
Submitted:
24 December 2024
Posted:
25 December 2024
You are already at the latest version
Abstract
The long-term protective effect of self-awareness in substance use disorders, described as a type of brain disease, is currently being discussed and is called tertiary prevention. The aim of this study was to demonstrate the contribution of a positive psychotherapy program implemented in tertiary prevention by repeatedly measuring patients’ levels of harm perception and result awareness. One-group pre-test post-test experimental model was used according to the quantitative method. The sample of the study consisted of 44 patients who applied to AMATEM and were diagnosed with substance use disorder and/or alcohol use disorder and comorbid bipolar disorder. Two groups were formed by taking into account comorbidities: The first group consisted of 30 individuals with substance use disorder and/or alcohol use disorder. The second group consisted of 14 patients diagnosed with bipolar disorder together with substance use disorder. The data were collected with the Uskudar Harm Perception Scale (USHPS) and the Uskudar Result Awareness Scale (USRAS), developed by Tarhan, Demirsoy and Tutgun-Ünal. As a result of the study, the pre-test and post-test scores of the patients differed, and their awareness levels increased after the psychotherapy program. It was understood that the program and measurement tools contributed to the tertiary prevention studies.
Keywords:
Substance use disorder
; bipolar
; tertiary prevention
; positive psychotherapy
; self-awareness
; harm perception
1. Introduction
With the increasing number of studies indicating that mindfulness-based interventions are more effective and permanent than traditional treatments in substance use disorders, it is emphasized that tertiary protection and prevention treatments are gaining strength but are open to development with their limited aspects. Mindfulness is defined as a method that derives its foundation from the Eastern meditation tradition and directs the person’s attention to what is happening in the present moment, while also adopting a non-judgmental and accepting approach [1] . Although this method has existed in the East for a very long time, it is reported that it has been used in the West for about thirty years and that it started with Kabat-Zinn [2] as a separate approach in psychotherapy [3].
Recently, it has been observed that mindfulness-based interventions have been frequently used in substance use disorders [4,5,6]. Substance use disorder is defined by characteristics such as gradually increasing the dose of the substance used by the person, the emergence of withdrawal symptoms when the person stops using the substance, unsuccessful attempts to quit, continuing to use the substance despite being harmed, spending a large portion of time searching for the substance, using more than the person intended, and not being able to control the use of the substance [7]. In the first edition of the DSM in 1952, substance use was addressed under the title of “Sociopathic Personality Disturbance” and the content of substance use was given very limited space. With DSM-III, a distinction was made for the first time between substance abuse and substance dependence, and it was emphasized that physiological dependence symptoms should be detected for the diagnosis of addiction. DSM-IV introduced a hierarchical approach to the diagnoses of substance abuse and substance dependence [8]. While “substance abuse” and “substance dependence” were evaluated as different disorders in DSM-IV-TR, these diagnoses were combined in DSM-5 and designated as “substance use disorder” [7]. In DSM-5, the sentence “persistently creating legal problems” was removed from the diagnostic criteria in DSM-IV-TR. While the substances that cause disorders related to substance use were divided into 11, they were divided into 10 in DSM-5. The classification in DSM-5 is as follows; alcohol, caffeine, cannabis, hallucinogens (phencyclidine is included in this group and the group is divided into phencyclidine and other hallucinogens), inhalants, opiates, sedative-hypnotics and anxiolytics, stimulants (amphetamine, cocaine and other stimulants), nicotine and other (or unknown substances). Unlike DSM-IV-TR, the diagnosis of multiple substance addiction is not included in DSM-5.
According to the literature, relapse has an important place in substance use problems. It is stated that stress, negative emotions, and cravings can be effective on relapse [9]. Unlike other treatments, mindfulness-based interventions are important in that they aim to develop awareness and acceptance by focusing on the present, emotional and physical sensations without making any judgments, increase the ability to regulate emotions and control impulsive behaviors. It is seen in the literature that there are many mindfulness-based intervention methods such as Mindfulness-Based Stress Reduction (MBSR), Mindfulness-Based Cognitive Therapy (MBCT), and Mindfulness-Based Relapse Prevention (MBRP). At the same time, the concept of mindfulness appears to be an important component in other 3rd Wave therapies such as Acceptance and Commitment Therapy and Dialectical Behavioral Therapy [10].
It is thought that mindfulness-based interventions will be effective in addressing problems related to emotion regulation seen in substance use disorders [11]. Mindfulness has positive effects on emotional regulation and provides improvement in emotional regulation [11,12,13]. It also has a reducing effect on impulsivity and impulsive behaviors associated with substance use problems [14]. Recent research indicates that mindfulness-based approaches are being applied in the management of substance addiction and have yielded positive outcomes [6,15,16].
