/article/44/2/159/328413.
- Dyar, O. J., Huttner, B., Schouten, J., and Pulcini, C. (2017). What is antimicrobial stewardship? Clinical Microbiology and Infection 23, 793–798. [CrossRef]
- Dyar, O. J., Moran-Gilad, J., Greub, G., and Pulcini, C. (2019). Diagnostic stewardship: are we using the right term? Clinical Microbiology and Infection 25, 272–273. [CrossRef]
- Fabre, V., Davis, A., Diekema, D. J., Granwehr, B., Hayden, M. K., Lowe, C. F., et al. (2023). Principles of diagnostic stewardship: A practical guide from the Society for Healthcare Epidemiology of America Diagnostic Stewardship Task Force. Infect Control Hosp Epidemiol 44, 178–185. [CrossRef]
- Donà, D., Barbieri, E., Daverio, M., Lundin, R., Giaquinto, C., Zaoutis, T., et al. (2020). Implementation and impact of pediatric antimicrobial stewardship programs: a systematic scoping review. Antimicrob Resist Infect Control 9. [CrossRef]
- Brigadoi, G., Rossin, S., Visentin, D., Barbieri, E., Giaquinto, C., Da Dalt, L., et al. (2023). The impact of Antimicrobial Stewardship Programmes in paediatric emergency department and primary care: a systematic review. Ther Adv Infect Dis 10. [CrossRef]
- Shah, P., Maheshwari, T., Patel, D., Patel, Z., Dikkatwar, M. S., and Rathod, M. M. (2024). An overview: Implementation and core elements of antimicrobial stewardship programme. Clin Epidemiol Glob Health 29. [CrossRef]
- Donà, D., Mozzo, E., Mardegan, V., Trafojer, U., Lago, P., Salvadori, S., et al. (2017). Antibiotics Prescriptions in the Neonatal Intensive Care Unit: How to Overcome Everyday Challenges. Am.
- WHO (2021). Antimicrobial stewardship interventions: a practical guide. Available at: https://www.who.int/europe/publications/i/item/9789289056267 (Accessed November 6, 2024).
- Barlam, T. F., Cosgrove, S. E., Abbo, L. M., Macdougall, C., Schuetz, A. N., Septimus, E. J., et al. (2016). Implementing an antibiotic stewardship program: Guidelines by the Infectious Diseases Society of America and the Society for Healthcare Epidemiology of America. Clinical Infectious Diseases 62, e51–e77. [CrossRef]
- Kinoshita, N., Komura, M., Tsuzuki, S., Shoji, K., and Miyairi, I. (2020). The effect of preauthorization and prospective audit and feedback system on oral antimicrobial prescription for outpatients at a children’s hospital in Japan. Journal of Infection and Chemotherapy 26, 582–587. [CrossRef]
- Barbieri, E., Bottigliengo, D., Tellini, M., Minotti, C., Marchiori, M., Cavicchioli, P., et al. (2021a). Development of a Weighted-Incidence Syndromic Combination Antibiogram (WISCA) to guide the choice of the empiric antibiotic treatment for urinary tract infection in paediatric patients: a Bayesian approach. Antimicrob Resist Infect Control 10. [CrossRef]
- Liberati, C., Donà, D., Maestri, L., Petris, M. G., Barbieri, E., Gallo, E., et al. (2024). Application of the Weighted-Incidence Syndromic Combination Antibiogram (WISCA) to guide the empiric antibiotic treatment of febrile neutropenia in oncological paediatric patients: experience from two paediatric hospitals in Northern Italy. Ann Clin Microbiol Antimicrob 23. [CrossRef]
- Regev-Yochay, G., Raz, M., Dagan, R., Roizin, H., Morag, B., Hetman, S., et al. (2011). Reduction in antibiotic use following a cluster randomized controlled multifaceted intervention: The Israeli judicious antibiotic prescription study. Clinical Infectious Diseases 53, 33–41. [CrossRef]
- Barbieri, E., De Luca, M., Minute, M., D’amore, C., Atti, M. L. C. D., Martelossi, S., et al. (2020). Impact and sustainability of antibiotic stewardship in pediatric emergency departments: Why persistence is the key to success. Antibiotics 9, 1–16. [CrossRef]
- Gerber, J. S., Jackson, M. A., Tamma, P. D., and Zaoutis, T. E. (2021). Antibiotic stewardship in pediatrics. Pediatrics 147. [CrossRef]
- Dona, D., Baraldi, M., Brigadoi, G., Lundin, R., Perilongo, G., Hamdy, R. F., et al. (2018). The Impact of Clinical Pathways on Antibiotic Prescribing for Acute Otitis Media and Pharyngitis in the Emergency Department. Pediatr Infect Dis J 37, 901–907. [CrossRef]