Mindfulness is an important approach in both treatment and relapse prevention, and it is noteworthy that the majority of studies are conducted by some researchers (such as Brewer, Shorey, Bowen, Wietkiewitz) in mindfulness-based studies. There are very few studies in Turkiye based on the concept of mindfulness. These studies are descriptive studies that provide theoretical information and have studied mindfulness as a personality trait [17,18]. It was observed that there is no study examining the effectiveness of mindfulness-based interventions in adults with substance use problems in Turkey. Research is needed to see the extent to which such interventions are effective in a Turkish sample [3]. There are two scales in the literature that aim to contribute to tertiary protection and prevention standards that include awareness-based intervention studies. The validity and reliability studies of the two scales, namely the 25-item and 6-factor Uskudar Result Awareness Scale (USRAS) and the 36-item and 10-factor Uskudar Harm Perception Scale (USHPS), developed by Tarhan, Demirsoy, and Tutgun-Ünal [19], were conducted on an experimental group with substance and alcohol use disorders and an undiagnosed control group in a sample of 1134 participants in Türkiye in 2023.
In this study, a program that includes group psychoeducation, individual therapy sessions, interaction groups, occupational therapy activities, and psychoeducation and attitude interviews for families, structured in accordance with the positive psychotherapy approach, will be applied to patients with substance use disorder and/or alcohol use disorder and bipolar disorder comorbidity. The contribution of the application to the increase in awareness will be compared by taking pre-test and post-test measurements using the USRAS and USHPS scales.
1.1. Positive Psychotherapy as a Tertiary Standard of Protection and Prevention
In the case of addictions, the primary goal of prevention is to prevent addiction from occurring or to alleviate it if it already exists. Primary prevention includes everything; it is the activity that attempts to prevent a certain addiction from developing in a person who has never used the substance in question before. Secondary prevention deals with patients who have had significant experience with a certain addictive substance; the aim is to reduce further harm. Tertiary prevention focuses on the rehabilitation and reintegration (programs, treatments, psychotherapies) of individuals who developed a disorder [20]. In tertiary prevention, the aim of therapies is to restore a healthy mental state. This requires professional psychologists and psychiatrists.
One of the basic protective factors used effectively in the fight against substance and alcohol use disorders is the family, which is also considered as an etiological element. Accordingly, positive family dynamics have a preventive effect in substance and alcohol use disorders [21]. Family dynamics, including secure attachment and empathy-driven behavioral interactions, are essential psychotherapeutic elements in individual psychotherapy. To ensure the successful treatment of substance use disorder, it is crucial that significant family members and loved ones participate in key stages of the treatment process. Consequently, the family is integral to the strategies and methods designed to combat alcohol and substance use disorder.
However, studies emphasizing hope as a protective factor are becoming increasingly common. In research exploring how resilience mediates the relationship between family support and hope, 647 individuals with substance use disorder completed questionnaires on family support, resilience, and hope. The study utilized structural equation modeling to conduct a moderated mediation analysis. Findings revealed that, besides the direct impact of family support on hope, there was a notable indirect effect via resilience. This indirect effect was significant in both the non-relapse and relapse groups. Additionally, the relationship between family support and resilience, as well as the link between resilience and hope, was influenced by the relapse experience. The results imply that enhancing resilience through interventions could be a promising strategy for boosting hope among substance addicts [22].
For individuals with substance use disorder, there's a link between their levels of anger, addiction profiles, and their depression and anxiety levels [23]. Studies suggest that higher levels of anger correlate with a more significant impact of substance use on daily life, as well as an increased desire to use substances. Consequently, anger assessment is regarded as vital in the treatment process for substance use disorder. Moreover, in those with alcohol and substance use disorders, appetite, nutritional status, and quality of life are closely linked [24].
The study also delves into the sociodemographic and clinical profiles of individuals with alcohol and substance use disorders who were treated at an AMATEM unit. This examination provides valuable insights into the demographics and clinical features of these patients. The study shows that men are more likely to seek treatment for these disorders compared to women, and their substance use often leads to family issues and high rates of job loss [25]. Interviews with 9 patients receiving treatment revealed that they experienced stigmatization, and dealt with various medical, psychological, social, legal, and economic challenges, which largely drove their motivation to pursue treatment [25,26].
On the other hand, factors such as socioeconomic level, ethnicity, exposure to migration, and inability to adapt to city life come to the fore as triggers for substance use [27]. Currently, the biopsychosocial framework is essential in addressing the treatment of alcohol and substance addiction [28]. This model does not reduce the disease to a medical focus; it predicts that the elements that cause the disease may be related to psychological and social contexts. This perspective, which takes into account the psychological and social elements of the person, takes into account that psychosocial characteristics may be related to substance use, and thus the medical perspective, which blames the person and claims that the source of the problems is solely the person himself, is rejected.
Since 1983, the institution that has received the most applications regarding alcohol and non-alcoholic psychoactive substance use in Türkiye, the number of applications made to AMATEM due to substance use was 78 in 1983, and this number reached 2917 in 1996. The data, accounting for repeated applications, shows that the number of individuals seeking treatment for substance use disorder for the first time was 665 in 1993, 882 in 1994, 984 in 1995, and 955 in 1996. By the first 10 months of 2006, this figure had risen to 1742. This trend indicates a growing substance use problem [29]. Consequently, the development of tertiary prevention and protection standards, which include long-term relapse prevention and awareness-based protective measures, has become increasingly crucial.
Furthermore, research shows that more than half of individuals with alcohol and substance use disorders start drinking again within a few months after detoxification. This relapse is frequently driven by negative emotional states, interpersonal conflicts, and social pressure [30,31,32,33,34]. Therefore, when establishing rehabilitation standards alongside awareness levels, it is crucial to design these standards to protect the patient from relapse as effectively as possible. At this point, incorporating the perspective of positive psychology into rehabilitation processes can be highly beneficial. Positive psychology sets itself apart from traditional psychological teachings. Its goal is not to supplant conventional psychology but to serve as a significant complement to it. Positive psychotherapy, meanwhile, is rooted in the principles of positive psychology [35].
Positive psychology aims to explore and implement strategies to enhance life satisfaction and happiness in both healthy individuals and those with clinical conditions [36,37,38,39]. Positive Activity Interventions (PAIs) refer to short, self-administered, and non-stigmatizing activities or exercises designed to foster positive emotions, thoughts, and behaviors, rather than focusing on correcting negative or pathological ones.
An investigation advocating for a pluralistic perspective on addiction addresses the problematic self-regulation of individuals with addictions from an existential positive viewpoint (also known as PP2.0) [40]. The study reveals that those addicted to substances, gambling, internet use, shopping, or eating often experience existential struggles that can explain the origin and maintenance of their addictions. Relational issues, guilt, avoiding responsibility, and a lack of life meaning are well-documented. At the core of this study is an inability to handle life's darker aspects and an inappropriate search for positive emotions, which are not naturally sourced from meaningful social interactions. Accordingly, the Meaning-Centered Approach (MCA) is proposed for addiction recovery, aiding clients in finding life's purpose and reintegrating into society. This existentially positive approach could serve as an essential complement to conventional addiction treatments. The research spotlights Positive Psychotherapy as a tertiary prevention and protection standard.
2. Materials and Methods
2.1. Research Design
The study employed a quantitative method, utilizing a one group pretest-posttest design among the experimental models. This design involves measuring the same dependent variable in a single group of participants both before (pretest) and after (posttest) administering a treatment [41]. In this study, it was decided to apply the single group model separately for two different groups.

Table 1.
Research Design.
| Group | Pre-test | Process | Post-test |
| G | Q1 | X | Q2 |
| G1: Substance Use Disorder and/or Alcohol Use Disorder G2: Substance Use Disorder and Mood Disorder |
Uskudar Result Awareness Scale, Uskudar Harm Perception Scale |
Individual Therapy, Interaction Group, Psychoeducation program | Uskudar Result Awareness Scale, Uskudar Harm Perception Scale |
2.2. Participants
The sample of the study consisted of 44 patients aged 18 and over who were diagnosed with substance use disorder and receiving inpatient treatment at AMATEM. As a result of the examinations, two groups were formed by taking into account comorbidities: The first group consisted of 30 individuals with substance use disorder and/or alcohol use disorder. The second group consisted of 14 patients diagnosed with bipolar disorder together with substance use disorder.
A total of 44 people participated in the study, 35 were male (79.5%) and 9 were female (20.9%). Of the 30 people included in the first group, 28 were male (93.3%) and 2 were female (6.7%). Of the 14 people constituting the second group, 7 were male (50%) and 7 were female (50%). In general, the ages of the patients in the study group ranged between 18-47, and the average age was 31. The ages of the patients in the first group ranged between 19-45, and the average age was 33. The ages of the second group ranged between 18-47, and the average age was 28.
2.3. Data Collection Tools
In the research, data were collected using a questionnaire that included the Uskudar Result Awareness Scale (USRAS), the Uskudar Harm Perception Scale (USHPS), and a demographic information form, all of which are valid and reliable tools.
2.3.1. Demographic Information Form
The demographic information form included questions about the participants' gender, age, education level, marital status, whether they have children, and their use and frequency of harmful substances.
2.3.2. Uskudar Result Awareness Scale (USRAS) and Uskudar Harm Perception Scale (USHPS)
The Uskudar Result Awareness Scale (USRAS) and the Uskudar Harm Perception Scale (USHPS), which were developed by Tarhan, Demirsoy and Tutgun-Ünal [19] and whose validity and reliability studies were conducted on a sample of 1134 participants in Türkiye were used in the study. In addition, the AMOS program was utilized to create a model from the factor structures using data from 400 participants (normal and substance use disorder groups). Confirmatory factor analysis was performed to verify the model, and acceptable goodness of fit values were obtained. The USRAS, consisting of 25 items and 6 factors, explained 58.49% of the total variance, with Cronbach’s Alpha value of .72 for internal consistency reliability. The USHPS scale, made up of 36 items and 10 factors, accounted for 56.36% of the total variance, with a Cronbach’s Alpha value of .83.