- Mcgonagle, E. A., Karavite, D. J., Grundmeier, R. W., Schmidt, S. K., May, L. S., Cohen, D. M., et al. (2023). Evaluation of an Antimicrobial Stewardship Decision Support for Pediatric Infections. Appl Clin Inform 14, 108–118. [CrossRef]
- Wei, X., Zhang, Z., Hicks, J. P., Walley, J. D., King, R., Newell, J. N., et al. (2019). Long-term outcomes of an educational intervention to reduce antibiotic prescribing for childhood upper respiratory tract infections in rural China: Follow-up of a cluster-randomised controlled trial. PLoS Med 16. [CrossRef]
- Goggin, K., Hurley, E. A., Bradley-Ewing, A., Bickford, C., Lee, B. R., Pina, K., et al. (2020). Reductions in Parent Interest in Receiving Antibiotics following a 90-Second Video Intervention in Outpatient Pediatric Clinics., in Journal of Pediatrics, (Mosby Inc.), 138-145.e1. [CrossRef]
- Demoly, P., Adkinson, N. F., Brockow, K., Castells, M., Chiriac, A. M., Greenberger, P. A., et al. (2014). International Consensus on drug allergy. Allergy: European Journal of Allergy and Clinical Immunology 69, 420–437. [CrossRef]
- Gomes, E. R., Brockow, K., Kuyucu, S., Saretta, F., Mori, F., Blanca-Lopez, N., et al. (2016). Drug hypersensitivity in children: Report from the pediatric task force of the EAACI Drug Allergy Interest Group. Allergy: European Journal of Allergy and Clinical Immunology 71, 149–161. [CrossRef]
- Chow, T., Patel, G., Mohammed, M., Johnson, D., and Khan, D. (2023). Delabeling penicillin allergy in a pediatric primary care clinic. Ann Allergy Asthma Immunol. 130, 667–669.
- Diane Ashiru-Oredope, Maria Richards, JaneGiles, and Louise Teare (2011). Does an antimicrobial section on a drug chart influence prescribing? pharmaceutical-journal.com/article/research/does-an-antimicrobial-section-on-a-drug-chart-influence-prescribing. Pharm J.
- Di Pentima, M. C., Chan, S., and Hossain, J. (2011). Benefits of a pediatric antimicrobial stewardship program at a children’s hospital. Pediatrics 128, 1062–1070. [CrossRef]
- Velasco-Arnaiz, E., Simó-Nebot, S., Ríos-Barnés, M., López Ramos, M. G., Monsonís, M., Urrea-Ayala, M., et al. (2020). Benefits of a Pediatric Antimicrobial Stewardship Program in Antimicrobial Use and Quality of Prescriptions in a Referral Children’s Hospital. Journal of Pediatrics 225, 222-230.e1. [CrossRef]
- Manice, C., Mularidhar, N., Campbell, J., and Nakamura, M. (2024). Implementation and perceived effectiveness of prospective audit and feedback and preauthorization by US pediatric antimicrobial stewardship programs. J Pediatric Infect Dis Soc 26, 117–122.
- Fratoni, A. J., Nicolau, D. P., and Kuti, J. L. (2021). A guide to therapeutic drug monitoring of β-lactam antibiotics. Pharmacotherapy 41, 220–233. [CrossRef]
- Abdul-Aziz, M. H., Brady, K., Pharm, M., Menino, †, Cotta, O., and Roberts, J. A. (2022). Therapeutic Drug Monitoring of Antibiotics: Defining the Therapeutic Range. Ther Drug Monit 44. Available at: http://journals.lww.com/drug-monitoring.
- Centers for Disease Control and Prevention (2021a). Core elements of hospital antibiotic stewardship programs. Available at: https://www.cdc.gov/antibiotic-use/hcp/core-elements/hospital.html (Accessed November 6, 2024).
- Zembles, T. N., Nakra, N., and Parker, S. K. (2022). Extending the Reach of Antimicrobial Stewardship to Pediatric Patients. Infect Dis Ther 11, 101–110. [CrossRef]
- Knowles, R., Chandler, C., O’neill, S., Sharland, M., and Mays, N. (2024). A systematic review of national interventions and policies to optimize antibiotic use in healthcare settings in England. Journal of Antimicrobial Chemotherapy 79, 1234–1247. [CrossRef]
- Newland, J. G., Stach, L. M., De Lurgio, S. A., Hedican, E., Yu, D., Herigon, J. C., et al. (2012). Impact of a prospective-audit-with-feedback antimicrobial stewardship program at a children’s hospital. J Pediatric Infect Dis Soc 1, 179–186. [CrossRef]
- Hersh, A. L., De Lurgio, S. A., Thurm, C., Lee, B. R., Weissman, S. J., Courter, J. D., et al. (2015). Antimicrobial Stewardship Programs in Freestanding Children’s Hospitals. Pediatric 135, 33–39. Available at: http://publications.aap.org/pediatrics/article-pdf/135/1/33/902628/peds_2014-2579.pdf.