When the dimensional structure of the Uskudar Result Awareness Scale is examined; Factor 1 (Items 1–7) is “Medium and Long-Term Plan”; Factor 2 (Items 8–11) is “Action”; Factor 3 (Items 12–15) is “Decision”; Factor 4 (Items 16–18) is “Short-Term Plan”; Factor 5 (Items 19–22) is “Emotion/Intention”; and Factor 6 (Items 23–25) was named as “Philosophy of Life”. The USRAS scale form is rated on a 5-point Likert type as “Strongly Disagree”, “Disagree”, “Neither/Nor Agree”, “Agree” and “Strongly Agree”. A minimum of “1” and a maximum of “5” points can be obtained from each item, and there are items that need to be scored reversely (8,9,10,12,13,14,15,16,18,19,20,21,22,23,24,25). Between 25 and 58 points is evaluated as “Low Result Awareness”; between 59 and 89 points is evaluated as “Medium Result Awareness”; and between 90 and 125 points is evaluated as “High Result Awareness”.
When the dimensional structure of the Uskudar Harm Perception Scale was examined; Factor 1 (Items 1–6) is “Objectivity and Long-Term Perceptual Blindness”; Factor 2 (Items 7–11) is “Stress Relief ”; Factor 3 (Items 12–156) is “Impulsivity and Subjective Reality Blindness”; Factor 4 (Items 17–19) is “Curiosity”; Factor 5 (Items 20–22) is “Harm Avoidance”; Factor 6 (Items 23–24) is “Sensation-seeking”; Factor 7(Items 25–27) is “Perception of Narcissism”; Factor 8 (Items 28–31) is “Perception of Hedonism”; Factor 9 (Items 32–33) is “Control”; and Factor 10 (Items 34–36) was named as “Intention”. The USHPS scale form is rated on a 5-point Likert type as “Strongly Disagree”, “Disagree”, “Neither/Nor Agree”, “Agree” and “Strongly Agree”. A minimum of “1” and a maximum of “5” points can be obtained from each item, and there are items that need to be scored reversely (5, 7, 8, 9, 10, 11, 17, 18, 20, 21, 22, 23, 24, 25, 26, 27, 30, 32, 33, 34, 35, 36). Between 36 and 83 points is evaluated as “Low harm perception/very high risk”; between 84 and 132 points is evaluated as “Moderate harm perception/moderate risk”; and between 133 and 180 points is evaluated as “High harm perception/low risk”.
2.4. Criteria for Inclusion/Exclusion
The study included groups of patients diagnosed with substance use disorder and/or alcohol use disorder, following the DSM-5 diagnostic criteria from the American Psychiatric Association, and who were undergoing inpatient treatment at the clinic. Furthermore, the criteria for diagnosing bipolar disorder were used to determine comorbidity. Individuals younger than 18 years old were not part of the study.
2.5. Procedures
Pilot Application: The online survey prepared as a data collection tool in the research was first applied to 3 people for trial purposes to test the comprehensibility of the questions. Subsequently, a preliminary application was tested on two patients receiving treatment at the AMATEM unit, supervised by a psychologist and in consultation with a psychiatrist. The pilot application encountered no problems, allowing the commencement of the broader field application.
Application of Scales: After the Ethics Committee's approval on December 30, 2022, an online survey including a Demographic Information Form, USRAS, and USHPS scales was administered to inpatient patients at AMATEM on a voluntary basis from October 1, 2023, to March 30, 2024. For those with substance use disorder, alcohol use disorder, and bipolar comorbidity, the survey was conducted on a portable computer under a psychologist's supervision, also on a voluntary basis, with data being collected during this period.
Intervention Program: Although the duration of the program applied to AMATEM patients varies according to the clinical condition of the patient, the generally applied program is as follows: an average of 3-4 individual therapy sessions per week (may be less or more frequent depending on the clinical condition of the patient) + 2 interaction groups per week + Structured group psychoeducation consisting of 9 sessions + Occupational therapy activities (painting, ceramics, marbling, handicrafts, kitchen workshop, music therapy, body movement therapy, sports) + Psychoeducation and attitude interviews with families. The Psychotherapy Program is applied 6 days a week. The steps of the 9-session Group Psychoeducation are as follows: (1) Substances and Alcohol, (2) Addiction, (3) Motivation, (4) Defining Feelings, (5) Desire-Emotion-Thought, (6) Risky situations, (7) Defining the shift, (8) Thought Traps, (9) Changing for Healing.
2.6. Data Processings and Statistical Analysis
For comparative analyses, whether the data show normal distribution is measured with normality tests. In order to examine the conformity of the two scale scores (USRAS and USHPS) used in the study to normal distribution, skewness and kurtosis values were calculated. Skewness and kurtosis values obtained from scale scores are considered sufficient for normal distribution to be between +3 and -3 [42,43,44]. According to the results of the normality test, it was observed that the skewness value of the scale scores was between -.059 and .963, and the kurtosis value was between -.512 and .829. Scale scores showed normal distribution.
A one-group t-test (one-sample t-test) was used to compare the scores obtained as a result of re-applying the USRAS and USHPS scales to the same group at certain intervals. Mean and standard deviation calculations were made for the average scores of the groups based on the total scale score. SPSS 26.0 statistics program was used for the analyses and comparison tests.
3. Results
First, the average scores of the patients included in the groups from the USRAS and USHPS scales were calculated. The pre-treatment measurements are given as pre-test scores, and the measurements after the intervention program are given as post-test scores in Table 2.
When Table 2 is examined, it is seen that the groups’ USRAS pre-test mean scores and post-test mean scores differ, and the post-test scores applied after the intervention program are significantly higher. Similarly, the USHPS post-test scores were found to be higher than the pre-test scores in all groups. USRAS pre-test and post-test scores showed “Medium result awareness”. USHPS pre-test and post-test scores showed “Moderate harm perception/moderate risk”. In line with the increase in the post-test scores, we can say that after the intervention program, it was observed that the results awareness and harm perception scores moved towards the low-risk group and the awareness level gradually increased. Then, it was tested with a one group t-test whether the increase in the mean scores of the groups created a statistically significant difference and the results are given in Table 3.
When Table 3 is examined, the pre-test and post-test scores of the groups differ significantly (p<0.01). As can be understood from the mean scores, the level of result awareness and harm perception of those with substance use disorder and/or alcohol use disorder in Group 1 is significantly higher after the intervention. The post-test scores of result awareness and harm perception of individuals with comorbid substance use disorder and bipolar disorder in Group 2 are significantly higher after the intervention. Thus, the levels of result awareness and harm perception for both groups have increased statistically significantly compared to the measurements at the time of their first application.
Thus, it is graphically shown in Figure 1 that the responses of the patients in both groups to the scales differed following the intervention program. Although it has been observed that the implemented program created awareness in patients, it is a process that requires long-term follow-up and these studies need to be repeated.
4. Conclusion and Discussion
In this study, the contribution of the Result Awareness and Harm Perception Scales, which were developed to be used in tertiary protection and prevention processes to measure the effectiveness of the awareness-based intervention program in patients with substance use disorder and comorbid bipolar disorder, was demonstrated by using them as pre-tests and post-tests. Unlike the measurements made at the beginning, it was observed that the harm perception and result awareness levels increased in the measurements made after the intervention program. The fact that these scales have the capacity to measure and evaluate whether people “know the natural consequences of their actions or are aware of whether they are experiencing harm and danger” with their sub-dimensions was proven by the comparison made with interval measurements in this study. The measurements also determine the low-medium-high risk sub-dimensions and provide a target-setting feature in personalized treatment and rehabilitation. The fact that the level can be measured again when the treatment or rehabilitation is completed gave us the treatment output. It was concluded that the findings obtained in the study have the potential to create a reference and infrastructure for future studies.
In the study of Tarter and colleagues [45] on opioid addiction, it is emphasized that improving the factors that cause and maintain addiction is essential for effective prevention. Similar to this study, in many addiction studies in the literature, it is clear that there is a need for measurement tools developed by incorporating psychometric processes in order to determine the factors that maintain addiction or, in other words, cause relapse, and that awareness of harm perception and consequences should be measured at certain intervals [3,6,9,17,18,19,29,30,33,45]. This will also make it easier to decide on the impact of the intervention program, as it will provide quantitative data.
Drawing on data from a 25-year study conducted by the Center for Education and Drug Abuse Research (CEDAR) at the University of Pittsburgh, assessment tools were developed to correspond to the three components of addiction etiology, specifically individual risk [46], environmental risk [47], and drug use topology [48]. When analyzing the measurement tools, problem severity (ranging from 0% to 100%) is assessed in several areas such as mental and physical health, behavior, social skills, and key environments including family, peers, school, and work. Crucially, the responses are scored immediately and automatically, enabling real-time sharing of results during the assessment. This approach eliminates the possibility of denial, as problem severity directly reflects the individual’s answers. Consequently, these tools are employed to measure the success of prevention programs [45]. The fact that the number of scales in question is more than 10 and the number of subscales is almost twice that, gives a clue that the scales and dimensions in this study can be used more practically in measurements.
Author Contributions
Conceptualization, N.T. and Ç.D.; methodology, N.T. and A.T.-Ü.; validation, A.T.-Ü.; formal analysis, A.T.-Ü.; investigation, Ç.D.; resources, N.T. and A.T.-Ü.; data curation, A.T.-Ü.; writing—original draft preparation, N.T. and A.T.-Ü. writing—review and editing, N.T., Ç.D. and A.T.-Ü.; visualization, A.T.-Ü.; supervision, N.T. and Ç.D.; project administration, N.T., Ç.D.; funding acquisition, N.T., Ç.D. and A.T.-Ü. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
This study received ethical approval from the Uskudar University Non-Interventional Research Ethics Committee report number of 61351342/December 2022-47 (28 December 2022). This study was performed according to the principles set out by the Declaration of Helsinki for the use of humans in experimental research.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Please contact the email nevzat.tarhan@uskudar.edu. tr to get the access of data.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Kabat-Zinn, J. Coming to our senses: Healing ourselves and the world through mindfulness; Hachette UK: 2005.
- Kabat-Zinn, J. An outpatient program in behavioral medicine for chronic pain patients based on the practice of mindfulness meditation: Theoretical considerations and preliminary results. General hospital psychiatry 1982, 4, 33-47. [CrossRef]
- Alpay, Ü.; Aydogdu, B.E.; Yorulmaz, O. The Effect of Mindfulness-Based Interventions on Adults' Substance Use: A Systematic Review. Addicta 2018, 5, 736-746. [CrossRef]
- Bowen, S. and A. Marlatt, Surfing the Urge: Brief Mindfulness-Based Intervention for College Student Smokers. Psychology of Addictive Behaviors, 2009. 23(4): p. 666-671.