- Zaffagnini, A., Rigotti, E., Opri, F., Opri, R., Simiele, G., Tebon, M., et al. (2024). Enforcing surveillance of antimicrobial resistance and antibiotic use to drive stewardship: experience in a paediatric setting. Journal of Hospital Infection 144, 14–19. [CrossRef]
- Rossin, S., Barbieri, E., Cantarutti, A., Martinolli, F., Giaquinto, C., Da Dalt, L., et al. (2021). Multistep antimicrobial stewardship intervention on antibiotic prescriptions and treatment duration in children with pneumonia. PLoS One 16, 1–14. [CrossRef]
- Opondo, C., Ayieko, P., Ntoburi, S., Wagai, J., Opiyo, N., Irimu, G., et al. (2011). Effect of a multi-faceted quality improvement intervention on inappropriate antibiotic use in children with non-bloody diarrhoea admitted to district hospitals in Kenya. BMC Pediatr 11. [CrossRef]
- Rahbarimanesh, A., Mojtahedi, S. Y., Sadeghi, P., Ghodsi, M., Kianfar, S., Khedmat, L., et al. (2019). Antimicrobial stewardship program (ASP): An effective implementing technique for the therapy efficiency of meropenem and vancomycin antibiotics in Iranian pediatric patients. Ann Clin Microbiol Antimicrob 18. [CrossRef]
- Wattier, R. L., Levy, E. R., Sabnis, A. J., Dvorak, C. C., and Auerbach, A. D. (2017). Reducing Second Gram-Negative Antibiotic Therapy on Pediatric Oncology and Hematopoietic Stem Cell Transplantation Services., in Infection Control and Hospital Epidemiology, (Cambridge University Press), 1039–1047. [CrossRef]
- Haque, A., Hussain, K., Ibrahim, R., Abbas, Q., Ahmed, S. A., Jurair, H., et al. (2018). Impact of pharmacist-led antibiotic stewardship program in a PICU of low/ middle-income country. BMJ Open Qual 7. [CrossRef]
- Taylor MG, P. DL. (2022). Antibiotic stewardship in the pediatric primary care setting. Pediatr Ann 51, 196–201.
- Frost HM, Hersh AL, and Hyun DY (2023). Next steps in ambulatory stewardship. Infect Dis Clin North Am. 37, 749–767.
- Dantuluri, K. L., Bonnet, K. R., Schlundt, D. G., Schulte, R. J., Griffith, H. G., Luu, A., et al. (2023). Antibiotic perceptions, adherence, and disposal practices among parents of pediatric patients. PLoS One 18. [CrossRef]
- Pagano, F., Amato, C., De Marco, G., Micillo, M., Cecere, G., Poeta, M., et al. (2023). Reduction in broad-spectrum antimicrobial prescriptions by primary care pediatricians following a multifaceted antimicrobial stewardship program. Front Pediatr 10. [CrossRef]
- Gerber, J. S., Prasad, P. A., Fiks, A. G., Localio, A. R., Grundmeier, R. W., Bell, L. M., et al. (2013). Effect of an outpatient antimicrobial stewardship intervention on broad-spectrum antibiotic prescribing by primary care pediatricians a randomized trial. JAMA - Journal of the American Medical Association 309, 2345–2352. [CrossRef]
- Gerber, J. S., Prasad, P. A., Fiks, A. G., Localio, A. R., Bell, L. M., Keren, R., et al. (2014). Durability of benefits of an outpatient antimicrobial stewardship intervention after discontinuation of audit and feedback. JAMA - Journal of the American Medical Association 312, 2569–2570. [CrossRef]
- Wei, X., Zhang, Z., Walley, J. D., Hicks, J. P., Zeng, J., Deng, S., et al. (2017). Effect of a training and educational intervention for physicians and caregivers on antibiotic prescribing for upper respiratory tract infections in children at primary care facilities in rural China: a cluster-randomised controlled trial. Lancet Glob Health 5, e1258–e1267. [CrossRef]
- Hamdy, R. F., Nedved, A., Fung, M., Fleming-Dutra, K. E., Liu, C. M., Obremskey, J., et al. (2022). Pediatric Urgent Care Providers’ Approach to Antibiotic Stewardship A National Survey. Pediatr Emerg Care 38. Available at: https://www.cdc.gov/drugresistance/pdf/threats-report/2019-.