- Brewer, J.A., et al., Mindfulness Training and Stress Reactivity in Substance Abuse: Results from a Randomized, Controlled Stage I Pilot Study. Substance Abuse, 2009. 30(4): p. 306-317.
- Witkiewitz, K.; Greenfield, B.L.; Bowen, S. Mindfulness-based relapse prevention with racial and ethnic minority women. Addictive Behaviors 2013, 38, 2821–2824.
- Association, A.P. Diagnostic and statistical manual of mental disorders: DSM-5; American psychiatric association: Washington, DC, 2013; Vol. 5.
- Güleç, G.; Köşger, F.; Eşsizoğlu, A. Alcohol and Substance Use Disorders in DSM-5 Current Approaches in Psychiatry 2015, 7, 448-460. [CrossRef]
- Carroll, H.; Lustyk, M.K.B. Mindfulness-Based Relapse Prevention for Substance Use Disorders: Effects on Cardiac Vagal Control and Craving Under Stress. Mindfulness 2018, 9, 488-499. [CrossRef]
- Turner, K. Mindfulness: The Present Moment in Clinical Social Work. Clin Soc Work J 2009, 37, 95-103. [CrossRef]
- Hoppes, K. The application of mindfulness-based cognitive interventions in the treatment of co-occurring addictive and mood disorders. CNS Spectrums 2006, 11, 829–851.
- Coffey, K.A.; Hartman, M. Mechanisms of Action in the Inverse Relationship Between Mindfulness and Psychological Distress. J Evid-Based Integr 2008, 13, 79-91. [CrossRef]
- Roemer, L.; Lee, J.K.; Salters-Pedneault, K.; Erisman, S.M.; Orsillo, S.M.; Mennin, D.S. Mindfulness and Emotion Regulation Difficulties in Generalized Anxiety Disorder: Preliminary Evidence for Independent and Overlapping Contributions. Behav Ther 2009, 40, 142-154, doi:DOI 10.1016/j.beth.2008.04.001.
- Murphy, C.; MacKillop, J. Living in the here and now: interrelationships between impulsivity, mindfulness, and alcohol misuse. Psychopharmacology 2012, 219, 527-536. [CrossRef]
- Bowen, S.; Chawla, N.; Collins, S.E.; Witkiewitz, K.; Hsu, S., Grow, J., ; ... ; Marlatt, A. Mindfulness-based relapse prevention for substance use disorders: A pilot efficacy trial. Substance abuse 2009, 30, 295-305. [CrossRef]
- Mermelstein, L.C.; Garske, J.P. A Brief Mindfulness Intervention for College Student Binge Drinkers: A Pilot Study. Psychol Addict Behav 2015, 29, 259-269. [CrossRef]
- Çatak, P.D.; Ögel, K.F.t.t.v.t.s.K.P., 13, 85–91. Mindfulness based therapies and therapeutic processes. Clinical Psychiatry 2010, 85-91.
- Ögel, K.; Sarp, N.; Gürol, D.T.; Ermağan, E. Investigation of mindfulness and factors affecting mindfulness in addicted and non-addicted individuals. Anatolian Journal of Psychiatry Journal 2014, 15, 282-288.
- Tarhan, N.; Demirsoy, Ç.; Tutgun-Ünal, A. Measuring the Awareness Levels of Individuals with Alcohol and Substance Use Disorders: Tertiary Prevention Standards and Development of Uskudar Result Awareness and Harm Perception Scales. Brain Sci 2023, 13. [CrossRef]
- Dóra, T.B.; Szalkai, Z. The specifics of services of prevention in the case of addictions. In Proceedings of 9th international conference on management (ICM), Szent István University Gödöllő, Hungary pp. 276-283.
- Derin, G.; Okudan, M.; Aşıcıoğlu, F.; Ankara: Türkiye Klinikleri, -. Family risk factors in alcohol and substance use disorders; Turkey Clinics: Ankara, Turkey, 2021.
- Cai, W.Q.; Wang, Y.J. Family Support and Hope among People with Substance Use Disorder in China: A Moderated Mediation Model. Int J Env Res Pub He 2022, 19. [CrossRef]
- Küçükerdönmez, Ö.; Urhan, M.; Köksal, E.B.v.D.D., 46(2), 147-156. Relationship between appetite, nutritional status and quality of life in individuals with alcohol and substance dependence. Journal of Nutrition and Diet 2018, 46, 147-156. [CrossRef]
- Asan, Ö.; Tıkır, B.; Okay, İ.T.; Göka, E. Sociodemographic and clinical features of patients with alcohol and substance use disorders in a specialized Unit. Journal of Dependence 2015, 16, 1-8.
- Arıkan, Z.; Yasin Genç, D.Ç.E.; Aslan, S.; Parlak, P.İ. Stigmatization of the patients and their relatives in alcohol and other substance dependencies. Journal of Dependence 2004, 52-56.