- Meesters, K., and Buonsenso, D. (2024). Antimicrobial Stewardship in Pediatric Emergency Medicine: A Narrative Exploration of Antibiotic Overprescribing, Stewardship Interventions, and Performance Metrics. Children 11. [CrossRef]
- Mistry, R. D., May, L. S., and Pulia, M. S. (2019). Improving antimicrobial stewardship in pediatric emergency care: A pathway forward. Pediatrics 143. [CrossRef]
- Nedved, A., Lee, B. R., Hamner, M., Wirtz, A., Burns, A., and El Feghaly, R. E. (2023). Impact of an antibiotic stewardship program on antibiotic choice, dosing, and duration in pediatric urgent cares. Am J Infect Control 51, 520–526. [CrossRef]
- Lucignano, B., Cento, V., Agosta, M., Ambrogi, F., Albitar-Nehme, S., Mancinelli, L., et al. (2022). Effective Rapid Diagnosis of Bacterial and Fungal Bloodstream Infections by T2 Magnetic Resonance Technology in the Pediatric Population. J Clin Microbiol 60. [CrossRef]
- del Rosal, T., Bote-Gascón, P., Falces-Romero, I., Sainz, T., Baquero-Artigao, F., Rodríguez-Molino, P., et al. (2024). Multiplex PCR and Antibiotic Use in Children with Community-Acquired Pneumonia. Children 11. [CrossRef]
- Norman-Bruce, H., Umana, E., Mills, C., Mitchell, H., McFetridge, L., McCleary, D., et al. (2024). Diagnostic test accuracy of procalcitonin and C-reactive protein for predicting invasive and serious bacterial infections in young febrile infants: a systematic review and meta-analysis. Lancet Child Adolesc Health 8, 358–368. [CrossRef]
- Milcent, K., Faesch, S., Guen, C. G. Le, Dubos, F., Poulalhon, C., Badier, I., et al. (2016). Use of Procalcitonin Assays to Predict Serious Bacterial Infection in Young Febrile Infants. JAMA Pediatr 170, 62–69. [CrossRef]
- Barbieri, E., Rossin, S., Giaquinto, C., Da Dalt, L., and Dona’, D. (2021b). A procalcitonin and C-reactive protein-guided clinical pathway for reducing antibiotic use in children hospitalized with bronchiolitis. Children 8. [CrossRef]
- Li, P., Liu, J. Le, and Liu, J. (2022). Procalcitonin-guided antibiotic therapy for pediatrics with infective disease: A updated meta-analyses and trial sequential analysis. Front Cell Infect Microbiol 12. [CrossRef]
- Katz, S. E., Crook, J., Gillon, J., Stanford, J. E., Wang, L., Colby, J. M., et al. (2021). Use of a Procalcitonin-guided Antibiotic Treatment Algorithm in the Pediatric Intensive Care Unit. Pediatric Infectious Disease Journal 40, 333–337. [CrossRef]
- Beaumont R, Tang K, and Gwee A. (2024). The Sensitivity and Specificity of Procalcitonin in Diagnosing Bacterial Sepsis in Neonates. Hosp Pediatr 14, 199–208.
- Martínez-González, N. A., Keizer, E., Plate, A., Coenen, S., Valeri, F., Verbakel, J. Y. J., et al. (2020). Point-of-care c-reactive protein testing to reduce antibiotic prescribing for respiratory tract infections in primary care: Systematic review and meta-analysis of randomised controlled trials. Antibiotics 9, 1–31. [CrossRef]
- Weragama, K., Mudgil, P., and Whitehall, J. (2021). Paediatric antimicrobial stewardship for respiratory infections in the emergency setting: A systematic review. Antibiotics 10. [CrossRef]
- Weragama, K., Mudgil, P., and Whitehall, J. (2022). Diagnostic Stewardship—The Impact of Rapid Diagnostic Testing for Paediatric Respiratory Presentations in the Emergency Setting: A Systematic Review. Children 9. [CrossRef]
- Cohen, J. F., Pauchard, J. Y., Hjelm, N., Cohen, R., and Chalumeau, M. (2020). Efficacy and safety of rapid tests to guide antibiotic prescriptions for sore throat. Cochrane Database of Systematic Reviews 2020. [CrossRef]
- Thibeault, R., Gilca, R., Côté, S., De Serres, G., Boivin, G., and Déry, et P. (2007). Antibiotic use in children is not influenced by the result of rapid antigen detection test for the respiratory syncytial virus. Journal of Clinical Virology 39, 169–174. [CrossRef]
- Rader, T. S., Stevens, M. P., and Bearman, G. (2021). Syndromic Multiplex Polymerase Chain Reaction (mPCR) Testing and Antimicrobial Stewardship: Current Practice and Future Directions. Curr Infect Dis Rep 23. [CrossRef]
- Lee, B. R., Hassan, F., Jackson, M. A., and Selvarangan, R. (2019). Impact of multiplex molecular assay turn-around-time on antibiotic utilization and clinical management of hospitalized children with acute respiratory tract infections. Journal of Clinical Virology 110, 11–16. [CrossRef]
- Rao, S., Lamb, M. M., Moss, A., Mistry, R. D., Grice, K., Ahmed, W., et al. (2021). Effect of Rapid Respiratory Virus Testing on Antibiotic Prescribing among Children Presenting to the Emergency Department with Acute Respiratory Illness: A Randomized Clinical Trial. JAMA Netw Open 4, 1–13. [CrossRef]
- Iran Keske, S. ¸, Zabun, B., Aksoy, K., Can, F., Palaog, E., Lu, ˘, et al. (2018). Rapid Molecular Detection of Gastrointestinal Pathogens and Its Role in Antimicrobial Stewardship. J Clin Microbiol 56. Available at: https://doi.org/10.