- Akbaş, G.E.; Mutlu, E. Addiction and treatment experiences of people undergoing substance abuse treatment. Community and Social Work 2016, 27, 101-122.
- Witkiewitz, K.; Greenfield, B.L.; Bowen, S. Mindfulness-based relapse prevention with racial and ethnic minority women. Addictive Behaviors 2013, 38, 2821-2824. [CrossRef]
- Saatçioğlu, Ö.; Evren, E.C.; Çakmak, D. Evaluation of cases with alcohol and substance abuse who were hospitalised between 1998-2002. Journal of Addiction 2003, 109-117.
- Yılmaz, A.; Can, Y.; Bozkurt, M.; Evren, C. Remission and relapse in alcohol and substance addiction. Current Approaches in Psychiatry 2014, 6, 243-256. [CrossRef]
- Evren, C.; Durkaya, M.; Dalbudak, E.; Çelik, S.; Çetin, R.; Çakmak, D. Factors associated with relapse in male alcohol abusers: A 12-month follow-up study. Düşünen Adam Journal of Psychiatry and Neurological Sciences 2010, 92-99.
- Gordon, A.J.; Zrull, M. Social Networks and Recovery - One Year after Inpatient Treatment. J Subst Abuse Treat 1991, 8, 143-152, doi:Doi 10.1016/0740-5472(91)90005-U.
- Walton, M.A.; Castro, F.G.; Barrington, E.H. The role of attributions in abstinence, lapse, and relapse following substance abuse treatment. Addict Behav. 1994, 19, 319-331.
- Irvin, J.E.; Bowers, C.A.; Dunn, M.E.; Wang, M.C. Efficacy of relapse prevention: A meta-analytic review. J Consult Clin Psych 1999, 67, 563-570, doi:Doi 10.1037/0022-006x.67.4.563.
- Tarhan, N. Positive psychology and psychotherapy in addiction. In Addiction diagnosis and treatment basic book, Dilbaz, N., Göğcegöz, I., Noyan, C.O., Kazan Kızılkurt, Ö., Eds. Nobel Medical Bookstores: Turkey, 2021; p. 419.
- Seligman, M.E.; Peterson, C. Positive clinical psychology. In A psychology of human strengths: Fundamental questions and future directions for a positive psychology Aspinwall, L.G., Staudinger, U.M., Eds. American Psychological Association: 2003; pp. 305–317.
- Donaldson, S.I.; Dollwet, M.; Rao, M.A. Happiness, excellence, and optimal human functioning revisited: Examining the peer-reviewed literature linked to positive psychology. J Posit Psychol 2015, 10, 185-195. [CrossRef]
- Kern, M.L.; Williams, P.; Spong, C.; Colla, R.; Sharma, K.; Downie, A.; Taylor, J.A.; Sharp, S.; Siokou, C.; Oades, L.G. Systems informed positive psychology. J Posit Psychol 2020, 15, 705-715. [CrossRef]
- Seligman, M.E. Positive psychology: A personal history. Annual review of clinical psychology 2019, 15, 1-23.
- Seligman, M.E. Flourish: A visionary new understanding of happiness and well-being; Simon and Schuster: 2011.
- Carreno, D.F.; Pérez-Escobar, J.A. Addiction in existential positive psychology (EPP, PP2.0): from a critique of the brain disease model towards a meaning-centered approach. Couns Psychol Q 2019, 32, 415-435. [CrossRef]
- Karasar, N. Scientific research method: concepts, principles, techniques; Nobel Publishing: Turkey, 2016.
- Groeneveld, R.A.; Meeden, G. Measuring Skewness and Kurtosis. The Statistician 1984, 33, 391-399.
- Hopkins, K.D.; Weeks, D.L. Tests for normality and measures of skewness and kurtosis: Their place in research reporting. Educational and Psychological Measurement 1990, 50, 717-729.
- Moors, J.J.A. The Meaning of Kurtosis - Darlington Reexamined. Am Stat 1986, 40, 283-284, doi:Doi 10.2307/2684603.
- Tarter, R.E.; Cochran, G.; Reynolds, M. Prevention of opioid addiction. Commonwealth 2018, 20.
- Vanyukov, M.M.; Kirisci, L.; Moss, L.; Tarter, R.E.; Reynolds, M.D.; Maher, B.S.; ...; Clark, D.B. Measurement of the risk for substance use disorders: phenotypic and genetic analysis of an index of common liability. Behavior genetics 2009, 39, 233-244.
- Kirisci, L.; Tarter, R.; Mezzich, A.; Ridenour, T.; Reynolds, M.; Vanyukov, M. Prediction of Cannabis Use Disorder between Boyhood and Young Adulthood: Clarifying the Phenotype and Environtype. Am J Addiction 2009, 18, 36-47. [CrossRef]
- Kirisci, L.; Tarter, R.E. Psychometric validation of a multidimensional schema of substance use topology: Discrimination of high and low risk youth and prediction of substance use disorder. J Child Adoles Subst 2001, 10, 23-33. [CrossRef]
Figure 1.
USRAS and USHPS Pre-Test and Post-Test Scores of the Groups (Cut-off point 2.5 was accepted as the median value).
Figure 1.
USRAS and USHPS Pre-Test and Post-Test Scores of the Groups (Cut-off point 2.5 was accepted as the median value).
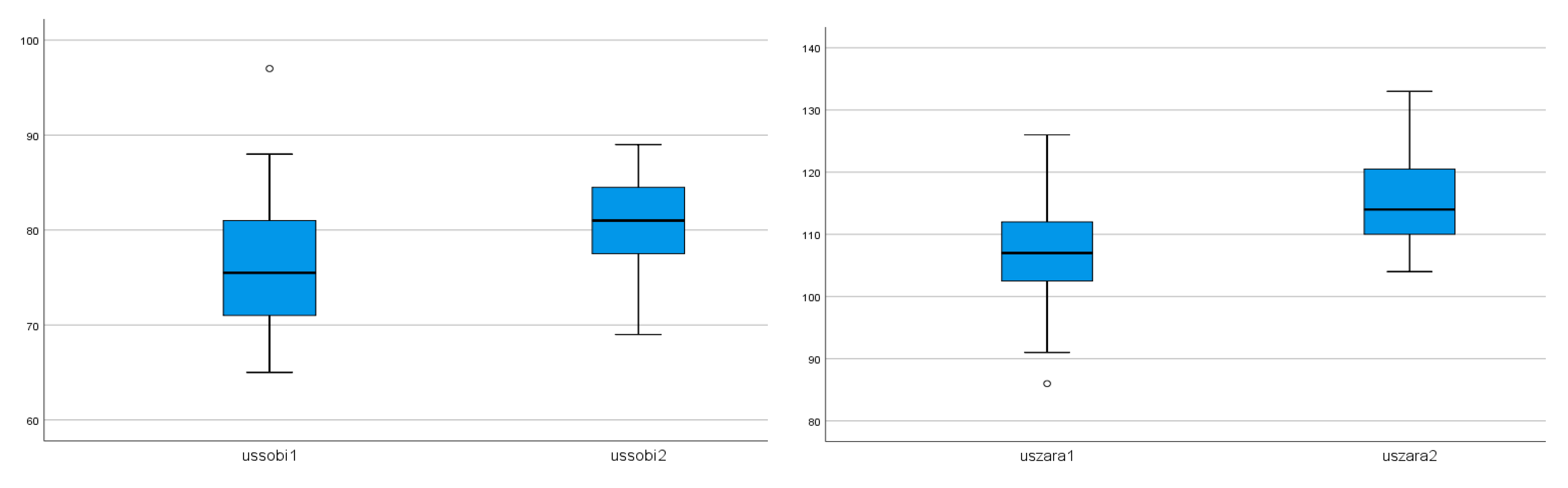
Table 2.
Average USRAS and USHPS Scores of Groups.
| Groups | USRAS1 | Sd1 | USRAS2 | Sd2 | USHPS1 | Sd1 | USHPS2 | Sd2 |
| G1: Substance Use Disorder and/or Alcohol Use Disorder (n=30) |
75,70 | 6,60 | 79,86 | 5,20 | 107,00 | 8,36 | 116,30 | 6,33 |
| G2: Substance Use Disorder and Mood Disorder (n=14) | 76,50 | 7,14 | 82,28 | 4,44 | 107,57 | 8,26 | 113,35 | 7,01 |
| Male (n=35) | 75,68 | 6,70 | 80,14 | 5,26 | 107,22 | 8,67 | 116,22 | 6,90 |
| Female (n=9) | 77,00 | 7,01 | 82,55 | 3,77 | 107,00 | 6,72 | 112,00 | 4,12 |
| Total (n=44) | 75,95 | 6,70 | 80,63 | 5,05 | 107,18 | 8,24 | 115,36 | 6,61 |
Table 3.
One Group T-Test Results by Groups.
| Groups* | X | Sd | t | df | p |
| Group1 USRAS1 (n=30) | 75,70 | 6,60 | 62,74 | 29 | ,00a |
| Group1 USRAS2 (n=30) | 79,86 | 5,20 | 84,05 | 29 | |
| Group1 USHPS1 (n=30) | 107,00 | 8,36 | 70,04 | 29 | ,00b |
| Group1 USHPS2 (n=30) | 116,30 | 6,33 | 100,61 | 29 | |
| Group2 USRAS1 (n=14) | 76,50 | 7,14 | 40,06 | 13 | ,00c |
| Group2 USRAS2 (n=14) | 82,28 | 4,44 | 69,26 | 13 | |
| Group2 USHPS1 (n=14) | 107,57 | 8,26 | 48,71 | 13 | ,00d |
| Group2 USHPS2 (n=14) | 113,35 | 7,01 | 60,48 | 13 |
The range is between 1-5. *Group1: Substance Use Disorder and/or Alcohol Use Disorder & Group2: Substance Use Disorder and Mood Disorder. aReference Group1 was calculated as USRAS1-2. bReference group1 was calculated as USHPS1-2. cReference group2 was calculated as USRAS1-2. dReference group2 was calculated as USHPS1-2.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