- McDonald, D., Gagliardo, C., Chiu, S., and Di Pentima, M. C. (2020). Impact of a rapid diagnostic meningitis/encephalitis panel on antimicrobial use and clinical outcomes in children. Antibiotics 9, 1–9. [CrossRef]
- Kosmeri, C., Giapros, V., Serbis, A., and Baltogianni, M. (2024). Application of Advanced Molecular Methods to Study Early-Onset Neonatal Sepsis. Int J Mol Sci 25. [CrossRef]
- Clodi-Seitz, T., Baumgartner, S., Turner, M., Mader, T., Hind, J., Wenisch, C., et al. (2024). Point-of-Care Method T2Bacteria®Panel Enables a More Sensitive and Rapid Diagnosis of Bacterial Blood Stream Infections and a Shorter Time until Targeted Therapy than Blood Culture. Microorganisms 12. [CrossRef]
- Banerjee, R., Komarow, L., Virk, A., Rajapakse, N., Schuetz, A. N., Dylla, B., et al. (2021). Randomized Trial Evaluating Clinical Impact of RAPid IDentification and Susceptibility Testing for Gram-negative Bacteremia: RAPIDS-GN. Clinical Infectious Diseases 73, E39–E46. [CrossRef]
- Leber, A. L., Everhart, K., Balada-Llasat, J. M., Cullison, J., Daly, J., Holt, S., et al. (2016). Multicenter evaluation of biofire filmarray meningitis/encephalitis panel for detection of bacteria, viruses, and yeast in cerebrospinal fluid specimens. J Clin Microbiol 54, 2251–2261. [CrossRef]
- Kadambari, S., Feng, S., Liu, X., Andersson, M., Waterfield, R., Fodder, H., et al. (2024). Evaluating the Impact of the BioFire FilmArray in Childhood Meningitis: An Observational Cohort Study. Pediatric Infectious Disease Journal 43, 345–349. [CrossRef]
- Banerjee, R., and Patel, R. (2023). Molecular diagnostics for genotypic detection of antibiotic resistance: current landscape and future directions. JAC Antimicrob Resist 5. [CrossRef]
- Pai, N. P., Vadnais, C., Denkinger, C., Engel, N., and Pai, M. (2012). Point-of-Care Testing for Infectious Diseases: Diversity, Complexity, and Barriers in Low- And Middle-Income Countries. PLoS Med 9. [CrossRef]
- Brigadoi, G., Gastaldi, A., Moi, M., Barbieri, E., Rossin, S., Biffi, A., et al. (2022). Point-of-Care and Rapid Tests for the Etiological Diagnosis of Respiratory Tract Infections in Children: A Systematic Review and Meta-Analysis. Antibiotics 11. [CrossRef]
- Tan, R., Kavishe, G., Luwanda, L. B., Kulinkina, A. V., Renggli, S., Mangu, C., et al. (2024). A digital health algorithm to guide antibiotic prescription in pediatric outpatient care: a cluster randomized controlled trial. Nat Med 30, 76–84. [CrossRef]
- Kiemde, F., Valia, D., Kabore, B., Rouamba, T., Kone, A. N., Sawadogo, S., et al. (2023). A Randomized Trial to Assess the Impact of a Package of Diagnostic Tools and Diagnostic Algorithm on Antibiotic Prescriptions for the Management of Febrile Illnesses Among Children and Adolescents in Primary Health Facilities in Burkina Faso. Clinical Infectious Diseases 77, S134–S144. [CrossRef]
- Porta, A., Hsia, Y., Doerholt, K., Spyridis, N., Bielicki, J., Menson, E., et al. (2012). Comparing neonatal and paediatric antibiotic prescribing between hospitals: A new algorithm to help international benchmarking. Journal of Antimicrobial Chemotherapy 67, 1278–1286. [CrossRef]
- Davey, P., Marwick, C. A., Scott, C. L., Charani, E., Mcneil, K., Brown, E., et al. (2017). Interventions to improve antibiotic prescribing practices for hospital inpatients. Cochrane Database of Systematic Reviews 2017. [CrossRef]
- Abel, K., Agnew, E., Amos, J., Armstrong, N., Armstrong-James, D., Ashfield, T., et al. (2024). System-wide approaches to antimicrobial therapy and antimicrobial resistance in the UK: the AMR-X framework. Lancet Microbe 5, e500–e507. [CrossRef]
- Moja, L., Zanichelli, V., Mertz, D., Gandra, S., Cappello, B., Cooke, G. S., et al. (2024). WHO’s essential medicines and AWaRe: recommendations on first- and second-choice antibiotics for empiric treatment of clinical infections. Clinical Microbiology and Infection 30, S1–S51. [CrossRef]
- Hsia, Y., Sharland, M., Jackson, C., Wong, I. C. K., Magrini, N., and Bielicki, J. A. (2019b). Consumption of oral antibiotic formulations for young children according to the WHO Access, Watch, Reserve (AWaRe) antibiotic groups: an analysis of sales data from 70 middle-income and high-income countries. Lancet Infect Dis 19, 67–75. [CrossRef]
- Wattier, R. L., Thurm, C. W., Parker, S. K., Banerjee, R., Hersh, A. L., Brogan, T. V., et al. (2021). Indirect Standardization as a Case Mix Adjustment Method to Improve Comparison of Children’s Hospitals’ Antimicrobial Use. Clinical Infectious Diseases 73, 925–932. [CrossRef]
- Yusuf, E., Versporten, A., and Goossens, H. (2017). Is there any difference in quality of prescribing between antibacterials and antifungals? Results from the first global point prevalence study (Global PPS) of antimicrobial consumption and resistance from 53 countries. Journal of Antimicrobial Chemotherapy 72, 2906–2909. [CrossRef]
- Hersh, A. L., Shapiro, D. J., Pavia, A. T., and Shah, S. S. (2011). Antibiotic prescribing in ambulatory pediatrics in the United States. Pediatrics 128, 1053–1061. [CrossRef]
- UKHSA (2024). AMR local indicators . https://fingertips.phe.org.uk/profile/amr-local-indicators#3. Available at: https://fingertips.phe.org.uk/profile/amr-local-indicators#3 (Accessed November 6, 2024).
- Sarma, J. B., Marshall, B., Cleeve, V., Tate, D., Oswald, T., and Woolfrey, S. (2015). Effects of fluoroquinolone restriction (from 2007 to 2012) on resistance in Enterobacteriaceae: Interrupted time-series analysis. Journal of Hospital Infection 91, 68–73. [CrossRef]
- Lawes, T., Lopez-Lozano, J. M., Nebot, C. A., Macartney, G., Subbarao-Sharma, R., Dare, C. R. J., et al. (2015). Effects of national antibiotic stewardship and infection control strategies on hospital-associated and community-associated meticillin-resistant Staphylococcus aureus infections across a region of Scotland: A non-linear time-series study. Lancet Infect Dis 15, 1438–1449. [CrossRef]
- Gagliotti, C., Nobilio, L., Milandri, M., and Moro, M. L. (2006). Macrolide Prescriptions and Erythromycin Resistance of Streptococcus pyogenes mycin-resistant. Available at: https://academic.oup.com/cid/article/42/8/1153/282887.
- Schroeder, M. R., and Stephens, D. S. (2016). Macrolide resistance in Streptococcus pneumoniae. Front Cell Infect Microbiol 6. [CrossRef]
- Shaughnessy, M. K., Amundson, W. H., Kuskowski, M. A., DeCarolis, D. D., Johnson, J. R., and Drekonja, D. M. (2013). Unnecessary Antimicrobial Use in Patients with Current or Recent Clostridium difficile Infection . Infect Control Hosp Epidemiol 34, 109–116. [CrossRef]
- Cooke, J., Stephens, P., Ashiru-Oredope, D., Charani, E., Dryden, M., Fry, C., et al. (2015). Longitudinal trends and cross-sectional analysis of English national hospital antibacterial use over 5 years (2008-13): Working towards hospital prescribing quality measures. Journal of Antimicrobial Chemotherapy 70, 279–285. [CrossRef]
- Keshavarzi, F. (2022). Practical Concerns about the Metrics and Methods of Financial Outcome Measurement in Antimicrobial Stewardship Programs: A Narrative Review. Iran J Med Sci 47, 394–405. [CrossRef]
- Zhang, Z., Dawkins, B., Hicks, J. P., Walley, J. D., Hulme, C., Elsey, H., et al. (2018). Cost-effectiveness analysis of a multi-dimensional intervention to reduce inappropriate antibiotic prescribing for children with upper respiratory tract infections in China. Tropical Medicine and International Health 23, 1092–1100. [CrossRef]
- Lubell, Y., Do, N. T. T., Nguyen, K. V., Ta, N. T. D., Tran, N. T. H., Than, H. M., et al. (2018). C-reactive protein point of care testing in the management of acute respiratory infections in the Vietnamese primary healthcare setting - A cost benefit analysis. Antimicrob Resist Infect Control 7. [CrossRef]
- Borek, A. J., Anthierens, S., Allison, R., McNulty, C. A. M., Anyanwu, P. E., Costelloe, C., et al. (2020). Social and contextual influences on antibiotic prescribing and antimicrobial stewardship: A qualitative study with clinical commissioning group and general practice professionals. Antibiotics 9, 1–15. [CrossRef]
- Goycochea-Valdivia, W. A., Melendo Pérez, S., Aguilera-Alonso, D., Escosa-Garcia, L., Martínez Campos, L., and Baquero-Artigao, F. (2022). Position statement of the Spanish Society of Paediatric Infectious Diseases on the introduction, implementation and assessment of antimicrobial stewardship programmes in paediatric hospitals. Anales de Pediatría (English Edition) 97, 351.e1-351.e12. [CrossRef]
- Poudel, A. N., Zhu, S., Cooper, N., Little, P., Tarrant, C., Hickman, M., et al. (2023). The economic burden of antibiotic resistance: A systematic review and meta-analysis. PLoS One 18. [CrossRef]
- Morel, C. M., Alm, R. A., Årdal, C., Bandera, A., Bruno, G. M., Carrara, E., et al. (2020). A one health framework to estimate the cost of antimicrobial resistance. Antimicrob Resist Infect Control 9. [CrossRef]
- Turner, R. B., Valcarlos, E., Loeffler, A. M., Gilbert, M., and Chan, D. (2017). Impact of an antimicrobial stewardship program on antibiotic use at a nonfreestanding children’s hospital. J Pediatric Infect Dis Soc 6, e36–e40. [CrossRef]
- Srinivasan, A. (2017). Antibiotic stewardship: Why we must, how we can. Cleve Clin J Med 84, 673–679. [CrossRef]
- Mendelson, M., Morris, A. M., Thursky, K., and Pulcini, C. (2020). How to start an antimicrobial stewardship programme in a hospital. Clinical Microbiology and Infection 26, 447–453. [CrossRef]
- Cosgrove, S. E., Hermsen, E. D., Rybak, M. J., File, T. M., Parker, S. K., and Barlam, T. F. (2014). Guidance for the Knowledge and Skills Required for Antimicrobial Stewardship Leaders. Infect Control Hosp Epidemiol 35, 1444–1451. [CrossRef]
- Wubishet, B. L., Merlo, G., Ghahreman-Falconer, N., Hall, L., and Comans, T. (2022). Economic evaluation of antimicrobial stewardship in primary care: a systematic review and quality assessment. Journal of Antimicrobial Chemotherapy 77, 2373–2388. [CrossRef]
- Villanueva, P., Coffin, S. E., Mekasha, A., McMullan, B., Cotton, M. F., and Bryant, P. A. (2022). Comparison of Antimicrobial Stewardship and Infection Prevention and Control Activities and Resources between Low-/Middle- and High-income Countries. Pediatric Infectious Disease Journal 41, S3–S9. [CrossRef]
- Ecdc (2022). Antimicrobial consumption in the EU/EEA (ESAC-NET) - AER for 2022. Available at: https://www.ecdc.europa.eu/en/publications-data/antimicrobial-consumption-eueea-esac-net-annual-.
- Kopsidas, I., Vergnano, S., Spyridis, N., Zaoutis, T., and Patel, S. (2020). A Survey on National Pediatric Antibiotic Stewardship Programs, Networks and Guidelines in 23 European Countries. Pediatric Infectious Disease Journal 39, E359–E362. [CrossRef]
- Centers for Disease Control and Prevention (2021b). Core Elements of Outpatient Antibiotic Stewardship The Core Elements of Outpatient Antibiotic Stewardship Facility Checklist. Available at: https://www.cdc.gov/antibiotic-use/hcp/core-elements/outpatient-antibiotic-stewardship.html#:~:text=The%20four%20core%20elements%20of,reporting%2C%20and%20education%20and%20expertise. (Accessed November 6, 2024).
- Keller, S. C., Cosgrove, S. E., Miller, M. A., and Tamma, P. (2022). A framework for implementing antibiotic stewardship in ambulatory care: Lessons learned from the Agency for Healthcare Research and Quality Safety Program for Improving Antibiotic Use. Antimicrobial Stewardship and Healthcare Epidemiology 2, 185–190. [CrossRef]
- Zakhour, J., Haddad, S. F., Kerbage, A., Wertheim, H., Tattevin, P., Voss, A., et al. (2023). Diagnostic stewardship in infectious diseases: a continuum of antimicrobial stewardship in the fight against antimicrobial resistance. Int J Antimicrob Agents 62. [CrossRef]
- Pansa, P., Hsia, Y., Bielicki, J., Lutsar, I., Walker, A. S., Sharland, M., et al. (2018). Evaluating Safety Reporting in Paediatric Antibiotic Trials, 2000–2016: A Systematic Review and Meta-Analysis. Drugs 78, 231–244. [CrossRef]
- Rudnick, W., Conly, J., Thirion, D. J. G., Choi, K., Pelude, L., Cayen, J., et al. (2023). Antimicrobial use among paediatric inpatients at hospital sites within the Canadian Nosocomial Infection Surveillance Program, 2017/2018. Antimicrob Resist Infect Control 12. [CrossRef]
- Wicha, S. G., Märtson, A. G., Nielsen, E. I., Koch, B. C. P., Friberg, L. E., Alffenaar, J. W., et al. (2021). From Therapeutic Drug Monitoring to Model-Informed Precision Dosing for Antibiotics. Clin Pharmacol Ther 109, 928–941. [CrossRef]
- Cojutti, P. G., Gatti, M., Bonifazi, F., Caramelli, F., Castelli, A., Cavo, M., et al. (2023). Impact of a newly established expert clinical pharmacological advice programme based on therapeutic drug monitoring results in tailoring antimicrobial therapy hospital-wide in a tertiary university hospital: Findings after the first year of implementation. Int J Antimicrob Agents 62. [CrossRef]
- Liu, L., Oza, S., Hogan, D., Chu, Y., Perin, J., Zhu, J., et al. (2016). Global, regional, and national causes of under-5 mortality in 2000–15: an updated systematic analysis with implications for the Sustainable Development Goals. The Lancet 388, 3027–3035. [CrossRef]
- Cox, J. A., Vlieghe, E., Mendelson, M., Wertheim, H., Ndegwa, L., Villegas, M. V., et al. (2017). Antibiotic stewardship in low- and middle-income countries: the same but different? Clinical Microbiology and Infection 23, 812–818. [CrossRef]
- Boracchini, R., Brigadoi, G., Barbieri, E., Liberati, C., Rossin, S., Tesser, F., et al. (2024). Validation of Administrative Data and Timing of Point Prevalence Surveys for Antibiotic Monitoring. JAMA Netw Open 7, e2435127. [CrossRef]
- Johnson, A. P., Ashiru-Oredope, D., and Beech, E. (2015). Antibiotic stewardship initiatives as part of the UK 5-year antimicrobial resistance strategy. Antibiotics 4, 467–479. [CrossRef]
- Giacobbe, D. R., Marelli, C., Guastavino, S., Mora, S., Rosso, N., Signori, A., et al. (2024). Explainable and Interpretable Machine Learning for Antimicrobial Stewardship: Opportunities and Challenges. Clin Ther 46, 474–480. [CrossRef]
- Feretzakis, G., Loupelis, E., Sakagianni, A., Kalles, D., Martsoukou, M., Lada, M., et al. (2020). Using machine learning techniques to aid empirical antibiotic therapy decisions in the intensive care unit of a general hospital in Greece. Antibiotics 9. [CrossRef]
- Beaudoin, M., Kabanza, F., Nault, V., and Valiquette, L. (2016). Evaluation of a machine learning capability for a clinical decision support system to enhance antimicrobial stewardship programs. Artif Intell Med 68, 29–36. [CrossRef]
- Liu, G. Y., Yu, D., Fan, M. M., Zhang, X., Jin, Z. Y., Tang, C., et al. (2024). Antimicrobial resistance crisis: could artificial intelligence be the solution? Mil Med Res 11. [CrossRef]
- Driesnack, S., Rücker, F., Dietze-Jergus, N., Bondarenko, A., Pletz, M. W., and Viehweger, A. (2024). A practice-based approach to teaching antimicrobial therapy using artificial intelligence and gamified learning. JAC Antimicrob Resist 6. [CrossRef]
- Howard, A., Aston, S., Gerada, A., Reza, N., Bincalar, J., Mwandumba, H., et al. (2024). Antimicrobial learning systems: an implementation blueprint for artificial intelligence to tackle antimicrobial resistance. Lancet Digit Health 6, e79–e86. [CrossRef]
- Stenehjem, E., Hersh, A. L., Buckel, W. R., Jones, P., Sheng, X., Evans, R. S., et al. (2018). Impact of implementing antibiotic stewardship programs in 15 small hospitals: A cluster-randomized intervention. Clinical Infectious Diseases 67, 525–532. [CrossRef]
- The Joint Commission (2016). New Antimicrobial Stewardship Standard. Joint Commission Perspectives 36.

Table 1.
Incremental costs and potential benefits of Antimicrobial Stewardship Programmes.
| Setting | Incremental cost | Potential saving/benefit |
|---|---|---|
| Inpatient | Clinical pathways implementation:
Implementation (operational) cost:
|
Direct costs:
Indirect costs:
|
| Outpatient | Medical consultations and revisits Nursing support and data monitoring Clinical pathways implementation:
Training for healthcare professionals:
|
Medical consultation for antimicrobial prescription Costs related to antimicrobial therapies (reimbursement by the payer) Prescription monitoring or review Ancillary tests (in Emergency Department) Medication costs |
Table 2.
Costs related to the patient colonised or infected with resistant pathogen in human health.
Table 2.
Costs related to the patient colonised or infected with resistant pathogen in human health.
| Direct costs: | Indirect costs: | Associated probabilities: |
|---|---|---|
Costs of any treatment or prophylaxis
Costs of long- term consequences of AMR infection
Out-of-pocket expenditure by the patient for care
Training of health care professionals and information/communication Legal and insurance costs
|
Productivity loss
Psychological impact on the patient and family (factored in as QALY) Financial burden on the government for disability benefits Hospital costs
Research and development of new antibiotics Additional costs non directly related to human health* |
Mortality (overall): deaths WITH a MDR infection Mortality (attributable): deaths FROM an MDR infection Morbidity:
Additional diagnostic procedures Screening programs Insurance to cover extra AMR costs |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



